selecting optimal antiangiogenic strategies for patients with hepatocellular carcinoma
TRANSCRIPT
Selecting Optimal Antiangiogenic
Strategies for Patients With
Hepatocellular Carcinoma
Thomas A. Abrams, MD
Assistant Professor of Medicine, Harvard Medical School
Senior Physician, Dana-Farber Cancer Institute

ACCREDITATION
This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation
Council for Continuing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and i3 Health.
The Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians.
The Postgraduate Institute for Medicine designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians
should claim only the credit commensurate with the extent of their participation in the activity.
The Postgraduate Institute for Medicine is accredited with distinction as a provider of continuing nursing education by the American
Nurses Credentialing Center’s Commission on Accreditation. This educational activity for 1.0 contact hours is provided by Postgraduate
Institute for Medicine.
INSTRUCTIONS TO RECEIVE CREDIT
In order to receive credit for this activity, participants must:
1. Participate in the live webinar
2. Complete and submit the posttest and activity evaluation via the link provided after the webinar
3. Download or print their Certificate of Credit
UNAPPROVED USE DISCLOSURE
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The
planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the
planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and
warnings.
DISCLAIMER
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional
development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures,
medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without
evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s
product information, and comparison with recommendations of other authorities.
COMMERCIAL SUPPORT
This activity is supported by an independent educational grant from Bayer HealthCare Pharmaceuticals Inc.

Disclosures
▶ Dr. Abrams discloses the following commercial
relationships:◼ Consulting/advisory board: Aduro Biotech, Bayer,
Bristol-Myers Squibb, Celgene, Genentech, Kaleido
◼ Research funding: Celgene, Lilly
▶ The PIM planners and managers, Trace Hutchison,
PharmD, Samantha Mattiucci, PharmD, CHCP, Judi
Smelker-Mitchek, MBA, MSN, RN, and Jan Schultz,
MSN, RN, CHCP have nothing to disclose
▶ i3 Health planners and managers have no relevant
financial relationships to disclose
Learning Objectives
▶ Describe the epidemiology of HCC and the etiologic
factors associated with disease development
▶ Review the rationale for angiogenesis inhibitor usage
for the treatment of advanced HCC
▶ Evaluate available HCC staging systems and their role
in treatment planning
▶ Assess data supporting the use of antiangiogenic
agents in first- and second-line treatment of advanced
HCC
HCC = hepatocellular carcinoma.
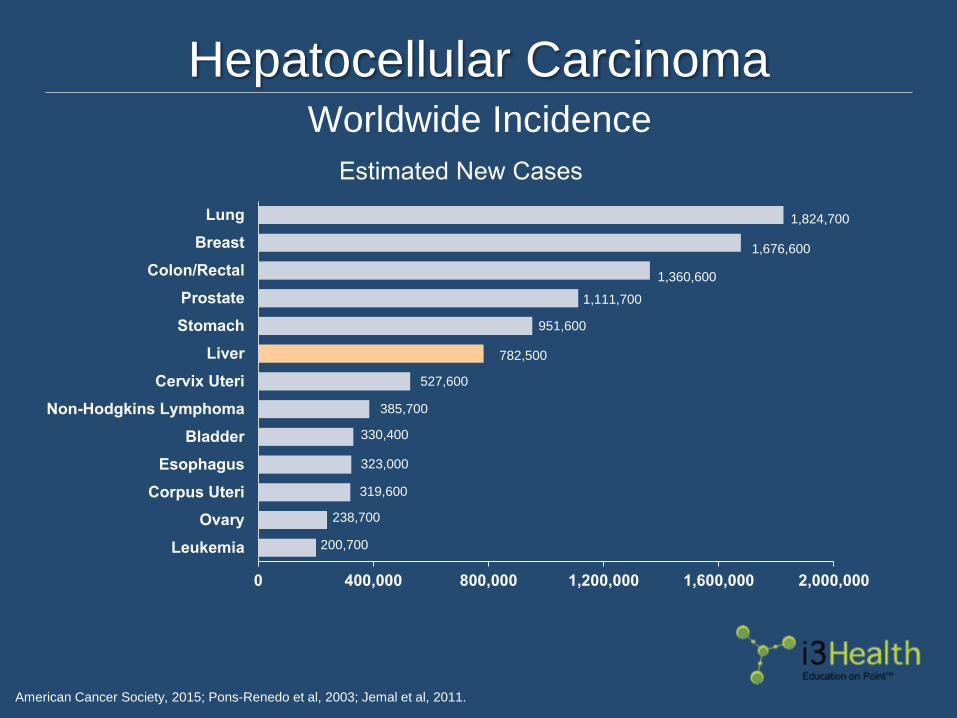
Hepatocellular Carcinoma
American Cancer Society, 2015; Pons-Renedo et al, 2003; Jemal et al, 2011.
Worldwide Incidence
1,824,700
1,676,600
1,360,600
1,111,700
951,600
782,500
527,600
385,700
330,400
323,000
319,600
238,700
200,700
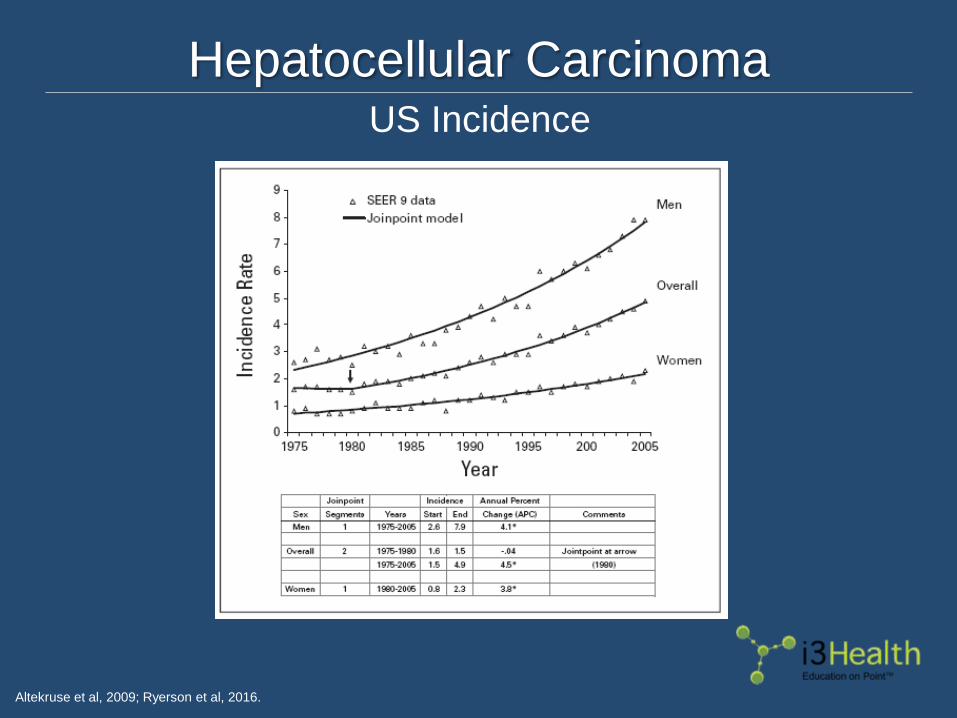
Hepatocellular Carcinoma
Altekruse et al, 2009; Ryerson et al, 2016.
US Incidence

