risk management/crisis plan - reed college · risk management plan ... communication, contingency...
TRANSCRIPT
ReedOutdoorProgramsandEducation
(ROPE)
RiskManagementPlan***
Emergency/CrisisPlan
Riskmanagementplanningistheprocessofreviewingallthedifferentaspectsofaprogramoreventorcourseandtodeterminewhatstepsneedtobetakentoensuresafetyandwell‐beingofallthepartiesinvolved.RiskManagementreferstothosewhoplanit,thosewhosponsorit,andthosewhoenjoytheactivityasaparticipant.Afteridentifyingrisks,itisnecessarytodeterminehowthatriskwillbemanaged.WhileworkingatReedCollegetherearethreewaystomanagerisk.
Reduceit. Transferit. Avoidit.
TheROPERiskManagementPlanisaroadmapofthestepstoensurethatriskshavebeenidentifiedandaprocesshasbeenestablishedtomanagetherisks.

2
3
RiskManagementandSafety
Thissectionofthemanualprovidesgoals,outlines,andproceduresforReedOutdoorProgramsEducationtofollowduringeachofitscourses.Thekindsofrisksacceptableforanindividualandindividualtravelareverydifferentfromthekindsofrisksacceptableforagroup
andgrouptravel.ReedCollegeoffersourstudentstheopportunitytopursueoutdoorpursuits,servicelearningprojects,andtravelbyexploringcommunitiesaroundthePacificNorthwest.Ourcoursesaresituatedinchallengingnaturalenvironments.ReedOutdoorProgramsandEducation
orROPEiscommittedtomanagingtherisksweassumeinordertomeetthegoalsofourprograms.Thefocusofoursafetystrategyisthreefold:
• Tocreateacultureofsafetywithourstaffandstudentsthrougheducation,training,and
informationdissemination.• Tocontinuallyimproveoursafetysupportsystemsofinformationgathering,
communication,contingencyplans,protocols,training,andinternalreviews.
• Tofosterexcellentrelationshipsinthecommunitieswherewetravel.GeneralOverview
ROPEplacesahighpriorityontherealisticmanagementofrisks.Becauseofthevariedterrainincludingmountains,rockwalls,whitewater,andoutdoorlivingcomponentsofourprogram,participationwithROPEcontainssomeelementsofrisk.Duetotherisksinherenttothis
program,ROPEcannotlegitimatelyofferaguaranteeofsafety.However,ouracuteawarenessofandfocusonproperriskmanagementdecreasesoverallriskandenablesustooperatewithinanacceptablelevelofrisk.
ThegoalofkeepingthegroupsafeandhealthyprecedesanydecisiontogorecreatingundertheguidanceofReedOutdoorProgramsandEducation.Itisimportantthateachindividualinthe
groupalsohasthisgoalinmindthroughouteachcourse,takingresponsibilityforhisorherownpersonalhealthandsafety.Asinotheraspectsoftheprogram,anexpeditionmentalityapplies.Poorchoicesonthepartofgroupmemberscanunnecessarilyputtherestofthegroupatrisk;
wisechoicesandtheinternalizationofourCoreValuedecision‐makingmakesthecoursesmootherforeveryone.
RiskManagementStatementROPEhasbeenentrustedwiththecareandeducationofitsstudentswhiletraveling.Assuch,thephysicalandemotionalhealthandwelfareofstudents,aswellasemployees,isofhighest
prioritytoROPE.Tothatendourriskmanagementplanincludesseveralkeycomponents:qualitystaff,informedstudents,contingencyplanning,andsupportservices(i.e.transportationandemergencycommunicationsystems).
QualityStaff
StaffatReedOutdoorProgramsandEducationwillbeexperiencedandqualifiededucators,
travelers,andoutdoorpeople.Instructorshavespecific,relevantexperienceandtrainingrelated

4
tothosesubjectsofwhichtheyareincharge.Weprepareourleadinstructorsforvariousoutdooractivitiesbyrequiringwildernessfirstresponder(WFR),swiftwaterrescue16‐hour
course,avalanche116‐hourcourse,andotherAmericanMountainGuideAssociation(AMGA)certificationswhenapplicableforspecifictechnicalactivitiesforquickandefficientresponsetoemergencysituations.Staffsareawareofstudentmedicalhistories,potentialenvironmental
hazards,andROPEsafetyandriskmanagementprotocols.InformedStudents
Engaginginoutdooractivitiesinvolvesinherentandotherrisks‐‐manyofwhichcannotbecontrolled.WhileReedOutdoorProgramsandEducationcannotguaranteesafety,itcananddoesstrivetomanagetheassociatedrisksandinformitsstudentsofthoserisks.ROPE
deliberatelyteachesstudentshowtoadaptbehavior,recognizeandmanagerisks,anddevelopexpertisetominimizepotentiallydangeroussituations.Studentsknowtheyareexpectedtoconductthemselvesresponsiblybypromotingtheirownsafetyandwell‐beingaswellasthatof
otherparticipantsandleaderswithintheprogram.Thus,studentsplayanimportantroleinourriskmanagementpractices.
ContingencyPlanning
Asapartofroutinelogisticalplanning,ROPEstaffmustcreatecontingencyplansonboththesmallandlargescales.Majorcontingencyplanningoccursatthebeginningofeachcourseduring
thepre‐destinationprocesswhentheEmergencyKitispreparedanddestination/river/trail/mountainsafetydiscussed.TheEmergencyKitiswiththegroupatalltimesandincludescallsheets,compass,andasatellitephone(whenapplicable).Throughoutthe
courseminorcontingencyplanningisanongoingprocesswhichoccursduringthepre‐coursecheckandbeforeeachriveroradventureouting.Duringthepre‐coursecheck,individualmapsmaybeconsulted,localnumbersforthesatellitephone,cellphone,andSPOTLocatorBeacon,
batterieschecked,andgroupsafety/risksdiscussed.Whilewecarryasatellitephoneonapplicablecoursesandacellphone,theriskmanagementplanneedstoincludecontingenciesincasetechnologyfails.
SupportServices
ROPEcarriesmedicalkitswiththematalltimes,aswellasOutdoorCallSheetswithemergency
contactnumbersforlocalemergencyservices.AGPS/SPOTEmergencyBeaconforemergencyandnon‐emergencysituationdescriptionsandlocationsisalsocarriedonexcursionsthatwarrantpossibleemergencysituations.Thiswillfacilitatecommunicationwiththedepartment
headduringregularcheck‐in/reportsandforemergencysituationswhenitmaybenecessarytonotifyparents,initiateevacuations,and/orbegininsuranceproceedings.
RiskManagementTeam
AssistantDirectorofPhysicalEducation/DirectorofROPE‐WillSymms
TheDirectorofROPEprovidesoversighttotheoverallmanagementandoperationofReedOutdoorProgramsandEducation.TheDirectorisresponsibleforproducingtherisk
managementmanualandmakingrevisionsasneeded.
5
MedicalAdvisor‐Dr.LizHatfield‐Keller
TheMedicalAdvisoristheresponsiblemedicaladvisorforReedOutdoorProgramsand
Education.
DirectorofPhysicalEducation‐MichaelLombardoTheDirectorofPhysicalEducationactsasdepartmentheadforPhysicalEducationdepartment,
whereReedOutdoorProgramsandEducationresides.S/heisactingdirectoroftheoutdoorprogramsiftheAssistantDirectorisunabletobereachedorperformhis/herduties.OutdoorSpecialist
TheOSistheleadspecialistinthefield‐facilitatinggroup.Thisindividualwillhaveavastarrayoftechnicalandmedicalskillsandactsinthefieldasthecollegerepresentative.
StudentSpecialist
Thestudentspecialisthasamoderatelevelofskillsandpossessesthemandatory80‐hrWildernessFirstRespondercertificationtoassisttheOutdoorSpecialistinmedicalassessmentsandevacuationswhennecessary.VehicleSafetyDrivingthevansisoneofthegreatestresponsibilitieswehaveatReedOutdoorProgramsand
Education.Statistically,thereismoredangerofanaccidentontheroadthananywhereelsewearewiththestudents,includingrivers.Itisimportanttorespectthisresponsibilityandtakeitonwiththeutmostcare.Driversmustpassthe15‐passengervehicle‐trainingprogramoperatedby
thevehiclecoordinatorforReedCollege,inordertooperatecollegevehicles.Additionalcertificationsarerequiredfortrailerdrivinganddrivingininclementconditions.ADMVbackgroundcheckisrequiredtoverifyacleandrivingrecordforeachpotentialoperator.
Anequallyimportantelementofsafetyisvehiclemaintenance.ThevehiclesandtrailersfallinlinewiththeReedOutdoorProgramsandEducationemphasisonprovidingaqualityexperience,
anditistheresponsibilityofallstaffmemberstomakesuretheyarewellmaintained.Tiresandfluidsshouldbecheckedfrequentlyandthevehiclesmustreceiveregularservice.ProblemsandserviceshouldbedocumentedandreportedtotheAssistantDirectorand/orVehicleCoordinator
forthecollege.Thestaffisalsoresponsibleforteachingthestudentstorespectandcarefortheequipment.ProgramEnvironmentsReedOutdoorProgramsandEducationviewssafetyasanintegralcomponenttothesuccessofitsprogramsandisvigilantinitscommitmenttosafetywithallROPEdestinations.Ifa
destinationisnotacceptableintermsofsecurityandgroupsafety,ROPEreservestherighttoalterorcancelaprogram.Examplesincludeflooding,volcaniceruptions,orforestfires.
TechnicalActivities
RockClimbing• AnOutdoorSpecialistshoulddirectlymonitorclimbingactivitiesatalltimes.
• Allgearshouldbeinspectedforexcessivewearordamage.
6
• Helmetsshouldbewornatalltimeswhileclimbingorbelayingunlessonanindoorwall.Itisadvisabletodesignatespecificareaswithinaclimbingsitewherehelmetsareworn.
• Helmetsshouldbewornforallfourthandfifthclasstravel.• Aback‐upbelayer/ropehandlershouldbeemployedunlesstheOutdoorSpecialistcan
ensurepeoplehaverequisiteskills,attention,anddedicationforbelayingone‐on‐one.
• Nopersonshouldlead‐climbunlessspecificallyapprovedbytheOutdoorProgramManager(AssistantDirectorofPhysicalEducation.)Inthiscaseleadingshouldalwaysbedoneonclimbswellbelowaperson’sactualleadingability.Generally,theOutdoorSpecialistshould
betheonlyleadclimberandbebelayedbysomeoneproficientatbelayingleadclimbers.• Allclimbsshouldbesetupwithmultiple,solid,independentanchors.Thestandardset‐up
includesatleastthreesolidanchorsindependentlylinkedtotwoopposinglockingcarabiners
usingseparatepiecesof1”tubularwebbing.• Ifusingboltsfortop‐ropeanchors,theseshouldbeinspectedthoroughlypriortouse.Ifyou
doubttheirintegrity,pickanotheranchororclimb.Alowerboltmayalsobeclippedfor
redundancy.• Afigureeightfollowthroughtieddirectlytotheharnessshouldbeusedforallclimbers.• Allstudentrappelersmustuseaseparatebelay.Onemaybelayarappelerusingeithera
figureeightorabowlineonacoilthatisalsoattachedtotherappelersharness.Whenrappellingsinglepitchesforthesakeoftheexperienceorduringparticipant’sfirstrappels,amuenteronamulequickreleasesystemishighlyencouraged.
• Noperson’sfeetshouldgohigherthansixfeetwhilebouldering.Spottingshouldbetaughtandusedwhilebouldering.
• OnrareoccasionsandwithpriorapprovaloftheAssistantDirector,studentsmayfollowan
OutdoorSpecialistonashortmulti‐pitchroute.Naturally,theOutdoorSpecialistwillleadwellwithintheircapability,andtheparticipantfollowerwilldemonstratethattheyareadeptatbelayingaleaderandcatchingleadfalls.Thisteamshouldbemonitoredinthe
eventtheyneedfurtherassistance.Theteamneedstohaveclimbedenoughtogethertowitnesseachother’sskillsinsteadofsimplytalkingabouttheirrespectiveclimbingability.
• Usegoodjudgment!Ifyouhaveagutfeelingorintuitionthatyoushouldorshouldnotbe
doingsomething,payattentiontothatfeeling.Pleasedonotlettheenthusiasmfortheexperienceovershadowyourindependentgoodjudgment.
Mountaineering Forourpurposes,mountaineeringincludestravelonorundersteepsnowslopeswhere
avalanchesmaybeafactor,glaciertravel,anytimewhenaniceaxeisnecessaryorprudent,
whenrope‐workisnecessary,orspendingextendedperiodsoftimeonsnowabovetimberline.
• AllOutdoorSpecialistsmustconsultwiththeAssistantDirectortodiscusstheeducational
outcomesandriskmanagementparticulartotheirtrip.• Avalanchedangergenerallyshouldbeassessedaslowtoverylowintheterrainbeing
traveled.Exceptionsinvolvetransceiversandsnowanalysisasanintegralpartsofthe
experienceandshouldtakeplaceinnomorethanmoderateterrain.• Participantsmusthaveparticipatedina“snowschool”sessiontolearntravelandself‐arrest
skillsbeforetheneedarisestoemploythoseskills.
• Allparticipantsshouldhaveadequateequipment.Warmclothes,raingear,water,food,awhistle,andacompassareaminimum.
7
• Afirstaidkit,extrafood,stove,pan,shelter,groundtarp,ensolitepad,shovel,andsleepingbagshouldaccompanygroupsonsnowsummitattempts.
• ParticipanttoOutdoorSpecialistratiosshouldnotexceed5:1.Thismayneedtobeaslowas3:1forcertainactivities.
• Aswithpurerockwork,allsnowandicerope‐workneedsmultiple,solid,independent
anchors.Thestandardset‐upincludesatleastthreesolidanchorsindependentlylinkedtotwoopposinglockingkarabinersusingseparatepiecesof1”tubularwebbing.
Rafting AllriversandrunsmustbeapprovedinadvancebytheAssistantDirectororDirectorof
PhysicalEducation.• OutdoorSpecialistsmustbefamiliarwiththerunonwhichtheyareteachingorguiding.
• AllOutdoorSpecialistsmustconsultwiththeAssistantDirectorofPhysicalEducationtodiscusstheeducationaloutcomesandriskmanagementparticulartotheirtrip.
• IfanOutdoorSpecialistdeemsittooriskytoundertakearunorcontinuedownariverfor
anyreason,theteamshouldplayitconservatively.• AllOutdoorSpecialistsmustwearafunctionalPFD,riverknife,andwhistle.• AllparticipantsshouldwearafullyfastenedPFDwhileonthewater.
• Whenpractical,aswimassessmentinapoolsettingshouldbedonepriortoatriporclassthatspendsagoodamountoftimeonorinwater.This150‐yardswimisgenerallynotusedasanadmissionrequirementbutgivestheOutdoorSpecialist(s)agoodideaofa
participant’scomfortinwater.• Boatsshouldsupporteachotheronthewaterinawaythattheycancommunicatewithand
lendsupporttooneanotherintimesofdifficulty.
• RescueandrepairkitsshouldaccompanyallReedCollegeraftingtrips.Thisshouldincludeover100’ofropecapableofbeingusedforadvantagesystems,prussiks,carabiners,1”tubularwebbingforanchors,apatchkit,andanairpump.Additionalsuppliesmaybe
requiredfromtheagencieswithwhomwework.• OutdoorSpecialistsmustgiveallparticipantsathoroughsafetytalkbeforeembarkingon
thewater.Thisshouldataminimumincludegeneralhazards,personoverboard,swimmer’s
position,footentrapment,strainersandholes,highside,andanunderstandingofhowtocatchathrowbag.
• Plannedswimsorperson‐overboarddrillsshouldonlytakeplaceinareasdeemed
appropriatebytheOutdoorSpecialists.
SeaKayaking,Canoeing,Sailing,andOtherWater‐BasedActivities• AllOutdoorSpecialistsmustconsultwiththeAssistantDirectorofPhysicalEducationto
discusstheeducationaloutcomesandriskmanagementparticulartotheirtrip.• AllparticipantsshouldwearfullyfastenedPFDswhileonthewater.• AllOutdoorSpecialistsmustwearafunctionalPFD,knife,andwhistle.
• Whenpractical,aswimassessmentinapoolsettingshouldbedonepriortoatriporclassthatspendsagoodamountoftimeonorinwater.This150‐yardswimgenerallyisnotusedasanadmissionrequirement,butgivestheSpecialist/sagoodideaofaparticipant’scomfort
inwater.• Ifconditionssuchaswaterflow,wind,orsurfheightaresubstantiallydifferentthan
anticipatedforagivenactivity,athoroughassessmentshouldbedonewithregardstothe
viabilityofachievingtheeducationaloutcomeswhilemanagingtheriskoftheactivity.The

8
OutdoorSpecialistsmaydecidetoincludetheAssistantDirectorofPhysicalEducationinthisdecision‐making.
Oneactivityonthemarginsofbeingclassifiedaswater‐basedisfishing.Fly‐fishinginslowmovingcurrentmaybeundertakenwithoutaPFDprovidedthewaterlevelisnotovertheparticipant’skneesandthereisgoodrun‐outfromtheareainwhichtheyarestanding.
TransportationReedOutdoorProgramandEducationrecognizesthattravelingbetweensitesduringthecourse
containsanelementofrisk.Dependinguponthevariousmethodsoftransportationavailable,staffshouldselectthesafestmodeoftransportationatthattime.
PublicTransportation
Tochooseappropriatetransportation,staffmembersmustselectthesafestvehicle,driver,androuteavailable.ReedOutdoorProgramandEducationstrivestoprovidesafeanddependable
transportation.RentedVehicles
ROPEmayrentvehiclestotransportstudents.RentalvehiclesareoperatedbyapprovedROPEstaff.Eachstaffmembermusthaveanapproveddrivingrecordandmustreviewandadheretotheapplicablelawsandconditionsforthestatesinwhichtravelwilltakeplace.
ROPEOwnedandOperatedVehicles
• Vanoccupancywillnotexceed14students.• Allpassengersmustwearseatbelts.• Eachvehiclemusthaveafireextinguisher,firstaidkid,andemergencykit.• Allstatelawsandspeedlimitsmustbefollowed.• Allvehicledocumentsmustbefilledoutpre‐andposttrip.• Thevehiclemustbesafetycheckedpriortoeachuse.
RiskAwarenessInadventureeducationprogramming,studentsdieeachyearfromtraumaandillness,andmany
studentsareinjured.Thegreatestnumberofdeathsinadventureprogrammingresultfromtransportationanddrowning.
Negligence
ThenumberoneliabilityyouhaveasOutdoorSpecialistsisnegligence.Thefollowingfourconditionsmustbepresenttoprovenegligence:(1)adutytoact,(2)aninjurymusthave
occurred,(3)abreachofduty,and(4)causation.
DueDiligence
DueDiligenceisyournumberoneprotectionasanOutdoorSpecialistwithReedOutdoor
ProgramsandEducation.Duediligencemeansgoingthedistance,doingyourhomework,anddoingwhatanyonewouldexpectofyouduringspecificsituationsandconditions.Ifyouhaveaquestionaboutthis,calltheROPEofficetoaskforadvice.Youcanalsopictureyourselfincourt
answeringquestionsaboutyourdecision‐makingprocessandhowyoudeterminedasituation
9
wasacceptable.Yourbiggeststrengthinreducingriskistounderstandyourhazardexposure,createplanstopreventhazardexposure,andmitigateconsequenceaseffectivelyaspossible.
Performthefollowingtothebestofyourabilitywhenmakingdecisions:
• Askyourselfwhatareyouaredoing(who,what,where,when,andhow).
• Doyourhomework/research(duediligence).Defineyourhazards.• Createrisk‐managementstrategiesincludingobjectivehazardavoidance.• Createsupportstrategies(transportation,medicalcare,andcommunication).
• Establisheffectivecontingencyplans.Whoareyourstudents?
Collegestudentsbetweentheagesof17‐24arethetypicalpopulationweserve.Knowtheirmedical,psychological,anddisciplinehistory.
PracticeDueDiligence
Gathergeneralinformation,understandregionalhazards,riverhazards/risks,snowconditions/risk,andupdatedtrailconditions.Researchandunderstandhowtheseissuesand
relatedriskswillaffectandinfluencethestudentgroup.• ROPEinvestigatestheseriskspriortodeparture.OutdoorSpecialistsareexpectedto
continuallyevaluatetheserisksduringthecourse.
ProgramAnalysis
AsOutdoorSpecialists,youhavetheinsightandtheknowledgetohelpROPEmakeeachcourse
safer.HelpROPElearnaboutopportunitiestomakethingssaferintermsofprogramphilosophy,leadershipstructure,policies/procedure,staffhiring,stafftraining,operations,medicalscreening,gearmalfunction/misuse,organizationalculture,and/ormiscommunications.
DiscriminationandHarassmentPolicyReedCollegeiscommittedtocreatingandmaintainingacommunityinwhichstudents,faculty,
andstaffcanwork,live,andlearntogetherinanenvironmentfreeofdiscriminationorharassmentbasedonrace,gender,nationalorigin,age,religion,sexualorientation,disability,oranyotherstatusorcharacteristicthatisprotectedbylaw.Thiscommunityextendsbeyondthe
campus’sphysicalboundariesandintothewildernesscontext.Membershipinthiscommunity,asgovernedbythehonorprinciple,imposesonstudents,faculty,andstaffanobligationtorespectthedignityandautonomyofothersandtotreatoneanothercivillyandwithoutregardto
factorsirrelevanttoparticipationinthelifeofthecollege.
Romanticorsexualrelationshipsthatmightbeappropriateinothercontextsmay,withinthecollegecommunity,createtheappearanceorfactofanabuseofpowerorofundueadvantage.Sensitivitytopossibleconflictsofinterestortomisuseofpowerisnecessaryincasesofother
romanticorsexualrelationshipswhereonepartnermaybeinapositionofpowerorauthorityoveranother(whichcanoccurbetweenfacultyandstaff,staffandstudents,orwithinthestaff,studentbody,orfaculty).
ProceduresfortheResolutionofComplaints:Thecollegehasbothprincipledreasonsandalegalobligationtoinvestigatepossibleviolationsof
itsantidiscriminationandharassmentpolicy.
10
ThehonorprincipleandthetraditionsofReedCollegeencouragetheinformalresolutionofcomplaints.Informalresolutionmayoccurthroughdirectdiscussion,throughmediationunder
theauspicesofthehonorcouncil,orwithadviceobtainedfromadesignatedofficerofthecollege(alistofsuchofficersispublishedandmaybeobtainedfromtheofficeofthepresident).
Complainantswishingadviceabouthowtoproceedwithacomplaintshouldconsultamemberofthehonorcounciloradesignatedofficerofthecollege.
Forfurtherinformation,consultthefullpolicystatementonantidiscriminationandharassment
intheGuidebookforReed.CopiesoftherelevantsectionsoftheStudentJudicialCode,staffhandbook,andrulesandproceduresofthefacultyareavailableinthestudentservicesoffice.
ROPEEMERGENCYSYSTEMS
Ourprogramhashadanexcellenttrackrecordofmanagingriskeffectively,andwewanttokeepthefocusonmanagingandavoidingriskinsteadofrespondingtoaccidents.Westrivetoengage
inadventurousactivitieswhereriskislimited.AnOutdoorSpecialistorStudentLeadershouldbeabletoarticulatewhyagivenactivitywasundertakenandwhatmerittheactivityhasinlightof
anyinherentrisksthatexist.Ifone’sexperiencedictatesthatthegroupshouldbemoreconservative,theStudentLeadershouldgivecredencetohisorherexperience.IfOutdoor
SpecialistsandStudentLeaderscontinuetomanageriskwell,theprogramshouldcontinuetothriveandexpand.
Decision‐Making,TakingChargeoftheSituation
Ifanemergencyoccurs,thedesignatedleadershipshouldtakedirectcontrolofthesituation.Itis
proventhat,incrisissituations,adirecthierarchyhelpsclarifywhatactionsshouldbetakeneveniftheOutdoorSpecialistchoosestosharetheirdecision‐makingresponsibility.Pleasediscussthis
hierarchyandyourcomfortwithhandlingemergencieswithyourco‐leadersand,ifappropriate,theAssistantDirectorbeforethetripstarts.
UsingtheCallGuide–RequestingAid
Whenavailable,mobilephonesshouldbecarriedonalloutdoortrips.Thatsaid,therearemanylocationswhereitisdifficulttocall;youcannotassumeatelephonewillworkaspartofyourrisk
managementplan.Asaleaderyoushouldfamiliarizeyourselfwithboththemobilephoneandthecallguidebeforebeginningthetrip.Confirmtheareatowhichyouaretravelinghas
resourceslistedinthecallguide.Ifnot,itisyourresponsibilitytofindthenearesthospitalandsherifflocationsandnumbersbeforeleavinghome.Ifyoucallintoaskforhelpfromtheoutdoor
programmanager,youshouldhaveclearinformationaboutthesituationcompletewithaSOAPnote,ifapplicable,aswellasyourproposedplanofaction.
