shoulder to shoulder mi zucker, md. a dr z lecture
TRANSCRIPT
SHOULDER to SHOULDER
MI Zucker, MD
A dr Z lecture
On common things of the shoulder that hurt
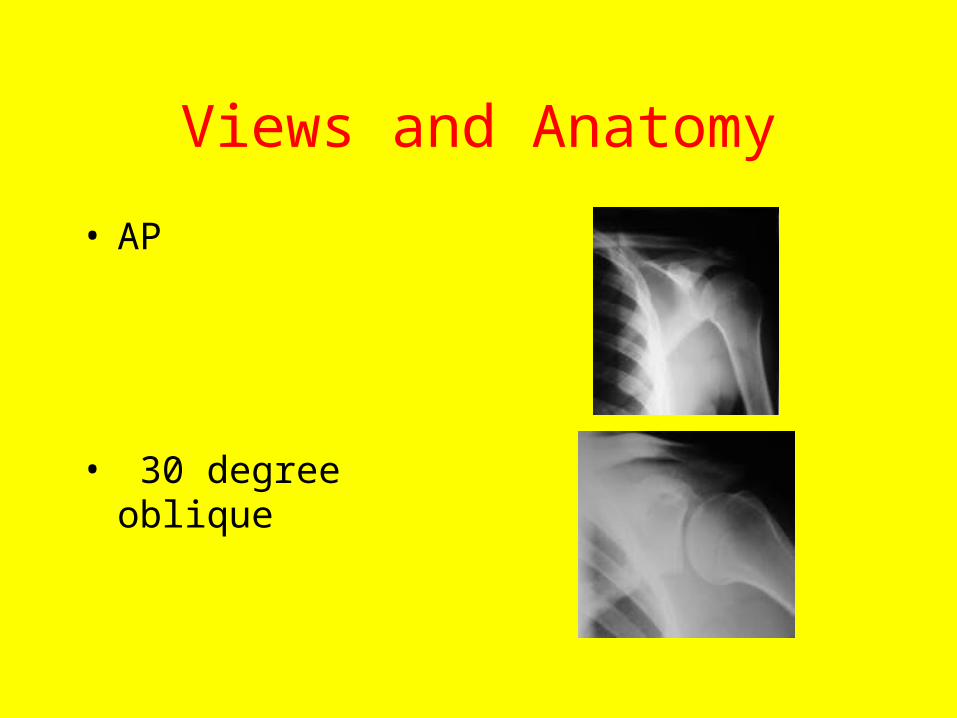
Views and Anatomy
• AP
• 30 degree oblique
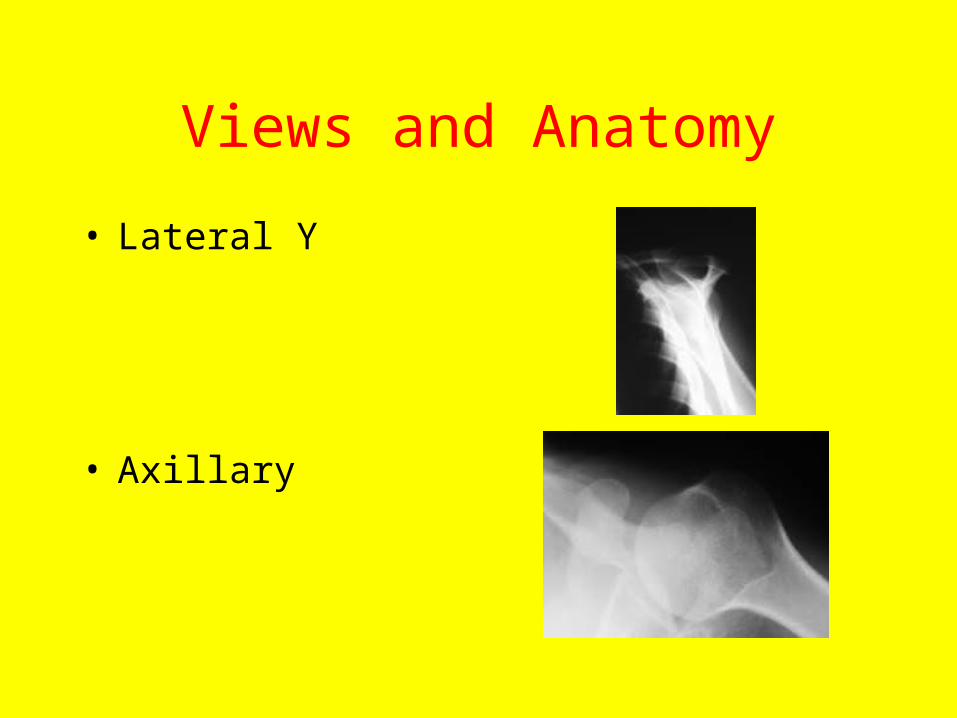
Views and Anatomy
• Lateral Y
• Axillary
TRAUMA
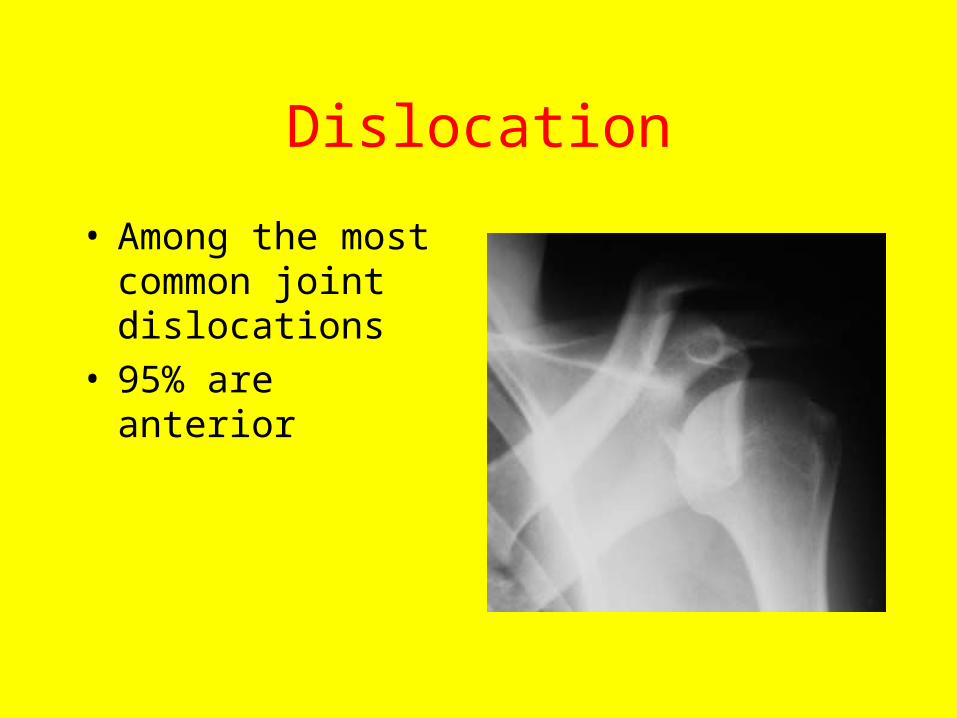
Dislocation
• Among the most common joint dislocations