HCC Risk Factors
▶ Cirrhosis: >90% of HCC cases in patients with
antecedent liver cirrhosis (all causes)
▶ Viral hepatitis infection◼ Hepatitis B virus (HBV)
– Can develop in HBV patients without cirrhosis
– Viral load a factor
◼ Hepatitis C virus (HCV): HCV treatment associated with risk
reduction
▶ Obesity, metabolic syndrome: likely through increased
incidence of NAFLD, NASH
NAFLD = non-alcoholic fatty liver disease; NASH = non-alcoholic steatohepatitis.
Chen et al, 2006; Omland et al, 2012; Van der Meer et al, 2012; Welzel et al, 2011.
HCC Risk Factors (cont.)
▶ Male sex: 4 x increase in incidence
▶ Alcoholic cirrhosis
▶ Rare causes◼ Aflatoxin exposure
◼ Hemochromotosis
◼ Porphyria
◼ Alpha-1 antitrypsin deficiency
◼ History of Fontan cardiac surgery
Chen et al, 2006; Omland et al, 2012; Van der Meer et al, 2012; Welzel et al, 2011.

Multistep Malignant Transformation
Tornillo et al, 2002; Verslype et al, 2007.
Potential Targets
Oxidative stress
and inflammation
Viral
oncogenesCarcinogens
Growth factorsTelomere
shortening
Cancer stem
cells
Loss of cell cycle
checkpointsApoptosis Angiogenesis
Normal
Liver
Hepatitis C
Hepatitis B
Ethanol
NASH
Liver
Cirrhosis
Dysplastic
Nodules
Epigenetic
Alterations
Genetic
Alterations
HCC
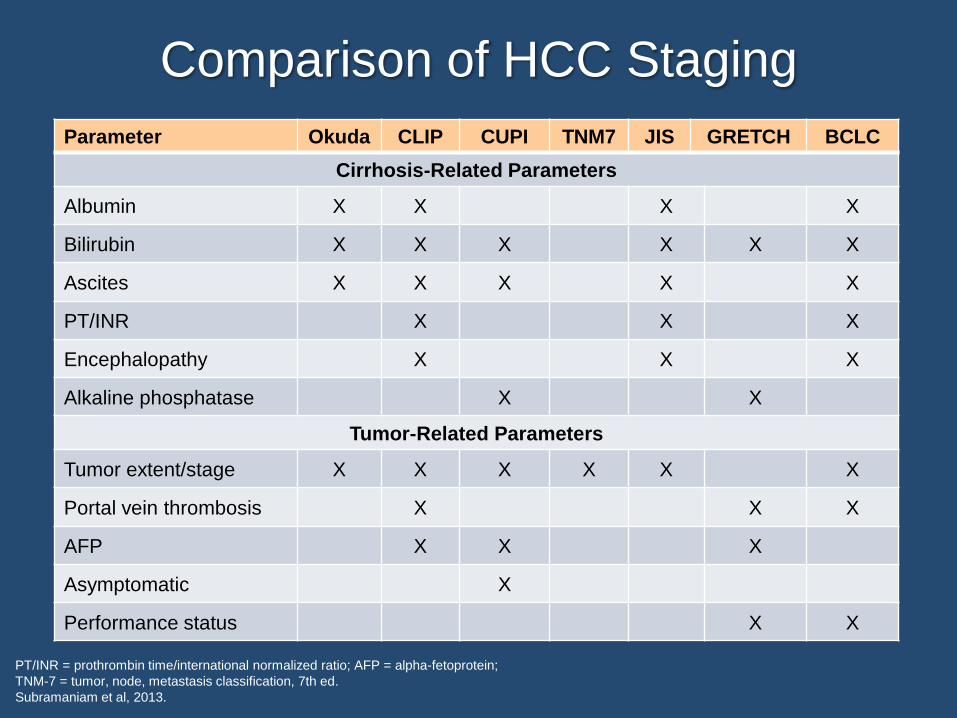
Comparison of HCC Staging
PT/INR = prothrombin time/international normalized ratio; AFP = alpha-fetoprotein;
TNM-7 = tumor, node, metastasis classification, 7th ed.
Subramaniam et al, 2013.
Parameter Okuda CLIP CUPI TNM7 JIS GRETCH BCLC
Cirrhosis-Related Parameters
Albumin X X X X
Bilirubin X X X X X X
Ascites X X X X X
PT/INR X X X
Encephalopathy X X X
Alkaline phosphatase X X
Tumor-Related Parameters
Tumor extent/stage X X X X X X
Portal vein thrombosis X X X
AFP X X X
Asymptomatic X
Performance status X X