UnscheduledLossofContact–SearchandRescue
Ifsomeoneisthoughtorknowntobelost,aquicksearchshouldbedoneimmediately.Ifthe
trip’sleadersareexperiencedwithgridsearchesandiftheydecidetheycandoaninitialsetquicklyandsafely,thisoptionmaybeentertained.Afterthreehoursofconductinganysearchor
ifotherwiseconsideredappropriatebytheleaders,theAssistantDirectorofPhysicalEducationatReedshouldbecontactedtodetermineifoutsideassistanceisnecessary.Onceoutside
11
agenciesarecontactedtoassistwithasearchtheleadersshouldacceptthattheynolongerhave
totalcontroloverthedirectionandnatureofthesearch.
Createemergencyplansforeachcourse!Eachcourseshouldhavethefollowingplans,asneeded.Togetherstaffneedstocreateanemergencyprocedureplantothinkaboutwhattodo
iftheworsthappens.
EmergencyProcedures• STOPandTHINK!
• Plan:Makeaplan• Review:Reviewandevaluatetheplan• Act:Implementtheappropriateplan(seebelow).
GenericDisasterPlans
EvacuationPlans
• Triggers• Stagesofpreparation• Taskteams/leadership
• Multipleroutes(riverevacuation,politicalunrest)• Designatedvehicles• Water,food,andfuel
• Communication• Emergencymedicine
“HunkerDown”Plans• Triggers• Stagesofpreparation
• Taskteams/leadership• Securetheareaofdebrisorhangingdangers• Water,food,fuel,shelter
• Communication• Medicalemergency
InitialResponseResponsestoincidentsvarywithseverity.Seriousincidentsarethosethatresultindeath,
threatenlimbs,orthelong‐termwell‐beingofanyindividual.Minorincidentsarethosethatdonotthreatenlife,limb,orthreatenthelong‐termwell‐beingofanyindividual.Thoughlesssevere,minorincidentsmaystillrequireapromptresponsesuchasavisittoaphysician.
MinorIncident:InformtheAssistantDirectortodetermineanappropriatecourseofaction.Filloutanincident/accidentreport(within3days)andemailtotheROPEoffice.
SeriousIncident:Stabilizethepatientasperyourtraining,notifytheAssistantDirectorimmediately,andifpossible,activateanemergencyresponsesystemortransportpatienttothe
besthospitalavailable.Allseriousincidentsmustberecordedinanincident/accidentreport.
12
Protocolformajorincidents,seriousinjury,ordeath:Contact911,thenAssistantDirectorofROPE,thencommunitysafety.
Allincidents,majorandminor,mustbereportedtothecampusasquicklyaspossible.Parentsalsoneedtimelyinformation.Forminorincidents,adirectemailtoAssistantDirectorsoffice
outliningtheincidentwillsuffice;theAssistantDirectorwillpassthisinformationalongtotheparents.Formajorincidents,theOutdoorSpecialistmustcontacttheAssistantDirectorviatelephoneasquicklyaspossible.TheAssistantDirectorandOutdoorSpecialistwilldecidewhen/
howtoproceed.CrisisManagementPlan
Acrisisisdefinedasaneventthatneedsanimmediateresponseandaction.Thiseventmaypresentlong‐termchallengestoROPE,itmaybealifeorlimbsituation,itmaybeastaffcrisis,and/oritmaybeanenvironmentalevent.
IncidentCommandSystem
IncidentCommander–PersoninCharge
TBA SafetyOfficial–On‐sitePersoninCharge
TBA
PublicInformation/PlanningOfficialTBA
ROPEAdministrationOfficial
TBA
DivisionofLaborEveryemergency,nomatterhowlargeorsmall,requiresthatcertaintasksorfunctionsbeperformed.Theorganizationcanexpandorcontractdependingonthesizeoftheemergencyand
thenumberofstaffavailable.• IncidentCommander–Responsiblefordevelopmentofschool’splanandoverall
managementofemergencysituations
o Developsworkingknowledgeoflocal/regionalagenciesastheon‐scenecontactforoutsideagenciesassignedtoanincident,documentingactivitiesasnecessary.
• SafetyOfficial–Monitorssafetyconditionsofanemergencysituationanddevelops
measuresforensuringthesafetyofstudents,staff,volunteers,andresponders,documentingactivitiesasnecessary.
o Ensureseveryoneknowstheplan,monitorsmedical,environmental,psychologicalfirst‐aid,foodandwaterneeds,andensuresallneedsaremet.
• PublicInformation/Planning/IntelligenceOfficial–Developsworkingknowledgeoflocalmedia,preparesmediareleases,andcoordinatesinformationwiththeIncidentCommander.
o AssiststheIncidentCommanderinthecollectionandevaluationofinformation
13
aboutanincidentasitdevelops,assistswithongoingplanningefforts,maintainsincidenttime‐log,anddocumentsactivities.
o Establishes/overseescommunicationcenteractivitiesduringanemergencybydevelopingaphonetreeforafter‐hourscommunication,documentingactivitiesasnecessary.
• AdministrationOfficial–Keepsallrecords
andensuresthereisapapertrailand
writtenlogofallactivity.
MediaAllstaffmustrefertotheAssistantDirector.ROPEassumesresponsibilityforissuingstatementsinan
emergency.• TheAssistantDirector,incooperationwith
thePublicInformationofficer,mayprepare
astatementtobeissuedtothemedia.• Updatethemediaregularly.Donotsay,“Nocomment.”• Donotarguewiththemedia.
• Maintainalogofalltelephoneinquiries,andrespondusingscriptforinquiries.MediaStatement
• Allmediastatementsmustcomefromtheofficeofpublicaffairs.
MediaResponse
"Wearefollowing
organizationalprotocol.
Duetotheemergency,wedo
nothavetimetodiscussit
withyou.Pleasecontactthe
officeofpublicaffairsfor
moreinformation.”

14
RiskMitigation–CreateContingencyPlans(Including“triggers”forsendingastudenthome.)
• LostStudent:Immediatelygathertheentiregrouptogether,gatherallinformation,createasearchplan,andcontactROPEdepartment.Then,notifylocalauthorities.Last,createaCommunicationPlan.
o Trigger:Studentsenthomeiftheydeliberatelysetouttoleavetheprogram;thiscreatesadangertotheirpersonalsafety.
• AlcoholandOtherDruguse:Immediatelygatherstaffandallinformation,contacttheROPEdepartment,andfollowguidelinesforreportingtoCommunitySafetyandStudentServiceOffice.
o Trigger:Studentissenthomeforusingdrugs/alcohol.
• EmergencyEvacuationGuidelines:ItisthepolicyofROPEtoevacuatestudentswithany
injurythatcouldcausepermanentdamageifnottreatedwiththepropermedicalcare(i.e.faciallacerations,jointlacerations,orinjuriestogenitalia).Studentsshouldbeevacuatedtothenearestlargecitywhereahigherlevelofcarecanbeadministered.
• CarAccident:CheckforsafetyandinjuriesofallO.S.andstudents,andcontactmedical
personnelifnecessary.Contactlocalauthorities,theROPEOffice,andtheinsurance
provider/carrentalcompany.o Trigger:Studentsenthomeforanyinjurylistedin“emergencyevacuation.”
• Misbehavior:InformstudentsofHonorPrinciplepriortotripssothatallinformationisknownbeforehand.Documentincidentsofmisbehavior,notifytheROPEoffice,notifythestudentandfollowtheguidelinesforHonorCaseinvestigations.
o Trigger:StudentsenthomebaseduponbreakingtheHonorPrinciple.
• PsychologicalEmergency:Contactqualifiedpersonnelimmediately.Iflocalhelpisnot
availableorqualified,contacttheROPEofficetofindaqualifiedprofessional.TheROPEofficewillimmediatelynotifythehealthcenter.Ensurethestudentisnotadangertohimself/herselforothers.Beginevacuation,ifnecessary.
o Trigger:StudentsenthomeifthelevelofpsychologicaldifficultyisbeyondthequalificationsorcomfortoftheOutdoorSpecialist.
• NaturalDisaster:Createcontingencyplansbeforeadisaster,examiningphysicalsafety,accommodation,food,transportation,andcommunication.IfthedisastercompromisesthesafetyofthestudentsorOutdoorSpecialist,beginevacuationplansimmediately.
ShareacopyofthecontingencyplanwiththeROPEoffice,whichwillcommunicatewithparents.
o Trigger:Sendstudentshomeifthenaturaldisastercreatesanenvironmentor
situationthatisunsafeforthegroup.Analternativelocationfortheprogramisanotheroption.
15
• SexualAssault:Ifassaultoccurs,immediatelycontactlocalauthoritiesanddirectorofROPE.Contactthedirector,astheROPEofficewillcontacttheappropriatecollege
officesandadvisorysexualassaultcounselor.o Trigger:Sendstudenthomebasedonstudentrequest.
• Death:Ensurephysicalandemotionalsafetyforthegroup.ContactlocalauthoritiesandtheROPEoffice,andtheROPEofficewillcontactparents.Createacommunicationplan.
o Trigger:Sendotherstudentshomeifmentaltraumaexists,and/orbystudentorparentrequest.
Fortheseexamples,itisimportantthestaffworkdirectlywiththeROPEofficetoensurerapidresponseinordertoworktogethertocreateanemergencyactionplanandacrisismanagementplanspecifictoeachincident.ROPEmitigatesriskwithplans,training,andexpertise.This
includesstafftraining,crisissimulationsduringstafforientation,incident/accidentreporting,evacuation,andstaffmedicaltraining.ROPEalsoutilizestheexpertisefromanadvisoryphysician,anadvisorycounselor,alegalcounsel,andaninsurancecounsel.
CommunicationCommunicationintheeventofaccidents,injuries,andillnessiscritical.Intheeventastudentis
ill(i.e.unabletoparticipateinclassesformorethan2days)orhasaninjury,whichrequiresavisittoaphysician,thehealthcentermustbecontacted.Inordertodoso,theassistantdirectorwillinitiateallcommunicationtothehealthcenterregardingparticipanthealthbasedofffield
instructor’sreport.DocumentLog/Records
ROPEstaffmustalwaysdocumentincidentsandnearmisses.MinorincidentsandseriousincidentsmustberecordedonanIncident/accidentreportform.Thepurposeofthesupplementalformsistodocumenttheobjectivefactsassociatedwithanygiven
incident/accident.Assuch,onlyknown,impartial,andobjectivefactsshouldberecorded.SOAPnotesshouldbecompletedforsignificantaccidentsandtheaccompanyingtreatment,andturnedintotheAssistantDirector.
PhoneLog
Recordphonecalls(numbers,person(s),andtime).
WitnessStatements
Getdescriptionof"what,where,who,andwhen”bywitnessesassoonaspossible.
16
SectionII
TreatmentandEvacuation
Guidelines
REV:8/8/201211:30AM
17
TreatmentandEvacuationGuidelines
TheseTreatmentandEvacuationGuidelinesaretheexclusivepropertyofReedOutdoorProgramsandEducationandmaybeusedonlybyROPEinstructorswhileleadingROPEcoursesinawildernesscontext.ThecontentsofthisdocumentarenottobecopiedorreproducedinanyformwithoutwrittenpermissionfromROPE.Theseprotocolshavebeendevelopedinconsultationwith________________________________,ROPEMedicalAdvisor.
MedicalAdvisorDutiesandResponsibilities
ThisservestodescribethedutiesandresponsibilitiesofDr.___________whoareservingastheMedicalAdvisorforReedOutdoorProgramsandEducation.
ROPEMedicalAdvisorDutiesandResponsibilitiesTheROPEMedicalAdvisorprovidesguidanceandadvisesROPEregardingstudentandstaffmedicalissuesrelatedtoparticipationonROPEcoursesoremploymentwithROPE.ReedOutdoorProgramsandEducationmakesfinaldecisionsregardingstudentparticipation,medicaltreatmentandevacuation.TheROPEMedicalAdvisor:
1. SupportsdevelopmentofROPEfieldmedicaltreatmentandevacuationprotocolsusedbyROPEinstructorsduringROPEprograms.
2. Reviewsprotocolsonaregularbasisandevaluatestheireffectiveness.
3. ProvidesadviceasneededastothedispositionofillorinjuredstudentsorfieldstaffduringROPEcourses.
4. ServesasaresourceregardingmedicalscreeningofstudentsorstaffforROPEprograms.
5. Providespost‐incidentreview.RoutinelyreviewsfieldmedicalpracticestoensureconsistencywithROPEprotocols.

18
UsingtheROPEWildernessMedicineProtocolPackage
INTRODUCTION
ROPEinstructorsandstaffareexpectedtooperateeffectivelyinchallengingenvironmentalconditionswithlimitedequipmentandsupplies.FrequentlyprovidershavelittleornoaccesstocommunicationwithamedicalprofessionalorEmergencyMedicalServicessupportsystems.Inadditiontorecognition,treatmentandpreventionofmedicalemergenciesinremotesettings,aanymemberoftheROPEstaffmustunderstandhowandwhentomakeanevacuationdecision.
Thisdocumentisintendedtoprovidedetailedrecommendationsontreatmentandevacuationguidelines.Theseprotocolsshouldbeadministeredbyinstructionalstaffwithappropriatetraininginwildernessmedicine.Theyshouldbeutilizedinawildernesscontextorwhenmedicalsupportisnotavailable.Theyshouldbeutilizedduringsanctionedprogramactivities.Theyshouldnotsubstitutefordefinitivemedicalcarewhenitisnecessaryandavailable.Theyarenotasubstitutefortraining.
Theseprotocolscontaininformationontheadministrationofbothover‐the‐counter(non‐prescription)andprescriptionmedications.Typicallytheadministrationofover‐the‐counter,medicationfallswithintherealmofsimplefirstaid.Theadministrationofover‐thecountermedicationtominorsrequiresparentalapproval,whichareobtainedthroughpre‐tripauthorizationformsorbycommunicatingwiththeparentsonacasebycasebasis.
AdministeringprescriptionmedicationsisusuallyrestrictedtolicensedmedicalprofessionalsorindividualsactingwithinestablishedEmergencyMedicalServicessystems.Someremotecoursesmaycarryprescriptionmedicationsasacomponentoftheirmedicalsupplies.Frequentlyindividualswillbringtheirownprescriptionmedicationsonatrip,especiallyonaninternationaltrip.Whilestaffmaynotbeadministeringthesemedications,havinginformationabouttheirusecanbeveryhelpful.
19
Onepotentialexceptiontotheguidelineofalicensedmedicalprofessionaladministeringaprescriptionmedicationistheuseofinjectableepinephrine.Thereareincreasingnumbersofstatelawsthatallowfortheadministrationofepinephrinetoanindividualexperiencingalifethreateningallergicreactionbya“layperson”.Oftentheepinephrineadministeredisthepatient’s.Thisislikelytobeanareaofcontinueddiscussionandevolvinglawsandregulationsintheensuingyears.
TheseprotocolsshouldbemodifiedinconsultationwiththeROPEMedicalAdvisor.Theprotocoldecisioncomponentofeachprotocolcoachesyouthroughpotentialmodifications.
DisclaimerThesedocumentsarenotasubstituteforprofessionalmedicalcareoradvice.
Introduction•WildernessMedicineOverview•TheRoleofaMedicalAdvisor•MedicalAdvisorJobDescription•ProtocolUseStatementProtocols•Abdominal•AllergicReactionsandAnaphylaxis•AltitudeIllnesses•Burns•CardiacEmergencies•CardiopulmonaryResuscitation•ChestTrauma•DentalProblems•Diabetes•Dislocations•EyesEarsNose•FemaleGenderMedicalIllnesses•FlulikeIllness.doc•HeadInjuries•HeatIllnesses
•Hypothermia•Lightning•LocalCold•MaleGenderMedicalIllnesses•MusculoskeletalInjuries•NeurologicalEmergencies•Poisoning•RespiratoryEmergencies•Shock•Skin•SnakesandLizards•SpidersandScorpions•SpinalInjuries•SubmersionIncidents•WildernessWoundManagement•ZoonosesExtras•DrugInformation•FirstAidKitContents•SOAPReportTemplate•VerbalSOAPTemplate
EvacuationWildernessMedicalTrainingCenter(WMTC)grantedthefollowinginformation.Attimestheevacuationofapatientmaybenecessaryfortheirtreatment.Allevacuationsinawildernessenvironmentcarrysomeinherentrisktomembersoftherescuepartyandthedecisionto
20
evacuateapatientshouldNOTbetakenlightly.Theneedforevacuationdependsontheseverityofthepatient’sinjuryorillnessandyourresources.Thetypeofevacuationdependsonthemobilityofthepatient,thesizeofyourpartyanditsresources,thedifficultyofterrain,theweatherandthedistanceinvolved.
TheTYPEofevacuationdependson:
• theseverityofthepatient’sinjuryorillnessandtheirmobility
• thesizeofyourpartyanditsresources
• thedifficultyofterrain
• theweather
LevelsofEvacuationThefollowingdefinitionsforlevelsofevacuationarecorrelatedtotheseverityofthepatient’sinjuryorillnessandhencetheurgencyandspeedoftheirevacuation.Everyeffortshouldbe
madetoaccuratelydiagnosethepatient’scurrentandanticipatedproblemssinceanincorrectdiagnosismayleadtoafalsesenseofurgencyandawillingnessonthepartoftherescuerstoacceptmoreriskthanthesituationwarrants.Ingeneral,rescuersshouldONLYbewillingto
acceptalevelofrisktheybelievetheycansafelymanagebasedontheirskillandtheforeseeableproblems.Unfortunately,notallproblemsareforeseeableandtheamountofriskanygivenrescueriswillingtoaccepttendstorisewiththeseverityofthepatient’sinjuryor
illness.Sinceitisimpossibletolegislatejudgement,whenindoubtrescuersmustbasetheirdecisionsonthe“worstcase”situationbothindiagnosingthepatientandevaluatingtheriskassociatedwiththeevacuation.Thatsaid,theriskofaminorinjuryorillnesstoarescueris
generallypresentduringmostevacuationsandunavoidableunderthecircumstances.
Level1
Thepatient’sinjuryorillnessisimmediatelylifethreateningandthepatientmaydiewithoutrapidhospitalintervention(e.g.:increasedICP,volumeshock,severerespiratorydistress,respiratorydistressinaneardrowningpatient,advanceddisease,moderatetosevere
hypothermia,HAPE/HACEetc.)
Level2
Thepatient’sinjuryorillnessispotentiallylifethreateningorwillresultinapermanent
disability;thepatientmaydevelopalifethreateningproblemthatrequireshospitalintervention(e.g.:concussionthatisgettingworse,systemicinfection,spine&cordinjuries,neardrowning(norespiratorydistress),etc.)
Level3
21
Thepatient’sinjuryorillnessisNOTlifethreatening,haslittleornopotentialtobecomelifethreatening,andmaybesuccessfullytreatedinthefieldwithnopermanentdisability;however,
thepatientisunabletoresumenormalactivitywithinareasonablelengthoftimeand/orrequiresadvancedassessment.(E.g.:concussionthatisgettingbetter,inunstableinjurieswithgoodCSM,reducedshoulder(dislocation)withgoodCSM,etc.)
Level4(noevacuation)
Thepatient’sinjuryorillnessisNOTlifethreatening,maybesuccessfullytreatedinthefield
withnopermanentdisability,andthepatientisabletoresumenormalactivitywithinareasonablelengthoftime.(E.g.:minorwounds,minorstableinjuries,minorenvironmentalinjuries,etc.)
WILDERNESSFIRSTRESPONDERANDALLERGICRESPONSETRAININGAllReedoutdoortripsthattraveltoareastwohoursormoreawayfrom“definitivecare”are
requiredtohavealeaderonthetripwithWFRaswellasOregon‐authorizedallergicresponsetraining.
SuchTrainedLeadersareExpectedto:
• Staywithinthescopeoftheirtraining,andifindoubt,followthewildernessguidelinesprovidedintheirtraining.
• KeepallWFR,CPRandOregon‐authorizedcertificationscurrentandonfilewiththe
DepartmentofPhysicalEducation.
• Takeuniversalprecautionsagainstbloodbornepathogens,makingsuretouseglovesandaCPRmask(whenappropriate)whenexposedtobodilyfluids.Biohazardsmustbedisposedofinanappropriatemanner,taggingtheseitemsandgivingthemtoAssistantDirector.
EmergencyCare
AllReedoutdoortripsthatatanytimearetwohoursormorefrom“definitivecare”shouldhaveatleastoneStudentLeaderorOutdoorSpecialistwithcurrentfirstaid,WFR,Oregon‐authorizedallergicresponse,andCardioPulmonaryResuscitationcertificates.WildernessFirstRespondertrainingandcertificationisgenerallyconsideredindustrystandardforthoseheadingintothewildernesscontext;thisisusuallydefinedbybeingovertwohoursfromclinicorhospitalcare.AllStudentLeadersandOutdoorSpecialistsareencouragedtoplayaproactiveroleinassessingemergencysituationsandprovidingcareforillnessesandinjuries,withthehopeofavoidingasmanymajormedicalsituationsaspossible.However,everyemergencysituationisuniqueandgoodjudgmentiscritical.Whetherandhowtoactinanemergencysituationcannotbedictated.
StudentleadersorOutdoorSpecialistsrespondingasvolunteerlaypersonstoemergencysituationsshouldusepracticesonlywithinthescopeoftheirtraining.Oneshouldalwaysactthoughtfullywiththebestinterestofthepersonhavingtheemergencyinmind.AStudentLeaderorOutdoorSpecialistrenderingvolunteeremergencycareshouldobtainverbal
22
permissionfromthepersonhavingtheemergencyforactionsthattheyintendtotakeincludingthespecificswheneverpossible.MedicalKits
MedicalkitsshouldbewellmaintainedbytheStudentLeadersandOutdoorSpecialists.Thecontentsshouldbecheckedbothbeforeandafteratriptomakesurethattheyarecomplete.Anoteshouldbeleftwiththekitstatingthatitiscomplete;iftherearemissingitemstheyshould
belistedcarefully.ThisnotethenshouldbesignedbyoneoftheStudentLeadersorOutdoorSpecialistsforthetrip.Alistoftheitemsthatwecarryinmedicalkitscanbefoundinthefrontpocketofthekitsthemselves.Medicalkitswithover‐the‐countermedicationssuchas
ibuprofen,acetaminophen,andantihistamines,maybeusedbyleaderswithaWildernessFirstRespondercertificatewhoareheadingintothewildernesscontext,asdefinedbybeingtwohoursormorefromclinicorhospitalcare.Epinephrineforuseintheeventofanaphylaxis
shouldbeavailabletothosewhohaveobtainedtherequiredOregon‐authorizedcertificateforlaypersons.
EMERGENCYSYSTEMS
Ourprogramhashadanexcellenttrackrecordofmanagingriskeffectively,andwewanttokeepthefocusonmanagingandavoidingriskinsteadofrespondingtoaccidents.Westrivetoengageinadventurousactivitieswhereriskislimited.AOutdoorSpecialistorStudentLeadershouldbeabletoarticulatewhyagivenactivitywasundertaken,andwhatmerittheactivityhasinlightofanyinherentrisksthatexist.Ifone’sexperiencedictatesthatthegroupshouldbemoreconservative,thentheStudentLeadershouldgivecredencetohisorherexperience.IfOutdoorSpecialistsandStudentLeaderscontinuetomanageriskwell,theprogramshouldcontinuetothriveandexpand.
Decision‐Making,TakingChargeoftheSituation
Ifanemergencyoccurs,thedesignatedleadershipshouldtakedirectcontrolofthesituation.It
isproventhatincrisissituations,adirecthierarchyhelpsclarifywhatactionsshouldbetaken,eveniftheleadSpecialistchoosestosharetheirdecision‐makingresponsibility.Pleasediscussthishierarchyandyourcomfortwithhandlingemergencieswithyourco‐leadersand,if
appropriate,theAssistantDirectorbeforethetripstarts.
UsingtheCallGuide–RequestingAid
Whenavailable,mobilephonesshouldbecarriedonalloutdoortrips.Thatsaid,therearemany
locationsfromwhichitisdifficulttocall;youcannotassumethatatelephonewillworkaspartofyourriskmanagementplan.Asaleader,youshouldfamiliarizeyourselfwithboththemobile
phoneandthecallguidebeforebeginningthetrip.Confirmthattheareatowhichyouaretravelinghasresourceslistedinthecallguide.Ifnot,itisyourresponsibilitytofindthenearesthospitalandsherifflocationsandnumbersbeforeleavinghome.Ifyoucallintoaskforhelp
fromtheoutdoorprogrammanager,youshouldhaveclearinformationaboutthesituation,completewithaSOAPnoteifapplicable,aswellasyourproposedplanofaction.
