skeletal muscle relaxants
DESCRIPTION
TRANSCRIPT
SKELETAL MUSCLE RELAXANTS -1
Speaker : Dr Rachana Menon
Learning Objective
Introduction
History
Physiology of Neuromuscular Junction
Acetylcholine – Synthesis ,Storage , Release
Nicotinic Receptor
Classification of SMR
Depolarizing agents
Directly acting agents
Drugs that act peripherally at neuromuscular junction or
muscle fibre itself or in cerebrospinal axis to reduce
muscle tone and cause muscle paralysis.
INTRODUCTION
HISTORY
The earliest known use of muscle relaxant drugs dates
back to the 16th century.
Natives of the Amazon Basin in South America . The
prey was shot by arrows dipped in curare
Curare, led to some of the earliest scientific studies
in pharmacology.
HISTORY
1935 – d tubocurarine, active
ingredient - Harold King of London,
working in Sir Henry Dale’s laboratory
1943, neuromuscular blocking drugs
became established as muscle
relaxants in the practice of
anaesthesia and surgery
HISTORY
Contd..
1967- Baird and Reid first reported on clinical
administration of the synthetic aminosteroid
pancuronium
1980-Introduction of vecuronium, an aminosteroid, and
atracurium.
• 1990’s Mivacurium, the first short-acting
nondepolarizing neuromuscular blocker was introduced
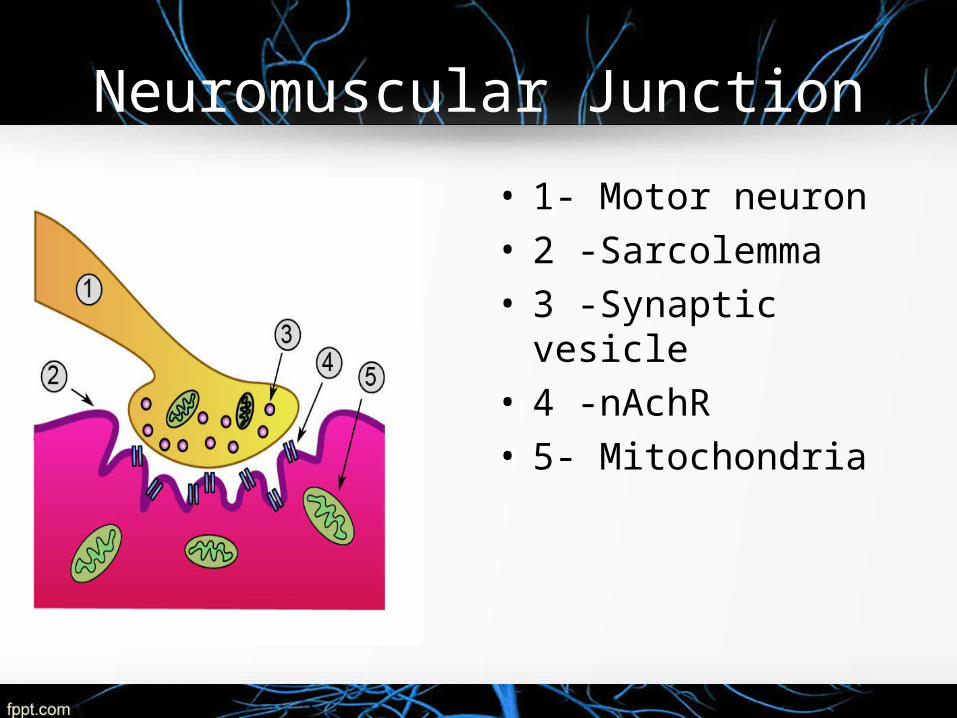
Neuromuscular Junction
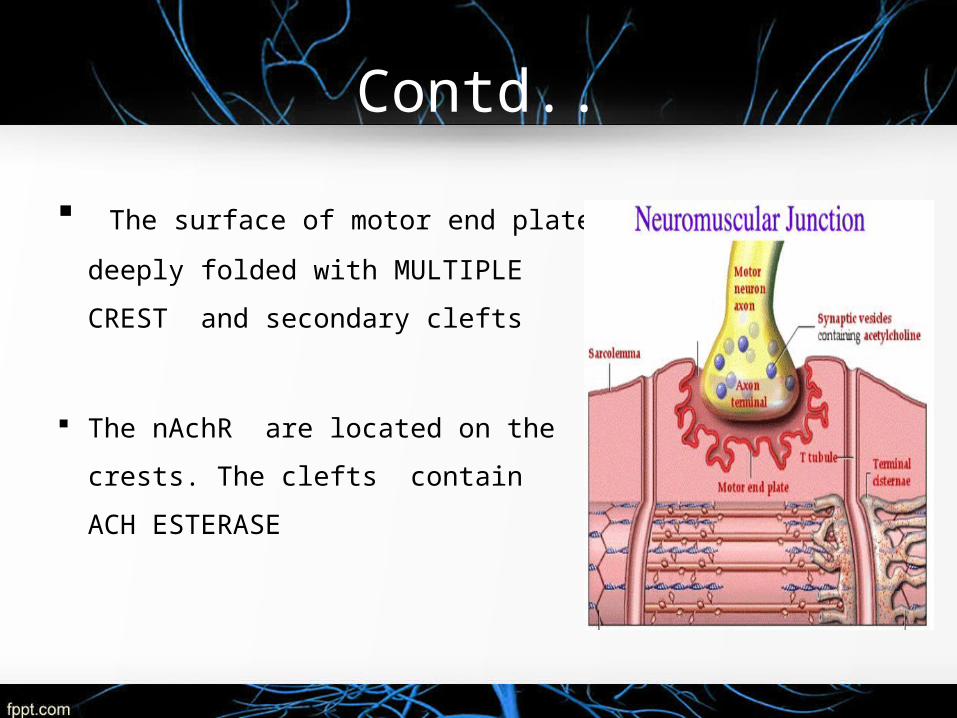
• 1- Motor neuron• 2 -Sarcolemma• 3 -Synaptic vesicle• 4 -nAchR• 5- Mitochondria
NNEUROMUSCULAR JUNCTION
The neuromuscular junction is made up of a
Motor neuron – Originate in the ventral horn of the
spinal cord.
As the axon of a motor neurone enters the structure of
skeletal muscle it forms many branches “Axon
terminals".
Synaptic end bulb – Bulbous swelling at the end of
axon terminal.
Contd..
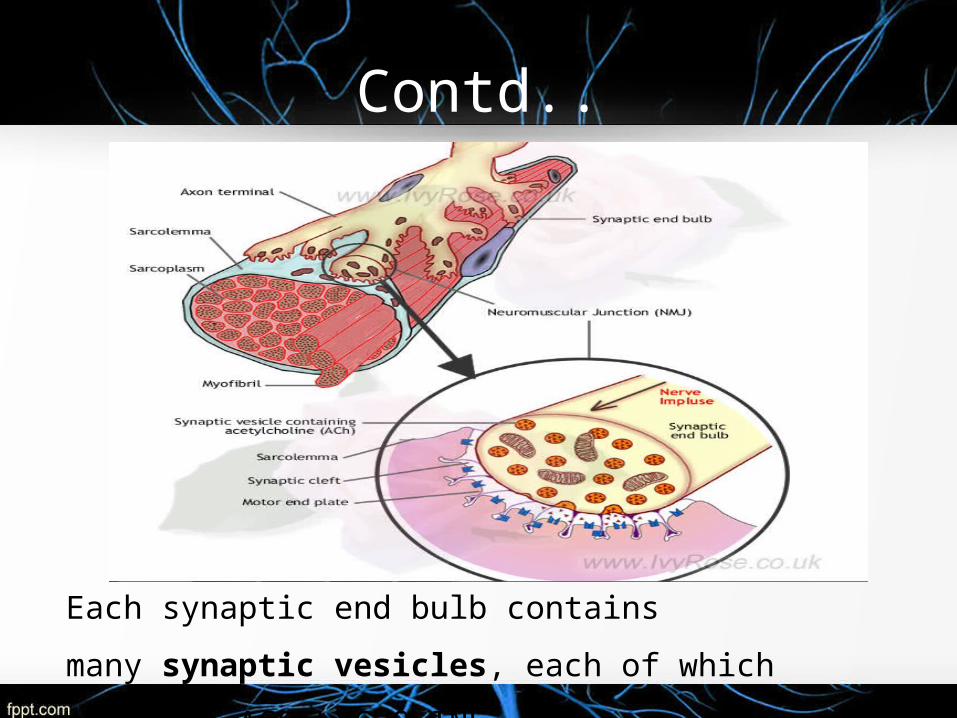
Each synaptic end bulb contains many synaptic
vesicles, each of which contains ACETLYCHOLINE.
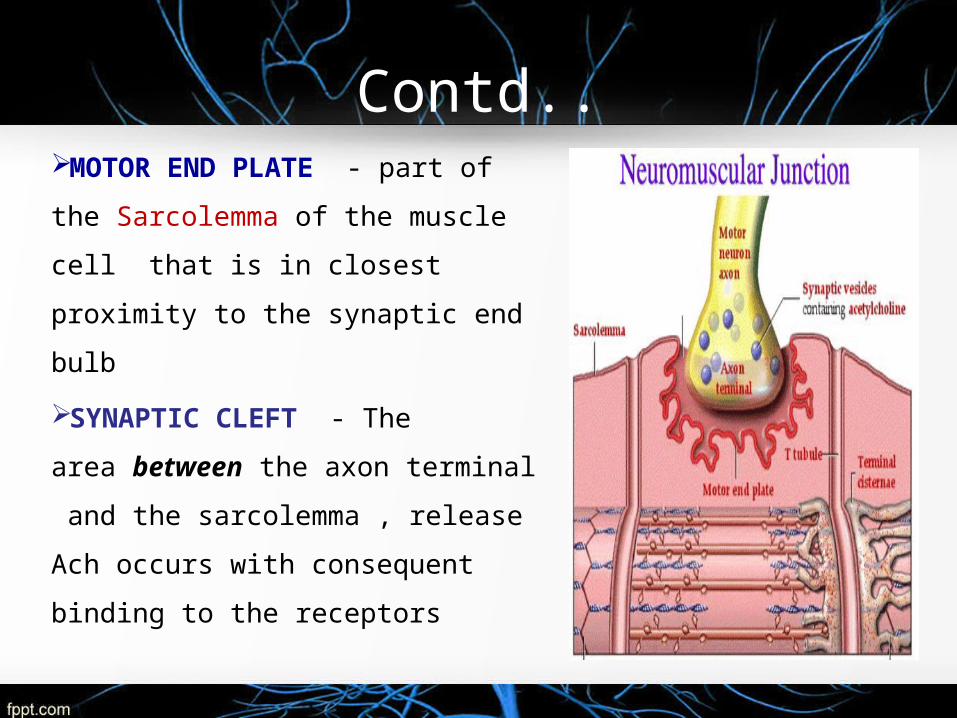
Contd..MOTOR END PLATE - part of
the Sarcolemma of the muscle cell
that is in closest proximity to the
synaptic end bulb
SYNAPTIC CLEFT - The
area between the axon terminal
and the sarcolemma , release Ach
occurs with consequent binding to
the receptors
Contd..
