respiratory drugs. i. bronchodilators bronchodilators are indicated for the treatment of asthma...
TRANSCRIPT
Respiratory drugs
I. Bronchodilators
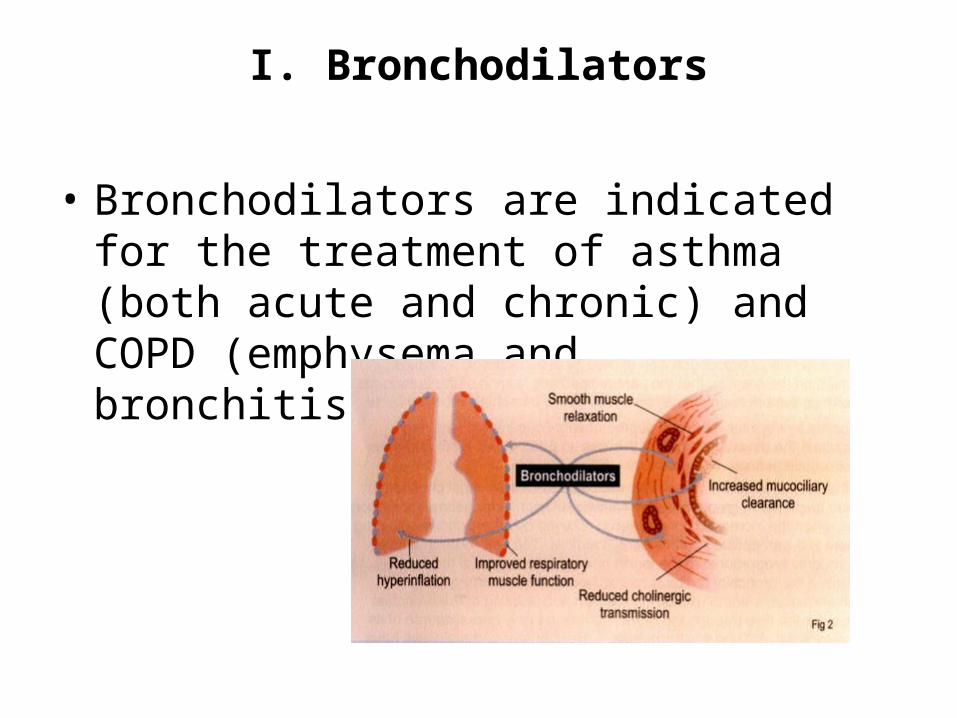
• Bronchodilators are indicated for the treatment of asthma (both acute and chronic) and COPD (emphysema and bronchitis).
• There are 3 major categories of bronchodilators: beta adrenergics, anticholinergics, and xanthines
A. Beta adrenergic bronchodilators1. adrenergic receptors
• In the late 1940’s, two types of adrenergic receptors were identified and were classified as α and β, based on their different responses to various adrenergic drugs.
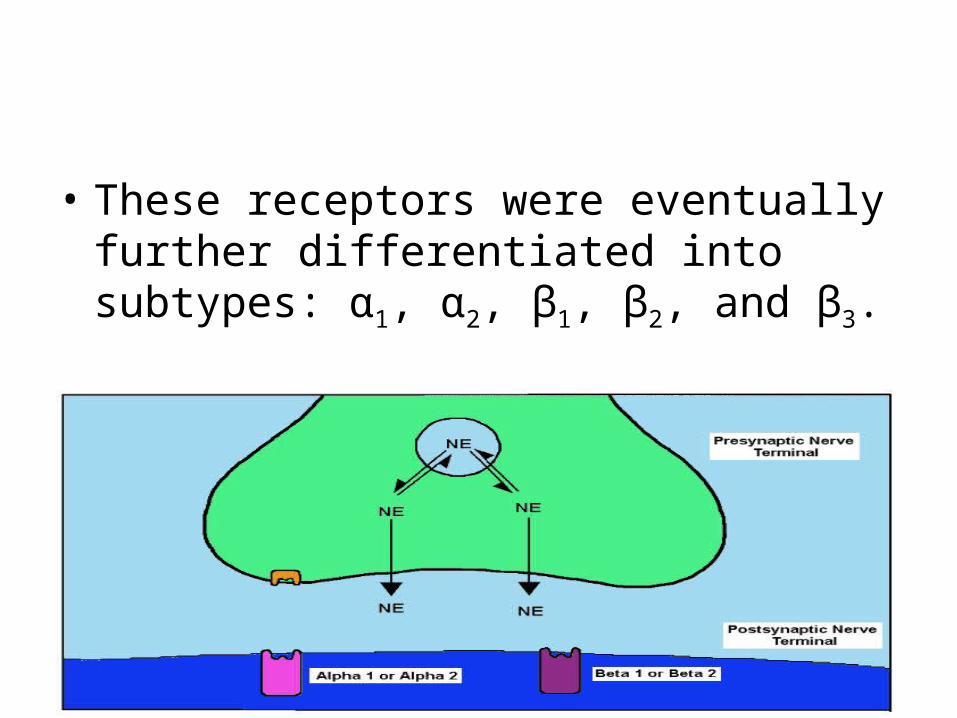
• These receptors were eventually further differentiated into subtypes: α1, α2, β1, β2, and β3.
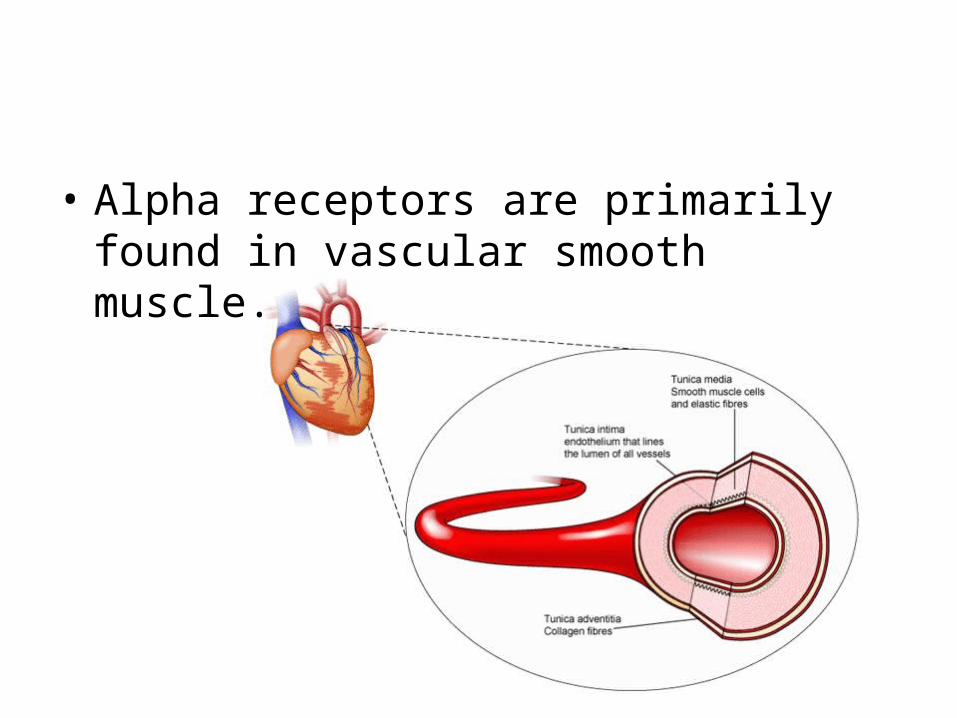
• Alpha receptors are primarily found in vascular smooth muscle.
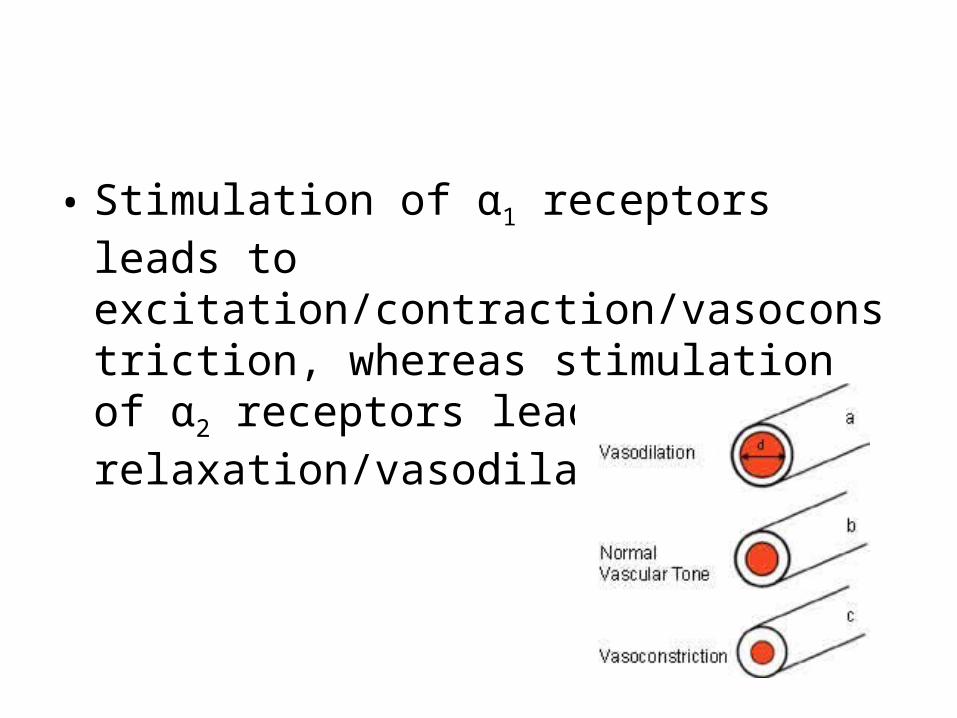
• Stimulation of α1 receptors leads to excitation/contraction/vasoconstriction, whereas stimulation of α2 receptors leads to relaxation/vasodilation.
• Beta receptors are found in fat cells and in both cardiac and smooth muscle.
