research article positional nystagmus in patients ......research article positional nystagmus in...
TRANSCRIPT

Research ArticlePositional Nystagmus in Patients Evaluated forDizziness and Imbalance
Richard A Roberts1 Samuel N Bittel2 and Richard E Gans3
1Alabama Hearing amp Balance Associates Inc Foley AL 36535 USA2Associated Audiologists Shawnee Mission KS 66204 USA3The American Institute of Balance Largo FL 33777 USA
Correspondence should be addressed to Richard A Roberts rrobertshearingandbalancenet
Received 31 August 2015 Accepted 3 January 2016
Academic Editor Sampath Prasad
Copyright copy 2016 Richard A Roberts et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
There is variability in the literature regarding the presence of positional nystagmus in healthy participants with reportedly normalvestibular and central nervous system function This ranges from 75 to 88 and raises an important clinical question If 88of healthy participants have positional nystagmus then how is the clinician to interpret the presence of positional nystagmus in apatient presenting with dizziness andor disequilibriumThe primary purpose of this investigation was to examine the prevalenceand characteristics of positional nystagmus in patients evaluated specifically for dizziness and imbalance Data was collected usingretrospective chart review 200 charts were randomly selected from all patients seen for evaluation of dizziness and imbalance over aperiod of eight months Clinicians independently reviewed the data from positional testing for each chart Nystagmus was presentif there was a clear slow and fast phase component and there were three beats in a 10 s time window Nystagmus direction andintensity data were collected Results indicate positional nystagmus is present in 105 to 21 of patients evaluated for dizzinessand imbalance Use of liberal criteria for determining presence of positional nystagmus (ie 3 beats in 20 sec) may account forhigher prevalence rates across other studies
1 Introduction
Evaluation for positional nystagmus is an essential com-ponent of the vestibular and equilibrium evaluation [1 2]This assessment subtest is sometimes referred to as staticpositional testing and is differentiated from Dix-Hallpikepositioningmaneuvers used to identify posterior and anteriorcanal benign paroxysmal positional vertigo (BPPV) [1 2]During this test protocol the clinician places the patient indifferent positions to look for provocation or modulationof nystagmus [1 3] Common test positions include supinehead right andor body right and head left andor body leftpositions The primary reason for moving the patient intothese positions is to alter the orientation of the labyrinthrelative to the earth gravitational vector [1 3] Changes inan existing spontaneous nystagmus or the provocation ofnystagmus due to the position can occur because of centralnervous system (CNS) involvement or peripheral vestibular
involvement Damage to the cerebellum Arnold-Chiari mal-formation multiple sclerosis vertebrobasilar insufficiencyand even medication effects may all cause vertical positionalnystagmus [1 4 5] von Brevern et al reported a varietyof types of nystagmus observed in various static positionsgeotropic ageotropic torsional and downbeat for patientswith definite migrainous vertigo [6] We have reported onageotropic horizontal nystagmus in patients with migrainouspositional vertigo (MPV) [7]
The presence of positional nystagmus could also be anindicator of peripheral vestibular involvement Of courseBPPV affecting the horizontal semicircular canals would beprovoked using these types of positions [8 9] Placing apatient with spontaneous nystagmus resulting from an acuteunilateral labyrinthine involvement into various positionsmay also alter the nystagmus Likewise when restorationof vestibular tone occurs with static compensation placingthe patient into different positions with varying levels of
Hindawi Publishing CorporationAdvances in OtolaryngologyVolume 2016 Article ID 6974836 10 pageshttpdxdoiorg10115520166974836
2 Advances in Otolaryngology
neural input from the periphery may provoke a positionalnystagmus since dynamic compensation may be incomplete[10] This positional nystagmus of peripheral origin wouldbe expected to be direction-fixed and horizontal with thefast phase of the nystagmus beating towards the intact earconsistent with Ewaldrsquos second law [3] An irritative orrecovery nystagmus whichmay deviate from this expectationand beat towards the involved ear is also possible [11]
While the presence of positional nystagmus has beenaddressed in normal controls [12 13] there are few reportsaddressing the presence of positional nystagmus in patientswith dizziness [14ndash16] Bertholon et al investigated thepresence of positional nystagmus in 490 consecutive patientspresenting to their facility with dizziness or imbalance [14]In their study both positioning (Dix-Hallpike) and staticpositions were considered The Dix-Hallpike positioning testis used to assess patients for posterior semicircular canalBPPV Interestingly when the participants with posteriorsemicircular canal BPPV are excluded these authors onlyobserved positional nystagmus in 78 of their participants(38) These authors did not include mental tasking duringtheir positional tests On the other hand these authors con-ducted their static positional testing with the patientrsquos visionenabled and eyes fixated on the examiners face Bertholonet al state that they did this so that no ldquonormalrdquo nystagmuswould be observedHowmany of the 490 patients would havepresented with positional nystagmus were this control not inplace is unknown
A second study which investigated positional nystagmusin patients with dizziness was completed by Aoki et al [15]The purpose of this investigation was to determine whichof the three different static positions was the most effectivein eliciting positional nystagmus Participants completed abody only maneuver a head only maneuver and a headand body maneuver Eye movement was recorded usingelectronystagmography (ENG) technology with eyes openunder darkened goggles From a total of 86 patients 34(40) had positional nystagmus in at least one of these threepositions There is no discussion of mental alerting tasks
Johkura et al reported that 49 (98) of their participantswith chronic dizziness had positional nystagmus while only161 (25) of their controls had positional nystagmus [16] Asin the study by Bertholon et al Johkura et al also attemptedto exclude participants with ldquonormalrdquo positional nystagmusProspective participants were excluded if positional nystag-muswas observed using ordinary Frenzel gogglesThere is nomention of the number of prospective participants excludedfor this reason
Although there are no other studies that specificallyaddress the presence of positional nystagmus in a patientpopulation with dizziness and imbalance there are studiesthat have investigated nystagmus in other types of patientpopulations For example Kiyomizu et al studied thepresence of nystagmus in patients with diagnosed psychi-atric problems using video-oculography [17] Although theirmethodology is not clear in terms of the number of positionstested or use of mental tasking the authors report thatpositional nystagmuswas observed in only 211 (48) of casesout of 227 patients with psychiatric disease Interestingly the
investigators also conducted similar testing in normal controlparticipants and found positional nystagmus in only one of107 participants which amounts to 09
Moubayed and Saliba report observing positional nystag-mus in 50 (13) of patients with vertebrobasilar insufficiencyand also 50 (13) of patients with normal vertebral arteryfunction [18] Again from the methodology it is not clearwhether the researchers usedmental tasking and also numberand type of positions that were incorporated but it is clearthat the investigators used ENG testing
From these studies it appears that there is a range preva-lence of positional nystagmus from a low of approximately8 reported by Bertholon et al to a high of 50 reported byMoubayed and Saliba Of course the specific methodologyused to assess participants for positional nystagmus is notalways clear from these reports Another interesting consid-eration is the fact that there are several studies which alsoreport a wide range of positional nystagmus in the healthynormal population These same studies range from a low of1 when normal controls are considered to a high of 88for studies specifically investigating positional nystagmusin healthy participants It is certainly intriguing that someauthors report up to 88 of patients of normal healthypatients while investigators testing for positional nystagmusin patient populations report much lower rates
The purpose of the current investigation is to report onthe prevalence of positional nystagmus in patients seen forevaluation of dizziness and disequilibrium Investigating thisis important because there appears to be much variability inthe literature This is further complicated by the wide rangeof reported prevalence of positional nystagmus in the normalhealthy populationThis is problematic for the clinician wheninterpreting nystagmus in the patient population as normal orabnormal We hypothesized that the prevalence of positionalnystagmus in our patient population would be similar to thatof Bertholon et al (when posterior canal BPPVwas excluded)and less than the higher values of 73ndash88 reported in theliterature for normal healthy participants
2 Methods
21 Participants A retrospective review of 200 charts frompatients assessed at The American Institute of Balancewas conducted Approval was obtained by the InstitutionalReview Board of The American Institute of Balance priorto initiation of this investigation The charts were selectedfrom all of the charts from patients seen for vestibular andequilibrium evaluation A table of random numbers was usedto create a list used to select charts in as random a manneras possible The data from 132 females and 68 males wereincluded in this study with an age range from 21 to 93 yearsMean age was 67 years
Although the focus of this investigationwas on the resultsof static positional testing it is important to acknowledge thatall patients underwent comprehensive evaluation by audi-ologists with specific training in vestibular assessment andmanagement Standard assessment for all patients includeddetailed discussion of history and symptoms rotary chairVNG vestibular evoked myogenic potential and postu-ral stability testing Pertinent to this investigation static
Advances in Otolaryngology 3