The surface of motor end plate
deeply folded with MULTIPLE
CREST and secondary clefts
The nAchR are located on the
crests. The clefts contain ACH
ESTERASE

ACETYLCHOLINESTERASE
Acetylcholinesterase ACh
Choline Acetate
Produced on the ribosomes of the motor neuron
Attached - thin collagen threads linking it to the basement
membrane
Found junctional gap clefts of the post-synaptic folds in
high concentrations
Acetylcholinesterase
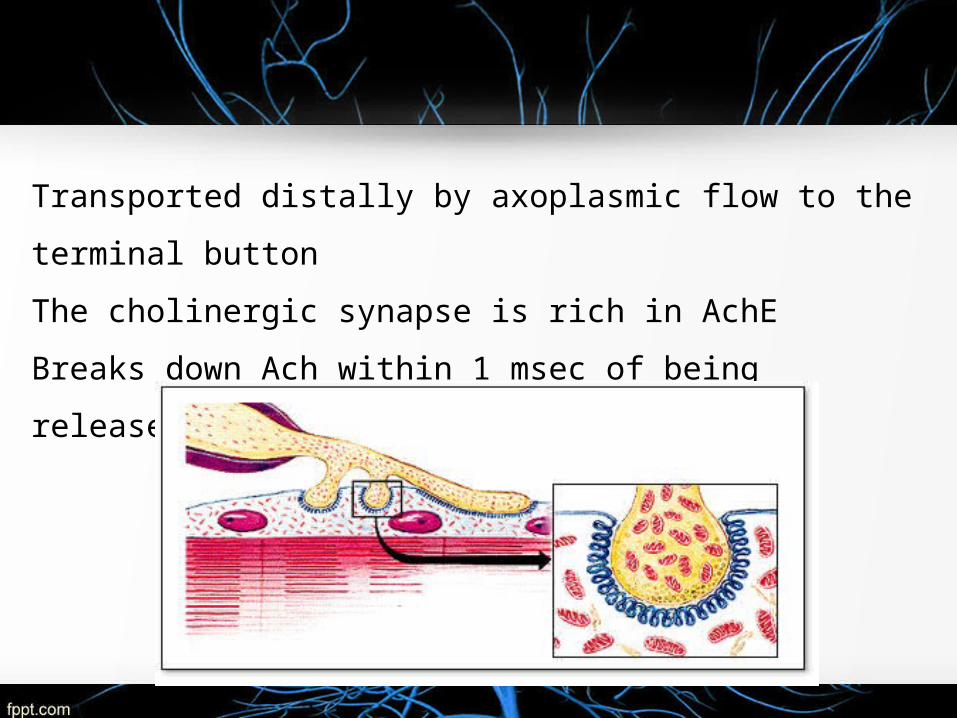
Transported distally by axoplasmic flow to the terminal button
The cholinergic synapse is rich in AchE
Breaks down Ach within 1 msec of being released.

SKELETAL MUSCLE RELAXANTS -1 ACETYLCHOLINE
SYNTHESIS STORAGE RELEASE
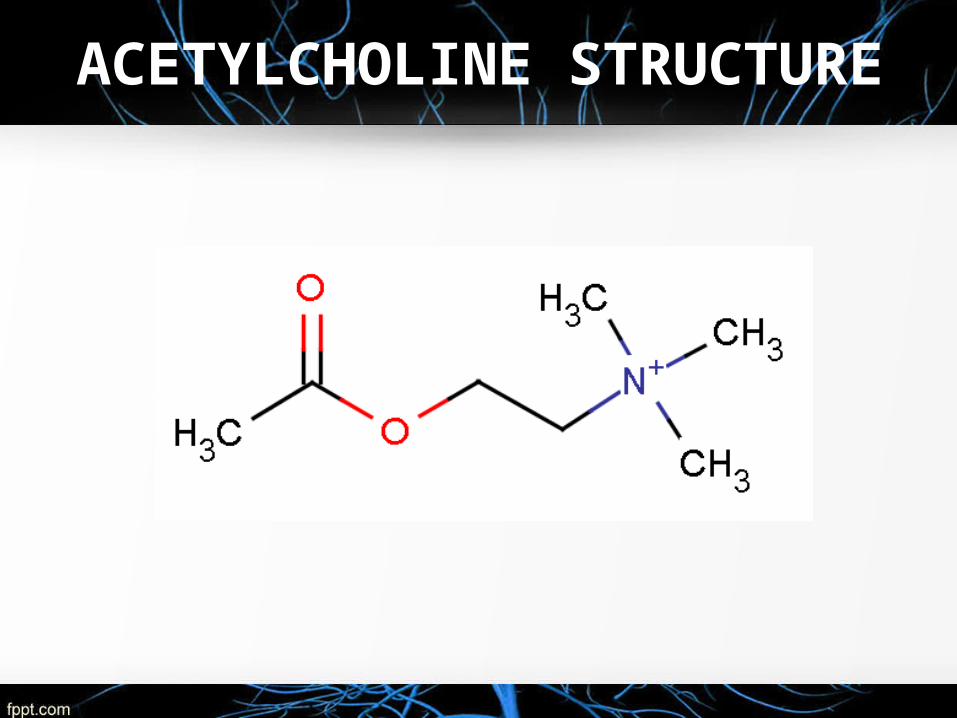
ACETYLCHOLINE STRUCTURE
SYNTHESIS
Acetic acid ester of choline
Synthesised inside the cholinergic nerve fibre
Choline
Acetyl-coenzyme A
Choline acetyltransferase-
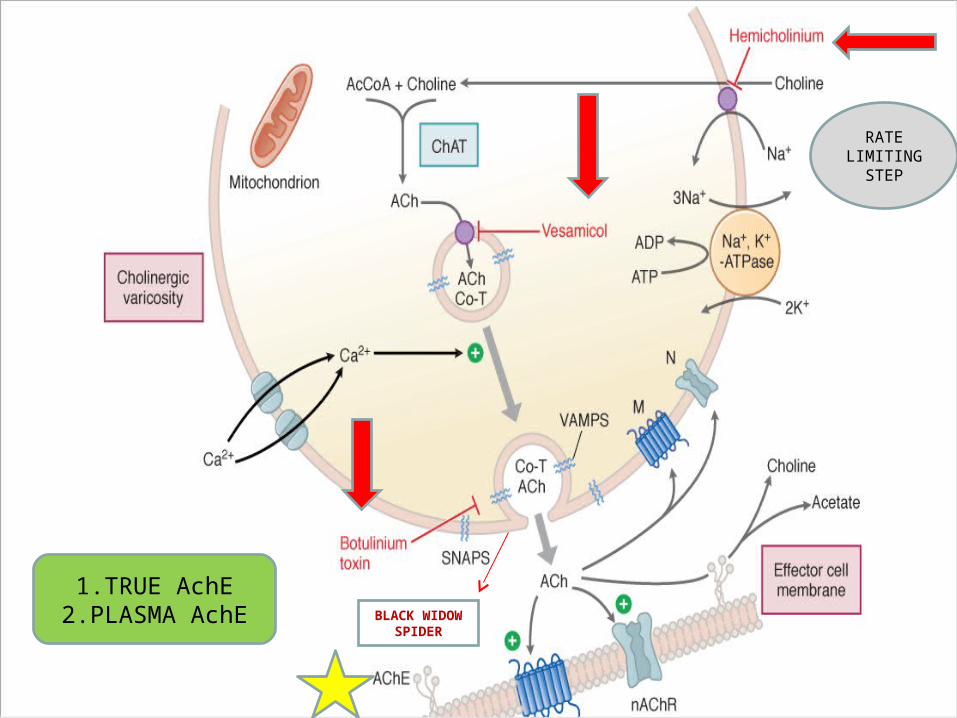
1.TRUE AchE2.PLASMA AchE BLACK WIDOW
SPIDER
RATE LIMITING
STEP
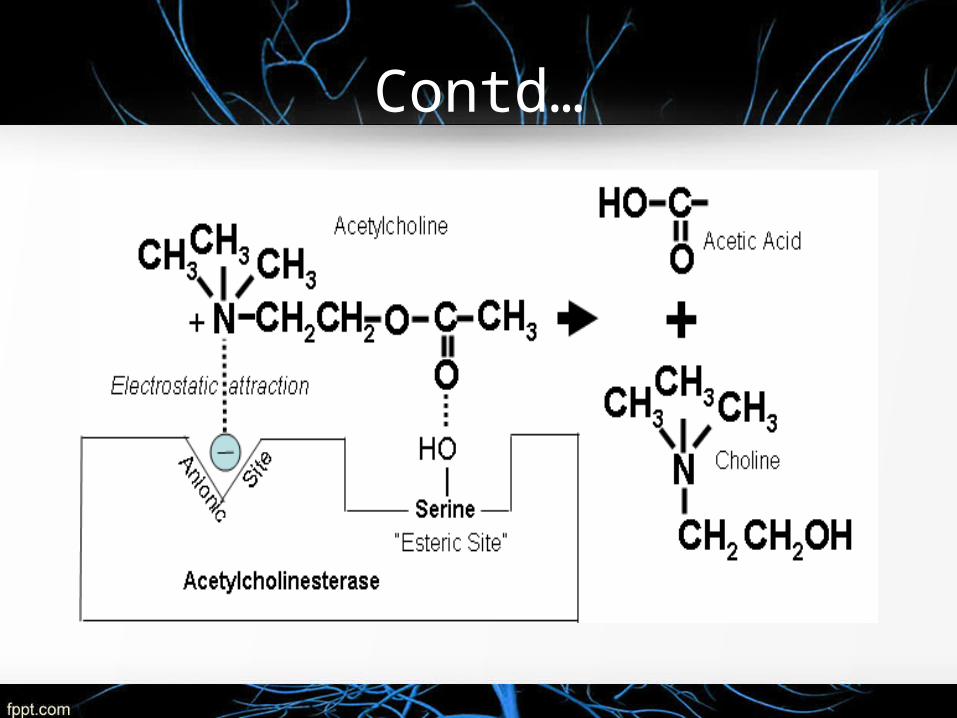
Contd…
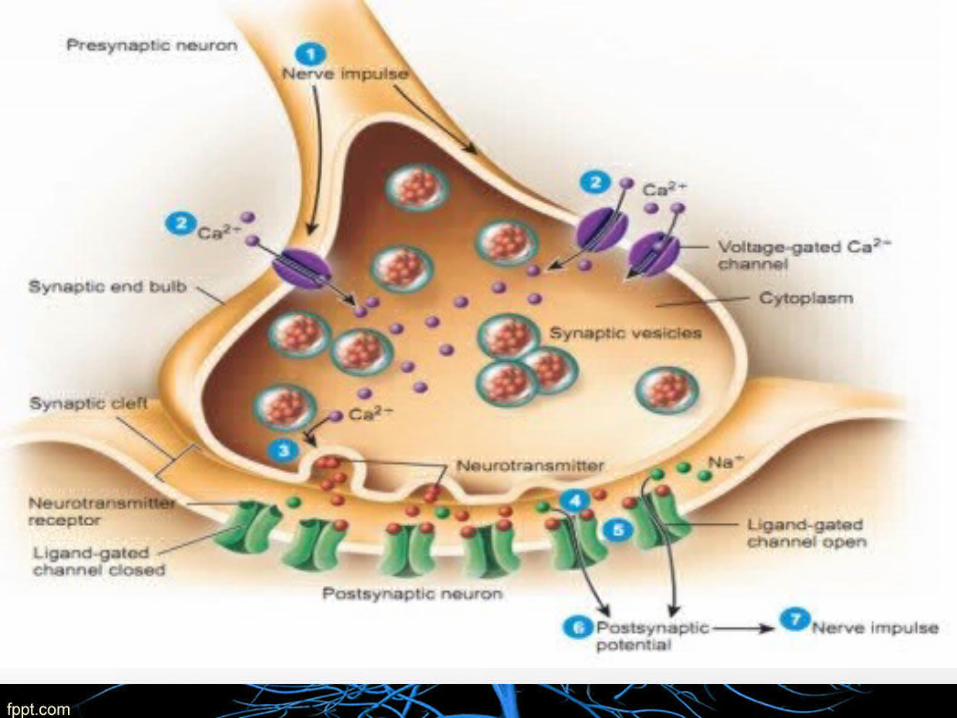
The events that translate an Action Potential, (a membrane-electrical event) into a mechanical event (contraction)

ACETYLCHOLINE RECEPTORS
NICOTINIC RECEPTOR
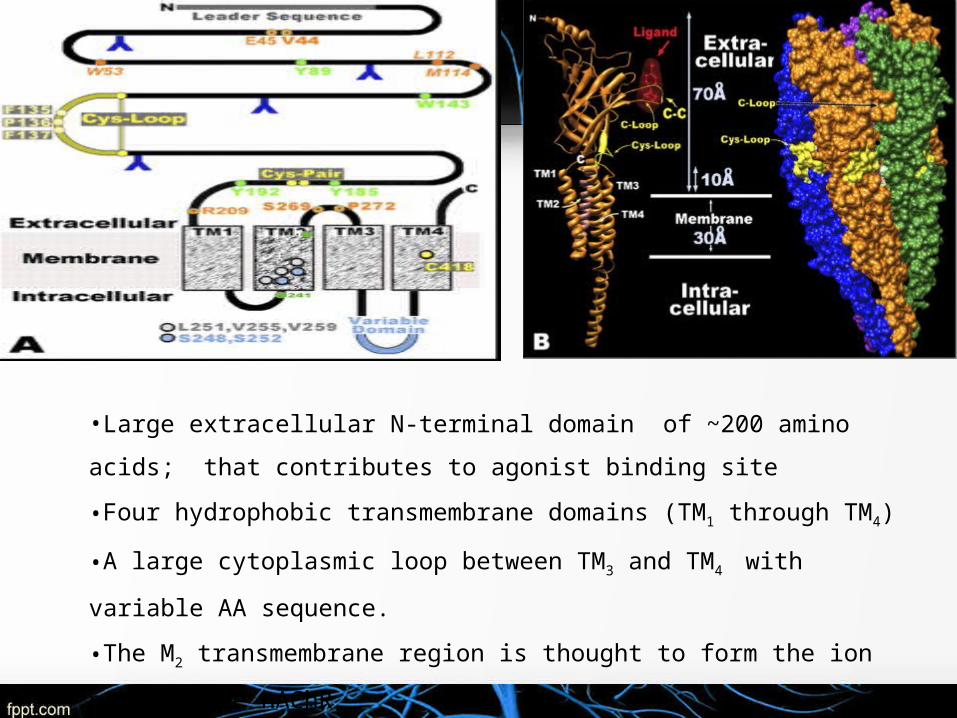
•Large extracellular N-terminal domain of ~200 amino acids; that contributes
to agonist binding site
•Four hydrophobic transmembrane domains (TM1 through TM4)
•A large cytoplasmic loop between TM3 and TM4 with variable AA sequence.
