sero-survey of equine infectious anemia, glanders and
TRANSCRIPT

SERO-SURVEY OF EQUINE INFECTIOUS ANEMIA, GLANDERS AND PIROPLASMOSIS IN FIVE
DRAUGHT EQUINE POPULATED URBAN AREAS OF PUNJAB
Thesis submitted in partial fulfillment of the requirements for the degree of
DOCTOR OF PHILOSOPHY
In
Clinical Medicine & Surgery
By
MUHAMMAD HAMMAD HUSSAIN D.V.M., M.Sc. (Hons.) CMS
FACULTY OF VETERINARY SCIENCES UNIVERSITY OF AGRICULTURE
FAISALABAD, PAKISTAN
October 2011

To, The Controller of Examinations, University of Agriculture, Faisalabad We, the supervisory committee, certify that the content and form of thesis submitted
by Mr. Muhammad Hammad Hussain, Reg. No. 95-ag-1001 have been found satisfactory
and recommend that it be processed for evaluation by the External Examiner(s) for the award
of degree.
SUPERVISORY COMMITTEE
Chairman ___________________________ (Prof. Dr. Ghulam Muhammad)
Member ___________________________ (Prof. Dr. Ijaz Javed Hassan)
Member ___________________________ (Prof. Dr. Muhammad Siddique)
DEDICATION
I would love to dedicate this manuscript to my loved ones: my
loving family, mentors, special friends and loves of my life. All
are truly the bright stars in my life.

i
ACKNOWLEDGEMENTS
I bend myself modestly in front of Almighty ALLAH the Lord of the worlds, the
Omnipotent, the Beneficent, the Merciful and the Gracious and thank Him for everything I have
been blessed with in my life. Peace and blessing of Allah be upon Holy Prophet Hazart
Muhammad (Peace be Upon Him), the Apostle of Allah, the greatest social reformer, and who is
the forever source of knowledge.
My deep sense of gratitude for my Supervisor, Prof. Dr. Ghulam Muhammad,
Department of Clinical Medicine & Surgery, for his dynamic supervision, auspicious guidance and
keen interest during my research work.
I express my profound sense of appreciation to Dr. Ijaz Javed Hassan, Professor
Department of Physiology & Pharmacology, for his technical guidance, constructive criticism and
needful help during the course of my study.
I am feeling dearth of words to express my gratitude and appreciation to Dr. Muhammad
Siddique (Late), Professor of Microbiology, for providing valuable suggestions, competent guidance
and boosting up my morale during the conduct of this study.
With deep emotions of benevolence and gratitude, I offer my appreciation to Prof. Dr.
Laeeq Akhtar Lodhi, (Dean FVS) for his skilful and ever inspiring intelligent guidance, absolute
friendly atmosphere during the completion of this project.
This work was supported in part by the University of Agriculture, Faisalabad through
provision of financial grant. I am extremely thankful to The Brooke Hospital for Animals,
Pakistan and especially Dr. M. Saleem, Leader, The Brooke Project, Faisalabad for provision of
support regarding collection of samples from Lahore, Gujranwala, Faisalabad and Multan.
I am sincerely and earnestly indebted to my parents, family members, beloved wife
daughter, son and friends who have always wished to see me glittering high on the skies of success.
(Muhammad Hammad Hussain)
Comment [D1]: He is dean now???

ii
List of Table
S. No. Title of the Table Page No.
Table-3.1
Sampling plan for the sero-survey of equine infectious anemia, galnders and piroplasmosis in 5 draught equine populated urban areas of Punjab 30
Table-1
Geographic and climatic characteristics of the 5 draught equine populated urban areas of Punjab selected for sero-survey of equine infectious anemia, glanders and piroplasmosis
44
Table-2 Reported equine population targeted for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
44
Table-3 Areas and equine type related distribution of samples (n=430) taken for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
48
Table-4 Sex related distribution of samples (n=430) taken for sero-survey of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
48
Table-5 Age related distribution of equines (n=430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
49
Table-6 Housing pattern observed in equines (n=430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
51
Table-7 Watering pattern used at work and home by the owners of equines (n=430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
51
Table-8 Number of equine owners practicing tick, fly and mosquito control measures in 5 draught equine populated urban areas of Punjab sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis.
52
Table-9 Hematological values recorded in equines (n=430) surveyed for sero-prevalence of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
57
Table-10 Comparison of hematological values recorded in horses (n=65), mules (n=33) and donkeys (n=332) sampled for sero-prevalence of equine infectious anemia, glanders and piroplasmposis in 5 draught equine populated urban areas of Punjab
58

iii
S. No. Title of the Table Page No.
Table-11 Comparison of hematological values found in male (n=295) and female (n=135) equines sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
59
Table-12 Comparison of hematological values found in 3 different age groups of equines sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
59
Table-13 Comparative Seroprevalence of equine glanders in 5 draught equine populated urban areas of Punjab 65
Table-14 Frequency of clinical signs in RBT positive (n=34) equines of 5 draught equine populated urban areas of Punjab sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis
66
Table-15 Comparative age related seroprevalence of glanders in equines (n=430) of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
67
Table-16 Sex related seroprevalence of glanders in equines (n=430) of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
68
Table-17 Haematological values in equines found sero-positive for glanders (n=34) in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
69
Table-18 Housing pattern observed in Rose Bengal Plate Agglutination Test (RBT) positive (n=34) and negative (n=396) equines surveyed for the seroprevalence of glanders in 5 draught equine populated urban areas of Punjab
70
Table-19 Prevalence of glanders in association with watering habits of owners (n=430) of 5 draught equine populated urban areas of Punjab surveyed for the seroprevalence of equine infectious anemia, glanders and piroplasmosis
70
Table-20 Bivariable analysis for predicting glanders in equines sampled from 5 draught equine populated urban areas of Punjab 72
Table-21 SPSS output of binary logistic regression analysis for predicting glanders in equines sampled from 5 draught equine populated urban areas of Punjab
73
Table-22 Seroprevalence of piroplasmosis in equines (n=430) of 5 draught equine
populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
77

iv
S. No. Title of the Table Page No.
Table-23 Clinical findings in the equines (n=430) of 5 draught equine populated
urban areas of Punjab found sero-positive (n=226) for piroplasmosis (T. equi and B. caballi)
78
Table-24 Seroprevalence of Theileria equi in the equines surveyed for the seroprevalence of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
79
Table-25 Comparative age related seroprevalence of T. equi infection in equines of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
80
Table-26 Comparative sex related dynamics of Theileria equi infection in 5 draught equine populated urban areas of Punjab surveyed for seroprevalence of equine infectious anemia, glanders and piroplasmosis
81
Table-27 Seroprevalence of Babesia caballi infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
84
Table-28 Comparative age related seroprevalence of B. caballi infection in 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
84
Table-29 Comparative sex related dynamics of Babesia caballi infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
85
Table-30 T. equi and B. caballi mixed infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
88
Table-31 Seroprevalence of T. equi and B. caballi mixed infection in 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
88
Table-32 Age related seroprevalence of mixed infection with Theileria equi and Babesia caballi in equines of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
89
Table-33 Sex related prevalence of mixed infection with Theileria equi and Babesia caballi in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
89
Table-34 Hematological values of horses found positive (n=53) for piroplasmosis in 5 draught equine populated urban areas of Punjab
94

v
S. No. Title of the Table Page No.
Table-35 Hematological values of donkeys found positive (n=191) for piroplasmosis in 5 draught equine populated urban areas of Punjab 95
Table-36 Hematological values of mules found positive (n=26) for piroplasmosis in 5 draught equine populated urban areas of Punjab 96
Table-37 Comparison of hematological values in equines (n=226) found positive for piroplasmosis in 5 draught equine populated urban areas of Punjab 97
Table-38 Comparison of housing pattern of equines (n=430) found positive (n=226)
and negative (n=204) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
102
Table-39 Seroprevalence of piroplasmosis with reference to presence of ticks on the cohorts in equines found positive (n=226) and negative (n=204) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
103
Table-40 Seroprevalence of piroplasmosis with reference to tick control practiced in equines found positive (n=226) and negative (n=204) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
104
Table-41 Preferred treatment protocol adopted by veterinarians and animal health workers (n=100) of 5 draught equine populated urban areas of Punjab in suspected cases of equine piroplasmosis
105
Table-42 Bivariable analysis for the seroprevalence of T. equi in equines (n=177) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
106
Table-43 SPSS output of binary logistic regression model for predicting T. equi infection in equines (n=177) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
107
Table-44 Bivariable analysis for the seroprevalence of B. caballi in equines (n=93) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
108
Table-45 SPSS output of binary logistic regression model for predicting B. caballi infection in equines (n=93) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
109
Table-46 Bivariable analysis for the seroprevalence of mix infection with T.equi and B. caballi in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
110

vi
S. No. Title of the Table Page No.
Table-47 SPSS output of binary logistic regression model for predicting mix infection with T.equi and B. caballi in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
111
Table-48 Bivariable analysis for the seroprevalence of piroplasmosis in equines (n=226) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
112
Table-49 SPSS output of binary logistic regression model for predicting piroplasmosis in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
113

vii
List of Figures
S. No. Title of the Figures Page No.
Figure-1
Map showing global distribution of equine infectious anemia (EIA) during last six months (July – December) of 2008
12
Figure-2 Map showing global distribution of equine glanders during last six months (July – December) 2008
17
Figure-3 Map showing the global distribution of equine piroplasmosis during last six months (July – December) of year 2008
25
Figure-4 Google maps showing the 5 sampled draught equine populated urban areas of province, Punjab, Pakistan
31
List of Plates
S. No. Title of the Figures Page No.
Plate-I Photograph showing the commercial ELISA kit (VMRD, Inc., USA) used for the serodiagnosis of equine infectious anemia
35
Plate-II Photograph showing the 96 well microtitration plate after completing the assay ready for visual determination and interpretation through plate ELISA reader
35
Plate-III Photograph showing the strong positive results of rose Bengal plate agglutination test for equine glanders
37
Plate-IV Photograph showing the micro-titration plate of commercial cELISA (VMRD, Inc., USA) used for the serodiagnosis of equine piroplasmosis during the study: Visual Determination
40
Plate-V Photograph showing the communal water troughs used by the draught equine owners during working hours
71
Plate-VI Photograph showing the communal water troughs used by the draught equine owners in the communal equine housings
71
Plate-VII Photograph showing the communal housing pattern used by owners of draught donkeys in the study areas
114
Plate-VIII Photograph showing the roof type being used in the construction of the communal draught equine housing systems in the study area
115
Plate-IX Photograph of tick infestation on the medial aspect of the thigh in a horse sampled during the study
116
Appendix
Title Page No.
Proforma for the recording of information regarding reo-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
168

CONTENTS
Acknowledgement ----------- i
List of Table ----------- ii
List of Figures ----------- vii
List of Plates ----------- vii
Appendix ----------- vii
CHAPTERS TITLE PAGE
1 INTRODUCTION 1
2 REVIEW OF LITERATURE 7
3 MATERIALS AND METHODS 28
4 RESULTS 42
5 DISCUSSION 117
6 SUMMARY 141
LITERATURE CITED 145 APPENDIX 168
________________________________________________

ABSTRACT
A cross-sectional epidemiological survey was conducted to check the seroprevalence of 3
reportable equine diseases viz., equine infectious anemia (EIA), glanders, and piroplasmosis
in 5 draught equine populated urban areas (Lahore, Gujranwala, Faisalabad, Multan and
Bahawalpur) of Punjab. Assuming the expected prevalence to be 50 percent (unknown status)
with confidence limits of 95% and a desired absolute precision of 5%, a total of 430 blood
and sera (comprising 332 donkeys, 65 horses and 33 mules) along with relevant information
were randomly collected. The samples were subjected to microscopic examination (thin and
thick Giemsa stained smears), hematological analysis and commercial enzyme linked
immunosorbant assay (ELISA). Sera were tested for EIA through ELISA (VMRD, Inc.,
USA), for glanders through rose Bengal plate agglutination test (RBT) and a commercial
competitive ELISA (cELISA, VMRD, Inc., USA) was used for piroplasmosis screening.
Positive and negative samples were identified on the basis of degree of agglutination (++ to
++++ considered positive) in case of RBT and as per instructions of the manufacturer
regarding ELISAs. Data thus generated was analyzed by using epidemiological software tools
(Epiinfo™, WINPEPI, Survey Toolbox and IBM SPSS). Results: Giemsa stained smears
were negative for blood parasite. None of the samples was positive for EIA, indicating
towards possible disease free status or failure of the disease to mount immune response in
sampled equine population. Seroprevalence of glanders was found to be 7.9% (n=34) with
highest prevalence in Lahore (11.6%) followed by Bahawalpur (10.3%), Multan (7.3%),
Faisalabad (6.7%) and Gujranwala (5.3%). Significantly different (P<0.05) seroprevalence
was recorded in horses (16.9%) than mules (12.1%) and donkeys (5.7%). Seroprevalence
recorded in young (< 5 years), adult (< 10 years) and old (> 10 years) equines was 7.9%,
9.2% and 5.2% respectively. Prevalence was significantly different (P<0.05) in males 5.7%
and female 12.59% equine. Multivariable analysis indicated that female equines (OR = 2.3,
95% CI= 1.16–4.77) and and those sharing water sources or access to communal water
troughs (OR =2.7, 95% CI=0.93-7.86) were more likely to be sero-positive for glanders.
Seroprevalence of piroplasmosis was found to be 52.5% (T. equi=41.2% and B.
caballi=21.6%; P<0.05) in the selected areas. Forty four (10.2%) sera were found positive for
both piroplasms (mixed infection). Significantly higher (P<0.05) seroprevalence was
recorded in Lahore (95.6%, n=66) than Faisalabad (64%, n=96) than Multan (52.9%, n=36),

Gujranwala (50.7%, n=38) and Bahawalpur (50%, n=34). Seroprevalence of piroplasmosis
was 69.2% in horses (T. equi=56.9%, n=37; B. caballi=24.6%, n=16) followed by 63.6% in
mules (T. equi 48.5%, n=16; B. caballi 30.3%, n=10) and 48.2% in donkeys (37.3%, n=124).
Adjusted analysis for possible confounding factors revealed that equines living alone or with
equine cohorts (OR=1.30, 95%CI=0.84–2.01), with ticks infested equine cohorts (OR=1.19,
95%CI=0.65-2.18) whose owners did not practice tick control (OR=1.43, 95%CI=0.93-2.21)
were more likely to be sero-positive for piroplasmosis. Hematological alterations observed in
RBT (glanders) positive equines regarding white blood cell counts, red blood cell counts,
hemoglobin concentrations and hematocrit in all there RBT positive equine species.
Macrocytic hyperchromic type of anemia was observed in all RBT positive horses, mules and
donkeys. Hematological analysis of piroplasmosis positive equines indicated decreased white
blood cell counts, red blood cell counts PCV and hemoglobin concentration values in
seropositive horses, donkeys and mules. Erythrocytic indices pointed towards microcytic
hyperchromic type of anemia in piroplasmosis sero-positive equines. In conclusion, the high
RBT based prevalence of equine glanders indicates towards possible endemic nature of this
disease in Pakistan. Potential role of communal water sources and faulty management in the
spread of equine glanders requires further investigations through carefully designed
experimental studies. Seroprevalence of piroplasmosis was alarmingly high in the selected
population which could be attributed to the faulty housing, lack of tick control practiced by
owners and lacuna regarding knowledge among animal health professionals about the correct
diagnosis and treatment of T. equi and B. caballi.

Chapter-I (Introduction)
1
CHAPTER-I
INRODUCTION
Equines have had deep, influential and enduring effects on human civilizations that started with
the domestication and then riding of the horse. And in an amazing way, they completely,
dramatically and almost instantaneously changed the face of the world. Among many purposes of
these animals, draught is the most beneficial use for mankind. A number of equine breeds are used
for draught purposes with the variation being largely geographic. Draught equines are versatile
breeds used today for a multitude of purposes, including draught equine showing, farming and
pneumatic cart pulling etc. These animals share the traits of strength, stamina, health, longevity,
patience and a docile temperament which made their presence vital to generations of pre-industrial
farmers.
The importance of equines in Pakistan is well known. According to Pakistan Livestock
Census (Anonymous, 2006) total equine population of Pakistan is about 4.77 millions. Major
proportion of equidae in Pakistan includes 4.2 million donkeys, 0.15 million mules and 0.34
million horses. About 33.33% donkey, 64.66% mule and 60.61% horse population is kept for non-
agricultural (mostly draught) purpose. These animals provide livelihood to the rural societies
living in arid, semi-arid and hilly regions through transport and draught. Whereas, a considerable
population of equines serves the purpose of transport as well as draught in the big industrial
metropolises, a small population of equines is used in army, police, racing industry and sports.
Equines like all other domestic species are susceptible to a variety of infectious diseases.
Chances of spread of infectious as well as vector born diseases are more in draught equine
population of urban areas where the contact among affected and healthy animals is frequent and

Chapter-I (Introduction)
2
inevitable. Spread of infectious diseases could occur through common feeding and watering
utensils, insect vectors and use of contaminated instruments for health as well as managemental
purposes (Radostits et al., 2007). Epidemiological studies are of utmost importance in these
congested areas with high disease pressure to develop health and management packages for the
better exploitation of equine resources. Managemental practices contributing to the spread of
diseases can be identified through such studies.
As alluded earlier, like all other species, equines can become victim of many conditions
caused by various pathogens of viral, bacterial and parasitic origin. Among these diseases, equine
infectious anemia, glanders and piroplasmosis are placed in the List B of equine diseases by
World Animal Health Organization formerly known as ‘Office Internationale Des Epizooties’
(OIE) and transport/export of horses from the countries having pockets of these OIE reportable
diseases are strictly prohibited (OIE , 2004).
The equine infectious anemia (EIA) is a potentially fatal viral blood borne disease of
family Equidae i.e., horse and horse family (Ishii and Ishitani, 1975; Higgins and Wright, 1993;
Radostits et al., 2007). Disease is caused by EIA virus of subfamily Lentiviridae of family
Retroviridae and is a close relative to Human Immunodeficiency Virus (HIV) (Montaginer et al.,
1984; Nakajima and Sugiura, 1994).
After getting infected, equines may exhibit one of the three clinical states of the disease i.e.
acute, chronic and inapparent. Inapparent carries are the animals mostly found positive on the
basis of serological diagnosis and pose same threat as infected horses to equine community,
because environmental and managemental stresses and indiscriminate use of steroids are known to
induce recurrence of EIA (Issel et al., 1990). Concerning EIA, no treatment or vaccination is

Chapter-I (Introduction)
3
available till now and stringent implementation of ‘test and destroy’ policy (OIE, 2004) is the only
control method available.
A scientifically validated diagnostic test is sine qua non for control and eradication of a
disease. For the serodiagnosis, many tests have been developed and implemented but among those
agar gel immuno diffusion (AGID) and enzyme liked immuno-sorbant assay (ELISA) were found
to be simple and reliable (OIE, 2004). Both the tests have their own pros and cons but use of
ELISA in prevalence studies is found to be more convenient and fruitful (Winston et al., 1987;
Pearson and Gipson, 1988; Cordes and Issel, 1996).
Equine infectious anemia has been reported from many countries of the world including
India (Uppal and Yadav, 1989; Singh et al., 1997). Although, vectors (horse fly and mosquito)
responsible for the transmission of EIA do occur in Pakistan, the occurrence of this disease has not
yet been reported. Documentation of presence or absence of EIA is important for equine health
planning as well as attaining disease free status to facilitate the export of these animals.
Glanders is another OIE list B respiratory disease of horse and akin thereto. It is caused by
gram negative bacteria Burkholderia mallei (Rotz et al., 2002). B. mallei is a host adapted parasite
(Waag and DeShazer, 2004) but it has also been reported in man (Srinivasan et al., 2001) and
other animal species (Smith et al., 1990). Glanders was a major cause of death in horses from
Middle Ages onward and as late as World War-I. It was found to be associated with fatal
secondary infections in humans (Wilkinson, 1981).
Glanders can occur in four different clinical forms viz. nasal, pulmonary, cutaneous
(Farcy) and pulmuno-cutaneous. Clinically, this disease is characterized by nasal discharge with or
without nasal septum ulcers, dyspnoea, nodules/ulcers on the body, and lymphadenitis /
lymphangitis. Transmission occurs through nasal or cutaneous discharge of clinically diseased

Chapter-I (Introduction)
4
animals, by aerosol routes and through communal water trough system by contamination
(Radostits et al., 2007).
Field diagnosis of glanders is made on clinical grounds by observing the signs and mallein
test. Mallein testing has several pitfalls. Firstly, it gives false positive results. Secondly, it is
difficult to conduct under field conditions and thirdly it requires 48 hours for measuring outcome
of the test. Over the years, many diagnostic tests viz., complement fixation test (CFT), indirect
hemagglutination test (IHA), modified-counter immuno electrophoresis test (mCIET), Rose
Bengal plate agglutination test (RBT) and enzyme-linked immunosorbant assay (ELISA) have
been developed for the sero-diagnosis of glanders and used in many seroprevalence based studies
on the disease. Falling back on the gold standard test (i.e. isolation of B. mallei) is not possible in
non-clinical cases (Naureen et al., 2007).
Although, stringent implementation of ‘test and slaughter’ policy have successfully
eradicated glanders from most of the developed parts of the world like USA, Canada, UK, and
Australia (Derbyshire, 2002), reports indicate that the disease is still prevalent in many developing
countries (Al-Ani, et al., 1998; Mota et al., 2000; Sabirovic et al., 2005; Witting et al., 2006)
including Pakistan (Naureen et al., 2007). Even though the incidence of disease is thought to be
much higher, only a few prevalence studies based on clinical cases and covering only very small
area have been conducted in Punjab (Nasreen, 1977; Vaid, 1981; Bashir, 1984). Need of the hour
is to conduct some prevalence studies to estimate the current status of glanders in Pakistan
(Muhammad et al., 1998, Saqib et al., 2003; Naureen et al., 2007).
Equine piroplasmosis, caused by Theileria equi and Babesia caballi (Knowles, 1988;
Friedhoff et al., 1990; Radostits et al., 2007; Zinora et al., 2007) is an emerging equine disease
worldwide (Shkap et al., 1998; Uilenberg, 2006; Vial and Gorenflot, 2006). The disease can occur

Chapter-I (Introduction)
5
in chronic to per acute forms, with T. equi causing more severe infections and signs as compared
to B. equi which usually exhibit chronic disease. Disease is transmitted through ticks of three
genera viz., Dermacentor, Rhipicephalus and Hyaloma (Yoshihara, 1997; Uilenberg, 2006; Vial
and Gorenflot, 2006).
Conventional diagnosis is based upon the demonstration of organisms in the Giemsa
stained blood smears under microscope (Knowles, 1988) or through transmission tests (Ali et al.,
1996). For the serological diagnosis, many tests are used viz. complement fixation test (Donnelly
et al., 1980; Weiland, 1986), indirect fluorescent antibody test (Zinora et al., 2007), enzyme linked
immunosorbant assay (Chahan et al., 2006), latex agglutination test (Xuan et al., 2001),
polymerized chain reaction (Alhassan et al., 2005), DNA Probes (Posnett and Ambrosio, 1989;
Posnett and Ambrosio, 1991) and loop-mediated isothermal amplification (LAMP) test (Alhassan
et al., 2007a; Alhassan et al., 2007b).
Throughout the world, disease is controlled through the therapeutic as well as prophylactic
use of imidocarb dipropinate and diminazine (Radostits et al., 2007; Vial and Gorenflot, 2006) and
implementation of tick (vector) control measures. To date, no vaccine is available for this disease
and for the proper eradication of disease stringent implementation of ‘test and slaughter policy’ is
advocated by Office International Des Epizooties, OIE (2004).
Not only the prevalence but also the presence of vector (ticks) of this important equine
disease is well established in our neighboring country India (Malhotra et al., 1978; Ali et al.,
1996; Ambawat et al., 1999). Although, we share almost similar climatic and geographic
conditions with India and prevalence of potential tick vectors is also reported from different areas
of Pakistan, our knowledge about the disease is limited to only a few studies based upon
conventional blood smear examination (Kokab, 1986; Khan et al., 1987). In view of the foregoing,

Chapter-I (Introduction)
6
there is a need to conduct some well-planned epidemiological studies to know the prevalence of
this disease and review our current control methods.
Adequate resources and careful planning are major components for conducting meaningful
prevalence studies for a disease. In resource poor countries like Pakistan, where funds for
screening of animal populations for the presence of a single disease are usually scarce, planning of
such study will require proper allocation of resources, suitable and practical sampling frame and
use of recent and cost effective epidemiological documentation tools on which our future studies
can be built. To address the problem of finances in resource poor economies, it is advisable that
wherever possible multiple disease prevalence methods should be adopted to determine the
incidence / prevalence of different diseases by using a single sample taken from single species of
animal.
Keeping the aforesaid in view, and considering lacunae regarding equine infectious anemia,
glanders and piroplasmosis in Pakistan, the present study has been planned with the following
objectives:
I. Define the exposure of equines in the selected areas to EIA, glanders and piroplasmosis
II. Determination of hematological alterations (if any) associated with these diseases
III. Determine the association of such host determinants as the age, breed and sex (if any) with
the occurrence of these diseases
IV. Investigate the possibility of attaining disease free status regarding EIA for the areas under
study
V. Conceptualize the control measures for these disease by analyzing epidemiological data
generated by the survey

CHAPTER-II (Review of Literature)
7
CHAPTER-II
REVIEW OF LITERATURE
I. Justification for the epidemiological surveys:
Draught horses, mules and donkeys not only pull the loads but also help sustain the livelihood of
their owners and families. Any disease or disability rendering these animals sick and unavailable
for work can have some serious effects on owner and his family. Draught work can also act as a
stress factor in these animals, reducing resistance to many diseases prevalent in the area
including infectious as well as many endoparasitic problems. Moreover, chances of spread of
infectious and vector borne diseases are more as these animals come in frequent contact with
each other through communal watering troughs, common feed mangers and at the rest stations.
In Pakistan, most of the draught equines survive in a sub-optimal productive state owing to stress
of diseases on one hand and poor nutrition on the other. That’s why any effort to increase their
productivity (draught power) under the situation can upset their physiological equilibrium and
lead to catastrophic results. Thus, exploitation of draught power from these animals is possible
only when diseases are brought under full control.
Among the two standard methods of disease management viz., control and eradication, disease
control is the only scientifically realistic or economically feasible method. This makes epidemic
disease control a desirable method for the developing world (Burridge, 1981). By performing
some meaningful epidemiological studies on epidemic diseases, most prevalent diseases can be
checked through some proven methods of control including identification and treatment of cases
and carriers, removal of reservoirs of infection, quarantine, sanitary measures and mass
immunization programs (Lawrence et al., 1993).

CHAPTER-II (Review of Literature)
8
II. Equine infectious anemia
II.a. The disease and the organism
Equine infectious anemia (EIA) is a blood borne, chronic viral disease of the Equidae. Clinically,
the disease is manifested by persistent infection with recurrent viremia cycles and fever episodes,
anemia, edema and weight loss (Cheevers and McGuire, 1985; Sellon et al., 1994; Radostits et
al., 2007). EIA virus has great historic significance because this was the first retrovirus proven to
be transmitted through insects (Stein et al., 1942), the first persistent virus for which ‘antigenic
drift’ was defined (Kono, 1972) and the first retrovirus disease for which a diagnostic test viz.,
Coggins Test was recommended (Coggins et al., 1972).
The disease can manifest itself in three forms viz., acute, chronic and inapparent. In rarely seen
severe acute form, the clinical signs are non-specific with elevated rectal temperature and
affected horse may die within 2-3 weeks. Usually the clinical picture of disease is variable with
many haematological and biochemical alterations like anemia, thrombocytopenia,
hypergammaglobinemia and elevated liver enzymes (Spyrou et al., 2003; Leroux et al., 2004;
Cullinane et al., 2007; Radostits et al., 2007). The animals often recover and remain carriers
throughout their life. Recovered animals may suffer from recurring clinical (chronic) disease,
which manifests itself with the signs of fever (105-108 °F), petechial hemorrhages, depression,
weight loss, dependent edema and anemia. This form is caused by new mutant EIAV strains
(Kono, 1972; Payne et al., 1987) and affected equine is often termed as “swamper” (Clabough et
al., 1991). The disease is more detrimental in its inapparent form as it poses the real threat to
other healthy horses. These carriers show negligible or no clinical signs and suffer from constant
viremia and thus may spread infection to other horses through biting insects and hypodermic

CHAPTER-II (Review of Literature)
9
needles etc., (Cordes and Issel, 1996). No seasonal, sex or age based association could be
ascertained on the basis of previous studies (Radostits et al., 2007).
II.b. Geographic distribution
Equine infectious anemia is worldwide in distribution (OIE, 2004) and since 2005 disease was
reported with/without clinical signs in 40 countries. According to World Animal Health
Database (Anonymous, 2008), during 2008, EIA has been reported at different levels in 20
countries (Canada, Chile, Costa Rica, Cuba, Denmark, Finland, Georgia, Greece, Iran, Ireland,
Israel, Lebanon, Mexico, Netherlands, Portugal, Russia, Spain, United Kingdom, United States
of America and Uruguay). During past few years, authors have reported the varying degree of
prevalence of EIA from different regions of world (Pare and Simard, 2004; Bicout et al., 2006;
Menzies and Patterson, 2006; Reynolds, 2006). A continuous surveillance is required to establish
and maintain the disease free status in a country as demonstrated by few Turkish workers (Turan,
et al., 2002; Ataseven and Arslan, 2005; Kirmizigȕl et al., 2009). It is feared that actual incidence
of EIA is more than our estimate, as many countries are still not conducting seroprevalence
studies to rule out or confirm the disease.
In Pakistan, to date, only one study regarding the investigations of EIA is available (Gill et al.,
2008), which indicates towards the possible disease free status of equines in Faisalabad
metropolis. In our neighbouring country (India), incidence of EIA is documented since the first
case was detected at Karnatika in 1987 (Uppal and Yadav, 1989). Since then the disease has been
reported from the states of Maharashtra, West Bengal, Haryana, Dehli and Indian Punjab as well
(Singh et al., 1997). Clinical disease has also been reported from neighbouring Islamic Republic
of Iran during recent years (Anonymous, 2008).

CHAPTER-II (Review of Literature)
10
II. c. Diagnostic methods
Since the first description of diseases in 1843, many diagnostic techniques (precipitin test,
hemagglutination, immune adherence, indirect hemagglutination and serum protein and lipid
changes) were used for the diagnosis of EIA but the confirmed serological diagnosis remained a
big issue until the development of Coggins test. Coggins and co workers (1972) developed an
agar gel immunodiffusion (AGID) test for the diagnosis of EIA. This test detects the
precipitating antibodies against group reactive and antigenically stable core protein p26 (Payne et
al., 1984). This test has stood the test of time and the positive AGID test result is reliable and
confirms virus presence (Issel and Cook, 1993). Like all the serological tests, the AGID has its
own limitations. For instance, horses suffering from the disease first time and tested with AGID
can test negative for antibodies. This can also be seen in cases of foals acquiring colostral
passive immunity from EIA test positive dams. The results can be obtained within 24-48 hrs
(Issel and Cook, 1993). Since 1972, this test has been used as a gold standard in many
comparative test evaluation and prevalence studies on EIA (OIE, 2004).
Enzyme-linked immunosorbent assay (ELISA) has been used since late 1980s for faster and
more sensitive serodiagnosis (Issel and cook, 1993). A more sensitive competitive ELISA
(cELISA) has been developed to detect antibodies against core p26 protein and investigators
have found a good correlation between AGID and cELISA (Soutullo et al., 2001; Piza et al.,
2007). As compared to AGID, the ELISA test is rapid and results are easier to interpret (Uppal
and Yadav, 1992; Issel and Cook, 1993; Cordes et al., 2001; Cullinane et al., 2007; Piza et al.,
2007; Susan et al., 2008). The chances of getting false positive results are more with ELISA as
compared to AGID as it is less specific. For this reason, OIE recommends that all ELISA
positive samples should be confirmed by performing AGID test. However, the low levels of p26

CHAPTER-II (Review of Literature)
11
antigen in the sample attained from horses suffering from initial bots of clinical disease can only
be detected through ELISA and often yield negative AGID test results (Cullinane et al., 2007;
Piza et al., 2007). Whenever rapid test results are needed, disease status is unknown and horses
are present at remote location, the ELISA becomes the test of choice (Issel and Cook, 1993;
Cullinane et al., 2007; Piza et al., 2007). Furthermore, ELISA also can be employed as an
international pre-movement screening test because of its sensitivity and rapidity (Cullinane et al.,
2007). Other techniques like immunoblot test and PCR have also been developed for the
diagnosis of EIA but their use is limited as a research tool only (Issel and Cook, 1993).
II.d. Treatment and control
To date no vaccine and cure is available for the EIA (OIE, 2004) and the control of disease
depends upon wide scale testing in population at risk and destruction / immobilization of infected
horses (Issel and cook, 1993; OIE, 2004; Issel et al., 2005). Disease has only been controlled in
developed countries through rigorous testing and destruction. For example, during the past two
and a half decades, the USA equine owners contributed about 600 million dollars for testing and
control of EIA which shows the amount of personal and financial efforts required to control the
disease. Vaccine development against EIA virus is still a great challenge (Issel et al., 2005).
As the disease has been present in neighbouring countries (India and most recently in Iran) to
whom we share porous borders and vectors (fly and mosquito) also exist in Pakistan, some
carefully planned prevalence studies are needed to confirm the disease status regarding EIA in
Pakistan.

