recognizing renal renal physiology failure - altru.org · post-obstructive uropathy ... bph or...
TRANSCRIPT

10/14/2013
1
Lisa M. Soltis, APRN, MSN, CCRN-CSC, CCNS,
FCCM
Recognizing Renal Failure
Renal Physiology
� Rid body of endogenous (bilirubin, urea, uric acid, creatinine) & exogenous wastes (medications).
� Maintain Homeostasis by regulating fluid, electrolyte, and acid- base balance.
Renal Physiology
�Secretion, excretion, & metabolism of hormones:
�Epoetin
�Calcitrol (active form of Vitamin D)
�Insulin (metabolism)
Renal Physiology
� The kidneys increase epoetin production in response to hypoxia.
� The kidneys release bicarbonate in response to respiratory acidosis.

10/14/2013
2
Renal AnatomyRenal Structure
�Nephrons:
� Approximately 1 million per kidney. After age 40, amount decreases by 10% every 10 years.
�Leads to decreased GFR
�Decreased ability to concentrate urine can lead to dehydration
Nephron Structure
� Each nephron is comprised of a glomerulus, which is made up of about 50 capillaries that are covered by epithelial cells.
� Bowman’s capsule covers each glomerulus.
10/14/2013
3
Renal Physiology
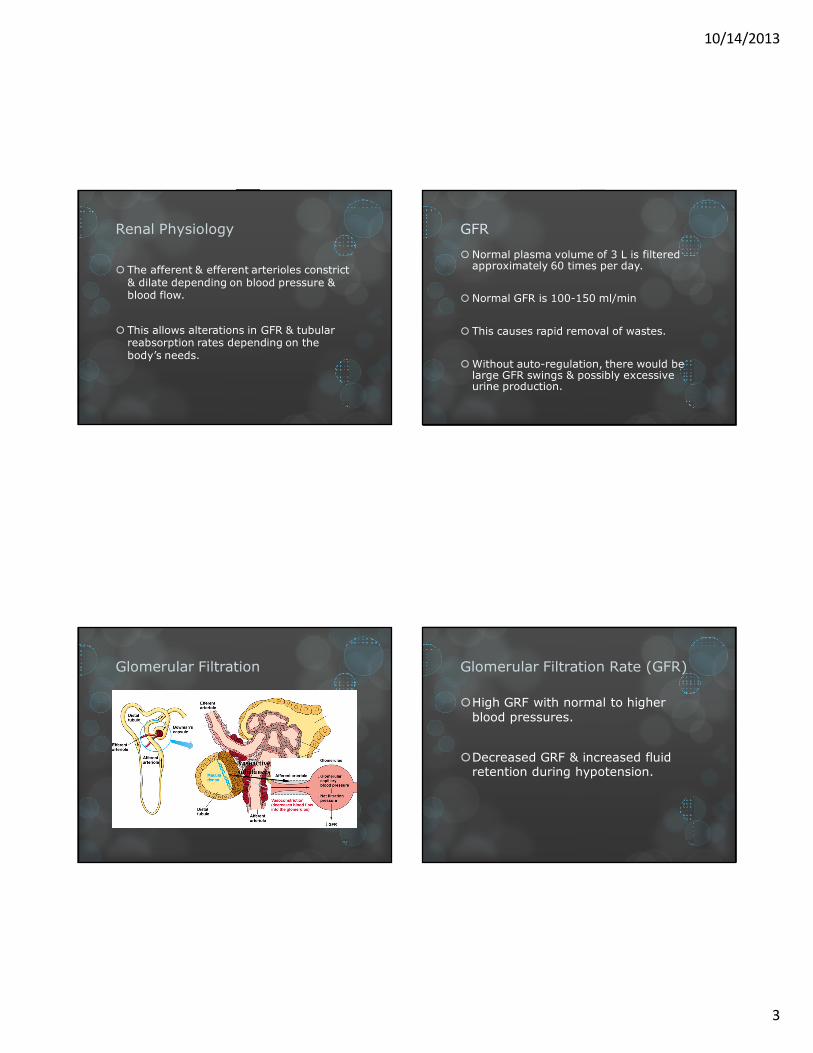
� The afferent & efferent arterioles constrict & dilate depending on blood pressure & blood flow.
� This allows alterations in GFR & tubular reabsorption rates depending on the body’s needs.
� Normal plasma volume of 3 L is filtered approximately 60 times per day.
� Normal GFR is 100-150 ml/min
� This causes rapid removal of wastes.
� Without auto-regulation, there would be large GFR swings & possibly excessive urine production.
GFR
Glomerular Filtration Glomerular Filtration Rate (GFR)
�High GRF with normal to higher blood pressures.
�Decreased GRF & increased fluid retention during hypotension.