positional testing was completed prior to bithermal caloricstimulation as some have observed that positional nystagmusis more likely following caloric testing [12] For patients witha history consistent with possible uncompensated vestibulardysfunction lateral headshake testing was also completedand dynamic visual acuity testing was completed alsoAuditory brainstem response was only performed on patientswithout recent imaging studies Electrocochleography wasonly performed on patients with a history consistent withMenierersquos disease Standard audiometric results were alsoobtained As common in most settings that conduct vestibu-lar testing all patients were asked to refrain from substancesthat are known to have the potential to influence evaluationresults for 48 hours This would include vestibular suppres-sant medications alcohol and nicotine
22 Instrumentation BinocularVNGrecordingswere obtainedusing a commercially available system to analyze record andquantify eye movements and nystagmus (balanceback Ket-tering OH USA) This VNG system uses infrared camerashoused within goggles that contain nonlaser infrared emit-ting diodes The infrared sources supply sufficient infraredldquolightingrdquo for high quality video imaging During data col-lection for positional testing a cover was kept in placethat shielded the eyes of the patient from any light Thisallowed testing to be completed in darkness but with eyesopen All eye movement video was recorded for the entireVNG exam and was available for replay if needed Eyemovement traces were printed and available in the chart ofeach patient Positional testing was conducted using a typicalexamination table with a padded surface (Winco Ocala FLUSA) Dimensions of the examination table were 2810158401015840 times 7210158401015840and a height of 3010158401015840
23 Procedures For all patients static positional tests wereperformed during the VNG evaluation after oculomotorgaze and Hallpike but prior to caloric testing Patients werepositioned on the examination table with the VNG gogglesin place and the cover on so that the patient was in totaldarkness (vision-denied)The patient was placed in the staticpositions as shown in Figures 1(a)ndash1(e) supine head righthead left body right and body left As shown in the figure theheadwas positionedwith the neck in slight flexion for supineAlso note the slight side flexion in body right and bodyleft positioning These positional tests were conducted in avision-denied condition Patients were held in each positionfor at least 15ndash20 seconds
Once the charts were chosen using the random selectionprotocol hard copies of the eye tracing data record for eachpositional test were analyzed Analysis was completed indi-vidually by four audiologists with specific clinical expertise investibular and equilibrium assessment All 200 records werereviewed by two examiners who were the first two authorsof this investigation Then the subgroup of traces that thetwo authors identified as having positional nystagmus wasreviewed by two additional audiologists The data from tenpatients with no positional nystagmus were also included inan attempt to observe any bias the additional audiologists
might have to call normal eye movements nystagmus Nys-tagmus was considered present if (1) there was an identifiablefast and slow component and (2) there were three beatsof nystagmus observed in a 10 s time window When theexaminer observed nystagmus and the VNG system softwarealso detected nystagmus the slow phase velocity (SPV) indegrees per second (∘s) calculated by the software algorithmwas recorded If the examiner identified nystagmus that wasnot detected by the software the SPV was calculated by handas with older strip-chart technology Hand measurement wasonly necessary for four patients
3 Results
The number of patients with positional nystagmus in at leastone position is shown in Figure 2 For a given participantwithpositional nystagmus the number of clinicians out of fourpossible who reported nystagmus as present is also shownFor 10 patients only one or two of the clinicians identifiedpositional nystagmus For 32 patients at least three or allfour clinicians were in agreement that positional nystagmuswas present If this data is used to create a range from aconservative estimate of prevalence of positional nystagmus(all four clinicians had to observe the nystagmus) to a liberalestimate of prevalence of positional nystagmus (only oneclinician had to observe the nystagmus) then the range isfrom 21 to 42 out of 200 patients In other words 105 to 21of the patients had positional nystagmus None of the normaltraces were identified as having positional nystagmus
Specific data regarding the 42 patients with positionalnystagmus is shown in Table 1 The reader should notethat the interpretation provided in this table is based onhistory symptoms and overall assessment results not justpositional nystagmus data Twenty-six of 132 female patients(197) and 16 of 68 male patients (235) had positionalnystagmus There was no difference in percentage of patientswith positional nystagmus based on gender 1205942 (1 119873 =200) = 02 119901 = 0655 Thirty-two of 42 patients (762)had nystagmus in only one or two positions There was nocorrelation between patient age and number of positions withnystagmus (119903 = 0037)
Only one patient had nystagmus in all five positionsThe number of test positions with nystagmus is plotted inFigure 3 Although visual inspection suggests a trend formore frequent positional nystagmus in supine head rightand head left position compared to body right and bodyleft position this did not reach statistical significance 1205942 (4119873 = 80) = 463 119901 = 0328 In Table 2 it can be seen thatdirection-fixed nystagmus was observed significantly moreoften in patients compared to direction-changing nystagmus1205942 (1 119873 = 42) = 952 119901 lt 005 Horizontal nystagmus was
more common than vertical nystagmus when the number ofpatients and the number of positions are considered Noneof the patients had nystagmus that changed direction withina single position Seven patients had nystagmus that hadboth vertical and horizontal component (mixed) or changeddirection in different positions Four patients exhibited anageotropic nystagmus and none had a geotropic nystagmus
4 Advances in Otolaryngology
(a)
(b) (c)
(d) (e)
Figure 1The five test positions are shown (a) supine (b) head right with 90∘ rotation (c) body right (d) head left with 90∘ rotation (e) bodyleft Reprinted with permission from AIB Education Foundation Press
The nystagmus mean slow phase velocity was 156∘s moreintense for the direction-changing nystagmus compared tothe direction-fixed nystagmus This was not significantlydifferent (119905 = minus184 df = 79 and 119901 = 006) Whenall nystagmus was considered regardless of direction theaverage slow phase velocity was 464∘s
When grouped by disorder it is not clear that one positionwas more likely to elicit positional nystagmus On the otherhand some patterns appear when nystagmus direction isconsidered as a function of disorder This is shown inFigure 4 Patients with CNS involvement tended to haveleft-beating nystagmus Those patients in the nonvestibulargroup more often had upbeating nystagmus In the groups
with unilateral BPPV there was a pattern that left-beatingnystagmus was observed more often with right posteriorcanal BPPV and right beating nystagmus was observed moreoften in patients with left posterior canal BPPV
4 Discussion
41 Prevalence of Positional Nystagmus Using a strict crite-rion that all four examiners had to independently identifynystagmus as present the prevalence of positional nystagmusin our 200 patients with dizziness and imbalance was only105 When the criterion was at its least restrictive only oneexaminer had to identify positional nystagmus Even using
Advances in Otolaryngology 5
73
11
21
42
1 of 4 2 of 4 3 of 4 4 of 4 TotalClinicians observing nystagmus
0
10
20
30
40
50
Patie
nts w
ith p
ositi
onal
nys
tagm
us
Figure 2 The number of patients with positional nystagmus in atleast one position is grouped by the number of clinicians out offour who observed nystagmus The total patients with positionalnystagmus across these four groups are also provided
1821
11
18
12
Supine Head right Head leftBody right Body leftTest position
0
5
10
15
20
25
Posit
ions
with
nys
tagm
us
Figure 3 The number of test positions with observed nystagmus isshown grouped by test position
this criterion the prevalence was only 21 and this includedvertical andhorizontal nystagmusThis differsmarkedly fromsome reports [12 13 19] Our results however are similar toprevalence rates reported by others for healthy participants[16 20 21] Recall that Hajioff et al only reported positionalnystagmus in 75 of their healthy participants [20] Hajioffet al reported that 27 of their healthy participants had posi-tional nystagmus [20] and Johkura et al reported positionalnystagmus in only 19 of their normal controls [16]
Using a participant group similar to the current studyBertholon et al reported that positional nystagmus waspresent in only 20 (100 of 490) of their patients referredfor otoneurological examination [14] This is close to ourfinding in a group of patients also referred for vestibular andequilibrium evaluation A key difference is that we obtaineddata in a vision-denied condition where visual fixation wasimpossible Bertholon et al only included patients withobservable positional nystagmus during visual fixation by thepatient on the clinicianrsquos face It is possible that more of theirpatients had positional nystagmus using their VNG tech-nique with no visual fixation but these were not discussedin the study
Johkura et al reported that 61 of their participants withchronic dizziness had positional nystagmus [16] Although
this is higher than the prevalence reported in our studyand also by Bertholon et al it is still much lower thanthat reported by others for participants without dizzinessInterestingly Barber and Wright observed that positionalnystagmus was more common if testing was performedafter calorics compared to positional testing prior to caloricstimulation [12] If the data of their participants who receivedcaloric stimulation first is excluded then the prevalence ofpositional nystagmus from their report decreases from82 to73This result is identical to that of Sunami et al [19] and atleast moves closer to Johkura et al [16] but is still higher thanour results This remains intriguing since we reiterate thatBarber and Wright as well as Sunami et al used reportedlyldquonormalrdquo participants while Johkura et al used patients withchronic dizziness
One of the methodological differences between the cur-rent study and some others reporting a higher prevalence ofpositional nystagmus is that the patients were not mentallytasked during positional testing Amental task such as askingpatients to answer questions or perform simple arithmetic isoften employed as a way to keep patients from suppressingnystagmus [22] McAuley et al as well as Barber andWrightspecifically state that mental alerting tasks were used to avoidsuppression of nystagmus [12 13] It is not clear whetherSunami et al used these procedures At the opposite end ofthe prevalence data Van der Stappen et al and Hajioff et alboth used mental alerting tasks and had results similar to thecurrent study [20 21] Based on the literature it is not clearthat a lack of mental alerting explains our smaller prevalenceof positional nystagmus