23
UnscheduledLossofContact–SearchandRescue
Ifsomeoneisthoughtorknowntobelost,aquicksearchshouldbedoneimmediately.Ifthetrip’sleadersareexperiencedwithgridsearches,andiftheydecidethattheycandoaninitial
setquicklyandsafely,thisoptionmaybeentertained.Afterthreehoursofconductinganysearch,orifotherwiseconsideredappropriatebytheleaders,theAssistantDirectorofPhysicalEducationatReedshouldbecontactedtodetermineifoutsideassistanceisnecessary.Once
outsideagenciesarecontactedtoassistwithasearch,theleadersshouldacceptthattheynolongerhavetotalcontroloverthedirectionandnatureofthesearch.
AccidentandIncidentReports
Allillnesses,injuries,ornearmissesmustbedocumentedonanIncidentReportingFormandsubmittedtotheAssistantDirector.SOAPnotesshouldbecompletedforsignificantaccidentsandtheaccompanyingtreatment.
MedicalProtocolsandStandingOrders
StandingOrder:AbdominalIllnessandInjury
GeneralCommentsGeneralizedabdominalcomplaintsarecommonandleadtochallengingdifferentialdiagnoses.Courseinstructorsmustbediligentintheinterviewandexaminationofthispatientfocusingnotondiagnosis,butonidentifyingcriticalevacuationtriggers.TreatmentforAbdominalIllnessandInjuryIfthepatientdoesnottriggertheevacuationcriteria:1. Allowthepatienttorestinapositionofcomfort.2. Maintainhydrationlevelswithclearfluids.Rehydratewithanelectrolytesolutionifthepatientisdehydrated.3. Blanddiet.TheBRATdietworkswell:Bananas,rice,applesauceandtoast.4. Consideranti‐diarrheals(e.g.ImodiumAD®orLomotil®)and/oranti‐emetics(e.g.Compazine®orPhenergan
®)asnecessarytomaintainhydrationlevels.5. Considerprophylacticanti‐motionsicknessmedication(e.g.meclizine,Dramamine®)toavoidnauseaand
vomiting.6. Ifthepatientisconstipated,aggressivelyhydrate,avoidhighfatfoodsandincreasegrains,vegetablesand
fruit,attempttostimulatebowelmovementswithcaffeineoralternatinghotandcoldliquidsandconsideralaxative(e.g.ExLax®).Iftreatmentisunsuccessfulconsidermanualremovalofthehardenedstools.
7. Monitorthepatientforworseningsignsandsymptoms.Ifthepatientdoesnotshowimprovementin12‐24hoursconsiderevacuation.
8. Ifevacuationispossiblewithinafewhours,givenothingbymouth.EvacuationGuidelinesforAbdominalInjuryorIllnessEvacuateRapidly:
Anypatientwith…
24
Abdominalpainthat:• Persistsgreaterthan12hours,especiallyifconstant.• Islocalized,especiallywithguarding,tenderness,distensionorrigidity.• Occurswithmovement,jarring,orfootstrike.
Orisassociatedwith:
• Signsandsymptomsofshock.• Bloodinthevomit,fecesorurine.• Persistentanorexia,vomitingordiarrheagreaterthan24hours.• Feverabove102°F(39°C).• Signsandsymptomsofpregnancy(historyofsexualactivity,amenorrhea,excessivefatigue,breast
tenderness,polyuriaandnausea).Evacuate:
•Anypatientwithabdominalpainthatdoesnotimprovewithtreatmentin12‐24hours.•Anypatientwithabdominalpainwhoisunabletostayhydrated.ProtocolDecision:ImodiumAD®isanover‐the‐counteranti‐diarrhealmedication.ExLax®isanover‐the‐counterlaxative.MeclizineandDramamine®areover‐thecountermotionsicknessmedications.Theadministrationofover‐thecountermedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.YourMedicalAdvisorshouldadviseyouontheuseanddoseofover‐the‐counteranti‐diarrheal,laxativemedicationandmotionsicknessmedicationsforminors.Ifyourprogramdoesnotcarryanti‐diarrheals,laxativesormotionsicknessmedicationsinthebackcountry,deletethesereferencesfromthetreatmentprotocol.Lomotil®isaprescriptionanti‐diarrhealmedicationandCompazine®andPhenergan®areprescriptionanti‐emeticmedications.Theadministrationofaprescriptionanti‐diarrhealmedicationorprescriptionanti‐emeticmedicationrequiresaphysician.Thesemedicationsmayalsobeself‐administeredbypatientswithaprescriptionforthem.Manualremovalofhardenedstoolsinapatientisaninvasiveprocedure.YourMedicalAdvisorshouldadviseyouinchoosingthisprocedureorincoachingapatienttoattemptremovaloftheirownstools.References:
EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“Gastrointestinal.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐70.Schimelpfenig,Tod.“AbdominalPain.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter18.SpecificProtocolsforWildernessEMSAbdominalPain.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“AbdominalInjuries.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter11.Tilton,Buck.“AbdominalIllnesses.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter29.
25
Wilkerson,JamesA.“AcuteAbdominalPain.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter13.
StandingOrder:AllergicReactionsandAnaphylaxis
GeneralCommentsTheincidenceoftrueanaphylaxisisrare.Mostallergicreactionscanbemanagedwithover‐the‐counteranti‐histamines.TreatmentforAllergicReactionsandAnaphylaxis1. Removetheallergenorthepatientfromtheoffendingenvironment.2. Administeroralantihistamines(e.g.diphenhydramine50mgPOevery4‐6hours).3. Ifpatientshowssignsandsymptomsofanaphylaxis(Swollenface,lipsandtongue;systemichives;respiratory
distress;inabilitytospeakinmorethanoneortwowordclusters;signsandsymptomsofshock)administerepinephrine.3ml/1:1000SQorIM.
4. Ifreactionreoccursortheepinephrineisineffective,continuetoadministerepinephrine.EvacuationGuidelinesforAllergicReactionsandAnaphylaxisEvacuateRapidly:
• Anypatientwhocontinuestoshowrespiratorycompromiseorsignsandsymptomsofshockaftertreatmentwithepinephrineandantihistamines.
Evacuate:
• Anypatientwhohasreceivedepinephrine.Continuetoprovideanti‐histaminesduringevacuation.ProtocolDecision:
Diphenhydramineisanover‐the‐counterantihistaminemedication.Theadministrationofover‐thecountermedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.YourMedicalAdvisorshouldadviseyouontheuseanddoseofover‐the‐counterantihistaminemedicationforminors.Ifyourprogramdoesnotcarryantihistaminesinthebackcountry,deletethissectionfromthetreatmentprotocol.Epinephrineisaprescriptionmedicationusedtotreatsevereallergicresponses.Thismedicationiscommonlypackagedinanauto‐injectorintendedtobeself‐administeredbypatientswithaprescriptionforit.Itisadvisablethatpatientswithaknownhistoryofanaphylaxisbringatleastthreetofourdosesofepinephrinewhentravelinginremoteenvironments.Participantsmayalsobringepinephrineinavialorglassampoulewithanaccompanyingsyringe.Theuseofepinephrinetomanageanaphylaxisiswellestablished,however,thethresholdforadministrationvarieswidely.Somephysiciansadvocateadministeringepinephrineifthepatient'sonlysymptomishives,othersadvocatewaitinguntildefinitivesignsandsymptomsofrespiratoryorcardiovascularcompromiseareevident.Thepossessionandadministrationofepinephrinebylaypeopleandoutdoorprogramsisacomplexissue.Thelawstatesyoucanonlypossessepinephrinethatisprescribedtoyou,and,ingeneral,youcanonlyuseitonyourself.Thereare,however,exceptionstothisstatement.
References:
26
EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“PositionStatement26:TheUseofEpinephrineintheTreatmentofAnaphylaxis.”AmericanAcademyofAllergyAsthma&Immunology.28Dec.2004.<http://www.aaaai.org/media/resources/position_statements/ps26.stm>Schimelpfenig,Tod.“Poisons,Stings,andBites.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter12.SpecificProtocolsforWildernessEMSAllergicReactions.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“AllergicReactionsandAnaphylaxis.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter28.WildernessFieldProtocolsProtocol1Anaphylaxis.2001.WildernessMedicalAssociates.2Dec.2004<http://www.wildmed.com/field_protocols/anaphylaxis_protocol05.01.html#top>Wilkerson,JamesA.“Allergies.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter20.
StandingOrder:BurnsGeneralCommentsLargeburnsareuncommoninthebackcountry,butevensmallburnscanbedebilitating,painfulanddifficulttokeepclean.Smallburnsarerelativelycommonbackcountryinjuries,typicallysecondarytohotwaterspills.TreatmentforBurns1. Ensurethesceneissafe.2. Immediatelyapplycoolcompressesorirrigateburnswithcoolwater.Smallareasofburn(<10%)maybe
soakedincoolwater.Avoidhypothermia.Removeclothingandconstrictingobjects(e.g.jewelry,watches,belts).
3. AssessandmanageAirway,BreathingandCirculationproblems.4. Gaugethedepth,extentandlocationoftheburns.5. Properlydresstheburnswithantibioticointment,burngelorsheets,Silvadene®creamor2ndSkin®covered
looselywithcleandressings.Inextendedcaresituationsdebridedeadskinaroundblistersthathaveself‐drainedandcleanseveraltimesdaily.Donotdrainintactblisters.
6. Painmedicationasneeded(NSAIDsoftenrecommended).7.Aggressivehydration.8.Ifsnowblindnessissuspected,providecoolwaterflushesoftheeyeandcoolcompresses.Restandavoidsun
exposureuntilsymptomsresolve.EvacuationGuidelinesforBurnsEvacuateRapidly:
• Anypatientwithsignsandsymptomsofanairwayburn.• Anypatientwithpartialorfullthicknessburnscoveringmorethan10%TBSA.• Anypatientwithpartialorfullthicknesscircumferentialburns.
Evacuate:
• Anypatientwithafullthicknessburn.• Anypatientwithburnstoaspecialfunctionarea:face,neck,hands,feet,armpits,orgroin.
27
• Anypatientwithaburnthatcannotbemanagedeffectivelyinthebackcountry.ProtocolDecision:Silvadene®creamisaprescriptiontopicalantibioticthatiseffectiveforburns.Theadministrationofanantibioticrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Apatientwithburnsmaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.Oxygenisrecommendedforallpatientswithburnstothefaceandairway.Theadministrationofoxygenrequiresaphysician.
References:“Burns.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐17.EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Forgey,William.“BurnManagement.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter7.Schimelpfenig,Tod.“Burns.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter8.SpecificProtocolsforWildernessEMSWounds.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>Stewart,CharlesE.“Burns.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter2.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“WildernessWoundMangament.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter15.Wilkerson,JamesA.“Burns.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter8.
StandingOrder:CardiacEmergenciesGeneralComments:
Differentialdiagnosisofnon‐traumaticchestpainischallenging.Thereforeanypatientexhibitingsignsandsymptomsofchestpainthatcannotbeattributedtoanon‐cardiacorigin,shouldbemanagedasiftheoriginiscardiac.TreatmentforCardiacEmergencies:1. Reduceanxietyandactivity.Placepatientinapositionofcomfort.Avoidwalkingifpossible.2. Administeroxygen,ifavailable.3. Assistpatientwithadministrationofhisorhernitroglycerin,0.4mgSLsprayortablet,mayberepeatedevery
5minutesforatotalofthreedosesifthesystolicBPremainsabove100mmHgorthepatienthasastrongradialpulse,andthepatienthasnottakenViagra®,Levitra®orCialis®for48hours.
4. Administerone‐adultaspirin(325mg)or3‐4babyaspirin(8lmgeach)every24hours.EvacuationGuidelinesforCardiacEmergencies:
28
EvacuateRapidly:
• Anypatientwithchestpainthatdoesnotrelieveasexpectedwithrestandmedication.Evacuate:
• Anypatientwithnon‐traumaticchestpainthatsubsidedwithrestormedication.• Anypatientwithchestpainthatisnotclearlymusculoskeletal,pulmonaryorgastrointestinal.
ProtocolDecision:Oxygenisrecommendedforallpatientswithcardiacchestpain.Theadministrationofoxygenrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Nitroglycerinisaprescriptionmedicationcommonlycarriedbypatientswithknowncardiachistory.Manypatientsareabletoself‐administerthismedication.Thecontraindicationsvary,specificallytheminimumsystolicbloodpressure.Aspirinisrecommendedforallcardiacchestpaininarangeofdoses.
References:ACLSProviderManual.Dallas,Texas:AmericanHeartAssociation,2002.BLSforHealthcareProviders.Dallas,Texas:AmericanHeartAssociation,2002.“Cardiac/Circulatory.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐1.EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Schimelpfenig,Tod.“RespiratoryandCardiacEmergencies.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter17.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“CardiacEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter23.
StandingOrder:ChestInjuriesGeneralCommentsIsolatedribinjuriesareoftenevacuatedduetopatientdiscomfort.Lunginjuryisaprimaryconcernsecondarytoablowtothechestwall.Specificdiagnosisisdifficult,butsignsandsymptomsofdifficultybreathing,especiallyatrest,shouldtriggerevacuation.Spontaneouspneumothorax,withoutablowtothechest,canoccurandoutdoorleadersshouldbeattentivetosuddencomplaintsofdifficultybreathing.TreatmentforChestInjuries1. Placethepatientinapositionofcomfortorontheinjuredside.2. Stabilizeanyinjuries.Forafracturedribslingandswatheortapetheaffectedside.Foraflailsegmentsplint
withabulkydressing.3. Foranopenchestinjurysealthewoundwithanocclusivedressingsecuredonallfoursides.4. Administeroxygenifavailable.Supportrespirationsifnecessary.5. Painmanagement.6. Periodicallyencouragethepatienttobreathedeeply.
29
7. MonitorforincreasingShortnessofBreath(SOB)atrestanddiminishingbreathsounds.EvacuationGuidelinesforChestInjuriesEvacuateRapidly:•Anypatientwithsignsandsymptomsofseriouschesttraumaorrespiratorydistress.•Anypatientexhibitingincreasingshortnessofbreath,especiallyatrest.•Anypatientwithdiminishedorabnormallungsounds.Evacuate:•Anypatientwithasuspectedriborclaviclefracture.ProtocolDecision:Apatientwithchesttraumamaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforitApatientwithchesttraumamaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
References:EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“ThoracicTrauma.”PHTLSBasicandAdvancedPrehospitalTraumaLifeSupport.St.Louis,Missouri:Mosby,2003.Chapter5.Schimelpfenig,Tod.“ChestInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter3.SpecificProtocolsforWildernessEMSChestInjury.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>Tilton,Buck.“ChestInjuries.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter10.Wilkerson,JamesA.“ChestInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter11.
StandingOrder:CardiopulmonaryResuscitation(CPR)GeneralComments:CPRcanbeaneffectivelifesustaininginterventionintheshort‐term;howeverthereisnoevidencethatprolongedCPRisvaluable.ThestandardsforperformingCPRarewellestablishedbytheAmericanHeartAssociation.ContraindicationstoCPRintheWildernessThereisnoreasontoinitiateCPRifthereis:
• Anysignoflifeinthepatient.• Dangertorescuers.• Dependentlividity.• Rigormortis.• Obviouslethalinjury(e.g.decapitation,frozen).• Awell‐definedDoNotResuscitate(DNR)status.
30
DiscontinuationofCPRintheWilderness
OnceinitiatedCPRshouldbecontinueduntil:
• Resuscitationissuccessful.• Therescuersareexhausted.• Therescuersareplacedindanger.• Thepatientisturnedovertomoredefinitivecare.• Thepatientispronounceddeadbyaqualifiedperson.• Thepatientdoesnotrespondtoprolongedresuscitativeefforts,greaterthan30minutes.
ProtocolDecision:ThestandardsforcontraindicationstoCPRarewelldefinedbytheAmericanHeartAssociation.Inawildernesscontext,severelyhypothermicor“frozen”patientspresentanadditionalcontraindication,unlessdeathcanbeestablishedwithacardiacmonitor.ThestandardsfordiscontinuingCPRarewelldefinedbytheAmericanHeartAssociation.Inawildernesscontext,itisrecommendedbytheWildernessMedicalSocietytoceaseresuscitativeeffortsafter30minutes.YourMedicalAdvisorshouldadviseyouinthisadditionalparameter.Whileavalanches,lightningandsubmersioncreateadditionalmechanismsfortraumaticcardiacarrestinawildernesssetting,theydonotrequireadditionalguidelinesforCPR.Theymaycreatecircumstancesrequiringprolongedrescuebreathingefforts.
References:ACLSProviderManual.Dallas,Texas:AmericanHeartAssociation,2002.Forgey,William.“MyocardialInfarction,AcuteCoronarySyndromes,andCPR.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter2.Goth,PeterandGeorgeGarnett.“NationalAssociationofEMSPhysiciansClinicalGuidelinesforDelayed/ProlongedTransportCardiorespiratoryArrest.”PrehospitalandDisasterMedicineVol.6No.3July‐Sept.1991:335‐339.SpecificProtocolsforWildernessEMSCardioPulmonaryResuscitation.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>Tilton,Buck.“CardiopulmonaryResuscitation.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter5.WildernessFieldProtocolsProtocol3CardiopulmonaryResuscitation(CPR).2001.WildernessMedicalAssociates.2Dec.2004<http://www.wildmed.com/field_protocols/cpr_protocol05.01.html#top>
StandingOrder:DentalEmergenciesGeneralCommentsDentalemergenciescanberemarkablypainfulanddebilitatingandunfortunatelycommononwildernesstrips.Therearesomesimpletoolsandtreatmentguidelinesthatmayallowaparticipanttofinishabackcountryexpeditioninrelativecomfort.TreatmentforDentalEmergencies
31
1. Cleanandrinsethemouth.Brushandflosstheteethifthepatientcantolerateit.2. Ifacrownorfillingislostorthetoothbreaks,coverthe“hole”withCavit®.Cavit®mayalsobeusedto“glue”
thecrownorfillinginplace.IfyoudonothaveCavit®trysugarlessgumorwax.3. Ifthetoothbreaksandthepulpisexposed,applyasmallpieceofcrushedaspirinto“cauterize”thepulp.4. Ifthetoothisknockedoutofthesocket,irrigatethetoothwithdisinfectedwaterandattempttoreplaceitin
thesocket.Iftoothcannotbereplaced,wrapinsterilegauzeandhavepatientcarrythetoothbetweentheircheekandgum.FacilitybasedprogramsmightconsiderSave‐a‐tooth®,aspecialfluidandcontainerthatmayextendthelifeofabrokentooth.
4. Applytopicaloilofcloveforpain.5. Painmedicationasneeded.6. Ifaperiodontalabscessissuspected,cleanandflossteeth,garglewithwarmsaltywater3‐4timesdaily,and
administerantibioticsandpainmedication.EvacuationGuidelinesforDentalEmergencies
Evacuate:•Anypatientwithatoothknockedoutofthesocket.•Anypatientwithabrokentoothwithexposedpulp.•Anypatientwithaperiodontalabscess.ProtocolDecision:Apatientwithdentalproblemsmaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Apatientwithdentalproblemsmaybenefitfromover‐the‐counterpainmedication,includingoilofclove.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.Theuseofaspirintocauterizetoothpulpisaggressive,butmaysignificantlyreducethepatient’spainandwillingnesstostayfedandhydratedAntibioticsarerecommendedforaperiodontalabscess.Theadministrationofanantibioticrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.
References:Auerbach,PaulS.“WildernessDentistryandManagementofFacialEmergencies.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter26.“Dentistry.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.5‐9.Schimelpfenig,Tod.“DentalEmergencies.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter23.SpecificProtocolsforWildernessEMSDentalInjury.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“CommonSimpleMedicalProblems.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter31.
32
StandingOrder:DiabeticEmergencies
GeneralComments
Well‐controlleddiabeticsperformwellinbackcountrysettings.Outdoorprogramsshoulddevelopascreeningprogramforeligibility;thiswillvaryonprogramtypeandlocation.Programsshouldalsohaveaplanformedicationstorageandadministrationandthediabeticparticipantshouldbringadequatesupplies(glucometer,sparebatteries,duplicatemedicationssuchasinsulin,glucagonhydrochloride,andglucosepasteortabs,syringesandketonestrips)andanestablishedsickdayplan.TreatmentforDiabeticEmergencies1. Checkbloodsugarusingthepatient’sglucometer.2. Ifhypoglycemiaissuspected,givetheawakepatientsugar(glutosepasteortabs,sweetliquids,table
sugarinwater)untiltheyregainanadequatelevelofresponsiveness.Ifthepatientisnotawake,placethepatientontheirsideandrubsugarintotheirgumsrepeatedlyuntiltheyregainanadequatelevelofresponsiveness.
3. Iftheunresponsive,hypoglycemicpatientdoesnotregainresponsiveness,administerglucagonhydrochlorideIM.
4. Ifhyperglycemiaissuspected,checkketonelevelswithketoneurinestrips.Assistthepatienttohydrateandadjustinsulindoseinaccordancewithhisorhersickdayplan.Ifthehyperglycemicpatientisunresponsive,donotadministerinsulin.
5. Checkbloodsugarfrequently.Havethepatientcontinuetoeatand/ormedicateuntilanadequatelevel(80‐120mg/dl)isobtained.
6. Ifunknownwhetherapatientissufferingfromhypoglycemiaorhyperglycemia,givesugartothepatient.EvacuationGuidelinesforDiabeticEmergenciesEvacuateRapidly:
•Anypatientwhoisunresponsiveduetoadiabeticemergency.Evacuate:
•Anydiabeticpatientwhoisunabletokeephisorhersugarlevelsundercontrolinabackcountrysetting.
•Anydiabeticpatientwhoexperiences:severaldaysofillness,hasvomitingordiarrheaformorethan6hours,hasmoderatetolargeamountsofketonesintheirurine,cannotmoderatetheirbloodsugarreadingswithadditionalinsulinorfeelsalossofcontrolofbloodsugarlevels.ProtocolDecision:Supportingadiabeticduringanemergencymayrequirestafftoadministerglucagoninjectionsandassessbloodsugarandketonelevels.YourdiabeticparticipantandyourMedicalAdvisorshouldadviseyouintheseprocedures.
References:
33
EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“Endocrine.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐27.Schimelpfenig,Tod.“Diabetes,SeizuresandUnresponsiveStates.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter9.SpecificProtocolsforWildernessEMSDiabetes.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“DiabeticEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter26.
StandingOrder:Dislocations
GeneralCommentsDislocationsoftheshoulder,digitandpatellaaremostcommon.Patientsmayhaveahistoryofchronicdislocations.Themechanismofinjurymaybedirectorindirect,andthedislocationmaybeassociatedwithotherinjuriessuchasfractures.Ingeneral,thedifficultyofreductionandtheamountoflong‐termcomplicationsbothincreasewithdelayinreductionattempts.TreatmentforDislocations1. Assesscirculation,sensationandmotion(CSM).2. ConsiderattemptingtoreducedislocationsoftheshoulderifevacuationtimeexceedsonehourorCSMhas
beencompromisedbythedislocation.Treatallotherdislocationsasunusablemusculoskeletalinjuries.3. Reductionisusuallyachievedbyapplyingslow,steadyandgentletraction‐in‐line(TIL).Relaxationiskey.Slow
downordiscontinueyourattemptifpainincreasessignificantlyoryoumeetresistance.4.Inunabletoreduceaftermultipleattempts,splintinthepositionfound.5. Afterreduction,Rest,Ice,CompressionandElevation(RICE)therapy,painmedicationandimmobilizationas
needed.6. Monitorcirculation,sensationandmotion(CSM)beforeandafterreductionand/orimmobilization.7. Passiverangeofmotion(ROM)2‐3timesperday,ortopatienttolerance.EvacuationGuidelinesforDislocationsEvacuateRapidly:•Anypatientwithanunreduceddislocation.•AnypatientwithalteredCSMafterreduction.Evacuate:•Anypatientwithafirsttimedislocation.•AnypatientwithalteredCSMpriortoreduction.•Anypatientunabletousethereducedjoint.•Anypatientwithpersistentpain.ProtocolDecision:Apatientwithadislocationmaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit

34
Apatientwithadislocationmaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.References:Auerbach,PaulS.“WildernessOrthopaedics.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter24.Forgey,William.“OrthopedicInjuries.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter8.Goth,PeterandGeorgeGarnett.“NationalAssociationofEMSPhysiciansClinicalGuidelinesforDelayed/ProlongedTransportDislocations.”PrehospitalandDisasterMedicineVol.8No.1Jan.‐Mar.1993:77‐80.Schimelpfenig,Tod.“FracturesandDislocations.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter5.SpecificProtocolsforWildernessEMSDislocations.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>Tilton,Buck.“Dislocations.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter13.“JointDislocations.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐64.
