serum ferritin and erythrocyte 2,3-dpg during quantitated phlebotomy and iron treatment
TRANSCRIPT

Scand J Haematol(l977) 19, 327-333
Serum Ferritin and Erythrocyte 2,3-DPG during Quantitated
Phlebotomy and Iron Treatment
GUNNAR BIRGEGARD,' CLAES HOG MAN,^ ANDREAS KILLANDER,' HANS LEVANDER,' BENGT SIMONSSON' & LEIF WIDE3
Department of Internal Medicine, 2 The Blood Center and 3 Department of Clinical Chemistry, University Hospital, Uppsala, Sweden
Serum ferritin and erythrocyte 2,3-DPG levels were followed in 3 healthy males who were phlebotomized to iron depletion and a moderate anaemia. In 2 of the subjects, the expected rise in DPG levels was seen but not in the third, in spite of a Hb concentration of 95 g/l. Serum ferritin levels were found to reflect changes in iron stores, and subnormal serum ferritin indicated depleted iron stores. However, there was no correlation between pre-phlebotomy ferntin levels and calculated iron stores. The conclusion is that no fixed ratio can be established between serum ferritin and iron stores. A single ferritin value within the normal range does not tell how large iron stores a person has. Changes in an individual's iron stores can, however, be detected by repeated ferritin estimations.
Key words: biphosphoglycerate (DPG) - iron stores - iron treatment - phlebotomy - serum ferritin
Accepted for publication June 4, 1977
Correspondence to: Gunnar Birgegbrd, Department of Internal Medicine, University Hospital, S-750 14 Uppsala, Sweden
It has been shown repeatedly that red cell biphosphoglycerate (DPG) increases in dif- ferent states of anaemia (Eaton & Brewer 1968, Hjelm 1969, Thomas et a1 1974). It is commonly believed that this is a favour- able compensatory mechanism, decreasing the affinity for oxygen of the Hb and there- by improving the delivery of oxygen to the tissues (Torrance et a1 1970). The in vivo regulation of DPG and the clinical im- portance of normal versus increased or decreased levels are still unknown, and no
longitudinal studies seem to have been made. In the present investigation, we have studied the DPG concentration during the development of a bleeding anaemia.
The second question initiating the present study was whether serum ferritin levels, being a reliable method of assessing iron deficiency (Walters et a1 1973, Siimes et a1 1974, Cook et a1 1974), also reflect the iron stores in a quantitative way, as has been claimed by Walters et a1 (1973). A phlebo- tomy experiment was used to empty the iron

328 BIRGEGARD, HOGMAN, KILLANDER, LEVANDER, SIMONSSON, WIDE
stores completely and produce anaemia in 3 healthy volunteers and after that iron stores were calculated. The anaemia was then treated with an iron-sorbitol-gluconic acid polymer (FerastralB), injected i.m. in a sub- optimal dose.
MATERIAL AND METHODS
3 healthy males, 32-35 years old, with normal routine haematological data were phlebotomized by repeated blood donations with an interval of at least 1 week, until a moderate degree of anae- mia (about 95 g HbA) was reached (Simonsson et a1 1977). After 8-10 phlebotomies, the Hb con- centration failed to rise during a 2-week period without further blood letting. The transferrin saturation was below 10 % and there was no stainable bone marrow haemosiderin, indicating iron depletion. The difference in total H b before and after phlebotomy was calculated from the blood volumes and H b concentrations at these times. This difference gives the part of the total iron loss accounted for by the change in Hb concentration. The rest of the total iron loss then must have been taken from the iron stores that can now be estimated. After correction for dietary intake and basal daily iron loss, the storage iron in the 3 subjects was estimated to 666, 522 and 750 mg, respectively. The calculations are presented in detail in a previous paper (Simons- son et a1 1977).
There are no indications that blood volume changes during the development and the remis- sion of a moderate anaemia (Norrby 1974). The actual blood volumes of the 3 subjects could not be determined and thus, it cannot be excluded that some fluctuations may have occurred during the experimental period. During iron deficiency, the absorption of dietary iron has been found to vary between 2.8 and 6.0 mg per d (Norrby 1974). The average value of 4.8 mg per d was used in the calculation of the iron balance during the phlebotomy period.
When the iron stores were depleted, 500 mg of iron (Ferastral) was given, i.m., twice with an interval of 1 week. The dose was chosen so that the injected iron would not be sufficient to bring the H b concentration back to pre-phlebotomy
levels, and in fact failed to do so by about 10 g/l. With a few exceptions, samples were collected weekly until 5 weeks after the first iron injection. The subjects rested for 15 min in the supine posi- tion before sampling.