10/14/2013
4
Creatinine Clearance
� Byproduct of muscle metabolism, excreted at a constant rate
� Reliable indicator of renal function
� CrCl = urine creatinine x urine volume/24 hrs
Renal Assessment
� Color, clarity, amount of urine
� Difficulty initiating urination or changes in stream
� Changes in urinary pattern
� Dysuria, nocturia, hematuria, pyuria
Assessment
� History of urinary problems
� Urinary or abdominal surgeries
� Smoking, alcohol use, number of sexual partners and type of sexual relationship
� Chance of pregnancy
� History of diabetes or other endocrine disorders
� History of kidney stones
Physical Assessment
� Obtain clean-catch urine specimen
� Color, odor, clarity
� Vital signs and skin assessment

10/14/2013
5
Diagnostic Tests
� Clean-catch urine
� 24-hour urine
� Culture and sensitivity
� BUN, creatinine and creatinine clearance
� Intravenous pyelogram (IVP)
� CT scan
� Renal scan
Diagnostic Tests
� Ultrasound
� Bladder scan
� Cystoscopy
� Uroflowmetry
Acute Renal Failure
� Sudden decline in kidney function, which results in decreased glomerular filtration rate (GFR) and decreased excretion of nitrogenous wastes, causing azotemia.
� Associated with oliguria &/or anuria.
� Overall incidence is up to 25% of hospitalized patients.
Acute Renal Failure Stages
Onset – 1-3 days with increased BUN and creatinine and possible decreased UOP
� Oliguric – UOP < 400/d, increased BUN,Creat, Phos, K, may last up to 14 d
� Diuretic – UOP as much as 4000 mL/d but no waste products, at end of this stage may begin to see improvement
� Recovery – things go back to normal or may remain insufficient and become chronic

10/14/2013
6
Etiologies
Causes divided into three classes:
• Pre-Renal (50%)
Pre-Renal Azotemia (high BUN)
• Intrinsic Renal
• Post-Renal
(< 10%)
Acute Renal Failure
� 70% of ARF patients have either Acute Tubular Necrosis (ATN) or pre-renal azotemia.
� Overall mortality is 25-64%.
� Patients with non-oliguric ARF have the best chance of recovery.
Acute Oliguric Renal Failure
� Urine output < 400 ml/day
� Severe renal dysfunction requiring some form of renal replacement therapy.
� Usually done to facilitate fluid removal.
Post-Obstructive Uropathy
� Functional or mechanical obstruction of urine outflow.
�Urine backflows
�Increased pressure on Bowman’s capsule leads to decreased GFR.