StandingOrder:Eyes,EarsandNoseTreatmentforEyes,EarsandNose:
1. Blackeyescanbetreatedwithcoolcompressesandpainmedication.2. Objectsintheeyeshouldbeflushedoutwithdisinfectedwaterordabbedoutwithacleancloth.Ifthe
objectisembeddedintheeyeitshouldbestabilizedandbotheyesbandaged.3. Objectsintheearmaybedrownedwithoil,wateroralcohol,ifneeded,andthenflushedoutwithan
irrigationsyringeorgraspedwithtweezersifvisible.4. Outerearinfectioncanbetreatedbykeepingtheeardryandflushingtheearwithdilutesolutionof
alcoholorvinegardaily.5. Bloodynosescanbemanagedbypinchingthenosejustbelowcartilageandleaningforward.Ifunableto
controlbleeding,considerpackingthenosewithgauze.EvacuationGuidelinesforEyes,EarsandNose:EvacuateRapidly:
• Anypatientwithanuncontrollablenosebleed.
Evacuate:• Anypatientwithpersistentvisionchanges,extraordinaryandpersistentsensitivitytolight,ordischargeof
fluidotherthantears,oranimbeddedobjectintheeye.• Anypatientwithanearinfectionnotrespondingtotreatment.
References:Auerbach,PaulS.“TheEyeintheWilderness.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter25.
35
Auerbach,PaulS.“WildernessDentistryandManagementofFacialInjuries.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter26.Forgey,William.“EyePathology.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter9.“GeneralSymptoms.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐1.Schimelpfenig,Tod.“CommonNon‐UrgentMedicalProblems.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter24.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“CommonSimpleMedicalProblems.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter31.Wilkerson,JamesA.“Eye,EarNose,andThroatDisorders.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter17.
StandingOrder:FemaleGenderMedicalConcerns
GeneralCommentsMostfemalegendermedicalconcernsaremanageableinabackcountrysetting.Itisimportanttocreateanenvironmentthatencouragesparticipantstodiscusstheseconcernswithtripleaders.Thedecisiontoallowpregnantgroupmembersonthetripshouldbeestablishedaheadoftime.TreatmentforFemaleGenderMedicalConcerns1. Bothdysmenorrheaandmittleschmerzcanbemanagedwithanalgesics,mildexerciseandheatpacks.2. Ifvaginitisissuspected,washthevaginalareathoroughlyandairdry.Considereitheranover‐the‐counter
anti‐fungal(e.g.Monistat®)oraprescriptionanti‐fungal(e.g.Diflucan®).3. Ifaurinarytractinfectionissuspected,restthepatient,provideaggressivehydration,aurinarytractanalgesic
(e.g.Pyridium®)andanantibiotic.4. Ifanectopicpregnancyissuspected,treatforshock.EvacuationGuidelinesforFemaleGenderMedicalConcernsEvacuateRapidly:•Anypatientwithsignsandsymptomsofurinarytractinfectionwhodevelopstendernessoverthekidneys.•Anypatientwithasuspectedectopicpregnancy(lowabdominal/pelvicpain,abnormalvaginalbleeding,signsandsymptomsofshock.)Evacuate:•Anypatientsuspectedofbeingpregnantorwithpregnancycomplications.•Anypatientwithvaginitisoraurinarytractinfectionthatdoesnotrespondtotreatment.ProtocolDecisionAnti‐fungalmedication(e.g.Monistat®)isrecommendedfortreatingvaginitisandaurinarytractanalgesic(e.g.Pyridium®)isrecommendedformanagingaurinarytractinfection.Theadministrationofover‐thecounteranti‐fungalandpainmedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
36
Prescriptionanti‐fungalmedicationandantibioticsarerecommendedfortreatingvaginitisandurinarytractinfections.Theadministrationofprescriptionanti‐fungalmedication(e.g.Diflucan®)andantibioticsrequiresaphysician.Thesemedicationsmayalsobeself‐administeredbypatientswithaprescriptionforthem.
References:EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“Genitourinary.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐87.“GynecologicalProblems.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐37.Schimelpfenig,Tod.“Gender‐SpecificMedicalConcerns.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter20.SpecificProtocolsforWildernessEMSUrinaryTractInfection.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“Gender‐SpecificEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter32.Wilkerson,JamesA.“GenitourinaryDisorders.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter18.
StandingOrder:Flu‐likeIllness
GeneralComments:Viral“flu‐like”illnessarecommononwildernessexpeditions.Theymayincludegastrointestinalsymptoms(nausea,vomitinganddiarrhea)orrespiratorysymptoms(cough,congestion,runnynose,sorethroat).Viralillnessesalsocauseaviralheadache,malaise,fatigue,low‐gradefever,muscleaches,bodyaches,etc.Fluisamedicallydistinctillnessfromthe“commoncold”.Itusuallyhasamoreabruptonsetthanacoldwithastrongeroverallimpactonthepatient.Theillnesscanpersistforseveralweeks.Managementisfocusedonsymptomaticreliefforthepatient.TreatmentforFlu‐likeIllness:
1.Generalmanagementforflu‐likeillnessissymptomatictreatment.2.Restandhydration.3.Handwashingandhygiene.4.Acetaminophen,aspirinorNSAIDsforfever,sorethroatheadacheandmuscleaches.5.Decongestants(e.g.pseudophedrine)forcongestion.6.Anti‐coughmedicationsasneeded(e.g.Robitussin®orhydrocodone).7.Blanddietforgastrointestinaldistress.
37
EvacuationGuidelinesforFlu‐likeIllness:EvacuateRapidly:Anypatientwithsignsandsymptomsofflu‐likeillnesswhodevelops:
• Stiffneck,severeheadache,difficultbreathingorwheezing.• Gastroenteritiswithpersistentorworseningabdominalpainover24hours,spikingfever,bloodydiarrhea
ordehydration.• Aninabilitytotolerateanyoralfluidsmorethan48hours,especiallyifaccompaniedbydiarrheavolume
losses,feverorvomiting.• Aheadachethatdoesnotrespondtotreatment,suddensevereheadaches,oraheadacheassociatedwith
alteredmentalstatus.
Evacuate:Anypatientwithsignsandsymptomsofflu‐likeillnesswhodevelops:
• Feverpersistingmorethan48hoursorishigh(>102°F/39°C).• Signsorsymptomsofpneumonia.Thisisusuallyassociatedwithincreasingshortnessofbreath,
decreasingexercisetolerance,worseningmalaiseandweaknesswithapredominanceofcough.• Anisolatedsorethroatwithfeverandaredthroatwithwhitepatches.• Asorethroatinconjunctionwithinabilitytoswallowwaterandmaintainadequatehydration.
ProtocolDecision:Arangeofover‐the‐countermedicationsincludingdecongestants,coughsuppressants,painmedicationsandfever‐reducingmedicationsmayhelppatientswithflu‐likeillness.Theadministrationofover‐thecounterdecongestants,coughsuppressants,painmedicationsandfever‐reducingmedicationstominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
References:“GeneralSymptoms.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐1.“Respiratory.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐10.Schimelpfenig,Tod.“CommonNon‐UrgentMedicalProblems.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter24.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“CommonSimpleMedicalProblems.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter31.Wilkerson,JamesA.“Eye,EarNose,andThroatDisorders.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter17.
38
StandingOrder:HeadInjuriesGeneralCommentsDecidingwhethertoevacuateapatientwhosustainsablowtotheheadandexhibitsonlyminorsymptomscanbechallengingforoutdoorleaders.Providingdetailedguidancecanbehelpful.TreatmentforMildHeadInjuriesConservativetreatmentwithcloseobservationfor24hoursinthefieldcanbedoneifthepatientwasawakeandalert(A+Ox3or4)orwasonlymomentarilydazedorstunned,butrecoveredappropriatelyandthepatientremainsawakewithoutnegativechangeinmentalstatusandhasonlytransientnauseaorvomiting.1.Monitorthepatientfordevelopingsignsofseriousheadinjury.2.Letthepatientrest,butwakethemupeveryfewhourstomonitorLOR.TreatmentforSeriousHeadInjuries1. Iftheinjuryisopen,usediffusepressurewithabulkydressingtocontrolbleeding.2. ManageAirway,BreathingandCirculation.Considerpositioningthepatientontheirside.3. Administeroxygenifavailable.4. Immobilizethespineandelevatetheheadatapproximately6‐8”(15‐20cm).EvacuationGuidelinesforHeadInjuriesEvacuateRapidly:•AnypatientwhoisnotA+Ox3or4.•Anypatientwithdistinctchangesinmentalstatus(disoriented,irritable,combative).•Anypatientwithpersistentvomiting,lethargy,excessivesleepiness,ataxia(extremeuncoordination),seizures,worseningheadacheorvisiondisturbances.
•Anypatientwithsignsofaskullfracture.Evacuate:•Anypatientwithalossofresponsiveness,whorecoverstoA+Ox3or4.•Anypatientwhosesignsandsymptoms(headache,nausea/vomiting,irritabilityorothersignsandsymptomsofmildheadinjury)donotshowimprovementafter24hours.
Observefor24Hours:•AnypatientwhowasassessedasA+Ox3or4.•Anypatientwithsignsandsymptomsofmildheadinjury.ProtocolDecisionHavingalossofresponsivenessprotocolisessentialforanorganization.Oxygenisrecommendedforallseriousheadinjuries.Theadministrationofoxygenrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.
References:EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Forgey,William.“TraumaticBrainInjury.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter4.
39
McCrory,PaulR.andKarenM.Johnston.“AcuteClinicalSymptomsofConcussionAssessingPrognosticSignificance.”ThePhysicianandSportsmedicineVol.30No.8August2002.“HeadTrauma.”PHTLSBasicandAdvancedPrehospitalTraumaLifeSupport.St.Louis,Missouri:Mosby,2003.Chapter8.Schimelpfenig,Tod.“BrainandSpinalCordInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter4.Tilton,Buck.“HeadInjuries.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter9.Wilkerson,JamesA.“HeadandNeckInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter16.
StandingOrder:Hypothermia
GeneralCommentsMostmild‐moderatelyhypothermicpatientsaremanagedeffectivelyinthefieldanddonotrequireevacuation.TreatmentforHypothermia1. Changetheenvironmentandfindshelter.Replacewetclothingwithdryclothingandaddwindand
waterprooflayers.Treatgently.2. Addinsulationunderandaroundthepatient.Considerahypothermiawrapformoderatelyandseverely
hypothermicpatients.Addexternalheatsourcesandwell‐insulatedheatpacksathands,feet,armpits,groin,andneck.
3. Encourageexerciseifthepatientisableandallowshiveringinadry,insulatedenvironment.4. Givewarm,sweet,non‐caffeinated,non‐alcoholicliquidsandencouragethepatienttoeatameal,iftheyare
able.5. Foraseverelyhypothermicpatient,administerwarm,humidifiedoxygen,ifavailable.Assistventilationsfor5‐
15minutespriortomovement.6. Avoidchestcompressionsifthereareanysignsoflifeorthepatientisrigidfromthecold.Performrescue
breathingduringevacuation.EvacuationGuidelinesforHypothermiaEvacuateRapidly:•Anypatientwithseverehypothermia.ProtocolDecision:
Thedecisiontowithholdchestcompressionsisawildernessprotocol.YourMedicalAdvisorshouldadviseyouonthedecisiontowithholdchestcompressions.
References:Auerbach,PaulS.“AccidentalHypothermia.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter5.Forgey,William.“Hypothermia.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter11.Giesbrecht,GordonG.“PrehospitalTreatmentofHypothermia.”WildernessandEnvironmentalMedicine122001:24‐31.Schimelpfenig,Tod.“ColdInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter9.StateofAlaskaColdInjuriesandColdWaterNearDrowningGuidelines.Revision01/96.HypothermiaPrevention,RecognitionandTreatment.
40
Articles,ProtocolsandResearchonLife‐savingskills.27Dec.2004.<http://www.hypothermia.org/protocol.htm>Stewart,CharlesE.“GeneralizedHypothermia.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter4.Tilton,Buck.“Cold‐InducedEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter16.Wilkerson,JamesA.“ColdInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter23.
StandingOrder:LightningGeneralCommentsLightningstrikescancauseavarietyofinjuriesincludingdeath.Thebestdefenseisastrongpreventionplanspecificforyourgeographicareaandgroupprofile.TreatmentforLightningInjuries1. Scenesafety:Lightningwillstriketwiceinthesamespot.2.AggressiveBasicLifeSupport:Rescuersshouldbepreparedtoprovideprolongedrescuebreathing.3. Thoroughpatientexamandtreatmentofanyinjuriesfound.4. Monitorcloselyforcardiovascular,respiratoryandneurologicalcollapse.EvacuationGuidelinesforLightningInjuriesEvacuateRapidly:•Anypatientshowingsignsofcardiovascular,respiratoryorneurologicalcompromise.Evacuate:•Anypatientstruckbylightningeveniftheyappearuninjured.
References:Auerbach,PaulS.“LightningInjuries.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter3.Forgey,William.“LightningInjuries.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter14.Gookin,John.“NOLSBackcountryLightningSafetyGuidelines.”Lander,Wyoming:TheNationalOutdoorLeadershipSchool,2000.Schimelpfenig,Tod.“LightningInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter13.Stewart,CharlesE.“ElectricalInjuries.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter9.Tilton,Buck.“Lightning.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter20.
StandingOrder:LocalColdInjuriesGeneralCommentsItispossibletoseebothfreezingandnon‐freezinglocalcoldinjuriesinthewildernesssetting.Bothcancauseinjuriesrangingfromminorirritationtosignificanttissuelossandpermanentdisability.TreatmentforLocalColdInjuries1.Ifnotfrozen:Warmtheinjurywithskin‐to‐skincontact,donotmassageoruseradiantheat.2.Iffrozen:Ifpossible,warmtheinjuryinacirculatingwarmwaterbathat99‐102°F(37‐39°C),otherwiseuseskin‐
to‐skincontact.Donotmassageoruseradiantheat.3.Protectblistersanddamagedtissue,avoidconstriction.Protectfromre‐freezing.Elevate.
41
4.Painmedicationasneeded.EvacuationGuidelinesforLocalColdInjuriesEvacuateRapidly:•Anypatientwithfullthicknessfrostbite.Evacuate:•Anypatientwithmorethanafew,small,isolatedclearfluidfilledblistersformedafterwarmingalocalcoldinjury.•Anypatientunabletousetheinjuredarea.•Anypatientunabletoprotecttheareafromcontinuedexposuretoacoldwetenvironmentorfromre‐freezing.•Anypatientwhosepaincannotbemanagedinthefield.ProtocolDecision:
Apatientwithlocalcoldinjurymaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Apatientwithlocalcoldinjurymaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
References:Auerbach,PaulS.“NonfreezingColdInjuries.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter7.Auerbach,PaulS.“Frostbite.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter8.Forgey,William.“Frostbite/ImmersionFoot.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter12.Schimelpfenig,Tod.“ColdInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter9.StateofAlaskaColdInjuriesandColdWaterNearDrowningGuidelines.Revision01/96.HypothermiaPrevention,RecognitionandTreatment.Articles,ProtocolsandResearchonLife‐savingskills.27Dec.2004.<http://www.hypothermia.org/protocol.htm>Stewart,CharlesE.“FrostbiteandColdInjuries.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter3.Tilton,Buck.“Cold‐InducedEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter16.Wilkerson,JamesA.“ColdInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter23.Wilkerson,JamesA.,CameronC.BangsandJohnS.Hayward.“Frostbite.”HypothermiaFrostbiteandOtherColdInjuries.Seattle,Washington:TheMountaineers,1986.Chapter7.Wilkerson,JamesA.,CameronC.BangsandJohnS.Hayward.“OtherLocalizedColdInjuries.”HypothermiaFrostbiteandOtherColdInjuries.Seattle,Washington:TheMountaineers,1986.Chapter8.
StandingOrder:MaleGenderIllnessandInjury
GeneralCommentsItcanbechallengingtodifferentiatebetweentraumaticandinfectiousproblemswiththemalegenitalia.Sincedelayincarecanresultinthelossofatesticle,treatmentshoulderrorontheconservativeside.
42
MaleGenderIllnessandInjury
1. Painmanagementasneeded,NSAIDsoftenrecommended.2. Coolcompresses.3. Elevation/supportofthetesticles.4. Iftesticulartorsionissuspectedconsiderselforassistedreductionoftheaffectedtesticle.5. Ifepididymitisissuspectedconsiderantibiotics.6. Ifinguinalherniaissuspected,attemptreduction.
EvacuationGuidelinesforMaleGenderIllnessandInjuryEvacuateRapidly:•Anypatientwithsuspectedtesticulartorsionthatdoesnotreduce.•Anypatientwithtesticularpainofunknownorigin.Evacuate:•Anypatientwithasuspectedepididymitis.•Anypatientwithaninguinalherniathatdoesnotreduceorreappearsafterreduction.ProtocolDecision:
Apatientwithinjuryorillnesstothemalegenitaliamaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtained
throughpre‐tripauthorizationformsoronacasebycasebasis.
Antibioticsarerecommendedforepididymitis.Theadministrationofanantibioticrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Ifyourprogramdoesnotcarryantibioticsinthebackcountry,deletethissectionfromthetreatmentprotocol.References:EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“Genitourinary.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐87.“MaleGenitalProblems.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.3‐77.Schimelpfenig,Tod.“Gender‐SpecificMedicalConcerns.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter20.SpecificProtocolsforWildernessEMSTesticularPain.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.
StandingOrder:MusculoskeletalInjuriesGeneralCommentsTreatmentandevacuationdecisionsofmusculoskeletalinjuriesarebasedonthepatient’sabilitytousetheinjuredarea.Useableinjuriesaresupportedandcanbekeptinthefieldorevacuatednon‐urgently.Un‐usableinjuriesareimmobilizedandevacuated.TreatmentforStrains,Sprains,TendonitisandMinorFractures
1. Assessinjuryforstabilityandusability.2. Assesscirculation,sensationandmotion(CSM).
43
RICETherapy• Rest:Getthepressureoffoftheinjurysite.• Ice:Cooltheareafor20minutes.• Compression:ElasticWrap,distaltoproximal.• Elevation:Abovethepatient’sheart.
1. Painmedicationasneeded.2. Allowtheinjurysitetopassivelywarm.3. Assessagainforusability.4. Supportusableinjurieswithtapeorotheradjuncts.5. ContinueRICETherapyasneeded.
***1. TreatmentforObviousFractures,OpenFracturesandUnusableInjuries2. Assessinjury.Checkcirculation,sensationandmotion(CSM).3. Iffractureisopen,thoroughlyirrigateandcleanwoundpriortomanipulatinginjury.4. Ifnecessary,usegentletraction‐in‐line(TIL)toestablishnormalanatomicalposition.Slowdownor
discontinueyourattemptifpainincreasessignificantlyoryoumeetresistance.Iftheboneendsdonotreduce,protectfromfreezingordrying.
5. Dresswounds.6. Splintinapositionoffunctionwithawell‐paddedandrigidsplint.7. Tractionsplintmid‐shaftfemoralfractures.8. RICEtherapy.Painmedicationasneeded.9. MonitorCSMbeforeandafterTILandsplinting.10. Monitorwoundsiteforinfectionandconsiderantibiotictherapyforopenfractures.
EvacuationGuidelinesforAthleticInjuriesandFracturesEvacuateRapidly:
• Anypatientwithanopenfracture.• AnypatientwithalteredCSM.
Evacuate:
• Anypatientwithanunusablemusculoskeletalinjury.
ProtocolDecision:
Thereductionofangulatedfracturesiswithinthescopeofurbanpre‐hospitalcareproviders,especiallyifthepatienthasalteredCSM.Thoughthisisnotawildernessprotocol,itispotentiallyviewedasaggressive.Apatientwithamusculoskeletalinjurymaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.
Apatientwithmusculoskeletalinjurymaybenefitfromover‐the‐counterpainmedication.Theadministrationof
over‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
Antibioticsarerecommendedforopenfractures.Theadministrationofanantibioticrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.References:
44
Auerbach,PaulS.“WildernessOrthopaedics.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter24.EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Forgey,William.“OrthopedicInjuries.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter8.“MusculoskeletalTrauma.”PHTLSBasicandAdvancedPrehospitalTraumaLifeSupport.St.Louis,Missouri:Mosby,2003.Chapter10.Schimelpfenig,Tod.“AthleticInjuries.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter6.Schimelpfenig,Tod.“FracturesandDislocations.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter5.Tilton,Buck.“AthleticInjuries.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter14.Tilton,Buck.“Fractures.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter12.
StandingOrder:NeurologicalEmergencies
GeneralCommentsStrokesarerareeventsinabackcountrysetting,butwhentheydooccurrequireimmediateevacuation.Seizuresareamorecommonoccurrence,fortunatelytheyarerarelylifethreatening.TreatmentforNeurologicalEmergencies
1. Forasuspectedstrokeortransientischemicattack(TIA),provideemotionalreassurance.Placethepatientinapositionofcomfortunlessunresponsive,thenplaceinstablesidepositionwiththeaffectedairwaysidedowntoprotecttheairway.Administeroxygen,ifavailable.Documentpreciselythetimeofonsetofsignsandsymptoms
2. Forapatientwithaseizure,protectfromharm,butdonotrestrain.Donotplacebitestickoranyotherobjectinmouth.Placethepatientonsidetomaintainopenairwayduringpost‐seizurerecoveryphase.Performacompletepatientassessmenttocheckforinjuries.Protectthepatient’sdignity.Administeroxygen,ifavailable.
3. Foranunresponsivepatientofunknownorigin,stabilizethespine,managetheairway,considerpositioningthepatientontheirsideandsearchforcluestothepatient’sunresponsivestate.Consideradministeringoralsugar.
EvacuationGuidelinesforNeurologicalEmergenciesEvacuateRapidly:
• AnypatientwithsignsandsymptomsofastrokeorTIA.• Anypatientwithmultipleseizuresinashorttimeperiod.• Anypatientwithpersistentunresponsivenessoralteredmentalstatus.
Evacuate:
• Anypatientwithafirsttimeseizure.• Anypatientwithaseizurethatoccurredinspiteofmedication(breakthroughseizure).• Anypatientwithanisolatedseizureofunknownorigin.
References:ACLSProviderManual.Dallas,Texas:AmericanHeartAssociation,2002.
45
BLSforHealthcareProviders.Dallas,Texas:AmericanHeartAssociation,2002.EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Schimelpfenig,Tod.“Diabetes,SeizuresandUnresponsiveStates.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter19.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“NeurologicalEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter25.
StandingOrder:PoisonsGeneralCommentsWhendealingwithpossiblepoisoninggatherdetailedinformationaboutwhatwasingested,howmuch,when,bodysizeandage,whatisinhisorherstomachandwasitintentional.CarbonmonoxidepoisoningfromstovesandlanternsinenclosedspacesandmotorvehicleexhaustiscommoninoutdoorrecreationaccordingtotheCentersforDiseaseControlandPrevention.Poisoningisdifficulttomanageinthefieldandisbestdealtwiththroughprevention.TreatmentforPoisons
1. Callthepoisoncontrolcenter(1‐800‐222‐1222),ifpossible.2. Ifpoisonisingestedandisnon‐corrosive,non‐petroleumbasedandthepatientisfullyresponsive:Induce
vomitingmanually.3. Ifpoisonisinhaled,removepatientfromexposure.Administeroxygen,ifavailable.Assistventilationsif
necessary.4. Ifpoisonisabsorbed,takeuniversalprecautionsandremovecontaminatedclothing.Brushdrypoison
off,flushareawithwaterandwashwithsoap.EvacuationGuidelinesforPoisoningEvacuateRapidly:
• Anypoisonedpatientwhohasanalteredlevelofresponsivenessorshowssignsofrespiratorydistress.Evacuate:
• Anypatientwhohasingestedquantitiesofapotentiallyharmfulsubstance.ContacttheAmericanAssociationofPoisonControlCentersat1‐800‐222‐1222foradvice.
ProtocolDecision:Oxygenisrecommendedforallinhaledpoisonpatients.Theadministrationofoxygenrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Ifyourprogramdoesnotcarryoxygeninthebackcountry,deletethissectionfromthetreatmentprotocol.References:Auerbach,PaulS.“ToxicPlantIngestions.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter58.
46
EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Forgey,William.“BotanicalEncounters.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter17.Keyes,LindaE.,RobertS.Hamilton,andJohnS.Rose.“CarbonMonoxideExposurefromCookinginSnowCavesatHighAltitude.”WildernessandEnvironmentalMedicine,12,2001:208‐212.Schimelpfenig,Tod.“Poisons,Stings,andBites.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter12.Stewart,CharlesE.“PlantsThatPoison.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter8.TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“PoisoningEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter27.
