reducing mmr
TRANSCRIPT
REDUCING MATERNAL MORTALITYThe contribution of the right to the highest attainable standard of health
PAUL HUNT AND JUDITH BUENO DE MESQUITA
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
I. Maternal mortality and the right to the highest attainable standard of health: the conceptual links . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
A. The scale of maternal mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
B. The causes and prevention of maternal mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
C. Legal protections provided by the right to health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
D. Freedoms and entitlements arising from the right to health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
E. The three delays model and its relationship to the right to health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
F. Other human rights . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
G. What are States’ right to health obligations to reduce maternal mortality? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
II. The right to the highest attainable standard of health: a framework for effective policies to reduce maternal mortality . . . . . . . . . . . . . . . . . 10
A. The benefits of a human rights-based approach to maternal mortality . . . . . . . . . . . . . . . . . . . . . . 11
B. The right to health and other key features, norms and principles of a human rights-based approach to maternal mortality policy making . . . . . . . . . . . . . . . . . . . . . . . . 11
C. What sort of actions might be required for a human rights-based policy for reducing maternal mortality? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
III. Reducing maternal mortality: the role of traditional human rights techniques . . . . . 14
A. Campaigning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
B. Taking court cases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
2 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
REDUCING MATERNAL MORTALITY The contribution of the right to the highest attainable standard of health
PAUL HUNT AND JUDITH BUENO DE MESQUITA
This publication has been produced with the assistance of the European Union and the United Nations PopulationFund (UNFPA). The contents of this publication are the sole responsibility of the University of Essex and can in noway be taken to reflect the views of the European Union or the United Nations Population Fund (UNFPA).
Cover photograph © Lucian Read/WpN, courtesy of UNFPA. A patient and her child at the Katsina Specialist Hospital in Nigeria. The hospitalhas a dedicated UNFPA-supported maternity ward specializing in pre- and post-natal care.

Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 3
Over half a million women die each year due to complications during pregnancy and birth. The vastmajority of these deaths are preventable.
At the Millennium Summit in 2000, States resolved to reduce maternal mortality by three quarters by theyear 2015. This commitment is encapsulated in theMillennium Development Goals, which derive from the Millennium Summit commitments, and which havecome to play a defining role in international develop-ment efforts. Goal 5 is a commitment to improve maternal health: the reduction of maternal mortality is an outcome chosen to assess progress in this regard.This resolve by States to reduce maternal mortality is not new. However, never before has the issue been given such prominence on the international development agenda.
Despite longstanding international commitments toreducing maternal mortality, so far progress has beendisappointing.2 This briefing illustrates how humanrights – and the right to the highest attainable standardof health (“right to health”) in particular – can contribute new impetus, frameworks and strategies for reducing maternal mortality.
In recent years, there has been increased recognitionthat reducing maternal mortality is not just an issue of development, but also an issue of human rights.Preventable maternal mortality occurs where there is afailure to give effect to the rights of women to health,equality and non-discrimination. Preventable maternalmortality also often represents a violation of a woman’sright to life.
Maternal health has a particularly close relationshipwith the right to the highest attainable standard ofhealth. This fundamental human right is recognised in the International Covenant on Economic, Social and Cultural Rights, as well as other internationalhuman rights treaties. The right to health includes entitlements to goods and services, including sexual and reproductive health care and information. Itrequires action to break down political, economic, socialand cultural barriers that women face in accessing theinterventions that can prevent maternal mortality. It requires participation by stakeholders in policy andservice development. And it requires accountability for maternal mortality. In short, the promotion and protection of the right to health demands actions that lead to a significant and sustained reduction inmaternal mortality.
This briefing introduces the contribution of the rightto the highest attainable standard of health to reducingmaternal mortality. This contribution is twofold. Theright to health provides: a) A framework for designing effective policies to
reduce maternal mortality;b) Tools and strategies for advocacy and accountability
for reducing maternal mortality.
Entitlements and obligations arising from the right to health underpin both of these contributions and aredescribed in the first chapter of this briefing. Policymaking and the role of traditional human rights tech-niques are explored in the second and third chaptersrespectively. This briefing indicates key contributions thatthe right to health can make in the context of policymaking and through the human rights community’s traditional techniques, such as letter writing campaigns,litigation and advocacy. It also indicates key actions thatmay be required by policy makers and the human rightscommunity. The briefing does not, however, providedetailed guidance on to how to operationalize the rightto health in the context of maternal mortality.
The right to health should lie at the heart of thehuman rights response to maternal mortality. The rightto health is intimately connected to other human rights– including the rights to life and education – which arealso highly relevant in the struggle against maternalmortality. While this briefing focuses on the right tohealth, it also gives some attention to the contributionof other human rights.3
INTRODUCTION
REDUCING
MATERNAL MORTALITY
IS NOT JUST AN ISSUE
OF DEVELOPMENT,
BUT ALSO AN ISSUE
OF HUMAN RIGHTS
INTRODUCTION
Globally, around 80 per cent of maternal deaths are dueto obstetric complications; mainly haemorrhage, sepsis,unsafe abortion, pre-eclampsia and eclampsia, and pro-longed or obstructed labour.9 Complications of unsafeabortions account for 13 per cent of maternal deathsworldwide, and 19 per cent of maternal deaths in South America.10
Almost all cases of maternal mortality are preventa-ble. An estimated 74 per cent of maternal deaths couldbe averted if all women had access to the interventionsfor preventing or treating pregnancy and birth compli-cations, in particular emergency obstetric care.11 Inmany countries with high maternal mortality rates,there is a need to increase provision of appropriate
quality services. Poverty, gender and other inequalities, a lack of information, weak health systems, a lack ofpolitical commitment, and cultural barriers are otherobstacles that need to be overcome if women are toaccess technical services and information that can often prevent maternal mortality and morbidity.
In the last twenty years, a series of international commitments and initiatives has pledged to reducematernal mortality. While many countries have madeprogress in reducing maternal mortality, progress hasstagnated or been reversed in many of the countrieswith the highest burden of maternal mortality:12 Mostparts of the world are off-track to meet the MDG targetof reducing maternal mortality.13
In 2000, the estimated number of maternal deathsworldwide was 529,000. 95 per cent of these deathsoccurred in Africa and Asia.4 While women in developedcountries have only a 1-in-2,800 chance of dying inchildbirth — and a 1-in-8,700 chance in some countries— women in Africa have a 1-in-20 chance. In severalcountries the lifetime risk is greater than 1 in 10.5
For every woman who dies from obstetric complica-tions, approximately 30 more suffer injuries, infectionand disabilities.6 In 1999, for example, WHO estimatedthat over 2 million women living in developing countriesremain untreated for obstetric fistula, a devastatinginjury of childbirth.
There is no single cause of death and disability formen between the ages of 15 and 44 that is close to themagnitude of maternal death and disability.7
Women living in poverty and in rural areas, andwomen belonging to ethnic minorities or indigenouspopulations, are among those particularly at risk.8
Complications from pregnancy and childbirth are theleading cause of death for 15-19 year old women andadolescent girls in developing countries.
