rhinoplasty, crooked nose - cloud object storage · emedicine.medscape.com emedicine specialties...
TRANSCRIPT

emedicine.medscape.com
eMedicine Specialties > Otolaryngology and Facial Plastic Surgery > Cosmetic Surgery
Rhinoplasty, Crooked Nose Steven H Dayan, MD, Clinical Assistant Professor, Department of Otolaryngology-Head and Neck Surgery, University of Illinois Anil R Shah, MD, Plastic Surgeon, Private Practice; Shefali I Shah, MD, Staff Physician, Department of Otolaryngology-Head and Neck Surgery, University of Illinois at Chicago Updated: Mar 18, 2009
Introduction
Problem
Correction of a twisted nose poses one of the greatest challenges in septorhinoplasty. Resulting from a myriad of causes, the surgeon's first task is to elucidate the etiology of the asymmetric nose and then plan surgical correction. In these circumstances, physicians must be able to make an accurate diagnosis to formulate an appropriate surgical plan. For proper and effective treatment, the surgeon must devise a therapeutic plan that takes into account balance, proportion, symmetry, and correction of nasal function.
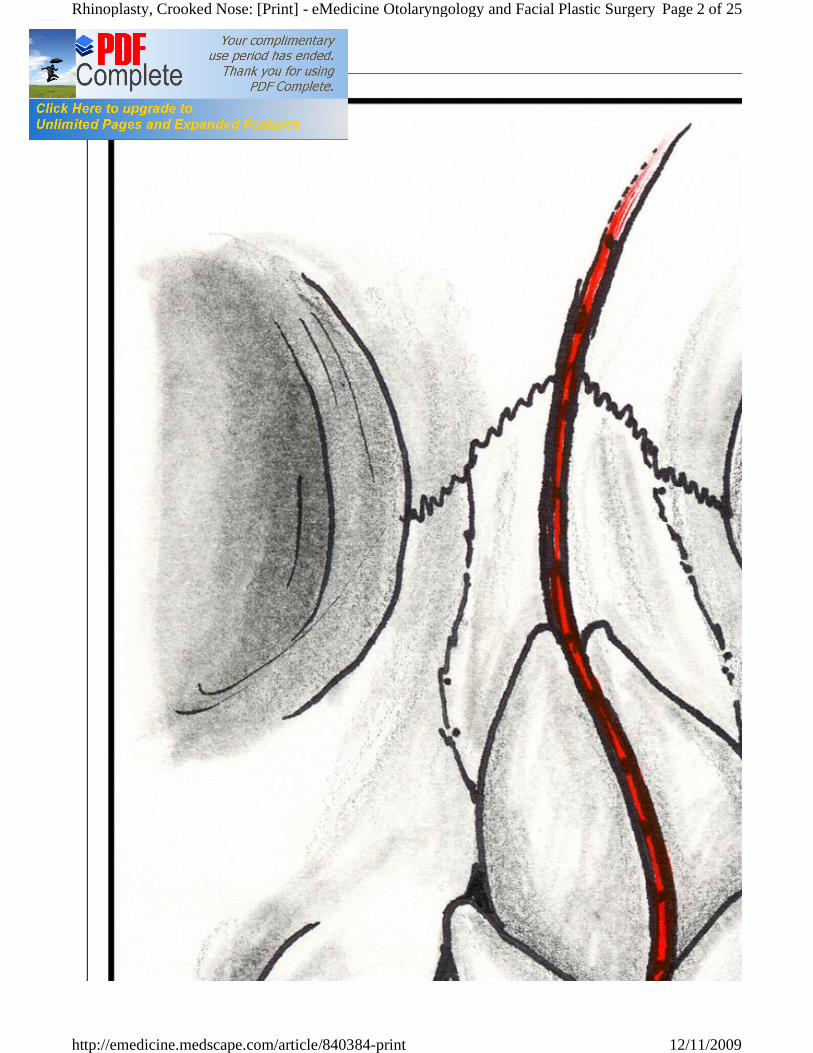
Familiarity with the crooked nose leads to appreciation of commonly associated anatomical abnormalities. Asymmetric noses are typically characterized by deviation of the bony upper third and/or the cartilaginous lower two thirds of the nose. Deviation is often sinusoid in nature (see Image 1), and the tip may or may not be midline.
Page 1 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
Page 2 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print

S-shaped crooked nose deformity.
These structural issues often contribute to nasal obstruction, further complicating optimal surgical management. Although one may be tempted to focus on contour deformities, adequate care must also involve complete correction of nasal obstruction.
Etiology
Trauma
Nasal bones are the most commonly fractured bones in the face, and fractured nasal bones are a leading cause of an asymmetric nose. Neglected or partially reduced nasal fractures usually result in a crooked nose associated with surface depressions and irregularities. These patients often present without prior medical attention, and many recount a history of progressive nasal changes following a traumatic event. Of the patients who do receive treatment following the incident, many find the treatment unsuccessful.
Patients with external nasal deformities frequently experience progressive nasal obstruction. Offending trauma leads to both septal deviation and disruption of traditional nasal support mechanisms. With loss of nasal support, internal and external nasal valve collapse may result.
Injury leading to a crooked nose may be secondary to a recent event or to years of scarring and contraction following previous trauma. Many people believe they were born with a deviated nose or that the condition was genetic; however, both patients and physicians alike frequently overlook childhood trauma as a common cause of crooked nose. Children are frequent recipients of trauma leading to progressive deviation. The noses of children are composed primarily of cartilage. The nasal bones are smaller, softer, more compliant, and capable of absorbing energy from the force of trauma.
Birth trauma may result in nasal septal deviation. Nasal septal deformities are estimated to occur in 1.25-23% of newborns. Forceps-assisted or breech delivery is often mentioned as the etiology of injury, but intrauterine forces may also be responsible for neonatal cartilage deformities. Fortunately, these deviations may be treated easily in the early neonatal period. A displaced septum can often be reduced at the bedside with a blunt forceps.
Nasal fractures commonly result from lateral forces. In this type of injury, the nose may appear deviated but is not. This illusion is caused by depression of a unilateral bony fragment. For example, unilateral trauma may in-fracture 1 nasal sidewall, creating the illusion of nasal dorsum deflection to the opposite side. This type of injury carries good prognosis for restoration of function.
A truly deviated nasal fracture occurs with greater frontal force and less lateral force. Greater force is needed from frontal impact to produce nasal fracture, as nasal bones are buttressed by frontal process of the maxilla, nasal spine, and perpendicular plate of the ethmoid. Direct frontal injury causes fracture and splays the nasal bones. The septum, which is the shock absorber of the nose, may fracture and be displaced from its pedestal. Nasal trauma associated with septal fracture requires a more extensive repair process.
Diseases of the septum and internal nose
Diseases of the septum and internal nose may cause resorption of supporting structures leading to collapse of nasal valves and deviation. Autoimmune or immunologic diseases are classic examples of disorders resulting in septal injury. Physicians may overlook this category of diseases while formulating a differential diagnosis of asymmetric nose etiology. Connective-tissue diseases play an important role in otolaryngology. Unless a correct diagnosis is made,
Page 3 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
many symptoms and anatomic abnormalities will recur or progress despite attempts at surgical correction.
Other diagnostic considerations include drug abuse and neoplastic processes. Nasal inhalation of cocaine leads to ulceration of nasal mucosa. With consistent use, mucosal atrophy and septal perforation may occur. In cases of neoplastic or polypoid disease, careful inspection of the nose reveals mucosal changes. Nasal bones and cartilage may become lateralized, creating asymmetries in the middle- and upper-third regions of the nose. The nasal surgeon needs to evaluate for these less obvious causes of a deviated nose.
Postsurgical
Many patients who seek either cosmetic or functional benefits of rhinoplasty are initially pleased with their new appearance. Years later, as the forces of healing begin to manifest, patients may become disappointed.
Rhinoplasty is a complex surgical procedure fraught with potential complications. Unfortunately, reduction rhinoplasty frequently results in loss of structural support and a weakened nose. A combination of scarring, gravity, and aging pulls the nose in different directions and can result in nasal collapse and deviation. Asymmetric or incomplete osteotomies result in deviation of the upper-third region of the nose and obvious step deformities. Despite complete and symmetric osteotomies, if the nasal structures responsible for the deviation are not corrected, the nasal pyramid may migrate back to its original position.
Surgical treatment of an operated nose can be difficult, as landmarks and tissue planes are unclear. The required approach and treatment plan must be strong in fundamental principles of returning nasal support and structure.
Presentation
Evaluation of the twisted nose begins with a thorough history and physical examination.
