scholarly project june 07072013
TRANSCRIPT

Implementation of a Screening Tool to Determine Eligibility for Thrombolytic
Therapy for Acute Ischemic Stroke Management in the Emergency Department
Darene Hall MSN, CCRN, GNP-BC, DNP (c)Scholarly Project
Stroke Program Manager•Adult/Geriatric NP
•Neurovascular
•Critical Care
•Mother
•Wife
•Grandmother of 3
Committee Members• Faculty Chair:
Kathleen A. Ennen PhD, RN, CNE• Has over 42 years of nursing experience which includes
work in cardiovascular intensive care units, teaching, and research in area of stroke recognition and prevention
• Clinical Mentor: Anne W. Alexandrov PhD, RN, CCRN, FAAN• Asst. Dean, DNP Program Director, and Professor at
University Alabama. Neurovascular Management Professor & NET SMART (Neurovascular Education and Training in Stroke Acute Reperfusion Therapy) Program Director. Health Outcomes Institute
What is your Stroke Risk Score?
Introduction and Background
• Stroke is the fourth leading cause of death in the U.S.
• Leading cause of long-term adult disability
• One of the leading hospital admitting diagnosis
(American Heart Association, 2013)
Global Significance
• 795, 000 people in the United States (U.S.) had a new or recurrent stroke
• Stroke killed more than 137,000 people a year
• 2010 - Americans paid about $74 billion in stroke-related medical costs and disability
(American Heart Association, 2013)
Institute of Medicine Summary Report
TO ERR IS HUMAN CROSSING THE QUALITY CHASM
ENVISIONING A NATIONAL HEALTH
CARE QUALITY REPORT
LEADERSHIP BY EXAMPLE
PRIORITY AREAS FOR NATIONAL
ACTION
http://www.acmq.org/education/iomsummary.pdf
Foreground: Local Significance• Heart disease and stroke are
first and third leading cause of death and disabilities
• 2004 -Heart disease and stroke killed over 73,000 Californians
• 2006 – the reported annual cost exceeded $48 billion
(California Heart Disease and Stroke Prevention and Treatment Task Force, 2007)
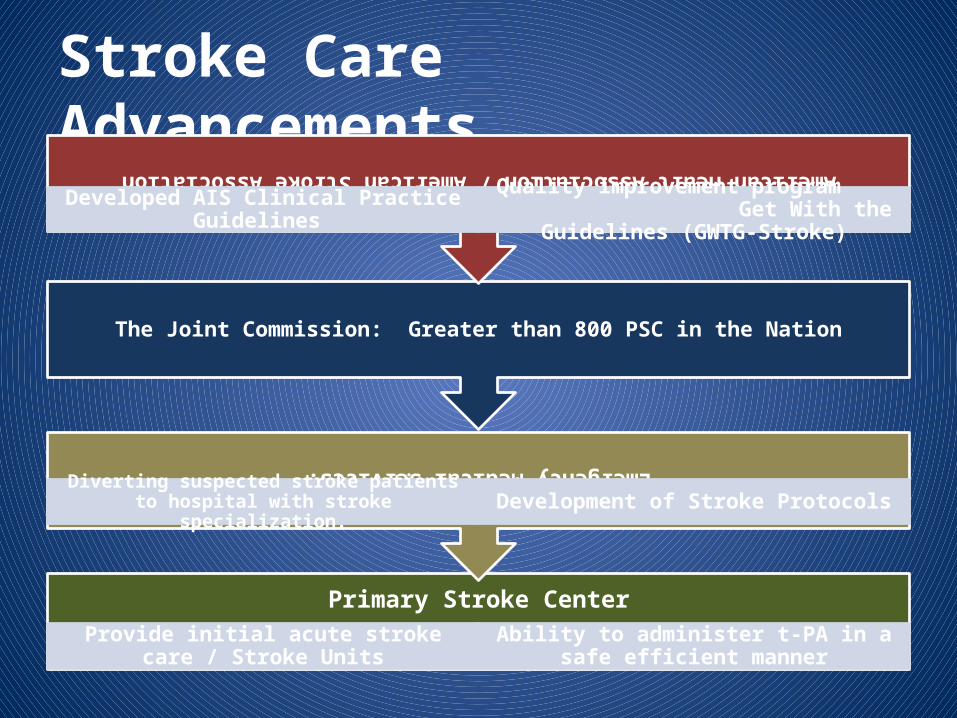
Stroke Care Advancements
Primary Stroke Center
Provide initial acute stroke care / Stroke Units Ability to administer t-PA in a safe efficient manner
Emergency Medical Services:
Diverting suspected stroke patients to hospital with stroke specialization. Development of Stroke Protocols
The Joint Commission: Greater than 800 PSC in the Nation
American Heart Association / American Stroke Association
Developed AIS Clinical Practice Guidelines Quality improvement program Get With the Guidelines (GWTG-Stroke)
Stroke Care Advancements Continues
Tissue-Type Plasminogen Activator (t-PA)
Proven intervention for acute ischemic
stroke
Class 1, evidence-based
recommendation for the AHA/ASA