These deeply shocking statistics and facts revealchronic and entrenched health inequalities. First, the burden of maternal mortality is borne disproportionatelyby developing countries. Second, in many countries, marginalised women, such as women living in povertyand ethnic minority and indigenous women, are morevulnerable to maternal mortality. Third, maternal mortali-ty and morbidity rates are often indicative of inequalitiesbetween men and women in their enjoyment of the rightto the highest attainable standard of health.
4 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
MATERNAL MORTALITY AND THE RIGHT TO HEALTH: THE CONCEPTUAL LINKS
MATERNAL MORTALITY AND THE RIGHT TO THE HIGHEST ATTAINABLE STANDARD OF HEALTH: THE CONCEPTUAL LINKS
I.
A. THE SCALE OF MATERNAL MORTALITY
B. THE CAUSES AND PREVENTION OF MATERNAL MORTALITY
Photograph © J. Isaac,courtesy of UNFPA.Mothers and children inDjibo, on the border withMali, Burkina Faso.
ALMOST ALL CASES OF MATERNAL
MORTALITY ARE PREVENTABLE
In recent years, there has been a deepening conceptualunderstanding of maternal mortality as a human rightsissue.14 Maternal mortality and morbidity are connectedto a number of human rights, in particular the right tothe highest attainable standard of health.
The right to the highest attainable standard of healthis legally protected by international human rightstreaties including the Convention on the Elimination ofAll Forms of Discrimination Against Women (CEDAW),and the International Covenant on Economic, Social andCultural Rights (ICESCR). It is also recognised in regionaltreaties, as well as by the domestic constitutions andlaws of many countries worldwide.
Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 5
The right to health takes into account an individual'sbiological and socio-economic preconditions, as well asa State's available resources. It is not a right to behealthy: it is a right to a variety of services, facilities,goods and conditions that promote and protect thehighest attainable standard of health.
The right to an effective and integrated health systemThe right to health should be broadly understood as an entitlement to an effective and integrated healthsystem, encompassing health care and the underlyingdeterminants of health, which is responsive to nationaland local priorities, and accessible to all.16 An equitable,well-resourced, accessible and integrated health systemis widely accepted as a vital pre-condition for guaran-teeing women’s access to the interventions that canprevent or treat the causes of maternal deaths.17
Entitlements to specific goods and services connected to reproductive health careThe right to health includes entitlements to a range ofhealth interventions which have an important role to
play in reducing maternal mortality. These include:
� Emergency obstetric care (EmOC);18
� A skilled birth attendant;19
� Education and information on sexual and reproductive health;20
� Safe abortion services where not against the law;21
� Other sexual and reproductive health care services,such as family planning services;22
� Primary health care services.23
The State has an obligation to provide these goods andservices in order to prevent maternal mortality. Particularattention must be given to EmOC. As Lynn Freedman hasemphasised: “We know from health research and experi-ence that not all interventions are equal... if the humanright in question is the right not to die an avoidabledeath in pregnancy and childbirth, then the first line ofappropriate measures that will move progressivelytoward the realisation of the right is the implementationof EmOC. In a human rights analysis, EmOC is not justone good idea among many. It is an obligation.” 24
C. LEGAL PROTECTIONS PROVIDED BY THE RIGHT TO HEALTH
D. FREEDOMS AND ENTITLEMENTS ARISING FROM
THE RIGHT TO HEALTH
International treaties include entitlements and corresponding obligations on States which are highlyrelevant in the context of reducing maternal mortality(Box 1). If fulfilled, these entitlements and obligationswould entail a reduction of maternal mortality. The features of the right to health are set out most fully in General Comments, which are authoritative interpretations of treaty provisions adopted by the bodies responsible for monitoring implementation of treaties.15 The following paragraphs draw on treaties and General Comments to set out key features of the right to health in the context of maternal mortality.
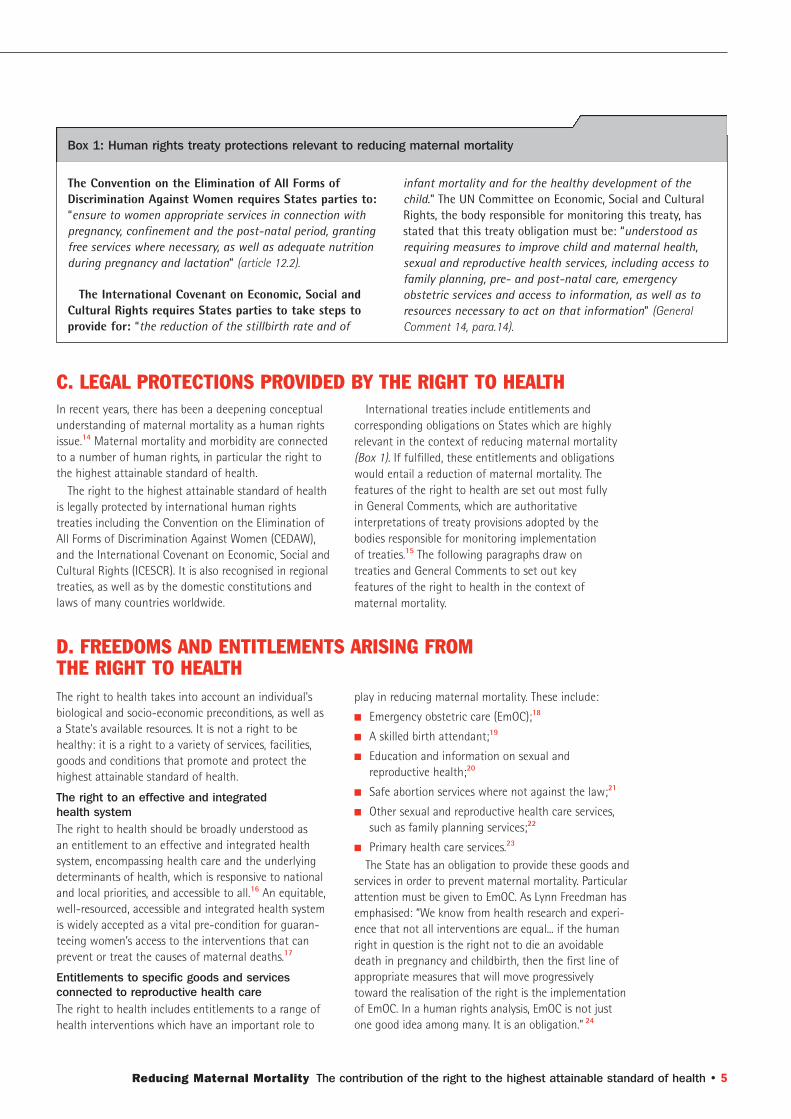
The Convention on the Elimination of All Forms ofDiscrimination Against Women requires States parties to:“ensure to women appropriate services in connection withpregnancy, confinement and the post-natal period, grantingfree services where necessary, as well as adequate nutritionduring pregnancy and lactation” (article 12.2).