•The M2 transmembrane region is thought to form the ion pore of the nAChR
• Short extracellular C terminus
(Cys-loop) defined by two cysteines (Cys) that in the
mammalian subunits are separated by 13 intervening amino
acids.
Subunits are classified into α- and non-α subunits based
on the presence of a Cys-Cys pair near the entrance to TM1.
Cys-Cys pair
• Required for agonist binding
• Presence designates the subunit as an α-subtype .
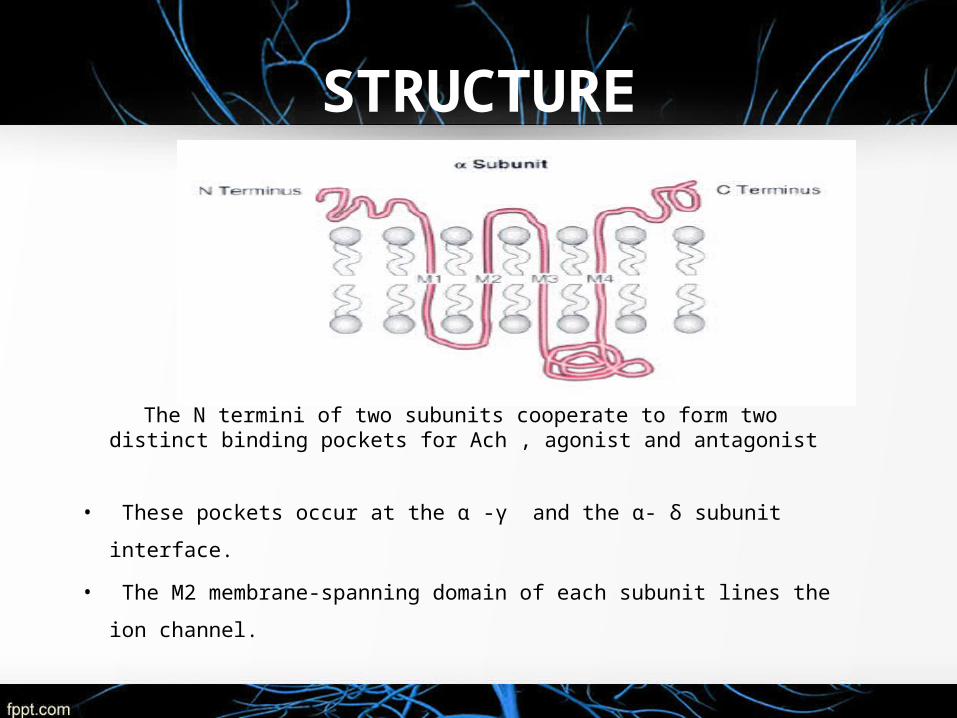
STRUCTURE
The N termini of two subunits cooperate to form two distinct binding pockets for Ach , agonist and antagonist
• These pockets occur at the α -γ and the α- δ subunit interface.
• The M2 membrane-spanning domain of each subunit lines the ion
channel.
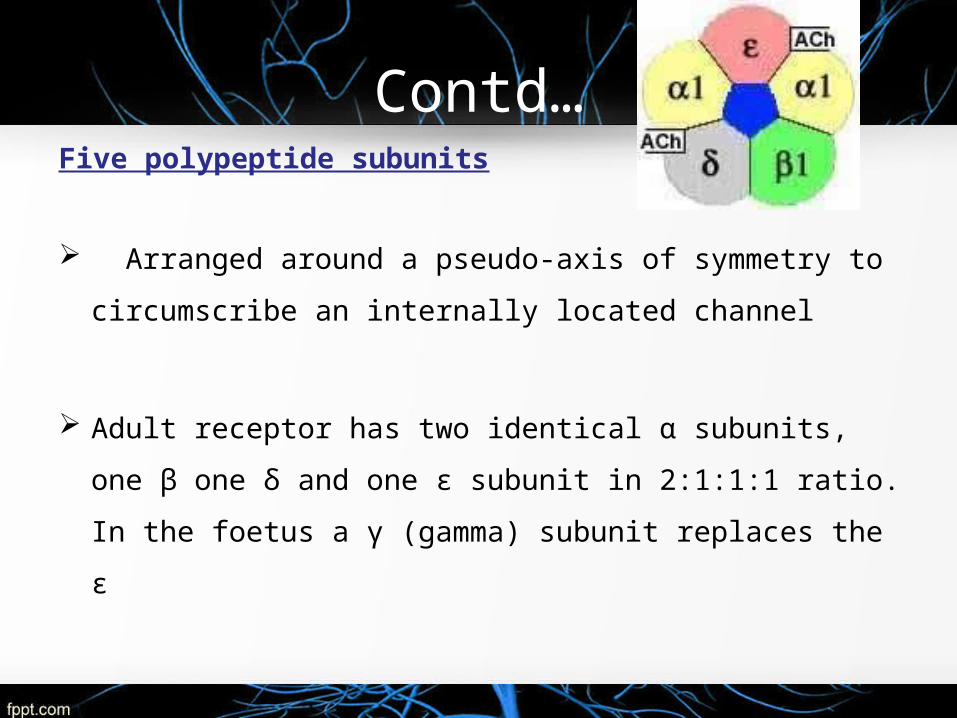
Contd…Five polypeptide subunits
Arranged around a pseudo-axis of symmetry to
circumscribe an internally located channel
Adult receptor has two identical α subunits, one β one δ
and one ε subunit in 2:1:1:1 ratio. In the foetus a γ
(gamma) subunit replaces the ε
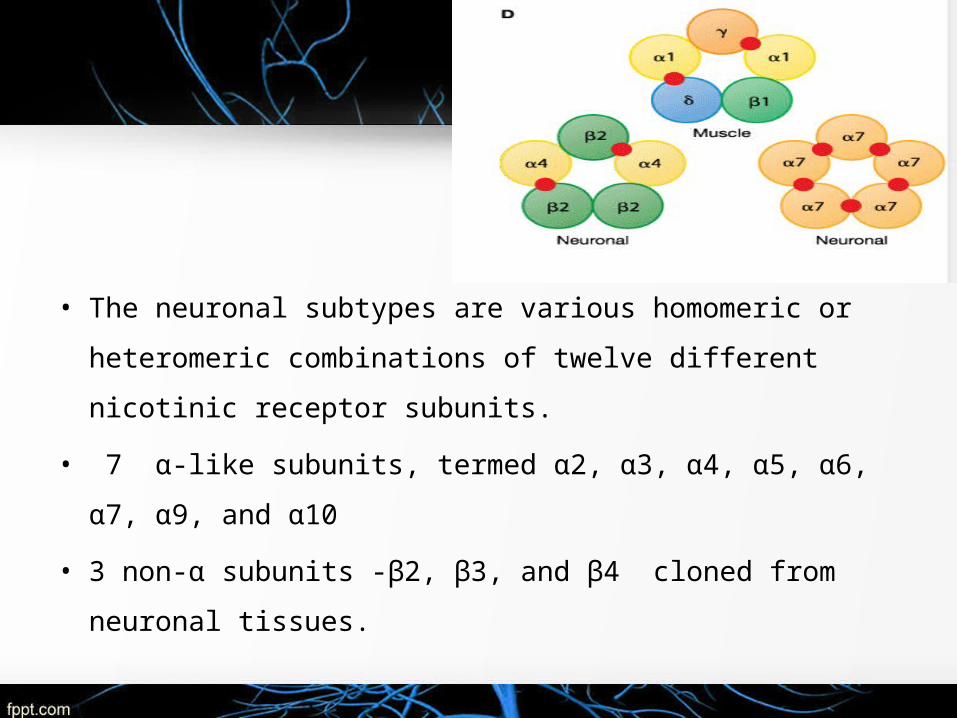
• The neuronal subtypes are various homomeric or heteromeric
combinations of twelve different nicotinic receptor subunits.
• 7 α-like subunits, termed α2, α3, α4, α5, α6, α7, α9, and α10
• 3 non-α subunits -β2, β3, and β4 cloned from neuronal
tissues.