StandingOrder:RespiratoryEmergenciesGeneralComments:Themostcommonlyreportedrespiratoryproblemsareupperrespiratoryinfectionsassociatedwithcoldsorflu‐likeillness.Otherrespiratoryemergenciesrangefromminorepisodesofhyperventilationandasthmatomoreseriousinfections,embolismsandsevereasthma.Agoodpatienthistorywillhelpyoudeterminethelikelycauseandcreatethemostappropriatemanagementplan.Cold,altitude,dehydrationandfatiguecanallbecomplicatingfactors.TreatmentforRespiratoryEmergencies:
1. Forsuspectedhyperventilation,calmthepatient,bedirectbutreassuring.Assistthepatienttoslowhisorherbreathing.Oxygenisnotindicated.
2. Forsuspectedpulmonaryembolism,administeroxygen,ifavailable.Placethepatientinapositionofcomfortandevacuaterapidly.
3. ForasuspectedUpperRespiratoryInfection(URI)allowthepatienttorestandhydrate.Considerover‐the‐counterdecongestantsandanalgesics.
4. Forsuspectedpneumonia,encouragepatienttocoughandbreathedeeply.Ensurethepatientstayshydrated.Givefever‐reducingmedications.Administeroxygen,ifavailable.Ifevacuationislengthy,administeroralantibiotics.
5. Forasuspectedasthmaattackhelpcalmthepatientandchangetheenvironment.Assistthepatient,ifnecessary,withhisorherbronchodilatorsorAlbuterolinhaler(2puffsevery5minutesupto12puffs)untilattackabates.Continuedmaintenancetreatmentisusually2puffsevery4hoursandasneeded.Encouragepursedlipbreathing.Administeroxygen,ifavailable.Providehydrationandrest.Apatientwithsevereasthmaunresponsivetotheirnormalmedicationsmayneedtreatmentwithsteroidsandepinephrine.
EvacuationGuidelinesforRespiratoryEmergencies:EvacuateRapidly:
•Anypatientwithsuspectedpulmonaryembolus.•Anypatientwithsignsorsymptomsofasevereasthmaattack.
Evacuate:
•Anypatientwithsuspectedpneumonia.
47
•Anypatientsufferingfromasthmawhoisunresponsivetomedicationorwithincreasingfrequencyand/ordurationofattacks.
ProtocolDecision:
Oxygenisrecommendedforallseriousrespiratoryemergencies.Theadministrationofoxygenrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Ifyourprogramdoesnotcarryoxygeninthebackcountry,deletethissectionfromthetreatmentprotocol.Arangeofover‐the‐countermedicationsincludingdecongestants,painmedicationsandfever‐reducingmedicationsmayhelppatientswithrespiratoryemergencies.Theadministrationofover‐thecounterdecongestants,painmedicationsandfever‐reducingmedicationstominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.Antibioticsarerecommendedforanypatientwithpneumonia.Theadministrationofanantibioticrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Albuterolisaprescriptionmedicationcommonlycarriedbypatientswithaknownasthmahistory.Manypatientsareabletoself‐administerthismedication.Peoplewithmildtomoderatecontrolledasthmaparticipateinoutdoorprograms.Theuseofepinephrinetomanagesevereasthmaiscontroversialandisnotlistedbythemanufacturerasan
indicationforuseoftheauto‐injectordevices.
References:Busse,WilliamW.andRobertF.Lemanske.Jr.“Asthma.”NewEnglandJournalofMedicineVol.344,No.5February1,2001:350‐362.EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule4Medical/BehavioralEmergenciesandObstetrics/Gynecology.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>“Respiratory.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐10.Schimelpfenig,Tod.“RespiratoryandCardiacEmergencies.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter17.SpecificProtocolsforWildernessEMSAsthma.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“RespiratoryEmergencies.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter24.WildernessFieldProtocolsProtocol6SevereAsthma.2001.WildernessMedicalAssociates.2Dec.2004<http://www.wildmed.com/field_protocols/joint_dis_protocol05.01.html#top>Wilkerson,JamesA.“RespiratoryDisorders.”MedicineforMountaineering5thed.Seattle,
StandingOrders:Shock
GeneralComments:
Serioustraumaticinjuryandlargeareasofsignificantburnsareunusualintheoutdoors.Themorecommonriskforshockmaybefromlossoffluidvolumefromsweating,vomiting,diarrheaandinadequatehydration.Outdoorleadersshouldfocusonearlyrecognitionandinterventiontocontrolfluidlossandmaintainpatientsinthefield.TreatmentforShock:
48
1. Treatbeforeserioussignsdevelop.2. Treatthecause.Keepthepatientcalm.3. Keepthepatientwarm.4. Keepthepatientflatwithlegselevatednomorethan12inches(30.5cm)(Headorlowerextremityinjury
mayprecludethis.)5. Consideradministeringoralfluidsinanextendedcaresituation(Ifpatientcantoleratethefluids,mental
statusisadequatetoswallowandthereisnoabdominalinjury.)6. Administeroxygen,ifavailable.7. Monitorthepatientcloselyfordeterioratingvitalsigns.
EvacuationGuidelinesSummaryEvacuateRapidly:
•Anypatientwithdecreasedlevelofresponsivenessorworseningvitalsigns.
Evacuate:
•Anypatientwhosevitalsignsdonotstabilizeorimproveovertime.ProtocolDecision:Oxygenisrecommendedforallpatientsexhibitingsignsandsymptomsofshock.Theadministrationofoxygenrequiresaphysician.
References:“ShockandFluidResuscitation.”PHTLSBasicandAdvancedPrehospitalTraumaLifeSupport.St.Louis,Missouri:Mosby,2003.Chapter6.Schimelpfenig,Tod.“Shock.”WildernessMedicine.Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter2.Tilton,Buck.“Shock.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter7.
StandingOrder:SkinIrritation
GeneralComments:Skinirritationscanoftenbepreventedthoughimprovedhygienepracticesandappropriateclothing.Theactiveingredientinpoisonivy,oakandsumacisurushiol.Thisoilcanbetransferredtotheskinregardlessofwhetherornottheplanthasitstraditionalshinythreeleavesinbloom.Inhaledsmokefromburningplantscanalsocauseasignificantreaction.Therearebarriercreamsforhypersensitiveindividuals.TreatmentforSkinIrritation:1.Fungalinfectionsoftheskincanbetreatedbywashingtheareathoroughlywithsoapandwater,airdryingand
applyingathinlayerof1%hydrocortisonecreamoratopicalanti‐fungal(e.g.Tinactin®).Considerprescriptionantifungals(e.g.Diflucan®)forsevereinfections.
2. Forasuspectedcontactwithpoisonivy,oakorsumac,washtheareaimmediatelyafterexposurewithsoapandcoolwater.ForhighlysensitivepersonsconsiderusingTecnu®orZanfel®asasoap.Washallclothesandequipmentthatmayhavebeenexposed.Oncetherashappears,applyathinlayerof1%hydrocortisonecreamorcalaminelotiontoreduceitching.Oralantihistaminesmayhelpreduceitching.
49
EvacuationGuidelinesforSkinIrritation:EvacuateRapidly:•Anypatientwithrespiratorydistressafterinhalingsmokefromburningpoisonivy,oakorsumac.
Evacuate:•Anypatientwithaskinirritationthatmakesthemtoouncomfortabletocontinue.ProtocolDecision:Anti‐fungalmedication(e.g.Tinactin®)isrecommendedfortreatingfungalinfectionsoftheskin.Theadministrationofover‐thecounteranti‐fungalmedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.Prescriptionanti‐fungalmedicationmaybeusefulintreatingfungalinfectionsoftheskin.Theadministrationofprescriptionanti‐fungalmedication(e.g.Diflucan®)requiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforitOver‐the‐counterantihistamines,topicalhydrocortisonecreamandcalaminelotionmaybehelpfulinmanagingthesymptomsofpoisonivy,oakandsumac.Theadministrationofover‐thecountermedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
References:Auerbach,PaulS.“Plant‐InducedDermatitis.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter57.“Skin.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.4‐38.
StandingOrder:NorthAmericanPitVipers,CoralSnakesandPoisonousLizardsGeneralCommentsFatalitiesduetoenvenomationbysnakesorlizardsareextremelyrareinNorthAmerica,thoughtissuelossisapossibility.Venomwillnotbeinjectedinallbites.Theinjuryshouldbemonitoredcloselyforsignsofenvenomation.Anti‐venomisavailableformostbites.TreatmentforBitesfromNorthAmericanPitVipers,CoralSnakesandPoisonousLizards1. Ensurethesceneissafe.Remaincalmandputthepatientatrest.Avoidwalkingifpossible.2. Removeconstrictingclothingandjewelryfromthebitesite.3. Washanddressthewound.4. Measureandmonitorswellingandsignsofenvenomation.Donotapplyice.5. Painmedicationsasneeded.6. Awideelasticbandagewrappeddistaltoproximalisrecommendedforcoralsnakebites.7. Splinttheextremityandkeepitatthesamelevelastheheart.8. Monitorforshockandcardiacandrespiratorydepression.EvacuationGuidelinesforBitesfromNorthAmericanPitVipers,CoralSnakesandPoisonousLizardsEvacuateRapidly:•Anypatientexhibitingshock,orcardiacorrespiratorydepression.•Anypatientwithsignsorsymptomsofenvenomation.
50
Evacuate:•Anypatientbittenbyapoisonoussnake,ideallybycarryingorslowlywalking.ProtocolDecision:Apatientwithasnakeorlizardbitemaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Apatientwithasnakeorlizardbitemaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.
References:
Auerbach,PaulS.“BitesbyVenomousReptilesintheAmericas.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter48.Forgey,William.“ReptileEnvenomations.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter20.Gold,BarryS.,RichardC.DartandRobertA.Barish.“BitesofVenomousSnakes.”NewEnglandJournalofMedicineVol.347,No.5,August1,2002:347‐356.Russell,FindlayE.SnakeVenomPoisoning.GreatNeck,NewYork:ScholiumInternationalInc.,1983.Schimelpfenig,Tod.“Poisons,Stings,andBites.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter12.Stewart,CharlesE.“BitesandStings.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter7.Tilton,Buck.“NorthAmericanBitesandStings.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter21.Wilkerson,JamesA.“AnimalBitesandStings.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter25.
StandingOrder:NorthAmericanSpidersandScorpions
GeneralCommentsManyspiderbitesareinitiallypainlessmakingitdifficulttoidentitythespecificspider.Fatalitiesarerare.Scorpionstingsarepainful,buttypicallyself‐limiting.SystemicreactionsarepossiblefromscorpionsintheextremesouthwesternUS.TreatmentforBitesandStingsfromNorthAmericanSpidersandScorpions1. Cleanthebite/stingsite.Continuetocleanthesiteifwounddoesnotheal.2. Icethebitesiteforpainandconsiderpainkillersforabdominalcramps.3. Monitorthebitesitefornecrosis.4. Monitorthepatientforsystemicsignsandsymptoms.EvacuationGuidelinesforBitesandStingsfromNorthAmericanSpidersandScorpionsEvacuateRapidly:•Anypatientexhibitingslurredspeech,difficultyswallowing,blurredvision,seizures,orrespiratoryorcardiovascularinvolvement.
51
Evacuate:•Anypatientwithasuspectedblackwidowspiderbite.•Anypatientwithawoundthatwillnotheal.ProtocolDecisionApatientwithaspiderbiteorscorpionstingmaybenefitfromprescriptionlevelpainmedication.Theadministrationofprescriptionpainmedicationrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.Apatientwithaspiderbiteorscorpionstingsmaybenefitfromover‐the‐counterpainmedication.Theadministrationofover‐thecounterpainmedicationtominorsrequiresparentalapproval,whichcanbeobtained
throughpre‐tripauthorizationformsoronacasebycasebasis.References:Auerbach,PaulS.“SpiderBites.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter46.Auerbach,PaulS.“ScorpionEnvenomation.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter47.Forgey,William.“ArthropodEnvenomations.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter21.MMWRWeekly45(21)May31,1996:433‐436.“NecroticArachnidism‐‐PacificNorthwest,1988‐1996.”CentersforDiseaseControlandPrevention.27Dec.2004.<http://www.cdc.gov/mmwr/preview/mmwrhtml/00042059.htm>Schimelpfenig,Tod.“Poisons,Stings,andBites.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter12.Stewart,CharlesE.“BitesandStings.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter7.Tilton,Buck.“NorthAmericanBitesandStings.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter21.Wilkerson,JamesA.“AnimalBitesandStings.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter25.
StandingOrder:SpinalInjuries
GeneralComments:Theutilizationofthefocusedspineassessmenttodeterminepresenceorabsenceofspinalinjuryhasbeenwellstudiedintheclinicalsetting.Outdoorleadersshouldbeattentivetosuspiciousmechanismsofinjury,takeearlyspinalprecautionswithpatientsandwhenappropriateusethefocusedspineassessmenttomakeacarefuldecisionaboutcontinuedimmobilization.FocusedSpineAssessment:Ifthepatienthasamechanismforspinalinjurybutdoesnotexhibitsignsandsymptomsofspinalinjuryduringthecompletepatientassessment;performafocusedspineassessmenttodeterminewhetherfurtherspinalimmobilizationiswarranted.FocusedSpineAssessment1. Patientmustbereliable:A+Ox3or4,sober,andhavenodistractions.2. PatientmusthavenormalCirculation(warm,pinkdigitsorgoodpedal/radialpulse),Sensation(nonumbness,
tinglingorunusualhotorcoldsensations)andMotion(unlessotherwiseexplainablebyanotherinjuryorillness)inallfourextremities.
52
3. Patientmustdenyspinalpainandtenderness.Ifpatientmeetsallcriteriafurtherspinalimmobilizationisnotwarranted.TreatmentforSuspectedSpinalInjury:Ifthepatientexhibitssignsandsymptomsofspinalinjuryduringeitherthepatientassessmentorthefocusedspineassessment:1. Stabilizethespineandcontroltheheadmanually.2. Checkcirculation,sensationandmotion(CSM)intheextremities.3. Establishneutralalignmentofthespine.4. Applyacervicalcollar.5. BEAMorlog‐rollthepatientintoacommerciallitterorontoabackboard.6. Securetheentirebodytothelitterorbackboardwithpaddingandstraps.7. Securetheheadtothelitterorbackboard.8. RecheckCSMintheextremities.9. Evacuate.EvacuationGuidelinesforSpinalInjuries:EvacuateRapidly:•Anypatientwhodemonstratessignsandsymptomsofneurologicalinjury.Evacuate:•Anypatientbeingtreatedforaspinalinjury,ideallyonacommerciallitteroronabackboard.ProtocolDecision:ThoughsomeurbanEMSsystemshaveadopteduseofafocusedspinalassessmentallowingpre‐hospitalproviderstomakeadecisionabouttheneedforspinalimmobilization,thisisstillessentiallyawildernessprotocolanditsuseshouldbediscussedwithROPEMedicalAdvisor.
References:EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>DomeierR.M.“PositionPaper,NationalAssociationofEMSPhysicians:Indicationsforprehospitalspinalimmobilization.”PrehospitalEmergencyCare3(3)1999:251–253.Forgey,William.“SpinalInjury.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter5.HoffmanJ.R.andW.R.Mower.“Out‐of‐hospitalcervicalspineimmobilization:Makingpolicyintheabsenceofdefinitiveinformation.”AnnalsofEmergencyMedicine37June2001:632–634.“SpinalTrauma.”PHTLSBasicandAdvancedPrehospitalTraumaLifeSupport.St.Louis,Missouri:Mosby,2003.Chapter9.Schimelpfenig,Tod.“BrainandSpinalCordInjuries.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter4.Tilton,Buck.“SpineInjuries.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter8.
53
WildernessFieldProtocolsProtocol4SpineInjuries.2001.WildernessMedicalAssociates.2Dec.2004.<http://www.wildmed.com/field_protocols/spine_man_protocol05.01.html#top>Wilkerson,JamesA.“HeadandNeckInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter16.
StandingOrder:SubmersionIncidents
GeneralCommentsRescuersafetyisparamountwhendealingwithsubmersionevents.Itiscommontounderestimatetheeffectsofwatercurrentandtemperatureontheabilityofbothrescuersandpatientstoavoidsubmersion.TreatmentforSubmersionInjuries1. Scenesafety:Reach,Throw,Row,Tow,Go!Getthepersonontoasafe,firmsurface.Donotenterthewater
toattemptrescueifyouhavenotbeentrained.2. AggressiveBasicLifeSupportwithsupplementaloxygen,ifavailable.EvacuationGuidelinesforSubmersionInjuriesEvacuateRapidly:•Anypatientwhodevelops:Wetlungsounds,productivecough,rapid,shallow,respirations,cyanosis,substernalburning,inabilitytotakeadeepbreath,irregularand/ordepressedheartrate,oradecreasedlevelofresponsiveness.Evacuate:•Anypatientwhowasunresponsiveatanytimeduringthesubmersion.ProtocolDecision:Oxygenisrecommendedforsubmersionvictims.Theadministrationofoxygenrequiresaphysician.Thismedicationmayalsobeself‐administeredbypatientswithaprescriptionforit.References:ACLSProviderManual.Dallas,Texas:AmericanHeartAssociation,2002.Auerbach,PaulS.“SubmersionIncidents.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter68.Forgey,William.“SubmersionInjuries.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter3.Harries,Mark.“ABCofResuscitationNearDrowning.”BMJVol.3276Dec.2003:1336‐1338.Schimelpfenig,Tod.“DrowningandColdWaterImmersion.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter14.StateofAlaskaColdInjuriesandColdWaterNearDrowningGuidelines.Revision01/96.HypothermiaPrevention,RecognitionandTreatment.Articles,ProtocolsandResearchonLife‐savingskills.27Dec.2004.<http://www.hypothermia.org/protocol.htm>Stewart,CharlesE.“Near‐Drowning.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter11.Tilton,Buck.“ImmersionandSubmersionIncidents.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter19.
StandingOrder:WoundsandInfection
54
GeneralCommentsWoundsandinfectionarecommonlyreportedmedicalproblemsinawildernesssetting.Establishedinfectionischallengingtomanagesoeffortsshouldbedirectedataggressivewoundcleaningandeffectivedressingtopreventinfectionandpromotehealing.TreatmentforWoundsandInfection1. Controlbleedingusingdirectpressureandelevation,pressuredressings,andinextremecases,tourniquets.2. Properlycleanthewound:Washyourhandsandputonyourgloves;Cleanaroundthewoundwithsoapand
water,anabrasionmaybeaggressivelyscrubbed,andrinsewithdisinfectedwater;Removeanyforeignmatterwithdisinfectedtweezersorbygentlybrushingitoutofthewound;Pressureirrigatethewoundwithdisinfectedwater(minimum½literrecommended).
3. Coverwoundwiththecleanestdressingavailableandbandage.Keepwoundmoistwithadressingcoatedwithantibioticointmentoratransparentfilmdressing.Ifthecutgapesopenlessthan1/2inch(1.3cm),approximatewoundedgeswithwoundclosurestrips.Monitorcirculation,sensationandmotion(CSM).Keepthedressingscleananddry.Changedressingsatleastevery24hours.Ifusingtransparentfilmdressings,dressingsmaybeleftinplaceuntilwoundheals.
4. Ifthecutcausesgapingofmorethan1/2inch(1.3cm)orwoundisinfected,packthewoundopenwet‐dryandkeepthewoundmoistduringevacuation.
5. Incaseofanamputation,wrapthepartinamoiststeriledressingandsealinaplasticbag.Immersethebagincoolwaterandtransportrapidlytothehospitalwiththepatient.
6. Considerremovinganimpaledobjectifitisthroughthecheek.Inremoteenvironmentsconsiderremovaliftheobjectisinanextremityandinterfereswithtransport.
7. Ifthewoundshowssignsandsymptomsofinfection:Hotsoaksfor20‐30minutesseveraltimesdaily;cleanthewoundfollowingthehotsoak;keepthepatienthydrated;considerpackingthewoundopen(wettodry)toallowdrainage;considerantibioticandfeverreducingtherapy.
EvacuationGuidelinesforWoundsandInfectionEvacuateRapidly:•Anypatientwithanamputation.•Anypatientwithanobjectstillimpaled.•Anypatientwithawoundthat:Isheavilycontaminated,opensajointspace,involvesunderlyingtendonsorligaments,wascausedbyananimalbite,isontheface,orwascausedbyacrushingmechanism.•Anypatientwithawoundthatshowssignsandsymptomsofseriousinfection.Evacuate:•Anypatientwithawoundthatcannotbeclosedinthefield.•Anypatientwithaninfectionthatdoesnotimprovewithin12‐24hours.ProtocolDecision:Tourniquetsareusedtomanageseverebleedinguncontrolledbydirectpressure.Thedecisiontoreleaseatourniquetinawildernessenvironmentiscontroversial.ROPEMedicalAdvisorshouldadviseyouonthecircumstancesunderwhichheorsheiscomfortablewithatourniquetbeingreleasedinthebackcountry.Closingwoundsisgenerallyconsideredaclinicalprocedure.ROPEMedicalAdvisorshouldadviseyouonthecircumstancesunderwhichheorsheiscomfortablewithwoundclosureinthebackcountryusingwoundclosurestripsorbutterflybandages.
55
Theremovalofimpaledobjectsiscontroversial.ROPEMedicalAdvisorshouldadviseyouonthecircumstancesunderwhichheorsheiscomfortablewiththeremovalofanimpaledobject.Antibioticsarerecommendedforallseriouslyinfectedwounds.Theadministrationofanantibioticrequiresaphysician.Thesemedicationsmayalsobeself‐administeredbypatientswithaprescriptionforthem.
References:
EmergencyMedicalTechnician‐Basic:NationalStandardCurriculumModule5Trauma.22June1995.NationalHighwayTrafficSafetyAdministrationUnitedStatesDepartmentofTransportation.2Dec2004.<www.nhtsa.dot.gov/people/injury/ems/pub/emtbnsc.pd>Goth,PeterandGeorgeGarnett.“NationalAssociationofEMSPhysiciansClinicalGuidelinesforDelayedorProlongedTransportWounds.”PrehospitalandDisasterMedicineVol.8No.3July‐Sep.1993:253‐255.Forgey,William.“WoundManagement.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter6.Schimelpfenig,Tod.“SoftTissueInjuries.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter7.SpecificProtocolsforWildernessEMSWounds.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>TheMerckManual16thEdition.Rathaway,NewJersey:Merck&Co.,Inc.,1992.Tilton,Buck.“WildernessWoundManagement.”WildernessFirstResponder2nded.Guilford,Connecticut:TheGlobePequotPress,2004.Chapter15.WildernessFieldProtocolsProtocol2WoundManagement.2001.WildernessMedicalAssociates.2Dec.2004.<http://www.wildmed.com/field_protocols/spine_man_protocol05.01.html#top>Wilkerson,JamesA.“Soft‐TissueInjuries.”MedicineforMountaineering5thed.Seattle,Washington:TheMountaineersBooks,2001.Chapter6.
StandingOrder:Zoonoses
GeneralCommentsThereisawide‐rangeofdiseasestransmittedfromanimalstohumans.TheonesweworryaboutthemostintheUnitedStatesare:TickFevers,WestNileVirus,Hantavirus,RabiesandPlague.Fielddiagnosiscanbeextremelydifficultandisunnecessary.Thepatientshouldbeassessedforahistoryofabiteandinregardstotheflu‐likeillnessevacuationcriteria.Educationaleffortsshouldfocusoneffectiveprevention.TreatmentforZoonoses1. Symptomaticmanagement,e.g.feverreducingmedication,painmedication,antihistaminesandantibiotic
therapy.2.Treatallmammalbitesasapotentialrabiesexposure.Cleanwoundthoroughlywithsoapanddisinfected
water.EvacuationGuidelinesforZoonosesEvacuateRapidly:•Anypatientwithamammalbiteforinitiationoftherabiesvaccine.Evacuate:•Anypatientwithahistoryofanembeddedtickwhodevelopsfever,rashandflu‐likesymptoms.•Anypatientwhotriggerstheflu‐likeillnessevacuationcriteria.

56
ProtocolDecision:Arangeofover‐the‐countermedicationsincludingantihistamines,painmedicationsandfever‐reducingmedicationsmayhelppatientswithazoonosis.Theadministrationofover‐thecounterantihistamines,painmedicationsandfever‐reducingmedicationstominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsoronacasebycasebasis.Antibioticsmaybehelpfulforpatientswithazoonosis.Theadministrationofanantibioticrequiresaphysician.Thesemedicationsmayalsobeself‐administeredbypatientswithaprescriptionforthem.
