encephalitis and postinfectiousencephalitis neuroscience ... diseases/encephalitis and... ·...
TRANSCRIPT

Encephalitis andPostinfectious Encephalitis
John E. Greenlee, MD, FAAN
ABSTRACTPurpose of Review: Encephalitis and postinfectious encephalitis represent twoimportant conditions for the neurologist, both in terms of their presentations asneurologic emergencies and their potential to cause death or serious neurologicimpairment. This article reviews the major infectious and noninfectious causes of en-cephalitis and discusses postinfectious encephalitis as an indirect effect of systemicillness.Recent Findings: Encephalitis caused by herpes simplex virus type 1 and WestNile virus are of major importance. In addition, within the past few years we havegained improved understanding of the neurologic syndromes caused by varicella-zoster virus, the recognition of enterovirus 71 as a significant human pathogen, andthe realization that encephalitis may also occur by autoimmune mechanisms re-quiring immunosuppressive therapy. We have also learned that postinfectious en-cephalitis may be recurrent rather than monophasic, and that children and adultsinitially diagnosed with postinfectious encephalitis may later develop classic mul-tiple sclerosis.Summary: Encephalitis and postinfectious encephalitis present as neurologic emer-gencies requiring prompt diagnosis and initiation of treatment. Important concerns areto identify infectious conditions requiring antibiotic or antiviral therapy and post-infectious or other autoimmune encephalitides requiring immunosuppression.
Continuum Lifelong Learning Neurol 2012;18(6):1271–1289.
INTRODUCTIONIn approaching patients with suspectedCNS infection, the first task for the neu-rologist, as discussed in the article ‘‘AcuteBacterial and Viral Meningitis,’’ is todetermine whether the patient has bac-terial meningitis requiring emergent an-tibiotic therapy. When evidence of focalor diffuse parenchymal involvement ispresent, however, an important diag-nostic consideration becomes whetherthe patient has encephalitis or a post-infectious illness in which systemicinfection has caused an immune re-sponse directed against myelin or otherantigens. In recent years, a third possi-bility has been recognized: encephalitismay represent an autoimmune response
directed against neuronal membraneantigens or intraneuronal proteins.The clinical and radiologic features ofthese three entitiesVencephalitis, post-infectious encephalomyelitis, and auto-immune encephalopathyVmay differsignificantly, and recognition of thesedifferences facilitates diagnosis. This ar-ticle reviews the presentation, diagnosis,and treatment of these three importantclinical entities.
ENCEPHALITISAlthough encephalitis is usually consid-ered in termsofviral infections,other agentsmay involve brain parenchyma aswell. Themost urgent question to ask is whether thepatientwill require antiviral or antimicrobial
Address correspondence toDr John E. Greenlee,University of Utah, ClinicalNeuroscience Center, 175North Medical Dr E, Salt LakeCity, UT 84132,[email protected].
Relationship Disclosure:
Dr Greenlee has served as anauthor and associate editorfor MedLink and for TheMerck Manual, and hasreviewed records regardinglitigation for Oliver Maner LLP.Dr Greenlee also holds a meritreview from the United StatesDepartment of VeteransAffairs.
Unlabeled Use of Products/Investigational Use
Disclosure: Dr Greenleereports no disclosure.
* 2012, American Academyof Neurology.
1271Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Review Article
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

therapy. Three viral infections are ofprimary concern: herpes simplex virus(HSV) encephalitis, CNS involvement byvaricella-zoster virus, and West Nile virusencephalitis. Other infectious encephalit-ides, although important, are less common.
