running head: too much data, not enough data...
TRANSCRIPT

Running Head: TOO MUCH DATA, NOT ENOUGH DATA 1
Too Much Data, Not Enough Data: Providing Relevance to Care Connectivity
Consortium Providers and Their Patients
Kathleen Merkley, MS, RN, FNP, ANP
Electronic Clinical Information Management Implementation Director
Intermountain Health Care
University of Utah College of Nursing
“In partial fulfillment of the requirements for the Doctor of Nursing Practice”

TOO MUCH DATA, NOT ENOUGH DATA 2
Table of Contents
Executive Summary ………………………………………………………………………………6
Introduction………………………………………………………………………………………..7
Significance of the Project………………………………………………………………………...9
Project Objectives………………………………………………………………………………..11
Search Strategy ...………………………………………………………………………………..12
Literature Review ………………………………………………………………………………..12
Meaningful Use Regulations for Electronic Health Records…………………………….13
The Importance of Interoperability………………………………………………………15
The Care Connectivity Consortium……………………………………………………...17
Data Overload – A Risk for Success……………………………………………………..18
Big Data – an Additional Consideration…………………………………………………20
Privacy and Security Burdens Associated with Increased Data ……………………....21
Taxonomy of Value Accrual…………………………………………………………….23
Clinical Document Architecture and the Continuity of Care Document………………..24
Data Sharing Model and Transferring of Information…………………………………..25
Ethical and Legal Considerations of Data Selection ……………………………………26
Shared Accountability in Data Exchange ……………………………………………….27
The Provider-Patient Relationship and Data Exchange …………………………………29
Trusting of Exchanged Data……………………………………………………………..30
Patients as Gatekeepers – Personally Controlled Health Records……………………….31
What Constitutes Appropriate Data ……………………………………………………..33
Moderators/Types of HIE Access ….……………………………………………………36