CHAPTER-II (Review of Literature)
12
Figure-1 Map showing global distribution of equine infectious anemia (EIA) during last six months (July – December) of 2008 (Anonymous, 2008)

CHAPTER-II (Review of Literature)
13
III. Glanders
III.a. The disease and the organism
Glanders is an anciently known disease of equids and has been described by Hippocrates
between 450 B.C. and 425 B.C. and a century later by Aristotle who named the infection
malleus, a Latin word for a malignant disease or epidemic (Minett, 1930). Apart from equines,
the organism can also cause disease in domestic and wild felids, dog, sheep & goat and camel
(Al-Ani and Roberson, 2007; Gregory and Waag, 2007). The disease is caused by Burkholderia
mallei (previously known as Loefflerella mallei, Pfeifferella mallei, Malleomyces mallei,
Actinobacillus mallei, Bacillus mallei and Pseudomonas mallei, (OIE, 2004). Burkholderia
mallei is Gram-negative, rods with rounded ends, 2-5 µ long and 0.5 µ wide, often stain
irregularly, and do not have capsules or form spores. B. mallei may have bipolar staining ‘safety
pin’ (Songer and Post, 2005). Capsular polysaccharide acts as an essential virulence factor for
this organism (Lopez et al., 2003). The organism produces toxins (extra-cellular enzymes) which
disrupt host cellular functions include pyocyanin, lecithenase, collagenase, and, lipase.
Pyocyanin interferes with terminal electron transfer, whereas lecithenase, collagenase, and lipase
are lytic in their action (Songer and Post, 2005). Recently, Russian workers (Narbutovich et al.,
2005) reported plasma coagulase (a thermostable enzyme) activity of natural and mutant strains
of B. mallei and B. pseudomallei. However, their exact role in pathogenesis is unknown.
There are three clinical forms of glanders viz., nasal, pulmonary and cutaneous (farcy) and the
course of disease may be acute, sub-acute or chronic (Hartwigk and Gerber, 1986). Furthermore,
an apparently carrier status (latent infection) is maintained by the recovered animals (Al-Ani and
Roberson, 2007; Gregory and Waag, 2007) that can result in to transmission of disease to
equines and humans. Spread of the organism can be due to direct contact through aerosol droplet

CHAPTER-II (Review of Literature)
14
and indirectly though contaminated feed, water and grooming utensils (Neubauer et al., 2005;
Al-Ani and Roberson, 2007: Gregory and Waag, 2007). Pulmonary form is observed in
practically all cases of the disease (Al Ani et al., 1998). The acute form of glanders occurs most
frequently in donkeys and mules (Udall, 1939; Hayes, 1968) and is often fatal within a month or
so (Minett, 1959). Davies (1955) proposed that in mules the course of disease is sub-acute as the
susceptibility of the mules seems to be mid way that of the horse and donkey. Chronic form of
disease usually occurs in horses (Dungworth, 1993) and animal remains sick for months then
dies or becomes carrier (Hungerford, 1990).
Acute glanders begins with chill and high fever of 106 to 108 °F (Udall, 1939). It is clinically
characterized by attacks of coughing, mucoid nasal discharge from one or more rarely both
nostrils, inspiratory dyspnoea, pneumonia, rapidly developing ulcers on nasal mucosa and
enlargement of submaxillary lymph nodes (Cole, 1942; Dalling, 1966; Hartwigk and Gerber,
1986, OIE, 2004; Radostits et al., 2007). Death occurs within a few days due to septicaemia (Al-
Ani, et al., 1987; Radostits et al., 2007).
Chronic form of the disease develops as a sequel to either clinical infection or non-fatal acute
cases and is manifested by progressive loss of body weight, a ‘run down appearance’ and
unthrifty hair coat (Al-Ani et al., 1998; Al-Ani and Roberson, 2007) and these chronically
infected equines are known reservoirs of disease in nature (Neubauer et al., 2005). In chronic
infection, nasal and skin forms commonly occur together. When the localization is chiefly
pulmonary, there is chronic cough, frequent epistaxis, laboured breathing, and febrile episodes.
Inflammatory nodules and ulcers develop in the nasal passages and give rise to a sticky yellow
discharge from one or both nostrils, accompanied by enlarged firm submaxillary lymph nodes
(OIE, 2004; Al-Ani and Roberson, 2007; Radostits et al., 2007; Saqib et al., 2008). In skin form

CHAPTER-II (Review of Literature)
15
(Farcy), lesions may occur in any part of body, but are more commonly present on areas exposed
to injury, such as hind legs (Dalling, 1966). In a collaborative study, a neurologic form of
glanders has been proposed in which equines had developed cross-stepping of hindquarters.
However, B. mallei could not be demonstrated in nervous tissue (Lopez et al., 2003).
The course of disease is usually acute in donkeys and horses usually suffer from chronic and
inapparent form of the disease, whereas the disease could manifest itself in both acute and
chronic forms in mules. (Al-Ani et al., 1998; Al-Ani and Roberson, 2007; Gregory and Waag,
2007). Risk of acquiring glanders found to be higher in old age animals and animals older than 2
years of age are more susceptible (Radostits et al., 2007; Al-Ani and Roberson, 2007). However,
some studies report that equines can get the disease at any age (Al-Ani et al., 1998; Saqib, 2003).
Hematological alterations associated with glanders are reported as marked increase in white
blood cell counts, anemia, below normal PCV and haemoglobin concentration (Saqib 2000;
Manso, 2003; Al Ani and Roberson, 2007; Saqib et al., 2008).
Overcrowding, unhygienic conditions, draught stress, contact with infected equines, sharing of
feed and water troughs and poor nutrition make the equine more susceptible to the glanders as
the chances of spread through infectious secretions are more from one animal to other under
these conditions (Henning, 1956, Al-Ani et al., 1987; Jerabek, 1994, Nagal et al., 1995;
Muhammad et al., 1998; Manso, 2003; Neubauer et al., 2005; Al-Ani and Roberson, 2007;
Gregory and Waag, 2007). Water can become contaminated with B. mallei through a diseased
equine and organism can remain there for the weeks to come (Gangulee et al., 1966; Al-Ani and
Roberson 2007; Gregory and Waag, 2007; Radostits, 2007). Glanders in equines can occur in
any season but mostly cases were reported in association with cold weather (Manso, 2003; Saqib
et al., 2003; Al-Ani and Roberson, 2007; Gregory and Waag, 2007).

CHAPTER-II (Review of Literature)
16
III.b. Geographic distribution
Aggressive control measures have essentially eradicated glanders from most of the developed
countries such as USA, Canada, UK, and Australia (Derbyshire, 2002). However, the disease is
prevalent in developing countries like Pakistan (Muhammad et al., 1998; Saqib et al., 2003;
Naureen et al., 2007; Naureen et al., 2008), India (Verma et al., 1990; Pawaiya and Chauhan,
2008), Iraq (Al-Ani, et al., 1998), China (Ma et al., 1986), Iran (Bazargani et al., 1996), United
Arab Emirates (Sabirovic et al., 2005; Witting et al., 2006), Brazil (Mota et al., 2000; Manso,
2003) and Turkey (Arun et al., 1999). The disease has been reported from Brazil, Eriteria, India,
Iran, Mangolia, Pakistan, Russia and Philippines between 2006 and 2008 (Anonymous, 2008).
A recent outbreak in India after almost 2 decades started in 2006 with clinical disease was
reported from Maharashtra, Uttar Pradesh, Punjab and Uttarakhand provinces (Pawaiya and
Chauhan, 2008). Disease outbreak has also been reported in equines of Lahore Polo Club,
Pakistan (Naureen et al., 2008). This recrudescence of disease in India and Pakistan could be
attributed to meager pittance (about Rs. 50 per equine in Pakistan) given to the glanders positive
equine owners for killing their animals (Muhammad et al., 1998; Saqib et al., 2003; Pawaiya and
Chauhan, 2008). This has forced the poor equine owners to avoid reporting any signs of the
disease to veterinarians and authorities, hiding of clinically affected equids to avoid testing,
selling of suspected or chronically infected equines to un aware persons belonging to some other
community or cities to compensate their economic losses (Muhammad et al., 1998; Saqib et al.,
2003; Gregory and Waag, 2007; Pawaiya and Chauhan, 2008; Saqib et al., 2008).

CHAPTER-II (Review of Literature)
17
Figure-2 Map showing global distribution of equine glanders during last six months (July – December) 2008

CHAPTER-II (Review of Literature)
18
III.c. Diagnostic methods
The mallein test is a corner stone for the diagnosis of equine glanders. The mallein is purified
protein derivative (PPD), available commercially. It is a solution of water-soluble protein
fractions of heat-treated Burkholderia mallei cells (OIE, 2004). Mallein test can be performed by
following three different methods: (i). intradermo–palpebral mallein test (ii). Opthalmic test (iii).
Sub-cutaneous Mallein test (OIE, 2004).
Mallein test has been widely and effectively used for the diagnosis of glanders but has
limitations in terms of sensitivity, particularly in clinical and advanced cases of the disease (Jana
et al., 1982; Verma, 1981; Neubauer et al., 2005). Indian workers (Misra and Arora, 1990) have
found serological cross-reactions between Pseudomonas mallei (old name of B. mallei) and some
other bacteria, whereas Iraqi workers (Al-Ani et al., 1993) encountered false positive mallein
reaction, particularly between B. mallei and Streptococcus equi (Strangles) infection. Also, the
mallein testing of glanders negative equines have been reported to yield positive CFT test results
for these animals (Hagebock, et al., 1993; Neubauer et al., 2005; Gregory and Waag, 2007). The
serological tests used for diagnosis of glanders include complement fixation test (Higgins and
Wright, 1998), micro-complement fixation test (Verma, 1990), avidin-biotin dot enzyme-linked
immunosorbent assay (Verma et al., 1990), micro–enzyme–linked immunosorbent assay (Al–
Ani et al., 1993), arrayed immunoblotting mehod (Katz et al., 1999), competitive enzyme-linked
immuno-assay (Katz et al., 2000), agglutination and precipitin tests (Gillespie and Timoney,
1981), counter immunoelectrophoresis (Jana et al., 1982), haemagglutination test (Gangulee et
al., 1966), haeagglutination inhibition tests, indirect haemagglutination test (Zhang and Lu,
1983; Ferster et al. 1986), Rose Bengal plate agglutination test (Naureen et al., 2007) and latex
agglutination test (Saqib et al., 2008).

CHAPTER-II (Review of Literature)
19
The complement fixation test (CFT) is reported to be 90 – 95 % sensitive but has its own
limitations especially regarding the sera from donkey, mule and pregnant mares having anti
complementary characteristics (Gregory and Waag, 2007). In the wake of limitations of CFT and
other serological tests, there is a need to develop tests using well characterized antigens to avoid
false positive results (Neubauer et al., 2005).
III.d. Treatment and control
Treatment of glanders is forbidden in countries where ‘Glanders and Farcy Act - 1899’ is
implemented. In Pakistan, legislation calls for detection and destruction of glanderous animals
(Farani, 1983). However, an incredibly low indemnity paid to the owners does not oblige or lure
them to let their animals be destroyed. As a salvage measure, equine owners sell their animals at
reduced price that leads to spread of disease in new areas (Muhammad et al., 1998). The
organism is sensitive to aminoglycosides, sulfonamides, tetracyclines and, quinolones,
nitrofurones and resistant to early ß-lactams and colistin, metronidazole, cephalexin (Darling and
Woods, 2004).
Experimental chemotherapy of glanders has been performed in equines, hamsters, guinea pigs,
and monkeys (Miller et al., 1948; Batmanove, 1991; Batmanove, 1993; Batmanove, 1994;
Iliukhin, et al., 1994; Manzeniuk et al., 1994; Muhammad et al., 1998; Russel et al., 2000;
Manzeniuk, 1995). Saqib and colleagues (2003) have reported an experimental cure of equine
glanders with a combination of enrofloxacin and trimethoprim + sulfadiazine with a 21-day
treatment protocol. In a recent case of laboratory-acquired glanders (Srinivasan et al., 2001), the
patient received imipenem and doxycycline intravenously for 1 month followed by oral
azithromycin and doxycycline for 6 months. This treatment regimen was successful and there
was no relapse of the disease. However, there is as yet no consensus recommendation for

CHAPTER-II (Review of Literature)
20
treatment of human/animal glanders, although there is extensive literature on antibiotic
susceptibility of B. mallei (Al-Ani and Roberson, 2007; Gregory and Waag, 2007).
Lack of stern implementation of Glanders and Farcy Act (1899) had made glanders a major
concern in Pakistan because of high incidence in endemic areas and the disease is thought to be
quite prevalent in many areas of Pakistan. To date, only a few prevalence studies based on the
screening of clinical cases have been conducted in Punjab (Nasreen, 1977; Vaid, 1981; Bashir,
1984). Glanders is an emerging disease and as such the cause of a serious concern for animal
health monitoring authorities and there is a dire need to conduct a seroprevalence study to
establish the current prevalence of this disease in Pakistan (Muhammad et al., 1998, Saqib et al.,
2003, Naureen et al., 2007).
IV. Equine Piroplasmosis
IV.a. The disease and the organisms
Equine Piroplasmosis is a tick borne protozoan disease of horse family (Knowles, 1988;
Friedhoff et al., 1990; Radostits et al., 2007; Zinora et al., 2007). The disease is caused by
hemotropic protozoa viz. Theileria equi and Babesia caballi and regarded as an emerging equine
disease all over the world (Shkap et al., 1998; Vial and Gorenflot, 2006; Uilenberg, 2006). The
disease was previously known as ‘Babesiosis’ but due to the recent research developments some
basic differences (extra-erythrocytic shizogony in T. equi) were found between the life cycles of
parasites resulting in the change in status of B. equi as Theileria equi (Vial and Gorenflot, 2006;
Zinora et al., 2007).
Incubation period of the diseases varies from 12-19 days for T. equi and 10-30 days for B. cabali.
T. equi infected animals usually exhibit more severe and acute form of disease as compared to B.
cabali infections which usually follows the chronic course (Shkap et al., 1998; Vial and

CHAPTER-II (Review of Literature)
21
Gorenflot, 2006; Radostits et al., 2007). Clinically, the disease can be categorized in four
different forms viz., peracute, acute, chronic and rare atypical forms. In peracute cases the
animals are usually found in moribund conditions or found dead. Fever, anorexia, depression,
icterus, hemoglobinuria, colic, regenerative hemolytic anemia and dissemminated intravascular
coagulopathies (DIC) are usually seen in acute form of piroplasmosis (Seifi et al., 2000;
Camacho et al., 2005).
Most common heamatological alterations associated with priplasmosis are Hemolytic anemia,
thrombocytopenia and decrease in hematocrit (PCV) values (De Waal et al., 1992; Taboada and
Merchant, 1991; Camacho et al., 2005). Significantly less hematocrit (PCV) was reported in non-
clinical seropositive horses as well by Camacho et al. (2005). Significantly lower RBC counts
and anemia was found to be more significantly associated with T. equi infected horses by
Camacho et al. (2005). T. equi is more virulent than B. caballi and results in more consistent
hemoglobinuria and death, while B. caballi causes persistent syndrome characterized by fever
and anemia (Henry, 1992; Camacho et al., 2005)
Chronic form of the disease usually follows the acute phase and observed clinical picture is
debility, loss of condition and exercise intolerance but most of the times these clinical signs
cannot be ascertained (Akkan et al., 2003) in case of serological studies. Sometimes a rare
atypical form is also seen with signs of gastro-enteritis, bronchopneumonia and abortions (Vial
and Gorenflot, 2006; Radostits et al., 2007).
Equines born and raised in the endemic areas enter into the carrier state of the disease which
compromises their draught potentials considerably (Abdelkebir et al., 2001). These carrier
animals are responsible for the maintenance of infection in endemic areas (Camacho et al.,
2005). Heavy draught stress, strenuous exercise and poor nutrition may results in to the

CHAPTER-II (Review of Literature)
22
recrudescent infection and clinical disease in these animals (Hailat et al., 1997; Seifi et al., 2000;
Camacho et al., 2005). Spleen is responsible for the immune response against hemoparasites and
its removal results in recrudescence of latent hemoparasitic infections, therefore, splenectomy
results in acute and fatal disease in case of clinically normal carrier animals (Abdelkebir et al.,
2001).
Ticks of three genera (Dermacentor, Rhipicephalus and Hyaloma) are responsible for the spread
of piroplasmosis all over the world (Ali et al., 1996). In ticks sexual reproduction of these
organisms takes place and they can transmit the disease trans-stadially and transovarially.
Iatrogenic spread of the disease can also occur through contaminated blood transfusion,
injections and surgical instruments (Yoshihara, 1997; Uilenberg, 2006; Vial and Gorenflot,
2006). Clinically, piroplasmosis should be differentiated from equine infectious anemia, surra,
dourine, African horse sickness and plant poisoning (Ali et al., 1996; Vial and Gorenflot, 2006;
Radostits et al., 2007).
Horses are more susceptible for B. caballi infections as compared to mules and donkeys (Acici et
al., 2008) and susceptibility to disease is directly proportional to the age of animal (Abdelkebir et
al., 2001). The chances of contracting T. equi infections were found more in donkeys then horses
and mules by Abdelkebir et al. (2001) but a recent study in Turkey contradict this finding were
T. equi infection was found least prevalent in donkeys (Acici et al., 2008). Only a handful of
authors have suggested sex dependent prevalence of B. caballi and T. equi (Shkap et al., 1998;
Rüegg et al., 2007). However, no such difference is reported based upon the sex of the equines
by many authors (Olivera and Garcia, 2001; Asgarali, et al., 2007; Karatepe et al., 2009).

CHAPTER-II (Review of Literature)
23
Various prevalence studies carried out to in the different regions of the world found that
prevalence of the T. equi increases with age of equines (Brüning, 1996; Oliver and Garcia, 2001;
Asgarali, et al., 2007; Rüegg et al., 2007; Karatepe et al., 2009). However, some authors did not
agree upon any difference between prevalence of T. equi and B. caballi according to age of
equines (Tenter et al., 1988; Shkap et al., 1998; Acici et al., 2008).
The higher prevalence of T. equi as compared with B. caballi, is mostly reported in the endemic
regions of the world (Barbosa et al., 1995; Ribeiro et al., 1999; Akkan et al., 2003; Boldbaatar et
al., 2005; Camacho et al., 2005; Asgarali, et al., 2007; Salim et al., 2008; Karatepe et al., 2009).
Which could be due to the fact the infections with T. equi are usually for life (Schien, 1988;
Rüegg et al., 2007; Rüegg et al., 2008) and B. caballi infections usually clear from the host in 1-
5 years (Rüegg et al., 2007; Rüegg et al., 2008). Prevalence of piroplasmosis can differ with
reference to locations as demonstrated by various studies based upon the differences found in the
climatic / geographic conditions, vector population, draught stress and equine keeping practices
(Heuchert et al., 1999; Skhap et al., 1998; Acici et al., 2008; Salim et al., 2008; Karatepe et al.,
2009). But selection of areas with similar geographic, climatic and equine management attributes
may lead to prevalence findings independent of locations (Abdelkebir et al., 2001; Chahan et al.,
2006).
Managemental conditions that favor the spread of T. equi includes congested and confined
housing resulting in the increased transtadial intrahost transfer among vectors and subsequently
transmission (Abdelkebir et al., 2001).

CHAPTER-II (Review of Literature)
24
IV.b. Geographic distribution
About 90% of world equine population lives in the areas endemic for equine piroplasmosis
(Schein, 1988) and this is an emerging threat worldwide. Since 2006, the incidence of disease
has been reported from 31 countries of the world. During 2008, the incidence disease has been
reported in equines from Argentina, Belize, Bolivia, Brazil, Chile, Colombia, Costa Rica,
Greece, Israel, Jordan, Malta, Martinique (France), Mexico, Morocco, Myanmar, Peru, Portugal,
Qatar, Russia, South Africa, Spain, Suriname, Switzerland, United Kingdom, USA, Uruguay,
and Zimbabwe (Anonymous, 2008).
Piroplasmosis is endemic in china, Brazil, Central Mangolia (Xuan et al., 2001), Morocco
(Abdelkebir et al., 2001), Tranidad (Asgarali, et al., 2007), Iran (Seifi et al., 2000), Spain
(Camacho et al., 2005). Various prevalence studies indicated sero-reactivity in Mangolia (88-
84%), South Africa (61-40%), Colombia (94-90%), Sudan (91-86%), Brazil (81-90%), Morocco
(69%) and Israel (76-80%). Disease was also frequently reported from India (Malhotra et al.,
1978).
However, in high endemic areas the clinical form of disease is usually seen rarely (Pfeifer et al.,
1995). Japan is considered free from piroplasmosis because no clinical case has been reported to
date (Ikadai et al., 2002). In recent years, researchers all over the world are on the look for the
current prevalence of piroplasmosis in various regions (Akkan et al., 2003; Boldbaatar et al.,
2005; Camacho et al., 2005; Asgarali, et al., 2007; Acici et al., 2008; Karatepe et al., 2009;
Salim et al., 2008).

CHAPTER-II (Review of Literature)
25
Figure-3 Map showing the global distribution of equine piroplasmosis during last six months (July – December) of year 2008

CHAPTER-II (Review of Literature)
26
IV.c. Diagnosis
Diagnosis can be made by the demonstration of intra-erythrocytic parasites in Giemsa stained
blood smears which is rarely probing (Knowles, 1988; Weiland and Reiter, 1988; Shkap et al.,
1998; Akkan et al., 2003; Acici et al., 2008; Salim et al., 2008) in chronic forms of disease and
endemic regions where low prasitemia is usually observed (Calder et al., 1996; Salim et al.,
2008). Transmission test can be performed for the conformation by transfusing about 500 ml
anticoagulant mixed blood of suspected animal to disease free equines (Ali et al., 1996).
For the sero-diagnosis of piroplasmosis different tests have been developed over the years.
Complement fixation test (CFT) remained a gold standard for many years (Donnnelly et al.,
1980; Weiland, 1986) but due to its limitations regarding provision of false positive/negative
results, alytical ingredient production, anticomplementory activity of many sera and the inability
of IgG (T), the major immunoglobulin isotype of equids, to fix the complement forced scientific
community to develop new tests (Abdelkebir et al., 2001). A more sensitive and specific indirect
fluorescent antibody test (IFAT) was developed and used by many scientists (Amerault et al.,
1979; Callow et al., 1979; Donnelley et al., 1980; Ribeiro et al., 1999; Akkan et al., 2003;
Zinora et al., 2007) but the test is not efficient for use with a large number of sera (Abdelkebir et
al., 2001).
Keeping in view the requirements of surveillance and prevalence studies ELISA was developed
(Knowles et al., 1991; Shkap et al., 1998) which is more sensitive and specific (Abdelkebir et
al., 2001). Later on a much improved competitive ELISA was developed for the diagnosis and
reported to be best to use for epidemiological studies (Abdelkebir et al., 2001; Ikadai et al.,
2002; Damdinsuren et al., 2005; Chahan et al., 2006; Huang et al., 2006; Salim et al., 2008). On
the basis of successful demonstration of sensitivity and specificity in various studies (Knowles et

CHAPTER-II (Review of Literature)
27
al., 1991; Shkap et al., 1998; Katz et al., 2000), ELISAs which detect the antibodies to
geographically conserved region of piroplasms are now one of the recommended tests for
piroplasmosis (OIE, 2004). Other tests developed for the confirmation includes PCR based
assays (Kappmeyer et al., 1993; Ali et al., 1996; Zintl et al., 2003; Alhassan et al., 2005; Salim
et al., 2008), DNA probes (Posnett and Ambrosio, 1989; Posnett and Ambrosio, 1991), latex
agglutination test (Xuan et al., 2001) and recently developed loop-mediated isothermal
amplification (LAMP) test (Alhassan et al., 2007a; Alhassan et al., 2007b). Latix agglutination
test developed by Japanese workers (Xuan et al., 2001) by using recombinant T. equi merozoite
antigen 1 (EMA-I) have shown identical comparable results with ELISA and can be trialed and
employed as an onsite screening tool for diagnosing T. equi infections.
IV.d. Treatment and control
Both T. equi and B. caballi respond to the babesiacidal drugs but T. equi is more refrectory to the
treatment than B. cabali (Vial and Gorenflot, 2006). Imidocarb can be used for therapeutic as
well as chemoprophylactic purposes and appears to be a drug of choice for eliminating the
carrier state. Recommended dose regimens for the T. equi is 4 mg/kg repeated four times at 72 hr
interval and two treatments of 2.2 mg/kg at 24 hr interval (Vial and Gorenflot, 2006; Radostits,
2007). However, T. equi infections can only be suppressed by treatment but complete elimination
of this parasite is not possible (de Waal, 1992; Knowles, 1996).
Although a few workers have tried to make a reliable vaccine (Kumar, et al., 2002), till today, no
vaccination is available for the piroplasmosis. So continuous disease surveillance, control of
vector (tick) population and implementation of test and slaughter policy forms the mainstay of
control programs (Radostits et al., 2007).

CHAPTER-III (Materials and Methods)
28
CHAPTER-III
MATERIALS AND METHODS
1. Study locales and settings
The study was conducted in 5 draught equine populated urban areas of Punjab, Pakistan.
Selection of the areas was made on the basis of reported district draught equine population
equine population in Livestock Census (Anonymous, 2006). For making the study more
meaningful and demographically diverse, 3 areas from Central (Faisalabad, Lahore and
Gujranwala Metropolises) and 2 areas (Multan and Bahawalpur Metropolises) from Southern
Punjab were selected. Wherever possible, the study area selection took into account the
presence of working areas of ‘Brooke Hospital for Animals’ in the selected cities to seek the
necessary cooperation by the draught equine owners and convenient sampling. The study
period spanned over 8 months from July 2007 to March 2008.
2. Sampling frame
As the prevalence of the diseases under study was unknown in Pakistan, the sample size was
calculated by considering the expected prevalence to be 50% with confidence limits of 95%
and a desired absolute precision of 5% to take maximum numbers of samples (Thrusfield,
2005). Samples size was calculated on the basis of following formula:
n = 1.962 Pexp(1 – Pexp) / d2
Where:
n = required sample size
Pexp = expected prevalence
d = desired absolute percision

CHAPTER-III (Materials and Methods)
29
The number of samples thus calculated was subjected to the following formula for the
estimation of required sample size (nadj):
nadj = (N X n) / (N + n)
Where:
N = total population
n = calculated sample size through formula
Stratification of the sampling units was performed by proportional allocation of
sampling units to the draught equine population in the selected areas (Table-3.1). Random
selection methods were used for the selection of areas to be sampled within each city and the
simple random sampling was performed on-site.
3. Recording of information
Information regarding owner’s particulars, animal’s details, cohorts, management, problem
history, treatment and clinical examination for the diseases under consideration was obtained
on a pre-designed proforma (Appendix-I).
4. Complete physical and clinical examination
Physical and clinical examination was performed and values regarding vital physiological
parameters and observations were entered in the proforma designed for the said purpose.
5. Samples collection
Samples were collected by using sterile vacutainers and labeled accordingly for
identification. For the serum, 10mL blood was drawn into a clot activator vacutainer without
anticoagulant. For the whole blood specimen, 4mL blood was collected into an anticoagulant
(Ethylenediaminetetraacetic acid (EDTA) @ 1 mg/ml) coated vacutainer. Thin and thick
smears on clean glass slides were made on-site and labeled accordingly.

CHAPTER-III (Materials and Methods)
30
Table-3.1 Sampling plan for the sero-survey of equine infectious anemia, galnders and piroplasmosis in 5 urban areas of Punjab
Urban Area
Total Draught
Horse
% of total selected draught
horse population
Samples Taken
Total Draught Donkey
% of selected draught donkey
population
Samples Taken
Total Draught
Mule
% of selected draught
mule population
Samples Taken
Faisalabad 6645 34.91 18 44144 37.20 123 3046 40.52 9
Lahore 4596 24.15 13 17386 14.65 50 721 9.59 6
Gujranwala 4612 24.23 14 18964 15.98 55 1841 24.49 6
Multan 1940 10.19 10 19076 16.07 52 954 12.69 6
Bahawalpur 1238 6.50 10 19076 16.07 52 954 12.69 6
19031 65 118646 332 7516 33
Total Samples Taken = 430

CHAPTER-III (Materials and Methods)
31
Figure-4: Google™ Maps showing the 5 sampled draught equine populated urban areas of province, Punjab, Pakistan

CHAPTER-III (Materials and Methods)
32
6. Samples transportation
These samples were transported to the postgraduate research laboratory of the
Department of Clinical Medicine & Surgery, University of Agriculture, Faisalabad, while
observing the critical requirement of temperature (4°C).
7. Sample processing
Hematological examination
Whole blood samples were subjected to hematological examination for red blood cell
(RBC) count, hemoglobin concentration (Hb), white blood cell (WBC) count packed cell
volume (PCV) and erythrocytic indices as per methods described by Coles (1986).
Erythrocyte indices (MCV, MCH and MCHC) were calculated to classify the type of
anemia (Coles, 1986, Thrall, 2004)
Serum collection
Serum was collected by following the recommendations of Benjamin (1978) and stored at
-40°C till further processing.
Thin and thick blood smear examination
Microscopic examination of Giemsa (Merk, Germany) stained thin and thick smears
(Henry, 1996) was conducted for any evidence of blood parasities (B. caballi, T. equi and
Trypanosoma)
Sero-diagnosis of equine infectious anemia
For this purpose commercial equine infectious anemia virus antibody test kit, ELISA
(VMRD, Inc., Pullman, USA) was used (Abdelkabir et al., 2001). For the Sample
processing and application on the ELISA kit, following methods described by the
manufacturer were followed:

CHAPTER-III (Materials and Methods)
33
Preparation
a. Warming up reagents: the serum samples, reagents and plate(s) were brought to the
room temperature before starting the test procedure.
b. Positioning controls and samples: Positive and negative controls in duplicate were
placed on different wells of the plate with each run. Samples were first placed in to non-
antigen coated plate and then transferred with multichannel micropipettor to the antigen-
coated plate. The control and serum sample IDs were recorded on the attached setup
record sheet. Plates were removed from the foil pouch and brought at room temperature.
d. Preparation of conjugate: 1X antigen-peroxidase conjugate (D) was prepared by
diluting 1 part of 100X D with 99 parts of conjugate diluting buffer (E).
e. Preparation of wash solution: 1X wash solution was prepared by adding one part of
the 10X wash solution concentrate (F) in 9 parts of deionized water.
f. Preparation of serum samples: undiluted serum samples were used for test.
Test Procedure
1. Loading controls and serum samples: 50 μl of controls and serum samples were
pipette into the antigen coated plate. Side of the plate was tapped several times for
ensuring coating of samples to the bottom of the wells. 10 minutes incubation was given
at room temperature (21-25°C).
2. Washing of wells: after incubation plate was washed once using ELISA washer
3. Addition of antigen-peroxidase conjugate: 50 μl of diluted antigen peroxidase
conjugate was added to each well and side of well tapped several times to ensure proper
coating. Plate was incubated again for 10 minutes at room temperature (21- 25°C).

