ruvalcaba syndrome: a case report
TRANSCRIPT
Eur J Pediatr (1984) 142: 301-303
Ruvalcaba syndrome: a case report
E. Bianchi 1, C. Livieri 1, M. Arico '1 , E. Cattaneo 1, A . F . Podesta '1, and G. Beluffi 2
1 Dipartimento di Pediatria, Universit~t di Pavia, Italy 2 Servizio di Radiologia Pediatrica
Abstract. An l l -year -o ld child with mental retardation and short stature was examined and found to be affected with some skeletal malformations. The clini- cal and radiological pattern of limb alterations was particularly suggestive of the features of Ruvalcaba syndrome.
A complete examination confirmed the diagnosis and showed ocular involve- ment. To the best of our knowledge this is first published confirmation of Ruval- caba syndrome.
Key words: Mental retardation - Osse- ous dysplasia - Brachyphalangy
Introduction
In 1971 Ruvalcaba et al. reported a new familial syndrome with osseous dysplasia and mental deficiency [2]. In their paper they described two male siblings affected by mental retardation, short stature, microcephaly, peculiar facies, narrow thoracic cage, hypoplastic genitals, hypoplastic skin lesions and skeletal deformities.
In particular, metacarpal and meta- tarsal lesions appeared to be very distinc- tive. Studies of the family revealed two maternal cousins with several of the de- scribed anomalies.
In this paper we describe a boy who presents clinical and radiological f~atu- res resembling those of Ruvalcaba's patients.
Case report
Pietro R., an Italian male, was the second child of unrelated healthy parents
Offprint requests to: Dott.EIena Bianchi, Dipartimento di Pediatria, Policlinieo S. Mat- teo, 1-27100 Pavia, Italy
Abbreviation: VER = visual evoked responses
(father 29 years old, mother 24 years old). His mother was gravida 3 para 3, and the two sisters were in good health. The familial history was unremarkable. Gestation was regular. BW was 2500 g, and the neonatal period was referred normal. The child suffered with recur- rent episodes of gastroenteritis until the age of 2 years. He was short in stature.
At the age of 11.4 years no pubertal signs were evident. Psychomotor and language development were retarded.
The boy was referred to our Depart- ment at the age of 11.4 years, because of short stature and mental retardation.
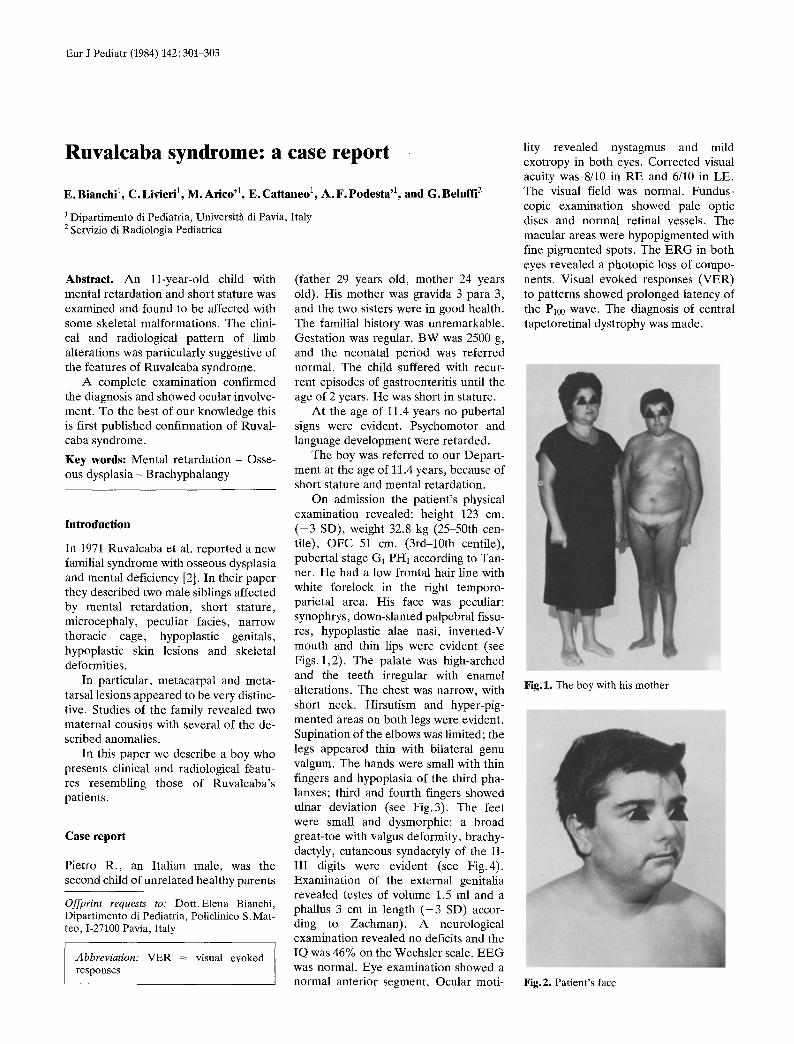
On admission the patient 's physical examination revealed: height 123 cm. ( - 3 SD), weight 32.8 kg (25-50th cen- tile), OFC 51 cm. (3rd-10th centile), pubertal stage G1 PH1 according to Tan- ner. He had a low frontal hair line with white forelock in the right temporo- parietal area. His face was peculiar: synophrys, down-slanted palpebral fissu- res, hypoplastic alae nasi, inverted-V mouth and thin lips were evident (see Figs. l ,2) . The palate was high-arched and the teeth irregular with enamel alterations. The chest was narrow, with short neck. Hirsutism and hyper-pig- mented areas on both legs were evident. Supination of the elbows was