respiratory problems in maternity hdu - oaa webcast problems in maternity hdu ... had been...
TRANSCRIPT

Respiratory Problems in Maternity HDU
Cathy Nelson-Piercy
Consultant Obstetric Physician
Professor of Obstetric Medicine
KCL Division of Women’s Health

Lecture Plan Page 1
Respiratory
Asthma
Pneumonia
Pulmonary oedema
Hypoxia ? Cause
PE
AFE
Cardiopulmonary arrest

Commonest respiratory problems on maternity HDU……
Desaturation post CS
Basal atelectasis
poor respiratory effort post GA
Pain from CS
ileus / constipation / distension / diaphragmatic splinting
Pneumonia
Pulmonary oedema
Page 2


7.8% pregnancies
conceived with ART

Pregnant Post partum
Obstetric 9% 70%
PPH 36%
Pre-eclampsia 2% 4%
HELLP 0.7% 2.5%
Non obstetric 91% 30%
Pneumonia 23% 4.3%
Pulmonary
oedema
1.9% 1.6%
Pelvic infection 1.9%
AKI 0.3% 0.8%
Asthma 8% 0.6%
Cardiovascular 8% 5.6%
GI 10% 4.5%
Neuro 9% 3.5%
Endo 12% 1.6%
Page 5
ICNARC, 2013


There were deficiencies in both routine care and in the treatment of attacks.
There was widespread under-use of preventer inhalers and excessive over-
reliance on reliever inhalers.
10% of those who died did so within one month of discharge from hospital
following treatment for asthma; at least 21% had attended an emergency
department at least once in the previous year.
Over half of those who died were being treated for mild or moderate asthma
at the time; experts concluded that this was mostly because neither
doctors nor patients themselves recognised how serious their asthma
really was.
19% of those who died were smokers and others, including many children,
were exposed to second-hand smoke in the home.
Some patients had not collected their prescriptions for preventative
treatment or did not attend regular asthma check-ups.
National Review of Asthma Deaths (NRAD) – Findings: Page 7

• Every hospital and GP practice should have a designated, named
clinician for asthma services.
• Better monitoring of asthma control; where loss of control is
identified, immediate action is required including escalation of
responsibility, treatment change and arrangements for follow-up.
• Better education is needed for doctors, nurses, patients and carers
to make them aware of the risks. They need to be able to recognise
the warning signs of poor asthma control and know what to do
during an attack.
• All patients should be provided with a personal asthma action plan
(PAAP), which can help them to identify if their asthma is
worsening and tell them how and when to seek help.
National Review of Asthma Deaths (NRAD) – Recommendations:
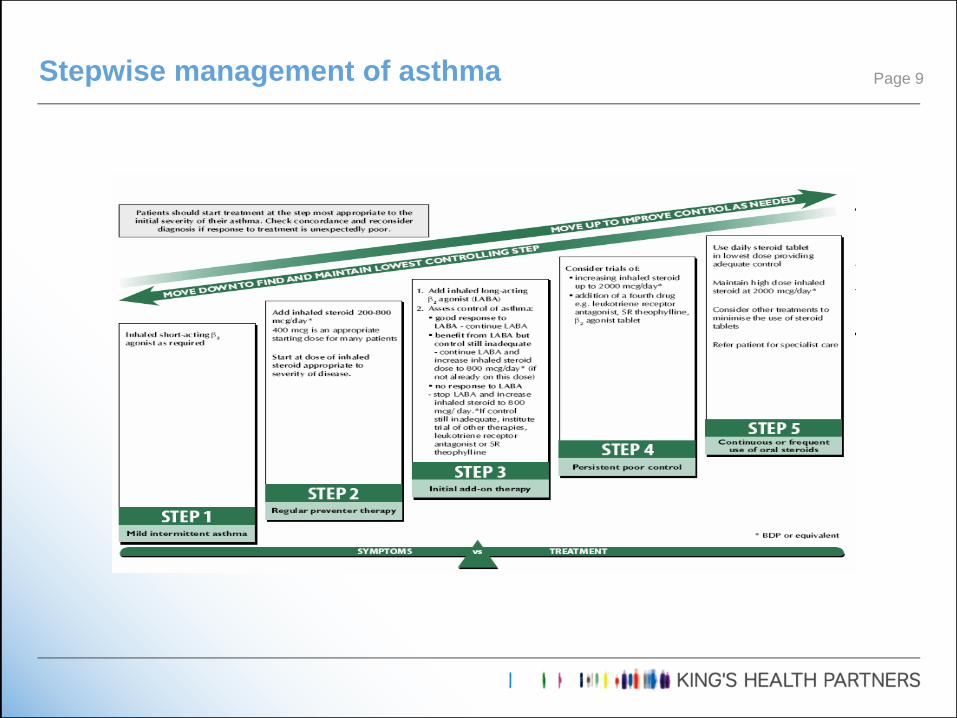
Stepwise management of asthma Page 9

Revised edition October 2014
Thorax 8th October

Levels of severity of acute asthma attacks in adults
Moderate asthma - Increasing symptoms
- PEF >50–75% best or predicted
- no features of acute severe asthma
Acute severe asthma Any one of:
- PEF 33–50% best or predicted
- respiratory rate ≥25/min
- heart rate ≥110/min
- inability to complete sentences in one breath
Life-threatening asthma Any one of the following in a patient with severe asthma:
Clinical signs Measurements
Altered conscious level PEF <33% best or predicted
Exhaustion SpO2 < 92%
Arrhythmia PaO2 < 8 kPa
Hypotension ’normal’ PaCO2 (4.6–6.0 kPa)
Cyanosis
Silent chest
Poor respiratory effort
Near-fatal asthma Raised PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
504-507