CHAPTER-III (Materials and Methods)
34
4. Washing of wells: After incubation plate was washed four times with the automated
ELISA plate washer.
5. Addition of substrate solution: Substrate Solution (50μl) was added to each well and
side of plate tapped several times to make sure the proper coating. Plate was incubated at
room temperature (21-25°C) for 15 minutes.
6. Addition of stop solution: 50 μl of stop solution was pipette into each well.
Immediately after addition of stop solution, change in color from blue to yellow was
observed. Side of the loaded assay plate was tapped several times for proper mixing.
7. Reading and recording the test result: After the addition of stop solution, the plate
was observed visually against the positive control and then on ELISA plate reader at
optical density (O.D.) reading wavelength 450nm. For the visual determination, any of
the test wells yielding colour development equal to the positive control serum was
considered positive and the wells showing colour development equal to or less than the
negative control serum was considered negative. Samples having O.D. greater than or
equal to that of positive control on microplate reader interpretation were considered
positive (Issel and Cook, 1993).

CHAPTER-III (Materials and Methods)
35
Plate-I Photograph showing the commercial ELISA kit (VMRD, Inc., USA) used for the serodiagnosis of equine infectious anemia Plate-II Photograph showing the 96 well microtitration plate after completing the assay ready for visual determination and interpretation through plate ELISA reader

CHAPTER-III (Materials and Methods)
36
Sero-diagnosis of glanders
Recently evaluated ‘Rose Bengal Plate Agglutination Test’ (RBT) was used for the
serodiagnosis of glanders. Antigen for the test was prepared as described by Naureen et
al. (2007). Briefly, 2 outbreak isolates present in the Department of Clinical Medicine &
Surgery, University of Agriculture, Faisalabad and China 5 strain were used for this
purpose. These were suspended in sterile phosphate buffer saline (PBH: pH 6.4) after
being evaluated for purity. Further these were used to seed the Roux flasks filled with
layers of glycerol-dextrose agar and incubated for one week at 37°C. Purity of the
growths were checked through Gram staining and harvesting was performed by adding
100 mL of phenol-saline (0.05% phenol in 0.85% sodium chloride solution). After gentle
agitation, the organisms were killed in water bath at 100°C by heating overnight. By
using the spectrophotometer, bacterial cell concentrations adjustment at 65 x 109 /
milliliter was performed and colored with Rose Bengal dye (1%). Centrifugation was
performed at 5,000 g for 20 minutes and re-suspension of sediment was performed in
NaOH lactic acid buffer (50mM, pH 3.5).
The test were performed as described by Naureen et al. (2007) and considered positive in
the presence of distinct agglutination with appearance of small or large rose-colored
flakes with 50 to 100% clarification of liquid (2–4 crosses) and negative if scored less
than 2 crosses.

CHAPTER-III (Materials and Methods)
37
Plate-III Photograph showing the strong positive (++++) results of rose Bengal plate agglutination test for equine glanders

CHAPTER-III (Materials and Methods)
38
Sero-diagnosis of equine piroplasmosis
Commercial Babesia caballi and Babesia equi antibody test kits, cELISA (VMRD, Inc.,
Pullman, USA) were used for this purpose (Abdelkabir et al., 2001). Sample processing,
application and interpretation were performed by following guidelines as provided by
manufacturer:
Preparation
a. Warming up reagents: Serum samples, reagesnts and plates were brought to the room
temperature (21-25°C)
b. Preparation of controls and samples: Serum samples, positive and negative controls
were diluted 1:2 with serum diluting buffer in non antigen coated transfer plates. Positive
and negative controls were run in duplicate and triplicate respectively on each plate.
Position of controls as well as serum samples was recorded on the setup record sheet.
d. Preparation of primary antibody: 1X primary antibody solution was made by
diluting 1 part of the 100X primary antibody with 99 parts of antibody diluting buffer.
e. Preparation of secondary antibody-peroxidase conjugate: 1X secondary antibody-
peroxidase conjugate was formed by diluting 1 part of the 100X secondary antibody-
peroxidase conjugate with 99 parts of antibody diluting buffer.
f. Preparation of washing solution: 1 part of the 10X wash solution concentrate was
diluted with 9 parts of distilled water to make 1X solution.
Test Procedure
1. Loading controls and serum samples: 50 μl of diluted controls and serum samples
were transferred to antigen coated plate through multichannel pipettor according to the
setup record. Loaded assay plate was tapped several times to ensure the proper coating of

CHAPTER-III (Materials and Methods)
39
solutions to the bottom of plate. Plate was then incubated for 30 minute at room
temperature (21-25°C).
2. Washing of wells: After incubation plate was washed 3 times by using an automatic
washer.
3. Adding primary antibody: Diluted 50 μl (1X) primary antibody was added to each
well and side of the loaded assay plate was tapped to ensure the proper coating of wells.
30 minutes incubation was provided at room temperature (21-25°C).
4. Washing of wells: Plate was washed 3 times after incubation in an automatic washer
5. Addition of secondary antibody-peroxidase conjugate: A 50 μl of diluted 1X
secondary antibody peroxidase conjugate was added to each well and side of well was
tapped to ensure proper coating. Plate was incubated at room temperature (21-25° C) for
30 minutes.
6. Washing of wells: Three times washing was performed after incubation
7. Addition of substrate solution: 50 μl of substrate solution was pipette in to each well
and side of well was tapped to make sure the proper coating of each well. Fifteen minutes
incubation was provided at room temperature (21-25°C)
8. Addition of stop solution: Stop solution (50 μl) was added to each well and side of
the well was tapped to ensure the mixing.
9. Reading and recording the test results: Plate reader was set at optical density (O.D.)
reading wavelength of 630 nm and plate was read.
10. Test Interpretation: Test was validated upon the points recommended by the
manufacturer and Percent inhibition (%I) was calculated by using the following formula:
Percent Inhibition (% I): = 100 - [(Sample O.D. x 100) ÷ (Mean Negative Control O.D.)]
Test sample producing ≥ 40% inhibition was declared positive and samples producing <
40% inhibition were considered negative.

CHAPTER-III (Materials and Methods)
40
Plate-IV Photograph showing the micro-titration plate of commercial cELISA (VMRD, Inc., USA) used for the serodiagnosis of equine piroplasmosis during the study: Visual Determination

CHAPTER-III (Materials and Methods)
41
Data analysis
Epidemiological data generated was analyzed by using the Epiinfo™ and other available
epidemiological softwares (WINPEPI; version 6.8 by J.H. Abramson; Survey Toolbox version
1.04 by Angus Cameron) to investigate different epidemiological attributes of these diseases.
Chi-square testing was performed to find out significant difference among sex, age and locations
based prevalence of the selected diseases. Univariate analysis was performed to calculate Odds
ratio (OR) for different determinants of disease. The associations between the outcome response
variables (sero-prevalence of EIA, glanders and piroplasmosis) and explainatory variables
(informations recorded through proforma) were estimated using binary logistic regression (IBM
SPSS Statistics 17.0 for Windows®, IBM Corporation, Route 100 Somers, New York, USA).
Individual animal was kept as unit of analysis for determining significance of association.
Outcome variables were dichotomized (0=negative and 1=positive) and response variables were
dichotomized or categorized wherever applicable. Bivariable screening was conducted and
variables yielding significant association at less than or equal 0.20 Wald P value were further
used in binary logistic regression model. A backward stepwise model was constructed. All
variables found significant in the initial screening model were kept at start and then based upon
likelihood ratio tests they were removed one by one. Hosmer-Lemeshow test, the Negelkerke R
square test and observed versus predicted values (Residual statistics) to identify outliers at 0.5
cut off point were used to assess the fit of the final models (Urdaz-Rodrihuez et al., 2009).

CHAPTER-IV (RESULTS)
42
CHAPTER-IV
RESULTS
For the current study 430 blood and serum samples were collected from 5 draught equine
populated urban areas (3 from central and 2 from southern Punjab) of Punjab to make the study
more diverse in terms of geography and climate. Geographic and climatic details of the studied
areas have been summarized in Table-1.
4.1. Geographic and Climatic Description of Selected Areas
Historical city of Lahore is the capital of province Punjab and the second largest city in Pakistan
with estimated population of 6.4 million people and population density of 3,566/km2. The city
lies 711 feet above the sea level with total land area of 404 km2 between 31°15′ and 31°45′ North
latitude and 74°01′ and 74°39′ East longitude. Weather of Lahore touches both extremes with
average maximum and minimum temperature in summer (May–July) can reach 36°C and 25°C
respectively, while in winter (December–February) temperature can drop to -1°C with average
maximum and minimum temperature of 19°C and 7°C respectively. The average annual rainfall
in Lahore is 452 mm.
With an estimated population of 2.7 million people the industrial city of Faisalabad is the third
largest city in Pakistan. Geographical coordinates of the city are 31°25′ North latitude and 73°05′
East longitude at an elevation of 605 feet above sea level. Climate of Faisalabad is extremely hot
in summer (mean maximum and minimum temperature, 39 and 27°C respectively) that may

CHAPTER-IV (RESULTS)
43
reach up to 50°C and at times drop below 0°C in winter (mean maximum temperature and mean
minimum temperature, 21°C and 6°C respectively) with average annual rainfall of 346 mm.
Gujranwala is the fifth largest city of Pakistan (estimated population 1.4 millions) and is located
700 feet above sea level at 32.16° North latitude and 74.18° East longitude. Climatic conditions
are extreme both in summer and winter with annual mean maximum temperatures of 30.9°C and
18.8°C respectively. Gujranwala receives 325 mm average annual rainfall.
One of the oldest inhabited cities of the world, ‘Multan’ with estimated population of 1.4
million people is the largest city in southern Punjab and sixth largest metropolis of Pakistan. The
city is situated between 30.12° North latitude and 71.27° East longitude about 710 feet above the
sea level. The city has extreme climatic conditions and temperature in summer can sear up to
52°C (mean maximum temperature 40.3°C) and fall up to -2°C (mean minimum temperature
5.8°C) in winter. The average annual rainfall in Multan is 127 mm.
City of Bahawalpur (Capital of former Princely State of Bahawalpur) lies 370 feet above sea
level and is situated between 25.59° North latitude and 73.19° East longitude. Bahawalpur
receives average 187 mm of rainfall annually. Climate is extremely hot in summer (mean
maximum temperature 40C and mean minimum temperature 28C) and milder (mean maximum
temperature 22C and mean minimum temperature 8C) in winter.

CHAPTER-IV (RESULTS)
44
Table-1 Geographic and climatic characteristics of the 5 draught equine populated urban areas of Punjab selected for sero-survey of equine infectious anemia, glanders and piroplasmosis
Metropolis Height from Sea Level (ft)
Geographic Coordinates Average Temperature
Latitude Longitude Summer °C Winter °C Av. Max.
Av. Min.
Av. Max.
Av. Min.
Lahore 712 31.55 74.34 36 25 19 7
Faisalabad 600 31.40 73.04 39 27 21 6
Gujranwala 744 32.16 74.19 38 24 21 6
Multan 710 30.18 71.47 40.3 23 27 5.8
Bahawalpur 370 29.37 71.68 40 28 30 14
Table-2 Reported equine population targeted for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab (Anonymous, 2006)
Area Sampled Horse Mule Donkey Total
Faisalabad 6645 3046 44144 53835
Lahore 4596 721 17386 22703
Gujranwala 4612 1841 18964 25417
Multan 1940 954 19076 21970
Bahawalpur 1238 954 19076 21268
Total 19031 7516 118646 145193

CHAPTER-IV (RESULTS)
45
4.2. Equine Population of Selected Areas
The total reported equine population providing draught power to the selected cities was 145,193
heads (Table-2). This population was comprised of horses (19031 heads), mules (7516 heads)
and donkeys (118646 heads) (Anonymous, 2006). Highest number of these equines dwelled in
Faisalabad (53,835 heads), followed by Gujranwala (25,417 heads), Lahore (22,703 heads),
Multan (21,970 heads) and Bahawalpur (21,268 heads). Donkey was the chief animal draught
power source in these areas as reported in Pakistan Livestock Census (Anonymous, 2006),
whose total population engaged in draught work in these areas was 118646 heads with highest
number reported in Faisalabad (44144 heads), followed by Multan and Bahawalpur (19076 heads
each), Gujranwala (18964 heads) and Lahore (17386 heads). According to Census (Anonymous,
2006), reported draught horses population in the study areas was 19031 heads (Table-2) which
was highest in Faisalabad (6645 heads), followed by Gujranwala (4612 heads), Lahore (4596),
Multan (1940 heads) and Bahawalpur (1238 heads). Total reported draught mule population of
targeted metropolises was 7516 heads. Highest number of mules engaged in draught work was
reported in Faisalabad (3046), followed by Gujranwala (1841 heads), Multan and Bahawalpur
(954 heads each) and Lahore (721 heads).
4.3. Demographic Characteristics of the Sampled Equine Population
4.3a. Locale and Equine Type Related Distribution of Samples
A total of 430 blood samples were collected from draught equines of areas under study (Table-
3). Depending upon the population proportion of each equine type, 332 donkeys, 33 mules and
65 horses were randomly sampled. Depending upon reported equine population of these areas

CHAPTER-IV (RESULTS)
46
(Anonymous, 2006), 150 equines (123 donkeys, 9 mules and 18 horses) from Faisalabad, 69 (50
donkeys, 6 mules and 13 horses) from Lahore, 75 (55 donkeys, 6 mules and 14 horses) from
Gujranwala, 68 (52 donkeys, 6 mules and 10 horse) each from Multan and Bahawalpur were
randomly selected and bled for blood and serum samples.
4.3b. Sex Related Distribution of Samples
Out of 430 equines sampled, 295 (68.6%) were male and 135 (31.4%) belonged to female sex
(Table-4). Blood and serum samples from 25 male horses (6 from Multan, 5 from Bahawalpur, 5
from Faisalabad, 4 from Lahore and 5 from Gujranwala) and 40 mares (4 from Multan, 5 from
Bahawalpur, 13 from Faisalabad and 9 each from Lahore and Gujranwala) were randomly
collected. Eighteen (18) male (3 from Multan, 2 from Bahawalpur, 6 from Faisalabad, 3 from
Lahore and 4 from Gujranwala,) and 15 female (2 from Gujranwala, 4 from Bahawalpur and 3
each from Faisalabad, Lahore and Multan) mules were bled for blood and serum samples. Blood
and serum samples from 332 donkeys having following sexual distribution: 252 males (37 from
Multan, 40 from Bahawalpur, 98 from Faisalabad, 34 from Lahore and 43 from Gujranwala) and
80 females (15 from Multan, 12 each from Gujranwala and Bahawalpur, 25 from Faisalabad and
16 from Lahore) were collected.
4.3c. Age Related Distribution of Samples
Equines sampled (n=430) for the current study were divided into three age groups (i) less than
equal to 5 years of age (n=138) (ii) 6-10 years of age (n=195) and (iii) more than 10 years of age
(n=97) to determine the possible association of diseases under study with age of animals. Out of
65 horses sampled for the study, 11 were less than equal to 5 years of age, 29 were 6-10 years of

CHAPTER-IV (RESULTS)
47
age and 25 horses were of more than ten years of age (Table-5). Distribution of sampled mule
population (n=33) according to age was 8, 18 and 7 respectively. Age related distribution of
sampled donkey population (n=332) was 119, 148 and 65 respectively. Area related age
distribution of equine samples is presented in Table-5.
4.4. Housing and Management Related Distribution of Samples
4.4a. Housing Pattern Adopted by Equine Owners of the Selected Locales
Analysis of housing pattern of sampled equine population (n=430) revealed the 46.3% of equines
were kept alone (199 heads), followed by 28.6% animals kept with other equine cohorts (123
heads) and 25.1% in mix herds (108 heads) with cattle, buffalo, sheep, goat, dogs and other
animals (Table-6). However, the difference observed in these housing practices among sampled
areas was statistically not significant, 2 (4df) =1.91, p =0.984.
4.4b. Watering Habits adopted by Equine Owners of the Selected Locales
Survey indicated that 320 (74.4%) equine owners provided water to their animals through
communal water troughs and shared buckets while at work. This trend was highest among the
equine owners of Lahore (82.6%), followed by Bahawalpur (76.5%), Faisalabad (74%),
Gujranwala (72%) and Multan (67.7%). However, this difference was not significant, 2 (4df)
=4.464, p=0.347. This pattern reversed when watering habit of owners at home was analyzed to
25.4% (109 heads) (Table-7) because most of the equines were kept alone. Use of common water
trough at home was recorded as 27.9% in Multan and Bahawalpur each followed by Lahore
(27.5%), Gujranwala (25.3%) and Faisalabad (22%). This difference regarding watering
practices at home was not significant between selected areas, 2 (4df) =1.031, p=0.905.

CHAPTER-IV (RESULTS)
48
Table-3 Areas and equine type related distribution of samples (n=430) taken for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Location Horse Mule Donkey Total
Multan 10 6 52 68
Bahawalpur 10 6 52 68
Faisalabad 18 9 123 150
Lahore 13 6 50 69
Gujranwala 14 6 55 75
Total 65 33 332 430
Table-4 Sex related distribution of samples (n=430) taken for sero-survey of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
Area Sampled Horses Mules Donkeys
Male Female Male Female Male Female
Multan 6 4 3 3 37 15
Bahawalpur 5 5 2 4 40 12
Faisalabad 5 13 6 3 98 25
Lahore 4 9 3 3 34 16
Gujranwala 5 9 4 2 43 12
Total 25 40 18 15 252 80

CHAPTER-IV (RESULTS)
49
Table-5 Age related distribution of equines (n = 430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Area
Sampled
Horses
(n=65)
Mules
(n=33)
Donkeys
(n=332)
< 5 Y 6-10 Y > 10Y < 5 Y 6-10 Y > 10Y < 5 Y 6-10 Y > 10 Y
Multan 0 8 2 2 3 1 21 26 5
Bahawalpur 1 7 2 2 4 0 12 23 17
Faisalabad 4 5 9 1 5 3 45 51 27
Lahore 5 4 4 1 4 1 24 20 6
Gujranwala 1 5 8 2 2 2 17 28 10
Total 11 29 25 8 18 7 119 148 65

CHAPTER-IV (RESULTS)
50
4.4c. Tick, Mosquito and Fly Control Measures Adopted by Equine Owners
Data related to tick, mosquito and fly control measures (Table-8) adopted by owners of sampled
equine population (n=430) revealed that only 25.8% (n=111) owners used tick control measures
in their routine practice and 39.8% (n=171) practiced some sort of fly and mosquito control
methods (Table-8). Whereas 148 equine owners did not employ any tick, mosquito and fly
control measures during their routine practice. The trend of using tick control measures was
significantly different, 2 (4df) =17.085, p < 0.01 in the equine owners of Multan (39.7%) and
Bahawalpur (36.8%) than Gujranwala (22.7%), Faisalabad (20.7%) and Lahore (15.9%).
Similarly, significantly different (2, 4df =29.109, p < 0.01) number of equine owners practiced
fly and mosquito control measures in Multan (61.8%) and Bahawalpur (54.4%) than equine
owners of Faisalabad (32.7%), Lahore (31.9%) and Gujranwala (28%).
4.5. Equine Infectious Anemia
In current study 430 blood and serum samples from 65 horses, 33 mules and 332 donkeys were
subjected to enzyme linked immunosorbent assay (ELISA) testing for detecting antibodies
against equine infectious anemia virus in 5 draught equine populated urban areas of Punjab.
However, all equines were found sero-negative for antibodies against EIA virus.

CHAPTER-IV (RESULTS)
51
Table-6 Housing pattern observed in equines (n=430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Location
Housing Pattern
Kept with non equine cohorts
(%)
Kept Alone (%) Kept with Equines (%)
Faisalabada 39 (26.0) 68 (45.3) 43 (28.7)
Lahorea 20 (28.9) 29 (42.0) 20 (28.9)
Gujranwalaa 19 (25.3) 35 (46.7) 21 (28.0)
Multana 16 (23.5) 34 (50.0) 18 (26.5)
Bahawalpura 14 (20.6) 33 (48.5) 21 (30.9)
Total 108 (25.1) 199 (46.3) 123 (28.6)
Values with same superscript are not significantly different (P > 0.05), 2 (4 df) =1.91, p = 0.98
Table-7 Watering pattern used at work and home by the owners of equines (n=430) sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Values with same superscript are not significantly different (P > 0.05), 2(4 df)=4.46, p = 0.347
LOCATION
Water at Work Water at Home
Communal water trough
(%)
Separate Bucket (%)
Communal water trough
(%)
Separate Bucket (%)
Multana 46 (67.7) 22 (32.3) 19 (27.9) 49 (72.1)
Bahawalpura 52 (76.5) 16 (23.5) 19 (27.9) 49 (72.1)
Faisalabada 111 (74.0) 39 (26.0) 33 (22.0) 117 (78.0)
Lahorea 57 (82.6) 12 (17.4) 19 (27.5) 50 (72.5)
Gujranwalaa 54 (72.0) 21 (28.0) 19 (25.3) 56 (74.7)
Total 320 (74.4) 110 (25.6) 109 (25.4) 321 (74.7)

CHAPTER-IV (RESULTS)
52
Table-8 Number of equine owners practicing tick, fly and mosquito control measures in 5 draught equine populated urban areas of Punjab sampled for sero-survey of equine infectious anemia, glanders and piroplasmosis.
Values with different superscript whole number differ significantly (P < 0.01)
Values with different superscript numbers differ significantly (P < 0.01)
Location Owners using tick Control methods (%)
Owners using fly & mosquito Control methods (%)
Multan 27 (39.7)a 42 (61.8)a
Bahawalpur 25 (36.8)a 37 (54.4)a
Faisalabad 31 (20.7)b 49 (32.7)b
Lahore 11 (15.9)b 22 (31.9)b
Gujranwala 17 (22.7)b 21 (28.0)b
Total 111 (25.8) 171(39.8)
Chi-Square 2 (4) 17.08 P = 0.002 2 (4) 29.11 P = 0.000

CHAPTER-IV (RESULTS)
53
4.6. Comparison of hematological findings in equines of 5 different areas
Data regarding hematological values of equines from 5 different areas is presented in Table-9.
Mean white blood cell (WBC) count was significantly higher (P < 0.05) in equines of
Bahawalpur (7.48 + 1.85) and Multan (7.25 + 2.11) than Faisalabad (6.38 + 2.12), Gujranwala
(6.81 + 1.89) and Lahore (6.39 + 1.94). Significantly lower (P < 0.05) mean red blood cell
(RBC) count was observed in equines of Lahore (5.42 + 1.36) as compared to the Bahawalpur
(6.11 + 150), Multan (5.99 + 1.94), Gujranwala (5.89 + 1.77) and Faisalabad (5.71 + 1.47).
There was not a significant difference (P > 0.05) between the values of mean hemoglobin (Hb)
concentration among equines of Lahore (9.87 + 2.01), Gujranwala (9.56 + 1.92), Faisalabad
(9.31 + 1.90) and Multan (9.30 + 2.36). However, these values were significantly higher (P <
0.05) than mean Hb concentration value in equines of Bahawalpur (7.35 + 1.77).
Highest value for mean packed cell volume (PCV) was recorded in blood samples of equines
from Bahawalpur (32.45 + 6.26) that was significantly higher (P < 0.05) than mean PCV values
observed in equines of Gujranwala (29.42 + 4.41), Faisalabad (29.36 + 5.94) and Multan (28.11
+ 5.74). Significantly lower (P < 0.05) mean hematocrit value (22.77 + 5.07) was recorded for
the equines of Lahore. There was a not significant difference (P > 0.05) in the values of mean
corpuscular volume (MCV) among equines of Faisalabad (54.64 + 17.30), Lahore (58.55 +
18.56), Gujranwala (54.68 + 20.61) and Bahawalpur (55.70 + 16.16). However, these values
were significantly higher (P < 0.05) than the equines of Multan (50.76 + 15.86). Significantly
lower (P < 0.05) value regarding mean corpuscular hemoglobin (MCH) was recorded in equines
of Multan (16.74 + 5.71) as compared to equines of Lahore (19.21 + 5.85), Faisalabad (17.60 +

CHAPTER-IV (RESULTS)
54
6.36) and Gujranwala (17.33 + 5.15). However, this MCH value (16.74 + 5.71) was significantly
higher (P < 0.05) than the equines of Bahawalpur (12.34 + 5.34). Mean corpuscular hemoglobin
concentrations (MCHC) were not significantly different (P > 0.05) among equines of Lahore
(34.16 + 9.40), Multan (33.52 + 7.86), Gujranwala (33.06 + 7.59) and Faisalabad (32.79 + 8.72)
but were significantly higher (P < 0.05) than equines of Bahawalpur (22.40 + 8.21).
4.6a. Comparison of hematological findings among horses, mules and donkeys
Analysis of data regarding the hematological findings in horses, mules and donkeys is presented
in Table-10. Mean white blood (WBC) counts were decreased in horses (6.65 + 2.16), mules
(6.82 + 2.12) and donkeys (6.77 + 1.91). These values were significantly different (P < 0.05)
from reference values for mules (9.40 + 2.89) and donkeys (9.75 + 3.29) but in horses this
difference was not significant (P > 0.05) from reference value (7.18 + 2.87). Mean red blood cell
(RBC) counts were not significantly different (P > 0.05) than respective reference values for
horses (5.28 + 1.18), mules (5.77 + 1.68) and donkeys (5.78 + 1.56). However, mean RBC
counts were significantly lower (P < 0.05) in horses than mules and donkeys (Table-10).
Significantly lower (P < 0.05) mean hemoglobin (Hb) concentration was observed in horses
(9.62 + 2.18) than reference value (10.93 + 1.81). Mean Hb concentrations were not significantly
lower (P > 0.05) in mules (9.24 + 2.05) than reference values (10.10 + 0.73). In donkeys mean
hemoglobin concentration (9.25 + 1.82) was not significantly higher (P > 0.05) than reference
value (9.01 + 1.13). There was not a significant difference (P > 0.05) among equines regarding
these values. Mean packet cell volume values for horses (28.59 + 5.30), mules (28.86 + 5.36)
and donkeys (29.22 + 5.48) were significantly lower (P < 0.05) than their respective reference

CHAPTER-IV (RESULTS)
55
values (37.75 + 4.57, 34.37 + 4.13 and 32.42 + 4.38 respectively). However, difference among 3
equine species was statistically not significant (P > 0.05).
There was a not significant difference (P > 0.05) regarding mean corpuscular volume (MCV)
among horses (56.30 + 14.65), mules (53.48 + 16.34) and donkeys (54.30 + 18.37). These values
were not significantly (P > 0.05) lower than their respective reference values (Table-10). Values
regarding mean corpuscular hemoglobin (MCV) indicated a not significant difference (P > 0.05)
between reference and observed values for all 3 equine species. MCV was significantly higher (P
< 0.05) in horses (19.82 + 7.28) than donkeys (17.09 + 5.50) and mules (16.93 + 5.29). There
was not a significant difference (P > 0.05) among equines regarding values of mean corpuscular
hemoglobin concentration (MCHC). These values were not significantly higher (P > 0.05) than
reference values in horses (34.17 + 7.57), mules (32.67 + 7.80) and donkeys (30.56 + 8.62).
4.6b. Comparison of Hematological findings on the basis of sex of equines
Analysis of hematological data on the basis of sex of equines is presented in Table-11. There was
a not significant difference (P > 0.05) in mean white blood cell (WBC) counts between male
(6.75 + 2.03) and female (6.86 + 2.00) equines. Similarly mean red blood (RBC) counts were
numerically but statistically not significantly higher (P > 0.05) in males (5.71 + 1.59) as
compared to females (5.64 + 1.61). A significant difference (P < 0.05) was observed between
males (9.25 + 2.01) and females (9.76 + 2.14) regarding mean hemoglobin (Hb) concentration.
Numerically higher value of mean packed cell volume (PCV) was recorded in female equines
(29.27 + 4.91) than males (29.08 + 5.74). However, this difference was statistically not
significant (P > 0.05). There was not a significant difference (P > 0.05) between male and female
equines regarding values of mean corpuscular volume (MCV), mean corpuscular hemoglobin

CHAPTER-IV (RESULTS)
56
(MCH) and mean corpuscular hemoglobin concentration (MCHC). In female equines MCV
(55.80 + 17.26), MCH (18.52 + 6.11) and MCHC (34.02 + 8.49) values were numerically higher
as compared to MCV (54.44 + 17.64), MCH (17.39 + 5.93) and MCHC (32.74 + 8.53) values in
males.
4.6c. Comparison of hematological findings on the basis of age of equines
Data regarding hematological examination in different age groups of equines is presented in
Table-12. Mean white blood cell (WBC) count was significantly higher (P < 0.05) in equines of
less than equal to 5 years (8.23 + 1.78) of age (group-I) followed by 6.65 + 1.43 and 4.94 + 1.68
in group-II (< 10 years) and III (> 10years) respectively. Similar pattern was observed regarding
mean red blood cell (RBC) counts with significantly higher (P < 0.05) count was found in
equines of group-I (6.38 + 1.65) followed by group-II (5.73 + 1.45) and III (4.74 + 1.26). Mean
hemoglobin concentration was significantly higher (P < 0.05) in group-I (9.66 + 1.98) and II
(9.43 + 1.91) as compared to group-III (8.67 + 1.99). There was not a significant difference (P >
0.05) among all three age groups regarding mean hematocrit (PCV) values with numerically
higher PCV was recorded in group-I (29.62 + 5.82) followed by group-II (29.07 + 5.63) and III
(28.58 + 5.29). There was a significant difference (P < 0.05) among values regarding mean
corpuscular volume (MCV) among equines of 3 groups with highest value recorded in group-III
(64.66 + 23.33) followed by group-II (53.20 + 14.14) and I (49.61 + 16.25). Similar pattern was
recorded regarding values of mean corpuscular hemoglobin (MCH) where significantly higher (P
< 0.05) MCH was recorded in group-III (19.89 + 7.12) followed by group-II (17.34 + 5.17) and I
(16.14 + 5.50). Mean corpuscular hemoglobin concentration was not significantly (P > 0.05)
different in group-I (33.70 + 9.06) and II (33.41 + 8.51) but these were significantly higher (P <
0.05) from group-III (30.90 + 7.17).