• 95% are anterior
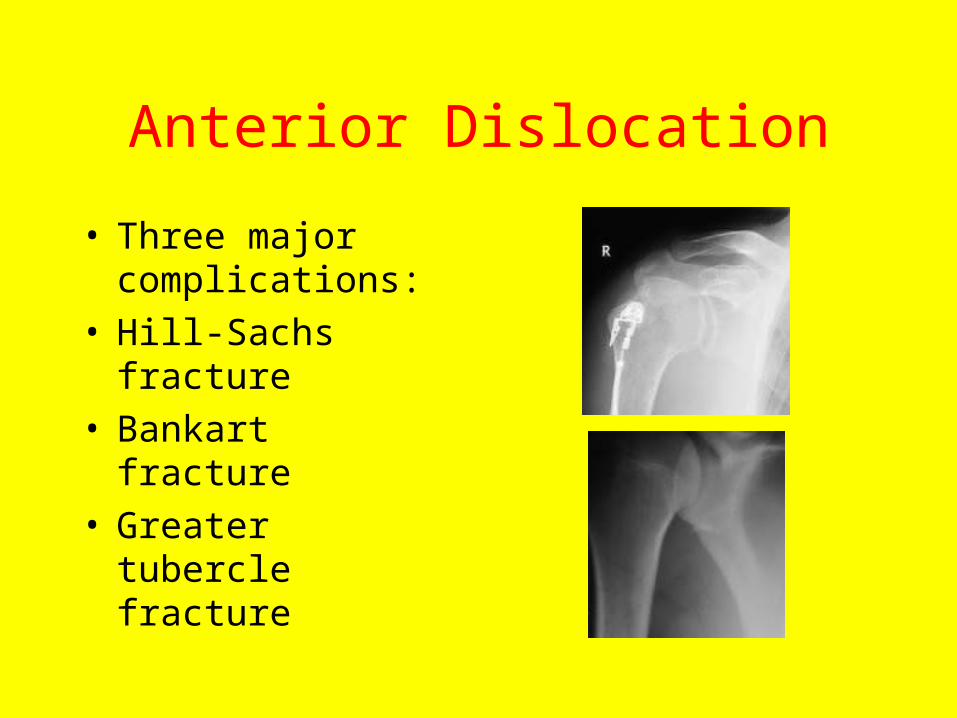
Anterior Dislocation
• Three major complications:
• Hill-Sachs fracture• Bankart fracture• Greater tubercle
fracture
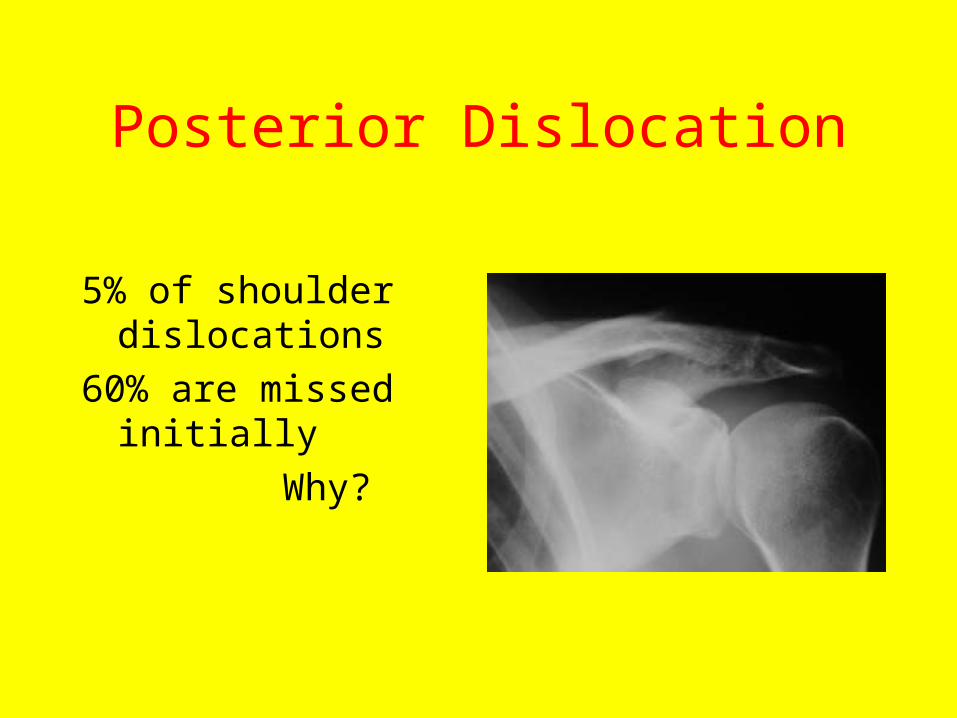
Posterior Dislocation
5% of shoulder dislocations
60% are missed initially
Why?
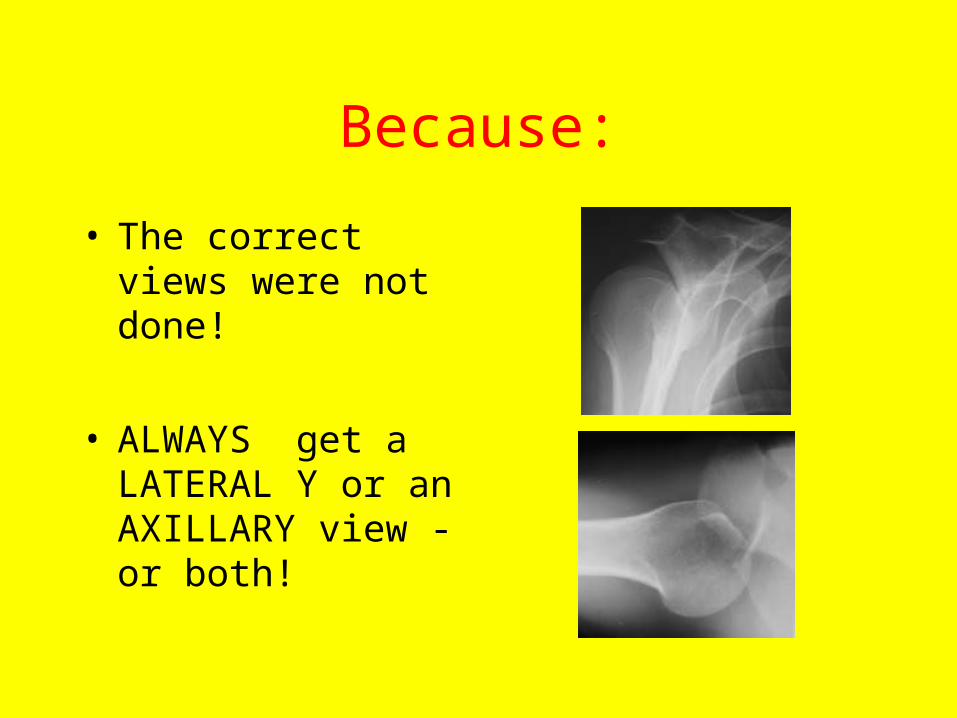
Because:
• The correct views were not done!
• ALWAYS get a LATERAL Y or an AXILLARY view -or both!