The benefits of intravenous t-PA in acute ischemic stroke is strongly time-dependent
Studies have shown, greater
neurological improvement at
90 days with early t-PA treatment
Fonarow et al. (2011b)
Problem• Despite proven benefits, CPG,
explicit goals for timely administration of t-PA
• Recent evidence: GWTG-Stroke– National U.S. registry database
and other studies
• Only one-third of AIS patients treated within recommended door-to-needle time guideline
(Fonarow et al., 2011b)
Proposed Change
•In emergency department providers (MD, NP, PA, RNs)P
•How does integrating the National Institute of Neurological Disorders and Stroke (NINDS) screening tool in the initial evaluation and treatment for acute stroke patients
I•Compared to no NINDS screening tool used for acute
stroke patientsC
•Improve sixty-minute door-to-needle thrombolytic treatment ratesO
•Over a three month timeframeT
Purpose and Scope of Proposed Change•To evaluate effectiveness of the NINDS thrombolytic screening tool on 60 minute TTRs
•Elevate clinicians’ performance in acute stroke management
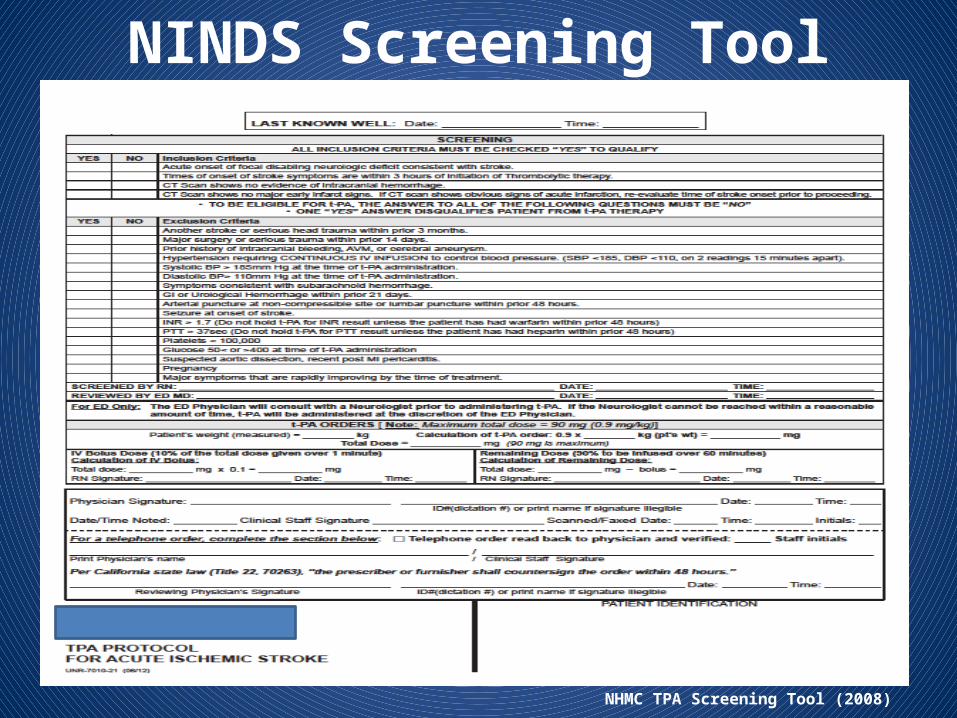
NINDS Screening Tool
NHMC TPA Screening Tool (2008)
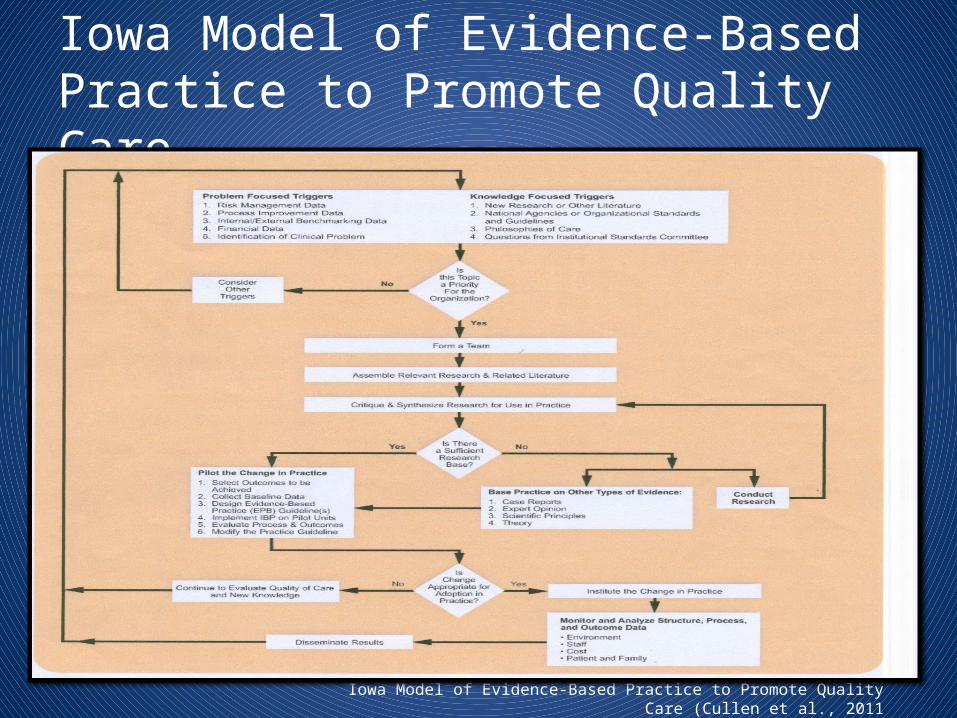
Iowa Model of Evidence-Based Practice to Promote Quality Care
Iowa Model of Evidence-Based Practice to Promote Quality Care (Cullen et al., 2011
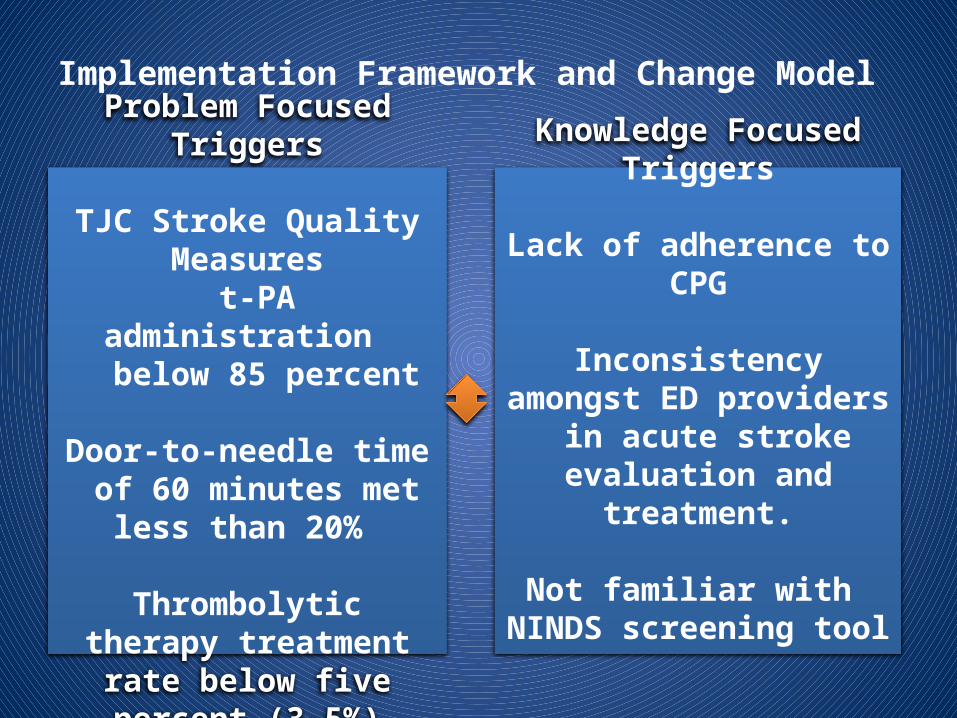
Implementation Framework and Change Model
Problem Focused Triggers
TJC Stroke Quality Measures t-PA administration
below 85 percent
Door-to-needle time of 60 minutes met less than 20%
Thrombolytic therapy treatment rate below five
percent (3-5%)
Knowledge Focused Triggers
Lack of adherence to CPG
Inconsistency amongst ED providers in acute stroke evaluation and treatment.
Not familiar with NINDS screening tool
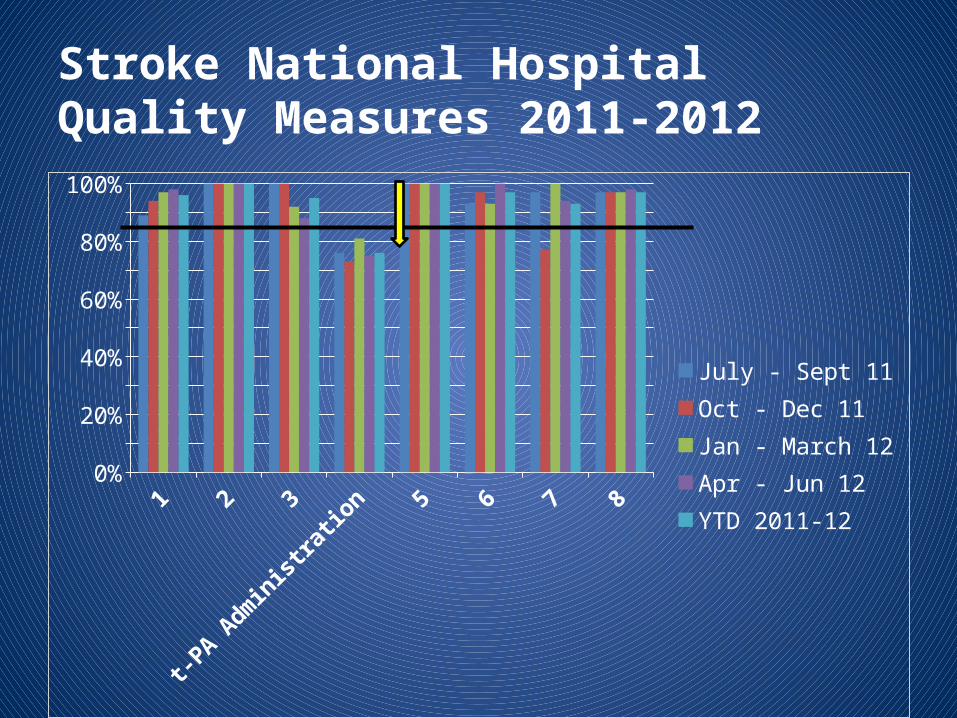
Stroke National Hospital Quality Measures 2011-2012
1 2 3
t-PA Administ
ration 5 6 7 80%
10%20%30%40%50%60%70%80%90%
100%
July - Sept 11Oct - Dec 11Jan - March 12Apr - Jun 12YTD 2011-12
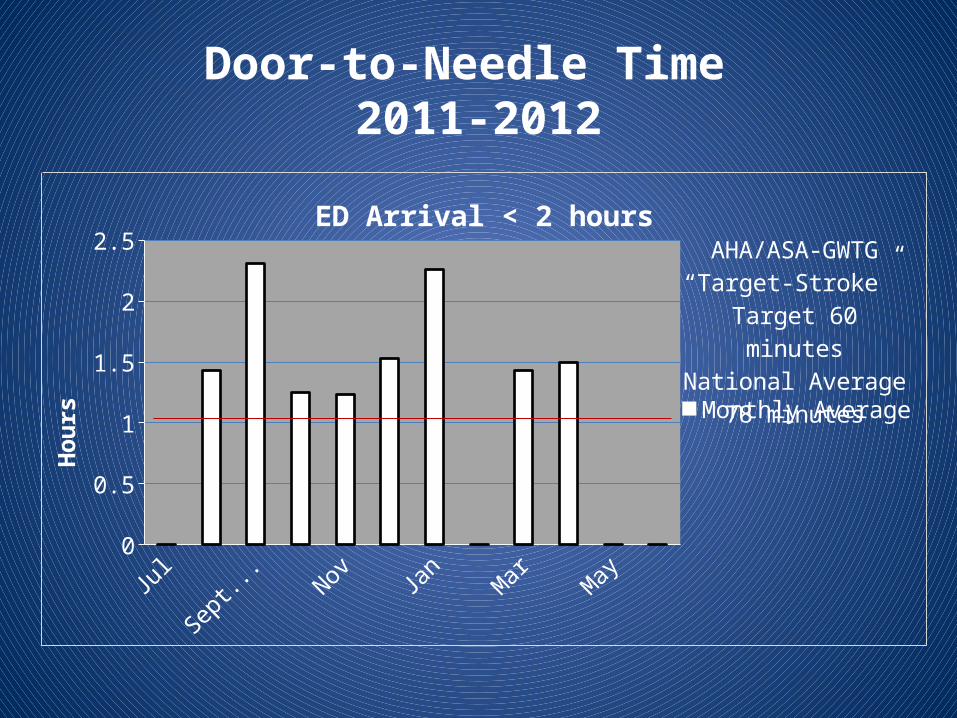
Door-to-Needle Time 2011-2012
July,11
Aug, 11
Sept, 1
1
Oct, 11
Nov, 11
Dec, 11
Jan, 1
2
Feb, 1
2
Mar, 12
Apr, 12
May, 1
2
Jun, 12
0
0.5
1
1.5
2
2.5ED Arrival < 2 hours
Monthly Average
Hour
s
AHA/ASA-GWTG“Target-Stroke”
Target 60 minutesNational Average
78 minutes
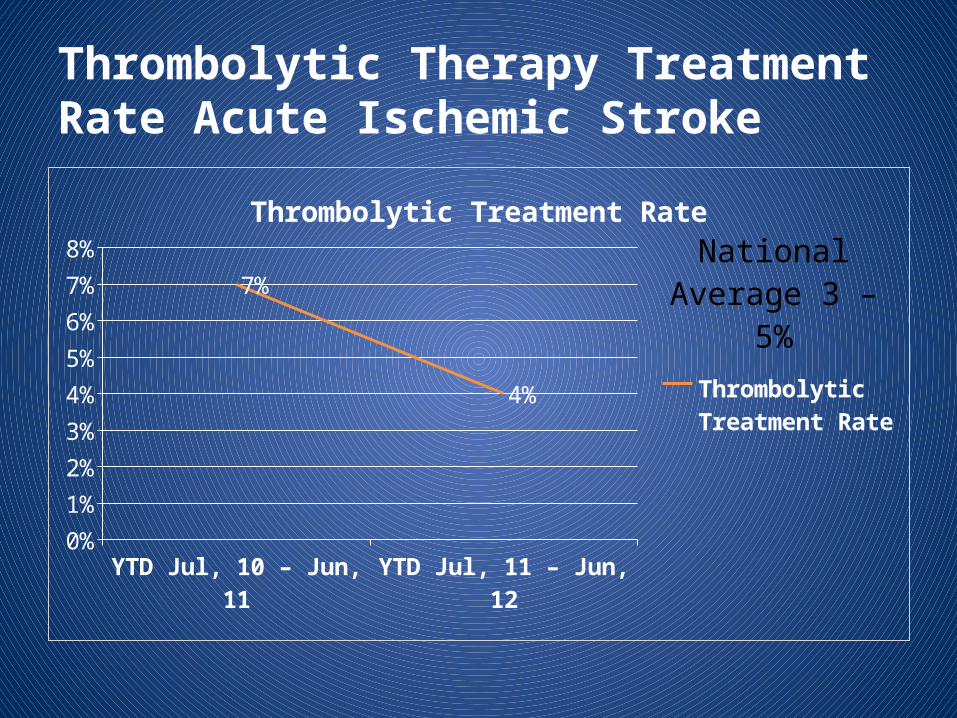
Thrombolytic Therapy Treatment Rate Acute Ischemic Stroke
YTD Jul, 10 – Jun, 11 YTD Jul, 11 – Jun, 120%
1%
2%
3%
4%
5%
6%
7%
8%
7%
4%
Thrombolytic Treatment Rate
Thrombolytic Treatment Rate
National Aver-age 3 – 5%
EBP Implementation Framework
Is this Topic a Priority
For the Organization?