CHAPTER-IV (RESULTS)
57
Table-9 Hematological values recorded in equines (n = 430) surveyed for sero-prevalence of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
Areas WBC/10³μL RBC/106 μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
Faisalabad 6.83 + 2.12b 5.71 + 1.47a 9.31 + 1.90a 29.36 + 5.94b 54.64+ 17.30a 17.60 + 6.36a 32.79 + 8.72a
Lahore 6.39 + 1.94b 5.42 + 1.36b 9.87 + 2.01a 22.77 + 5.07c 58.55 + 18.56a 19.21 + 5.85a 34.16 + 9.40a
Gujranwala 6.81 + 1.89b 5.89 + 1.77a 9.56 + 1.92a 29.42 + 4.41b 54.68 + 20.61a 17.33 + 5.15a 33.06 + 7.59a
Multan 7.25 + 2.11a 5.99 + 1.94a 9.30 + 2.36a 28.11 + 5.74b 50.76 + 15.86b 16.74 + 5.71b 33.52 + 7.86a
Bahawalpur 7.48 + 1.85a 6.11 + 1.50a 7.35 + 1.77b 32.45 +6.26a 55.70 + 16.16a 12.34 + 5.34c 22.40 + 8.21b
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with different alphabetic superscript s are significantly (P < 0.05) different from each other

CHAPTER-IV (RESULTS)
58
Table-10 Comparison of hematological values recorded in horses (n = 65), mules (n = 33) and donkeys (n = 332) sampled for sero-prevalence of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Animal
WBC/10³μL RBC/106 μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
Reference Value
7.18 + 2.87 5.93 + 2.81 10.93 + 1.81 37.75 + 4.57 63.66 18.43 28.95
Horse
6.65 + 2.16NSa 5.28 + 1.18NSb 9.62 + 2.18Sa 28.59 + 5.30Sa 56.30 + 14.65a 19.82 + 7.28a 34.17 + 7.57
Reference Value
9.40 + 2.89 5.74 + 2.62 10.10 + 0.73 34.37 + 4.13 59.88 17.59 29.38
Mule
6.82 + 2.12Sa 5.77 + 1.68NSa 9.24 + 2.05NSa 28.86 + 5.36Sa 53.48 + 16.34a 16.93 + 5.29b 32.67 + 7.80
Reference Value
9.75 + 3.29 5.88 + 2.65 9.01 + 1.13 32.42 + 4.38 55.13 15.32 27.79
Donkey
6.77+ 1.91Sa 5.78 + 1.56NSa 9.25 + 1.82NSa 29.22 + 5.48Sa 54.30 + 18.37a 17.09 + 5.50b 30.56 + 8.62
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with different superscript alphabetic are significantly (P < 0.05) different from each other
Values with ‘NS’ superscript are not significantly (P > 0.05) different from their respective reference values
Values with ‘S’ superscript are significantly (P < 0.05) different from their respective reference values
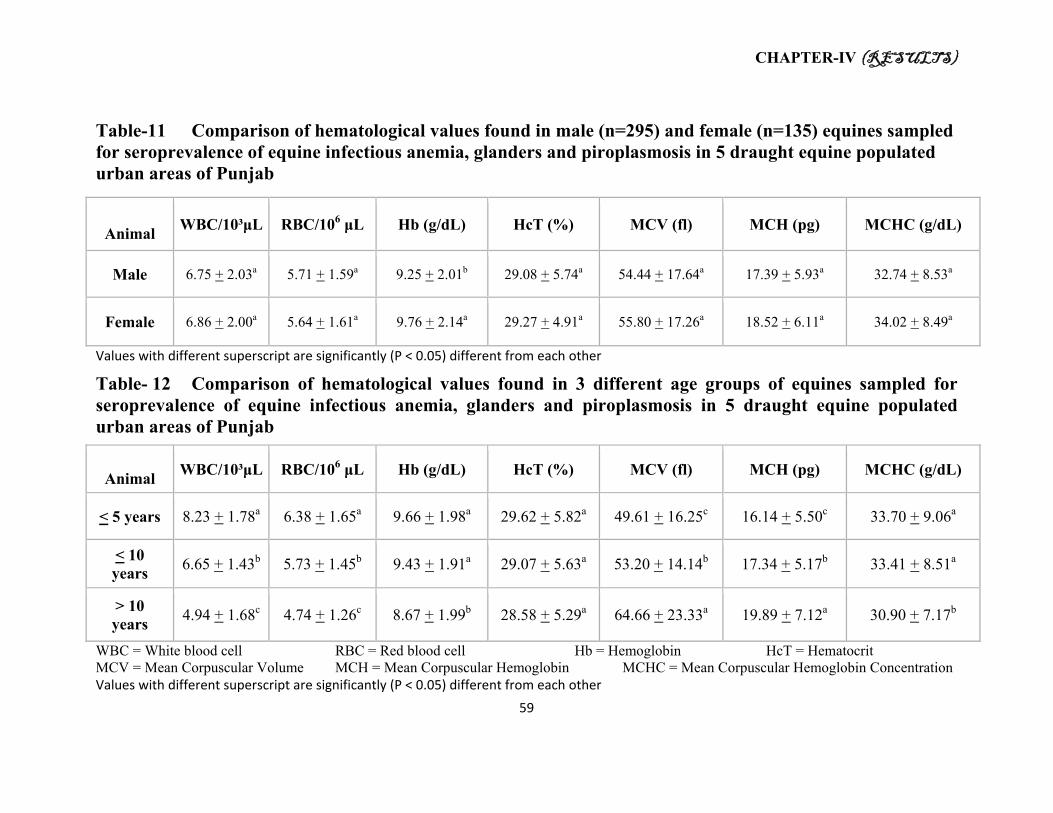
CHAPTER-IV (RESULTS)
59
Table-11 Comparison of hematological values found in male (n=295) and female (n=135) equines sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Animal
WBC/10³μL RBC/106 μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
Male 6.75 + 2.03a 5.71 + 1.59a 9.25 + 2.01b 29.08 + 5.74a 54.44 + 17.64a 17.39 + 5.93a 32.74 + 8.53a
Female 6.86 + 2.00a 5.64 + 1.61a 9.76 + 2.14a 29.27 + 4.91a 55.80 + 17.26a 18.52 + 6.11a 34.02 + 8.49a
Values with different superscript are significantly (P < 0.05) different from each other
Table- 12 Comparison of hematological values found in 3 different age groups of equines sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab
Animal
WBC/10³μL RBC/106 μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
< 5 years 8.23 + 1.78a 6.38 + 1.65a 9.66 + 1.98a 29.62 + 5.82a 49.61 + 16.25c 16.14 + 5.50c 33.70 + 9.06a
< 10 years
6.65 + 1.43b 5.73 + 1.45b 9.43 + 1.91a 29.07 + 5.63a 53.20 + 14.14b 17.34 + 5.17b 33.41 + 8.51a
> 10 years
4.94 + 1.68c 4.74 + 1.26c 8.67 + 1.99b 28.58 + 5.29a 64.66 + 23.33a 19.89 + 7.12a 30.90 + 7.17b
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration Values with different superscript are significantly (P < 0.05) different from each other

CHAPTER-IV (RESULTS)
60
4.7. Equine Glanders
Rose Bengal Plate Agglutination (RBT) test based screening of the serum samples (n = 430)
revealed that overall seroprevalence of glanders (Table-13) in equine population of studied areas
was 7.9% (n = 34).
4.7a. Area Related Seroprevalence of Equine Glanders
Numerically higher seroprevalence of equine glanders (Table-13) was found in draught equines
of Lahore 11.6% (n=8) followed by Bahawalpur (10.3%, n=7), Multan (7.3%, n=5), Faisalabad
(6.7%, n=10) and Gujranwala (5.3%, n=4). However, this difference in prevalence of glanders in
studied areas was not statistically significant, 2 (4df) =2.84, P=0.584.
4.7b. Clinical Signs Observed in RBT Positive Equines
Analysis of data regarding clinical signs found in RBT positive equines (Table-14) indicated that
pale and congested mucous membranes (58.8%) was the most frequent clinical finding followed
by loss of stamina (41.2%), fever (38.2%), anorexia (38.2%), cough (29.4%), lymph node
swelling (21.6%), nasal discharge (14.7%) and dyspnea (8.8%). In one male donkey orchitis
(2.9%) was also observed.
4.7c. Seroprevalence of Glanders in 3 Different Species of Equids
Species related analysis of data indicated (Table-13) that prevalence of glanders was
significantly different (P<0.01) in horses (16.92%, n = 11) and mules (12.12%, n = 4) than
donkeys (5.72%, n=19), 2 (2df) =10.23, P=0.006. Among horses of five draught populated

CHAPTER-IV (RESULTS)
61
areas, prevalence of glanders was highest in horses of Lahore (23.1%) followed by Multan and
Bahawalpur (20% each), Faisalabad (16.7%) and Gujranwala (7.1%). Prevalence of glanders in
mules of Lahore, Bahawalpur and Multan was 16.7%. One mule serum from Faisalabad
(prevalence 11.1%) gave positive RBT reaction. No mule of Gujranwala was found positive for
glanders. Four donkeys (8.0%) from Lahore were found seropositive for glanders followed by 4
(7.7%) from Bahawalpur, 2 (3.8%) from Multan, 6 (4.9%) from Faisalabad and 3 (5.4%) from
Gujranwala. There was no significant difference (P>0.05) among horses, mules and donkeys
with in different metropolises regarding sero-prevalence of glanders.
4.7d. Age Related Seroprevalence of Equine Glanders
Numerically higher but statistically non-significant, 2 (2df) =1.47, P=0.477 seroprevalence of
glanders (Table-15) was found in equines belonging to group-2 (6-10Y) i.e. 9.2% (n=18),
followed by 11 equines (7.9%) in group-1 (less than equal to 5 Y) and 5.2% (n=5) in animals of
age group-3 (more than 10Y). Similar seroprevalence pattern was recorded in horses where 7
animals (24.1%) were found sero-reactive in group-2 followed by 2 young horses (18.2%) in
group-1 and 2 old horses (8.0%) in group-3. Higher seroprevalence of glanders was noted in
mules belonging to age group-3 i.e. 14.3% (n=1) followed by 12.5% in group-1 (n=1) and 11.1%
in group-2 (n=2). Prevalence of glanders was numerically higher (6.7%) in donkeys of group-1,
where 8 animals were found sero-reactive followed by 6.1% (n=9) in group-2 and 3.1% (n=2) in
age group-3.

CHAPTER-IV (RESULTS)
62
4.7e. Sex Related seroprevalence of Equine Glanders
Significantly higher seroprevalence (12.6%) of equine glanders (Table-16) was found in female
equines (n=135) as compared to male (n=295) animals where it was 5.8%, 2 (1df)
=5.94, P=0.014. Out of 65 horses (25 male and 40 female), 20% (n=8) female and 12% (n=3)
male serum samples were positive for RBT. Seroprevalence of glanders in male mules (n=18)
was higher 16.7% (n=3) as compared to females (6.7%, n=1). Eleven out of 252 male donkeys
(4.4%) were tested RBT positive and prevalence of glanders in female donkeys was 10% (n=8).
However, these differences in seroprevalence of glanders regarding sex of equines within each
species were statistically not significant (P>0.05).
4.7f. Hematological analysis of the RBT positive equine blood samples
Hematological analysis of the equines found seropositive for glanders indicated that there was
not significant (P > 0.05) increase (8.15 + 2.77) in the mean leukocyte counts in horses (n = 11)
than their respected reference value (Table-17). Whereas in mules (n =4) a not significant (P >
0.05) decrease (8.27 + 3.23) than reference white blood cell (WBC) count (9.40 + 2.89) was
observed. Significantly lower (P < 0.05) mean WBC count (7.52 + 1.80) than normal reference
value was observed in Rose Bengal plate agglutination test (RBT) positive donkeys (n =19).
However, these values were not significantly (P > 0.05) different among horses, mules and
donkeys.
In RBT positive horses mean red blood cell (RBC) count (4.16 + 0.62) was significantly lower
(P < 0.05) than reference value (5.93 + 2.81). This difference was also observed in RBC counts
of RBT positive donkeys where mean RBC count (4.10 + 0.57) was significantly (P < 0.05)
lower than the reference value (5.88 + 2.65). Mean RBC count was numerically lower (4.76 +

CHAPTER-IV (RESULTS)
63
1.38) in sero-reactive mules than reference value (5.74 + 2.62). There wasn’t a significant
difference (P > 0.05) among horses, mules and donkeys regarding these counts.
Mean hemoglobin (Hb) concentration was found numerically higher in horses (11.70 + 1.73),
mules (10.45 + 2.27) and donkeys (10.57 + 1.47) than their respective reference values (Table-
17). However, this difference in mean Hb concentration among horses, mules and donkeys was
statistically not significant (P > 0.05).
Mean packed cell volume (PCV) in RBT positive horses was statistically not significantly (P >
0.05) lower (29.29 + 4.57) than normal value (37.75 + 4.57). This was also reflected by the
mean hematocrit value of donkeys (31.51 + 4.68) and mules (30.28 + 3.77). There wasn’t a
significant difference (P > 0.05) in mean PCV values among different equines. On the basis of
erythrocytic indices (Table-17) macrocytic hyperchromic type of anemia was observed in RBT
positive horses (n = 11), mules (n =4) and donkeys (n =19).
4.7g. Prevalence of equine glanders with reference to housing pattern of equines
Data regarding housing pattern of equines (Table-18) sampled for seroprevalence of glanders
revealed 16 (47.1%) out of 34 seropositive animals were kept alone, while 9 (26.5%) equines
were kept with equine cohorts and 9 (26.5%) were managed with other animals (small and large
ruminants, dogs etc.). This prevalence was higher in equines kept in mix herds (9.1%) followed
by animals kept alone (8.7%) and managed with equine cohorts (7.9%). However, housing was
not significantly associated with seropositivity, 2 (2df) =0.11, P=0.94.
4.7h. Prevalence of glanders with reference to watering habits of the draught equine owners

CHAPTER-IV (RESULTS)
64
Analysis of the watering methods adopted by owners (Table-19) of RBT positive equines (n=34)
revealed that 30 (88.2%) animals were given water through the communal water troughs either at
work or home. Only 4 (11.8%) positive equines were given water through separate buckets at
work and home. Equines drinking water through communal water toughs were more likely to be
seropositive for glanders (OR=2.71, 95% CI 0.94-7.83) as compared to equines given water
through separate buckets. However, this difference was not significant, 2 (1df) =3.6, P=0.058.
4.6i. Multivariable analysis for the equine glanders
In total 6 variables were used in initial bivariable screening and out of these only equine species
(P=0.006), sex (P=0.014) and watering methods adopted by equine owners (P=0.058) were
significantly associated with high prevalence of glanders (Wald P < 0.2). Metropolis (p=0.58),
age (0.477) and housing (0.774) were not significantly associated with sero-prevalence of
glanders (Wald P>0.2) (Table-20). All variables yielding Wald P < 0.2 were entered into a
multivariable regression model which resulted in no variable remaining significantly associated
with the sero-prevalence of glanders (P>0.05) except equine species and therefore, no
multivariable model was left to present. However, when equine species was removed from a
biological perspective and model was built by keeping sex and watering together, the results
showed being a female equine (OR=2.3, 95% CI=1.13-4.69) and drinking water at communal
water trough (OR=2.6, 95% CI=0.90-7.69) had more chances of contracting glanders (Table-21).
Based upon Hosmer-Lemeshow test and the Negelkerke R Square this seemed to be reasonably
good fit model to the data (Chi-square=4.244. df=2, P=0.120 and 0.051 respectively). However,
this assumption was not found to be strictly significant in statistical terms.

CHAPTER-IV (RESULTS)
65
Table-13 Comparative Seroprevalence of equine glanders in 5 draught equine populated urban areas of Punjab
Location Samples done
Horses
(Prev. %)
Mules
(Prev. %)
Donkey
(Prev. %) Total (Prev. %)
Multana 68 (10H, 6M, 52D) 2 (20.0)a 1 (16.7)a 2 (3.8)a 5 (7.3)a
Bahawalpura 68 (10H, 6M, 52D) 2 (20.0)a 1 (16.7)a 4 (7.7)a 7 (10.3)a
Faisalabada 150 (18H, 9M, 123D) 3 (16.7)a 1 (11.1)a 6 (4.9)a 10 (6.7)a
Lahorea 69 (13H, 6M, 50D) 3 (23.1)a 1 (16.7)a 4 (8.0)a 8 (11.6)a
Gujranwalaa 75 (14H, 6M, 55D) 1 (7.1)a 0 (0.0)a 3 (5.5)a 4 (5.3)a
Totala 430 (65H, 33M, 332D) 11 (16.9)1 4 (12.1)1 19 (5.7)2 34 (7.9%)
H = Horse M = Mule D = Donkey
Values with similar superscript alphabets in a column are not significantly (P > 0.05) different
Values with different superscript whole number in a row differ significantly, 2 (2df) =10.23, P=0.006

CHAPTER-IV (RESULTS)
66
Table-14 Frequency of clinical signs in RBT positive (n=34) equines of 5 draught equine populated urban areas of Punjab sampled for seroprevalence of equine infectious anemia, glanders and piroplasmosis
Symptoms
Frequency of Clinical Sign
Percentage (%)
Fever 13 38.2
Mucous Membrane (Pale, Congested) 20 58.8
Anorexia 13 38.2
Respiratory Signs
Nasal Discharge 5 14.7
Cough 10 29.4
Dyspnea 3 8.8
Stamina Loss 14 41.2
Lymph Node Swelling 8 21.6
Others
Orchitis 1 2.9

CHAPTER-IV (RESULTS)
67
Table-15 Comparative age related seroprevalence of glanders in equines (n=430) of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
Values with similar superscript alphabets in a row are not significantly (P > 0.05) different, 2(2, n=430) = 1.47, P= 0.477
Equine
Samples Taken
(age group distribution)
Age Group (Prev. %)
< 5 Y
(n= 141)
< 10 Y
(n = 193)
> 10Y
(n = 96)
Horses 65 (11,29,25) 2 (18.2)a 7 (24.1)a 2 (8.0)a
Mules 33 (8,18,7) 1 (12.5)a 2 (11.1)a 1 (14.3)a
Donkeys 332 (119,148,65) 8 (6.7)a 9 (6.1)a 2 (3.1)a
Total 430 (138, 195, 97) 11 (7.9)a 18 (9.2)a 5 (5.2)a

CHAPTER-IV (RESULTS)
68
Table-16 Sex related seroprevalence of glanders in equines (n=430) of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
Area Sampled Samples Taken Horses (Prev.%) Mules (Prev.%) Donkeys (Prev.%)
Male Female Male Female Male Female
Multan H (6♂, 4♀)
M (3♂, 3♀)
D (37♂, 15♀)
1 (16.7) 1 (25.0) 0 (0.0) 1 (33.3) 1 (2.7) 1 (6.7)
Bahawalpur H (5♂, 5♀)
M (2♂, 4♀)
D (40♂, 12♀)
1 (20.0) 1 (20.0) 1 (50.0) 0 (0.0) 3 (7.5) 1 (8.3)
Faisalabad H (5♂, 13♀)
M (6♂, 3♀)
D (98♂, 25♀)
1 (20.0) 2 (15.4) 1 (16.7) 0 (0.0) 3 (3.1) 3 (12.0)
Lahore H (4♂, 9♀)
M (3♂, 3♀)
D (34♂, 16♀)
0 (0.0) 3 (33.3) 1 (33.3) 0 (0.0) 3 (8.8) 1 (6.3)
Gujranwala H (5♂,9♀)
M (4♂, 2♀)
D (43♂, 12♀)
0 (0.0) 1 (11.1) 0 (0.0) 0 (0.0) 1 (2.3) 2 (16.7)
Total H (25♂, 40♀)
M (18♂, 15♀)
D (252♂, 80♀)
3 (12.0)a 8 (20.0)a 3 (16.7)a 1 (6.7)a 11 (4.4)a 8 (10.0)a
Values with similar superscript alphabets in a row are not significantly (P > 0.05) different
Overall prevalence between two sexes differ significantly (P<0.05), 2 (1, n=430) = 5.94, P=
0.014

CHAPTER-IV (RESULTS)
69
Table-17 Haematological values in equines found sero-positive for glanders (n=34) in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Animal
WBC/10³μL RBC/106 μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
Reference Value
7.18 + 2.87 5.93 + 2.81 10.93 + 1.81 37.75 + 4.57 63.66 18.43 28.95
Horse (n = 11)
8.15 + 2.77NSa 4.16 + 0.62sa 11.70 + 1.73NSa 29.29 + 4.75HSa 71.74 + 14.59NSa 28.42 + 4.39NSa 40.87 + 9.47NSa
Reference Value
9.40 + 2.89 5.74 + 2.62 10.10 + 0.73 34.37 + 4.13 59.88 17.59 29.38
Mule (n = 4)
8.27 + 3.23NSa 4.76 + 1.38NSa 10.45 + 2.27NSa 30.28 + 3.77NSa 68.83 + 26.33NSa 24.02 + 10.33NSa 34.82 + 8.53NSa
Reference Value
9.75 + 3.29 5.88 + 2.65 9.01 + 1.13 32.42 + 4.38 55.13 15.32 27.79
Donkey (n = 19)
7.52 + 1.80Sa 4.10 + 0.57Sa 10.57 + 1.47HSa 31.51 + 4.68NSa 77.79 + 13.52NSa 26.24 + 5.07NSa 34.03 + 5.36NSa
Total (n = 34)
7.81 + 2.27 4.20 + 0.71 10.92 + 1.69 30.65 + 4.60 74.78 + 15.49 26.68 + 5.62 36.33 + 7.72
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with ‘NS’ superscript are non significantly (P > 0.05) different from the reference value Values with ‘S’ superscript are significantly (P < 0.05) different from the reference value Values with same alphabetic superscript are non significantly (P > 0.05) different from each other

CHAPTER-IV (RESULTS)
70
Table-18 Housing pattern observed in Rose Bengal Plate Agglutination Test (RBT) positive (n=34) and negative (n=396) equines surveyed for the prevalence of glanders in 5 draught equine populated urban areas of Punjab
Region
RBT Positive Equines Housing Pattern RBT Negative Equine Housing Pattern
Alone With Equine Others Total Alone With Equine Others Total
Multan 1 2 2 5 33 16 14 63
Bahawalpur 5 1 1 7 28 20 13 61
Faisalabad 6 2 2 10 62 41 37 140
Lahore 2 3 3 8 27 17 17 61
Gujranwala 2 1 1 4 33 20 18 71
Total 16 9 9 34 183 114 99 396
Table-19 Prevalence of glanders in association with watering habits of owners (n = 430) of 5 draught equine populated urban areas of Punjab surveyed for the seroprevalence of equine infectious anemia, glanders and piroplasmosis
Region
RBT Positive Equines RBT Negative equines
Communal Water Troughs
Separate Watering Total
Communal Water Troughs
Separate Watering Total
Multan 4 1 5 42 21 63
Bahawalpur 6 1 7 46 15 61
Faisalabad 9 1 10 102 38 140
Lahore 7 1 8 50 11 61
Gujranwala 4 0 4 50 21 71
Total 30 4 34 290 106 396

CHAPTER-IV (RESULTS)
71
Plate-V Photograph showing the communal water troughs used by the draught equine owners during working hours
Plate-VI Photograph showing the communal water troughs used by the draught equine owners in the communal equine housings

CHAPTER-IV (RESULTS)
72
Table-20 Bivariable analysis for predicting glanders in equines sampled from 5 draught equine populated urban areas of Punjab
S. No. Exposure Variable Comparison Chi Square df P OR 95% CI Wald P
1 Metropolis 2.84 4 0.58 0.597
Multan Gujranwala 1.409 0.362 5.47 0.621
Bahawalpur Gujranwala 2.037 0.569 7.29 0.274
Faisalabad Gujranwala 1.268 0.384 4.18 0.697
Lahore Gujranwala 2.32 0.668 8.11 0.185
2 Species of equine 10.23 2 0.006 0.009
Horse Donkey 3.35 1.51 7.44 0.003
Mule Donkey 2.27 0.72 7.12 0.159
3 Sex
Female Male 5.94 1 0.014 2.35 1.163 4.77 0.017
4 Age groups 1.47 2 0.477 0.485
6 to 10 5 or less 1.59 0.535 4.74 0.402
more than 10 5 or less 1.87 0.673 5.2 0.23
5 Housing Pattern
Kept with non equine cohorts Kept alone or with equines
0.082 1 0.774 0.89 0.403 1.96 0.774
6 Watering Methods
Communal Separate 3.6 1 0.058 2.7 0.931 7.86 0.067

CHAPTER-IV (RESULTS)
73
Table-21 SPSS output of binary logistic regression analysis for predicting glanders in equines sampled from 5 draught equine populated urban areas of Punjab
Variables in the Equation
B S.E. Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Lower Upper
Step 1a Sex .838 .362 5.359 1 .021 2.311 1.137 4.696
Watering Methods .969 .546 3.144 1 .076 2.635 .903 7.690
Constant -3.578 .538 44.281 1 .000 .028
a. Variable(s) entered on step 1: Sex, Watering Methods.

CHAPTER-IV (RESULTS)
74
4.8. Equine Piroplasmosis
Out of 430 serum samples collected from studied areas, 226 (52.5%) were found cELISA
positive for piroplasmosis (Theileria equi, Babesia caballi or mix infection) (Table-22). No
piroplasm could be seen in the Giemsa stained blood smears. Seroprevalence of T. equi was
significantly higher, 2 (1df) = 38.07, P= 0.00 i.e. 41.2% (n=177) as compared to B. caballi
(n=93, 21.6%). A significant difference regarding this seroprevalence was observed between the
equines of Lahore (95.6%) and others metropolises, 2 (4df) = 24.49, P<0.01. Seroprevalence of
piroplasmosis was found to be 64% in equines of Faisalabad followed by Multan (52.9%),
Gujranwala (50.7%) and Bahawalpur (50%). Difference regarding prevalence of piroplasmosis
in equines of Faisalabad, Multan, Gujranwala and Bahawalpur was not significant, 2 (3df) =
5.99, P= 0.112.
4.8a. Clinical Signs Found in Equines Tested Positive for Piroplasmosis
Analysis of clinical examination data (Table-23) indicated that anorexia (n=47) was mostly
observed non specific clinical finding followed by debility (n=18) in equines found seropositive
for piroplasmosis. More specific clinical findings in decreasing order were pale mucous
membranes (n=47), fever (n=31), congested mucous membranes (n=21), eyelid edema with
muco-purrulent discharge (n=20), edema of the distal limb (n=12), enlarged lymph nodes (n=10)
and patechial hemorrhages on the mucous membranes (n=5).

CHAPTER-IV (RESULTS)
75
4.8b. Seroprevalence of Theileria equi Infection the Equines of Selected Areas
Out of 430 equine serum samples collected from studied areas, 177 (41.2%) were found sero-
positive on the basis of commercial competitive enzyme linked immunosorbent assay (VMRD,
USA).
4.8c. Area Related Seroprevalence of Theileria equi Infection
Highest seroprevalence of Theileria equi (Table-24) was recorded in the equines Lahore (66.7%)
followed by those of Faisalabad (42%), Multan (35.3%), Bahawalpur (33.8%) and Gujranwala
(28%). This difference in seroprevalence was significant between Lahore and other metropolises,
2 (4df) =26.41, P<0.01. However, seroprevalence of T. equi in Faisalabad, Multan, Bahawalpur
and Gujranwala was not significantly different, 2 (3df) =4.56, P=0.206.
4.8d. Equine Species Dependant Seroprevalence of Theileria equi Infection
Among three species of sampled draught equine population (n=430), significantly different
seroprevalence,2 (2df) =9.39, P=0.009 (Table-24) of T. equi was found in horses i.e. 56.9%
(n=37) than mules (48.5%, n=16) and donkeys (37.3%, n=124). Prevalence of T. equi was
recorded highest in horses of Lahore, where all the 13 (100%) animals were found sero-positive.
This prevalence was recorded in descending order as 70% (n=7), 50% (n=5), 38.9% (n=7) and
35.7% (n=5) in horses of Multan, Bahawalpur, Faisalabad and Gujranwala respectively.
Prevalence of T. equi infection in mules of Lahore was 100% (n=6), followed by 66.7% (n=4) in
mules of Multan. Third highest prevalence was recorded in the mules of Faisalabad i.e. 44.4%
(n=4) followed by 16.7% (n=1) each in Bahawalpur and Gujranwala respectively. Out of 124

CHAPTER-IV (RESULTS)
76
cELISA positive donkey sera, highest prevalence (54%) was recorded in Lahore where 27
animals were found positive followed by 42.3% (n=52), 32.7% (n=17), 27.3% (n=15) and 25%
(n=13) in Faisalabad, Bahawalpur, Gujranwala and Multan respectively.
4.8c. Age Related Seroprevalence of Theileria equi Infection
Analysis of age related data of Theileria equi positive equine population (n=177) is presented in
Table-25 indicated towards higher prevalence of T. equi in horses of age group-I (5 Years or
less) i.e. 72.7% followed by 60% in group-III (above 10 Years) and 48.3% in group-II (6-10
Years). Relatively steady pattern of T. equi prevalence was observed in mules where prevalence
increased with age of animals i.e. 25%, 55.6% and 57.1% in group-I, II and III. Highest
prevalence of T. equi was observed in donkeys of age group-II (39.9%) followed by group-III
(36.9%) and group-I (34.4%). Overall prevalence of T. equi increased with age in equines i.e.
36.9, 42.6 and 44.3 percent in group-I, II and III respectively. However, there was no significant
difference found among the seroprevalence regarding 3 age groups, 2 (2df) =1.56, P=0.457.
4.8d. Sex Dependant Seroprevalence of Theileria equi Infection
Prevalence of Theileria equi was not significantly different, 2 (1df) =0.93, P=0.45 (42.7%,
n=126) in male equines (Table-26) as compared to females (37.8%, n=51). Out of 65 (25 male
and 40 female) horses, this prevalence was higher in male horses (64%) as compared to females
(52.5%). Analysis of serum samples from mules (n=33) revealed that out of 18 males 10 were
sero-positive (55.5%) and 6 (40%) out of 15 females were sero-reactive for T. equi. Out of 332
donkeys sera, 100 (39.7%) males and 24 (30%) females were found sero-positive for Theileria
equi.