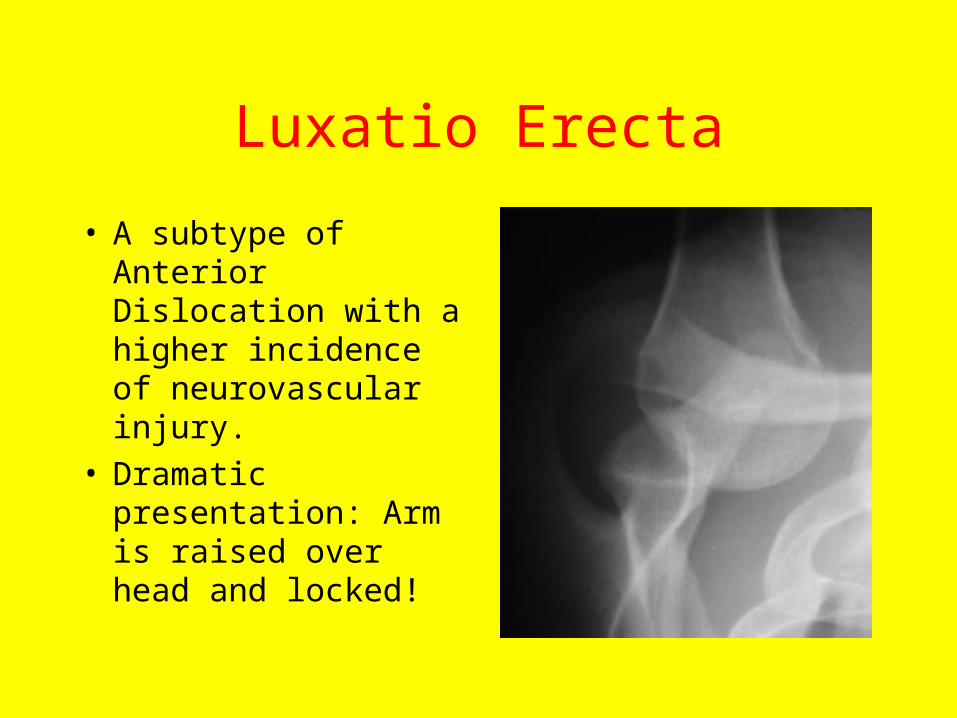
Luxatio Erecta
• A subtype of Anterior Dislocation with a higher incidence of neurovascular injury.
• Dramatic presentation: Arm is raised over head and locked!
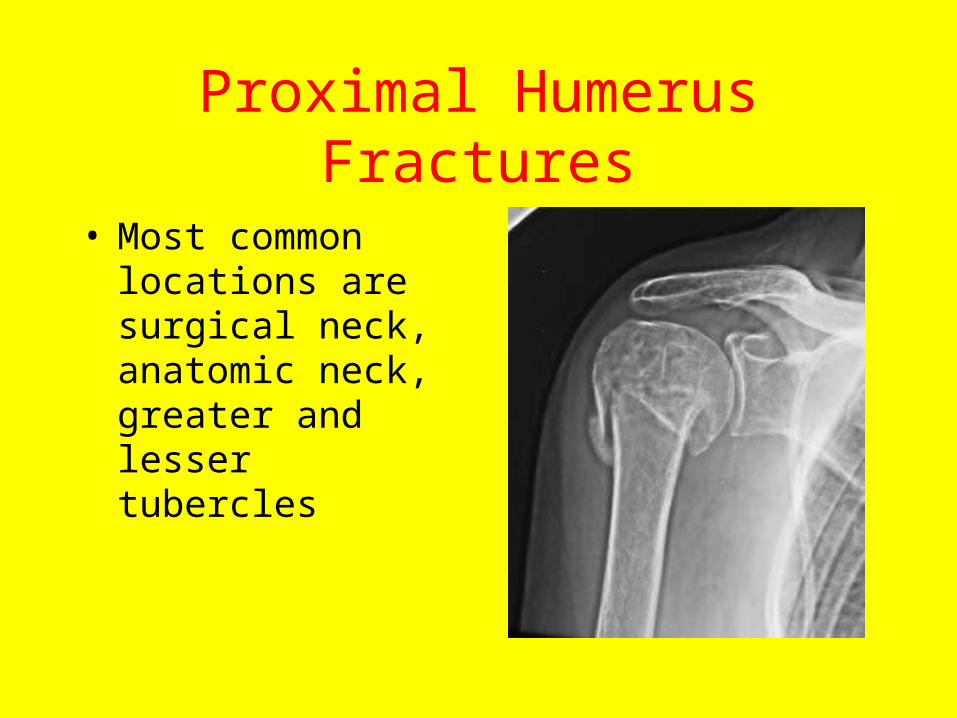
Proximal Humerus Fractures
• Most common locations are surgical neck, anatomic neck, greater and lesser tubercles
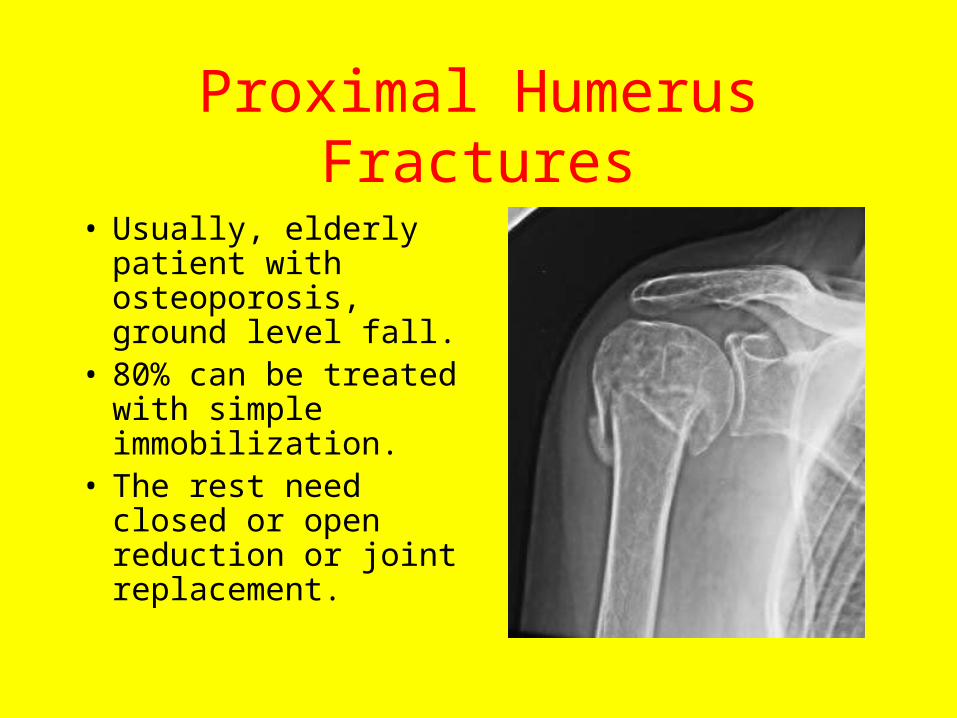
Proximal Humerus Fractures
• Usually, elderly patient with osteoporosis, ground level fall.
• 80% can be treated with simple immobilization.
• The rest need closed or open reduction or joint replacement.