The current investigation incorporated five specific testpositions Barber and Wright [12] and Sunami et al usedeight test positions [19] One might argue that using a greaternumber of test positions may lead to a higher prevalenceof positional nystagmus However McAuley et al reportthe highest prevalence of positional nystagmus of all thestudies reviewed and used only one more position (6) thanthe current study [13] Hajioff et al tested for positionalnystagmus in nine different positions and only observednystagmus in 27 of their participants [20] The number ofpositions does not seem to be the main influencing factor onprevalence of positional nystagmus
Given the variability among studies one must alsoconsider the methodology used to classify the presence ofnystagmus Several reports do not indicate this in theirmethodology [16 19ndash21] In the current study the criteriafor presence of nystagmus were as follows (1) an identifiablefast and slow component and (2) three beats of nystagmusobserved in a 10 s time window Barber and Wright consid-ered nystagmus as present when there were three consecutivebeats with a recognizable slow and fast component [12] Theytermed this a burst of nystagmus and then classified eachburst as either ldquodoubtful possible nystagmusrdquo ldquodoubtfulprobable nystagmusrdquo or ldquounequivocal nystagmusrdquo Withineach of these categories nystagmus was further classifiedas either persistent or intermittent The authors report thatpositional nystagmus was observed in 397 of 888 positionstested Yet 40 of these instances of positional nystagmuswere classified as either ldquodoubtful possible nystagmusrdquo or
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Advances in Otolaryngology
neural input from the periphery may provoke a positionalnystagmus since dynamic compensation may be incomplete[10] This positional nystagmus of peripheral origin wouldbe expected to be direction-fixed and horizontal with thefast phase of the nystagmus beating towards the intact earconsistent with Ewaldrsquos second law [3] An irritative orrecovery nystagmus whichmay deviate from this expectationand beat towards the involved ear is also possible [11]
While the presence of positional nystagmus has beenaddressed in normal controls [12 13] there are few reportsaddressing the presence of positional nystagmus in patientswith dizziness [14ndash16] Bertholon et al investigated thepresence of positional nystagmus in 490 consecutive patientspresenting to their facility with dizziness or imbalance [14]In their study both positioning (Dix-Hallpike) and staticpositions were considered The Dix-Hallpike positioning testis used to assess patients for posterior semicircular canalBPPV Interestingly when the participants with posteriorsemicircular canal BPPV are excluded these authors onlyobserved positional nystagmus in 78 of their participants(38) These authors did not include mental tasking duringtheir positional tests On the other hand these authors con-ducted their static positional testing with the patientrsquos visionenabled and eyes fixated on the examiners face Bertholonet al state that they did this so that no ldquonormalrdquo nystagmuswould be observedHowmany of the 490 patients would havepresented with positional nystagmus were this control not inplace is unknown
A second study which investigated positional nystagmusin patients with dizziness was completed by Aoki et al [15]The purpose of this investigation was to determine whichof the three different static positions was the most effectivein eliciting positional nystagmus Participants completed abody only maneuver a head only maneuver and a headand body maneuver Eye movement was recorded usingelectronystagmography (ENG) technology with eyes openunder darkened goggles From a total of 86 patients 34(40) had positional nystagmus in at least one of these threepositions There is no discussion of mental alerting tasks
Johkura et al reported that 49 (98) of their participantswith chronic dizziness had positional nystagmus while only161 (25) of their controls had positional nystagmus [16] Asin the study by Bertholon et al Johkura et al also attemptedto exclude participants with ldquonormalrdquo positional nystagmusProspective participants were excluded if positional nystag-muswas observed using ordinary Frenzel gogglesThere is nomention of the number of prospective participants excludedfor this reason
Although there are no other studies that specificallyaddress the presence of positional nystagmus in a patientpopulation with dizziness and imbalance there are studiesthat have investigated nystagmus in other types of patientpopulations For example Kiyomizu et al studied thepresence of nystagmus in patients with diagnosed psychi-atric problems using video-oculography [17] Although theirmethodology is not clear in terms of the number of positionstested or use of mental tasking the authors report thatpositional nystagmuswas observed in only 211 (48) of casesout of 227 patients with psychiatric disease Interestingly the
investigators also conducted similar testing in normal controlparticipants and found positional nystagmus in only one of107 participants which amounts to 09
Moubayed and Saliba report observing positional nystag-mus in 50 (13) of patients with vertebrobasilar insufficiencyand also 50 (13) of patients with normal vertebral arteryfunction [18] Again from the methodology it is not clearwhether the researchers usedmental tasking and also numberand type of positions that were incorporated but it is clearthat the investigators used ENG testing
From these studies it appears that there is a range preva-lence of positional nystagmus from a low of approximately8 reported by Bertholon et al to a high of 50 reported byMoubayed and Saliba Of course the specific methodologyused to assess participants for positional nystagmus is notalways clear from these reports Another interesting consid-eration is the fact that there are several studies which alsoreport a wide range of positional nystagmus in the healthynormal population These same studies range from a low of1 when normal controls are considered to a high of 88for studies specifically investigating positional nystagmusin healthy participants It is certainly intriguing that someauthors report up to 88 of patients of normal healthypatients while investigators testing for positional nystagmusin patient populations report much lower rates
The purpose of the current investigation is to report onthe prevalence of positional nystagmus in patients seen forevaluation of dizziness and disequilibrium Investigating thisis important because there appears to be much variability inthe literature This is further complicated by the wide rangeof reported prevalence of positional nystagmus in the normalhealthy populationThis is problematic for the clinician wheninterpreting nystagmus in the patient population as normal orabnormal We hypothesized that the prevalence of positionalnystagmus in our patient population would be similar to thatof Bertholon et al (when posterior canal BPPVwas excluded)and less than the higher values of 73ndash88 reported in theliterature for normal healthy participants
2 Methods
21 Participants A retrospective review of 200 charts frompatients assessed at The American Institute of Balancewas conducted Approval was obtained by the InstitutionalReview Board of The American Institute of Balance priorto initiation of this investigation The charts were selectedfrom all of the charts from patients seen for vestibular andequilibrium evaluation A table of random numbers was usedto create a list used to select charts in as random a manneras possible The data from 132 females and 68 males wereincluded in this study with an age range from 21 to 93 yearsMean age was 67 years
Although the focus of this investigationwas on the resultsof static positional testing it is important to acknowledge thatall patients underwent comprehensive evaluation by audi-ologists with specific training in vestibular assessment andmanagement Standard assessment for all patients includeddetailed discussion of history and symptoms rotary chairVNG vestibular evoked myogenic potential and postu-ral stability testing Pertinent to this investigation static
Advances in Otolaryngology 3
positional testing was completed prior to bithermal caloricstimulation as some have observed that positional nystagmusis more likely following caloric testing [12] For patients witha history consistent with possible uncompensated vestibulardysfunction lateral headshake testing was also completedand dynamic visual acuity testing was completed alsoAuditory brainstem response was only performed on patientswithout recent imaging studies Electrocochleography wasonly performed on patients with a history consistent withMenierersquos disease Standard audiometric results were alsoobtained As common in most settings that conduct vestibu-lar testing all patients were asked to refrain from substancesthat are known to have the potential to influence evaluationresults for 48 hours This would include vestibular suppres-sant medications alcohol and nicotine
22 Instrumentation BinocularVNGrecordingswere obtainedusing a commercially available system to analyze record andquantify eye movements and nystagmus (balanceback Ket-tering OH USA) This VNG system uses infrared camerashoused within goggles that contain nonlaser infrared emit-ting diodes The infrared sources supply sufficient infraredldquolightingrdquo for high quality video imaging During data col-lection for positional testing a cover was kept in placethat shielded the eyes of the patient from any light Thisallowed testing to be completed in darkness but with eyesopen All eye movement video was recorded for the entireVNG exam and was available for replay if needed Eyemovement traces were printed and available in the chart ofeach patient Positional testing was conducted using a typicalexamination table with a padded surface (Winco Ocala FLUSA) Dimensions of the examination table were 2810158401015840 times 7210158401015840and a height of 3010158401015840
23 Procedures For all patients static positional tests wereperformed during the VNG evaluation after oculomotorgaze and Hallpike but prior to caloric testing Patients werepositioned on the examination table with the VNG gogglesin place and the cover on so that the patient was in totaldarkness (vision-denied)The patient was placed in the staticpositions as shown in Figures 1(a)ndash1(e) supine head righthead left body right and body left As shown in the figure theheadwas positionedwith the neck in slight flexion for supineAlso note the slight side flexion in body right and bodyleft positioning These positional tests were conducted in avision-denied condition Patients were held in each positionfor at least 15ndash20 seconds