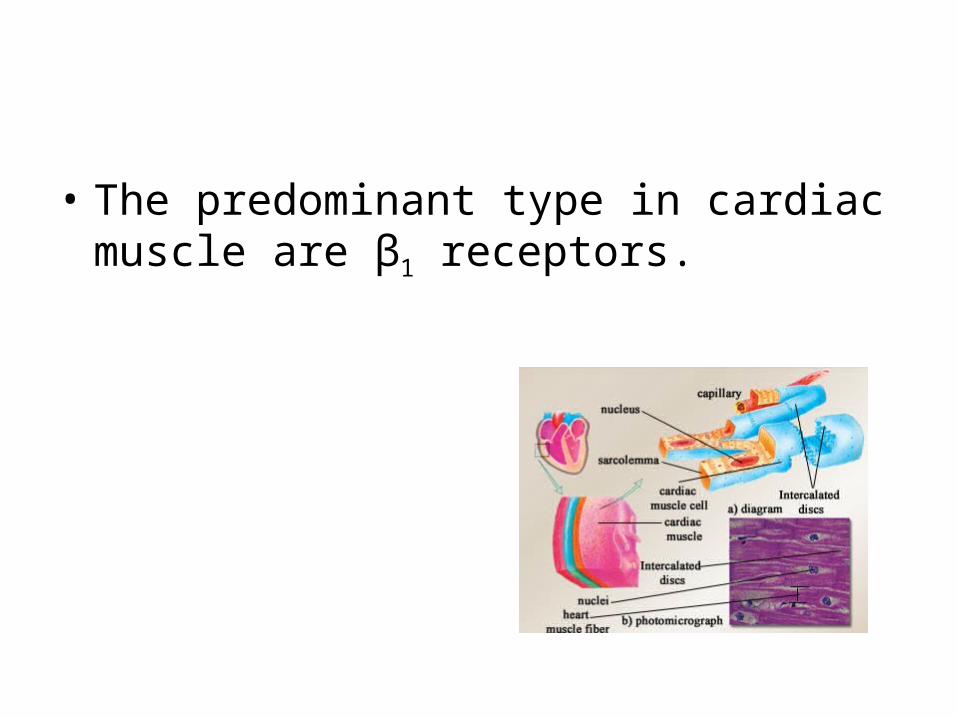
• The predominant type in cardiac muscle are β1 receptors.
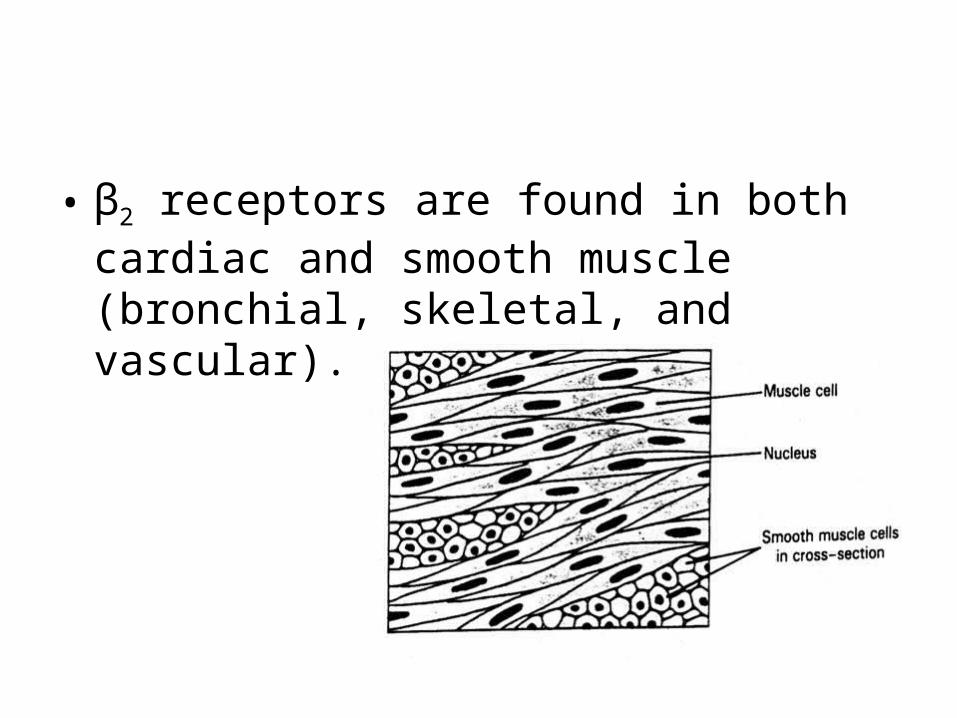
• β2 receptors are found in both cardiac and smooth muscle (bronchial, skeletal, and vascular).
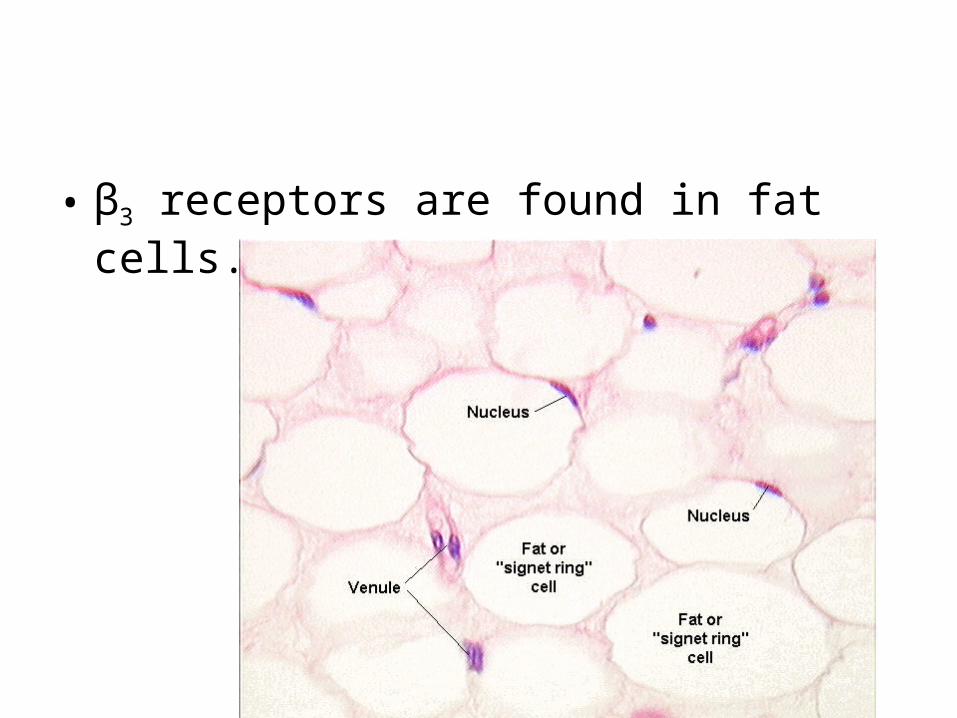
• β3 receptors are found in fat cells.
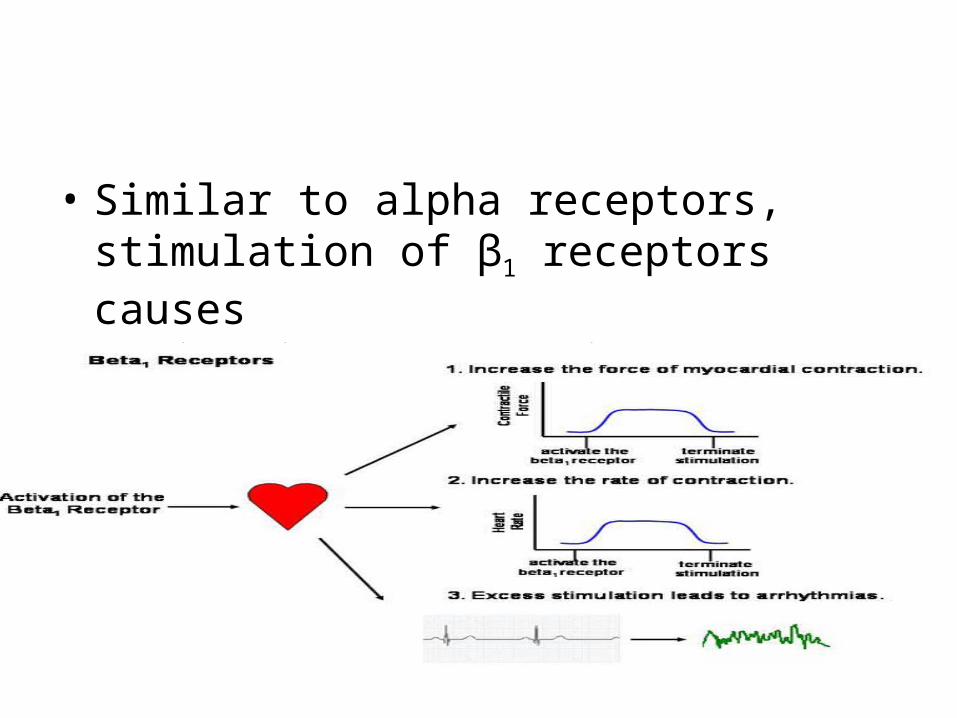
• Similar to alpha receptors, stimulation of β1 receptors causes excitation/contraction/vasoconstriction
• and stimulation of β2 receptors causes relaxation/vasodilation.
2. beta adrenergic agents
• The beta adrenergic bronchodilators are classified chemically as catecholamines (or derivatives of catecholamines).
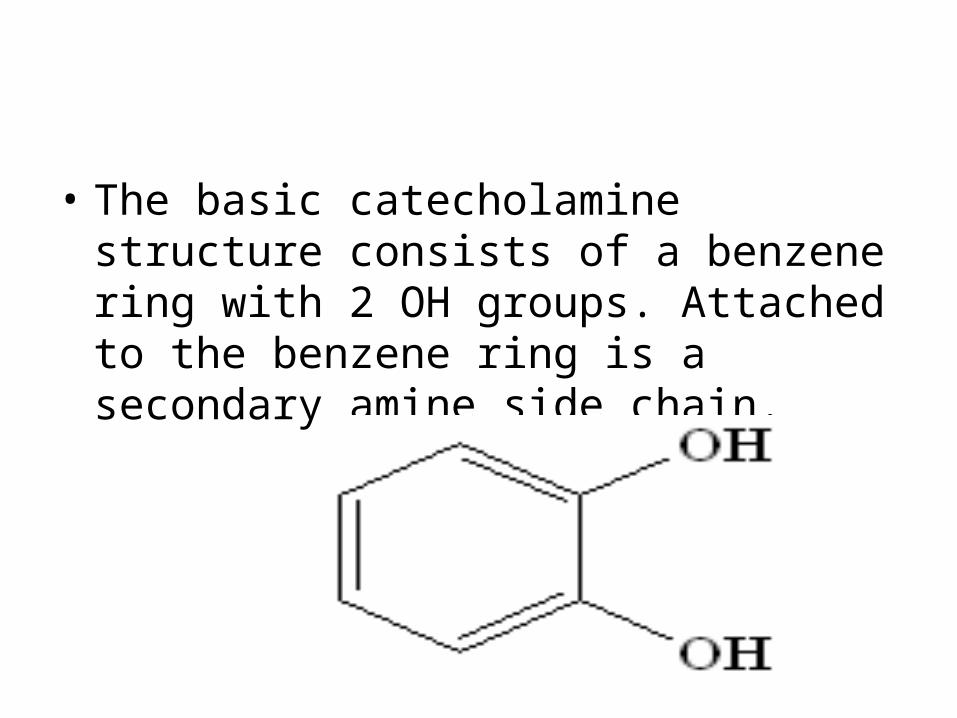
• The basic catecholamine structure consists of a benzene ring with 2 OH groups. Attached to the benzene ring is a secondary amine side chain.