Acromio-clavicular Joint Injuries: The players
• Acromio-clavicular ligament
• Ac joint capsule• Coraco-clavicular
ligament
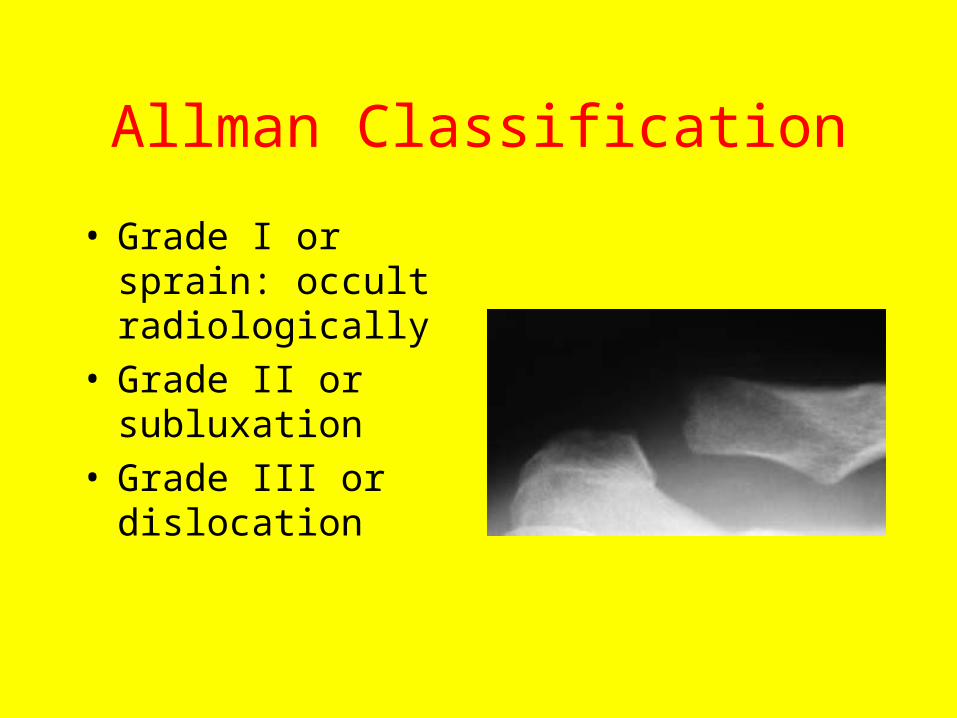
Allman Classification
• Grade I or sprain: occult radiologically
• Grade II or subluxation
• Grade III or dislocation
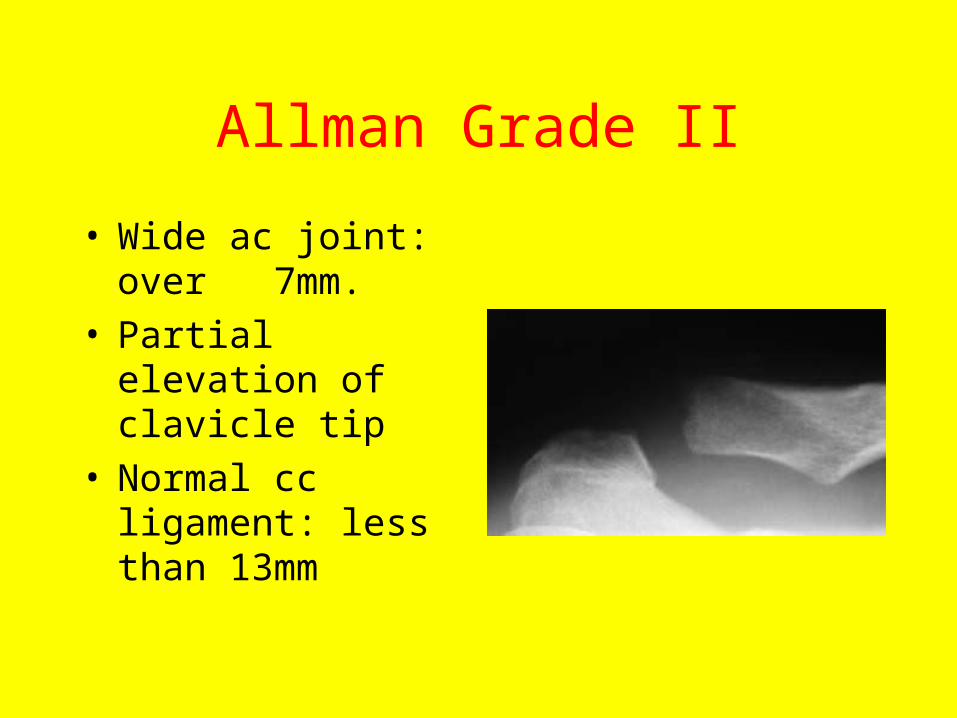
Allman Grade II
• Wide ac joint: over 7mm.
• Partial elevation of clavicle tip
• Normal cc ligament: less than 13mm
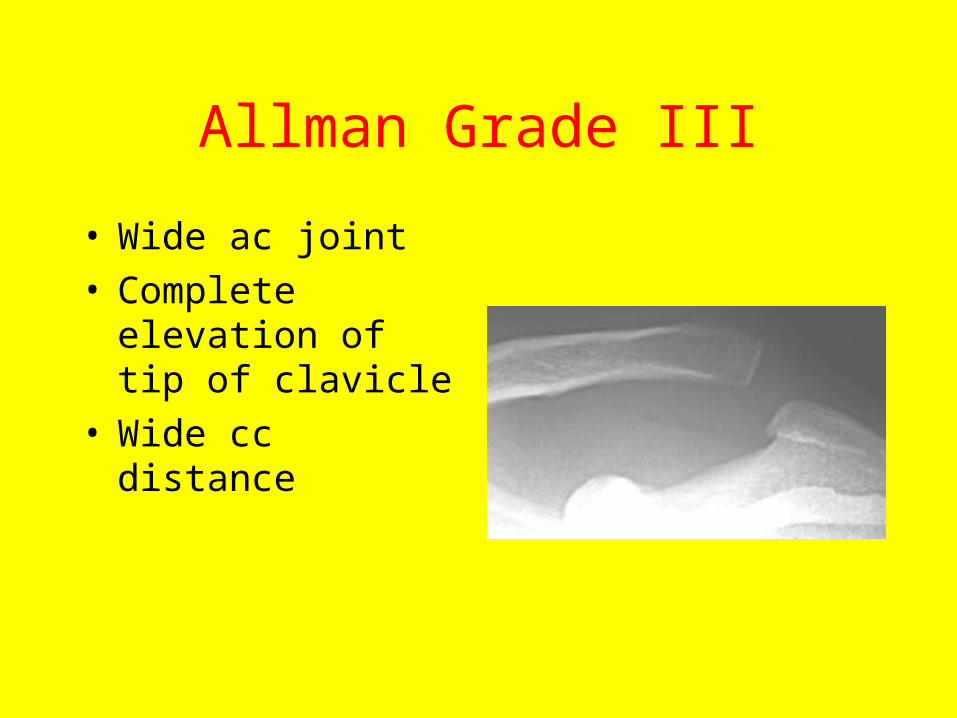
Allman Grade III
• Wide ac joint• Complete elevation of
tip of clavicle• Wide cc distance