Yes
Stroke Core Quality Performance Measures
•Nationally reported
•Required to maintain Stroke Center designation status
•Reported to CMS (reimbursements tied to quality measures in the near future)
•ASA proposed 60 minute DTN as a new core measure (reimbursement tied to quality)
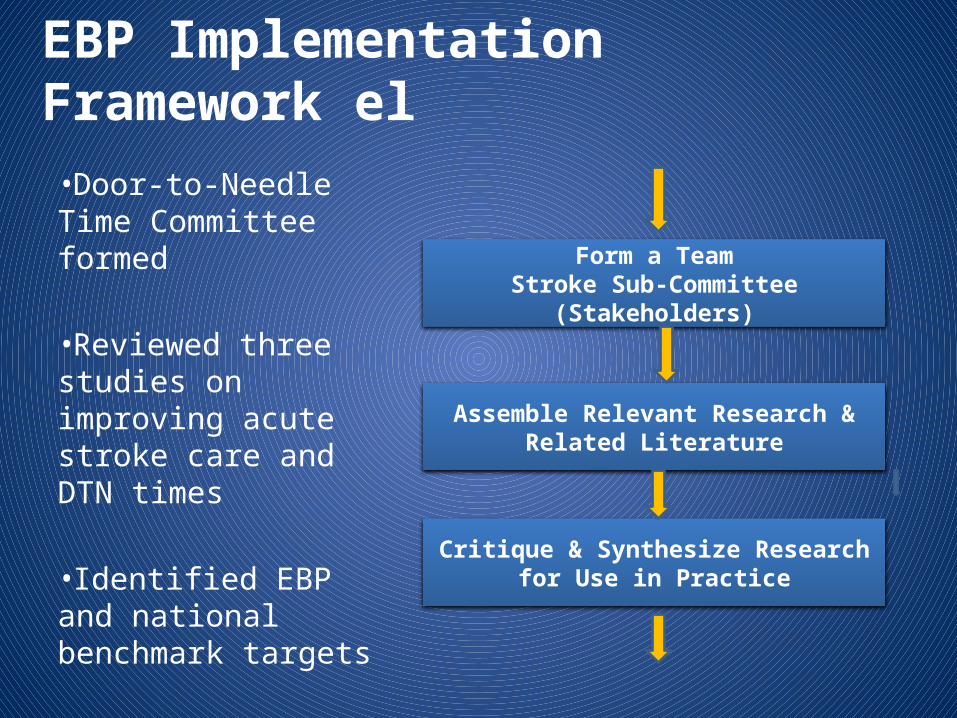
EBP Implementation Framework el•Door-to-Needle Time Committee formed
•Reviewed three studies on improving acute stroke care and DTN times
•Identified EBP and national benchmark targets
Form a TeamStroke Sub-Committee (Stakeholders)
Assemble Relevant Research & Related Literature
Critique & Synthesize Research for Use in Practice
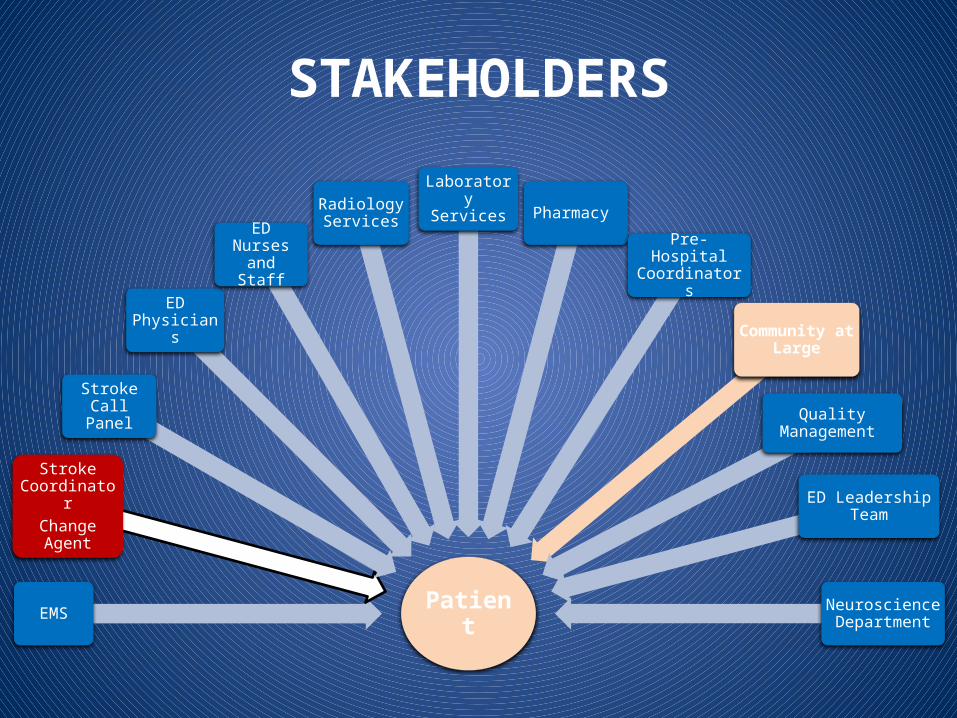
STAKEHOLDERS
PatientEMS
Stroke Coordinator
Change Agent
Stroke Call Panel
ED Physicians
ED Nurses and Staff
Radiology Services
Laboratory Services Pharmacy
Pre-Hospital Coordinators
Community at Large
Quality Management
ED Leadership Team
Neuroscience Department
NHMC Stroke-subcommittee, 2012
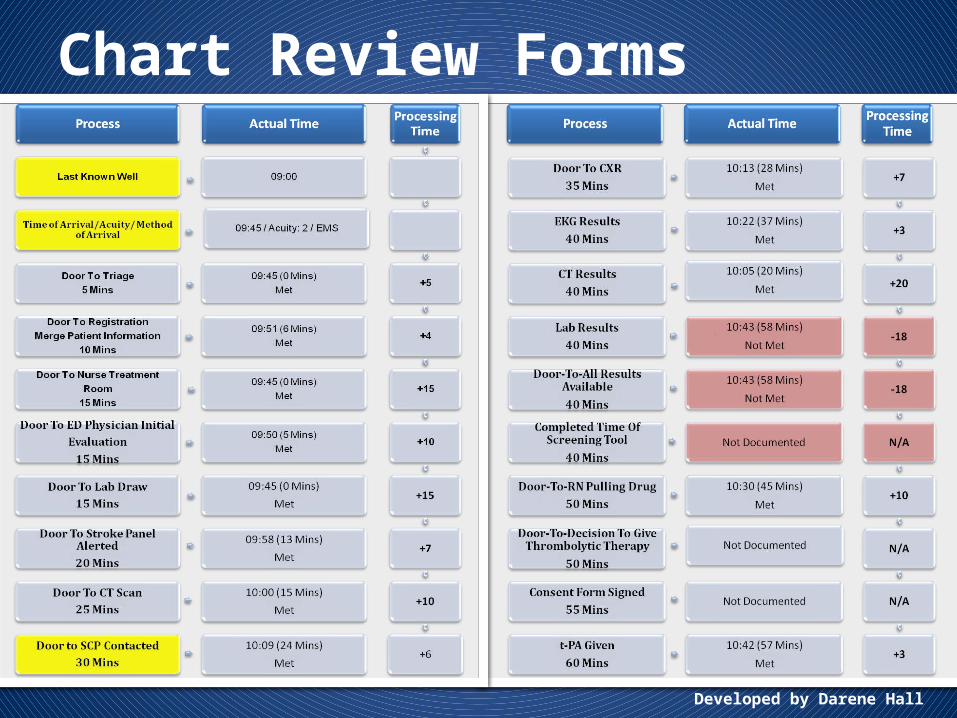
Chart Review Forms
Developed by Darene Hall
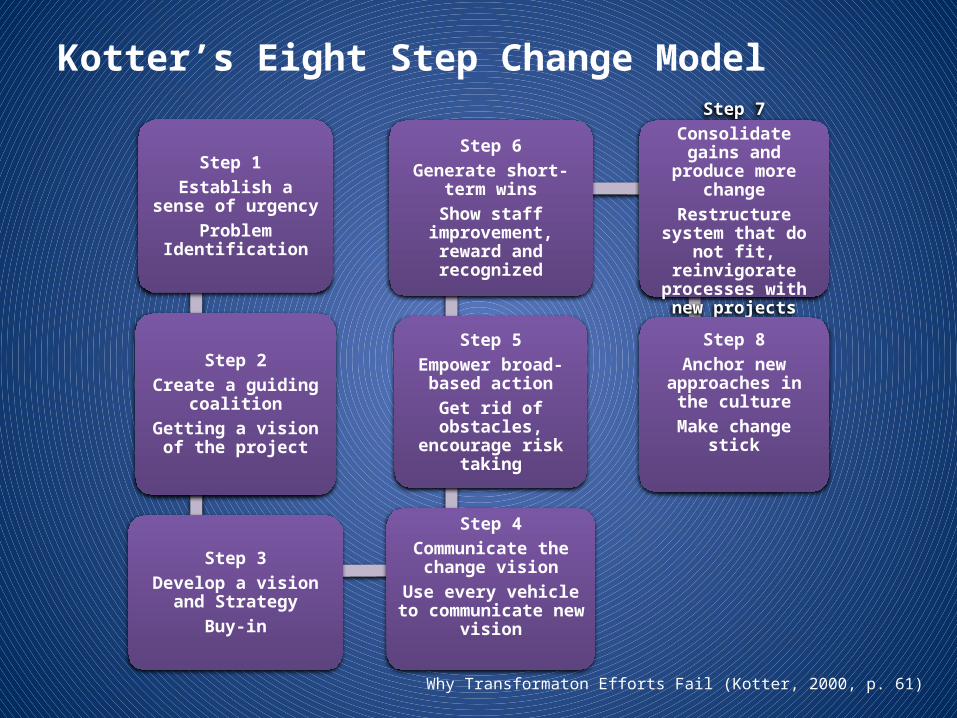
Kotter’s Eight Step Change Model
Step 1 Establish a sense of
urgencyProblem Identification
Step 2Create a guiding
coalitionGetting a vision of the
project
Step 3Develop a vision and
StrategyBuy-in
Step 4Communicate the change
visionUse every vehicle to
communicate new vision
Step 5Empower broad-based
actionGet rid of obstacles,
encourage risk taking
Step 6Generate short-term
winsShow staff improvement,
reward and recognized
Step 7Consolidate gains and produce more change
Restructure system that do not fit, reinvigorate
processes with new projects
Step 8Anchor new
approaches in the culture
Make change stick
Why Transformaton Efforts Fail (Kotter, 2000, p. 61)
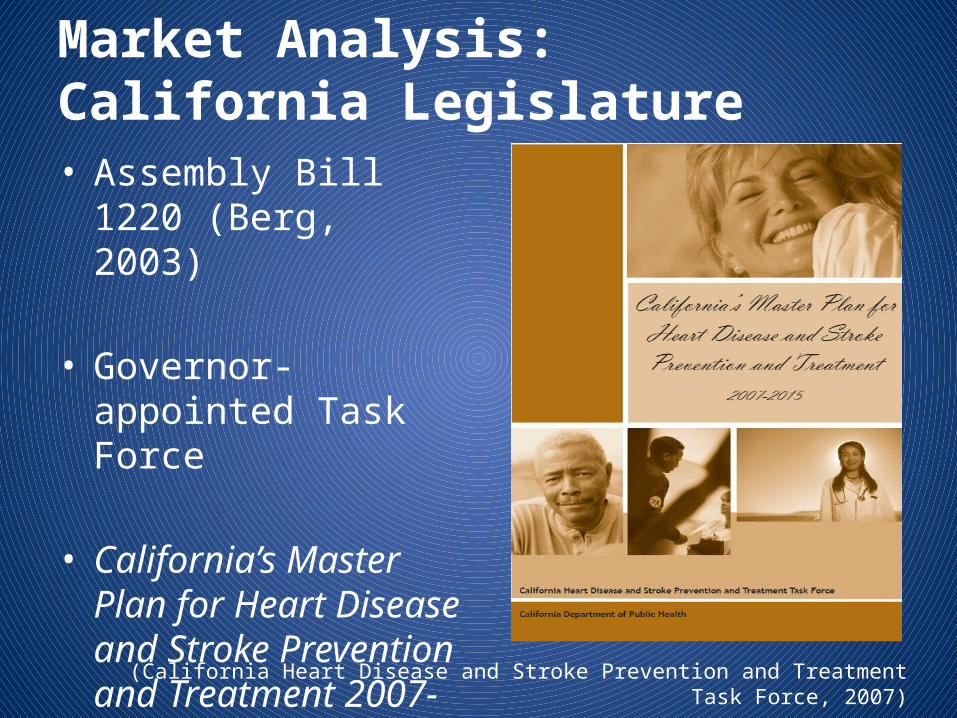
Market Analysis: California Legislature• Assembly Bill 1220
(Berg, 2003)
• Governor-appointed Task Force
• California’s Master Plan for Heart Disease and Stroke Prevention and Treatment 2007-2015
(California Heart Disease and Stroke Prevention and Treatment Task Force, 2007)
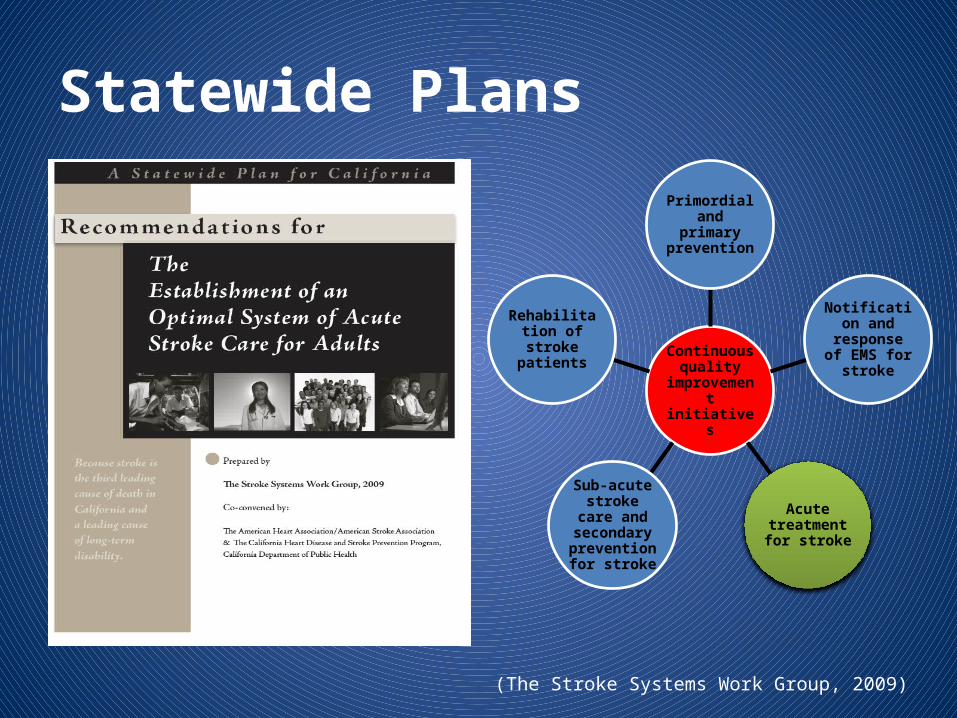
Statewide Plans
Continuous quality
improvement initiatives
Primordial and primary prevention
Notification and response
of EMS for stroke