• The composition of the side chain is related to the type of receptor the drug has a preference for:
• the LARGER the side chain, the MORE SPECIFIC is the receptor interraction.
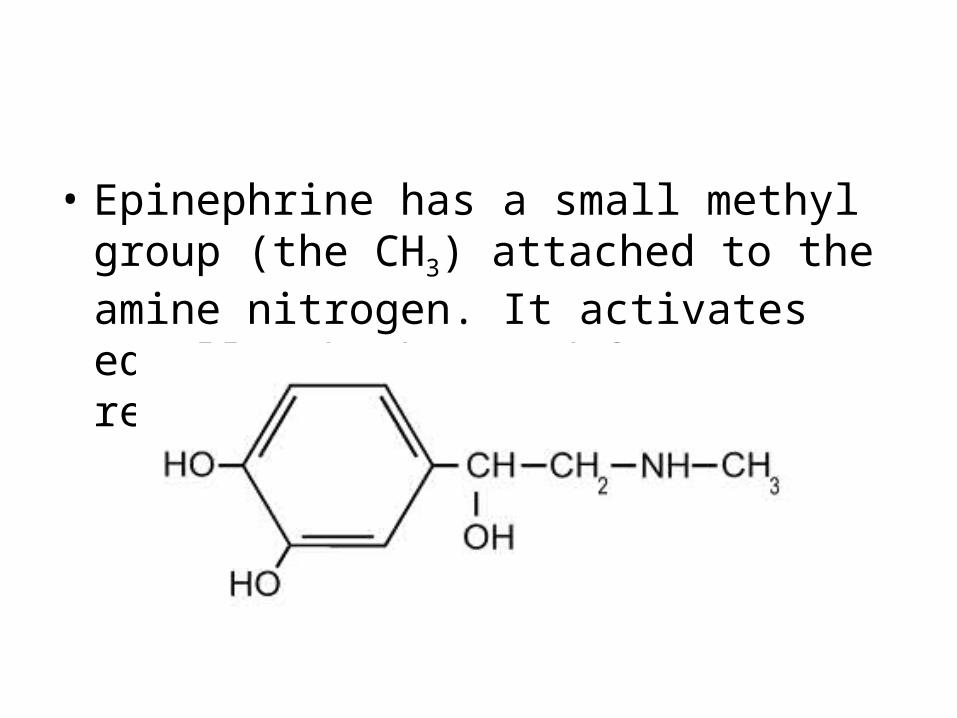
• Epinephrine has a small methyl group (the CH3) attached to the amine nitrogen. It activates equally, both α and β receptors.
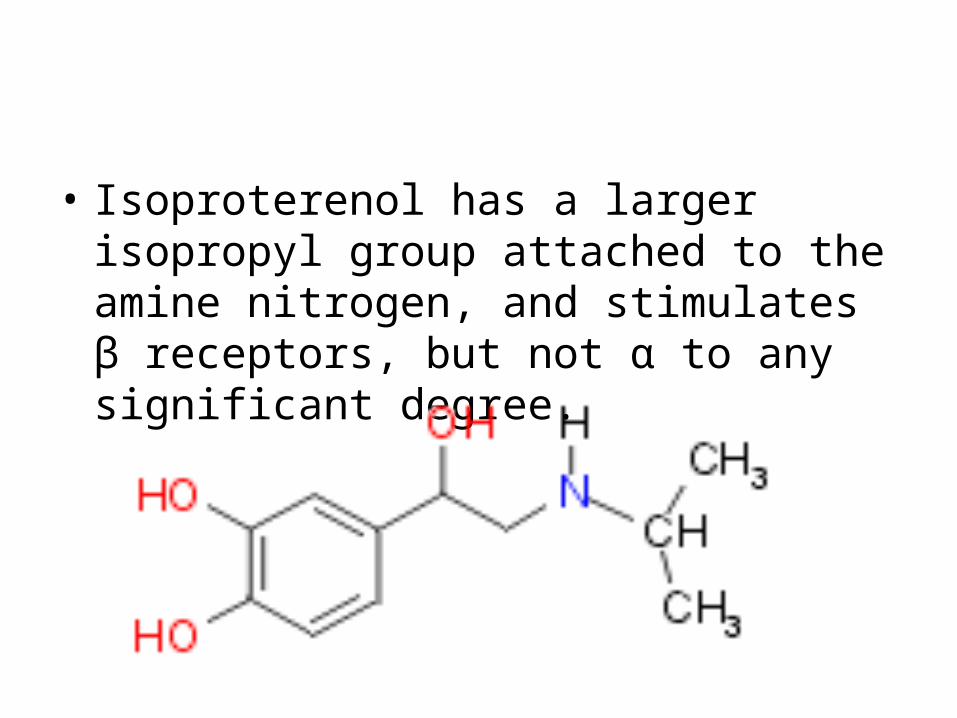
• Isoproterenol has a larger isopropyl group attached to the amine nitrogen, and stimulates β receptors, but not α to any significant degree.
• Many bronchodilators have an even larger group (t-butyl or bigger) attached to the amine nitrogen. These drugs are specific for β2 receptors.
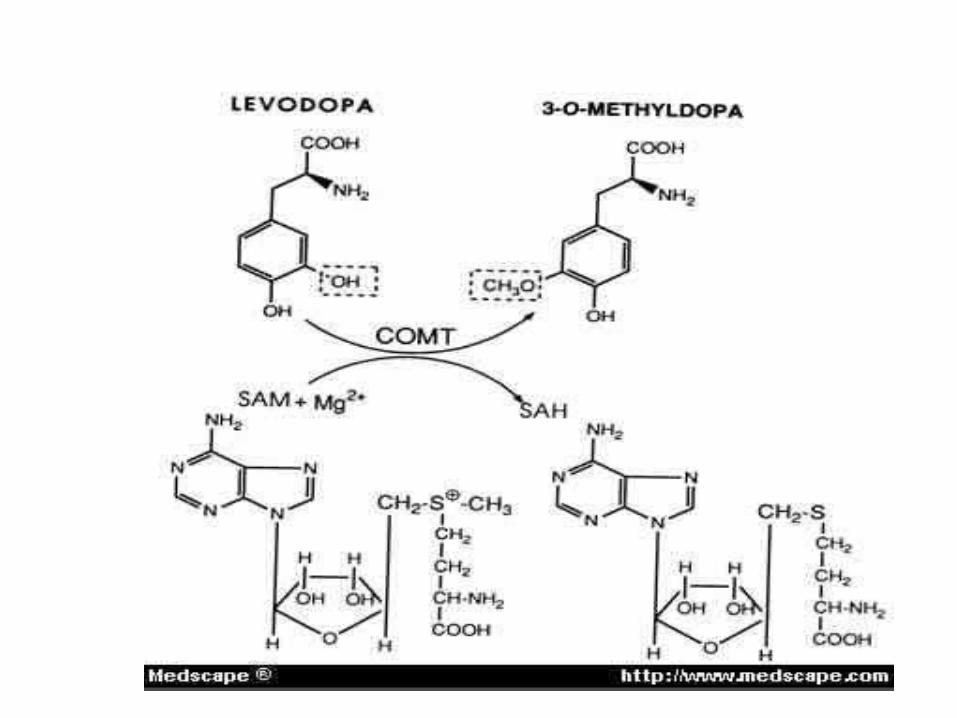
• Catecholamines are rapidly inactivated by the enzyme catechol-O-methyltransferase (COMT), found throughout the body.
• This enzyme forms an ether linkage through its attachment of a methyl group to the OH group on C-3 of benzene.
• This inactivation limits the duration of action of catecholamine drugs to a few hours.