The International Covenant on Economic, Social andCultural Rights requires States parties to take steps toprovide for: “the reduction of the stillbirth rate and of
Box 1: Human rights treaty protections relevant to reducing maternal mortality
infant mortality and for the healthy development of thechild.” The UN Committee on Economic, Social and CulturalRights, the body responsible for monitoring this treaty, hasstated that this treaty obligation must be: “understood asrequiring measures to improve child and maternal health,sexual and reproductive health services, including access tofamily planning, pre- and post-natal care, emergencyobstetric services and access to information, as well as toresources necessary to act on that information” (GeneralComment 14, para.14).
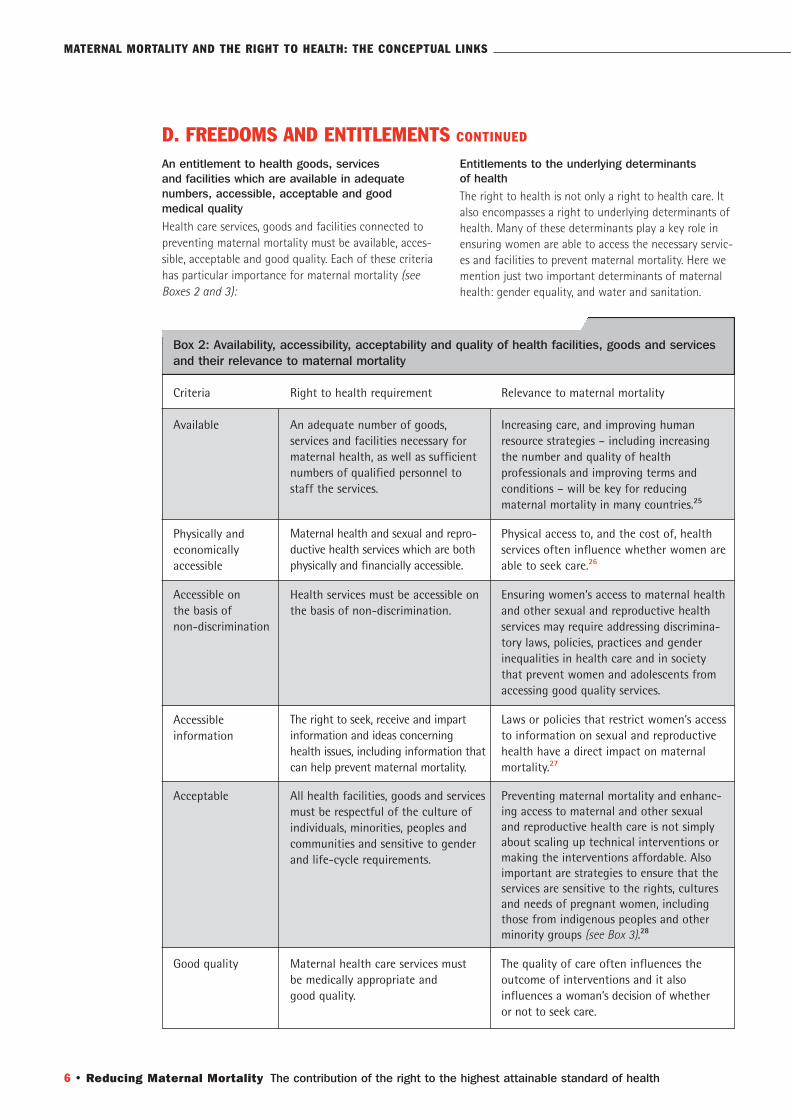
An entitlement to health goods, services and facilities which are available in adequate numbers, accessible, acceptable and good medical quality
Health care services, goods and facilities connected topreventing maternal mortality must be available, acces-sible, acceptable and good quality. Each of these criteriahas particular importance for maternal mortality (seeBoxes 2 and 3):
Entitlements to the underlying determinants of health The right to health is not only a right to health care. Italso encompasses a right to underlying determinants ofhealth. Many of these determinants play a key role inensuring women are able to access the necessary servic-es and facilities to prevent maternal mortality. Here wemention just two important determinants of maternalhealth: gender equality, and water and sanitation.
6 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
D. FREEDOMS AND ENTITLEMENTS CONTINUED
Available
Physically and economically accessible
Accessible on the basis of non-discrimination
Accessible information
Acceptable
Good quality
Box 2: Availability, accessibility, acceptability and quality of health facilities, goods and servicesand their relevance to maternal mortality
Criteria Right to health requirement Relevance to maternal mortality
An adequate number of goods, services and facilities necessary formaternal health, as well as sufficientnumbers of qualified personnel tostaff the services.
Maternal health and sexual and repro-ductive health services which are bothphysically and financially accessible.
Health services must be accessible onthe basis of non-discrimination.
The right to seek, receive and impartinformation and ideas concerninghealth issues, including information thatcan help prevent maternal mortality.
All health facilities, goods and servicesmust be respectful of the culture ofindividuals, minorities, peoples andcommunities and sensitive to genderand life-cycle requirements.
Maternal health care services must be medically appropriate and good quality.
Increasing care, and improving humanresource strategies – including increasingthe number and quality of health professionals and improving terms and conditions – will be key for reducing maternal mortality in many countries.25
Physical access to, and the cost of, healthservices often influence whether women areable to seek care.26
Ensuring women’s access to maternal healthand other sexual and reproductive healthservices may require addressing discrimina-tory laws, policies, practices and genderinequalities in health care and in societythat prevent women and adolescents fromaccessing good quality services.
Laws or policies that restrict women’s accessto information on sexual and reproductivehealth have a direct impact on maternalmortality.27
Preventing maternal mortality and enhanc-ing access to maternal and other sexual and reproductive health care is not simplyabout scaling up technical interventions or making the interventions affordable. Alsoimportant are strategies to ensure that theservices are sensitive to the rights, culturesand needs of pregnant women, includingthose from indigenous peoples and otherminority groups (see Box 3).28
The quality of care often influences theoutcome of interventions and it also influences a woman’s decision of whether or not to seek care.
MATERNAL MORTALITY AND THE RIGHT TO HEALTH: THE CONCEPTUAL LINKS
Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 7
In the village of San José de Secce and the communities of Oqopeqa, Punkumarqiri, Sañuq and Laupay in Ayacucho district, Peru, an assessment by non-governmental organisa-tions showed that there were various barriers to using health services in these communities, which had very high maternalmortality rates. In addition to the distance that had to be travelled to the establishment, the inability to pay fortransport or care and the lack of health personnel and equipment, the main barrier was reluctance on the part ofthe population to use health facilities offered by the state.This situation was reflected in the high percentage of women(94 per cent) giving birth at home, compared with 6 per centwho gave birth in health centres.
The state health services did not take account of local cultural conceptions of health and sickness. The populationhad no trust in the ability of the personnel or the servicesand viewed attending a health facility as inconvenient orrisky and therefore resisted using the facilities.