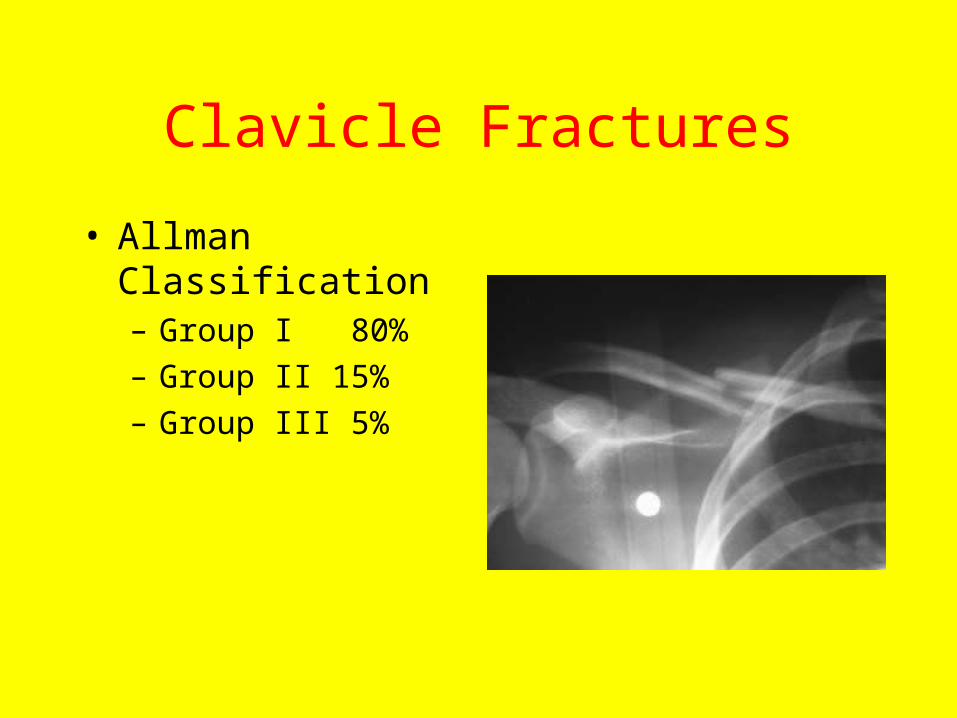
Clavicle Fractures
• Allman Classification– Group I 80%
– Group II 15%
– Group III 5%
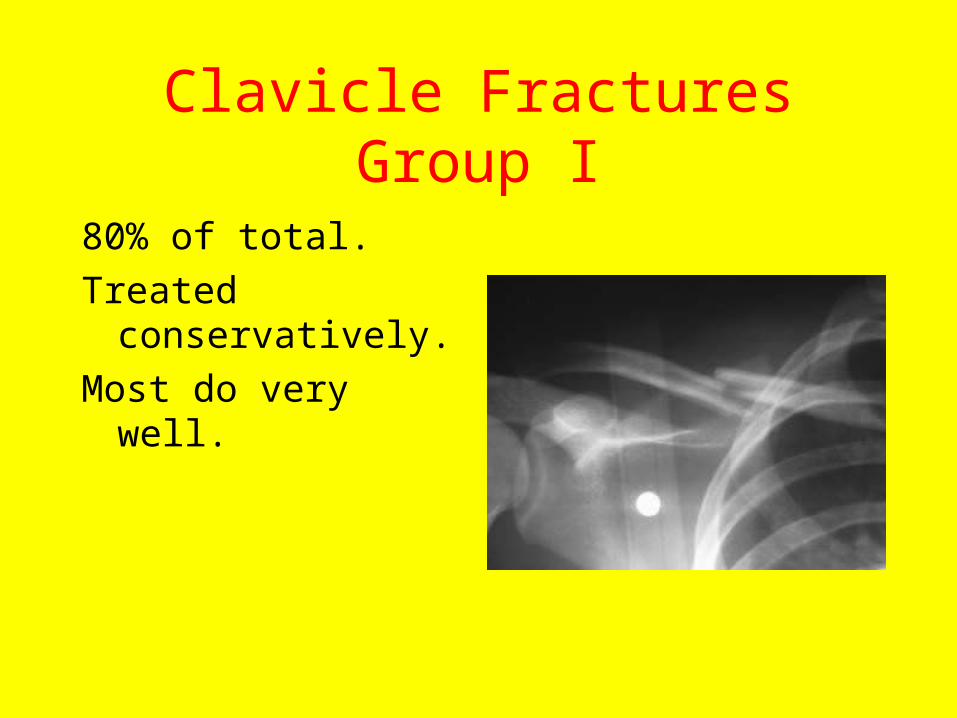
Clavicle Fractures Group I
80% of total.
Treated conservatively.
Most do very well.

Clavicle Fractures Group II
• 15%. Guarded prognosis; initially treated conservatively but may need delayed surgery
• Neer Type I: Intact cc ligament
• Neer Type II: Torn cc ligament
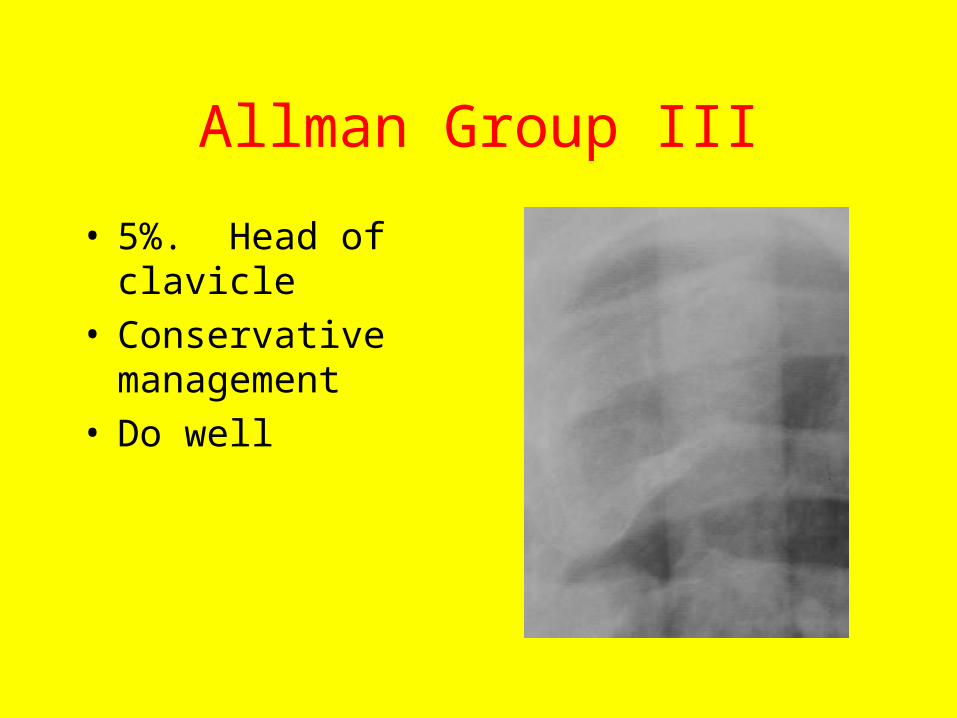
Allman Group III
• 5%. Head of clavicle• Conservative
management• Do well