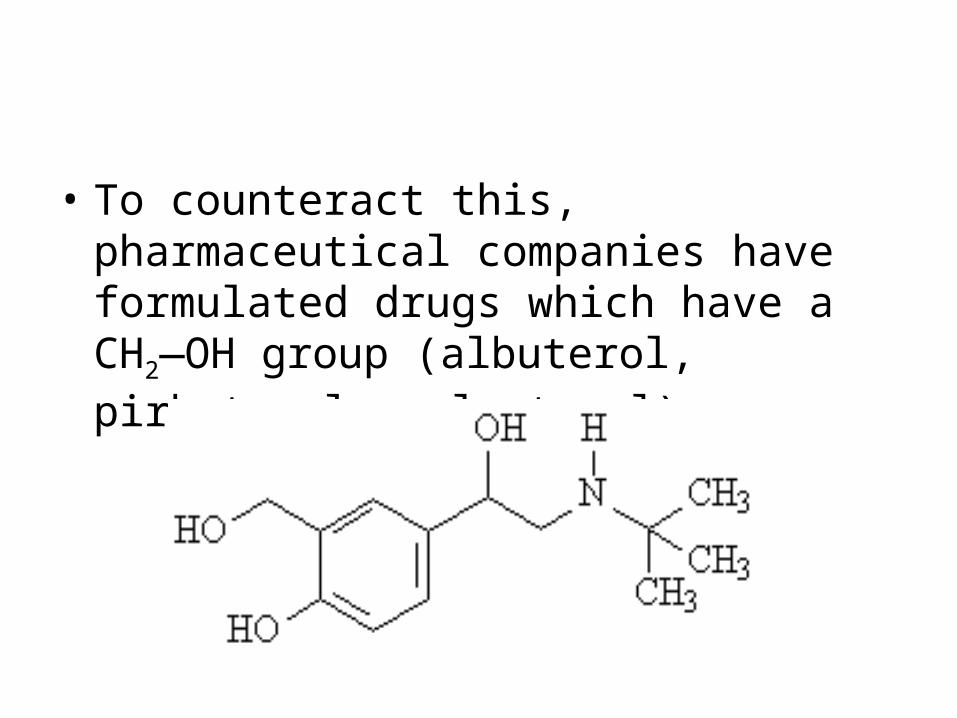
• To counteract this, pharmaceutical companies have formulated drugs which have a CH2—OH group (albuterol, pirbuterol, salmeterol);
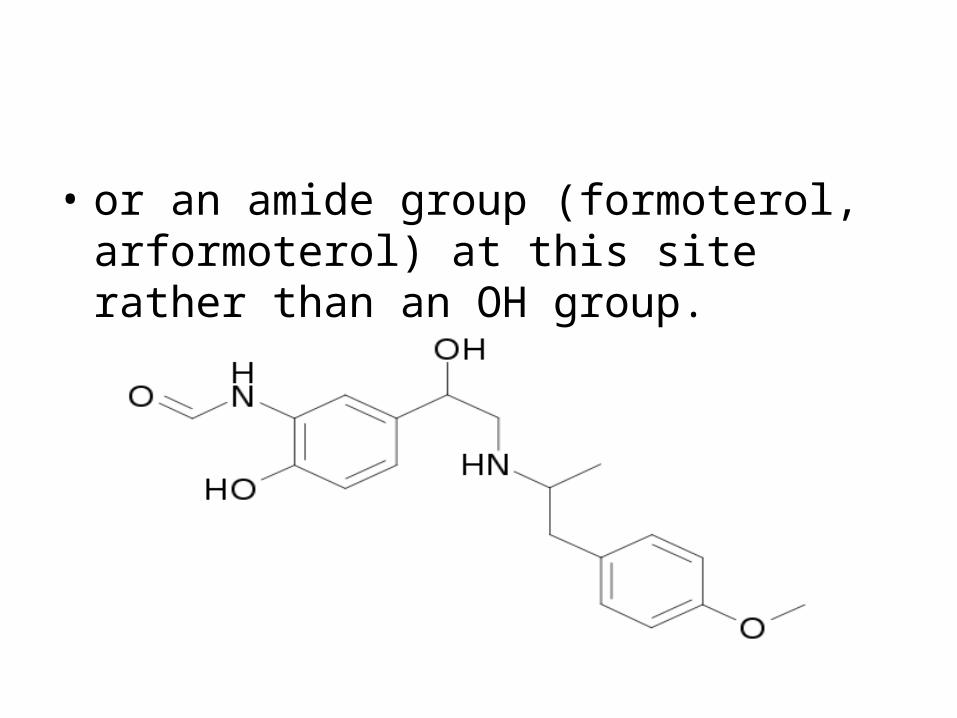
• or an amide group (formoterol, arformoterol) at this site rather than an OH group.
• This has effectively doubled or quadrupled the duration of the drug.
• Catecholamines are not normally administered orally because they undergo Phase II biotransformations in the GI tract (attachment of a sulfate or glucuronate at C-4) which inactivates them.
3. Bronchodilator mechanism of action
• Although some adrenergic bronchodilators can stimulate α and β1 receptors, the majority of these agents have selective β2 actions.
• Attachment to a β2 receptor leads to activation of a G protein on the cytoplasmic side of the membrane.
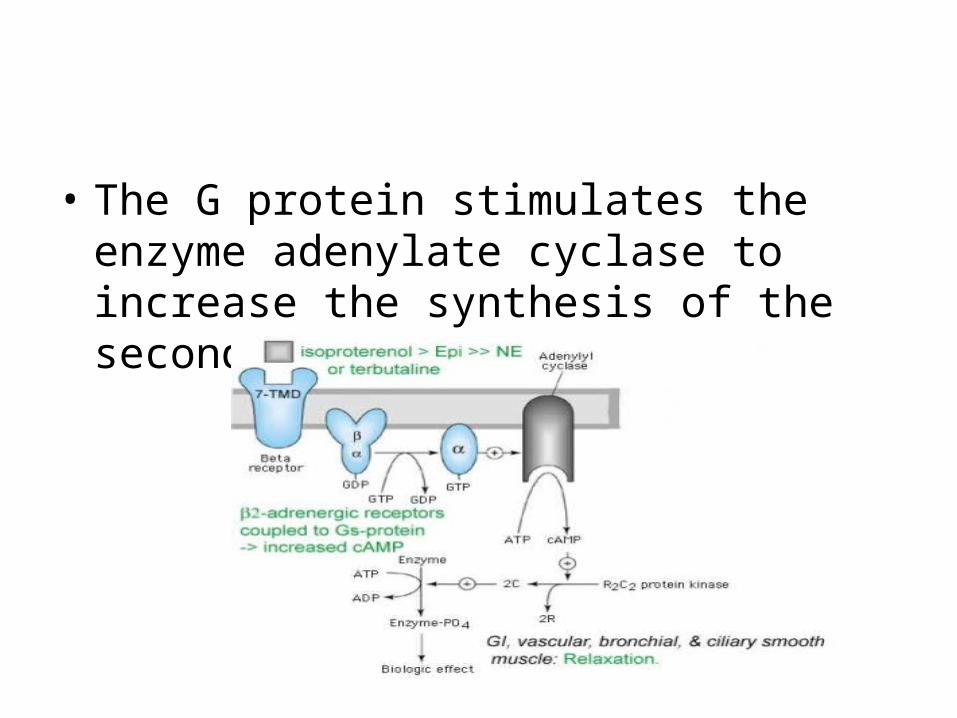
• The G protein stimulates the enzyme adenylate cyclase to increase the synthesis of the secondary messenger cAMP.
• An increase in cAMP results in an increase in the inactivation of a myosin kinase, causing smooth muscle relaxation.
• Beta adrenergic bronchodilators are indicated for the relaxation of airway smooth muscle in treating asthma and COPD.
• They are the most widely used and are believed to be the most effective agents for short term relief of asthma.
• Long term control is generally most effectively achieved with an inhaled corticosteroid.
4. Very short acting agents
• Very short acting agents have an onset on between 1-5 minutes and a duration of less than 3 hours.
• a. epinephrine (Adrenalin CI, Epinephrine Mist, AsthmaHaler Mist, AsthmaNefrin, Epi Pen)
• onset: minutes
• duration: 1-3 hours
• Epinephrine stimulates both α and β receptors, and therefore has a number of effects.
• It is a powerful bronchodilator that also causes elevation of blood pressure, tachycardia, headache, and insomnia.
• It has been administered by inhalation using a metered dose inhaler, MDI (Primatene Mist) or small volume nebulizer, SVN.
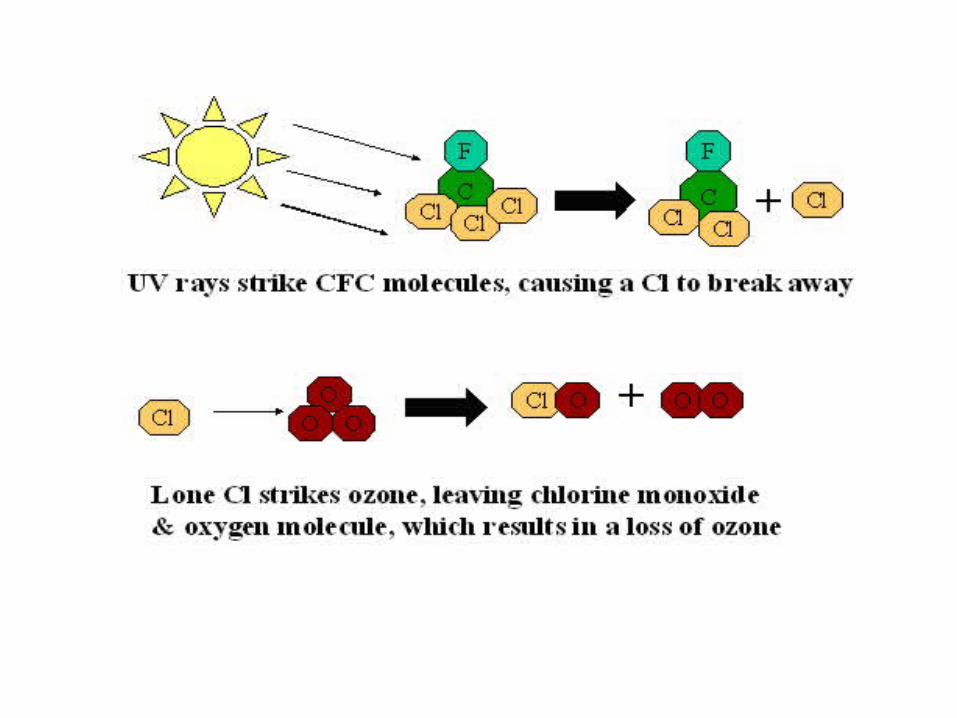
• The FDA has determined that traditional MDI’s which use a CFC propellant cannot be sold in the U.S. after December 2008 (according to the Montreal Protocol, which attempts to limit CFC’s in the atmosphere).
• Wyeth, which produces Primatene Mist has not released a version with the required hydrofluoralkane, HFA propellant as of January 2009.
• Epinephrine is also available in a pre-measured form (EpiPen) for intramuscular injections, and targeted for individuals susceptible to anaphylactic reactions
b. isoproterenol (Isuprel)
• Isoproterenol has both β1 and β2 actions and is only available today parenterally, to treat patients in shock or who experience bronchospasm during anesthesia. It is no longer manufactured for use in a SVN.