limited; the legs appeared thin with bilateral genu valgum. The hands were small with thin fingers and hypoplasia of the third pha- lanxes; third and fourth fingers showed ulnar deviation (see Fig.3). The feet were small and dysmorphic: a broad great-toe with valgus deformity, brachy- dactyly, cutaneous syndactyly of the II- III digits were evident (see Fig.4). Examination of the external genitalia revealed testes of volume 1.5 ml and a phallus 3 cm in length ( - 3 SD) accor- ding to Zachman). A neurological examination revealed no deficits and the IQ was 46% on the Wechsler scale. E E G was normal. Eye examination showed a normal anterior segment. Ocular moti-
lity revealed nystagmus and mild exotropy in both eyes. Corrected visual acuity was 8/10 in RE and 6/10 in LE. The visual field was normal. Fundus- copic examination showed pale optic discs and normal retinal vessels. The macular areas were hypopigmented with fine pigmented spots. The E R G in both eyes revealed a photopic loss of compo- nents. Visual evoked responses (VER) to patterns showed prolonged latency of the Pa00 wave. The diagnosis of central tapetoretinal dystrophy was made.
Fig.1. The boy with his mother
Fig.2. Patient's face

302
Fig.3. Physical (a) and radiological (b) features of the hands
Laboratory data revealed normal blood routine te~ts; urine analysis dis- closed intermittent microhaematuria and urine cultures were repeatedly negative. Chromosome analysis was 46,XY. Inte- stinal malabsorption was excluded. Growth hormone (after insulin-induced hypoglycemia and after L-dopa admin- istration) plasma levels were normal. An LH-RH test showed normal prepubertal values. Adrenal and thyroid function was normal.
Radiological examination
Skull examination revealed the presence of multiple Wormian bones; in the region of the lambda deep vascular groo- ves were evident. There was slight ante- rior wedging of the vertebral bodies at the thoraco-lumbar junction. There was mild dorsal kyphosis. The long bones showed no abnormalities. Examination under loading of the lower limbs showed genua recurvata, more evident on the right side. In the hands the III-Vth meta- carpal bones were shorter than normal and showed at their ends a "mushroom" appearance. At the base and at the pro-
ximal third of the diaphysis of the Vth metacarpal some lacunae were visible. There was mild radial deviation of the first finger and ulnar deviation of III- IVth fingers; the Vth finger and the ter- minal phalanx of III-Vth fingers were hypoplastic. The carpal bone age was 11.7 years (TW2) (see Fig. 3).
The metatarsal bones were short; particularly the I lnd on left was shorter than the contralateral. There was a mushroom appearance of the proximal ends of the II-Vth metatarsal bones (see Fig. 4); the phalanxes of the II-V fingers were shortened. The hallux was in a val- gus position and its basal phalanx sho- wed scalloping of the distal end, while the terminal phalanx was short and broad.