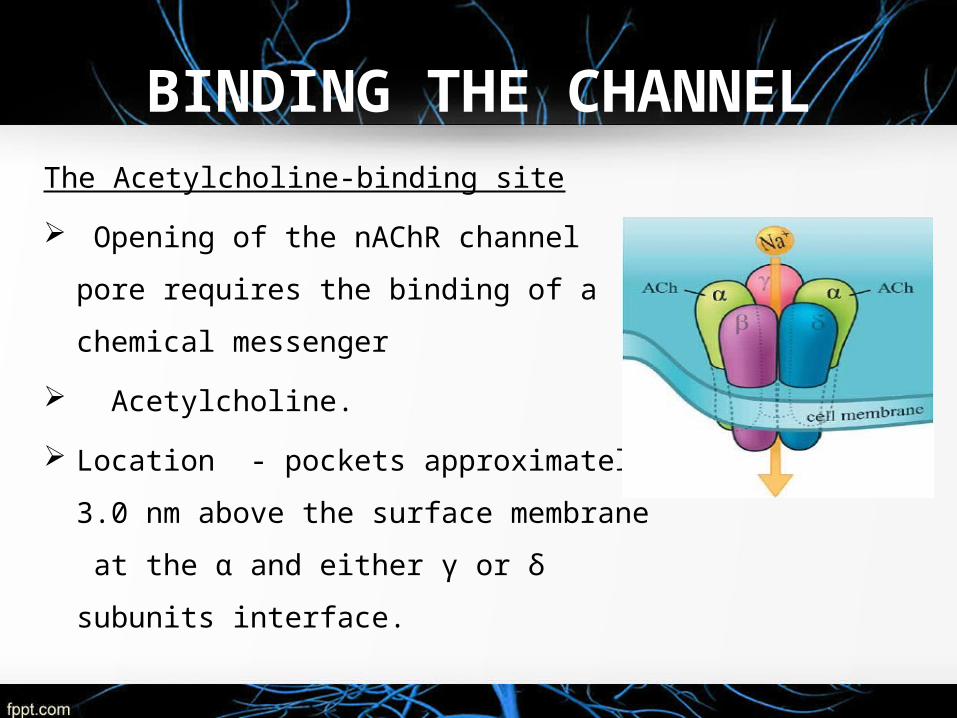
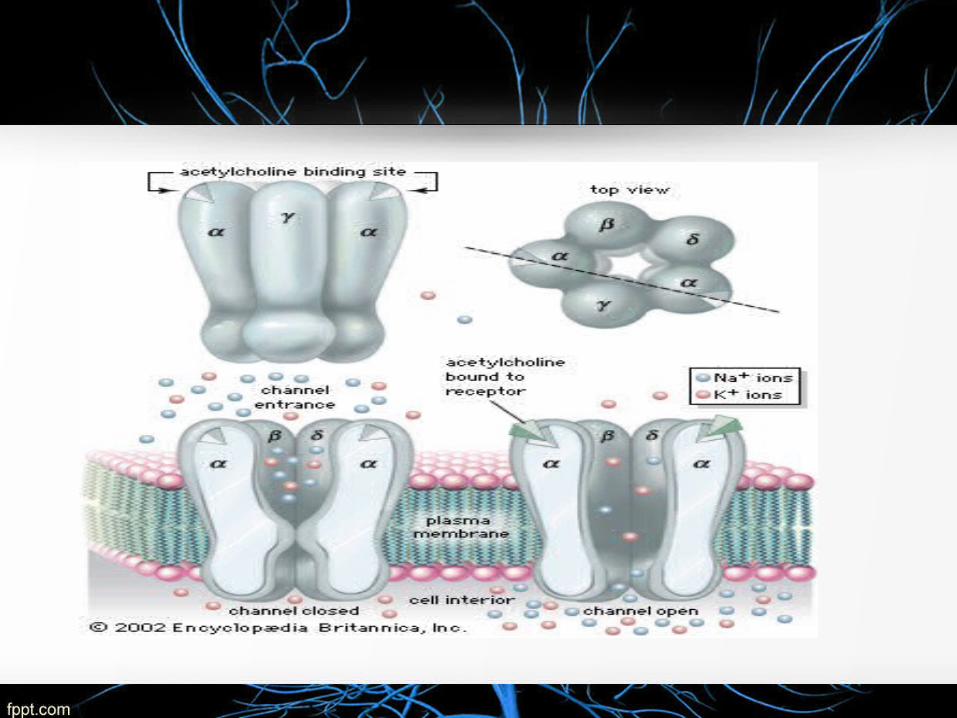
BINDING THE CHANNELThe Acetylcholine-binding site
Opening of the nAChR channel pore
requires the binding of a chemical
messenger
Acetylcholine.
Location - pockets approximately 3.0
nm above the surface membrane at the
α and either γ or δ subunits interface.
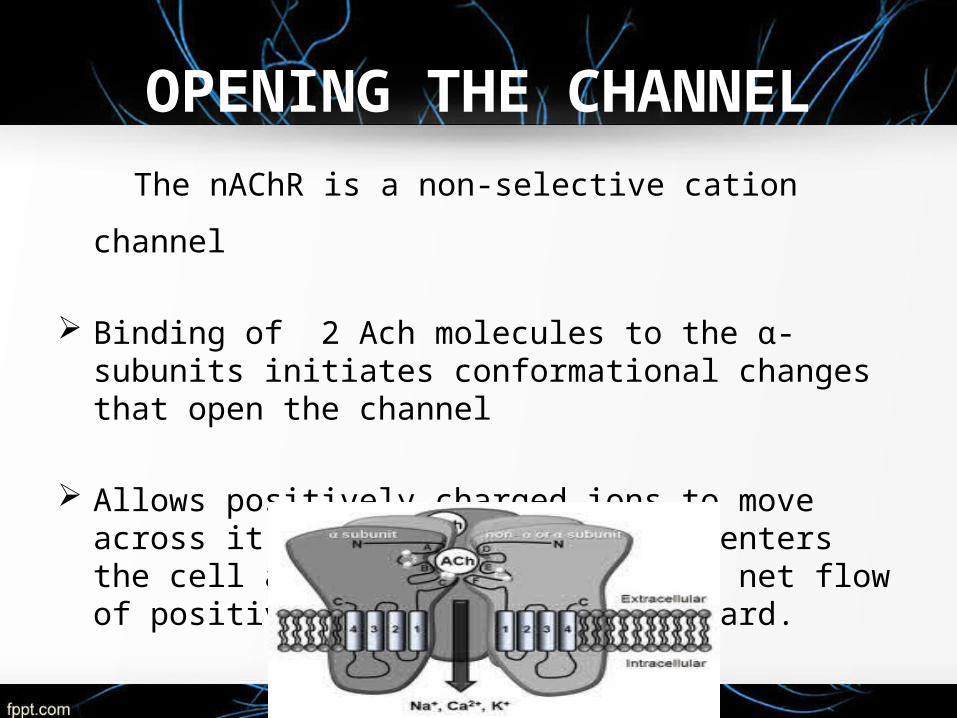
OPENING THE CHANNEL
The nAChR is a non-selective cation channel
Binding of 2 Ach molecules to the α-subunits initiates conformational changes that open the channel
Allows positively charged ions to move across it; in
particular, sodium enters the cell and potassium exits. The net flow of positively-charged ions is inward.
The cell becomes less negative compared with the
extracellular surroundings.
When a threshold of –50mV is achieved (from a resting
potential of –80mV), voltage- gated Na open, thereby
increasing the rate of depolarisation and resulting in an
End plate potential (EPP) of 50-100mV.
Triggers the muscle action potential
Muscle contraction
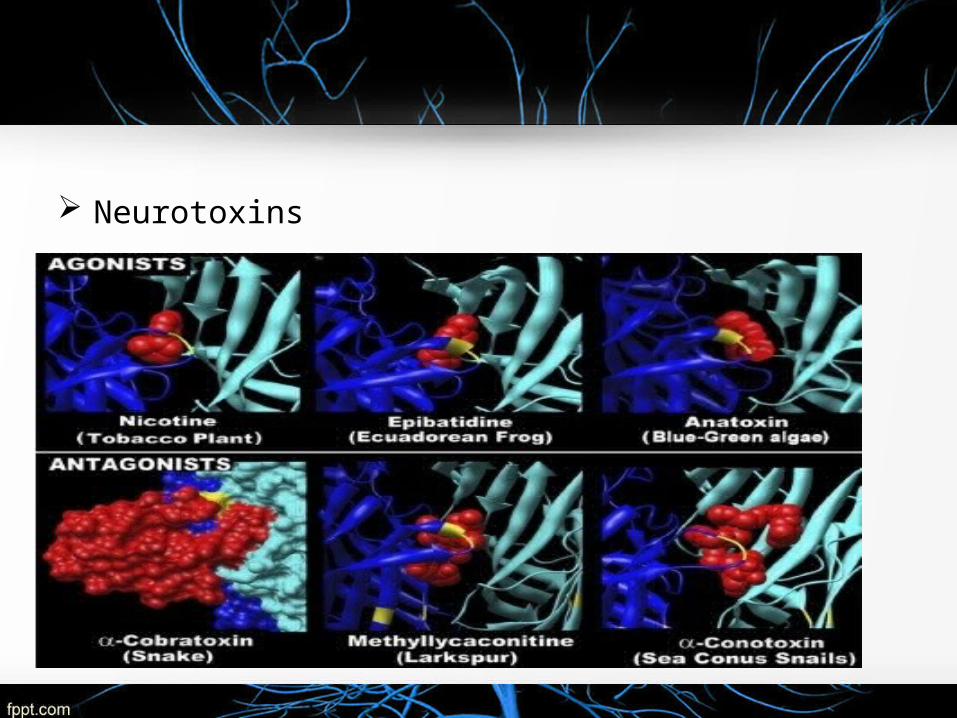
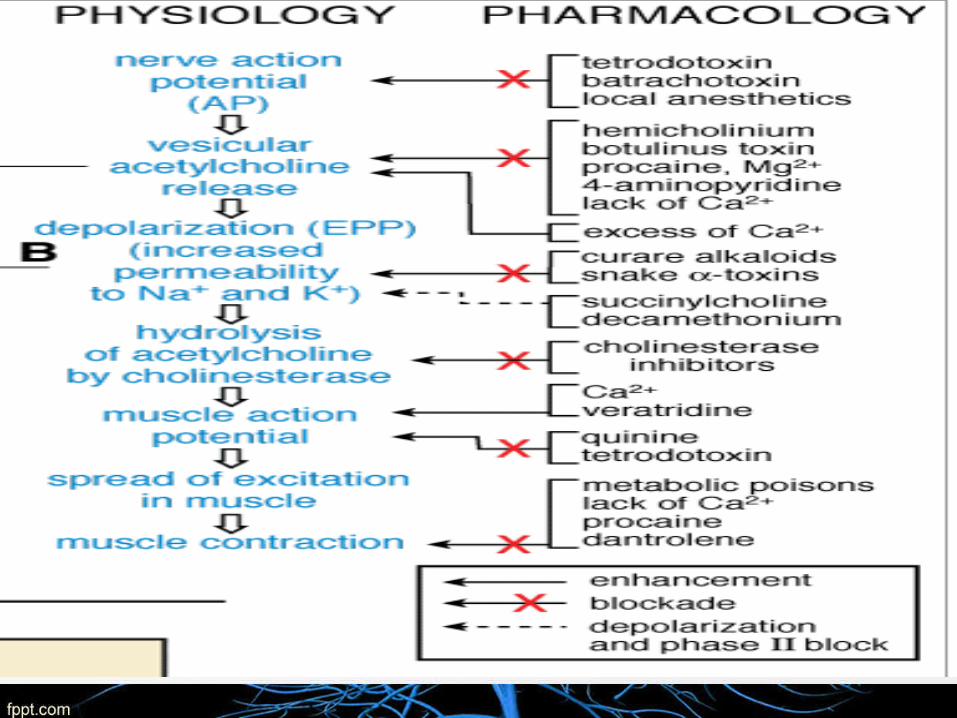
Neurotoxins
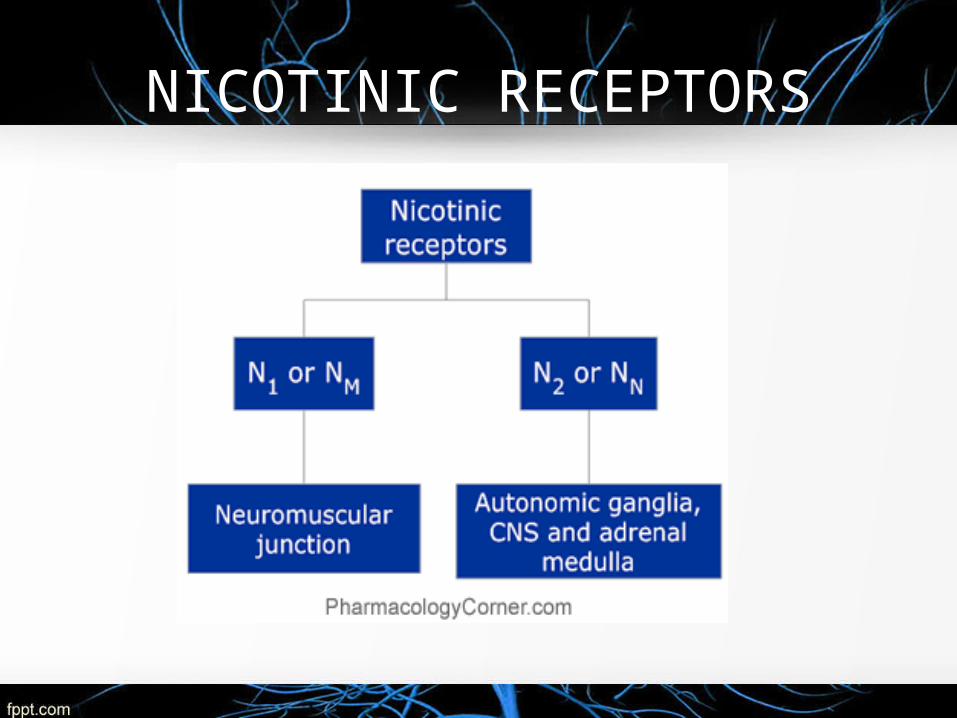
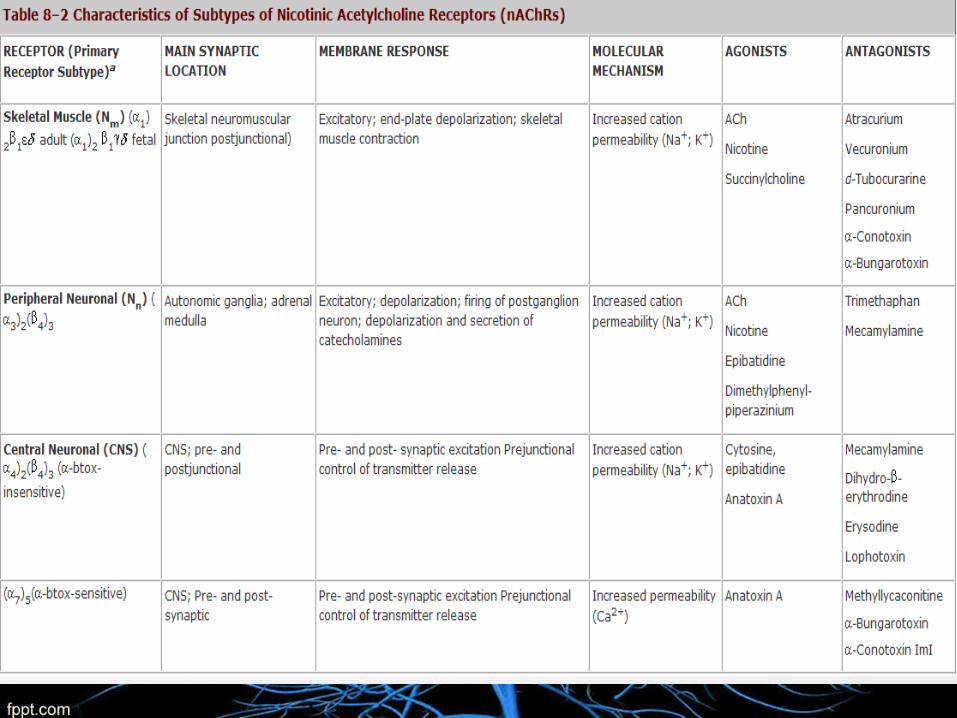
NICOTINIC RECEPTORS

SKELETAL MUSCLE RELAXANTS
PERIHERALLY ACTING CENTRALLY ACTING
SMR - Why Required ?