TOO MUCH DATA, NOT ENOUGH DATA 3
Accessing Appropriate Data …….………………………………………………………38
Presentation of Received Data…………………………………………………………...40
Reconciliation of Received and Existing Data…………………………………………..41
Are Data Requirements Different Between Caregivers and Patient Types ……………..42
Theoretical Framework ………………………………………………………………………….44
Implementation…………………………………………………………………………………..46
Evaluation Plan…………………………………………………………………………………..51
Project Results…………………………………………………………………………………...54
Relevant Data by Specialty……………………………………………………….….......54
What Constitutes Relevant Data for Critical Care Patients……………………….……..56
Top Five Types of Priority Data Related to Specialty………………………….………..57
Presentation of Exchanged Data - Separate or Integrated……………………………….58
Reconciliation of All Data……………………………………………………………….58
What Makes Data Trustworthy…………………………………………………..………59
Time Limits of Different Types of Exchanged Data…………………………………….60
Discussion………………………………………………………………………………………..63
Project Recommendations……………………………………………………………………….66
Summary…………………………………………………………………………………………67
References………………………………………………………………………………………..68
Tables
Table 1- Data Value Classification Taxonomy …..……………………………………………...23
Table 2 - ED Physician Access of Data from a HIE ….…………………………………………43
Table 3 - ED Physician Preference of Data Display ………………………………….…………43
TOO MUCH DATA, NOT ENOUGH DATA 4
Table 4 - Relevant Data Points to be Surveyed …………………………………………………47
Table 5 - Time Line for Survey Completion ……………………………………………………52
Table 6 – Survey Participant Breakdown………………………………………………………..54
Table 7 – Relevant Data by Specialty……………………………………………………………55
Table 8 – Relevant Data for Critical Patients……………………………………………………56
Table 9 – What Makes Data Trustworthy…………………………………………………….....59
Table 10 – Relevant Data for LIPs in 2003……………………………………………………...64
Figures
Figure 1 - Data Value Classifications…………………………………………………………... 24
Figure 2 – Identification of Most Valuable Data………………………………………………..36
Figure 3 – Presentation of Received Data………………………………………………………40
Figure 4 – Reconciliation of Received and Existing Data………………………………………41
Figure 5 - DIKW Framework……………………………………….…………………………...45
Figure 6 – Top Five Data Types by Specialty…………………………………………………...58
Figure 7 – Useful Lifecycle of Data Types………………………………………………………62
Appendices
Appendix A- IRB Approval………………………………………………………………….....75
Appendix B – List of CCC Committees……………………………………………………......79
Appendix C – Pre-Survey Letter ……………………………………………………………….81
Appendix D – Survey Invitation Letter CCC Members………………………………….……..84
Appendix E – Survey Invitation Letter Intermountain Healthcare Participants………………..86
Appendix F – Thank You Letter ……………………………………………………………….88
Appendix G – CCC Recommendations………………………………………………………...90
TOO MUCH DATA, NOT ENOUGH DATA 5
Appendix H – Electronic Data Relevance Survey – Emergency……………………….……….96
Appendix I –Electronic Data Relevance Survey – Inpatient Nursing …………………….…..104
Appendix J – Electronic Data Relevance Survey – Inpatient……………………………….…112
Appendix K– Electronic Data Relevance Survey – Primary Care……………………………..120
Appendix L – Electronic Data Relevance Survey – Electronic Copy …………………………128
Appendix M – Electronic Data Relevance Survey – Pediatrics………………………………..136
Appendix N – Electronic Data Relevance Survey – Primary Care Nursing…………………...144
Appendix O – Relevant Data by Specialty……………………………………………………..152
Appendix P – Relevant Emergent Data………………………………………………………...159
Appendix Q - Presentation of Exchanged Data – Separate or Integrated……………………...164
Appendix R – Reconciliation of Exchanged Data……………………………………………..167
TOO MUCH DATA, NOT ENOUGH DATA 6
Executive Summary
The Care Connectivity Consortium (CCC), a consortium of five leading U.S. healthcare
organizations was recently formed to help promote electronic transfer of health information
across the country. Electronic health information transfer has also become a mandate for
“Meaningful Use” in a recent provision of the American Recovery and Reinvestment Act.
Working from the hypotheses that more data are not always helpful when transferred
electronically, this DNP scholarly project identified what electronic data are relevant to specialty,
patient type, patient acuity and chronicity of illness by surveying CCC clinicians. It also
determined what clinicians consider to be trustable data, what data should be exchanged during
emergent situations and what time limitations may be placed on certain data categories. Survey
questions on these topics were determined after an extensive review of the literature.
The following Essentials of Doctoral Education for Advanced Nursing Practice criteria
helped guide this project development. These include: Essential I: Scientific Underpinnings for
Practice, Essential II: Organizational and Systems Leadership for Quality Improvement and
Systems Thinking, Essential III: Clinical Scholarship and analytical Methods for Evidence Based
Practice, Essential IV: Utilizing Information Systems/Technology for the Improvement and
Transformation of Health Care, Essential VI: Interprofessional Collaboration for Improving
Patient and Population Health Outcomes, Essential VII: Clinical Prevention and Population
Health for Improving the Nation’s Health, and Essential VIII: Advanced Nursing Practice
(2006).
The philosophical foundation of the project is based on the Data-Information-
Knowledge-Wisdom (DIKW) theoretical framework taken from the Graves and Corcoran (1989)
article “The Study of Nursing Informatics”. Methodology for the project was modeled in part
using a modified Delphi technique. The survey was administered electronically or by paper
survey to 159 CCC clinicians across the country. Evaluation of results was accomplished with
the help of content experts from the CCC. The final evaluation relating to the success of the
project will be realized if survey recommendations are incorporated into the CCC data exchange
structure, which is outside the DNP project scope
Relevant, pertinent and timely electronic data passed through a health information
exchange must become a recognized and critical component in providing better patient care.
Knowing and understanding the exact health information that specific providers need at certain
point in the treatment process will only enhance the quality of care given to patients. This survey
has begun the exploratory process of identifying what health information should be exchanged.
TOO MUCH DATA, NOT ENOUGH DATA 7
A 65-year-old male from the Midwest is vacationing on the West Coast. He arrives at
6:00 a.m. to a local emergency department complaining of chest pain for the last 60 minutes. He
has a history of congestive heart failure and Type II Diabetes Mellitus. He is immediately given
oxygen, an aspirin, IV access is obtained, cardiac enzymes are drawn and an ECG is ordered.
The ECG reveals equivocal changes. The patient care nurse is asked to locate an old ECG
obtained two weeks ago from an emergency department in his home town. She spends the next
45 minutes contacting his hospital’s health information management (HIM) department, having
the patient sign a release of information, faxing it, re-contacting the HIM department who had
sent the ECG to the wrong fax number and finally, watching it spit out of the fax machine.
Precious time has been lost if the patient is indeed infarcting his heart muscle.
The scenario described above demonstrates that the ability to rapidly transfer patient
information between health care systems is currently inadequate. Because of the rapid pace of
emergency care, delays in accessing health information can impact outcomes. Yet there is hope
on the horizon. Data transfer is becoming a recognized and critical component in providing
better patient care.
The Care Connectivity Consortium (CCC), a consortium of five leading healthcare
organizations including Intermountain Healthcare, Mayo Clinic, Kaiser-Permanente, Group
Health and Geisinger Health Systems was formed in late 2011 to help promote the electronic
transfer of health information across the country. The CCC considers the development of
electronic medical information transfer as a crucial care support tool needed in healthcare
reform. First, support tools for patient identification, patient directed consents and authorization
will need to emerge in order to achieve the envisioned shared accountability models of
healthcare reform.
TOO MUCH DATA, NOT ENOUGH DATA 8
Next an inquiry surfaces related to the actual types of data that should be exchanged to
provide better coordination and improved care. Currently the CCC provides only the patient’s
problems, medication and allergy lists between its members. Very little information is currently
available on what types of data are appropriate to exchange. No precedence has yet been set on
this subject. It is hoped this project will help define these standards.
Working from the hypothesis that more data are not always helpful, this project attempted
to determine what additional data elements should be exchanged related to patient type, age,
severity and chronicity of the illness and requesting caregiver. The goal was to identify which
data exchanged is clinically pertinent to care providers receiving and caring for patients from
another care setting.
The long term clinical implications of this project will attempt to deliver health
information that will provide care givers with the right data at the right time and in the right
place across health care systems, regardless of organizational borders. This will ultimately lead
to better patient care.
Significance of the Project
It was the assumption of this project that knowing and understanding the specific health
information providers require at a certain point in the treatment process will not only enhance the
quality of care and services, but lead to better informed decisions, promote patient safety,
advance health outcomes, prompt stronger patient-provider relationships and decrease health
care expenditures. Several groups have facilitated, supported or reviewed this project. They
include the Care Connectivity Consortium Network Information Technology (IT) Board, the
Health Information Technology (IT) Standards Committee, Health Level 7 (HL7), and the Utah
Health Information Network (UHIN).
TOO MUCH DATA, NOT ENOUGH DATA 9
The first group is the CCC Network IT Board. This is the governing body of the CCC.
Membership includes representatives from all five consortium members. They approved group
participation in the survey process and helped identify and administer surveys to various
provider types within the consortium. This group will review the survey results; determine if the
recommendations are applicable and then, if so, will implement them into the CCC data
exchange process.
The Health IT Standards Committee falls under the Office of the National Coordinator
(ONC) for Health Information Technology (Office of Health Information Technology, 2012).
They have developed the Standard and Operability Framework (S&I Framework) with the
objective to create a robust, repeatable process that will enable the ONC to execute initiatives
that will help improve interoperability and adoption of standards and health information
technology. This committee is interested in the survey results because of their charge to develop
interoperability specifications to support health outcomes and healthcare priorities.
HL7 is an international IT standards development body that provides a framework for the
exchange, integration, sharing and retrieval of electronic health information. These standards
help define how information is packaged and communicated from one party to another (HL7,
2012). Because this group is studying care plan initiatives and what data should be included they
are also interested in survey results as they determine a care plan initiative data set.
The Utah Health Information Network (UHIN) has been working with the national health
care community since 1993 to develop a secure and efficient electronic data exchange network
for hospitals in Utah (Utah Health Information Network, 2012). They have working
relationships with 90% of hospitals and care providers in the state. They are also attentive to the
TOO MUCH DATA, NOT ENOUGH DATA 10
survey results as they are the group that defines what data should be exchanged between Utah
providers, hospitals and clinics.
Shareholders in this project have included CCC providers who have participated in the
project and then will be held accountable to use the shared data that has been defined as
pertinent. Patients seeking care at consortium facilities who must provide access to their data are
also vital in this process.
Project Objectives
To accomplish the goal of identifying which data exchanged is clinically pertinent to care
providers receiving and caring for patients from another care setting the following objectives
have been met.
1. A literature search explored: a) the importance of data sharing, b) associated federal
regulation, c) potential implications of data overload, d) development of a taxonomy
of value accrual, e) data sharing models, f) ethical and legal considerations of data
selection, g) shared accountability, h) the provider patient relationship, i) patients as
gatekeepers of their health information, j) what constitutes appropriate data, k) what
makes data trustworthy, l) presentation of received data, m) reconciliation of
disparate data that is exchanged and n) identification of data elements and related
patient populations and provider needs to be examined.
2. Based on the literature review, a survey was developed with potential data elements
to be exchanged and was distributed to consortium members for their input as to
importance and necessity.
3. The survey was administered to providers in various specialty areas who care for
different patient types. IRB approval was received for this.
TOO MUCH DATA, NOT ENOUGH DATA 11
4. Lastly, the survey results were analyzed and recommendations were made regarding
additional data elements that should be included in electronic data sharing related to
patient type and provider specialty. These recommendations were sent to the CCC
Network IT Board to be used as input on what future data should be shared with
consortium members.
Search Strategy
An extensive literature search was performed using Pub Med and CINAHL databases, the
Department of Health and Human Services, National Health Information Exchange, Office of
Health Information Technology (2012), HL7, Integrating the Healthcare Enterprise (IHE), and
Utah Health Information Network websites, as well as reviewing numerous issues of the Journal
of the American Medical Informatics Association (JAMIA). The terms health information
exchange, provider, care coordination, meaningful use regulations, continuity of care documents,
alert fatigue, national health information network, shared accountability, person health records,
data relevance and theoretical model were used in the search. In this document “provider” or
“clinician” is defined as a medical doctor, doctor of osteopathic medicine, nurse practitioner,
physician assistant or registered nurse. Licensed independent practitioner (LIP) is defined as a
medical doctor, doctor of osteopathic medicine, nurse practitioner or physician assistant.
Literature Review
Health information exchanges involves sharing of clinical, financial and demographic
data among health care stakeholders in support of care delivery, financing, public health
surveillance, research, and other health system activities. Balfour et al. (2009) reports, “Use of
these systems results in improvements in quality of care such as avoidance of redundant tests”
TOO MUCH DATA, NOT ENOUGH DATA 12
(p.11). Information exchange may also prevent hospital admissions related to medication
allergies, errors, or interactions and lowers costs of caring for chronically ill patients.
Johnson et al. (2011) recognizes that Americans increasingly seek healthcare from
multiple organizations because of insurance restrictions, availability of specialists and ease of
travel. The process of accessing information across disparate systems is difficult, particularly
when patients don’t remember where care was provided. This leads to incomplete patient data.
“This knowledge ‘blind spot’ increases healthcare costs when previously performed tests and
procedures must be duplicated to provide decisions makers with data” (p. 690).
Various studies on coordination of care indicate that people with multiple chronic
conditions are more likely to be hospitalized, see a variety of physicians, take several
prescription drugs and be visited at home by health workers. Furthermore, the poor coordination
of care has been associated with poor clinical outcomes such as unnecessary hospitalization,
duplicate tests, conflicting clinical advice and adverse drug reactions. All this suggests a need
for better care coordination and information sharing among providers (Burton, Anderson, Kues,
2004). Sharing of patient information is also known to provide higher quality at lower cost.
Meaningful Use Regulation for Electronic Health Records
Electronic health records (EHR) are becoming more widespread throughout the United
States. However the transition has been slow and cumbersome. Blumenthal and Tavenner
(2010) believe that the Health Information Technology for Economic and Clinical Health Act
(HITECH) sponsored by the Obama administration and passed by the 2009 Congress will
provide the health care community with a transformational opportunity to break through these
barriers.
TOO MUCH DATA, NOT ENOUGH DATA 13
The HITECH provision of the American Recovery and Reinvestment Act of 2009
provides billions of dollars in incentives for adoption and use of health information technology
by Medicare and Medicaid providers over the next ten years. To receive the financial incentives,
licensed independent practitioners and hospitals must achieve “Meaningful Use” (MU) of an
electronic health record. They are required to comply with a set of core objectives which
initially focus on entering in basic information (demographics, vital signs, active medications,
allergies, up-to date problem lists and active diagnoses) but will soon include incorporating lab
results, issuing reminders for care, providing specific patient education, clinical documentation,
decision support, disease and medication management, as well as quality and safety measures
(Office of Health Information Technology, 2012).
Another explicit goal of the act is a provider-to-provider data exchange which is essential
for the long-term success of the Affordable Care Act of 2010 (Rudin, Volk, Simons & Bates,
2011). Maslove, Rizk & Lowe (2012) agree that these required computer-based technologies
used to produce, manage and share health-related information, grouped under the umbrella term
“Health Information Technology” (HIT) are a means to improve the quality, safety, and
efficiency of health care delivery in a growing number of countries.
The recent HITECH economic stimulus package contains considerable funding for the
development of health information technology architecture that will support the nationwide
electronic exchange. This exchange will also be a means of providing research and surveillance
data. Most important however, Francis believes that, “What the provider records about the
patient – and what the provider recommends with respect to the patient will no longer reside in
the microcosm of a single office” (2010, p. 36). When expressed in these terms, one can see
how the HITECH provision will be “meaningful” to both patients and providers.
TOO MUCH DATA, NOT ENOUGH DATA 14
The Importance of Interoperability
Interoperability is the term used to define the ability of information technology (IT)
systems to exchange information and is the key element of the CCC. A vision of interoperability
and its benefits was defined in 2001. Since that time, important advances toward the goal have
been made related to a number of government initiates (Kuperman, 2011). The Office of the
National Coordinator for Health Information Technology (ONC) within the Health and Human
Services Department chartered a National Health Information Network Trial Implementations
project in 2010. The purpose of the project was to demonstrate data exchange among operational
health-information exchanges. The project sought to demonstrate that eight interoperability
scenarios could be technically accomplished. These scenarios included:
1. EHR-laboratory results – incorporate new lab results into the ordering provider’s
HER,
2. Emergency responder - provide the provider with access to the patient’s data in an
emergency scenario,
3. Medication management – support access to the patient’s medication and allergy data in a
medication reconciliation scenario,
4. Quality – communicate quality-related information from a provider organization to
another organization,
5. Social security administration (SSA) – allow the SSA to retrieve the patient’s data to
make a disability-benefits determination,
6. Bio-surveillance – data collection to support situational awareness, event detection and
outbreak management,
TOO MUCH DATA, NOT ENOUGH DATA 15
7. Consumer access to clinical information – allow consumers to access their data via a
personal health record, and
8. Consumer empowerment – allow the consumer to authorize the provider to have a view
of his or her data (National Health Information Network, p. 678).
When viewing this list, the potential and importance of sharing health care data across systems
become very apparent.
One specific model of interoperability, called the health information exchange (HIE) has
emerged to address patient-centered information access. The HIE “attempts to make available on
an incremental and local basis, comprehensive patient-centered information access where care is
needed” (Frisse, p 51). Early evaluations of HIEs reveal they make a difference in patient care
but have not yet begun to reach their potential.
One HIE now in operation, The Memphis Health Information Exchange, claims that more
information available to providers will uniformly impact provider-patient communication in
positive ways. Frisse (2010) says, “Our limited experience suggests that such data can be of
great anecdotal aid during acute situations by allowing patients and their physicians to begin with
a greater common knowledge of past medical history” (p.56). He reports that because of the
HIE, providers and patients have seen a new vision of care. At the institutional level, it has also
demonstrated that sharing patient data across traditional health organization boundaries is a low
cost solution for better patient care.
Of the more than one hundred HIEs in the United States, few are fully operational. Even
fewer have advanced data exchange capabilities such as providing access to comprehensive data
that may originate from many different medical practices in the form of aggregate patient-centric
records (Rudin et al., 2011). Multiplicity of systems with multiple HIEs requirements is a major
TOO MUCH DATA, NOT ENOUGH DATA 16
barrier. Interoperability remains elusive, yet there is hope on the horizon as healthcare
organizations begin to recognize its value to the patient, the provider, the organization and
national healthcare as a whole.
A side benefit of robust health information exchanges must also be examined in the
public health domain. Public health officials could survey disease trends and recognize
variations. This rapid surveillance could lead to timely interventions as well as lives saved.
Health information exchanges could also improve patient safety by tracking preventable deaths
and medication errors. Improved quality of care could be more easily tracked and healthcare
costs might be more easily assessed (Yasnoff, 2010). Currently some data is already exchanged
in public health departments across the country which is impacting health care for the better.
The Care Connectivity Consortium
In 2011, Kaiser-Permanente, Mayo Clinic, Geisinger Health Systems, Group Health
Cooperative and Intermountain Healthcare joined forces in an interoperability and data sharing
collaboration- the CCC. Each of the systems has individually demonstrated the value of health
IT by improving the quality of care for patients across the continuum of care. The consortium is
working together to expand the understanding of what type of data transfer is possible in
connected healthcare systems and to demonstrate better and safer care through better data
availability. The focus will be on accelerating the process to form the National Health
Information Network or NHIN (MTBC, 2011).
The CCC is creating a future where timely access to health information results in patient-
centered, community-wide, evidence-based care (2012. Securely connecting care givers to
patient data regardless of organizational boundaries, ensures better-informed decisions and
stronger patient-provider relationships.
TOO MUCH DATA, NOT ENOUGH DATA 17
George Halvorson, CEO of Kaiser-Permanente believes that the importance of such and
initiative cannot be overstated:
This collaborative effort exists because we all have reached the same conclusion about
linking and sharing patient-specific data. Our five organizations share the common
mission of improving healthcare in the United States and our belief is that when doctors
have real-time data about patients, care is better and effective (Intermountain
Stories, 2011, p.3).
It is the goal of the collaboration to accelerate the implementation of national health IT
standards. One concern of this type of data exchange is violation of patient privacy. Marc
Probst, chief information officer of Intermountain Healthcare asserts that “Patient privacy and
security are the overarching priorities” (Intermountain Stories, 2011, p. 2).
As stated above, currently the consortium only exchanges patient medication, problem
and allergy lists. Intermountain has been tasked with identifying what constitutes additional
appropriate data elements. This charge comes with the mission of identifying what information
will be meaningful to providers without jeopardizing patient-provider relationship, identifying
associated ethical and legal issues and determining what constitutes too much data.
Data Overload – A Risk for Success?
In As You Like It, William Shakespeare claims, “Why then, can one desire too much of a
good thing?” Indeed, can there be too much of a good thing when it relates to patient data?
Providers perform many tasks in their daily work which require summarization of data to
identify pertinent clinical information. As technology makes more data available, the challenges
of data overload become increasingly important. “Much attention has been given to the notion of
evidence-based medicine and how to address the information needs of providers to answer
TOO MUCH DATA, NOT ENOUGH DATA 18
clinical questions and support decision-making” (Tielman, Van Vleck, Stein, Stetson, &
Johnson, 2007, p. 761). Less attention, however, has been focused on how to help providers
navigate the substantial amount of clinical data that is accruing for each individual patient,
A practicing physician, Westby Fisher (2012) stresses providers are accumulating too
much data and not enough appropriate information. Another provider, Jennifer Dennard (2012)
says providers are swimming in too much electronic data. When observing the extensive patient
information in a hospital electronic health record (EHR) and then connecting two or more
institutions together the pool of information becomes even larger. It may then be difficult to
differentiate what information is actually pertinent.
Pho (2012) alleges that too much data- whether it is written or on a screen – can
overwhelm physicians and potentially place patients at harm. Review of test results can
specifically be overwhelming. He believes curating test results by ordering abnormal ones, will
really be the true power of electronic test reporting. The Wolters Kluwer Health 2011 Point-of-
Care Survey found that the second largest barrier to technology adoption by primary care
physicians is “Too much data, not enough actionable information” (32%) preceded only by “Too
expensive” (40%).
The downside of too much data, according to Daigh (2002) is that “A data dump will
waste a physician’s time, destroying the original intent of medical records with meaningless
repetition and templates, satisfying demands of third-party payers but not of physicians’
thoughtful review and analysis” (p. 1). Fisher (2012) avows that providers need better
information, not more of it. “We don’t need to know what ‘type’ of order we entered, for
instance, we need more time with our patients and less time with data entry” (p.3). Deciding
TOO MUCH DATA, NOT ENOUGH DATA 19
what information goes and what stays in the medical record must be considered the priority as
we move forward.
A phenomenon known as “Alert Fatigue” should also be taken into consideration when
considering the issue of too much data. Alert fatigue results because of repeated exposures to
alerts from various decision support mechanisms such as medication allergies , drug-drug
interactions, vital sign abnormalities, unsaved data etc. leading to a decline in user
responsiveness (Cash, 2009).
A limited literature review notes that it is a well-recognized fact that when providers are
exposed to frequent clinical decision support alerts they may eventually stop responding to them.
This is thought to be related to issues such as alert irrelevance and cognitive overload (Embi &
Leonard, 2012). Can the same assumptions be made about irrelevant and repetitive data?
Most of the criteria related to types of data sharing have not yet been specified for the
National Health Information Exchange, but official statements suggest that they will require
advanced HIE functionality in the form of “access to comprehensive patient data” (Department
of Health and Human Service, 2010, p.1). What is comprehensive patient data? This is a
question this project has helped to resolve.
Big Data – an Additional Consideration
If “comprehensive data” isn’t enough to create concern, a new concept called “big data”
must be added to the equation. Richmond (2012) says there has been a recent data explosion.
He calls hospitals “factories of data” (p. 2).
Big data, as described by the McKinsey Global Institute (2011) is, “Datasets whose size
is beyond the ability of typical database software tools to capture, store, manage and analyze”
(p.3). Big data can be considered both blight and an opportunity. Having such a paucity of data
TOO MUCH DATA, NOT ENOUGH DATA 20
makes is possible to do things never before possible. “Greater volumes of data to sift through to
find critical insights (the proverbial needle in the digital haystack) is a growing problem for
companies, organizations and governments the world over,” (Richmond, 2012, p.1).
The McKinsey Global Institute (2011) believes that correct management of this
information can generate significant financial value across certain sectors of the world-wide
economy, health care being one of those sectors. There is a huge opportunity for healthcare as a
whole. Much of this data if used correctly has the potential to reduce healthcare costs. Again
Richmond (2012) emphasizes that healthcare providers have a long way to go before they can,
Come even close to realizing value creation, efficiency improvements and cost savings.
A highly fragmented data environment begets disconnected strategies and uncoordinated
decision making. By connecting the dots and leveraging the power and promise of data
assets, hospitals can improve the practice, delivery, and economics of healthcare. To
accomplish these ambitious goals, hospitals need to first make some significant changes
in how they handle big data (p. 3).
Privacy and Security Burdens Associated with Increased Data
A patient is referred to a cardiologist’s office to see the nurse practitioner for new onset
congestive heart failure. The patient’s medical history contains information about a recent visit
with a dermatologist for a mole removal. If data were to be exchanged, would it need to include
information regarding the dermatology visit or just pertinent data about the ED visit three days
ago for chest pain? When does data stop being helpful and become a data dumping ground?
Many clinicians will avow that they want access to all of a patient’s data or worse yet
none at all. They want to start a patient encounter with a “clean slate”. Would it make more
sense to provide the clinician with a subset of relevant data potentially increasing its usage and
TOO MUCH DATA, NOT ENOUGH DATA 21
then providing the ability to obtain additional and logical segments as needed? Can a clinician
agree to the concept of limiting the data that should be exchanged? These are questions that are
yet to be answered.
Today, many systems have defined clinical summaries as the vehicle for data exchange.
A summary may contain up to 300 pages of information. This is a sizeable amount of data for
any clinician to digest. If these 300 pages have been exchanged from one site to another, is the
receiving clinician accountable for all data contained in this clinical summary? Jutta Williams,
Compliance Officer at Intermountain Healthcare believes he is. She posits that because of the
large volume of information exchanged, everyone’s liability is increased and she recommends
that a HIE should bring in only information that is relevant and has been parsed appropriately
(personal conversation, July 17, 2012).
Ms. Williams advocates using the “minimum necessary” standard identified in the Health
Insurance Portability and Accounting Act (HIPAA) as a go forward strategy with data exchange.
The minimum necessary standard asserts that
Protected health information should not be used or disclosed when it is not necessary to
satisfy a particular purpose or carry out a function. It requires entities to evaluate
practices and enhance safeguards as needed to limit unnecessary or inappropriate access
to and disclosure of protected health information (Department of Health and Human
Services, 2012, p.1).
This guideline was developed to protect patients, but perhaps it might also protect clinicians if
used in a similar context with data exchange (HIPPA Regulations, 2012). One thing becomes
apparent, information should be shared responsibly but only that information which is necessary
should be distributed.
TOO MUCH DATA, NOT ENOUGH DATA 22
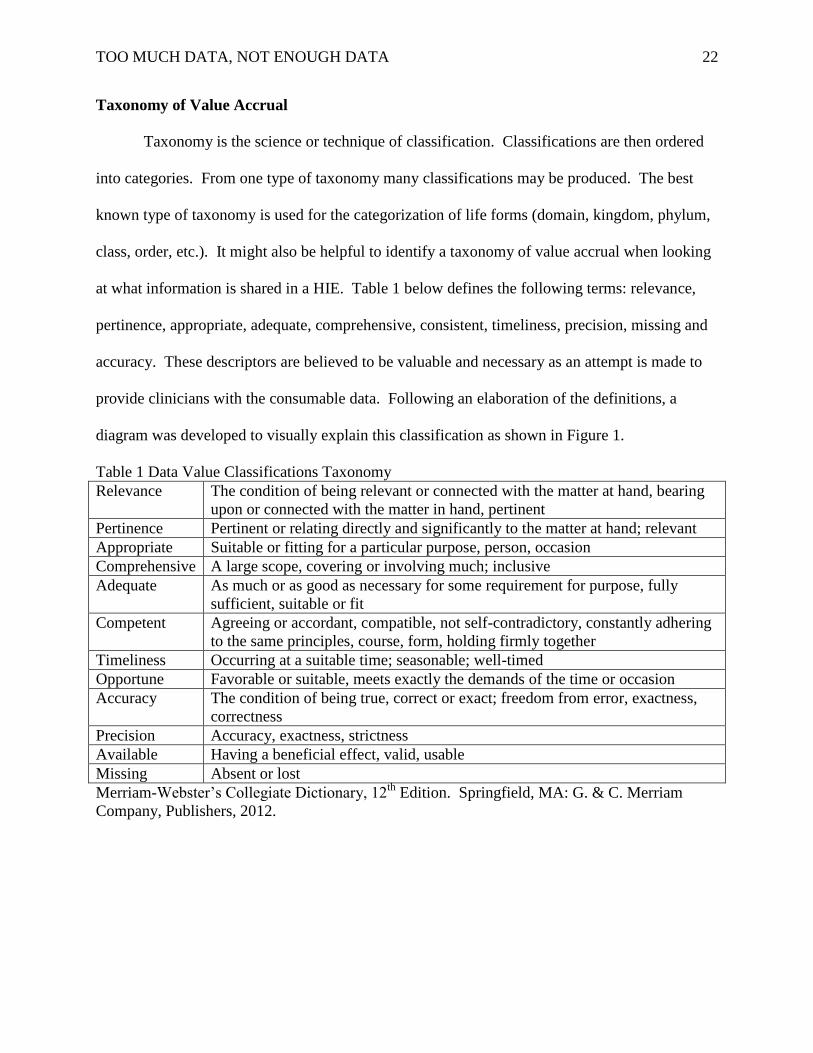
Taxonomy of Value Accrual
Taxonomy is the science or technique of classification. Classifications are then ordered
into categories. From one type of taxonomy many classifications may be produced. The best
known type of taxonomy is used for the categorization of life forms (domain, kingdom, phylum,
class, order, etc.). It might also be helpful to identify a taxonomy of value accrual when looking
at what information is shared in a HIE. Table 1 below defines the following terms: relevance,
pertinence, appropriate, adequate, comprehensive, consistent, timeliness, precision, missing and
accuracy. These descriptors are believed to be valuable and necessary as an attempt is made to
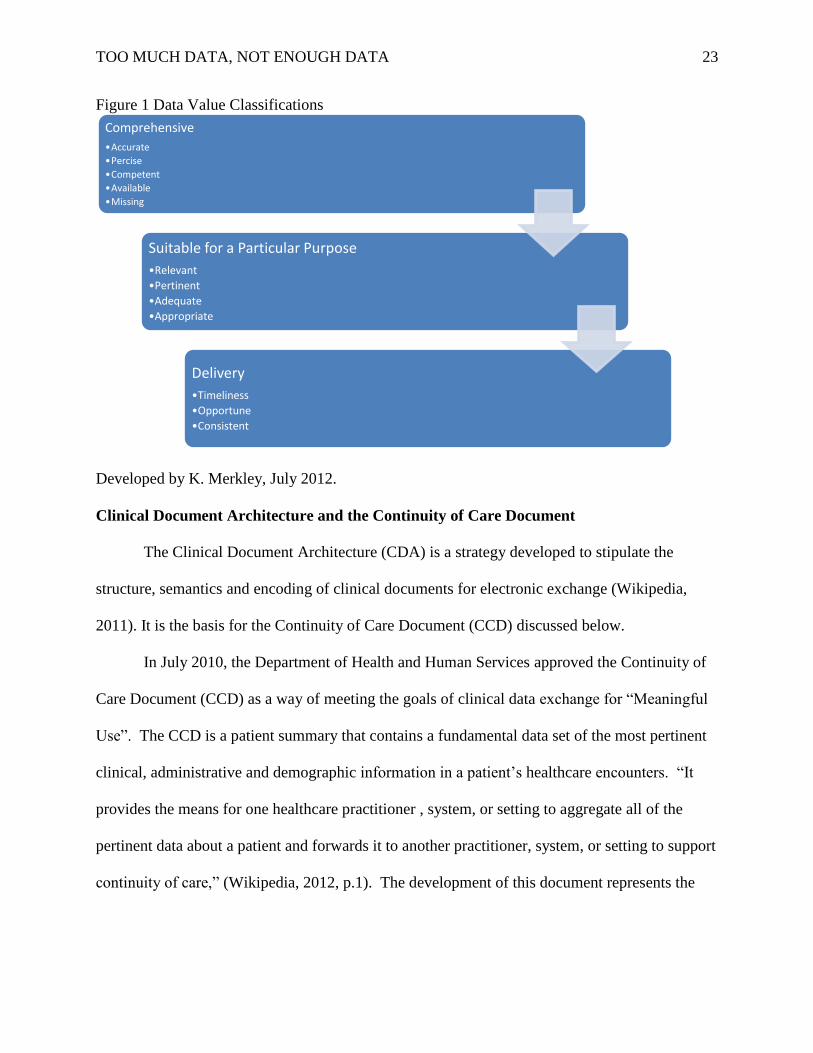
provide clinicians with the consumable data. Following an elaboration of the definitions, a
diagram was developed to visually explain this classification as shown in Figure 1.
Table 1 Data Value Classifications Taxonomy
Relevance The condition of being relevant or connected with the matter at hand, bearing
upon or connected with the matter in hand, pertinent
Pertinence Pertinent or relating directly and significantly to the matter at hand; relevant
Appropriate Suitable or fitting for a particular purpose, person, occasion
Comprehensive A large scope, covering or involving much; inclusive
Adequate As much or as good as necessary for some requirement for purpose, fully
sufficient, suitable or fit
Competent Agreeing or accordant, compatible, not self-contradictory, constantly adhering
to the same principles, course, form, holding firmly together
Timeliness Occurring at a suitable time; seasonable; well-timed
Opportune Favorable or suitable, meets exactly the demands of the time or occasion
Accuracy The condition of being true, correct or exact; freedom from error, exactness,
correctness
Precision Accuracy, exactness, strictness
Available Having a beneficial effect, valid, usable
Missing Absent or lost
Merriam-Webster’s Collegiate Dictionary, 12th
Edition. Springfield, MA: G. & C. Merriam
Company, Publishers, 2012.
TOO MUCH DATA, NOT ENOUGH DATA 23
Figure 1 Data Value Classifications
Developed by K. Merkley, July 2012.
Clinical Document Architecture and the Continuity of Care Document
The Clinical Document Architecture (CDA) is a strategy developed to stipulate the
structure, semantics and encoding of clinical documents for electronic exchange (Wikipedia,
2011). It is the basis for the Continuity of Care Document (CCD) discussed below.
In July 2010, the Department of Health and Human Services approved the Continuity of
Care Document (CCD) as a way of meeting the goals of clinical data exchange for “Meaningful
Use”. The CCD is a patient summary that contains a fundamental data set of the most pertinent
clinical, administrative and demographic information in a patient’s healthcare encounters. “It
provides the means for one healthcare practitioner , system, or setting to aggregate all of the
pertinent data about a patient and forwards it to another practitioner, system, or setting to support
continuity of care,” (Wikipedia, 2012, p.1). The development of this document represents the
Comprehensive
•Accurate
•Percise
•Competent
•Available
•Missing
Suitable for a Particular Purpose
•Relevant
•Pertinent
•Adequate
•Appropriate
Delivery
•Timeliness
•Opportune
•Consistent
TOO MUCH DATA, NOT ENOUGH DATA 24
work of various national and international committees whose goal was to standardize a
continuity of care data set.
The CCD then is a minimum data set that includes provider information, insurance
information, patient’s health status (allergies, medications, vital signs, diagnoses, problem list,
recent procedures), recent care provided, as well as recommendations for a care plan and the
reason for the referral or transfer (Burton et al., 2004). In addition family history, genome
information, psychosocial information, and public health data are considered as important and
should be included.
In a research study looking at the CCD as it relates to interoperability and HIE, D’Amore
(2010) highlighted “the promise of CCDs for population health and recommended changes for
future interoperability standards” (p. 3). In addition, the CCD recommends a compliant structure
for the transfer of free-text as well as codified data. A great deal of effort has previously gone
into this body of standardized data. This information was helpful as the project survey was built.
Data Sharing Model and Transferring of Information
The most important feature required to institute a national HIE is the ability to ensure
that all electronic health systems exchange data is in a universal language. The National Health
Information Network’s President’s Council of Advisors on Science and Technology, (2010)
recommends this universal language be able to accommodate current hospital EMRs as well as
new recordkeeping systems and formats. The only requirement would be the ability to send and
receive data in a language structured as individual data elements (i.e. a mammography result)
together with metadata that delivers an annotation for each piece of data.
An example of this would be a 74-year-old female who has lived in several different
states in the past 30 years. She has had mammograms performed at various hospitals and clinics.
TOO MUCH DATA, NOT ENOUGH DATA 25
Her provider needs to retrieve numerous images of her breast tissue to determine whether a
current lump is a new finding. If a universal data exchange language was available, the data
elements the provider could retrieve would include all of her previous mammograms regardless
of the state in which they were performed. He would be able to review these images in a similar
manner as someone doing a Google search.
A national infrastructure for finding and controlling access to health data requires a
foundation titled “data-element access services” or DEAS. Of course it makes sense the fewer
DEAS the more feasible the project. The National Health Information Network, President’s
Council of Advisors on Science and Technology, (2010) recommend DEAS be interoperable
with the ability to communicate in accordance to a single Federal standard. In response to the
HITECH directive, the ONC is currently attempting to identify features on how to best to
operationalize these services.
The CCC has developed a DEA service amongst its members to transfer health care data.
One of its missions is to demonstrate the ease with which this can be exchanged. How should
states or healthcare organizations establish and operate DEAS? This is one of many questions
which must be answered as soon as possible if HIE is to become feasible.
Ethical and Legal Considerations of Data Selection
Is it a legal liability when providers access other providers’ data and then don’t review it?
There is little information on this topic. As case law offers little guidance on the liability of a
provider acting on clinical information made available but not requested, this topic needs
additional study (Burton et al., 2004).
The legal position on clinical decision support systems is also unclear, but reviews
suggests that” parsimonious or tailored warnings” do not raise the liability risk of system
TOO MUCH DATA, NOT ENOUGH DATA 26
manufacturers and providers as long as systems are designed well and providers continue to use
their best medical judgment (Kesselheim, Creswell, Phansalka, Bates, & Sheikh, 2011, p. 2312).
Can this recommendation be inferred when sharing either limited or extreme amounts of data in
HIE?
Data exchange also presents numerous ethical challenges. Little is known about patients’
attitudes toward sharing their clinical data with different providers. Privacy issues and
unwillingness to share certain data such as a history of mental illness or sexually transmitted
diseases may prevent any patient information from being exchanged (Burton et al., 2004).
Francis (2010) suggests that the information the provider, “Records about the patient –
and what the provider recommends with respect to the patient – will no longer reside in the
microcosm of a single office” (p.40). Both the patient’s confidences and the provider’s actions
will be theoretically accessible to others. An additional risk which cannot be ignored is that
providers might characterize or stigmatize patients as they react to data that previously might not
have been available to them.
Another ethical issue potentially surfaces when patients refuse to share all of their patient
information. A HIE can be undermined by the liberty of a patient. Does a patient have a
fundamental right to remain ambiguous? A HIE can only send and receive the data the patient is
willing to share. A patient may exert the right of owning their data. The difficulty comes when
the receiver obtains only parts of the data, which may be potentially dangerous for the patient.
How can providers emancipate patients to share all of their data? They should educate them on
reasons why it is important to be transparent about their data.
Shared Accountability in Data Exchange
TOO MUCH DATA, NOT ENOUGH DATA 27
Current Meaningful Use requirements advocate for patients to access their own medical
data. Presently many health systems share their data with patients and the number will grow.
Intermountain Healthcare has a portal called “My Health” where patients can view lab and
procedure results. No provider information (hospital discharge summaries, progress notes, etc.)
is disclosed at this time (personal communication, Select Health representative, July 20, 2012).
Several studies have documented the experience and benefits of incorporating patient-
generated data into their electronic medical records. An electronic blood pressure trial
demonstrated that home blood pressure monitoring with electronic communication through
secure email with a clinical pharmacist nearly doubled the number of people whose blood
pressure was controlled (Greene et al., 2008). A randomized trail done in 2009, showed
improved glycemic control in patients with Type 2 diabetes who had home glucose monitoring
with electronic communication with a care manager (Evert, Trence, Catton & Huynh, 2009).
Secure email access between provider and patient has also demonstrated improved care time and
time again.
Future MU requirements may require that patients will control what clinicians can access
from their data. This is called a shared data accountability model. This model prompts the
question that if patients are directing the contents of their medical records should they shoulder
more of the burden of responsibility. Currently if a patient omits sharing information, clinicians
are not responsible for the burden of that liability (personal conversation, Jutta Williams, July 17,
2012). There is also a case to be made that withholding information may increase health care
costs (unnecessarily repeating tests, etc.). How will privacy and secrecy, when secrecy may be
considered harmful, play out as patients manage their own health data? Will there truly be a
shared accountability? This is yet to be seen.
TOO MUCH DATA, NOT ENOUGH DATA 28
The Provider–Patient Relationship and Data Exchange
Provider patient trust is a two way relationship that has the real potential of being placed
in jeopardy because of information exchange. Balancing patients’ autonomy and best interests
may be difficult at times, but it should always be presumed that the provider’s role is patient-
focused. The provider must trust that patients have given them accurate information. This
relationship was previously encapsulated, but “with the advent of interoperable ERHs this
encapsulated trust relationship is exposed. It exposes both information about the patient and
what the provider did – or did not – do” (Francis, 2010, p. 37).
Public support of electronic health information exchange is crucial moving forward. In a
2012 Cornell University study by Ancker, Edwards, Miller, & Kaushal, 2012). New York
residents supported HIE among healthcare providers believing it would improve their medical
care. They also supported emergency data access without consent. Survey respondents
expressed some concerns about privacy and security but were supportive whether the
architecture involved a provider sending data to another provider, a provider sending data to a
patient who would then pass it on to another provider, or a provider accessing data from other
institutions.
In light of potential patient concerns about privacy, the National Committee on Vital
Health Statistics has argued that patients should be able to mask defined categories of sensitive
health information in interoperable EHRs. “If patients only have the option to opt into or out of
a system, they have no guarantee that information in their records is seen on a limited, need-to-
know basis” (Watson, 2006, p.2).
TOO MUCH DATA, NOT ENOUGH DATA 29
Patients are increasingly entering their own data into personal health records related to
their insurance companies or internet health website. In many institutions this information
becomes part of the system’s EHR (Francis, 2010).
There is no argument that interoperable electronic medical records create new, more
powerful, and more accurate means for oversight that allows trust to be validated by structures
external to the physician-patient relationship. But, they also “create new, more powerful means
for access to individual information that require in turn transparency, patient consent and
oversight of how the data are used if patient trust is to be maintained” (Francis, 2010, p. 46).
Trusting of Exchanged Data
A critically ill neonate is transferred to a tertiary NICU after delivery. The infant’s
mother had tested negative for Group B strep prior to delivery. This testing was done in another
health network. Can this data be trusted or should the test be repeated? Clinicians often trust the
familiar and can be very context dependent. A radiology reading performed by a colleague holds
much more credence than does a reading by a radiologist in another system. Electronic data
from another facility can certainly compound the uncertainty of an already precarious situation.
What makes exchanged data trustworthy? This has become a new question in medical
informatics and very little information has been published on this subject. Jay Jacobsen, a
medical ethicist and infectious disease physician at the University of Utah defines three issues
with trusting electronic data: 1) The originator of the data is unknown, 2) The effort of obtaining
the data is often based on convenience, and 3) Providers have been taught to be suspicious and to
think independently (personal communication, June 22, 2012).
Statistics show that for every five out of 100 electronic transfers of data there is difficulty
associating the correct data to the right patient. One figure implies that 20% of data exchanged
TOO MUCH DATA, NOT ENOUGH DATA 30
nationally may be wrong. Placed in a community data exchange perspective, only six out of 10
data elements may be accurate (Rand Survey, 2011). Obviously this rate is unacceptable, but
until precision is improved, do clinicians turn their backs on the data elements that are accurate?
Many clinicians would admit their clinical practice is driven by worries of risk. There
must be a change in this mentality. There is risk in everything and this is a world of uncertainty.
Clinicians need to be reminded the likelihood of all things being equal, the patient will be better
served if data is shared. The term “status quo ante data” needs to be changed to “status quo data
exchange”. Trust must begin to be used in appropriate ways. Only then will health care
providers begin to improve efficiency and health care costs.
Patients as the Gatekeepers – Personally Controlled Health Records
In the not too distant past, a patient’s access to his medical records was extremely
limited. The wrath of the nurse could be fierce when a patient or family member was caught
reading the nurses notes which were hung temptingly at the end of the bed. Gradually the
pendulum has swung the other way. A new paradigm of information sharing and patient access
has recently been seen in Brazil. The provider writes the order for the lab tests, but the patient is
responsible for selecting the lab. The results are returned only to the patient and he must notify
the provider of the results.
In the United States, Weitzman, Helemen, Kaci, & Mandl, (2009) recently promoted an
innovative approach for bringing improved data into the clinical arena called the personally
controlled health record (PCHR). “This is an individually controlled Web-based platform that
integrates personally reported, as well as clinically and administratively sourced data over sites
of care and time” (p.2). Currently PCHRs are not standards driven and few provide simple
methods for transporting records among different EHR products. Recently Microsoft and
TOO MUCH DATA, NOT ENOUGH DATA 31
Google, who both maintain web-based PCHRs, agreed to allow exchange of information
between their respective PCHR systems without charge to the patient (National Health
Information Network, 2010).
A survey of over 500 patients, obtained by Friction and Davies (2009) showed extreme
interest by both clinicians and patients in using a similar concept, called a Personal Health
Record (PHR). This would routinely be used for accessing and exchanging health information,
including medication reconciliation, patient history and education. A positive element of
personal health records is that they are “owned” by the patient which imparts the beginnings of
interoperability.
One of the tenets of future Meaningful Use requirements has patients controlling their
own health information. Eva Powell (2012), the director of health information technology
programs at the National Partnership for Women and Families believes this is an extremely
positive thing for patients. It allows them to make choices down to a single data item level.
They may choose whether to share the fact that they are on a psychotropic medication, have been
recently treated for a sexually transmitted infection (STI) or had an abortion at age sixteen.
Powell believes it is a concept whose time has come. Or has it?
From an informatics standpoint, it could be very difficult to offer the required MU
technology to allow these choices to be easily selected and blocked. These are high expectations
which may require extensive time and expensive development platforms. From a provider
standpoint, are we allowing the patient to practice medicine? If the patient will soon be
delivering a baby, is the psychotropic medication they are taking, the abortion at age sixteen and
previous STI important information that could impact the delivery and health of the mother and
newborn. This goes back to the concepts of relevance and pertinence. Regardless of the
TOO MUCH DATA, NOT ENOUGH DATA 32
concerns, a new nursing role will emerge that will require education to help patients understand
the implications about the data they choose not to disclose.
A study reviewing attitudes of pediatric patients and their families regarding data sharing,
reported that a majority of patients/families were willing to share personal health information
with other providers to support patient care or public health reviews which support health
supervision and research. They expressed concern about sharing family income and
transmittable disease information. Willingness to share health data by category was not
associated with patient’s age, race or health status, the number of children in the household or
income. “There was no association between reported income level and willingness to share with
public health in any information category” (Weitzman et al., 2009, p. 2).
The National Health Information Exchange (2012) believes the participation of patients
in their own healthcare could substantially improve care, especially in the management and
treatment of chronic conditions such as diabetes and obesity. Access to electronic personal
health information and interfaces make it easy for the public and private healthcare organizations
to enable providers and patients to collaborate in informed decision making.
There may also be significant cultural barriers related to sharing of PHI. These barriers
appear important but at this point in time have not yet been well defined.
What Constitutes Appropriate Data?
Work done by Van Vleck et al. (2007) suggests the feasibility and benefits of an
automated patient summary sheet in the primary care arena to recap key pieces of information, is
essential. It should also be deemed essential to have a deeper understanding of what
information is of most importance to providers when reviewing a patient’s medical record. This
understanding has begun to be explored by this project.
TOO MUCH DATA, NOT ENOUGH DATA 33
In an exploratory study that looked at factors which motivated and affected HIE usage by
Vest, Jasperson, Hongwei, Gamm & Ohsfeldtl. (2011), several important inferences were made
related to relevant data requirements and patient type:
1. While HIE provides access to previously inaccessible externally generated
information, not every encounter requires that type of information such as patients with
select conditions or injuries.
2. The main advantage of HIE appears to be access to diagnostic tests, existing
treatments and previous diagnoses.
3. Patient complexity and usage are correlated.
4. Time constraints present a barrier to HIE usage indicating that information must be
valuable enough to motivate the provider to spend time accessing it.
5. Directly placing the information made available by HIE into the organization’s HIE
removes barriers to seeking information.
6. For complex patients, the minimum information provided by the HIE system is not
sufficient.
7. Usage was less likely in emergency departments for unfamiliar patients. Patient
familiarity was deemed undesirable because it is indicative of patients with inappropriate
sources of care.
8. There appears to be a relationship between facility repeat patients, and the association
between payer type and usage (p.147).
In a series of structured interviews with residents at New York-Presbyterian Hospital,
Van Vleck et al. (2007) attempted to identify phrases in the medical record that each physician
perceived to be relevant when describing a patient’s history. Primary data sources for provider
TOO MUCH DATA, NOT ENOUGH DATA 34
review included all types of clinical data. Discharge summaries were excluded to persuade
clinicians to use other primary data sources.
During the structured interview process, physicians underlined 824 phrases that they
considered relevant to explaining the patient’s history. Subjects developed a list of
categories considered relevant to the process of patient familiarization and applied one to
each phrase of interest. These categories included: labs and tests, problem and
treatment, history, findings, allergies, meds, plan and identifying information (p. 763).
In every instance, the resident first located the admission note and read it thoroughly.
They next skimmed through the progress notes until they reached the last one. All study
participants said they would have referenced the discharge summary if it had been made
available. Simple rules based on location in the medical record may provide a useful start to
identifying data to include in a summary. The resident reviews mimicked the traditional
categories of the medical record. “Providers follow this methodology and hence future work
summarizing patient history should consider this structure, as it is core to the clinical thought
process” (Van Vleck, et al., 2007, p. 763).
Van Vleck et al. (2007) also attempted to study how providers visualize lab result trends
by mirroring everyday working conditions. Study results identified the importance of logical
tools that could aid in the rapid understanding of large volumes of information (such as graphs or
charts representing laboratory data).
Are the data requirements different between specialties and the patients they care for?
Vest et al. (2011) asserts that previous research argues for the examination of information
technology in children separately from adult populations due to the particular vulnerabilities and
unique needs of this population. Zeng, Climino and Zou. (2002) maintain that dependent on the
TOO MUCH DATA, NOT ENOUGH DATA 35
clinical tasks at hand, only certain subsets of data (referred to as views) are of interest to
providers. Providing appropriate views may be one way to address the problem of too much
data.
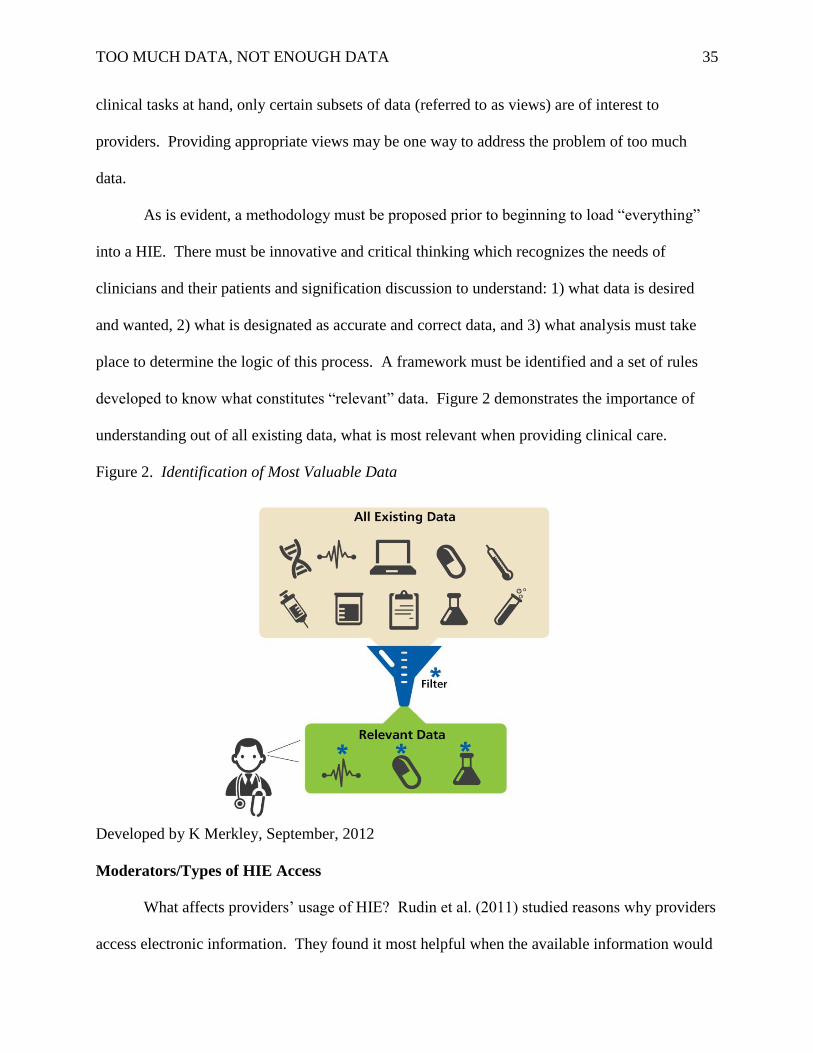
As is evident, a methodology must be proposed prior to beginning to load “everything”
into a HIE. There must be innovative and critical thinking which recognizes the needs of
clinicians and their patients and signification discussion to understand: 1) what data is desired
and wanted, 2) what is designated as accurate and correct data, and 3) what analysis must take
place to determine the logic of this process. A framework must be identified and a set of rules
developed to know what constitutes “relevant” data. Figure 2 demonstrates the importance of
understanding out of all existing data, what is most relevant when providing clinical care.
Figure 2. Identification of Most Valuable Data
Developed by K Merkley, September, 2012
Moderators/Types of HIE Access
What affects providers’ usage of HIE? Rudin et al. (2011) studied reasons why providers
access electronic information. They found it most helpful when the available information would
TOO MUCH DATA, NOT ENOUGH DATA 36
save time, help them avoid phone calls, when patients had trouble communicating, and to review
a pattern of patient visits (numerous clinics), and if there was ease of data access. Providers did
not find information helpful when it had gaps or was difficult to access or when notes were
locked (Shapiro, Kannry, Kushniruk & Kuppman, 2007).
Particular medical specialties showed different patterns of utilization. There was
intensive use amongst hospitalists and specialty services when caring for inpatients. ED
practitioners and pediatricians were more likely to access information when the patient history
was incomplete. Pathologists did not find the electronic information helpful, and no primary
care providers were studied. Regardless, the study stressed that for adoption the system must be
easy to use, meaningful data must be passed and it must fit provider workflows. (Shapiro,
Kannry, Kushniruk & Kuppman, 2007)
Gadd, Ho, Cala, Blakemore, Chen & Frisse, (2010) from Vanderbilt University looked at
a combination of factors related to user views on HIE usability in a product they were
implementing. They used a “technology acceptance model” called TAM. They determined that
the perception of a HIE was positive and that the product needed to be easy to use and provide
applicable information.
Hayrinen, Saranto, & Nykanen, (2007) in a review of the research literature looked at 55
studies related to the exchange of health information in Finland. Positive factors for adoption
identified included the quality of the data and the criteria of completeness and accuracy.
Structured data entry seemed to include more detailed data.
O’Malley, Grossman, Cohen, Kemper, & Pham (2009) suggest that a patient summary
may be the most appropriate way to establish electronic health information interoperability. A
patient summary includes patient history, allergies, active problems, test/procedure results, and
TOO MUCH DATA, NOT ENOUGH DATA 37
medications. However, further information can be included, depending on the intended purpose
of the summary and anticipated context of use. At the present time the CCC is sharing only part
of the patient summary (allergies, active problems and medications).
Accessing Appropriate Data
An understanding of how providers access data has been described in a classic study by
Krikelas (1983). The study identifies two types of activities, the first identified as “information
gathering” such as journal reading to keep current and “information seeking” which is done to
meet a perceived need for additional information. Before beginning to seek information, the
provider must decide whether to pursue new information at all.
Gorman and Helfund (1995) disclose results of a study of office-based physicians which
revealed that although as many as two questions arose for every three patients they cared for,
only 30% of these questions were actively pursued. They studied factors which motivated
primary care providers to answer clinical questions. It was determined that these providers were
more likely to pursue an answer to a question if they knew a definitive answer existed or if they
concluded that patient’s condition was urgent.
They report, “primary care providers are concerned and curious, but busy and practical.
While caring for patients, they have many questions about optimal management, but they invest
their time and effort pursuing questions only when they expect a direct, immediate benefit,”
(Gorman & Helfund, 1995, p. 118). Implications for accessing data can be extrapolated from
this study in that the provider must be shown straightforward and immediate benefits to help
solve the problems of patient care. No amount or type of data given to a provider can improve
patient care unless it is accessed. A goal should be established which requires delivery of data
providing timely answers to all clinical questions.
TOO MUCH DATA, NOT ENOUGH DATA 38
Zeng, et al. (2002) reasons all types of medical data can be categorized into three groups
– source-oriented views (which organize data on the basis of where they were collected); time-
oriented views (which primarily use time to organize data); and concept-oriented views (which
center on clinical concepts, such as diseases or organ systems (p. 294). They hypothesize that
instead of presenting caregivers with patient data in chronological order, organized by the source
of the information (labs, radiology), a knowledge based system organized around clinical
concepts such as disease or organ systems is a better way to present information, improve
retrieval precision and reduce the information burden.
When using concept oriented views, a user would enter a clinical term and select from a
list of matching concepts. For example if a patient has congestive heart failure, after selecting
“Radiology Reports”, the system returns a list of radiology reports related to congestive heart
failure. This structure shows exciting potential for reducing information overload. “On average,
each concept-oriented view contained only a fraction of all information about patients,” making
the process more time efficient (Zeng et al., 2002, p 300).
An ethnographic qualitative study done by Unertl, Johnson, & Lorenzi (2012) studied six
Memphis emergency departments (EDs) and eight ambulatory clinics in an attempt to understand
the relationship between HIE and clinical workflows at multiple sites. Two key workflow
processes surfaced across these sites. Nurse access to the system was motivated to identify
recent hospital visits with a goal to retrieve specific information for licensed independent
practitioners (LIP) use. LIPs use of the HIE was more global. The authors believe their research
“addressed a significant gap in the knowledge about the front-line impact of HIE on patient care
delivery” (p. 400). They also believe that the impact of a HIE system on patient care rarely
delivers clear-cut financial benefits.
TOO MUCH DATA, NOT ENOUGH DATA 39
It is also important to consider the possibility of bringing forward historical compliance
information? Did the patient fill all his scripts, cancel an appointment, or go to an alternative
health care provider? How many times did the patient access data online, delete data or initiate
corrections. This information would provide important compliance details which could be
factored into the total equation.
Presentation of Received Data
Once data has been received from another healthcare organization it should be presented
to clinicians using data visualization tools that have meaning to clinicians. These visualization
tools must display connections between different data presentations. Should data received be
presented to clinicians in a single document form or incorporated into the patient’s current
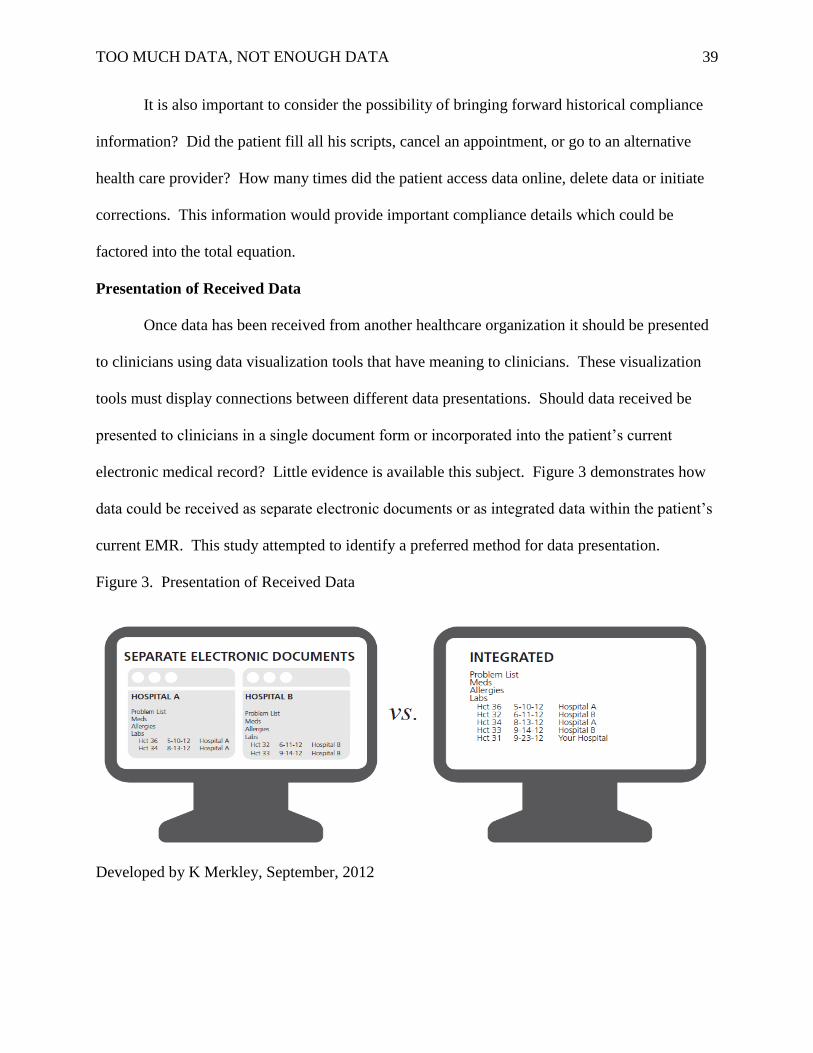
electronic medical record? Little evidence is available this subject. Figure 3 demonstrates how
data could be received as separate electronic documents or as integrated data within the patient’s
current EMR. This study attempted to identify a preferred method for data presentation.
Figure 3. Presentation of Received Data
Developed by K Merkley, September, 2012
TOO MUCH DATA, NOT ENOUGH DATA 40
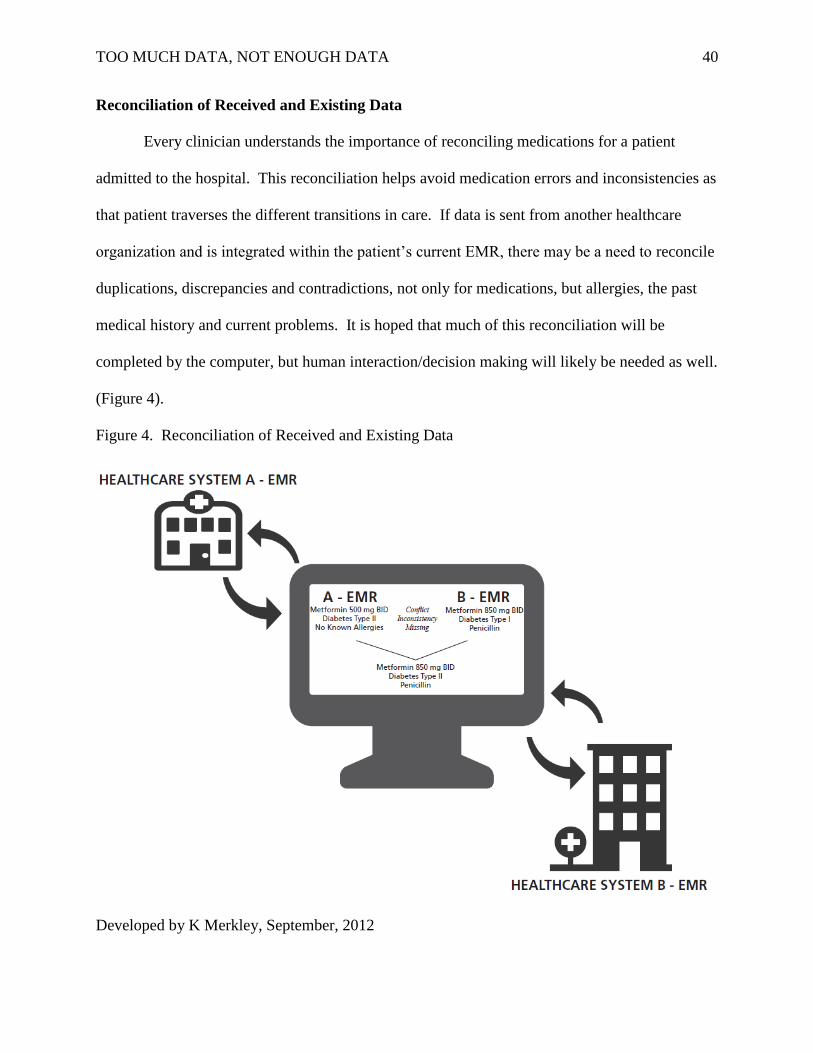
Reconciliation of Received and Existing Data
Every clinician understands the importance of reconciling medications for a patient
admitted to the hospital. This reconciliation helps avoid medication errors and inconsistencies as
that patient traverses the different transitions in care. If data is sent from another healthcare
organization and is integrated within the patient’s current EMR, there may be a need to reconcile
duplications, discrepancies and contradictions, not only for medications, but allergies, the past
medical history and current problems. It is hoped that much of this reconciliation will be
completed by the computer, but human interaction/decision making will likely be needed as well.
(Figure 4).
Figure 4. Reconciliation of Received and Existing Data
Developed by K Merkley, September, 2012
TOO MUCH DATA, NOT ENOUGH DATA 41
Questions related to reconciliation of data were also addressed in this scholarly project.
They included asking if a clinician should be required to reconcile data between two institutions,
and if reconciliation was mandated who should perform it (the LIP caring for the patient in the
receiving institution, the nurse caring for the patient in the receiving institution, the first licensed
care giver encountering the patient in the receiving institution or should reconciliation be
dependent on the type of data shared; such as a pharmacist reconciling medications, a physician
reconciling labs and a nurse reconciling patient goals)?
Are Data Requirements Different Between Caregivers and Patient Types?
It is important to remember the amount and quality of information available to health care
professionals in patient care has an impact both on the outcomes and continuity of that care,
Hayrinen et al. (2007). With that mandate in mind it must be understood that all providers
access data at various times and in various ways.
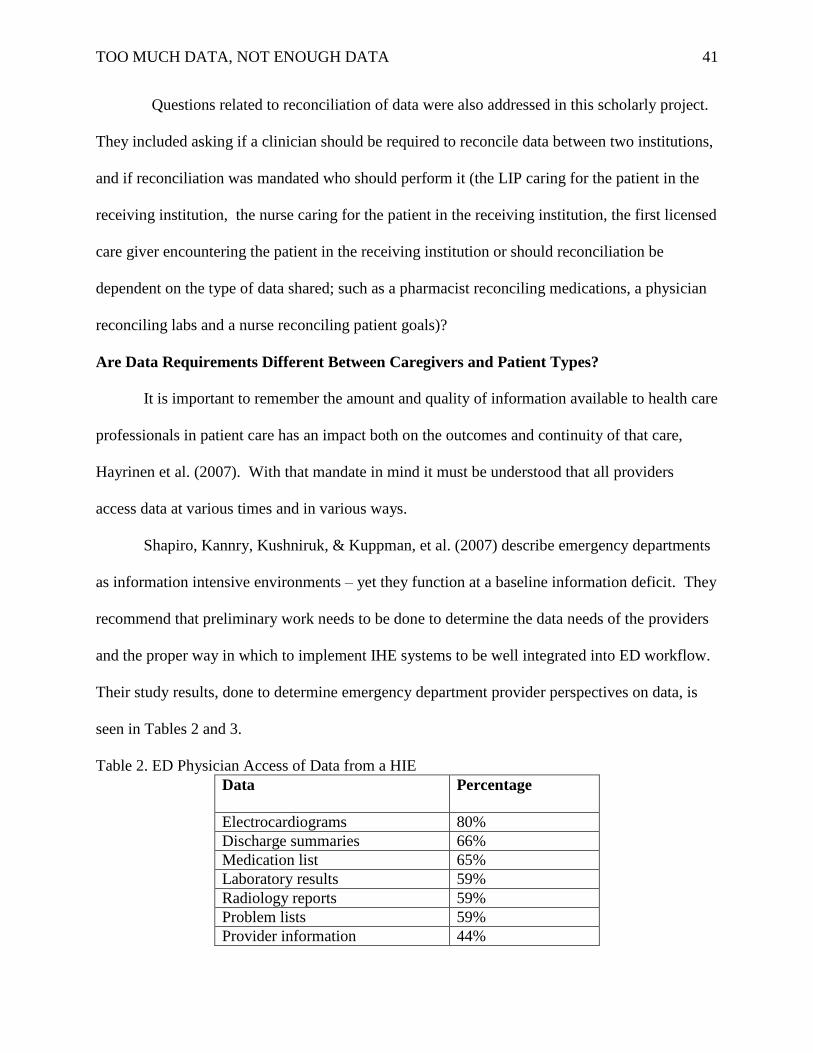
Shapiro, Kannry, Kushniruk, & Kuppman, et al. (2007) describe emergency departments
as information intensive environments – yet they function at a baseline information deficit. They
recommend that preliminary work needs to be done to determine the data needs of the providers
and the proper way in which to implement IHE systems to be well integrated into ED workflow.
Their study results, done to determine emergency department provider perspectives on data, is
seen in Tables 2 and 3.
Table 2. ED Physician Access of Data from a HIE
Data
Percentage
Electrocardiograms 80%
Discharge summaries 66%
Medication list 65%
Laboratory results 59%
Radiology reports 59%
Problem lists 59%
Provider information 44%
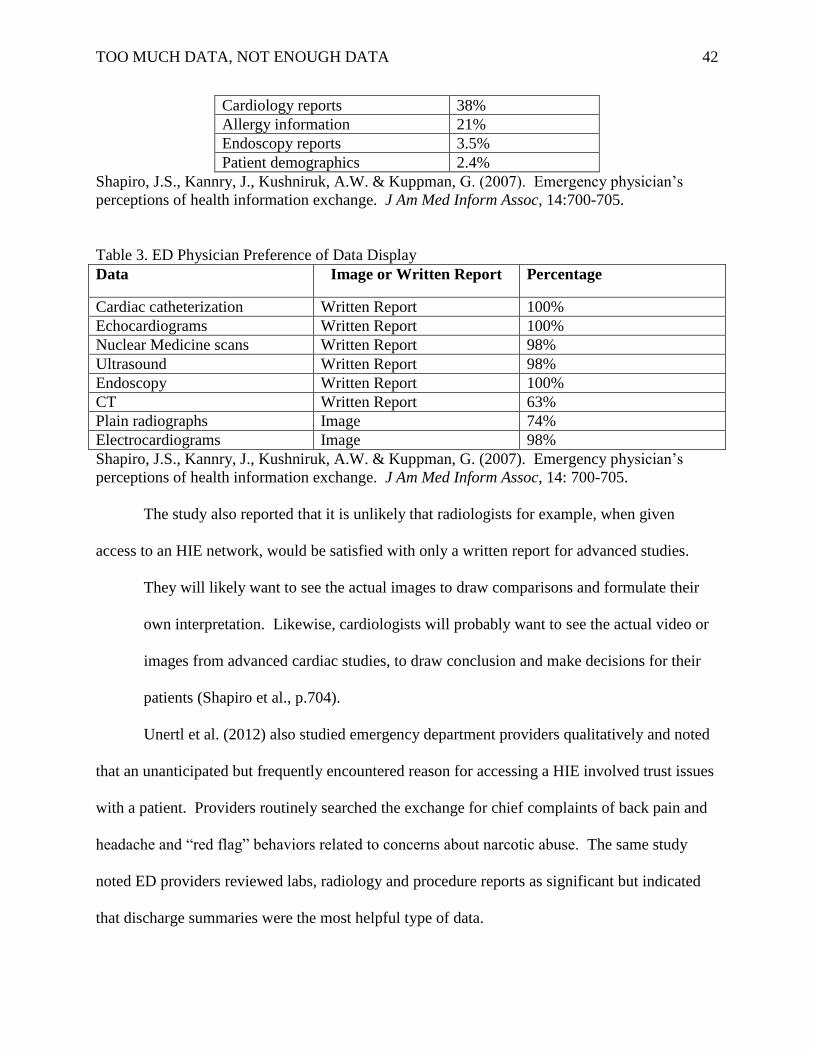
TOO MUCH DATA, NOT ENOUGH DATA 42
Cardiology reports 38%
Allergy information 21%
Endoscopy reports 3.5%
Patient demographics 2.4%
Shapiro, J.S., Kannry, J., Kushniruk, A.W. & Kuppman, G. (2007). Emergency physician’s
perceptions of health information exchange. J Am Med Inform Assoc, 14:700-705.
Table 3. ED Physician Preference of Data Display
Data Image or Written Report Percentage
Cardiac catheterization Written Report 100%
Echocardiograms Written Report 100%
Nuclear Medicine scans Written Report 98%
Ultrasound Written Report 98%
Endoscopy Written Report 100%
CT Written Report 63%
Plain radiographs Image 74%
Electrocardiograms Image 98%
Shapiro, J.S., Kannry, J., Kushniruk, A.W. & Kuppman, G. (2007). Emergency physician’s
perceptions of health information exchange. J Am Med Inform Assoc, 14: 700-705.
The study also reported that it is unlikely that radiologists for example, when given
access to an HIE network, would be satisfied with only a written report for advanced studies.
They will likely want to see the actual images to draw comparisons and formulate their
own interpretation. Likewise, cardiologists will probably want to see the actual video or
images from advanced cardiac studies, to draw conclusion and make decisions for their
patients (Shapiro et al., p.704).
Unertl et al. (2012) also studied emergency department providers qualitatively and noted
that an unanticipated but frequently encountered reason for accessing a HIE involved trust issues
with a patient. Providers routinely searched the exchange for chief complaints of back pain and
headache and “red flag” behaviors related to concerns about narcotic abuse. The same study
noted ED providers reviewed labs, radiology and procedure reports as significant but indicated
that discharge summaries were the most helpful type of data.
TOO MUCH DATA, NOT ENOUGH DATA 43
In a 2011 study of a regional HIE of emergency departments and clinics, Johnson et al.
(2011) acknowledged users accessed the HIE just under seven percent of the time for all
encounters, with “higher rates of access for repeat visits, for patients with co-morbidities, for
patients known to have data in the exchange and at sites providing HIE access to both nurses and
licensed independent practitioners” (p. 609). Discharge summaries and lab results were most
frequently retrieved. Providers discerned that by having additional information, repeat testing
was prevented and hospitalizations were avoided.
Very little information is available to determine what the clinical information needs are
required for other specialties at this time. Similar studies with new study populations will need
to be conducted to gain this information. This project addressed some of the gaps in this area. It
is important that the process of building trust by providing relevant data begin now.
Theoretical Framework
T.S. Eliot asks, “Where is the wisdom we have lost in knowledge? Where is the
knowledge we have lost in information” (1934). The philosophical foundations of the Data-
Information-Knowledge-Wisdom (DIKW) framework will be utilized to guide this project. The
Graves and Corcoran (1989) article, “The Study of Nursing Informatics” identifies data,
information and knowledge as foundational concepts for this area of nursing.
In 2008, the American Nurses Association revised the Scope and Standards for Nursing
Informatics to include the additional concept of wisdom. Although this framework is based on
nursing informatics theory it can be useful to the health care community in general (Matney,
Brewster, Sward, Cloyes, & Staggers, 2011) and specifically to this project because the data
elements identified will be used to gain information and knowledge.
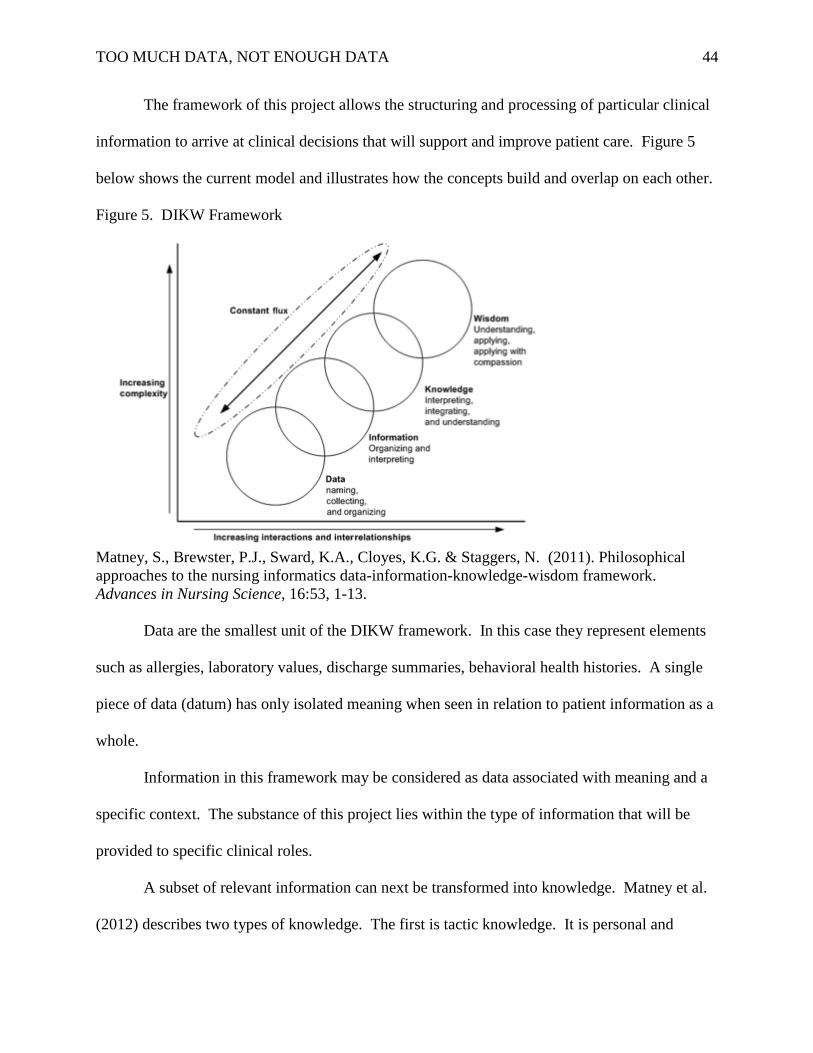
TOO MUCH DATA, NOT ENOUGH DATA 44
The framework of this project allows the structuring and processing of particular clinical
information to arrive at clinical decisions that will support and improve patient care. Figure 5
below shows the current model and illustrates how the concepts build and overlap on each other.
Figure 5. DIKW Framework
Matney, S., Brewster, P.J., Sward, K.A., Cloyes, K.G. & Staggers, N. (2011). Philosophical
approaches to the nursing informatics data-information-knowledge-wisdom framework.
Advances in Nursing Science, 16:53, 1-13.
Data are the smallest unit of the DIKW framework. In this case they represent elements
such as allergies, laboratory values, discharge summaries, behavioral health histories. A single
piece of data (datum) has only isolated meaning when seen in relation to patient information as a
whole.
Information in this framework may be considered as data associated with meaning and a
specific context. The substance of this project lies within the type of information that will be
provided to specific clinical roles.
A subset of relevant information can next be transformed into knowledge. Matney et al.
(2012) describes two types of knowledge. The first is tactic knowledge. It is personal and
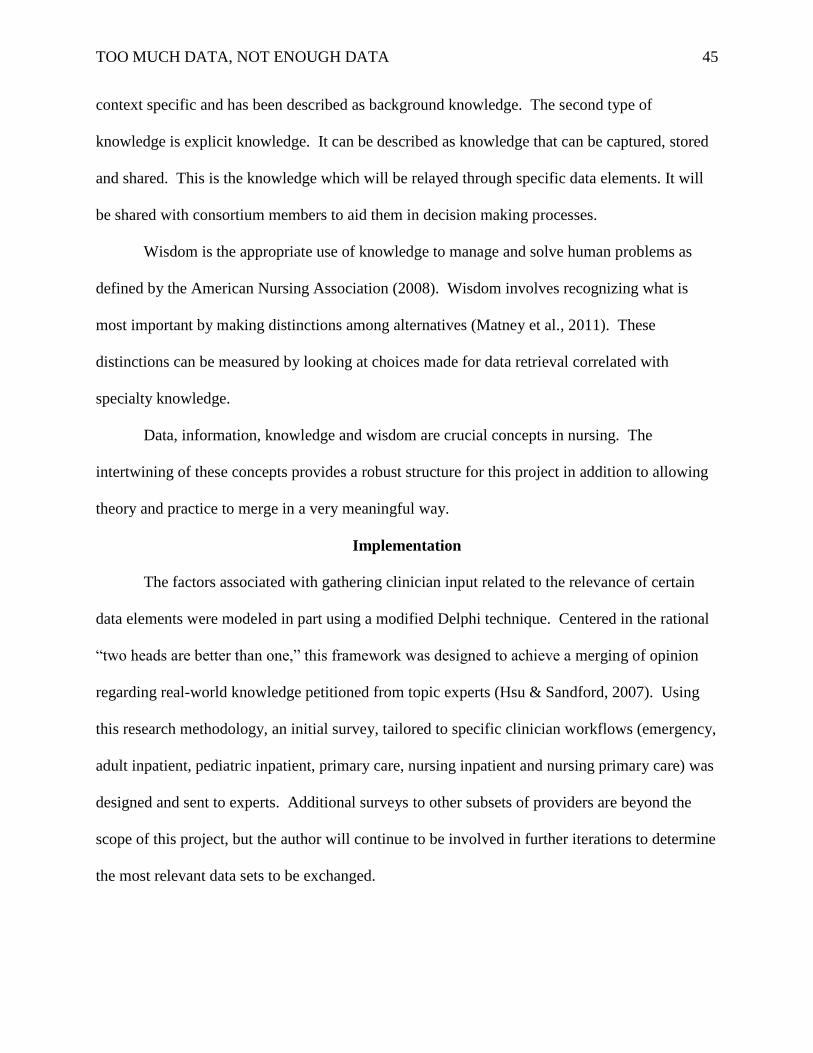
TOO MUCH DATA, NOT ENOUGH DATA 45
context specific and has been described as background knowledge. The second type of
knowledge is explicit knowledge. It can be described as knowledge that can be captured, stored
and shared. This is the knowledge which will be relayed through specific data elements. It will
be shared with consortium members to aid them in decision making processes.
Wisdom is the appropriate use of knowledge to manage and solve human problems as
defined by the American Nursing Association (2008). Wisdom involves recognizing what is
most important by making distinctions among alternatives (Matney et al., 2011). These
distinctions can be measured by looking at choices made for data retrieval correlated with
specialty knowledge.
Data, information, knowledge and wisdom are crucial concepts in nursing. The
intertwining of these concepts provides a robust structure for this project in addition to allowing
theory and practice to merge in a very meaningful way.
Implementation
The factors associated with gathering clinician input related to the relevance of certain
data elements were modeled in part using a modified Delphi technique. Centered in the rational
“two heads are better than one,” this framework was designed to achieve a merging of opinion
regarding real-world knowledge petitioned from topic experts (Hsu & Sandford, 2007). Using
this research methodology, an initial survey, tailored to specific clinician workflows (emergency,
adult inpatient, pediatric inpatient, primary care, nursing inpatient and nursing primary care) was
designed and sent to experts. Additional surveys to other subsets of providers are beyond the
scope of this project, but the author will continue to be involved in further iterations to determine
the most relevant data sets to be exchanged.
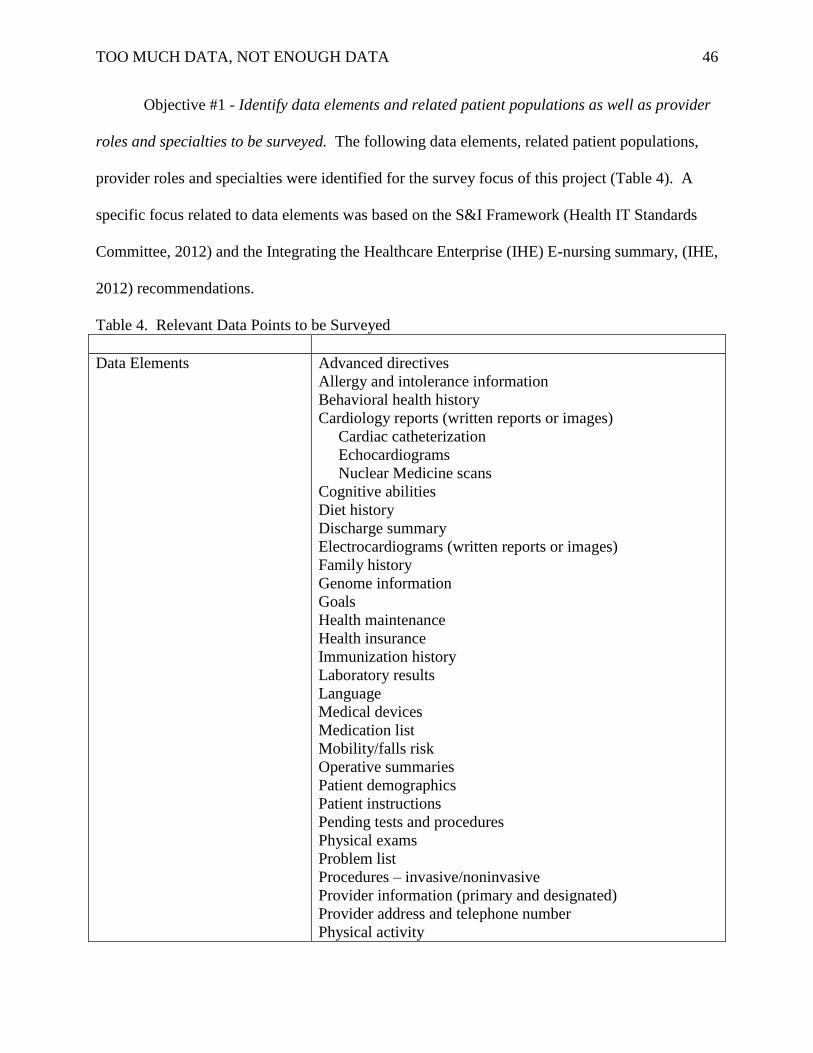
TOO MUCH DATA, NOT ENOUGH DATA 46
Objective #1 - Identify data elements and related patient populations as well as provider
roles and specialties to be surveyed. The following data elements, related patient populations,
provider roles and specialties were identified for the survey focus of this project (Table 4). A
specific focus related to data elements was based on the S&I Framework (Health IT Standards
Committee, 2012) and the Integrating the Healthcare Enterprise (IHE) E-nursing summary, (IHE,
2012) recommendations.
Table 4. Relevant Data Points to be Surveyed
Data Elements Advanced directives
Allergy and intolerance information
Behavioral health history
Cardiology reports (written reports or images)
Cardiac catheterization
Echocardiograms
Nuclear Medicine scans
Cognitive abilities
Diet history
Discharge summary
Electrocardiograms (written reports or images)
Family history
Genome information
Goals
Health maintenance
Health insurance
Immunization history
Laboratory results
Language
Medical devices
Medication list
Mobility/falls risk
Operative summaries
Patient demographics
Patient instructions
Pending tests and procedures
Physical exams
Problem list
Procedures – invasive/noninvasive
Provider information (primary and designated)
Provider address and telephone number
Physical activity
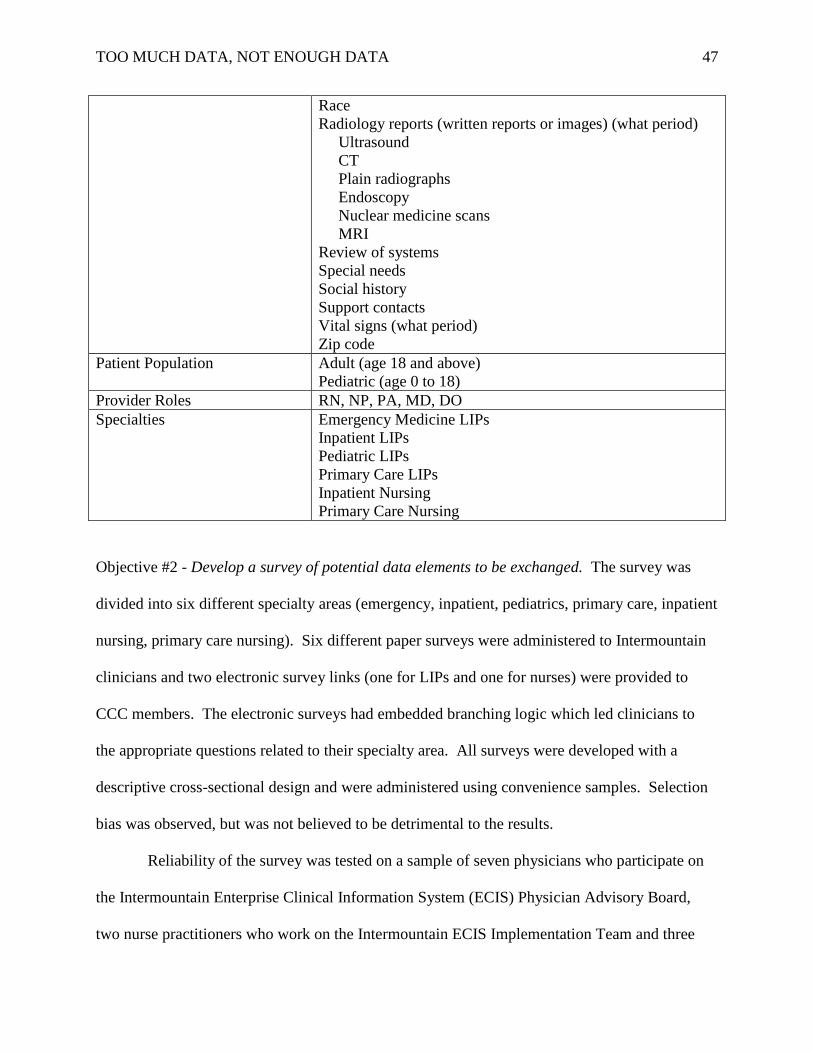
TOO MUCH DATA, NOT ENOUGH DATA 47
Race
Radiology reports (written reports or images) (what period)
Ultrasound
CT
Plain radiographs
Endoscopy
Nuclear medicine scans
MRI
Review of systems
Special needs
Social history
Support contacts
Vital signs (what period)
Zip code
Patient Population Adult (age 18 and above)
Pediatric (age 0 to 18)
Provider Roles RN, NP, PA, MD, DO
Specialties Emergency Medicine LIPs
Inpatient LIPs
Pediatric LIPs
Primary Care LIPs
Inpatient Nursing
Primary Care Nursing
Objective #2 - Develop a survey of potential data elements to be exchanged. The survey was
divided into six different specialty areas (emergency, inpatient, pediatrics, primary care, inpatient
nursing, primary care nursing). Six different paper surveys were administered to Intermountain
clinicians and two electronic survey links (one for LIPs and one for nurses) were provided to
CCC members. The electronic surveys had embedded branching logic which led clinicians to
the appropriate questions related to their specialty area. All surveys were developed with a
descriptive cross-sectional design and were administered using convenience samples. Selection
bias was observed, but was not believed to be detrimental to the results.
Reliability of the survey was tested on a sample of seven physicians who participate on
the Intermountain Enterprise Clinical Information System (ECIS) Physician Advisory Board,
two nurse practitioners who work on the Intermountain ECIS Implementation Team and three
TOO MUCH DATA, NOT ENOUGH DATA 48
nurses who attend the Intermountain System Informatics Nursing Council. An attempt was made
to find two clinicians from each specialty area and this was accomplished with the exception of
having only one primary care nursing representative test the survey. Variations in the inpatient
and primary care nursing surveys were minimal so reliability was considered adequate as results
correlated with the inpatient nursing and LIP surveys.
The survey took less than ten minutes to complete. The ten minute timeframe was
determined by observing the ECIS Physician Advisory Board and recording how long it took
them to complete the information. Institutional Review Board (IRB) approval was obtained from
the University of Utah and Intermountain Healthcare before data collection was begun
(Appendix A). Privacy of respondents was strictly protected. No participant information was
collected. Study materials were electronically stored in a secure file within the Intermountain
Study Quizmo tool. Only study personnel had access to the data. When it became apparent that
CCC responses would be limited, the author asked to include University of Utah physicians at
Primary Children’s Medical Center and the 2012 DNP cohort. An amendment application was
made to the IRB and approved (Appendix A).
Objective #3- Distribute survey to consortium members. The surveys were taken to the
CCC Network IT Board where it was presented for approval on October 22, 2012 (Appendix B).
Each consortium member was given the option to participate. Those members who agreed to
participate were given the electronic survey links and were responsible to disseminate the
information to each organization’s team leaders. These organization team leaders distributed the
survey link to clinical operation leaders (ex: a cardiology department chair at Mayo Rochester,
ED department chair at Kaiser-Permanente) who distributed them to appropriate clinicians in
each facility. The actual method of recruitment was defined by these clinical operation leaders.
TOO MUCH DATA, NOT ENOUGH DATA 49
The University of Utah 2012 DNP Cohort was also sent an electronic survey link and asked to
respond. CCC members and the University of Utah 2012 DNP Cohort answered 65 electronic
surveys.
Paper surveys were administered to Intermountain Healthcare clinicians from August 22
to November 9, 2012. LIP groups surveyed included the corporate Emergency Department
Development Team, hospitalist teams at Intermountain Medical Center and Primary Children’s
Medical Center, the Medical Informatics Primary Care User Group, and an ED nurse practitioner
group at PCMC. Two Intermountain primary care groups were also surveyed. Nursing groups
surveyed included the corporate Emergency Department Development Team, the Nursing
Informatics User Group (NUG) and the Integrated Care Management team.
Inclusion criteria for provider roles consisted of any registered nurse or licensed
independent practitioner (defined as MD, DO, NP, or PA). Response rates were expected to be
at least 25-30 per consortium member, but turned out to be much less. Intermountain
respondents answered 95 surveys. A pre-survey letter from Intermountain Healthcare’s CMO
was sent out prior to the survey link (Appendix C). An initial letter of invitation, which
contained the survey link for consortium members, was sent out two days later (Appendices D).
The pre-survey and invitation letters were attached to the paper survey for all Intermountain
clinicians (Appendices C & E). A thank-you email was sent to each person who responded
electronically (Appendix F). Verbal thanks were given to Intermountain paper survey
participants along with cookies/brownies.
Objective #4 – Analyze survey results and make recommendations regarding what
additional data elements should be included in CCC electronic data sharing. Data results were
collected by the researcher and analyzed by a statistician hired to review the results. Results
TOO MUCH DATA, NOT ENOUGH DATA 50
were calculated using Microsoft Excel. A report was compiled and shared with the CCC
Network IT board (Appendix G).
Evaluation Plan
Objective #1 - Identify data elements and related patient populations as well as provider
roles and specialties to be surveyed. The data elements used in this cross-sectional self-
administered survey were obtained using results from an extensive literature review. Inclusion
of patient populations, clinician roles and specialty recommendations came from CCC experts.
Validity of selected data elements were surmised because of the broad national and international
oversight provided by S&I Framework and the IHE E-nursing Summary.
Objective #2 - Develop a survey of potential data elements to be exchanged. Survey
reliability was verified using a small group of local Intermountain clinicians. Internal
consistency reliability was measured using Cronbach’s alpha, with a result of 0.81. Construct
validity was also measured using expert clinician assessments of the thoroughness of data
element options. This was achieved through the project’s content expert’s review. Internal
consistency was further measured by evaluating responses separated by consortium members,
after the results had been returned.
Objective #3- Distribute survey to consortium members. Success of this objective was
related to the number of responses received. No previous surveys had been administered to the
CCC. It was unclear what the response would be. The author was hopeful that between 125 and
150 surveys would be returned based on the large number of clinicians employed by these
healthcare corporations. Actual survey responses were approximately 159. No power was
assigned to the study because of its pilot nature.
The survey time line is outlined in Table 5 below:
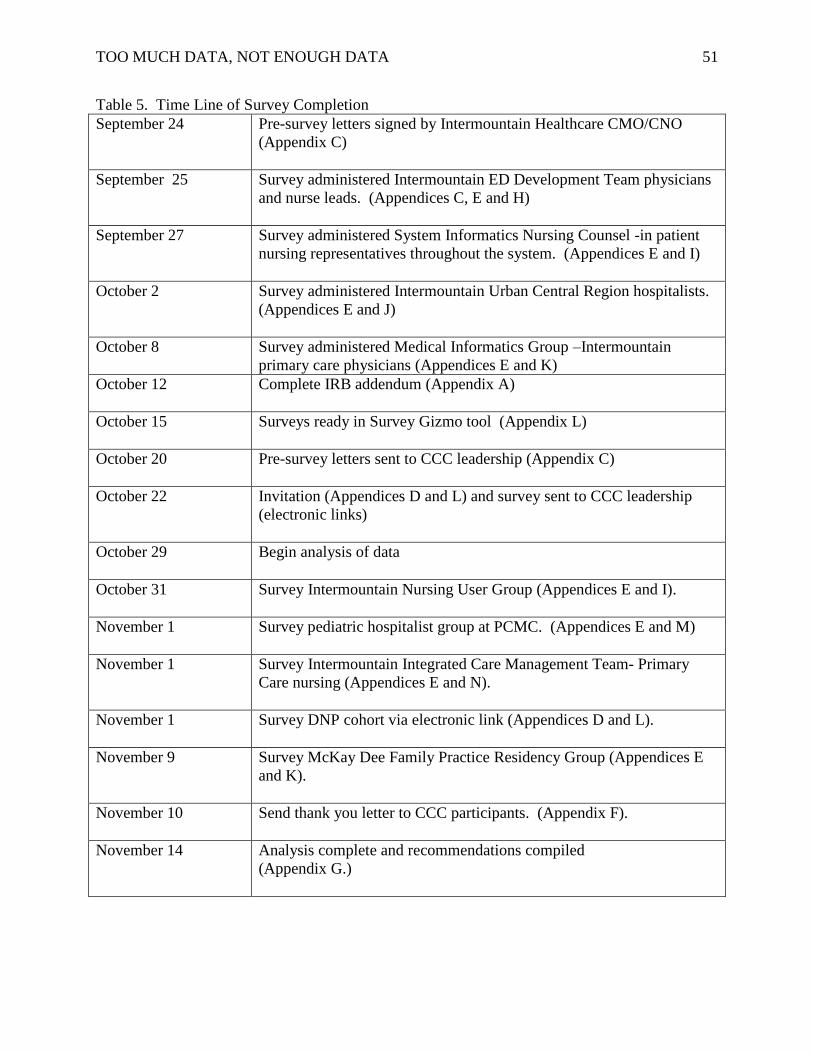
TOO MUCH DATA, NOT ENOUGH DATA 51
Table 5. Time Line of Survey Completion
September 24 Pre-survey letters signed by Intermountain Healthcare CMO/CNO
(Appendix C)
September 25 Survey administered Intermountain ED Development Team physicians
and nurse leads. (Appendices C, E and H)
September 27
Survey administered System Informatics Nursing Counsel -in patient
nursing representatives throughout the system. (Appendices E and I)
October 2 Survey administered Intermountain Urban Central Region hospitalists.
(Appendices E and J)
October 8 Survey administered Medical Informatics Group –Intermountain
primary care physicians (Appendices E and K)
October 12 Complete IRB addendum (Appendix A)
October 15 Surveys ready in Survey Gizmo tool (Appendix L)
October 20 Pre-survey letters sent to CCC leadership (Appendix C)
October 22 Invitation (Appendices D and L) and survey sent to CCC leadership
(electronic links)
October 29 Begin analysis of data
October 31 Survey Intermountain Nursing User Group (Appendices E and I).
November 1 Survey pediatric hospitalist group at PCMC. (Appendices E and M)
November 1 Survey Intermountain Integrated Care Management Team- Primary
Care nursing (Appendices E and N).
November 1 Survey DNP cohort via electronic link (Appendices D and L).
November 9 Survey McKay Dee Family Practice Residency Group (Appendices E
and K).
November 10 Send thank you letter to CCC participants. (Appendix F).
November 14
Analysis complete and recommendations compiled
(Appendix G.)
TOO MUCH DATA, NOT ENOUGH DATA 52
Objective #4 – Analyze survey results and make recommendations regarding what
additional data elements should be included in CCC electronic data sharing. Data analytics
included evaluation of relevant data by specialty, understanding of what constitutes trustable
data, emergent data that should be exchanged in the event of a life-threatening situation, time
limits of different types of data, presentation of received data and reconciliation of received and
existing data. This field assessment analysis was considered an exploratory investigation and in
many ways a cultural readiness assessment. An attempt was made to understand the actual needs
for data exchange. Programming requirements were in essences gathered and then refined using
descriptive statistical analysis.
Data relevance study findings will be submitted to the Care Connectivity Consortium
(CCC) Governing Board, IHE and HL7 (US standard governance boards). The final evaluation
relating to the success of this objective will be known if any or all of these recommendations are
incorporated into the actual CCC data exchange structure. The incorporation of the
recommendations is outside the scope of the DNP scholarly project. In addition, the author will
submit an article for publication to The Journal of the American Medical Informatics Association
and will apply to present at the American Medical Informatics Association (AMIA) and the
Health Information Management Systems Society (HIMSS) national conferences in 2013.
Project Results
Survey respondents equaled 159 (Table 6 for a breakdown of participants). Key
respondents for this project included Intermountain clinicians who willingly completed the data
relevance paper survey, the CCC clinicians and the 2012 University of Utah DNP cohort who
completed the electronic survey. A key barrier encountered was the length of time required for
IRB approval and the input of the surveys into the Intermountain survey tool. This led to a
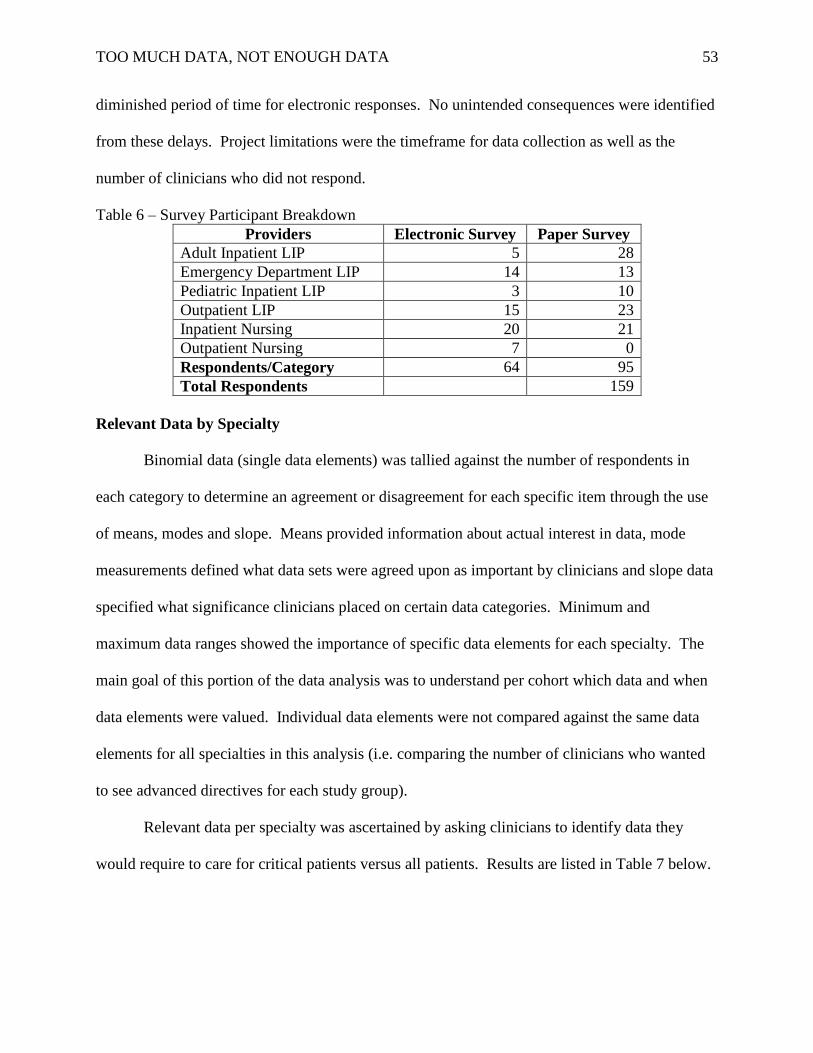
TOO MUCH DATA, NOT ENOUGH DATA 53
diminished period of time for electronic responses. No unintended consequences were identified
from these delays. Project limitations were the timeframe for data collection as well as the
number of clinicians who did not respond.
Table 6 – Survey Participant Breakdown
Providers Electronic Survey Paper Survey
Adult Inpatient LIP 5 28
Emergency Department LIP 14 13
Pediatric Inpatient LIP 3 10
Outpatient LIP 15 23
Inpatient Nursing 20 21
Outpatient Nursing 7 0
Respondents/Category 64 95
Total Respondents 159
Relevant Data by Specialty
Binomial data (single data elements) was tallied against the number of respondents in
each category to determine an agreement or disagreement for each specific item through the use
of means, modes and slope. Means provided information about actual interest in data, mode
measurements defined what data sets were agreed upon as important by clinicians and slope data
specified what significance clinicians placed on certain data categories. Minimum and
maximum data ranges showed the importance of specific data elements for each specialty. The
main goal of this portion of the data analysis was to understand per cohort which data and when
data elements were valued. Individual data elements were not compared against the same data
elements for all specialties in this analysis (i.e. comparing the number of clinicians who wanted
to see advanced directives for each study group).
Relevant data per specialty was ascertained by asking clinicians to identify data they
would require to care for critical patients versus all patients. Results are listed in Table 7 below.
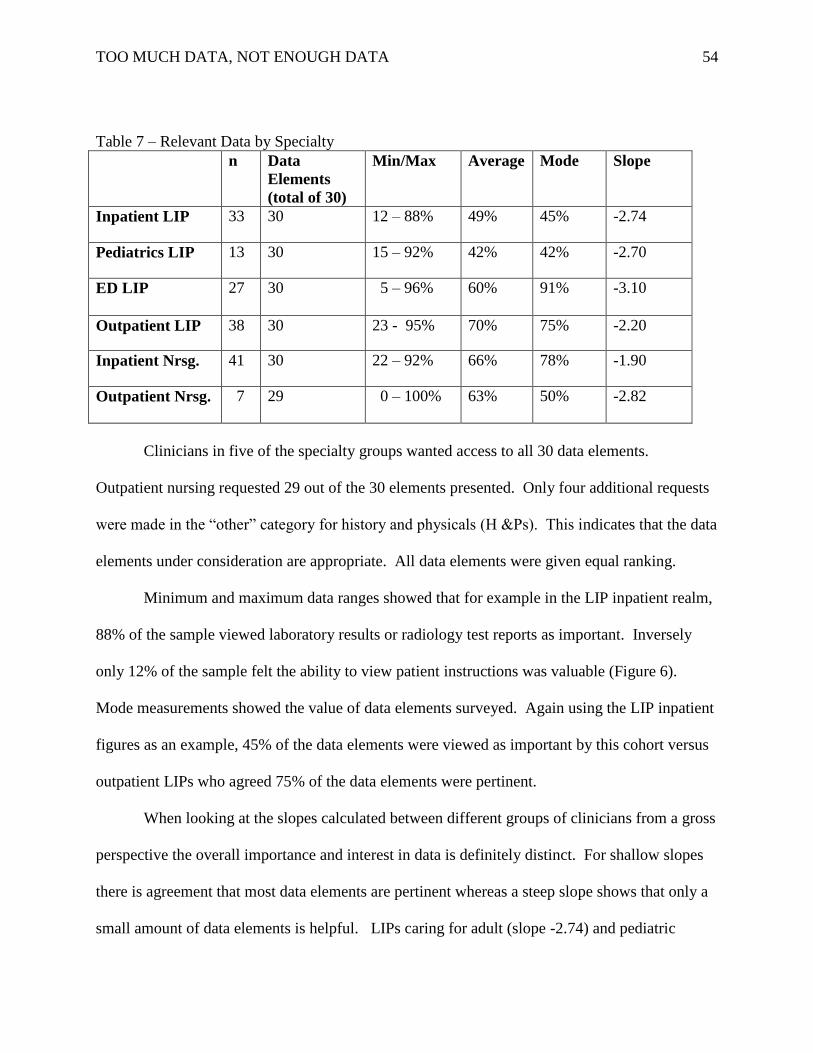
TOO MUCH DATA, NOT ENOUGH DATA 54
Table 7 – Relevant Data by Specialty
n Data
Elements
(total of 30)
Min/Max Average Mode Slope
Inpatient LIP 33 30 12 – 88% 49% 45% -2.74
Pediatrics LIP 13 30 15 – 92% 42% 42% -2.70
ED LIP 27 30 5 – 96% 60% 91% -3.10
Outpatient LIP 38 30 23 - 95% 70% 75% -2.20
Inpatient Nrsg. 41 30 22 – 92% 66% 78% -1.90
Outpatient Nrsg. 7 29 0 – 100% 63% 50% -2.82
Clinicians in five of the specialty groups wanted access to all 30 data elements.
Outpatient nursing requested 29 out of the 30 elements presented. Only four additional requests
were made in the “other” category for history and physicals (H &Ps). This indicates that the data
elements under consideration are appropriate. All data elements were given equal ranking.
Minimum and maximum data ranges showed that for example in the LIP inpatient realm,
88% of the sample viewed laboratory results or radiology test reports as important. Inversely
only 12% of the sample felt the ability to view patient instructions was valuable (Figure 6).
Mode measurements showed the value of data elements surveyed. Again using the LIP inpatient
figures as an example, 45% of the data elements were viewed as important by this cohort versus
outpatient LIPs who agreed 75% of the data elements were pertinent.
When looking at the slopes calculated between different groups of clinicians from a gross
perspective the overall importance and interest in data is definitely distinct. For shallow slopes
there is agreement that most data elements are pertinent whereas a steep slope shows that only a
small amount of data elements is helpful. LIPs caring for adult (slope -2.74) and pediatric
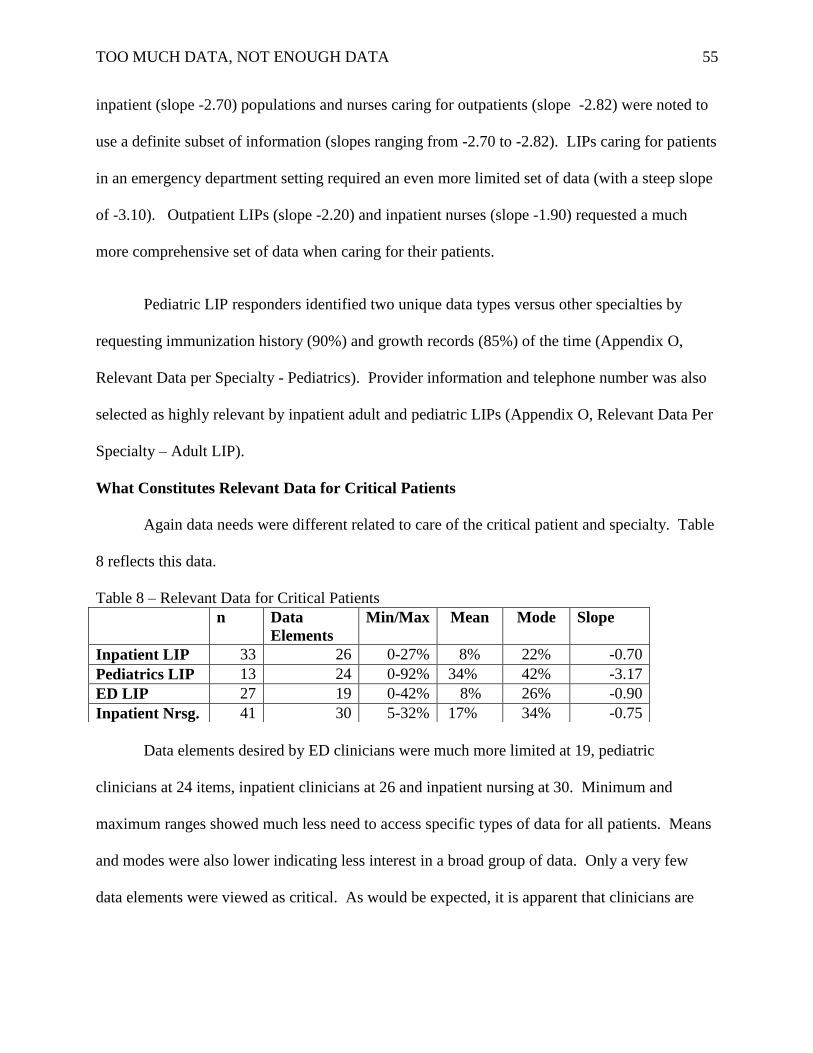
TOO MUCH DATA, NOT ENOUGH DATA 55
inpatient (slope -2.70) populations and nurses caring for outpatients (slope -2.82) were noted to
use a definite subset of information (slopes ranging from -2.70 to -2.82). LIPs caring for patients
in an emergency department setting required an even more limited set of data (with a steep slope
of -3.10). Outpatient LIPs (slope -2.20) and inpatient nurses (slope -1.90) requested a much
more comprehensive set of data when caring for their patients.
Pediatric LIP responders identified two unique data types versus other specialties by
requesting immunization history (90%) and growth records (85%) of the time (Appendix O,
Relevant Data per Specialty - Pediatrics). Provider information and telephone number was also
selected as highly relevant by inpatient adult and pediatric LIPs (Appendix O, Relevant Data Per
Specialty – Adult LIP).
What Constitutes Relevant Data for Critical Patients
Again data needs were different related to care of the critical patient and specialty. Table
8 reflects this data.
Table 8 – Relevant Data for Critical Patients
Data elements desired by ED clinicians were much more limited at 19, pediatric
clinicians at 24 items, inpatient clinicians at 26 and inpatient nursing at 30. Minimum and
maximum ranges showed much less need to access specific types of data for all patients. Means
and modes were also lower indicating less interest in a broad group of data. Only a very few
data elements were viewed as critical. As would be expected, it is apparent that clinicians are
n Data
Elements
Min/Max Mean Mode Slope
Inpatient LIP 33 26 0-27% 8% 22% -0.70
Pediatrics LIP 13 24 0-92% 34% 42% -3.17
ED LIP 27 19 0-42% 8% 26% -0.90
Inpatient Nrsg. 41 30 5-32% 17% 34% -0.75
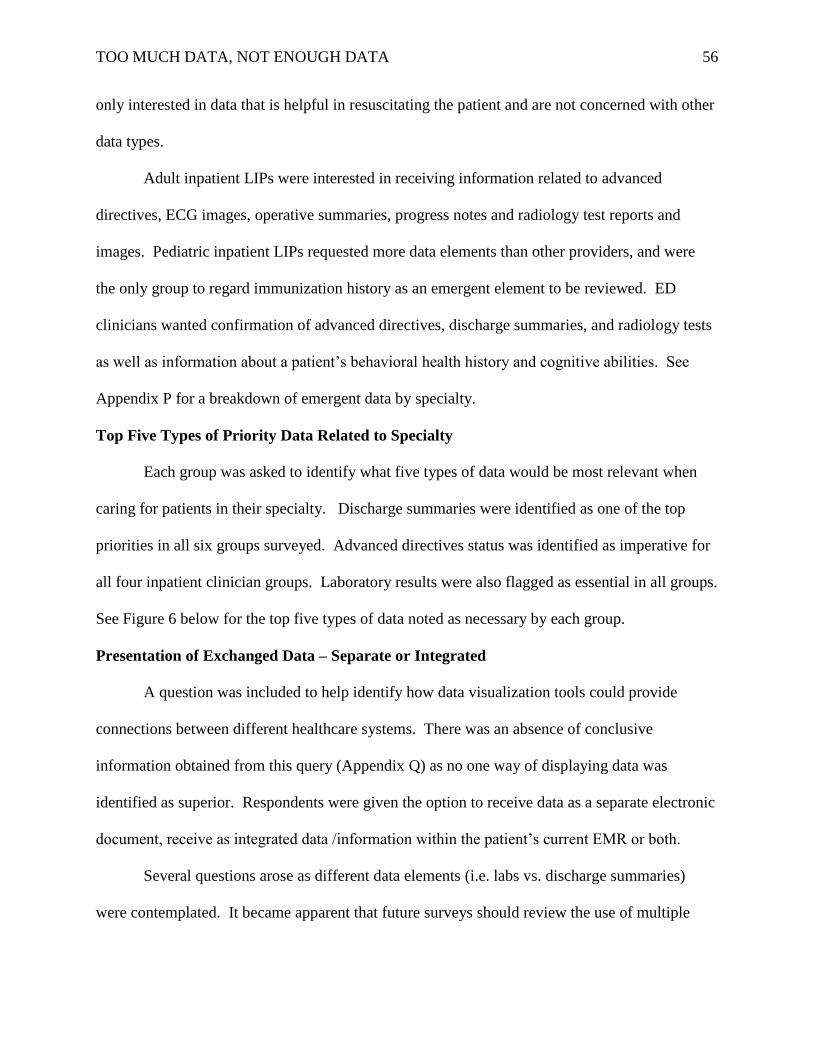
TOO MUCH DATA, NOT ENOUGH DATA 56
only interested in data that is helpful in resuscitating the patient and are not concerned with other
data types.
Adult inpatient LIPs were interested in receiving information related to advanced
directives, ECG images, operative summaries, progress notes and radiology test reports and
images. Pediatric inpatient LIPs requested more data elements than other providers, and were
the only group to regard immunization history as an emergent element to be reviewed. ED
clinicians wanted confirmation of advanced directives, discharge summaries, and radiology tests
as well as information about a patient’s behavioral health history and cognitive abilities. See
Appendix P for a breakdown of emergent data by specialty.
Top Five Types of Priority Data Related to Specialty
Each group was asked to identify what five types of data would be most relevant when
caring for patients in their specialty. Discharge summaries were identified as one of the top
priorities in all six groups surveyed. Advanced directives status was identified as imperative for
all four inpatient clinician groups. Laboratory results were also flagged as essential in all groups.
See Figure 6 below for the top five types of data noted as necessary by each group.
Presentation of Exchanged Data – Separate or Integrated
A question was included to help identify how data visualization tools could provide
connections between different healthcare systems. There was an absence of conclusive
information obtained from this query (Appendix Q) as no one way of displaying data was
identified as superior. Respondents were given the option to receive data as a separate electronic
document, receive as integrated data /information within the patient’s current EMR or both.
Several questions arose as different data elements (i.e. labs vs. discharge summaries)
were contemplated. It became apparent that future surveys should review the use of multiple
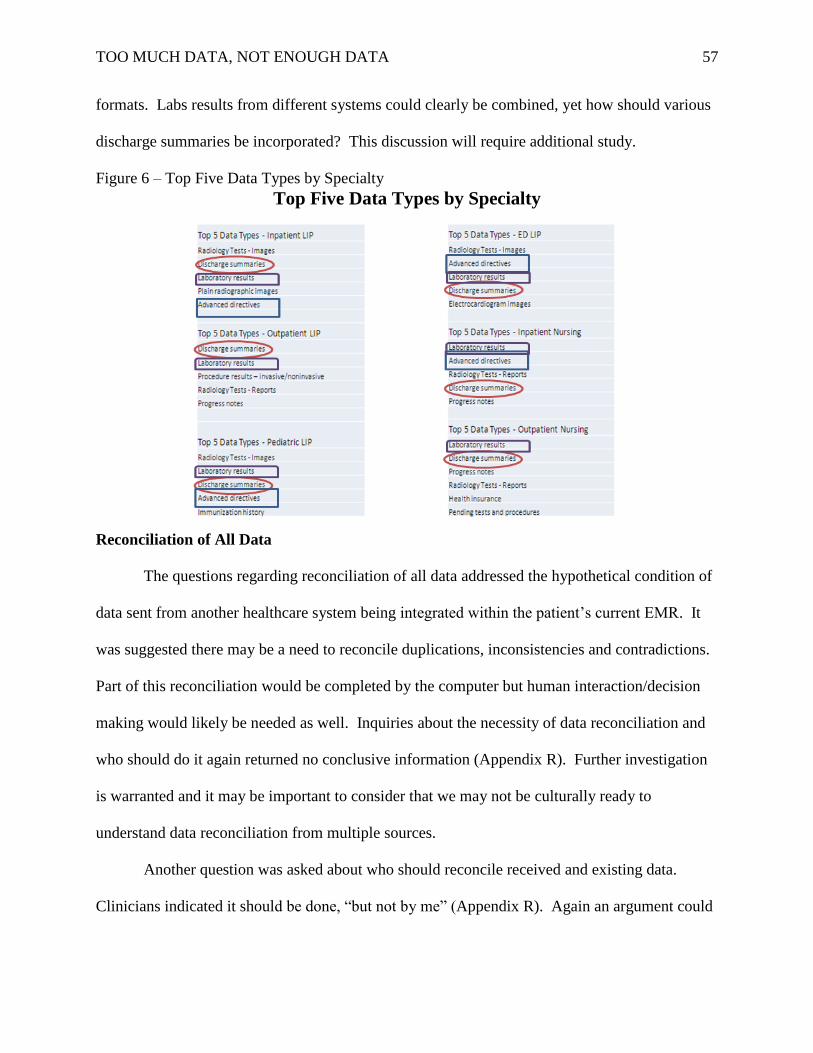
TOO MUCH DATA, NOT ENOUGH DATA 57
formats. Labs results from different systems could clearly be combined, yet how should various
discharge summaries be incorporated? This discussion will require additional study.
Figure 6 – Top Five Data Types by Specialty
Top Five Data Types by Specialty
Reconciliation of All Data
The questions regarding reconciliation of all data addressed the hypothetical condition of
data sent from another healthcare system being integrated within the patient’s current EMR. It
was suggested there may be a need to reconcile duplications, inconsistencies and contradictions.
Part of this reconciliation would be completed by the computer but human interaction/decision
making would likely be needed as well. Inquiries about the necessity of data reconciliation and
who should do it again returned no conclusive information (Appendix R). Further investigation
is warranted and it may be important to consider that we may not be culturally ready to
understand data reconciliation from multiple sources.
Another question was asked about who should reconcile received and existing data.
Clinicians indicated it should be done, “but not by me” (Appendix R). Again an argument could
TOO MUCH DATA, NOT ENOUGH DATA 58
be made that clinicians don’t have enough intellectual experience around this concept. This
question will also require additional study.
What Makes Data Trustworthy
Clinicians indicated overwhelming positive responses (very important or important) to
six of eight choices. The exceptions were questions related to provider type and reimbursement,
which are mixed. The take away message from this section indicates clinicians understand the
basic issues of data provenance and integrity and would use integrated data if it were cleansed
and readily available (Table 9).
Table 9 – What Makes Data Trustworthy?
Question Scale (1-5)
1. Strong working relationship with out of network provider 3.1
2. The reputation of the organization sending the data 3.6
3. Integrity of the health data exchange 4.1*
4. Knowing the type of provider who ordered the procedure 2.3
5. The complexity of the patient 3.3
6. Tests can be repeated and reimbursed 3.5
7. Data organized in a reliable, intuitive format 3.9*
8. Data integrity 4.2*
Time Limits of Different Types of Exchanged Data
Clinicians responded to eight questions asking about useful data ranges (from one 1 week
to five years) for vital signs, laboratory results, procedures, previously administered medications,
TOO MUCH DATA, NOT ENOUGH DATA 59
radiographs, electrocardiograms, problem lists and discharge summaries. Results showed bi-
modal distributions requesting data either immediately or long-term for labs, procedures,
radiographs, electrocardiograms, problem lists and discharge summaries Time ranges for
medications showed a varied distribution indicating clinicians wished to review a medication
history throughout the continuum of care. Vital signs data was identified by clinicians as to be
helpful only in the recent past (Figure 7).
DNP Essentials
The following Essentials of Doctoral Education for Advanced Nursing Practice criteria
from the American Association of Colleges of Nursing (2006) were addressed in this project:
Essential I: Scientific Underpinnings for Practice. An extensive literature review was
completed on this topic. A survey was then designed and the data collected was
statistically analyzed.
Essential II: Organizational and Systems Leadership for Quality Improvement and
Systems Thinking. Working with Intermountain and other CCC members, a survey was
designed representing all healthcare systems. It is thought that results will improve the
quality of patient care with better access to pertinent data.
Essential III: Clinical Scholarship and Analytical Methods for Evidence-Based Practice.
Use of evidence based practice guidelines helped form the basis of survey development.
Essential IV: Utilizing Information Systems/Technology for the Improvement and
Transformation of Health Care. Through the use of HIT and interoperability, content
obtained from this project and instituted through the CCC begins the process of data
transfer and subsequent healthcare transformation.
TOO MUCH DATA, NOT ENOUGH DATA 60
Essential VI: Interprofessional Collaboration for Improving Patient and Population
Health Outcomes. This project enables collaboration across numerous healthcare
organizations and specialties.
Essential VII – Clinical Prevention and Population Health for Improving the Nation’s
Health: Recommendations to the CCC and national standard governance bodies will
allow for pertinent transfer of data throughout the country promoting preventative and
improved health for those patients who participate in electronic health information
exchanges.
Essential VIII– Advanced Nursing Practice. Survey creation, administration and
subsequent recommendations will assist in improving the care of patients as they are
cared for in various healthcare organizations.
The stated criteria helped guide this project in an attempt to provide a deeper
understanding of the roles of organizational and system leadership as well as playing an
increased part in health care policy.
Discussion
Discussion of Main Findings
The data set gathered and surveyed appears to be sufficient for recommendations made to
the Care Connectivity Consortium and the standard organizations, IHE and H7. The survey
indicates that the more specific the clinician realm of care, the less data needed in caring for
patients. ED LIPs require a relatively limited subset of information, inpatient LIPs both in the
adult and pediatric realm require slightly more but primary care providers’ and inpatient nurses
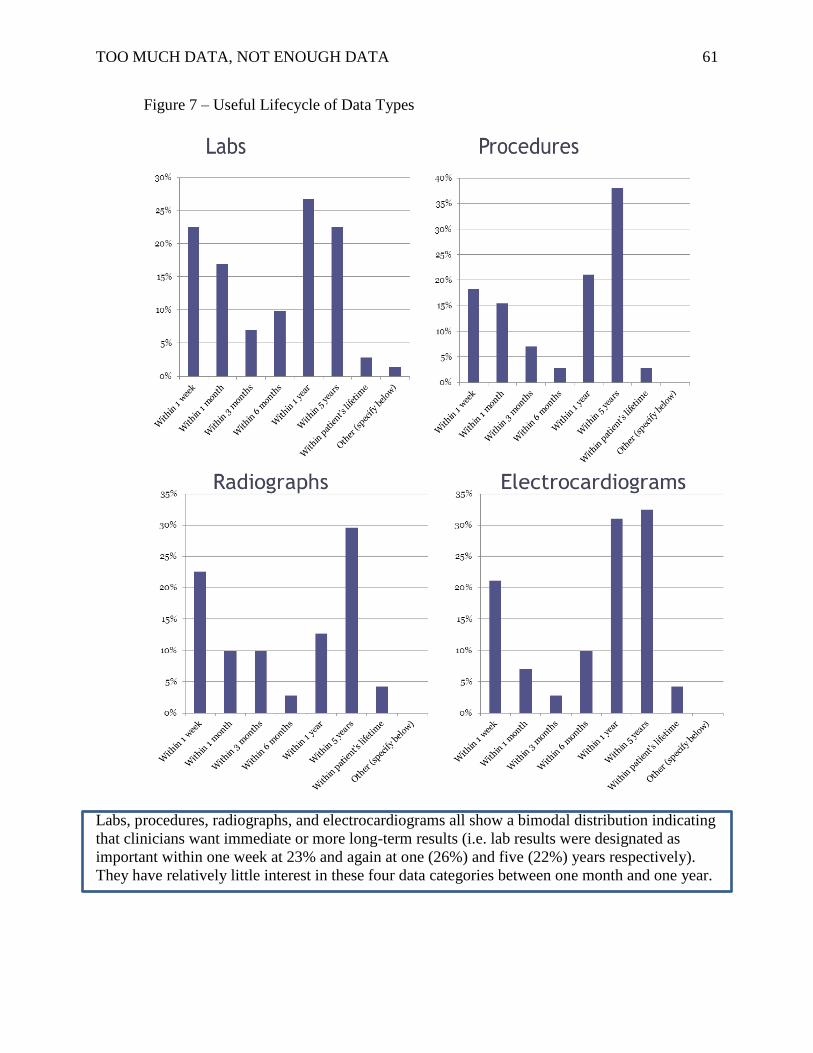
TOO MUCH DATA, NOT ENOUGH DATA 61
Figure 7 – Useful Lifecycle of Data Types
Labs, procedures, radiographs, and electrocardiograms all show a bimodal distribution indicating
that clinicians want immediate or more long-term results (i.e. lab results were designated as
important within one week at 23% and again at one (26%) and five (22%) years respectively).
They have relatively little interest in these four data categories between one month and one year.
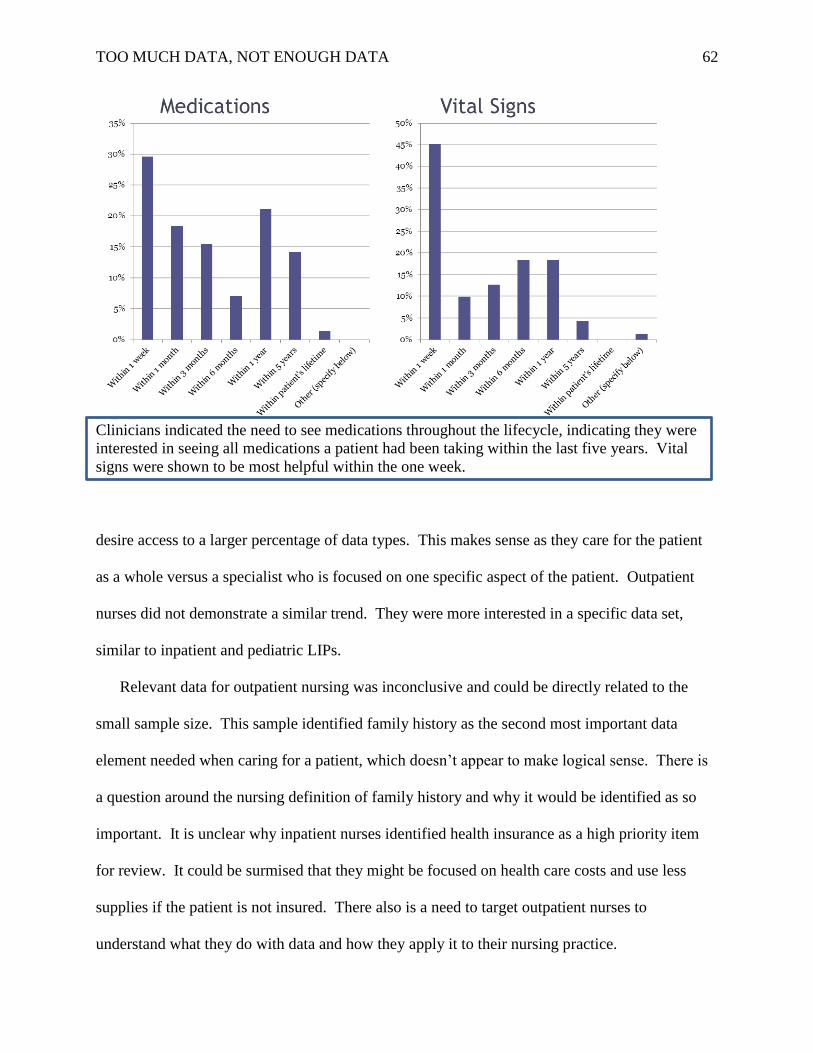
TOO MUCH DATA, NOT ENOUGH DATA 62
Clinicians indicated the need to see medications throughout the lifecycle, indicating they were
interested in seeing all medications a patient had been taking within the last five years. Vital
signs were shown to be most helpful within the one week.
desire access to a larger percentage of data types. This makes sense as they care for the patient
as a whole versus a specialist who is focused on one specific aspect of the patient. Outpatient
nurses did not demonstrate a similar trend. They were more interested in a specific data set,
similar to inpatient and pediatric LIPs.
Relevant data for outpatient nursing was inconclusive and could be directly related to the
small sample size. This sample identified family history as the second most important data
element needed when caring for a patient, which doesn’t appear to make logical sense. There is
a question around the nursing definition of family history and why it would be identified as so
important. It is unclear why inpatient nurses identified health insurance as a high priority item
for review. It could be surmised that they might be focused on health care costs and use less
supplies if the patient is not insured. There also is a need to target outpatient nurses to
understand what they do with data and how they apply it to their nursing practice.
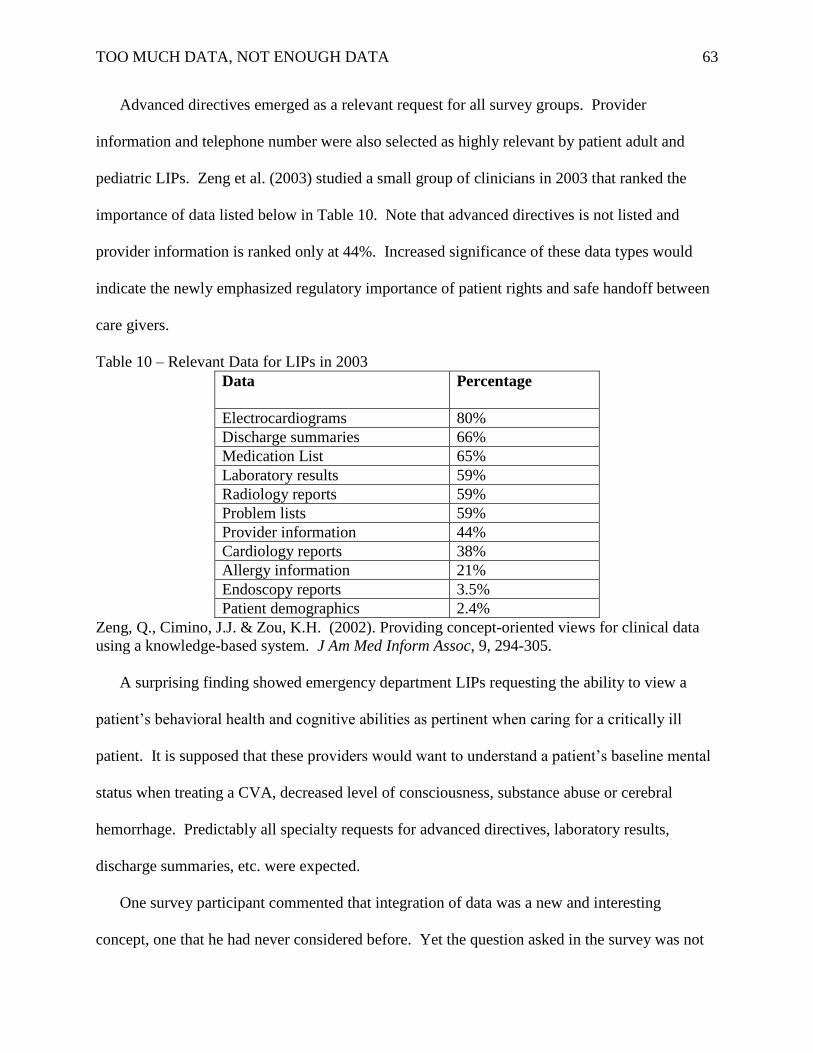
TOO MUCH DATA, NOT ENOUGH DATA 63
Advanced directives emerged as a relevant request for all survey groups. Provider
information and telephone number were also selected as highly relevant by patient adult and
pediatric LIPs. Zeng et al. (2003) studied a small group of clinicians in 2003 that ranked the
importance of data listed below in Table 10. Note that advanced directives is not listed and
provider information is ranked only at 44%. Increased significance of these data types would
indicate the newly emphasized regulatory importance of patient rights and safe handoff between
care givers.
Table 10 – Relevant Data for LIPs in 2003
Data
Percentage
Electrocardiograms 80%
Discharge summaries 66%
Medication List 65%
Laboratory results 59%
Radiology reports 59%
Problem lists 59%
Provider information 44%
Cardiology reports 38%
Allergy information 21%
Endoscopy reports 3.5%
Patient demographics 2.4%
Zeng, Q., Cimino, J.J. & Zou, K.H. (2002). Providing concept-oriented views for clinical data
using a knowledge-based system. J Am Med Inform Assoc, 9, 294-305.
A surprising finding showed emergency department LIPs requesting the ability to view a
patient’s behavioral health and cognitive abilities as pertinent when caring for a critically ill
patient. It is supposed that these providers would want to understand a patient’s baseline mental
status when treating a CVA, decreased level of consciousness, substance abuse or cerebral
hemorrhage. Predictably all specialty requests for advanced directives, laboratory results,
discharge summaries, etc. were expected.
One survey participant commented that integration of data was a new and interesting
concept, one that he had never considered before. Yet the question asked in the survey was not
TOO MUCH DATA, NOT ENOUGH DATA 64
as specific as it should have been. As stated above, integration of numeric data such as labs and
vital signs makes a great deal of sense. Not as clear is the process to integrate text documents
such as discharge summaries and progress notes. Information gleaned from this question
illustrates this is not an all or none proposal. Each piece of data should be evaluated individually
to determine the value of integration with other like data or to keep the information independent.
These survey questions did not take into account that different data types might require
different manners of reconciliation. Text documents such as discharge summaries would not
require reconciliation whereas lab results and medication lists would. As with the question of
exchanged data, each piece of data should be separately assessed.
Findings about data trustworthiness revealed varied results on two questions related to
provider and reimbursement. It could be argued these questions were used as the reverse balance
questions asked in the survey. For survey questions developed in a Likert scales format it is
recommended that for balance, both positive and negative questions should be asked. Future
work should include re-evaluation of these two topics. Overall there was an indication that each
of the clinical specialties appears to be ready to exchange information between healthcare
systems.
A better understanding of the useful lifecycle of data types denoted the importance of
providing current (one week to three months) and long-term (five years to a complete history)
access to different types of data. A full medication history was regarded as necessary and vital
signs information was viewed as valuable only from one week to three months.
Policy and Practice Implications
This study may be considered exploratory research and there is much work yet to be
accomplished. There will be numerous iterations before concrete recommendations can be
TOO MUCH DATA, NOT ENOUGH DATA 65
made. However this is the beginning of HIT advancements that will affect interoperability. This
research will not have an immediate effect on policy and practice, but it is informing and shaping
the quality of health information exchange based on the correct data to be exchanged, the
presentation, reconciliation, trustworthiness and the useful lifecycle.
Strengths and Limitations of the Study
The strengths of the study include the following: 1) The study answered real questions
relating to standards development today based on the work done by HL7, S&I Framework and
the CCC; 2) The study is grounded in reality, data was an actual working set of information that
clinicians use; 3) Ground breaking research questions covered topics not currently well
researched; 4) A broad group of clinicians was surveyed from across the country; and 5) It is
important that these questions have been answered.
Study limitations included: 1) Ambiguity in some of the questions. An example being
what is the definition of family history as indicated as important by the responses of outpatient
nursing cohort; 2) Outpatient nursing sample size; 3) Location information was not collected (it
was only known that electronic surveys were completed by Consortium members other than
Intermountain Healthcare and the University of Utah 2012 DNP cohort). Although this
information is not pertinent when the data is collated, it will matter as further analysis is done,
because it is impossible to define if there is a representative sample; 4) The survey groups may
have been too broad, the sample population should have been limited to less than six subgroups);
and 5) Development and implementation of the electronic survey was more challenging than
expected. This limited responses from CCC clinicians.
Project Recommendations
TOO MUCH DATA, NOT ENOUGH DATA 66
Future work related to this topic will be continuing iterations of this survey, focusing on
specific cohorts, additional work to understanding differences in presentation, attempting to
understand what efforts needs to be accomplished related to reconciliation as it links to data
types and identifying priority of data integration in health information exchange
This project is considered exploratory research and is only in the beginning of discovery.
Because there is little current information on this subject, any additional information obtained
will continue to bring high value to the process of electronic health information exchange.
Although not within the scope of this DNP project, the author and content experts will continue
to be involved in expanding this project. Using a modified Delphi approach, additional surveys
will be given to CCC clinicians to refine recommendations for appropriate data exchange.
Specific focus will be on display of shared data and how information should be reconciled.
Summary
Relevant, pertinent and timely electronic data passed through a HIE must become a
recognized and critical component in providing better patient care. It is evident that more data
are not always helpful and in fact may adversely affect both the patient and the provider.
Knowing and understanding the exact health information that specific providers need at certain
point in the treatment process will only enhance the quality of care given to patients. This survey
has begun the exploratory process of identifying what that exact health information includes and
the analysis that must occur to establish the logic of this process
TOO MUCH DATA, NOT ENOUGH DATA 67
References
American Association of Colleges of Nursing. (2006). The essentials of doctoral education for
advanced nursing practice. Washington, D.C., 3-27.
American Nurses Association. Nursing informatics scope and standards of practice. Silver
Spring, MD nursebooks.org:2008.
Ancker, J.S., Edwards, A.M., Miller, M.C. & Kaushal, R. (2012). Consumer perceptions of
electronic health information exchange. American Journal of Preventive Medicine 43(1),
76-80.
Balfour, D.C., Evan, S., Januska, J., Lee, H.Y., Lewis, S.J., Nolan, S.R., Noga, M., Stemple, C.
& Thapar, L. (2009). Health information technology – results from a roundtable
discussion. Journal of Managed Care Pharmacy, 15, 10-17.
Blumenthal, D. &Tavenner, M. (2010). The “Meaningful Use” regulation for electronic health
records. New England Journal, 363(6), 501-504.
Burton, L.C., Anderson, G.F & Kues, I.W. (2004). Using electronic health records to help
coordinate care. The Milbank Quarterly, 82(3), 457-481.
Cash, J.J. (2009). Alert fatigue. American Journal of Health, 66(1), 2098-2101.
Care Connectivity Consortium. (2012). Available online @
http://centerfortotalhealth.org/tag/care-connectivity-consortium/
Daigh, R. (2012). Too much data, not enough information. Available online @
http://www.md- it.com/too-much-data-not-enough-information. Accessed May 19,
2012.
D’Amore, J.D. (2011). The promise of the CCD: Challenges and opportunity for quality
improvement and population health. J Am Med Inform Assoc., 210, 1-10.
TOO MUCH DATA, NOT ENOUGH DATA 68
Denard, J. (2012). Swimming in too much EMR data, Available online @
http://www.emrandehr.com/2012/05/31/swimming-in-too-much-emr-data. Accessed 5-
23-2012.
Department of Health and Human Services. Final Rule. 2010. Available online@
http://www.ofr.gov/OFRUpload/OFR Data/2010-17207_PI.pdf , Accessed 5-23-2012.
Eliot, T.S. (1934). The Rock. Farber and Faber, London, England.
Embi, P.J. & Leonard, A.C. (2012). Evaluating alert fatigue over time to EHR-based clinical
trial alerts: Findings from a randomized controlled study. Journal American Medical
Informatics Association, doi: 10.1136/amiajnl-2011-00743.
Evert. A., Trence, D., Catton. & Huynh, P., (2009). Continuous glucose monitoring technology
for personal use: An educational program that educates and supports the patient.
Diabetes Education, 35(4), 565-580.
Fricton, J.R. & Davies, D. (2010). Personal health records to improve health information
exchange and patient safety. J Am Med Inform Assoc., 12, 1-10.
Fisher, W.G. Doctors are downing in too much data, not enough appropriate information.
Available online @ http://medcitynews.com/2012/03/doctors-are-drowning-in-too-much-
data-not-enough-appropriate-information/. Accessed 5-23-12.
Francis, L. P. (2010). The physician-patient relationship and a national health information
network. Journal of Law, Medicine and Ethics, Spring, 36-49.
Frisse, M.E. (2010). Health information exchange in Memphis: Impact on the physician-patient
relationship. (2010). Journal of Law, Medicine and Ethics, Spring, 50-57.
Gadd, C.S., Ho, Y.W., Cala, M.C., Blakemore, D., Chen, Q., Frisse, M.E. & Johnson, K.B.,
(2011). User perspectives on the usability of a regional health information exchange.
TOO MUCH DATA, NOT ENOUGH DATA 69
J AmMed Inform Assoc., 18, 711-716.
Graves, J.R. & Corcoran, S. (1989). An overview of nursing informatics. Journal of Nursing
Scholarship, 29, 227-231.
Green, B.B., Cook, A.J., Ralston, J.D., Fikshman, P.A., Catx, S.L., Carlson, D., Tyll. L., Larson,
E.B., & Thompson, R.S. (2008). Effectiveness of home blood pressure monitoring. Web
communication and pharmacist care on hypertension control: A randomized controlled
trial. JAMA, 299(24), 2857-67.
Gorman, P.N. & Helfand, M. (1995). Information seeking in primary care: How physicians
choose which clinical questions to pursue and which to leave unanswered. Medical
Decision Making, 15:2, 113-119.
HIPPA regulations. (2012). Available online @
http://www.hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/minimumnecessary.
html. Accessed 6-14-12.
HL7. (2012). Available online @ http://www.hl7.org/implement/standards/. Accessed 7-4-12.
Hayrinen, K., Saranto, K., Nykanen, P. (2007). Definition, structure, content, use and impacts of
electronic health records: A review of the research literature. International Journal of
Medical Informatics, 22, 291-304.
Hsu, C.C., Sandford, B.A. (2007). The Delphi technique: Making sense of consensus. Practical
Assessment, Research and Evaluation, 12(10), 1-8.
IHE. (2012). Accessed 7-5-12. IHE patient care coordination, technical framework
supplement. Available online @
http://www.ihe.net/Technical_Framework/upload/IHE_PCC_TF_Supplement_eNursingS
ummary_PC_2010-06-01.pdf. 1-17. Accessed 6-2-12.
TOO MUCH DATA, NOT ENOUGH DATA 70
Intermountain Stories, (2011). Available online @
https://my.intermountain.net/intermountainstories /Documents/CO-2011-04-11.pdf.
Accessed 7-14-12
Johnson, K.B., Unertl, K.M., Chen, Q, Lorenzi, N.M., Nikan, H., Bailey, J. & Frisse, M. (2011).
Health information exchange usage in emergency departments and clinics: The who,
what and why. J Am Med Inform Assoc., 18, 690-697.
Kesselheim, A.S., Creswell, K., Phansalkar, S., Bates, D.W. & Sheikh, A. (2011). Clinical
decision support systems could be modified to reduce ‘alert fatigue’ while still
minimizing the risk of litigation. Health Affairs 30(12), 2310-2317.
Krikelas, J. (1983). Information seeking behavior: Patterns and concepts. Drexel Library
Quarterly, 19, 5-20.
Kuperman, G.J. (2011). Health-information exchange: Why are we doing it and what are we
doing? Journal American Medical Informatics Association, 18,678-682.
Matney, S., Brewster, P.J., Sward, K.A., Cloyes, K.G. & Staggers, N. (2011). Philosophical
approaches to the nursing informatics data-information-knowledge-wisdom framework.
Advances in Nursing Science, 16(53), 1-13.
Maslove, D.M., Rizk, N. & Lowe, H.J. (2012). Computerized physician order entry in the
critical care environment: A review of current literature. Journal of Intensive Care
Medicine, 26(3), 165-171.
McKinsey and Company. (2011). Available online @ www.mckinsey.com.mgi, 1-3.
Accessed 6-10-12.
MCTB. (2011). Available online @ http://222.mtbc.com/learnaingcenter/index,php/care-
connectivity-consortium-to-demonstrate-feasibility-of-cross-country-data-exchange .
TOO MUCH DATA, NOT ENOUGH DATA 71
(1-3). Accessed 5-21-2012.
Merriam-Webster’s Collegiate Dictionary, 12th
Edition. Springfield, MA: G. &C. Merriam
Company, Publishers, 2012.
National Health Information Exchange. Available online @
http://www.healthit.hhs.gov/portal/server.pt/community/healhit-hhs-gov-nibn-
exchange/1407. Accessed 12 June 2012.
National Health Information Network, President’s Council of Advisors on Science and
Technology, (2010). Report to the president realizing the full potential of health
information technology to improve healthcare for Americans: the path forward.
Available online @ http://www.whitehouse.gov/sites/default/files/microsites/ostp/pcast-
health-it-report.pdf. Accessed 7-6-12.
O’Malley, A.S., Grossman, J.M., Cohen, G.R., Kemper, N.M. & Pham, H.H. (2009). Are
electronic medical records helpful for care coordination? Experiences of physician
practices. J Am Med Inform Assoc., 251, 177-185.
Office of Health Information Technology. 2012. Available online @
http://healthit.hhs.gov/blog/faca/index.php/2010/12/10/onc-seeks-comment-on-standards-
and-interoperability-framework-initiatives-by-december-23-2010/. Accessed 7-4-12.
Pho, K. Too much data can overwhelm physicians and harm patients. 2012. Available online
@ http://www.kevinmd.com/blog/2010/10/data-overwhelm-physicians-harm-
patients.html. Accessed 6-12-12.
Rand Survey Meta Data Repository (2011). Available online @
https://mmicdata.rand.org/meta/?section=survey&surveyid=60&display=. Accessed
7- 21-12.
TOO MUCH DATA, NOT ENOUGH DATA 72
Richmond, R. (2012). Why hospitals continue to fail in “connect the dots” with their data, and
what they can do to change. (2012). Available online @
http://thehealthcareblog.com/blog/2012/02/01/why-hospitals-continue-to-fail-in-
%E2%80%98connecting-the-dots%E2%80%99-with-their-data-and-what-they-can-do-
to-ch/. Accessed 7-21-12.
Rudin, R., Volk, L., Simon, S. & Bates, D. (2011). What affects clinicians’ usage of health
information exchange. Applied Clinical Informatics, 1(3), 250-262.
Shakespeare, W. (1961). As you like it. Fawcett Press, New York, NY.
Shapiro, J.S., Kannry, J., Kushniruk, A.W. & Kuppman, G. (2007). Emergency physicians’
perceptions of health information exchange. J Am Med Inform Assoc, 14:
700-705.
Tielman, T., Van Velck, M.A., Stein, D.M., Stetson, P.D. & Johnson, S.B. (2007). Assessing
data relevance for automated generation of a clinical summary. AMIA 2007
Symposium Proceedings, 761-765.
Unertl, K.M., Johnson, K.B. & Lorenzi, N.M. (2012). Health information exchange technology
on the front lines of healthcare: Workflow factors and patterns of use. J Am Med Inform,
19, 392-400.
Utah Health Information Network. (2012). Available online @ http://www.uhin.org/.
Accessed 7-4-12.
Van Vleck, T.T., Stein, D.M., Stetson, P.D., & Johnson, S.B. (2007). Assessing data relevance
for automated generation of a clinical summary. AMIA2007 Symposium Proceedings,
761-765.
Vest, J.R., Hongwei, Z., Jasperson, J., Gamm, L.D. & Ohsfeldt, R.L. (2011). Factors motivating
TOO MUCH DATA, NOT ENOUGH DATA 73
and affecting health information exchange usage. Journal American Medical Informatics
Association, 18, 143-149.
Vest, J.R., Jasperson, J., Hongwei, H., Gamm, L.D. & Ohsfeldt, R.L. (2011). Use of health
information exchange system in the emergency care of children. BMC Medical
Informatics and Decision Making, 11(78), 1-10.
Watson, N. (2006). Patients should have to opt in or out of national electronic records.
Available online @ http://www.bmj.com/content/suppl/2006/06/23/332.7556.DC1, 1-4.
Accessed 7-22-12.
Weitzman, E.R., Kelemen, S., Kaci, L. & Mandl, K.D. (2009). Willingness to share personal
health record data for care improvement and public health: A survey of experienced
personal health record users. BMC Medical Informatics and Decision Making. Available
online @ http://www.biomedcentral.com/1472-6947/12/39. Accessed 6-24-12.
Wikipedia. (2012). Clinical Document Architecture. Available online @
http://en.wikipedia.org/wiki/Clinical_Document_Architecture. Accessed 6-21-12
Wolters-Kluwer Health 2011 Point-of-Care Survey. Available online @
http://www.wolterskluwerhealth.com/News/Documents/White%20Papers/Wolters%20Kl
uwer%20Health%20Survey%20Executive%20Summary-Media.pdf. Accessed 6-21-12.
Yasnoff, W.A. National Health Infrastructure. Available online @
http://www.ehcca.com/presentations/HIPAA5/yasnoff.pdf. Accessed 10-13-12.
Zeng, Q., Cimino, J.J. & Zou, K.H. (2002). Providing concept-oriented views for clinical data
using a knowledge-based system. J Am Med Inform Assoc, 9, 294-305.