H b concentration was measured by the cyanmet- haemoglobin method. Duplicate estimates were made and the difference between duplicates in no case exceeded 2 %.
Serum iron concentration was estimated according to the principles of Heilmeyer & Plotner (1937), and Lindvall & Andersson (1961). The unsaturated iron binding capacity (UIBC) was determined by the method of Cartwright & Wintrobe (1949). Before the inj. of i.m. iron, total iron binding capacity (TIBC) was measured. The assumption was made that this remained constant after the inj. and serum iron was then calculated by mea- suring UIBC (by titrating with iron to the satura- tion point) and subtracting UIBC from TIBC.
Ferritin assay. The ferritin assay method is a solid phase radioimmunoassay utilizing labelled ferritin, as described by Wide & Birgegird (1977). The ferritin was conjugated with an 1251-labelled ester to a high specific radioactivity and allowed to compete with the serum sample ferritin for the free antigen-binding sites on anti-ferritin anti- bodies, indirectly coupled to cyanogen-bromide activated polysaccharide particles. There is no international reference standard for ferritin and various laboratories use their own internal ferritin standards. As a consequence, normal range for serum ferritin varies between laboratories, the mean for adult males varying between 56.9 pg/l (Halliday et a1 1975), and 176 pg/l (Prieto et a1 1975). The reason for this may be that ferritin preparations with a varying degree of purity have been used. Furthermore, Stauffer & Greenham (1976) have shown that variations in iron con- tent of the ferritin molecule are of importance both in the estimation of ferritin protein by the method of Lowry et a1 (Stauffer & Greenham 1976) and for the immunoreactivity (Porter 1974). We had no evidence for the homogeneity of the ferritin preparation available. For all these rea- sons we have chosen to express our results in arbitrary units/l, and the geometric mean for a population of 25 healthy young men was given
FERRITIN AND DPG DURING PHLEBOTOMY 329
'11 160-
*-.140.
120-
100-
the value of 100 (range, expressed as 95 % limits: 40-246). These figures correspond fairly well with figures given in pg/l by several investigators (Cook et a1 1974, Siimes et a1 1974, Walters et a1 1973). The detection limit was 4.6 arb U/I. The intra- assay variation was 4.7 %, when calculated as the average standard error of the mean duplicates of the test samples giving an inhibition between 20 and 80 % of total bound. The inter- plus intra- assay variation calculated as the coefficient of variation from 9 repeated assays of control sam- ples on 3 levels of ferritin concentration was 4.4 % for 180 arb U/1, 6.5 % for 73 arb U/1, and 8 % for 19 arb U/I.
0 - 0 -1L.O
-12,o
-10,o
Erythrocyte biphosphoglycerate (DPG) concentra- tion was determined in neutralized perchloric acid extracts of blood using coupled optical enzymic tests (Adam 1962, Ericson & de Verdier 1972). The extracts were stored at -70° until analyzed and all samples from the same subject were as- sayed simultaneously.
-14.0
-12.0
-10.0
RESULTS
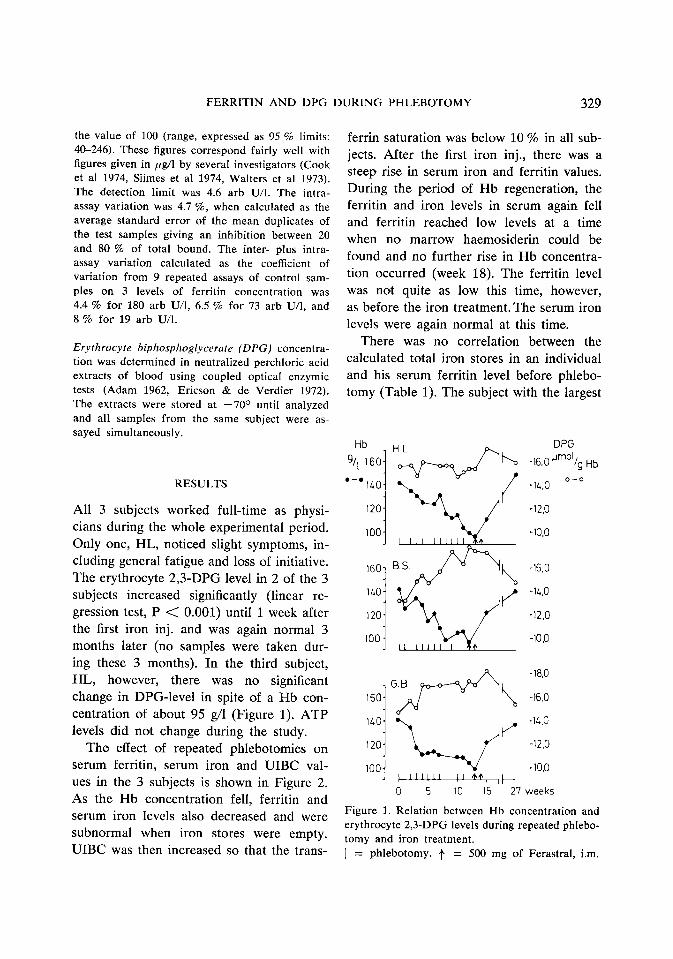