Once the charts were chosen using the random selectionprotocol hard copies of the eye tracing data record for eachpositional test were analyzed Analysis was completed indi-vidually by four audiologists with specific clinical expertise investibular and equilibrium assessment All 200 records werereviewed by two examiners who were the first two authorsof this investigation Then the subgroup of traces that thetwo authors identified as having positional nystagmus wasreviewed by two additional audiologists The data from tenpatients with no positional nystagmus were also included inan attempt to observe any bias the additional audiologists
might have to call normal eye movements nystagmus Nys-tagmus was considered present if (1) there was an identifiablefast and slow component and (2) there were three beatsof nystagmus observed in a 10 s time window When theexaminer observed nystagmus and the VNG system softwarealso detected nystagmus the slow phase velocity (SPV) indegrees per second (∘s) calculated by the software algorithmwas recorded If the examiner identified nystagmus that wasnot detected by the software the SPV was calculated by handas with older strip-chart technology Hand measurement wasonly necessary for four patients
3 Results
The number of patients with positional nystagmus in at leastone position is shown in Figure 2 For a given participantwithpositional nystagmus the number of clinicians out of fourpossible who reported nystagmus as present is also shownFor 10 patients only one or two of the clinicians identifiedpositional nystagmus For 32 patients at least three or allfour clinicians were in agreement that positional nystagmuswas present If this data is used to create a range from aconservative estimate of prevalence of positional nystagmus(all four clinicians had to observe the nystagmus) to a liberalestimate of prevalence of positional nystagmus (only oneclinician had to observe the nystagmus) then the range isfrom 21 to 42 out of 200 patients In other words 105 to 21of the patients had positional nystagmus None of the normaltraces were identified as having positional nystagmus
Specific data regarding the 42 patients with positionalnystagmus is shown in Table 1 The reader should notethat the interpretation provided in this table is based onhistory symptoms and overall assessment results not justpositional nystagmus data Twenty-six of 132 female patients(197) and 16 of 68 male patients (235) had positionalnystagmus There was no difference in percentage of patientswith positional nystagmus based on gender 1205942 (1 119873 =200) = 02 119901 = 0655 Thirty-two of 42 patients (762)had nystagmus in only one or two positions There was nocorrelation between patient age and number of positions withnystagmus (119903 = 0037)
Only one patient had nystagmus in all five positionsThe number of test positions with nystagmus is plotted inFigure 3 Although visual inspection suggests a trend formore frequent positional nystagmus in supine head rightand head left position compared to body right and bodyleft position this did not reach statistical significance 1205942 (4119873 = 80) = 463 119901 = 0328 In Table 2 it can be seen thatdirection-fixed nystagmus was observed significantly moreoften in patients compared to direction-changing nystagmus1205942 (1 119873 = 42) = 952 119901 lt 005 Horizontal nystagmus was
more common than vertical nystagmus when the number ofpatients and the number of positions are considered Noneof the patients had nystagmus that changed direction withina single position Seven patients had nystagmus that hadboth vertical and horizontal component (mixed) or changeddirection in different positions Four patients exhibited anageotropic nystagmus and none had a geotropic nystagmus
4 Advances in Otolaryngology
(a)
(b) (c)
(d) (e)
Figure 1The five test positions are shown (a) supine (b) head right with 90∘ rotation (c) body right (d) head left with 90∘ rotation (e) bodyleft Reprinted with permission from AIB Education Foundation Press
The nystagmus mean slow phase velocity was 156∘s moreintense for the direction-changing nystagmus compared tothe direction-fixed nystagmus This was not significantlydifferent (119905 = minus184 df = 79 and 119901 = 006) Whenall nystagmus was considered regardless of direction theaverage slow phase velocity was 464∘s
When grouped by disorder it is not clear that one positionwas more likely to elicit positional nystagmus On the otherhand some patterns appear when nystagmus direction isconsidered as a function of disorder This is shown inFigure 4 Patients with CNS involvement tended to haveleft-beating nystagmus Those patients in the nonvestibulargroup more often had upbeating nystagmus In the groups
with unilateral BPPV there was a pattern that left-beatingnystagmus was observed more often with right posteriorcanal BPPV and right beating nystagmus was observed moreoften in patients with left posterior canal BPPV
4 Discussion
41 Prevalence of Positional Nystagmus Using a strict crite-rion that all four examiners had to independently identifynystagmus as present the prevalence of positional nystagmusin our 200 patients with dizziness and imbalance was only105 When the criterion was at its least restrictive only oneexaminer had to identify positional nystagmus Even using
Advances in Otolaryngology 5
73
11
21
42
1 of 4 2 of 4 3 of 4 4 of 4 TotalClinicians observing nystagmus
0
10
20
30
40
50
Patie
nts w
ith p
ositi
onal
nys
tagm
us
Figure 2 The number of patients with positional nystagmus in atleast one position is grouped by the number of clinicians out offour who observed nystagmus The total patients with positionalnystagmus across these four groups are also provided
1821
11
18
12
Supine Head right Head leftBody right Body leftTest position
0
5
10
15
20
25
Posit
ions
with
nys
tagm
us
Figure 3 The number of test positions with observed nystagmus isshown grouped by test position
this criterion the prevalence was only 21 and this includedvertical andhorizontal nystagmusThis differsmarkedly fromsome reports [12 13 19] Our results however are similar toprevalence rates reported by others for healthy participants[16 20 21] Recall that Hajioff et al only reported positionalnystagmus in 75 of their healthy participants [20] Hajioffet al reported that 27 of their healthy participants had posi-tional nystagmus [20] and Johkura et al reported positionalnystagmus in only 19 of their normal controls [16]
Using a participant group similar to the current studyBertholon et al reported that positional nystagmus waspresent in only 20 (100 of 490) of their patients referredfor otoneurological examination [14] This is close to ourfinding in a group of patients also referred for vestibular andequilibrium evaluation A key difference is that we obtaineddata in a vision-denied condition where visual fixation wasimpossible Bertholon et al only included patients withobservable positional nystagmus during visual fixation by thepatient on the clinicianrsquos face It is possible that more of theirpatients had positional nystagmus using their VNG tech-nique with no visual fixation but these were not discussedin the study
Johkura et al reported that 61 of their participants withchronic dizziness had positional nystagmus [16] Although
this is higher than the prevalence reported in our studyand also by Bertholon et al it is still much lower thanthat reported by others for participants without dizzinessInterestingly Barber and Wright observed that positionalnystagmus was more common if testing was performedafter calorics compared to positional testing prior to caloricstimulation [12] If the data of their participants who receivedcaloric stimulation first is excluded then the prevalence ofpositional nystagmus from their report decreases from82 to73This result is identical to that of Sunami et al [19] and atleast moves closer to Johkura et al [16] but is still higher thanour results This remains intriguing since we reiterate thatBarber and Wright as well as Sunami et al used reportedlyldquonormalrdquo participants while Johkura et al used patients withchronic dizziness
One of the methodological differences between the cur-rent study and some others reporting a higher prevalence ofpositional nystagmus is that the patients were not mentallytasked during positional testing Amental task such as askingpatients to answer questions or perform simple arithmetic isoften employed as a way to keep patients from suppressingnystagmus [22] McAuley et al as well as Barber andWrightspecifically state that mental alerting tasks were used to avoidsuppression of nystagmus [12 13] It is not clear whetherSunami et al used these procedures At the opposite end ofthe prevalence data Van der Stappen et al and Hajioff et alboth used mental alerting tasks and had results similar to thecurrent study [20 21] Based on the literature it is not clearthat a lack of mental alerting explains our smaller prevalenceof positional nystagmus
The current investigation incorporated five specific testpositions Barber and Wright [12] and Sunami et al usedeight test positions [19] One might argue that using a greaternumber of test positions may lead to a higher prevalenceof positional nystagmus However McAuley et al reportthe highest prevalence of positional nystagmus of all thestudies reviewed and used only one more position (6) thanthe current study [13] Hajioff et al tested for positionalnystagmus in nine different positions and only observednystagmus in 27 of their participants [20] The number ofpositions does not seem to be the main influencing factor onprevalence of positional nystagmus
Given the variability among studies one must alsoconsider the methodology used to classify the presence ofnystagmus Several reports do not indicate this in theirmethodology [16 19ndash21] In the current study the criteriafor presence of nystagmus were as follows (1) an identifiablefast and slow component and (2) three beats of nystagmusobserved in a 10 s time window Barber and Wright consid-ered nystagmus as present when there were three consecutivebeats with a recognizable slow and fast component [12] Theytermed this a burst of nystagmus and then classified eachburst as either ldquodoubtful possible nystagmusrdquo ldquodoubtfulprobable nystagmusrdquo or ldquounequivocal nystagmusrdquo Withineach of these categories nystagmus was further classifiedas either persistent or intermittent The authors report thatpositional nystagmus was observed in 397 of 888 positionstested Yet 40 of these instances of positional nystagmuswere classified as either ldquodoubtful possible nystagmusrdquo or
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Otolaryngology 3
positional testing was completed prior to bithermal caloricstimulation as some have observed that positional nystagmusis more likely following caloric testing [12] For patients witha history consistent with possible uncompensated vestibulardysfunction lateral headshake testing was also completedand dynamic visual acuity testing was completed alsoAuditory brainstem response was only performed on patientswithout recent imaging studies Electrocochleography wasonly performed on patients with a history consistent withMenierersquos disease Standard audiometric results were alsoobtained As common in most settings that conduct vestibu-lar testing all patients were asked to refrain from substancesthat are known to have the potential to influence evaluationresults for 48 hours This would include vestibular suppres-sant medications alcohol and nicotine