BCLC Staging
BCLC = Barcelona Clinic Liver Cancer; ECOG PS = Eastern Cooperative Oncology Group performance status.
Llovet et al, 1999.
BCLC StageECOG
PS
Tumor Size/Number, Vascular
Involvement, Etc
Child-Pugh
Score
0 Very early 0 Solitary <2 cm nodule A
A Early 0Solitary <5 cm nodule or up to 3
nodules each ≤3 cmA - B
B Intermediate 0 Large/multinodular A - B
C Advanced 1-2Portal venous invasion and/or
extrahepatic spread (N+ or M+)A - B
D Terminal >2 Any of the above C
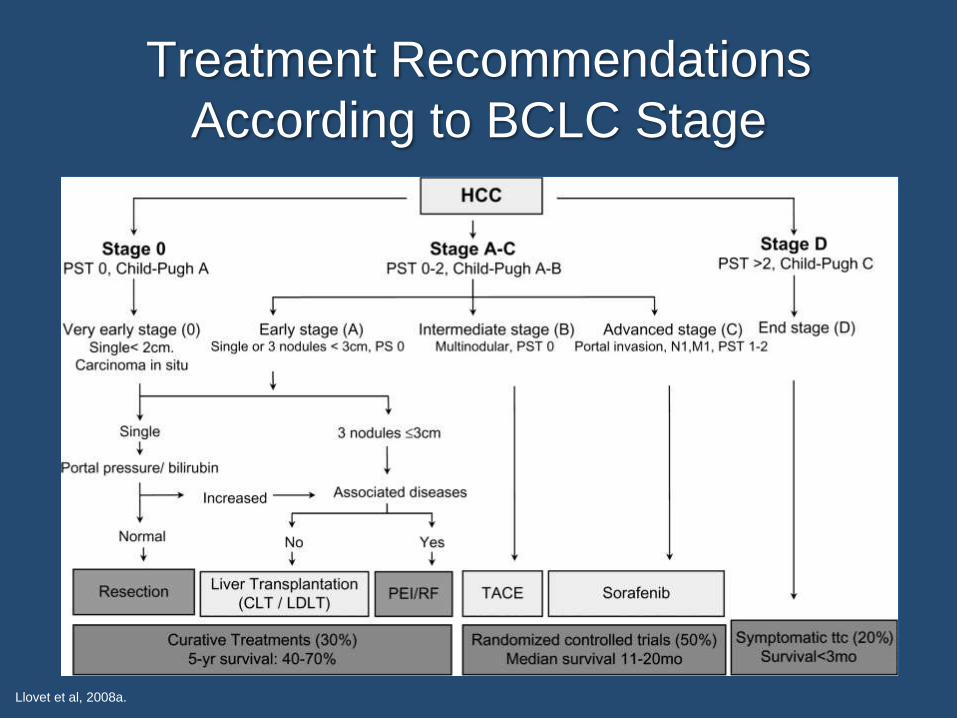
Treatment Recommendations
According to BCLC Stage
Llovet et al, 2008a.
Case Study: Mr. LT
▶ 58-year-old man with a history of chronic HCV
infection and cirrhosis
▶ Had not seen his PCP in several years
▶ Presents with several months of abdominal
pain, fatigue, and weight loss
▶ PE notable for 5.5-cm mass in the right upper
quadrant, palmar erythema, and spider
angiomata
PCP = primary care provider; PE = physical examination.

Case Study: Mr. LT (cont.)
▶ Routine laboratories notable for AST/ALT 2.5 x ULN,
bilirubin 0.9 mg/dL, albumin 3.3 g/dL, PT/INR WNL,
platelet count 80 x 109/L
▶ MRI scan of the abdomen reveals an 8-cm mass in the
right liver with early washout, tumor thrombus in the
portal vein, and hilar adenopathy
▶ Chest CT scan shows multiple metastatic nodules
throughout the lungs
▶ AFP >100,000 ng/mL
AST/ALT = aspartate transaminase/alanine transaminase; ULN = upper limit of normal;
PT/INR = prothrombin time/international normalized ratio; WNL = within normal limits;
MRI = magnetic resonance imaging; CT = computed tomography; AFP = alpha-fetoprotein

Case Study: Mr. LT (cont.)
▶ Pop Quiz

Case Study: Mr. LT (cont.)
▶ What treatment would you recommend for this
patient?
a. Sorafenib
b. Radioembolization
c. Chemoembolization
d. Radiofrequency ablation
e. Liver transplantation
Case Study: Mr. LT (cont.)
▶ What treatment would you recommend for this
patient?
a. Sorafenib
b. Radioembolization
c. Chemoembolization
d. Radiofrequency ablation
e. Liver transplantation

Angiogenesis in HCC
▶ HCC is characterized by an excess of angiogenic
factors produced by:◼ Tumor cells
◼ Vascular endothelial cells
◼ Immune cells
◼ Surrounding tumor microenvironment
▶ VEGF is an important mediator in hepatocarcinogenesis◼ Regulated by oncogenic gene mutations, hormones, and
cytokines
▶ VEGF creates a vascular network of leaky vessels and
abnormal vascular structure and function
Ghouri et al, 2017.

Sorafenib: A Multikinase Inhibitor
Adapted from Wilhelm et al, 2008.
NucleusNucleus
EGF/HGF
Angiogenesis:Differentiation
Proliferation
Migration
Tubule formation
MEK
ERKEGF/HGF
PDGF
VEGF
Proliferation
Survival
RAS
Vascular Cell
Autocrine loopParacrinestimulation
HIF-2
Mitochondria
Mitochondria
Apoptosis
RAS
RAF
MEK
ERK
Apoptosis
RAF
Tumor Cell
PDGFR-b VEGFR-2
Inhibits tumor growth and vascularization through a series of antiangiogenic
and antiproliferative effects

SHARP: Phase III Trial of
Sorafenib in Advanced HCC
OS = overall survival.
Llovet et al, 2008b.
Arm 2 (placebo) N=303
Eligibility▶ Advanced stage HCC▶ ECOG PS ≤2▶ Child-Pugh A▶ No prior treatment▶ Age ≥18 years
Arm 1 (sorafenib) N=299
602 pts randomly assigned
1:1 for 90% power to detect a
40% increase in OS
R
A
N
D
O
M
I
Z
E
Study Design▶ Double blind, placebo-
controlled▶ 121 sites primarily in North
America and Europe▶ Primary end point: OS

SHARP: Baseline Characteristics
Llovet et al, 2008b.