Between 1999 and 2001, in consultation with the commu-nities in question, a culturally-adapted project to providesexual and reproductive health services was put into effect.The project promoted communication between health
Box 3: Culturally acceptable maternal health services in Peru
professionals and the community, user participation, and acloser relationship between traditional midwives and healthpersonnel. In health centres, the environment of the deliveryroom and care given during prenatal checkups, delivery andthe postnatal period were adapted to make them culturallysensitive. These measures included creating a private environ-ment, with curtains to keep out draughts and anyone notassociated with the birth, as well as the provision of a bedand a sturdy rope, so that women could give birth in anupright position, or squatting and gripping the rope, as theywished. The protocol for care also stipulated, among others,that the person attending the birth should speak Quechuaand preferably be female. In addition, in accordance with thebeliefs of the communities, the protocol included the require-ment to deliver the placenta to the family member presentso that it could be buried, and the opportunity for the userto remain in the health facility for up to eight days. Accordingto an assessment, after the project was implemented, therewas a great increase in deliveries at health centres.
Source: adapted from Amnesty International, Peru: Poor andexcluded women – denial of right to maternal and child health,2006.
Gender equality: Behind maternal mortality is a failure to guarantee women’s human rights. This is often manifested in, among others, low status ofwomen and girls, poor access to information and care,early age of marriage and restricted mobility.29 Genderequality has an important role to play in preventingmaternal mortality. Gender equality and empowermentlead to greater demand by women for family planningservices, antenatal care and safe delivery. The Conventionon the Elimination of Discrimination Against Womenprovides that States Parties “agree to pursue by all appro-priate means and without delay a policy of eliminatingdiscrimination against women” and that they “shall take all appropriate measures to eliminate discriminationagainst women in the field of health care in order toensure, on a basis of equality of men and women, access to health care services, including those related to family planning.” 30
Water and sanitation: Water and sanitation must be ensured for the provision of prenatal care and emer-gency obstetric care. Water and sanitation are essentialelements of the right to health.
FreedomsIn addition to the numerous entitlements associated withthe right to health, this human right includes a number offreedoms. In the context of maternal mortality, relevantfreedoms include freedom from discrimination; harmfultraditional practices, such as early marriage; and violence.
Photograph © P. Delargy,courtesy of UNFPA. StopGender DiscriminationAgainst Women, Liberia.
THE RIGHT TO HEALTH
ENCOMPASSES AN ENTITLEMENT
TO UNDERLYING DETERMINANTS
OF HEALTH
1.
2.
3.
As well as its relationship to the right to health, maternal mortality has a close relationship to otherhuman rights. Preventable maternal mortality often represents a violation of the right to life. Other humanrights that have a bearing on maternal mortality
include the right to decide freely on the number andspacing of one’s children and the right to education.These human rights can also be integrated into strategies to reduce maternal mortality (see Chapters II and III).
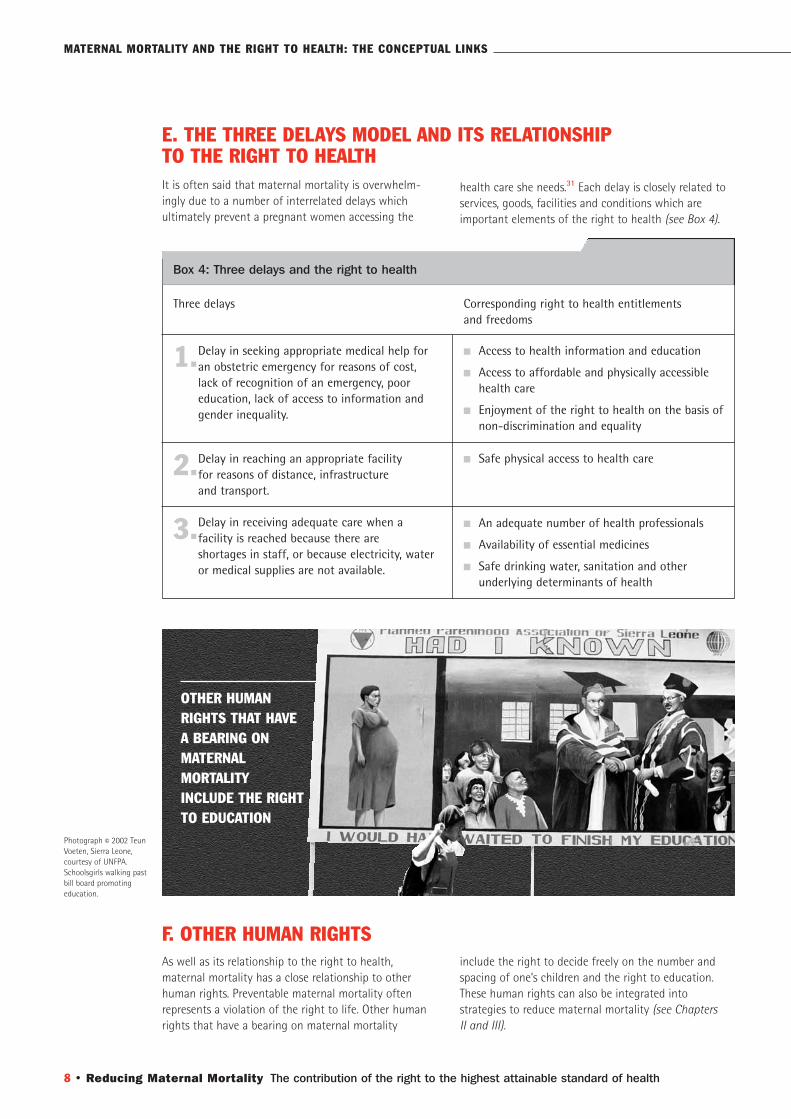
It is often said that maternal mortality is overwhelm-ingly due to a number of interrelated delays which ultimately prevent a pregnant women accessing the
health care she needs.31 Each delay is closely related toservices, goods, facilities and conditions which areimportant elements of the right to health (see Box 4).
8 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
E. THE THREE DELAYS MODEL AND ITS RELATIONSHIP
TO THE RIGHT TO HEALTH
F. OTHER HUMAN RIGHTS
Delay in seeking appropriate medical help foran obstetric emergency for reasons of cost,lack of recognition of an emergency, pooreducation, lack of access to information andgender inequality.
Delay in reaching an appropriate facility for reasons of distance, infrastructure and transport.
Delay in receiving adequate care when a facility is reached because there are shortages in staff, or because electricity, wateror medical supplies are not available.
Box 4: Three delays and the right to health
Three delays Corresponding right to health entitlements and freedoms
� Access to health information and education
� Access to affordable and physically accessible health care
� Enjoyment of the right to health on the basis of non-discrimination and equality
� Safe physical access to health care
� An adequate number of health professionals
� Availability of essential medicines
� Safe drinking water, sanitation and other underlying determinants of health
Photograph © 2002 TeunVoeten, Sierra Leone, courtesy of UNFPA.Schoolsgirls walking pastbill board promoting education.