References:Auerbach,PaulS.“Tick‐BorneDiseases.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter45.Auerbach,PaulS.“Wilderness‐AcquiredZoonoses.”WildernessMedicine5thed.St.Louis,Missouri:Mosby,2007.Chapter53.Forgey,William.“Tick‐TransmittedDiseases.”WildernessMedicalSocietyPracticeGuidelinesforWildernessEmergencyCare5thed.Guilford,Connecticut:TheGlobePequotPress,2006.Chapter22.“InfectiousDiseases.”UnitedStatesSpecialOperationsCommand.SpecialOperationsForcesMedicalHandbook.Jackson,Wyoming:TetonNewMedia,2001.Chapter13,5‐33.Schimelpfenig,Tod.“Poisons,Stings,andBites.”WildernessMedicine,Mechanicsburg,Pennsylvania:StackpoleBooks,2000.Chapter12.SpecificProtocolsforWildernessEMSRabies.Version1.2May19,1994.TheWildernessEmergencyMedicalServicesInstitute.2Dec.2004.<http://www.wemsi.org/specific.html>Stewart,CharlesE.“BitesandStings.”EnvironmentalEmergencies.Baltimore,Maryland:Williams&Wilkins,1990.Chapter7.
57
ReedCollegeCourseDrugKitAdministeringprescriptionmedicationsisusuallyrestrictedtolicensedmedicalprofessionalsorindividualsactingwithinestablishedEmergencyMedicalServicessystems.Somecoursesmaycarryprescriptionmedicationsasacomponentoftheirmedicalsuppliesincludingepinephrine.NotetoROPEstaff:Thereareincreasingnumbersofstatelawsthatallowfortheadministrationofepinephrinetoanindividualexperiencingalifethreateningallergicreactionbya“layperson”.Mostcommonlytheepinephrineadministeredisthepatient’s,andthestaffmemberassiststhepatient.Thisislikelytobeanareaofcontinueddiscussionandevolvinglawsandregulationsintheensuingyears.Frequentlyindividualswillbringtheirownprescriptionmedicationsonatrip,especiallyonaninternationalcourseortrip.Whileyoumaynotbeadministeringthesemedications,havingsomebasicinformationabouttheiruses,doses,sideeffectsandcontraindicationswillbehelpful.Typicallytheadministrationofnon‐prescription,orover‐the‐counter,medicationfallswithintherealmofsimplefirstaid.Havingsomepainmedications,anti‐histamines,anti‐fungalsandantacidsmayhelpmanagesomeone’ssymptomsandallowthemtoremaininthebackcountry.Beforeadministeringanymedicationreadtheprotocols,confirmthedosage,readthelabelandconfirmthemedication,askthepatientaboutprevioushistorywiththismedicationandanyknownallergies,askthepatientiftheyarecurrentlyonanymedicationandifso,reviewtheprotocolsforcontraindications.Theadministrationofover‐thecountermedicationtominorsrequiresparentalapprovalwhichcanbeobtainedthroughpre‐tripauthorizationformsorbycommunicatingwiththeparentsonacasebycasebasis.PleasenotethatthefollowingmedicationinformationisformedicationavailableintheUnitedStates.OutsideoftheUnitesStatesmedicationmaycarrydifferenttradenames.SomemedicationavailableonlybyprescriptionintheUnitedStatesmaybeavailablewithoutaprescriptioninothercountriesandmaybepreparedindifferentdosing.IfyoupurchasemedicationoutsideoftheUnitedStatesyoushouldbeawareofqualitycontrolconcernsinmanufacturingthesemedications,andyoushouldconfirmclassification,dose,indication,contraindicationandpossiblesideeffectsbeforeadministeringit.Alldosingisindicatedforadults.PediatricdosingshouldbedictatedbyourMedicalAdvisor,Dr.Hatfield‐Keller.Abbreviations:
PO:OralSQ:SubcutaneousinjectionIM:Intramuscularinjection
58
DrugInformationProvidedOnAnalgesic(Painkillers)‐Over‐The‐Counter Acetaminophen(e.g.Tylenol) Aspirin(e.g.Bayer,Ecotrin) Ibuprofen(e.g.Advil,Motrin) Ketoprofen(e.g.OrudisKT) Naproxen(e.g.Aleve) Phenazopyridinehydrochloride(e.g.Pyridium,Uristat)Analgesics(Painkillers)‐Prescription Hydrocodonebitartrate/acetominophen(e.g.Vicodin) Oxycodone/acetominophen(e.g.Percocet,Roxicet)Anti‐Allergy‐Over‐The‐Counter Phenylephrine(e.g.Neo‐Synephrine) Hydrocortisoneacetate(e.g.Cortaid) Diphenhydraminehydrochloride(e.g.Benadryl) Pseudoephedrinehydrochloride(e.g.Sudafed)Bronchodilator‐Prescription AlbuterolEpinephrine‐Prescription Epinephrine(e.g.AdrenalinorEpiPen)Antibiotic‐Over‐The‐Counter PolymyxinBsulfate/bacitracin(e.g.Polysporin)Antibiotic‐Prescription Erythromycin TrimethoprimSulfamethoxazole(e.g.SeptraorBactrim) Cephalexin(e.g.Keflex) Ciprofloxacinhydrochloride(e.g.Cipro)Anti‐Fungal‐Over‐The‐Counter Tolnaftate(e.g.Tinactin) Miconazolenitrate(e.g.Monistat3)Anti‐Fungal‐Prescription Fluconazole(e.g.Diflucan)Anti‐Emetics(Anti‐Vomiting)andAnti‐Acids‐Over‐The‐Counter Calciumcarbonate(e.g.Tums,Maalox) Bismuthsubsalicylate(e.g.Pepto‐Bismol)Anti‐Emetics(Anti‐Vomiting)andAnti‐Acids‐Prescription Prochlorperazine(e.g.Compazine) Promethazine(e.g.Phenergan)Anti‐Vertigo(Anti‐MotionSickness)‐Over‐The‐Counter Meclizine(e.g.Antivert,Bonine)Anti‐Vertigo(Anti‐MotionSickness)‐Prescription Scopolamine(e.g.Trans‐DermScop)Anti‐Diarrheal‐Over‐The‐Counter Loperamidehydrochloride(e.g.Imodium)Anti‐Diarrheal‐Prescription Diphenoxylatehydrochloridewithatropinesulfate(e.g.Lomotil)
59
AltitudeMedications‐Prescription Acetazolamide(e.g.Diamox) Dexamethasone(e.g.Decadron) Nifedipine(e.g.Procardia)
Analgesics(Painkillers)‐Over‐The‐Counter
Acetaminophen(e.g.Tylenol)
Classification:Non‐narcoticanalgesic,antipyretic
Dose:650mg/4‐6hoursPO(Regularstrength),1000mg/6hoursPO(Extrastrength).Maximumdose4g/24hours
PO.
Indications:Forreliefofpainduetoheadache,coldandfludiscomfort,minormuscleandjointdiscomfortand
menstrualcramps.Forreductionoffever.Especiallyusefulforthoseallergictoaspirinoraspirin‐containing
products.Doesnotcontrolinflammation.
Contraindications:Hypersensitivity,activealcoholism,liverdisease,hepatitis.Acetaminophenisacommon
ingredientinover‐the‐counterpain,coldandflumedicine.Becarefulofaccidentaloverdoseincombinationwith
otherproducts.
SideEffects:Hypersensitivityisrare.
Aspirin(e.g.Bayer,Ecotrin)
Classification:Analgesic,Non‐SteroidalAnti‐InflammatoryDrug(NSAID),antipyretic,anticoagulant.
Dose:325‐650mg/4hoursPO(Regularstrength),500‐1000mg/4‐6hoursPO(Extrastrength),162‐325mg/24hours
POforcardiacchestpain.Maximumdose4g/24hoursPO.
Indications:Forreliefofpainduetoheadache,coldandfludiscomfort,minormuscleandjointdiscomfortand
menstrualcramps.Forreductionoffever.Controlsinflammation.Canbeusedto“cauterize”exposedtoothpulp.
Foruse
withcardiacchestpain.
Contraindications:Allergicsensitivity.Gastrointestinalbleeding,bleedingdisorders,impairedliverfunction.Do
notgivetochildrenunder12.
SideEffects:Gastrointestinaldistress,allergicreaction.
Ibuprofen(e.g.Advil,Motrin)
Classification:Analgesic,Non‐SteroidalAnti‐InflammatoryDrug(NSAID),antipyretic.
Dose:400‐800mg/4‐8hoursPO.Maximumdose2400mg/24hoursPO.
Indications:Forsymptomaticreliefofpainassociatedwithheadache,colds,flu,frostbite,toothache,arthritis,
60
burnsandmenstrualcramps.Maybeusedtoreducefever.Forpainofinflammationandreductionof
inflammationassociatedwithmuscle,jointandover‐useinjuries.
Contraindications:Activepepticorgastrointestinalulcer,gastrointestinalbleedingdisorder,historyof
hypersensitivitytoaspirinorotherNSAIDs.
SideEffects:Nausea,epigastricpain,dizzinessandrash.
Ketoprofen(e.g.OrudisKT)
Classification:Analgesic,Non‐SteroidalAnti‐InflammatoryDrug(NSAID).
Dose:75mg/8hrsPO
Indications:Forsymptomaticreliefofpainassociatedwithheadache,colds,flu,frostbite,toothache,arthritis,
burnsandmenstrualcramps.Maybeusedtoreducefever.Forpainofinflammationandreductionof
inflammationassociatedwithmuscle,jointandover‐useinjuries.
Contraindications:Activepepticorgastrointestinalulcer,gastrointestinalbleedingdisorder,historyof
hypersensitivitytoaspirinorotherNSAIDs.
SideEffects:Nausea,diarrheaandepigastricpain.
Naproxen(e.g.Aleve)
Classification:Analgesic,Non‐SteroidalAnti‐InflammatoryDrug(NSAID).
Dose:550mg/12hrsPO
Indications:Forsymptomaticreliefofpainassociatedwithheadache,colds,flu,frostbite,toothache,arthritis,
burnsandmenstrualcramps.Maybeusedtoreducefever.Forpainofinflammationandreductionof
inflammationassociatedwithmuscle,jointandover‐useinjuries..
Contraindications:HypersensitivitytoaspirinorotherNSAIDs.
SideEffects:Nausea,constipation,abdominalpain,headache,dizzinessanddrowsiness.
Phenazopyridinehydrochloride(e.g.Pyridium,Uristat)
Classification:Urinarytractanalgesic
Dose:100‐200mg/6‐8hrsPO
Indications:Forsymptomaticreliefofburning,pain,urgencyandfrequencyassociatedwithurinarytract/bladder
infections.Shouldbeusedconcurrentlywithanantibiotic.
Contraindications:Hypersensitivity.Renal/liverinsufficiency.
SideEffects:Headache,gastrointestinaldisturbanceandrash.Dyestainsclothing.
Analgesics(Painkillers)‐Prescription
61
Hydrocodonebitartrate/acetominophen(e.g.Vicodin)
Classification:Narcoticanalgesic,antitussive.
Dose:5‐10mg/4‐6hoursPO
Indications:Formoderatetoseverepain.Narcotic.Goodformusculoskeletal
anddentalpain.Goodforpeopleallergictocodeine.Suppressescoughreflex.
Contraindications:Hypersensitivity.
SideEffects:Sedation,decreaseinbloodpressure,sweatingandflushedface,drowsinessanddizziness.
Oxycodone/acetominophen(e.g.Percocet,Roxicet)
Classification:Narcoticanalgesic.
Dose:5‐10mg/4hoursPO
Indications:Forseverepain.
Contraindications:Hypersensitivity.CautionwithCNSdepression,respiratorydepression,seizuresandshock.
SideEffects:Drowsiness,dizziness,hypotension,anorexia,nausea,vomitingandconstipation.
Anti‐Allergy‐Over‐The‐CounterPhenylephrine(e.g.Neo‐Synephrine)
Classification:Nasaldecongestant
Dose:Blownosebeforemedicationisadministered,tiltheadback,apply2‐3dropsor1‐2spraysineachnostril.
Wait5minutesbetweennostrils.
Indications:Forreliefofnasalcongestionthataccompaniescoldsandallergies.Maybeusefultohelpstop
nosebleed.Maybeusefultorelievesinus“squeeze”associatedwithdiving.
Contraindications:Severehypertension,ventriculartachycardia,pancreatitis,hepatitis,thrombosis,heartdisease,
narrowangleglaucoma.
SideEffects:Reboundnasalcongestionduetooveruse(>3days),stinging,burning,dryingofnasalmucosa.
Hydrocortisoneacetate(e.g.Cortaid)
Classification:Glucocorticoid
Dose:Topical1%cream,2‐4times/day
Indications:Forreliefofpainanditchingofnematocyststings,poisonivy,oakandsumac,insectbitesandother
allergicskinreactions.Mayhelpdryupoozingrashofallergicskinreactions.
Contraindications:Seriousinfections,viral,fungalortubercularskinlesions.
SideEffects:Itching,rednessandirritation.
62
Diphenhydraminehydrochloride(e.g.Benadryl)
Classification:Antihistamine
Dose:25‐50mgper4‐6hours
Indications:Fortemporaryreliefofrespiratoryallergysymptomsandcoldsymptoms.Helpsrelievetheitchingof
allergicskinreactions.Usefulintreatmentofmoderateallergicandanaphylacticreactions.Maybeusedasamild
sedativeandforinsomnia.Mayhelpalleviateseasickness.Canbeusedtotreatdistonicreations.
Contraindications:Hypersensitivity,acuteasthmaattack,glaucoma,pepticulcer,hypertensionandCOPD.
SideEffects:Drowsiness,dizziness,weakness,hypotension,drymouth,thickeningbronchialsecretionsandurinary
retention.
Pseudoephedrinehydrochloride(e.g.Sudafed)
Classification:Nasaldecongestant
Dose:60mgper4‐6hours
Indications:Decongestantusefulintreatingupperairwaysinusesandnasalpassages.Useofmorethat5daysmay
causereverseeffects.
Contraindications:Severehypertension,coronaryarterydisease,lactatingwomen,MAOinhibitortherapy.
SideEffects:Nervousnessrestlessness,insomnia,tremblingandheadache.
Bronchodilator‐PrescriptionAlbuterol
Classification:Bronchodilator
Dose:Twopuffsofmetereddoseinhaler(MDI)withuseofaspacerevery4hoursandasneeded.
Indications:Shortnessofbreathorrespiratorydifficultythoughttobesecondarytoreactiveairwaydysfunction
(asthma)orHAPE.
Contrainidications:Tachycardiasecondarytounderlyingheartcondition.
SideEffects:Palpitations,tachycardiaandtremor.
Epinephrine‐PrescriptionEpinephrine(e.g.AdrenalinorEpiPen)
Classification:Bronchodilator,antiallergenic,cardiacstimulant.
Dose:.3ml1:1000SQorIM.Repeatasnecessary.
Indications:Forsevereallergicreactionsincludinganaphylaxisandstatusasthmaticus.
Contraindications:Notruecontraindicationswithanaphylaxis.Hypertension,cardiacdisease,glaucomaand
63
shock.
SideEffects:Increasedheartrate,nervousness,dizziness,lightheadedness,nauseaandheadache.
Antibiotic‐Over‐The‐CounterPolymyxinBsulfate/bacitracin(e.g.Polysporin)
Classification:Antibiotic
Dose:Topical
Indications:Containsingredientsforpreventionofinfectioninminorwounds.Worksasalubricant,offerssome
relieffromitching.
Contraindications:Hypersensitivity.
SideEffects:Hypersensitivityreactions‐burning,itching,inflammation,contactdermatitis.
Antibiotic‐PrescriptionErythromycin
Classification:Antibiotic
Dose:250mg/6hrsfor5days.Takewithfood.
Indications:Forsinus,pulmonary,ear,eye,respiratoryandsofttissueinfections.
Contraindications:Hypersensitivity,liverdisease,hepatitis.
SideEffects:Abdominaldiscomfortandcramping,nausea,vomiting,diarrheaandrash.
TrimethoprimSulfamethoxazole(e.g.SeptraorBactrim)
Classification:Antibiotic
Dose:Singlestrengthtabletcontains80mgtrimethoprimand400mgsulfamethoxazole.Doublestrengthtablet
contains160mgtrimethoprimand800mgsulfamethoxazole.Doseis2singlestrengthtabletsor1doublestrength
tablet/12hoursPO.Recommendedlength,5daysforUTIandinfectiousdiarrhea,10‐14daysforkidneyinfection.
Indications:Formarinewounds,kidney,ear,sinusandsomerespiratoryinfections.Bestforurinarytract
infections.Workswithinfectiousdiarrheaifciprofloxacinunavailable.
Contraindications:Hypersensitivity,anemia.
SideEffects:Nausea,vomiting,diarrhea,decreasedappetite,stomachcramps,headache.
Cephalexin(e.g.Keflex)
Classification:Antibiotic
Dose:250‐500mgper6hoursforatleast5days.
Indications:Forskin,bone,pnuemoniaandurinarytractinfections.
Contraindications:Hypersensitivity.Sensitivitytopenicillins.
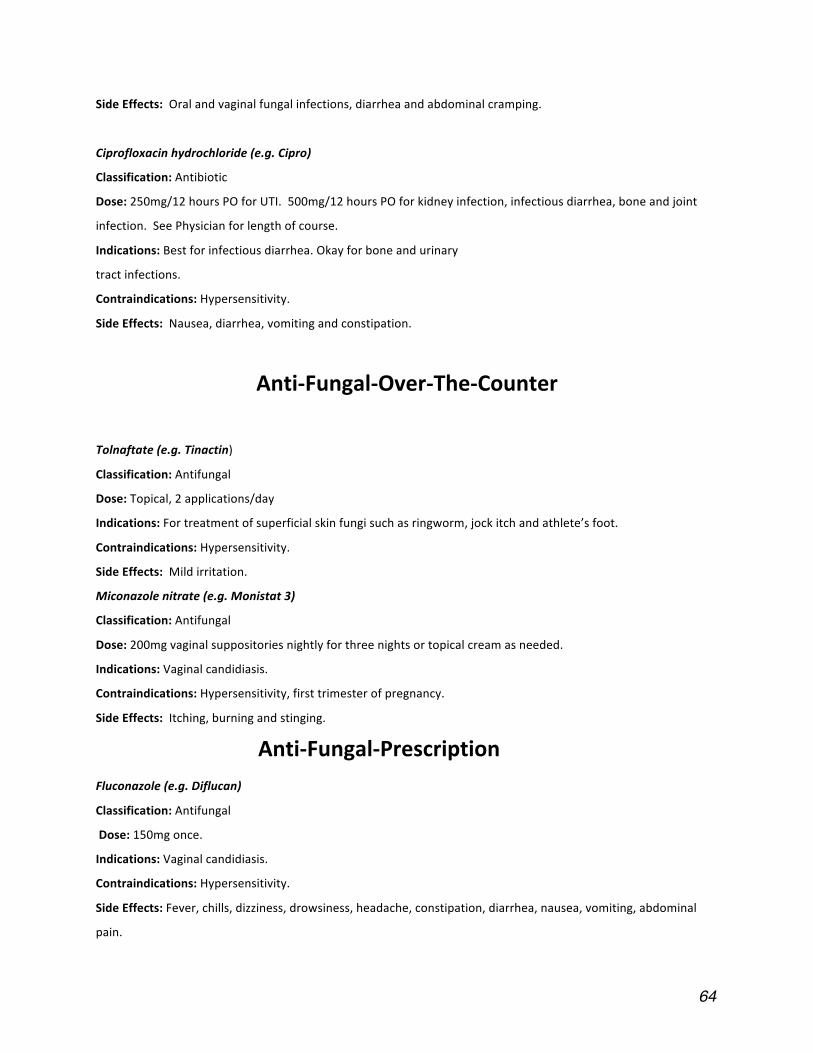
64
SideEffects:Oralandvaginalfungalinfections,diarrheaandabdominalcramping.
Ciprofloxacinhydrochloride(e.g.Cipro)
Classification:Antibiotic
Dose:250mg/12hoursPOforUTI.500mg/12hoursPOforkidneyinfection,infectiousdiarrhea,boneandjoint
infection.SeePhysicianforlengthofcourse.
Indications:Bestforinfectiousdiarrhea.Okayforboneandurinary
tractinfections.
Contraindications:Hypersensitivity.
SideEffects:Nausea,diarrhea,vomitingandconstipation.
Anti‐Fungal‐Over‐The‐Counter
Tolnaftate(e.g.Tinactin)
Classification:Antifungal
Dose:Topical,2applications/day
Indications:Fortreatmentofsuperficialskinfungisuchasringworm,jockitchandathlete’sfoot.
Contraindications:Hypersensitivity.
SideEffects:Mildirritation.
Miconazolenitrate(e.g.Monistat3)
Classification:Antifungal
Dose:200mgvaginalsuppositoriesnightlyforthreenightsortopicalcreamasneeded.
Indications:Vaginalcandidiasis.
Contraindications:Hypersensitivity,firsttrimesterofpregnancy.
SideEffects:Itching,burningandstinging.
Anti‐Fungal‐PrescriptionFluconazole(e.g.Diflucan)
Classification:Antifungal
Dose:150mgonce.
Indications:Vaginalcandidiasis.
Contraindications:Hypersensitivity.
SideEffects:Fever,chills,dizziness,drowsiness,headache,constipation,diarrhea,nausea,vomiting,abdominal
pain.
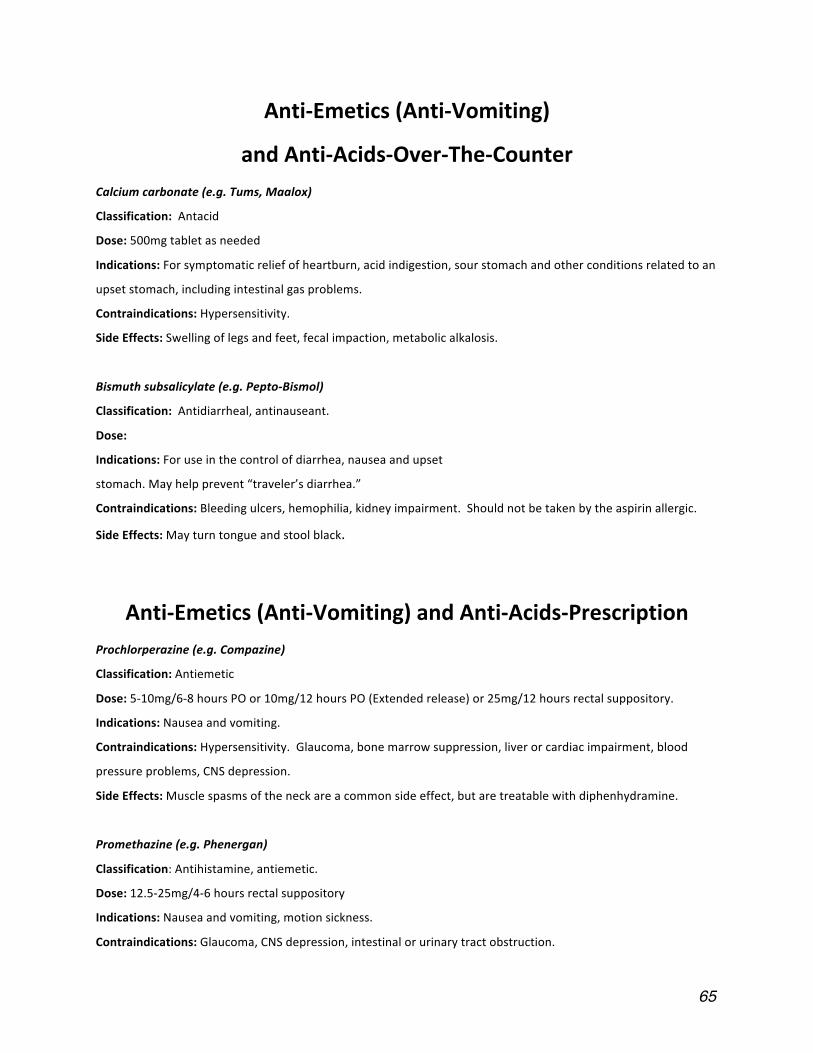
65
Anti‐Emetics(Anti‐Vomiting)
andAnti‐Acids‐Over‐The‐CounterCalciumcarbonate(e.g.Tums,Maalox)
Classification:Antacid
Dose:500mgtabletasneeded
Indications:Forsymptomaticreliefofheartburn,acidindigestion,sourstomachandotherconditionsrelatedtoan
upsetstomach,includingintestinalgasproblems.
Contraindications:Hypersensitivity.
SideEffects:Swellingoflegsandfeet,fecalimpaction,metabolicalkalosis.
Bismuthsubsalicylate(e.g.Pepto‐Bismol)
Classification:Antidiarrheal,antinauseant.
Dose:
Indications:Foruseinthecontrolofdiarrhea,nauseaandupset
stomach.Mayhelpprevent“traveler’sdiarrhea.”