TOO MUCH DATA, NOT ENOUGH DATA 74
Appendix A
IRB Applications and Addendums
TOO MUCH DATA, NOT ENOUGH DATA 75
From: [email protected] Sent: Friday, August 17, 2012 10:28 AM To: Kathleen Merkley Subject: ERICA IRB New Study Approval
IRB: IRB_00058678
PI: Kathleen Merkley
Title: Electronic Data Relevance
Study
Thank you for submitting your request for approval of this study. The IRB has administratively reviewed your application and a designated IRB member has determined that your study is exempt from further IRB review, under 45 CFR 46.101(b), Category 2, from
the Federal regulations governing human research. It is the policy of the University of Utah that all human subject research which is exempt under this section will be conducted in accordance with (1) the Belmont report (http://ohrp.osophs.dhhs.gov/humansubjects/guidance/belmont.htm ), (2) this institution's administrative procedures to ensure valid
claims of exemption, and (3) orderly accounting for such activities. All research involving human subjects must be approved or exempted by the IRB before the research is conducted (http://www.research.utah.edu/irb/guidelines/pdf/IGS/IGS-ExemptResearch.pdf).
Since this determination is not an approval, it does not expire or need renewal. This determination of exemption from continuing IRB review only applies to the research study as submitted to the IRB
and you are expected to follow the protocol as outlined. Before
implementing any changes in the study, you must submit an amendment application to the IRB and secure either approval or a determination of exemption.
Please remember to submit final IRB approval from Intermountain Healthcare to the University Utah IRB by way of Amendment. If you have questions about this, please contact our office at 581-3655 and we will be happy to assist you. Thank you again for submitting your proposal.
Click IRB_00058678 to view the application. Please take a moment to complete our customer service survey. We
appreciate your opinions and feedback.
TOO MUCH DATA, NOT ENOUGH DATA 76
TOO MUCH DATA, NOT ENOUGH DATA 77