10/14/2013
7
Etiologies of Post-Renal ARF
� Stones
� BPH or Prostate Cancer
� Ureteral Stricture
� UTIs, Bladder Tumors
� Blood Clots Blocking the Foley!!!
� Medications
Right Hydronephrosis
Hyrdro-nephrosis
Tumor
Management
� Diagnosis confirmed by hydronephrosis on renal ultrasound, CT Abdomen/Pelvis
� Treatment: Treat underlying cause!
� Irrigate the Bladder with Sterile Water
� Foley catheter, stents, nephrostomy tubes.
Pre-Renal Etiologies
� Anything that prevents adequate blood flow to the kidneys can cause pre-renal ARF

10/14/2013
8
Pre-Renal ARF (Pump)
�Decreased Cardiac Output:
� Cardiogenic Shock
� Heart Failure
� Arrhythmias
� Drugs: Digoxin, β-blockers
Pre-Renal ARF (Pressure)
�Systemic Vasodilation:
�Distributive Shock: Anaphylactic, Septic, Neurogenic, Adrenal
�Drugs: Anti-hypertensives, vasodilators such as nitrates, morphine, etc.
Pre-Renal ARF (Volume)
� INTRAVASCULAR VOLUME DEPLETION:◦ Burns
◦ GI Hemorrhage
◦ Dehydration
◦ Third Spacing
◦ Diuretics
◦ Diarrhea
◦ Excessive NGT Output
Pathophysiology
� Baroreceptors sense decreased BP
� Renin-angiotensin-aldosterone activated
� Vasoconstriction (angiotensin II)
� Na+ & H20 reabsorbed

10/14/2013
9
Pathophysiology
� Prolonged lack of blood flow due to hypotension or vasoconstriction can lead to destruction of the renal tubules.
� This is called acute tubular necrosis (ATN).
Etiologies of Intrinsic ARF/ATN
�Vasoconstriction:
�From prolonged shock
�Drugs: vasopressors
�Prolonged dehydration
Etiologies of ATN
�Toxicity:
�Drugs: Amphotericin, Aminoglycosides
�Ionic Contrast Dyes: CT, Angio, etc
�Pigments: Rhabdomyolysis
Vascular Causes of Intrinsic ARF
� Vascular Diseases:
� Lupus Vasculitis, Renal Scleroderma
� Renal Artery Stenosis
� Renal Vein Occlusion
� Thromboembolic Disease (emboli, TTP)

10/14/2013
10
ATN
� Inflammation:
� If it is caused by inflammation, multiple organs
are usually involved.
� I.E. Systemic Inflammatory Response (SIRS) &
Multi-Organ Dysfunction Syndrome (MODS)
ATN
� Majority of interstitial ARF cases
� Sloughing of tubular epithelial cells obstructs the lumen of the proximal tubule
� This obstruction causes back pressure
� This decreases GFR
Myoglobinuric ATN
� Rhabdomyolysis causes wide-spread muscle breakdown.
� Myoglobin causes renal tubular damage
� Direct nephrotoxin
� Can block renal tubules
Who Gets Rhabdo?
�Trauma:
�Crush injuries
�Long-bone fractures
�Other:
�Found down after prolonged period

10/14/2013
11
Diagnosis of Rhabdomyolysis
� Urine dips positive for occult blood
� No red blood cells on microscopy
� Creatnine rises usually > 2 mg/dl/day
� Elevated CK
Treatment
� Volume, Volume, Volume
� Alkalinize urine with bicarb drip (controversial)
� Watch for hyperkalemia
� Due to massive muscle breakdown
Radiocontrast Nephropathy
� ARF within 48 hours of administration of hyperosmolar ionic contrast dyes
� CT scans, arteriograms, cardiac catheterization
� Contrast induces vasoconstriction
� Leads to endothelial cell injury in the vessels of the renal medulla
Radiocontrast Nephropathy
� This leads to a rapid/sustained decrease in renal plasma flow (RPF)
� Induces medullary hypoxemia
� This causes ischemic tubular injury/ATN
� Can directly damage tubular cells
� Usually resolves in about 2 weeks