Acute treatment for
stroke
Sub-acute stroke care
and secondary prevention for
stroke
Rehabilitation of stroke patients
(The Stroke Systems Work Group, 2009)
Risk and Barriers• Efficiency in acute ischemic stroke management
• Lack of stroke symptom recognition
• Failure to seek urgent help
• Non-urgent triage of stroke patients EMS and ED Staff
• Delayed CT scans
• Inefficiency in-hospital emergency processes of stroke care
(Carter-Jones, 2010)
Risk and Barriers• ED nurses insufficient level of comfort in
assessing acute stroke patient
• Infrequent feedback regarding nurses performance and patient outcome
• Environmental issues – Staffing– Competing priorities– Patient and family needs
Johnson, Cohn, and Bakas (2011)
Kotter’s eight step model: Step-Five
Empower based –action (get rid of obstacles and encourage risk
taking
Literature Review• Alberts et al. (2000) reported Primary Stroke
Centers improve care of patients with stroke (Level I, Grade A)
• Fonarow et al. (2011) reported 60 minutes DTN times were achieved in less than 26.2% of acute ischemic patients (Level III, Grade B)
Literature Review• Jauch et al. (2013) reported hospital should
have an organized protocol for emergency evaluation of patient with suspected strokeMeta-analysis (Level I, Grade A)
• Fonarow et al. (2011) reported t-PA is a proven intervention for AIS patients, Class 1 evidence-based recommendation from the AHA/ASA (Level III, Grade B)
Literature Review• Adams et al. (2007) reported ED physicians
evaluation of acute stroke patients should be brief and thorough within 60 minutes of arrival in the ED Meta-Analysis (Level 1, Grade A)
• Adams et al. (2007) also reported physicians should review the criteria used in the NINDS trial to determine patient eligibility for thrombolytic therapy Meta-Analysis (Level 1, Grade A)
Literature Review• Fonarow et al (2011) reported time-to-treatment
with t-PA is a good determinant of patient 90-day and 1-year functional outcome (Level III, Grade B)
• Jauch et al. (2013) reported healthcare institution should organize a multidisciplinary QI committee to review and monitor stroke care quality benchmarks, indicators, EBPs, and outcome Meta- Analysis (Level 1, Grade A)
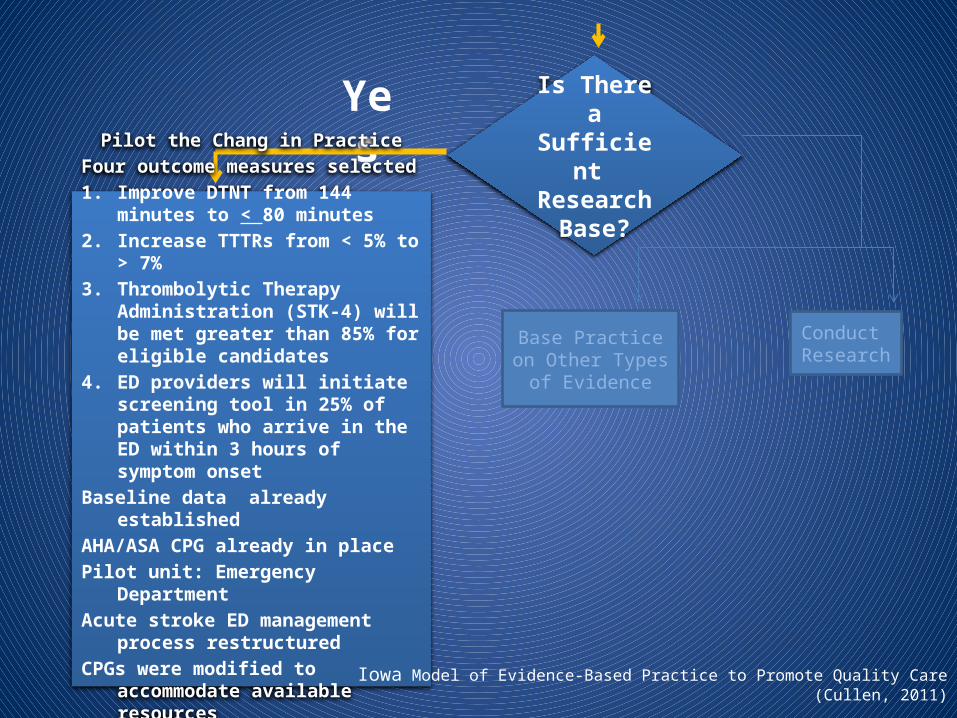
Is There a Sufficient Research
Base?