Herpes SimplexVirus EncephalitisHSV encephalitis (Table 2-1) representsonly 10% to 15% of cases of viral en-cephalitis in the United States. How-ever, it remains the most important ofviral encephalitides, because it is bothlethal if untreated and the only viralencephalitis for which therapy has beenproven effective in clinical trials. HSV isubiquitous in human populations. Twosubtypes of HSV infect humans: HSVtype 1 (HSV1) and HSV type 2 (HSV2).HSV1 is most commonly acquired inearly childhood. HSV2 is more commonlysexually transmitted and thus usuallyacquired during adolescence or adult-hood. Both agents persist in neuronswithin sensory ganglia. Limited evidencesuggests that HSV1 may also persistwithin the CNS.1 HSV1 is responsible for90% of cases of HSV encephalitis inadults; of these cases roughly two-thirdsrepresent reactivated infection.2
The pathogenesis of HSV encephali-tis is not well understood. Encephalitishas been postulated to follow spread ofvirus from trigeminal ganglia throughsensory fibers to the meninges over-lying temporal lobes and orbitofrontalcortex.3 Alternatively, encephalitis couldarise following reactivation of a latentvirus within the brain.1
HSV encephalitis affects men andwomen equally and may occur at any age.There is no seasonal incidence of infec-tion. Impaired host immunity is not arisk factor for HSV encephalitis, but theinfection may progress more graduallyin immunocompromised individuals.4
HSV encephalitis is usually unilateral butmay also be bilateral. The virus has a
predilection for orbitofrontal cortexand temporal lobes, with many cases alsoinvolving the cingulate cortex. The vi-rus is able to infect neurons, glia, andependyma. Vascular congestion and pe-techial hemorrhages may be present.Progression of the infection results in ex-tensive, frequently hemorrhagic, destruc-tion of the brain.5
HSV encephalitis presents with analmost universal triad of headache (inover 90% of cases), fever, and alterationin mental status, at times preceded bysymptoms of nonspecific mild illness.Changes inmental status at presentationmay range from confusion, frank psy-chosis, or somnolence to stupor or coma.Temporal lobe involvement may resultin seizures characterized by olfactory orgustatory hallucinations, or deja vu phe-nomena.6 Examination may reveal subtleor overt corticospinal tract signs or signssuggesting temporal lobe dysfunction.6
These may include upper-quadrant vi-sual field defects; aphasia when the dom-inant hemisphere is involved; and, whenthe infection is bilateral, loss of ability tostore and recall new information. Occa-sional patients will exhibit papilledemaat presentation. Rare patients may pre-sent with evidence of injury to other partsof the CNS, including occipital lobes andbrainstem, without temporal lobe involve-ment.7 Focal or generalized seizures,however, may occur at any point duringacute illness or after recovery.
CSF in HSV encephalitis typically con-tains a lymphocytic pleocytosis of 50 ormore cells/2L (median 130 cells/2L).6 Inoccasional patients, however, cell countmay be normal.6 Although HSV ence-phalitis is frequently hemorrhagic, thepresence or absence of red blood cellsin CSF does not differentiate HSV en-cephalitis from encephalitis due to othercauses.6 Median CSF protein concen-tration is 80 mg/dL but may range fromnormal to over 700 mg/dL; CSF glucoseconcentration is usually normal.6 MRI
KEY POINTS
h The most urgent questionto ask in the case of apatient with suspectedCNS infection is, ‘‘Doesthe patient requireimmediate antibiotic orantiviral therapy?’’
h Viral agents of primaryconcern are herpessimplex virus,varicella-zoster virus,and West Nile virus.
h Herpes simplex virusencephalitis remainsthe major cause ofnonepidemic fatalencephalitis.
h Herpes simplex virusencephalitis presentswith an almost universaltriad of headache,fever, and alterationin mental status.
h Temporal lobeinvolvement in herpessimplex virus encephalitismay result in seizurescharacterized byolfactory or gustatoryhallucinations, or deja vuphenomena.
1272 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 2-1 Major Infectious Agents Associated With Encephalitis
Agent (Vector)GeographicDistribution
PeakSeasonalIncidence
High-RiskPopulations Acute Diagnosis Treatment
VirusesHerpessimplex virus