Contraindications:Bleedingulcers,hemophilia,kidneyimpairment.Shouldnotbetakenbytheaspirinallergic.
SideEffects:Mayturntongueandstoolblack.
Anti‐Emetics(Anti‐Vomiting)andAnti‐Acids‐PrescriptionProchlorperazine(e.g.Compazine)
Classification:Antiemetic
Dose:5‐10mg/6‐8hoursPOor10mg/12hoursPO(Extendedrelease)or25mg/12hoursrectalsuppository.
Indications:Nauseaandvomiting.
Contraindications:Hypersensitivity.Glaucoma,bonemarrowsuppression,liverorcardiacimpairment,blood
pressureproblems,CNSdepression.
SideEffects:Musclespasmsoftheneckareacommonsideeffect,butaretreatablewithdiphenhydramine.
Promethazine(e.g.Phenergan)
Classification:Antihistamine,antiemetic.
Dose:12.5‐25mg/4‐6hoursrectalsuppository
Indications:Nauseaandvomiting,motionsickness.
Contraindications:Glaucoma,CNSdepression,intestinalorurinarytractobstruction.
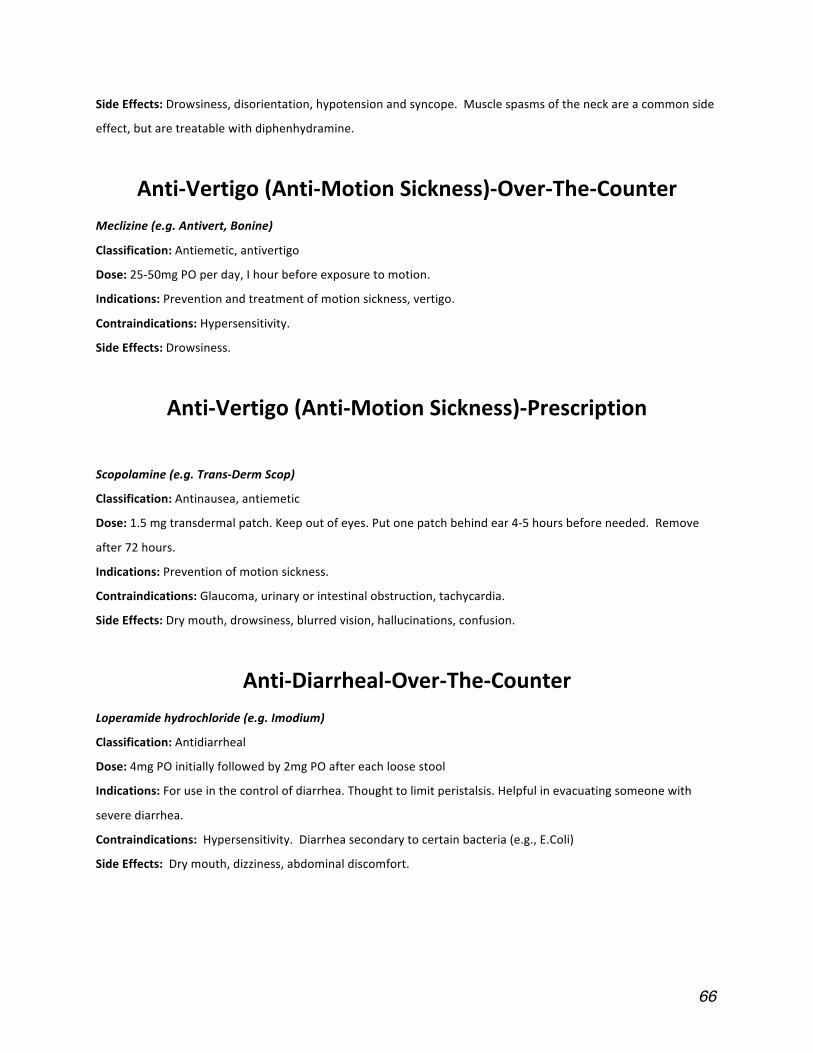
66
SideEffects:Drowsiness,disorientation,hypotensionandsyncope.Musclespasmsoftheneckareacommonside
effect,butaretreatablewithdiphenhydramine.
Anti‐Vertigo(Anti‐MotionSickness)‐Over‐The‐CounterMeclizine(e.g.Antivert,Bonine)
Classification:Antiemetic,antivertigo
Dose:25‐50mgPOperday,Ihourbeforeexposuretomotion.
Indications:Preventionandtreatmentofmotionsickness,vertigo.
Contraindications:Hypersensitivity.
SideEffects:Drowsiness.
Anti‐Vertigo(Anti‐MotionSickness)‐Prescription
Scopolamine(e.g.Trans‐DermScop)
Classification:Antinausea,antiemetic
Dose:1.5mgtransdermalpatch.Keepoutofeyes.Putonepatchbehindear4‐5hoursbeforeneeded.Remove
after72hours.
Indications:Preventionofmotionsickness.
Contraindications:Glaucoma,urinaryorintestinalobstruction,tachycardia.
SideEffects:Drymouth,drowsiness,blurredvision,hallucinations,confusion.
Anti‐Diarrheal‐Over‐The‐CounterLoperamidehydrochloride(e.g.Imodium)
Classification:Antidiarrheal
Dose:4mgPOinitiallyfollowedby2mgPOaftereachloosestool
Indications:Foruseinthecontrolofdiarrhea.Thoughttolimitperistalsis.Helpfulinevacuatingsomeonewith
severediarrhea.
Contraindications:Hypersensitivity.Diarrheasecondarytocertainbacteria(e.g.,E.Coli)
SideEffects:Drymouth,dizziness,abdominaldiscomfort.
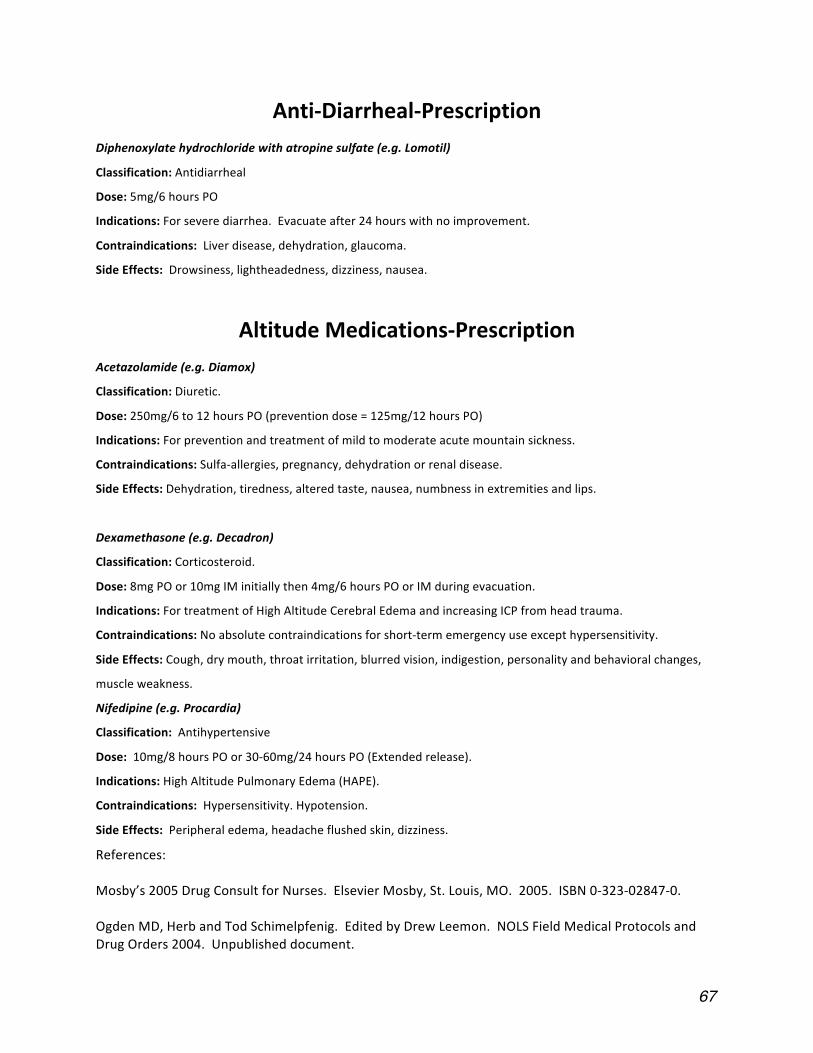
67
Anti‐Diarrheal‐PrescriptionDiphenoxylatehydrochloridewithatropinesulfate(e.g.Lomotil)
Classification:Antidiarrheal
Dose:5mg/6hoursPO
Indications:Forseverediarrhea.Evacuateafter24hourswithnoimprovement.
Contraindications:Liverdisease,dehydration,glaucoma.
SideEffects:Drowsiness,lightheadedness,dizziness,nausea.
AltitudeMedications‐PrescriptionAcetazolamide(e.g.Diamox)
Classification:Diuretic.
Dose:250mg/6to12hoursPO(preventiondose=125mg/12hoursPO)
Indications:Forpreventionandtreatmentofmildtomoderateacutemountainsickness.
Contraindications:Sulfa‐allergies,pregnancy,dehydrationorrenaldisease.
SideEffects:Dehydration,tiredness,alteredtaste,nausea,numbnessinextremitiesandlips.
Dexamethasone(e.g.Decadron)
Classification:Corticosteroid.
Dose:8mgPOor10mgIMinitiallythen4mg/6hoursPOorIMduringevacuation.
Indications:FortreatmentofHighAltitudeCerebralEdemaandincreasingICPfromheadtrauma.
Contraindications:Noabsolutecontraindicationsforshort‐termemergencyuseexcepthypersensitivity.
SideEffects:Cough,drymouth,throatirritation,blurredvision,indigestion,personalityandbehavioralchanges,
muscleweakness.
Nifedipine(e.g.Procardia)
Classification:Antihypertensive
Dose:10mg/8hoursPOor30‐60mg/24hoursPO(Extendedrelease).
Indications:HighAltitudePulmonaryEdema(HAPE).
Contraindications:Hypersensitivity.Hypotension.
SideEffects:Peripheraledema,headacheflushedskin,dizziness.
References:Mosby’s2005DrugConsultforNurses.ElsevierMosby,St.Louis,MO.2005.ISBN0‐323‐02847‐0.OgdenMD,HerbandTodSchimelpfenig.EditedbyDrewLeemon.NOLSFieldMedicalProtocolsandDrugOrders2004.Unpublisheddocument.
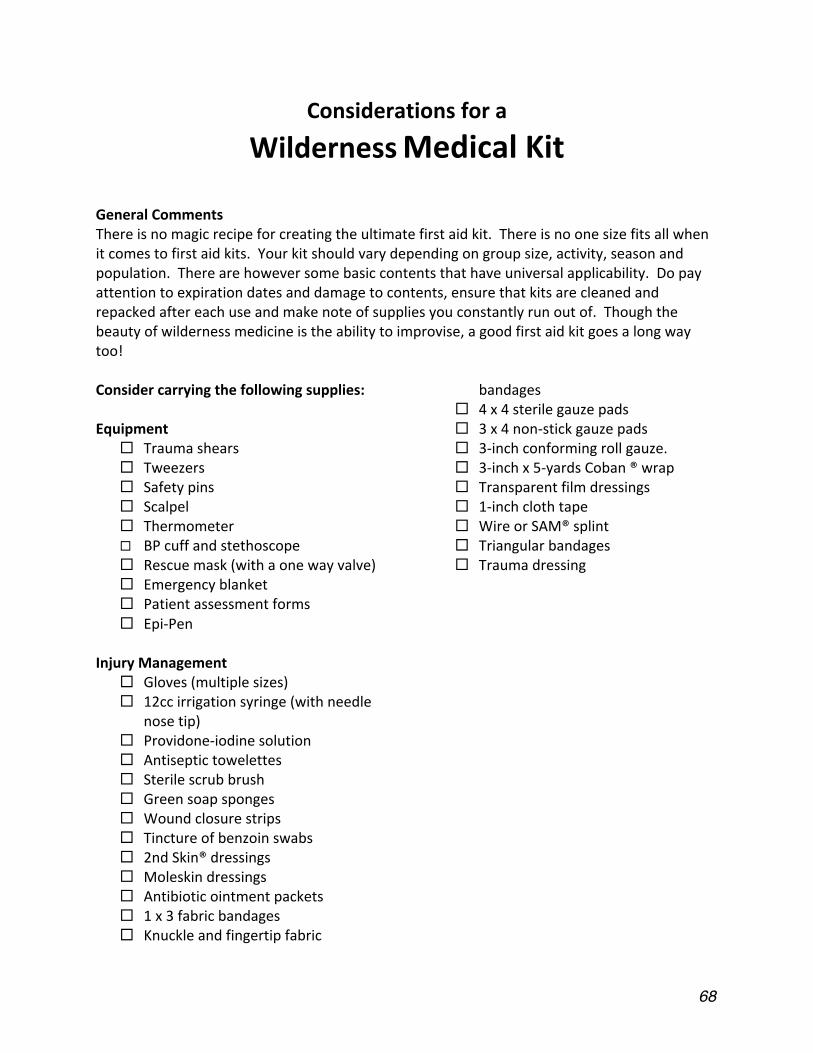
68
Considerationsfora
WildernessMedicalKit
GeneralCommentsThereisnomagicrecipeforcreatingtheultimatefirstaidkit.Thereisnoonesizefitsallwhenitcomestofirstaidkits.Yourkitshouldvarydependingongroupsize,activity,seasonandpopulation.Therearehoweversomebasiccontentsthathaveuniversalapplicability.Dopayattentiontoexpirationdatesanddamagetocontents,ensurethatkitsarecleanedandrepackedaftereachuseandmakenoteofsuppliesyouconstantlyrunoutof.Thoughthebeautyofwildernessmedicineistheabilitytoimprovise,agoodfirstaidkitgoesalongwaytoo!Considercarryingthefollowingsupplies:Equipment
Traumashears Tweezers Safetypins Scalpel Thermometer BPcuffandstethoscope Rescuemask(withaonewayvalve) Emergencyblanket Patientassessmentforms Epi‐Pen
InjuryManagement
Gloves(multiplesizes) 12ccirrigationsyringe(withneedle
nosetip) Providone‐iodinesolution Antiseptictowelettes Sterilescrubbrush Greensoapsponges Woundclosurestrips Tinctureofbenzoinswabs 2ndSkin®dressings Moleskindressings Antibioticointmentpackets 1x3fabricbandages Knuckleandfingertipfabric
bandages 4x4sterilegauzepads 3x4non‐stickgauzepads 3‐inchconformingrollgauze. 3‐inchx5‐yardsCoban®wrap Transparentfilmdressings 1‐inchclothtape WireorSAM®splint Triangularbandages Traumadressing
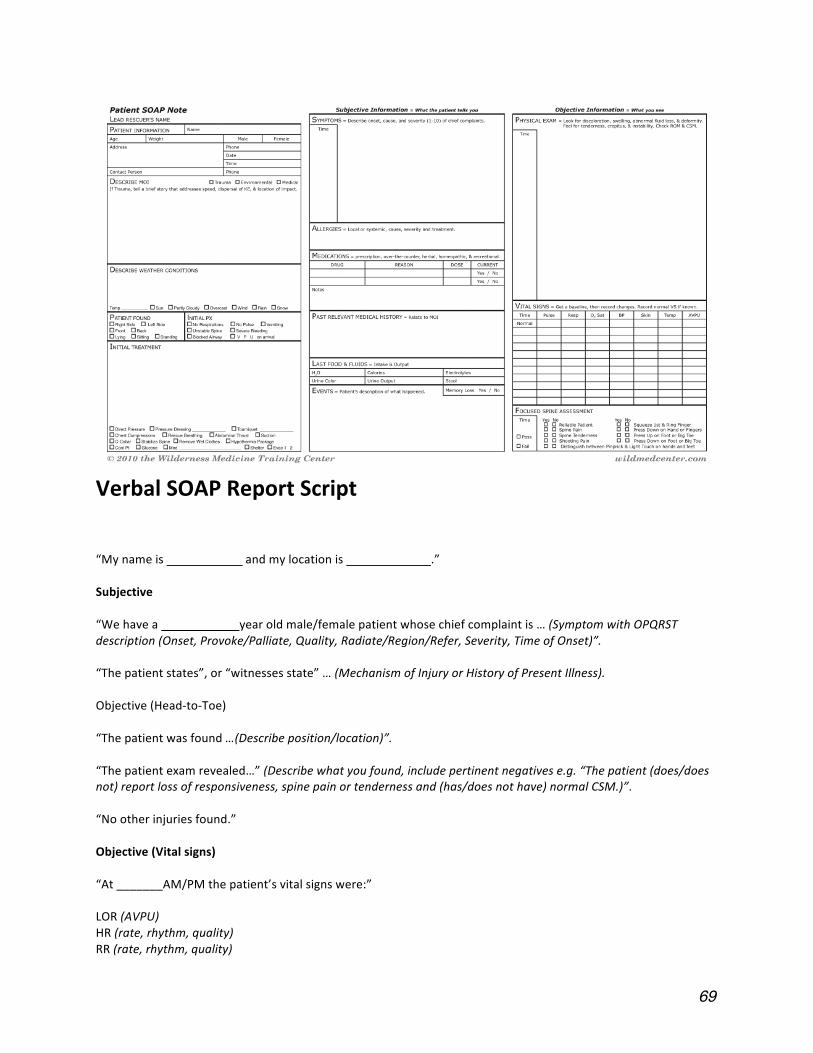
69
VerbalSOAPReportScript
“Mynameis andmylocationis .”Subjective“Wehavea yearoldmale/femalepatientwhosechiefcomplaintis…(SymptomwithOPQRSTdescription(Onset,Provoke/Palliate,Quality,Radiate/Region/Refer,Severity,TimeofOnset)”.“Thepatientstates”,or“witnessesstate”…(MechanismofInjuryorHistoryofPresentIllness).Objective(Head‐to‐Toe)“Thepatientwasfound…(Describeposition/location)”.“Thepatientexamrevealed…”(Describewhatyoufound,includepertinentnegativese.g.“Thepatient(does/doesnot)reportlossofresponsiveness,spinepainortendernessand(has/doesnothave)normalCSM.)”.“Nootherinjuriesfound.”Objective(Vitalsigns)“At_______AM/PMthepatient’svitalsignswere:”LOR(AVPU)HR(rate,rhythm,quality)RR(rate,rhythm,quality)
70
SCTM(color,temperature,moisture)BP(Systolic/Diastolic)Pupils(PERRL)TºObjective(PatientHistory)
“Thepatientreportedthefollowinghistory.”Symptoms:“Inadditiontothechiefcomplaintpatienthas….”Allergies:“Patientisallergicto….”Medications:“Patientistaking….”Pertinentmedicalhistory:“Patienthasahistoryof….”Lastintake/output:(Describerecenturine/boweloutput,waterandfoodintake.)Events:(Describepertinentrecenteventsoreventsthatmayhavecausedtheproblem.)Assessment“BasedonthisMechanismofInjurythereis/isnotapossiblespineinjury.”“Possibleproblemsinclude….”Plan“Basedonafocusedspineassessmentwehavedecidedtocontinue/discontinuespineimmobilization.”“Wewillimmobilize/treatthe by…(Describetreatmentforallpossibleproblems).”“Ourevacuationplanis....”“Werequestthefollowingsupplies/support…”Anticipatedproblems“Wewillmonitorfor…(Listanticipatedproblemsandresponses).“
71
SectionIV
Forms
72
Acknowledgement of Risk Form
ForusewithReedCollegeoutdoorprogrammingthatusesUnitedStatesForestServiceandtheNationalParksServicelandsandrivers.
MuchofthelanguageusedhereinwasadoptedfromtheNationalOutdoorLeadershipSchoolandotherorganizations’acknowledgementofriskforms.
Name:______________________________________ Date:___________________
Activity:________________________________________________________________
InconsiderationofTheReedInstitute,itsagents,employees,trustees,officers,contractorsandallotherpersonsorentitiesassociatedwithit(hereafterreferredtoas“ReedCollege”),Iagreeasfollows:
AlthoughReedCollegehastakenreasonablestepstoprovidemewithskilledstaffandappropriateequipmentfortheactivitythatIamabouttoundertake,Iacknowledgethatthisactivityhasrisk,includinginherentrisksthatcannotbeeliminatedwithoutdrasticallyalteringthecharacterofthisactivity.Thesameelementsthathelpcreatetheuniquecharacterofthisactivitymayalsobethesameelementthatcauseslossordamagetomyequipment,accidentalinjury,illness,orinextremecases,permanenttrauma,disabilityordeath.IunderstandthatReedCollegedoesnotwanttoreducemyenthusiasmfortheactivity,butthinksthatitisimportantformetobeinformedinadvancedabouttheactivities’inherentrisks.Thefollowdescribesmany,butnotall,ofthoserisks.
ReedCollege’soutdoorclassesandrecreationalactivitiesgenerallytakeplaceintheoutdoorenvironmentwhereparticipantsaresubjecttonumerousrisks,bothenvironmentalandotherwise.Activitiesmayvarydependingonthecourseoradvertisedevent,butoftenincludehiking,backpacking,mountaineering,rockandiceclimbing,rappelling,whitewaterraftingandkayaking,seakayaking,canoeing,bicycling,skiing,scubadivingorcaving.Otheractivitiesmaybeundertakendependingupontheintentoftheclassorouting.
Theseactivitiesmayoccurinremoteplacesasignificanttimeanddistanceawayfrommedicalfacilitiesordefinitivecare;thedifficultyofcommunicationandtransportationmaysignificantlydelayevacuationandtransporttoamedicalfacility.
Mealsareusuallypreparedoversmallportablestoves,althoughsometimesgroupsalsocookoveropenfires.ReedCollege’sstandardwatertreatmentprocessuseseitherboilingorhalides,specificallyacommercialformofiodinethatkillsmostvirusesandparasites,butmaynotkillcryptosporidium.Risksgenerallyassociatedwithcampingincludecuts,burns,blisters,diarrhea,flu‐likesymptoms,andfallingtimberorrock.
Travelisbyvehicle,onfoot,raft,kayaks,canoe,sailboat,horseback,skis,snowshoes,andbyothermeans.Thistravelmaybeoverroughunpredictableoff‐trailterrain,boulderfields,downedtrees,rivers,whitewaterrapids,steepslopes,slipperyrocks,snowandice,glaciatedterrain,oceantidesandcurrents,wavesandreefs.Associatedrisksincludecollision,slipping,falling,beinghitbyobjects,strikingobjects,capsizing,anddrowning,inadditiontoenvironmentalrisks.
Environmentalrisksandhazardsincluderapidlymoving,deeporcoldwater;insects,snakesandpredators;falling,rollingorshiftingrock;lightning,avalanches,flashfloods,rapidlychangingweather,andotherunpredictableforcesofnature.Possibleinjuriesmayincludedehydration,sunburn,heatexhaustionandheatstroke,frostbite,hypothermia,highaltitudeillnesses,andothermildorseriousconditions.
Decisionsaremadebytheinstructorsandstudents,oftenwhileimmersedinthewildernesscontext.Thesedecisionsaredependentuponavarietyofperceptionsandevaluationsthatbytheirnatureareimpreciseand

73
subjecttoerrorinjudgement.Studentsmayexperienceunsupervisedtimeduringperiodswheretheinstructorisnotneededfortheirtechnicalexpertise.Atallpointsintimethestudentsareresponsiblefortheirownsafety,andshouldalsotakeownershipforthesafetyofotherstudentsontheexperience.
IamawarethattheproposedReedCollegeactivityincludestheriskofinjuryordeathtomyself.Irecognizethatthedescriptionofrisksgivenaboveisnotcomplete,andthatotherunknownorunanticipatedrisksmayresultinpropertyloss,injury,ordeath.Iagreetoassumetheresponsibilityfortheinherentrisksinthisactivity,boththoseidentifiedinthisdocumentaswellasthosenotidentified.Myparticipationinthisactivityisvoluntary,thatnooneisforcingmetoparticipate,andthatIamparticipatingwithfullknowledgeoftheinherentrisks.IamawarethatthereareotherclassesoractivitiesthatIcouldtakeordoinstead.
IdeclarethatIamgoodenoughphysicalfitnesstoparticipateintheactivityoutlinedabove.IfIhavemedicalconcernsrelatedtotheactivity,IhaveverifiedwithmyphysicianthatIamphysicallyandpsychologicallyabletoparticipateintheexperience.Allinformationonthemedicalformistrueandcompletetothebestofmyknowledge.IauthorizeReedCollegetoobtainorprovideemergencyhospitalization,surgical,ormedicalcareforme.