SHARP: Baseline Characteristics
(cont.)
Llovet et al, 2008b.
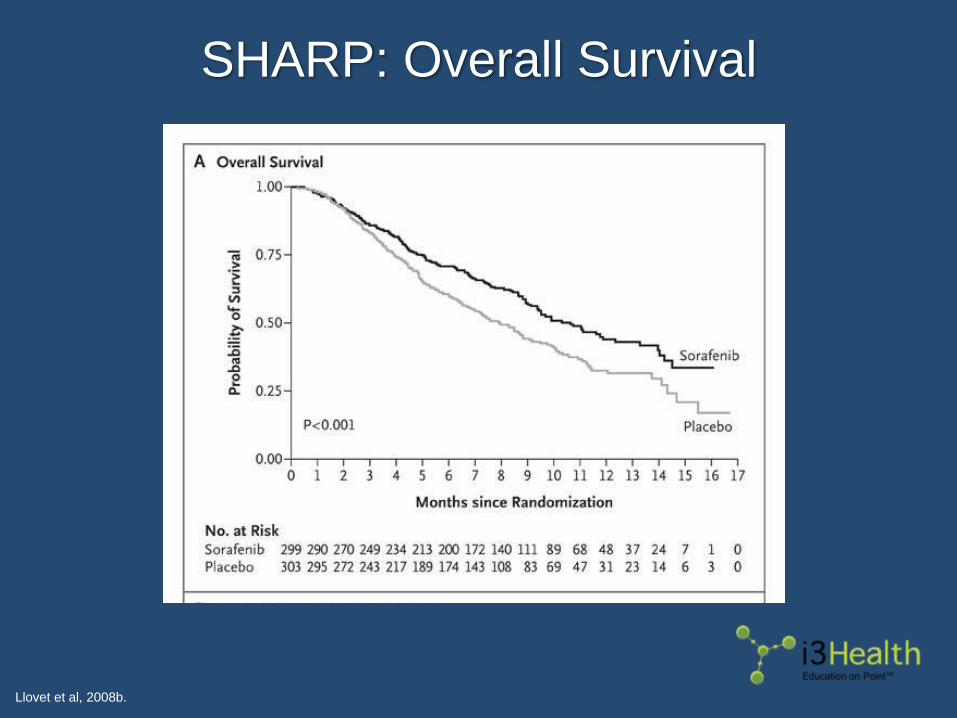
SHARP: Overall Survival
Llovet et al, 2008b.
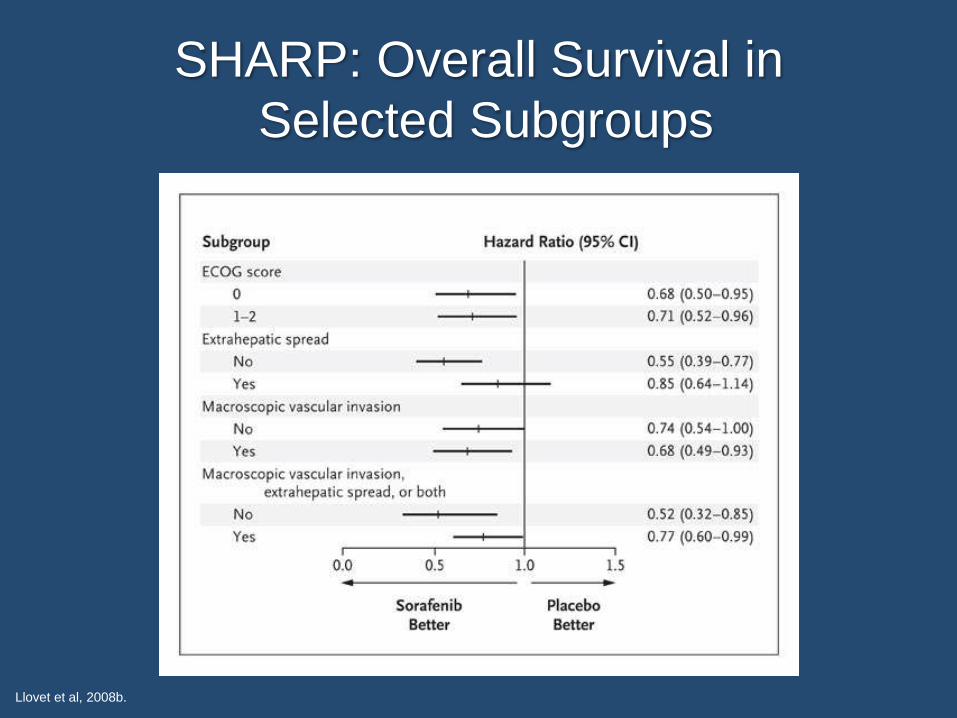
SHARP: Overall Survival in
Selected Subgroups
Llovet et al, 2008b.
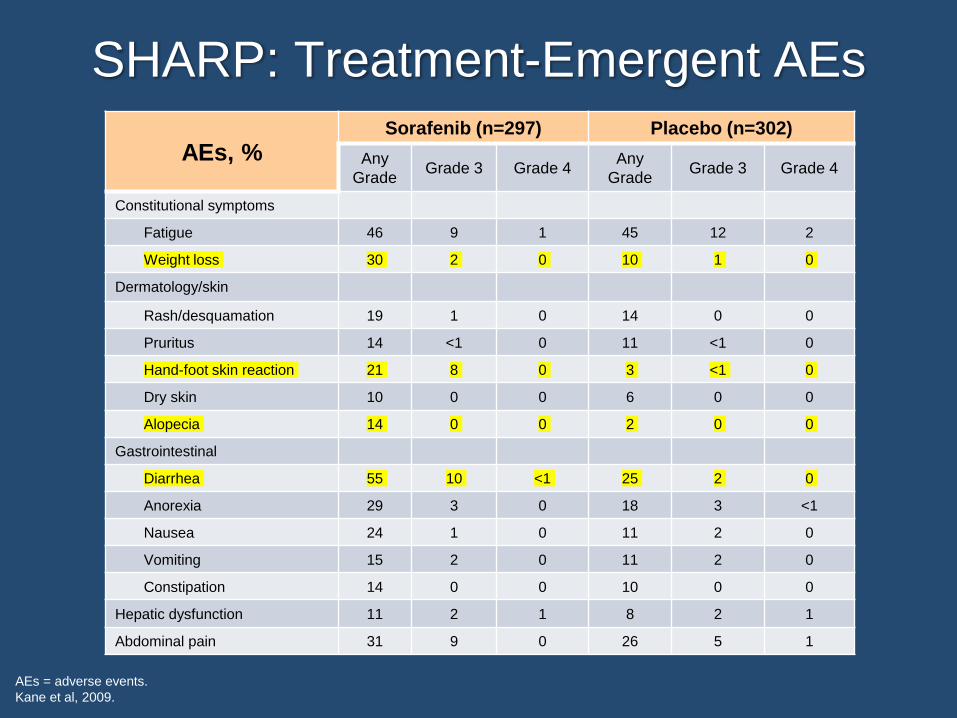
SHARP: Treatment-Emergent AEs
AEs = adverse events.
Kane et al, 2009.
AEs, %Sorafenib (n=297) Placebo (n=302)
Any
GradeGrade 3 Grade 4
Any
GradeGrade 3 Grade 4
Constitutional symptoms
Fatigue 46 9 1 45 12 2
Weight loss 30 2 0 10 1 0
Dermatology/skin
Rash/desquamation 19 1 0 14 0 0
Pruritus 14 <1 0 11 <1 0
Hand-foot skin reaction 21 8 0 3 <1 0
Dry skin 10 0 0 6 0 0
Alopecia 14 0 0 2 0 0
Gastrointestinal
Diarrhea 55 10 <1 25 2 0
Anorexia 29 3 0 18 3 <1
Nausea 24 1 0 11 2 0
Vomiting 15 2 0 11 2 0
Constipation 14 0 0 10 0 0
Hepatic dysfunction 11 2 1 8 2 1
Abdominal pain 31 9 0 26 5 1
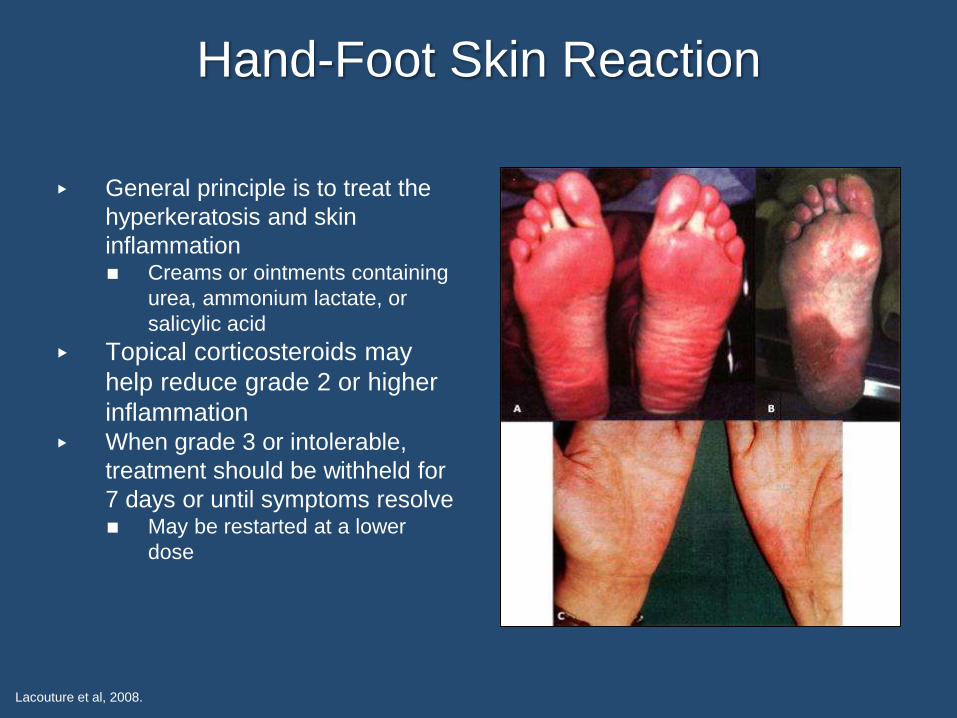
Hand-Foot Skin Reaction
▶ General principle is to treat the
hyperkeratosis and skin
inflammation◼ Creams or ointments containing
urea, ammonium lactate, or
salicylic acid
▶ Topical corticosteroids may
help reduce grade 2 or higher
inflammation▶ When grade 3 or intolerable,
treatment should be withheld for
7 days or until symptoms resolve◼ May be restarted at a lower
dose
Lacouture et al, 2008.