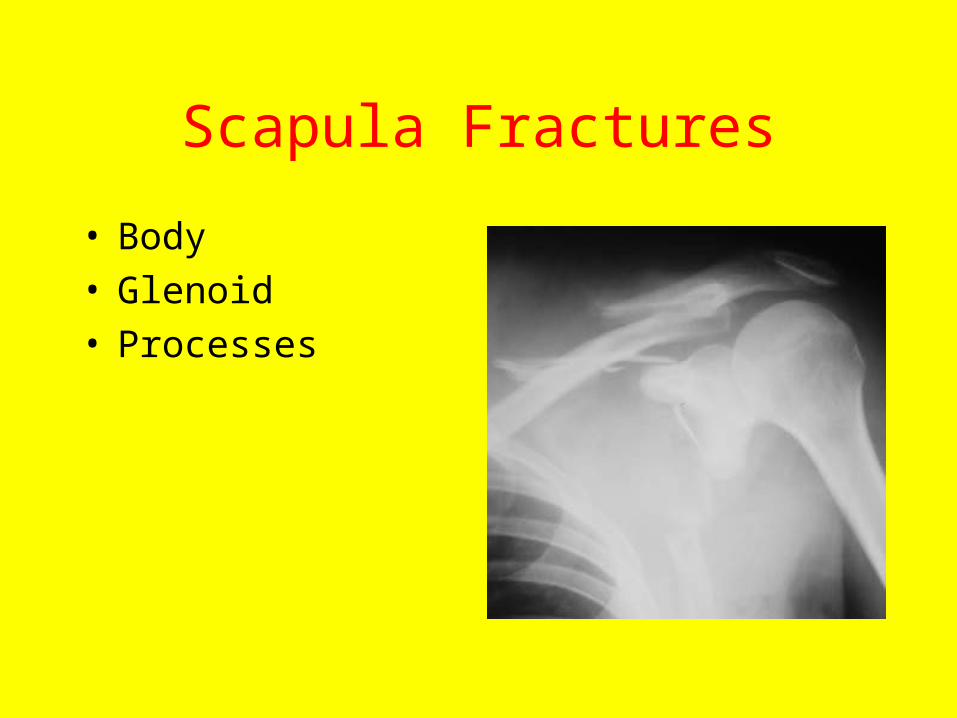
Scapula Fractures
• Body• Glenoid• Processes
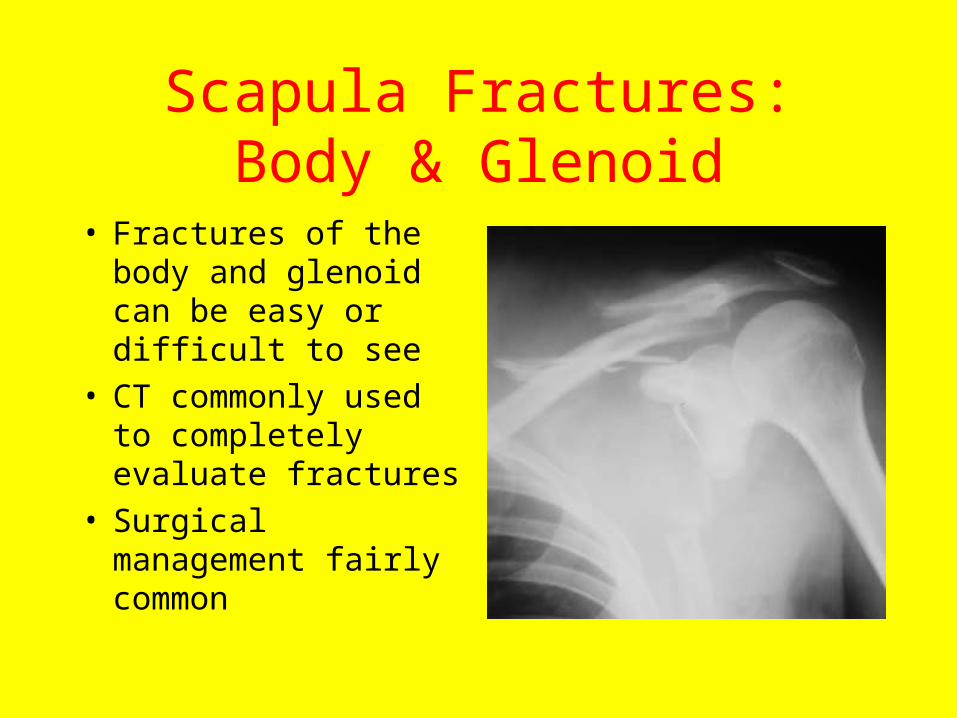
Scapula Fractures: Body & Glenoid
• Fractures of the body and glenoid can be easy or difficult to see
• CT commonly used to completely evaluate fractures
• Surgical management fairly common
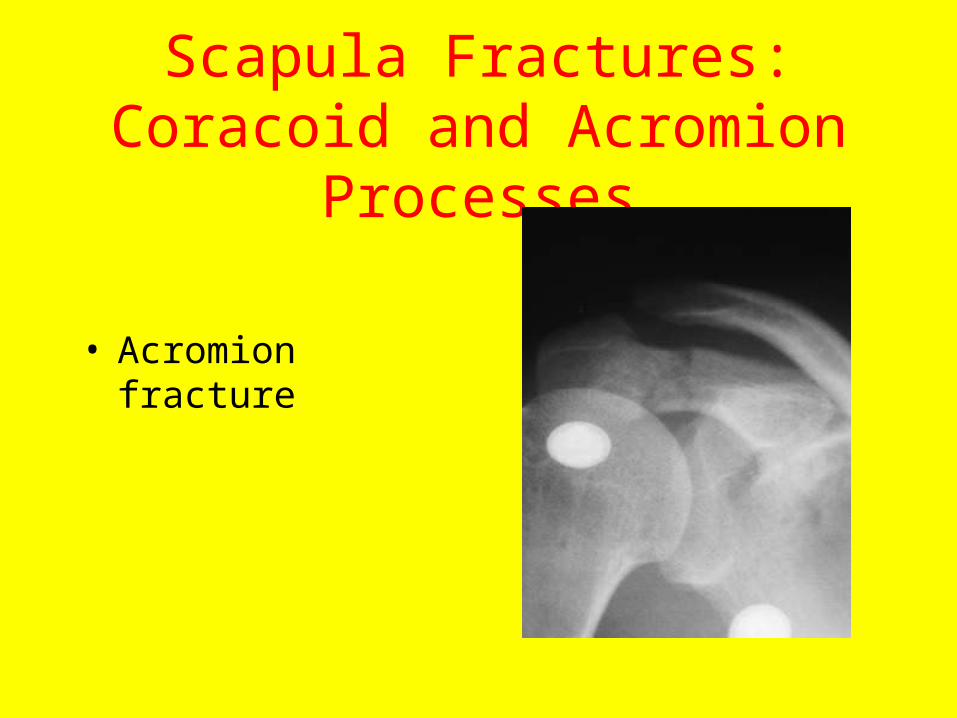
Scapula Fractures: Coracoid and Acromion Processes
• Acromion fracture

Kid Fractures
• Salter-Harris physis injuries
• This is a displaced
SH I
Things that hurt that aren’t acute trauma