IV pyelography failed to reveal any abnormality. Computed axial tomo- graphy excluded any encephalic abnor- malities.
Subsequently, the boy started puber- tal development at the age of 12.5 years. Now, at 14.2 years old he is in good gen- eral health, but mental deficiency is ev- ident. His physical parameters are:
Fig.4. Physical (a) and radiological (b) fea- tures of the feet
height 139 cm ( - 3 SD); weight 43.2 kg (25th centile). Bone age is 11.5-12 years (TW2). Pubertal stages are G3 PH3.
Discussion
Clinical and radiological features of the present case closely resemble those of Ruvalcaba's patients. So we thought that any other bone dysplasia associated with mental retardation need not be consider- ed for the differential diagnosis.
From examination of Table 1 we can appreciate only some minimal differen- ces between the present and the pre- viously reported cases. Ectodermal ano- malies observed by Ruvalcaba (areas of hypoplastic skin and enlarged areola) are here "substituted" by the presence of some moderately hyperchromic areas on the legs, a forelock, and enamel changes.
Radiological examination more than confirmed the above described anoma- lies but failed to show spinal osteochon- dritis. It is possible however that, as in previous cases, this anomaly will become more evident after puberty. The next

Table 1. Features of the syndrome
Abnormalities Ruvalcaba's cases Present
Males
1 2
case Females
3 4
General
Mental deficiency
Short stature
Delayed adolescence
Craniofacial
Microcephaly
Downslanted palpebral fissure
Narrow and small nose
Narrow maxilla-Crowded teeth
Skeletal
Narrow trunk
Scoliosis
Kyphosis
Osteochondritis of spine
Limitation of joint extension
Prominent elbows
Short limbs
Short hands
Short metacarpals
Short phalanxes
Small feet
Short metatarsals
Urogenital
Undescended hypoplastic testicles
Hypoplastic genitals
Abnormal position of kidney
Cutaneous
Enlarged areola
Areas of hypoplastic skin
Partial albinism
Hirsutism
Other
Inguinal hernia
Enamel alterations
Microhaematuria
Ocular involvement
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
- +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ +
+ + +
+ + +
? + +
-- + +
- - + +
+ + +
- ? +
+ + -
+ + +
- ? +
- - ? - -
+ + +
m
m
+ +
+ +
+ +
+ +
+ +
+
?
m
+
+
+
+
+
303
radiological survey will be able to clarify this possibility.
Ocula r i nvo lvemen t was not r epo r t ed previously. In our case re t inal degenera - t ion was ev ident and a m o d e r a t e functio- nal i m p a i r m e n t was conf i rmed by the electrophysiological study.
The ev idence of i n t e rmi t t en t micro- h a e m a t u r i a led us to explore renal mor- phology and funct ion, bu t at the end of the diagnost ic work-up a renal malfor- ma t ion or i m p a i r e m e n t could be exclu- ded.
A comple te endocr ine s tudy and the l abora to ry tests al lowed us to exclude in tes t inal ma labso rp t ion and any ho rmo- nal cause of shor t s ta ture , for which a d e m o n s t r a b l e cause is actually no t avail- able.
Ruva lcaba suggested a possible X-lin- ked semi -dominan t m o d e of inher i t ance for this disorder . In our family no more affected pa t ien ts are repor ted , bu t the ma te rna l fea tures (see Fig. 1) seem to suggest the possible p resence of an af- fected gene in the ma te rna l line.
It may be of in teres t to r e m e m b e r tha t in 1977 H u n t e r et al. [1] r epo r t ed th ree genera t ions of one family tha t sho- wed a r e m a r k a b l e r e semblance to the pa t ien ts r epo r t ed by Ruva lcaba et al. However , H u n t e r et al. did not consider his r epo r t ed pedigree to have the above syndrome.
R e f e r e n c e s
1. Hunter AGW, McAlpine PJ, Rudd NL, Fraser FC (1977) A "new" syndrome of mental retardation with characteristic facies and brachyphalangy. J Med Genet 14 : 430-437
2. Ruvalcaba RHA, Reichert A, Smith DW (1971) A new familial syndome with osse- ous dysplasia a n d mental deficiency. J Pediatr 79 : 450-455
Received December 31, 1983 / Accepted April 15, 1984