History
Symptoms of nasal obstruction, rhinitis, or epistaxis may indicate nasal valve collapse or septal deviation. Do not overlook medical or seasonal allergies, because such conditions are necessary components of a complete history.
Physical examination
The physical examination encompasses a systematic and thorough evaluation of the nose. Beginning with an external nasal exam, the nose is analyzed in relation to the entire face. Detailed and systematic facial analysis is a time-honored and learned skill that is instrumental in diagnosing structural nasal pathology. Evaluate symmetry and balance of facial aesthetic units separately and in conjunction with nasal structures. Balancing the nose against any asymmetries of the face is important. Skin type and patient age are also important factors that must be considered.
Narrow the focus to the nose and determine the nature of the deviation (ie, decide if it is a true deviation or an illusion secondary to a unilateral collapsed upper lateral cartilage). Appreciate involvement of the upper bony third of the nose and/or the middle cartilaginous vault.
Detailed attention and analysis of the nasal tip determines if the tip is midline or also deviated. Proper evaluation of the tip is a prerequisite to determining the most appropriate surgical approach. Palpation of the nose for bony irregularities, location of the anterior septal angle, and evaluation of tip support are integral parts of the physical exam. Basal view of the nose may highlight a caudal septum deviation.
During inspiration, watch for a collapsing ala, which impedes air entry. This is a sign of external valve collapse and is observed more commonly in individuals who have undergone aggressive reduction rhinoplasty. The crooked nose very often is driven by a deviating or fractured septum.
Page 4 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
Evaluation of the septal relationship to nasal turbinates is necessary, as compensatory turbinate hypertrophy can contribute to nasal obstruction. The attachment of the upper lateral cartilage to the septum ideally creates an angle of 9-15°. Any angle less than this suggests internal valve compromise.
If a positive Cottle maneuver, performed by retracting the cheek skin laterally, conveys relief from obstruction, suspect internal valve collapse. Acoustic rhinometry may objectively define this obstruction but has not been proven necessary in clinical practice.
A complete internal nasal examination, repeated with the aid of a topical decongestant, allows better visualization of the posterior and dorsal septum. Constriction of the nasal mucosa improves appreciation of obstructing etiology.
Following the history and physical examination, photographic documentation is performed. Photography plays a vital role in preoperative management of the asymmetric nose. It functions as a tool in diagnosis and planning of therapeutic procedures. Photography allows the surgeon to precisely record nasal abnormalities. With the aid of digital cameras and computer-generated imaging systems, surgical alterations may be demonstrated clearly to the patient.
Postoperatively, photography serves to document immediate outcome and functions as a historical record to follow surgical changes.
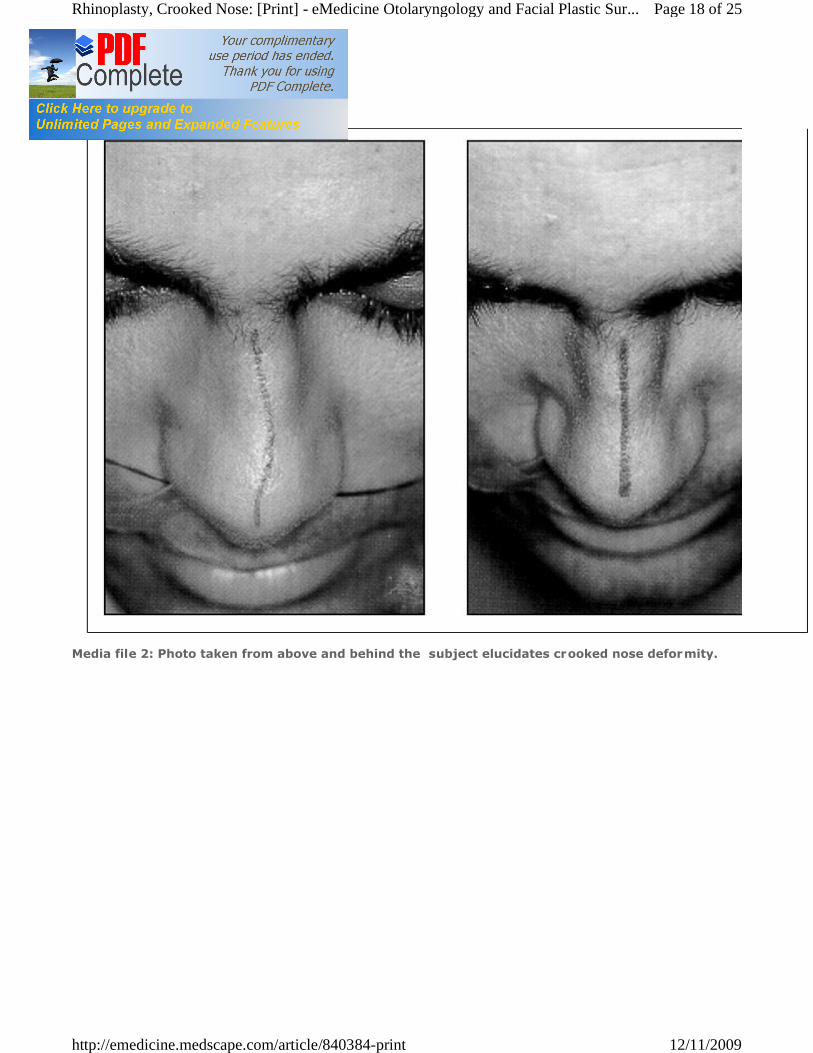
Photography may play a role in medicolegal issues. In addition to standard rhinoplasty photographs, other views are helpful in documenting the crooked nose. A photographic view from above and behind the nose is a good reference for intraoperative viewing (see Image 2). A straight object, such as a tongue blade, placed down the midline of the nose highlights asymmetries of the twisted nose. Another benefit may be obtained from a single light source, allowing for natural shadows that accentuate nasal deviation.
Page 5 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
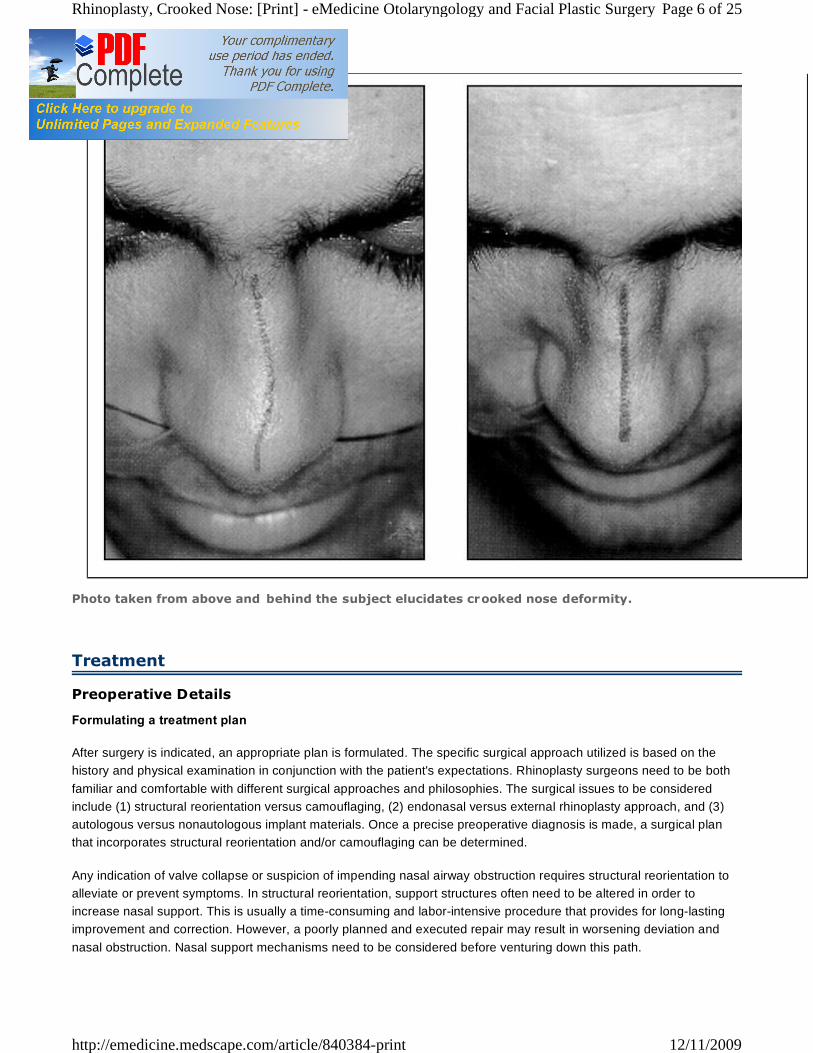
Photo taken from above and behind the subject elucidates crooked nose deformity.