• Rotator cuff disease (impingement syndrome)• Calcific bursitis• CPPD disease• Osteoarthritis• Inflammatory arthritis• Septic arthritis/osteomyelitis• Malignancy• AVN
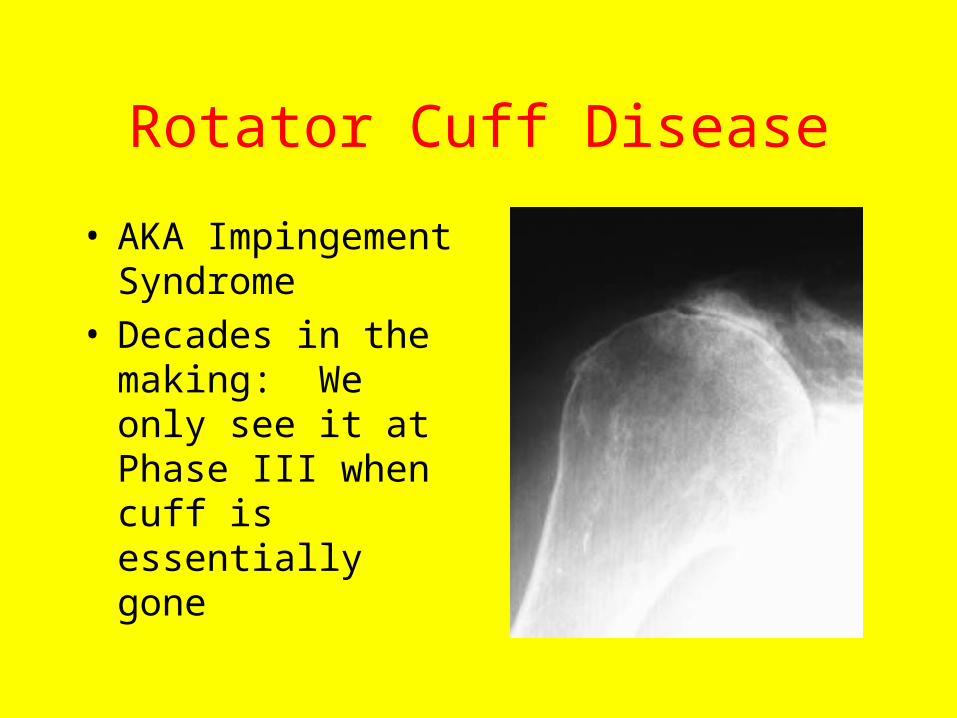
Rotator Cuff Disease
• AKA Impingement Syndrome
• Decades in the making: We only see it at Phase III when cuff is essentially gone
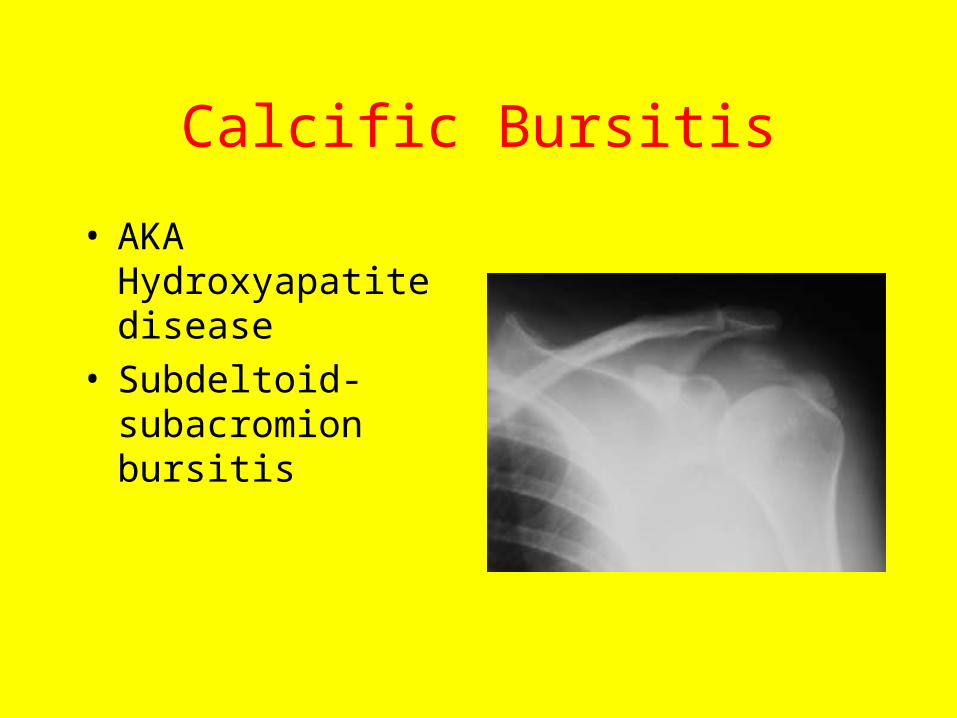
Calcific Bursitis
• AKA Hydroxyapatite disease
• Subdeltoid-subacromion bursitis
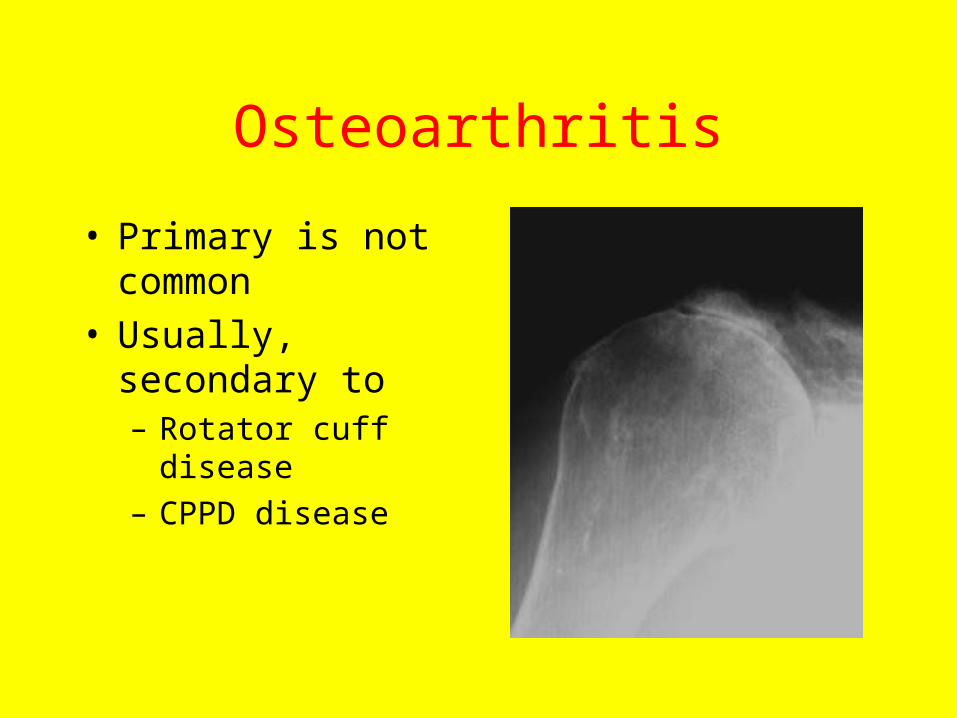
Osteoarthritis
• Primary is not common
• Usually, secondary to – Rotator cuff disease
– CPPD disease