CHAPTER-IV (RESULTS)
77
Table-22 Seroprevalence of piroplasmosis in equines (n=430) of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis Metropolis (Samples Taken)
T. equi Positive (Prevalence)
B. caballi Positive (Prevalence)
Mix infection (Prevalence)
Total (Prevalence) (T. equi + B. caballi)
Multan
(n = 68) 24 (39.7) 12 (17.6) 5 (7.4) 36 (52.9)b
Bahawalpur
(n = 68) 23 (33.8) 11 (16.2) 4 (5.9) 34 (50.0)b
Faisalabad
(n = 150) 63 (42.0) 33 (22.0) 17 (11.3) 96 (64.0)b
Lahore
(n = 69) 46 (66.7) 20 (28.9) 12 (17.4) 66 (95.7)a
Gujranwala
(n = 75) 21 (28.0) 17 (22.7) 6 (8.0) 38 (50.7)b
Total 177 (41.2)a 93 (21.6)b 44 (10.2) 226 (52.6)
Values with different superscript alphabets in the column differ significantly, 2 (4df)=24.49, P<0.01)
Values with different superscript alphabets in the rows differ significantly, 2
(1df)=38.07, P<0.01)

CHAPTER-IV (RESULTS)
78
Table-23 Clinical findings in the equines (n = 430) of 5 draught equine populated urban areas of Punjab found sero-positive (n=226) for piroplasmosis (T. equi and B. caballi)
Clinical Finding T. equi + B. caballi + T. equi & B. caballi
Fever 23 8 9
anorexia 38 9 19
Pale Mucous Membranes 35 12 16
Congested Mucous Membranes 16 5 6
Patechial Hamorrhages on M. M. 4 1 4
Edema of the Distal Limb 11 1 5
Enlarged Lymph Nodes 5 5 7
Asthenia (Debility) 14 4 4
Eyelid edema with muco-purulent discharge 17 3 8
Polyuria 0 3 5
Colic 5 2 2
Small & dry feces 3 2 3

CHAPTER-IV (RESULTS)
79
Table-24 Seroprevalence of Theileria equi infection in the equines surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis from 5 draught equine populated urban areas of Punjab
Location Samples Examined
Horses
(Prevalence %)
Mules
(Prevalence %)
Donkey
(Prevalence %)
Total
(Prevalence %)
Multan 68 (10H, 6M, 52D) 7 (70.0) 4 (66.7) 13 (25.0) 24 (35.3)b
Bahawalpur 68 (10H, 6M, 52D) 5 (50.0) 1 (16.7) 17 (32.7) 23 (33.8)b
Lahore 69 (13H, 6M, 50D) 13 (100) 6 (100) 27 (54.0) 46 (66.7)a
Gujranwala 75 (14H, 6M, 55D) 5 (35.7) 1 (16.7) 15 (27.3) 21 (28.0)b
Faisalabad 150 (18H, 9M, 123D) 7 (38.9) 4 (44.4) 52 (42.3) 63 (42.0)b
Total 430 (65H, 33M, 332D) 37 (56.9)a 16 (48.5)b 124 (37.3)b 177 (41.2)
Values with different superscript alphabets in the column differ significantly, 2 (4df) =26.41, P<0.01
Values with different superscript whole number in a row differ significantly, 2 (2df) =9.39, P=0.009
H: Horse M: Mule D: Donkey

CHAPTER-IV (RESULTS)
80
Table-25 Comparative age related seroprevalence of T. equi infection in equines of 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
Type of
Equine
Samples Examined
(<5y, < 10y, > 10y)
No. of equines positive for T. equi in each
age group (Prevalence %)
< 5 Y < 10 Y > 10Y
Horses 65 (11,29,25) 8 (72.7) 14 (48.3) 15 (60)
Mules 33 (8,18,7) 2 (25) 10 (55.6) 4 (57.1)
Donkeys 332 (119,148,65) 41 (34.4) 59 (39.9) 24 (36.9)
Total 430 (138, 195, 97) 51 (36.9)a 83 (42.6)a 43 (44.3)a
Values with similar superscript alphabets are not significantly different, 2 (2df) =1.56, P=0.457
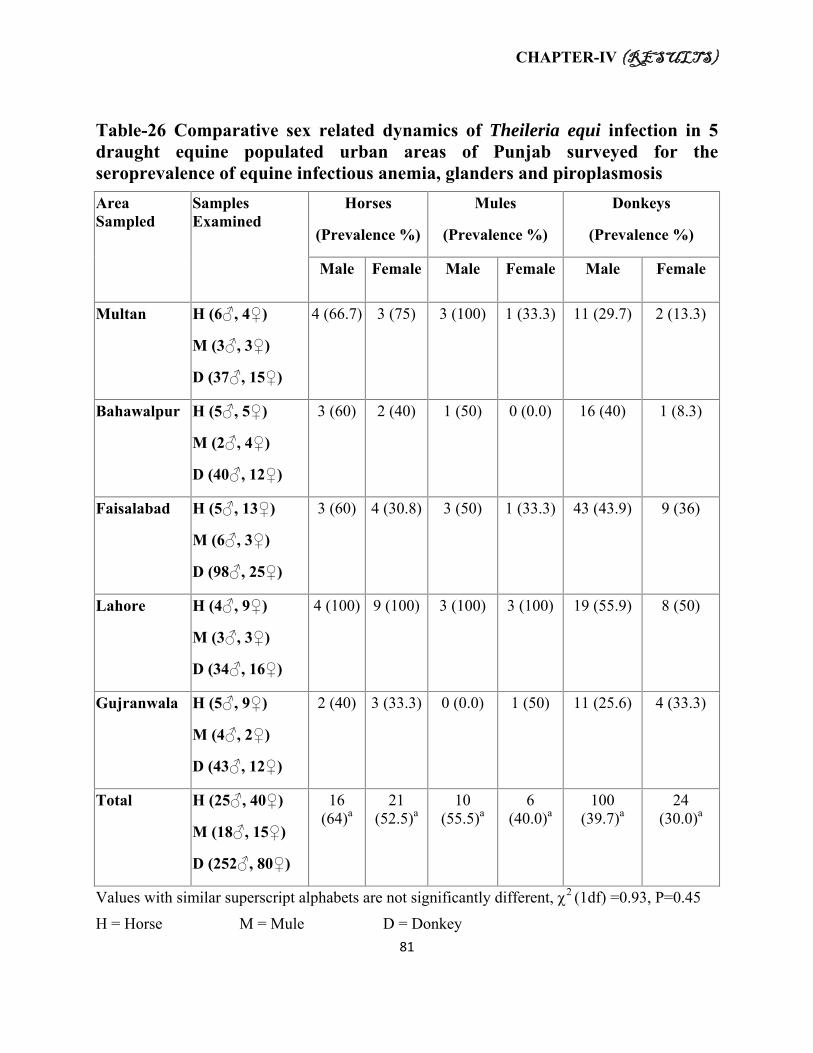
CHAPTER-IV (RESULTS)
81
Table-26 Comparative sex related dynamics of Theileria equi infection in 5 draught equine populated urban areas of Punjab surveyed for the seroprevalence of equine infectious anemia, glanders and piroplasmosis
Area Sampled
Samples Examined
Horses
(Prevalence %)
Mules
(Prevalence %)
Donkeys
(Prevalence %)
Male Female Male Female Male Female
Multan H (6♂, 4♀)
M (3♂, 3♀)
D (37♂, 15♀)
4 (66.7) 3 (75) 3 (100) 1 (33.3) 11 (29.7) 2 (13.3)
Bahawalpur H (5♂, 5♀)
M (2♂, 4♀)
D (40♂, 12♀)
3 (60) 2 (40) 1 (50) 0 (0.0) 16 (40) 1 (8.3)
Faisalabad H (5♂, 13♀)
M (6♂, 3♀)
D (98♂, 25♀)
3 (60) 4 (30.8) 3 (50) 1 (33.3) 43 (43.9) 9 (36)
Lahore H (4♂, 9♀)
M (3♂, 3♀)
D (34♂, 16♀)
4 (100) 9 (100) 3 (100) 3 (100) 19 (55.9) 8 (50)
Gujranwala H (5♂, 9♀)
M (4♂, 2♀)
D (43♂, 12♀)
2 (40) 3 (33.3) 0 (0.0) 1 (50) 11 (25.6) 4 (33.3)
Total H (25♂, 40♀)
M (18♂, 15♀)
D (252♂, 80♀)
16 (64)a
21 (52.5)a
10 (55.5)a
6 (40.0)a
100 (39.7)a
24 (30.0)a
Values with similar superscript alphabets are not significantly different, 2 (1df) =0.93, P=0.45
H = Horse M = Mule D = Donkey

CHAPTER-IV (RESULTS)
82
4.8e. Seroprevalence of Babesia caballi Infection
In the studied equine population (n=430) of 5 areas, 93 sera were found positive for antibodies
against B. caballi infection and seroprevalence was found to be 21.6% (Table-27).
4.8f. Area Related Seroprevalence of Babesia caballi Infection
Seroprevalence of B. caballi infection (Table-27) in descending order was found to be 28.9, 22.7,
22, 17.6 and 16.2 percent in Lahore (n=20), Gujranwala (n=17), Faisalabad (n=33), Multan
(n=12) and Bahawalpur (n=11) respectively. However, this prevalence difference was not
statistically significant, 2 (4df) =4.09, P=0.394.
4.8g. Equine Species Related Seroprevalence of Babesia caballi Infection
Highest prevalence of B. caballi (Table-27) was observed in mules (30.3%) followed by horses
(24.6%) and donkeys (20.2%). However, this difference was not statistically significant, 2 (2df)
=2.218, P=0.33. Out of 65 horse sera from 5 different areas, highest prevalence was observed in
Lahore i.e. 30.8% (n=4) followed by 30% (n=3) in Multan, 28.6% (n=4) in Gujranwala, 20%
(n=2) in Bahawalpur and 16.7% (n=3) in Faisalabad. Within the mule species highest
seroprevalence was recorded in Lahore (50%) followed by Gujranwala (33.3%), Faisalabad
(33.3%), Multan (16.7%) and Bahawalpur (16.7%). Babesia caballi seroprevalence was highest
in donkeys of Lahore where 13 (26%) animals were found cELISA positive followed by
Faisalabad (21.9%), Gujranwala (20%), Bahawalpur and Multan (15.4% each).

CHAPTER-IV (RESULTS)
83
4.8h. Age Related Seroprevalence of Babesia caballi Infection
Age related dynamics of B. caballi are given in Table-28. Higher seroprevalence of B. caballi
was found in age group-III (more than 10 years) i.e. 27.8% (n=27) followed by group-II (6-10
years) 22.6% (n=44) and group-I (5 years or less) where it was found as 15.9% (n=22). The
difference in seroprevalence between group-III and group-I was found to be significant, 2 (1df)
=4.88, P=0.02. However, in general this seroprevalence was not significantly affected by
different age groups, 2 (2df) =4.938, P=0.085. Highest seroprevalence was observed in horses of
age group-I (27.3%) followed by group-II (24.1%) and III (24%). Mule sera from age group-III
reacted most (57.1%) to commercial B. caballi antibody test kit cELISA as compared to animals
in group-I (37.5%) and II (16.7%). Sero-prevalence of B. caballi increased with age in donkeys
with lowest prevalence was recorded in animals of group-I (13.4%) that increased to 22.9% and
26.1% in group-II and III respectively.
4.8i. Sex Related Seroprevalence of Babesia caballi Infection
There wasn’t a significant difference, 2 (1df) =0.002, P=0.96 regarding the sero-prevalence of
B. caballi in two sexes of equines (Table-29). Higher prevalence (21.7%, n=64) was recorded in
male as compared to female (21.5%, n=29) equines. Prevalence of B. caballi was higher 44% in
male horses (n=11) as compared to 12.5% in females (n=5). Relatively less difference in
prevalence was observed in male (33.3%, n=6) and female (26.7%, n=4) mules. Out of total 252
male donkeys, 47 (18.6%) were found sero-positive that was lower than the females (25%,
n=20).

CHAPTER-IV (RESULTS)
84
Table-27 Seroprevalence of Babesia caballi infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Location Samples Examined Horses (Prev. %)
Mules (Prev. %)
Donkey (Prev. %)
Total (Prev. %)
Multan 68 (10H, 6M, 52D) 3 (30.0) 1 (16.7)
8 (15.4) 12 (17.6)a
Bahawalpur 68 (10H, 6M, 52D) 2 (20.0) 1 (16.7) 8 (15.4) 11 (16.2)a
Faisalabad 150 (18H, 9M, 123D) 3 (16.7) 3 (33.3) 27 (21.9) 33 (22.0)a
Lahore 69 (13H, 6M, 50D) 4 (30.8) 3 (50.0) 13 (26.0) 20 (28.9)a
Gujranwala 75 (14H, 6M, 55D) 4 (28.6) 2 (33.3) 11 (20.0) 17 (22.7)a
Total 430 (65H, 33M, 332D) 16 (24.6)1 10 (30.3)1 67 (20.2)1 93 (21.6)
Values with similar superscript alphabets are not significantly different, 2 (4df) =4.09, P=0.394
Values with similar superscript whole number are not significantly different, 2 (2df) =2.21, P=0.33
Table-28 Comparative age related seroprevalence of B. caballi infection in 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
Type of Equine
Samples Taken
(<5y, < 10y, > 10y)
No. of equines positive for B. caballi in each age group (Prevalence %)
< 5 Y < 10 Y > 10Y
Horses 65 (11,29,25) 3 (27.3)a 7 (24.1)a 6 (24)a
Mules 33 (8,18,7) 3 (37.5)a 3 (16.7)a 4 (57.1)a
Donkeys 332 (119,148,65) 16 (13.4)a 34 (22.9)a 17 (26.1)a
Total 430 (138, 195, 97) 22 (15.9)3 44 (22.5)1,3 27 (27.8)1
Values with similar superscript alphabet in a column are not significantly different (P > 0.05)
Values with different superscript whole number in the row are significantly different (P < 0.05)

CHAPTER-IV (RESULTS)
85
Table-29 Comparative sex related dynamics of Babesia caballi infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Area Sampled Samples Taken Horses (Prevalence %)
Mules (Prevalence %)
Donkeys (Prevalence %)
Male Female Male Female Male Female
Multan H (6♂, 4♀)
M (3♂, 3♀)
D (37♂, 15♀)
2 (33.3) 1 (25.0) 0 (0.0) 1 (33.3) 6 (16.2) 2(13.3)
Bahawalpur H (5♂, 5♀)
M (2♂, 4♀)
D (40♂, 12♀)
2 (40.0) 0 (0.0) 1 (50.0) 0 (0.0) 7 (17.5) 1(8.3)
Faisalabad H (5♂, 13♀)
M (6♂, 3♀)
D (98♂, 25♀)
2 (40.0) 1 (7.7) 2(33.3) 1(33.3) 19 (19.4) 8 (32.0)
Lahore H (4♂, 9♀)
M (3♂, 3♀)
D (34♂, 16♀)
2 (50.0) 2 (22.2) 1(33.3) 2 (66.7) 8 (23.5) 5(31.3)
Gujranwala H (5♂, 9♀)
M (4♂, 2♀)
D (43♂, 12♀)
3 (60.0) 1 (11.1) 2 (50.0) 0 (0.0) 7 (16.3) 4(33.3)
Total H (25♂, 40♀)
M (18♂, 15♀)
D (252♂, 80♀)
11 (44.0)a 5 (12.5)a 6 (33.3)a 4 (26.7)a 47 (18.6)a 20 (25.0)a
Values with similar superscript alphabet are not significantly different, 2 (1df) =0.002, P=0.96

CHAPTER-IV (RESULTS)
86
4.8j. Seroprevalence of Mixed Infection of Theileria equi and Babesia caballi
A total of 44 (10.2%) out of 430 equines were found sero-positive for both T. equi and B. caballi
(Table-30).
4.8k. Area Related Seroprevalence of Mixed Infection
Analysis of data presented in Table-31 revealed that highest sero-prevalence of mix infection
was in Lahore (17.4%) followed by Faisalabad (11.3%), Gujranwala (8%), Multan (7.4%) and
Bahawalpur (5.9%). Chi square analysis revealed that this prevalence was not significantly
different, 2 (4df) =6.469, P=0.167 in equines of Lahore, Faisalabad, Gujranwala, Multan and
Bahawalpur.
4.8l. Equine Species Related Seroprevalence of Mix Infection
Data regarding equine species related mix infection seroprevalence of B. caballi and T. equi is
presented in Table-31. Analysis indicated that mix infection was higher in mules (15.1%) of
studied population followed by horses (12.3%) and donkeys (9.3%). Prevalence of mix infection
in mules, horses and donkeys was found to be statistically not significantly different, 2 (2df)
=1.464, P=0.481. Mix infection was higher in horses of Lahore (30.8%) followed by of
Faisalabad (11.1%), Multan (10%), Gujranwala (7.1%) and Bahawalpur (0%). In mules (n=33),
mix infection was highest in Lahore (50%) followed by Faisalabad (22.2%). No mule sera from
Gujranwala, Multan and Faisalabad were found sero-positive for mix infection. Highest
prevalence of mix infection was found in donkeys of Faisalabad (10.6%) followed by donkeys of
Lahore (10), Gujranwala (9.1%), Multan (7.7%) and Bahawalpur (7.7%).

CHAPTER-IV (RESULTS)
87
4.8m. Age Related Seroprevalence of Mixed Infection
Higher prevalence (14.4%) of mix infection was recorded in equines of age group-III (more than
10 years) where 14 equines were found sero-reactive to both B. caballi and T. equi commercial
cELISA test kits followed by 10.8% (n=21) and 6.5% (n=9) in group-II (6-10 years) and I (5
years or less) respectively (Table-32). However, this difference was statistically not significant,
2 (2df) =3.99, P=0.136. Computed age based sero-prevalence of mixed infection in horses was
18.2% in age group-I followed by 16% and 6.9% in group-III and II. In mules (n=33), highest
prevalence (28.6%) was observed in group-III followed by 12.5% in group I and 11.1% in group-
II. In donkeys (n=332), sero-prevalence of mix infection increased with age and lowest
prevalence (5.04%) was observed in animals of age group-I that increased to 11.5 and 12.3
percent in group-II and group-III. However, all these differences were found to be statistically
not significant on chi square analysis (P > 0.05).
4.8n. Sex Related Seroprevalence of Mixed Infection
Data regarding sex related seroprevalence of mixed infection revealed that 29 out of 295 male
and 15 out of 135 female equines were found sero-positive for both prioplasms (Table-33). This
seroprevalence of mix infection was higher in females (11.1%) than males (9.8%). However, this
difference was statistically not significant, 2 (1df) =0.165, P=0.684.

CHAPTER-IV (RESULTS)
88
Table-30 T. equi and B. caballi mixed infection in 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Table-31 Seroprevalence of T. equi and B. caballi mixed infection in 5 draught equine populated urban areas of Punjab surveyed for prevalence of equine infectious anemia, glanders and piroplasmosis
Location Samples Examined
Horses (Prevalence %)
Mules (Prevalence %)
Donkeys (Prevalence %)
Total (Prevalence %)
Multan 68 (10H, 6M, 52D)
1 (10.0) 0 (0.0) 4 (7.7) 5 (7.4)a
Bahawalpur 68 (10H, 6M, 52D)
0 (0.0) 0 (0.0) 4 (7.7) 4 (5.9)a
Faisalabad 150 (18H, 9M, 123D)
2 (11.1) 2 (22.2) 13 (10.6) 17 (11.3)a
Lahore 69 (13H, 6M, 50D)
4 (30.8) 3 (50.0) 5 (10.0) 12 (17.4)a
Gujranwala 75 (14H, 6M, 55D)
1 (7.1) 0 (0.0) 5 (9.1) 6 (8.0)a
Total 430 (65H, 33M,332D)
8 (12.3)1 5 (15.1)1 31 (9.3)1 44 (10.2)
Values with similar superscript alphabet in column are not significantly different, 2 (4df) =6.469, P=0.167
Values with similar superscript whole number in a row are not significantly different, 2 (2df) =1.464, P=0.481
T. equi + T. equi - Total
B. caballi + 44 (10.2%) 49 (11.4%) 93 (21.6%)
B. caballi - 133 (30.9%) 204 (47.4%) 337 (78.4%)
177 (41.2%) 253 (58.8%) 430 (100%)

CHAPTER-IV (RESULTS)
89
Table-32 Age related seroprevalence of mixed infection with Theileria equi and Babesia caballi in equines of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Equine Species Samples Taken Number of equines positive for B. caballi & T. equi in each age group (Prevalence %)
(<5y, < 10y, > 10y) < 5 Y < 10 Y > 10Y
Horses 65 (11,29,25) 2 (18.2) 2 (6.9) 4 (16)
Mules 33 (8,18,7) 1 (12.5) 2 (11.1) 2 (28.6)
Donkeys 332 (119,148,65) 6 (5.0) 17 (11.5) 8 (12.3)
Total 430 (138, 195, 97) 9 (6.5)a 21 (10.8)a 14 (14.4)a
Values with similar superscript alphabet are not significantly different, 2 (2df) =3.99, P=0.136
Table-33 Sex related prevalence of mixed infection with Theileria equi and Babesia caballi in equines of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Values with similar superscript alphabet are not significantly different, 2 (1df) =0.165, P=0.684
Total Examined B. caballi positive T. equi positive Mix Infection
295 Male 64 (21.7%) 126 (42.7%) 29 (9.8%)a
135 Female 29 (21.5%) 51 (37.8%) 15 (11.11%)a
Total 93 (21.6%) 177 (41.2%) 44 (10.2%)

CHAPTER-IV (RESULTS)
90
4.8o. Hematological Analysis of Piroplasmosis Positive Equine Blood Samples
Results of hematological analysis of equines found sero-positve for T. equi and B. caballi are
described in Table-34, 35, 36 and 37.
Hematological analysis results regarding the horses (n=53) found sero-positive for
piroplasmposis (Theileria equi and Babesia equi) is presented in Table-34. Significantly lower
(P<0.05) than reference value mean white blood (WBC) cell counts were observed in horses
positive for T. equi (6.01+1.79), B. caballi (5.33+1.77) and mix infection (5.27+1.87). However,
these values were not statistically different (P>0.05) among horses positive for T. equi, B. caballi
and mix infections. A statistically not significant difference (P>0.05) was observed regarding
mean RBC counts among horses found positive for T. equi (5.61+1.26), B. caballi (5.31+1.15)
and mixed infection (5.25+1.38). Although, these values were numerically lower than reference
RBC count value (5.93+2.81) but this difference was not significant (P>0.05). Mean hemoglobin
concentration was significantly lower (P<0.05) than reference value (10.93+1.89) in T. equi
(9.55+2.00) and B. caballi (9.28+2.24) sero-reactive horses. However, mean Hb concentration
found in mix infection positive horses (9.81+2.7) was not significantly lower (P>0.05) than
reference value. There was not a significant difference (P>0.05) among horses found positive for
T. equi, B. caballi and mix infection. Packed cell volume (PCV) was significantly lower
(P<0.05) in horses sero-positive for T. equi (28.69+4.07), B. caballi (26.08+2.93) and mix
infection (27.63+2.91) than the reference value (37.75+4.57). Difference between mean packed

CHAPTER-IV (RESULTS)
91
cell volume among horses sero-positive for T. equi, B. caballi and mix infection was not
significant (P>0.05). Erythrocytic indices indicated presence of microcytic hyperchromic type of
anemia in horses found seropositive for T. equi, B. caballi and mixed infection.
Hematological data regarding donkeys (n=191) found sero-positive for T. equi, B. caballi and
mix infection is presented in Table-35. Significantly lower (P < 0.05) than reference value (9.75 +
3.29) mean white blood count was observed in donkeys found sero-positive for T. equi (6.41 +
1.98), B. caballi (6.15 + 1.96) and mix infection (5.96 + 2.00). Mean red blood cell counts were
not significantly (P > 0.05) lower than the reference values with lowest mean RBC count was
observed in donkeys found positive for both T. equi and B. caballi (5.16 + 2.00) followed by B.
caballi (5.22 + 1.48) and T. equi (5.52 + 1.48) seropositive donkeys. Mean hemoglobin
concentration was not significantly (P > 0.05) different from reference value (9.01 + 2.65) in
donkeys sero-positive for B. caballi (9.01 + 1.86), T. equi (8.88 + 1.88) and mix infection (8.83 +
1.88). A significantly lower (P < 0.05) mean packed cell volume values were recorded in
donkeys cELISA positive for mix infection (29.57 + 5.42), T. equi (29.07 + 5.74) and B. caballi
(28.28 + 5.31). Mean corpuscular volume values were 60.88, 58.58 and 56.01 (fl) in mix
infection, B. caballi and T. equi positive donkeys respectively. Mean corpuscular hemaoglobin
(pg) was 18.55 in B. caballi positive donkeys followed by 18.18 and 16.99 in mix infection and
T. equi positive donkeys respectively. Mean corpuscular hemoglobin concentration (g/dL)

CHAPTER-IV (RESULTS)
92
numerically higher in donkeys seropositive for B. caballi (32.79) followed by 31.46 and 30.45 in
T. equi and mix infection positive donkeys respectively. On the basis of eryhtrocytic indices
macrocytic hyperchromic type of anemia was observed in all three types of sero-positive
animals.
Hematological data regarding piroplasmosis affected mules (n = 26) is presented in the Table-36.
Mean white blood cell counts were found to be significantly lower (P < 0.05) than reference
values (9.40 + 2.89) in mules seropositive for T. equi (6.94 + 2.28) , B. caballi (6.26 + 2.52) and
mix infection (5.92 + 2.68). However, difference between T. equi, B. caballi and mix infection
seropositive mules regarding WBC counts were statistically not significant (P > 0.05). Mean red
blood cell counts were not significantly lower (P > .05) than reference value in B. caballi (5.70 +
1.91), T. equi (5.27 + 1.3) and mix infection (5.00 + 0.55) sero positive mules. Mean
hemoglobin concentrations in mules seropositive for T. equi (9.69 + 2.01), B. caballi (9.00 +
2.31) and mix infection (9.32 + 2.15) were not significantly (P > 0.05) different than reference
value (10.10 + 0.73). Recorded values regarding mean packed cell volume for T. equi (29.45 +
4.04), B. caballi (29.22 + 4.42) and mix infection (31.16 + 4.01) sero reactive mules were
significantly lower (P < 0.05) than reference value (34.37 + 4.13). Mean corpuscular volume
values were 63.04, 55.10 and 59.67 (fl) in mix infection, B. caballi and T. equi positive mules
respectively. Mean corpuscular hemaoglobin (pg) was 16.57, 18.73 and 19.1 in B. caballi, mix

CHAPTER-IV (RESULTS)
93
infection and T. equi positive mules. Mean corpuscular hemoglobin concentration (g/dL) was
numerically higher in donkeys seropositive for T. equi (33.38) followed by 30.73 and 29.92 in B.
caballi and mix infection positive mules respectively.
Hematological data regarding the comparison of piroplasmosis affected horses (n =45), mules (n
= 21) and donkeys (n = 160) is presented in Table-37. Mean white blood cell (WBC) counts
were significantly (P < 0.05) lower in horses (5.90 + 1.79), donkeys (6.86 + 2.30) and mules
(6.41 + 1.96) than their respective reference values. Comparatively mean WBC count was
significantly (P > 0.05) lower in horses than piroplasmosis sero-positive mules and donkeys.
Mean red blood cell (RBC) counts were numerically but statistically not significantly lower (P >
0.05) than reference values in horses (5.57 + 1.21), donkeys (5.48 + 1.47) and mules (5.54 +
1.69). Mean hemoglobin concentration was significantly lower (P < 0.05) than reference value
(10.93 + 1.89) in piroplasmosis seropositive horses (9.41 + 1.95). However, Hb. concentrations
were not statistically significantly lower (P > 0.05) than reference values in seropositive donkeys
(8.92 + 1.81) and mules (9.45 + 2.15). Mean packed cell volume (PCV) values were significantly
lower (P < 0.05) than reference values in piroplasmosis seropositive horses (27.95 + 4.57),
donkeys (28.64 + 5.66) and mules (28.93 + 4.10).

CHAPTER-IV (RESULTS)
94
Table-34 Hematological values of horses found positive (n = 53) for piroplasmosis in 5 draught equine populated urban areas of Punjab
PIROPLASMOSIS
POSITIVE
PARAMETERS WBC/10³μL RBC/10μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
REFERENCE 7.18 + 2.87 5.93 + 2.81 10.93 + 1.89 37.75 + 4.57 63.66 18.43 28.95
T. equi
(N = 37) Mean 6.01 + 1.79Sa
5.61 +
1.26a 9.55 + 2Sa 28.69 + 4.07Sa 53.65 17.82 33.73
B. caballi
(N = 16) Mean 5.33 + 1.77Sa
5.31 +
1.15a 9.28 + 2.24Sa 26.08 + 2.93Sb 52.34 18.69 35.59
Mix Infection
(N = 8) Mean 5.27+ 1.87Sa
5.25 +
1.38a 9.81+ 2.7NSa 27.63 + 2.91S* 57.27 20.41 35.79
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with ‘NS’ superscript are non significantly (P > 0.05) different from the reference value Values with ‘S’ superscript are significantly (P < 0.05) different from the reference value Values with same alphabetic superscript are non significantly (P > 0.05) different from each other

CHAPTER-IV (RESULTS)
95
Table-35 Hematological values of donkeys found positive (n = 191) for piroplasmosis in 5 draught equine populated urban areas of Punjab
PIROPLASMOSIS
POSITIVE
PARAMETERS WBC/10³μL RBC/10μL Hb (g/dL) HcT (%)
MCV
(fl)
MCH
(pg)
MCHC
(g/dL)
REFERENCE 9.75 + 3.29 5.88 + 2.65 9.01 + 1.13 32.42 + 4.38 55.13 15.32 27.79
T. equi (N = 124) Mean 6.41 + 1.98 Sa 5.52 +1.48NSa 8.88 + 1.88NSa 29.07 + 5.74Sa 56.01 16.99 31.46
B. caballi (N = 67) Mean 6.15 + 1.96 Sa 5.22 + 1.48NSa 9.01 + 1.86NSa 28.28 + 5.31Sa 58.58 18.55 32.79
Mix (N = 31) Mean 5.96 + 2Sa 5.16 + 1.5NSa 8.83 + 2.09NSa 29.57 + 5.42Sa 60.88 18.18 30.45
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with ‘NS’ superscript are non significantly (P > 0.05) different from the reference value Values with ‘S’ superscript are significantly (P < 0.05) different from the reference value Values with same alphabetic superscript are non significantly (P > 0.05) different from each other

CHAPTER-IV (RESULTS)
96
Table-36 Hematological values of mules found positive (n = 26) for piroplasmosis in 5 draught equine populated urban areas of Punjab
PIROPLASMOSIS
POSITIVE
Parameters WBC/10³μL RBC/10μL Hb (g/dL) HcT (%) MCV (fl) MCH (pg) MCHC (g/dL)
REFERENCE 9.40 + 2.89 5.74 + 2.62 10.10 + 0.73 34.37 + 4.13 59.88 17.59 29.38
T. equi
(N = 16) Mean 6.94 + 2.28Sa 5.27 + 1.3NSa 9.69 + 2.01NSa 29.45 + 4.04 Sa 59.67 19.1 33.38
B. caballi
(N = 10) Mean 6.26 + 2.52Sa 5.7 + 1.91NSa 9 + 2.31NSa 29.22 + 4.42Sa 55.1 16.57 30.73
Mix
(N = 5) Mean 5.92 + 2.68Sa 5 + 0.55NSa 9.32 + 2.15NSa 31.16 + 4.01Sa 63.04 18.73 29.92
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with ‘NS’ superscript are non significantly (P > 0.05) different from the reference value Values with ‘S’ superscript are significantly (P < 0.05) different from the reference value Values with same alphabetic superscript are non significantly (P > 0.05) different from each other

CHAPTER-IV (RESULTS)
97
Table-37 Comparison of hematological values in equines (n = 226) found positive for piroplasmosis in 5 draught equine populated urban areas of Punjab
PIROPLASMOSIS
POSITIVE
Parameters WBC/10³μL RBC/10μL Hb
(g/dL)
HcT
(%)
MCV
(fl)
MCH
(pg)
MCHC
(g/dL)
Horses
(N = 45)
Reference 7.18 + 2.87 5.93 + 2.81 10.93 + 1.89 37.75 + 4.57 63.66 18.43 28.95
Mean 5.9 + 1.79 Sb 5.57 + 1.21 9.41 + 1.95S 27.96 + 4.1S 52.54 17.67 34.03
Donkeys
(N = 160)
Reference 9.75 + 3.29 5.88 + 2.65 9.01 + 1.13 32.42 + 4.38 55.13 15.32 27.79
Mean 6.41 + 1.96 Sa 5.48 + 1.47 8.92 + 1.81 28.64 + 5.66S 55.8 17.31 32.13
Mules
(N = 21)
Reference 9.40 + 2.89 5.74 + 2.62 10.10 + 0.73 34.37 + 4.13 59.88 17.59 29.38
Mean 6.86 + 2.3 Sa 5.54 + 1.69 9.45 + 2.15 28.93 + 4.1S 56.69 17.98 32.94
WBC = White blood cell RBC = Red blood cell Hb = Hemoglobin HcT = Hematocrit
MCV = Mean Corpuscular Volume MCH = Mean Corpuscular Hemoglobin MCHC = Mean Corpuscular Hemoglobin Concentration
Values with ‘NS’ superscript are non significantly (P > 0.05) different from the reference value Values with ‘S’ superscript are significantly (P < 0.05) different from the reference value Values with same alphabetic superscript are non significantly (P > 0.05) different from each other

CHAPTER-IV (RESULTS)
98
4.8p. Seroprevalence of Equine Piroplasmosis in Association with Housing Pattern of Equines
Analysis of data regarding the housing pattern of piroplasmosis sero-positive (n=226) and
negative (n=204) equines (Table-38) showed that 105 (46.5%) sero-positive equines were kept
alone, 59 (26.1%) managed with other equine cohorts and 62 (27.4%) equines were kept with
animals other than equines (cattle, buffalo, sheep, goat & dog). Univeriate analysis indicated that
equines kept alone or with equine cohorts were more likely to be positive for piroplasmosis
(OR=1.30, 95%CI=0.84-2.01). However, this difference was statistically not significant, 2 (2df)
=2.061, P=0.357.
4.8q. Seroprevalence of Equine Piroplasmosis in Association with Presence of Ticks on Cohorts
Analysis of data related to presence and absence of ticks on sampled equines and their cohorts is
reflected in table-39. In total, presence of ticks in cohorts was observed in 71 animals (16.5%).
Out of these equines, 38 (16.8%) were found positive for piroplasmopsis and 33 (16.2%) were
sero-negative. No significant difference regarding the prevalence of piroplasmosis in equines
living with tick infested and tick free cohorts was observed, 2 (1df) =0.032, P=0.859. Out of
226 equines found seropositive for piroplasmosis ticks were present on equines cohorts of 15
(6.6%) animals. Whereas, non equine (cattle, buffalo, sheep, goat and dog) cohorts of 23 (10.2%)
sero-reactive equines were tick infested. Odds of contracting piroplasmosis were found to be
more in equines living with tick positive equine cohorts (OR: 1.19, CI 95% 0.65-2.18) and non
equine cohorts (OR: 2.04, CI 95% 0.73-5.69) as compared to the equines living alone or with
cohorts having no ticks. However, when presence and absence of ticks was compared along with

CHAPTER-IV (RESULTS)
99
the housing pattern of studied equine population, no significant difference was observed, 2 (2df)
=1.898, P=0.387.
4.8r. Effect of Employing Tick Control Measures on Seroprevalence of Equine Piroplasmosis
Out of 111 equines where owners reported use of tick control measures 51 (45.9%) were found
seropositive for piroplasmosis. Whereas 54.8% (n=175) of those equines whose owners practiced
no tick control methods were positive for piroplasmosis (Table-40). Although equines belonging
to the owners who were not using tick control measures appeared to be more likely to contract
piroplasmosis (OR=1.43, 95% CI=0.93-2.21) but this difference was not significant, 2 (1df)
=2.624, P=0.105. A significant difference was observed regarding the seroprevalence among
equines of Lahore (2=4.326, df=1, P=0.038) when compared for the tick control used or not.
No significant difference (P>0.05) was observed regarding this among equines of other areas.
However, a significant difference (2=13.65, df=4, P=0.008) was observed regarding
seroprevalence of piroplasmosis between Lahore and other areas when compared for the tick
control.
4.8s. Treatment Chosen by the Veterinarians and Animal Health Workers against Piroplasmosis
Twenty veterinarians and animal health workers were randomly interviewed from each 5
sampled areas about their knowledge and understanding about recommended treatments for
Babesia caballi and Theileria equi (Table-41). Out of 100 respondents 88 veterinarians and
animal health workers told that they prefer to use recommended imidocarb treatment (2.2mg/kg,
two treatments at 24 hour intervals) in suspected cases. Only 12 veterinarians and animal health

CHAPTER-IV (RESULTS)
100
workers showed awareness and desire to use recommended Theileria equi treatment (4 mg/kg, 4
times at 72 hour intervals). Only 30% of these respondents reported to look at the stained blood
smears before starting the treatment in suspected cases.
4.8t. Multivariable Analysis Regarding Prevalence of Equine Piroplasmosis
Regarding seroprevalence of equine piroplasmosis 7 variables were used for initial bivariable
screening. Analysis was conducted regarding sero-positivity of T. equi, B. caballi, mix infection
and piroplasmosis in general. Out of these variables, metropolis (P<0.001), equine species
(P=0.009) and use of tick control measures (P=0.017) were significantly associated with high
prevalence of T. equi (Wald P < 0.2) and sex (P=0.33), age (0.26), housing (0.58) and presence
of ticks on cohorts (0.75) were not significantly associated with sero-prevalence of T. equi (Wald
P>0.2) (Table-42). Variables yielding Wald P < 0.2 were entered into a multivariable regression
model which resulted in only one variable remaining significant i.e. metropolis (P<0.001) so no
further model building was possible (Table-43).
Only age (P=0.085), presence of ticks on cohorts (P=0.016) and housing pattern of equines
(P=0.034) were significantly associated (Wald P < 0.2) with seroprevalence of B. caballi and
were entered into a model (Table-44). Housing pattern and age were knocked out at first and
second step and only presence of ticks on cohorts was significantly associated with prevalence of
B. caballi (P=0.017) (Table-45). Therefore, there was not a multivariable model to present for B.
caballi prevalence.
During bivariable analysis regarding the sero-prevalence of mix infection (T.equi and B. caballi),
metropolis (P=0.167), age (P=0.136), presence of ticks on cohorts (P=0.014), housing (P=0.186)

CHAPTER-IV (RESULTS)
101
and the use of tick control measures (P=0.119) were selected (P<0.2) for multivariate model
building (Table-46). Variables housing pattern, use of tick control, metropolis and age were
removed from the model at each step and only presence of ticks on cohorts was found
significantly associated with prevalence of mixed infection (P=0.016) (Table-47). This showed
that no multivariable model building was possible in this case.
Bivariable analysis regarding seroprevalence of piroplasmosis indicated metropolis (P<0.001),
equine species (P=0.003), age (P=0.182) and use of tick control (P=0.106) were the variables
significant enough (Wald P < 0.2) to be included in multivariable analysis (Table-48). However,
use of tick control measures and age were deleted from the model at subsequent steps. Resulting
final model suggested (Table-49) the prevalence of piroplasmosis in various equine species
might vary based on the different metropolis. For further analysis, categorical variables
(metropolis and equine species) were collapsed and tested for interaction term. For this purpose,
two new variables were created one comparing the prevalence of piroplasmosis in Lahore with
all other metropolis and other comparing the prevalence in horses with mules and donkeys. The
model was re-run with these new variables and interaction term to assess the inference that effect
of metropolis varies by equine species. However, inclusion of the interaction term did not
improve the fit of the model.