TOO MUCH DATA, NOT ENOUGH DATA 78
Appendix B
List of CCC Committees
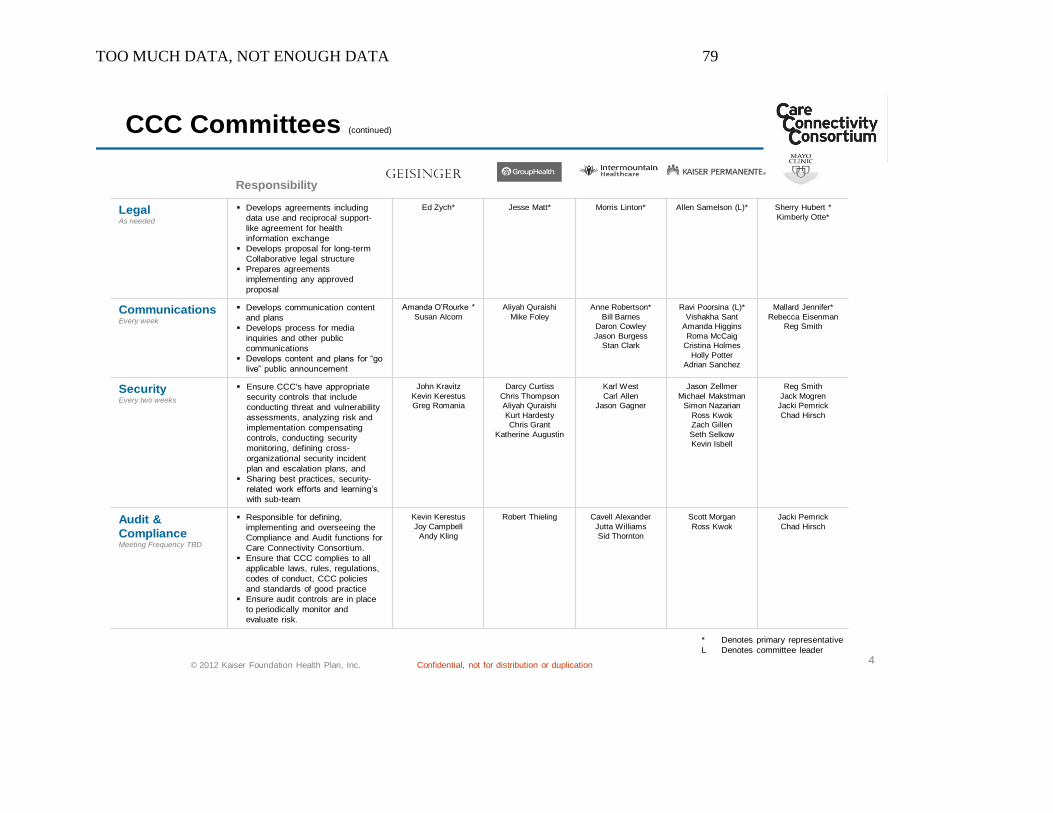
TOO MUCH DATA, NOT ENOUGH DATA 79
4© 2012 Kaiser Foundation Health Plan, Inc. Confidential, not for distribution or duplication
CCC Committees (continued)
LegalAs needed
Develops agreements including
data use and reciprocal support-
like agreement for health
information exchange
Develops proposal for long-term
Collaborative legal structure
Prepares agreements
implementing any approved
proposal
Ed Zych* Jesse Matt* Morris Linton* Allen Samelson (L)* Sherry Hubert *
Kimberly Otte*
CommunicationsEvery week
Develops communication content
and plans
Develops process for media
inquiries and other public
communications
Develops content and plans for “go
live” public announcement
Amanda O’Rourke *
Susan Alcorn
Aliyah Quraishi
Mike Foley
Anne Robertson*
Bill Barnes
Daron Cowley
Jason Burgess
Stan Clark
Ravi Poorsina (L)*
Vishakha Sant
Amanda Higgins
Roma McCaig
Cristina Holmes
Holly Potter
Adrian Sanchez
Mallard Jennifer*
Rebecca Eisenman
Reg Smith
SecurityEvery two weeks
Ensure CCC's have appropriate
security controls that include
conducting threat and vulnerability
assessments, analyzing risk and
implementation compensating
controls, conducting security
monitoring, defining cross-
organizational security incident
plan and escalation plans, and
Sharing best practices, security-
related work efforts and learning’s
with sub-team
John Kravitz
Kevin Kerestus
Greg Romania
Darcy Curtiss
Chris Thompson
Aliyah Quraishi
Kurt Hardesty
Chris Grant
Katherine Augustin
Karl West
Carl Allen
Jason Gagner
Jason Zellmer
Michael Makstman
Simon Nazarian
Ross Kwok
Zach Gillen
Seth Selkow
Kevin Isbell
Reg Smith
Jack Mogren
Jacki Pemrick
Chad Hirsch
Audit &
ComplianceMeeting Frequency TBD
Responsible for defining,
implementing and overseeing the
Compliance and Audit functions for
Care Connectivity Consortium.
Ensure that CCC complies to all
applicable laws, rules, regulations,
codes of conduct, CCC policies
and standards of good practice
Ensure audit controls are in place
to periodically monitor and
evaluate risk.
Kevin Kerestus
Joy Campbell
Andy Kling
Robert Thieling Cavell Alexander
Jutta Williams
Sid Thornton
Scott Morgan
Ross Kwok
Jacki Pemrick
Chad Hirsch
Responsibility
* Denotes primary representative
L Denotes committee leader

TOO MUCH DATA, NOT ENOUGH DATA 80
Appendix C
PreSurvey Letter
TOO MUCH DATA, NOT ENOUGH DATA 81
September 23, 2012
You are one of a small group of clinicians that has been invited to provide feedback on a study
looking at the relevance of different types of data that can be exchanged within the Care
Connectivity Consortium (CCC). As you recall, the CCC is a consortium of five leading U.S.
healthcare organizations, including Mayo (Grouphealth, Geisinger, and Kaiser Permanente)
which was recently formed to help promote electronic transfer of health information across the
country.
Working from the hypotheses that more data are not always helpful when transferred
electronically, this study will attempt to identify what electronic data are relevant to specialty,
patient type, patient acuity and chronicity of illness. It will also determine what clinicians
consider to be trustworthy data, how exchanged data should be reconciled if there are
discrepancies and what time limitations may be placed on certain data categories.
Taking part in this survey is completely voluntary; however, I fully support the premise of this
important project and strongly encourage you to participate. The more surveys that are
completed, the more likely the results will be reliable. This information may only be obtained
with your help. I sincerely appreciate you taking the time to provide us with your valuable input
in this important endeavor.
Sincerely,
Brent Wallace, MD
Chief Medical Officer
Intermountain Healthcare
TOO MUCH DATA, NOT ENOUGH DATA 82
September 23, 2012
You are one of a small group of nurses that has been invited to provide feedback on a study
looking at the relevance of different types of data that can be exchanged within the Care
Connectivity Consortium (CCC). The CCC is a consortium of five leading U.S. healthcare
organizations, including Intermountain Healthcare which was recently formed to help promote
electronic transfer of health information across the country. This information will be merged
with recommendations already obtained from the Utah Health Information Network (UHIN).
Working from the hypotheses that more data are not always helpful when transferred
electronically, this study will attempt to identify what electronic data are relevant to nurses
related to specialty, patient type, patient acuity and chronicity of illness. It will also determine
what nurses consider to be trustworthy data, how exchanged data should be reconciled if there
are discrepancies and what time limitations may be placed on certain data categories.
Taking part in this survey is completely voluntary; however, I fully support the premise of this
important project and strongly encourage you to participate. The more surveys that are
completed, the more likely the results will be reliable. This information may only be obtained
with your help. I sincerely appreciate you taking the time to provide us with your valuable input
in this important endeavor.
Sincerely,
Kim Henrichsen. RN, MS
Chief Nursing Officer
Intermountain Healthcare

TOO MUCH DATA, NOT ENOUGH DATA 83
Appendix D
Invitation Letter – CCC Members
TOO MUCH DATA, NOT ENOUGH DATA 84
From: Kathleen Merkley/Chris Wood
Sent: September 10, 2012
To: XXXXXX
Subject: Providing Data Relevance to Care Connectivity Consortium Members
October 19, 2012
We are writing to ask for your participation in a survey that we are conducting through the Care
Connectivity Consortium. We are asking clinicians like you to reflect on the types of electronic
data you would find helpful when caring for a patient who has come to your facility from another
healthcare system.
Your responses to this survey are very important and will help in advancing the transfer of
relevant data between healthcare systems. As part of the survey, we are also asking you to
consider what makes you trust the data you are receiving.
This is a short survey and should take you no more than ten minutes to complete. Please click on
the link below to go to the survey website (or copy and paste the survey link into your Internet
browser) to acccess the survey.
Survey Link: http://www.surveygizmo.com/s3/1048374/Electronic-Data-Relevance-Survey
Your participation in this survey is entirely voluntary and all of your responses will be kept
confidential. No personally identifiable information will be associated with your responses in
any reports of this data. Should you have an further questions or comments, please feel free to
contact [email protected] or 801.633.1579.
We appreciate your time and consideration in completing this survey. Thank you for
participating in this study. It is only through the help of feedback from clinical experts that we
can provide appropriate data to help guide the direction of the CCC data exchange.
Many thanks,
Kathleen Merkley,APRN, MS, FNP Chris Wood, MD
ECIM Implementation Medical Director, InformationSystems
Intermountain Healthcare Intermountain Healthcare

TOO MUCH DATA, NOT ENOUGH DATA 85
Appendix E
Invitation Letter – Intermountain Healthcare Participants
TOO MUCH DATA, NOT ENOUGH DATA 86
From: Kathleen Merkley/Chris Wood
Subject: Providing Data Relevance to Care Connectivity Consortium Members
August 31, 2012
We are asking Intermountain clinicians to participate in a survey about electronic data relevance.
This is being done in conjunction with a larger survey of the Care Connectivity Consortium
(CCC) a group of health care organizations across the United States who recently formed to help
promote electronic transfer of health information across the country. Would you please reflect
on the types of electronic data you would find helpful when caring for a patient who has come to
your facility from another healthcare system.
Your responses to this survey are very important and will help in advancing the transfer of
relevant data between healthcare systems. As part of the survey, we are also asking you to
consider what makes you trust the data you are receiving. This is a short survey and should take
you no more than ten minutes to complete.
Your participation in this survey is entirely voluntary and all of your responses will be kept
confidential. No personally identifiable information will be associated with your responses in
any reports of this data. Should you have an further questions or comments, please feel free to
contact [email protected] or 801.633.1579.
We appreciate your time and consideration in completing this survey. Thank you for
participating in this study. It is only through the help of feedback from clinical experts that we
can provide appropriate data to help guide the direction of the CCC data exchange.
Many thanks,
Kathleen Merkley,APRN, MS, FNP Chris Wood, MD
ECIM Implementation Medical Director, InformationSystems
Intermountain Healthcare Intermountain Healthcare

TOO MUCH DATA, NOT ENOUGH DATA 87
Appendix F
Thank You Letter
TOO MUCH DATA, NOT ENOUGH DATA 88
From: Kathleen Merkley/Chris Wood
Sent: October 7, 2012
To: XXXXX
Subject: Providing Data Relevance to Care Connectivity Consortium Members
October 7, 2012
Thank you for agreeing to participate in this survey. Your inputs will be extremely valuable in
our efforts to determine which data components should be included related to provider type,
patient acuity, severity and chronicity, as well as how data can be considered more trustable and
timely.
As a respondent, the results of the survey will be displayed on the CCC Wiki by the end of
November. Thank you for your participation and please know the time you spent in providing
feedback will be utilized to enhance data sharing between consortium members.
Sincerely,
Kathleen Merkley,APRN, MS, FNP Chris Wood, MD
ECIM Implementation Medical Director, InformationSystems
Intermountain Healthcare Intermountain Healthcare

TOO MUCH DATA, NOT ENOUGH DATA 89
Appendix G
Recommendations – Care Connectivity Consortium
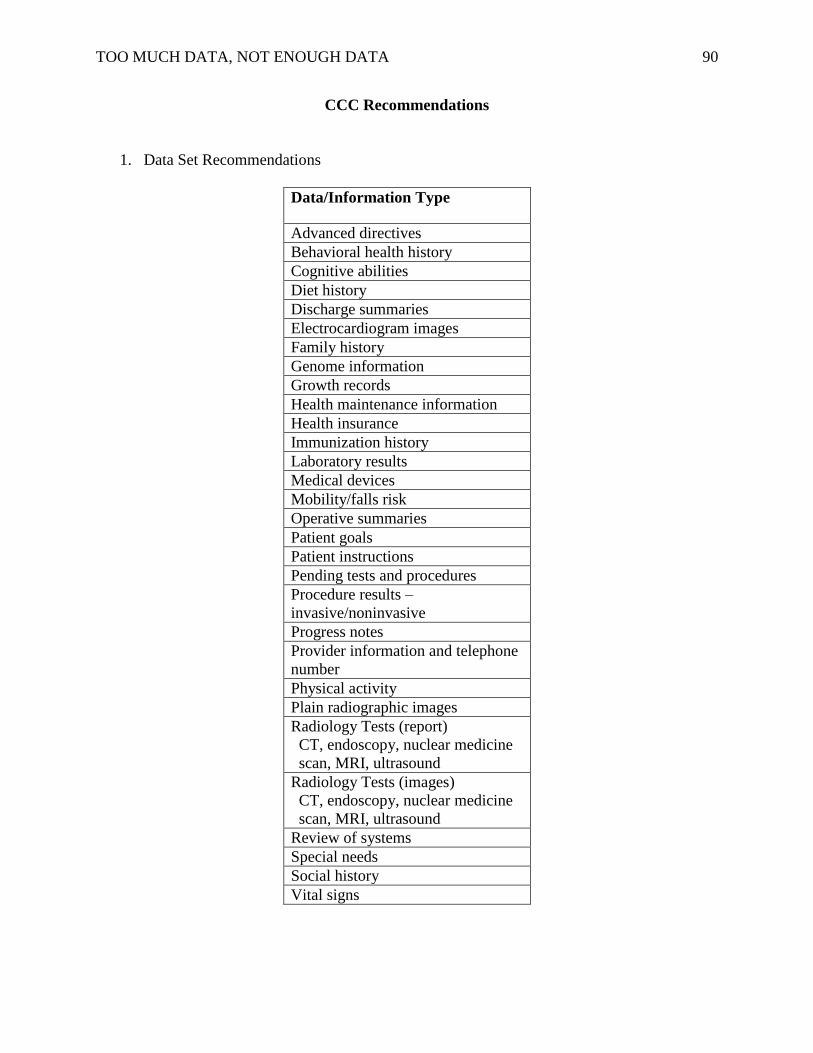
TOO MUCH DATA, NOT ENOUGH DATA 90
CCC Recommendations
1. Data Set Recommendations
Data/Information Type
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
Radiology Tests (report)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
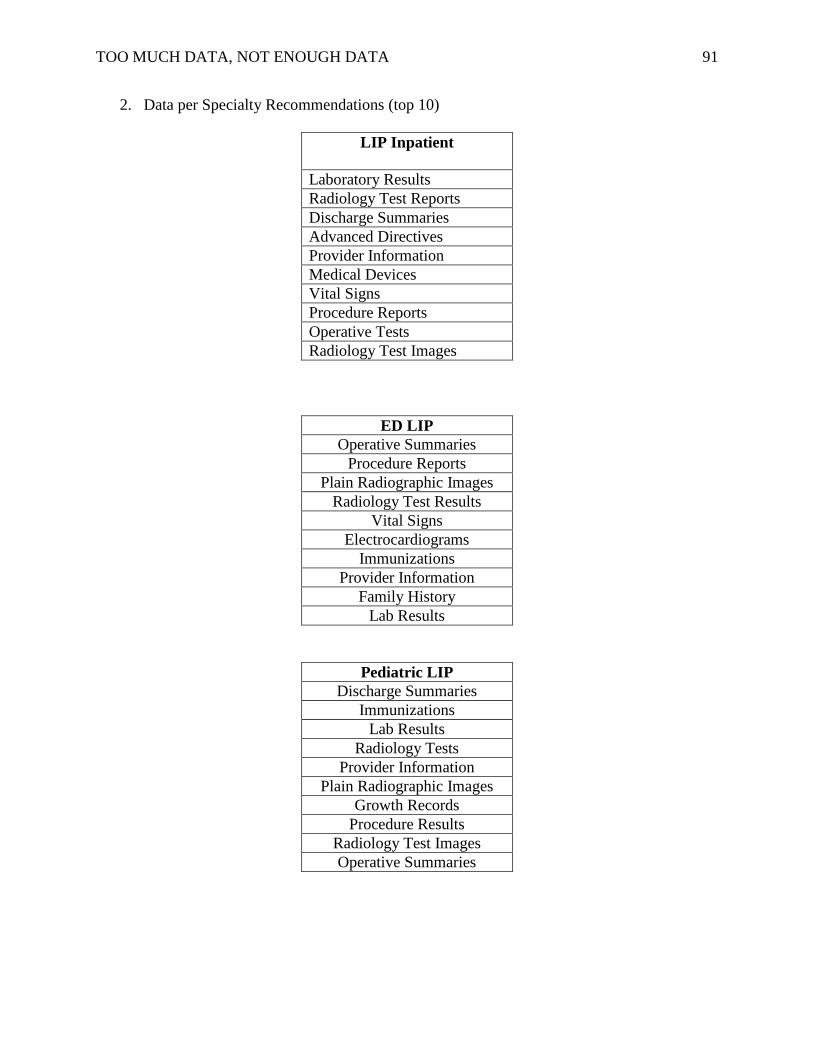
TOO MUCH DATA, NOT ENOUGH DATA 91
2. Data per Specialty Recommendations (top 10)
LIP Inpatient
Laboratory Results
Radiology Test Reports
Discharge Summaries
Advanced Directives
Provider Information
Medical Devices
Vital Signs
Procedure Reports
Operative Tests
Radiology Test Images
ED LIP
Operative Summaries
Procedure Reports
Plain Radiographic Images
Radiology Test Results
Vital Signs
Electrocardiograms
Immunizations
Provider Information
Family History
Lab Results
Pediatric LIP
Discharge Summaries
Immunizations
Lab Results
Radiology Tests
Provider Information
Plain Radiographic Images
Growth Records
Procedure Results
Radiology Test Images
Operative Summaries
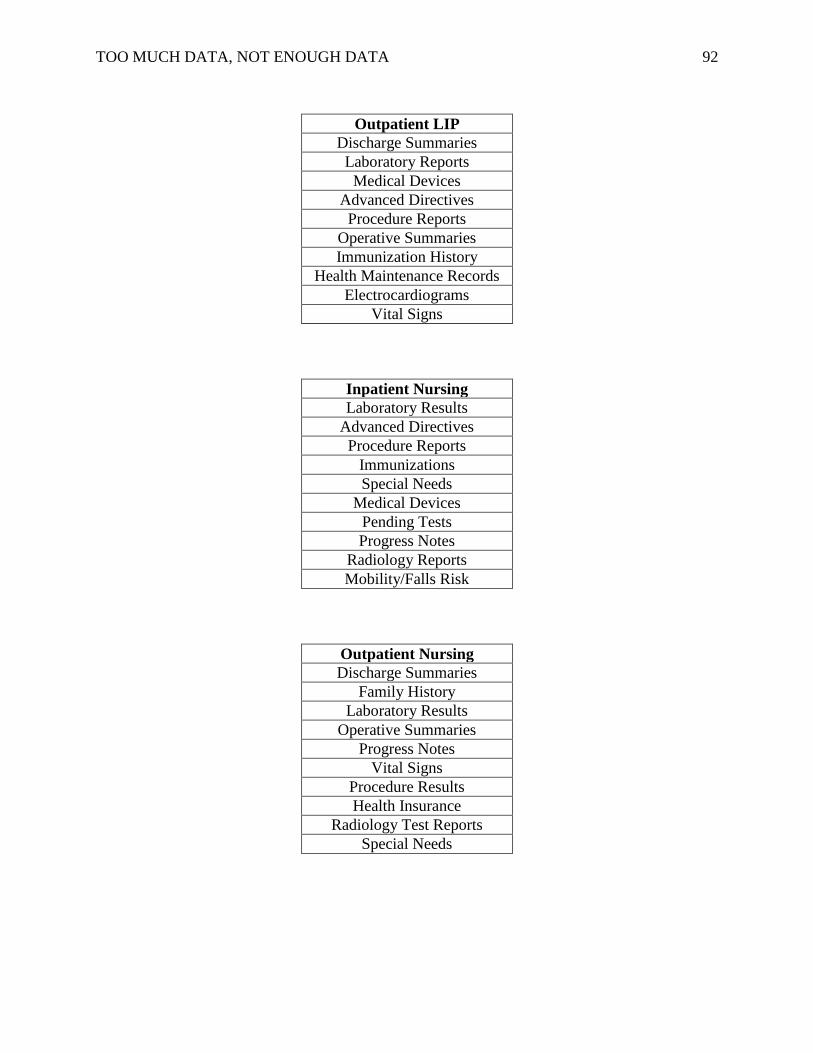
TOO MUCH DATA, NOT ENOUGH DATA 92
Outpatient LIP
Discharge Summaries
Laboratory Reports
Medical Devices
Advanced Directives
Procedure Reports
Operative Summaries
Immunization History
Health Maintenance Records
Electrocardiograms
Vital Signs
Inpatient Nursing
Laboratory Results
Advanced Directives
Procedure Reports
Immunizations
Special Needs
Medical Devices
Pending Tests
Progress Notes
Radiology Reports
Mobility/Falls Risk
Outpatient Nursing
Discharge Summaries
Family History
Laboratory Results
Operative Summaries
Progress Notes
Vital Signs
Procedure Results
Health Insurance
Radiology Test Reports
Special Needs
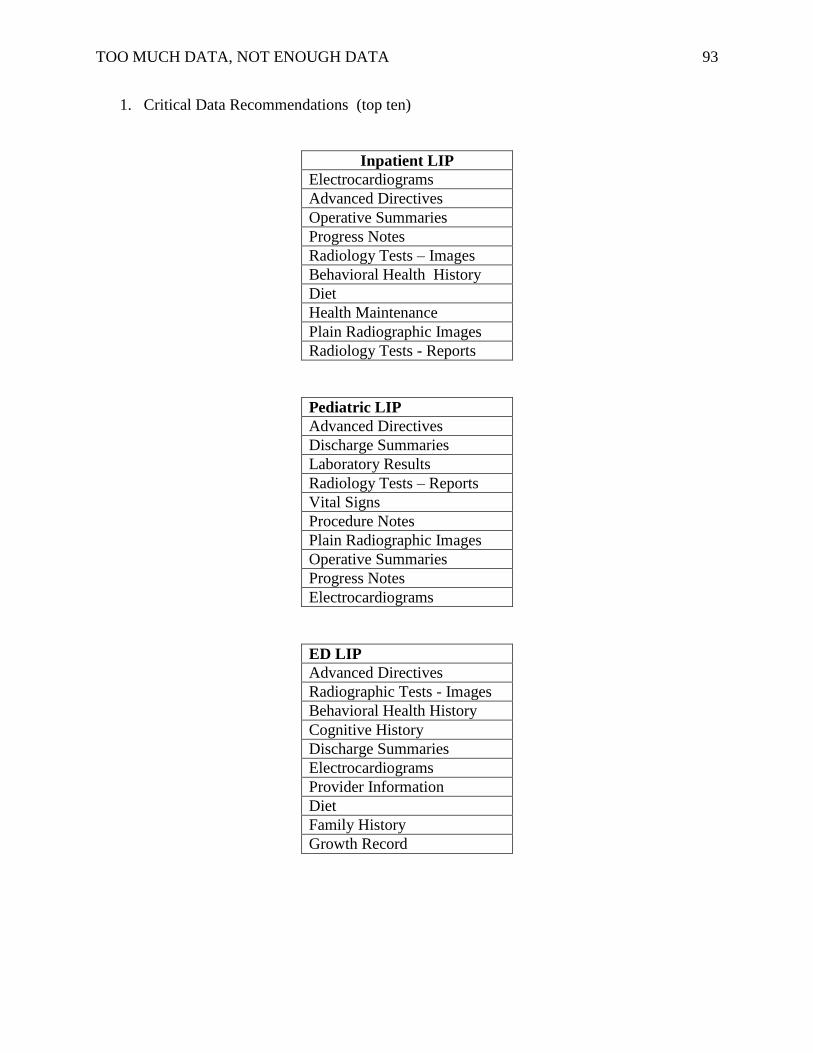
TOO MUCH DATA, NOT ENOUGH DATA 93
1. Critical Data Recommendations (top ten)
Inpatient LIP
Electrocardiograms
Advanced Directives
Operative Summaries
Progress Notes
Radiology Tests – Images
Behavioral Health History
Diet
Health Maintenance
Plain Radiographic Images
Radiology Tests - Reports
Pediatric LIP
Advanced Directives
Discharge Summaries
Laboratory Results
Radiology Tests – Reports
Vital Signs
Procedure Notes
Plain Radiographic Images
Operative Summaries
Progress Notes
Electrocardiograms
ED LIP
Advanced Directives
Radiographic Tests - Images
Behavioral Health History
Cognitive History
Discharge Summaries
Electrocardiograms
Provider Information
Diet
Family History
Growth Record
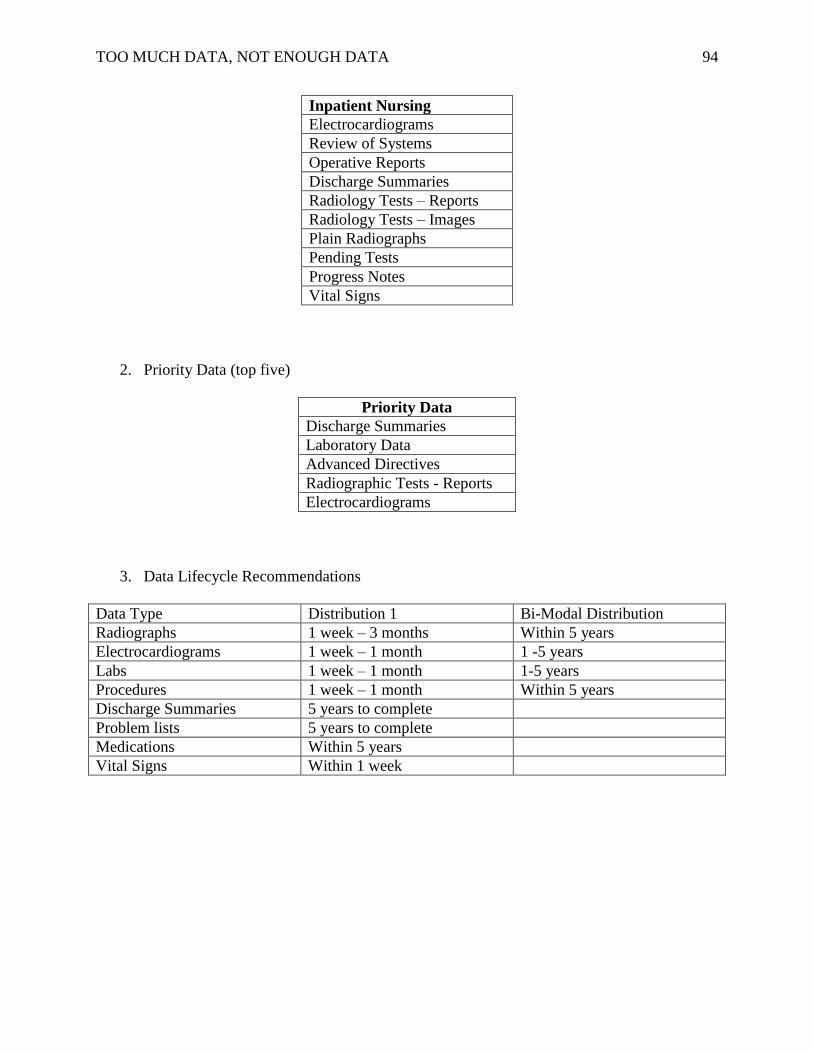
TOO MUCH DATA, NOT ENOUGH DATA 94
Inpatient Nursing
Electrocardiograms
Review of Systems
Operative Reports
Discharge Summaries
Radiology Tests – Reports
Radiology Tests – Images
Plain Radiographs
Pending Tests
Progress Notes
Vital Signs
2. Priority Data (top five)
Priority Data
Discharge Summaries
Laboratory Data
Advanced Directives
Radiographic Tests - Reports
Electrocardiograms
3. Data Lifecycle Recommendations
Data Type Distribution 1 Bi-Modal Distribution
Radiographs 1 week – 3 months Within 5 years
Electrocardiograms 1 week – 1 month 1 -5 years
Labs 1 week – 1 month 1-5 years
Procedures 1 week – 1 month Within 5 years
Discharge Summaries 5 years to complete
Problem lists 5 years to complete
Medications Within 5 years
Vital Signs Within 1 week