All 3 subjects worked full-time as physi- cians during the whole experimental period. Only one, HL, noticed slight symptoms, in- cluding general fatigue and loss of initiative. The erythrocyte 2,3-DPG level in 2 of the 3 subjects increased significantly (linear re- gression test, P < 0.001) until 1 week after the first iron inj. and was again normal 3 months later (no samples were taken dur- ing these 3 months). In the third subject, HL, however, there was no significant change in DPG-level in spite of a Hb con- centration of about 95 g/1 (Figure 1). ATP levels did not change during the study.
The effect of repeated phlebotomies on serum ferritin, serum iron and UIBC val- ues in the 3 subjects is shown in Figure 2. As the Hb concentration fell, ferritin and serum iron levels also decreased and were subnormal when iron stores were empty. UIBC was then increased so that the trans-
140-
120-
100 -
ferrin saturation was below 10 % in all sub- jects. After the first iron inj., there was a steep rise in serum iron and ferritin values. During the period of Hb regeneration, the ferritin and iron levels in serum again fell and ferritin reached low levels at a time when no marrow haemosiderin could be found and no further rise in Hb concentra- tion occurred (week 18). The ferritin level was not quite as low this time, however, as before the iron treatment. The serum iron levels were again normal at this time.
There was no correlation between the calculated total iron stores in an individual and his serum ferritin level before phlebo- tomy (Table 1). The subject with the largest
-18.0
-16.0
-1L.O
-12.0
-10.0
0 5 10 15 27 weeks
Figure 1. Relation between Hb concentration and erythrocyte 2,3-DPG levels during repeated phlebo- tomy and iron treatment. I = phlebotomy. f = 500 mg of Ferastral, i.m.

330 BIRGEGARD, HOGMAN, KILLANDER, LEVANDER, SIMONSSON, WIDE
I L O j ( 500mg iron i.m
120 Hb I g'l
Se 300.'
200- !
100-
50-
20-
UIBC
1
0
D a
0 3 6 9 12 15 18 21 24 27weeks * a * * * * . * .
0 0 Ph'ebo- 0 , 0 0 0 0 0 0
tomy 0 0 a n m m n D
Figure 2. The effect of repeated phlebotomies and iron treatment on Hb concentration, serum iron, UIBC and serum ferritin levels in the three subjects. 0 = GB, 0 = BS, 0 = HL.
calculated iron pool, HL, had the lowest serum ferritin, 75 arb UA. The relation be- tween the fenitin levels of the subjects was kept throughout the study.
DISCUSSION
Previous studies showing a negative correla- tion between Hb concentration (or red cell mass) and red cell DPG demonstrate great

FERRlTlN AND DPG DURING PHLEBOTOMY 331
TABLE 1 Serum ferritin values before phlebototny and calculated totol iron stores in the 3 subjects
HL 75 750 BS 130 522 GB 180 666
individual variations (Valeri & Fortier 1969). Slawsky et a1 (1972) found a poor correlation between individual values of DPG and the Hb concentration in iron deficient anaemias. In the present longi- tudinal study, the DPG pattern during pro- gressive bleeding anaemia was different in the 3 volunteers. In 2 of them the DPG level mirrored the Hb level rather well whereas in the third person, no DPG in- crease was seen during a 12-week period. This subject was the one who had the highest initial DPG level and he was also the only one who noticed any symptoms. Any causal relationship between these facts is of course only speculative.