CHAPTER-IV (RESULTS)
102
Table-38 Comparison of housing pattern of equines (n=430) found positive (n=226) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
Values with same superscript alphabet are not significantly different, 2 (2df) =2.061, P=0.357
Area Sampled
Housing Pattern observed in piroplasmosis positive equines
Total equines Positive for piroplasmosis
Alone With Equines
With other animals
Multan 18 7 6 31
Bahawalpur 19 6 5 30
Faisalabad 37 19 23 79
Lahore 20 16 18 54
Gujranwala 11 11 10 32
Total 105a (46.5%) 59a (26.1%) 62a (27.4%) 226

CHAPTER-IV (RESULTS)
103
Table-39 Seroprevalence of piroplasmosis with reference to presence of ticks on the cohorts in equines found positive (n=226) and negative (n=204) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
Area Sampled
Piroplasmosis positive and tick
infested cohorts
Piroplasmosis negative and ticks
infested cohorts
Ticks on
Equine
Cohorts
Ticks on
other
Cohorts
Total Ticks on Equine
Cohorts
Ticks on
other
Cohorts
Total
Faisalabad 6 8 14 3 5 8
Lahore 4 7 11 1 2 3
Gujranwala 2 7 9 2 4 6
Multan 2 1 3 0 8 8
Bahawalpur 1 0 1 2 6 8
Total (%) 15a 23a 38 (16.8) 8 25 33 (16.2)
Values with same superscript alphabet are not significantly different, 2 (2df) =1.898, P=0.387.

CHAPTER-IV (RESULTS)
104
Table-40 Seroprevalence of piroplasmosis with reference to tick control practiced in equines found positive (n=226) and negative (n=204) for equine piroplasmosis in 5 draught equine populated urban areas of Punjab
Area Sampled
Piroplasmosis Negative Piroplasmosis Positive
Tick Control Used
Tick Control not Used
Tick Control Used
Tick Control not Used
Multan 13 24 14 17
Bahawalpur 17 21 8 22
Faisalabad 15 56 16 63
Lahore 5 10 6 48
Gujranwala 10 33 7 25
Total (%) 60 144 51 175

CHAPTER-IV (RESULTS)
105
Table-41 Preferred treatment protocol adopted by veterinarians and animal health workers (n=100) of 5 draught equine populated urban areas of Punjab in suspected cases of equine piroplasmosis
Location
Veterinarians / animal health workers interviewed
regarding preferred treatment against suspected
equine piroplasmosis cases
Prefer B. caballi treatment
(%)
Prefer T. equi treatment
(%)
Faisalabad 18 (90.00) 2 (10.00)
Lahore 15 (75.00) 5 (25.00)
Gujranwala 19 (95.00) 1 (5.00)
Multan 17 (85.00) 3 (15.00)
Bahawalpur 19 (95.00) 1 (5.00)
Total 88 (88.00) 12 (12.00)

CHAPTER-IV (RESULTS)
106
Table-42 Bivariable analysis for the seroprevalence of T. equi in equines (n=177) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
S. No. Exposure Variable Comparison Chi Square df Wald P Odds Ratio 95% CI Lower Upper
1 Metropolis 26.41 4 <0.001 Multan Gujranwala 1 0.349 1.403 0.691 2.848 Bahawalpur Gujranwala 1 0.452 1.314 0.645 2.678 Faisalabad Gujranwala 1 0.042 1.862 1.023 3.391 Lahore Gujranwala 1 0.00 5.143 2.528 10.464 2 Species of equine 9.39 2 0.009 Horse Donkey 1 .004 2.217 1.293 3.8 Mule Donkey 1 .213 1.579 0.77 3.237 All others Donkey Sex 3 Female Male 0.931 1 0.335 0.814 0.536 1.236 4 Age groups 1.568 2 0.457 5 or less More than 10y 1 0.257 0.736 0.434 1.25 6-10 Years More than 10y 1 0.774 0.931 0.57 1.521 5 Tick on Cohorts No ticks on cohorts 0.105 1 0.746 0.918 0.546 1.544 6 Housing 1.077 2 0.583 Alone Non equine cohorts 1 0.793 1.065 0.663 1.712 With Equine Non equine cohorts 1 0.508 0.836 0.493 1.419 7 Tick Control Not Used Used 5.731 1 0.017 1.742 1.103 2.752

CHAPTER-IV (RESULTS)
107
Table-43 SPSS output of binary logistic regression model for predicting T. equi infection in equines (n=177) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Variables
B S.E. Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Lower Upper
Step 2a Metropolis 22.685 4 .000
Multan(1) .418 .365 1.307 1 .253 1.519 .742 3.107
Bahawalpur(2) .339 .366 .854 1 .355 1.403 .684 2.876
Faisalabad(3) .617 .307 4.049 1 .044 1.854 1.016 3.383
Lahore(4) 1.619 .364 19.824 1 .000 5.049 2.476 10.299
Tick Controlled -.462 .243 3.624 1 .057 .630 .392 1.014
Constant -.848 .262 10.475 1 .001 .428
a. Variable(s) entered on step 1: Metropolis, Tick Control Used.

CHAPTER-IV (RESULTS)
108
Table-44 Bivariable analysis for the seroprevalence of B. caballi in equines (n=93) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
S. No. Exposure Variable Comparison Chi Square df Wald P Odds Ratio 95% CI Lower Upper
1 Metropolis 4.092 4 0.394 Multan Gujranwala 1 0.457 0.731 0.32 1.669 Bahawalpur Gujranwala 1 0.331 0.658 0.284 1.528 Faisalabad Gujranwala 1 0.91 0.962 0.495 1.87 Lahore Gujranwala 1 0.387 1.393 0.658 2.948 2 Species of equine 2.218 2 0.33 Horse Donkey 1 0.422 1.292 0.691 2.412 Mule Donkey 1 0.178 1.72 0.781 3.786 Sex 3 Female Male 0.002 1 0.96 0.987 0.602 1.62 4 Age groups 4.938 2 0.085 5 or less More than 10y 1 0.029 0.414 0.171 0.999 6-10 Years More than 10y 1 0.323 0.716 0.347 1.477 5 Tick on Cohorts No ticks on cohorts 5.816 1 0.016 1.978 1.128 3.468 6 Housing 6.782 2 0.034 Alone Non equine cohorts 1 0.018 0.519 0.301 0.894 With Equine Non equine cohorts 1 0.037 0.523 0.284 0.963 7 Tick Control Not Used Used 0.073 1 0.788 1.076 0.633 1.828

CHAPTER-IV (RESULTS)
109
Table-45 SPSS output of binary logistic regression model for predicting B. caballi infection in equines (n=93) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Variables in the Equation
B S.E. Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Variables Lower Upper
Step 3a Ticks on Cohorts .682 .286 5.672 1 .017 1.978 1.128 3.468
Constant -1.418 .133 113.295 1 .000 .242
a. Variable(s) entered on step 3: Ticks on Cohorts.

CHAPTER-IV (RESULTS)
110
Table-46 Bivariable analysis for the seroprevalence of mix infection with T.equi and B. caballi in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
S. No. Exposure Variable Comparison Chi Square df Wald P Odds Ratio
95% CI Lower Upper
1 Metropolis 6.469 4 0.167 Multan Gujranwala 1 0.885 0.913 0.265 3.138 Bahawalpur Gujranwala 1 0.621 0.719 0.194 2.664 Faisalabad Gujranwala 1 0.439 1.47 0.554 3.897 Lahore Gujranwala 1 0.096 2.421 0.855 6.856 2 Species of equine 1.464 2 0.481 Horse Donkey 1 0.463 1.363 0.596 3.117 Mule Donkey 1 0.291 1.734 0.625 4.813 Sex 3 Female Male 0.165 1 0.684 1.147 0.593 2.217 4 Age groups 3.993 2 0.136 5 or less More than 10y 1 0.05 0.414 0.171 0.999 6-10 Years More than 10y 1 0.366 0.716 0.347 1.477 5 Tick on Cohorts No ticks on cohorts 6.04 1 0.014 2.372 1.172 4.801 6 Housing 3.366 2 0.186 Alone Non equine cohorts 1 0.127 0.572 0.279 1.173 With Equine Non equine cohorts 1 0.133 0.509 0.22 1.175 7 Tick Control Not Used Used 2.511 1 0.119 1.949 0.843 4.509

CHAPTER-IV (RESULTS)
111
Table-47 SPSS output of binary logistic regression model for predicting mix infection with T.equi and B. caballi in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
Variables in the Equation
B S.E. Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Variables Lower Upper
Step 5a Ticks on Cohorts .864 .360 5.759 1 .016 2.372 1.172 4.801
Constant -2.359 .188 157.618 1 .000 .095
a. Variable(s) entered on step 1: Ticks on Cohorts.

CHAPTER-IV (RESULTS)
112
Table-48 Bivariable analysis for the seroprevalence of piroplasmosis in equines (n=226) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
S. No. Exposure Variable Comparison Chi Square
df Wald P
Odds Ratio
95% CI Lower Upper
1 Metropolis 24.493 4 0.00 Multan Gujranwala 1 0.725 1.126 0.581 2.181 Bahawalpur Gujranwala 1 0.861 1.061 0.547 2.057 Faisalabad Gujranwala 1 0.158 1.495 0.855 2.614 Lahore Gujranwala 1 0.00 4.837 2.325 10.064 2 Species of equine 11.408 2 0.003 Horse Donkey 1 0.002 2.419 1.369 4.273 Mule Donkey 1 0.095 1.881 0.896 3.948 Sex 3 Female Male 1.535 1 0.215 0.773 0.514 1.162 4 Age groups 3.41 2 0.182 5 or less More than 10y 1 0.087 0.633 0.375 1.069 6-10 Years More than 10y 1 0.585 0.872 0.533 1.426 5 Tick on Cohorts No ticks on cohorts 0.032 1 0.859 1.047 0.629 1.745 6 Housing 2.061 2 0.357 Alone Non equine cohorts 1 0.436 0.829 0.517 1.329 With Equine Non equine cohorts 1 0.684 0.684 0.407 1.151 7 Tick Control Not Used Used 2.624 1 0.106 1.43 0.927 2.206

CHAPTER-IV (RESULTS)
113
Table-49 SPSS output of binary logistic regression model for predicting piroplasmosis in equines (n=44) of 5 draught equine populated urban areas of Punjab surveyed for the prevalence of equine infectious anemia, glanders and piroplasmosis
B S.E. Wald df Sig. Exp(B)
95% C.I.for EXP(B)
Variables Lower Upper
Step 1a Metropolis 22.572 4 .000
Multan(1) .154 .343 .201 1 .654 1.167 .595 2.286
Bahawalpur(2) .093 .344 .073 1 .787 1.097 .559 2.152
Faisalabad(3) .489 .291 2.825 1 .093 1.631 .922 2.886
Lahore(4) 1.616 .379 18.151 1 .000 5.031 2.392 10.578
Animal 11.139 2 .004
Horse(1) .912 .300 9.265 1 .002 2.489 1.384 4.476
Mule(2) .667 .390 2.931 1 .087 1.949 .908 4.182
Constant -.525 .247 4.494 1 .034 .592
a. Variable(s) entered on step 1: Metropolis, Animal.

CHAPTER-IV (RESULTS)
114
Plate-VII Photograph showing the communal housing pattern used by owners of draught donkeys in the study areas

CHAPTER-IV (RESULTS)
115
Plate-VIII Photograph showing the roof type being used in the construction of the communal draught equine housing systems in the study area

CHAPTER-IV (RESULTS)
116
Plate-IX Photograph of tick infestation on the medial aspect of the thigh in a horse sampled during the study
CHAPTER-V (DISCUSSION)
117
CHAPTER-V
DISCUSSION
Current project was conducted to access the seroprevalence of three OIE (International Animal
Health Organization) listed equine diseases in 5 draught equine populated urban areas of Punjab,
Pakistan. Checking of current disease status through prevalence studies is important to
judge/estimate the disease load in a population and make some practical control strategies.
Prevalence studies are always costly and require exclusive resources for the travelling and
sample collection, therefore, multiple disease epidemiological studies are advocated to address
these problems. This study was focused to estimate the seroprevalence of equine infectious
anemia (EIA), glanders and piroplasmosis in draught equines of selected areas through testing
their sera by utilizing respectively enzyme linked immunosorbant assay (EIA), Rose Bengal
plate agglutination test (Glanders) and competitive ELISA (Piroplasmosis). Draught equine
population (horses, mules and donkeys) of these areas is usually kept in suboptimal management
and housing conditions that favors the spread of communicable diseases. Moreover, poor
nutrition and draught stress compromise their immune system and favor the diseases spread.
In the areas under study, draught equine population was dominated by donkeys followed by
horses and mules. This high donkey population was due to the economical limitations of owners,
less feeding and space requirements by these animals along with more docile temperament. It is
foreseen that this donkey population will rise further in future as waning financial conditions of
the owners and decline in use of horse drawn carriages (Tangas) in the cities make horse keeping
unaffordable for them. Equine owners of the studied areas preferred to keep female horses over

CHAPTER-V (DISCUSSION)
118
males because of less behavioral problems like dominance and fighting were associated with
them. However, male donkeys were kept in higher numbers as compared to horses because of
less frequent behavioral problems associated with them.
5.1. Equine Infectious Anemia: Sero-epidemiological Findings
Equine infectious anemia posses a great diagnostic challenge to the scientific community. Over
the years many tests have been devised and validated for the diagnosis and control of the disease
but no test came near the qualities of a perfect diagnostic solution regarding this disease. The
ability of EIA virus to undergo antigenic drift causes harm to sensitivity and specificity of many
tests (Issel and Cook, 1993). The diagnostic dilemma continued till the development of some
more specific and sensitive ELISAs against some static regions of the virus. These tests are more
suited for the screening purposes as compared to AGID with certain advantages of being quick
and more reliable in diagnosing the early infections (Parė and Simard, 2004; Piza et al., 2007).
The commercial ELISA (VMRD, Inc., USA) used in the current study detects the antibodies
against EIA virus p26 (static region) gene in affected equine sera. The sensitivity (100%) and
specificity (100%) was well established by different laboratory (Susan et al., 2008) and field
studies (Cullinane et al., 2007). The test is approved by the United States Department of
Agriculture (USDA) for the field and laboratory diagnosis of EIA.
Although, heamatological values indicated towards presence of anemia in most of the equine
during this study, sampled draught equine population of the studied metropolises found to be free
from antibodies against equine infectious anemia virus on the basis of enzyme linked
immunosorbant assay (ELISA). Cause of these anemic findings can be attributed to the

CHAPTER-V (DISCUSSION)
119
nutritional deficiencies and other blood parasitic disease like piroplasmosis and trypanosomiasis.
This finding is in accord with results reported by Gill et al. (2008) as they found no sero-reactive
animal for EIA in randomly selected equines of Faisalabad region may be ascribed to the failure
of the organism to mount a response or the absence of the disease in the sampled equine
population, which was also suggested by the preceding studies of some Turkish workers (Turan
et al., 2002; Ataseven and Arslan, 2005 and Kirmizigȕl et al., 2009). Further investigations in
this regard with new locale, wider sample size with molecular techniques are required to
strengthen the claims of disease free status regarding EIA of the selected areas and Pakistan.
5.2. Equine Glanders: Sero-epidemiological Findings
Over the years glanders has been controlled in many countries though strict implementation of
test and slaughter policy but the disease still persists in equines of many developing countries
and threatens the public health through its zoonotic potentials and as a potential agent of
bioterrorism and warfare (Gregory and Waag, 2007; Pawaiya and Chauhan, 2008). Many sero-
diagnostic assays like complement fixation test (CFT), indirect hemagglutination test (IHAT),
counter immunoelectrophoresis test (CIET) indirect fluorescent antibody test (IFAT) and enzyme
–linked immunosorbent assays (ELISAs) have been developed and evaluated for their diagnostic
efficiency in different forms of the disease to address the clinical and bacteriological difficulties
in diagnosis (Neubauer et al., 2005; Naureen et al., 2007; Saqib et al., 2008). Over the years,
need has been felt for the development of some simple, quick and field diagnostic assay to
complement mallien testing (Naureen et al., 2007) in order to address the limitations of the
mallein in terms of its sensitivity, cross-reactivity with streptococcus aureus (causative organism
of strangles) to produce false positive results and time consumption (48 hours) to reach the

CHAPTER-V (DISCUSSION)
120
diagnosis. In this study Rose Bengal plate agglutination test (RBT) was used to estimate
seroprevalence of glanders. The test was developed by the Russian workers (OIE, 2004) which
further recently evaluated by Naureen and co-workers (2007) and was found to carry good
diagnostic efficiency.
On the basis of Rose Bengal Plate Agglutination (RBT) test, the overall seroprevalence of
glanders was found to be 7.9% in the studied equine population. This finding indicates towards
the possible endemic nature of glanders in the draught equines in the selected metropolises. This
finding concord with past research studies and reports of a few recent clinical outbreaks in the
Punjab province, where the authors indicated towards possible high prevalence of glanders
(Nasreen, 1977; Vaid, 1981; Bashir, 1984; Muhammad et al., 1998; Saqib et al., 2003, Naureen
et al., 2007; Saqib et al., 2008).
5.2a. Area Based Seroprevalence of Equine Glanders
Study indicates that seroprevalence of equine was not significantly different in 5 selected
metropolis (2=2.84, 4df, P=0.58) that indicates towards endemic nature of this disease in
selected areas. One possible reason for this could be that most of the equines belonged to the
poor owners who share almost identical socioeconomic status and husbandry practices.
However, higher seroprevalence of glanders in Lahore may be attributed to the outbreak of
glanders in recent years as described by Naureen et al. (2007) and Saqib et al. (2008). Moreover,
being a large industrial city and major hub of economic activities the metropolis attracts owners
along with their draught equines from neighboring towns and cities to seek the work
opportunities. Within city, equines are usually put to work in close groupings and kept under

CHAPTER-V (DISCUSSION)
121
inadequate management which probably precipitates the spread of glanders in this area.
Moreover, relatively consistent seroprevalence found in studied metropolises could be attributed
to the climatic and draught stress, poor nutrition and care provided to draught equines by the
owners owing to their poor economic situation. Similar has been reported by various authors
elsewhere (Muhammad et al., 1998; Manso, 2003; Neubauer et al., 2005; Al-Ani and Roberson,
2007; Gregory and Waag, 2007)
Study indicates towards possible rise in the current prevalence of glanders in future as the
diseased animals are well recognized by the owners and they prefer to sale their sick animals to
unaware owners of other areas/cities over getting them destroyed by the authorities for a meager
compensation. Furthermore, chances of spread also increase through the buying and selling of
apparently healthy carriers sold in the large markets present in each area, where animals and
buyers come across from distant areas. (Muhammad et al., 1998; Saqib, 2000)
5.2b. Clinical Signs Observed in RBT Positive Equines
Glanders sero-positive animals showed clinical signs of the disease in variable intensity. Because
majority of these animals were not in the clinical stage of the disease, most of the signs observed
were not specific: like congested mucous membranes, loss of stamina, fever, anorexia. More
specific signs indicating a respiratory tract involvement were cough, nasal discharge and
dyspnea. Orchitis was found in only one male donkey. These signs are comparable with previous
reports by different workers (Saqib et al., 2003; Al-Ani and Roberson, 2007; Gregory and Wagg,
2007; Naureen et al.2007 and Saqib et al.2008).

CHAPTER-V (DISCUSSION)
122
5.2c. Species, Age and Sex based Seroprevalence of Glanders
Significant difference (P<0.01) was observed regarding the seroprevalence of glanders between
horses and donkeys but the differences between horse vs. mule and mule vs. donkey were not
significant (P>0.05). This could be attributed to the differences in presentation of disease in these
equine species as reported by the other workers (Al-Ani et al., 1998; Muhammad et al., 1998;
Al-Ani and Roberson 2007, Gregory and Wagg, 2007) who reported that the course of disease is
usually chronic in horses and donkeys mostly suffer from acute disease, whereas, the disease can
manifest itself in both acute and sub acute forms in mules. Another possible reason for this
difference could be that equines owners are well familiar with clinical picture of glanders and
avoid bringing equines in clinical state (usually donkeys and mules) for work and veterinary
advice.
No significant (P>0.05) difference in seroprevalence of glanders was observed among 3 different
age groups of equines. Relatively higher prevalence rates were observed in age group-II (6-10
years) and I (less than equal to 5 years) than older equines of group-III (more than 10 years). In
general the seroprevalence was found to be higher in young and middle aged animals as
compared to old. Incidence of glanders as documented elsewhere (Dungworth, 1993; Radostits et
al., 2007) found to be higher in old age and equines older than 2 years of age were found more
susceptible (Al-Ani and Roberson, 2007). This high prevalence in relatively young equines could
also be attributed to the fact that equines in these areas were put to work in early age and poorly
managed, which might be favouring spread of the disease. In addition, clinical form of the
disease is frequently seen in aged equines so they are usually culled or not put to work
intentionally in order to avoid them being noticed and destroyed by the authorities as owners are

CHAPTER-V (DISCUSSION)
123
well familiar with the Glanders and Farcy Act. Same has been reported by Al-Ani et al. (1987),
Al-Ani and Roberson (2007), Naureen et al. (2007) and Pawaiya and Chauhan (2008).
Seroprevalence of glanders was significantly higher (2 =5.94 (1df), P=0.014) in female equines
as compared to males. Univariate analysis has indicated the same that female equines were more
likely to be positive for glanders (OR 2.3, 95%CI 1.16-4.77). This finding differs from the
reports of Al-Ani et al. (1987), Neuber et al. (2005) and Al-Ani and Roberson (2007) who
reported no significant association between sex and glanders. However, the higher
seroprevalence found in female equines in this study could be attributed to the relatively less
numbers of females enrolled in the sampled equine populations. Moreover, the female equines
usually face an added stress of breeding along with malnutrition and heavy draught work that
might weaken their immune response to endemic diseases.
5.2d. Prevalence of Equine Glanders with Reference to Housing Pattern of Equines
Seroprevalence of glanders was not found to be associated (P>0.05) with housing pattern of the
equines sampled. Numerical differences regarding seroprevalence were observed among 3 types
of housing practices. However, comparatively higher percentage of equines found sero-positive
for glanders were kept alone or with equine cohorts. This difference could be due to the
congested and unhygienic conditions of the communal housing systems in case of equines kept
with equines. Moreover, draught equines although kept alone but working in local tanga stands,
grain and green markets have higher chances of contracting the disease because of greater
interaction with other infected equines. Similar findings has been reported by other researcher as
well (Lovell, 1935; Al-Ani et al., 1987; Muhammad et al., 1998; Saqib et al., 2003; Al-Ani and

CHAPTER-V (DISCUSSION)
124
Roberson, 2007) who reported that overcrowding, unhygienic conditions and poor nutrition
make the equine more susceptible to the disease. The higher seroprevalence in equines kept with
non equine cohorts could be attributed to the fact that they are usually kept for the fodder
carriage and tend to get less attention regarding feeding and management by the owners who
consider them animals of less economical importance. However, had this been a clinical study
the effect of housing may have been different in various housing patterns adopted by the owners.
5.2e. Prevalence of glanders with reference to watering habits of the equine owners
Seroprevalence of glanders was found more in equines having access to the communal water
troughs either at work or home however this difference was not significant (P>0.05). However,
univariate analysis indicated that equines drinking water through communal water troughs were
more likely to be sero-positive (OR 2.7, 95% CI 0.931-7.86). Water can become contaminated
with B. mallei through a diseased equine and organism can survive there for the weeks to come
(Miller et al., 1948; Gangulee et al., 1966). Usually these water troughs are without running
stream and stagnant water sources is shared by many equines working on the roads. Moreover,
sharing of buckets for watering is fairly common in equine owners. These watering methods
used by the owners might be contributing towards the spread of disease. Similar has been quoted
by the different workers (Hutyra et l., 1949, Gangulee et al., 1966; Al-Ani and Roberson, 2007;
Radostits et al., 2007) who stated that contaminated utensils, food, water and congested housing
are causes for spread of glanders.
5.3. Equine Piroplasmosis: Sero-epidemiological Findings
CHAPTER-V (DISCUSSION)
125
Piroplasmosis caused by Theileria equi and Babesia caballi is an important disease of horses
with serious health and economic impact. For the years, diagnosis of the disease remained a
challenge for the researchers and veterinarians as the conventional Giemsa stained smears are
rarely conclusive and most of the serological tests have the many problems including reporting
false positive / negative results (Donnelley et al., 1980; Ribeiro et al., 1999; Abdelkebir et al.,
2001; Akkan et al., 2003; Zinora et al., 2007). Similar had been observed during the study where
examination of Giemsa stained blood smears were found inconclusive for either T. equi or B.
caballi.
Competitive ELISAs used in the current study were recognized by OIE on the basis of
validations provided by the works of Knowles et al. (1991), Shkap et al. (1998), Kappmeyer, et
al. (1999) and Katz et al. (2000).
Seroprevalence of piroplasmosis (T. equi, B. caballi or mixeded infection) was found to be
52.5% in the studied metropolises which shows the widespread nature of the problem. Moreover,
seroprevalence of Theileria equi (41.2%) was significantly higher (2=38.07 (1df), P<0.01) as
compared to B. caballi (21.6%). These findings are in line with those found by various authors in
Brazil, (Barbosa et al., 1995; Ribeiro et al., 1999), Japan (Ikadai et al., 2001), Mongolia
(Boldbaatar et al., 2005), Spain (Camacho et al., 2005), Trinidad (Asgarali et al., 2007) and
Turkey (Akkan et al., 2003; Karatepe et al., 2009). These authors invariably reported the
comparatively higher prevalence of T. equi than B. caballi in different endemic regions of the
world. However, some workers (Xuan et al., 2001; Chahan et al., 2006; Torina et al., 2007)
reported an equitable distribution in some regions of China owing to similar distribution of
vector populations. A serologically higher seroprevalence of T. equi noted in this study could be

CHAPTER-V (DISCUSSION)
126
due to the fact that infected equines usually become life-long carriers of the infections and
infections with B. caballi usually subsides in 4-5 years (Shkap et al., 1998; Vial and Gorenflot,
2006; Rüegg et al., 2007; Rüegg et al., 2008).
The prevalence of piroplasmosis was significantly higher (P<0.01) in equines of Lahore as
compared to the Faisalabad, Multan, Gujranwala and Bahawalpur. This difference could be due
to the more favorable climatic conditions that favor the spread of tick vectors. Furthermore, the
trend of using tick control measures was significantly lower (P<0.01) in equine owners of Lahore
than other areas. Similar findings have been reported elsewhere, with authors reporting
differences in prevalence of disease in the areas based upon presence of tick vectors and faulty
management (Shkap et al., 1998; Asgarali, et al., 2007; Karatepe et al., 2009). Another possible
reason for this higher prevalence could be attributed to the presence of more carrier animals in
the area as equines born and raised in endemic areas usually enter into the carrier state of
piroplasmosis (Abdelkebir et al., 2001; Camacho et al., 2005).
5.3a. Clinical Signs Found in Equines Tested Positive for Piroplasmosis
Though the aim of the study was not to pick the clinical cases of piroplasmosis but data
regarding seropositive equines was analyzed to seek the most frequent clinical signs observed in
these animals to suggest possible clinical indicators of piroplasmosis. Anorexia and debility are
two non specific signs found frequently in piroplasmosis positive equines. The specific clinical
signs found were pale mucous membranes, fever, congested mucous membranes, eyelid edema
with muco-purrulent discharge, edema of the distal limb, enlarged lymph nodes and patechial
hemorrhages on the mucous membrabes. These observations have also been reported by Roberts

CHAPTER-V (DISCUSSION)
127
et al. (1962), Hailat et al. (1997), Seifi et al. (2000) in clinical and sub clinical forms of the
piroplasmosis. However, many authors reported that equines in the endemic areas may adapt to
the piroplasmosis where the disease would prevail in its latent form (Abdelkebir et al., 2001;
Camacho et al., 2005; Chahan et al., 2006; Asgarali et al., 2007) and the stress may lead to
development of clinical disease in these equines.
5.3b. Seroprevalence of Theileria equi: Sero-epidemiological findings
Current study suggested that under the prevailing conditions in the sampled metropolises,
Theileria equi is the major contributor (41.2%) of piroplasmosis. This finding is in agreement
with those reports depicting that in general prevalence of T. equi infection is usually higher in the
endemic regions of the world (Barbosa et al., 1995; Ribeiro et al., 1999; Boldbaatar et al., 2005;
Camacho et al., 2005; Asgarali, et al., 2007; Karatepe et al., 2009). However, some studies
document the relatively less difference in prevalence of T. equi and B. caballi (Shkap et al.,
1998; Heuchert et al., 1999) and the possible reason for this difference could be selection of the
equines population for study. In these studies target equine population usually belonged to
privately owned well managed horses receiving good nutrition and owners/managers could be
well aware of utilizing vector control methods. However, the current study differs from above
because all the equines selected were kept for draught purpose and usually were managed under
poor management, improper housing and high draught stress, which could be a possible cause of
this higher prevalence found.
Seroprevalence of T. equi was found to be significantly higher (P<0.01) in equines of Lahore
than of other four cities. This could be due to the difference observed in tick control measures

CHAPTER-V (DISCUSSION)
128
adopted, as the owners reported significantly lower use of tick control measures than other areas.
Similar findings have been reported by various authors (Heuchert et al., 1999; Skhap et al.,
1998; Acici et al., 2008; Karatepe et al., 2009: Salim et al., 2008) in their respective studies
based upon the differences found in the climatic / geographic conditions, vector population,
draught stress and equine keeping practices.
Seroprevalence of T. equi infection found in horses was significantly higher (P<0.01) as
compared to donkeys and mules. Possible reason for this could be that the horses have less vigor
and strength to bear the heavy draught burden which can be more easily managed by the mules
and donkeys. These findings regarding T. equi prevalence are in line with those reported by
Torina et al, (2007) and Acici et al, (2008) who reported higher seroprevalence of B. caballi in
donkeys as compared with horses in Sicily and Turkey. Moreover, prevalence of T. equi
infection in equine species was higher in Lahore as compared to other 4 areas. So the higher
draught stress, significantly lesser tick control employed and malnutrition may compromise the
immune system of animals and make them more vulnerable to already prevailing T. equi
infections.
Seroprevalence of T. equi infection observed in this study was not found significantly (P>0.05)
associated with age of equines. However, seroprevalence increased with the age of equines and
more prevalence was observed in older equines as compared to young ones. Similar has been
presented by various authors (Bruning, 1996; Oliver and Garcia, 2001; Asgarali, et al. 2007;
Rüegg et al., 2007; Rüegg et al., 2008; Karatepe et al., 2009) in their respective studies and
possible reason could be that once infected with T. equi equines remain carriers throughout their

CHAPTER-V (DISCUSSION)
129
life. However, a few authors have not mentioned any significant relationship between prevalence
of T. equi and B. caballi infections and age of equines (Tenter et al., 1988; Shkap et al., 1998).
No significant (P>0.05) difference was found between either sexes of equines on the basis of T.
equi seroprevalence and these findings are in accord with those reported by Oliver and Garcia
(2001), Asgarali, et al. (2007) and Karatepe et al,(2009). However, Shkap et al. (1998) and
Rüegg et al. (2007) found a higher sero-positivity in mares and geldings as compared to stallions
which could be due to the different level of care, grooming and attention these animals were
getting according to their importance for owners. The numerically higher sero-positivity found in
males as compared to females could be due to the large proportion of male equines enrolled for
sampling as compared to females.
5.3c. Prevalence of Babesia caballi: Sero-epidemiological Findings
Significantly (P<0.01) lower seroprevalence of B. caballi (21.6%) was found in the present study
as compared with T. equi and this finding is in line with those reported by Heuchert et al., (1999)
and Karatepe et al. (2009) in different regions of Brazil and Turkey. This is also in accord with
those researchers who reported that less prevalence of B. caballi could be attributed to the fact
that it clears away from the body in few years and generally responds well to the recommended
dosage of imidocarb treatment (Bruning, 1996; Ali et al., 1996; Rüegg et al., 2007; Rüegg et al.,
2008).
Seroprevalence of B. caballi infection found in the study was not significantly different (P=0.39)
in 5 selected metropolises and similar has been reported by researchers from other countries
(Heuchert et al., 1999; Karatepe et al., 2009). However, a numerically higher number of B.