22 Instrumentation BinocularVNGrecordingswere obtainedusing a commercially available system to analyze record andquantify eye movements and nystagmus (balanceback Ket-tering OH USA) This VNG system uses infrared camerashoused within goggles that contain nonlaser infrared emit-ting diodes The infrared sources supply sufficient infraredldquolightingrdquo for high quality video imaging During data col-lection for positional testing a cover was kept in placethat shielded the eyes of the patient from any light Thisallowed testing to be completed in darkness but with eyesopen All eye movement video was recorded for the entireVNG exam and was available for replay if needed Eyemovement traces were printed and available in the chart ofeach patient Positional testing was conducted using a typicalexamination table with a padded surface (Winco Ocala FLUSA) Dimensions of the examination table were 2810158401015840 times 7210158401015840and a height of 3010158401015840
23 Procedures For all patients static positional tests wereperformed during the VNG evaluation after oculomotorgaze and Hallpike but prior to caloric testing Patients werepositioned on the examination table with the VNG gogglesin place and the cover on so that the patient was in totaldarkness (vision-denied)The patient was placed in the staticpositions as shown in Figures 1(a)ndash1(e) supine head righthead left body right and body left As shown in the figure theheadwas positionedwith the neck in slight flexion for supineAlso note the slight side flexion in body right and bodyleft positioning These positional tests were conducted in avision-denied condition Patients were held in each positionfor at least 15ndash20 seconds
Once the charts were chosen using the random selectionprotocol hard copies of the eye tracing data record for eachpositional test were analyzed Analysis was completed indi-vidually by four audiologists with specific clinical expertise investibular and equilibrium assessment All 200 records werereviewed by two examiners who were the first two authorsof this investigation Then the subgroup of traces that thetwo authors identified as having positional nystagmus wasreviewed by two additional audiologists The data from tenpatients with no positional nystagmus were also included inan attempt to observe any bias the additional audiologists
might have to call normal eye movements nystagmus Nys-tagmus was considered present if (1) there was an identifiablefast and slow component and (2) there were three beatsof nystagmus observed in a 10 s time window When theexaminer observed nystagmus and the VNG system softwarealso detected nystagmus the slow phase velocity (SPV) indegrees per second (∘s) calculated by the software algorithmwas recorded If the examiner identified nystagmus that wasnot detected by the software the SPV was calculated by handas with older strip-chart technology Hand measurement wasonly necessary for four patients
3 Results
The number of patients with positional nystagmus in at leastone position is shown in Figure 2 For a given participantwithpositional nystagmus the number of clinicians out of fourpossible who reported nystagmus as present is also shownFor 10 patients only one or two of the clinicians identifiedpositional nystagmus For 32 patients at least three or allfour clinicians were in agreement that positional nystagmuswas present If this data is used to create a range from aconservative estimate of prevalence of positional nystagmus(all four clinicians had to observe the nystagmus) to a liberalestimate of prevalence of positional nystagmus (only oneclinician had to observe the nystagmus) then the range isfrom 21 to 42 out of 200 patients In other words 105 to 21of the patients had positional nystagmus None of the normaltraces were identified as having positional nystagmus
Specific data regarding the 42 patients with positionalnystagmus is shown in Table 1 The reader should notethat the interpretation provided in this table is based onhistory symptoms and overall assessment results not justpositional nystagmus data Twenty-six of 132 female patients(197) and 16 of 68 male patients (235) had positionalnystagmus There was no difference in percentage of patientswith positional nystagmus based on gender 1205942 (1 119873 =200) = 02 119901 = 0655 Thirty-two of 42 patients (762)had nystagmus in only one or two positions There was nocorrelation between patient age and number of positions withnystagmus (119903 = 0037)
Only one patient had nystagmus in all five positionsThe number of test positions with nystagmus is plotted inFigure 3 Although visual inspection suggests a trend formore frequent positional nystagmus in supine head rightand head left position compared to body right and bodyleft position this did not reach statistical significance 1205942 (4119873 = 80) = 463 119901 = 0328 In Table 2 it can be seen thatdirection-fixed nystagmus was observed significantly moreoften in patients compared to direction-changing nystagmus1205942 (1 119873 = 42) = 952 119901 lt 005 Horizontal nystagmus was
more common than vertical nystagmus when the number ofpatients and the number of positions are considered Noneof the patients had nystagmus that changed direction withina single position Seven patients had nystagmus that hadboth vertical and horizontal component (mixed) or changeddirection in different positions Four patients exhibited anageotropic nystagmus and none had a geotropic nystagmus
4 Advances in Otolaryngology
(a)
(b) (c)
(d) (e)
Figure 1The five test positions are shown (a) supine (b) head right with 90∘ rotation (c) body right (d) head left with 90∘ rotation (e) bodyleft Reprinted with permission from AIB Education Foundation Press
The nystagmus mean slow phase velocity was 156∘s moreintense for the direction-changing nystagmus compared tothe direction-fixed nystagmus This was not significantlydifferent (119905 = minus184 df = 79 and 119901 = 006) Whenall nystagmus was considered regardless of direction theaverage slow phase velocity was 464∘s
When grouped by disorder it is not clear that one positionwas more likely to elicit positional nystagmus On the otherhand some patterns appear when nystagmus direction isconsidered as a function of disorder This is shown inFigure 4 Patients with CNS involvement tended to haveleft-beating nystagmus Those patients in the nonvestibulargroup more often had upbeating nystagmus In the groups
with unilateral BPPV there was a pattern that left-beatingnystagmus was observed more often with right posteriorcanal BPPV and right beating nystagmus was observed moreoften in patients with left posterior canal BPPV
4 Discussion
41 Prevalence of Positional Nystagmus Using a strict crite-rion that all four examiners had to independently identifynystagmus as present the prevalence of positional nystagmusin our 200 patients with dizziness and imbalance was only105 When the criterion was at its least restrictive only oneexaminer had to identify positional nystagmus Even using
Advances in Otolaryngology 5
73
11
21
42
1 of 4 2 of 4 3 of 4 4 of 4 TotalClinicians observing nystagmus
0
10
20
30
40
50
Patie
nts w
ith p
ositi
onal
nys
tagm
us
Figure 2 The number of patients with positional nystagmus in atleast one position is grouped by the number of clinicians out offour who observed nystagmus The total patients with positionalnystagmus across these four groups are also provided
1821
11
18
12
Supine Head right Head leftBody right Body leftTest position
0
5
10
15
20
25
Posit
ions
with
nys
tagm
us
Figure 3 The number of test positions with observed nystagmus isshown grouped by test position
this criterion the prevalence was only 21 and this includedvertical andhorizontal nystagmusThis differsmarkedly fromsome reports [12 13 19] Our results however are similar toprevalence rates reported by others for healthy participants[16 20 21] Recall that Hajioff et al only reported positionalnystagmus in 75 of their healthy participants [20] Hajioffet al reported that 27 of their healthy participants had posi-tional nystagmus [20] and Johkura et al reported positionalnystagmus in only 19 of their normal controls [16]
Using a participant group similar to the current studyBertholon et al reported that positional nystagmus waspresent in only 20 (100 of 490) of their patients referredfor otoneurological examination [14] This is close to ourfinding in a group of patients also referred for vestibular andequilibrium evaluation A key difference is that we obtaineddata in a vision-denied condition where visual fixation wasimpossible Bertholon et al only included patients withobservable positional nystagmus during visual fixation by thepatient on the clinicianrsquos face It is possible that more of theirpatients had positional nystagmus using their VNG tech-nique with no visual fixation but these were not discussedin the study
Johkura et al reported that 61 of their participants withchronic dizziness had positional nystagmus [16] Although
this is higher than the prevalence reported in our studyand also by Bertholon et al it is still much lower thanthat reported by others for participants without dizzinessInterestingly Barber and Wright observed that positionalnystagmus was more common if testing was performedafter calorics compared to positional testing prior to caloricstimulation [12] If the data of their participants who receivedcaloric stimulation first is excluded then the prevalence ofpositional nystagmus from their report decreases from82 to73This result is identical to that of Sunami et al [19] and atleast moves closer to Johkura et al [16] but is still higher thanour results This remains intriguing since we reiterate thatBarber and Wright as well as Sunami et al used reportedlyldquonormalrdquo participants while Johkura et al used patients withchronic dizziness
One of the methodological differences between the cur-rent study and some others reporting a higher prevalence ofpositional nystagmus is that the patients were not mentallytasked during positional testing Amental task such as askingpatients to answer questions or perform simple arithmetic isoften employed as a way to keep patients from suppressingnystagmus [22] McAuley et al as well as Barber andWrightspecifically state that mental alerting tasks were used to avoidsuppression of nystagmus [12 13] It is not clear whetherSunami et al used these procedures At the opposite end ofthe prevalence data Van der Stappen et al and Hajioff et alboth used mental alerting tasks and had results similar to thecurrent study [20 21] Based on the literature it is not clearthat a lack of mental alerting explains our smaller prevalenceof positional nystagmus