SHARP vs Asia-Pacific Study
TTP = time to progression; RR = response rate.
Llovet et al, 2008b; Cheng et al, 2009.
SHARP Asia-Pacific
Randomization Sorafenib vs Placebo Sorafenib vs Placebo
End pointHazard ratio
(95% CI)P value
Hazard ratio
(95% CI)P value
OS10.7 vs 7.9 mo
0.69 (0.55-0.87)<0.001
6.5 vs 4.2 mo
0.68 (0.50-0.93)0.014
TTP5.5 vs 2.8 mo
0.58 (0.45-0.74)<0.001
2.8 vs 1.4 mo
0.57 (0.42-0.79)<0.001
RR 2% vs 1% 3.3% vs 1.3%

Case Study: Mr. LT (cont.)
▶ Pop Quiz
Case Study 2 (cont.)
▶ Six months post-sorafenib, Mr. LT develops
progressive disease. What would you now
recommend?
a. FOLFOX
b. Liposomal doxorubicin
c. Regorafenib
d. Repeat chemoembolization

Case Study 2 (cont.)
▶ Six months post-sorafenib, Mr. LT develops
progressive disease. What would you now
recommend?
a. FOLFOX
b. Liposomal doxorubicin
c. Regorafenib
d. Repeat chemoembolization

Regorafenib in HCC: Rationale
▶ Multikinase inhibitor that differs from sorafenib by the
addition of a lone fluorine atom
▶ Despite similar molecular structure, it differentially
inhibits tyrosine kinases such as VEGFR1, RET, FGFR-
1, and c-KIT
▶ Has metabolites that allow the agent to continue to have
effect despite 1-week washout period
Trojan & Waidmann, 2016.