Two previous investigations of ferritin levels during phlebotomy have been re- ported. Walters et al (1973) compared pre- phlebotomy ferritin values and calculated iron stores and found a close correlation. He expressed this relation as an equation and stated that ‘direct measurement of a segment of the body ferritin pool appears to give a valid indication of total iron body stores both in normal subjects and in those with iron deficiency and iron overload. The present data suggest that 1 ltg of ferritin per 1 of serum represents about 8 mg of storage iron’.
However, it is obvious from their own results that there is a wide range of varia- tion in serum ferritin values between sub-
jects with the same calculated amount of storage iron. For instance, 5 subjects with about 300 mg of storage iron vary between 25 and 125 ;cg/l in serum ferritin, and 5 subjects with a serum ferritin level around 50 p g A vary between 150 and 600 mg in calculated iron stores.
In the second phlebotomy experiment presenting ferritin values (Jacobs et a1 1972), the authors do not attempt to cal- culate a fixed ratio between ferritin values and iron stores. The figures given for pre- phlebotomy ferritin levels and calculated iron stores do not indicate the existence of such a ratio.
Our results support the view that the se- rum ferritin level is not correlated to ab- solute iron stores in a way to permit quan- titation of these stores in an individual from a single ferritin value within the nor- mal range. The correlation seems to be close enough, however, to make it pos- sible to distinguish groups of subjects with varying iron stores (Jacobs et a1 1972, Wal- ters et a1 1973, Birgegird et a1 1977). The present study shows that serum ferntin levels reflect changes in iron stores in an individual during a controlled experiment. This indicates that a change in the magni- tude of an individual’s iron stores can be detected if repeated serum ferritin estima- tions are made. Irrespective of the initial level, serum ferritin reached subnormal levels in all 3 subjects when iron stores were depleted. This supports the view that true iron deficiency can be reliably detected by serum ferritin estimations. We feel that it is important to make these distinctions to avoid undue importance being given to single ferritin values which fall within the normal range.
Figure 1 shows that UIBC falls after the iron inj. The fall is rather slow, however,
332 BIRGEGARD, HOGMAN, KILLANDER, LEVANDER, SIMONSSON, WIDE
and even though the serum iron is high, there is some unsaturated transferrin. The explanation is probably that the iron- sorbitol gluconic acid injected is a very stable compound, having a slow exchange of iron, and that the preparation is free from iron ions.
There was a sharp rise in serum ferritin values after parenteral iron treatment. This rise was temporary and probably reflected the induction of ferritin synthesis caused by iron (Linder & Munro 1973, Zahringer et a1 1976, Millar 1975). Serum ferritin then fell and stabilized at a level between 50 and 70 % of the initial level in each individual. At this time, the serum iron was normal, but there was no stainable marrow haemo- siderin. The Hb concentration did not con- tinue to rise, in spite of the fact that pre- phlebotomy levels still had not been reached. The absence of marrow haemosiderin and the halt in Hb rise indicate that iron defi- ciency had again developed, this time be- cause of the iron consumption in the pro- cess of restoring Hb concentration to nor- mal levels. However, serum ferritin levels were within the normal range, and the rea- son for this is uncertain.
Marrow haemosiderin staining is a rather insensitive measure of iron stores and small amounts of stored iron may have been present even if the staining was negative. The calculated utilization of the iron prepa- ration given was high, about 70 % (Simons- son et a1 1977). During the first 3 d after inj., 15-20 % of the iron was excreted in the urine. There are no reliable figures in the literature for iron absorption from food during parenteral iron treatment. It is prob- ably low, though, hardly more than 1 mg/d. It is, therefore, unlikely that there were other than very small iron stores during this period. This raises the question of
whether serum ferritin levels at this time reflect iron stores or were still influenced by the recent enhancement of synthesis, caused by the iron inj. Further reason is thereby given for being cautious in the clinical evaluation of a single ferritin value within the normal range.
ACKNOWLEDGEMENTS
This study was supported by grants from the Swedish Medical Research Council and National Defence Research Institute, Stockholm, Sweden.
REFERENCES
Adam H (1962) Adenosin-5-trifosfat. In H-U Berg- meyer (ed) Methoden der enzymatischen Ana- lyse, pp 539-58. Verlag Chernie, Weinheim.
Anderson N S E & Grafford K (1976) Studies on an iron poly (sorbitol gluconic acid) complex for parenteral use in man. In J Fielding (ed) Symposium on Ferastral. Scand J Haematol, Suppl.
Birgeggrd G , Hogman C, Killander A & Wide L (1977) Serum ferritin levels in male blood donors. Vox Sang 5 (in press).