CHAPTER-V (DISCUSSION)
130
caballi sero-positive equines were found in Lahore possibly owing to more suitable conditions
prevailing there for the persistence and spread of this parasite.
There was not association found between seroprevalence of B. caballi infection and equine
species (P=0.33). Only numerical differences were found possibly due to the differences in the
sampled proportions of these equines. However, horses, mules and donkeys of metropolis Lahore
suffer more from the disease as compared to the equines of other locations.
Age was not found to be significantly associated with the seroprevalence of B. caballi infection
(P=0.08), however, the rate of sero-positivity was generally higher in old equines as compared to
young animals. This finding was in accord with those found by Abdelkebir et al. (2001), Balkaya
and Erdogmus (2006) and Acici et al. (2008) who reported the prevalence of B. caballi is
independent of age of equines in their studied areas.
The prevalence of B. caballi in the studied areas was not dependent (P>0.05) upon the sex of
equines and similar findings are also quoted elsewhere by different workers (Oliver and Garcia,
2001; Asgarali, et al., 2007; Karatepe et al., 2009).
5.3d. Mixed Infection of Theileria equi and Babesia caballi: Sero-epidemiological Findings
Sero-positivity for mixed infection with T. equi and B. caballi was found in 10.2% samples.
Mixed infection of piroplasmosis is a common feature and has frequently been reported in
varying intensities by different workers according to the prevailing conditions, vector
populations and circulating prioplasms from Brazil (Heuchert et al., 1999), Iran (Seifi et al.,

CHAPTER-V (DISCUSSION)
131
2000), Japan (Ikadai et al., 2002), Spain (Camacho et al., 2005), Trinidad (Asgarali et al., 2007)
and Turkey (Acici et al., 2008).
No significant difference (P=0.167) was observed in the seroprevalence of mixed infection
regarding 5 selected areas. Moreover, mixed infection of piroplasmosis was found to be
independent of equine species. This has been reported also by Acici et al. (2008) who found no
difference regarding mixed infection in three species in belonging to different areas of Black Sea
region of Turkey. Similarly, no significant differences (P > 0.05) were observed regarding mixed
infections in different age groups and sex of equines and this finding is in accord with those
reported by Balkaya and Erdogmus, (2006), Acici et al. (2008), Rüegg et al. (2007) and Rüegg et
al. (2008).
5.3e. Seroprevalence of Piroplasmosis and Housing Pattern of Equines
Different housing pattern were not found associated with seroprevalence of piroplasmosis
(P>0.05), however, computed odds ratio indicated that equines living alone/with equine cohorts
in these metropolises were more likely to be positive for piroplasmosis (OR 1.30, 95% CI 0.84-
2.01) as compared to those managed with non equine cohorts and usually kept for the domestic
draught purpose. Similar has been reported by many studies as well that chances of contracting
the prioplasmosis were higher in those areas where equines have greater interaction with each
other or other domestic animals which favors the spread of tick infestation (Heuchert at al.,
1999; Camacho et al., 2005; Karatepe et al., 2009).
5.3f. Seroprevalence of Piroplasmosis with Reference to Presence of Ticks and Use of Tick Control Measures

CHAPTER-V (DISCUSSION)
132
Adjusted analysis for possible confounding factors revealed that equines living with tick infested
equine cohorts (OR = 1.19, 95% CI 0.65–2.18) and non equine cohorts (OR = 2.04, 95% CI
0.73-5.69) were more likely to be sero-positive for piroplasmosis. However, in statistical terms
this difference was not significant (P>0.05). Seroprevalence of piroplasmosis was not
significantly associated with the used of tick control measures by the equine owners. However,
seroprevalence was found to be higher in equines and areas where owners were not giving much
emphasis on using tick vector control (OR=1.43, 95%CI=0.93-2.21). These findings are in
agreement with those reported by Heuchert et al. (1999), Barbosa et al. (1995), Abdelkebir et al.
(2001) and Chahan et al. (2006) who found out a positive correlation between piroplasmosis and
tick infestation in equines and their equine or non equine cohorts. However, there is still a need
to establish the possible tick vector responsible for the spread of equine piroplasmosis in
Pakistan.
5.3g. Treatment Chosen by the Veterinarians and Animal Health Workers against Suspected Piroplasmosis in Equines
A structured interview of practicing veterinarians and animal health workers responsible for
equine disease management in their respective areas indicated that a lacunae regarding the
correct diagnosis and treatment of equine prioplasmosis exists, which could be a leading cause
for higher seroprevalence found in this study. As indicated in the results, that majority of
veterinarians and animal health workers were not familiar with the separate treatment protocol
recommended for B. caballi and T. equi, were using only the therapeutic dose of imidocarb
diapropionate recommended for the treatment of B. caballi infections. This is due to the fact that
they were relying just only upon the clinical signs for making the presumptive diagnosis and
almost always were not using any Giemsa stained smear examination or other serological tests

CHAPTER-V (DISCUSSION)
133
for diagnosing the condition. Conducting workshops, lectures and seminars regarding
piroplasmosis its diagnosis and correct treatment as reported by several authors (Ali et al., 1996;
Hailat et al., 1996; Seifi et al., 2000; Vial and Gorenflot, 2006) can address this issue in future.
5.3h. Comparison of Hematological Findings in Equine Species
A comparison of the hematological values of equines originating from 5 different locations
revealed significantly higher mean white blood cell (WBC) counts in the animals of Bahawalpur
and Multan. This may relate to the relatively higher seroprevalence of glanders in the equines of
these areas. Similar findings regarding the alterations in WBC counts associated with glanders
have also been reported previously by Saqib (2002). Mean red blood counts (RBC) were found
to be significantly lower in equines of Lahore as compared to equines of other areas and this
could be associated with the higher seroprevalence of piroplasmosis in the equines of this
metropolis. Mean heamoglobin concentration, hematocrit, MCV and MCH were sifnigicantly
different in equines of Bahawalpur and Multan as compared to the other areas and this could be
attributed to the nutritional status of these animals. Because of the extreme heat and dryness and
deprivation from proper nutrition, the equines of these areas tend to suffer more from heat related
disorders like anhydrosis or non perspiration also described by Jenkinson et al. (2007).
Moreover, the study was conducted during the hot and dry months of the year (July – August) in
the said locations when the draught equines were suffering more from heat stress and
dehydration. In short, these variations can be due to the difference in the climatic, nutritional,
management and disease burden of the equines in the study areas.

CHAPTER-V (DISCUSSION)
134
Differences were observed among horses, mules and donkeys regarding WBC and RBC counts,
hemoglobin concentration and packed cell volume. Comparison of hematological values found in
this study revealed significantly (P < 0.05) lower mean white blood cell counts than reference
values in donkeys and mules. Although, some workers (Nayeri, 1978; Reece, 1997) found total
WBC numbers of donkeys highest among domestic animals but lower values were also observed
elsewhere by Zinkl et al. (1990). Moreover, these difference could be due to the physiological
and pathological variations like age, nutritional and health status, pregnancy and lactation stage
as described by Reece (1997). However, this difference was not significant (P > 0.05) among
horses. Mean RBC counts were significantly lower in horses as compared to mules and donkeys
which could be due to the fact that these values are species specific (Gul et al., 2007). Generally
the horses of the studies areas had significantly lower mean Hb concentration than reference
values but mules and donkeys had mean Hb concentrations comparable with reference values.
These differences could be due to the fact that horses generally are more frequently underfed as
compared to mules and donkeys. Mean hematocrit was found to be significantly lower (P < 0.05)
than the reference values in all the equine types which could be due to the effect of mild
dehydration (Thrall, 2004). A not significant difference (P > 0.05) was observed among horses,
mules and donkeys regarding MCV, MCH and MCHC.
Hematological alterations regarding mean WBC and RBC counts were not significantly different
(P > 0.05) between male and female equines. Similar findings were observed by Nayeri (1978)
Reece (1997), Al-Busadah and Homeida (2005) and Gul et al. (2007) where they found a not
significant difference regarding hematological values between healthy male and female equines.
Mean hemoglobin concentration, packed cell volume and erythrocytic indices were found to be

CHAPTER-V (DISCUSSION)
135
towards higher end in females as compared to males which could be due to the lower numerical
proportion of sampled females as compared to male animals as well as females tend to get more
care as compared to males due to their breeding potentials.
Analysis of hematological values regarding the age of equines suggested that mean WBC and
RBC counts and hemoglobin concentration were significantly higher (P < 0.05) in young animals
and tend to decrease with age. Similar findings were reported by Zinkl (1990) and Gul et al.
(2007).
5.3i. Hematological analysis of equine blood samples found sero-positive for glanders and piroplasmosis
Glanders
Mean white blood cell (WBC) counts were not significantly higher than reference values in
horses but in mules these values were below normal and significantly low in donkeys. Mean red
blood cell counts (RBC) were also found below than reference values in horses, donkeys and
mules showing anemia. Mean hemoglobin concentrations were found higher than reference
values in all 3 equine types. Mean packed cell volume (PCV) was found lower than reference
values in horses, mules and donkeys. On the basis of erythrocytic indices macrocytic
hyperchromic type of anemia was established in horses, mules and donkeys. These
hematological findings are in line as described by other researchers (Saqib 2000; Saqib et al.,
2003; Al Ani and and Roberson, 2007; Saqib et al., 2008)

CHAPTER-V (DISCUSSION)
136
Piroplasmosis
Hematological analysis of the prioplasmosis sero-positive equines revealed marked decrease in
white blood cell counts (WBC), packed cell volume (PCV) and hemoglobin (Hb.) concentrations
regarding horses and mules. However, there was no decrease of Hb. Concentration below
reference values in donkeys. Erythrocytic indices indicated presence of microcytic hyperchromic
type of anemia in horses found seropositive for T. equi, B. caballi and mixed infection, while in
donkeys macrocytic hyperchromic was noted. Erythrocytic indices in mules revealed normocytic
hyperchromic, microcytic hyperchromic, and macrocytic hyperchromic type of anemia in T.
equi, B. caballi and mixed infections. These findings are in accord with those reported by various
researchers (de Waal 1992; Hailat et al., 1997; Seifi et al., 2000; Camacho et al., 2005; Asgarali
et al., 2007; Zobba et al., 2008) regarding RBC counts, Hb concentration and PCV, they found
values of varying degree of lower levels according to clinical and subclinical infections.
Similarly more severe anemia was recorded in equines suffering from T. equi infections when
compared with those suffering from B. caballi infections.

CHAPTER-V (DISCUSSION)
137
CONCLUSIONS
Equine Infectious Anemia
1. All equines were found sero-negative for equine infectious anemia (EIA) tested by
enzyme linked immunosorbent assay (ELISA).
Equine Glanders
1. The RBT based prevalence (7.9%) of equine glanders indicates towards endemic nature
of this disease in Pakistan.
2. Seroprevalence of equine glanders was not significantly associated with sampling locales,
equine species and age.
3. Female equines were more likely to be sero-positive for equine glanders (OR=2.3,
95%CI=1.13-4.69)
4. Equines sharing communal watering sources (toughs & buckets) are more likely to be
sero-positive for glanders (OR=2.71, 95%CI=0.94-7.83)
Equine Piroplasmosis
1. Seroprevalence of piroplasmosis was found alarmingly high (52.5%) in the sampled
equine population
2. Seroprevalence of piroplasmosis was found to be significantly higher in equines of
Lahore than those of other metropolises
3. Seroprevalence of piroplasmosis was significantly higher in horses than other equine
species
4. Mixed infection with Theileria equi and B. caballi was found to be 10.2% in the equines
of sampled areas
5. Seroprevalence of Theileria equi (41.2%) was significantly higher than that of B. caballi
(21.62%)

CHAPTER-V (DISCUSSION)
138
6. Seroprevalence of Theileria equi was significantly different with reference to areas
sampled (higher in Lahore than other areas) and equine species sampled (higher in horses
than mules and donkeys).
7. Equines belonging to owners who don’t practice tick control were found more likely to
be sero-positive for T. equi (OR=1.74, 95% CI=1.10-2.75)
8. Seroprevalence of B. caballi was independent of location, species, sex and age.
9. Equines living with tick infested cohorts were more likely to be sero-positive for B.
caballi (OR=1.97, 95% CI=1.13-3.47) and mixed infection (OR=2.37, 95% CI=1.17-
4.80)
10. Equines living alone or with equine cohorts were more likely to be sero-positive for B.
caballi infection (OR=1.92, 95%CI=1.17-3.15)
11. Lack of tick control measures adopted by equine owners and lack of knowledge among
animal health professionals about the correct diagnosis and treatment of T. equi and B.
caballi might be responsible for the high seroprevalence of piroplasmosis in studied
areas.

CHAPTER-V (DISCUSSION)
139
UNIQUE ATTRIBUTES OF THE PRESENT STUDY
1. Prevalence of equine infectious anemia (EIA), glanders and piroplasmosis was
investigated over a wide geographic region for the first ever time in Pakistan
2. Risk factors for responsible for spread equine glanders and piroplasmosis were
scientifically investigated
3. Some of the lacunae and drawbacks of previous studies were addressed in this study

CHAPTER-V (DISCUSSION)
140
FUTURE OUTLOOK AND RECOMMENDATIONS
1. Sero-negative findings regarding equine infectious anemia indicate towards the possible
EIA free status of the studied draught equine populated urban areas of Punjab, which
should be further certified by conducting more epidemiologic studies with different
settings and locales to attain a possible disease free status regarding EIA.
2. Potential role of communal water troughs in the spread of equine glanders requires
further investigations through carefully designed experimental studies. Equine owners,
vets and animal health workers should be given awareness about possible spread of
equine glanders through communal water troughs and faulty practices.
3. Glanders & Farcy Act should be revised regarding compensations & implemented strictly
to control and eradicate glanders in Pakistan
4. Future studies are required to identify the possible tick vectors responsible for spread and
maintenance of piroplasmosis in the region through conventional and molecular
techniques to understand the epidemiology of disease and devise control measures
5. Equine owners should be educated to adopt proper tick control measures to check the
spread of piroplasmosis
6. Veterinarians and animal health workers should administer the standard treatment
regimen recommended for each type of piroplasm (T. equi or B. caballi) after proper
diagnosis to control the disease

CHAPTER-VI (SUMMARY)
141
CHAPTER-VI
SUMMARY
Equine infectious anemia (EIA), glanders and piroplasmosis (Theileria equi and Babesia caballi
infections) are the three World Animal Health Organization (OIE) listed equine diseases with
serious economic and health effects. Keeping in view the scarce epidemiological information
available regarding these diseases in Pakistan, a cross-sectional sero-epidemiological study was
designed to investigate prevalence of these diseases in 5 draught equine populated urban areas of
Punjab province, Pakistan. Subordinate objectives included determination of hematological
alterations associated with these diseases and formulating a conceptual framework of control
measures on the basis of epidemiological data generated.
Four hundred and thirty (430) blood and serum samples were randomly collected from 5 selected
urban areas of Punjab (Lahore, Gujranwala, Faisalabad, Multan and Bahawalpur). Sample size
was calculated for the expected prevalence of 50 percent (unknown disease status) with
confidence limits of 95% and a desired absolute precision of 5%. Relevant information on each
disease was collected on a predesigned proforma. Hematological parameters studied were red
blood cell (RBC) count, hemoglobin concentration (Hb), white blood cell (WBC) count packed
cell volume (PCV) and erythrocytic indices. Giemsa stained thin and thick blood smears were
also examined microscopically for the presence of piroplasms.
Serum samples were subjected to commercial enzyme linked immunosorbant assay (ELISA,
VMRD, Inc., USA) for EIA, Rose Bengal plate agglutination test (RBT) for glanders and
commercial competitive ELISA (cELISA, VMRD, Inc., USA) for piroplasmosis status. Positive
and negative ELISA results were interpreted as per the criteria given by the manufacturers of the

CHAPTER-VI (SUMMARY)
142
commercial kits. For RBT, positive samples were identified on the basis of degree of agglutination
(+++ and ++++ considered positive). Data were analyzed using softwares (WINPEPI, EPiCalc,
Survey Tool Box and SPSS) for contributing risk factors by calculating Chisquare values,
multivariable analysis and calculations of odds ratio (OR).
None of the serum sample was found positive for EIA which is reflective of a possible disease free
status of the selected equine communities or the failure of the disease to mount an immune
response.
Sero-prevalence of glanders was found to be 7.9% (n=34) with highest prevalence in Lahore
(11.6%) followed by Bahawalpur (10.3%), Multan (7.3%), Faisalabad (6.7%) and Gujranwala
(5.3%). Significantly higher (P<0.01) prevalence was recorded in horses (16.9%) and mules
(12.1%) than in donkeys (5.7%). Sero-prevalence recorded in young (<5 years; 7.9%), adult
(<10years; 9.2%) and old (>10years; 5.2%) equines were statistically not significantly different
(P>0.05). Significantly higher (P<0.05) seroprevalence was recorded in females (12.6%) as
compared to males (5.76%). Analysis for the possible confounding factors indicated that females
equines (OR = 2.3, 95% CI= 1.16–4.77) and those sharing water sources or access to communal
water troughs (OR =2.7, 95% CI=0.93-7.86) were more likely to be sero-positive.
Over all seroprevalence of piroplasmosis was found to be 52.5% (T. equi =41.2% and B. caballi
=21.6% ; P<0.05) in the selected areas. Forty four (10.2%) sera were found positive for both
piroplasms (mix infection). Significantly higher (P<0.05) prevalence was recorded in Lahore
(95.6%, n=66) followed by Faisalabad (64%, n=96), Multan (52.9%, n=36), Gujranwala (50.7%,
n=38) and Bahawalpur (50.0%, n=34). Seroprevalence of T. equi infection was significantly
different among equine species (P<0.01) and in equines of Lahore (P<0.01). Equine age and
gender based differences in seroprevalence of T. equi infection were non-significant (P>0.05). B.

CHAPTER-VI (SUMMARY)
143
caballi and mixed infection seroprevalence was not found significantly different (P>0.05) in
selected areas, equine species, 3 age groups and both sexes of equines. Adjusted analysis for
possible confounding factors revealed that equines living alone or with equine cohorts (OR=1.30,
95%CI=0.84–2.01), with tick infested equine cohorts (OR=1.19, 95%CI=0.65-2.18) or whose
owners did not practice tick control (OR=1.43, 95%CI=0.93-2.21) were more likely to be sero-
positive for piroplasmosis.
In general, hematologic alterations observed in the equines were indicative of anemia and chronic
infections with significant differences observed (P<0.05) in mean WBC counts, mean RBC
counts, mean Hb concentration, PCV, MCV and MCH in selected metropolises. Hematological
alterations observed in RBT positive (glanders positive) equines were indicative of mild
leukocytosis (P>0.05) in horses and decreased WBC counts in mules (P>0.05) and donkeys
(P<0.05). Mean RBC counts were significantly (P<0.05) lower in sero-positive horses and
donkeys but this difference was not significant (P > 0.05) in mules. Mean Hb concentrations were
higher (P>0.05) in horses, mules and donkeys than reference values. Mean PCV was lower
(P>0.05) in RBT positive individuals of 3 equine species. Differences among species regarding
mean WBC counts, RBC counts, Hb. concentrations and PCV (hematocrit) were not significant
(P>0.05). Macrocytic hyperchromic anemia was observed in all RBT positive horses, mules and
donkeys.
Hematologic analysis of equines sero-positive for prioplasmosis indicated a marked decrease
(P<0.05) in WBC counts, lower (P>0.05) mean RBC counts, significantly (P < 0.05) lower mean
PCV and lower (P>0.05) mean Hb concentration. Erythrocytic indices pointed towards microcytic
hyperchromic type of anemia in sero-positive horses, donkeys and mules sero-positive for
piroplasmosis.

CHAPTER-VI (SUMMARY)
144
In conclusion, the study results indicated towards possibility of acquiring disease free status
regarding EIA in studied areas particularly. Therefore, further studies with different
epidemiological settings, larger sample size and use of molecular techniques is obviously
warranted. The alarmingly high prevalence of glanders underscores the need to step up efforts for
control / eradication of disease from the region through revisiting of Glanders and Farcy Act and
strict implementation of ‘Test and Slaughter’ policy. Future epidemiological studies based upon
molecular techniques should be undertaken to determine prevalence of the disease in other regions
of Pakistan and scientific evaluation of possible risk factors involved in spread of glanders in
Pakistan. The present study highlights the lack of knowledge among veterinarians and animal
health workers regarding epidemiology, treatment and control of piroplasmosis. Furthermore,
education of equine owners regarding control of ticks and improvements in management practices
is required to control the alarmingly high seroprevalence of piroplasmosis. Future studies to
identify the potential vectors (e.g., ticks) responsible for spread and maintenance of equine
piroplasmosis as well as control program suited to the local context is also obviously warranted.

LITERATURE CITED
145
Literature Cited
Abdelkebir, R., H. Sahibi, S. Lasri, W. C. Johnson, L. S. Kappmeyer, A. Hamidouch, D. P.
Knowles and W. L. Goff, 2001. Validation of a competitive enzyme-linked
immunosorbent assay for diagnosing Babesia equi infections of Moroccan origin and its
use in determining the seroprevalence of B. equi in Morocco. J. Vet. Diag. Invest., 13:
249-251.
Acici, M., S. Umur, T. Guvenc, H. H. Arslan and M. Kurt, 2008. Seroprevalence of equine
babesiosis in the Black Sea region of Turkey. Parasitol. Int., 57: 198-200
Akkan, H. A., M. Karaca, M. Tutuncu, S. Deger, I. Keles and Z. Agaoglu, 2003. Serologic and
microscopic studies on babesiosis in horses in the eastern border of Turkey. J. Eq. Vet.
Sci., 181-183
Al-Ani, F. K., A .K. Delaimi and A. H. Ali, 1987. Glanders in horses: Clinical and
epidemiological studies in Iraq. Pak. Vet. J., 7:126–129.
Al-Ani, F. K., 1993. Glanders in Horses - A Review. Sud. J. Vet. Sci. Anim. Husb., 32 :1–9.
Al-Ani, F. K., O. F. Al-Rawashdeh, A. H. Ali and F. K. Hassan, 1998. Glanders in horses:
clinical, biochemical and serological studies in Iraq. Vet. Arhiv, 68:155–162.
Al-Ani, F. K. and J. Roberson, 2007. Glanders in horses: A review of the literature. Vet. Arhiv,
77: 203-218
Al-Bosadah, K. A. and A. M. Homeida, 2005. Some physical variables, biochemical and
haematological parameters in Hassawi ass. Sientific Journal of King Faisal University, 6:
145-152

LITERATURE CITED
146
Alhassan A., W. Pumidonming , M. Okamura , H. Hirata , B. Battsetseg , K. Fujisaki , N.
Yokoyama and I. Igarashi, 2005. Development of a single-round and multiplex PCR
method for the simultaneous detection of Babesia caballi and Babesia equi in horse
blood. Vet. Parasitol., 129(1-2):43-9.
Alhassan, A., O. M. M. Thekiso, N. Yokoyama, N. Inoue, M. Y. Motloang, P. A. Mbati, H. Yin,
Y. Katayama, T. Anzai, C. Sugimoto and I. Igarashi, 2007a. Development of loop-
mediated isothermal amplification (LAMP) method for diagnosis of equine
piroplasmosis. Vet. Parasitol., 143: 155-160
Alhassan, A., Y. Govind, N. T. Tam, O. M. M. Thekisoe, N. Yokoyama, N. Inoue and I.
Igarashi, 2007b. Comparative evaluation of sensitivity of LAMP, PCR and in vitro
culture methods for the diagnosis of equine piroplasmosis. Parasitol. Res., 100: 1165-
1168
Ali, S., C. Sugimoto and M. Onuma, 1996. Equine piroplasmosis. J. Equine Vet. Sci., 7: 67-77
Ambawat H. K, D. V. Malhotra, S. Kumar and S. Dhar, 1999. Erythrocyte associated haemato-
biochemical changes in Babesia equi infection experimentally produced in donkeys. Vet.
Parasitol., 85(4):319-24
Amerault, T. E., W. M. Freriches and D. Stiller, 1979. Comparative serologic study of equine
piroplasmosis with the card test and complement fixation tests. American J. Vet. Res., 40:
529-531
Anonymous, 2006. Pakistan Livestock Census. Agriculture Census Organization, Government of
Pakistan, Statistics Division.

LITERATURE CITED
147
Anonymous, 2008. World Animal Health Information Database (WAHID). . Disease
information. (http://oie.int/wahid-prod/public.php?page=home). Date accessed 24-12-
2008
Arun, S., H. Neubauer, A. Gurel, G. Ayyidiz, B. Kuscu, T. Yesidere, H. Meyer and W.
Hermanns, 1999. Equine glanders in Turkey. Vet. Rec., 144:255–258.
Asgarali, Z., D. K. Coombs, F. Mohammed, M. D. Campbell and E. Caesar, 2007. A serological
study of Babesia caballi and Theileria equi in Thoroughbreds in Trinidad. Vet.
Parasitol., 144: 167-171.
Ataseven, V. S. and H. H. Arslan, 2005. Equine infectious anemia in mules, donkeys, and horses:
epidemiologic studies in the different geographic regions of Turkey. J. Equine Vet. Sci.,
25: 439-441
Balkaya, I. and S. Z. Erdogmus, 2006. Investigation of prevalence of Babesia equi (Laveran,
1901) and Babesia caballi (Nuttall, 1910) in horses by serological methods in Elazig and
Malatya province. F. Ü. Sağ. Bil. Vet. Derg., 20: 61-63.
Barbosa, I. P., R. Bȍse, B. Peymann and K. T. Friedhoff, 1995. Epidemiological aspects of
equine babesioses in a herd of horses in Brazil. Vet. Parasitol., 58: 1-8
Bashir, A., 1984. Incidence and epidemiology of glanders in and around Fasialabad. M.Sc.
Thesis, Department of Veterinary Microbiology, Univ. of Agriculture, Faisalabad.
Batmanov, V. P., 1991. Sensitivity of Pseudomonas mallei to fluoroquinolones and their
effectiveness in experimental glanders (in Russian). Antibiot. Khimioter., 39: 33–7.
Batmanov, V. P., 1993. Treatment of experimental glanders with combinations of sulfazine or
sulfamonomethoxine with trimethoprim (in Russian). Antibiot. Khimioter., 38: 18-22

LITERATURE CITED
148
Batmanov, V. P., 1994 Sensitivity of Pseudomonas mallei to tetracyclines and their efficacy in
experimental glanders. Antibiot. Khimioter., 36: 31–34.
Bazargani, T. T., H. Tadjbakhs, A. Badii and T. Zahraei, 1996. The outbreak of glanders in some
racehorses in three states of Iran. J. Equine Vet. Sci., 16: 232–236.
Benjamin, M. M., 1978. Outline of Veterinary Clinical Pathology. The Iwoa State University
Press, USA.
Bicout, D. J., R. Carvalho, K. Chalvet-Monfray and P. Sabatier, 2006. Distribution of equine
infectious anemia in horses in the north of Minas Gerais State, Brazil. J. Vet. Diag.
Invest., 18: 479-82
Boldbaatar, D., X. Xuan, B. Battsetseg, I. Igarashi, B. Battur, Z. Batsukh, B. Bayambaa and K.
Fujisaki, 2005. Epidemiological study of equine piroplasmosis in Mongolia. Vet.
Parasitol., 127: 29-32
Brüning, A., 1996. Equine piroplasmosis an update on diagnosis, treatment and prevention. Br.
Vet. J.,152: 139-151
Burridge, M.J., 1981. Epidemiological approaches to diseases control. In Ristic, M. and
McIntyre, I. (ed), Diseases of Cattle in the Tropics. Martinus Nijhof Publishers,
Netherlands.
Calder, J. A., G. R. Reddy, L. P. Chieves, C. H. Courteny, R. Little, J. R. Livengood, R. A.
Norval and S. C. J. B. Dame, 1996. Monitoring Babesia bovis infections in cattle by
using PCR based tests. J. Clin. Microbiol., 11: 2748-2755

LITERATURE CITED
149
Callow, L. L., W. McGregor, B. Rodwell, R. Rogers, G. Fraser, D. Mahoney and G. Robertsob,
1979. Evaluation of an indirect fluorescent antibody test to diagnose Babesia equi and
Babesia cabali infection in horses. Australian Vet. J., 55: 555-559
Camacho, A. T., F. J. Guitian, E. Pallas, J. J. Gestal, A. S. Olmeda, M. A. Habela, S. R. Telford
III and A. Spielman, 2005. Theileria (Babesia) equi and Babesia caballi infections in
horses in Galicia, Spian. Trop. Anm. Health Prod., 37: 293-302
Chahan, B., S. Zhang, J. Seo, C. Nakamura, G. Zhang, H. Bannai, Z. Jian, H. Inokuma, K.
Tuchiya, Y. Sato, H. Kabeya, S. Maruyama, T. Mikami and X. Xuan, 2006.
Seroepidemiological evidence for the possible presence of Babesia (Theileria) equi and
Babesia caballi infections in donkeys in Western Xinjiang, China. J. Vet. Med. Sci., 68:
753-755
Cheevers, W. P. and T. C. McGuire, 1985. Equine Infectious virus: immunopathogenesis and
persistence. Rev. Inf. Dis., 7: 83-87.
Clabough, D. L., D. Gebhard and M. T. Flaherty, 1991. Immune-mediated thrombocytopenia in
horses infected with equine infectious anemia virus. J. Virol., 65: 6242-6251.
Coggins, L., N. L. Norcross and S. R. Nusbauma, 1972. Diagnosis of Equine Infectious Anemia
virus by immunodiffusion test. American J. Vet. Res., 33: 11-18.
Cole, T. W., 1942. Glanders. In: Keeping Livestock Healthy - Year Book of Agriculture. United
States Department of Agriculuture. United States Govt. Printing Office, pp: 409–412.
Coles, E. H., 1986. Veterinary Clinical Pathology, 4th Ed. W. B. Saunders Co., Philadelphia,
USA