RESORCE: Phase III Trial of
Regorafenib in Post-Sorafenib HCC
POD = progression of disease.
Bruix et al, 2017.
Placebo (n=194)
Eligibility▶ Advanced stage HCC with
documented POD on sorafenib treatment
▶ ECOG PS 0 or 1▶ BCLC stage B or C▶ Child-Pugh A▶ Age ≥18 years
Regorafenib 160 mg
daily, 3 weeks on/1 week
off (n=379)
573 pts randomly assigned
2:1 for 90% power to detect a
43% increase in OS
R
A
N
D
O
M
I
Z
E
Study Design▶ Double blind, placebo-
controlled▶ 152 sites in North and
South America, Europe, Australia, and Asia
▶ Primary end point: OS

RESORCE: Baseline Characteristics
Bruix et al, 2017.
Characteristic Regorafenib (n=379) Placebo (n=194)
Male 88% 80%
Age, median years (range) 64 (19-85) 62 (23-83)
Race
White 36% 35%
Asian 41% 40%
Black 2% 1%
Other/not reported 21% 24%
Geographic region Asia 38% 38%
ECOG PS, 0/1 65%/35% 67%/33%
Etiology of HCC
Alcohol abuse 24% 28%
HBV 38% 38%
HCV 21% 21%
NASH 7% 7%
Other 7% 5%
Unknown 17% 16%
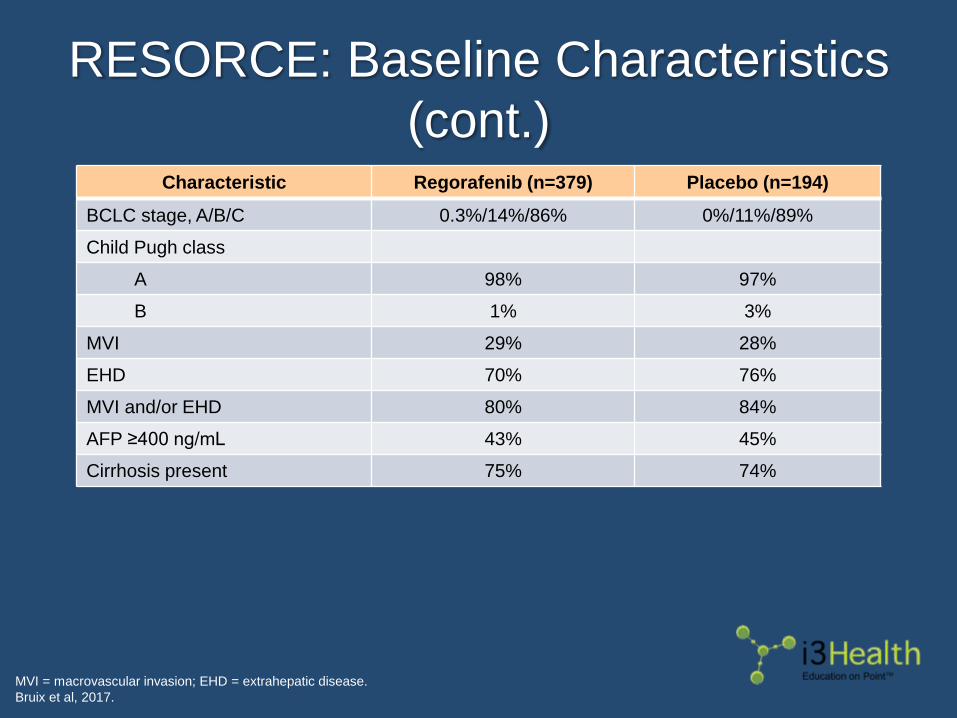
RESORCE: Baseline Characteristics
(cont.)
MVI = macrovascular invasion; EHD = extrahepatic disease.
Bruix et al, 2017.
Characteristic Regorafenib (n=379) Placebo (n=194)
BCLC stage, A/B/C 0.3%/14%/86% 0%/11%/89%
Child Pugh class
A 98% 97%
B 1% 3%
MVI 29% 28%
EHD 70% 76%
MVI and/or EHD 80% 84%
AFP ≥400 ng/mL 43% 45%
Cirrhosis present 75% 74%
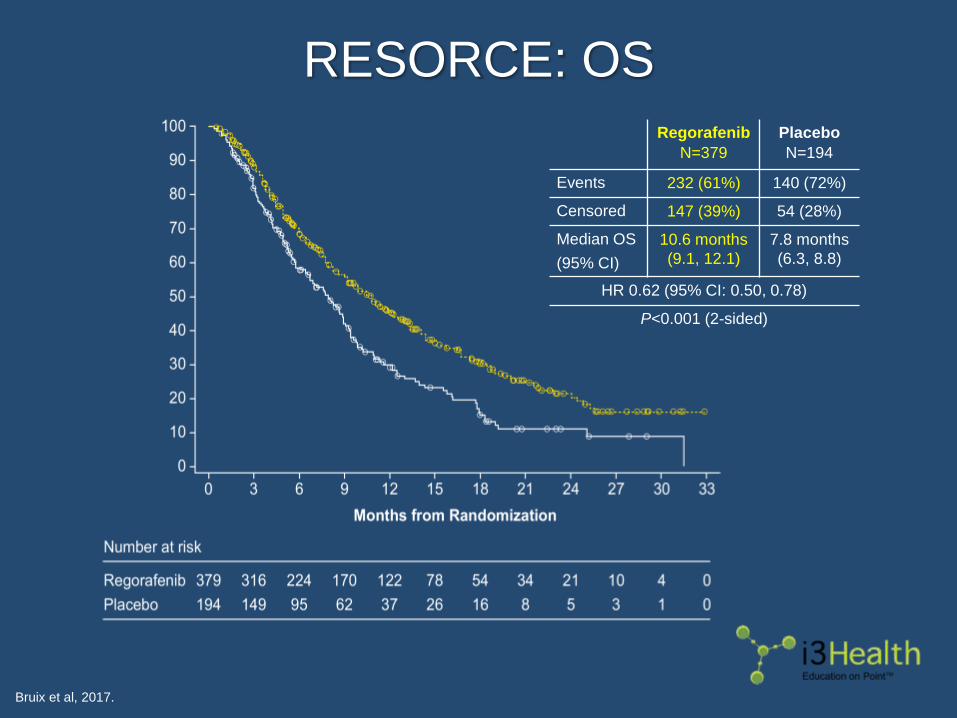
RESORCE: OS
Bruix et al, 2017.
Regorafenib
N=379
Placebo
N=194
Events 232 (61%) 140 (72%)
Censored 147 (39%) 54 (28%)
Median OS
(95% CI)
10.6 months
(9.1, 12.1)
7.8 months
(6.3, 8.8)
HR 0.62 (95% CI: 0.50, 0.78)
P<0.001 (2-sided)

RESORCE: OS Subgroup Analysis
Bruix et al, 2017.