Treatment
Preoperative Details
Formulating a treatment plan
After surgery is indicated, an appropriate plan is formulated. The specific surgical approach utilized is based on the history and physical examination in conjunction with the patient's expectations. Rhinoplasty surgeons need to be both familiar and comfortable with different surgical approaches and philosophies. The surgical issues to be considered include (1) structural reorientation versus camouflaging, (2) endonasal versus external rhinoplasty approach, and (3) autologous versus nonautologous implant materials. Once a precise preoperative diagnosis is made, a surgical plan that incorporates structural reorientation and/or camouflaging can be determined.
Any indication of valve collapse or suspicion of impending nasal airway obstruction requires structural reorientation to alleviate or prevent symptoms. In structural reorientation, support structures often need to be altered in order to increase nasal support. This is usually a time-consuming and labor-intensive procedure that provides for long-lasting improvement and correction. However, a poorly planned and executed repair may result in worsening deviation and nasal obstruction. Nasal support mechanisms need to be considered before venturing down this path.
Page 6 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print

Camouflaging techniques can be used alone or in conjunction with structural procedures. In camouflaging methods, an implant material is placed into a well-defined deformity, creating the illusion of correction. Camouflaging is a valuable technique in isolated deformities without nasal obstruction. This method may not achieve complete correction of the deviation, and the possibility of residual deformities and graft visibility remains. However, when this method is performed properly, it can be performed efficiently, and existing support structures are not jeopardized.
At times, the benefits of both techniques are used in tandem. Minor residual asymmetries that may follow structural reorientation procedures are amenable to camouflaging techniques.
Endonasal versus external rhinoplasty approach
Both the endonasal and external rhinoplasty approaches are used in correcting the deviated nose, but their indications may differ.
Many physicians have preference for one technique over another. The method that provides an individual surgeon with the best chance for successful outcome takes precedence. However, in general terms, the status of the tip and degree of septal deformity play an important role in determining the recommended approach.
A deviated tip or one that requires significant attention is better addressed by the external rhinoplasty approach. The external approach allows the surgeon to view tip structures in broad relief. Deviating septal forces or misaligned lower lateral cartilages are more readily apparent using the external rhinoplasty approach. Improved control and placement of cartilage grafts are benefits associated with the external approach.
The severely obstructed nose requiring reorientation of underlying support structures is more readily corrected using the external rhinoplasty approach. This approach allows complete visualization of nasal structures and provides the surgeon with the best chance for symmetric reconstruction. Stenting grafts are placed more easily using the external rhinoplasty approach, and stabilizing sutures can be placed with accuracy. However, the surgeon must realize that by opening the nose, existing support mechanisms will be compromised. Opening the nose also adds time to the surgical procedure. The often maligned transcolumellar incision scar has become a nonissue since meticulous closure and inapparent scar are the rule.
The endonasal approach to repair the twisted nose has more limited indications. In the absence of airway compromise, the deviated nose confined to upper- and middle-third regions of the nose can be treated using the endonasal technique.
An intercartilaginous incision allows access to the middle-third region without affecting a symmetric attractive tip. Precise pockets can be easily created for camouflaging grafts. Ideally, grafts are placed just above the perichondrium or just under the periosteum. If the implant is placed too superficial, it may become visible, palpable, and at risk for extrusion. Therefore, attention is given intraoperatively to delineating proper tissue planes. One must be especially vigilant in the previously operated or traumatized nose, in which correct tissue planes may be obscured.
Nasal obstruction associated with middle vault or bony deviation can be treated through an endonasal approach, albeit a difficult task for the expert and the occasional rhinoplasty surgeon. Stenting grafts are placed into precise pockets, and extensive septal work is performed through intranasal incisions. Overdeveloped or misplaced pockets may allow grafts to become visible or to migrate. This can result in worsening obstruction. However, when mastered, this technique provides an efficient and elegant method for correcting the deviated obstructed nose.
Implant materials
Some form of implant material may be required for correction of the deviated nose. The choice of implant is important in determining the ultimate outcome. Over the years, many different materials have been used, but little argument exists that the ideal implant material is autologous.
Page 7 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
Septal cartilage is the implant of choice because it has a proven track record and is harvested from the same surgical field. When septal cartilage reserves are limited, auricular cartilage is a good alternative. However, auricular cartilage is generally not firm enough to stent a buckled septum.
Curved conchal cartilage provides an appropriate shape for alar batten grafts and for filling dorsal concavities. In camouflaging techniques, crushing the cartilage improves malleability, allowing the cartilage to conform to existing structures. This may also increase resorbability. Some physicians maintain that resorbed cartilage is replaced with fibrous scar tissue. They contend that this scar tissue maintains the desirable shape and form created by the implant.
Firm, strong implants required for building support structures and reinforcing weakened ones can also be obtained from autologous sources. Costal cartilage and calvarial bone can be shaped to replace major support structures of the nose.
The confluence of the sixth, seventh, and eighth ribs provides ample material for use. Removing perichondrium and taking a center cut of cartilage helps to avoid warping of the graft. Smaller and thinner cartilage from the ninth, tenth, and eleventh ribs can also be used. Advantages of harvesting these ribs include decreased pain, decreased carving time, and reduced risk for pleural leak.
The benefits of autologous costal cartilage have to be weighed against potential morbidity of a chest wound and possible pleural violation. Before closing the chest wound, check the pleura for tears. The anesthesiologist can check for a pleural leak by increasing intrathoracic pressure after saline is irrigated into the surgical area. If a leak is present, bubbles will appear. Follow-up with a chest radiograph is recommended.
Calvarial bone is harvested from the parietal scalp and can be sculpted with a rotating drill. However, its use as a dorsal graft may feel unnatural, and dural violation, although rare, is a known risk.
Although autologous materials are implants of choice, the associated increased operating time and morbidity may not be consistent with the nature of the procedure, especially when performing minor camouflaging improvements.
If septal and auricular cartilage are not available, and the patient is unwilling to undergo costal cartilage or calvarial bone harvest, homologous irradiated rib graft material may be useful. This material has been used successfully at the University of Illinois for the last 10 years.
Both resorption and successful reconstruction have been reported with long-term follow-up. Although Welling found a resorption rate of 75%, Kridel and Konoir proved that irradiated rib graft used in nasal reconstruction benefits 97% of patients. Resorption was rare; however, when it did occur, resorption was associated with infection. In individuals judged to have resorption, graft material was replaced with fibrous tissue, allowing for maintenance of form. This material was treated with irradiation to decrease the risk for viral transmission.
Similar to harvesting autologous costal material, perichondrium is removed, and a center cut is used to prevent warping.
Acellular dermis (AlloDerm) has been used extensively for the last 5 years at the University of Illinois to camouflage minor irregularities of the dorsum. When excess autologous fascia or soft tissue is unavailable, AlloDerm draped over dorsal irregularities can provide a smooth dorsum. It can also be rolled into a desirable shape to help camouflage a specific defect. Since the implant is acellular, the risk of viral transmission is highly unlikely.
Alloplastic materials, such as silicone and Medpor, have poor track records because such materials may extrude and become infected. In addition, these materials may feel or appear unnatural. Gore-Tex, however, when restricted to the dorsum, has been used successfully to camouflage defects. Gore-Tex is soft and pliable and promotes easy carving, shaping, and handling. It fits nicely into precise pockets and allows for tissue ingrowth. Furthermore, it can be easily removed if necessary.
Page 8 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print

Although Gore-Tex is considered a safe material, the discerning physician must recognize its potential for rejection, infection, and extrusion. When placed in the tip, risk for exposure and infection is amplified. Godin reported a 2.2% infection rate with Gore-Tex placement into the nose. Soaking the implant in antibiotic solution and attention to sterile technique may decrease risk of infection.
Intraoperative Details
Correcting the deviated septum
A crooked nose is almost always associated with a crooked septum. Anderson felt that every crooked nose had an underlying septal deformity. Perhaps the most difficult problem to correct is the deviated nose caused by a fractured, buckled, or deviated dorsal septum. Crooked noses treated without addressing a deviated septum may lead to persistent deviation.
In the crooked nose, the posterior septum is usually closer to the midline than the dorsal edge. Therefore, the greater the dorsal resection, the closer the new septal edge is to midline. Constanian, recognizing this common anomaly, recommended removing existing dorsal humps first. Tardy also stressed the importance of correcting septal deformities as the initial surgical event.
Deviating cartilage not included in the vital 1.5 cm dorsal caudal L strut can be resected without concern for loss of middle-vault support. Bony obstruction and deviations of the perpendicular plate of the ethmoid and vomer may be rongeured gently.
Deviations and spurs isolated to the center of the septum contribute more toward symptoms of airway obstruction than to external nasal appearance. When the dorsal caudal L strut is also included in the deviation, greater septal contribution is made to the overall appearance of the crooked nose.