MATERNAL MORTALITY AND THE RIGHT TO HEALTH: THE CONCEPTUAL LINKS
OTHER HUMAN
RIGHTS THAT HAVE
A BEARING ON
MATERNAL
MORTALITY
INCLUDE THE RIGHT
TO EDUCATION

The responsibilities created by international humanrights law provide a basis for ensuring accountabilityand determining which actors are responsible for reducing maternal mortality.
States that have ratified ICESCR, CEDAW and otherinternational treaties, or that have national constitutionsguaranteeing the right to health, have a legal obligationto realise the right to health. Other relevant stakeholders – including international organisations, private providersof health care, families and communities – also haveresponsibilities.32
States have three primary obligations towards theright to health:
� Respect: States must not interfere with the right to health, for example by adopting discriminatorypolicies or laws;
� Protect: States must ensure that third parties (e.g. non-state actors) do not infringe the enjoymentof the right to health;
� Fulfil: States must take positive steps to realise theright to health, such as policy, legislative, budgetaryand administrative measures.
These obligations mean that States must take steps toensure women can access maternal health care andother relevant sexual and reproductive health services.This may require actions including increasing resourcesto the relevant services within the health sector, devel-oping a policy and plan of action, developing more serv-ices and improving staffing ratios, improving transportto existing services, and addressing social, cultural andeconomic reasons why women do not access services.
The obligation to progressively realise the right to healthInternational law does not expect States to instanta-neously provide all goods, services and facilities relevantto the right to health. Instead, States are expected totake concrete and deliberate steps to progressively
realise the right to health. These steps may include legal,policy and administrative measures. What is expected ofa State depends on the resources available to it – inother words, the same is not expected of a rich and of a poor State. Where resources are limited, States are expected to prioritise certain key interventions, including those that will help guarantee maternalhealth,33 and in particular EmOC.
Although subject to progressive realisation andresource constraints, the right to health imposes variousobligations of immediate effect. These immediate obligations include ensuring the realisation of the rightto health on a non-discriminatory basis; the provision ofprimary healthcare, safe water and adequate sanitation;and equitable distribution of all health facilities, goodsand services.
International assistance and cooperationThe right to health requires high-income States to assist low-income States in their efforts to reducematernal mortality.34 This responsibility is also reflectedin international development commitments such asMillennium Development Goal 8, which is a commit-ment to develop a global partnership for development.High-income States should, for example, ensure thatreducing maternal mortality is adequately reflected intheir development assistance contributions and policies.They should also undertake other measures such asrefraining from the proactive recruitment of health professionals from developing countries where thiswould result in staffing shortages that hamper thereduction of maternal mortality.35
The duty of high-income States to assist low-income States does not deprive the latter of their own obligations to progressively realise the right tohealth. Low-income States must still undertake meas-ures within their domestic resources, and supplementdomestic with international resources where necessaryand possible.
Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 9
G. WHAT ARE STATES’ RIGHT TO HEALTH OBLIGATIONS
TO REDUCE MATERNAL MORTALITY?
THE RIGHT TO HEALTH REQUIRES HIGH-INCOME STATES
TO ASSIST
LOW-INCOME STATES IN THEIR EFFORTS TO REDUCE
MATERNAL MORTALITY
10 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
Human rights violations are both a cause and conse-quence of poverty and ill-health. Respect for humanrights can enhance poverty reduction and improvehealth outcomes.
A human rights-based approach explicitly integrateshuman rights norms, standards and principles into programmes, plans and policies to reduce maternal mortality. While there is no set formula for a humanrights-based approach, key characteristics include:
� Making the realisation of human rights – such as therights of women to life, health, and non-discrimina-tion, the main objective of maternal mortality-related policies and programmes;
� Ensuring that human rights guide, and are integrated
into, policies and programmes at all stages – fromdevelopment to implementation;
� Enhancing the capacity of rights-holders to claimtheir rights, and the capacity of duty-bearers to fulfiltheir obligations; 36
Drawing on the relationship between health, povertyand human rights, in recent years a number of donors,and international and civil society organisations havepromoted, or adopted, a human rights-based approachto health policies and programmes, including in thecontext of maternal health (see Boxes 5-7).
Today, a number of useful resources are available whichcan help policy makers integrate human rights into mater-nal mortality policies and programmes (see Boxes 5-6).
THE RIGHT TO THE HIGHEST ATTAINABLE STANDARD OF HEALTH: A FRAMEWORK FOR EFFECTIVE POLICIES TO REDUCE MATERNAL MORTALITY
II.
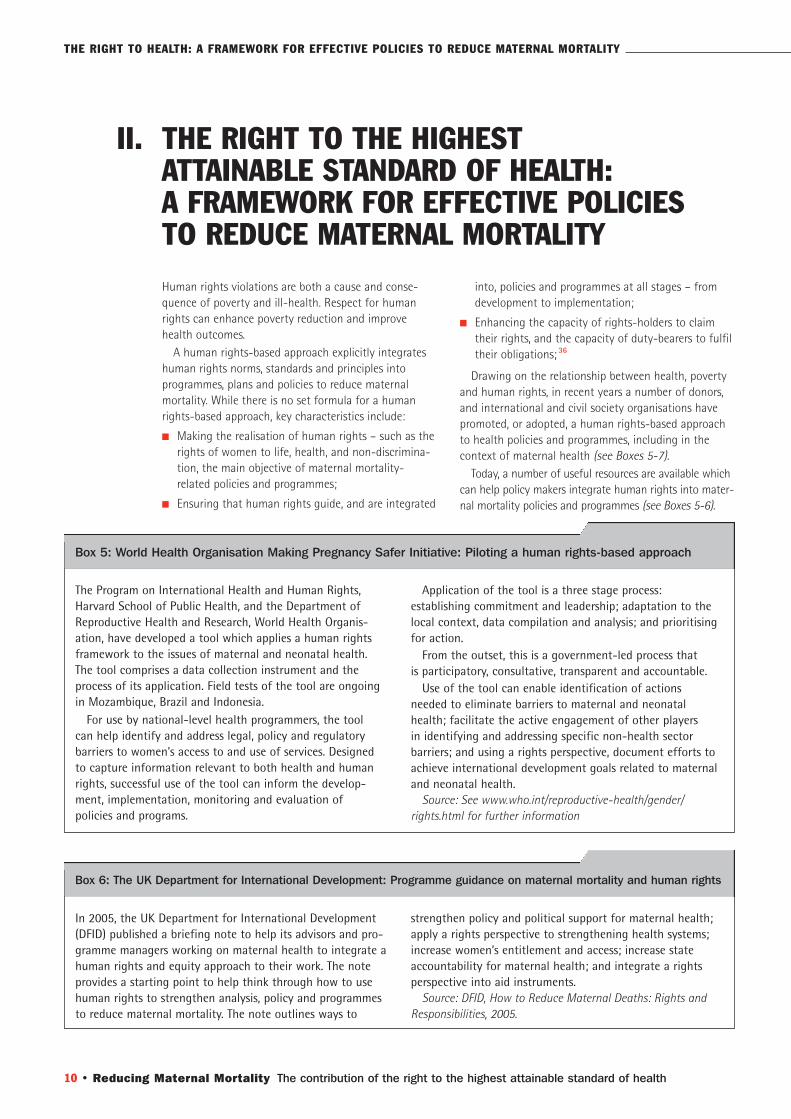
The Program on International Health and Human Rights,Harvard School of Public Health, and the Department ofReproductive Health and Research, World Health Organis-ation, have developed a tool which applies a human rightsframework to the issues of maternal and neonatal health.The tool comprises a data collection instrument and theprocess of its application. Field tests of the tool are ongoingin Mozambique, Brazil and Indonesia.