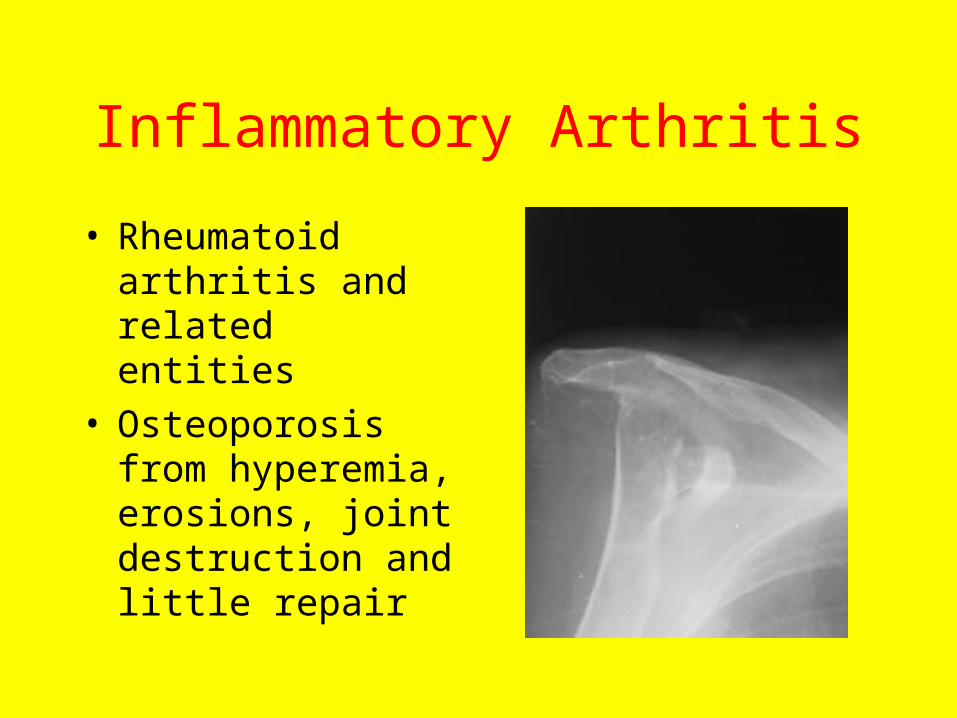
Inflammatory Arthritis
• Rheumatoid arthritis and related entities
• Osteoporosis from hyperemia, erosions, joint destruction and little repair

Infection
• Infection of joint or bone or both
• Any destructive process that crosses a joint is most likely infection
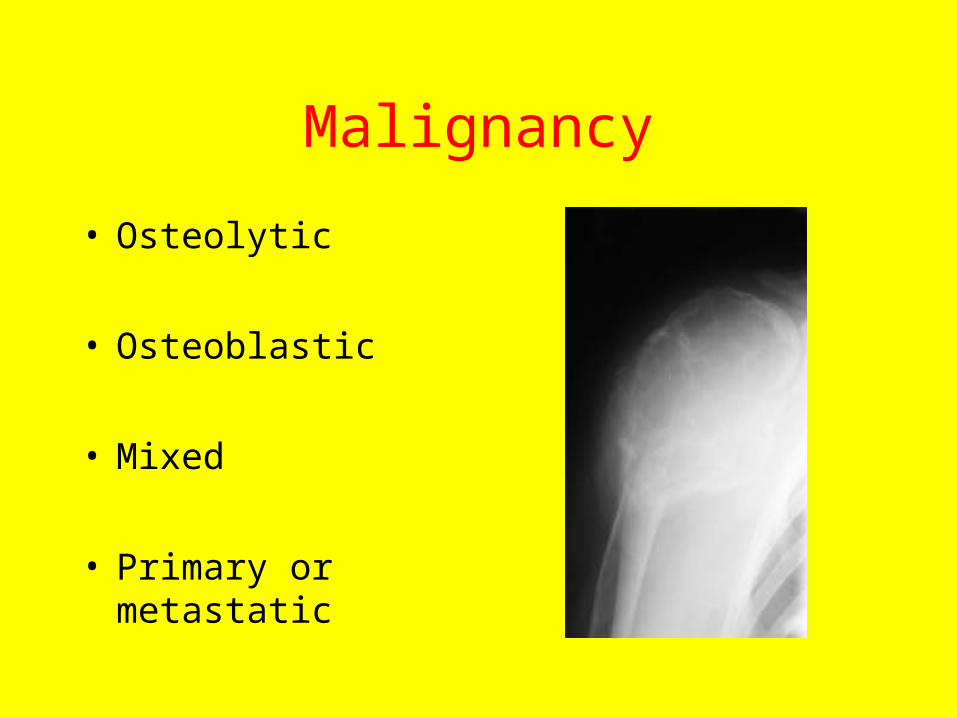
Malignancy
• Osteolytic
• Osteoblastic
• Mixed
• Primary or metastatic
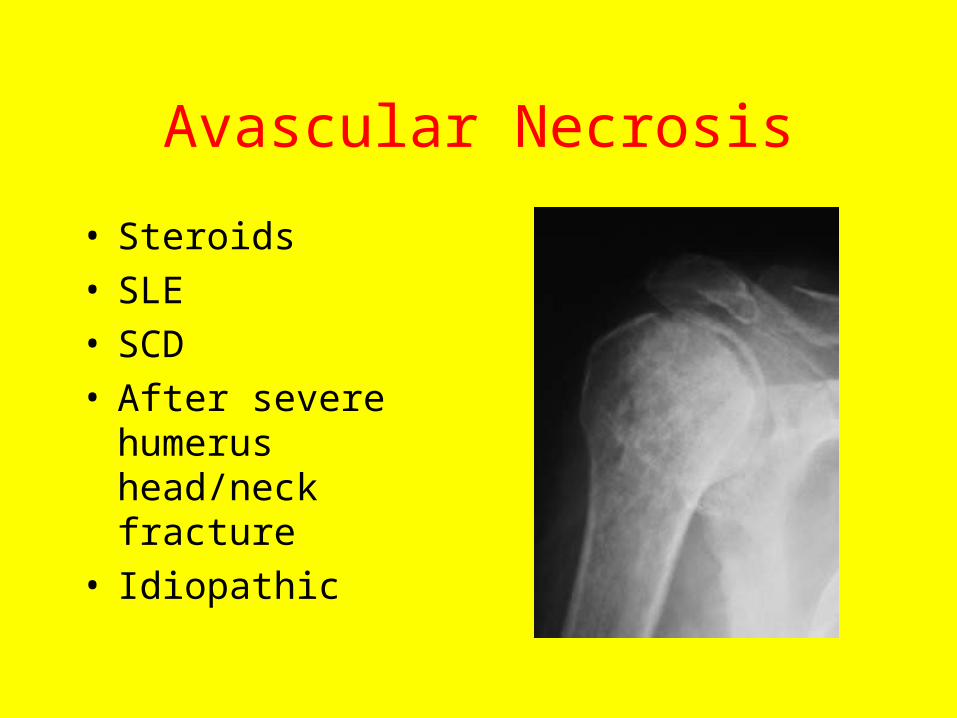
Avascular Necrosis
• Steroids• SLE• SCD• After severe humerus
head/neck fracture• Idiopathic

GOODBYE
• Copyright 2004
MI Zucker