Bothwell T H & Finch C A (1968) Iron losses in man. In G Blix (ed) Occurrence, causes and pre- vention of nutritional anaemias. Symp VI, pp 104-12. Swedish Nutrition Foundation. Alm- quist & Wiksell, Uppsala.
Cartwright G E & Wintrobe M M (1949) Chem- ical, clinical and immunological studies on the products on human plasma fractionation. XXXIX. The anaemia of injection. Studies on the iron binding capacity of serum. J Clin Zn- vest 28, 86-98.
Cook J D, Lipschitz D A, Laughton Ch, Miles E M & Finch C A (1974) Serum ferritin as a measure of iron stores in normal subjects. A m J Clin Nutr 27, 681-87.
Eaton J W & Brewer G J (1968) The relationship between red cell, 2,3-diphosphoglycerate and levels of Hb in the human. Proc Nat Acad Sci (Wash) 61, 756.
Ericson A & de Verdier C-H (1972) A modified method for determination of 2,3-diphospho-

FERRITIN AND DPG DURING PHLEBOTOMY 333
glycerate in erythrocytes. Scand J CIin Lab In-
Halliday J W, Gera K L & Powell L W (1975) Solid phase radioimmunoassay for serum ferri- tin. Clin Chim Acta 58, 207.
Heilmeyer L & Plotner K (1937) Das Serumeisen und die Eisenmangelkrankheit. Fischer-Verlag, Jena.
Hjelm M (1969) The content of 2,3-diphospho- glycerate and some other phosphocompounds in human erythrocytes from healthy adults and subjects with different types of anaemia. For- svarsmedicin 5, 219-26.
Jacobs A, Miller F, Wonvood M, Beamish M R & Wardrop C A (1972) Ferritin in the serum of normal subjects and patients with iron defi- ciency and iron overload. Brit Med J 4, 206-08.
Linder M C & Munro H N (1973) Metabolic and chemical features of ferritin, a series of iron- inducible tissue proteins. Am J Pathol 72, 263- 82.
Lindvall S & Anderson N S E (1961) Studies on a new intramuscular haematinic iron sorbitol. Br J Pharmacol 17, 358.
Millar J (1975) Subcellular localization of iron during accelerated ferritin synthesis. FEBS Let- ters 59, 198-202.
Norrby A (1974) Iron absorption studies in iron deficiency. Scand J Haematol 10, Suppl No 20.
Porter F S (1974) The effect of iron content on the behaviour of human ferritin in an inhibi- tion-type radioimmunoassay. J Lab Clin Med
Prieto J, Barry M & Sherlock S (1975) Serum ferritin in patients with iron overload and with acute and chronic liver diseases. Gastroenterol
vest 29, 85-90.
83, 147-52.
68, 525-33.
Siimes M A, Addiego J E & Dallman P R (1974) Ferritin in serum: diagnosis of iron deficiency and overload in infants and children. Blood 43,
Simonsson B, Birgeglrd G, Killander A & Levan- der H (1977) Ferastral treatment of the three healthy phlebotomized males. Scand J Haematol (in press).
Slawsky Ph & Desforges J F (1972) Erythrocyte 2,3-diphosphoglycerate in iron deficiency. Arch Int Med 129, 914-17.
Stauffer C E & Greenham C C (1976) Sources of error in measuring ferritin. CIin Chem 22, 1755.
Thomas I11 F H M, Lefrak S S, Irwin R S, Fritts Jr H W & Caldwell P R B (1974) The oxy- hemoglobin dissociation curve in health and dis- ease. Role of 2,3-diphosphoglycerate. A m J Med 57, 331-48.
Torrance J, Jacobs P, Restrepo A, Eschbach J, Lenfant C & Finch C A (1970) Intraerythrocytic adaptation to anaemia. N Engl J Med 283, 165.
Valeri C R & Fortier N L (1969) Red-cell-mass deficit and erythrocyte 2,3-DPG levels. For- svarsmedicin 5, 212-18.
Walters G 0, Miller F M & Wonvood M (1973) Serum ferritin concentration and iron stores in normal subjects. J Clin Pathol 26, 77&72.
Wide L & Birgegird G A (1977) A solid phase radioimmunoassay for serum ferritin using l=I- labelled femtin. Uppsala J Med Sci 82, 15-19.
Zahringer J, Baliga B S & Munro H N (1976) Novel mechanism for translational control in regulation of ferritin synthesis by iron. Proc Nat Acad Sci 73, 859-61.
581-90.