When resection alone is not adequate or desirable to strengthen the deviated septum, scoring the concave side of septal cartilage may release the spring. Permanent Mustarde-type mattress sutures also may be helpful to correct septal deviations.
The caudal anterior septum is often displaced off the maxillary crest, which results in tip deviation. Corrective efforts include swinging the septum back onto its pedestal. This is performed by excising a triangular wedge of cartilage from the inferior septum at the posterior septal angle. The septal base is then stabilized to the maxillary crest periosteum with a strong, permanent suture.
Bilateral stenting sandwich grafts may be necessary to provide support and form to a weakened or flaccid deviating septum. Stenting grafts are also indicated following resection of a vertical wedge of deviating septum that extends up to and through the dorsal septal edge. This dorsally bisected and deviated septum needs to be reconstituted to prevent middle vault collapse.
Place stenting sandwich grafts in the submucoperichondrial plane. When placed on both sides of the deviation, the stents provide a straight and reinforced septum. These grafts can be created from a strong piece of excised septal cartilage or bony perpendicular plate of ethmoid bone. If using bone, small holes can be drilled into the bone with a 3-mm drill bit. Care must be taken when performing this procedure on ethmoid bone because it is fragile and may fracture easily.
Strong, permanent suture is used to secure the stenting grafts that sandwich the flimsy, fractured, and weakened septum. Although firm, straight, resected septum is the stenting material of choice, costal cartilage, calvarial bone, iliac crest, and irradiated rib have all been used successfully. In the severely deviated septum too weak to support surrounding structures, subtotal septal reconstruction may be necessary.
Page 9 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Surgery
12/11/2009http://emedicine.medscape.com/article/840384-print
Dorsal 1-1.5-cm septal strut is necessary for maintaining structure and form to the nose. Failure to maintain this L strut results in saddling, columellar retraction, and tip ptosis. In these situations, the vital 1.5-cm septal L strut needs to be reconstituted. Through the external approach, the deformed septum can be removed and the L strut replaced with harvested material. Costal cartilage is the author's material of choice. Others have success with calvaria bone and irradiated rib. Costal cartilage has the benefit of being outside the nasal field, allowing for harvest by a second team while the nose is being opened.
In subtotal septal reconstruction, cartilage can be fashioned into an L strut and sutured to remaining cartilage. The caudal end of the graft can be secured to the maxillary crest if necessary. The tip may then be set at the desired projection and rotation.
Structural reorientation through endonasal approach
In cases in which a twisted nose is accompanied by a lateral wall defect causing obstruction, treatment may be performed via the endonasal approach. Although visualization is less than with the external rhinoplasty approach, combination of structural stenting and camouflaging may be adequate to achieve a straight dorsum. This approach allows for functional improvement without disrupting a well-supported tip.
Spreader grafts, often harvested from septal cartilage, measure 8-25 mm in length, 3-6 mm in height, and 1-4 mm in thickness. The grafts are placed into a precise submucoperichondrial pocket adjacent to the septum, in between the upper lateral cartilage and septum. This splint increases internal valve angle, opens the airway, and provides symptom-free breathing. Making sure that the pocket extends up to the dorsum is important; otherwise, this graft can potentially worsen obstruction. However, unlike spreader grafts placed via the external approach, internally placed grafts provide little width to the nasal dorsum. This can be a potential advantage in the already appropriate sized nose.
Once obstruction has been remedied, attention turns toward correcting residual asymmetries that contribute to the crooked appearance of the nose. Placing camouflaging onlay grafts is a valuable technique for balancing dorsal irregularities and creating the illusion of a straight nose.
Intercartilaginous incisions provide access to the supraperichondrial plane through which dorsal onlay grafts are placed. To prevent migration, a precise pocket is created. If uncertainty exists with regard to stability of the graft, transcutaneous sutures can be used. A 5-0 Prolene suture placed through the skin, the graft, and back through the skin is tied loosely over a nonadhesive gauze bolster. This suture is removed 5-7 days later.
The endonasal approach is a valuable method in treating the deviated nose. However, when severe obstruction exists, or nasal deviation is secondary to a deformed septum, correction is better performed through an external approach.
Structural reorientation through an external approach
All deviated noses can be treated with an external approach, although this may not always be necessary. Most deviated noses have a component of nasal obstruction, deflected septum, and asymmetric nasal tip. In these situations, camouflaging techniques alone are not adequate or appropriate to improve airway compromise and severe deviation. Therefore, an external approach, including structural reorientation, is the procedure of choice.
Care must be taken when opening the nose to identify cartilage that may be encased in scar tissue. Disrupted scarred tissue planes can make dissection more difficult and lead to increased bleeding and postoperative edema. Principles of patience and meticulous dissection are necessary for a successful surgical outcome.
After raising the skin-soft tissue envelope over the tip and mid dorsum, elevate the midline dorsal periosteum. This effectively releases underlying structures from the skin-soft tissue envelope. Prior to performing any reconstructive techniques, release all structural attachments. The scroll is divided as lower lateral cartilages are released from upper lateral cartilages. Medial and intermediate cruses of the lower lateral cartilages are released from septal attachments
Page 10 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
and from each other. Upper lateral cartilages are released from septal attachments. After freeing all attachments, deviating structures can be identified, isolated, and corrected.
On occasion, releasing the attachments is all that is necessary to allow components to spring back into the midline. More often, a persistently deviated septum is encountered. Septal corrective maneuvers, as described earlier, can then be instituted.
The twisted nose frequently has a narrowed middle vault component and, at times, has a compromised valve. Although these defects improve following septal corrective measures, further treatment is usually necessary to obtain a straight nose and functional airway.
Placement of spreader grafts is a reliable and long-lasting method to obtain increased dorsal width and enlarge the internal valve area. Spreader grafts are placed between the septum and upper lateral cartilage. Common indications forplacement of spreader grafts include a lateral traumatic force that has created an illusion of a deviated nose or a fractured septum that has buckled to one side, creating a true deviation to the opposite side. With time, the deviation worsens, and internal valve collapse occurs, leading to nasal obstruction.
Unilateral dorsal concavity that persists despite septal correction and stenting grafts may be corrected effectively with a planoconvex spreader graft placed in between the upper lateral cartilage and septum. Although the graft can be placed through an endonasal approach, placement of this graft is facilitated by the external approach. Greater correction of the concavity is achieved through the external approach because the upper lateral cartilage is displaced further laterally. This graft is sandwiched between the upper lateral cartilage, dorsal septum, and the other upper lateral cartilage. Spreader grafts will improve airway obstruction, widen the dorsum, and correct concavity.
Several authors describe techniques for balancing the asymmetric middle vault. Pontius describes placement of a sidewall spreading suture that lifts a depressed upper lateral cartilage with a suture to the opposite nasal bone. A triangular spreader graft is occasionally used with this technique. Similarly, Dayan describes a suture from the nasal bones to the upper lateral cartilage with a unilateral spreader for dorsal septal asymmetries. Both Guyuron and Toriumi both describe a differential septal suture for correcting minor deformities of the middle vault. By differentially suturing the upper lateral cartilages to the spreader graft/septum complex, vectors can be created to pull the middle vault in the necessary direction.
Camouflaging onlay grafts may mask any remaining minor asymmetries of the dorsum. Onlay grafts can be fixated easily and accurately with 5-0 polydioxanone (PDS) suture in the external approach.
Tip work usually follows once a straight dorsum is attained. Tip straightening, sculpting, and support reconstitution of tip support are routine measures used to create symmetry. A skin-soft tissue envelope is closed over the stable corrected dorsum.
A period of edema and healing is routine and has to be explained fully to the patient. At the University of Illinois, patients are told that the nose will only achieve 70% of its healing capacity at 1 year and that further healing and contraction can be expected up to and after the first year.