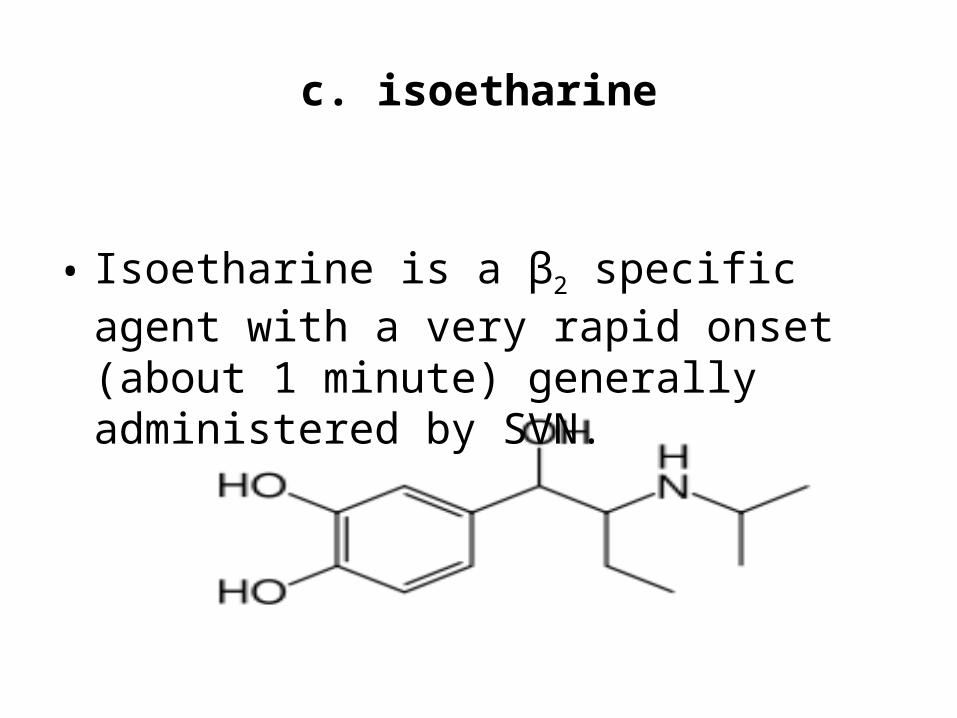
c. isoetharine
• Isoetharine is a β2 specific agent with a very rapid onset (about 1 minute) generally administered by SVN.
5. Short acting agents
• Short acting agents have an onset of between 1-15 minutes and a duration of up to 8 hours.
• Technically, they are not catecholamines, but are derivatives of catecholamine that are not as susceptible to deactivation by COMT.
a. metaproterenol (Alupent)
• This is administered via SVN or orally as it is not susceptible to inactivation in the GI tract.
b. albuterol (Teva’s Proair HFA; Schering Plough’s Proventil HFA; and
GlaxoSmithKline’s Ventolin HFA)
• These are all newly formulated bronchodilators. Albuterol is also available via SVN and in an oral formulation.
c. levalbuterol (Xopenex, Xopenex HFA)
• Levalbuterol is available as a SVN solution or in a MDI.
d. pirbuterol (Maxair Autohaler)
• is administerd via MDI. The manufacturer does not yet have an available HFA associated brand, and has been granted additional time to reformulate an HFA version.
6. Long acting agents
• Long acting agents have an onset of 15-20 minutes and a duration of up to 12 hours.

• Each of the drugs in this category are characterized by their larger, more nonpolar side chains.
• This is significant in that it allows the drug to actually diffuse into the phospholipid bilayer of the membrane and anchor the drug to the membrane.
• This leads to a continuous activation of the receptor and is the basis for the longer duration of action of drugs in this class.
• These long acting agents are not “rescue” drugs.
• A shorter acting agent should also be prescribed for asthmatic patients who need additional bronchodilator therapy.
• It is suggested that a long acting agent be introduced in the treatment of asthma once it is established that symptoms are not being controlled by regular low doses of inhaled corticosteroids.
• Using both an inhaled corticosteroid and a long acting β2 agonist often results in a decrease of asthma symptoms.
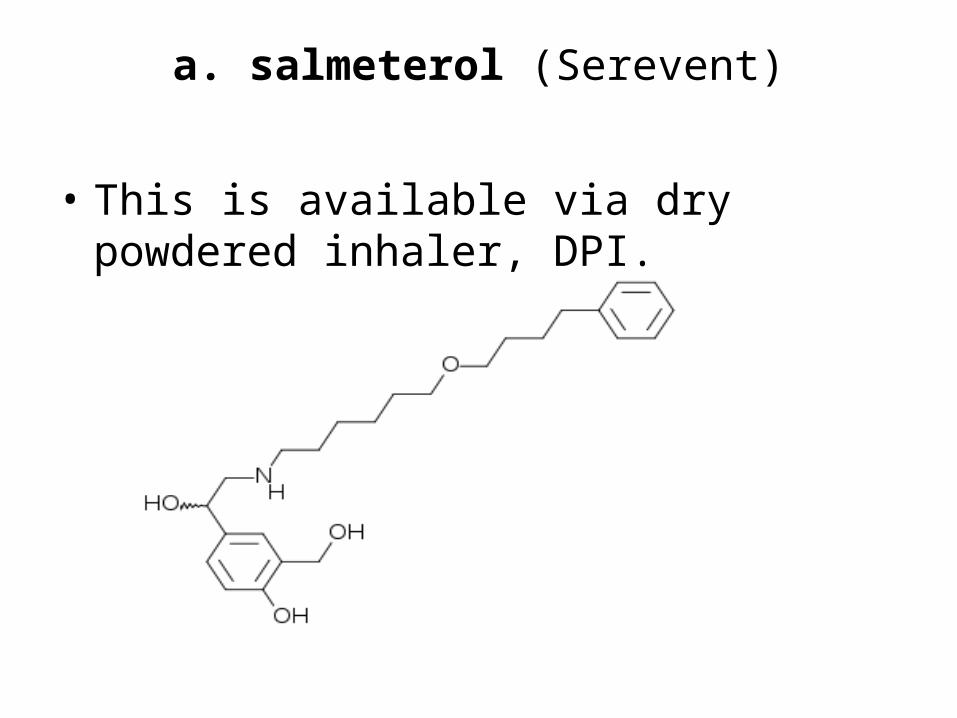
a. salmeterol (Serevent)
• This is available via dry powdered inhaler, DPI.
b. formoterol fumurate (Foradil Aerolizer, Perforomist)
• Foradil Aerolizer is administered via DPI. Perforomist, administered via SVN solution was approved by the FDA in 2007.
c. Advair Diskus
• Advair Diskus is a combination of salmeterol and the corticosteroid fluticasone.
• Patients on Advair have demonstrated better asthma control compared to those taking either drug separately.
d. arformoterol (Brovana)
• This medication, available via SVN solution has been approved by the FDA for maintenance of COPD.
7. Adverse effects of beta adrenergics
• The adverse effects of beta adrenergic bronchodilators include:
• dizziness,
• headache,
• insomnia,
• increases in blood pressure,
• nausea,
• nervousness,
• tachycardia,
• developed tolerance to bronchodilator effect,
• and the asthma paradox (an increase in death or near death situations).
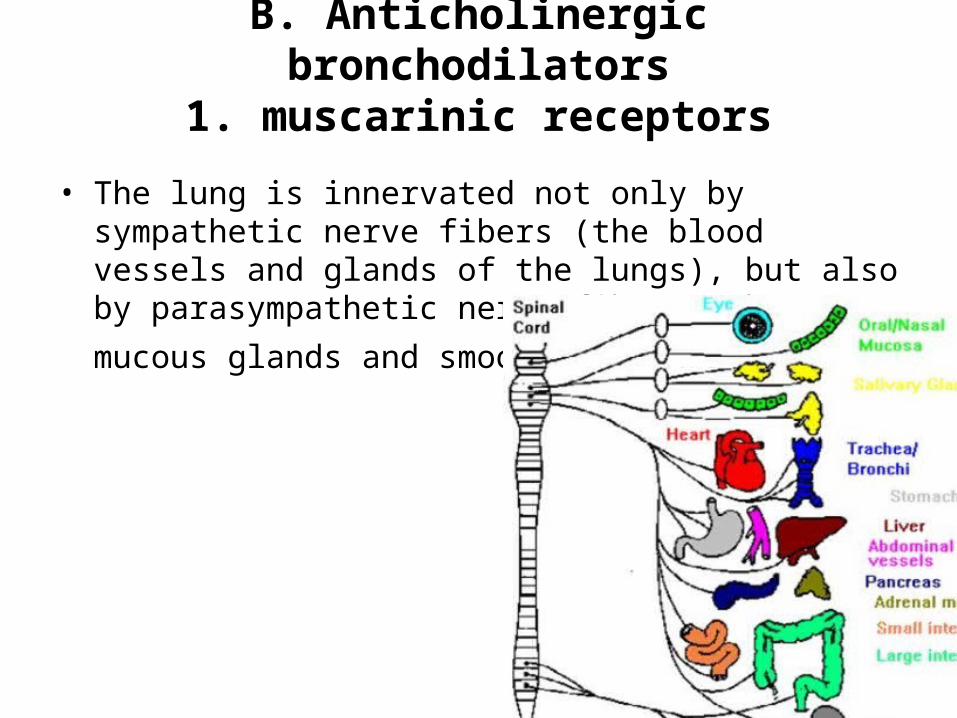
B. Anticholinergic bronchodilators1. muscarinic receptors
• The lung is innervated not only by sympathetic nerve fibers (the blood vessels and glands of the lungs), but also by parasympathetic nerve fibers (the mucous
glands and smooth muscle).
• The parasympathetic branch includes the vagus nerves, which release acetylcholine and therefore are labeled cholinergic.
• The receptors which bind acetylcholine are termed muscarinic receptors.
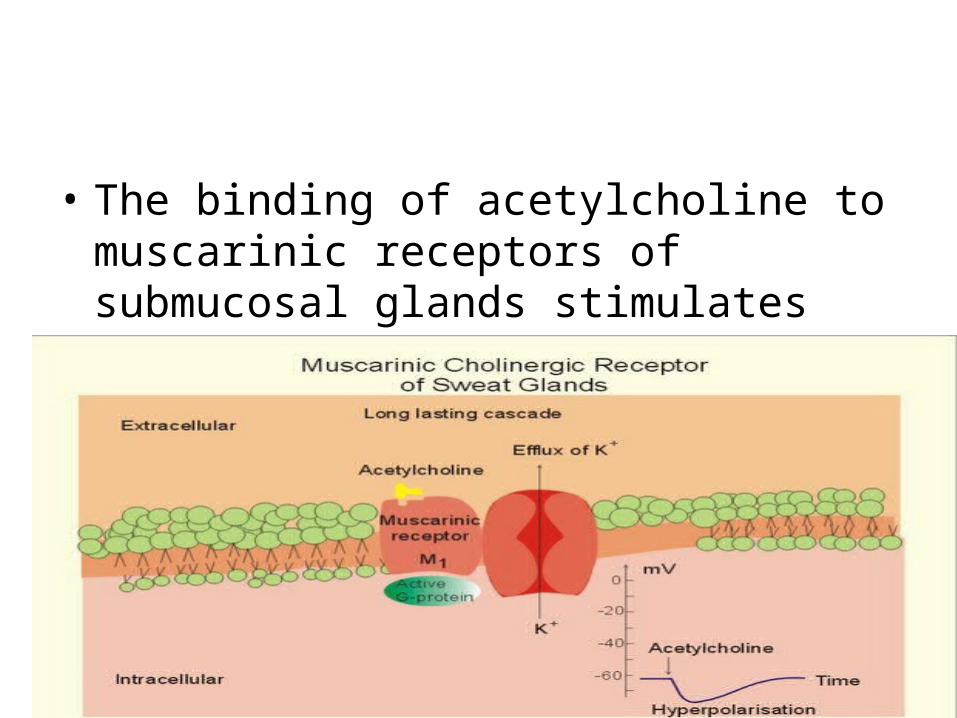
• The binding of acetylcholine to muscarinic receptors of submucosal glands stimulates secretion.