Ubiquitous Noseasonalincidence
N/A; course of infectionmay be atypical inindividuals who areimmunosuppressed
CSF PCR Acyclovir
Varicella-zostervirus
Ubiquitous Noseasonalincidence
Individuals who areimmunocompromised
CSF PCR, IgM andIgG antibodies
Acyclovir
Cytomegalovirus Ubiquitous Noseasonalincidence
Individuals who areimmunocompromised,especially thosewith HIV
PCR Ganciclovir;foscarnet
West Nile virus(mosquito)
Entire UnitedStates
Summerand earlyfall
Individuals who areimmunocompromisedand older adults
CSF IgM Supportive
St Louisencephalitisvirus (mosquito)
Entire UnitedStates,especially theMidwest,MississippiRiverregions, andTexas
Summerand earlyfall
Older adults CSF IgM Supportive
Eastern equineencephalitisvirus (mosquito)
Easternseaboard,Gulf coast(includingTexas), andthe upperMidwestregions
Summerand earlyfall
Children and olderadults
CSF IgM Supportive
Enteroviruses Worldwide Summerand earlyfall
Individuals with IgGdeficiency, includingthose treated withrituximab
PCR Supportive(pleconaril)
Nonviral AgentsTreponemapallidum
N/A N/A AIDS Serology (rapidplasma reagenttest, CSF, VenerealDisease ResearchLaboratory test,fluoresceintreponemaantibody test)
Penicillin orceftriaxone
Continued on next page
1273Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

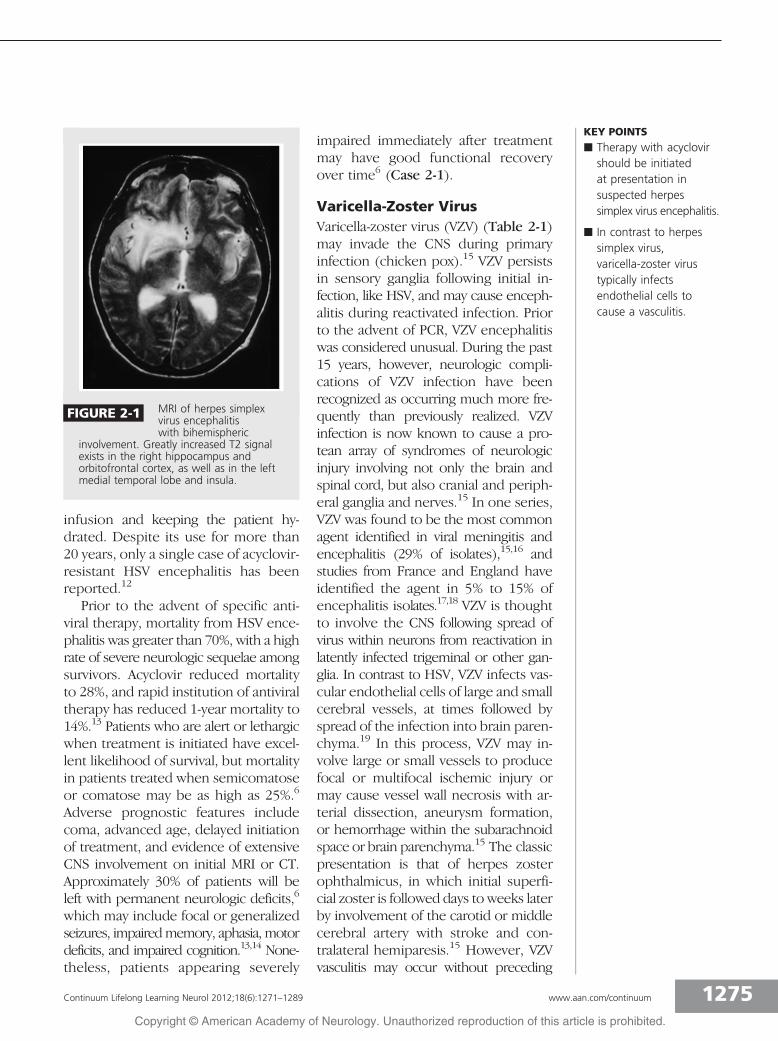
with and without gadolinium adminis-tration, the initial diagnostic procedureof choice, will usually demonstrate al-tered signal and gadolinium enhance-ment within the temporal lobe andmay also show involvement of insula,orbitofrontal cortex, or cingulate gyrus(Figure 2-1). MRI abnormalities inother regions of the cortex or brainstemwithout temporal lobe involvement donot exclude HSV encephalitis.5 CT withcontrast and EEG are less sensitive but,used together, may provide diagnosticinformation when MRI is not available.8
Specific diagnosis of HSV encephali-tis is made by amplification of viral DNAfrom CSF using PCR methods. Overalldiagnostic accuracy of PCR in patientswith brain biopsy-proven HSV encepha-litis is 98%.9 In some patients PCR maybe negative at presentation because oflow copy numbers of DNA in CSF. Inthese cases, repeat CSF PCR in 4 to 7 daysmay be positive.10 Diagnostic yield of PCRfalls to 21% in patients after 2 weeks of
antiviral treatment.9 Determination ofantibody titers is not of value in theacute diagnosis of HSV encephalitis. How-ever, comparison of serum versus CSFantibodies todetect intrathecal productionof antibody may be useful retrospec-tively and in rare cases may provide diag-nostic information when PCR is negative.11
The advent of acyclovir revolution-ized the treatment of HSV encephalitis.This agent inhibits HSV synthesis bycompeting with deoxyguanosine triphos-phate as a substrate for DNA polymeraseand causing DNA chain termination.4
Acyclovir is converted to its pharma-cologically active monophosphate formby virally encoded thymidine kinaseand thus becomes active only in in-fected cells.4 Acyclovir is administeredat 10 mg/kg body weight every 8 hoursfor 3 weeks. Complications of acyclovirtherapy are usually mild. The major ther-apeutic concern is nephrotoxicity dueto deposition of drug crystals; this isavoided by both controlling the rate of
Continued
Agent (Vector)GeographicDistribution
PeakSeasonalIncidence
High-RiskPopulations Acute Diagnosis Treatment
Rickettsiarickettsii (RockyMountainspotted fever,tick)
Entire UnitedStates; 960% ofcases present inNorth Carolina,Oklahoma,Arkansas,Tennessee, andMissouri
April toSeptember
N/A Serology(acute andconvalescentsera)
Tetracyclines orchloramphenicola
Listeriamonocytogenes
N/A N/A Infants, older adults,and individuals who areimmunocompromised
Bacterialculture (PCR)
Ampicillin
Mycoplasmapneumoniae
N/A N/A N/A Serology (PCR) Tetracycline,doxycycline, orerythromycinb
a Tetracyclines are usually avoided in younger children because they may stain teeth. However, because Rocky Mountain spotted fever(RMSF) has significant risk of causing fatal disease, doxycycline is recommended for both children and adults with suspected RMSF, withthe assumption that a single course of antibiotics may not affect teeth to a significant degree.
b Tetracyclines are avoided in younger children with M. pneumoniae infection because of their detrimental effect on dental enamel.