Base Practice on Other Types of
Evidence
Conduct Research
Yes
Pilot the Chang in PracticeFour outcome measures selected1. Improve DTNT from 144 minutes to <
80 minutes2. Increase TTTRs from < 5% to > 7%3. Thrombolytic Therapy Administration
(STK-4) will be met greater than 85% for eligible candidates
4. ED providers will initiate screening tool in 25% of patients who arrive in the ED within 3 hours of symptom onset
Baseline data already establishedAHA/ASA CPG already in placePilot unit: Emergency DepartmentAcute stroke ED management process
restructuredCPGs were modified to accommodate
available resources
Iowa Model of Evidence-Based Practice to Promote Quality Care (Cullen, 2011)
Methods• System change project (divided in 2 phases)
1. Organizational paradigm shift to an EBP model2. Broader investigation of the effectiveness of the
NINDS screening to on 60-minute TTRs
• National Institute of Health Certification completed March 18, 2012
• CITI Basic Course completed September 16, 2013 (required by Dignity Health Corporation)
Methods• Northridge Hospital Medical Center IRB
approval letter January 27, 2013
• RMUoHP IRB approval letter January 29, 2013
• ED providers trained on the use of the NINDS screening tool – December 2012 /January 2013
Methods• Collaboration:
– Stroke sub-committee of stakeholders– ED staff involved with planning and implementation – (“Go Live” February 1, 2013)– Completion of project: April 30, 2013
• Data abstracted concurrently from patient’s charts – MedHost® (ED EMR)– Nurses and physician notes– Stroke Program had an established QI program
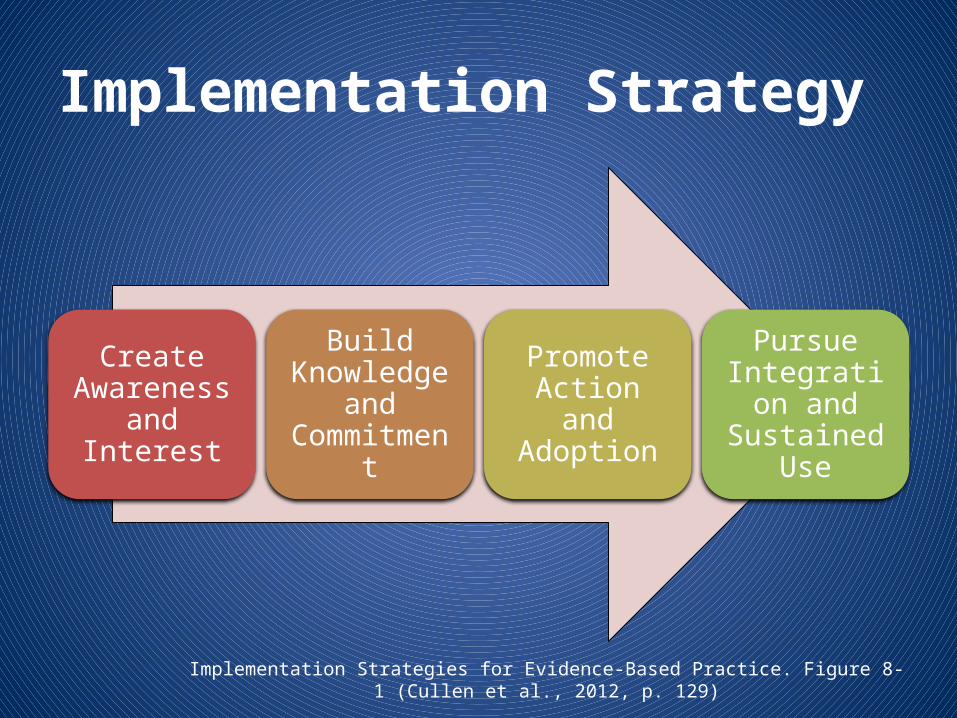
Implementation Strategy
Create Awareness
and Interest
Build Knowledge
and Commitment
Promote Action and Adoption
Pursue Integration
and Sustained Use
Implementation Strategies for Evidence-Based Practice. Figure 8-1 (Cullen et al., 2012, p. 129)
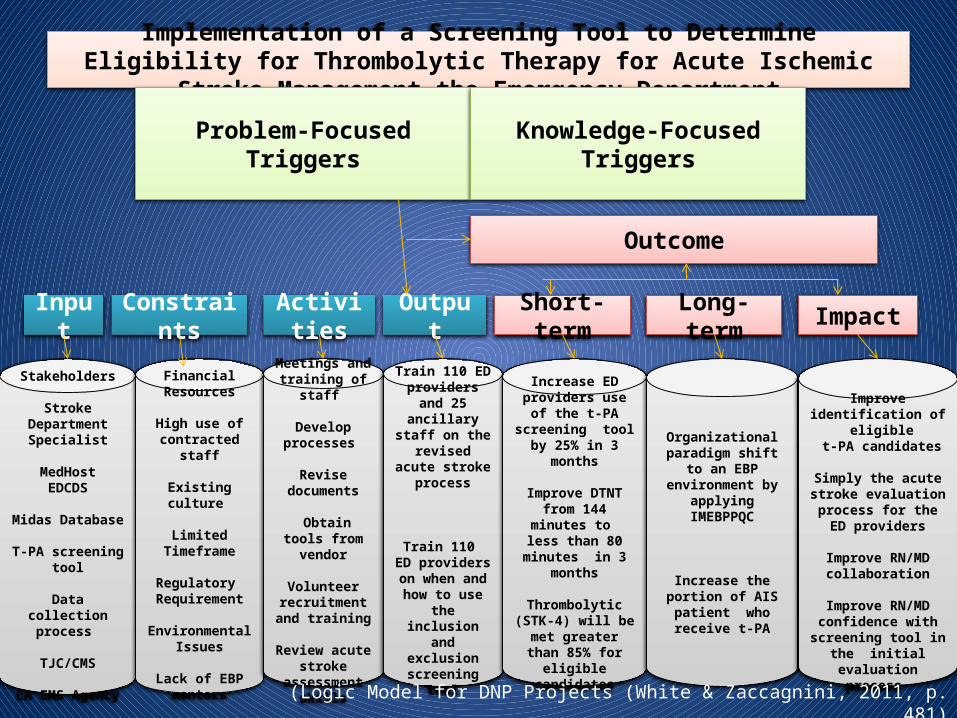
Implementation of a Screening Tool to Determine Eligibility for Thrombolytic Therapy for Acute Ischemic Stroke Management the Emergency Department
Problem-Focused Triggers Knowledge-Focused Triggers
Outcome
Input Constraints Activities Output Short-term Long-term Impact
Stakeholders
Stroke Department Specialist
MedHostEDCDS
Midas Database
T-PA screening tool
Data collection process
TJC/CMS
LA EMS Agency
Financial Resources
High use of contracted staff
Existing culture
Limited Timeframe
Regulatory Requirement
Environmental Issues
Lack of EBP mentors
Meetings and training of staff
Develop processes
Revise documents
Obtain tools from vendor
Volunteer recruitment and
training
Review acute stroke assessment
skills
Train 110 ED providers and 25 ancillary staff on the revised acute
stroke process
Train 110 ED providers on
when and how to use the inclusion
and exclusion screening tool
Increase ED providers use of the t-PA
screening tool by 25% in 3 months
Improve DTNT from 144 minutes to less
than 80 minutes in 3 months
Thrombolytic (STK-4) will be met greater
than 85% for eligible candidates
Organizational paradigm shift to an EBP environment by applying IMEBPPQC
Increase the portion of AIS patient who
receive t-PA
Improve identification of eligible
t-PA candidates
Simply the acute stroke evaluation process for
the ED providers
Improve RN/MD collaboration
Improve RN/MD confidence with
screening tool in the initial evaluation process
(Logic Model for DNP Projects (White & Zaccagnini, 2011, p. 481)
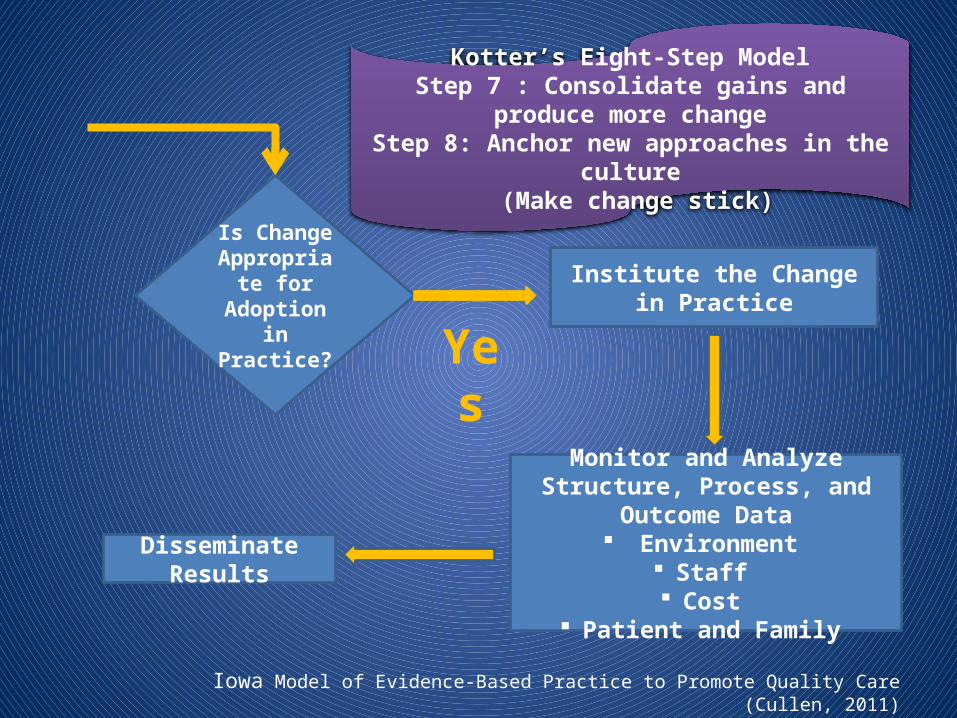
Is Change Appropriate for Adoption in Practice?