Management of a crooked bony dorsum
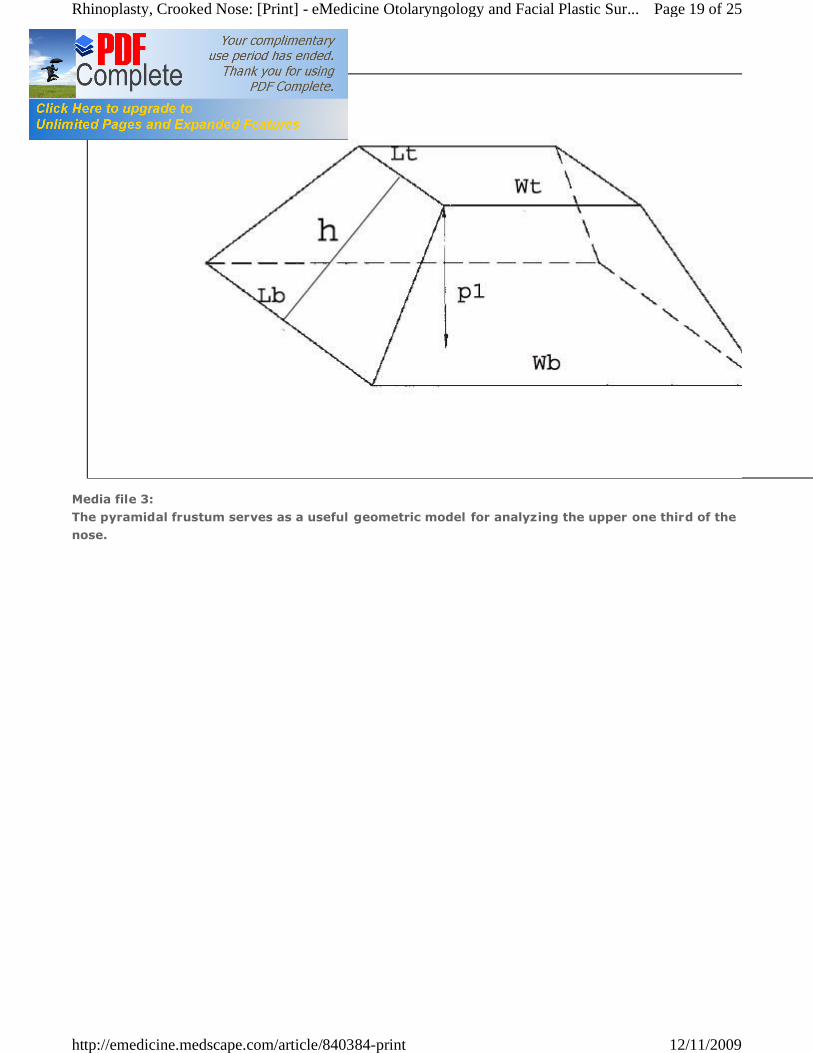
Properly evaluating the bony upper-third region of the nose is important; at times, this region is the sole deviating factor of a crooked dorsum. Other times, the upper-third region of the nose contributes to deviation by directing the middle vault in the opposite direction. The upper one third of the nose can be likened to a pyramidal frustum (also known as a truncated pyramid). By analyzing the various lengths of each side, the rhinoplasty surgeon can choose the precise location and number of osteotomies to be performed.
The severely deviated bony dorsum is best corrected first (see Image 3). This provides a base on which the middle-
Page 11 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
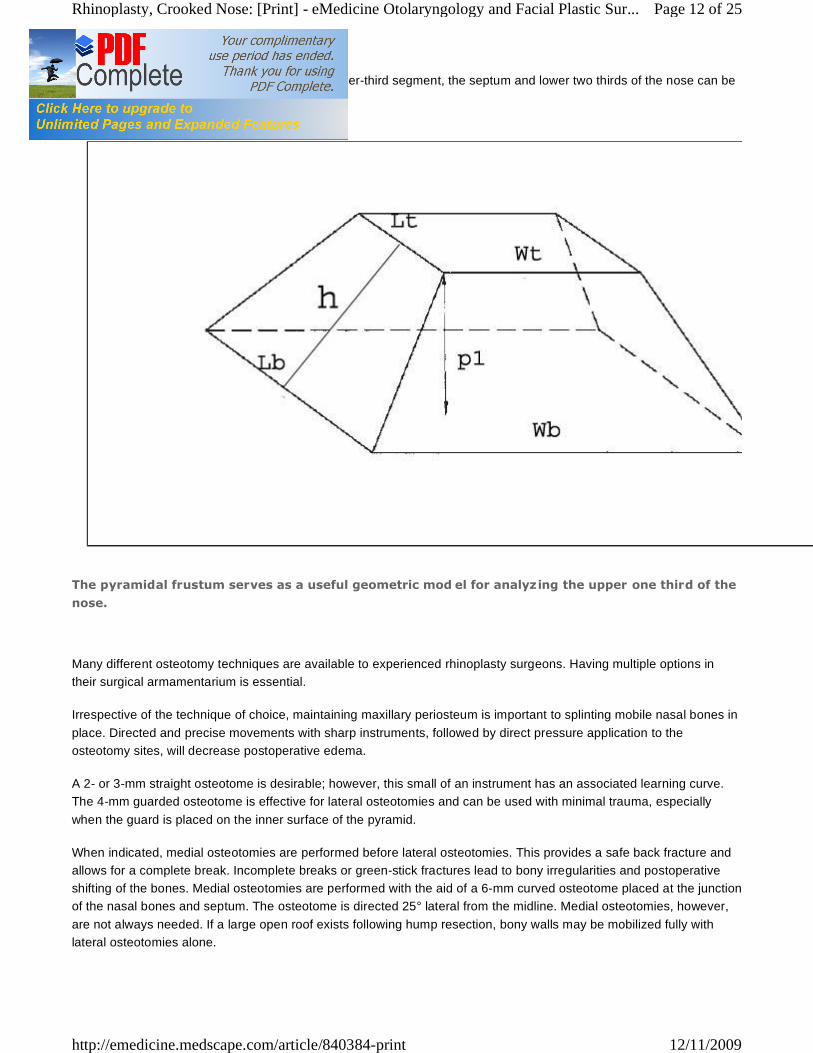
third region can be set. In the mildly deviated upper-third segment, the septum and lower two thirds of the nose can be addressed first.
The pyramidal frustum serves as a useful geometric mod el for analyzing the upper one third of the
nose.
Many different osteotomy techniques are available to experienced rhinoplasty surgeons. Having multiple options in their surgical armamentarium is essential.
Irrespective of the technique of choice, maintaining maxillary periosteum is important to splinting mobile nasal bones in place. Directed and precise movements with sharp instruments, followed by direct pressure application to the osteotomy sites, will decrease postoperative edema.
A 2- or 3-mm straight osteotome is desirable; however, this small of an instrument has an associated learning curve. The 4-mm guarded osteotome is effective for lateral osteotomies and can be used with minimal trauma, especially when the guard is placed on the inner surface of the pyramid.
When indicated, medial osteotomies are performed before lateral osteotomies. This provides a safe back fracture and allows for a complete break. Incomplete breaks or green-stick fractures lead to bony irregularities and postoperative shifting of the bones. Medial osteotomies are performed with the aid of a 6-mm curved osteotome placed at the junction of the nasal bones and septum. The osteotome is directed 25° lateral from the midline. Medial osteotomies, however, are not always needed. If a large open roof exists following hump resection, bony walls may be mobilized fully with lateral osteotomies alone.
Page 12 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print

Lateral osteotomies are usually performed in a high-low-high direction. This path allows for protection of the nasal airway at the nasal base by initiating osteotomy at an elevated (high) position on the pyriform aperture. This leaves a triangle of bone at the base of the pyriform aperture (Webster triangle), avoiding compromise of the nasal airway width. The osteotome then travels in a low path along the mid dorsum to maximize narrowing and then back high to prevent over-narrowing of the nasal root. If the nasal bones do medialize, internal stabilization with splints may be necessary to prevent support without outward migration.
In cases of a wide nasal base, over-narrowing is less of a concern, and a low initiated osteotomy is appropriate. If the nasal root is also wide, then this osteotomy can be kept at a low position. Osteotomy techniques designed specifically for the deviated nose include unilateral osteotomy and the open-book method.
Intermediate osteotomy
Often a unilateral force will cause collapse of one sidewall, creating the illusion of a nose that is deviated to the opposite side. Similarly, performing a unilateral osteotomy can give the impression of a crooked nose or a nose directed toward the opposite direction. This can be a valuable tool if an overly convex sidewall gives the illusion of a nose that deviates to the ipsilateral side. This sidewall can be narrowed with a single lateral osteotomy, effectively shortening the sidewall and giving the impression of directing the nose back toward the midline.
The open-book method is a logical technique to correct the deviated nose. By performing osteotomies in sequential order from the nondeviated lateral nasal sidewall, across the pyramid, toward the deviating or convex lateral sidewall, the deviated bony third region can be placed in midline.