TOO MUCH DATA, NOT ENOUGH DATA 95
Appendix H
Electronic Data Relevance Emergency Survey
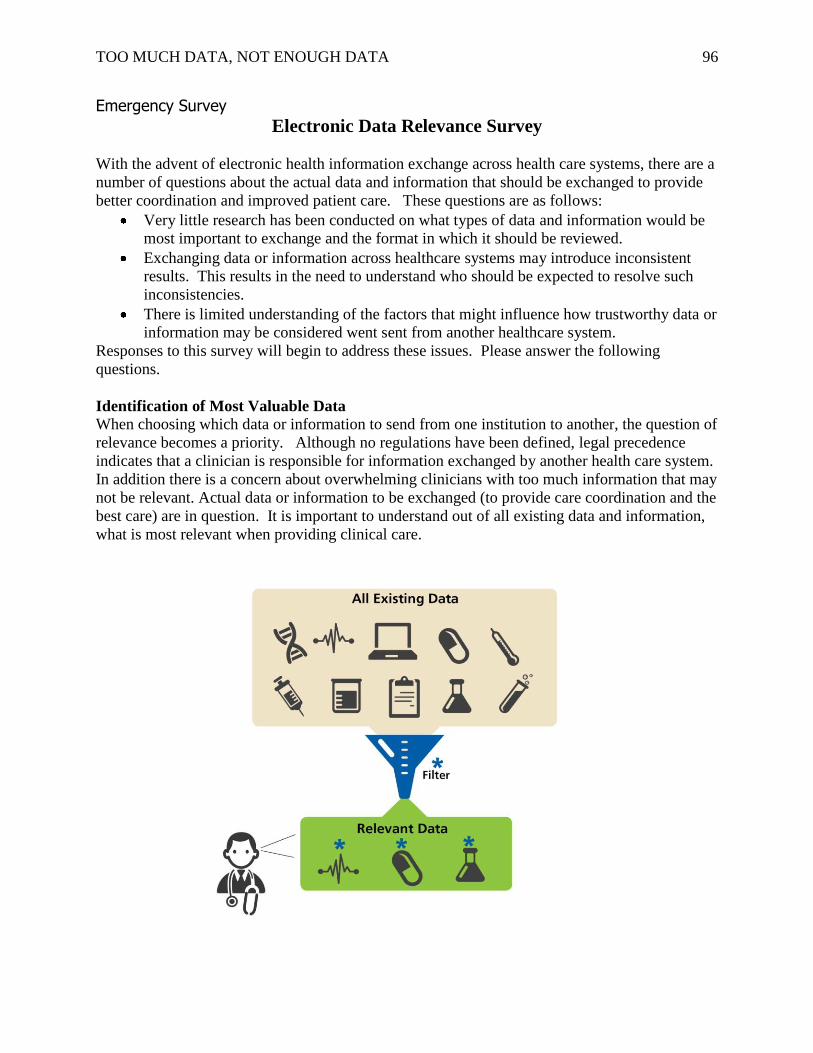
TOO MUCH DATA, NOT ENOUGH DATA 96
Emergency Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data and information would be
most important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
results. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for information exchanged by another health care system.
In addition there is a concern about overwhelming clinicians with too much information that may
not be relevant. Actual data or information to be exchanged (to provide care coordination and the
best care) are in question. It is important to understand out of all existing data and information,
what is most relevant when providing clinical care.
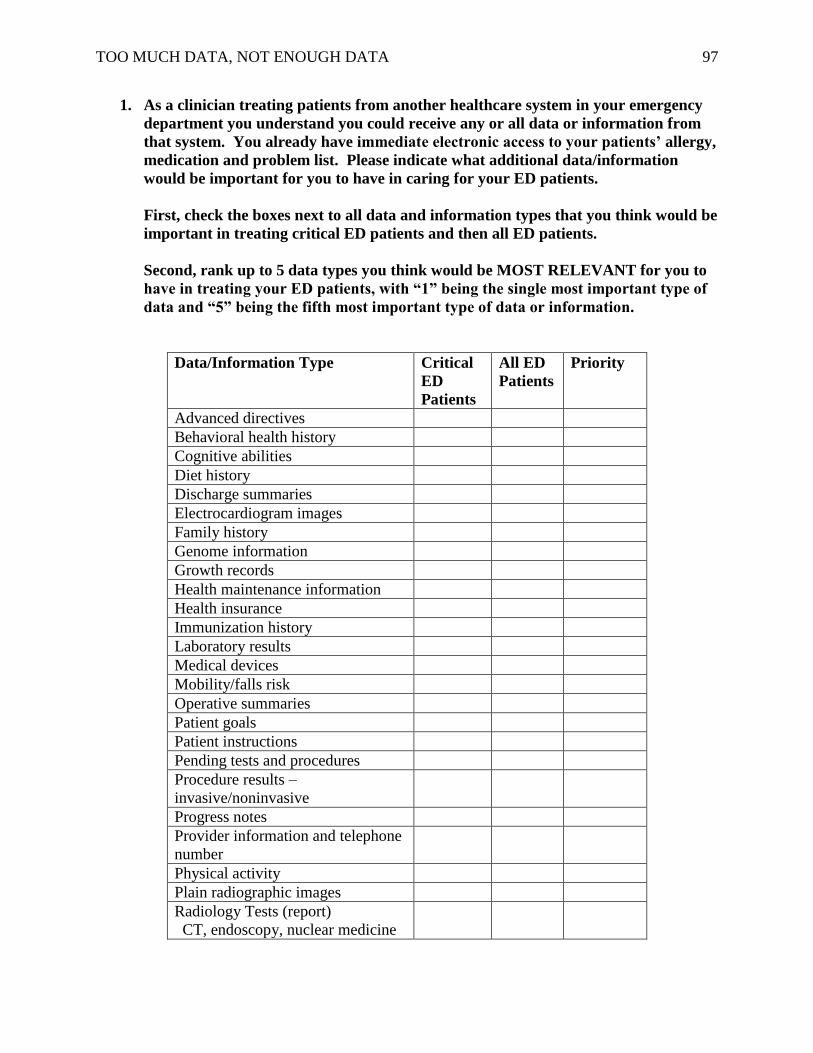
TOO MUCH DATA, NOT ENOUGH DATA 97
1. As a clinician treating patients from another healthcare system in your emergency
department you understand you could receive any or all data or information from
that system. You already have immediate electronic access to your patients’ allergy,
medication and problem list. Please indicate what additional data/information
would be important for you to have in caring for your ED patients.
First, check the boxes next to all data and information types that you think would be
important in treating critical ED patients and then all ED patients.
Second, rank up to 5 data types you think would be MOST RELEVANT for you to
have in treating your ED patients, with “1” being the single most important type of
data and “5” being the fifth most important type of data or information.
Data/Information Type Critical
ED
Patients
All ED
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
Radiology Tests (report)
CT, endoscopy, nuclear medicine
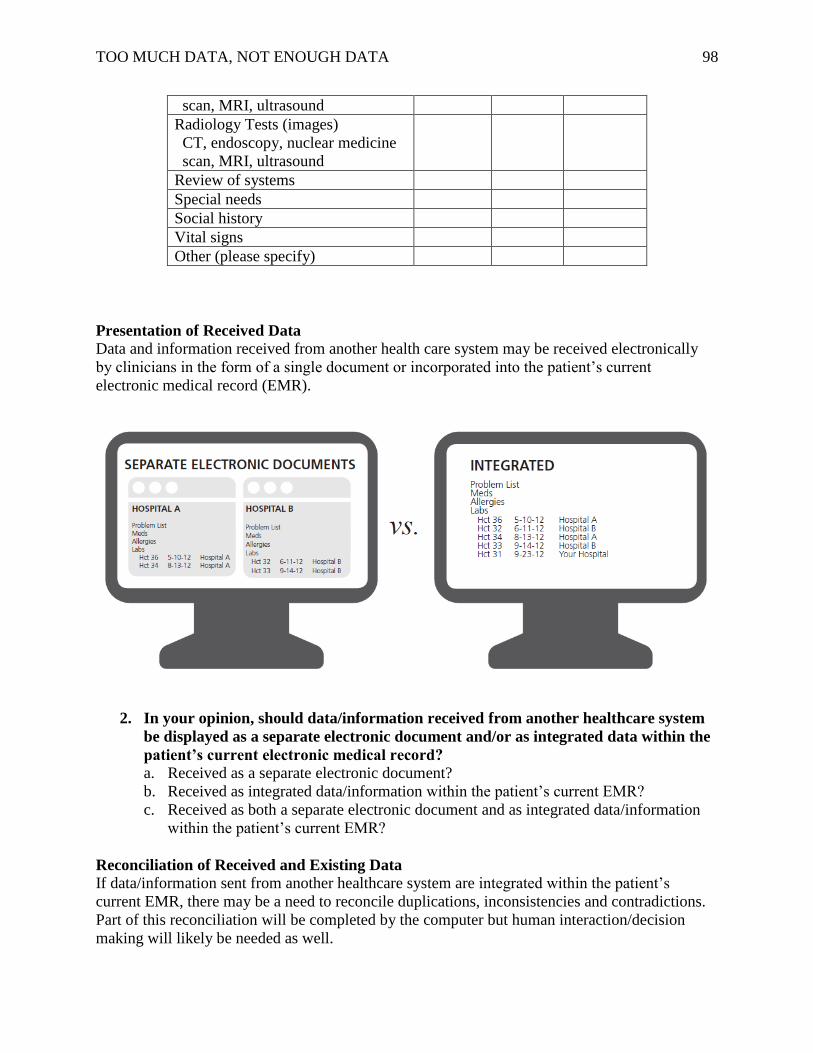
TOO MUCH DATA, NOT ENOUGH DATA 98
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
2. In your opinion, should data/information received from another healthcare system
be displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
a. Received as a separate electronic document?
b. Received as integrated data/information within the patient’s current EMR?
c. Received as both a separate electronic document and as integrated data/information
within the patient’s current EMR?
Reconciliation of Received and Existing Data
If data/information sent from another healthcare system are integrated within the patient’s
current EMR, there may be a need to reconcile duplications, inconsistencies and contradictions.
Part of this reconciliation will be completed by the computer but human interaction/decision
making will likely be needed as well.
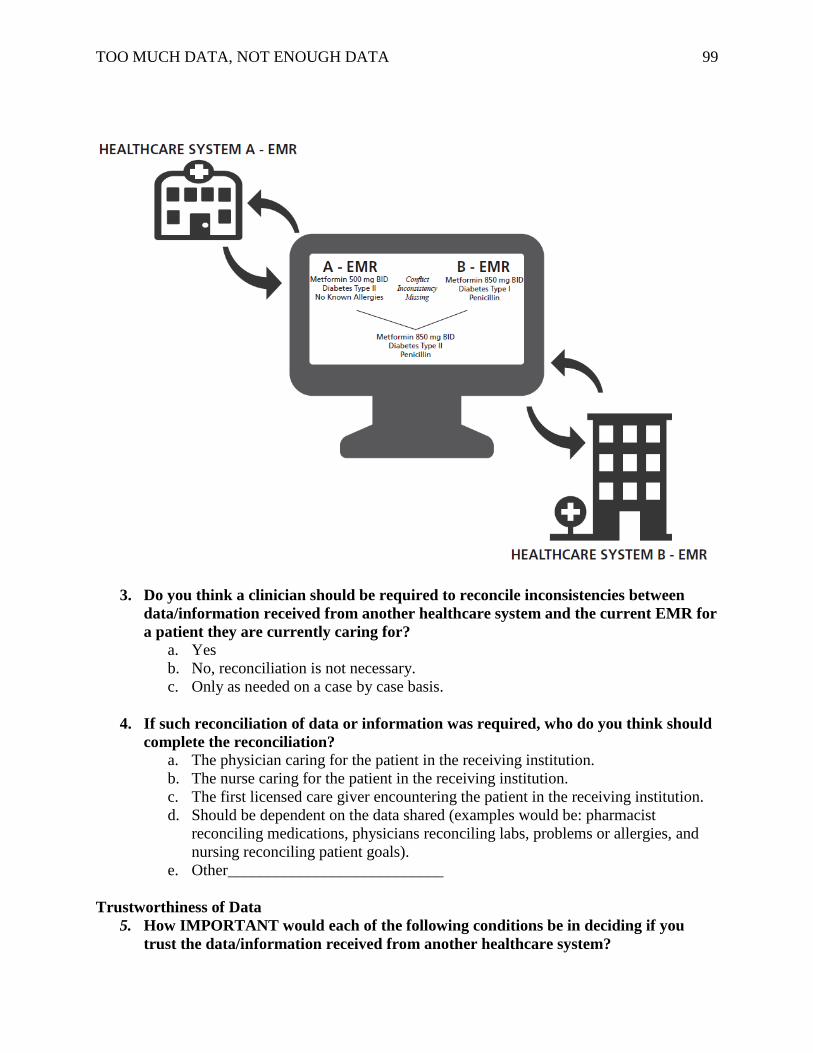
TOO MUCH DATA, NOT ENOUGH DATA 99
3. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
4. If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
Trustworthiness of Data
5. How IMPORTANT would each of the following conditions be in deciding if you
trust the data/information received from another healthcare system?
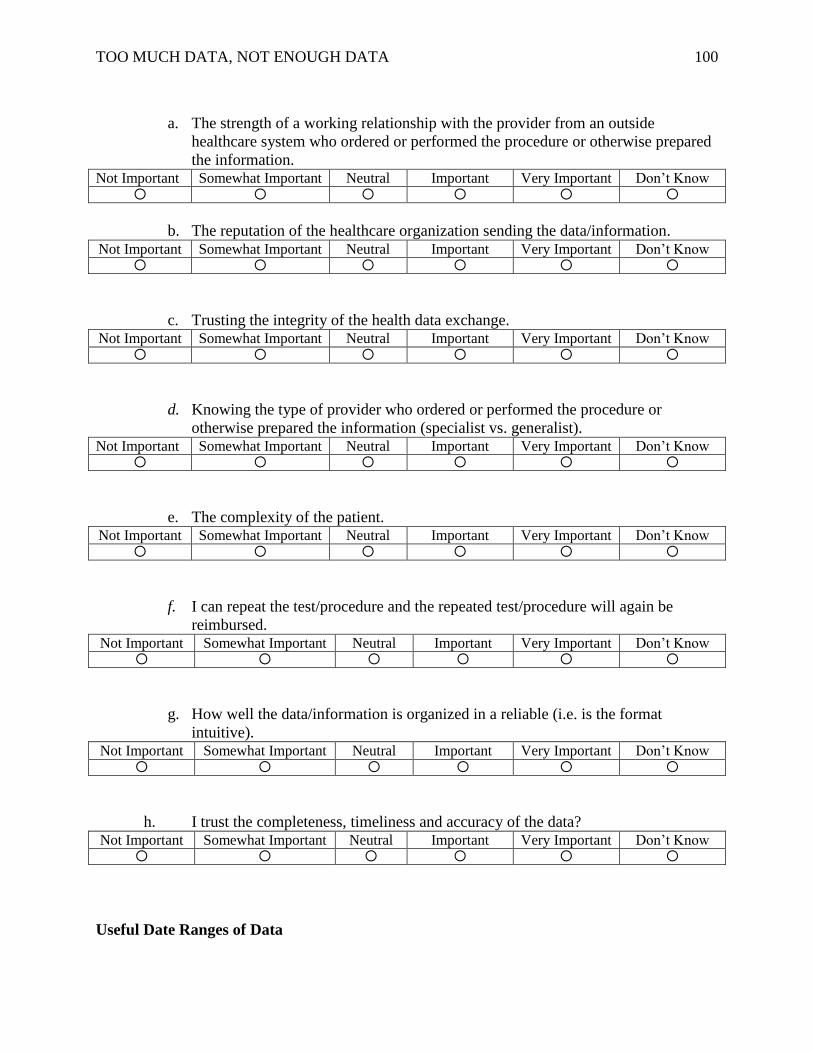
TOO MUCH DATA, NOT ENOUGH DATA 100
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data/information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data/information is organized in a reliable (i.e. is the format
intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
Useful Date Ranges of Data
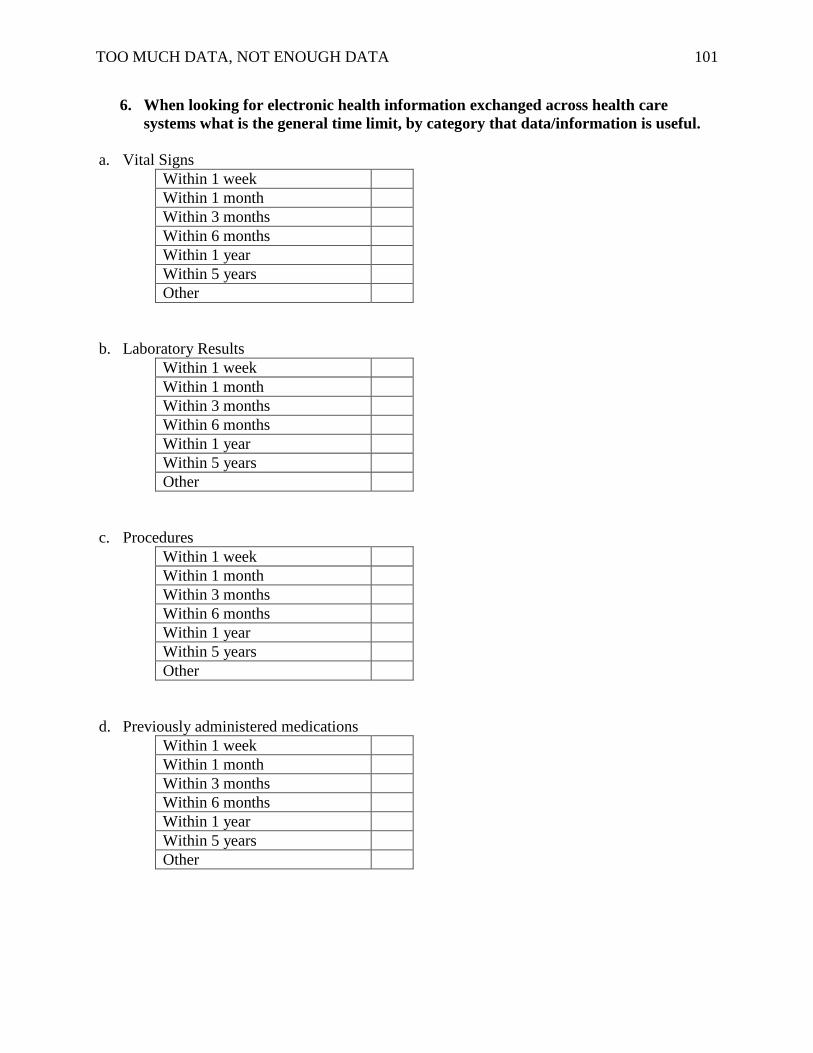
TOO MUCH DATA, NOT ENOUGH DATA 101
6. When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
a. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
b. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
c. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
d. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
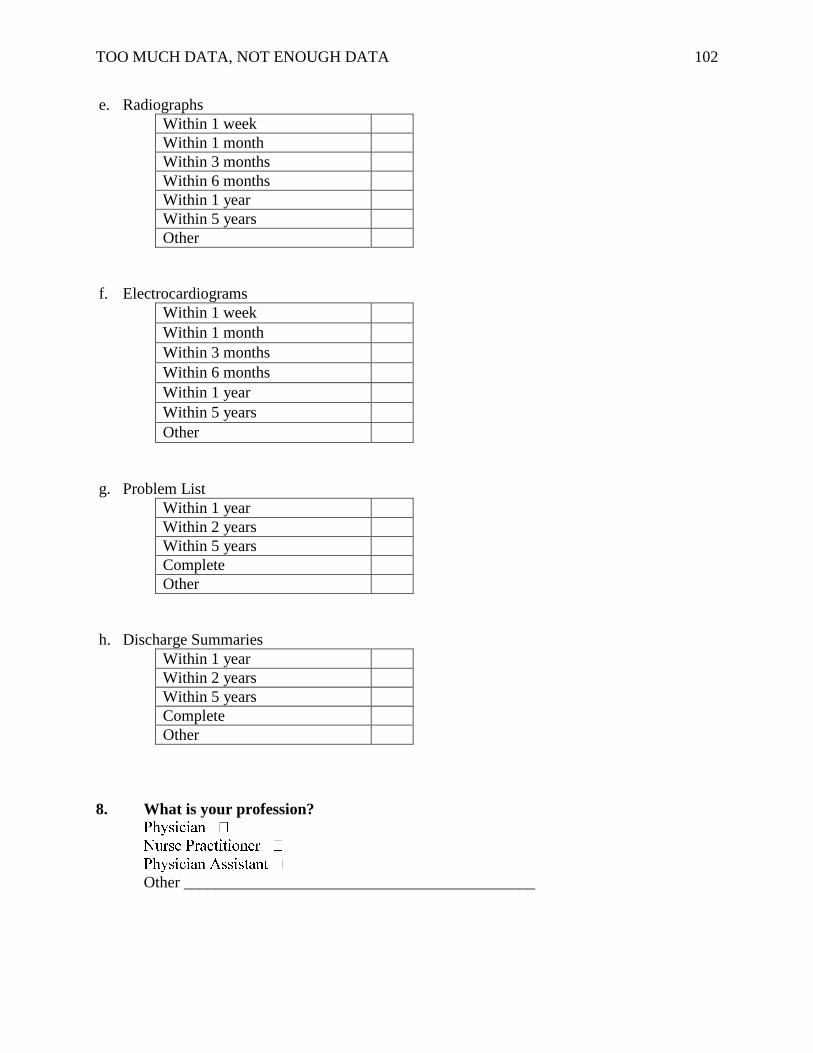
TOO MUCH DATA, NOT ENOUGH DATA 102
e. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
f. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
g. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
h. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your profession?
Other ____________________________________________

TOO MUCH DATA, NOT ENOUGH DATA 103
Appendix I
Electronic Data Relevance Survey – Inpatient Nursing
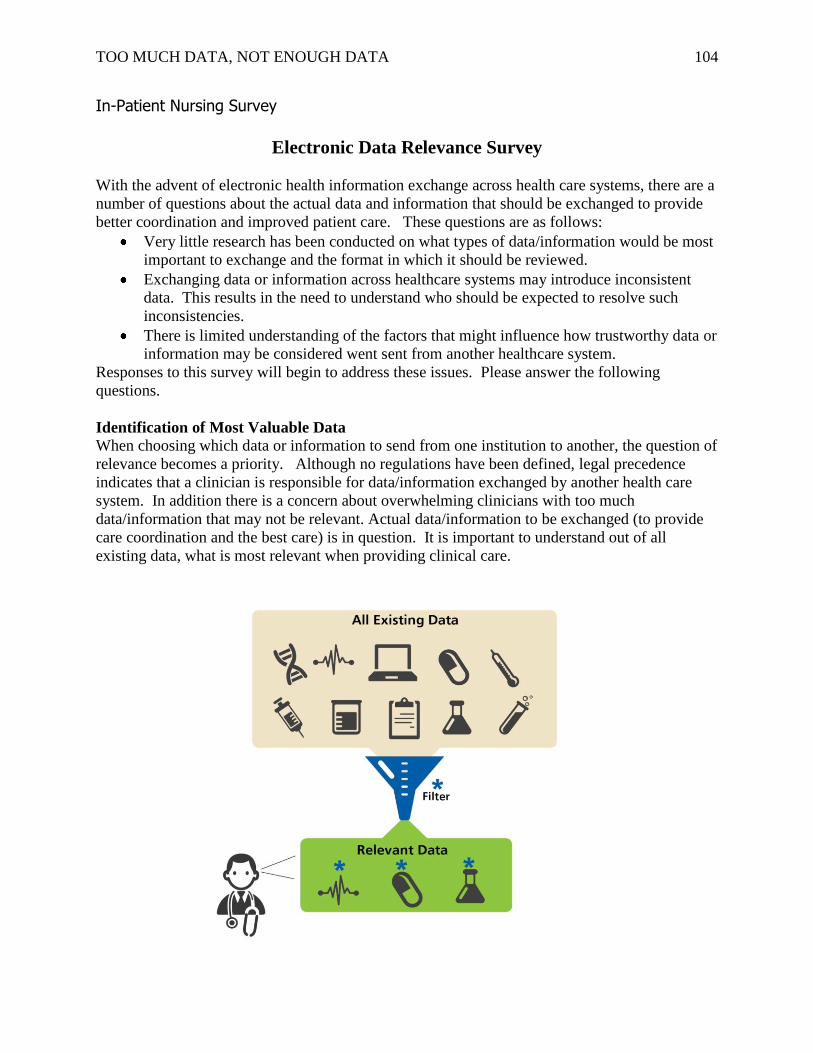
TOO MUCH DATA, NOT ENOUGH DATA 104
In-Patient Nursing Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data/information would be most
important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
data. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for data/information exchanged by another health care
system. In addition there is a concern about overwhelming clinicians with too much
data/information that may not be relevant. Actual data/information to be exchanged (to provide
care coordination and the best care) is in question. It is important to understand out of all
existing data, what is most relevant when providing clinical care.
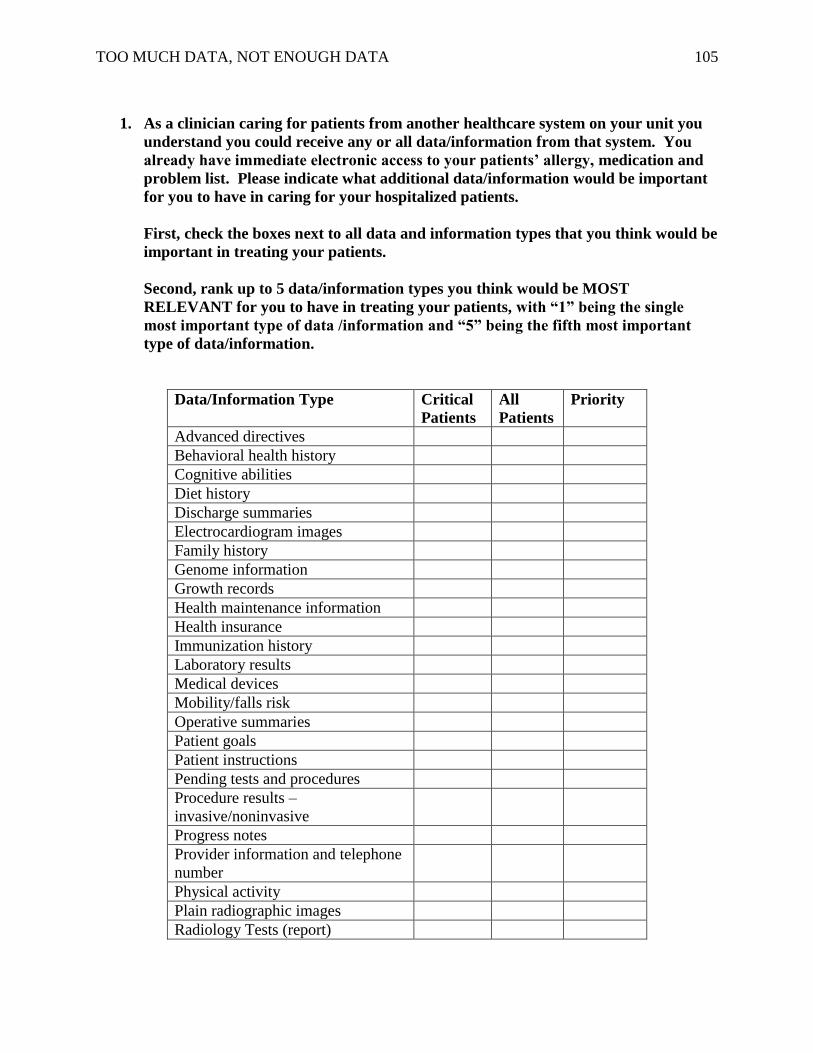
TOO MUCH DATA, NOT ENOUGH DATA 105
1. As a clinician caring for patients from another healthcare system on your unit you
understand you could receive any or all data/information from that system. You
already have immediate electronic access to your patients’ allergy, medication and
problem list. Please indicate what additional data/information would be important
for you to have in caring for your hospitalized patients.
First, check the boxes next to all data and information types that you think would be
important in treating your patients.
Second, rank up to 5 data/information types you think would be MOST
RELEVANT for you to have in treating your patients, with “1” being the single
most important type of data /information and “5” being the fifth most important
type of data/information.
Data/Information Type Critical
Patients
All
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
Radiology Tests (report)
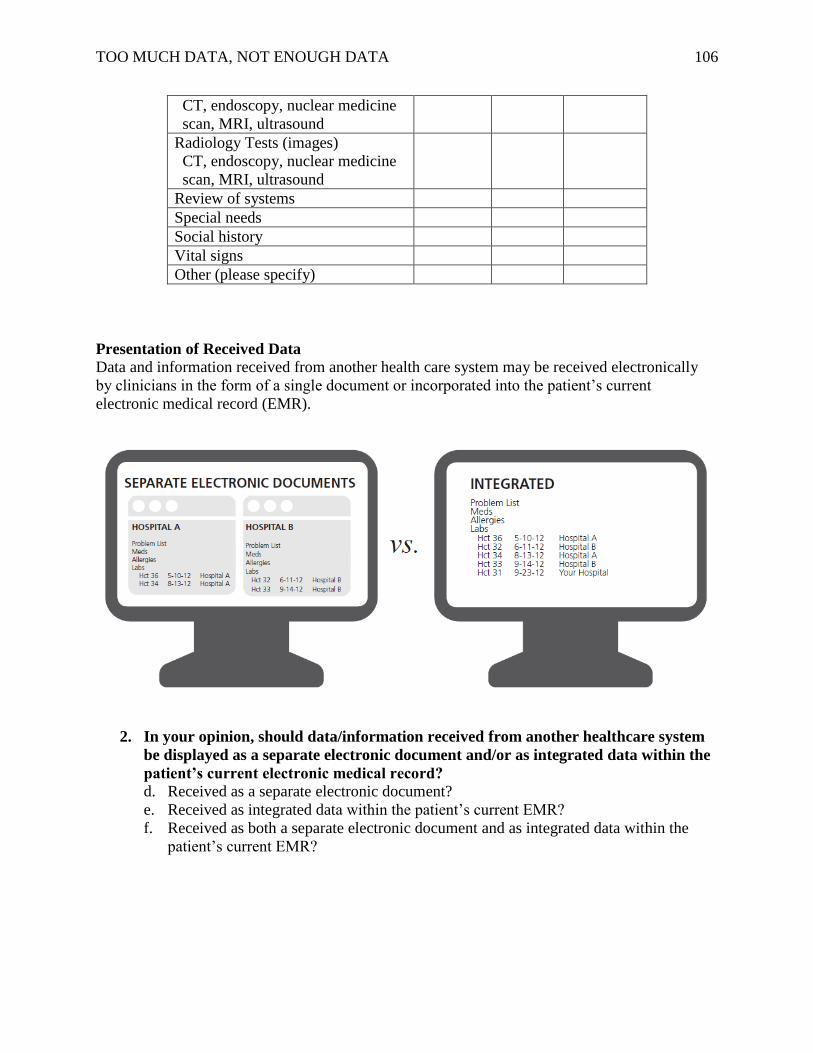
TOO MUCH DATA, NOT ENOUGH DATA 106
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
2. In your opinion, should data/information received from another healthcare system
be displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
d. Received as a separate electronic document?
e. Received as integrated data within the patient’s current EMR?
f. Received as both a separate electronic document and as integrated data within the
patient’s current EMR?
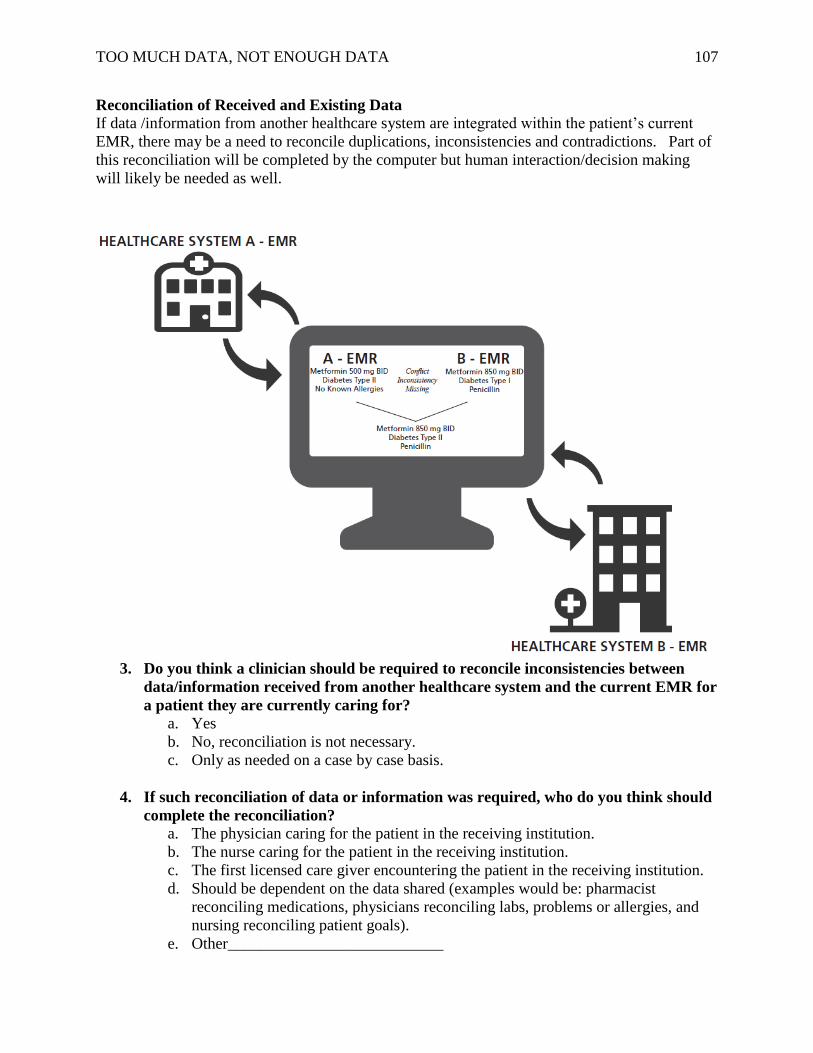
TOO MUCH DATA, NOT ENOUGH DATA 107
Reconciliation of Received and Existing Data
If data /information from another healthcare system are integrated within the patient’s current
EMR, there may be a need to reconcile duplications, inconsistencies and contradictions. Part of
this reconciliation will be completed by the computer but human interaction/decision making
will likely be needed as well.
3. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
4. If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
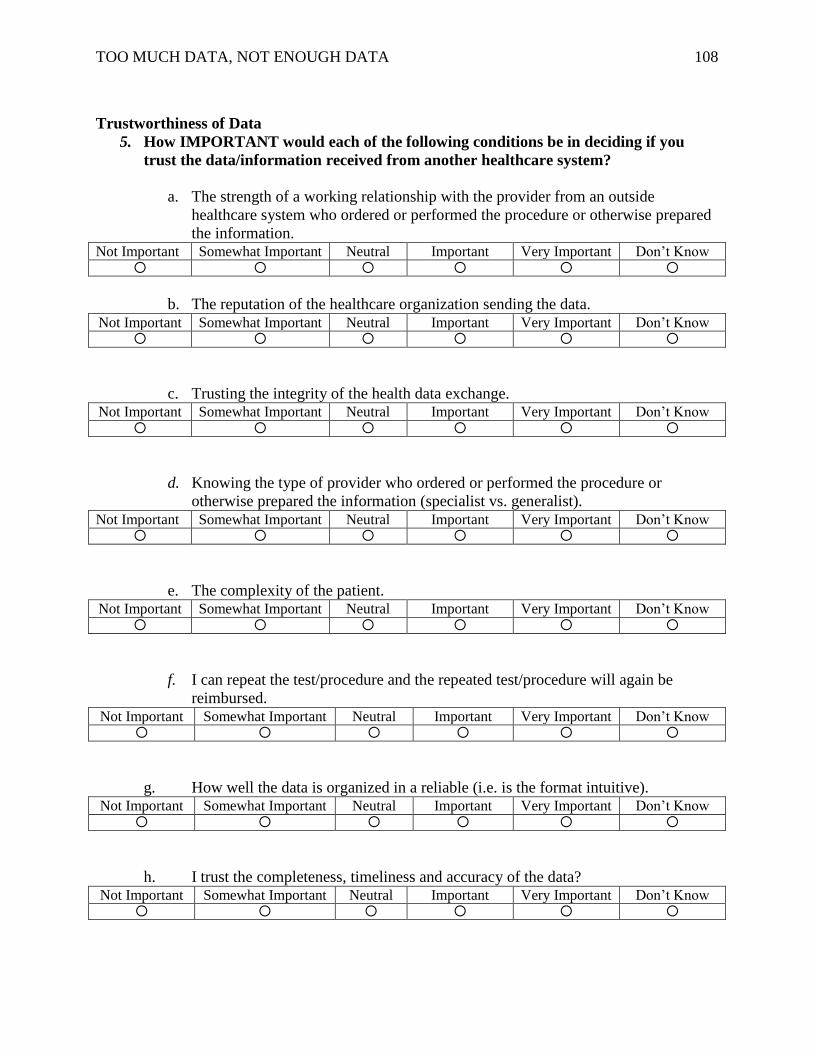
TOO MUCH DATA, NOT ENOUGH DATA 108
Trustworthiness of Data
5. How IMPORTANT would each of the following conditions be in deciding if you
trust the data/information received from another healthcare system?
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data is organized in a reliable (i.e. is the format intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
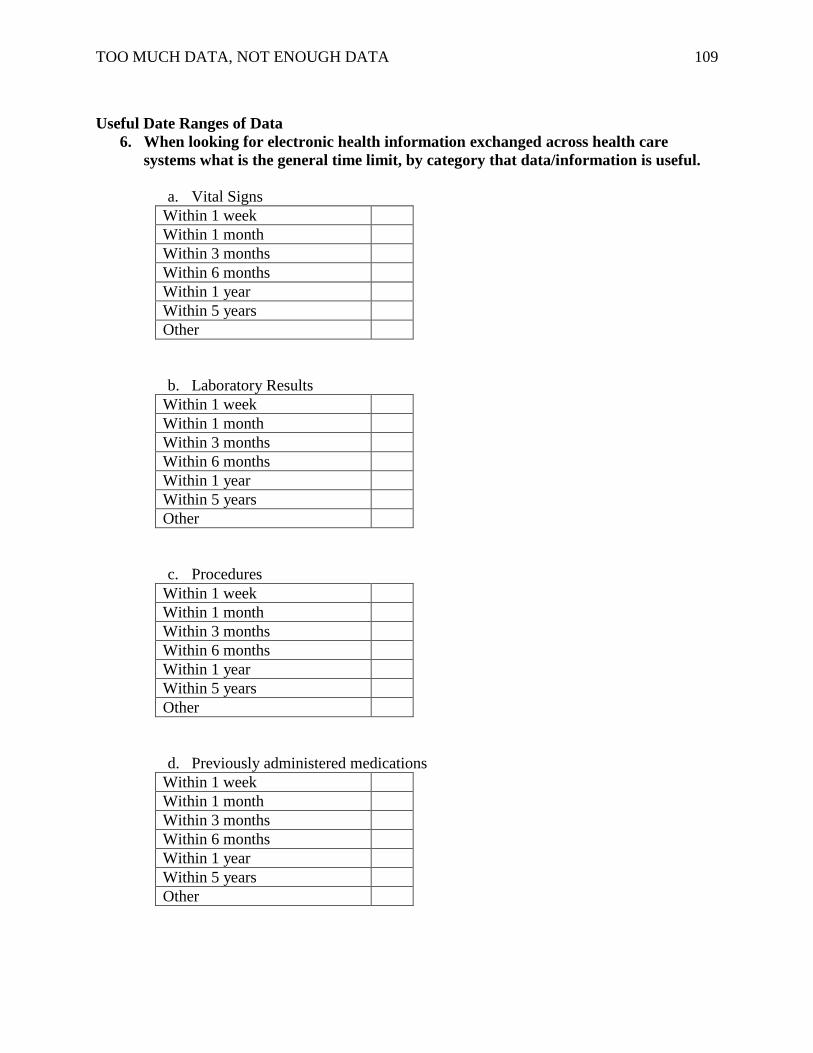
TOO MUCH DATA, NOT ENOUGH DATA 109
Useful Date Ranges of Data
6. When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
a. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
b. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
c. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
d. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
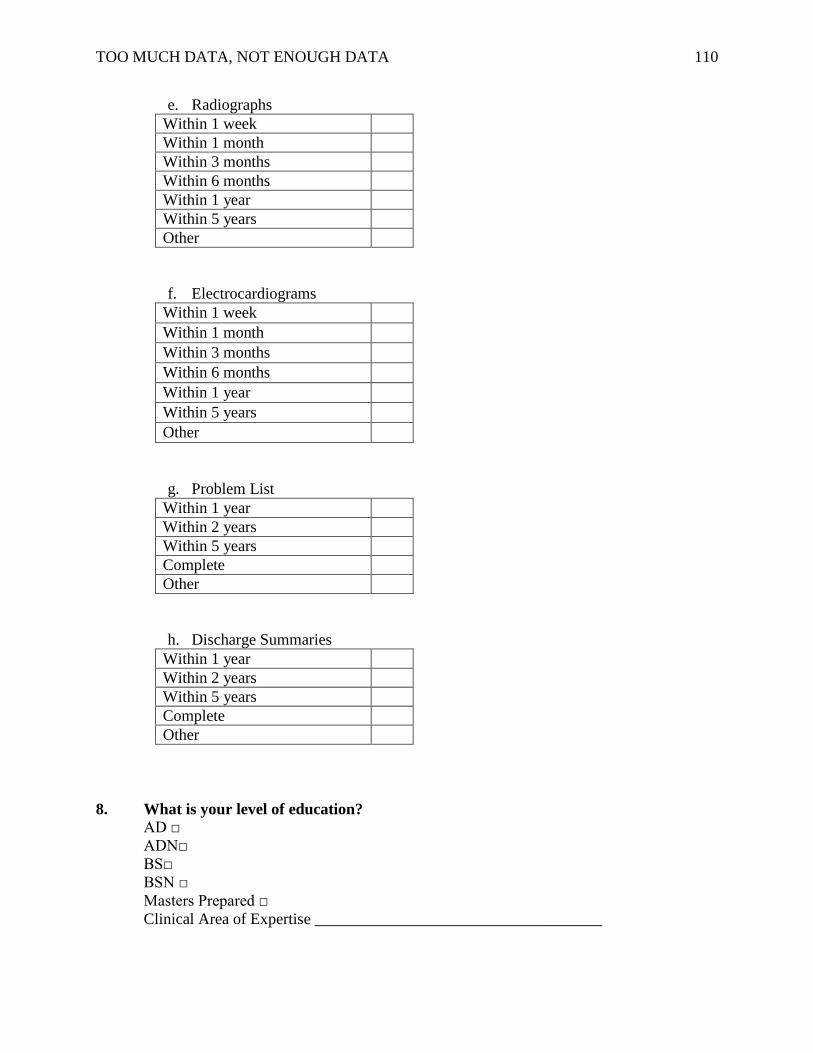
TOO MUCH DATA, NOT ENOUGH DATA 110
e. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
f. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
g. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
h. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your level of education?
AD □
ADN□
BS□
BSN □
Masters Prepared □
Clinical Area of Expertise ____________________________________

TOO MUCH DATA, NOT ENOUGH DATA 111
Appendix J
Electronic Data Relevance Survey – Inpatient
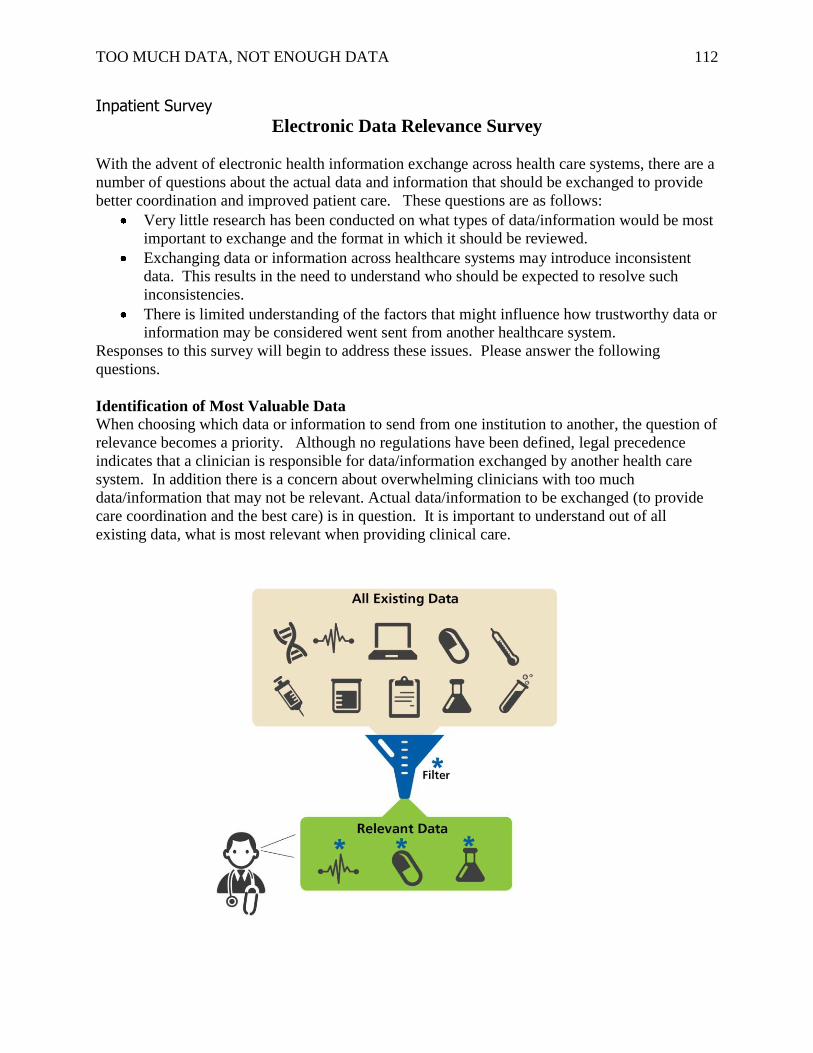
TOO MUCH DATA, NOT ENOUGH DATA 112
Inpatient Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data/information would be most
important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
data. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for data/information exchanged by another health care
system. In addition there is a concern about overwhelming clinicians with too much
data/information that may not be relevant. Actual data/information to be exchanged (to provide
care coordination and the best care) is in question. It is important to understand out of all
existing data, what is most relevant when providing clinical care.
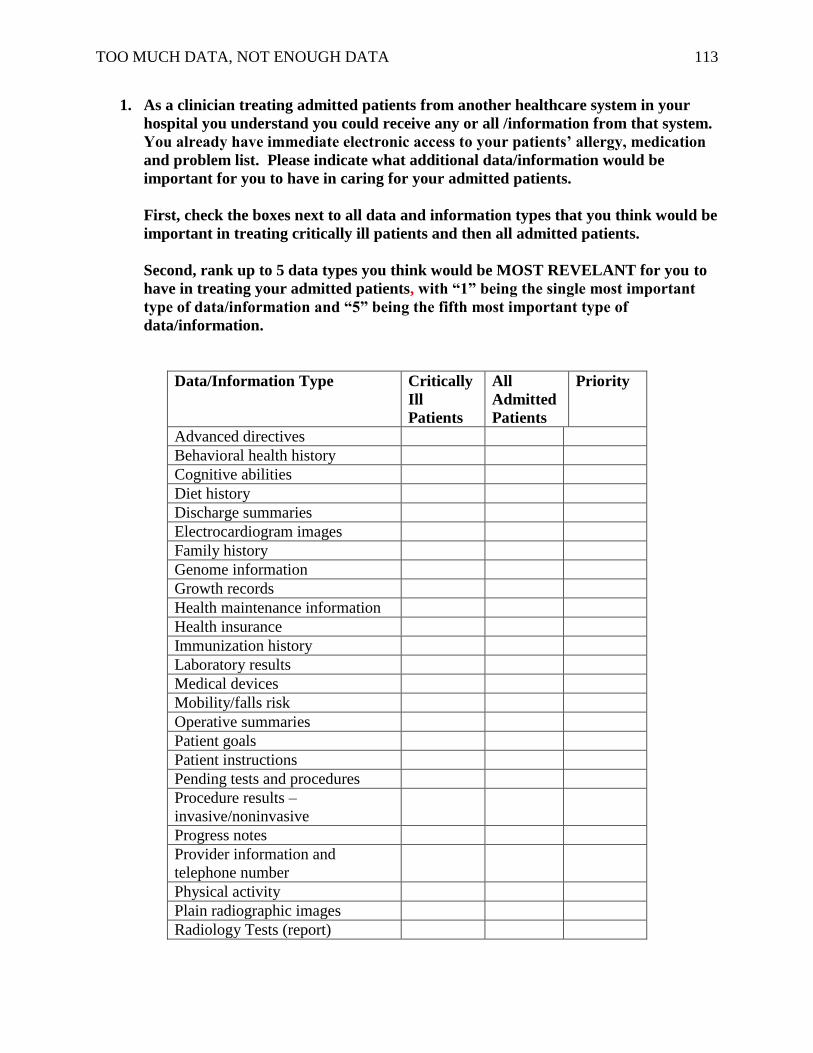
TOO MUCH DATA, NOT ENOUGH DATA 113
1. As a clinician treating admitted patients from another healthcare system in your
hospital you understand you could receive any or all /information from that system.
You already have immediate electronic access to your patients’ allergy, medication
and problem list. Please indicate what additional data/information would be
important for you to have in caring for your admitted patients.
First, check the boxes next to all data and information types that you think would be
important in treating critically ill patients and then all admitted patients.
Second, rank up to 5 data types you think would be MOST REVELANT for you to
have in treating your admitted patients, with “1” being the single most important
type of data/information and “5” being the fifth most important type of
data/information.
Data/Information Type Critically
Ill
Patients
All
Admitted
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and
telephone number
Physical activity
Plain radiographic images
Radiology Tests (report)
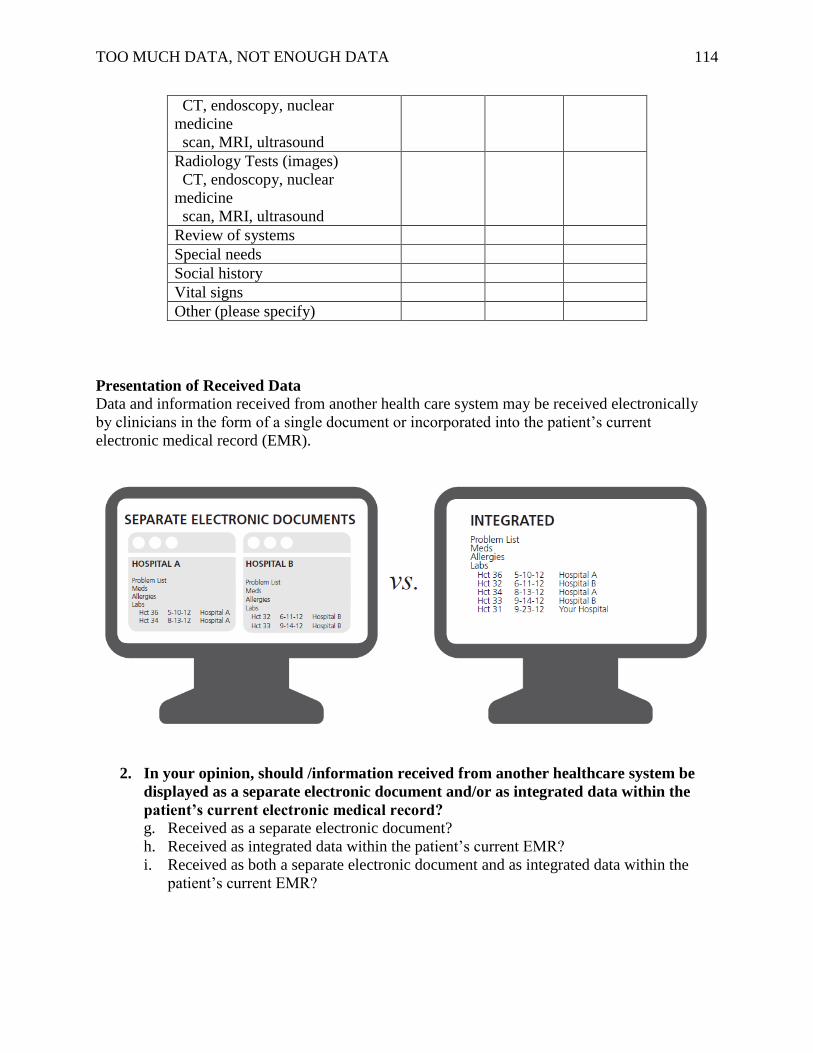
TOO MUCH DATA, NOT ENOUGH DATA 114
CT, endoscopy, nuclear
medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear
medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
2. In your opinion, should /information received from another healthcare system be
displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
g. Received as a separate electronic document?
h. Received as integrated data within the patient’s current EMR?
i. Received as both a separate electronic document and as integrated data within the
patient’s current EMR?
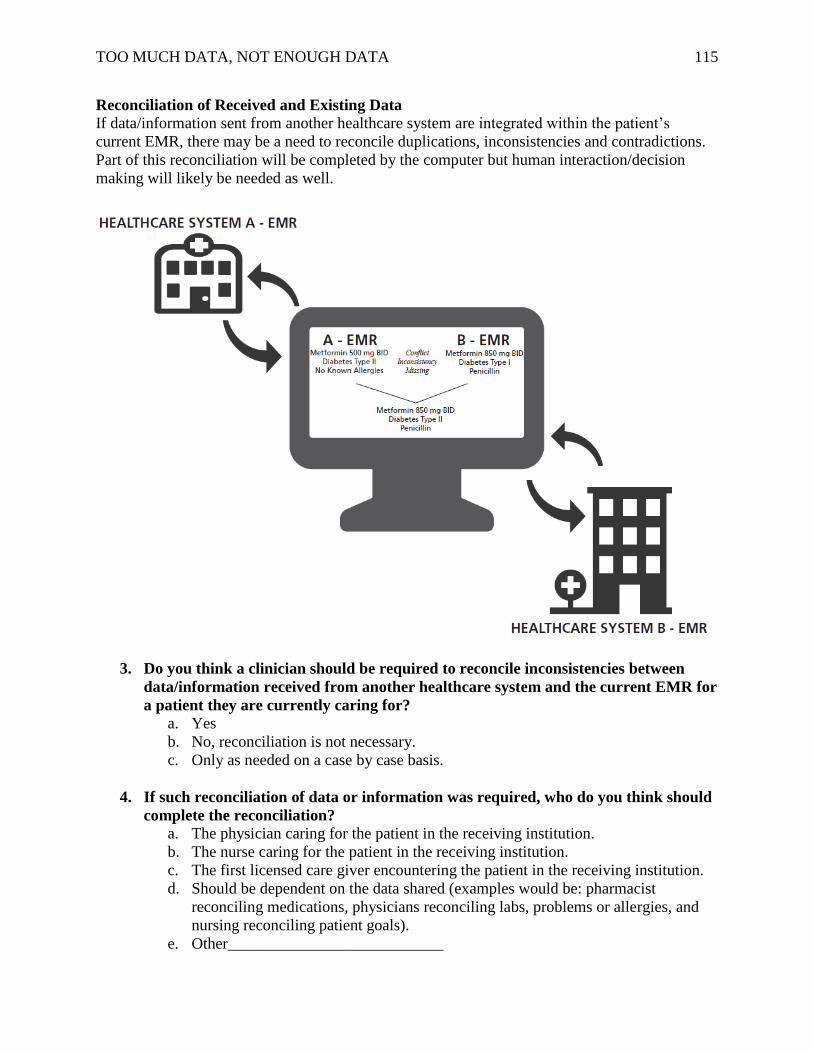
TOO MUCH DATA, NOT ENOUGH DATA 115
Reconciliation of Received and Existing Data
If data/information sent from another healthcare system are integrated within the patient’s
current EMR, there may be a need to reconcile duplications, inconsistencies and contradictions.
Part of this reconciliation will be completed by the computer but human interaction/decision
making will likely be needed as well.
3. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
4. If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
TOO MUCH DATA, NOT ENOUGH DATA 116
Trustworthiness of Data
5. How IMPORTANT would each of the following conditions be in deciding if you
trust the data/information received from another healthcare system?
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data is organized in a reliable (i.e. is the format intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
TOO MUCH DATA, NOT ENOUGH DATA 117
Useful Date Ranges of Data
6. When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
a. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
b. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
c. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
d. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
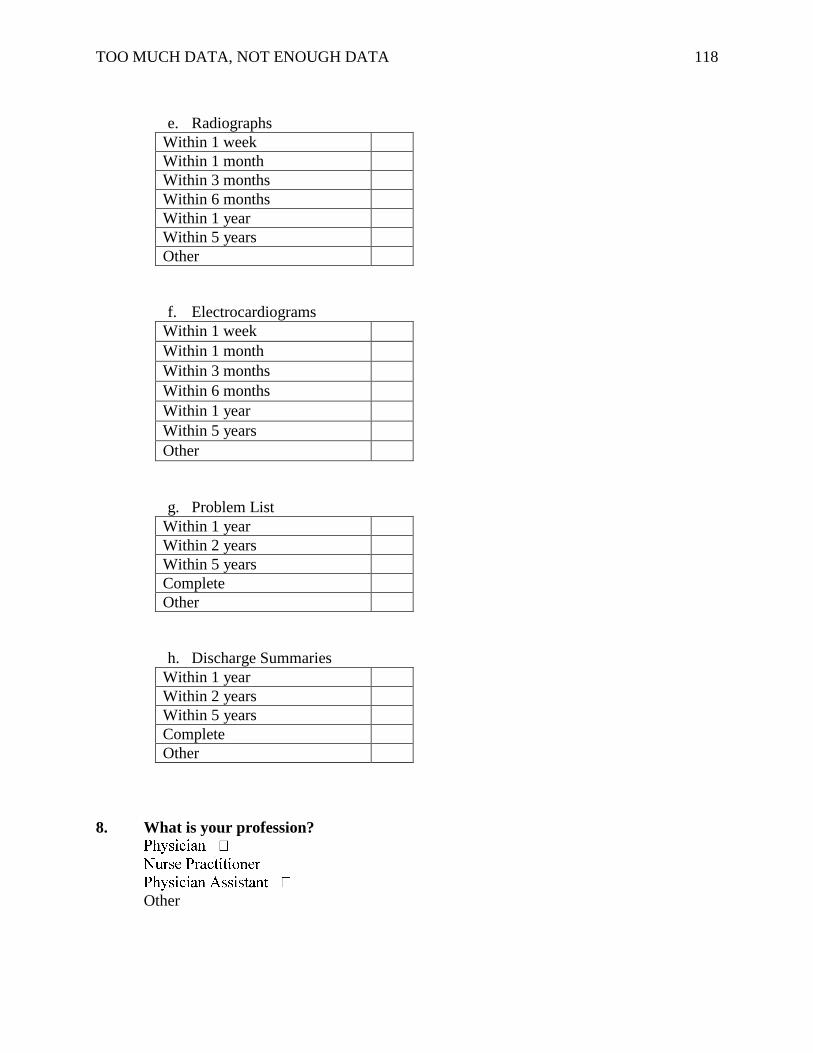
TOO MUCH DATA, NOT ENOUGH DATA 118
e. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
f. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
g. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
h. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your profession?
Other