Institute the Change in Practice
Monitor and Analyze Structure, Process, and Outcome Data
Environment Staff Cost
Patient and Family
Disseminate Results
Iowa Model of Evidence-Based Practice to Promote Quality Care (Cullen, 2011)
Kotter’s Eight-Step ModelStep 7 : Consolidate gains and produce more change
Step 8: Anchor new approaches in the culture (Make change stick)
Yes
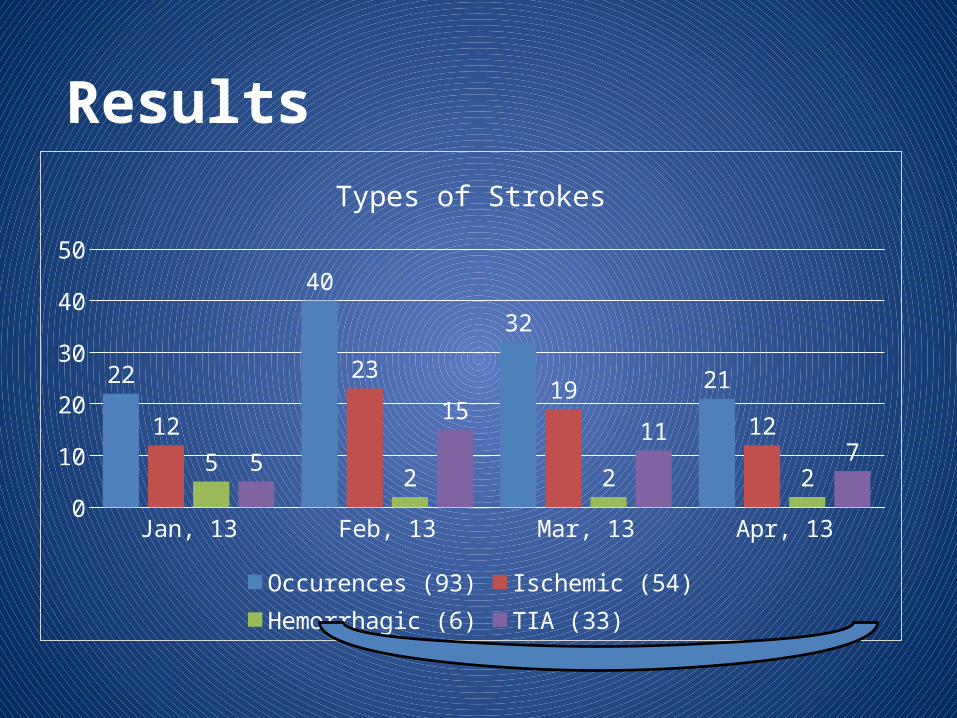
Results
Jan, 13 Feb, 13 Mar, 13 Apr, 1305
1015202530354045
22
40
32
21
12
2319
12
52 2 2
5
1511
7
Types of Strokes
Occurences (93) Ischemic (54) Hemorrhagic (6) TIA (33)
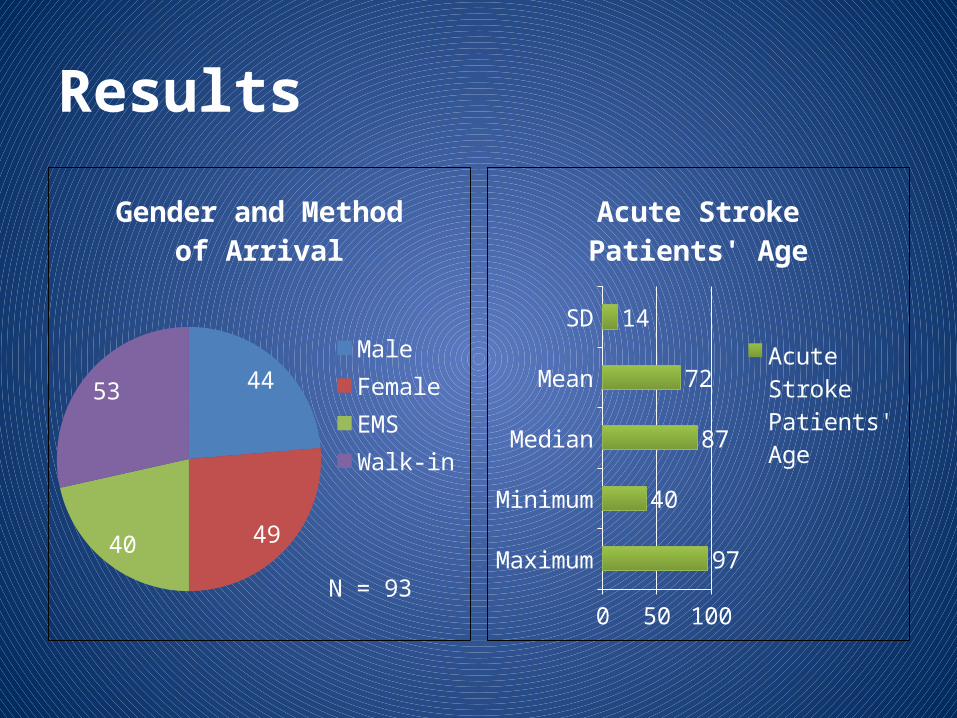
Results
44
4940
53
Gender and Method of Arrival
MaleFemaleEMSWalk-in
N = 93Maximum
Minimum
Median
Mean
SD
0 40 80
97
40
87
72
14
Acute Stroke Patients' Age
Acute Stroke Patients' Age
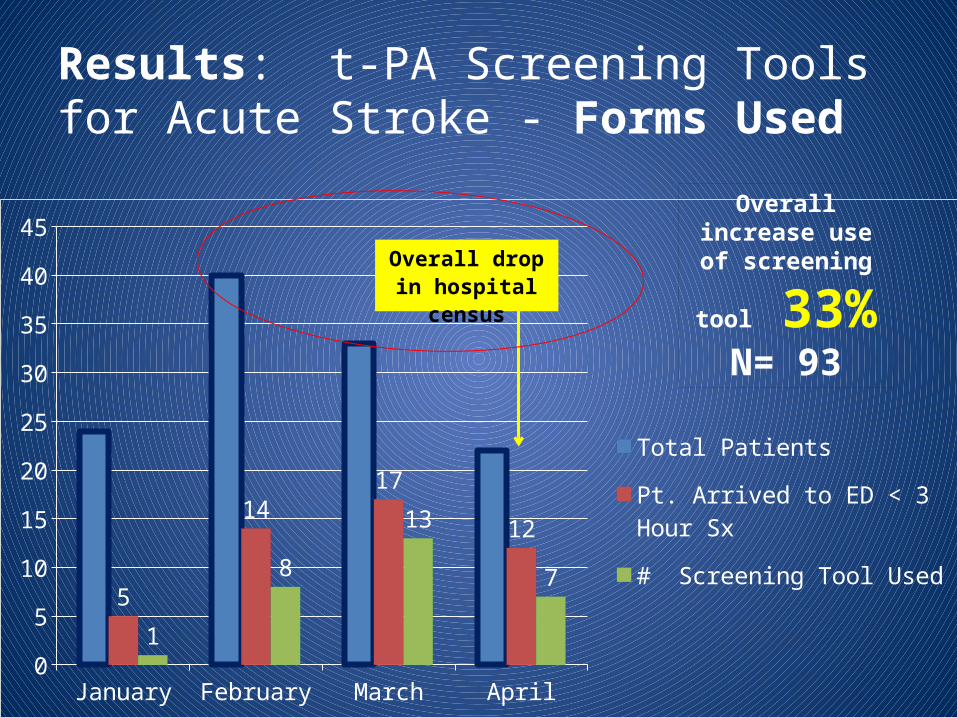
Results: t-PA Screening Tools for Acute Stroke - Forms Used
January February March April0
5
10
15
20
25
30
35
40
45
5
1417
12
1
8
13
7
Total Patients
Pt. Arrived to ED < 3 Hour Sx
# Screening Tool Used
Overall drop in hospital census
Overall increase use of screening
tool 33% N= 93
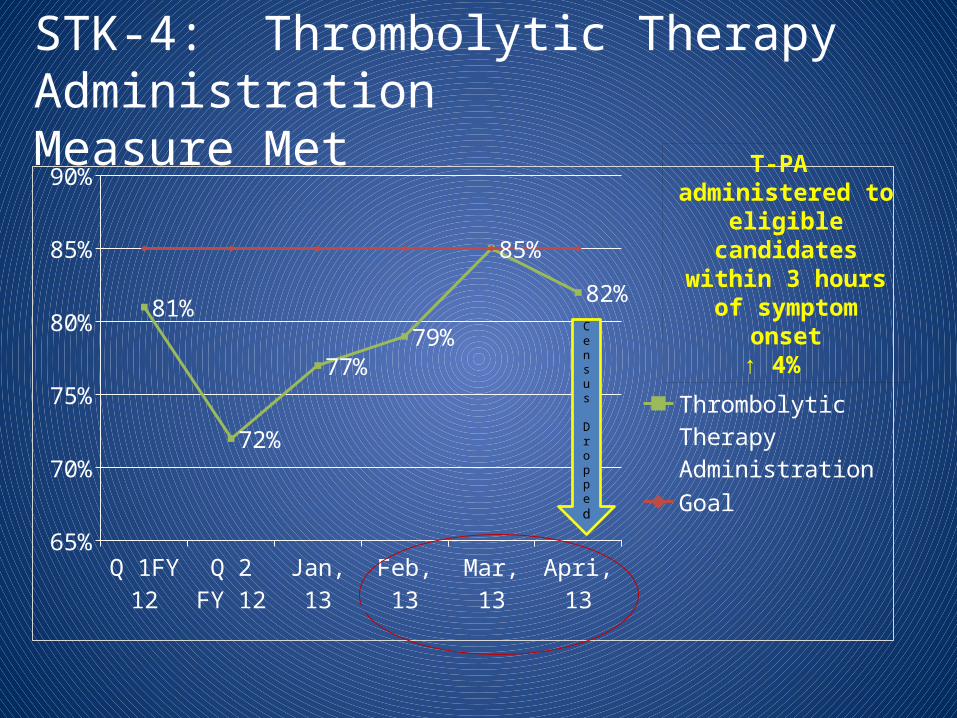
STK-4: Thrombolytic Therapy Administration Measure Met
Q 1FY 12
Q 2 FY 12
Jan, 13 Feb, 13 Mar, 13 Apri, 1365%
70%
75%
80%
85%
90%
81%
72%
77%79%
85%
82%
Thrombolytic Therapy Administration