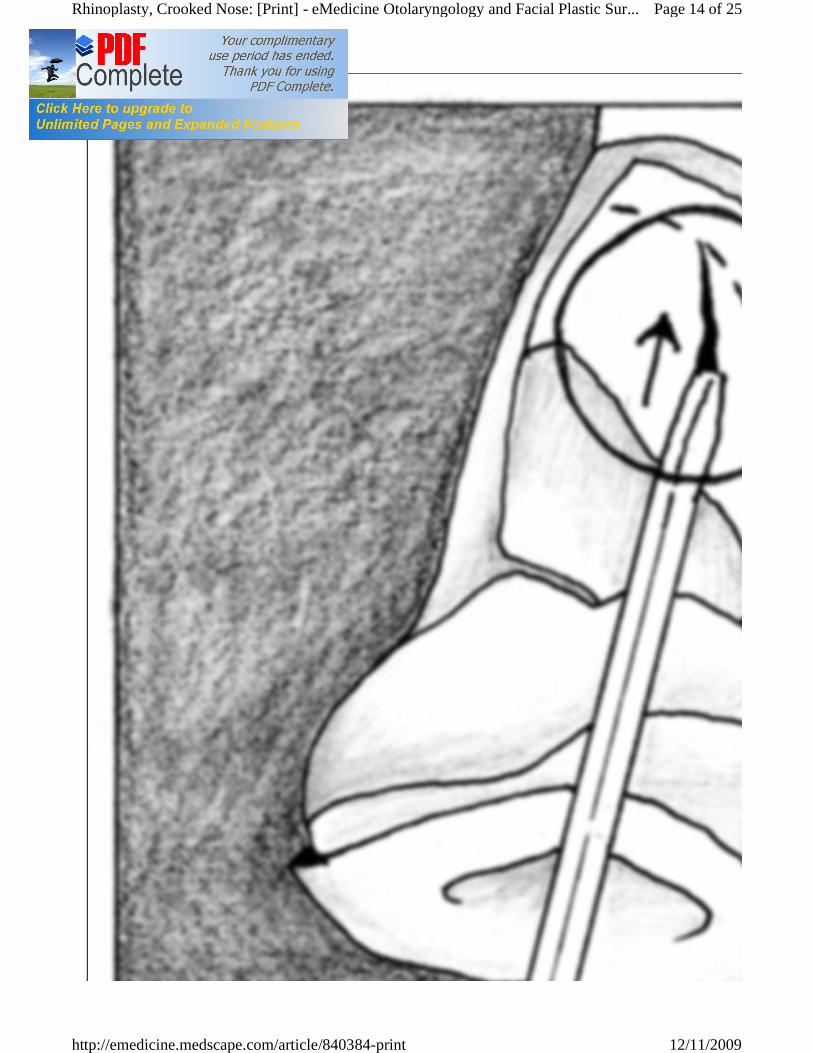
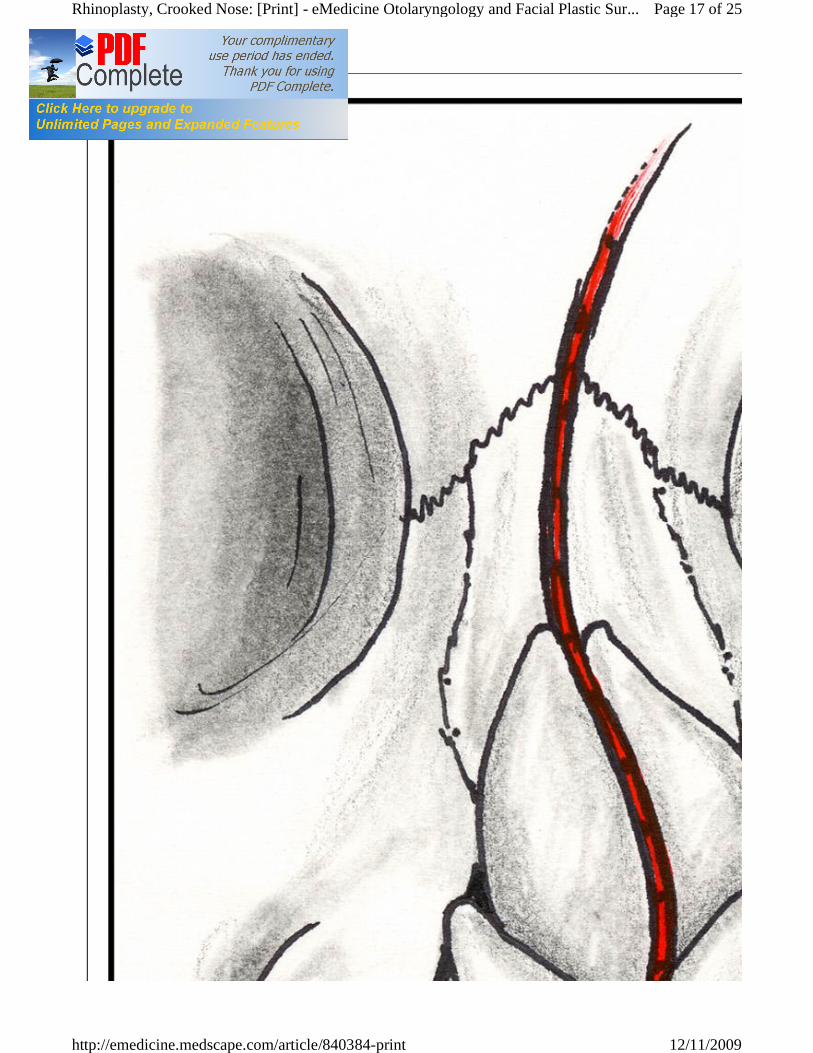
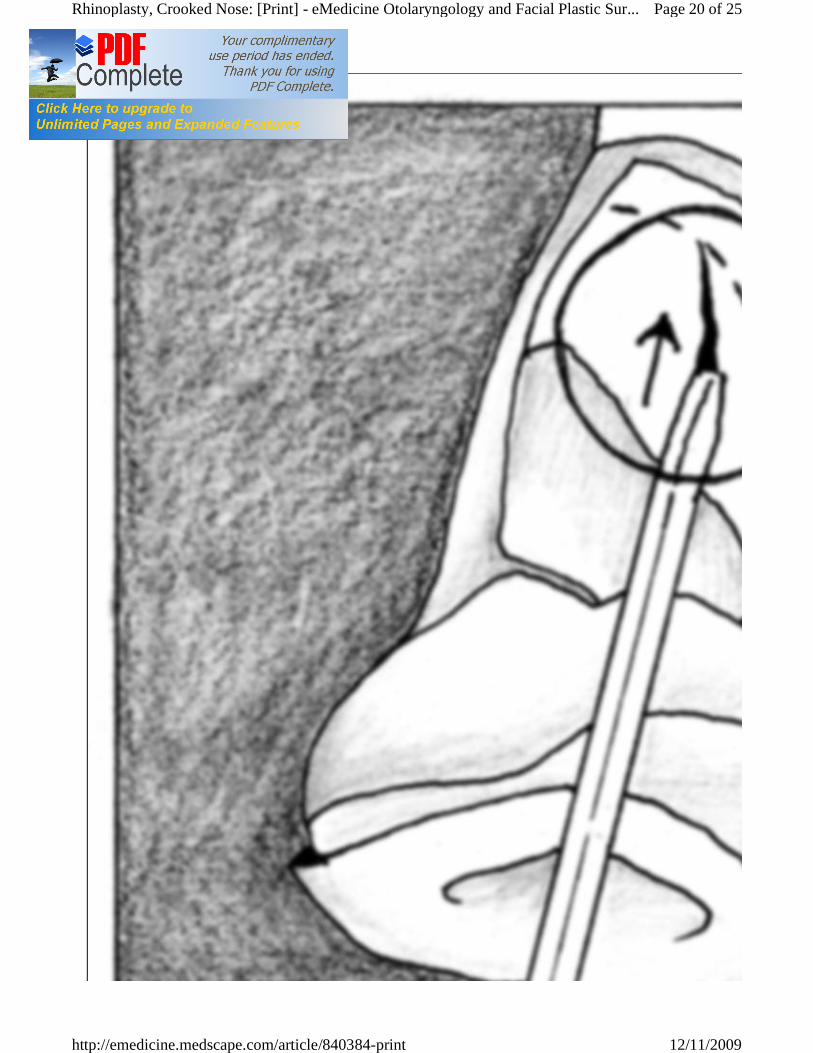
The intermediate osteotomy is a valuable tool for shortening an overly convex lateral wall (see Image 4). Perform the intermediate osteotomy before the lateral osteotomy; otherwise, the osteotomy will be attempted on mobile bony segments, and comminution of the sidewall may occur.
Page 13 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Page 14 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print

Intermediate osteotomy is completed prior to initiating lateral osteotomy.
Sliding osteotomies are started intranasally at the pyriform aperture. The osteotome is introduced through a mucosal incision situated just proximal to the inferior turbinate.