1. In conjunction with GA
2. Painful muscle conditions
3. Spastic neurological conditions
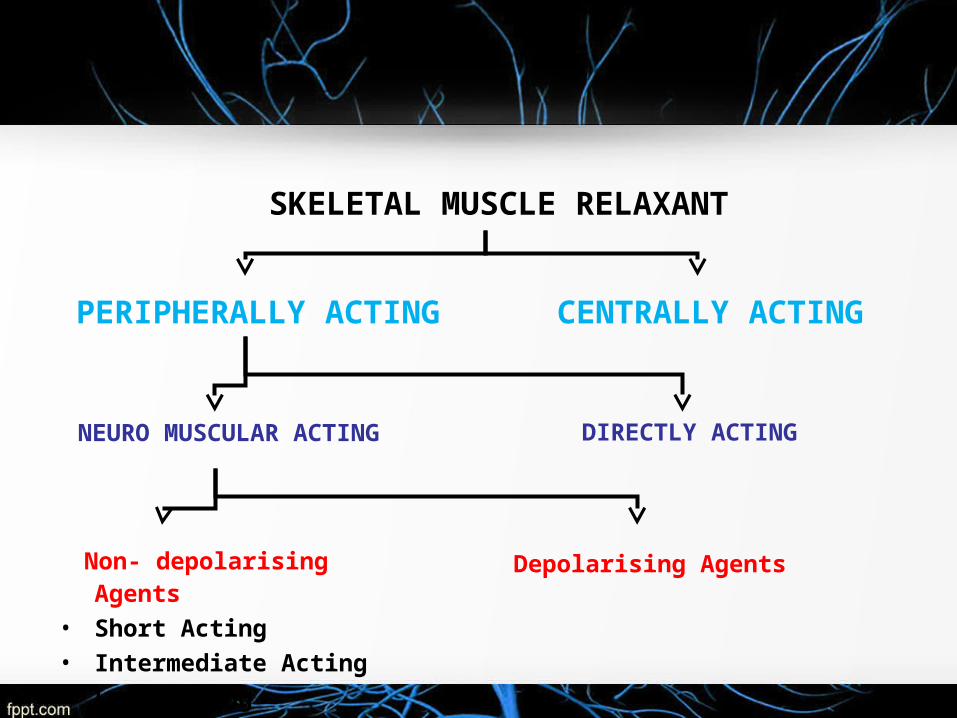
SKELETAL MUSCLE RELAXANT
PERIPHERALLY ACTING CENTRALLY ACTING
NEURO MUSCULAR ACTING DIRECTLY ACTING
Non- depolarising Agents
• Short Acting
• Intermediate Acting
• Long acting
Depolarising Agents
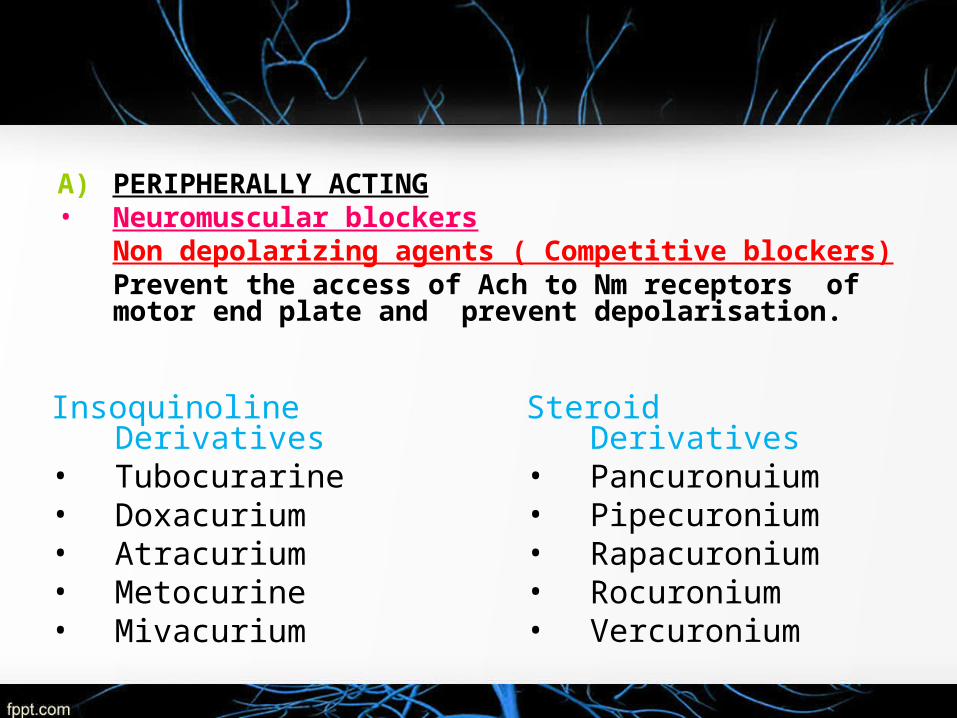
A) PERIPHERALLY ACTING• Neuromuscular blockers
Non depolarizing agents ( Competitive blockers)Prevent the access of Ach to Nm receptors of motor end plate and prevent depolarisation.
Insoquinoline Derivatives• Tubocurarine• Doxacurium• Atracurium• Metocurine• Mivacurium
Steroid Derivatives• Pancuronuium• Pipecuronium• Rapacuronium• Rocuronium• Vercuronium

Depolarizing agents
• Produce excessive depolarisation which persist for longer duration at NMJ
• Resistant to hydrolysis by true AchE present in synaptic cleft
– Suxamethonium (Succinylcholine)– Decamethonium
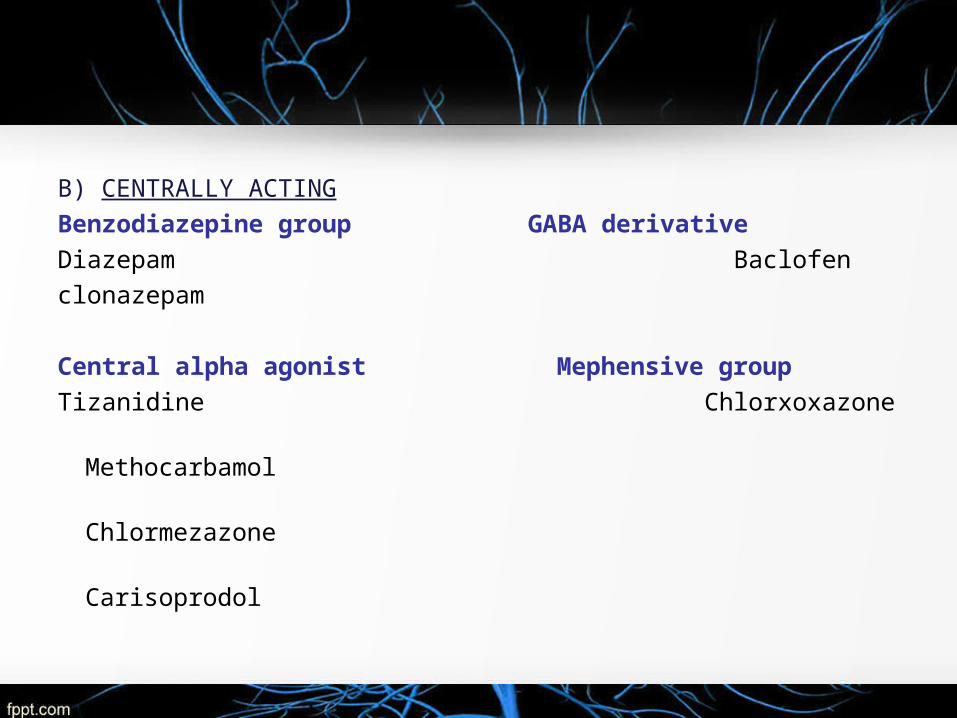
B) CENTRALLY ACTING
Benzodiazepine group GABA derivative
Diazepam Baclofen
clonazepam
Central alpha agonist Mephensive group
Tizanidine Chlorxoxazone
Methocarbamol
Chlormezazone
Carisoprodol
DEPOLARISING AGENTS
SUCCINYL CHOLINE
Also known as suxamethonium
Introduced by Thesleff and by Foldes and colleagues in 1952
Is a nicotinic acetylcholine receptor agonist
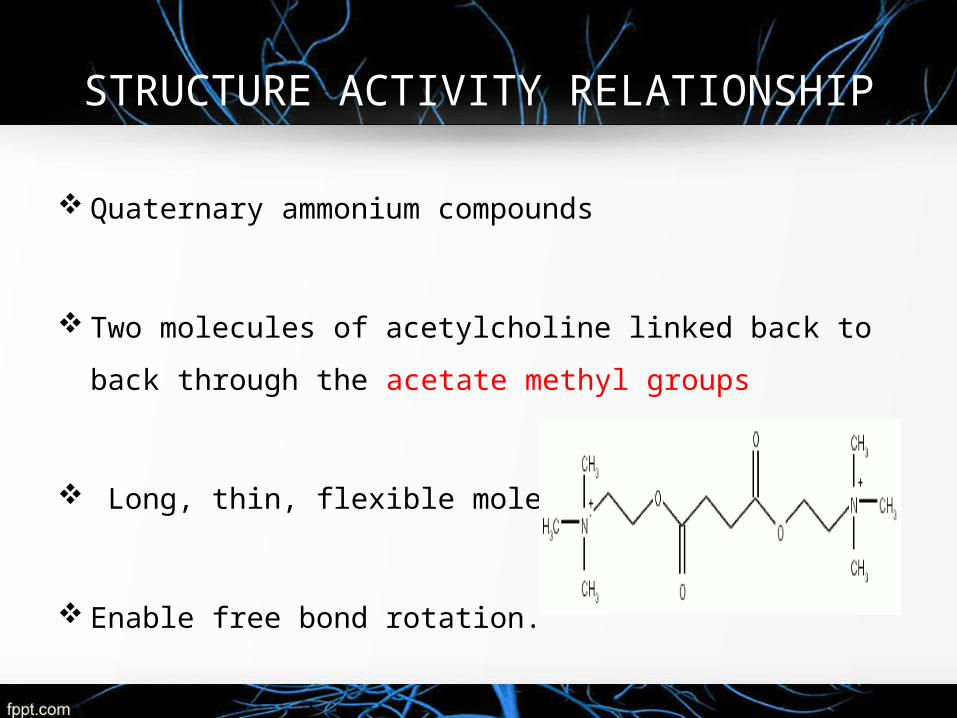
STRUCTURE ACTIVITY RELATIONSHIP
Quaternary ammonium compounds
Two molecules of acetylcholine linked back to back through
the acetate methyl groups
Long, thin, flexible molecule.