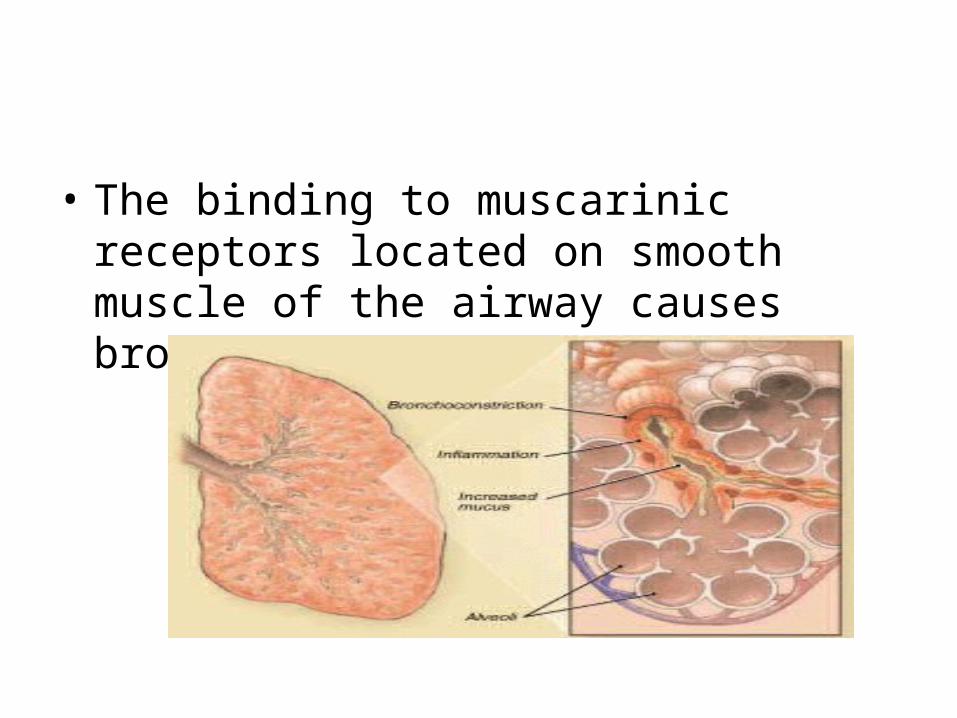
• The binding to muscarinic receptors located on smooth muscle of the airway causes bronchoconstriction.
• There are 5 subtypes of muscarinic receptors all linked to various G proteins, with a couple of different effects.
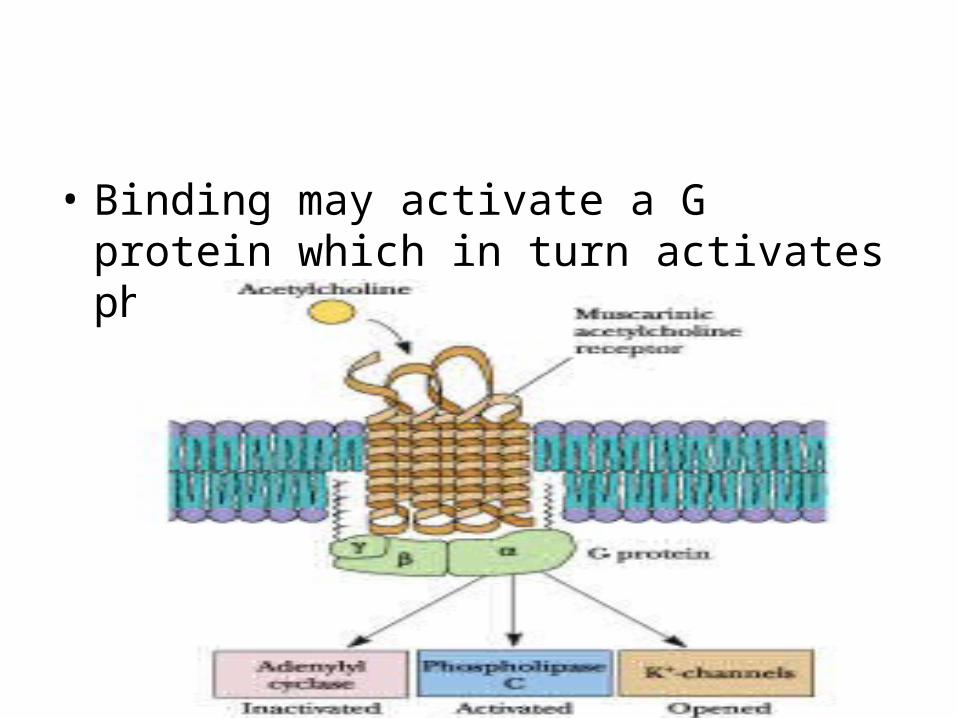
• Binding may activate a G protein which in turn activates phospholipase C.
• This initiates a cascade which ultimately leads to intracellular Ca2+ increase and either smooth muscle contraction or release of secretions from glands.
• Or, binding activates a G protein which inhibits adenylate cyclase and therefore inhibits the secondary messenger, cAMP.
• (Remember cAMP is necessary for smooth muscle relaxation as well as decreases in intracellular Ca2+).
• By blocking muscarinic receptors, anticholinergic agents cause bronchodilation as well as inhibition of secretion release from mucous glands.
• The discovery of this class of drugs arose from the use of the leaves of Datura stramonium in India for treating asthma. These leaves contain atropine, a potent inhibitor of acetylcholine.
2. anticholinergic agentsa. ipratropium bromide (Atrovent, Atrovent
HFA)
• This agent is administered via SVN or MDI. It is indicated for the treatment of COPD (maintenance prevention of airflow obstruction).
• Its onset of action is about 15 minutes and its duration is about 4-6 hours, about the same as the short acting beta adrenergics.
• However, it peaks more slowly (1-2 hours) compared to the beta adrenergics (5 minutes- 1 hour).
b. combination ipratropium bromide and albuterol
• Combivent, via MDI with CFC propellant should still be available. Combivent is anticipated to have an HFA product in 2010 or 2011.
• DuoNeb, via SVN)
c. tiotropium bromide (Spiriva)
• This agent was approved in 2005. Its long duration of action (24 hours) allows for once daily dosing. It is administered via DPI.
3. Adverse effects of anticholinergics
• The adverse effects associated with anticholinergic bronchodilators include:
• Mydriasis (pupil dilation) and cycloplegia (the lens remains “flattened” and does not thicken).
• These 2 effects can reduce drainage of the aqueous humor, leading to increased pressure in patients with glaucoma.
• Drying effects (dry mouth, lack of tears, trouble urinating, constipation)
• Increased heart rate.
C. Xanthine bronchodilators1. mechanism of action
• The mechanism by which xanthines cause bronchodilation is not conclusively known.
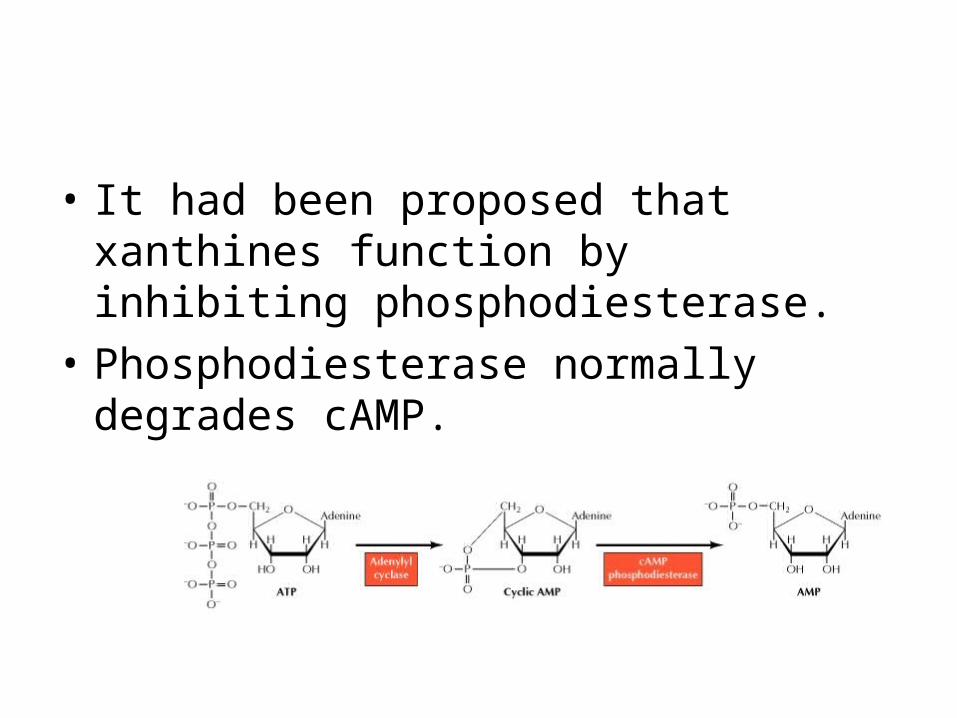
• It had been proposed that xanthines function by inhibiting phosphodiesterase.
• Phosphodiesterase normally degrades cAMP.
• By preventing this, cAMP concentrations are increased and, as with the beta adrenergics, increases in cAMP lead to relaxation of bronchial smooth muscle.
• Researchers are not positive, however, that this is the actual or only mechanism at play. An alternative theory suggests that the xanthines block adenosine.
• Adenosine is a naturally occurring compound that binds to and stimulates alpha receptors.
• By blocking these alpha receptors, the xanthines can prevent the smooth muscle contraction that is normally mediated by α1 stimulation.