Often, completing the break between the medial and lateral osteotomy can be aided with a percutaneous osteotomy performed at the apex of 2 osteotomy pathways. A 1- or 2-mm osteotome swiftly driven through the skin is effective and causes little trauma. The skin incision can be expected to heal well and without scarring. Complete lateral wall osteotomy can also be performed by a percutaneous osteotomy situated through a single stab skin incision on the nasal dorsal sidewall or through an intranasal mucosal incision. The osteotome is marched up the sidewall in a postage stamp manner. Proponents of this method argue that the osteotomy is completed with greater accuracy and less trauma.
Irrespective of the method favored, attention to proper technique is necessary to achieve a straight nose. Prior to initiating the osteotomy, mark proposed paths on the nasal dorsal sidewall skin to guide proper osteotomy placement. Guarding against imprecise, traumatic, asymmetric, and incomplete osteotomies ensures a successful outcome.
Postoperative Details
Following extensive septal work, maintaining nasal stability is important. Commercially available Xomed septal splints can be secured to both sides of the septum and mattress, sutured together with a heavy nylon suture. Silastic or radiographic film splints are just as effective and less cumbersome to the patient. Internal packing is minimized to a thin piece of nonadhesive gauze that is removed on the evening of surgery or the next morning.
External stabilization of the nose begins with a layer of nonadhesive gauze, cut to match the length of the dorsum, ending just at the supratip region. Starting on one dorsal sidewall, a longitudinal piece of micropore tape is wrapped around the tip and then back up the other dorsal sidewall. This dressing keeps the tip in the desired position.
Successive placement of horizontally directed tape is as follows: (1) The first piece is placed across the supratip with enough pressure to obliterate dead space. (2) Subsequent pieces march up the dorsum to the nasal root. A cast keeps the mobile nasal bones in place and protects the nose from external force. (3) Casting and tape material remain in place for 7 days. Following removal of the dressing, the dorsum may tend to migrate back to its deviated position.
Nasal exercise, instituted by correct placement of digital pressure, may be helpful until nasal bones have achieved greater stability.
Outcome and Prognosis
Surgical management of the crooked nose is deceivingly complex. Symptoms of nasal obstruction are common.
Nasal valve collapse, the degree of septal deformity, and tip status will help guide the surgeon to the appropriate approach for effective improvement.
Properly diagnosing deviating forces and treating them accordingly is imperative. Direct attention to the upper-third region as well as the lower two thirds of the nose.
Whether camouflaging techniques and/or structural reorientation are used, the rhinoplasty surgeon needs to be well versed in the different methods and philosophies of managing the crooked nose.
Future and Controversies
Page 15 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
The future of crooked nose surgery may lie in future implant materials that are universally tolerated and not rejected. Obviously, this currently remains theoretical. In 2006, Gurlek et al reported their experience with custom-made high-density porous polyethylene extended spreader grafts.1 Twenty patients had acceptable surgical results without extrusion. Mendelsohn described similar results with 40 patients.2 Further studies are necessary to determine the efficacy and reliability of implantable materials. Some authors have noticed short-term success with biodegradable polymers, such as polylactides, which have stability for at least 7 months. The main limitation with the use of these polymers is that they may extrude and cause infection.3 Genetically created cartilage from tissue banks may someday represent a viable alternative to autogenous harvested cartilage, without the donor site morbidity and time required for harvest.
Multimedia
Page 16 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Page 17 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Media file 1:
S-shaped crooked nose deformity.
Media file 2: Photo taken from above and behind the subject elucidates crooked nose deformity.
Page 18 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Media file 3:
The pyramidal frustum serves as a useful geometric model for analyzing the upper one third of the
nose.
Page 19 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Page 20 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
Media file 4:
Intermediate osteotomy is completed prior to initiating lateral osteotomy.
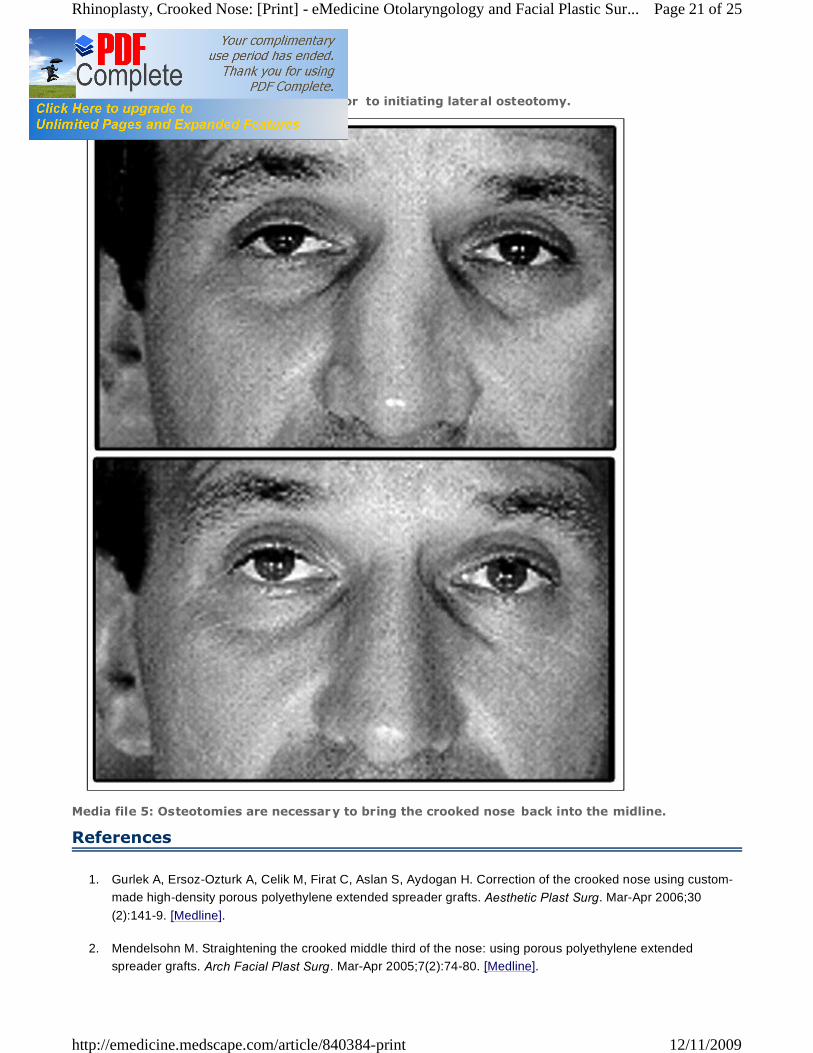
Media file 5: Osteotomies are necessary to bring the crooked nose back into the midline.
References
1. Gurlek A, Ersoz-Ozturk A, Celik M, Firat C, Aslan S, Aydogan H. Correction of the crooked nose using custom-made high-density porous polyethylene extended spreader grafts. Aesthetic Plast Surg. Mar-Apr 2006;30(2):141-9. [Medline].
2. Mendelsohn M. Straightening the crooked middle third of the nose: using porous polyethylene extended spreader grafts. Arch Facial Plast Surg. Mar-Apr 2005;7(2):74-80. [Medline].
Page 21 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
3. Watzinger F, Wutzl A, Wanschitz F, Ewers R, Turhani D, Seemann R. Biodegradable polymer membrane used as septal splint. Int J Oral Maxillofac Surg. May 2008;37(5):473-7. [Medline].
4. Achauer BM, VanderKam VM, Celikoz B, Jacobson DG. Augmentation of facial soft-tissue defects with Alloderm dermal graft. Ann Plast Surg. Nov 1998;41(5):503-7. [Medline].
5. Anderson JR. Straightening the crooked nose. Trans Am Acad Ophthalmol Otolaryngol. Jul-Aug 1972;76(4):938-45. [Medline].
6. Andrews JT, Schoenrock LD. Photodocumentation. In: Bailey BJ, et al, eds. Head and Neck Surgery - Otolaryngology. 2nd ed. Philadelphia, Pa: Lippincott-Raven; 1998.
7. Briant TD, Middleton WG. The management of severe nasal septal deformities. J Otolaryngol. Apr 1985;14(2):120-4. [Medline].
8. Bujia J. Determination of the viability of crushed cartilage grafts: clinical implications for wound healing in nasal surgery. Ann Plast Surg. Mar 1994;32(3):261-5. [Medline].
9. Calhoun KH. Introduction to rhinoplasty. In: Bailey BJ, et al, eds. Head and Neck Surgery - Otolaryngology. 2nd ed. Philadelphia Pa: Lippincott-Raven; 1998.
10. Constantian MB. An algorithm for correcting the asymmetrical nose. Plast Reconstr Surg. May 1989;83(5):801-11. [Medline].
11. Constantian MB. The incompetent external nasal valve: pathophysiology and treatment in primary and secondary rhinoplasty. Plast Reconstr Surg. Apr 1994;93(5):919-31; discussion 932-3. [Medline].