TOO MUCH DATA, NOT ENOUGH DATA 119
Appendix K
Electronic Data Relevance Survey – Primary Care
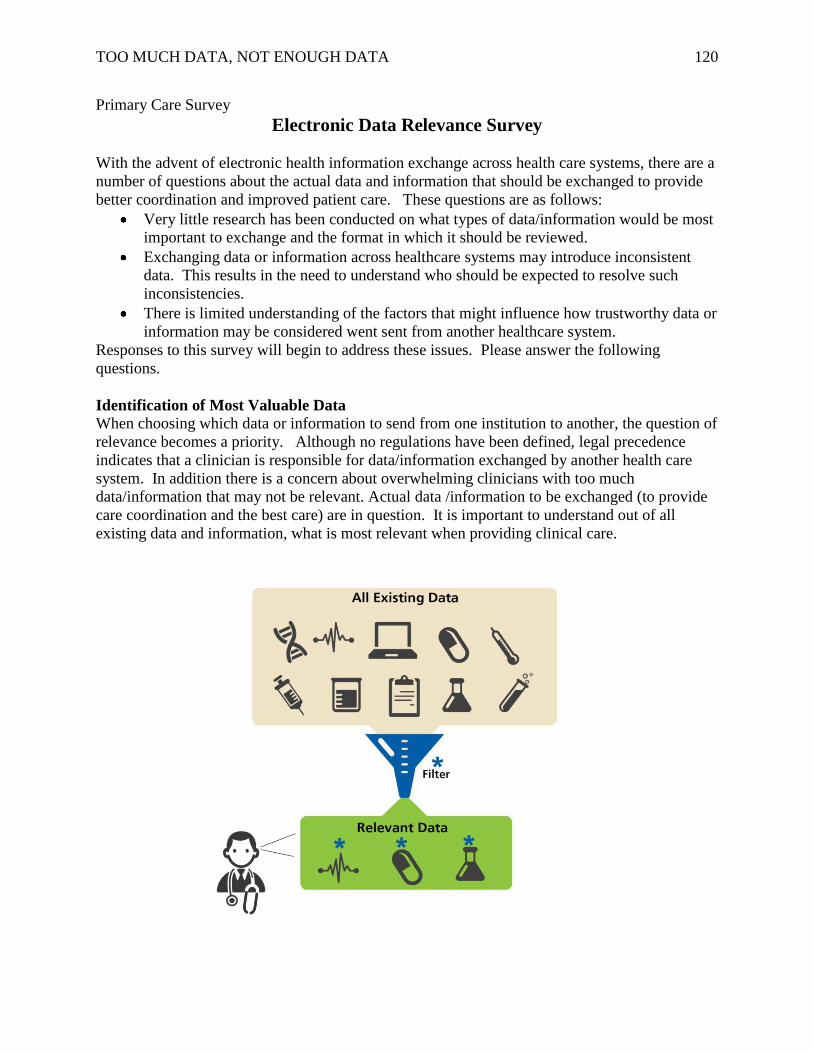
TOO MUCH DATA, NOT ENOUGH DATA 120
Primary Care Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data/information would be most
important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
data. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for data/information exchanged by another health care
system. In addition there is a concern about overwhelming clinicians with too much
data/information that may not be relevant. Actual data /information to be exchanged (to provide
care coordination and the best care) are in question. It is important to understand out of all
existing data and information, what is most relevant when providing clinical care.
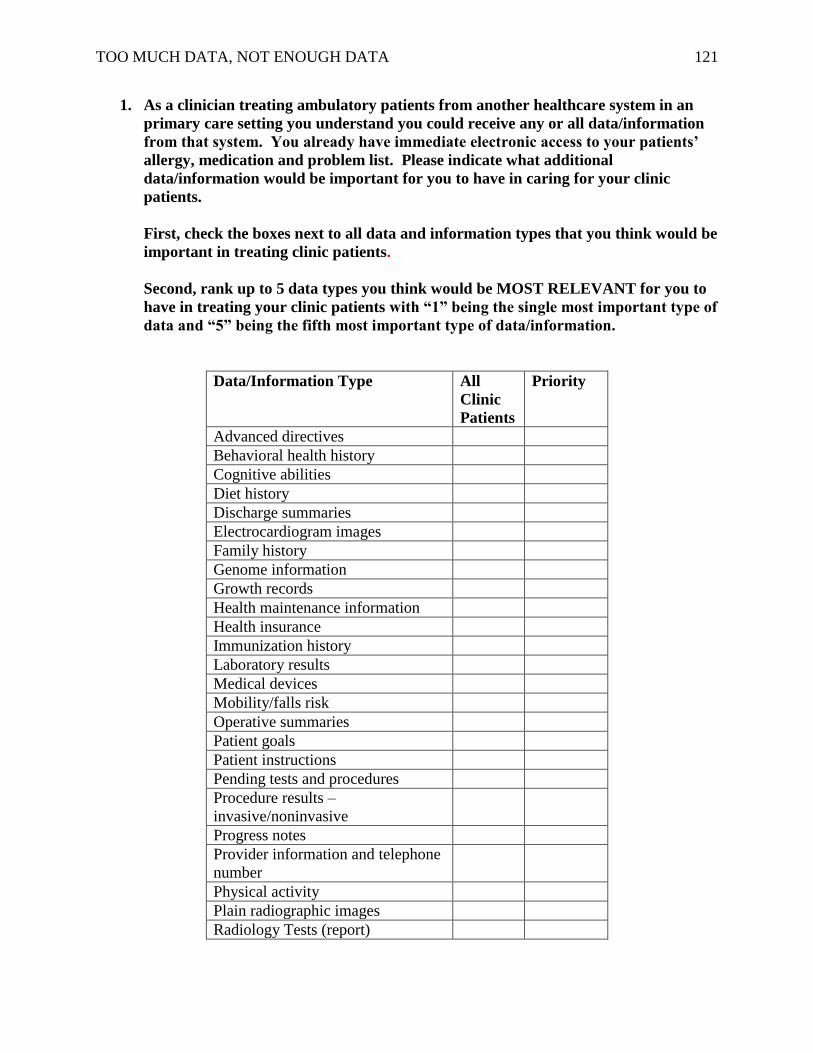
TOO MUCH DATA, NOT ENOUGH DATA 121
1. As a clinician treating ambulatory patients from another healthcare system in an
primary care setting you understand you could receive any or all data/information
from that system. You already have immediate electronic access to your patients’
allergy, medication and problem list. Please indicate what additional
data/information would be important for you to have in caring for your clinic
patients.
First, check the boxes next to all data and information types that you think would be
important in treating clinic patients.
Second, rank up to 5 data types you think would be MOST RELEVANT for you to
have in treating your clinic patients with “1” being the single most important type of
data and “5” being the fifth most important type of data/information.
Data/Information Type All
Clinic
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
Radiology Tests (report)
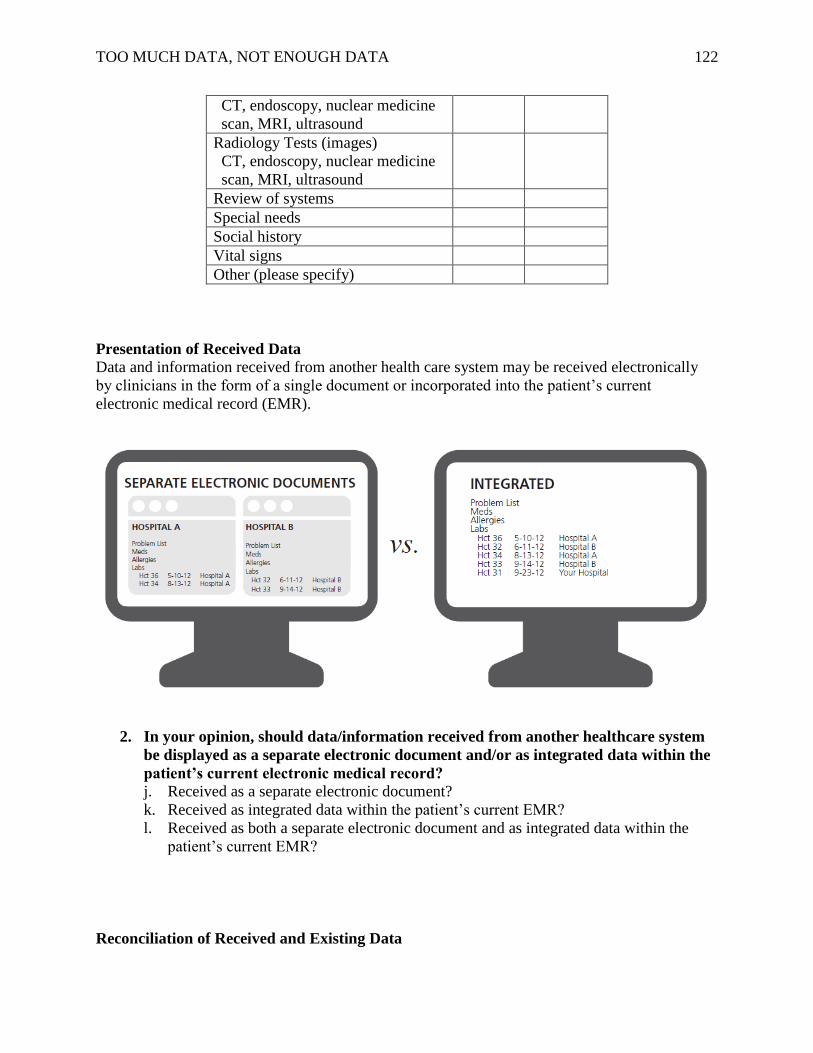
TOO MUCH DATA, NOT ENOUGH DATA 122
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
2. In your opinion, should data/information received from another healthcare system
be displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
j. Received as a separate electronic document?
k. Received as integrated data within the patient’s current EMR?
l. Received as both a separate electronic document and as integrated data within the
patient’s current EMR?
Reconciliation of Received and Existing Data
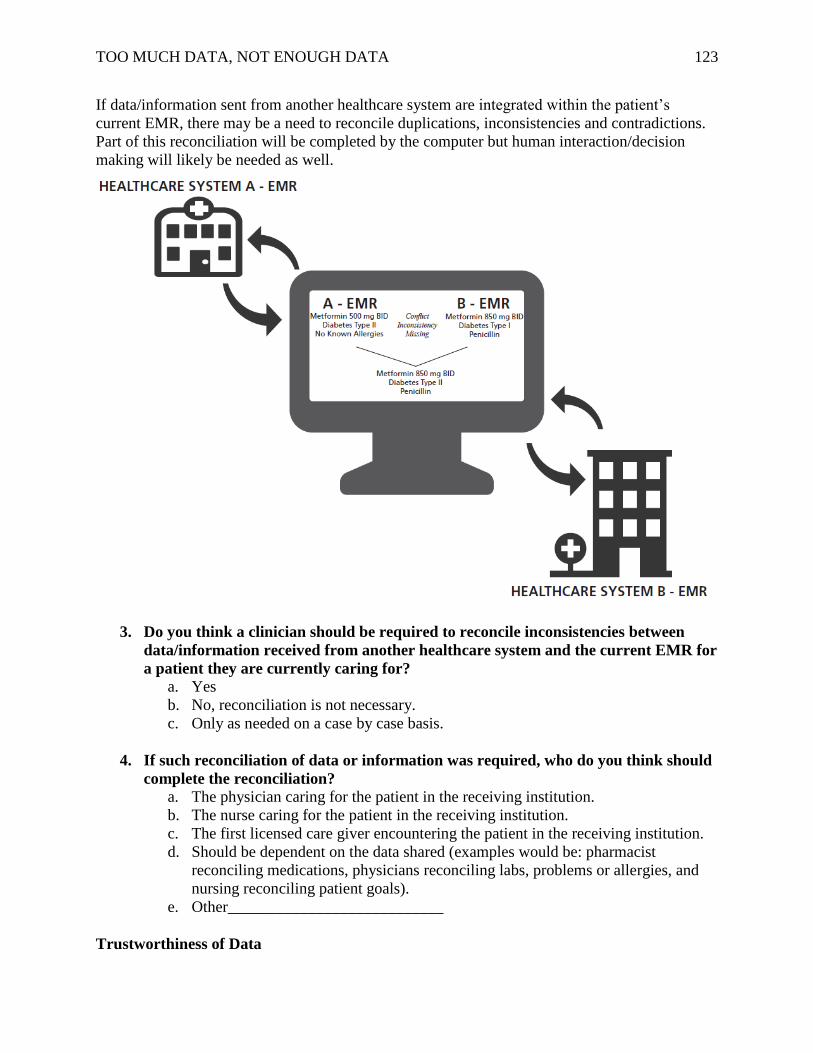
TOO MUCH DATA, NOT ENOUGH DATA 123
If data/information sent from another healthcare system are integrated within the patient’s
current EMR, there may be a need to reconcile duplications, inconsistencies and contradictions.
Part of this reconciliation will be completed by the computer but human interaction/decision
making will likely be needed as well.
3. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
4. If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
Trustworthiness of Data
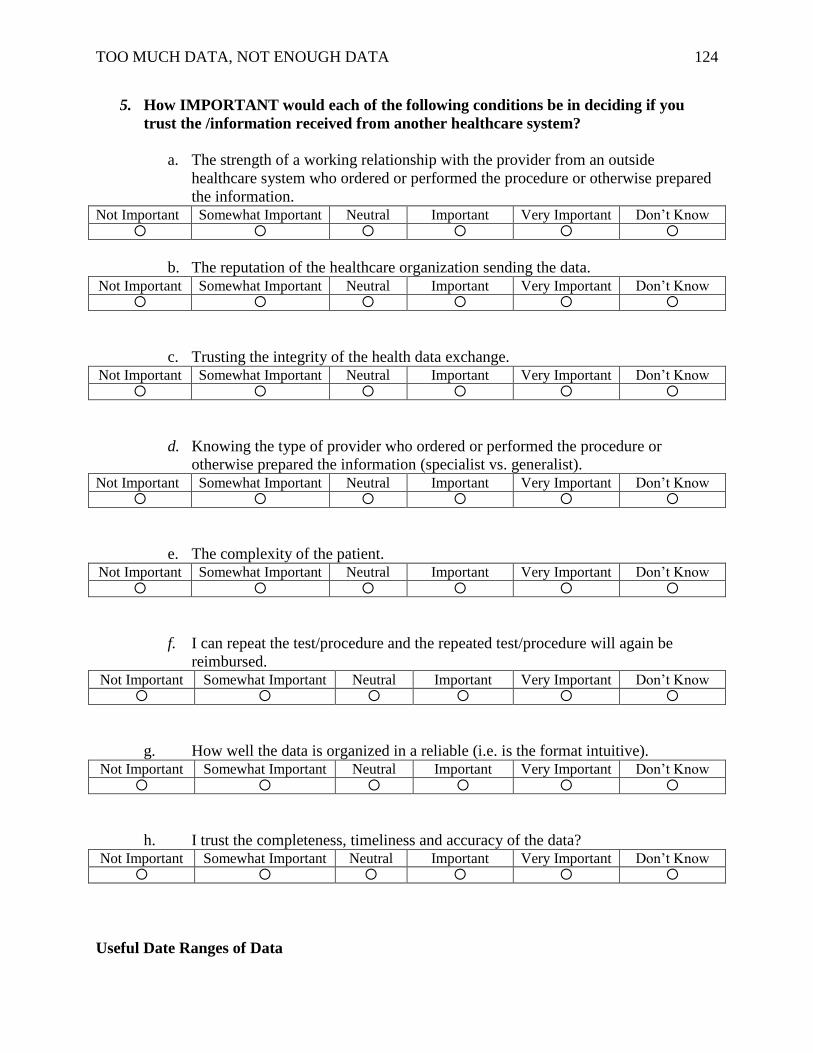
TOO MUCH DATA, NOT ENOUGH DATA 124
5. How IMPORTANT would each of the following conditions be in deciding if you
trust the /information received from another healthcare system?
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data is organized in a reliable (i.e. is the format intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
Useful Date Ranges of Data
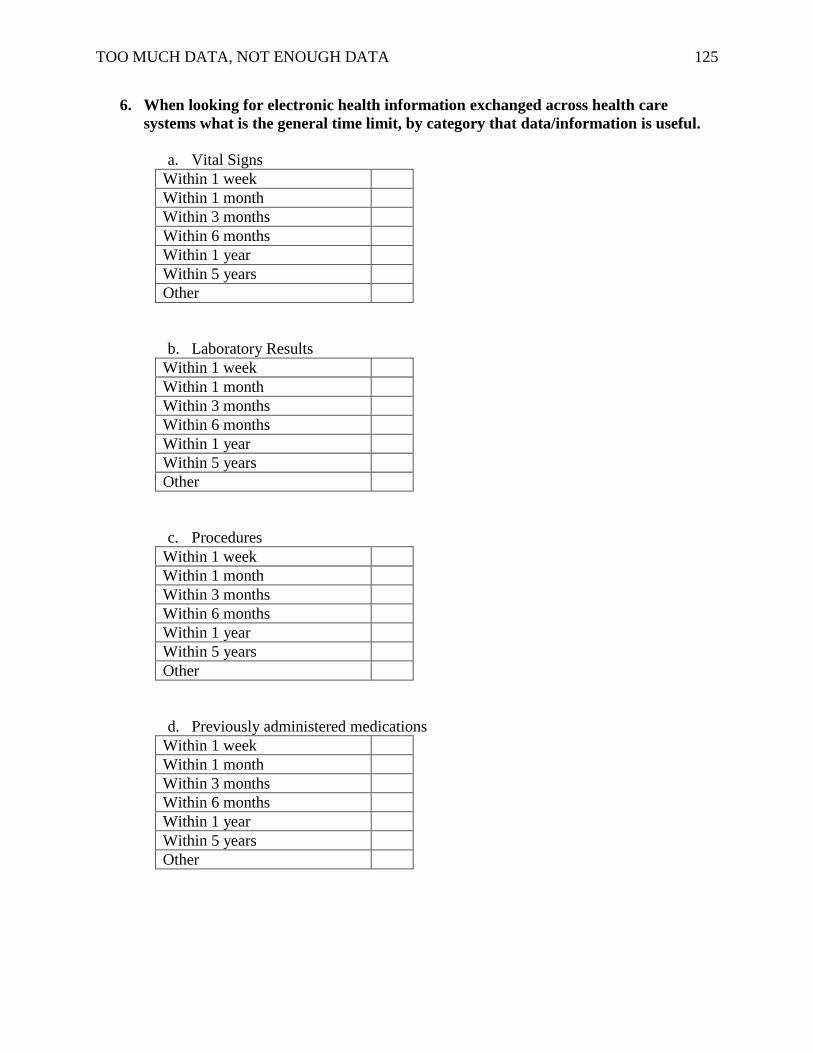
TOO MUCH DATA, NOT ENOUGH DATA 125
6. When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
a. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
b. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
c. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
d. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
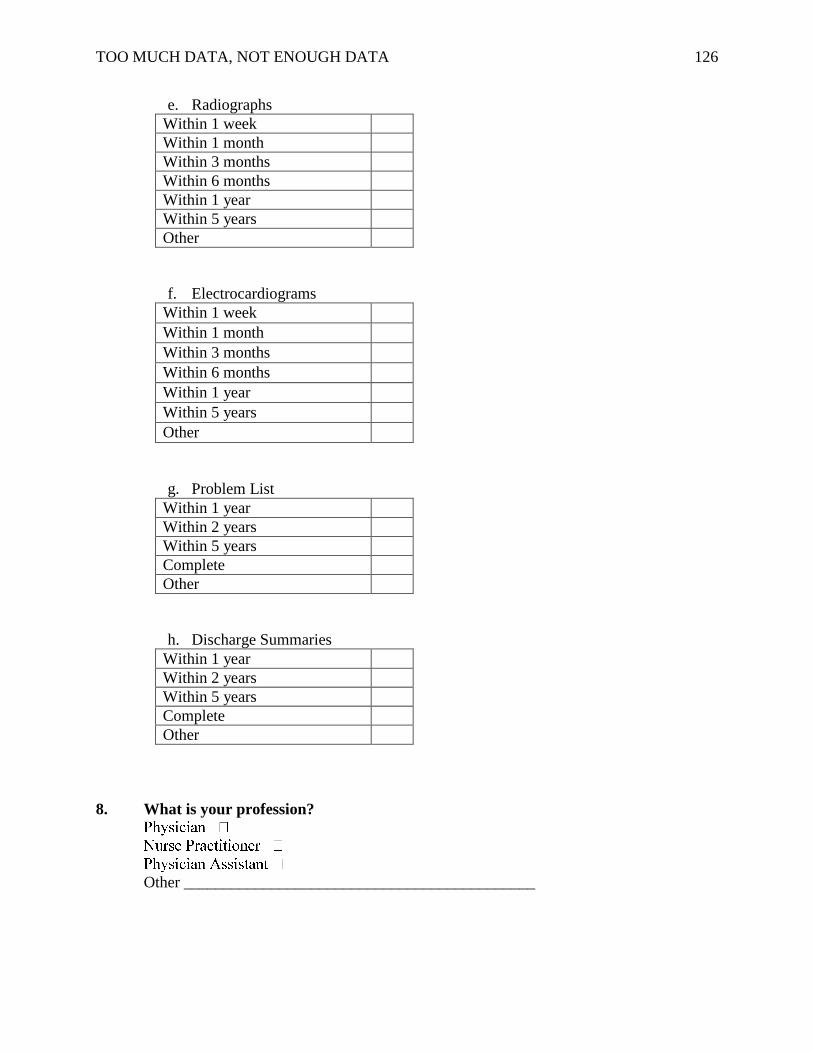
TOO MUCH DATA, NOT ENOUGH DATA 126
e. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
f. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
g. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
h. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your profession?
Other ____________________________________________

TOO MUCH DATA, NOT ENOUGH DATA 127
Appendix L
Electronic Data Relevance Survey – Electronic Copy
TOO MUCH DATA, NOT ENOUGH DATA 128
Electronic Survey
Electronic Data Relevance Survey
Welcome to the Electronic Data Relevance Survey. Thank you for taking some time to provide
your feedback.
With the advent of electronic health information exchange across healthcare systems, there are a
number of issues about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These issues include the following:
Very little research has been conducted on what types of data and information would be
most relevant to exchange and the format in which they should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
results. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered to be when received from another healthcare system.
Responses to this survey will help begin to address these issues. Please answer the questions that
follow.
Identification of Most Relevant Data
When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for information exchanged by another healthcare system.
In addition there is a concern about overwhelming clinicians with too much information that may
not be relevant. Actual data or information to be exchanged (to provide care coordination and the
best care) are in question. It is important to understand out of all existing data and information,
what is most relevant when providing clinical care.
The figure below is intended to illustrate the idea of identifying the most relevant information to
share between healthcare systems.
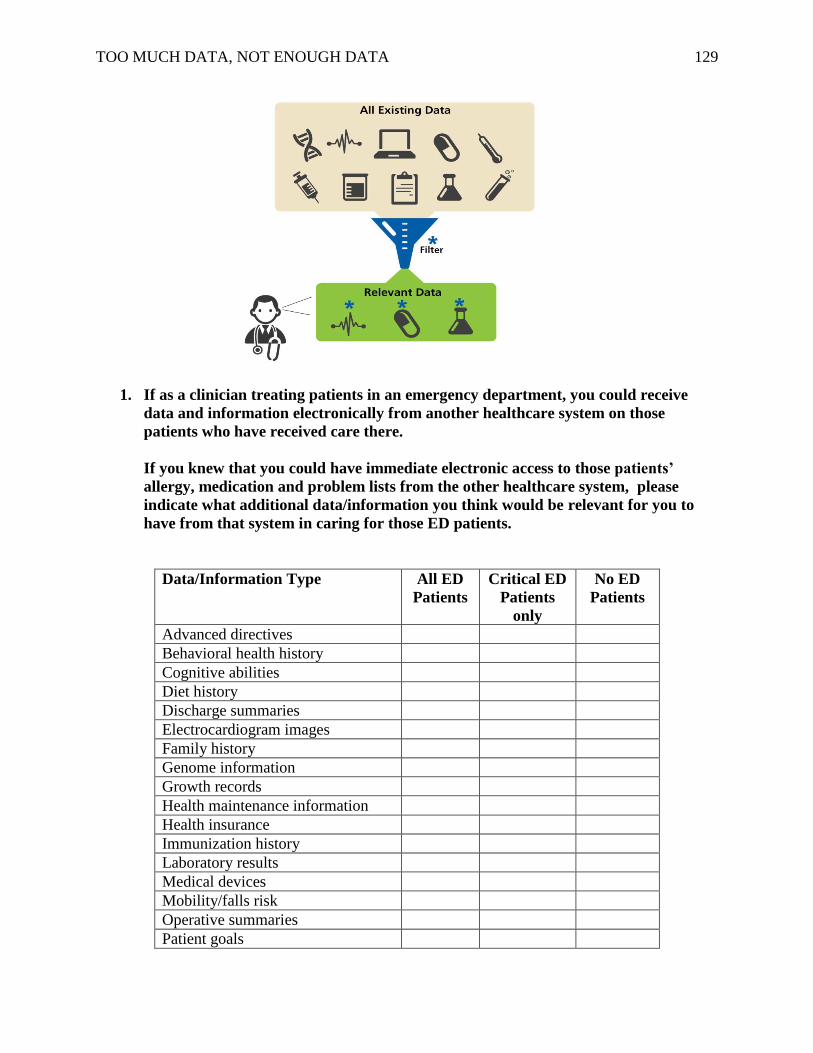
TOO MUCH DATA, NOT ENOUGH DATA 129
1. If as a clinician treating patients in an emergency department, you could receive
data and information electronically from another healthcare system on those
patients who have received care there.
If you knew that you could have immediate electronic access to those patients’
allergy, medication and problem lists from the other healthcare system, please
indicate what additional data/information you think would be relevant for you to
have from that system in caring for those ED patients.
Data/Information Type All ED
Patients
Critical ED
Patients
only
No ED
Patients
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
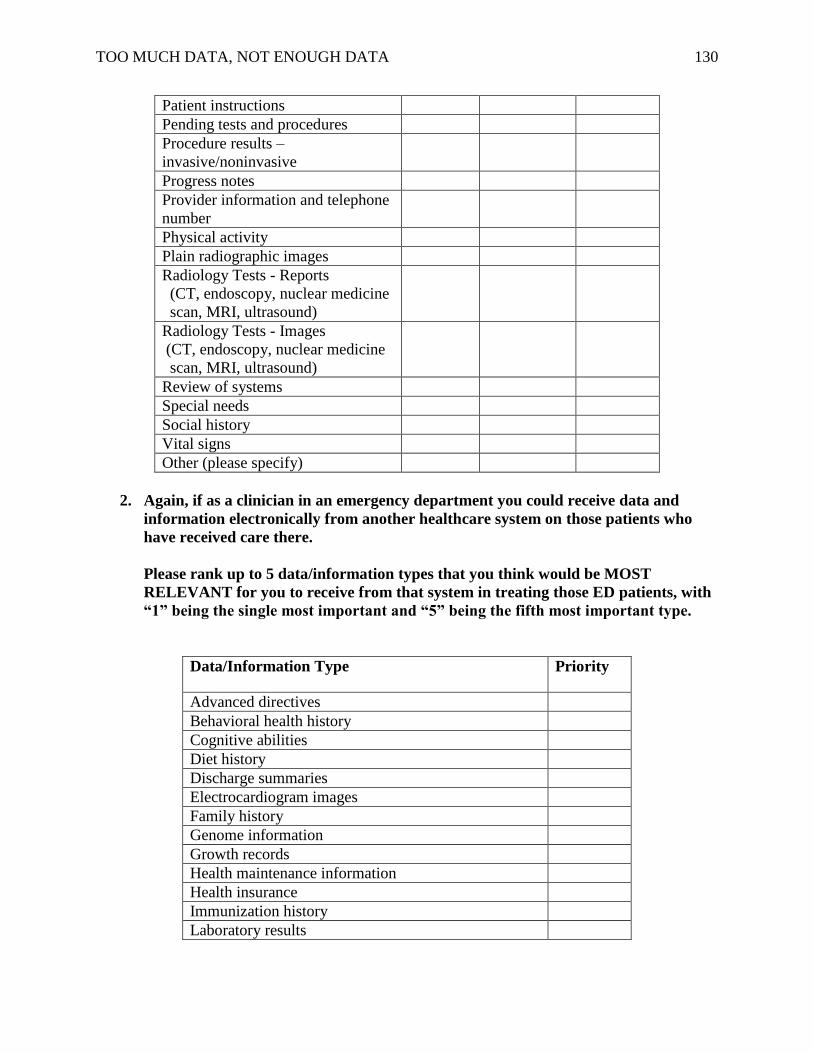
TOO MUCH DATA, NOT ENOUGH DATA 130
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
Radiology Tests - Reports
(CT, endoscopy, nuclear medicine
scan, MRI, ultrasound)
Radiology Tests - Images
(CT, endoscopy, nuclear medicine
scan, MRI, ultrasound)
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
2. Again, if as a clinician in an emergency department you could receive data and
information electronically from another healthcare system on those patients who
have received care there.
Please rank up to 5 data/information types that you think would be MOST
RELEVANT for you to receive from that system in treating those ED patients, with
“1” being the single most important and “5” being the fifth most important type.
Data/Information Type Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
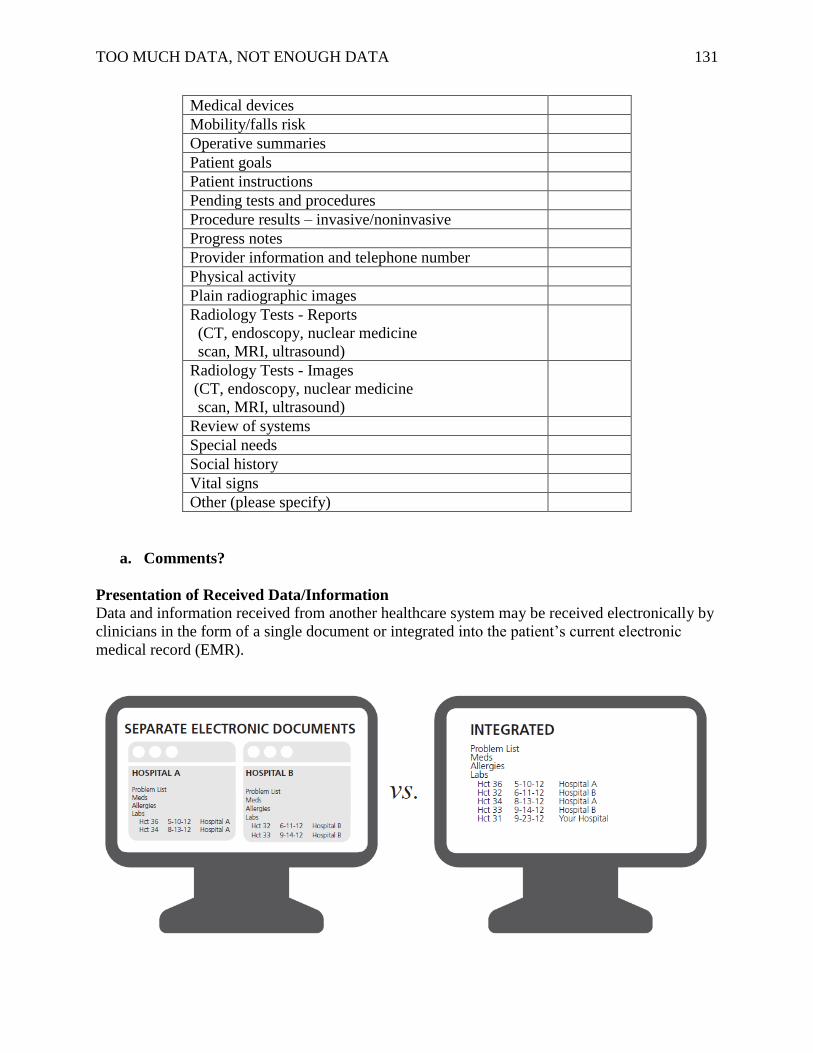
TOO MUCH DATA, NOT ENOUGH DATA 131
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results – invasive/noninvasive
Progress notes
Provider information and telephone number
Physical activity
Plain radiographic images
Radiology Tests - Reports
(CT, endoscopy, nuclear medicine
scan, MRI, ultrasound)
Radiology Tests - Images
(CT, endoscopy, nuclear medicine
scan, MRI, ultrasound)
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
a. Comments?
Presentation of Received Data/Information
Data and information received from another healthcare system may be received electronically by
clinicians in the form of a single document or integrated into the patient’s current electronic
medical record (EMR).
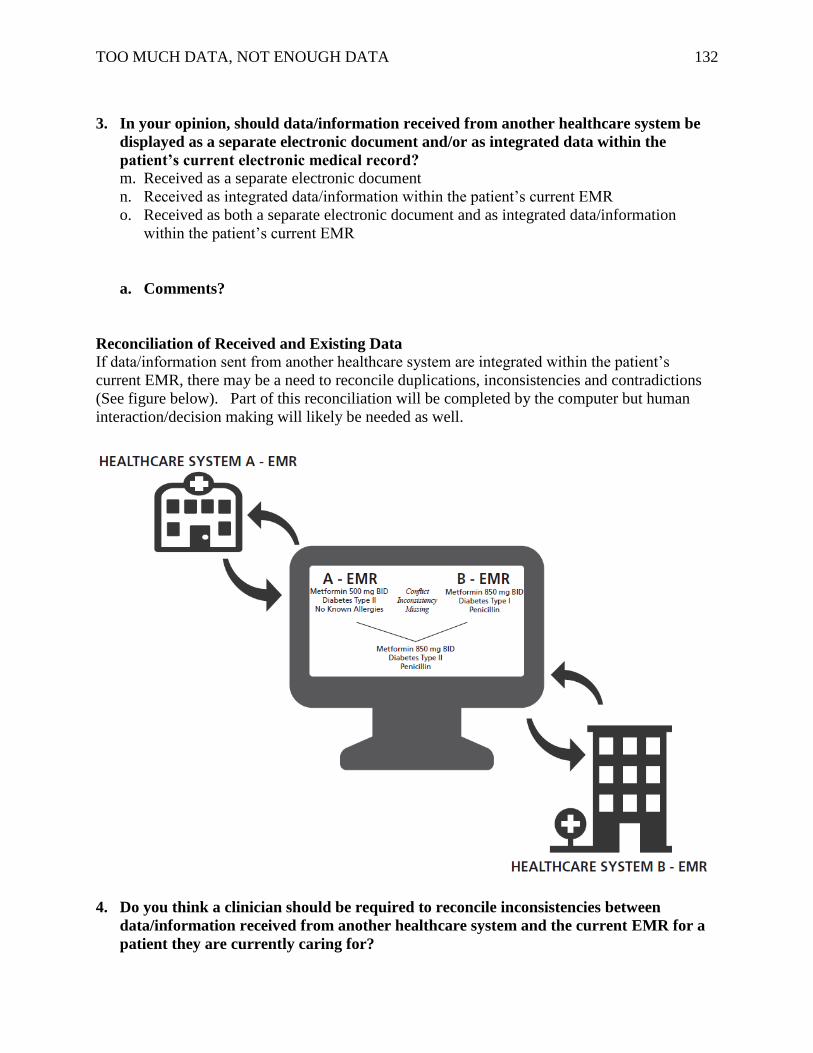
TOO MUCH DATA, NOT ENOUGH DATA 132
3. In your opinion, should data/information received from another healthcare system be
displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
m. Received as a separate electronic document
n. Received as integrated data/information within the patient’s current EMR
o. Received as both a separate electronic document and as integrated data/information
within the patient’s current EMR
a. Comments?
Reconciliation of Received and Existing Data
If data/information sent from another healthcare system are integrated within the patient’s
current EMR, there may be a need to reconcile duplications, inconsistencies and contradictions
(See figure below). Part of this reconciliation will be completed by the computer but human
interaction/decision making will likely be needed as well.
4. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for a
patient they are currently caring for?
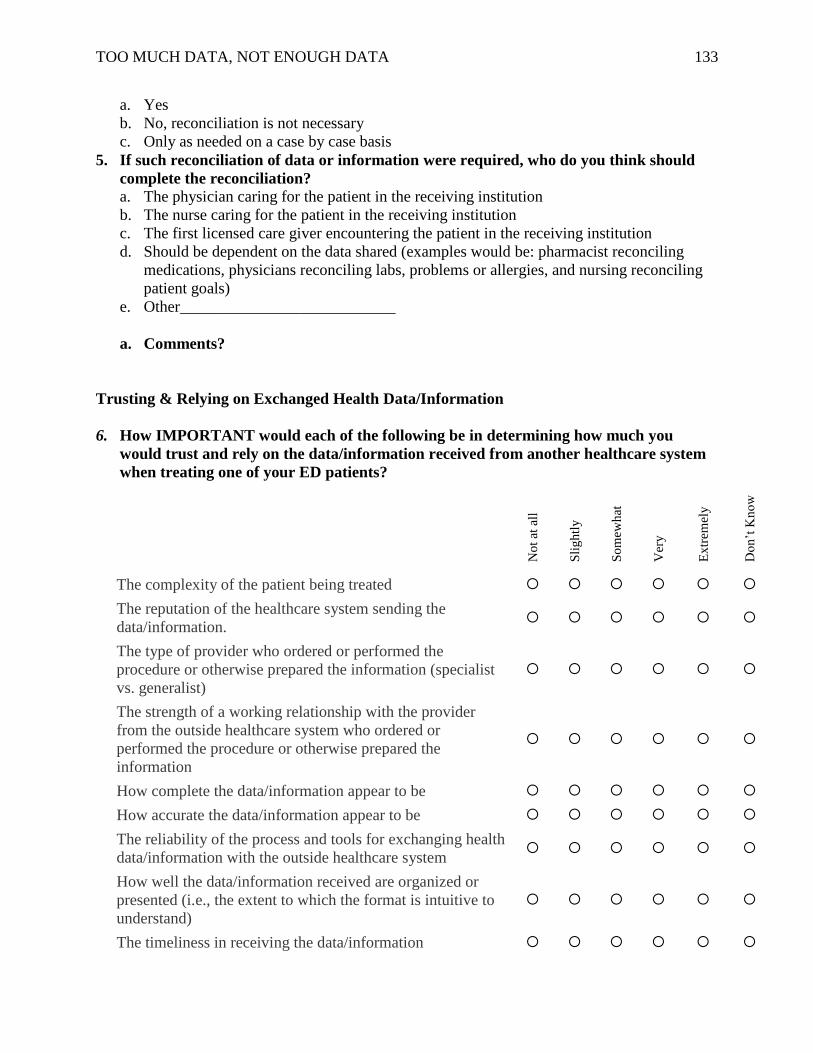
TOO MUCH DATA, NOT ENOUGH DATA 133
a. Yes
b. No, reconciliation is not necessary
c. Only as needed on a case by case basis
5. If such reconciliation of data or information were required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution
b. The nurse caring for the patient in the receiving institution
c. The first licensed care giver encountering the patient in the receiving institution
d. Should be dependent on the data shared (examples would be: pharmacist reconciling
medications, physicians reconciling labs, problems or allergies, and nursing reconciling
patient goals)
e. Other___________________________
a. Comments?
Trusting & Relying on Exchanged Health Data/Information
6. How IMPORTANT would each of the following be in determining how much you
would trust and rely on the data/information received from another healthcare system
when treating one of your ED patients?
No
t at
all
Sli
gh
tly
So
mew
hat
Ver
y
Ex
trem
ely
Do
n’t
Kn
ow
The complexity of the patient being treated
The reputation of the healthcare system sending the
data/information.
The type of provider who ordered or performed the
procedure or otherwise prepared the information (specialist
vs. generalist)
The strength of a working relationship with the provider
from the outside healthcare system who ordered or
performed the procedure or otherwise prepared the
information
How complete the data/information appear to be
How accurate the data/information appear to be
The reliability of the process and tools for exchanging health
data/information with the outside healthcare system
How well the data/information received are organized or
presented (i.e., the extent to which the format is intuitive to
understand)
The timeliness in receiving the data/information
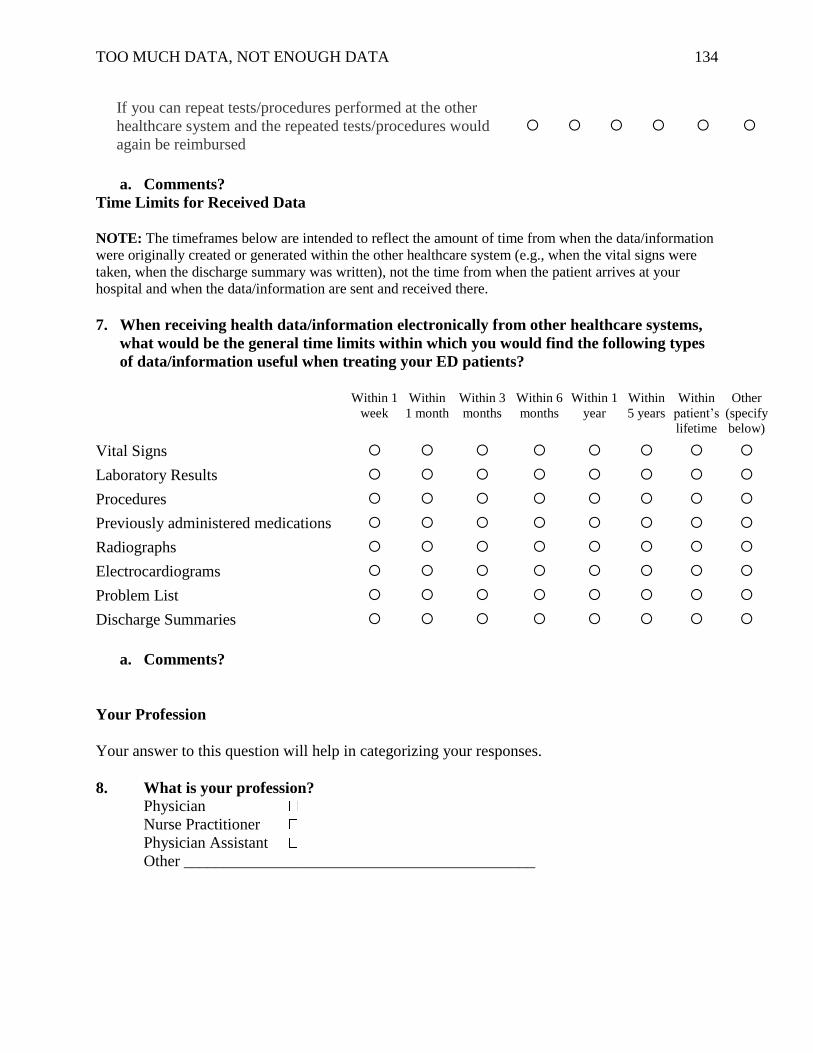
TOO MUCH DATA, NOT ENOUGH DATA 134
If you can repeat tests/procedures performed at the other
healthcare system and the repeated tests/procedures would
again be reimbursed
a. Comments?
Time Limits for Received Data
NOTE: The timeframes below are intended to reflect the amount of time from when the data/information
were originally created or generated within the other healthcare system (e.g., when the vital signs were
taken, when the discharge summary was written), not the time from when the patient arrives at your
hospital and when the data/information are sent and received there.
7. When receiving health data/information electronically from other healthcare systems,
what would be the general time limits within which you would find the following types
of data/information useful when treating your ED patients?
Within 1
week
Within
1 month
Within 3
months
Within 6
months
Within 1
year
Within
5 years
Within
patient’s
lifetime
Other
(specify
below)
Vital Signs
Laboratory Results
Procedures
Previously administered medications
Radiographs
Electrocardiograms
Problem List
Discharge Summaries
a. Comments?
Your Profession
Your answer to this question will help in categorizing your responses.
8. What is your profession?
Physician
Nurse Practitioner
Physician Assistant
Other ____________________________________________