The current investigation incorporated five specific testpositions Barber and Wright [12] and Sunami et al usedeight test positions [19] One might argue that using a greaternumber of test positions may lead to a higher prevalenceof positional nystagmus However McAuley et al reportthe highest prevalence of positional nystagmus of all thestudies reviewed and used only one more position (6) thanthe current study [13] Hajioff et al tested for positionalnystagmus in nine different positions and only observednystagmus in 27 of their participants [20] The number ofpositions does not seem to be the main influencing factor onprevalence of positional nystagmus
Given the variability among studies one must alsoconsider the methodology used to classify the presence ofnystagmus Several reports do not indicate this in theirmethodology [16 19ndash21] In the current study the criteriafor presence of nystagmus were as follows (1) an identifiablefast and slow component and (2) three beats of nystagmusobserved in a 10 s time window Barber and Wright consid-ered nystagmus as present when there were three consecutivebeats with a recognizable slow and fast component [12] Theytermed this a burst of nystagmus and then classified eachburst as either ldquodoubtful possible nystagmusrdquo ldquodoubtfulprobable nystagmusrdquo or ldquounequivocal nystagmusrdquo Withineach of these categories nystagmus was further classifiedas either persistent or intermittent The authors report thatpositional nystagmus was observed in 397 of 888 positionstested Yet 40 of these instances of positional nystagmuswere classified as either ldquodoubtful possible nystagmusrdquo or
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Advances in Otolaryngology
(a)
(b) (c)
(d) (e)
Figure 1The five test positions are shown (a) supine (b) head right with 90∘ rotation (c) body right (d) head left with 90∘ rotation (e) bodyleft Reprinted with permission from AIB Education Foundation Press
The nystagmus mean slow phase velocity was 156∘s moreintense for the direction-changing nystagmus compared tothe direction-fixed nystagmus This was not significantlydifferent (119905 = minus184 df = 79 and 119901 = 006) Whenall nystagmus was considered regardless of direction theaverage slow phase velocity was 464∘s
When grouped by disorder it is not clear that one positionwas more likely to elicit positional nystagmus On the otherhand some patterns appear when nystagmus direction isconsidered as a function of disorder This is shown inFigure 4 Patients with CNS involvement tended to haveleft-beating nystagmus Those patients in the nonvestibulargroup more often had upbeating nystagmus In the groups
with unilateral BPPV there was a pattern that left-beatingnystagmus was observed more often with right posteriorcanal BPPV and right beating nystagmus was observed moreoften in patients with left posterior canal BPPV
4 Discussion
41 Prevalence of Positional Nystagmus Using a strict crite-rion that all four examiners had to independently identifynystagmus as present the prevalence of positional nystagmusin our 200 patients with dizziness and imbalance was only105 When the criterion was at its least restrictive only oneexaminer had to identify positional nystagmus Even using
Advances in Otolaryngology 5
73
11
21
42
1 of 4 2 of 4 3 of 4 4 of 4 TotalClinicians observing nystagmus
0
10
20
30
40
50
Patie
nts w
ith p
ositi
onal
nys
tagm
us
Figure 2 The number of patients with positional nystagmus in atleast one position is grouped by the number of clinicians out offour who observed nystagmus The total patients with positionalnystagmus across these four groups are also provided
1821
11
18
12
Supine Head right Head leftBody right Body leftTest position
0
5
10
15
20
25
Posit
ions
with
nys
tagm
us
Figure 3 The number of test positions with observed nystagmus isshown grouped by test position
this criterion the prevalence was only 21 and this includedvertical andhorizontal nystagmusThis differsmarkedly fromsome reports [12 13 19] Our results however are similar toprevalence rates reported by others for healthy participants[16 20 21] Recall that Hajioff et al only reported positionalnystagmus in 75 of their healthy participants [20] Hajioffet al reported that 27 of their healthy participants had posi-tional nystagmus [20] and Johkura et al reported positionalnystagmus in only 19 of their normal controls [16]
Using a participant group similar to the current studyBertholon et al reported that positional nystagmus waspresent in only 20 (100 of 490) of their patients referredfor otoneurological examination [14] This is close to ourfinding in a group of patients also referred for vestibular andequilibrium evaluation A key difference is that we obtaineddata in a vision-denied condition where visual fixation wasimpossible Bertholon et al only included patients withobservable positional nystagmus during visual fixation by thepatient on the clinicianrsquos face It is possible that more of theirpatients had positional nystagmus using their VNG tech-nique with no visual fixation but these were not discussedin the study
Johkura et al reported that 61 of their participants withchronic dizziness had positional nystagmus [16] Although
this is higher than the prevalence reported in our studyand also by Bertholon et al it is still much lower thanthat reported by others for participants without dizzinessInterestingly Barber and Wright observed that positionalnystagmus was more common if testing was performedafter calorics compared to positional testing prior to caloricstimulation [12] If the data of their participants who receivedcaloric stimulation first is excluded then the prevalence ofpositional nystagmus from their report decreases from82 to73This result is identical to that of Sunami et al [19] and atleast moves closer to Johkura et al [16] but is still higher thanour results This remains intriguing since we reiterate thatBarber and Wright as well as Sunami et al used reportedlyldquonormalrdquo participants while Johkura et al used patients withchronic dizziness
One of the methodological differences between the cur-rent study and some others reporting a higher prevalence ofpositional nystagmus is that the patients were not mentallytasked during positional testing Amental task such as askingpatients to answer questions or perform simple arithmetic isoften employed as a way to keep patients from suppressingnystagmus [22] McAuley et al as well as Barber andWrightspecifically state that mental alerting tasks were used to avoidsuppression of nystagmus [12 13] It is not clear whetherSunami et al used these procedures At the opposite end ofthe prevalence data Van der Stappen et al and Hajioff et alboth used mental alerting tasks and had results similar to thecurrent study [20 21] Based on the literature it is not clearthat a lack of mental alerting explains our smaller prevalenceof positional nystagmus
The current investigation incorporated five specific testpositions Barber and Wright [12] and Sunami et al usedeight test positions [19] One might argue that using a greaternumber of test positions may lead to a higher prevalenceof positional nystagmus However McAuley et al reportthe highest prevalence of positional nystagmus of all thestudies reviewed and used only one more position (6) thanthe current study [13] Hajioff et al tested for positionalnystagmus in nine different positions and only observednystagmus in 27 of their participants [20] The number ofpositions does not seem to be the main influencing factor onprevalence of positional nystagmus
Given the variability among studies one must alsoconsider the methodology used to classify the presence ofnystagmus Several reports do not indicate this in theirmethodology [16 19ndash21] In the current study the criteriafor presence of nystagmus were as follows (1) an identifiablefast and slow component and (2) three beats of nystagmusobserved in a 10 s time window Barber and Wright consid-ered nystagmus as present when there were three consecutivebeats with a recognizable slow and fast component [12] Theytermed this a burst of nystagmus and then classified eachburst as either ldquodoubtful possible nystagmusrdquo ldquodoubtfulprobable nystagmusrdquo or ldquounequivocal nystagmusrdquo Withineach of these categories nystagmus was further classifiedas either persistent or intermittent The authors report thatpositional nystagmus was observed in 397 of 888 positionstested Yet 40 of these instances of positional nystagmuswere classified as either ldquodoubtful possible nystagmusrdquo or
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
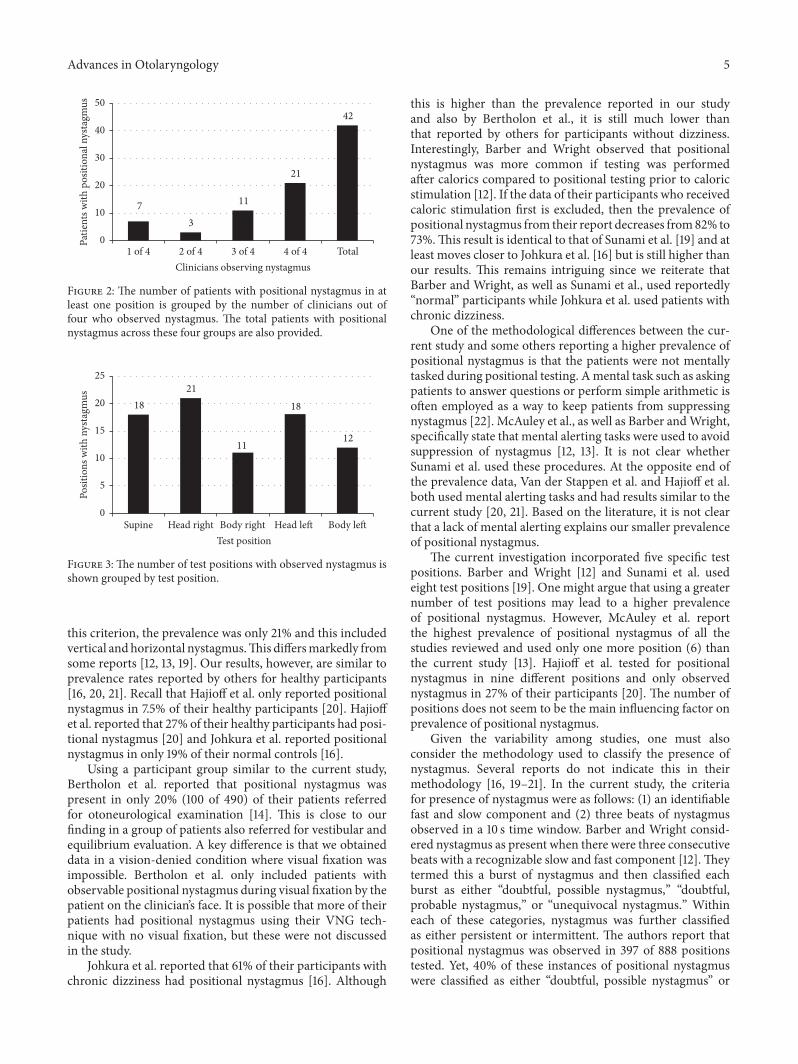
Advances in Otolaryngology 5
73
11
21
42
1 of 4 2 of 4 3 of 4 4 of 4 TotalClinicians observing nystagmus
0
10
20
30
40
50
Patie
nts w
ith p
ositi
onal
nys
tagm
us
Figure 2 The number of patients with positional nystagmus in atleast one position is grouped by the number of clinicians out offour who observed nystagmus The total patients with positionalnystagmus across these four groups are also provided
1821
11
18
12
Supine Head right Head leftBody right Body leftTest position
0
5
10
15
20
25
Posit
ions
with
nys
tagm
us
Figure 3 The number of test positions with observed nystagmus isshown grouped by test position
this criterion the prevalence was only 21 and this includedvertical andhorizontal nystagmusThis differsmarkedly fromsome reports [12 13 19] Our results however are similar toprevalence rates reported by others for healthy participants[16 20 21] Recall that Hajioff et al only reported positionalnystagmus in 75 of their healthy participants [20] Hajioffet al reported that 27 of their healthy participants had posi-tional nystagmus [20] and Johkura et al reported positionalnystagmus in only 19 of their normal controls [16]
Using a participant group similar to the current studyBertholon et al reported that positional nystagmus waspresent in only 20 (100 of 490) of their patients referredfor otoneurological examination [14] This is close to ourfinding in a group of patients also referred for vestibular andequilibrium evaluation A key difference is that we obtaineddata in a vision-denied condition where visual fixation wasimpossible Bertholon et al only included patients withobservable positional nystagmus during visual fixation by thepatient on the clinicianrsquos face It is possible that more of theirpatients had positional nystagmus using their VNG tech-nique with no visual fixation but these were not discussedin the study
Johkura et al reported that 61 of their participants withchronic dizziness had positional nystagmus [16] Although