12. Constantian MB, Clardy RB. The relative importance of septal and nasal valvular surgery in correcting airway obstruction in primary and secondary rhinoplasty. Plast Reconstr Surg. Jul 1996;98(1):38-54; discussion 55-8. [Medline].
13. Daniel RK. Rhinoplasty and rib grafts: evolving a flexible operative technique. Plast Reconstr Surg. Oct 1994;94(5):597-609; discussion 610-1. [Medline].
14. Dayan SH, Shah AR. A suture suspension technique for improved repair of a crooked nose deformity. Ear Nose Throat J. Nov 2004;83(11):743-4. [Medline].
15. Dingman RO, Converse JM. The clinical management of facial injuries and fractures of the facial bones. In: McCarthy JG, Converse JM, eds. Reconstructive Plastic Surgery. 2nd ed. Philadelphia, Pa: WB Saunders; 1977:599-724.
16. Dingman RO, Natvig P. Surgery of Facial Fractures. Philadelphia, Pa: WB Saunders; 1964:267-294.
17. Ducic Y, Hilger PA. Surgical correction of the deviated septum. Facial Plast Clin North Am. 1999;7:319-331.
18. Fanous N. Unilateral osteotomies for external bony deviation of the nose. Plast Reconstr Surg. Jul 1997;100(1):115-23. [Medline].
19. Fomon S. The Surgery of Injury and Plastic Repair. Baltimore, Md: The Williams & Wilkins Co; 1939:614-831.
20. Frodel JL Jr, Marentette LJ, Quatela VC, Weinstein GS. Calvarial bone graft harvest. Techniques, considerations, and morbidity. Arch Otolaryngol Head Neck Surg. Jan 1993;119(1):17-23. [Medline].
Page 22 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
21. Godin MS, Waldman SR, Johnson CM Jr. The use of expanded polytetrafluoroethylene (Gore-Tex) in rhinoplasty. A 6-year experience. Arch Otolaryngol Head Neck Surg. Oct 1995;121(10):1131-6. [Medline].
22. Gray LP. Early treatment of septal deformity and associated abnormalities. In: Maxwell E, ed. Modern Trends in Diseases of the Ear, Nose, and Throat. London: Butterworths; 1972:219-240.
23. Guyuron B, Behmand RA. Caudal nasal deviation. Plast Reconstr Surg. Jun 2003;111(7):2449-57; discussion 2458-9. [Medline].
24. Kim DW, Toriumi DM. Management of posttraumatic nasal deformities: the crooked nose and the saddle nose. Facial Plast Surg Clin North Am. Feb 2004;12(1):111-32. [Medline].
25. Kridel RW, Konior RJ. Irradiated cartilage grafts in the nose. A preliminary report. Arch Otolaryngol Head Neck Surg. Jan 1993;119(1):24-30; discussion 30-1. [Medline].
26. Littlejohn MC, Bailey B, Yoo JK. Granulomatous diseases of the head and neck. In: Bailey B, et al, eds. Head and Neck Surgery - Otolaryngology. 2nd ed. Philadelphia, Pa: Lippincott-Raven; 1998.
27. Murakami CS, Cook TA, Guida RA. Nasal reconstruction with articulated irradiated rib cartilage. Arch Otolaryngol Head Neck Surg. Mar 1991;117(3):327-30; discussion 331. [Medline].
28. Ortiz-Monasterio F, Olmedo A, Oscoy LO. The use of cartilage grafts in primary aesthetic rhinoplasty. Plast Reconstr Surg. May 1981;67(5):597-605. [Medline].
29. Owen GO, Parker AJ, Watson DJ. Fractured-nose reduction under local anaesthesia. Is it acceptable to the patient?. Rhinology. Jun 1992;30(2):89-96. [Medline].
30. Podoshin L, Gertner R, Fradis M, Berger A. Incidence and treatment of deviation of nasal septum in newborns. Ear Nose Throat J. Aug 1991;70(8):485-7. [Medline].
31. Pontius AT, Leach JL Jr. New techniques for management of the crooked nose. Arch Facial Plast Surg. Jul-Aug 2004;6(4):263-6. [Medline].
32. Shah AR, Constantinides M. Aligning the bony nasal vault in rhinoplasty. Facial Plast Surg. Feb 2006;22(1):3-8. [Medline].
33. Sheen JH. Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. Feb 1984;73(2):230-9. [Medline].
34. Sherris DA, Kern EB. The versatile autogenous rib graft in septorhinoplasty. Am J Rhinol. May-Jun 1998;12(3):221-7. [Medline].
35. Stoksted P, Ladefoged C. Crushed cartilage in nasal reconstruction. J Laryngol Otol. Aug 1986;100(8):897-906. [Medline].
36. Stoksted P, Schønsted-Madsen U. Traumatology of the newborn's nose. Rhinology. Jun 1979;17(2):77-82. [Medline].
37. Stranc MF, Robertson GA. A classification of injuries of the nasal skeleton. Ann Plast Surg. Jun 1979;2(6):468-74. [Medline].
38. Stucker FJ Jr, Bryarly RC, Shockley WW. Management of nasal trauma in children. Arch Otolaryngol. Mar 1984;110(3):190-2. [Medline].
Page 23 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
39. Tardy ME. Rhinoplasty: The Art and the Science. Philadelphia, Pa: WB Saunders; 1997:1-98.
40. Toriumi DM, Ries WR. Innovative surgical management of the crooked nose. Facial Plast Clin North Am. 1997;1:63-77.
41. Welling DB, Maves MD, Schuller DE, Bardach J. Irradiated homologous cartilage grafts. Long-term results. Arch Otolaryngol Head Neck Surg. Mar 1988;114(3):291-5. [Medline].
Keywords
crooked nose, rhinoplasty, nose job, asymmetric nose, twisted nose, deviated nose, post-traumatic nasal deformity, crooked nose, deviated septum, nasal trauma, broken nose, external nasal deformity, nasal septal deviation, nasal fracture, fractured septum, crooked dorsum, deviated dorsum
Contributor Information and Disclosures
Author
Steven H Dayan, MD, Clinical Assistant Professor, Department of Otolaryngology-Head and Neck Surgery, University of Illinois Disclosure: Nothing to disclose.
Coauthor(s)
Anil R Shah, MD, Plastic Surgeon, Private Practice Anil R Shah, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngic Allergy, American Academy of Otolaryngology-Head and Neck Surgery, and Triological Society Disclosure: Nothing to disclose.
Shefali I Shah, MD, Staff Physician, Department of Otolaryngology-Head and Neck Surgery, University of Illinois at Chicago Shefali I Shah, MD is a member of the following medical societies: American Academy of Facial Plastic and Reconstructive Surgery and American Academy of Otolaryngology-Head and Neck Surgery Disclosure: Nothing to disclose.
Medical Editor
Paul S Nassif, MD, FACS, Consulting Surgeon, Facial Plastic and Reconstructive Surgery, Spalding Drive Cosmetic Surgery and Dermatology Paul S Nassif, MD, FACS is a member of the following medical societies: Alpha Omega Alpha, American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngology-Head and Neck Surgery, American College of Surgeons, and California Medical Association Disclosure: Nothing to disclose.
Pharmacy Editor
Francisco Talavera, PharmD, PhD, Senior Pharmacy Editor, eMedicine Disclosure: Nothing to disclose.
Managing Editor
Dean Toriumi, MD, Department of Otolaryngology, Associate Professor, University of Illinois Medical Center Disclosure: Nothing to disclose.
Page 24 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print
CME Editor
Christopher L Slack, MD, Otolaryngology-Facial Plastic Surgery, Private Practice, Associated Coastal ENT; Medical Director, Treasure Coast Sleep Disorders Christopher L Slack, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngology-Head and Neck Surgery, and American Medical Association Disclosure: Nothing to disclose.
Chief Editor
Arlen D Meyers, MD, MBA, Professor, Department of Otolaryngology-Head and Neck Surgery, University of Colorado School of Medicine Arlen D Meyers, MD, MBA is a member of the following medical societies: American Academy of Facial Plastic and Reconstructive Surgery, American Academy of Otolaryngology-Head and Neck Surgery, and American Head and Neck Society Disclosure: Covidien Corp Consulting fee Consulting; US Tobacco Corporation unstricted gift unknown
Further Reading © 1994- 2009 by Medscape. All Rights Reserved (http://www.medscape.com/public/copyright)
Page 25 of 25Rhinoplasty, Crooked Nose: [Print] - eMedicine Otolaryngology and Facial Plastic Sur...
12/11/2009http://emedicine.medscape.com/article/840384-print