TOO MUCH DATA, NOT ENOUGH DATA 135
Appendix M
Electronic Data Relevance Survey – Pediatrics
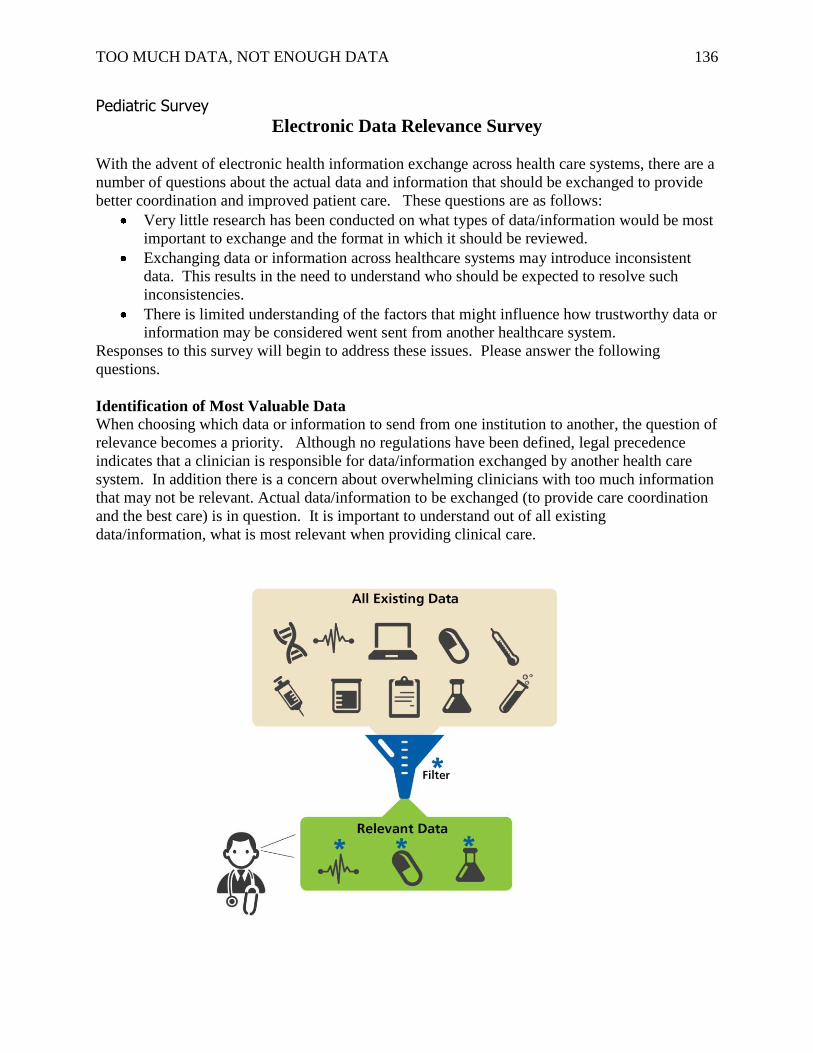
TOO MUCH DATA, NOT ENOUGH DATA 136
Pediatric Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data/information would be most
important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
data. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for data/information exchanged by another health care
system. In addition there is a concern about overwhelming clinicians with too much information
that may not be relevant. Actual data/information to be exchanged (to provide care coordination
and the best care) is in question. It is important to understand out of all existing
data/information, what is most relevant when providing clinical care.
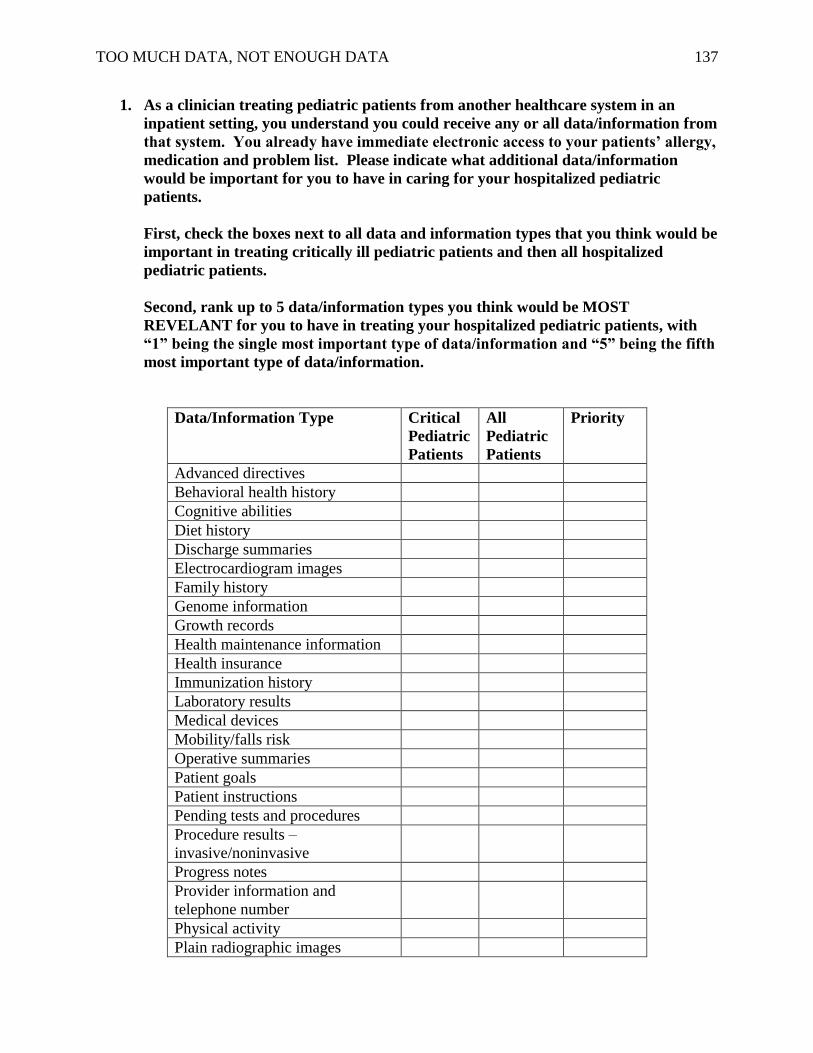
TOO MUCH DATA, NOT ENOUGH DATA 137
1. As a clinician treating pediatric patients from another healthcare system in an
inpatient setting, you understand you could receive any or all data/information from
that system. You already have immediate electronic access to your patients’ allergy,
medication and problem list. Please indicate what additional data/information
would be important for you to have in caring for your hospitalized pediatric
patients.
First, check the boxes next to all data and information types that you think would be
important in treating critically ill pediatric patients and then all hospitalized
pediatric patients.
Second, rank up to 5 data/information types you think would be MOST
REVELANT for you to have in treating your hospitalized pediatric patients, with
“1” being the single most important type of data/information and “5” being the fifth
most important type of data/information.
Data/Information Type Critical
Pediatric
Patients
All
Pediatric
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and
telephone number
Physical activity
Plain radiographic images
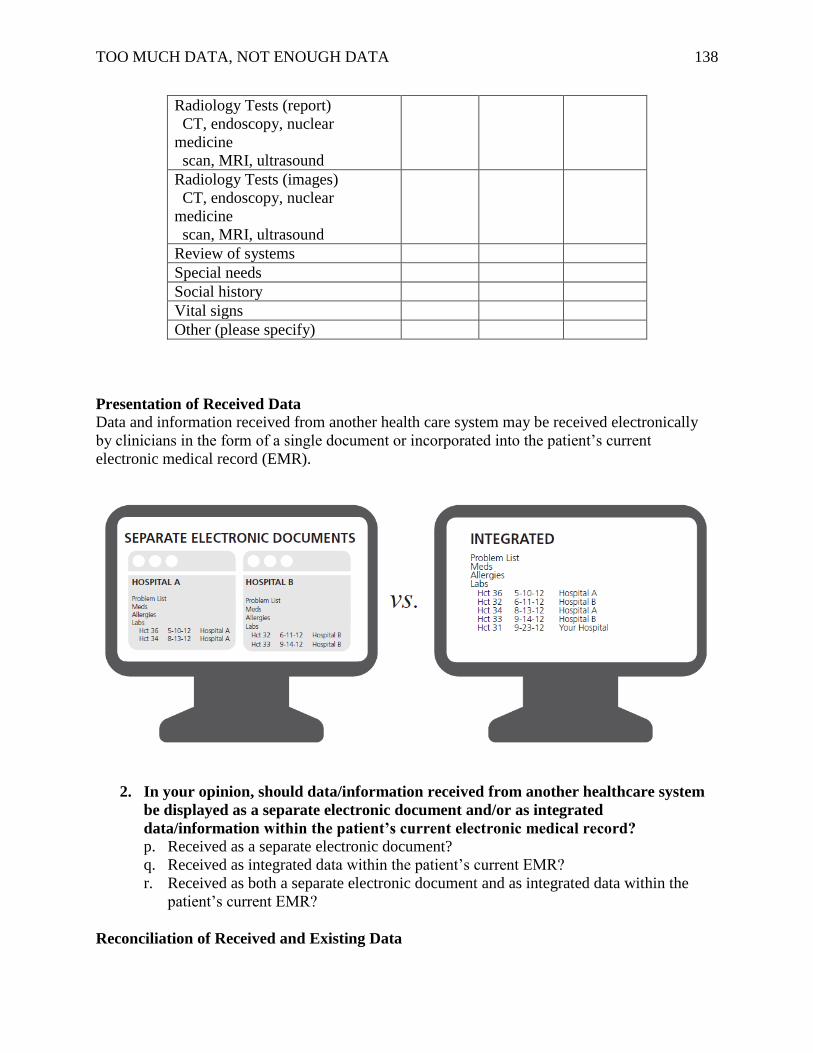
TOO MUCH DATA, NOT ENOUGH DATA 138
Radiology Tests (report)
CT, endoscopy, nuclear
medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear
medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
2. In your opinion, should data/information received from another healthcare system
be displayed as a separate electronic document and/or as integrated
data/information within the patient’s current electronic medical record?
p. Received as a separate electronic document?
q. Received as integrated data within the patient’s current EMR?
r. Received as both a separate electronic document and as integrated data within the
patient’s current EMR?
Reconciliation of Received and Existing Data
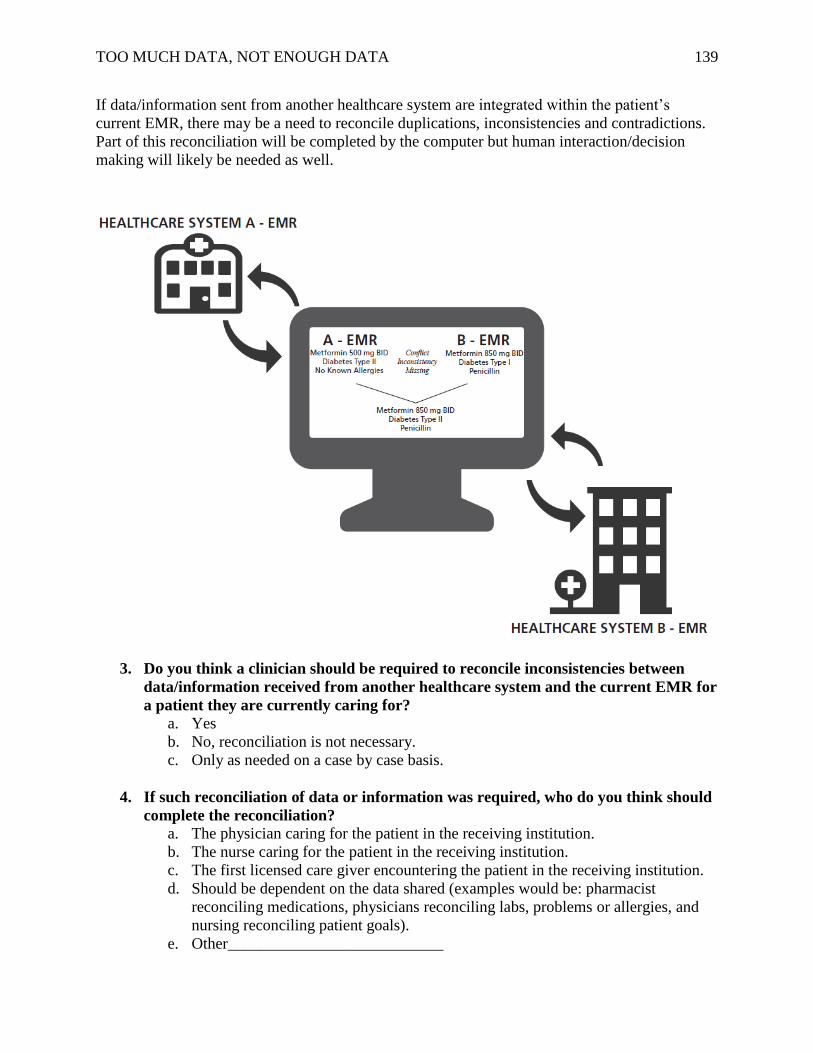
TOO MUCH DATA, NOT ENOUGH DATA 139
If data/information sent from another healthcare system are integrated within the patient’s
current EMR, there may be a need to reconcile duplications, inconsistencies and contradictions.
Part of this reconciliation will be completed by the computer but human interaction/decision
making will likely be needed as well.
3. Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
4. If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
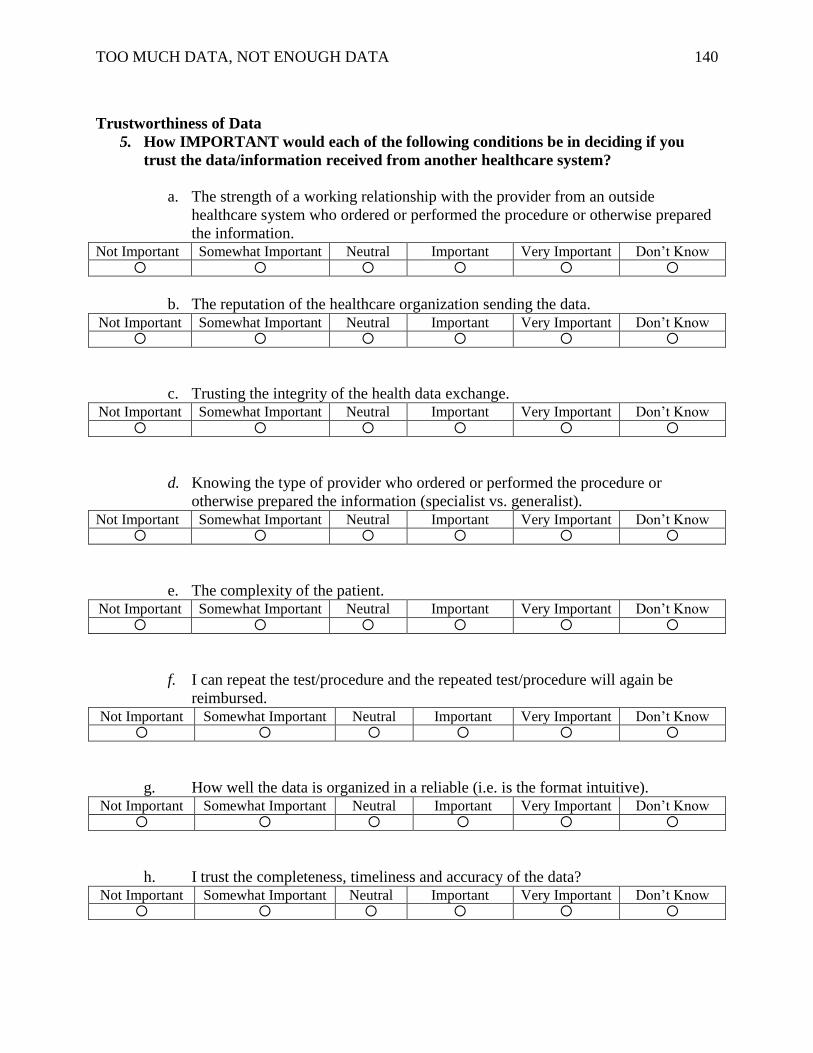
TOO MUCH DATA, NOT ENOUGH DATA 140
Trustworthiness of Data
5. How IMPORTANT would each of the following conditions be in deciding if you
trust the data/information received from another healthcare system?
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data is organized in a reliable (i.e. is the format intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
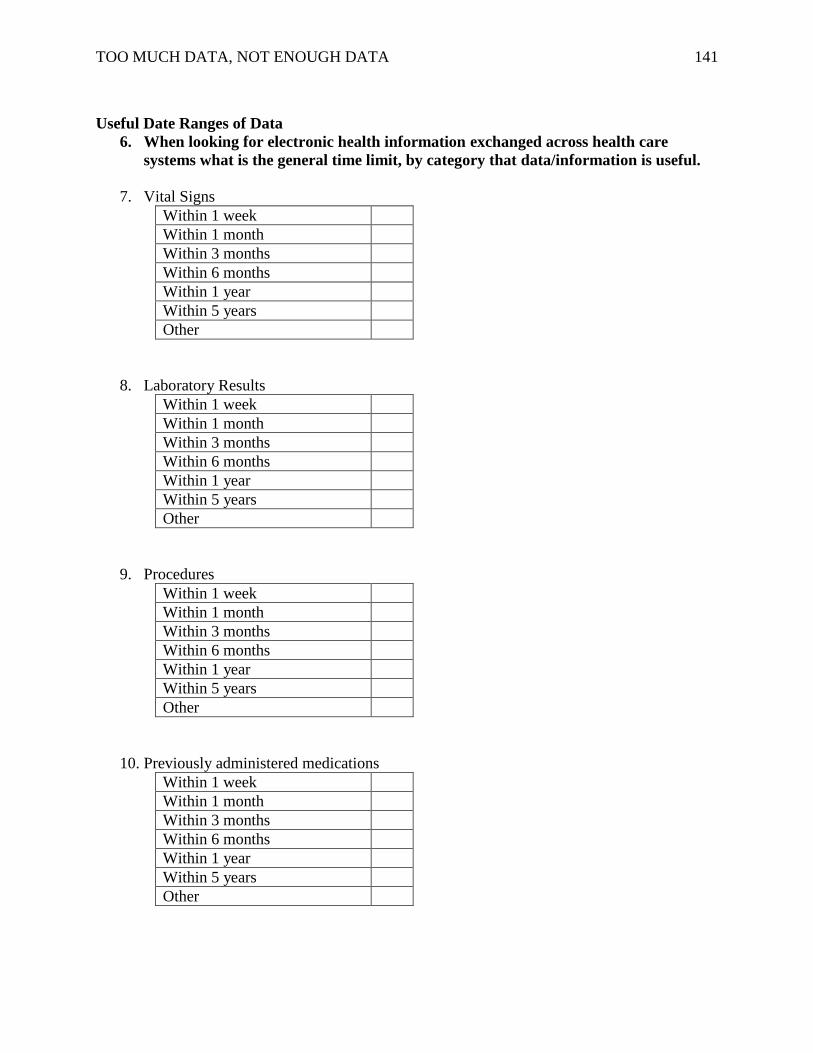
TOO MUCH DATA, NOT ENOUGH DATA 141
Useful Date Ranges of Data
6. When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
7. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
8. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
9. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
10. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
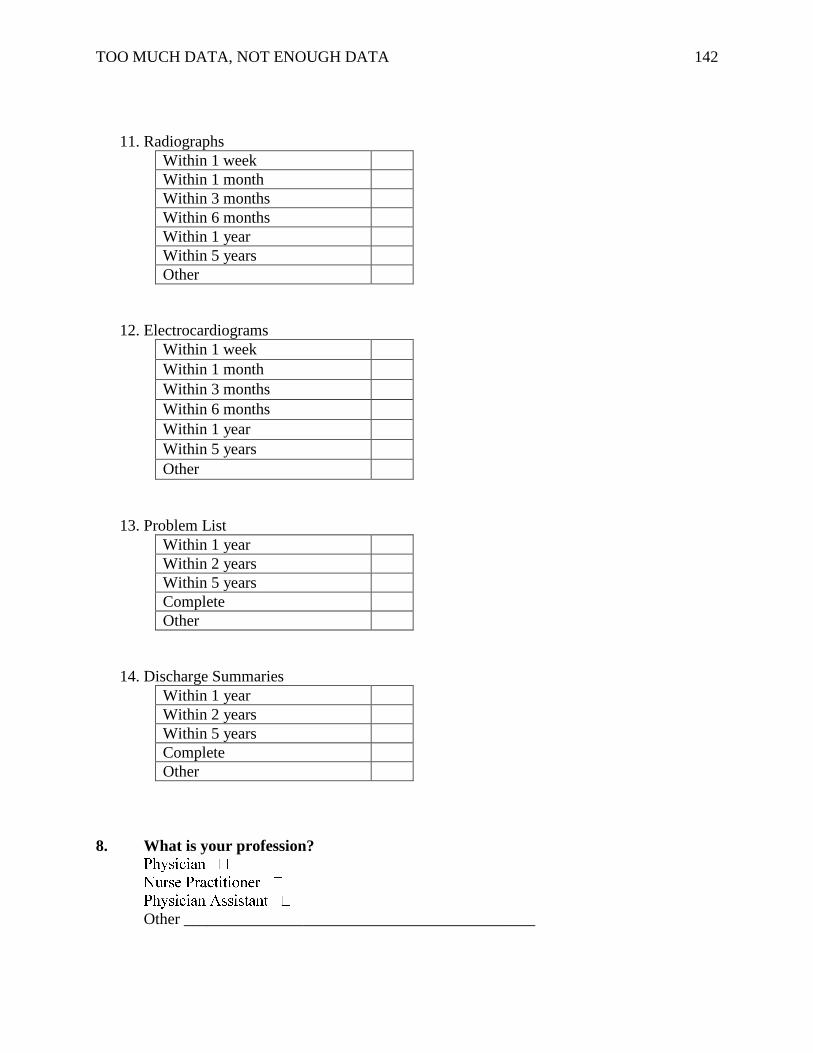
TOO MUCH DATA, NOT ENOUGH DATA 142
11. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
12. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
13. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
14. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your profession?
Other ____________________________________________

TOO MUCH DATA, NOT ENOUGH DATA 143
Appendix N
Electronic Data Relevance Survey – Primary Care Nursing
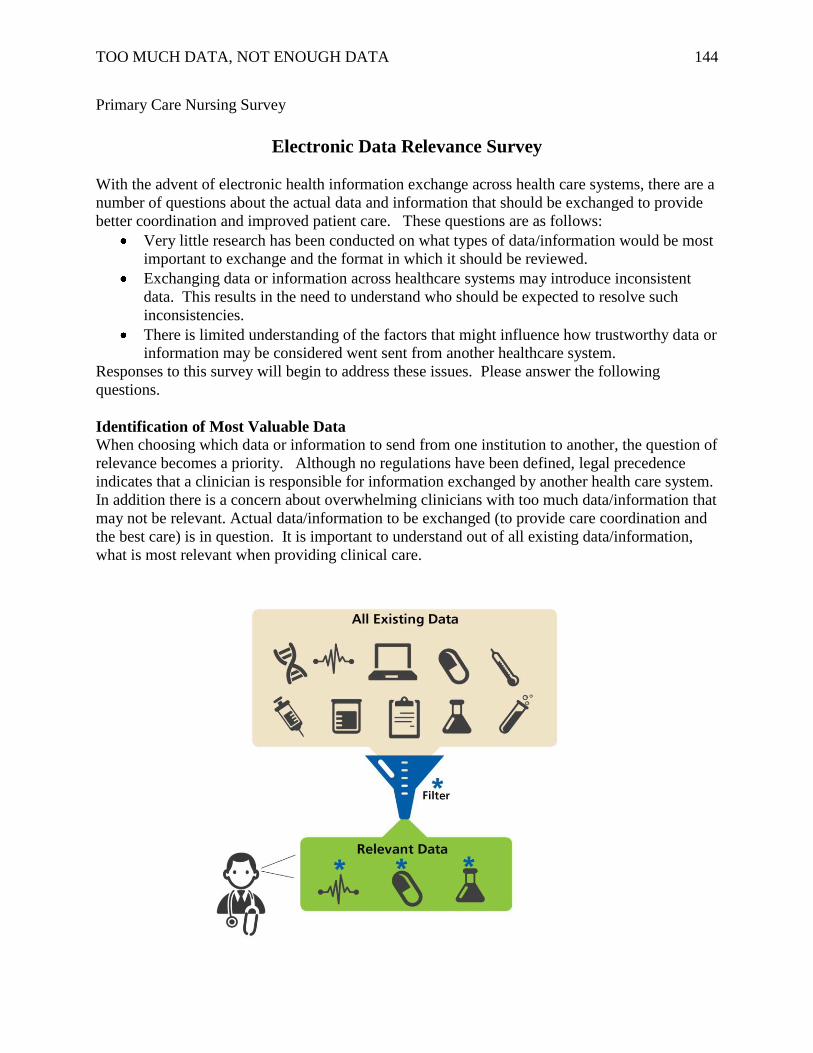
TOO MUCH DATA, NOT ENOUGH DATA 144
Primary Care Nursing Survey
Electronic Data Relevance Survey
With the advent of electronic health information exchange across health care systems, there are a
number of questions about the actual data and information that should be exchanged to provide
better coordination and improved patient care. These questions are as follows:
Very little research has been conducted on what types of data/information would be most
important to exchange and the format in which it should be reviewed.
Exchanging data or information across healthcare systems may introduce inconsistent
data. This results in the need to understand who should be expected to resolve such
inconsistencies.
There is limited understanding of the factors that might influence how trustworthy data or
information may be considered went sent from another healthcare system.
Responses to this survey will begin to address these issues. Please answer the following
questions.
Identification of Most Valuable Data When choosing which data or information to send from one institution to another, the question of
relevance becomes a priority. Although no regulations have been defined, legal precedence
indicates that a clinician is responsible for information exchanged by another health care system.
In addition there is a concern about overwhelming clinicians with too much data/information that
may not be relevant. Actual data/information to be exchanged (to provide care coordination and
the best care) is in question. It is important to understand out of all existing data/information,
what is most relevant when providing clinical care.
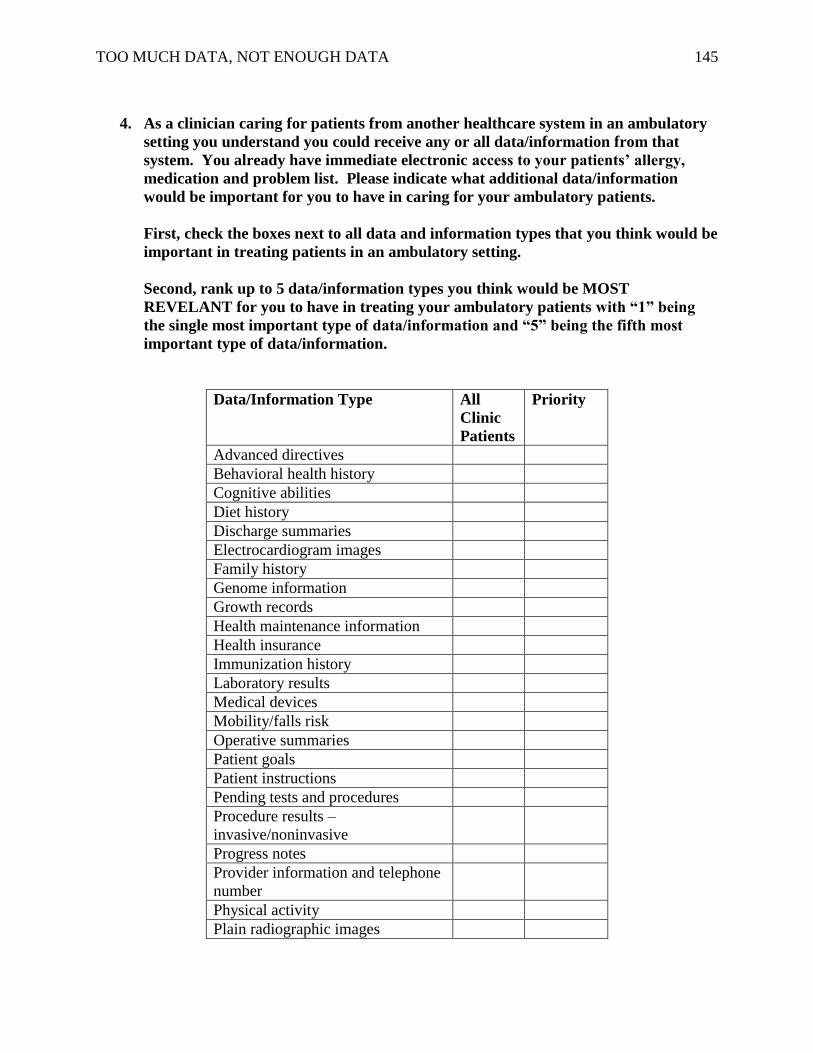
TOO MUCH DATA, NOT ENOUGH DATA 145
4. As a clinician caring for patients from another healthcare system in an ambulatory
setting you understand you could receive any or all data/information from that
system. You already have immediate electronic access to your patients’ allergy,
medication and problem list. Please indicate what additional data/information
would be important for you to have in caring for your ambulatory patients.
First, check the boxes next to all data and information types that you think would be
important in treating patients in an ambulatory setting.
Second, rank up to 5 data/information types you think would be MOST
REVELANT for you to have in treating your ambulatory patients with “1” being
the single most important type of data/information and “5” being the fifth most
important type of data/information.
Data/Information Type All
Clinic
Patients
Priority
Advanced directives
Behavioral health history
Cognitive abilities
Diet history
Discharge summaries
Electrocardiogram images
Family history
Genome information
Growth records
Health maintenance information
Health insurance
Immunization history
Laboratory results
Medical devices
Mobility/falls risk
Operative summaries
Patient goals
Patient instructions
Pending tests and procedures
Procedure results –
invasive/noninvasive
Progress notes
Provider information and telephone
number
Physical activity
Plain radiographic images
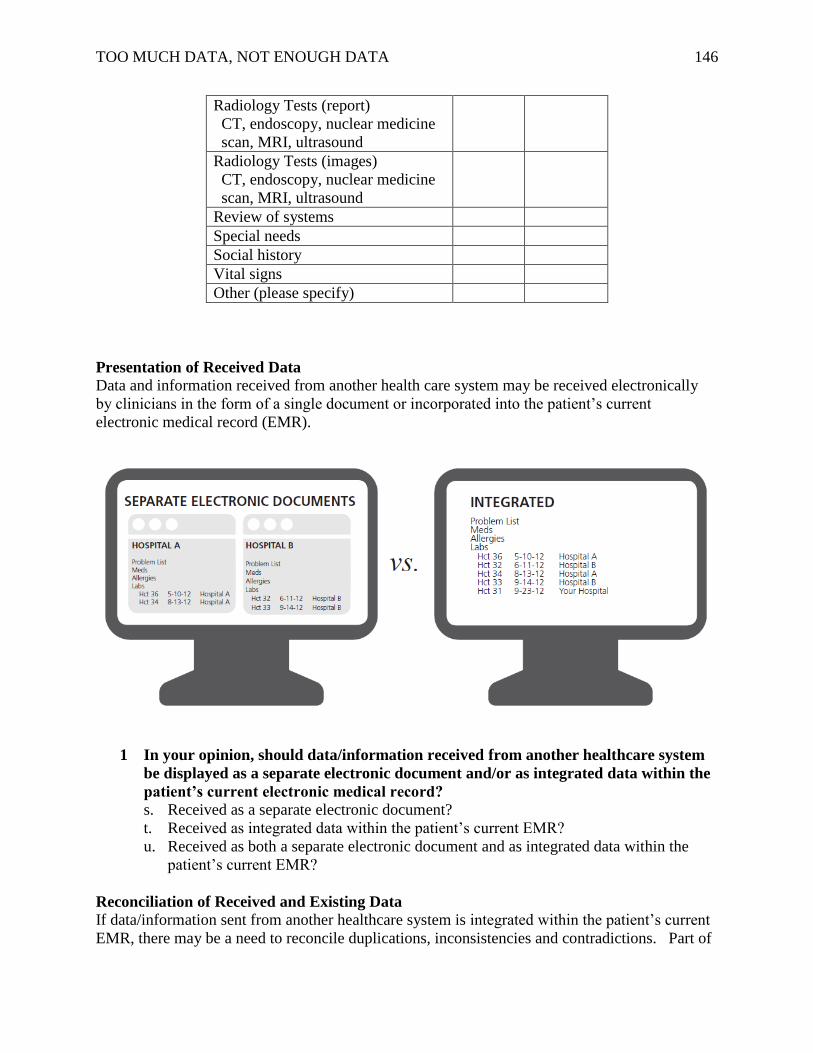
TOO MUCH DATA, NOT ENOUGH DATA 146
Radiology Tests (report)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Radiology Tests (images)
CT, endoscopy, nuclear medicine
scan, MRI, ultrasound
Review of systems
Special needs
Social history
Vital signs
Other (please specify)
Presentation of Received Data
Data and information received from another health care system may be received electronically
by clinicians in the form of a single document or incorporated into the patient’s current
electronic medical record (EMR).
1 In your opinion, should data/information received from another healthcare system
be displayed as a separate electronic document and/or as integrated data within the
patient’s current electronic medical record?
s. Received as a separate electronic document?
t. Received as integrated data within the patient’s current EMR?
u. Received as both a separate electronic document and as integrated data within the
patient’s current EMR?
Reconciliation of Received and Existing Data
If data/information sent from another healthcare system is integrated within the patient’s current
EMR, there may be a need to reconcile duplications, inconsistencies and contradictions. Part of
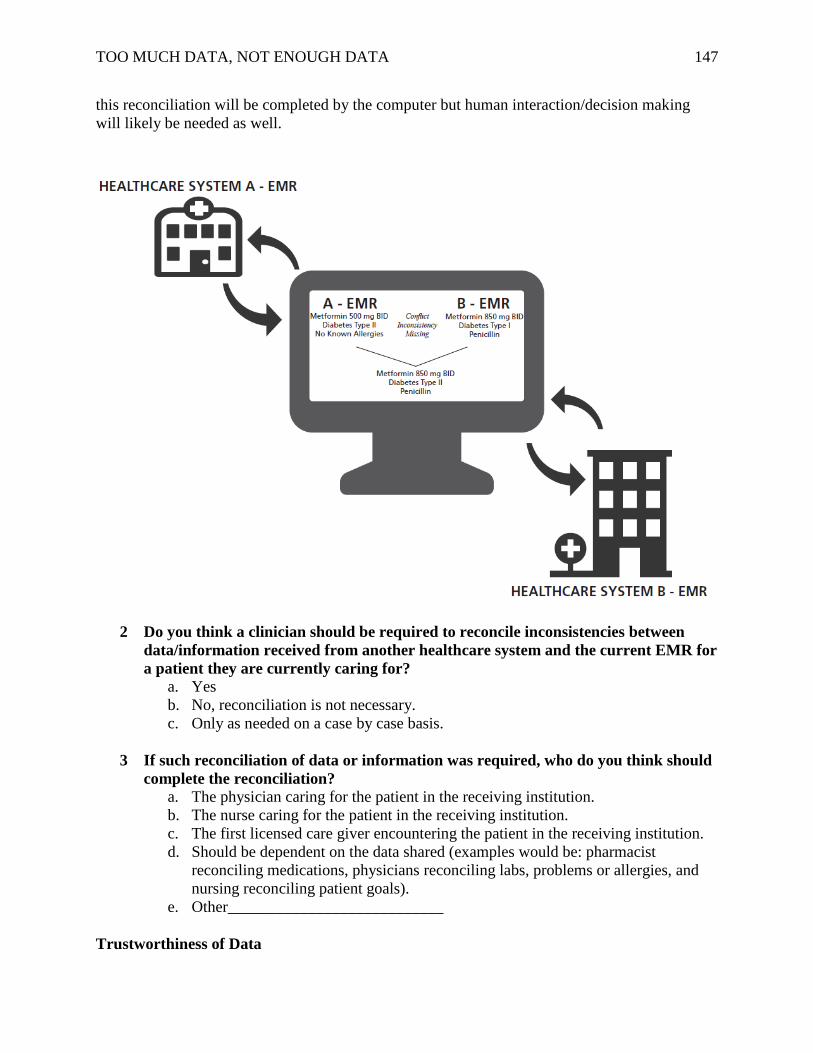
TOO MUCH DATA, NOT ENOUGH DATA 147
this reconciliation will be completed by the computer but human interaction/decision making
will likely be needed as well.
2 Do you think a clinician should be required to reconcile inconsistencies between
data/information received from another healthcare system and the current EMR for
a patient they are currently caring for?
a. Yes
b. No, reconciliation is not necessary.
c. Only as needed on a case by case basis.
3 If such reconciliation of data or information was required, who do you think should
complete the reconciliation?
a. The physician caring for the patient in the receiving institution.
b. The nurse caring for the patient in the receiving institution.
c. The first licensed care giver encountering the patient in the receiving institution.
d. Should be dependent on the data shared (examples would be: pharmacist
reconciling medications, physicians reconciling labs, problems or allergies, and
nursing reconciling patient goals).
e. Other___________________________
Trustworthiness of Data
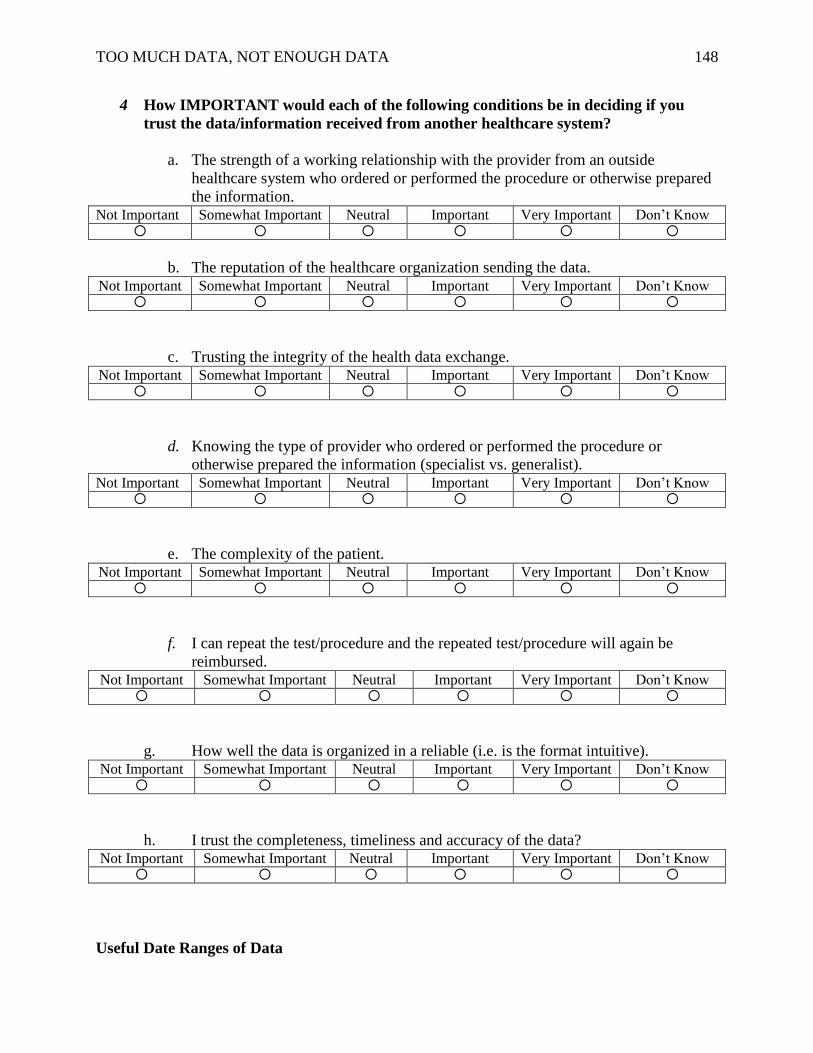
TOO MUCH DATA, NOT ENOUGH DATA 148
4 How IMPORTANT would each of the following conditions be in deciding if you
trust the data/information received from another healthcare system?
a. The strength of a working relationship with the provider from an outside
healthcare system who ordered or performed the procedure or otherwise prepared
the information. Not Important Somewhat Important Neutral Important Very Important Don’t Know
b. The reputation of the healthcare organization sending the data. Not Important Somewhat Important Neutral Important Very Important Don’t Know
c. Trusting the integrity of the health data exchange. Not Important Somewhat Important Neutral Important Very Important Don’t Know
d. Knowing the type of provider who ordered or performed the procedure or
otherwise prepared the information (specialist vs. generalist). Not Important Somewhat Important Neutral Important Very Important Don’t Know
e. The complexity of the patient. Not Important Somewhat Important Neutral Important Very Important Don’t Know
f. I can repeat the test/procedure and the repeated test/procedure will again be
reimbursed. Not Important Somewhat Important Neutral Important Very Important Don’t Know
g. How well the data is organized in a reliable (i.e. is the format intuitive). Not Important Somewhat Important Neutral Important Very Important Don’t Know
h. I trust the completeness, timeliness and accuracy of the data? Not Important Somewhat Important Neutral Important Very Important Don’t Know
Useful Date Ranges of Data
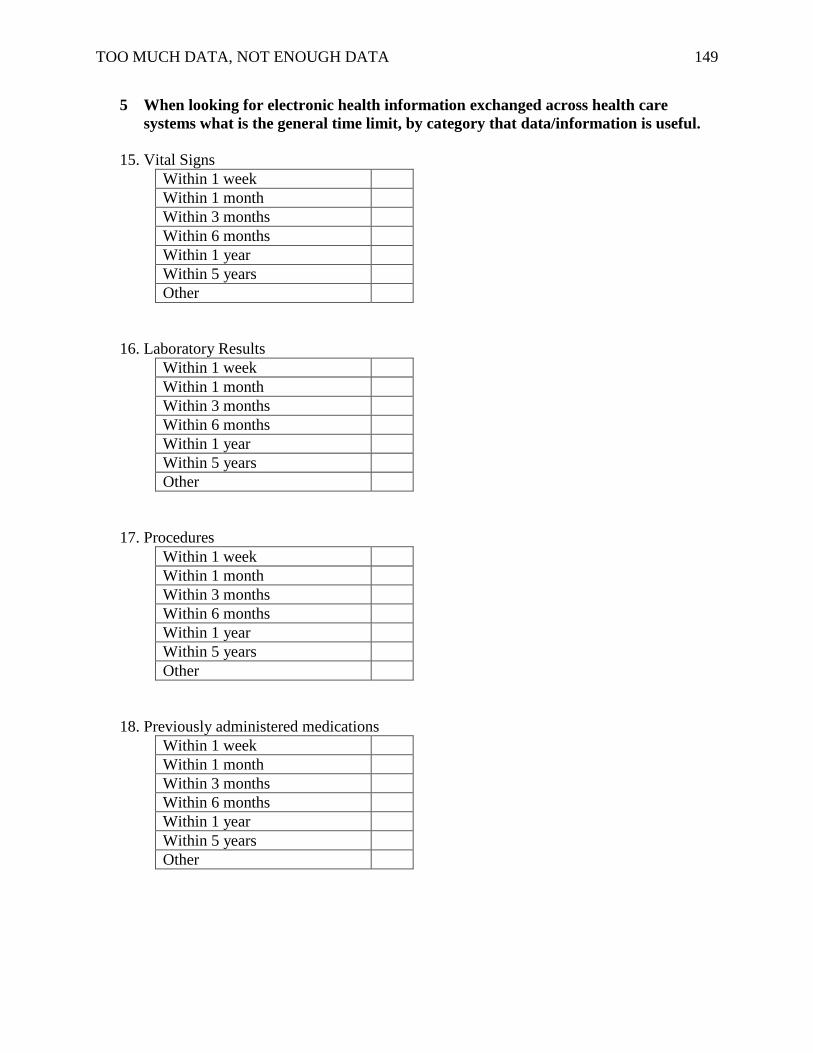
TOO MUCH DATA, NOT ENOUGH DATA 149
5 When looking for electronic health information exchanged across health care
systems what is the general time limit, by category that data/information is useful.
15. Vital Signs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
16. Laboratory Results
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
17. Procedures
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
18. Previously administered medications
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
TOO MUCH DATA, NOT ENOUGH DATA 150
19. Radiographs
Within 1 week
Within 1 month
Within 3 months
Within 6 months
Within 1 year
Within 5 years
Other
20. Electrocardiograms
Within 1 week Within 1 month Within 3 months Within 6 months Within 1 year Within 5 years Other
21. Problem List
Within 1 year
Within 2 years
Within 5 years
Complete
Other
22. Discharge Summaries
Within 1 year
Within 2 years
Within 5 years
Complete
Other
8. What is your level of education?
AD □
ADN□
BS□
BSN □
Masters Prepared □
Clinical Area of Expertise ____________________________________