this is higher than the prevalence reported in our studyand also by Bertholon et al it is still much lower thanthat reported by others for participants without dizzinessInterestingly Barber and Wright observed that positionalnystagmus was more common if testing was performedafter calorics compared to positional testing prior to caloricstimulation [12] If the data of their participants who receivedcaloric stimulation first is excluded then the prevalence ofpositional nystagmus from their report decreases from82 to73This result is identical to that of Sunami et al [19] and atleast moves closer to Johkura et al [16] but is still higher thanour results This remains intriguing since we reiterate thatBarber and Wright as well as Sunami et al used reportedlyldquonormalrdquo participants while Johkura et al used patients withchronic dizziness
One of the methodological differences between the cur-rent study and some others reporting a higher prevalence ofpositional nystagmus is that the patients were not mentallytasked during positional testing Amental task such as askingpatients to answer questions or perform simple arithmetic isoften employed as a way to keep patients from suppressingnystagmus [22] McAuley et al as well as Barber andWrightspecifically state that mental alerting tasks were used to avoidsuppression of nystagmus [12 13] It is not clear whetherSunami et al used these procedures At the opposite end ofthe prevalence data Van der Stappen et al and Hajioff et alboth used mental alerting tasks and had results similar to thecurrent study [20 21] Based on the literature it is not clearthat a lack of mental alerting explains our smaller prevalenceof positional nystagmus
The current investigation incorporated five specific testpositions Barber and Wright [12] and Sunami et al usedeight test positions [19] One might argue that using a greaternumber of test positions may lead to a higher prevalenceof positional nystagmus However McAuley et al reportthe highest prevalence of positional nystagmus of all thestudies reviewed and used only one more position (6) thanthe current study [13] Hajioff et al tested for positionalnystagmus in nine different positions and only observednystagmus in 27 of their participants [20] The number ofpositions does not seem to be the main influencing factor onprevalence of positional nystagmus
Given the variability among studies one must alsoconsider the methodology used to classify the presence ofnystagmus Several reports do not indicate this in theirmethodology [16 19ndash21] In the current study the criteriafor presence of nystagmus were as follows (1) an identifiablefast and slow component and (2) three beats of nystagmusobserved in a 10 s time window Barber and Wright consid-ered nystagmus as present when there were three consecutivebeats with a recognizable slow and fast component [12] Theytermed this a burst of nystagmus and then classified eachburst as either ldquodoubtful possible nystagmusrdquo ldquodoubtfulprobable nystagmusrdquo or ldquounequivocal nystagmusrdquo Withineach of these categories nystagmus was further classifiedas either persistent or intermittent The authors report thatpositional nystagmus was observed in 397 of 888 positionstested Yet 40 of these instances of positional nystagmuswere classified as either ldquodoubtful possible nystagmusrdquo or
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
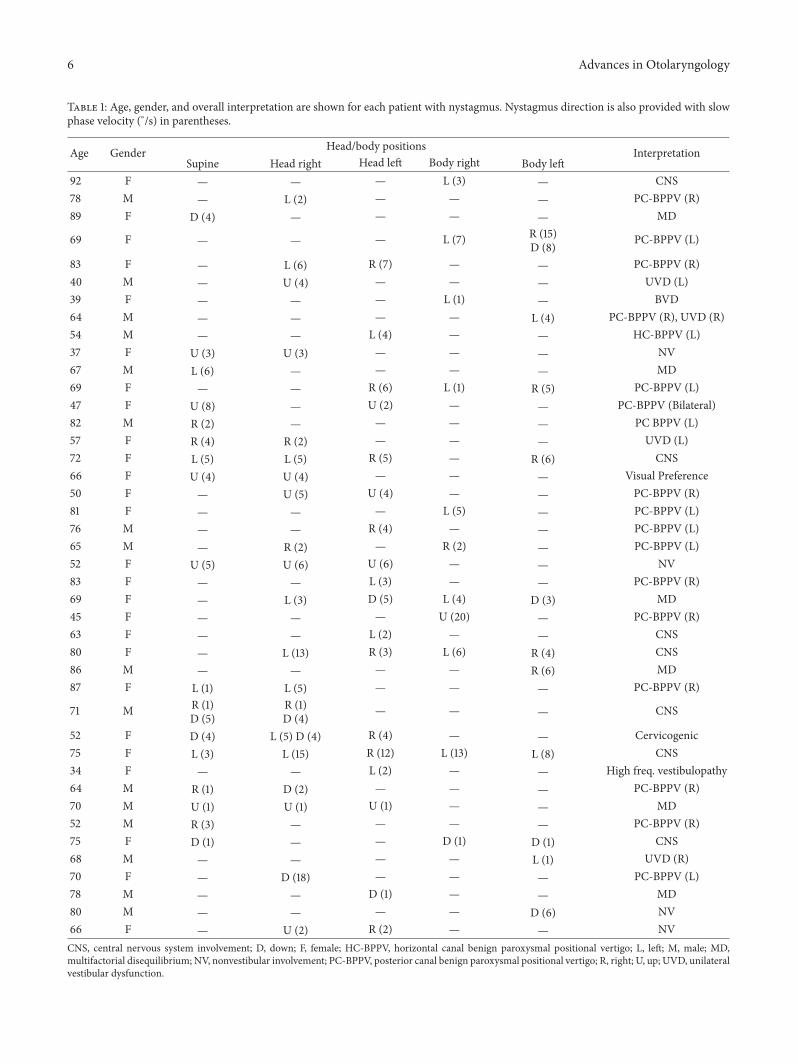
6 Advances in Otolaryngology
Table 1 Age gender and overall interpretation are shown for each patient with nystagmus Nystagmus direction is also provided with slowphase velocity (∘s) in parentheses
Age Gender Headbody positions InterpretationSupine Head right Head left Body right Body left
92 F mdash mdash mdash L (3) mdash CNS78 M mdash L (2) mdash mdash mdash PC-BPPV (R)89 F D (4) mdash mdash mdash mdash MD
69 F mdash mdash mdash L (7) R (15)D (8) PC-BPPV (L)
83 F mdash L (6) R (7) mdash mdash PC-BPPV (R)40 M mdash U (4) mdash mdash mdash UVD (L)39 F mdash mdash mdash L (1) mdash BVD64 M mdash mdash mdash mdash L (4) PC-BPPV (R) UVD (R)54 M mdash mdash L (4) mdash mdash HC-BPPV (L)37 F U (3) U (3) mdash mdash mdash NV67 M L (6) mdash mdash mdash mdash MD69 F mdash mdash R (6) L (1) R (5) PC-BPPV (L)47 F U (8) mdash U (2) mdash mdash PC-BPPV (Bilateral)82 M R (2) mdash mdash mdash mdash PC BPPV (L)57 F R (4) R (2) mdash mdash mdash UVD (L)72 F L (5) L (5) R (5) mdash R (6) CNS66 F U (4) U (4) mdash mdash mdash Visual Preference50 F mdash U (5) U (4) mdash mdash PC-BPPV (R)81 F mdash mdash mdash L (5) mdash PC-BPPV (L)76 M mdash mdash R (4) mdash mdash PC-BPPV (L)65 M mdash R (2) mdash R (2) mdash PC-BPPV (L)52 F U (5) U (6) U (6) mdash mdash NV83 F mdash mdash L (3) mdash mdash PC-BPPV (R)69 F mdash L (3) D (5) L (4) D (3) MD45 F mdash mdash mdash U (20) mdash PC-BPPV (R)63 F mdash mdash L (2) mdash mdash CNS80 F mdash L (13) R (3) L (6) R (4) CNS86 M mdash mdash mdash mdash R (6) MD87 F L (1) L (5) mdash mdash mdash PC-BPPV (R)
71 M R (1)D (5)
R (1)D (4) mdash mdash mdash CNS
52 F D (4) L (5) D (4) R (4) mdash mdash Cervicogenic75 F L (3) L (15) R (12) L (13) L (8) CNS34 F mdash mdash L (2) mdash mdash High freq vestibulopathy64 M R (1) D (2) mdash mdash mdash PC-BPPV (R)70 M U (1) U (1) U (1) mdash mdash MD52 M R (3) mdash mdash mdash mdash PC-BPPV (R)75 F D (1) mdash mdash D (1) D (1) CNS68 M mdash mdash mdash mdash L (1) UVD (R)70 F mdash D (18) mdash mdash mdash PC-BPPV (L)78 M mdash mdash D (1) mdash mdash MD80 M mdash mdash mdash mdash D (6) NV66 F mdash U (2) R (2) mdash mdash NVCNS central nervous system involvement D down F female HC-BPPV horizontal canal benign paroxysmal positional vertigo L left M male MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo R right U up UVD unilateralvestibular dysfunction
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
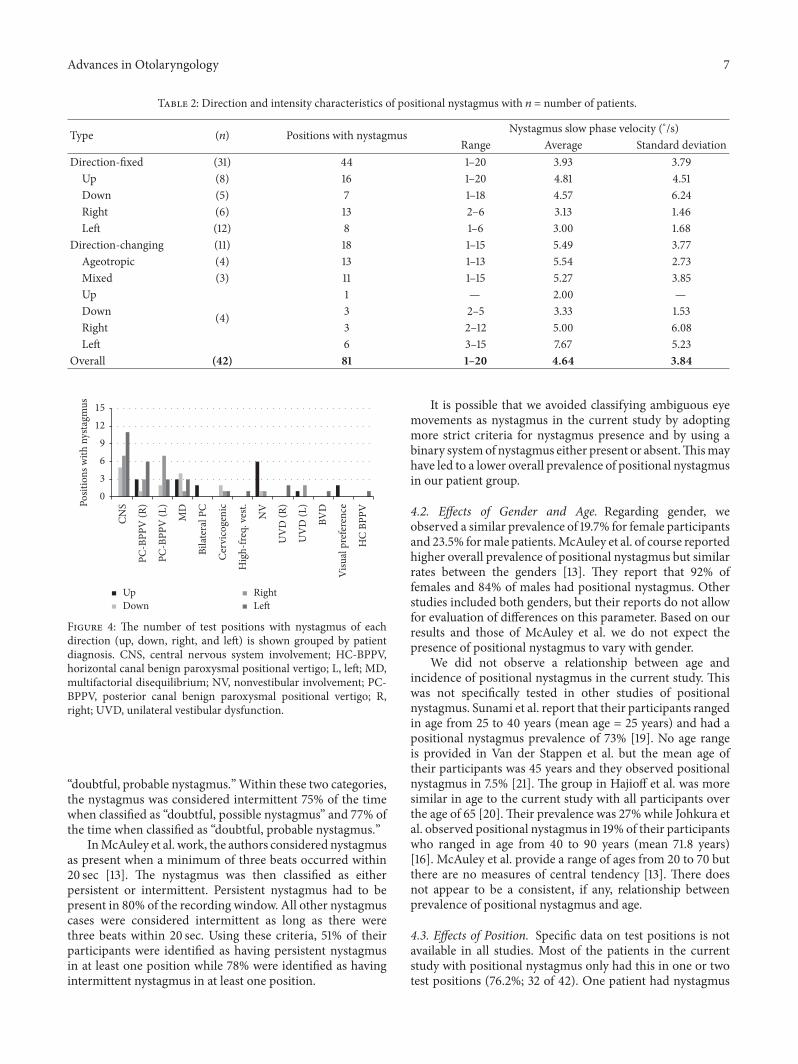
Advances in Otolaryngology 7
Table 2 Direction and intensity characteristics of positional nystagmus with 119899 = number of patients
Type (119899) Positions with nystagmus Nystagmus slow phase velocity (∘s)Range Average Standard deviation
Direction-fixed (31) 44 1ndash20 393 379Up (8) 16 1ndash20 481 451Down (5) 7 1ndash18 457 624Right (6) 13 2ndash6 313 146Left (12) 8 1ndash6 300 168
Direction-changing (11) 18 1ndash15 549 377Ageotropic (4) 13 1ndash13 554 273Mixed (3) 11 1ndash15 527 385Up
(4)
1 mdash 200 mdashDown 3 2ndash5 333 153Right 3 2ndash12 500 608Left 6 3ndash15 767 523
Overall (42) 81 1ndash20 464 384
0369
1215
Posit
ions
with
nys
tagm
us
CNS
MD
Bilat
eral
PC
Cer
vico
geni
c
Hig
h-fre
q v
est
NV
BVD
UV
D (R
)
UV
D (L
)
Visu
al p
refe
renc
e
HC
BPPV
PC-B
PPV
(R)
PC-B
PPV
(L)
UpDown
RightLeft
Figure 4 The number of test positions with nystagmus of eachdirection (up down right and left) is shown grouped by patientdiagnosis CNS central nervous system involvement HC-BPPVhorizontal canal benign paroxysmal positional vertigo L left MDmultifactorial disequilibrium NV nonvestibular involvement PC-BPPV posterior canal benign paroxysmal positional vertigo Rright UVD unilateral vestibular dysfunction
ldquodoubtful probable nystagmusrdquoWithin these two categoriesthe nystagmus was considered intermittent 75 of the timewhen classified as ldquodoubtful possible nystagmusrdquo and 77 ofthe time when classified as ldquodoubtful probable nystagmusrdquo
InMcAuley et al work the authors considered nystagmusas present when a minimum of three beats occurred within20 sec [13] The nystagmus was then classified as eitherpersistent or intermittent Persistent nystagmus had to bepresent in 80 of the recording window All other nystagmuscases were considered intermittent as long as there werethree beats within 20 sec Using these criteria 51 of theirparticipants were identified as having persistent nystagmusin at least one position while 78 were identified as havingintermittent nystagmus in at least one position
It is possible that we avoided classifying ambiguous eyemovements as nystagmus in the current study by adoptingmore strict criteria for nystagmus presence and by using abinary systemof nystagmus either present or absentThismayhave led to a lower overall prevalence of positional nystagmusin our patient group
42 Effects of Gender and Age Regarding gender weobserved a similar prevalence of 197 for female participantsand 235 formale patientsMcAuley et al of course reportedhigher overall prevalence of positional nystagmus but similarrates between the genders [13] They report that 92 offemales and 84 of males had positional nystagmus Otherstudies included both genders but their reports do not allowfor evaluation of differences on this parameter Based on ourresults and those of McAuley et al we do not expect thepresence of positional nystagmus to vary with gender
We did not observe a relationship between age andincidence of positional nystagmus in the current study Thiswas not specifically tested in other studies of positionalnystagmus Sunami et al report that their participants rangedin age from 25 to 40 years (mean age = 25 years) and had apositional nystagmus prevalence of 73 [19] No age rangeis provided in Van der Stappen et al but the mean age oftheir participants was 45 years and they observed positionalnystagmus in 75 [21] The group in Hajioff et al was moresimilar in age to the current study with all participants overthe age of 65 [20]Their prevalence was 27 while Johkura etal observed positional nystagmus in 19 of their participantswho ranged in age from 40 to 90 years (mean 718 years)[16] McAuley et al provide a range of ages from 20 to 70 butthere are no measures of central tendency [13] There doesnot appear to be a consistent if any relationship betweenprevalence of positional nystagmus and age
43 Effects of Position Specific data on test positions is notavailable in all studies Most of the patients in the currentstudy with positional nystagmus only had this in one or twotest positions (762 32 of 42) One patient had nystagmus
8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Advances in Otolaryngology
in all five test positionsThis differs from Sunami et al whoseparticipants tended to have nystagmus in more positions[19] Only 29 of their participants had nystagmus in oneor two test positions They report that 11 (7 of 65) actuallyhad nystagmus in all eight of their test positions FromTable 1 of the paper by McAuley et al 30 (13 of 43)of their participants with positional nystagmus had eitherintermittent or persistent nystagmus in all six test positions[13] Only 14 of these participants had nystagmus in one ortwo positions Based on these data there is disparity betweenstudies not only in terms of overall prevalence of positionalnystagmus but also in the frequency across positions when itis observed
There was no significant effect of test position in ourstudy McAuley et al also indicate that their distribution ofnystagmus was similar for all positions [13] It is interestingthat in our study 50 (21 of 42) of patients had nystagmus inhead right position 43 (18 of 42) had nystagmus in supineposition and 43 also had nystagmus in head left positionThis agrees with Sunami et al for head right position whofound nystagmus in 51 (33 of 65) of participants [19] Theirprevalence rates were slightly lower for supine and higher forhead left position Also Sunami et al report the highest ratesof nystagmus with lateral positioning to the right (63 41 of65) and left (58 38 of 65) [19]