RESORCE: Treatment-Emergent AEs
HFSR = hand-foot skin reaction.
Bruix et al, 2017.
AEs
Regorafenib
n=374
Placebo
n=193
Any
GradeGr 3 Gr 4
Any
GradeGr 3 Gr 4
HFSR 53% 13% NA 8% 1% NA
Fatigue 41% 9% NA 32% 5% NA
Hypertension 31% 15% <1% 6% 5% 0
Bilirubin increased 29% 10% 1% 18% 8% 3%
AST increased 25% 10% 1% 20% 10% 2%
Ascites 16% 4% 0 16% 6% 0
Anemia 16% 4% 1% 11% 5% 1%
Hypophosphatemia 10% 8% 1% 2% 2% 0
Lipase increased 7% 5% 2% 3% 2% 0
Case Study: Mr. DS
▶ 54-year-old man with advanced HCC in the
setting of chronic HCV
▶ Started on sorafenib 6 weeks ago
▶ After several dose reductions, his
desquamating rash has not improved. Also has
difficult-to-control diarrhea and fatigue
▶ Has decided that he cannot continue on
sorafenib
▶ Not interested in clinical trials

Case Study: Mr. DS (cont.)
▶ Pop Quiz

Case Study: Mr. DS (cont.)
▶ What treatment would you recommend for this
patient?
a. FOLFOX
b. Liposomal doxorubicin
c. Lenvatinib
d. Regorafenib
Case Study: Mr. DS (cont.)
▶ What treatment would you recommend for this
patient?
a. FOLFOX
b. Liposomal doxorubicin
c. Lenvatinib
d. Regorafenib

Lenvatinib: A New Option in HCC
▶ Oral, multitargeted inhibitor of:◼ VEGF receptors VEGFR1 (FLT1), VEGFR2 (KDR), and
VEGFR3 (FLT4)
◼ FGFR1, 2, 3, and 4
◼ PDGFRα, KIT, and RET
▶ Approved for recurrent or metastatic iodine-refractory
thyroid cancer and in renal cell carcinoma in
combination with everolimus following prior
antiangiogenic therapy
Lenvima® prescribing information, 2017.

REFLECT Phase III: Lenvatinib vs
Sorafenib as First-Line Therapy
NI = noninferiority; PFS = progression-free survival.
Cheng et al, 2017.
Sorafenib
400 mg twice daily
(n=476)
Eligibility▶ Unresectable HCC with no
prior treatment
▶ ECOG PS 0 or 1
▶ BCLC stage B or C
▶ Child-Pugh A
▶ Age ≥18 years
Lenvatinib 8 or 12 mg
daily based on body
weight; 8 mg for <60 kg
(n=478)
954 pts randomly assigned
1:1 to detect NI in OS
R
A
N
D
O
M
I
Z
E
Study Design▶ Open-label, randomized NI
study▶ Primary end point: OS▶ Secondary end points:
PFS, TTP

REFLECT: Outcomes
ORR = overall response rate.
Cheng et al, 2017.
Outcomes Lenvatinib Sorafenib HR
Median OS, mo
(95% CI)13.6 (12.1-14.9) 12.3 (10.4-13.9) 0.92 (0.79-1.06)
Median PFS, mo
(95% CI)7.4 (6.9-8.8) 3.7 (3.6-4.6) 0.66 (0.57-0.77)
Median TTP, mo
(95% CI)8.9 (7.4-9.2) 3.7 (3.6-5.4) 0.63 (0.53-0.73)
ORR, n (%) 115 (24%) 44 (9%)

REFLECT: Treatment-Emergent AEs
▶ Grade 3 and higher events were more common in the
lenvatinib arm (57% vs 49%)
▶ Most common AEs in the lenvatinib arm:◼ Hypertension (42% overall with 23% grade ≥3)
◼ Diarrhea (39%)
◼ Decreased appetite (34%)
◼ Weight loss (31% with 8% grade ≥3)
◼ Fatigue (30%)
▶ Grade 3 HFSR was more common in the sorafenib arm
(11% vs 3%)
Cheng et al, 2017.

Ramucirumab
▶ Anti-VEGFR2 monoclonal antibody approved for the
treatment of gastric and colon cancers
▶ In the REACH trial, patients were randomly assigned to
ramucirumab vs placebo after progression on sorafenib◼ Although the primary end point of OS was not met,
a prespecified population of patients with baseline
AFP ≥400 ng/mL and Child-Pugh scores of 5 or 6 demonstrated
a significant OS advantage vs placebo
Zhu et al, 2017.

REACH: OS in Child-Pugh 5/6 and
AFP ≥400 ng/mL
Zhu et al, 2017.

Key Takeaways
▶ Sorafenib and regorafenib are the only agents approved for
advanced HCC◼ Both are multikinase inhibitors with prominent antiangiogenic effects
◼ Sorafenib is approved for first-line treatment
◼ Regorafenib is approved for second-line treatment after sorafenib
failure or intolerance
▶ In a head-to-head phase III trial, lenvatinib was shown to be
noninferior to sorafenib and may be considered an alternative to
sorafenib, particularly in patients with intolerance
▶ Important to recognize the class-wide side effects of these agents
(eg, hand-foot skin reaction, hypertension, diarrhea, weight loss)
and employ timely interventions to optimize treatment outcomes
Questions?