• The xanthines are now generally reserved for those asthmatic and COPD patients whose symptoms remain poorly controlled despite receiving regular treatment with low dose inhaled corticosteroids and a bronchodilator (β2 adrenergic or anticholinergic).
• The very low cost of the xanthines is a consideration for economically disadvantaged patients or those in countries where health care resources are limited.
2. xanthine agents a. theophylline
• (Asmalix, Bronkodyl, Elixophyllin, Quibron-T, Respbid, Sustaire, Theobid, Theodur, Theostat, Theovent, Uniphyl)
• This is available via immediate release and timed release capsules and tablets, syrup, elixir, and injection.
b. aminophylline (Phyllocontin, Truphylline)
• This is a salt of theophylline which releases free theophylline after administration. It is available as anhydrous aminophylline (86% theophylline) or aminophylline dihydrate (79% theophylline)
c. oxtriphylline
• This is also a salt which releases 64% theophylline.
3. Adverse effects of xanthines
• The most frequently reported adverse effects associated with xanthines are:
• anxiety,
• nausea,
• tachycardia,
• and vomiting.
• Other adverse effects include
• angina,
• anorexia,
• arrhythmias,
• headache,
• insomnia
• and seizures.
II. Mast cell stabilizers
• Mast cell stabilizers are also known as cromones. They are indicated as prophylactic therapy in the management of mild asthma.
• They inhibit inflammation by preventing degranulation of mast cells, which blocks the release of the chemical mediators of inflammation.
• Their mechanism of action is not completely understood, but is believed to involve stopping Ca2+ influx into mast cells.
• Ca2+ is necessary for release of granules containing mediators of inflammation (histamine, SRS-A) from the mast cell.
• Mast cell stabilizers are not as effective as inhaled corticosteroids, but their inclusion along with a standard dose of an inhaled corticosteroid appears to improve asthma control.
• Generally, younger patients are more likely to respond favorably to this treatment regimen.
• Daily use of a mast cell stabilizer also has reduced the need for bronchodilator rescue in some clinical trials.
1. cromolyn sodium (Intal)
• This is available via SVN, MDI (HFA)
• It is also found in a nasal spray (Nasalcrom) for the prophylactic treatment of seasonal and nonseasonal allergic rhinitis.
• In terms of effectiveness, cromolyn sodium is comparable to theophylline, yet fewer side effects are reported with its use.
• When therapy is first initiated, nasal congestion may be experienced by some patients.
• Sneezing, cough, nasal itching, or burning have also been reported.
2. nedocromil sodium (Tilade CFC- free)
• Available in a MDI (HFA)
• 3. Adverse effects of mast cell stabilizers:
• throat irritation, cough, dry mouth, wheezing
III. CorticosteroidsA. Corticosteroids administered by
inhalation• Corticosteroids administered by inhalation
are indicated for the long-term control of asthma.
• They may decrease the need for systemic corticosteroids.
• Inhalation corticosteroids are being recommended by many physicians as the first-line maintenance therapy for adults with daily or frequent asthma symptoms.
• At present there are seven FDA approved inhaled corticosteroids available, and others are in development:
• 1. beclomethasone (QVAR)
• 2. budesonide (Pulmicort)
• 3. flunisolide (AeroBid)

• 4. fluticasone (Flovent)
• 5. triamcinolone (Azmacort)
• 6. mometasone (Asmanex Twisthaler)
• 7. ciclesonide (Alveso)
• The goal of all inhaled corticosteroids is to:
• produce long-lasting therapeutic effects at the site of action
• minimize systemic side effects
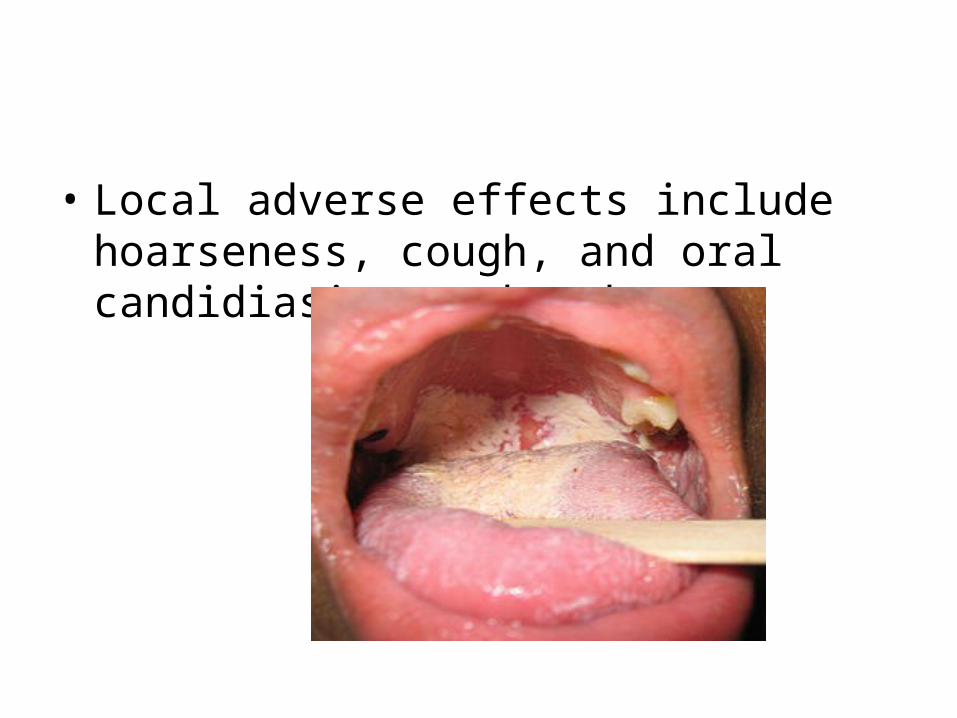
• Local adverse effects include hoarseness, cough, and oral candidiasis or thrush.
B. Corticosteroids administered intranasally
• Nasal-spray corticosteroids are considered the most effective drugs for treating severe allergic rhinitis.
• They suppress important stress and other hormones in the HPA (hypothalamic-pituitary-adrenal) axis.
• The suppression of these hormones blocks the inflammatory response that triggers an allergic attack. Nasal-spray corticosteroids include:
• 1. triamcinolone (Nasacort)
• 2. mometasone furoate (Nasonex)
• 3. fluticasone (Flonase)
• 4. beclomethasone (Beconase, Vancenase)
• 5. flunisolide (Nasalide)

• 6. budesonide (Rhinocort)
• 7. ciclesonide (Omnaris)
• Side effects of nasal steroids may include:
• Dryness, burning, stinging in the nasal passage
• Sneezing
• Headaches and nosebleed (uncommon)
C. Corticosteroids administered systemically: asthma
• Corticosteroids may be administered systemically (PO, rectally, IM, IV) in the treatment of asthma.
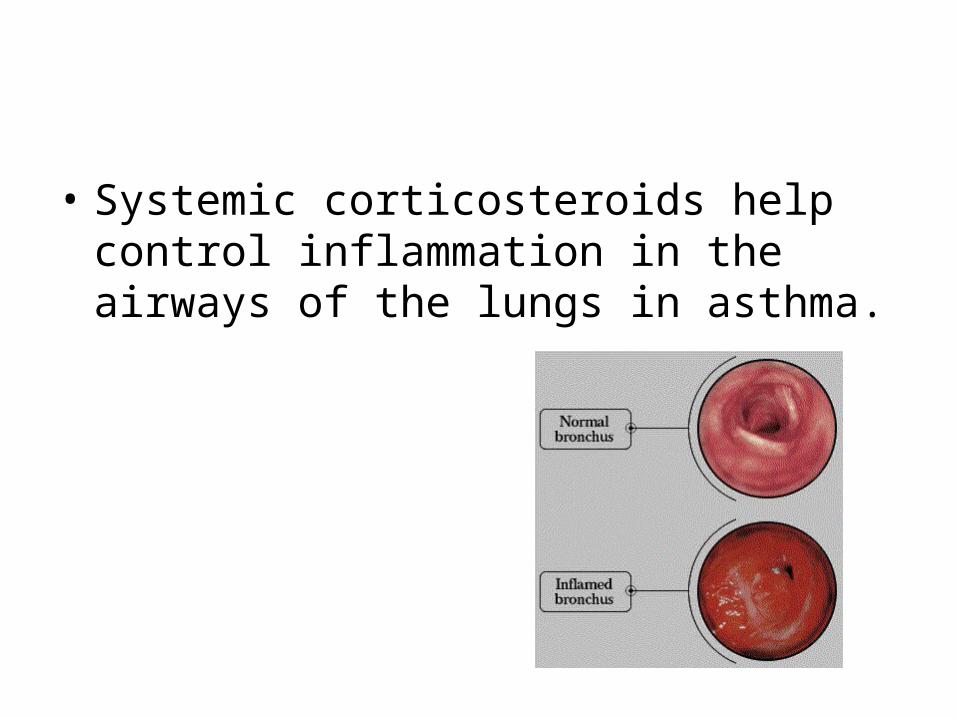
• Systemic corticosteroids help control inflammation in the airways of the lungs in asthma.
• They are used to:
• achieve relief of some asthma symptoms during a moderate or severe asthma attack (they are not rescue drugs, though)
• Get control of symptoms when starting long-term treatment of asthma after an initial diagnosis.
• Corticosteroids may make the episode shorter and prevent early recurrence of episodes.
• Oral medications are generally used for 5 to 7 days and then stopped.
• People with severe persistent asthma may need to take corticosteroids by mouth daily or every other day to control their symptoms.