Goal
T-PA administered to eligible candidates within 3 hours of symptom onset
↑ 4%
Census
Dropped
Results
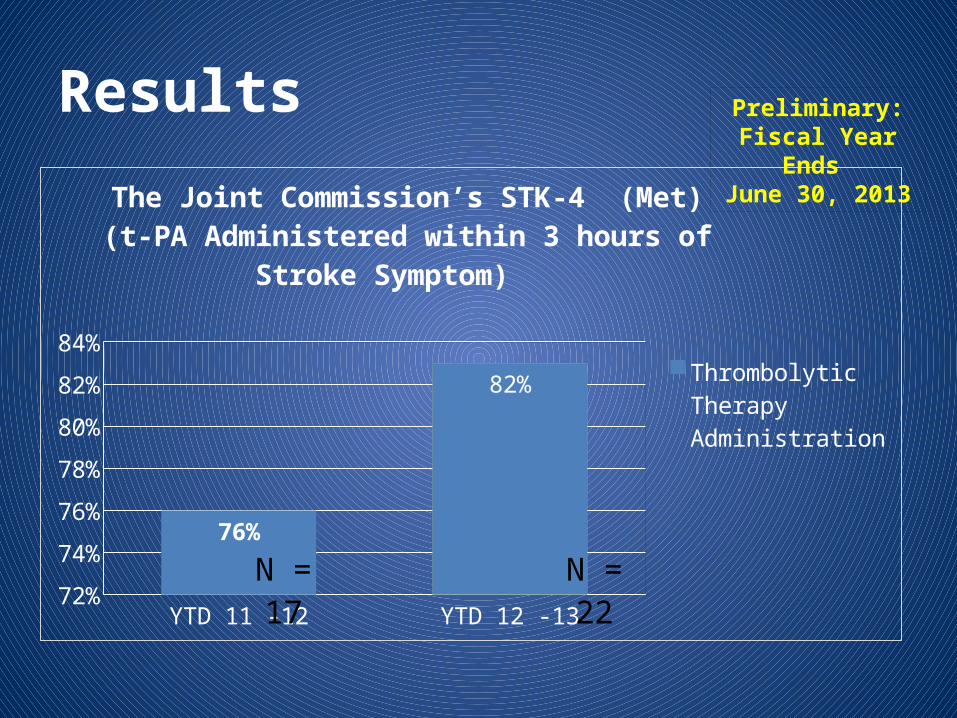
YTD 11 -12 YTD 12 -1372%
74%
76%
78%
80%
82%
84%
76%
82%
The Joint Commission’s STK-4 (Met)(t-PA Administered within 3 hours of Stroke Symptom)
Thrombolytic Therapy Administration
N = 22
N = 17
Preliminary: Fiscal Year Ends
June 30, 2013
Results
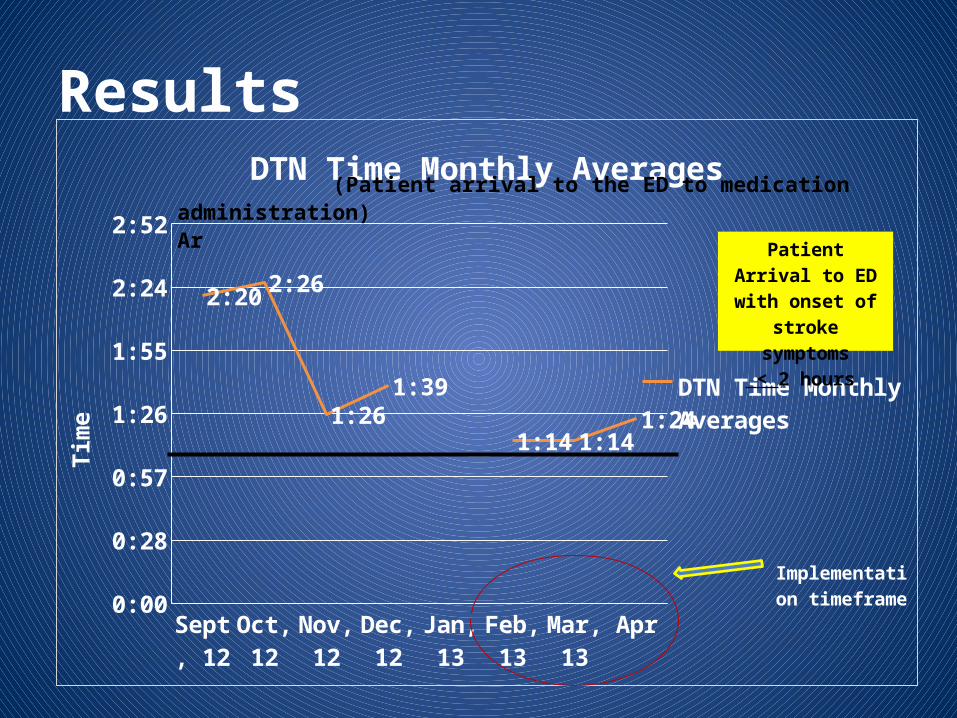
Sept, 12
Oct, 12
Nov, 12
Dec, 12
Jan, 13
Feb, 13
Mar, 13
April, 13
0:00
0:28
0:57
1:26
1:55
2:24
2:52
2:20 2:26
1:261:39
1:14 1:141:24
DTN Time Monthly Averages
DTN Time Monthly Av-erages
Tim
e
Implementation timeframe
(Patient arrival to the ED to medication administration)Ar
Patient Arrival to ED with onset of stroke symptoms
< 2 hours
Results
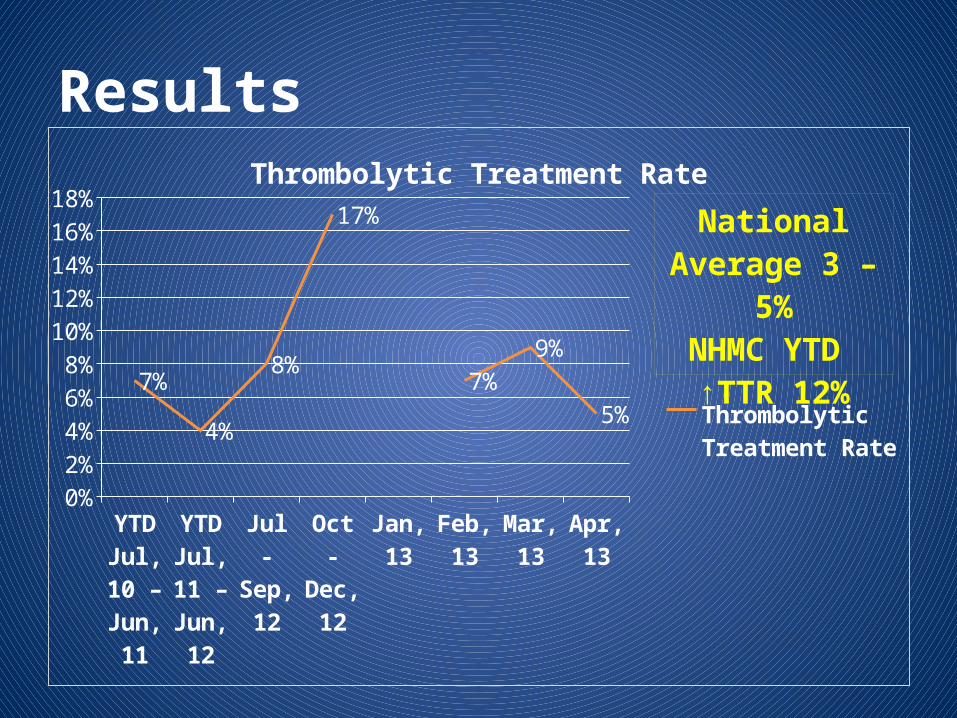
YTD Jul, 10 – Jun,
11
YTD Jul, 11 – Jun,
12
Jul - Sep, 12
Oct - Dec, 12
Jan, 13
Feb, 13
Mar, 13
Apr, 13
0%2%4%6%8%
10%12%14%16%18%
7%
4%
8%
17%
7%9%
5%
Thrombolytic Treatment Rate
Thrombolytic Treatment Rate
National Aver-age 3 – 5%
NHMC YTD ↑TTR 12%
Results
In emergency department providers, how does integrating the NINDS screening tool in the initial evaluation and treatment for acute
stroke patients compared to no NINDS screening tool used for acute stroke patients
improve 60-minute DTN TTRs over a three month timeframe?