TOO MUCH DATA, NOT ENOUGH DATA 151
Appendix O
Relevant Data by Specialty
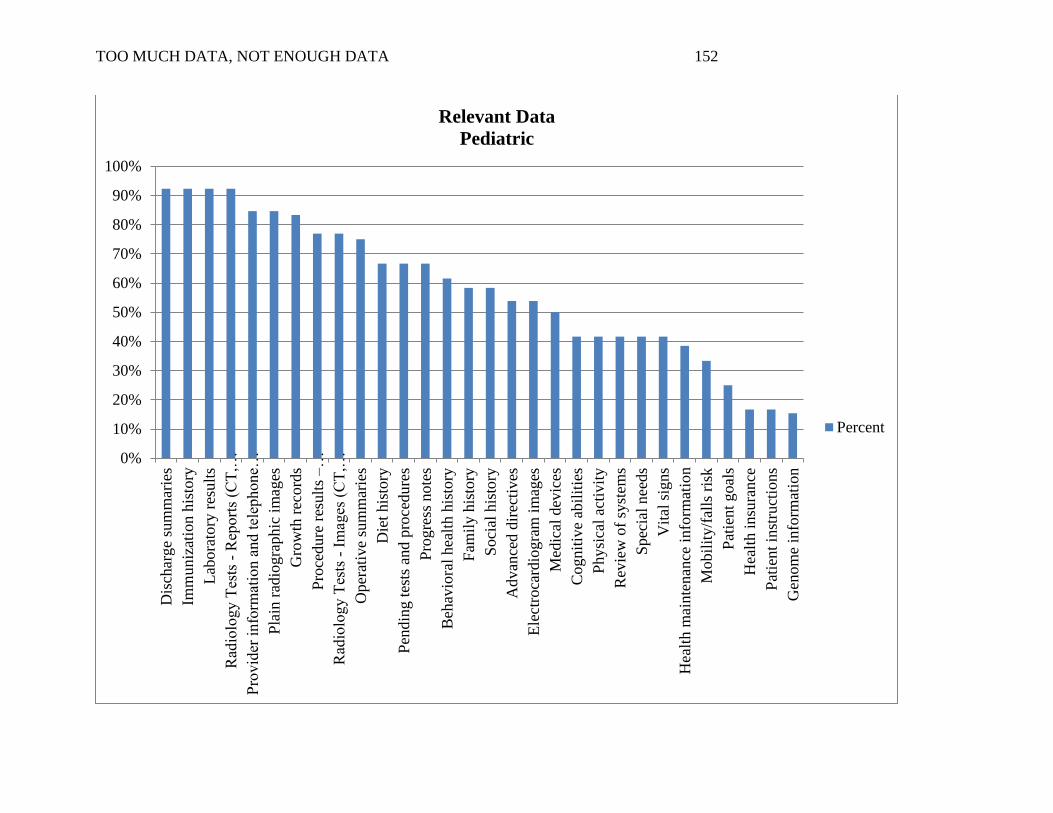
TOO MUCH DATA, NOT ENOUGH DATA 152
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%D
isch
arge
sum
mar
ies
Imm
un
izat
ion
his
tory
Lab
ora
tory
res
ult
s
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Pro
vid
er i
nfo
rmat
ion a
nd t
elep
hone…
Pla
in r
adio
gra
phic
im
ages
Gro
wth
rec
ord
s
Pro
cedure
res
ult
s –
…
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Oper
ativ
e su
mm
arie
s
Die
t his
tory
Pen
din
g t
ests
and p
roce
dure
s
Pro
gre
ss n
ote
s
Beh
avio
ral
hea
lth h
isto
ry
Fam
ily h
isto
ry
Soci
al h
isto
ry
Advan
ced d
irec
tives
Ele
ctro
card
iogra
m i
mag
es
Med
ical
dev
ices
Cognit
ive
abil
itie
s
Physi
cal
acti
vit
y
Rev
iew
of
syst
ems
Spec
ial
nee
ds
Vit
al s
igns
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Mobil
ity/f
alls
ris
k
Pat
ient
goal
s
Hea
lth i
nsu
rance
Pat
ient
inst
ruct
ions
Gen
om
e in
form
atio
n
Relevant Data
Pediatric
Percent
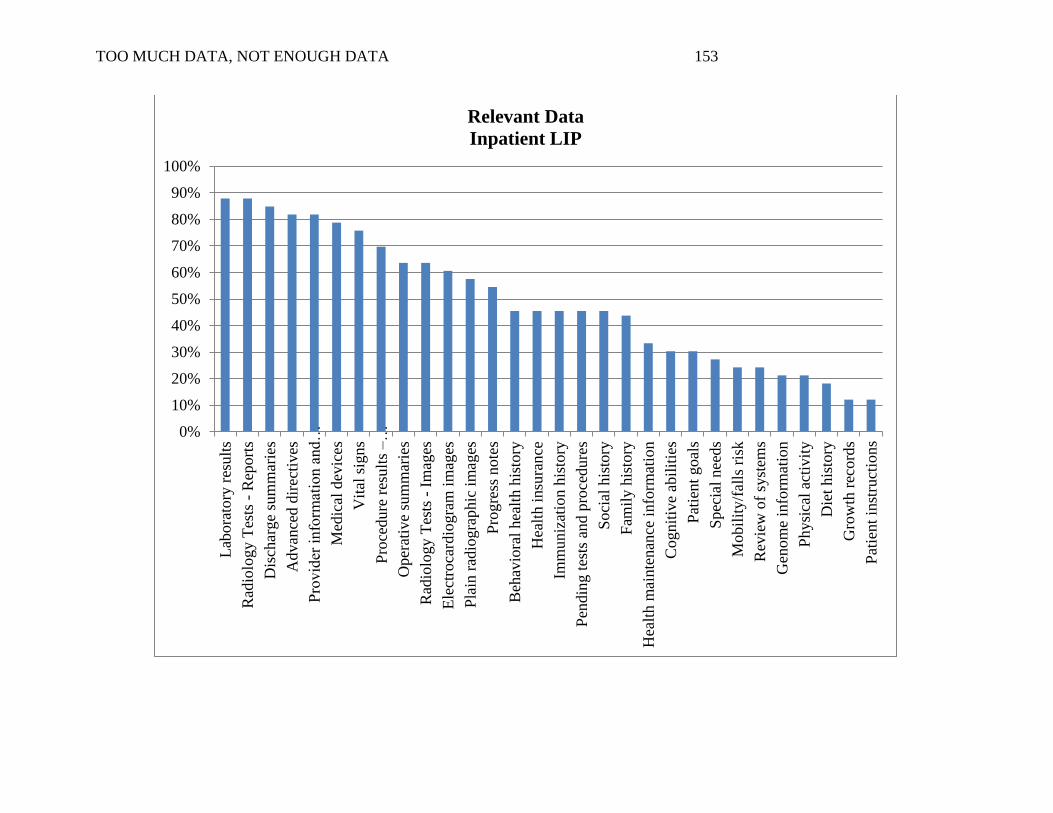
TOO MUCH DATA, NOT ENOUGH DATA 153
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Lab
ora
tory
res
ult
s
Rad
iolo
gy T
ests
- R
eport
s
Dis
char
ge
sum
mar
ies
Advan
ced d
irec
tives
Pro
vid
er i
nfo
rmat
ion
and…
Med
ical
dev
ices
Vit
al s
igns
Pro
cedure
res
ult
s – …
Oper
ativ
e su
mm
arie
s
Rad
iolo
gy T
ests
- I
mag
es
Ele
ctro
card
iogra
m i
mag
es
Pla
in r
adio
gra
phic
im
ages
Pro
gre
ss n
ote
s
Beh
avio
ral
hea
lth h
isto
ry
Hea
lth i
nsu
rance
Imm
uniz
atio
n h
isto
ry
Pen
din
g t
ests
and p
roce
dure
s
Soci
al h
isto
ry
Fam
ily h
isto
ry
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Cognit
ive
abil
itie
s
Pat
ient
goal
s
Spec
ial
nee
ds
Mobil
ity/f
alls
ris
k
Rev
iew
of
syst
ems
Gen
om
e in
form
atio
n
Physi
cal
acti
vit
y
Die
t his
tory
Gro
wth
rec
ord
s
Pat
ient
inst
ruct
ion
s
Relevant Data
Inpatient LIP
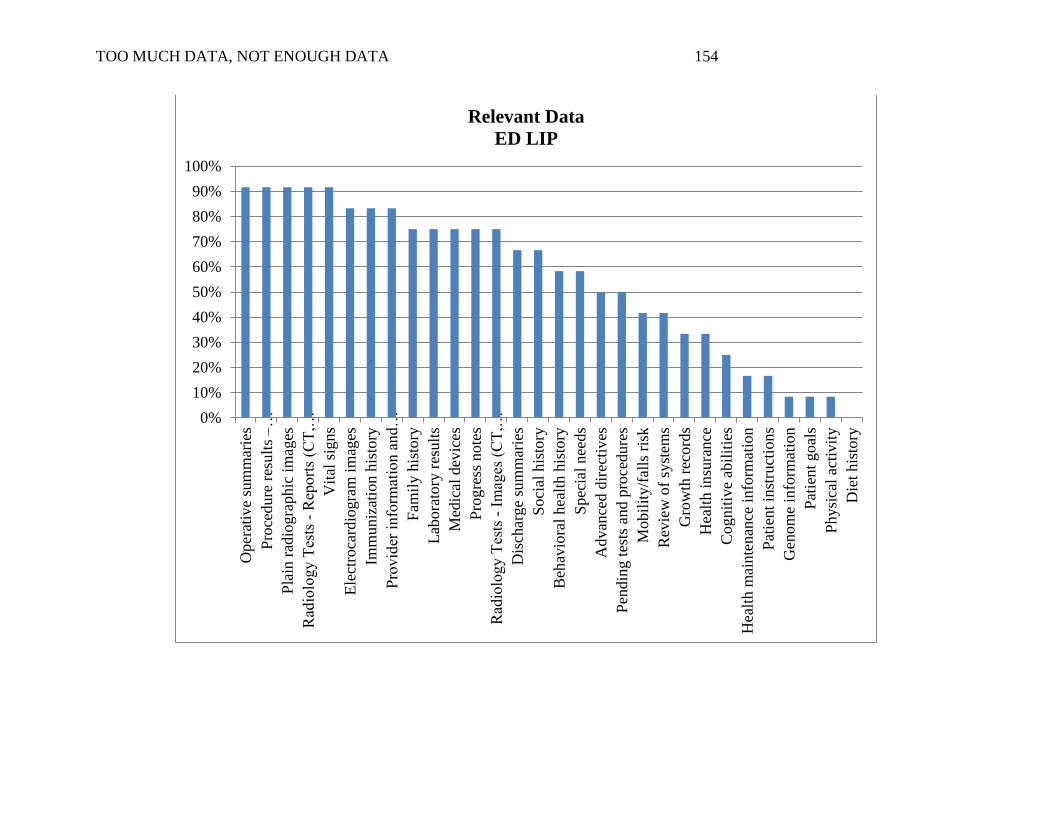
TOO MUCH DATA, NOT ENOUGH DATA 154
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oper
ativ
e su
mm
arie
s
Pro
cedure
res
ult
s –
…
Pla
in r
adio
gra
phic
im
ages
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Vit
al s
igns
Ele
ctro
card
iogra
m i
mag
es
Imm
uniz
atio
n h
isto
ry
Pro
vid
er i
nfo
rmat
ion a
nd…
Fam
ily h
isto
ry
Lab
ora
tory
res
ult
s
Med
ical
dev
ices
Pro
gre
ss n
ote
s
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Dis
char
ge
sum
mar
ies
Soci
al h
isto
ry
Beh
avio
ral
hea
lth h
isto
ry
Spec
ial
nee
ds
Advan
ced d
irec
tives
Pen
din
g t
ests
and p
roce
dure
s
Mobil
ity/f
alls
ris
k
Rev
iew
of
syst
ems
Gro
wth
rec
ord
s
Hea
lth i
nsu
rance
Cognit
ive
abil
itie
s
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Pat
ient
inst
ruct
ions
Gen
om
e in
form
atio
n
Pat
ien
t goal
s
Physi
cal
acti
vit
y
Die
t his
tory
Relevant Data
ED LIP
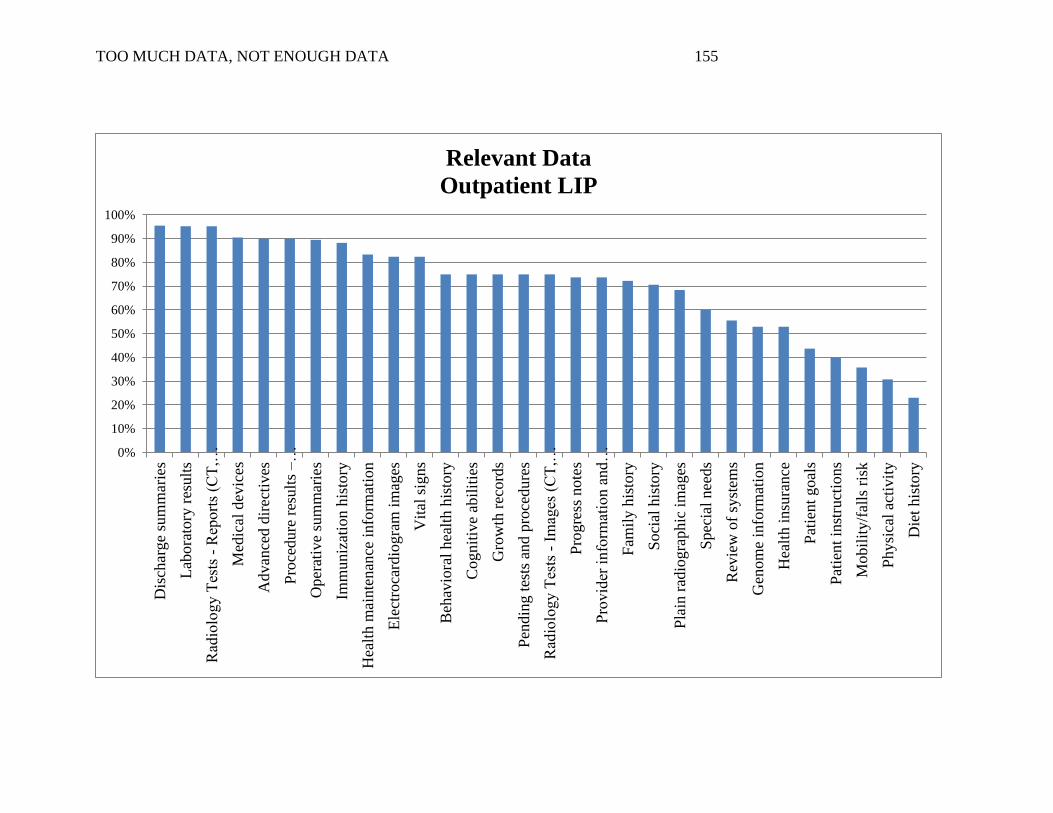
TOO MUCH DATA, NOT ENOUGH DATA 155
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Dis
char
ge
sum
mar
ies
Lab
ora
tory
res
ult
s
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Med
ical
dev
ices
Advan
ced d
irec
tives
Pro
cedure
res
ult
s – …
Oper
ativ
e su
mm
arie
s
Imm
uniz
atio
n h
isto
ry
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Ele
ctro
card
iogra
m i
mag
es
Vit
al s
igns
Beh
avio
ral
hea
lth h
isto
ry
Cognit
ive
abil
itie
s
Gro
wth
rec
ord
s
Pen
din
g t
ests
and p
roce
dure
s
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Pro
gre
ss n
ote
s
Pro
vid
er i
nfo
rmat
ion a
nd…
Fam
ily h
isto
ry
Soci
al h
isto
ry
Pla
in r
adio
gra
phic
im
ages
Spec
ial
nee
ds
Rev
iew
of
syst
ems
Gen
om
e in
form
atio
n
Hea
lth i
nsu
rance
Pat
ient
goal
s
Pat
ient
inst
ruct
ion
s
Mobil
ity/f
alls
ris
k
Physi
cal
acti
vit
y
Die
t his
tory
Relevant Data
Outpatient LIP
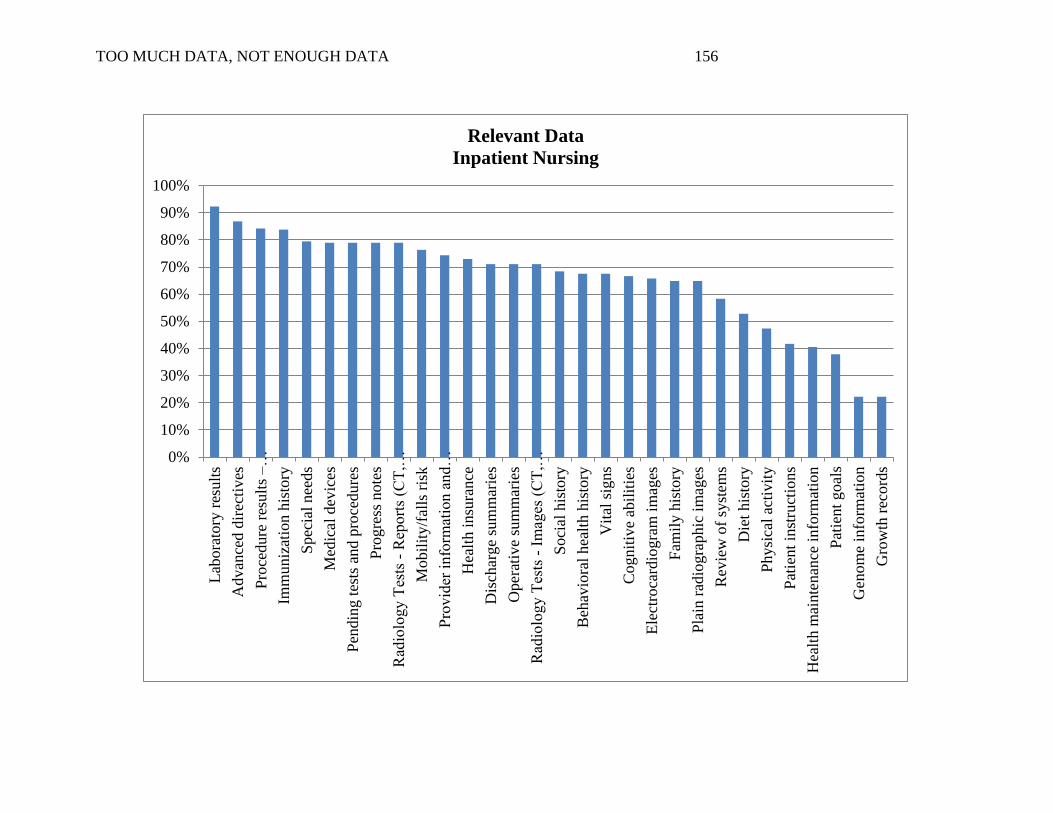
TOO MUCH DATA, NOT ENOUGH DATA 156
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Lab
ora
tory
res
ult
s
Advan
ced d
irec
tives
Pro
cedure
res
ult
s – …
Imm
uniz
atio
n h
isto
ry
Spec
ial
nee
ds
Med
ical
dev
ices
Pen
din
g t
ests
and p
roce
dure
s
Pro
gre
ss n
ote
s
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Mobil
ity/f
alls
ris
k
Pro
vid
er i
nfo
rmat
ion a
nd…
Hea
lth i
nsu
rance
Dis
char
ge
sum
mar
ies
Oper
ativ
e su
mm
arie
s
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Soci
al h
isto
ry
Beh
avio
ral
hea
lth h
isto
ry
Vit
al s
igns
Cognit
ive
abil
itie
s
Ele
ctro
card
iogra
m i
mag
es
Fam
ily h
isto
ry
Pla
in r
adio
gra
phic
im
ages
Rev
iew
of
syst
ems
Die
t his
tory
Physi
cal
acti
vit
y
Pat
ient
inst
ruct
ions
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Pat
ient
goal
s
Gen
om
e in
form
atio
n
Gro
wth
rec
ord
s
Relevant Data
Inpatient Nursing
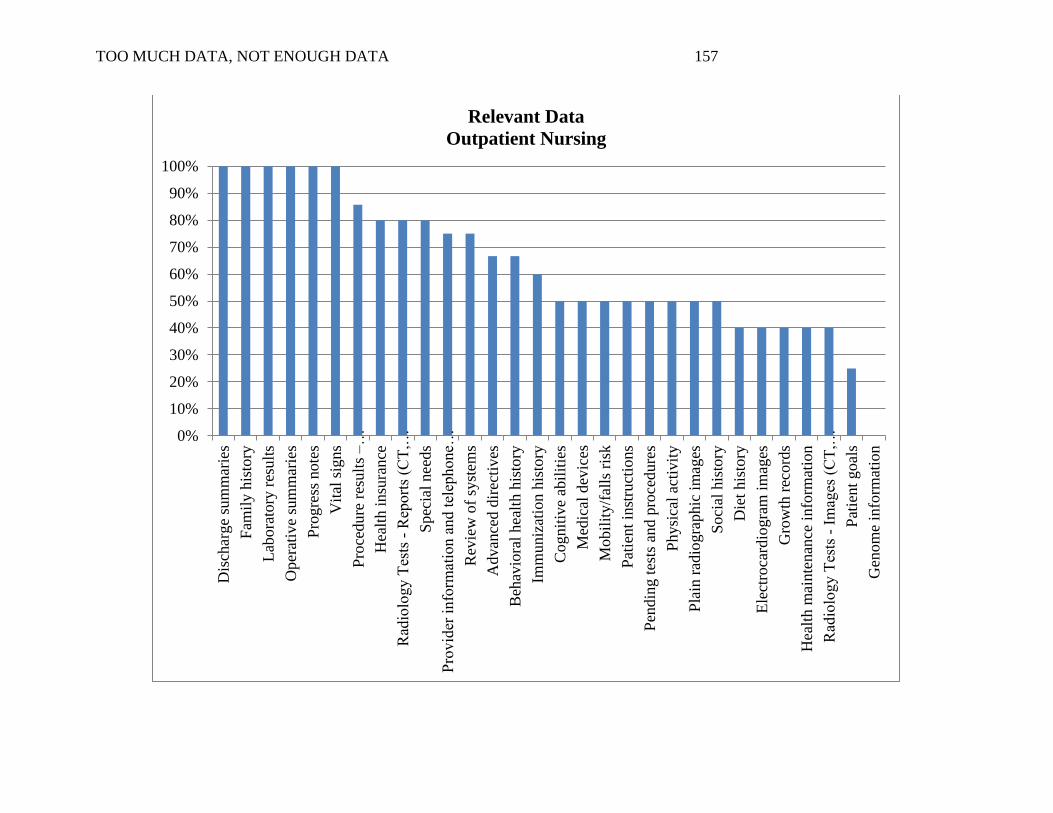
TOO MUCH DATA, NOT ENOUGH DATA 157
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Dis
char
ge
sum
mar
ies
Fam
ily h
isto
ry
Lab
ora
tory
res
ult
s
Oper
ativ
e su
mm
arie
s
Pro
gre
ss n
ote
s
Vit
al s
igns
Pro
cedure
res
ult
s – …
Hea
lth i
nsu
rance
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Spec
ial
nee
ds
Pro
vid
er i
nfo
rmat
ion a
nd t
elep
hone…
Rev
iew
of
syst
ems
Advan
ced d
irec
tives
Beh
avio
ral
hea
lth h
isto
ry
Imm
uniz
atio
n h
isto
ry
Cognit
ive
abil
itie
s
Med
ical
dev
ices
Mob
ilit
y/f
alls
ris
k
Pat
ient
inst
ruct
ions
Pen
din
g t
ests
and p
roce
dure
s
Physi
cal
acti
vit
y
Pla
in r
adio
gra
phic
im
ages
Soci
al h
isto
ry
Die
t his
tory
Ele
ctro
card
iogra
m i
mag
es
Gro
wth
rec
ord
s
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Pat
ient
goal
s
Gen
om
e in
form
atio
n
Relevant Data
Outpatient Nursing

TOO MUCH DATA, NOT ENOUGH DATA 158
Appendix P
Relevant Emergent Data
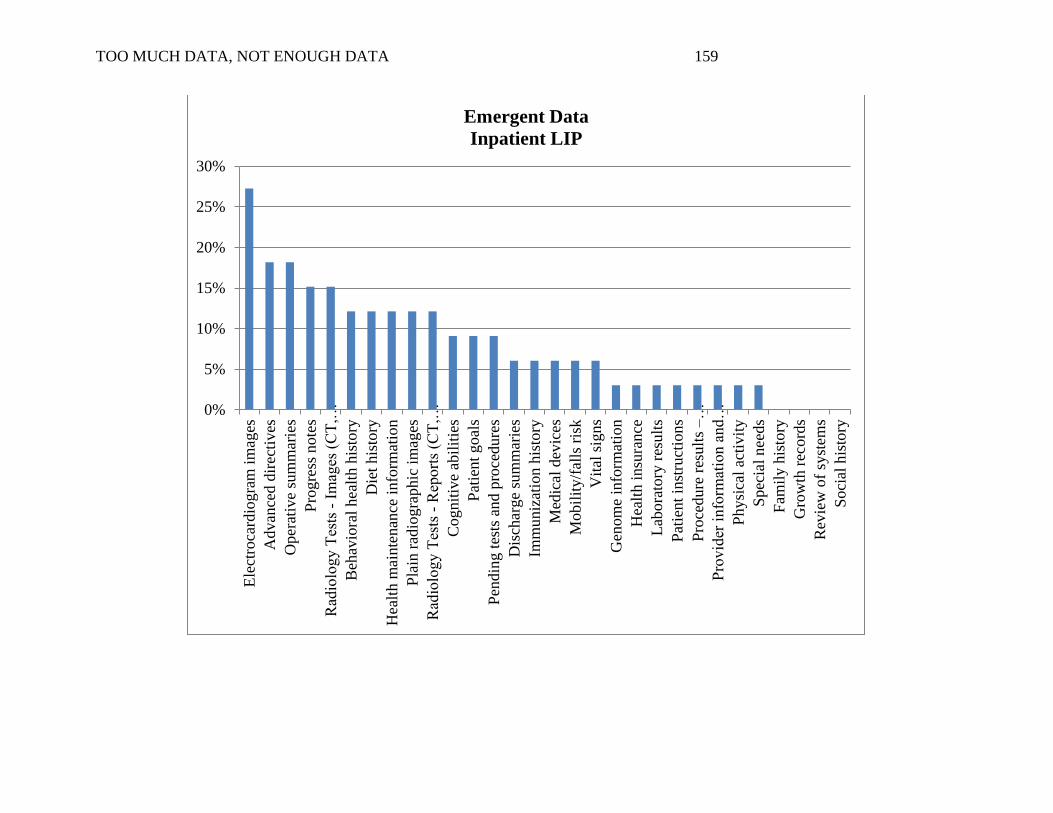
TOO MUCH DATA, NOT ENOUGH DATA 159
0%
5%
10%
15%
20%
25%
30%
Ele
ctro
card
iogra
m i
mag
es
Advan
ced d
irec
tives
Oper
ativ
e su
mm
arie
s
Pro
gre
ss n
ote
s
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Beh
avio
ral
hea
lth h
isto
ry
Die
t his
tory
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Pla
in r
adio
gra
phic
im
ages
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Cognit
ive
abil
itie
s
Pat
ient
goal
s
Pen
din
g t
ests
and p
roce
dure
s
Dis
char
ge
sum
mar
ies
Imm
uniz
atio
n h
isto
ry
Med
ical
dev
ices
Mobil
ity/f
alls
ris
k
Vit
al s
igns
Gen
om
e in
form
atio
n
Hea
lth i
nsu
rance
Lab
ora
tory
res
ult
s
Pat
ient
inst
ruct
ions
Pro
cedure
res
ult
s – …
Pro
vid
er i
nfo
rmat
ion a
nd…
Physi
cal
acti
vit
y
Spec
ial
nee
ds
Fam
ily h
isto
ry
Gro
wth
rec
ord
s
Rev
iew
of
syst
ems
Soci
al h
isto
ry
Emergent Data
Inpatient LIP
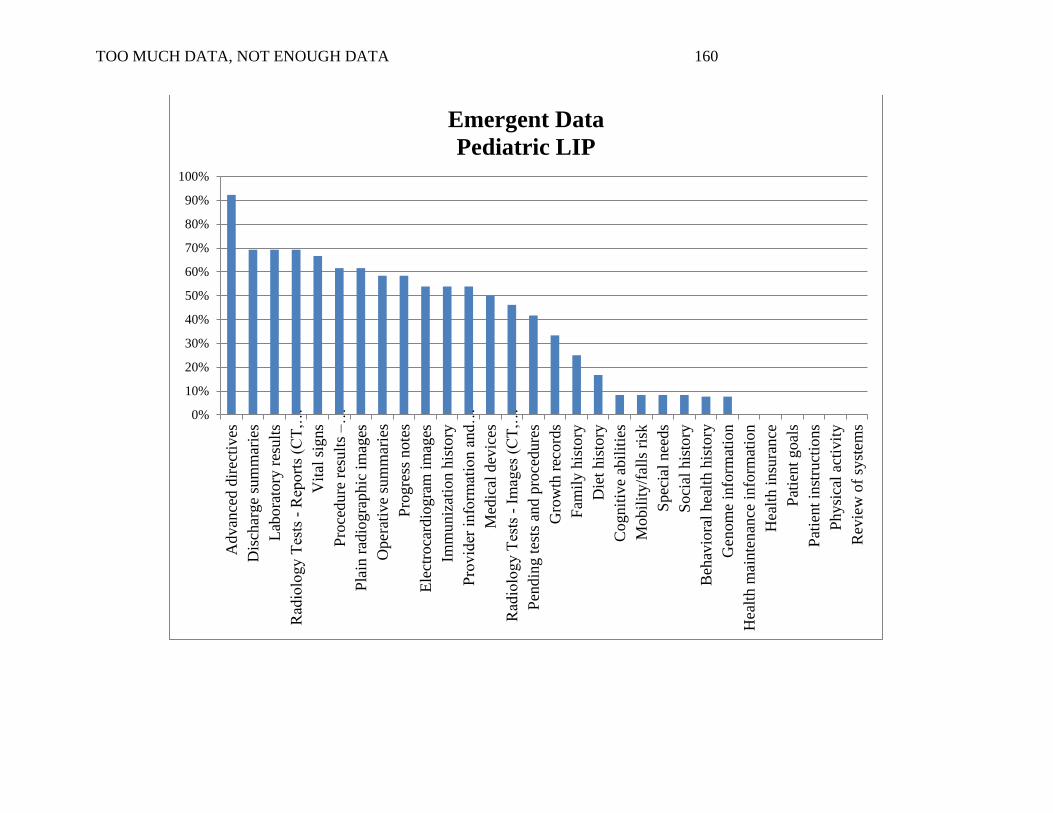
TOO MUCH DATA, NOT ENOUGH DATA 160
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Advan
ced d
irec
tives
Dis
char
ge
sum
mar
ies
Lab
ora
tory
res
ult
s
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Vit
al s
igns
Pro
cedure
res
ult
s – …
Pla
in r
adio
gra
phic
im
ages
Oper
ativ
e su
mm
arie
s
Pro
gre
ss n
ote
s
Ele
ctro
card
iogra
m i
mag
es
Imm
uniz
atio
n h
isto
ry
Pro
vid
er i
nfo
rmat
ion a
nd…
Med
ical
dev
ices
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Pen
din
g t
ests
and p
roce
dure
s
Gro
wth
rec
ord
s
Fam
ily h
isto
ry
Die
t his
tory
Cognit
ive
abil
itie
s
Mobil
ity/f
alls
ris
k
Spec
ial
nee
ds
Soci
al h
isto
ry
Beh
avio
ral
hea
lth
his
tory
Gen
om
e in
form
atio
n
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Hea
lth i
nsu
rance
Pat
ient
goal
s
Pat
ient
inst
ruct
ions
Physi
cal
acti
vit
y
Rev
iew
of
syst
ems
Emergent Data
Pediatric LIP
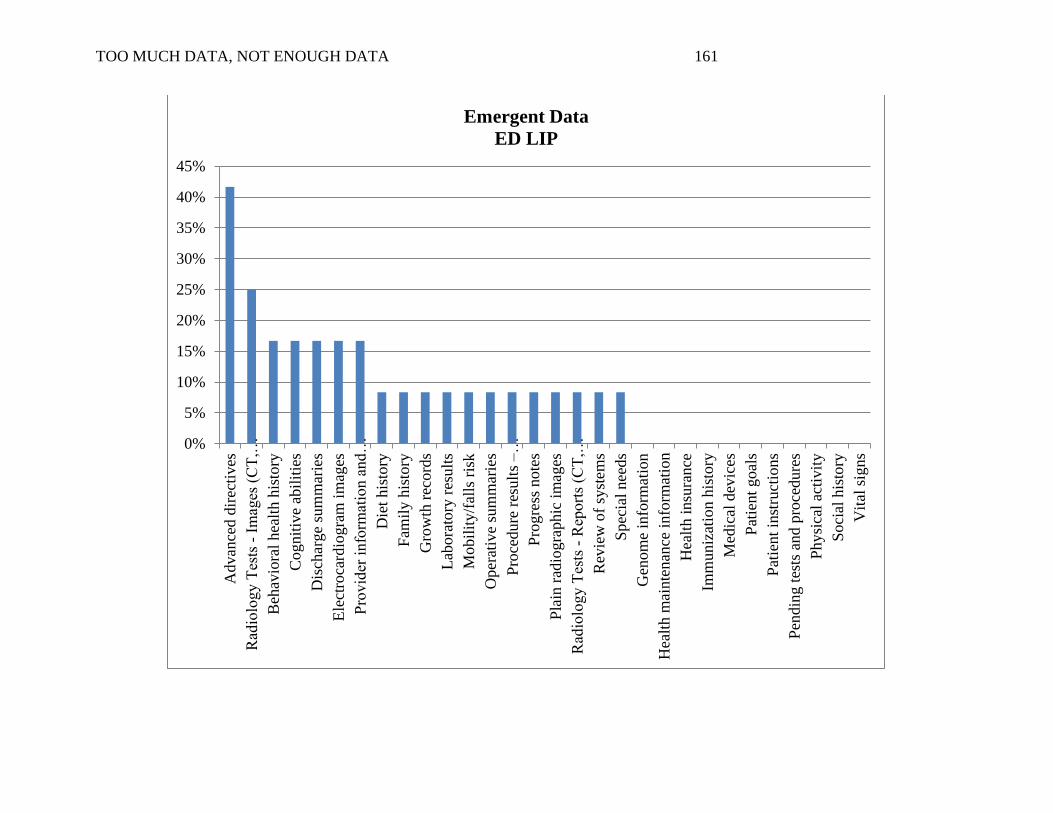
TOO MUCH DATA, NOT ENOUGH DATA 161
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Advan
ced d
irec
tives
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Beh
avio
ral
hea
lth h
isto
ry
Cognit
ive
abil
itie
s
Dis
char
ge
sum
mar
ies
Ele
ctro
card
iogra
m i
mag
es
Pro
vid
er i
nfo
rmat
ion a
nd…
Die
t his
tory
Fam
ily h
isto
ry
Gro
wth
rec
ord
s
Lab
ora
tory
res
ult
s
Mobil
ity/f
alls
ris
k
Oper
ativ
e su
mm
arie
s
Pro
cedure
res
ult
s – …
Pro
gre
ss n
ote
s
Pla
in r
adio
gra
phic
im
ages
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Rev
iew
of
syst
ems
Spec
ial
nee
ds
Gen
om
e in
form
atio
n
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Hea
lth i
nsu
rance
Imm
un
izat
ion
his
tory
Med
ical
dev
ices
Pat
ient
go
als
Pat
ient
inst
ruct
ions
Pen
din
g t
ests
and p
roce
dure
s
Physi
cal
acti
vit
y
Soci
al h
isto
ry
Vit
al s
igns
Emergent Data
ED LIP
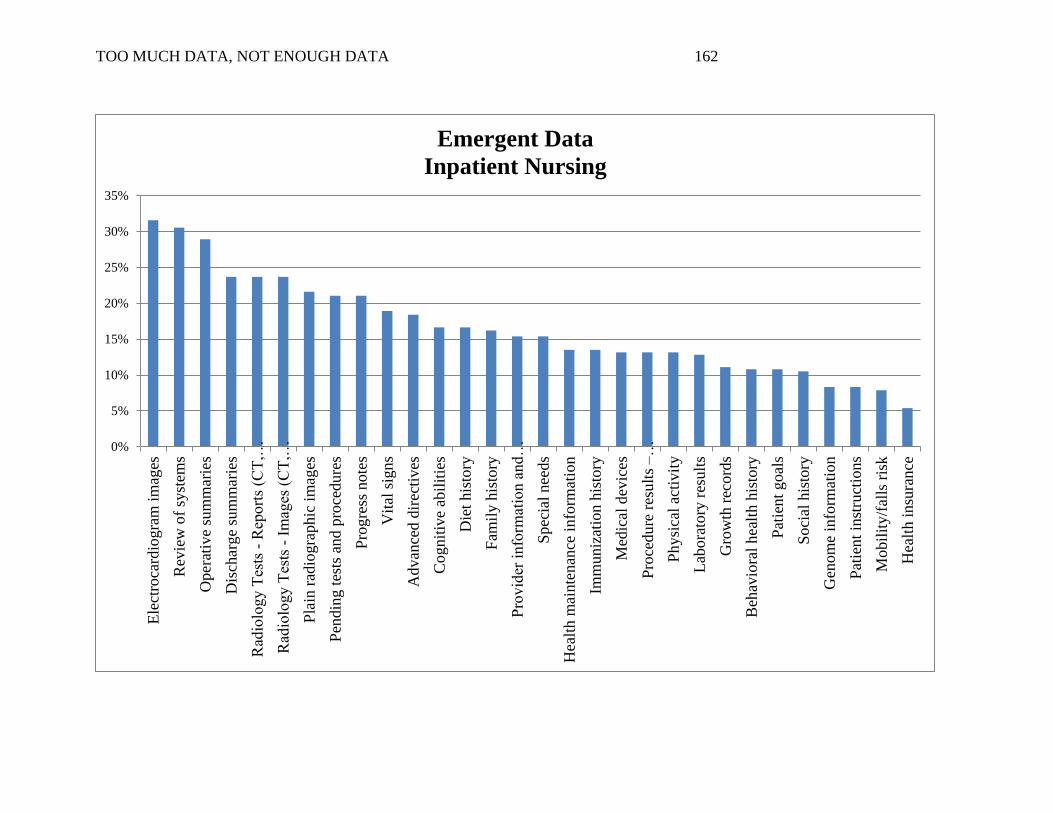
TOO MUCH DATA, NOT ENOUGH DATA 162
0%
5%
10%
15%
20%
25%
30%
35%
Ele
ctro
card
iogra
m i
mag
es
Rev
iew
of
syst
ems
Oper
ativ
e su
mm
arie
s
Dis
char
ge
sum
mar
ies
Rad
iolo
gy T
ests
- R
eport
s (C
T,…
Rad
iolo
gy T
ests
- I
mag
es (
CT
,…
Pla
in r
adio
gra
phic
im
ages
Pen
din
g t
ests
and p
roce
dure
s
Pro
gre
ss n
ote
s
Vit
al s
igns
Advan
ced d
irec
tives
Cognit
ive
abil
itie
s
Die
t his
tory
Fam
ily h
isto
ry
Pro
vid
er i
nfo
rmat
ion a
nd…
Spec
ial
nee
ds
Hea
lth m
ainte
nan
ce i
nfo
rmat
ion
Imm
uniz
atio
n h
isto
ry
Med
ical
dev
ices
Pro
cedure
res
ult
s –
…
Phy
sica
l ac
tivit
y
Lab
ora
tory
res
ult
s
Gro
wth
rec
ord
s
Beh
avio
ral
hea
lth h
isto
ry
Pat
ient
goal
s
Soci
al h
isto
ry
Gen
om
e in
form
atio
n
Pat
ient
inst
ruct
ions
Mobil
ity/f
alls
ris
k
Hea
lth i
nsu
ran
ce
Emergent Data
Inpatient Nursing

TOO MUCH DATA, NOT ENOUGH DATA 163
Appendix Q
Presentation of Exchanged Data – Separate or Integrated
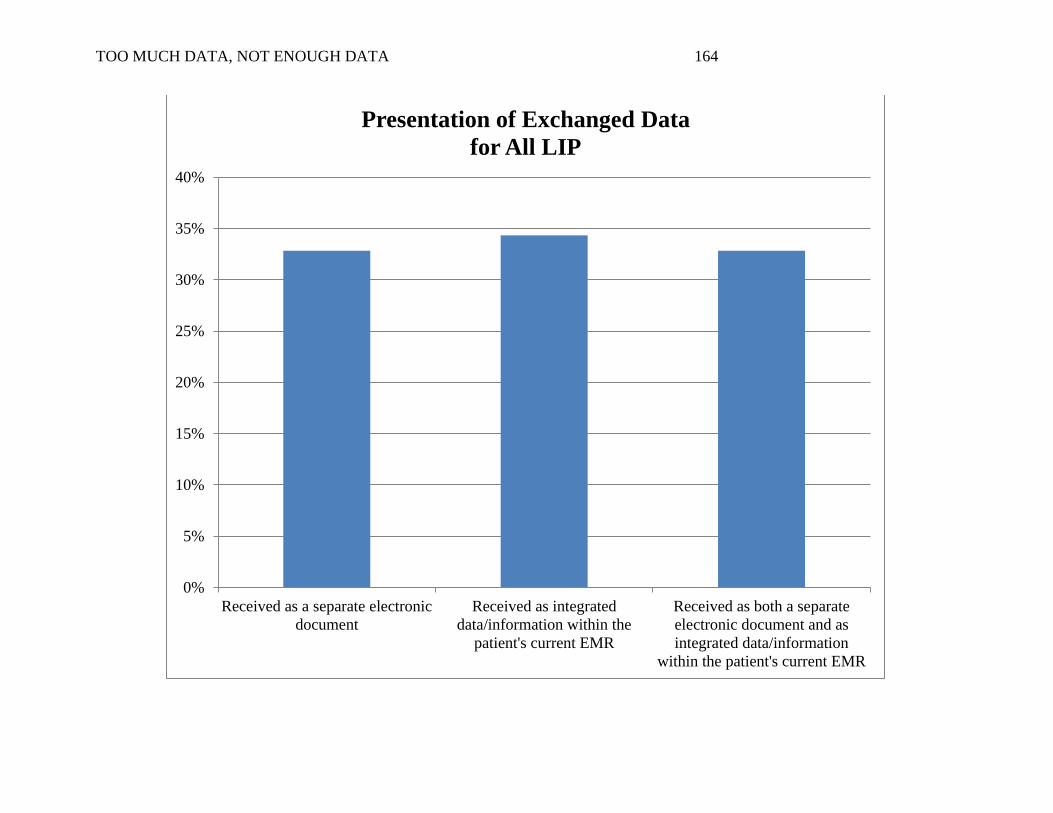
TOO MUCH DATA, NOT ENOUGH DATA 164
0%
5%
10%
15%
20%
25%
30%
35%
40%
Received as a separate electronic
document
Received as integrated
data/information within the
patient's current EMR
Received as both a separate
electronic document and as
integrated data/information
within the patient's current EMR
Presentation of Exchanged Data
for All LIP
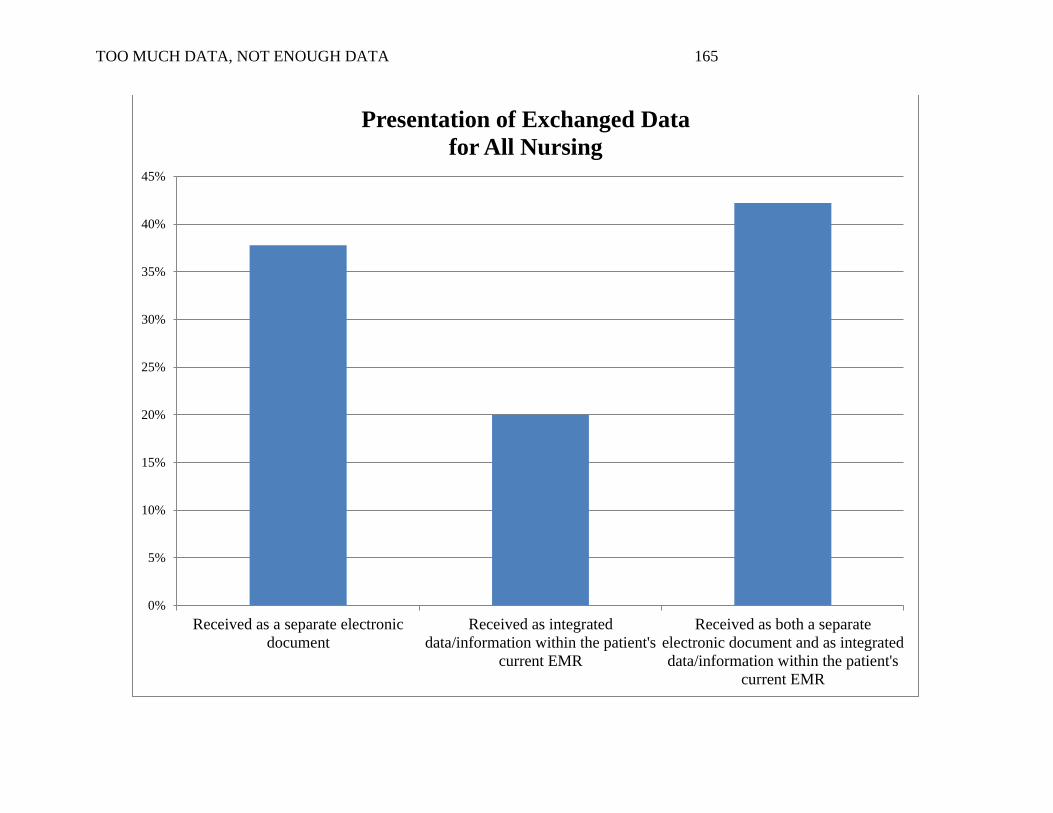
TOO MUCH DATA, NOT ENOUGH DATA 165
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Received as a separate electronic
document
Received as integrated
data/information within the patient's
current EMR
Received as both a separate
electronic document and as integrated
data/information within the patient's
current EMR
Presentation of Exchanged Data
for All Nursing

TOO MUCH DATA, NOT ENOUGH DATA 166
Appendix R
Reconciliation of Exchanged Data
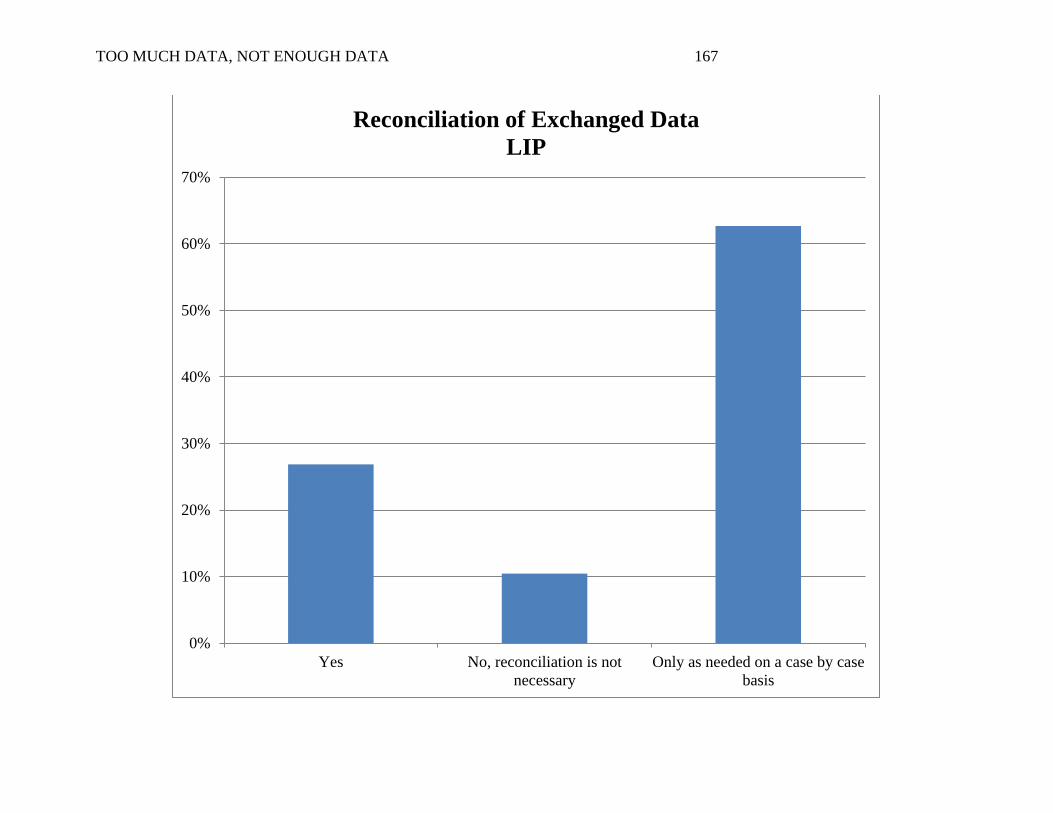
TOO MUCH DATA, NOT ENOUGH DATA 167
0%
10%
20%
30%
40%
50%
60%
70%
Yes No, reconciliation is not
necessary
Only as needed on a case by case
basis
Reconciliation of Exchanged Data
LIP
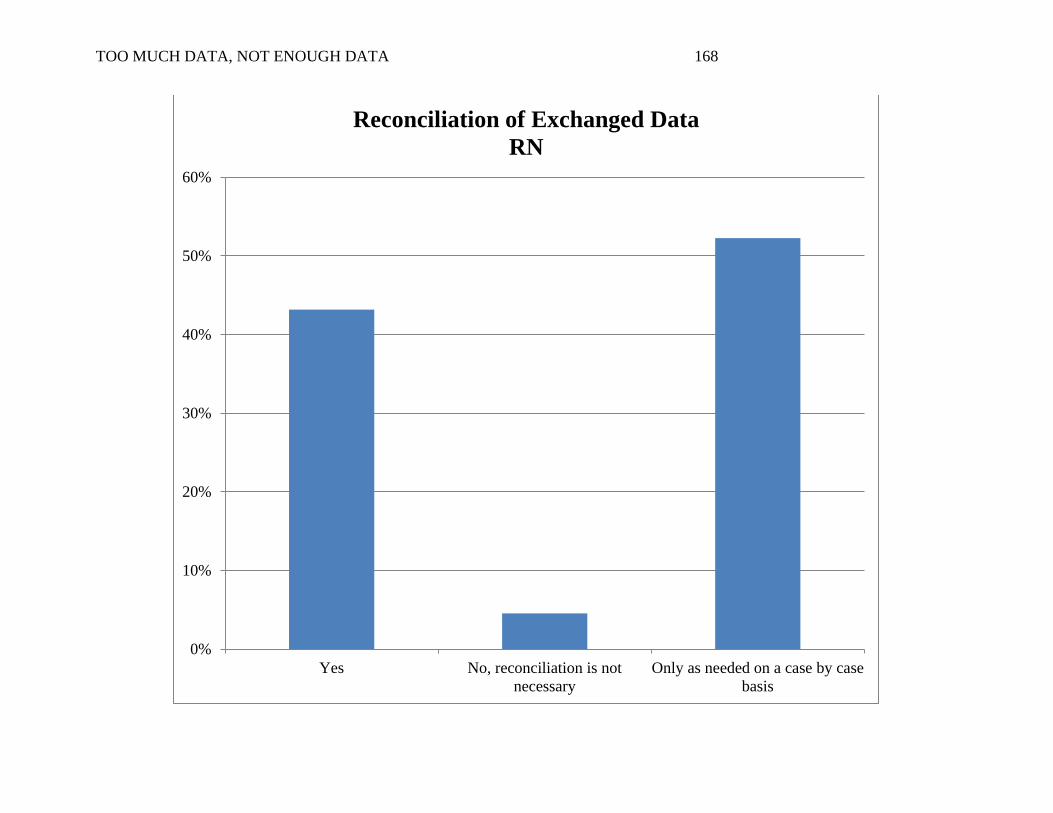
TOO MUCH DATA, NOT ENOUGH DATA 168
0%
10%
20%
30%
40%
50%
60%
Yes No, reconciliation is not
necessary
Only as needed on a case by case
basis
Reconciliation of Exchanged Data
RN
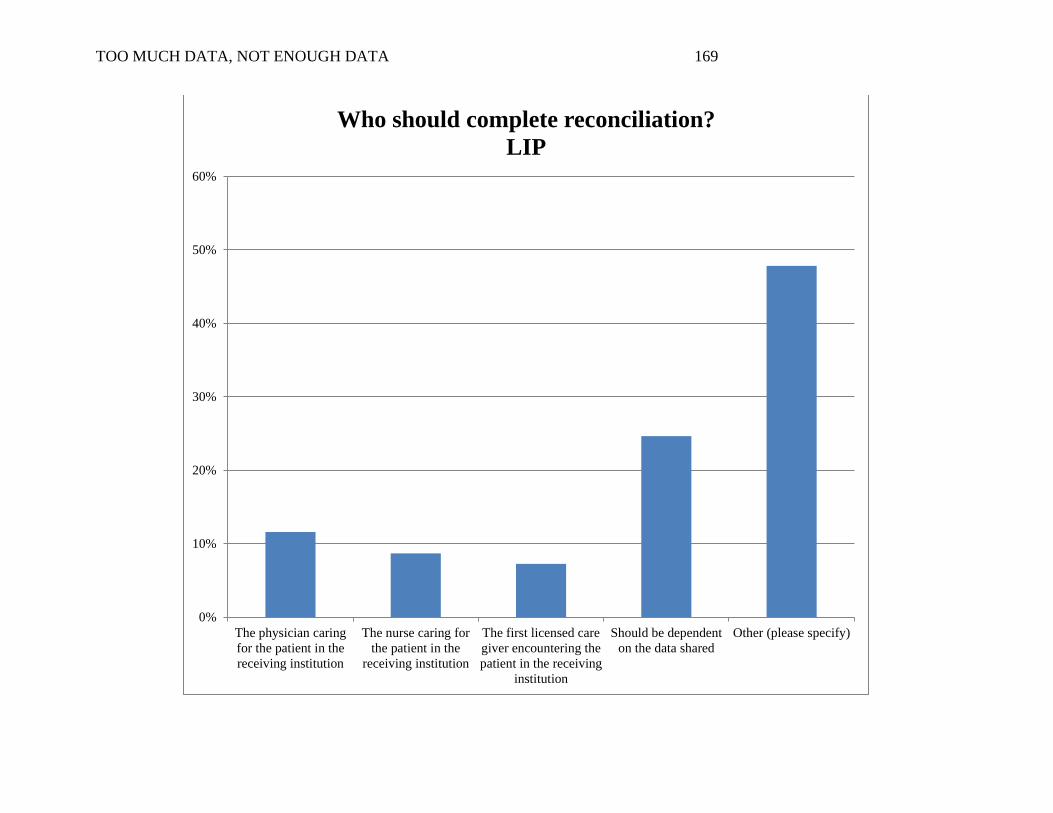
TOO MUCH DATA, NOT ENOUGH DATA 169
0%
10%
20%
30%
40%
50%
60%
The physician caring
for the patient in the
receiving institution
The nurse caring for
the patient in the
receiving institution
The first licensed care
giver encountering the
patient in the receiving
institution
Should be dependent
on the data shared
Other (please specify)
Who should complete reconciliation?
LIP
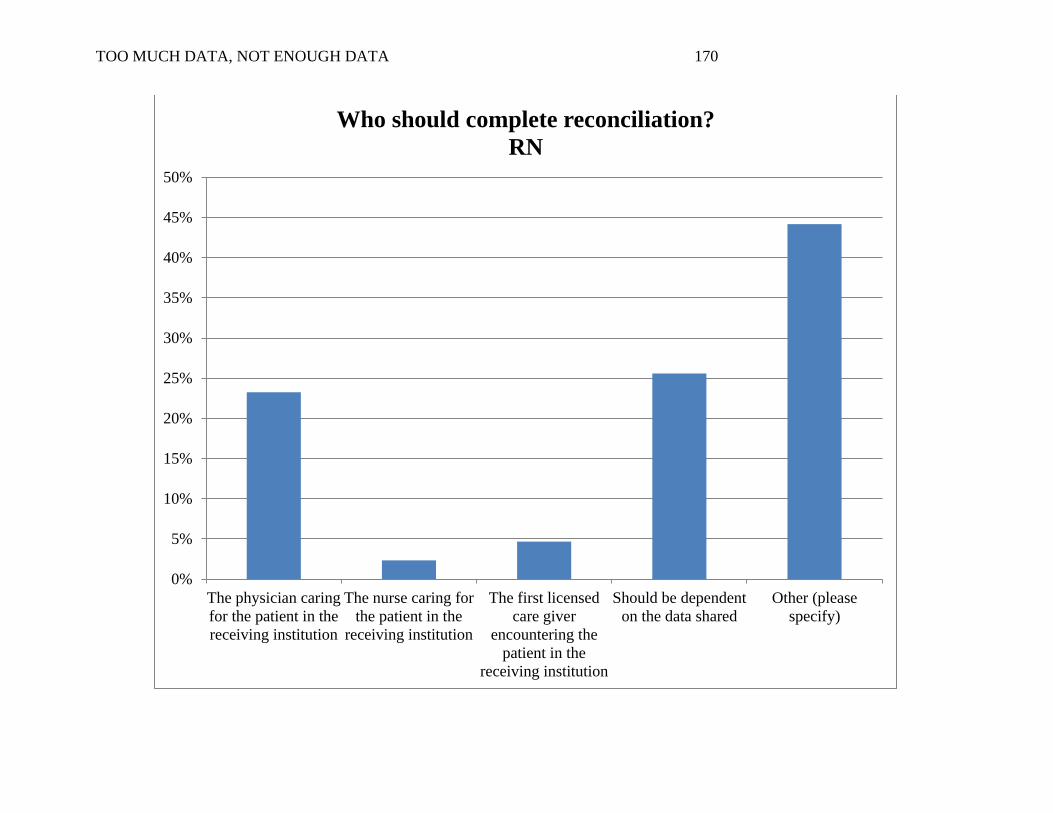
TOO MUCH DATA, NOT ENOUGH DATA 170
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
The physician caring
for the patient in the
receiving institution
The nurse caring for
the patient in the
receiving institution
The first licensed
care giver
encountering the
patient in the
receiving institution
Should be dependent
on the data shared
Other (please
specify)
Who should complete reconciliation?
RN

TOO MUCH DATA, NOT ENOUGH DATA 171