How to Claim Credit
To claim your certificate of credit,
complete the evaluation at:
www.i3Health.com/HCC
References
Altekruse SF, McGlynn KA & Reichman ME (2009). Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from
1975 to 2005. J Clin Oncol, 27(9):1485-1491. DOI:10.1200/jco.2008.20.7753
American Cancer Society (2015). Global cancer facts & figures. 3rd edition. Available at: https://www.cancer.org/content/dam/cancer-
org/research/cancer-facts-and-statistics/global-cancer-facts-and-figures/global-cancer-facts-and-figures-3rd-edition.pdf
Bruix J, Qin S, Merle P, et al (2017). Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment
(RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol, 389(10064):56-66. DOI:10.1016/s0140-
6736(16)32453-9
Chen CJ, Yang HI, Su J, et al (2006). Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA,
395(1):65-73. DOI:10.1001/jama.295.1.65
Cheng A, Finn RS, Qin S, et al (2017). Phase III trial of lenvatinib (LEN) vs sorafenib (SOR) in first-line treatment of patients (pts) with
unresectable hepatocellular carcinoma (uHCC). J Clin Oncol (ASCO Annual Meeting Abstracts), 35(suppl). Abstract 4001.
Cheng AL, Kang YK, Chen Z, et al (2009). Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular
carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol, 10(1):25-34. DOI:10.1016/s1470-
2045(08)70285-7
D’Amico G, Garcia-Tsao G & Pagliaro L (2006). Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118
studies. J Hepatol, 44(1):217-231. DOI:10.1016/j.jhep.2005.10.013
Ghouri YA, Mian I & Rowe JH (2017). Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog, 16:1.
DOI:10.4103/jcar.Jcar_9_16
Jemal A, Bray F, Center MM, et al (2011). Global cancer statistics. CA Cancer J Clin, 61(2):69-90. DOI:10.3322/caac.20107
Kane RC, Farrell AT, Madabushi R, et al (2009). Sorafenib for the treatment of unresectable hepatocellular carcinoma. Oncologist, 14(1):95-
100. DOI:10.1634/theoncologist.2008-0185
Lacouture et al (2008). Evolving strategies for the management of hand–foot skin reaction associated with the multitargeted kinase inhibitors
sorafenib and sunitinib. Oncologist, 13(9):1001-1011. DOI:10.1634/theoncologist.2008-0131
Lenvima® (lenvatinib) prescribing information (2017). Eisai Inc. Available at: http://www.lenvima.com/pdfs/prescribing-information.pdf
Llovet JM, Brú C, Bruix J (1999). Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis, 19(3):329-38.
Llovet JM, Di Bisceglie AM, Bruix J, et al (2008a). Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst,
100(10):698-711. DOI:10.1093/jnci/djn134
.
References
Llovet JM, Ricci S, Mazzaferro V, et al (2008b). Sorafenib in advanced hepatocellular carcinoma. NEJM, 359:378-390.
DOI:10.1056/nejmoa0708857
Omland LH, Jepsen P, Krarup H, et al (2012). Liver cancer and non-Hodgkin lymphoma in hepatitis C virus-infected patients: results from the
DANVIR cohort study. Int J Cancer, 130(10):2310-2317. DOI:10.1002/ijc.26283
Pons-Renedo F & Llovet JM (2003). Hepatocellular carcinoma: a clinical update. MedGenMed, 5(3):11.
Ryerson AB, Eheman CR, Altekruse SF, et al (2016). Annual report to the nation on the status of cancer, 1975-2012, featuring the increasing
incidence of liver cancer. Cancer, 122(9):1312-1337. DOI:10.1002/cncr.29936
Scheithauer W & Blum J (2004). Coming to grips with hand-foot syndrome. Insights form clinical trials evaluating capecitabine. Oncology
(Williston Park), 18(9):1161-1168, discussion 1173-1176, 1181-1184.
Sherman M, Peltekian KM & Lee C (1995). Screening for hepatocellular carcinoma in chronic carries of hepatitis B virus: incidence and
prevalence of hepatocellular carcinoma in a North American urban population. Hepatology, 22(2):432-438.
Subramaniam S, Kelley RK & Venook AP (2013). A review of hepatocellular carcinoma (HCC) staging systems. Chin Clin Oncol, 2(4):33.
DOI:10.3978/j.issn.2304-3865.2013.07.05
Tornillo L, Carafa V, Sauter G, et al (2002). Chromosomal alterations in hepatocellular nodules by comparative genomic hybridization: high-
grade dysplastic nodules represent early stages of hepatocellular carcinoma. Lab Invest, 82(5):547:553.
Trojan J & Waidmann O (2016). Role of regorafenib as second-line therapy and landscape of investigational treatment options in advanced
hepatocellular carcinoma. J Hepatocell Carcinoma, 3:31-36. DOI:10.2147/JHC.S112537
van der Meer AJ, Veldt BJ, Feld JJ, et al (2012). Association between sustained virological response and all-cause mortality among patients
with chronic hepatitis C and advanced hepatic fibrosis. JAMA, 308(24):2584-2593. DOI:10.1001/jama.2012.144878
Verslype C, De Keyzer F, Libbrecht L, et al (2007). Diffusion-weighted MRI for detection of hepatocellular carcinoma in patients with hepatic
cirrhosis: a correlation to histology and imaging follow-up. The 58th Annual Meeting of the American Association for the Study of Liver
Diseases. Abstract 24.
Welzel TM, Graubard BI, Zeuzem S, et al (2011). Metabolic syndrome increases the risk of primary liver cancer in the United States: a study in
the SEER-Medicare database. Hepatology, 54(2):463-471. DOI:10.1002/hep.24397
Wilhelm SM, Adnane L, Newell P, et al (2008). Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and
PDGF receptor tyrosine kinase signaling. Mol Cancer Ther, 7(10):3129-3140. DOI:10.1158/1535-7163.mct-08-0013
Zhu AX, Baron AD, Malfertheiner P, et al (2017). Ramucirumab as second-line treatment in patients with advanced hepatocellular carcinoma.
Analysis of REACH Trial results by Child-Pugh score. JAMA, 3(2):235-243. DOI:10.1001/jamaoncol.2016.4115