10/14/2013
12
RCN Risk Factors
� Common in diabetics with renal insufficiency
� Increased risk with:
� Dehydration
� Class III/IV Heart Failure
� Chronic Liver Disease
RCN Prevention
� N-acetylcysteine (Mucomyst)
� Fenoldopam (Corlopam)
� HYDRATION with NS
� Only intervention consistently shown in to
decrease incidence of RCN
Avoid Contrast, If Possible
� Avoid iodinated contrast scans--MRI/MRA dye is non-iodinated
� Abdominal Ultrasound instead of CT Scan
� If the test is absolutely necessary:
� Iso-osmolar contrast decreases risk of RCN
Lab Results
� Electrolytes
� Hyperkalemia possible
� Glucose
� May be high or low
� Creatnine/BUN
� Both elevated
� WBC, Hgb/Hct
� Determine if infection or anemia are causes
� Urinanalysis
10/14/2013
13
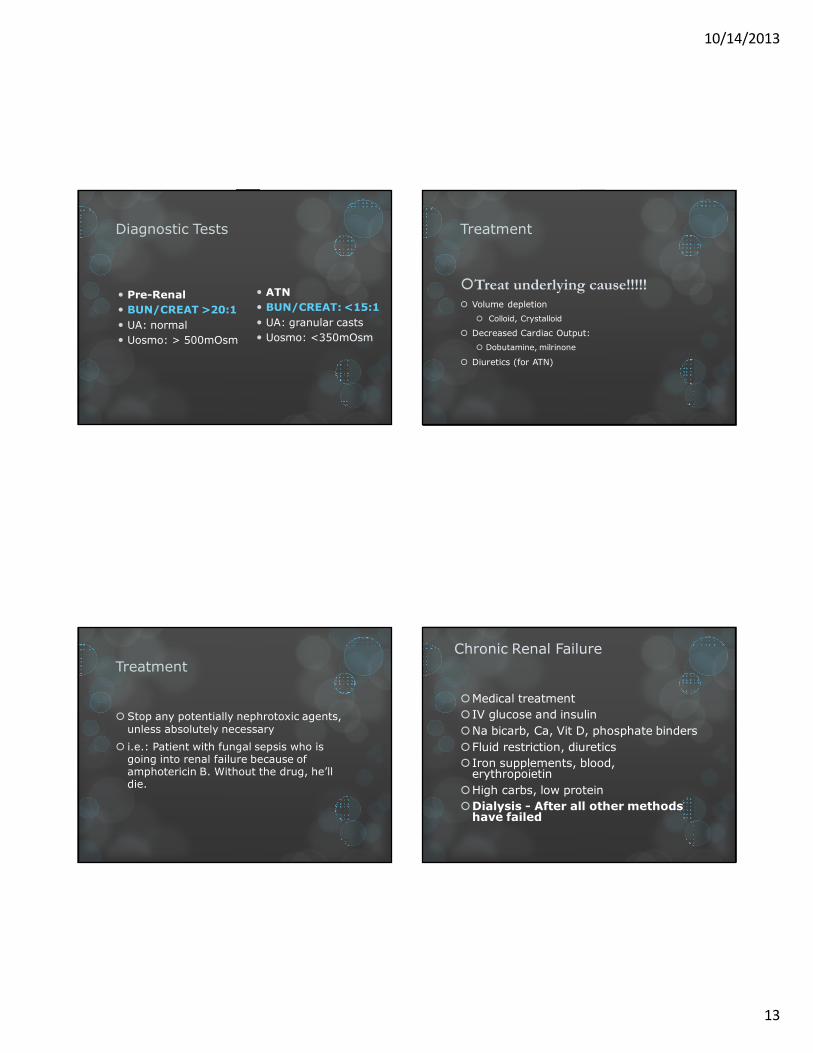
Diagnostic Tests
� Pre-Renal
� BUN/CREAT >20:1
� UA: normal
� Uosmo: > 500mOsm
� ATN
� BUN/CREAT: <15:1
� UA: granular casts
� Uosmo: <350mOsm
Treatment
�Treat underlying cause!!!!!
� Volume depletion
� Colloid, Crystalloid
� Decreased Cardiac Output:
� Dobutamine, milrinone
� Diuretics (for ATN)
Treatment
� Stop any potentially nephrotoxic agents, unless absolutely necessary
� i.e.: Patient with fungal sepsis who is going into renal failure because of amphotericin B. Without the drug, he’ll die.
Chronic Renal Failure
�Medical treatment
� IV glucose and insulin
�Na bicarb, Ca, Vit D, phosphate binders
�Fluid restriction, diuretics
� Iron supplements, blood, erythropoietin
�High carbs, low protein
�Dialysis - After all other methods have failed