Enable free bond rotation.
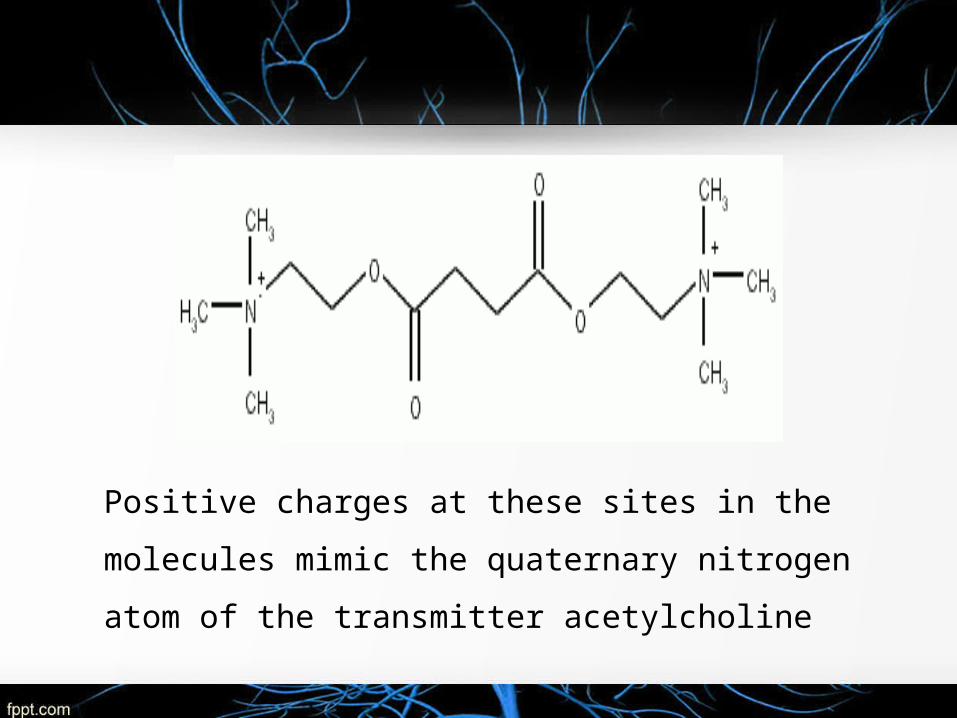
Positive charges at these sites in the molecules mimic
the quaternary nitrogen atom of the transmitter
acetylcholine
MECHANISM OF ACTION
Affinity and sub maximal intrinsic activity for NM receptors
Analouge of Ach
Longer durations at the neuromuscular junction -
resistance to AChE
Do not dissociate from receptors quickly
SCh reacts with Nm receptor – Open Na+ channels
Prolonged persistant depolarisation
Brief period of repetitive excitation
Flaccid paralysis of muscle
Elicit transient and repetitive muscle excitation FASICULATIONS
Neural release of Ach will result in binding of Ach to receptors on a already depolarised plate
• FLACCID PARALYSIS
• This initial depolarization block of
NEUROMUSCULAR TRANSMISSION AND FLACCID
PARALYSIS PHASE l BLOCK
The Na+ receptors at the end-plate and
the perijunctional zone remain
inactivated and junctional transmission
is blocked.
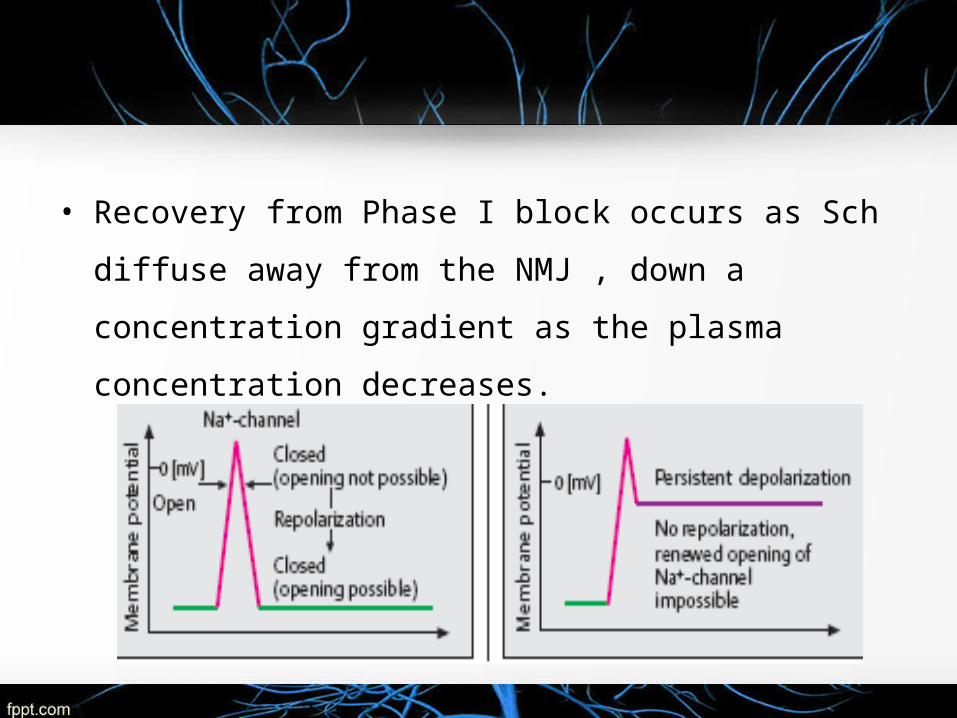
• Recovery from Phase I block occurs as Sch diffuse away
from the NMJ , down a concentration gradient as the
plasma concentration decreases.
Prolonged exposure to succinylcholine, the initial end plate
depolarization decreases membrane becomes repolarized.
Despite this repolarization, the membrane desensitized.
Phase II Block (Desensitizing)
Contd…
Unclear mechanism
The channels behave as if they are in a prolonged closed state.Neurotransmission remains blocked through out
1.Presynaptic block reducing the synthesis and
mobilization of ACh
2.Post junctional receptor desensitization
3.Activation of the Na-K ATPase pump by initial
depolarization, which repolarizes it
Contd…
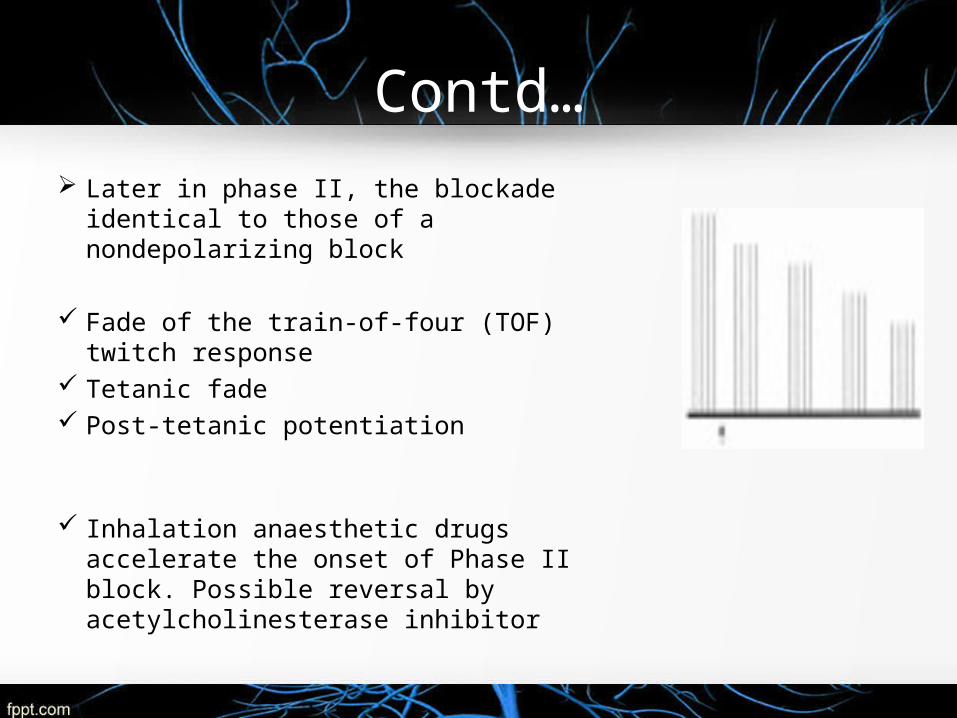
Later in phase II, the blockade identical to those of a nondepolarizing block
Fade of the train-of-four (TOF) twitch response
Tetanic fade Post-tetanic potentiation
Inhalation anaesthetic drugs accelerate the onset of Phase II block. Possible reversal by acetylcholinesterase inhibitor
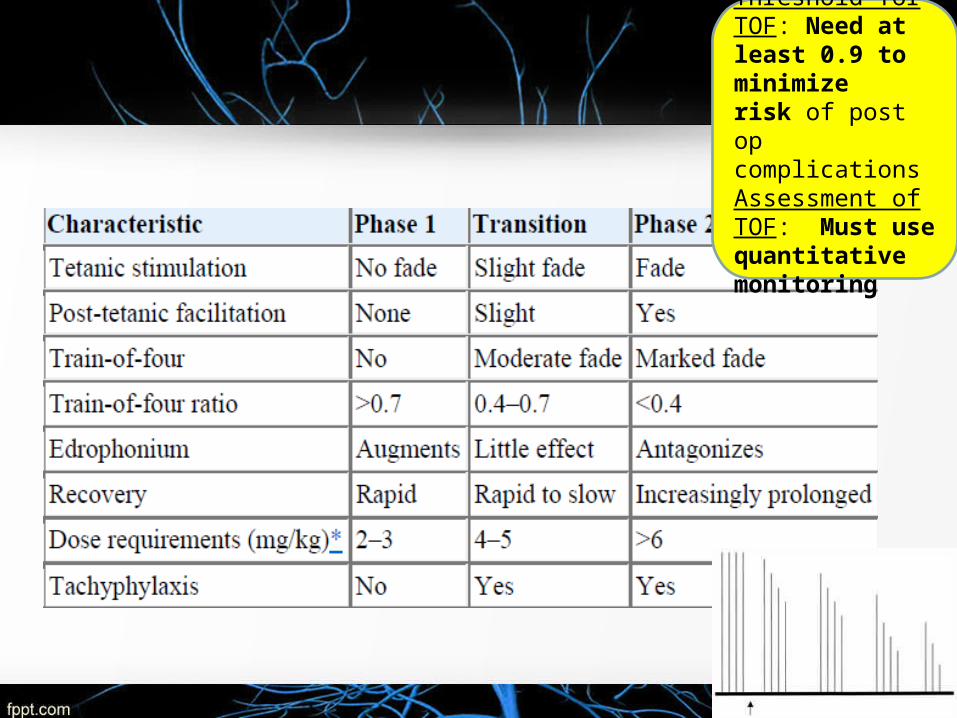
Threshold for TOF: Need at least 0.9 to minimize risk of post op complicationsAssessment of TOF: Must use quantitative monitoring
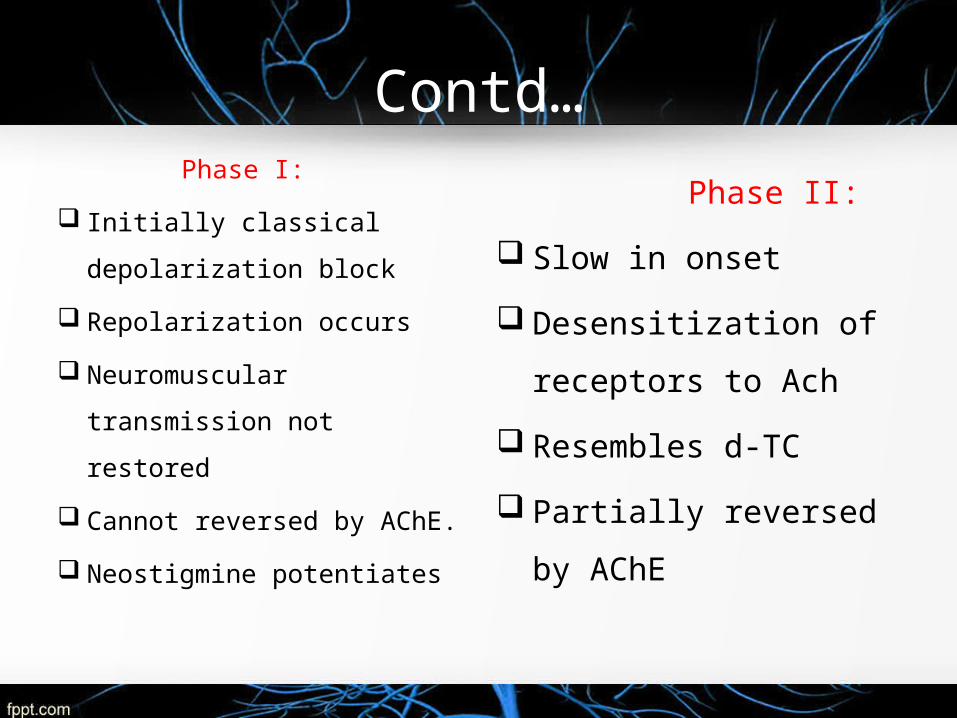
Contd… Phase I:
Initially classical
depolarization block
Repolarization occurs
Neuromuscular
transmission not restored
Cannot reversed by AChE.