1274 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
infusion and keeping the patient hy-drated. Despite its use for more than20 years, only a single case of acyclovir-resistant HSV encephalitis has beenreported.12
Prior to the advent of specific anti-viral therapy, mortality from HSV ence-phalitis was greater than 70%, with a highrate of severe neurologic sequelae amongsurvivors. Acyclovir reduced mortalityto 28%, and rapid institution of antiviraltherapy has reduced 1-year mortality to14%.13 Patients who are alert or lethargicwhen treatment is initiated have excel-lent likelihood of survival, but mortalityin patients treated when semicomatoseor comatose may be as high as 25%.6
Adverse prognostic features includecoma, advanced age, delayed initiationof treatment, and evidence of extensiveCNS involvement on initial MRI or CT.Approximately 30% of patients will beleft with permanent neurologic deficits,6
which may include focal or generalizedseizures, impairedmemory, aphasia, motordeficits, and impaired cognition.13,14 None-theless, patients appearing severely
impaired immediately after treatmentmay have good functional recoveryover time6 (Case 2-1).
Varicella-Zoster VirusVaricella-zoster virus (VZV) (Table 2-1)may invade the CNS during primaryinfection (chicken pox).15 VZV persistsin sensory ganglia following initial in-fection, like HSV, and may cause enceph-alitis during reactivated infection. Priorto the advent of PCR, VZV encephalitiswas considered unusual. During the past15 years, however, neurologic compli-cations of VZV infection have beenrecognized as occurring much more fre-quently than previously realized. VZVinfection is now known to cause a pro-tean array of syndromes of neurologicinjury involving not only the brain andspinal cord, but also cranial and periph-eral ganglia and nerves.15 In one series,VZV was found to be the most commonagent identified in viral meningitis andencephalitis (29% of isolates),15,16 andstudies from France and England haveidentified the agent in 5% to 15% ofencephalitis isolates.17,18 VZV is thoughtto involve the CNS following spread ofvirus within neurons from reactivation inlatently infected trigeminal or other gan-glia. In contrast to HSV, VZV infects vas-cular endothelial cells of large and smallcerebral vessels, at times followed byspread of the infection into brain paren-chyma.19 In this process, VZV may in-volve large or small vessels to producefocal or multifocal ischemic injury ormay cause vessel wall necrosis with ar-terial dissection, aneurysm formation,or hemorrhage within the subarachnoidspace or brain parenchyma.15 The classicpresentation is that of herpes zosterophthalmicus, in which initial superfi-cial zoster is followed days to weeks laterby involvement of the carotid or middlecerebral artery with stroke and con-tralateral hemiparesis.15 However, VZVvasculitis may occur without preceding
KEY POINTS
h Therapy with acyclovirshould be initiatedat presentation insuspected herpessimplex virus encephalitis.
h In contrast to herpessimplex virus,varicella-zoster virustypically infectsendothelial cells tocause a vasculitis.
FIGURE 2-1 MRI of herpes simplexvirus encephalitiswith bihemispheric
involvement. Greatly increased T2 signalexists in the right hippocampus andorbitofrontal cortex, as well as in the leftmedial temporal lobe and insula.
1275Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

cutaneous zoster, herpes zoster ophthal-micus, or oticus and may involve vir-tually any vascular territory within thebrain or spinal cord. VZV vasculitis maybe more severe in patients with AIDS orother immunosuppression.15 CSF usu-ally reveals a mononuclear pleocytosis,at times with red blood cells. Hypogly-corrhachia may be present.15,20 VZV en-cephalitis is diagnosed by detection ofVZV IgG in CSF; in some patients anti-VZV IgM can be detected as well.15
Oligoclonal bands are commonly presentand are reactive with VZV proteins.15
PCR has a lower diagnostic sensitivity,and although it is helpful in confirmingthe diagnosis, a negative PCR result doesnot exclude VZV.15 Treatment of VZV
encephalitis is with acyclovir, 10 mg/kgevery 8 hours for a minimumof 14 days.Oral prednisone, 1mg/kg given daily for5 days, may be used to treat the inflam-matory component of the vasculitis; moreprolonged treatment is avoided topreventsteroid-induced immunosuppression.15
West Nile VirusWest Nile virus (WNV) (Table 2-1) is asingle-stranded RNA virus that belongsto the family Flaviviridae.21,22 Culex spe-cies mosquitoes (predominantly Culextarsalis and Culex pipiens) serve as theprimary vector for human infection. Thevirus infects multiple species of animalsand birds, in particular birds of the fam-ily Corvidae (eg, crows, jays, magpies,
KEY POINT
h Varicella-zoster virusvasculitis may occurwithout preceding rashand may involve virtuallyany vascular territorywithin the brain orspinal cord.