For use by national-level health programmers, the tool can help identify and address legal, policy and regulatorybarriers to women’s access to and use of services. Designedto capture information relevant to both health and humanrights, successful use of the tool can inform the develop-ment, implementation, monitoring and evaluation of policies and programs.
Box 5: World Health Organisation Making Pregnancy Safer Initiative: Piloting a human rights-based approach
Application of the tool is a three stage process: establishing commitment and leadership; adaptation to thelocal context, data compilation and analysis; and prioritising for action.
From the outset, this is a government-led process that is participatory, consultative, transparent and accountable.
Use of the tool can enable identification of actions needed to eliminate barriers to maternal and neonatalhealth; facilitate the active engagement of other players in identifying and addressing specific non-health sector barriers; and using a rights perspective, document efforts toachieve international development goals related to maternaland neonatal health.
Source: See www.who.int/reproductive-health/gender/rights.html for further information
In 2005, the UK Department for International Development(DFID) published a briefing note to help its advisors and pro-gramme managers working on maternal health to integrate ahuman rights and equity approach to their work. The noteprovides a starting point to help think through how to usehuman rights to strengthen analysis, policy and programmesto reduce maternal mortality. The note outlines ways to
Box 6: The UK Department for International Development: Programme guidance on maternal mortality and human rights
strengthen policy and political support for maternal health;apply a rights perspective to strengthening health systems;increase women’s entitlement and access; increase stateaccountability for maternal health; and integrate a rightsperspective into aid instruments.
Source: DFID, How to Reduce Maternal Deaths: Rights andResponsibilities, 2005.
THE RIGHT TO HEALTH: A FRAMEWORK FOR EFFECTIVE POLICIES TO REDUCE MATERNAL MORTALITY
The precise features of a human rights-based approachwill often be determined by the local context. However,a range of common norms and standards integral tohuman rights should always be at the heart of humanrights-based policies.
The right to the highest attainable standard of health In the context of maternal mortality, the right to health should be at the centre of the human rights-basedapproach. This is because right to health freedoms andentitlements – as described in the previous chapter – correspond very closely with those actions required toreduce maternal mortality. These freedoms and entitle-ments can be used as a framework for effective policies,programmes and projects for reducing maternal mortality.
Equality and non-discrimination Equality and non-discrimination are fundamentalhuman rights principles and are also integral elementsof the right to health. They are important for efforts to reduce maternal mortality in three important, interrelated respects:
a) First, these principles support prioritization of inter-ventions that can guarantee women’s enjoyment ofthe right to health on the basis of non-discrimina-tion and equality. Guaranteeing the right to healthon the basis of gender equality demands that Statesundertake measures to reduce preventable deathfrom pregnancy and childbirth;
b) Second, they require action to prioritise effortstowards those at risk of maternal mortality, such as women living in poverty and in rural areas orbelonging to indigenous groups, and adolescent girls (see Box 7). They underpin efforts to assess andaddress why these women are particularly vulnerable
to maternal mortality, such as a lack of access to necessary health services, and political and socialmarginalisation;
c) Third, policies which promote non-discrimination and equality (as well as dignity, cultural sensitivity,privacy and confidentiality) in the clinical setting can improve patient-provider relationships andencourage women to seek health care.
A policy that is animated by human rights, including theright to health, is likely to be more effective, equitable,inclusive, non-discriminatory and participatory. In thecontext of maternal mortality policies, these featureshelp to empower women.
On account of its grounding in law, widespreadacceptance by the international community and detailedframework of relevant norms and obligations, the rightto health and other relevant human rights provide legitimacy and a legal framework for policies and programmes that prevent maternal mortality. The widespread acceptance of human rights can mean that
they are a useful platform for building consensusamong a range of stakeholders – governments, inter-national organisations, donors and civil society – withrespect to developing and implementing policies.
While States are primarily responsible for humanrights under international law, human rights can beintegrated into the policies and programmes of a rangeof actors, not just States. Given the benefits of a humanrights-based approach, human rights should inspirechanges in the work of other actors including healthprofessionals, international organisations, the privatesector and civil society.
Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 11
A. THE BENEFITS OF A HUMAN RIGHTS-BASED APPROACH TO
MATERNAL MORTALITY
B. THE RIGHT TO HEALTH AND OTHER KEY FEATURES, NORMS AND
PRINCIPLES OF A HUMAN RIGHTS-BASED APPROACH TO MATERNAL
MORTALITY POLICY MAKING
As part of a national strategy to address the needs of the poorestand most underserved communities, the Ecuador country programmeof the United Nations Population Fund (UNFPA) has financed aninnovative project in Otavalo to improve the quality and scope ofreproductive health care provided to Quechua-speaking communi-ties. This support allowed the Jambi Huasi health clinic, establishedin 1994, to expand and upgrade its services, initiate an outreachprogramme, provide reproductive health education and informationto women, men and adolescents and introduce a referral system for obstetric complications. Jambi Huasi provides both modern and traditional medical treatment, as well as family planning advice and services. The traditional healers draw from a “pharmacy”of over 3,600 native plants used for medicinal purposes. The uniquecombination of services has made Jambi Huasi a very popular clinicreaching over 1,000 people per month coming from as far away as 50 kilometres. As Quechua communities learn more about reproductive health issues and how to take better care of their children and newborns, the contraceptive prevalence rate has risenfrom 10 to 40 per cent in areas served by Jambi Huasi. Jambi Huasiis moving from a “pilot” project to public policies, influencing theMinistry of Health for the inclusion of cultural perspectives in their work.
Source: The United Nations Common Learning Resource Guide, 2007.
Box 7: UNFPA: Cultural Sensitivity in Ecuador
12 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
Participation
The right to health includes an entitlement to partici-pate in health policymaking at the local, national andinternational levels. This entitlement applies at all stagesof a policy or programme cycle: assessment, analysis,implementation, monitoring and evaluation.38
Meaningful participation by relevant stakeholders,including those who are often marginalised in policymaking processes such as people living in poverty,women and adolescent girls, will help develop moreeffective and sustainable programmes, reduce exclusionand enhance accountability.
Participation by women is also particularly importantfor another reason: it helps elevate their position frompassive clients to active citizens that are workingtogether with policy makers and service providers.