LITERATURE CITED
150
Cordes, T. and C. J. Issel, 1996. Equine Infectious Anemia: a status report on its control. United
States Department of Agriculture (USDA)
Cordes, T. R., C. J. Issel, E. N. Ostlund and B. J. Schmitt, 2001. Equine Infectious Anemia.
United States Department of Agriculture (USDA)
Cullinane, A., M. Quinlivan, M. Nelly, H. Patterson, R. Kenna, M. Garvey, S. Gildea, P. Layons,
M. Flynn, P. Galvin, M. Neylon and K. Jankowska, 2007. Diagnosis of equine infectious
anemia during the 2006 outbreak in Ireland. Vet Rec., 161: 647-652
Dalling, S.T., 1966. International Encyclopedia of Veterinary Medicine. Vol II. Sweet and
Maxwell Ltd. London, pp: 1169–1173.
Damdinsuren, B., X. Xuan, B. Battsetseg, I. Igarashi, B. Battur, Z. Batuskh, B. Bayambaa and K.
Fujisaki, 2005. Epidemiological study of equine piroplasmosis in Mangolia. Vet.
Parasitol., 127: 29-32
Darling, R. G., and J. B. Woods, 2004. USAMRIID’s Medical Management of Biological
Causalities Handbook. Operational Medicine Department, U.S. Army Medical Research
Institute of Infectious Diseases, Fort Detrick, Maryland, USA
Davies, G. O., 1955. Gaiger and Davies’s Veterinary Pathology and Bacteriology. 4th Ed.
Bailliere, Tindall and Cox, London. pp: 389–398.
Derbyshire, J. B., 2002. Eradication of glanders in Canada. Canadian Vet. J., 43: 722-726.
De Waal, D. T., 1992. Equine piroplasmosis: a review. Br. Vet. J., 148: 6-14

LITERATURE CITED
151
Donnelly, J., L. Joyner, O. Graham-Jones and C. Ellis. 1980. A comparison of the complement
fixation and fluorescent antibody tests in a survey of the prevalence of Babesia caballi in
horses in the Sultanate of Oman. Trop. Anm. Health Prod., 12: 50-60
Dungworth, D.L., 1993. Glanders. In: Pathology of Domestic Animals. K.V.F. Jubb, Peter, C.
Kennedy and Nigel Palmer (Eds.). Vol. II. 4th Ed. Academic Press Inc., USA. pp: 553–
555.
Farani, M., 1983. The Glanders and Farcy Act, 1899. In: Livestock Law Manual. FAO Rome,
Italy. pp: 142-147.
Ferster, L. N., V. A. Zharkova, N. P. Khrapova and E. A. Volkov, 1986. Possible use of the
indirect hemagglutination reaction for determining the sensitivity of the bacteria of
glanders and melioidosis to antibiotics. Antibiot. Med. Biotekhnol., 31: 454-456.
Friedhoff, K. T., A. M. Tenter and I. Müller, 1990. Haemoparasites of Equines: impact on
international trade of horses. Rev. Sci. Tech., 9: 1187-1194
Gangulee, R. C., G. P. Sen and G. L. Sharma, 1966. Serological diagnosis of glanders by
haemagglutination test. Ind. Vet. J., 43: 386.
Gill, F. R., M. H. Hussain, G. Muhammad, M. K. Mansoor, M. A. Hafeez, M. Q. Bilal and U.
Tahir, 2008. Enzyme linked immunosorbant assay (ELISA) based seronegative findings
on the investigations of equine infectious anemia in Faisalabad Metropolis (Pakistan). In:
Proceedings of 29th World Veterinary Congress held on July, 27-31 at Vancouver,
Canada.
LITERATURE CITED
152
Gillespie, J. H. and J. F. Timoney, 1981. Hagan and Bruner’s Infectious Diseases of Domestic
Animals. Comstock Pubulishing Associates, Cornell University Press, Ithach, New York,
USA. pp: 55–60.
Gregory, B. C. and D. M. Wagg, 2007. Glanders. In:Medical Aspects of Biological Warfare. US
Army Medical Department Center and School, Fort Sam Houston, Texas.
Gul, S. T., M. Ahmad, A. Khan and I. Hussain, 2007. Haemato-biochemical observations in
apparently healthy equine species. Pak. Vet. J., 27: 155-158
Hagebock, J. M., L. K. Schlater, W. M. Freriches and D. P. Olson, 1993. Serologic response to
the mallien test for glanders in solipeds. J. Vet. Diag. Invest., 5: 97-99
Hailat, N. Q., S. Q. Lafi, A. M. Al-Darraji and F. K. Al-Ani, 1997. Equine babesiosis associated
with strenuous exercise: clinical and pathological studies in Jordan. Vet. Parasitol., 69:1-
8
Hartwigk, H. and H. Gerber, 1986. Infectious Diseases. In: Equine diseases. Hanns-Jurgern
Wintzer. (ed.) Springer Verlag, New York, USA. pp: 371–373.
Hayes, M. H., 1968. Veterinary Notes for Horse Owners. 16th Ed. Revis., Donald Tutt. Arco Pub.
Co. Inc. New York, USA, pp: 229–236.
Henry, M. M., 1992. Hemolytic anemia. In: Robinson N. E., (ed), Current Therapy in Equine
Medicine, 3rd Ed. W. B. Saunders, New York, USA, pp: 495-501
Heuchert, C. M. S., V. de Giulli Jr, D. F. de Athaide, R. Böse and K. T. Friedhoff, 1999.
Seroepidemiologic studies on Babesia equi and Babesia caballi infections in Brazil. Vet.
Parasitol., 85: 1-11

LITERATURE CITED
153
Higgins, A. J. and I. M. Wright, 1993. The Equine Manual. Saunders Publisher, China. pp: 27-30
Higgins, A. J. and I. M. Wright, 1998. The Equine Manual. W.B. Saunders, Co. London. pp: 77–
79.
Huang, X., X. Xuan, N. Yokoyama, Y. Katamaya, T. Anzai and I. Igarashi, 2006. Evaluation of
enzyme-linked immunosorbent assay with recombinant antigens for the serodiagnosis of
equine Babesia infections. Vet. Parasitol., 140: 158-161
Hungerford, T. G., 1990. Hungerford’s Diseases of Livestock. 9th Ed. McGraw Hill Book Co.,
Sydney.
Hutyra, F., J. Marek, and R. Manninger, 1949. Special Pathology and Therapeutics of the
Diseases of Domestic Animals. 5th Eng. Ed. Vol I Bailliere Tindall and Cox, London. pp:
722-773.
Ikadai, H., A. Nagai, X. Xuan, I. Igarashi, T. Kamio, N. Tsuji, T. Oyamada, N. Suzuki and K.
Fujisaki, 2002. Seroepidemiologic studies on Babesia caballi and Babesia equi infections
in Japan. J. Vet. Med. Sci., 64: 325-328
Iliukhin, V. I., V. V. Alekseev, I. V. Antonov, S. T. Savchenko and N. A. Lozovaia,1994.
Effectiveness of treatment of experimental glanders after aerogenic infection. Antibiot.
Khimioter. 39: 45–48.
Ishii, S., and R. Ishitani, 1975. Equine Infectious Anemia. Advances in Veterinary Science and
Comparative Medicine, 19: 195-222
Issel, C. J., J. M. MacManus and S. D. Hagius, 1990. Equine Infectious Anemia: prospects for
control. Develop. Biol. Stand., 72: 49-57.

LITERATURE CITED
154
Issel, C. J. and R. F. Cook, 1993. A review of techniques for the serologic diagnosis of equine
infectious anemia. J. Vet. Diag. Invest.., 5: 137.
Issel, C. J., W. Wright and W. M. Sr.-Lucille, 2005. Equine infectious anemia (EIA): 25 years
and $600,000,000 later. Ed. Dis. Quarterly, 14(1): 2
Jana, A. M., A. K. Gupta, G. Pandya, R. D. Verma and K. M. Rao, 1982. Rapid diagnosis of
glanders in equines by counter-immuno-electrophoresis. Ind. Vet. J., 59: 5–9.
Jenkinson, D, E., E. Y. Hugh and B. L. Douglas, 2007. Equine sweating and anhidrosis. Vet.
Dermatol., 18: 2-11
Kappmeyer, L. S., L. E. Perryman and D. P. Knowles, 1993. A Babesia equi gene encodes a
surface protein with homology to Theileria species. Mol. Biochem. Parasitol., 62: 121-
124
Kappmeyer, L. S., L. E. Perryman, S. A. Hines, T. V. Baszler, J. B. Katz, S. G. Hennager and D.
P. Knowles, 1999. Detection of equine antibodies to Babesia caballi recombinant B.
caballi rhoptry-associated protein 1 in a competitive-inhibition enzyme-linked
immunosorbent assay. J. Clin. Microbiol., 37, 2285–2290.
Karatepe, B., M. Karatepe, A. Cakmak, Z. Karaer and G. Ergün, 2009. Investigation of
seroprevalence of Theileria equi and Babesia caballi in horses in Nigde province,
Turkey. Trop. Anim. Hlth. Prod., 41: 109-113
Katz, J. B., L. P. Chiever, S. G. Hennager, J. M. Nicholson, T. A. Fisher and P. E. Byers, 1999.
Serodiagnosis of equine piroplasmosis, dourine and glanders using an arrayed immuno-
blotting method. J. Vet. Diagn. Invest., 11: 292–294.
LITERATURE CITED
155
Katz, J. B, R. Dewald and J. Nicholson, 2000. Procedurally similar competitive immuno-assay
system for the diagnosis of Babesia equi, Babesia cabali, Trypanosoma equiperdum, and
Burkholderia mallei infection in horses. J. Vet. Diagn. Invest., 12: 46–50.
Khan, M. Q., B. Hayat and C. S. Hayat, 1987. Prevalence of blood parasites in equines in and
around Faisalabad. Pak. Vet. J., 3: 113-116
Kirmizigȕl, A. H., Y. Yildrim, E. Gȍkçe and V. S. Ataseven, 2009. Serologic evaluation of
equine infectious anemia in Kars and Ardahan – Turkey. Kafkas Ȕniv. Vet. Fak. Derg.,
15: 77-80
Knowles, R. C., 1988. Equine babesiosis: epidemiology, control and chemotherapy. J. Equine
Vet. Sci., 8: 61-64
Knowles, D. P., L. E. Perryman, L. S. Kappmeyer and S. G. Hennager, 1991. Detection of
equine antibody to Babesia equi meroziotes protein by a monoclonal antibody-based
competitive inhibition enzyme-linked immunosorbent assay. J. Clinical Microbiol., 29:
2956-2958
Knowles, D. P., 1996. Control of Babesia equi parasitemia. Parasitol Today, 12: 195-198
Kokab, R., 1986. Observations on blood parasites of ungulates of N. W. F. P. (Pakistan). M. Sc.
Thesis, Department of Zoology, University of Peshawar.
Kono, Y., 1972. Development of immunity after immunization and infection with avirulent,
attenuated and virulent equine infectious anemia viruses. In: Proceedings, 3d
international conference on equine infectious diseases; 17-21 Paris. Basel: Karger: 242-
254.

LITERATURE CITED
156
Kumar, S., D. V. Malhotra, S. Dhar and A. K. Nichani, 2002. Vaccination of donkeys against
Babesia equi using killed merozoite immunogen. Vet. Parasitol., 106: 19-33
Lawrence, P. R., K. Lawrence, J.T. Dijkman and P. H. Starkey,1993. Research for development
of animal traction in West Africa. Proceedings of the Fourth Workshop of the West
Africa Animal Traction Network held in Kano, Nigeria, 9-13 July 1990. International
Livestock Centre for Africa (ILCA), Addis Ababa, Ethiopia.
Leroux, C., J. L. Cadore and R. C. Montelaro, 2004. Equine infectious anemia virus (EIAV):
what has HIV’s country cousin got to tell us? Vet. Res., 35: 482-512
LiPuma, J. J., 2007. Update on Burkholderia nomenclature and resistance. Clin. Microbiol.
Newsletter, 29: 65-69
Lopez, J., J. Copps, C. Wilhelmsen, R. Moore, J. Kubay, M. St-Jacques, S. Halayko, C.
Kranendonk, S. Toback, D. DeShazer, D. L. Fritz, M. Tom and D. E. Woods, 2003.
Characterization of experimental equine glanders. Microb. Infect., 5: 1125-1131.
Lovell, R., 1935. Intradermal mallein test. J. Royal Army, Vet. Corps, 6:69–70.
Ma, C. L., S. M. Fan, X. Wang, L. Jiang and S. Q. Fang, 1986. Diagnosis of glanders in horses
by the indirect fluorescent antibody (IFA) technique. Chinese J. Vet. Sci. Technol., 9: 3-5.
Malhotra D. V., D. P. Banerjee and O. P. Gautam, 1978. Prevalence of latent cases of Babesia
equi infection in some parts of North West India as measured by the capillary
agglutination test. Equine Vet. J., 10(1):24-6.
Manso, H., 2003. Glanders. Eq. Dis. Quarterly, 12 (1): 2-3

LITERATURE CITED
157
Manzeniuk, I. N., Dorokhin, V. V. and Svetoch, E. A., 1994. The efficacy of antibacterial
preparations against Pseudomonas mallei in in-vitro and in-vivo experiments (in
Russian). Antibiot. Khimioter., 39: 26–30.
Manzeniuk, I. N., Manzeniuk, O. I., Filonov, A. V., Stepanshin, I. G. and Svetoch, E. A., 1995.
Resistance of Pseudomonas mallei to tetracyclines: assessment of the feasibility of
chemotherapy (in Russian). Antibiot. Khimioter., 40: 40–44.
Menzies F. and T. Patterson, 2006. Description of the first case of equine infectious anemia in
Northern Ireland. Vet. Rec., 159: 753-754.
Miller W., L. Pannel, L. Cravitz, A. Tanner and M. Ingalls, 1948. Studies on certain biological
characteristics of Malleomyces mallei and Malleomyces pseudomallei I. Morphology,
cultivation, viability, and isolation from contaminated specimens. J. Bacteriol., 55: 115-
126.
Minett, F.C., 1930. Glanders. In: A System of Bacteriology in Relation to Medicine. Vol.1. H.
M. Stationary Office, London.
Minett F. C., 1959. Glanders and melioidosis. In: Infectious Diseases of Animals. Vol.1.
Diseases Due to Bacteria. A.W. Stableforth and I.A. Galloway (eds.) Butterworths
Scientific Publications, London, UK. pp: 296-309.
Misra, V. C. and A. K. Arora, 1990. Serological cross-reaction between Pseudomonas mallei and
other bacteria. Ind. J. Comp. Micro. Imm. Inf. Dis., 11: 28–31.
Montaginer, L., C. Dauguet and C. Axler, 1984. Anew type of retrovirus isolated from patients
presenting with lymphadenopathy and acquired immunodeficiency syndrome: Structure

LITERATURE CITED
158
and antigenic relatedness with EIA virus. Annals of Virology (Pasteur Institute). 135:
119-134.
Mota, R. A., M. F. Brito, F. J. Castro and M. Massa, 2000. Mormo em equideos nos Estados de
Pernambuco e Alagoas. Pes. Vet. Bras., 20: 155–159.
Muhammad, G., M.Z. Khan and M. Athar, 1998. Clinico–microbiological and therapeutic
aspects of glanders in equines. J. Equine Sci., 9: 93–96.
Nakajima, H. and T. Sugiura, 1994. Equine Infectious Anemia- Research in Japan on the
virology, immunology, pathogenesis and control. J. Equine Sci., 5: 1-19
Narbutovich, N. I., L. V. Lomova, N. P. Ageeva, V. T. Kucheriaeva and I. K. Seimova, 2005.
Some properties of plasma coagulase of the causative agent of glanders and melioidosis.
Zhurnal Mikrobiol. Epidemiol. Immunobiol., 3: 87-89.
Nasreen, N., 1977. A study on the incidence of glanders at Lahore. M.Sc. Thesis, College of
Veterinary Science, University of Agriculture, Faisalabad.
Naureen, A., M. Saqib, G. Muhammad, M. H. Hussain and M. N. Asi, 2007. Comparative
evaluation of Rose Bengal plate agglutination test, mallein and some conventional
serological tests for diagnosis of equine glanders. J. Vet. Diag. Invest., 19(4): 362-7.
Naureen, A., M. Saqib, M. N. Asi, M. H. Hussain and G. Muhammad, 2008. On-site test for
equine glanders. Eq. Dis. Quarterly, 17 (1): 3-4
Nayeri, G. D., 1978. Blood characteristics of the adult donkey. Zentrablatt Veterinarmed, 25:
541-547

LITERATURE CITED
159
Neubauer, H., L. D. Sprangue, R. Zacharia, H. Tomaso, S. Al Dhouk, R. Wernery, U. Wernery
and H. C. Scholz, 2005. Serodiagnosis of Burkholderia mallei infection in horse: State-
of-art and perspective. J. Vet. Med. Series B, 52: 201-205
OIE, 2004. Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (mammals, birds
and bees). 5th ed., Office International Des Epizootics, Paris.
Olivera M., and F. G. Garcia, 2001. Seroprevalencia de Babesiosis Equine en Caballos Pura
Sandre de Carrera en Haras de los Estados Aragua y Caraboba. Rev. Fac. Cs. Vets.
Parasitol. UCV.,42-3-13
Parė, J. and C. Simard, 2004. Comparison of commercial enzyme-linked immunosorbent assays
and agar gel immunodiffusion tests for the serodiagnosis of equine infectious anemia.
Canadian J. Vet. Res., 68: 254-8
Pawaiya, R. V. S. and R. S. Chauhan, 2008. A review on glanders – a re-emerging zoonosis in
India. Indian Veterinary Journal, 32(1): 1-14
Payne, S., B. Parrekh, R. C. Montelaro and C. J. Issel, 1984. Genomic alternation associate with
persistent infections by equine infectious anemia virus, a retrovirus. J. Gen. Virol., 65:
1395-1399.
Payne, S. L., O. Salinovich, S. M. Nauman, C. J. Issel and R. C. Montelaro, 1987. Course and
extent of variation of equine infectious anemia virus during parallel persistent infections.
J. Virol., 61: 66-70.
Pearson, J. E. and C. A. Gipson, 1988. Standardization of equine infectious anemia
immunodiffusion and C-ELISA test and their application to control of the disease in the
United States. Equine Vet. Sci., 8: 46-49.

LITERATURE CITED
160
Pfeifer B. I., R. Böse, B. Peymann and K. T. Friedhoff, 1995. Epidemiological aspects of equine
babesiosis in a herd of horses in Brazil. Vet. Parasitol., 58: 1-8
Piza, A. S. T., A. R. Pereira, M. T. Terreran, O. Mozzer, A. Tanuri, P. E. Brandao and L. J.
Richtzenhain, 2007. Serodiagnosis of equine infectious anemia by agar gel
immunodiffusion and ELISA using a recombinant p26 viral protein expressed in
Escherichia Coli as antigen. Prev. Vet. Med., 78: 239-245.
Posnett, E. S. and R. E. Ambrosio, 1989. Repetitive DNA probes for the detection of Babesia
equi. Mol. Biochem. Prasitol., 34: 75-78
Posnett, E. S. and R. E. Ambrosio, 1991. DNA probes for the detection of Babesia cabilli.
Prasitol., 102: 357-365
Radostits, O. M., C. C. Gay, K. W. Hinchcliff and P. D. Constable, 2007. Veterinary Medicine:
A textbook of diseases of cattle, horses, sheep, pigs and goat. 10th Ed. W. B. Saunders
Co., Philadelphia, USA.
Reece, W. O., 1997. Physiology of Domestic Animals. Williams and Wilkins, New York, USA.
Reynolds D., 2006. Equine infectious anemia in Ireland. Vet. Rec., 159: 219.
Ribeiro, M. F. B., J. O. Costa and A. M. Guimaräes, 1999. Epidemiological aspects of Babesia
equi in horses in Minas Gerais, Brazil. Vet. Res. Com., 23: 385-390.
Roberts, E. D., L. G. Morehouse, J. H. Gainer and H. A. McDaniel, 1962. Equine piroplasmosis.
J. Am. Vet. Med. Assoc., 141:1323-1329.
Rotz, L. D., A. S. Khan, S. R. Lillibridge, S. M. Ostroff and J. M. Hughes, 2002. Public health
assessment of potential biological terrorism agents. Emerg. Infect. Dis. 8: 225–230

LITERATURE CITED
161
Rüegg, S. R., P. Torgerson, P. Deplazes and A. Mathis, 2007. Age-dependent dynamics of
Theileria equi and Babesia caballi infections in southwest Mongolia based on IFAT
and/or PCR prevalence data from domestic horses and ticks. Parasitology, 134: 939-947
Rüegg, S. R., D. Heinzmann, A. D. Barbour and P. R. Torgerson, 2008. Estimation of the
transmission dynamics of Theileria equi and Babesia caballi in horses. Parasitology, 135:
555-565
Russell, P., Eley, S. M. and Ellis, J., 2000. Comparison of efficacy of ciprofloxacin and
doxycycline against experimental melioidosis and glanders. J. Antimicrob. Chemother.,
45: 813–818.
Sabirovic, M., L. Raw, S. Hall and N. Gibbens, 2005. International disease monitoring, April to
June 2005. Vet. Rec., 157: 333-336.
Salim, B. O. M., S. M. Hassan, M. A. Bakheit, A. Alhassan, I. Igarashi, P. Karanis and M. B.
Abdelrahman, 2008. Diagnosis of Babesia caballi and Theileria equi infections in horses
in Sudan using ELISA and PCR. Parasitol. Res., 103: 1145 - 1150
Saqib, M., 2000. Clinico–haematological and therapeutic studies on glanders in equines. M. Sc.
(Hons.), Department of Clinical Medicine & Surgery, University of Agriculture,
Faisalabad
Saqib, M., G. Muhammad, M. Athar and M. H. Hussain, 2003. Glanders. Equine Dis. Quart., 12:
2–3.

LITERATURE CITED
162
Saqib, M., A. Naureen, G. Muhammad, M. H. Hussain and M. N. Asi, 2008. Clinico-
hematological parameters and therapeutic studies in equine glanders. In: Proceedings of
29th World Veterinary Congress held on 27-30 July at Vancouver, Canada, pp: 1379
Saqib, M., A. Naureen, G. Muhammad, M. H. Hussain and M. N. Asi, 2008. Development and
evaluation of a more accurate test viz., latex agglutination test (LAT) for field diagnosis
of equine glanders in developing countries. In: Proceedings of 29th World Veterinary
Congress held on 27-30 July at Vancouver, Canada, pp: 1383
Seifi, H. A., M. Mohri and K. Sardari, 2000. A mixed infection of Babesia equi and Babesia
caballi in a racing colt: A report from Iran. J. Eq. Vet. Sci., 20: 858-860
Sellon, D. C., F. J. Fuller and T. C. McGuire, 1994. The immunopathogenesis of equine
infectious anemia virus. Virus Res., 32: 111-138.
Schein, E., 1988. Babesiosis of Domestic Animals and Man. CRC Press Inc., Boca Raton,
Florida
Shkap V., I. cohen, B. Leibovitz, Savitsky, E. Pipano, G. Avni, S. Shofer, U. Giger, L.
Kappmeyer and D. Knowles. 1998. Seroprevalence of Babesia equi among horses in
Israel using competitive inhibition ELISA and IFA assays. Vet. Parasitol., 76: 251-259.
Singh, G., S. S. Rathor and G. Singh, 1997. Serological evidence of equine infectious anemia in
horses in north India: a note. Indian J. Virol., 13: 73-74.
Smith, G.R., A.D. Pearson and M.T. Parker, 1990. Pasteurella infections, tularaemia, glanders
and meliodosis. In: Toply and Wilson’s Principle of Bacteriology, Mycology and
Immunolgy. Geoffrey, R. Smith and Charles S.F. Easmon (Eds). Vol. III. 8th Ed.

LITERATURE CITED
163
Songer, J. G. and K. W. Post, 2005. Veterinary Microbiology: Bacterial and Fungal Agents of
Animal Diseases. Elsevier Saunders. Missouri, USA. pp: 154-62.
Soutullo, A., V. Verwimp, M. Riveros, R. Pauli and G. Tonarelli, 2001. Design and validation of
ELISA for equine infectious anemia (EIA) diagnosis using synthetic peptides. Vet.
Microbiol., 79: 111-121
Spyrou, V., M. Papanastassopoulou, V. Psychas, Ch. Billinis, M. Koumbati, J. Vlemmas and G.
Koptopoulos, 2003. Equine infectious anemia in mules: virus isolation and pathogenicity
studies. Vet. Micobiol., 95: 49-59
Srinivasan, A., C. N. Kraus, D. DeShazer, P. M. Becker, J. D. Dick, L. Spacek, J. G. Bartlett, W.
R. Byrne and D. L. Thomas, 2001. Glanders in a military research microbiologist. N.
Engl. J. Med., 345: 256–258.
Stein, C. D., J. C. Lotze and L. O. Mott, 1942. Transmission of equine infectious anemia by the
stablefly, Stomoxys calcitrans, the horse fly, Tabanus sulcifrons (Macquart), and by
injection of minute amounts of virus. American J. Vet. Res., pp: 183-193.
Susan, D., G. Dallas, H. Mills and P. Burr, 2008. Assessment of 2 commercial ELISAs for EIA
and EVA serology. Biobest, UK.
(http://www.biobest.co.uk/assets/files/diagnostics/serological-testing.pdf)
Taboada, J. and S. R. Merchant, 1991. Babesiosis of companion animals and man. Vet. Clinics N.
Am: Small Animal Practice, 21: 103-123
Tenter, A. M., M. J. Otte, C. A. Gonzales and Y Abuabara, 1988. Prevalence of piroplasmosis in
equines in the Colombian province of Cordoba. Trop. Anim. Hlth., Prod., 20: 93-98

LITERATURE CITED
164
Thrall, M. A., 2004. Veterinary Hematology and Clinical Chemistry. Lippincott Williams &
Wilkins, Philadelphia, USA
Thrusfield, M., 2005. Veterinary Epidemiology. 2nd Ed. Blackwell Science Ltd. U.K.
Torina A., J. Vicente, A. Alongi, S. Scimeca, R. Tulra, S. Nicosia, V. Di Marco, S. Caracappa
and J. de la Fuente, 2007. Observed prevalence of tick-borne pathogens in domestic
animals in Sicily, Itlay during 2003-2005. Zoon. Pub. Hlth., 54:8-15
Turan, N., H. Yilmaz, A. Uysal and M. Arslan, 2002. Seronegative findings on the investigations
of equine infectious anemia in the Marmara region of Turkey. TȔBITAK, 26: 299-302
Udall, D. A., 1939. Practice of Veterinary Medicine. Published by Author. Ithaca, New York,
USA. pp: 539–546.
Uilenberg, G., 2006. Babesia – A historical overview. Veterinary Parasitology, 138: 3-10.
Uppal, P. K. and M. P. Yadav, 1989. Occurance of equine infectious anemia in India. Vet. Rec.,
124: 514-515.
Uppal, P. K. and M. P. Yadav, 1992. Application of competitive ELISA in the diagnosis of
equine infectious anemia. Current Sci., 63: 332-333
Urdaz-Rodriguez, J. H., G. T. Fosgate, A. R. Alleman, D. O. Rae, G. A. Donovan and P.
Melendez, 2009. Seroprevalence estimation and management factors associated with high
herd seropositivity for Anaplasma marginale in commercial dairy farms of Puerto Rico.
Trop. Anim. Hlth. Prod., 41: 1439-1448
Vaid, M.Y., M.A. Muneer and M. Naeem, 1981. Studies on the incidence of glanders at Lahore.
Pak. Vet. J., 1: 75.

LITERATURE CITED
165
Verma, R. D., 1981. Glanders in India with special reference to if incidence and epidemiology.
Ind. Vet. J., 58: 177–183.
Verma, R. D., 1990. A micro-complement fixation test for identifiatin of Pseudomonas mallei. J.
Remount. Vet. Crops., 29: 1–5.
Verma R. D., J. K. Sharma, K. S. Venkateswaran and H. V. Batra, 1990. Development of an
avidin-biotin dot enzyme-linked immunosorbent assay and its comparison with other
serological tests for diagnosis of glanders in equines. Vet. Microbiol,. 25(1):77-85.
Vial, H. J. and A. Gorenflot, 2006. Chemotherapy against babesiosis. Vet. Parasitol., 138: 147-
160.
Waag, D. M., and D. DeShazer, 2004. Glanders: new insights into an old disease. In: Biological
Weapons Defense: Infectious Diseases and Counterbioterrorism. Lindler L.E., LeBeda
F.J., Korch G.W., (eds). Totowa, NJ, Humana Press Inc. pp: 209-237
World Animal Health Information Database (WAHID), 2008. Weekly disease information.
(http://oie.int/wahid-prod/public.php?page=home).Date accessed 24-12-2008
Weiland, G., 1986. Species-specific serodiagnosis of equine piroplasma infections by means of
complement fixation test (CFT), immunofluorescence (IFA), and enzyme-linked
immunosorbent assay (ELISA). Vet. Parasitol., 20: 43-48
Weiland, G. and Reiter, I., 1988. Methods for the measurement of the serological response to
Babesi. In: Ristic, M. (Ed.), Babesiosis of Domestic Animals and Man. CRC press, Boca
raton, FL, pp: 144-162.
Wilkinson, L., 1981. Glanders: medicine and veterinary medicine in common pursuit of a
contagious disease. Med. Hist., 25(4): 363–384.

LITERATURE CITED
166
Winston, S., S. Fiscus, L. Hesterberg, T. Matsushita, M. Mildbrand, J. Porter and Y. Teramoto,
1987. Rapid detection of viral specific antibodies by Enzyme-linked immunosorbent
assay (ELISA). Vet. Immunol. Immnopathol., 17: 453-464.
Witting, M. B., P. Wohlsein, R. M. Hagan, S. AlDahouk, H. Tomaso, H. C. Scholz, K. Nikalaou,
R. Wernery, U. Wernery, J. Kinne, M. Elschner and H. Neubauer, 2006. Glanders-a
comprehensive review. Ein Ubersichtsreferat rotzerkrankung Deutsche Tierarzliche
Wochenschrift, 113: 323-330.
Xuan, X., I. Igarashi, T. Tanaka, S. Fukumoto, H. Nagasawa, K. Fujisaka and T. Mikami, 2001.
Detection of Babesia equi in horses by a latex agglutination test using recombinant
EMA-1. Clin. Diag. Lab. Immunol., 8: 645-646
Yoshihara, T., 1997. Equine piroplasmosis. J. Anim. Protoz., 11: 1-7
Zobba, R., M. Ardu, S. Niccolini, B. Chessa, L. Manna, R. Cocco and M. L. P. Parapaglia, 2008.
Clinical and laboratory findings in equine piroplasmosis. J. Eq. Vet. Sci., 28: 301-308
Zhang, W. D. and Z. B. Lu, 1983. Application of an indirect haemagglutination test for the
diagnosis of glanders and melioidiosis. Chinese. J. Vet. Med. Zhongguo-Shouyi-Zazhi., 9:
8–9.
Zinora A., D. K. Coombs, F. Mohammad, M. D. Campbell and E. Caesar, 2007. A serological
study of Babesia cabali and Theileria equi in Thoroughbreds in Trinidad. Vet. Parasitol.,
144: 167-171
Zinkl, J. G., D. Mae, P. G. Merida, T. B. Faver and J. A. Humble, 1990. Reference ranges and
influence of age and sex on hematologic and serum biochemical values in donkeys (Equs
asinus). American J. Vet. Res., 51: 408-413

LITERATURE CITED
167
Zintl, A., G. Mulchay, H. E. Skerrett, S. M. Taylor and J. S. Gray, 2003. Bebesia divergens, a
bovine blood parasite of veterinary and zoonotic importance. Clin. Microbiol. Rev., 16:
622-636.

168
APPENDIX
Proforma for the recording of information regarding reo-survey of equine infectious anemia, glanders and piroplasmosis in 5 draught equine populated urban areas of Punjab

169

170

171