Case 2-1Just before traveling back to her college, a 21-year-old woman reportedsmelling an unusual, extremely unpleasant odor that was inapparentto everyone else in her family. Upon arriving at college, she went to bed.Her roommate was unable to waken her the next morning, and she wasbrought to the emergency department. Neurologic examination revealeda deeply somnolent woman who did not respond to voice but would reactto pain or to loud noise. The patient was without evidence of meningealirritation, and optic discs were flat. Neurologic examination revealed aright-sided hyperreflexia and right Babinski sign. MRI showed increasedsignal in the left temporal lobe, insula, and cingulate gyrus on T2 andfluid-attenuated inversion recovery (FLAIR) images, with enhancement inthese areas following gadolinium. CSF contained 41 red blood cells/2L and327 white blood cells/2L, 87% lymphocytes and 13% polymorphonuclearleukocytes, protein concentration of 271 mg/dL, and glucose concentrationof 73 mg/dL. The patient was given acyclovir. PCR analysis, reported 2 dayslater, was positive for HSV1. Acyclovir was continued for 21 days. Overthat period of time the patient regained consciousness but remainedsignificantly cognitively impaired. She left college for 18 months andduring that time had very slow improvement in intellectual function.Although psychological testing at the end of that time indicated persistentloss of cognitive abilities, she was able to return to school and resumework in her major field of study. She did well scholastically but found thatretention of new information was significantly more difficult for her thanhad been the case prior to her illness.
Comment. This patient’s initial olfactory symptoms are classic fortemporal lobe seizures and in patients presenting to the emergencydepartment should raise the question of herpes simplex virus encephalitisand suggest initiation of acyclovir if evidence of inflammation is present onCSF examination. The time course of this patient’s recovery, extending overmany months, is common in patients after herpes simplex virus encephalitis.
1276 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

ravens). Large ‘‘die-offs’’ of corvids havebeen reported to precede some WNVoutbreaks in humans. WNV producesinfection predominantly in the summerand early autumn, when mosquitoes aremost active. The virus has been identi-fied in all US states except Alaska andHawaii, and human infections havebeen reported in almost all of these states.In 2011, 690 cases were reported, of which474 cases represented neuroinvasive dis-ease with 43 deaths (www.cdc.gov/ncidod/dvbid/westnile/surv&controlCaseCount11_detailed.htm). Only 20%of patients develop symptomatic infec-tion, most commonly West Nile fever,which is typically characterized by malaise,fatigue, anorexia, headache, nausea, vom-iting, myalgia, fever, eye pain, and a non-specific maculopapular rash. West Nilefever usually lasts less than 7 days, althoughoccasional patients may remain symp-tomatic for as long as 6 weeks.21 Lessthan 1% of infected patients developneuroinvasive disease, which is morecommon in elderly and transplant pa-tients. Neuroinvasive WNV infection maypresent as meningitis, which is clinicallyindistinguishable from other viral men-ingitides; as encephalitis; or as a polio-myelitis with infection of spinal motorneurons (Case 2-2). West Nile enceph-alitis usually presents with fever, head-ache, and altered mental status, stupor,or coma. Signs of parenchymal involve-ment may include stupor or coma, cere-bellar ataxia, or movement disorders,including tremor, myoclonus, and par-kinsonian symptoms.23 The most-fearedcomplication of neuroinvasive WNV in-fection is a syndrome of acute flaccidparalysis (Case 2-2).23 Occasional pa-tients may also develop chorioretinitisor vitritis. CSF in neuroinvasive WNVinfection typically shows a mild eleva-tion in pressure (less than 250 mmH2O),lymphocytic pleocytosis, mild elevationof protein concentration, and a normalblood to CSF ratio of glucose concen-
tration. Cell count is usually 50 cells/2Lto 260 cells/2L but may be as high as2600 cells/2L and may be heavilypolymorphonuclear, particularly at pre-sentation.20,23 In one series, cell countwas normal in 20% of patients.24 Occa-sional patients have low sodium levelsindicative of the syndrome of inappro-priate antidiuretic hormone secretion.MRI is often normal, although occasionalpatients will have areas of increasedsignal on T2 and FLAIR imaging in thesubstantia nigra, basal ganglia, andthalamus.25 A single, acute CSF speci-men positive for WNV-specific IgM an-tibodies is diagnostic of ongoing WNVinfection.25 PCR is less reliable. Pairedsera positive for WNV-specific IgM an-tibodies (a fourfold or greater rise intiter from the ‘‘acute’’ serum, obtained0 to 7 days after symptom onset, andthe ‘‘convalescent’’ serum, obtained 14to 21 days after illness onset) also pro-vide serologic confirmation. Treatmentof WNV encephalitis is supportive.Prognosis for recovery after encepha-litis is good, although recovery may beextremely prolonged. The likelihood ofcomplete recovery after West Nile flac-cid paralysis is poor.23,25
Other Arthropod-BorneEncephalitidesA variety of other arthropod-borne agentsmay infect humans and cause neurologicdisease (Table 2-1). All but two of theseagents are carried by mosquitoes, andrates of infection peak in midsummerthrough early autumn. The exceptionsto this rule are Colorado tick fever andPowassan virus encephalitis, which aremost frequent in late spring and earlysummer. Prior to the occurrence ofWNV in the United States, St Louis en-cephalitis had been the most commonarthropod-borne cause of encephalitis,and Eastern equine encephalitis virusthe most dangerous. Other, less com-mon agents include viruses of the
KEY POINTS
h Neuroinvasive West Nilevirus infection maypresent as meningitis,encephalitis, or apoliomyelitislikesyndrome of flaccidparalysis.
h Diagnosis of neuroinvasiveWest Nile virus is made bydetection of antiviral IgMantibody in CSF.
1277Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

California/LaCrosse serogroups, Powassanvirus, and Colorado tick fever virus.Although laboratories routinely test forWestern equine encephalitis virus, nohuman case of the infection has beenreported since 1994 (diseasemaps.usgs.gov/wee_historical.html).
St Louis encephalitis virus, like WNV,is a mosquito-borne virus that is a mem-ber of the family Flaviviridae. Cases ofneuroinvasive St Louis encephalitis havebeen reported from almost every state,but most occur in the central Midwestand Texas. St Louis encephalitis normallyoccurs as scattered rural cases but mayalso cause periodic urban epidemics.St Louis encephalitis resembles neuro-invasive West Nile disease, with the ex-ception that cases of poliomyelitis areuncommon. Like WNV, St Louis enceph-alitis virus producesmore severe diseasein older adults. CSF findings are similarto those seen in West Nile encephalitis.
Diagnosis, as in the case of neuroinva-sive WNV infection, is by CSF IgM or byrise in antibody titers.
Easternequineencephalitis virus (EEEV)is an agentofwading andmigratory birds.26
The virus is found predominantly alongthe Atlantic seaboard, the Gulf of Mexicocoast, and states abutting Lake Michigan(Indiana, Michigan, and Wisconsin). Inci-dental exposure or spread of the virusinto other mosquito species facilitatesthe spread of the virus into humans orother species. Although the virus doesnot usually produce severe infection inits natural hosts, it can produce severeepizootic infection in flocks of turkeys orin exotic or game-farm birds, as well asinfections in horses. EEEV encephalitisis rare in humans, and reported casesover the past 4 decades have averagedonly five cases annually. EEEV infectionsare less likely to be asymptomatic than areinfections with other arthropod-borne
KEY POINT
h St Louis encephalitismay occur as isolatedcases or as urbanoutbreaks.
Case 2-2During a late-summer weekend, an emergently hospitalized 48-year-oldman was diagnosed with Guillain-Barre syndrome due to Epstein-Barr virus(EBV). The patient had been in good health until 10 days prior toadmission, when he had a mild systemic illness with fever and myalgiasthat quickly resolved. On the day of admission, he awoke with bilateralleg weakness that subsequently involved his arms. Lumbar puncturerevealed 32 cells/2L, 81% lymphocytes, 11% monocytes, and 8%neutrophils, with a protein concentration of 120 mg/dL, and a glucoseconcentration of 72 mg/dL. CSF PCR detected EBV DNA. By the time theneurologist saw the patient, he was in respiratory distress, with normalcranial nerves and sensory examination but with flaccid upper and lowerextremities. Gadolinium-enhanced MRI showed increased signal in anteriorhorns at several levels in cervical and thoracic spine. WNV IgM wasdetected in both serum and CSF, with evidence of intrathecal antibodyproduction. The patient became ventilator dependent, could not beweaned, and died several weeks later after ventilatory support wasterminated at the request of the patient and his family.
Comment. Neuroinvasive WNV infection may cause meningitis,encephalitis, or a poliomyelitis with destruction of anterior horn cells.The virus should be a diagnostic consideration in patients presenting withany of these clinical features in summer or early autumn. EBV produceslatent infection of B lymphocytes, and EBV DNA can thus be present inCSF in any infection resulting in a lymphocytic pleocytosis and may notsignify that EBV is the causative agent.
1278 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

agents, in particular in individuals at theextremes of life. In individuals between 4and 55 years of age, the ratio of in-apparent EEEV infections to cases ofencephalitis is 29:1. In contrast, the ra-tio in infants is 8:1, and the ratio inindividuals over 55 years of age is 16:1.27
EEEV encephalitis is frequently precededby a prodromal illness, which may in-clude fever, headache, and abdominalpain that may occasionally be severeenough to mimic an acute abdominalemergency.28 Onset of the encephalitisis frequently abrupt and severe, partic-ularly in children or older adults. Presen-tation as a meningitis is unusual, andnearly 70% of patients present in stuporor coma.28 Focal signs of corticospinalor extrapyramidal dysfunction may bepresent, and the illness may be com-plicated by focal or generalized seizures.Overall mortality approaches 36%, with35% of survivors having significant neu-rologic impairment.28
Enteroviral EncephalitisEnteroviruses are small, unenvelopedsingle-stranded RNA viruses within thefamily Picornaviridae (Table 2-1). Althoughover 70 serotypes of enteroviruses havebeen identified, coxsackievirus A9 andechoviruses E7, E9, E11, E19, and E30have accounted for 70% of all culturedisolates from CSF. Enteroviruses are dis-seminated by fecal-oral spread. Enter-oviral infections tend to cluster duringsummer months, when conditions ofsanitation tend to be most relaxed, butmay also occur throughout the year.Although enteroviruses are most com-monly associated with viral meningitis(see preceding article), they may alsocause encephalitis and, rarely, paralyticdisease. Enterovirus 71 most com-monly causes the childhood conditionshand, foot, and mouth disease andherpangina. Hand, foot, and mouth dis-ease is characterized by oral ulcers and acutaneous rash, whereas lesions in her-
pangina are confined to the oropharynx.In addition, however, enterovirus 71 mayproduce more severe disease with involve-ment of brainstem or, less frequently,of cortex, cerebellum, or spinal ventralroots.29 CSF findings in enteroviralmeningoencephalitis are typically amild lymphocytic pleocytosis, mild ele-vation of protein concentration, and nor-mal glucose concentration.20 During thefirst 24 to 48 hours of infection, CSFmay contain a mixture of polymorpho-nuclear leukocytes and lymphocytes.20
MRI studies are usually unremarkablebut have shown cerebral or hippocampallesions in some patients.30 Enterovirus 71has been associated with MRI abnor-malities in brainstem and, less frequently,cortex or cerebellum; these may be bestseen on diffusion-weighted images.31
Pleconaril, an antiviral drug that bindsto a hydrophobic pocket in the major pro-tein of the enterovirus capsid VP1, has beenshown to be of modest benefit in cases ofenteroviral CNS infections but is not ap-proved for use in the United States.32,33
Other Viral AgentsMumps virus was formerly a majorcause of viral meningoencephalitis buthas essentially disappeared as a causa-tive agent of meningoencephalitis inthe Western world following introduc-tion of widespread immunization. Themouse arenavirus, lymphocytic chorio-meningitis virus, may cause meningitisor encephalitis in individuals exposed toinfectedmice or hamsters (Table 2-1).34
The infection is rarely fatal, but recoverycan be prolonged, and the infection isone of the few viral CNS infections thatmay cause hypoglycorrhachia. ParvovirusB19, the agent of the childhood con-dition erythema infectiosum (fifth dis-ease), may cause encephalitis in bothchildren and adults.35 A number of vi-ruses typically produce infections in im-munocompromised patients and do soonly infrequently in healthy individuals.
KEY POINTS
h Although enteroviralencephalitis occurspredominantly duringsummer months,sporadic cases occurthroughout the year.
h Lymphocyticchoriomeningitis virusencephalitis is associatedwith exposure to mice orinfected pet hamsters.
1279Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Cytomegalovirus is classically associatedwith encephalitis in neonates but mayalso cause encephalitis in adults andwas a major complication of AIDS priorto the widespread use of highly activeantiretroviral therapy. The virus mayalso cause encephalitis in other groupsof immunocompromised patients andoccasionally in individuals withoutunderlying disease.36 Herpesviruses 6(HHV-6, associated with roseola infan-tum) and HHV-7 are frequent agents ofearly childhood infection and in thissetting may result in convulsions and,rarely, encephalopathy.37 HHV-6 hasalso been associated with encephalitis,often involving limbic structures, intransplant or other immunosuppressedindividuals. In one study, HHV-6 wasdetected in the CSF of 40% of patients
with encephalitis of otherwise unde-termined cause, suggesting that it is anunderappreciated causative agent forviral encephalitis.38 EBV has been as-sociated with a wide variety of neuro-logic syndromes, including meningitis,encephalitis, and postinfectious enceph-alitis. Although the virus is almost cer-tainly responsible for cases of encephalitis,the association of EBV with individualcases is made difficult by the fact thatthe virus produces latent infection of lym-phocytes, so detection of EBV by PCRmethods in patients with CSF pleocyto-sis may or may not indicate that thevirus is the causative agent. Treatmentof cytomegalovirus encephalitis hasbeen with ganciclovir, with foscarnet usedas an alternative agent33 (Table 2-2).Controlled trials of therapy have not
KEY POINT
h Human herpesvirus 6 isa cause of encephalitisin transplant patients.