44 Nystagmus Direction and Intensity In the currentstudy the direction-fixed positional nystagmus was observedalmost three times more often (738) than direction-changing nystagmus (262) This is very similar to the pro-portions reported by McAuley et al for positional nystagmusin the horizontal plane [13] McAuley et al reported that70 of their participants had a direction-fixed nystagmusand 30 had a direction-changing nystagmus Sunami etal still reported that most participants had direction-fixednystagmus but this accounted for 462 of all the participantswith positional nystagmus [19]
When positional nystagmus was present it was morelikely to occur in the horizontal plane than in the verticalplane Only four participants in Sunami et al had verticalnystagmus [19] It is noted that these authors reportedtorsional and mixed nystagmus in 31 (20 of 65) of partic-ipants Although we were unable to observe purely torsionalnystagmus in the current study patients with recordablevertical and horizontal components were included It is likelythat some of these patients would have been included in themixed group of Sunami et al bringing our data into closeragreement This may also suggest that the relative prevalenceof horizontal versus vertical positional nystagmus is probablynot as different as suggested in their data when only these twocategories are considered
Overall there is agreement among most studies of posi-tional nystagmus regarding intensity The average slow phasevelocity in the current investigation was 464∘s We foundno difference in intensity for participants with direction-fixedcompared to those with direction-changing nystagmus Vander Stappen et al reported that one of their participants had a6∘s positional nystagmus and two had slow phase velocities(SPVs) of 4∘s [21] Averaged together this is 467∘s Johkura
et al report mean SPVs of 079ndash401∘s [16] McAuley et alreport a mean SPV of 504∘s [13]
45 Nystagmus by Diagnosis The main purpose of thisinvestigation was not to determine the types of positionalnystagmus observed with different diagnoses Our patientswere not divided evenly by diagnosis and we recognize thelimitation of describing nystagmus characteristics for specificgroups when only small samples are available Howeversome interesting patterns do emerge when we considernystagmus direction For our patients with posterior canalBPPV and nystagmus in static positions there was a tendencyfor the nystagmus to beat away from the involved earRotary nystagmus during positioning testing (Dix-Hallpike)is characteristic but the presence of positional nystagmus isnot appreciated in the literature One explanation for thepresence of this type of positional nystagmus may be thatthe brainstem is attempting to compensate for the abnormalneural activity from the involved side during provocation ofsymptoms This could lead to inhibition of neural activityfrom the involved side leading to a brainstem-level asym-metry favoring the unaffected side during certain positionsThis would be expected based on Ewaldrsquos law with the fastphase of a nystagmus response beating towards the side withgreater neural activity (healthy ear) Jacobson et al providean excellent description of the process of recovery nystagmusbut central compensation is explained nicely also [11]
Adding further support of the 16 patients with unilateralBPPV 13 were specifically checked for positional nystagmusafter treatment of BPPV Eleven of these had no positionalnystagmus after the BPPV was cleared by repositioningmaneuvers This may support that the nystagmus observedin static positional testing for these individuals was related toa compensation process at the brainstem level in response tothe abnormal neural activity ultimately due to the presenceof otoconial debris in the affected semicircular canal Oncethe debris is cleared the brainstem neural activity returns tonormal and the positional nystagmus is no longer present
Four of our patients had findings that were inconsistentwith vestibular involvement Three of these patients hadupbeating nystagmus in at least one position and the fourthhad a downbeating nystagmus Vertical nystagmus is oftenreported with CNS involvement or pharmacologic influence[3 23] In these four cases a specific diagnosis could notbe determined except that the results did not appear to beconsistent with vestibular dysfunction
Our patients with positional nystagmus who were diag-nosed with CNS involvement most often had a left-beatingnystagmus Vertical nystagmus is commonwithCNS involve-ment [23] but horizontal nystagmus is also reported [6 7]Five of these seven patients had either a direction-changingpositional nystagmus or vertical nystagmus These findingsare often reported with CNS involvement or pharmacologic(positional alcohol nystagmus) effects Only two of thesepatients had horizontal nystagmus in a single position andin both cases this was a left-beating nystagmus which couldbe related to the location of their lesion It is interesting tonote that McAuley et al reported that of their participantswith direction-fixed nystagmus 47 had a leftward fast phase
Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Otolaryngology 9
compared to only 23 with a rightward fast phase [13]No explanation is given for this It is interesting that Coatsconsidered this enough to have potentially attributed sucha finding to an imprinted motor pattern possibly created byreading [24]
5 Conclusions
Historically many clinicians have held that a certain preva-lence of ldquonormalrdquo positional nystagmus exists in the healthypopulation This is supported in the literature by severalstudies in patients with reportedly intact vestibular and CNSfunction [12 13 19 24] These studies indicate that 73ndash88of patients with no reported health issues have positionalnystagmusThere is also a growing body of literature indicat-ing that positional nystagmus is not as common in healthypatients [16 20 21] ranging from only 75 to 27 Theresults of our investigation are in agreement with the lattercited investigations and suggest that positional nystagmusmay only be present in 105 to 21 of patients evaluated fordizziness and imbalance
Abbreviations
BPPV Benign paroxysmal positional vertigoCNS Central nervous systemENG ElectronystagmographyMPV Migrainous positional vertigos SecondsSPV Slow phase velocityVNG Videonystagmography
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The authors are grateful to Patricia Harrington Au D andKenton S Tarver Au D for examining patient data tracesfor the presence of positional nystagmus
References
[1] T Brandt ldquoPositional and positioning vertigo and nystagmusrdquoJournal of the Neurological Sciences vol 95 no 1 pp 3ndash28 1990
[2] R Gans and W Yellin ldquoAssessment of vestibular functionrdquo inAudiology Diagnosis R Roeser M Valente and H Hosford-Dunn Eds pp 540ndash566 Thieme New York NY USA 2007
[3] R Roberts and R Gans ldquoBackground technique interpre-tation and usefulness of positionalpositioning testingrdquo inBalance FunctionAssessment andManagement G Jacobson andN Shepard Eds pp 171ndash196 Plural Publishing Inc San DiegoCalif USA 2008
[4] R Baloh and V Honrubia Clinical Neurophysiology of theVestibular System OxfordUniversity Press NewYorkNYUSA3rd edition 2001
[5] R Leigh and D Zee The Neurology of Eye Movements OxfordUniversity Press New York NY USA 3rd edition 2001
[6] M von Brevern A Radtke A H Clarke and T LempertldquoMigrainous vertigo presenting as episodic positional vertigordquoNeurology vol 62 no 3 pp 469ndash472 2004
[7] R A Roberts R E Gans and A H Kastner ldquoDifferentiationof migrainous positional vertigo (MPV) from horizontal canalbenign paroxysmal positional vertigo (HC-BPPV)rdquo Interna-tional Journal of Audiology vol 45 no 4 pp 224ndash226 2006
[8] R Baloh ldquoHorizontal benign positional vertigordquoNeurology vol44 article 2214 1994
[9] G C Appiani G Catania and M Gagliardi ldquoA liberatorymaneuver for the treatment of horizontal canal paroxysmalpositional vertigordquo Otology and Neurotology vol 22 no 1 pp66ndash69 2001
[10] D Zee ldquoVestibular adaptationrdquo in Vestibular Rehabilitation SHerdman Ed pp 77ndash87 F A Davis Company PhiladelphiaPa USA 2nd edition 2000
[11] G P Jacobson R Pearlstein J Henderson J H Calder and JRock ldquoRecovery nystagmus revisitedrdquo Journal of the AmericanAcademy of Audiology vol 9 no 4 pp 263ndash271 1998
[12] H Barber and G Wright ldquoPositional nystagmus in normalsrdquoAdvances in Oto-Rhino-Laryngology vol 19 pp 276ndash285 1973
[13] J R McAuley J D Dickman W Mustain and V KAnand ldquoPositional nystagmus in asymptomatic human sub-jectsrdquo OtolaryngologymdashHead and Neck Surgery vol 114 no 4pp 545ndash553 1996
[14] P Bertholon S Tringali M B Faye J C Antoine and CMartin ldquoProspective study of positional nystagmus in 100consecutive patientsrdquo Annals of Otology Rhinology and Laryn-gology vol 115 no 8 pp 587ndash594 2006
[15] S Aoki Y Arai and N Kikuchi ldquoAn effective maneuver ofpositional test by turning of the head and body togetherrdquo AurisNasus Larynx vol 35 no 1 pp 37ndash40 2008
[16] K Johkura T Momoo and Y Kuroiwa ldquoPositional nystagmusin patients with chronic dizzinessrdquo Journal of Neurology Neuro-surgery and Psychiatry vol 79 no 12 pp 1324ndash1326 2008
[17] K Kiyomizu K Matsuda K Torihara et al ldquoNystagmus usingvideo-oculography in psychiatric patientsrdquo European Archivesof Oto-Rhino-Laryngology vol 266 no 8 pp 1167ndash1174 2009
[18] S P Moubayed and I Saliba ldquoVertebrobasilar insufficiencypresenting as isolated positional vertigo or dizziness a double-blind retrospective cohort studyrdquo Laryngoscope vol 119 no 10pp 2071ndash2076 2009
[19] K Sunami R Tochino T Zushi et al ldquoPositional and position-ing nystagmus in healthy subjects under videonystagmoscopyrdquoActa Oto-Laryngologica Supplementum vol 554 pp 35ndash372004
[20] D Hajioff R M Barr-Hamilton N R Colledge S J Lewis andJ A Wilson ldquoRe-evaluation of normative electronystagmogra-phy data in healthy ageingrdquo Clinical Otolaryngology amp AlliedSciences vol 25 no 4 pp 249ndash252 2000
[21] A Van der Stappen F L Wuyts and P H Van de HeyningldquoComputerized electronystagmography normative data revis-itedrdquoActa Oto-Laryngologica vol 120 no 6 pp 724ndash730 2000
[22] H O Barber and GWright ldquoRelease of nystagmus suppressionin clinical electronystagmographyrdquo Laryngoscope vol 77 no 6pp 1016ndash1027 1967
10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 Advances in Otolaryngology
[23] T Brandt Vertigo Its Multisensory Syndromes Springer Lon-don UK 1991
[24] A C Coats ldquoComputer-quantified positional nystagmus innormalsrdquo American Journal of OtolaryngologymdashHead and NeckMedicine and Surgery vol 14 no 5 pp 314ndash326 1993
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
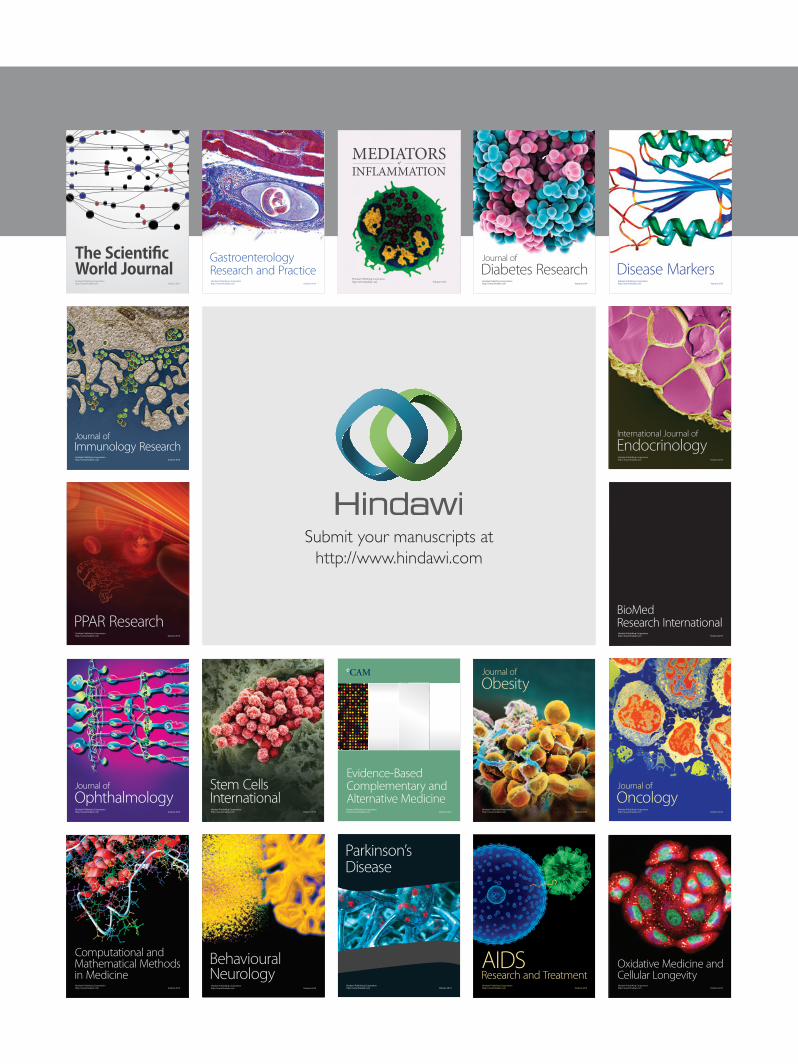
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom