respiratory distress in newborns
TRANSCRIPT

Respiratory distress in Newborn
Download more documents and slide shows on The Medical Post [ www.themedicalpost.net ]
Dr. Kalpana MallaMD Pediatrics
Manipal Teaching Hospital

FREQUENT CAUSES
• Medical• TTNB – transient tachypnoea • RDS(HMD)• Aspiration syndromes• Pneumonia/sepsis• PPHN• CCF• Acidosis

FREQUENT CAUSES
• Surgical• Pneumothorax• Diaphragmatic hernia• TEF• Lobar emphysema• Phrenic nerve paralysis

Resp distress – above downwards
1) Airway obstruction A) Nasal – choanal atresia nasal edemaB) Oral cavity – macroglossia, micrognathia, GlosoptosisC) Laryngeal obstruction – laryngeal web - Subglottic stenosis of larynx - Laryngomalacia - cord paralysis

Resp distress – above downwards
D) Neck obstruction – cystic hygroma - cong goitreE) Tracheal obsruction – - Tracheomalacia - TEF - Tracheal stenosis

2) Lung parenchyma
• Aspiration syndrome (MAS)• Resp distress syndrome (HMD)• TTNB• Pneumonia • Pleural effusion• Pulmonary hemorrhage• Air leak – Pneumothorax, pneumomediastinum

3) Developmental defects
• Agenesis of lung• Hypoplasia of lung• Diagphratic hernia• Tracheal agenesis• TEF

4) Extrapulmonary
• B. asphyxia• CCF• Metabolic acidosis• Persistent pulmonary hypertension

TRANSIENT TACHYPNEA OF THE NEWBORN
GENERAL ASPECTS
• Occasionally called respiratory distress syndrome type II
• Mild and self-limited• Usually term infants, C/S and
maternal IV fluids associated• The distinctive features of
transient tachypnea are sudden recovery of the infant
Pathogenesis
• Secondary to slow absorption of fetal lung fluid resulting in decreased pulmonary compliance and tidal volume and increased dead space

CLINICAL MANIFESTATIONS
• Increased RR, no retractions, mild cyanosis - relieved by minimal oxygen (<40%)
• Expiratory grunting• Recover rapidly within 3 days • Lungs are generally clear
without rales or rhonchi

CXR
• Prominent pulmonary vascular markings
• Fluid lines in the fissures• Over aeration• flat diaphragms• occasionally, pleural fluid

CXR
• Distinguishing from HMD may be difficult
• Absence reticulogranular pattern or air bronchograms in CXR

TREATMENT
• Nothing to do• General supportive measures• Oxygen• IVF• Ventilation not required• Subsides on its own

HYALINE MEMBRANE DISEASE

INCIDENCE
• Common in premature infants • Incidence is inversely proportional
to gestational age and birth weight
• 60–80% in < 28 wk of gestational age
• 15–30% in between 32 and 36 wk
• 5% > 37 wk• Rare at term


INCREASED RISK FACTORS
• Infants of diabetic mothers• Delivery before 37 wk
gestation• Multifetal pregnancies• Cesarean section delivery• Precipitous delivery• Asphyxia• Cold stress• History of previously affected
infants

DECREASED RISK FACTORS
• Chronic or pregnancy-associated hypertension
• Maternal opiate addiction• Prolonged rupture of
membranes• Antenatal corticosteroid use

PATHOPHYSIOLOGY
• Surfactant deficiency - decreased production and secretion
• Present in amn.fluid:28-30wks, mature levels after 35 wks
• Surfactant reduce surface tension and prevent the collapse alveoli
• Alveolar atelectasis, hyaline membrane formation, and interstitial edema make the lungs less compliant, so greater pressure is required to expand the small alveoli and airways

PATHOPHYSIOLOGY (CONTD…)
• Decreased lung compliance- insufficient alveolar ventilation – result in hypercapnia
• Combination of hypercapnia, hypoxia, and acidosis → pulmonary arterial vasoconstriction → increased R → L shunting through the foramen ovale and ductus arteriosus → Pulmonary blood flow is reduced → ischemic injury cap endothelium & alveolar epithelium → leak of plasma (proteinaceous material) into the alveolar spaces

PATHOPHYSIOLOGY (CONTD…)
• leak of plasma (proteinaceous material) into the alveolar spaces →combine with fibrin & necrotic alveolar pneumocytes & form hyaline membrane
• Hyaline membranes: coagulum of sloughed cells and exudate, plastered against epithelial basement membrane

CLINICAL MANIFESTATIONS
• Resp distress - tachypnea , Intercostal and subcostal retractions Nasal flaring
• Grunting • Cyanosis - relatively
unresponsive to oxygen • Progressive worsening of
cyanosis and dyspnea • Breath sounds : harsh tubular
quality, fine rales

PROGRESSION • Severity peaks at 24-48 hours, resolution
by 72-96 hours (without surfactant therap • If not treated, BP may fall;
fatigue, cyanosis, and pallor increase, and grunting disappears as the condition worsens
• Apnea and irregular respirations : ominous
• Mixed respiratory-metabolic acidosis
• Respiratory failure

OUTCOME
• Death is rare on the 1st day • Death occurs at 2 -7 days• Associated with alveolar air
leaks (interstitial emphysema, pneumothorax) and pulmonary hemorrhage or IVH

DIAGNOSIS
• CXR : fine reticular granularity of the parenchyma and air bronchograms : typical pattern developing at 6–12hr

Diffused reticulogranular pattern

• CXR- Later:• ground glass
opacity • ABG :
progressive hypoxemia, hypercapnia, and variable metabolic acidosis

Ground glass opacity
DIFFERENTIAL DIAGNOSIS
• Early-onset sepsis: group B streptococcus
• Pneumonia • Cyanotic heart disease • Persistent pulmonary HTN • Transient tachypnea of
newborn

DIFFERENTIAL DIAGNOSIS
• Spontaneous pneumothorax• Pleural effusion• Diaphragmatic hernia • Lobar emphysema
PREVENTION
• Prevention of prematurity • Lecithin:sphingomyelin ratio in
amniotic fluid: >2 means mature lungs <1.5 means HMD
• Betamethasone to women 48hr before the delivery - between 24 and 34 wk of gestation- 6mg IM for 4 doses 12 hrs apart or 12 mg IM for 2 doses 12 hrs apart

PREVENTION (CONTD…)
• First dose of surfactant into the
trachea of symptomatic premature baby immediately after birth (prophylactic) or during the first few hours of life (early rescue)

TREATMENT: SUPPORTIVE
• Avoid hypothermia • IV Calories and fluids • Warm humidified oxygen • CPAP : prevents collapse of
surfactant-deficient alveoli • Assisted ventilation • High-frequency ventilation (HFV )
SURFACTANT THERAPY : DEFINITIVE TREATEMENT
• Multidose endotracheal instillation : 4ml/kg
• Treatment (rescue) is initiated as soon as possible in the 1st 24hr of life
• Dose repeated - via the ET tube 6–12hrly for a total of 2-4 doses
• Appropriate monitoring equipment must also be available - radiology, blood gas laboratory, and pulse oximetry
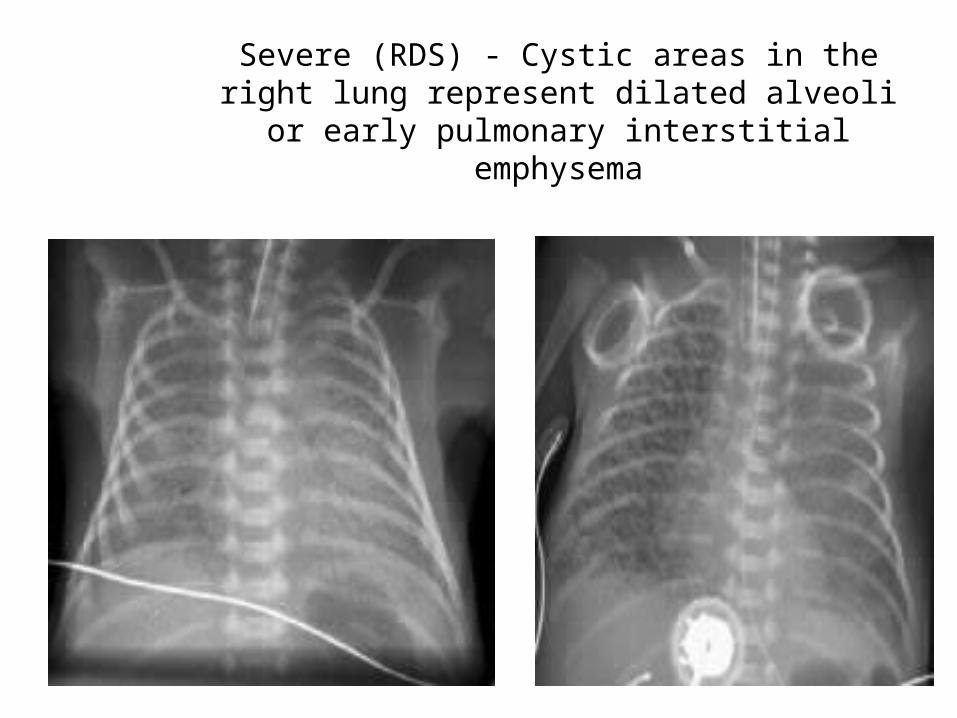
Severe (RDS) - Cystic areas in the right lung represent dilated alveoli or early
pulmonary interstitial emphysema

Acute Complications• Air Leak Syndromes
– Consider with sudden change in condition
– More common if baby receiving ventilatory support
– Pneumothorax most common• Therapy
– None if stable– Oxygen 100%– Thorocentesis: Needle or tube
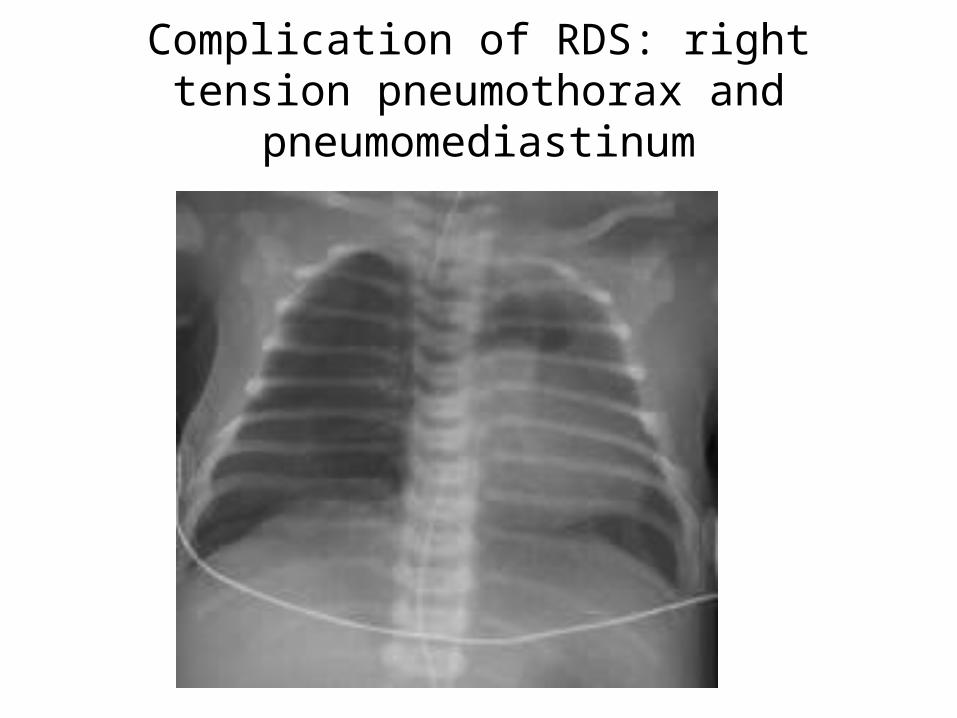
Complication of RDS: right tension pneumothorax and
pneumomediastinum