10/14/2013
14
Dialysis
� ½ of patients with CRF eventually require dialysis
� Diffuse harmful waste out of body
� Control BP
� Keep safe level of chemicals in body
� 2 types
� Hemodialysis
� Peritoneal dialysis
Peritoneal Dialysis
� Abdominal lining filters blood
� 3 types
� Continuous ambulatory
� Continuous cyclical
� Intermittent
03/05/2011
Dialysis
� Peritoneal dialysis
� Semipermeable membrane
� Catheter inserted through abdominal wall into peritoneal cavity
� Cost less
� Fewer restrictions
� Can be done at home
� Risk of peritonitis
� 3 phases – inflow, dwell and outflow
� Automated peritoneal dialysis
� Done at home at night
� Maybe 6-7 times /week
� CAPD
� Continous ambulatory peritoneal dialysis
� Done as outpatient
� Usually 4 X/d
Hemodialysis
� 3-4 times a week
� Takes 2-4 hours
� Machine filters
blood and returns it
to body

10/14/2013
15
Chronic Renal Failure
� Hemodialysis
� Vascular access
�Temporary – subclavian or femoral
�Permanent – shunt, in arm
� Care post insertion
� Can be done rapidly
� Takes about 4 hours
� Done 3 x a week
Types of Access
�Temporary site: subclavian or femoral
�Permanent: shunt, in arm
�AV fistula�Surgeon constructs by combining an artery
and a vein
�3 to 6 months to mature
�AV graft�Man-made tube inserted by a surgeon to
connect artery and vein
�2 to 6 weeks to mature
Hemodialysis
� Absolute Indications: Severe fluid, electrolyte imbalances, refractory acidosis, severe uremic symptoms
� Relative Indications: Moderate fluid or electrolyte imbalances, moderate uremic symptoms
Continuous vs. Intermittent Dialysis
�Continuous Renal Replacement Therapy (CRRT): Indicated in hemodynamically unstable patients who can’t tolerate dramatic fluid shifts. Can change Rx quickly.� OPTIMIZES FLUID BALANCE
�Hemodialysis: good if hemodynamically stable, better for rapid removal of toxins

10/14/2013
16
Temporary CatheterAV Fistula & Graft
What This Means For You
� No BP on same arm as fistula
� Protect arm from injury
� Control obvious hemorrhage
� Bleeding will be arterial
� Maintain direct pressure
� No IV on same arm as fistula
� A thrill will be felt – this is normal
Nursing Considerations
� Make sure the dressing remains intact
� Do not push or pull on the catheter
� Do not disconnect any of the catheters
� Always transport the patient and bags/catheters as one piece
� Never inject anything into catheter

10/14/2013
17
Dialysis Related Problems
� Lightheaded –give fluids
� Hypotension
� Dysrhythmias
� Disequilibration Syndrome
� At end of early sessions
� Confusion, tremor, seizure
� Due to decrease concentration of blood versus brain leading to cerebral edema
Complications of HD
�Myocardial Ischemia
�Osmotic Shifts: cerebral edema
�Bacteremia
Chronic Renal Failure
� Nursing diagnosis
� Excess fluid volume
� Imbalanced nutrition
� Altered renal perfusion
� Ineffective coping
� Risk for infection
� Risk for injury
Chronic Renal Failure
� Nursing care
� Frequent monitoring
� Hydration and output
� Cardiovascular function
� Respiratory status
� E-lytes
� Nutrition
� Mental status
� Emotional well being
� Ensure proper medication regimen
� Skin care
� Bleeding problems
� Care of the shunt
� Education to client and family
10/14/2013
18
Questions?