• Corticosteroids administered in the treatment of asthma include:
• 1. dexamethasone (Cortastat, Decadrol, Decadron, Dexasone, Primethasone)
• 2. methylprednisolone (depMedalone, DepoMedrol, Depoject, Depopred, Duralone, Medralone, Medrol)
• 3. prednisolone (Articulose, Cotolone, Delta-Cortef, Hydeltrasol, Key-Pred, Nor-Pred, Orapred, Pediapred, Prednisol, Prelone)
• 4. prednisone (Cordrol, Deltasone, Liquid Pred, Orasone, Prednicot, Sterapred)
•

• 5. triamcinolone (Amcort, Clinacort, Triamolone, Triamonide, Trilone)
Adverse effects of systemic corticosteroids
• If systemic steroids have been prescribed for one month or less, the following side effects may arise:
• increased appetite

• Weight gain
• Sleep disturbance
• Almost everyone on systemic steroids for more than a month suffers from some adverse effects. These may include any of the following:
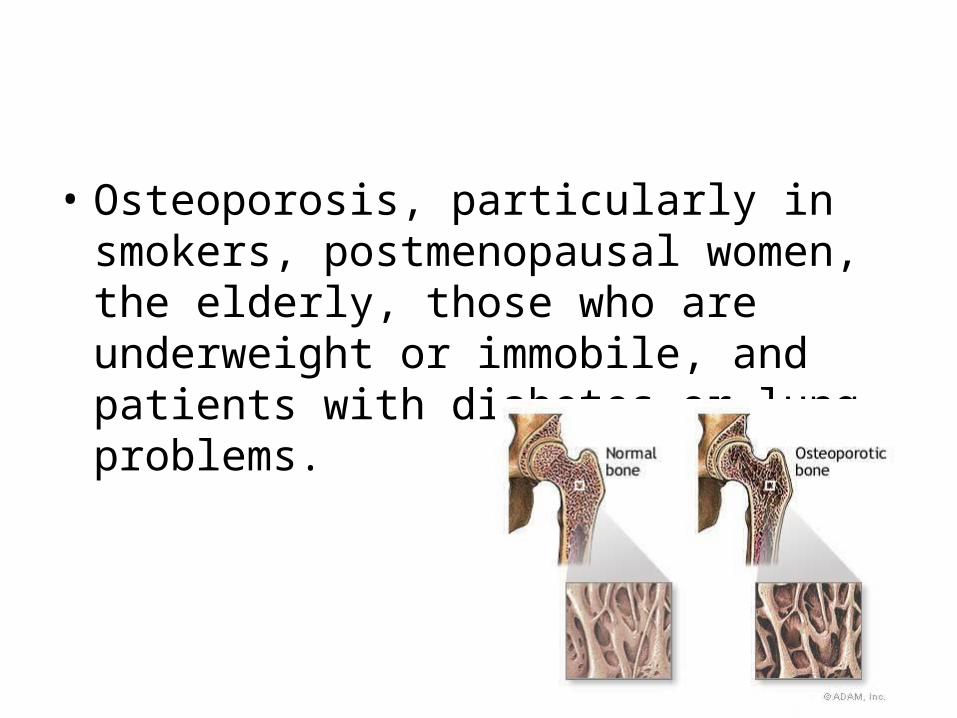
• Osteoporosis, particularly in smokers, postmenopausal women, the elderly, those who are underweight or immobile, and patients with diabetes or lung problems.
• Precipitation or aggravation of diabetes mellitus
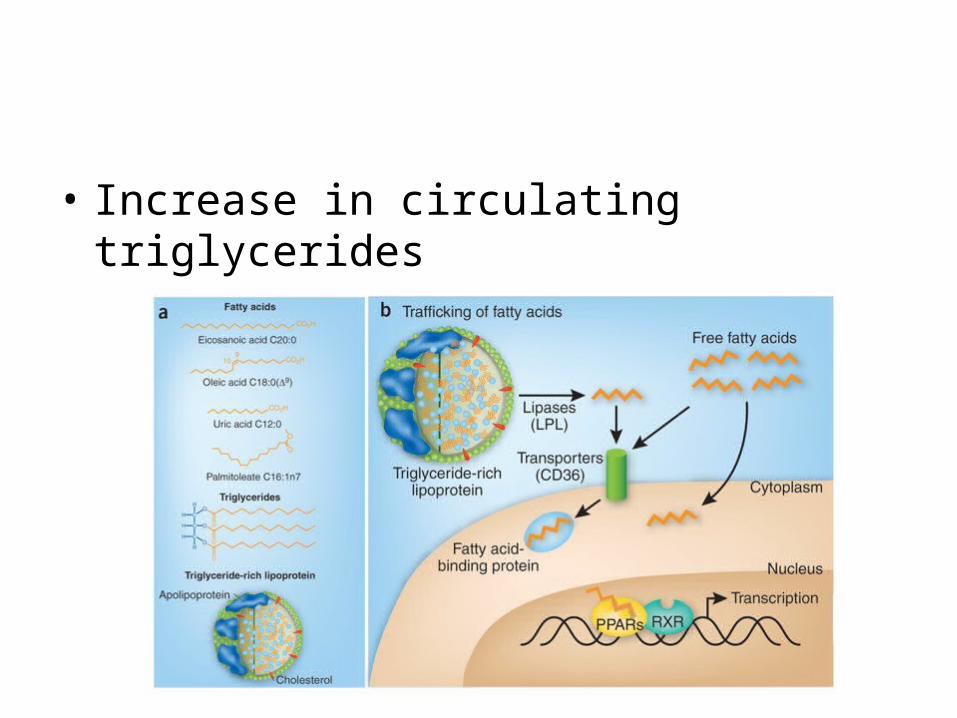
• Increase in circulating triglycerides
• A redistribution of body fat onto the face
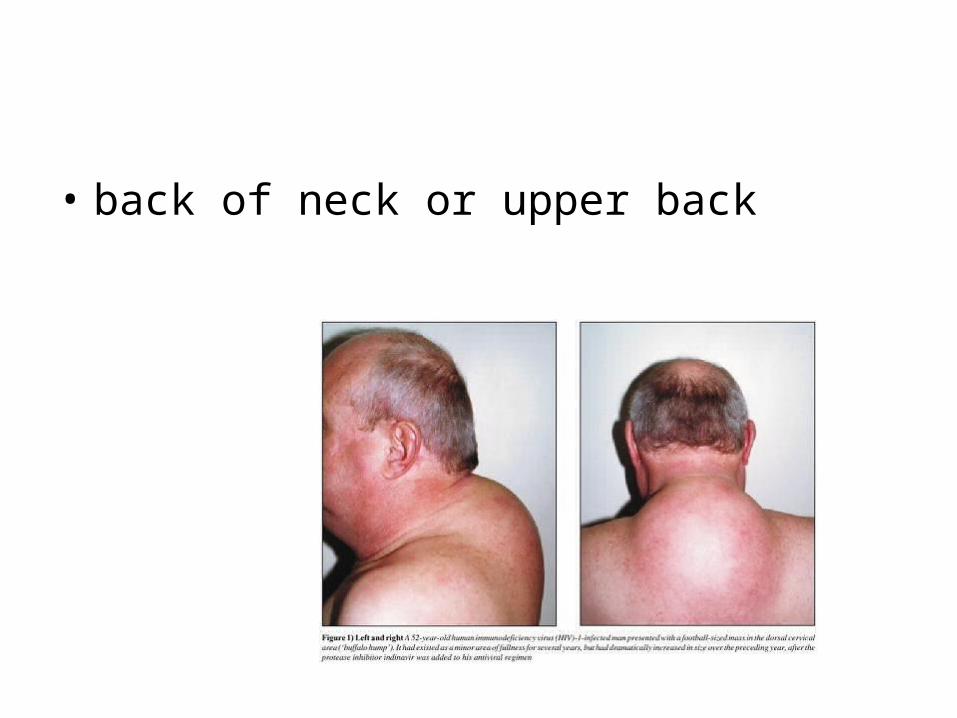
• back of neck or upper back
• or the trunk
• Salt retention: leg swelling, raised blood pressure, weight increase and heart failure.
• Psychological effects including insomnia, mood changes, increased energy, excitement, delirium or depression.

• Skin problems such as thinning and acne
IV. AntihistaminesA. histamine
• When a sensitized individual comes into contact with antigen, mast cells and basophils release histamine.
• The intensity of allergic symptoms is proportional to the amount of histamine released.
• Histamine dilates small blood vessels and capillaries which produces a transient decrease in blood pressure.
• This can result in hypotension and circulatory collapse with large histamine concentrations.
• Dilation of cerebral blood vessels stimulates pain receptors causing throbbing headache (histaminic cephalgia).
• Histamine also causes fluids to leak out of capillaries, causing congestion in nasal mucous membranes and edema and/or hives in the skin.
• Histamine also irritates sensory nerve endings, resulting in itching and pain.
• Histamine produces contraction of the smooth muscle of the bronchioles by stimulating H1 receptors, leading to breathing difficulties.
B. H1 receptor antagonists
• These drugs are used to relieve acute reactions in which histamine has already been released.
• They are usually administered orally as they are well absorbed from the GI tract. Antihistamines are classified as 1st or 2nd generation.
C. 1st generation antihistamines
• 1st generation antihistamines are characterized by nonselective interaction with both peripheral and central histamine receptors.
• They cause dryness and sedation along with relief of allergy symptoms.
• In addition, they depress sensory nerve activity, thus relieving itching and pain. 1st generation antihistamines include:
1. brompheniramine (Dimetapp Allergy):
• 12-24 mg every 12 hours
2. chloropheniramine (Chlor-Trimeton):
• 2-4 mg every 4-6 hr; available OTC
3. clemastine (Tavist):
• 1.34-2.68 mg BID, available OTC
4. diphenhydramine (Benadryl)
• 25-50 mg every 4-6 hr, sedative dose 50 mg at bedtime, available OTC
5. promethazine (Phenergan):
• 12.5 mg QID, sedative dose 25-50 mg at bedtime
6. triprolidine pseudoephedrine (Actifed):
• 2.5 mg triprolidine, 60 mg pseudoephedrine; every 4-8 hours up to 4 doses/day
D. 2nd generation antihistamines
• 2nd generation antihistamines are more selective for peripheral H1 receptors and therefore, are not sedating or drying.
• They have equal antiallergic activity to 1st generation drugs. 2nd generation antihistamines include:
1. cetirizine (Zyrtec):
• 5 or 10 mg, once a day; available OTC
• If theophylline and Zyrtec are both prescribed, the dose of theophylline will probably need to be reduced.
• Zyrtec can be administered with either erythromycin or ketaconazole, and does not lead to an increased risk of heart irregularities that is seen when these drugs are taken with some of the other 2nd generation antihistamines.
• Zyrtec does cause sleepiness in about 14% of patients.
2. fexofenadine (Allegra):
• 60 mg bid, or 180 mg once daily, also OTC
• Clinical studies indicate that co-administration with either erythromycin or ketoconazole enhances Allegra absorption, which increases the bioavailability of Allegra.
•
• Aluminum/magnesium antacids may decrease Allegra absorption, therefore decreasing its effectiveness.
3. loratadine (Claritin):
• 10 mg/day, also OTC
4. azelastine (Astelin)
• Available, by prescription as a nasal spray for treatment of allergic rhinitis.
5. desloratadine (Clarinex)
• 5 mg once daily