Give supplementary oxygen to all hypoxaemic patients with acute severe
asthma to maintain an SpO2 level of 94–98%. Lack of pulse oximetry
should not prevent the use of oxygen.
Use high-dose inhaled β2 agonists as first line agents in patients with
acute asthma and administer as early as possible. Reserve intravenous
β2 agonists for those patients in whom inhaled therapy cannot be used
reliably.
In severe asthma that is poorly responsive to an initial bolus dose of β2
agonist, consider continuous nebulisation with an appropriate nebuliser.
Give steroids in adequate doses in all cases of acute asthma attack.
Add nebulised ipratropium bromide (0.5 mg 4–6 hourly) to b2 agonist
treatment for patients with acute severe or life-threatening asthma or
those with a poor initial response to b2 agonist therapy.
Consider giving a single dose of IV magnesium sulphate to patients with
acute severe asthma (PEF <50% best or predicted) who have not had a
good initial response to inhaled bronchodilator therapy.
Management of acute asthma: Recommendations Page 12

Indications for admission to intensive care or high-dependency units
include patients requiring ventilatory support and those with acute
severe or life-threatening asthma who are failing to respond to therapy,
as evidenced by:
• deteriorating PEF
• persisting or worsening hypoxia
• hypercapnia
• arterial blood gas analysis showing fall in pH or rising H+ concentration
• exhaustion, feeble respiration
• drowsiness, confusion, altered conscious state
• respiratory arrest
REFERRAL TO INTENSIVE CARE
Page 13

Nebulized beta2 agonists + ipratropium
Oxygen – sats 94-98%
Oral / intravenous corticosteroids
Mg SO4
Intravenous theophylline
Intravenous beta 2 agonists
Consider delivery if ventilation required
Acute severe asthma - summary
Acute asthma is very unusual in labour

CXRs are safe in pregnancy
MgS04 is safe for acute severe asthma; 1.2g vs. 4g
Remember

Normal oxygen saturations do not exclude critical illness
Eg. Diabetic ketoacidosis
Serum bicarbonate (18-22 mmol/l)
ABGs
PH
O2
CO2
Bicarbonate
Base excess
Lactate
Arterial Blood Gases
Acidosis is bad
Tachypnoea is sepsis until proved otherwise

6/10/06

Bacterial – same organisms, same treatment
Amoxycillin
Cefuroxime
Clarithromycin
Gentamycin
AVOID tetracycline / doxycycline
Viral
Varicella Zoster
Influenza
Pneumonia

UKOSS study Sept – Dec 2009
All admitted pregnant women with confirmed H1N1
Interim report, n = 182
Cases Controls
BMI >30 29 19
Asthma 16 5
H1N1 in pregnancy

UKOSS study Sept – Dec 2009 (n=256, 1220 controls)
20% admitted to ITU
Fewer symptoms
Less likely to have been treated with antivirals within 2 days of symptoms
Increase risk of preterm delivery
(Pierce et al. BJOG 2011; 342)
Systematic review and meta-analysis (n=610 782)
OR mortality: pandemic flu seasonal flu
Obesity 2.74 (95% CI 1.56-4.8) 30.1 (95% CI 1.74-2.39)
Pregnancy 0.99 (95% CI 0.67-1.46) 1.07 (95% CI 0.79-1.45)
(Mertz et al. BMJ 2013; 347:f5061)
H1N1 in pregnancy


Case 133 year old womanReadmitted day 5 post emLSCS (for pre-eclampsia) c/o SOB and wheezyHad been discharged home day 3 post LSCS – well
O/EBreathless, sweaty SaO2 70% on RA; 100% on 15LBP 170/90 P75 SRUrine: 1+ proteinCVS: Raised JVP, HS normalChest – bilateral wheezing, scattered crepsAbdo – soft, non tenderPeripheral oedema to thighs
AIR
pH 7.49
PaCO2 4.1
PaO2 6.2
BEx 0.6

Echo normal; Diagnosis = postpartum pre-eclampsia

Pre-eclampsia
Reduced colloid osmotic pressure
Iatrogenic
Fluid shifts
Beware syntocinon
Beware NSAIDs
Cardiac
Peripartum cardiomyopathy
Mitral stenosis
Pulmonary oedema

n = 210,631; 16 units; 1999 - 2003.
1087 severe pre-eclampsia or eclampsia (5.2/1000)
151 serious complications
82 (39/10,000) having eclamptic seizures and
49 (23/10,000) requiring ICU admission.
82 eclampsia
45 occurred antenatally (55%)
18 before admission to the maternity unit
11 in labour (13%)
26 following delivery (32%).
25 pulmonary oedema (2.3% of cases)
6 renal dialysis (0.55% of cases).
Yorkshire Critical Care Group
BJOG. 2005; 112:875-80

Sibai et al. AJOG 1987; 156: 1174-9.
9 yrs, n = 37 (78% black)
Incidence = 2.9% (cf. 2.3% Yorkshire)
Higher incidence in older, multigravid patients
30% antepartum (90% pre-existing hypertension)
70% postpartum (Xs colloid / crystalloid)
4 maternal deaths; PNM = 53%
Pulmonary oedema in Pre-eclampsia

Oxygen
Stop IV fluids
Diuretics
Diamorphine
Investigate cause = ECHO
PPCM = Deliver / ACEI
Thromboprophylaxis
Management of pulmonary oedema


• Collaborative clinical leadership at an early stage
is essential for optimal Mx
• Include physicians, microbiology and virology,
intensive care, anaesthesiology, neonatology
• All pregnant women presenting with respiratory
symptoms should have oxygen saturation
performed at admission
• Request lactate / venous gas in suspected sepsis
• Not all breathessness and / or chest pain = PE
• Tachypnoea is sepsis until proved otherwise
Learning points - Respiratory

Thank you for your attention!