Acute Complications• Intracranial Hemorrhage
– More common at lower gestational ages– Rare above 33 weeks gestation
• Suspect if there is a sudden change in condition
• May coincide with development of air leak
• Signs: change in Fontanel, perfusion

MECONIUM ASPIRATION
GENERAL ASPECTS
• Meconium-stained amniotic fluid is found in 10–15% of births
• Meconium aspiration pneumonia develops in 5% of such cases
• 30% of them require mechanical ventilation
• 3–5% expire

Risk Factors for Meconium Passage
• Post term pregnancy• Pre-eclampsia - eclampsia• Maternal hypertension• Maternal diabetes mellitus• Abnormal fetal heart rate• IUGR• Oligohydramnios

• Precise mechanisms remain unclear • Theory - to explain the passage of meconium in
utero - The fetal bowel has little peristaltic action and the anal sphincter is contracted
• It is thought that hypoxia and academia cause the anal sphincter to relax, whilst at the same time increase the production of motilin, which promotes peristalsis.
AETIOIOGY

Meconium Aspiration SyndromePathophysiology
Meconium Aspiration SyndromePathophysiology
Airway obstruction of large and small airways
Inflammation and edema
Protein leak
Inflammatory Mediators
Direct toxicity of meconium constituents =
chemical pneumonitis
Surfactant dysfunction or inactivation
Effects of in utero hypoxemia and acidosis
Altered pulmonary vasoreactivity (PPHN)

Meconium Aspiration SyndromeDiagnosis
Meconium Aspiration SyndromeDiagnosis
Known exposure to meconium
stained amniotic fluid
Respiratory symptoms not explained
by other cause
R/O pneumonia, RDS
Spontaneous air leak

CLINICAL MANIFESTATIONS
• Either in utero or with the 1st breath meconium is aspirated into the lungs
• Tachypnea, retractions, grunting, and cyanosis : small airway obstruction
• Partial obstruction of some airways may lead to pneumothorax or pneumomediastinum
• Overdistention of the chest prominent
• Tachypnea may persist for many days or even several weeks

INVESTIGATIONS
CXR - diffuse, patchy infiltrates, consolidation, atelectasis, air leaks, hyperinflation
• ABG

Infant ActiveInfant Depressed
Intrapartum suctioning of mouth, nose, pharynx
Intubate and suction trachea
Other resuscitation as indicated
Observe
Meconium in Amniotic Fluid

Meconium Aspiration SyndromeTreatment
Meconium Aspiration SyndromeTreatment
• Ventilation strategiesAvoid air leak, check CXR Generous O2Ventilator
• Steroids ( controversial)
• Antibiotics (ampicillin, gentamicin)
• Surfactant
• Inhaled Nitric Oxide

Other Things to Watch For
• Hypoxia• Acidosis• Hypoglycemia• Hypocalcemia• End-organ damage due to perinatal
asphyxia
PREVENTION
• Fetal distress - initiating prompt delivery
• Immediate DeLee suctioning of the oropharynx after the head is delivered

PROGNOSIS
• High incidence long term pulmonary problems include -
• At 6 months - 23% MAS with regular bronchodilator therapy*
• symptomatic cough, wheezing, and persistent hyperinflation for up to 5–10 yr.

Meconium Aspiration SyndromeOutcome
Meconium Aspiration SyndromeOutcome
The ultimate prognosis depends on the extent of CNS injury from asphyxia - Increased risk of poor
neurologic outcome due to perinatal insult - seizures, CP, mental retardation

Thank youDownload more documents and slide shows on The
Medical Post [ www.themedicalpost.net ]