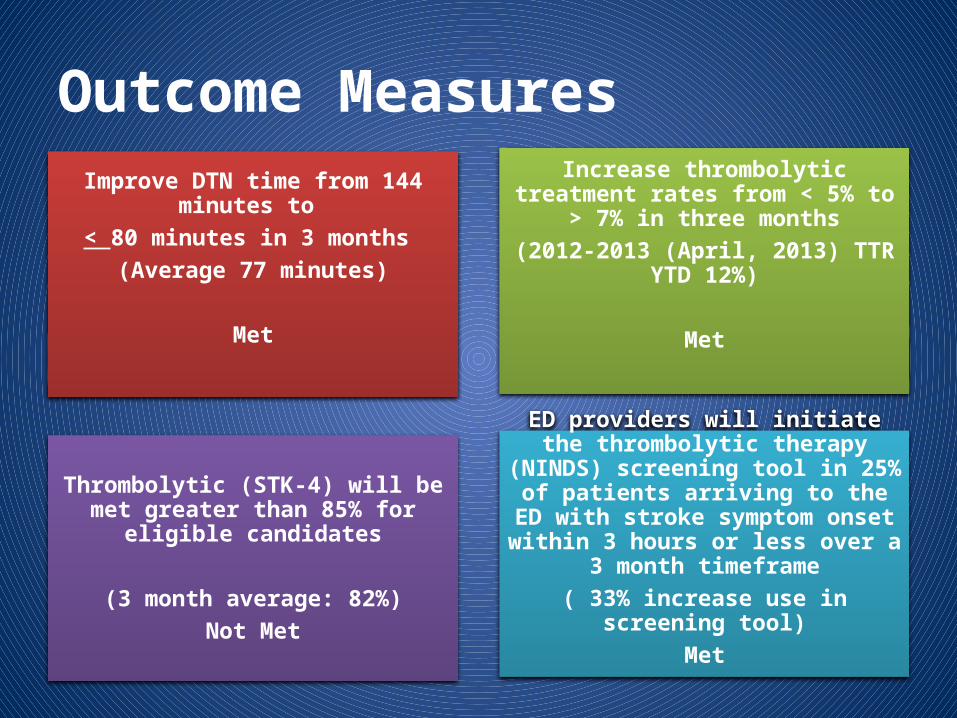
Outcome MeasuresImprove DTN time from 144 minutes to
< 80 minutes in 3 months (Average 77 minutes)
Met
Increase thrombolytic treatment rates from < 5% to > 7% in three months
(2012-2013 (April, 2013) TTR YTD 12%)
Met
Thrombolytic (STK-4) will be met greater than 85% for eligible candidates
(3 month average: 82%)Not Met
ED providers will initiate the thrombolytic therapy (NINDS) screening tool in 25% of
patients arriving to the ED with stroke symptom onset within 3 hours or less
over a 3 month timeframe( 33% increase use in screening tool)
Met
Conclusion
• Implementation of a complex evidence-based system change project in an environment with multiple internal barriers required:
– Heavy emphasis on relationship building
– Communication networks
– Well-coordinated interfaces between professionals and structures in the workplace
(Malloch and Porter-O'Grady, 2009)
Conclusion
• Project represented a collaborative multidimensional interdisciplinary EBP approach to improving acute stroke management process in a department
• Ideas and suggestion for future work– Need for more EBP mentors and educators– Streamline EMR documentation systems– Acute stroke data management system
Sustainability
• TJC stroke center designation status requires maintaining CQI program
• Continue DTN time meetings (identify further opportunities for improvements)
• Code Stroke Policy updates (in-patient) to include screening tool
• Phase II: Conduct Research on effectiveness of the NINDS tool on 60-minute DTN TTRs in patient with AIS (in process)
NHMC Core Stroke Team and Neuroscience Director
ReferenceAdams, E. A. (2007). Guidelines for the early management of adult with ischemic stroke. Stroke:
Journal of the American Heart Association, VOLUME , 38, 1655-1711. doi:10.1161/STROKEAHA.107.181486
Alberts, M. J., Latchaw, R. E., Jagoda, A., Wechsler, L. R., Crocco, T., George, M. G., & Walker, M. D. (2011). Revised and updated recommendations for the establishment of primary stroke centers. A summary statement from the Brain Attack Coalition. Stroke: Journal of the American Heart Association, VOLUME , 2651-2665. doi:10.1161/STROKE.AHA.111.615336
American Heart Association. (2013, May 20). American Heart Association. Retrieved from Heart and stroke association statistics : http://www.heart.org/HEARTORG/General/Heart-and-Stroke-Association-Statistics_UCM_319064_SubHomePage.jsp
California Assembly Bill No. 1220. (2013 1-2). Bill Documents. From California Stats. of 2003, Chapter 395: http://leginfo.ca.gov/cgi-bin/postquery?bill_number=ab_1220&sess=0304
ReferenceCalifornia Heart Disease and Stroke Prevention and Treatment Task Force. (2007). California’s
Master Plan for Heart Disease and Stroke 2007-2015. Sacramento, CA: California Department of Public Health.
Carter-Jones, C. R. (2010, February 19). Stroke thrombolysis: Barriers to implementation. International Emergency Nursing, VOLUME , 1-5. doi:10.1016/j.ienj.2010.02.005
Committee on Enhancing Federal Quality Healthcare Programs. (2002). Leadership by example: Coordinating government roles in improving health care quality (J. Corrigan & B. Smith, Eds.). Washington DC: National Academy Press. Retrieved from http://www.nap.edu/books/0309086183/html
Committee on Identifying Areas for Quality Improvement. (2003). Priority areas for national action: Transforming health care quality (K. Adams & J. Corrigan, Eds.). Washington DC: National Academy Press. Retrieved from http://books.nap.edu/books/0309085438/html/index.html
ReferenceCommittee on Quality of Health Care in America. (2001). Envisioning the national health care
quality report (J. Corrigan, M. Hurtado, & E. Swift, Eds.). Washington DC: National Academy Press. Retrieved from http://search.nap.edu/books/030907343X/index.html
Committee on Quality of Health Care in America: Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press. Retrieved from http:/books.nap.edu/books/0309068371/html/index.html
Cullen, L., Hanrahan, K., Tucker, S., Rempel, G., & Jordon, K. (2012). Evidence-based practice building block: Comprehensive strategies, tools, and tips (1st ed.). Iowa City, IA: Nursing Research and Evidence-Based Practice Department of Nursing Services and Patient Care, University of Iowa Hospitals and Clinics.
Fonarow, G. C., Smith, E. E., Saver, J. L., Reeves, M. J., Bhatt, D. L., Grau-Sepulveda, M. V., . . . Schwamm, L. H. (2011). Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: Patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation: Journal of the American Heart Association, VOLUME , 750-758. Retrieved from http://circ.ahajounals.org/content/early/2011/02/03/CIRCULATIONAHA.110.974675
ReferenceFonarow, G. C., Smith, E. E., Saver, J. L., Reeves, M. J., Hernandez, A. F., Peterson, E. D., . . .
Schwamm, L. H. (2011, September 1). Improving door-to-needle times in acute ischemic stroke. The design and rationale for the American Heart Association/American Stroke Association’s Target: Stroke initiative. Stroke: Journal of The American Heart Association, VOLUME , 2983. doi:10.1161/STROKEAHA.111.621342
Kotter, J. P. (2000, March-April). Leading Change: Why transformation efforts fail. Harvard Business Review, VOLUME , 59-67.
Malloch, K., & Porter-O’Grady, T. (2009). Making sense of transformation: Quantum realities in a new age. In K. Malloch & T. Porter-O’Grady (Eds.), The quantum leader: Applications for the new world of work (pp. 1-19). Sudbury, MA: Jones and Bartlett.
National Academy of Science. (1999, November 1). To err is human: Building a safer health system. Retrieved from Institute of Medicine of the National Academies website: http://search.nap.edu/books/030907343X/html
ReferencesRoger, V. L., Go, A. S., Lloyd-Jones, D. M., Benjamin, E. J., Berry, F. D., Borden, W. B., . . . Turner, M.
B. (2011, December 15). Heart disease and stroke statistics – 2012 Update: A report from the American Heart Association. Circulation: Journal of the American Heart Association, VOLUME , 1-223. doi:10.1161/CIR.0B013E31823AC046
White, K. W., & Zaccagnini, M. E. (2011). A template for the DNP scholarly project. In M. E. Zaccagnini & K. W. White (Eds.), The doctorate of nursing practice essentials. A new model for advanced practice nursing (pp. 451-496). Sudbury, MA: Jones and Bartlett Publishers.