Participation by women, including those women mostat risk of maternal mortality, raises important questionsabout national or local participatory processes. Itrequires us to ask questions such as: who representswomen in local communities? Are there power dynamicsthat shape who is invited to participate and that needto be transcended? Ensuring participation may requireaction such as building capacity for participation bypoor and other marginalised women
Monitoring
Monitoring and accountability are integral human rightsprinciples, as well as key features of the right to health,and can help reduce maternal mortality.
Monitoring is important in order to assess the scale ofmaternal mortality, its causes, and whether measures are
being taken to address the problem.
Indicators can be used to help monitor progress andto highlight where policy adjustments may be needed.Commonly used health indicators such as the maternalmortality ratio have an important role in this respect.However, the right to health requires that such indica-tors are disaggregated on grounds including urban/rural,race and ethnicity. Some new indicators not commonlyfound in the health literature are also needed, for exam-ple to help monitor access to information on sexual andreproductive health, participation and accountability.39
Accountability
A human rights-based approach to maternal mortalityrequires that duty bearers are accountable for bothmaternal mortality, and for implementing policies andprogrammes to reduce its incidence.
Accountability devices can include a range of institu-tions and processes within and beyond government,ranging from impact assessments (see Box 8) and policyreview processes, to parliamentary processes, ombuds,courts and tribunals. These mechanisms should be usedto clarify who has the responsibility to do what,whether or not they have done it, and if they have notdone it, the device should explore why not and identifyappropriate redress.
Accountability procedures can help establish whenduty bearers are facing obstacles in realising the right to health, and support them in meeting their right tohealth duties. An accountability device also should iden-tify good practices for reducing maternal mortality, aswell as those who should take credit for them.
B. THE RIGHT TO HEALTH AND OTHER KEY FEATURES CONTINUED
The Humanist Committee on Human Rights, a Dutch non-governmental organisation, has developed a Health Rights ofWomen Assessment Instrument (HerWAI), a tool to enhancelobbying activities for better implementation of women’shealth rights. The instrument sets out six steps for analysinga policy that affects women’s health rights:
1] identifying the policy and the groups and rights mostaffected by it;
2] identifying the Government’s national and internationalright to health commitments;
3] describing the capacity of the Government to implementthe policy (e.g. what factors may inhibit the Government’sability to implement the policy);
4] assessing the impact of the policy on human rights;
Box 8: The Human Rights of Women Assessment Instrument (HeRWAI): Government policies on eclampsia in Bangladeshand the impact on the right to health
5] describing the Government’s human rights obligations,and whether the Government is meeting these;
6] identifying recommendations and action.
The HeRWAI analysis links what is happening in a countryto what should be happening according to that country’shuman rights obligations. It can help civil society hold aGovernment to account for its human rights obligations.
The assessment can be applied to assess maternal healthpolicies and their impact on the right to health. For example,Naripokkho, a civil society-organisation in Bangladesh, usedthe HeRWAI tool to assess maternal health policies in Bangla-desh, their impact on the right to health of women, andmake recommendations to the Government of Bangladesh.
Source: Humanist Committee on Human Rights, HealthRights of Women Impact Assessment, 2006.
THE RIGHT TO HEALTH: A FRAMEWORK FOR EFFECTIVE POLICIES TO REDUCE MATERNAL MORTALITY

There are many stakeholders and activities that affectmaternal health. A human rights-based approach can beapplied in the context of work of Governments, interna-tional organisations, donors and civil society. It can beapplied to policy work, clinical practice, and to supportcivil society empowerment.
The following are some non-comprehensive sugges-tions of the sorts of actions which may be required for a human rights-based approach to maternal mortalitypolicies. Policies should:
� Integrate human rights, including sexual and reproductive health rights. Where policies alreadyexist, they should be reviewed from a human rightsperspective and amended as appropriate;
� Be informed by, and respond to, an evidence-basedassessment of the causes of maternal mortality;
� Be developed through a participatory process, involving the input of women and communities mostaffected by maternal mortality;
� Be subject to an impact assessment to determinetheir anticipated impact on reducing maternal mortality and promoting human rights;
� Be designed to strengthen the health system, including addressing human resource shortages;
� Enshrine a commitment to non-discrimination andequality through giving particular attention to the rightto health of the most vulnerable women (see Box 9);
� Incorporate indicators and benchmarks for reducingmaternal mortality. Indicators should be disaggre-gated according to region, rural/urban location, race and ethnicity, and age, with a view to promotingequitable enjoyment of the right to health;
� Clearly set out the responsibilities of various actorsfor reducing maternal mortality, including, whereappropriate, the international and domestic humanrights obligations of States;
� Strengthen the capacity of duty bearers to giveeffect to their right to health and other humanrights obligations. This may require diverse actions,from human rights training for policy makers andhealth providers, to increasing the budget for, andprioritization of, maternal health;
� Strengthen the capacity of rights-holders to claimtheir right to health and other human rights in thecontext of maternal mortality.
Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health • 13
C. WHAT SORT OF ACTIONS MIGHT BE REQUIRED
FOR A HUMAN RIGHTS-BASED POLICY
FOR REDUCING MATERNAL MORTALITY?
“The Nepal Safer Motherhood Project adopted an ‘all inclusive’ approach with the aim of saving the maximumnumber of women’s lives. In 2004, a study measuring the utilisation of emergency obstetric care (EmOC) foundthat the principal users of services were high caste Brahmin/Chettri women. In one district, the rate of use per 1000 population was over four times greater for thehigher caste women than for all other women. This hascalled attention to the need to target resources so that lower caste groups and Janajatis (ethnic groups) can use
Box 9: Universal coverage and the targeting of excluded groups
EmOC services at the same rate as that attained by theBrahmin/Chettri women – both to save maximum lives and to be truly inclusive. The cost of providing services forthe poorest and socially excluded will be higher than for the more accessible, high caste women. While this calls for difficult political choices, it may also allow informeddefensible choices. It also highlights the need to monitorwho benefits.”
Source: DFID, How to Reduce Maternal Deaths: Rights andResponsibilities, 2005.
A HUMAN-RIGHTS BASED
APPROACH TO MATERNAL
MORTALITY REQUIRES THAT
DUTY BEARERS ARE ACCOUNTABLE
FOR MATERNAL MORTALITY
Photograph © LilySolmssen, courtesy ofUNFPA. Income-gener-ating activities are animportant component of the programmesorganized at the FamilyWelfare Centres. Womanare given lessons insewing and knitting atthis Centre located nearLahore, Pakistan.
14 • Reducing Maternal Mortality The contribution of the right to the highest attainable standard of health
In the 1990s, gender-based violence was identified as a violation of human rights and this helped the globalcampaign on violence against women gather momen-tum. By the same token, the human rights communityshould be challenged to give greater attention to mater-nal mortality in their work, and mount a global humanrights campaign against maternal mortality – which,where preventable, often represents a violation of therights to life and health.
The human rights community must be urged toremonstrate and demonstrate about maternal mortality
just as loudly as it complains about extrajudicial execu-tions, arbitrary detention, unfair trials and prisoners ofconscience. Persistently high maternal mortality rates,coupled with the fact that all States are committed toreduce by three quarters the maternal mortality ratio by2015, suggests that the time is ripe for such an initia-tive.