Neostigmine potentiates
Phase II:
Slow in onset
Desensitization of
receptors to Ach
Resembles d-TC
Partially reversed by
AChE

PHARMACOKINETICS Rapid onset of effect and ultra short duration of action.
Not absorbed orally
Does not cross BBB, placenta
I.V route - initiation dose 0.5 – 1 mg/kg .tracheal intubation
in adults is 1.0 – 1.5 mg/ kg.
Cheeks,abdomen,neck,limb,face, respiratory paralysis
Apnoea within 1 min.Brief duration of action 6-11 min
Elimination - rapid hydrolysis by plasma cholinesterase in
liver
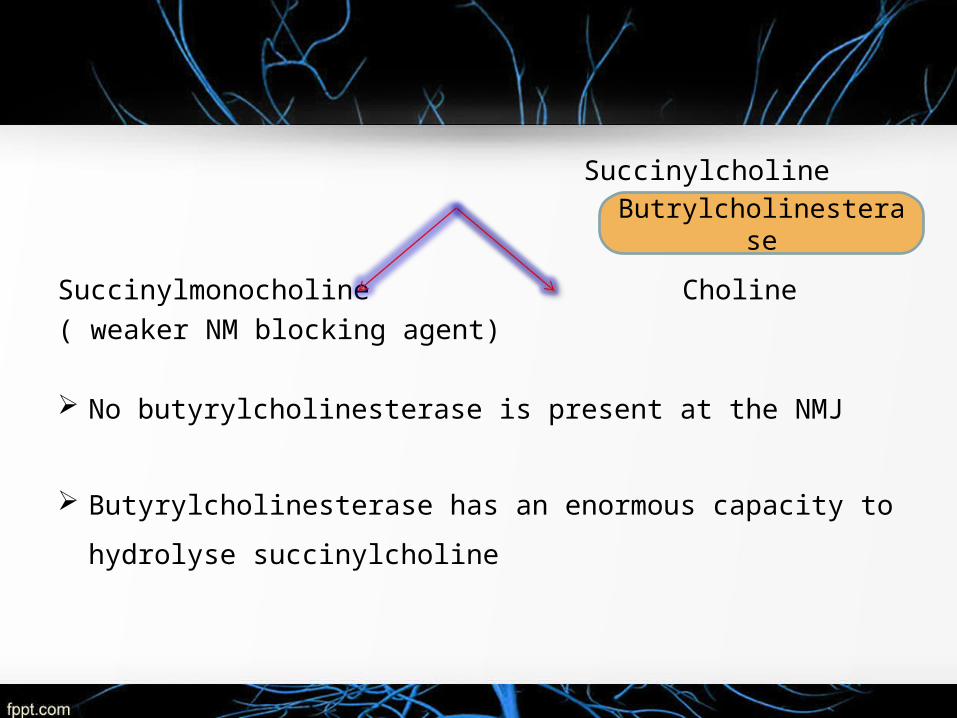
Succinylcholine
Succinylmonocholine Choline( weaker NM blocking agent)
No butyrylcholinesterase is present at the NMJ
Butyrylcholinesterase has an enormous capacity to hydrolyse
succinylcholine
Butrylcholinesterase
Only 10% of the administered drug reaches the
neuromuscular junction.
Influences the onset and duration of action of Sch by
controlling the rate at which the drug is hydrolyzed before it
reaches and after it leaves the NMJ.

Factors that have been found to lower butyrylcholinesterase activity
Liver disease Advanced age, malnutrition, pregnancy Burns OCPs, MAO inhibitors Ecothiophate, cytotoxic drugs Anticholinesterase drugs Neoplastic disease Tetrahydroaminacrine Hexafluorenium

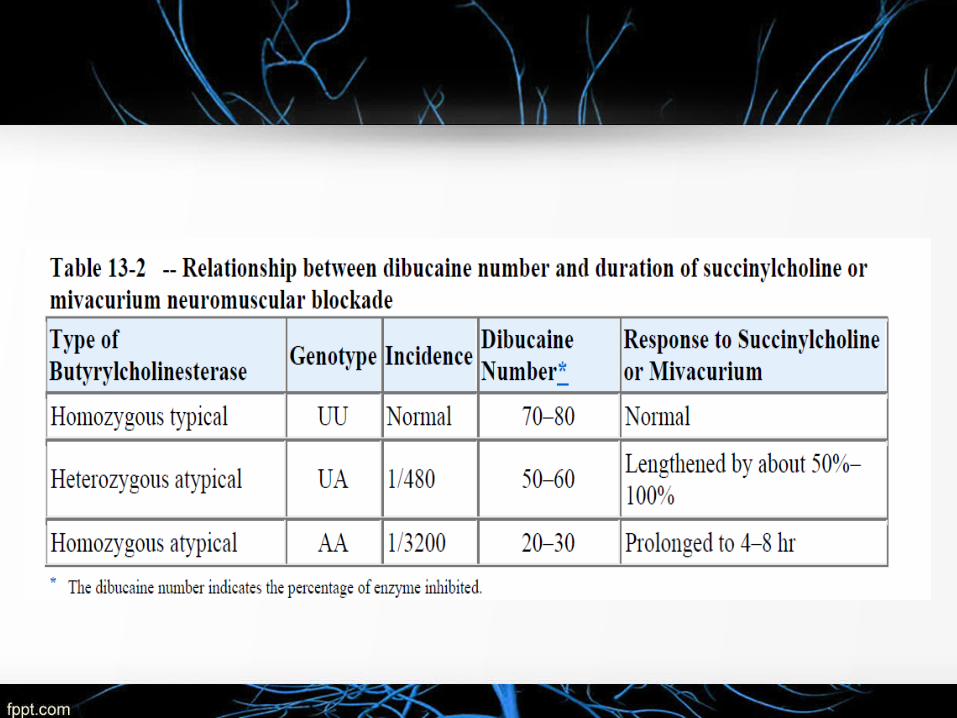
DIBUCAINE TEST
Patient with abnormal genetic variant of
butyrylcholinesterase ,Sch induced neuromuscular
blockade can be significantly prolonged
Dibucaine inhibits normal butyrylcholinesterase to a far
greater extent than it does the abnormal enzyme.
Contd…
• Under standardized test conditions Dibucaine inhibits
The normal enzyme about 80%
The abnormal enzyme about 20%
Many other genetic variants of butyrylcholinesterase
have been identified, dibucaine-resistant variants are the
most important
DIBUCAINE NUMBER
Measure of the ability of the person to metabolise Sch,
identify at risk patients.
Doesnot measure the concentration of enzyme in plasma
Efficiency of enzyme to hydrolyse the substrate.
THERAPUETIC USES
Adjuvant to General anaesthesia-Rapid-sequence
induction of anaesthesia- (DOC)1.0 mg/kg
succinylcholine facilitate ETintubation at 60 seconds
Assisted ventilation
To prevent trauma during ECT
Before administering the intubating dose of succinylcholine
A small dose of nondepolarizing neuromuscular blocker is
commonly given 2 mins. This defasciculating dose of
attenuate increases in intragastric and intracranial
pressure
minimize the incidence of fasciculations in response to
succinylcholine.
DRUG INTERACTION
Antichloniesterase -Neostigmine / Pyridostigmine.
Sch should not be administered to re establish
neuromuscular blockade - produces relaxation that will
last up to 60 minutes with administration of neostigmine
(5 mg).
Such prolongation can partly be explained by inhibition of
butyrylcholinesterase
• .
Combination of Lithium and succinylcholine resulted in
an additive inhibition.
Verapamil potentiates the neuromuscular block.
Bambuterol, produces marked causes prolongation of
Sch induced blockage.
Esmolol causes only minor prolongation of blockage
ADVERSE REACTIONS
Hyperkalemia Arrhythmias Malignant hyperthermia Master muscle rigidity Increased IOP, ICP Increased IGP Myalgia- lysine acetylsalicylate Succinylcholine apnoea FDA BLACK BOX WARNING IN YOUNG MALES
[Rosenberg Anesthesiology 77: 1054, 1992]
Succinylcholine apnoea
Occasionally succinylcholine produces prolonged apnoea due
to lack of normal plasma (pseudo) cholinesterase levels.
Treatment:
Artificial respiration until the muscle power returns.
Fresh blood or plasma transfusion to restore
cholinesterase enzyme level.
No specific antidote is available
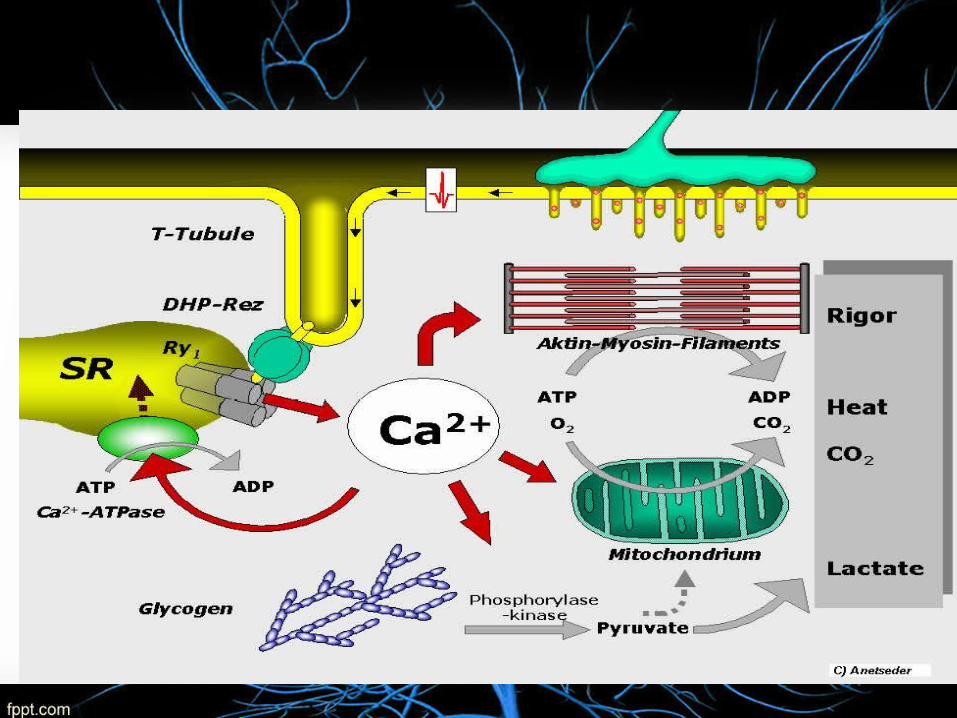
MALIGNANT HYPERTHERMIA
Rare life-threatening condition
Autosomal dominant disorder
Volatile anaesthetic agents and succinylcholine
Major defects in RYR1, DHPR, CACNA1S triadin
and FK 506
C/F :sustained muscle contraction and hyperpyrexia
MANAGEMENT
Dantrolene 2mg/kg I.V.
Procainamide - ventricular fibrillation
Rapid cooling
Inhalation of 100% oxygen
Control of acidosis should be considered adjunct
therapy in malignant hyperthermia
DECAMETHONIUM
2 quaternary ammoniums with a 10-carbon chain in
between,
• It's about 2x as potent as succinylcholine
• Derived from decamethylenediamine,
• Partial agonist of the nicotinic acetylcholine receptor.
contd…
• Persistant depolarisation
• Character of muscle responseto indirect tetanic
stimulation during partial block -Well-sustained
contraction
Does not produce unconsciousness or anesthesia, and
its effects may cause considerable psychological
distress while simultaneously making it impossible for a
patient to communicate
DIRECTLY ACTING AGENTS
SPASMOLYTICS
SPASTICITY
• It is a motor neuron disorder characterized by skeletal muscle rigidity, exaggerated tendon jerks and paralysis of affected muscles.
Causes• Cerebral palsy• Stroke• Multiple sclerosis• Traumatic brain injury• Anoxia• Neurodegenerative disease
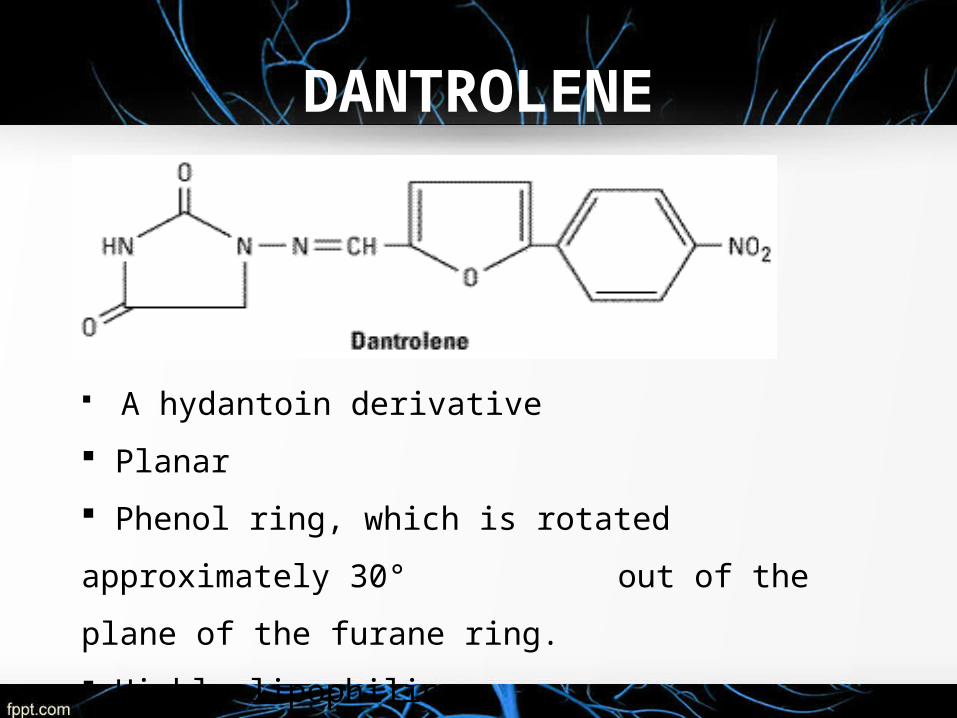
DANTROLENE
A hydantoin derivative
Planar
Phenol ring, which is rotated approximately 30°
out of the plane of the furane ring.
Highly lipophilic

Contd..• Phenytoin analouge
• Antispastic action lie outside CNS
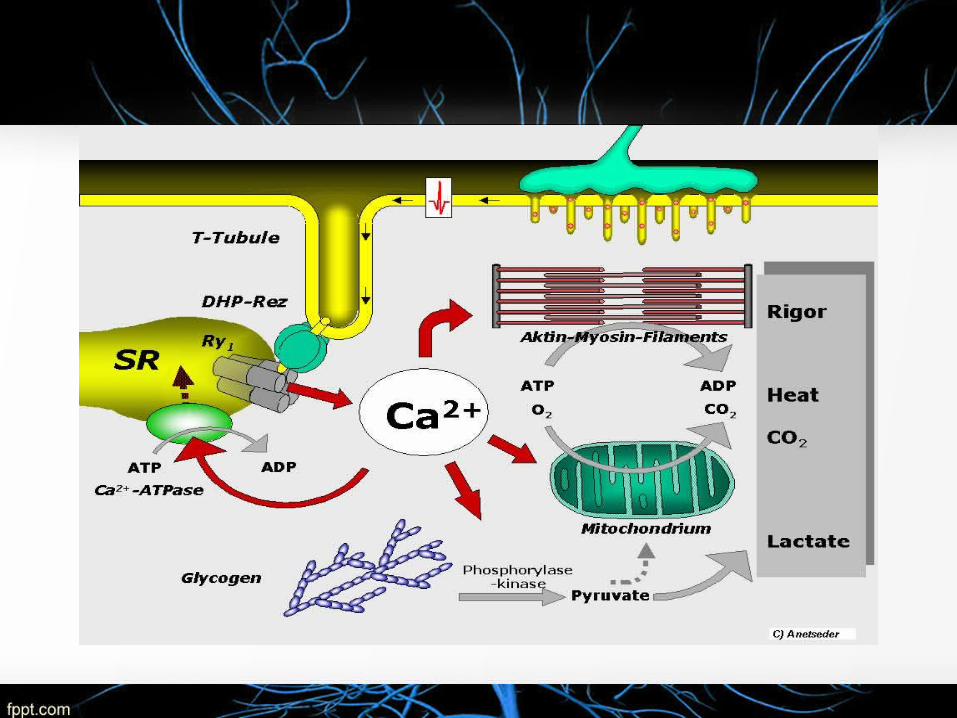
• The L-type channel with its T-tubular location serves as the
voltage sensor receiving the depolarizing activation signal.
• Inhibits Ca2+ release from the sarcoplasmic reticulum of skeletal
muscle by limiting the capacity of Ca2+ and calmodulin to
activate RYR-1
PHARMACOKINETICS
Poorly absorbed orally
Penetrates brain and produces sedation
Metabolized in liver into 5-hydroxydantrolene
Excreted in kidney.
T 1/2 9 -12 hrs.
Dose: 25-100 mg 4 times daily
THERAPEUTIC USES
UMN disorders – paraplegia, hemiplegia, cerebral palsy
DOC: Malignant hyperthermia (2.5 – 4 mg/kg)• Prophylactic dantrolene administration before trigger-free
GA for MH-susceptible patients has been recommended
Neuroleptic malignant syndrome: 1 – 2.5 mg/kg
Heat stroke.
ADVERSE EFFECTS
• Sedation- facilitated GABA – depression of brain stem • Malaise• Light headedness• Muscular weakness• Diarrhea • Hepatitis• Neonates are at risk of ‘floppy child syndrome’ –C/s

Drug Interactions
Diltiazem/ Verapamil
Severe cardiovascular collapse, arrhythmias, myocardial depressions, and hyperkalemia.
Vecuronium : Neuromuscular blockade is prolonged.
CNS depressants: Sedative action is potentiated.
Combined OCPS and HRT may enhance liver toxicity.
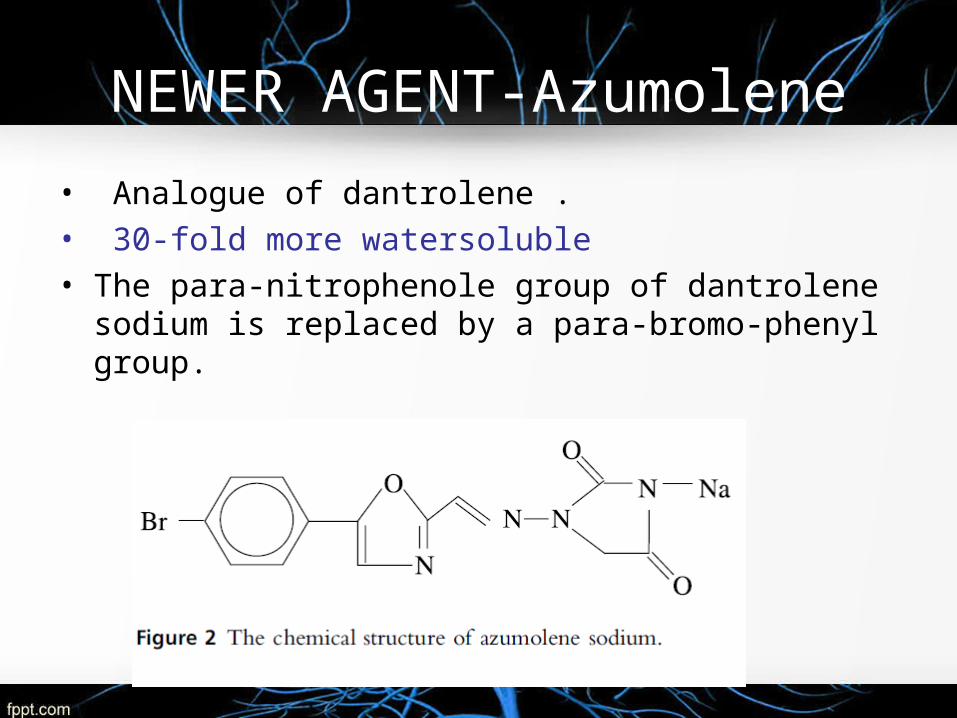
NEWER AGENT-Azumolene
• Analogue of dantrolene . • 30-fold more watersoluble• The para-nitrophenole group of dantrolene sodium is
replaced by a para-bromo-phenyl group.
• Equipotent to dantrolene in the treatment and prevention
of the clinical manifestations of an MH crisis
Same potency as Dantrolene in
• Inducing relaxation in porcine skeletal muscle in vitro.
• In vivo, even more potent in inhibiting gastronemius
muscle twitches
QUININE Dual action in skeletal muscle:
Acts directly on the muscle fibre increases the tension
response
Increases the refractory period
Decreases the excitability of the motor end-plate
Makes the muscle less susceptible to repetitive neural
stimuli
Less Responsive To Acetylcholine
• The typical adult dosing for nocturnal leg cramps is 260 mg at bedtime.
Adverse events:• Thrombocytopenia• Hypersensitivity reactions • QT prolongation
• FDA Warns of Risks with Unapproved Use of Malaria Drug Qualaquin