IrepresentthatIamfullycapableofparticipatinginthisactivitywithoutcausingharmtomyselforothers.Therefore,I,andmyparent(s)orguardian,ifIamaMinor,assumeandacceptfullresponsibilityformeandforinjury,death,andlossofpersonalpropertyandexpensessufferedbymeandthemasaresultofthosedangersandrisksidentifiedherein,andthoseinherentrisksanddangersnotspecificallyidentified,andasaresultofmynegligenceinparticipatinginthisactivity.
I,andmyparent(s)orguardian,ifIamaminor,haveread,understood,andacceptedthetermsandconditionstatedhereinandacknowledgethatthisagreementshallbeeffectiveandbindinguponmyself,myheirs,assigns,personalrepresentativeofestate,andallofmyfamilymembers.
PrintedName
Signature Date
Ifthestudentisunder18,Iamsigningthisasparentorguardiantoreflectmyagreementtoindemnify(thatis,protectbypaymentorreimbursement)Reedfromanyclaimwhichmaybebroughtbyoronbehalfofthestudent,oranymemberofthestudent’sfamily,forinjuryorlossresultingfromthoseinherentrisksoftheactivity,describedandnotdescribedabove,andfromthenegligenceofthestudent.
PrintedName
Signature Date
InAddition:
Waiver and Release
AlargepercentageoftheUnitedStatesForestService,theNationalParksService,andotherfederallandmanagementagenciesdonotallowserviceproviderssuchasReedCollegetobereleasedbytheirstudentsfromliabilityforinjuryorotherlossesoccurringoncertainpubliclands.InthoseareasReedCollegeislimitedtotheattachedAcknowledgementofRiskform.Youractivitymayincludetravelandactivitiesthatisnotonthesepubliclands;ReedCollegeseeksadditionalprotectionforthistravelandactivities.
Pleasereadthefollowingcarefullyandsignbelow:
IhavereadandunderstandtheattachedAcknowledgementofRiskagreement,andconfirmitsrepresentationsandagreetoallitsprovisionsasthoughtheywerefullysetforthinthisdocumentagain.
74
Exceptwithrespecttoaninjurythatoccursonpubliclandswhoserulesandregulationsprohibitmydoingso,Iacknowledgeandassumeallrisksofthecourseoractivity,knownorunknown,inherentorotherwise.InadditionIagree,formyself,myheirsandmypersonalrepresentatives,todefend,holdharmless,indemnify,releaseandforeverdischargeReedCollege,anditscurrentandformertrustees,officers,employees,agents,insurers,successorsandassigns(hereinaftercollectivelyknownas“representatives),fromandagainstanyandallclaims,demands,actionsorcausesofactions,whetherknoworunknown,relatingtoorarisingoutoforinconjunctionwithanydamage,deathorotherconsequencestorealorpersonalproperty,anyaccident,illness,personalinjury,deathorotherconsequencesthatmayresultinmyparticipationintheactivities,orparticipationofanyotherparticipant,whethersuchactionisauthorizedasapartoftheactivitiesorwhethersuchdamageorotherconsequenceiscausedbythefaultornegligenceofReedCollegeoritstrustees,officers,employees,oragents.
Clearthinkingisnecessaryforthisactivity,thereforeIagreetoabstainfromtheuseofalcoholornon‐prescriptiondrugsbeforeandforthedurationoftheactivity.AdditionallyIaffirmthatIhavenochroniccondition,disability,orotherhealthconcernsthatwouldmakemyparticipationintheseactivitiesinadvisable.
IagreetosubmitanydisagreementunderthisWaiverandReleasefirsttoconfidentialmediation.Ifconfidentialmediationdoesnotresolvetheissue,Iagreetosubmitthedisagreementtobindingarbitration.ThisarbitrationshalltakeplaceinPortland,OregonandshallbeconductedaccordingtotherulesoftheAmericanArbitrationAssociation.Theprevailingpartyinanyarbitrationshallbeentitledtorecoveritsattorneys’andexpertfeesandothercosts,disbursementsandexpensesincurredbeforeandduringarbitration,asthearbitratormayadjudgereasonable.Further,IagreethatthisreleaseshallbegovernedbyandconstruedaccordingtothestateofOregon.
IunderstandthatthisreleaseisvoluntaryinthatthereareotherclassesoractivitiesthatIcouldchoosetoundertake.Ihavereadthisreleaseandunderstanditfully.IunderstandthatsigningthisreleaseisaconditionofmyparticipationintheactivitiesandthatthisWaiverandReleaseislegallybindingonme.And,Iunderstandthat,amongotherthings,IamagreeingtoindemnifyReedCollegeanditsrepresentativesforinjuries,damagesorlossesthattheymaycauseandgivingupcertainrightstosueReedCollegeanditsrepresentativesforinjuries,damages,orlossesthatImayincur.
IASSUMEALLRISKSASSOCIATEDWITHTHEACTIVITIES,WHETHERORNOTSPECIFIEDINTHISWAIVERANDRELEASE,ANDUNDERSTANDTHATREEDCOLLEGEISNOTAGUARANTOROFMYSAFETYINCONNECTIONWITHMYPERFORMANCEOFTHEACTIVITIES.
Inwitnessthereof,Ihavecausedthisreleasetobeexecutedthis__________dayof__________________,20___.
PrintedName
Signature Date
Theparentorguardianmustsignbelowifthestudentisunder18yearsofage.InconsiderationofReedCollege’sallowingthestudenttoparticipateintheactivity,theundersignedparent(s)orguardianagreetoreleaseReedCollegefromanyclaimtheparent(s)orguardianmayhavebecauseofinjuryorlosssufferedbythestudent,includinginjuryorlossclaimedtobecausedbythenegligenceofReedCollege.Inaddition,theparent(s)orguardianagreetoprotectandindemnifyReedCollegefromanyclaimandrelatedexpensesorfees,broughtatanytimebythestudentorbyanyoneonthestudent’sbehalf,orbyanymemberofthestudent’sfamily,orbyanothercourseparticipant,arisingoutofthestudent’senrollmentorparticipationintheactivity.Theundersignedalsoagreetothetermsofmediationandarbitrationoutlinedabove.ThisindemnityincludesclaimsofReedCollege’snegligence.
PrintedNameofParent(s)orGuardian
Signature Date
Signature
75
Health and Diet Questionnaire ReedOutdoorProgramandEducation(R.O.P.E.)
Thisinformationisforthetripleaders’informationonlyandiscompletelyconfidential
Name:_________________________________Trip:_____________________________________
Phone(school):_________________
EmergencyContact:_______________________________________Relationship:________________EmergencyContactPhone:(___)_________________
R.O.P.ETripInformation
ReedOutdoorProgramandEducationTripscanbemulti‐daywildernessexpeditionsinremotesettings,whereevacuationtomodernhospitalfacilitiesisnotimmediatelypossible.Youmustexpectextremeweatherconditionsrangingfromsnowstormstosleettoextremeheatandhumidity.Suddenenvironmentalchangesaretobeexpectedandanticipated.DependingonwhatactivityyoupursueinyourR.O.P.ETrip,youmayberequiredtocarryaheavyloadupuneven,steepterrain;paddleforextendedperiods;sleepoutdoors;experiencelong,toughdays;andpreparemealsandsetupcamp.Besurethatyouareabletoberesponsibleforyourself.
Participant:PleasecircleYESorNOforeachquestion.Eachmustbeanswered,butkeepinmindthata“YES”answerdoesnotnecessarilymeanyouwillnotbeabletoattendyourR.O.P.E.Trip.
GeneralMedicalHistory
Doyoucurrentlyorhaveyoueverhad:
1.Respiratoryproblems?Asthma? 1.YESNO
2.Gastrointestinaldisturbances? 2.YESNO
3.Diabetes? 3.YESNO
4.Hypertension? 4.YESNO
5.Bleedingorblooddisorders? 5.YESNO
6.Hepatitisorotherliverdiseases? 6.YESNO
7.Neurologicalproblems?Epilepsy? 7.YESNO
8.Seizures? 8.YESNO
9.Dizzinessorfaintingepisodes? 9.YESNO
10.Treatmentormedicationformenstrualcramps? 10.YESNO
11.Disordersoftheurinaryorreproductivetract? 11.YESNO
12.Anyotherhealthcomplaint?__________________ 12.YESNO
13.DoyouseeaMedical/Physicalspecialistofanykind? 13.YESNO
14.Areyoupregnant? 14YESNO
76
15.Treatmentorcounselingwithamentalhealthprofessional? 15.YESNO
16.Cardiacproblems? 16.YESNO
Diet
17.Areyouavegetarian? 17.YESNO
Ifyes,howstrictareyou?(willyoueatfishorchicken?Areyouvegan?)_________________________________________________________________________________
_________________________________________________________________________________
18.Ifyouarevegetarianorvegan,pleaselistsomeofthemealsthatyouparticularlyenjoy:__________
_________________________________________________________________________________
19.Pleaselistanyfoodsthatyouparticularlydespise:________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
Muscle/SkeletalInjuries
Doyoucurrentlyorhaveyoueverhad:
20.Knee,hip,ankle,shoulder,arm,orbackinjuries(includingsprains)and/oroperations?
Ifso,pleaseexplain:_______________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
Allergies/Medications
21.Anyallergies?Toinsectbitesorbeestings? 21.YESNO
Ifyes,pleaselistthem,alongwiththeirseverity:_________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
22.Areyouallergictoanymedications?____________________________ 22.YESNO
23.Areyoucurrentlytakinganymedications? 23.YESNO
Medication Dosage SideEffects/Restrictions
______________________________________________________________________________________________________
77
______________________________________________________________________________________________________
______________________________________________________________________________________________________
24.Yearoflasttetanusimmunization:______.Ifyoucannotremember,wasit
withinthepastfiveyears? 24.YESNO
TheReedOutdoorProgramandEducationrecommendacurrenttetanusimmunization
25.DoyouhaveahistoryoffrostbiteorAcuteMountainSickness? 25.YESNO
26.Doyouhaveahistoryofheatstrokeorotherheatrelatedillness? 26.YESNO
Fitness
27.Doyouexerciseregularly? 27.YESNO
Activity Frequency Duration/Distance IntensityLevel
(Easy/moderate/competitive)
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
28.Doyousmoke?Ifso,howmuch?_____________________________ 28.YESNO
29.Swimmingability(CHECKONE):___Non‐swimmer ___Recreational___Competitive
PLEASEREADCAREFULLYANDSIGN
Theinformationprovidedaboveisacompleteandaccuratestatementofanyphysicalandpsychologicalconditionswhichmayaffectmyparticipationinthistrip.Irealizethatfailuretodisclosesuchinformationcouldresultinseriousharmtomeandfellowparticipants.IagreetoinformtheReedOutdoorProgramandEducation(R.O.P.E.)shouldtherebeanychangeinmyhealthstatuspriortothestartofthetrip.Onthebasisofthebackgroundinformationatthebeginningofthisform,andwhatIknoworsuspectaboutmyphysicalandpsychologicalhealth,IamfullycapableofparticipatinginthisR.O.P.ETrip.
IunderstandthatifIhavethepotentialforasevereallergicreactiontobeestings,insectbites,food,poisonoak,orothersubstancesthatmightbefoundintheoutdoor,itismyresponsibilitytobringthepropermedicationwithmeonthistrip.
Participant’sSignature:______________________________________Date:___________________
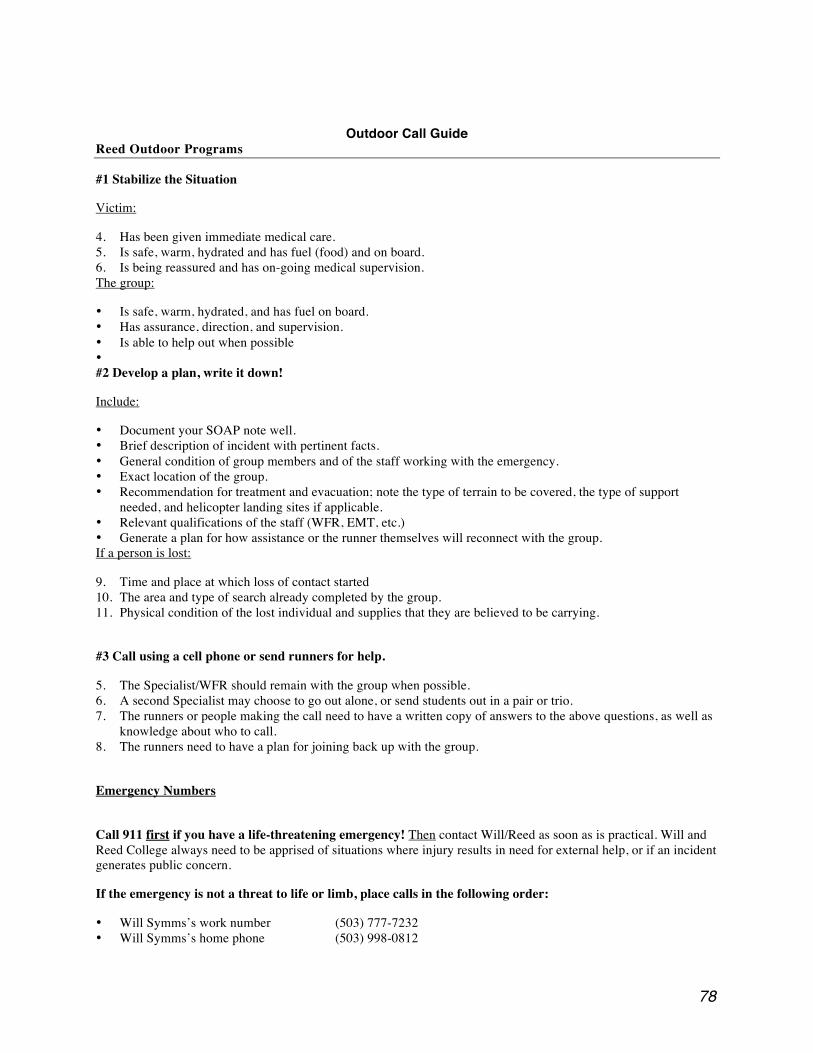
78
Outdoor Call Guide Reed Outdoor Programs
#1 Stabilize the Situation
Victim:
4. Has been given immediate medical care. 5. Is safe, warm, hydrated and has fuel (food) and on board. 6. Is being reassured and has on-going medical supervision. The group:
• Is safe, warm, hydrated, and has fuel on board. • Has assurance, direction, and supervision. • Is able to help out when possible • #2 Develop a plan, write it down!
Include:
• Document your SOAP note well. • Brief description of incident with pertinent facts. • General condition of group members and of the staff working with the emergency. • Exact location of the group. • Recommendation for treatment and evacuation; note the type of terrain to be covered, the type of support
needed, and helicopter landing sites if applicable. • Relevant qualifications of the staff (WFR, EMT, etc.) • Generate a plan for how assistance or the runner themselves will reconnect with the group. If a person is lost:
9. Time and place at which loss of contact started 10. The area and type of search already completed by the group. 11. Physical condition of the lost individual and supplies that they are believed to be carrying.
#3 Call using a cell phone or send runners for help.
5. The Specialist/WFR should remain with the group when possible. 6. A second Specialist may choose to go out alone, or send students out in a pair or trio. 7. The runners or people making the call need to have a written copy of answers to the above questions, as well as
knowledge about who to call. 8. The runners need to have a plan for joining back up with the group.
Emergency Numbers
Call 911 first if you have a life-threatening emergency! Then contact Will/Reed as soon as is practical. Will and Reed College always need to be apprised of situations where injury results in need for external help, or if an incident generates public concern.
If the emergency is not a threat to life or limb, place calls in the following order:
• Will Symms’s work number (503) 777-7232 • Will Symms’s home phone (503) 998-0812
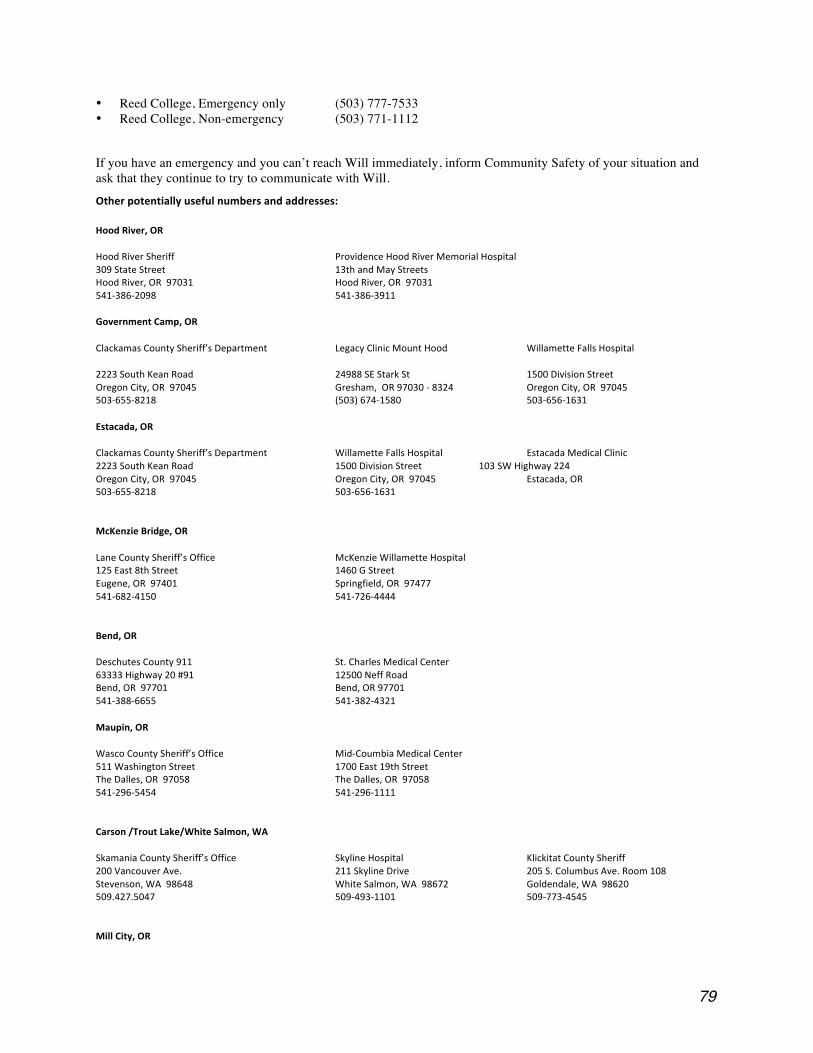
79
• Reed College, Emergency only (503) 777-7533 • Reed College, Non-emergency (503) 771-1112
If you have an emergency and you can’t reach Will immediately, inform Community Safety of your situation and ask that they continue to try to communicate with Will.
Otherpotentiallyusefulnumbersandaddresses:
HoodRiver,OR
HoodRiverSheriff ProvidenceHoodRiverMemorialHospital309StateStreet 13thandMayStreetsHoodRiver,OR97031 HoodRiver,OR97031541‐386‐2098 541‐386‐3911
GovernmentCamp,OR
ClackamasCountySheriff’sDepartment LegacyClinicMountHood WillametteFallsHospital
2223SouthKeanRoad 24988SEStarkSt 1500DivisionStreetOregonCity,OR97045 Gresham,OR97030‐8324 OregonCity,OR97045503‐655‐8218 (503)674‐1580 503‐656‐1631
Estacada,OR
ClackamasCountySheriff’sDepartment WillametteFallsHospital EstacadaMedicalClinic2223SouthKeanRoad 1500DivisionStreet 103SWHighway224OregonCity,OR97045 OregonCity,OR97045 Estacada,OR503‐655‐8218 503‐656‐1631
McKenzieBridge,OR
LaneCountySheriff’sOffice McKenzieWillametteHospital125East8thStreet 1460GStreetEugene,OR97401 Springfield,OR97477541‐682‐4150 541‐726‐4444
Bend,OR
DeschutesCounty911 St.CharlesMedicalCenter63333Highway20#91 12500NeffRoadBend,OR97701 Bend,OR97701541‐388‐6655 541‐382‐4321
Maupin,OR
WascoCountySheriff’sOffice Mid‐CoumbiaMedicalCenter511WashingtonStreet 1700East19thStreetTheDalles,OR97058 TheDalles,OR97058541‐296‐5454 541‐296‐1111
Carson/TroutLake/WhiteSalmon,WA
SkamaniaCountySheriff’sOffice SkylineHospital KlickitatCountySheriff200VancouverAve. 211SkylineDrive 205S.ColumbusAve.Room108Stevenson,WA98648 WhiteSalmon,WA98672 Goldendale,WA98620509.427.5047 509‐493‐1101 509‐773‐4545
MillCity,OR
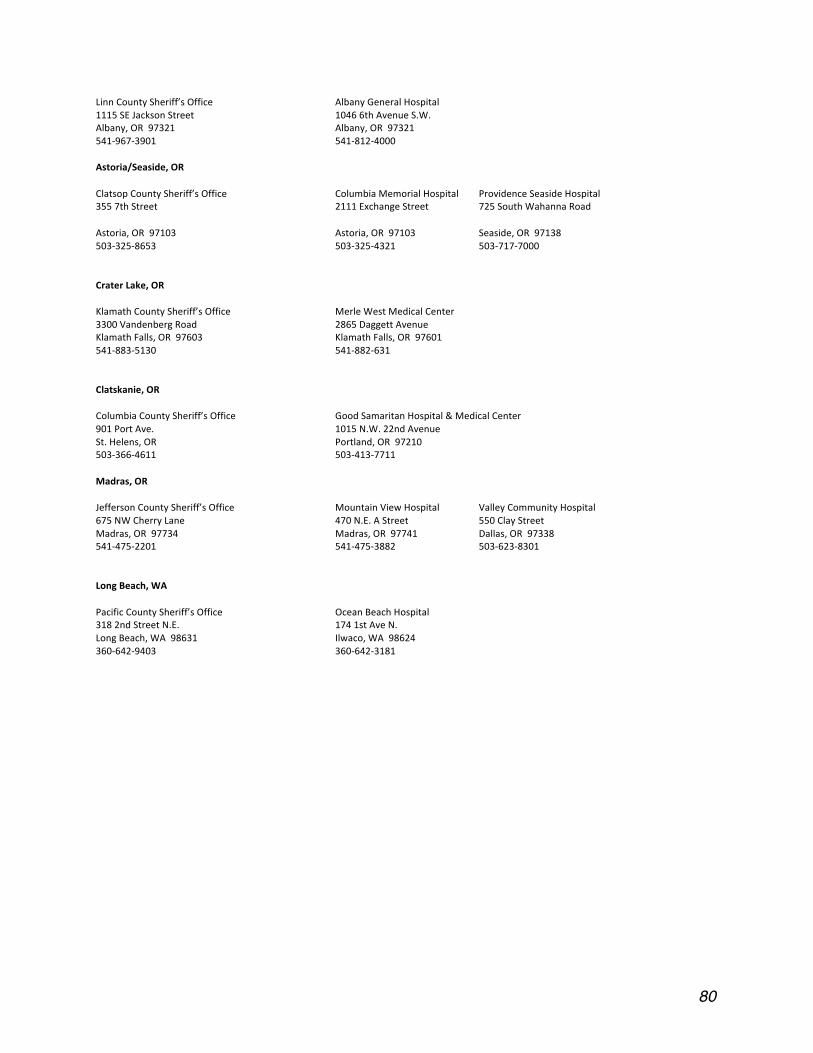
80
LinnCountySheriff’sOffice AlbanyGeneralHospital1115SEJacksonStreet 10466thAvenueS.W.Albany,OR97321 Albany,OR97321541‐967‐3901 541‐812‐4000
Astoria/Seaside,OR
ClatsopCountySheriff’sOffice ColumbiaMemorialHospital ProvidenceSeasideHospital3557thStreet 2111ExchangeStreet 725SouthWahannaRoad
Astoria,OR97103 Astoria,OR97103 Seaside,OR97138503‐325‐8653 503‐325‐4321 503‐717‐7000
CraterLake,OR
KlamathCountySheriff’sOffice MerleWestMedicalCenter3300VandenbergRoad 2865DaggettAvenueKlamathFalls,OR97603 KlamathFalls,OR97601541‐883‐5130 541‐882‐631
Clatskanie,OR
ColumbiaCountySheriff’sOffice GoodSamaritanHospital&MedicalCenter901PortAve. 1015N.W.22ndAvenueSt.Helens,OR Portland,OR97210503‐366‐4611 503‐413‐7711
Madras,OR
JeffersonCountySheriff’sOffice MountainViewHospital ValleyCommunityHospital675NWCherryLane 470N.E.AStreet 550ClayStreetMadras,OR97734 Madras,OR97741 Dallas,OR97338541‐475‐2201 541‐475‐3882 503‐623‐8301
LongBeach,WA
PacificCountySheriff’sOffice OceanBeachHospital3182ndStreetN.E. 1741stAveN.LongBeach,WA98631 Ilwaco,WA98624360‐642‐9403 360‐642‐3181