A human rights campaign against avoidable maternalmortality would inevitably lead to other crucial issues,not least the vital importance of constructing effectivehealth systems that are accessible to all.
Human rights can make a contribution to reducing mater-nal mortality in several ways, not just in the context ofdesigning effective and equitable polices and programs.
Traditional human rights techniques, such as namingvictims, naming and shaming violators, letter writingcampaigns, advocacy and lobbying, and taking courtcases are all strategies that can help address maternalmortality.40 Human rights can also help us change howmaternal mortality is viewed and why it matters, from a“natural” occurrence and a loss of productivity, to anissue of social injustice,41 thereby strengtheningdemands that maternal mortality is addressed.
Some of these traditional techniques may face somedifficulties in the context of maternal mortality. Forexample, they tend to rely on the identification of a vio-lator. However, responsibility for maternal mortality maybe attributable to multiple actors, including familymembers, health professionals and facilities, the relevantState, and the international community.42 However, thatdoes not stop many maternal deaths from being ahuman rights violation — and this violation must berecognised, investigated precisely to determine whereresponsibility lies, and to better ensure accountabilitywith a view to appropriate policy changes.
In recent years, courts have played an increasing role inprotecting the right to the highest attainable standardof health. Among the most significant developments arethose relating to access to medicines (e.g. see Box 10).Maternal mortality has not yet been given the sameamount of attention by the human rights community.
Litigation may support particular goals – such as the provision of emergency obstetric care and particulardrugs required in this regard, although it may be less effective in addressing some of the structuralinequalities and problems underlying maternalmortality.43
REDUCING MATERNAL MORTALITY: THE ROLE OF TRADITIONAL HUMAN RIGHTS TECHNIQUES
III.
A. CAMPAIGNING
B. TAKING COURT CASES
This case concerned provision of the antiretroviral medica-tion, Nevirapine, which can prevent mother-to-child trans-mission of HIV. The Government provided Nevirapine at onlytwo research and training sites per province. The drug couldalso be obtained from private medical providers. As a result,mothers and their babies who did not have access to theresearch and training sites, and who could not afford
Box 10: Minister of Health v. Treatment Action Campaign, South African Constitutional Court
access to private health care, were unable to gain access toNevirapine. The court held that the State’s limited provisionof Nevirapine was unreasonable. It ordered that theGovernment act without delay to provide, inter alia, the drugin public hospitals and clinics when medically indicated.
Source: South African Constitutional Court Judgement CCT8/02, 5 July 2002.
REDUCING MATERNAL MORTALITY: THE ROLE OF THE TRADITIONAL HUMAN RIGHTS TECHNIQUES

NOTES II
18 CEDAW, General Recommendation 24, paras. 2and 27.
19 CEDAW, General Recommendation 24, para. 2.
20 CEDAW, General Recommendation 24, para. 18.
21 UN human rights bodies have also held that absolute legal prohibitions on abortioncan violate the rights to life and health where they contribute to maternal mortality.For example, in its Concluding Observations on Colombia (UN doc A/54/38, para. 393),CEDAW noted, with great concern: “That abortion, which is the second cause of maternal deaths in Colombia, is punishable as an illegal act. No exceptions are made tothat prohibition, including where the mother’slife is in danger or to safeguard her physical or mental health or in cases where the mother has been raped... The Committeebelieves that legal provisions on abortion constitute a violation of the rights of women to health and life and of article 12 of the Convention.”
22 CEDAW, General Recommendation 24, paras. 2and 23.
23 General Comment 14, paras. 14, 21, CEDAW, General Recommendation 24, para.27; ICPD, para. 8.25. The Millennium Projecthas emphasised the importance of universal access to reproductive health care through the primary health care system: see UNMillennium Project, Taking Action: Achieving Gender Equality and Empowering Women, Report of the Taskforce on Education and Gender Equality, London, 2005.
24 L. Freedman, “Using Human Rights in MaternalMortality Programs: From Analysis to Strategy,”75 International Journal of Obstetrics andGynecology 2001.
25 Millennium Project, see note 5.
26 Millennium Project, see note 5.
27 R. Cook, B. Dickens et al, see note 3.
28 J. Shiffman, A.Garces del Valle, “PoliticalHistories and Disparities in Safe Motherhoodbetween Guatemala and Honduras”, 32(1) Population and Development Review, 2006.
29 DFID, How to Reduce Maternal Deaths: Rightsand Responsibilities, 2005.
30 CEDAW, article 12.1.
31 D. Maine, Safe Motherhood Programs: Optionsand Issues, Columbia University, 1991.
32 General Comment 14, para. 42.
33 General Comment 14, para. 44.
34 ICESCR, article 2.
35 See, for example, the Special Rapporteur’sreport to the General Assembly (A/60/348); J. Bueno de Mesquita, M. Gordon, The International Migration of Health Workers: a Human Rights Analysis(Medact, 2005).
36 For further information on a rights-basedapproach, see Frequently Asked Questions on a Human Rights-based Approach toDevelopment Cooperation, OHCHR, 2006.
37 DfID, see note 29; L. Freedman, “ShiftingVisions: ‘Delegation’ Policies and the Building of a ‘Rights-based’ Approach to MaternalMortality”, 57(3) Journal of the AmericanMedical Women’s Association 2002; K. Hawkins,K. Newman, D. Thomas, C. Carlson, Developinga Human Rights-based Approach to AddressingMaternal Mortality: Desk Review, DfID HealthResource Centre, 2005; Millennium Project, seenote 5; R. Cook, B. Dickens, see note 3; UNSpecial Rapporteur on the right to the highestattainable standard of health, report to theGeneral Assembly, September 2006, A/61/338.
38 OHCHR, see note 36.
39 For further information and suggestions ofappropriate indicators, see report of the SpecialRapporteur to the Human Rights Commission,3 March 2006, E/CN/4/2006/48, paras. 22-61,and annex.
40 Some human rights organisations are starting to focus more on maternal mortality,e.g. Maternal Mortality in Herat Province,Afghanistan: the Need to Protect Women’sRights, Physicians for Human Rights, 2002;Perú: Mujeres Pobres y Excluidas: la Negacióndel Derecho a la Salud Materno-Infantil,Amnesty International, 2006.
41 A. Yamin, “The Future in the Mirror:Incorporating Strategies for the Defence andPromotion of Economic, Social and CulturalRights into the Mainstream Human RightsAgenda”, 27 Human Rights Quarterly 2005.
42 Comparable complexity arises in relation to some civil and political rights, such as “disappearances”. Of course, the formal legalposition is that the State is responsible for any proven violations.
43 Yamin, see note 41.
University of Essex, Colchester, Essex, CO4 3SQ, UK TEL +44 (0)1206 872558EMAIL [email protected] www2.essex.ac.uk/human_rights_centre/
United Nations Population Fund220 East 42nd St., New York, NY 10017, U.S.A.