TABLE 2-2 Acute Treatment of Encephalitis
Condition orAgent
TherapeuticAgent Dose and Duration of Treatment
Herpes simplexencephalitis
Acyclovir 10 mg/kg every 8 hours for 3 weeks
Varicella-zosterencephalitis
Acyclovir 10 mg/kg every 8 hours for 10 to 14 days
Cytomegalovirusencephalitis
Ganciclovir Ganciclovir: 5 mg/kg every 12 hours for14 to 21 days
Foscarnet Foscarnet: 60 mg/kg every 8 hours for 2 to3 weeks
Enterovirusencephalitis
Pleconaril Not available in the United States
Syphilis Penicillin 20 million U/d IV for 10 days
Rocky Mountainspotted fever
Doxycycline Adults: 100 mg every 12 hours
Children: 2.2 mg/kg every 12 hours
Listeriamonocytogenes
Ampicillin Adults: 1 g/IV to 2 g/IV every 3 to 4 hours
Mycoplasmapneumoniae
Doxycycline Adults: 100 mg every 12 hours Children:2.2 mg/kg every 12 hours
Erythromycin Adults: 250 mg to 1000 mg every 6 hoursdepending on severity of infection
Children 30 mg/kg/d to 50 mg/kg/d in fourdivided doses
1280 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

been reported for HHV-6 encephalitis;ganciclovir, foscarnet, and acyclovirhave been used in individual patients.
Rabies virus is a rare cause of viral en-cephalitis in Western countries but re-mains a significant concern in countrieswhere dogs are not routinely vaccinated.In the United States, rabies is most fre-quently associatedwith bat bites and lessoften with bites from raccoons, skunks,and foxes. Treatment of animal bites in-cludes cleaning of the infected wound,injection of rabies immunoglobulin, andimmunization with human diploid cellrabies vaccine (www.cdc.gov/rabies/exposure/). Only five individuals areknown to have survived rabies. One sur-viving patient was treated with inducedcoma using ketamine, midazolam, andphenobarbital.39,40 The possibility ofrabies should be considered in patientsknown to have suffered animal bites orto have been exposed to bats, and inpatients fromunderdeveloped countries.It is important to remember that theincubation period of rabies may be upto several years and that the puncturewounds produced by bat bites may beso small as to escape detection.41
Encephalitis Caused byNonviral AgentsA number of treatable bacterial and otherorganisms may produce brain parenchy-mal involvement to mimic viral encepha-litis (Table 2-1). Meningovascular syphilismay present with subacutely or acutelyprogressive symptoms, and parenchy-mal changes that resemble HSV enceph-alitis may be seen on MRI (Figure 2-2).42
Listeria monocytogenes may producerhombencephalitis or brainstem enceph-alitis in both immunosuppressed andimmunologically healthy individuals. L.monocytogenes may occasionally pro-duce cortical encephalitis resemblingHSV encephalitis on MRI.43 Mycoplasmahas most commonly been associatedwith postinfectious encephalitis (see
below) but may also involve the CNSacutely. Rickettsia rickettsii, the agentof Rocky Mountain spotted fever, canproduce a cerebral vasculopathy and maydo so in the absence of a cutaneous rash.44
The disease, spread by ticks, occurs inmost states but is prevalent along theMid-Atlantic seaboard. Cases occur through-out the year but are most commonbetween April and September (www.cdc.gov/rmsf/stats/). Other rickettsialspecies, including Rickettsia prowazekii,the agent of epidemic typhus, have alsobeen associated with human infection.45
Treatment regimens for these infectionsare shown in Table 2-2.
Autoimmune EncephalitisAn emerging concern in the diagnosisof patients presenting with encephalitisis the recognition that paraneoplastic andother autoimmune conditionsmay presentas limbic or other encephalitis (Table 2-3).An encephalitic presentationVusuallylimbic encephalitisVhas been reportedwith paraneoplastic autoantibodies, such
KEY POINT
h Rocky Mountainspotted fever maycause systemic andCNS infection in theabsence of acutaneous rash.
FIGURE 2-2 MRI showing temporal lobe andhippocampal involvementsuggestive of herpes simplex
virus encephalitis in a patient with meningovascularsyphilis who presented with stupor.
1281Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

as anti-Hu, anti-Ri, or anti-Ma1 or Ma2, aswell as in patients expressing a numberof autoantibodies against neural surfaceantigens, including the NMDA receptor(NMDAR), the !-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid recep-tor (AMPAR), the metabotropic glutamatereceptor subunit mGluR5, componentsof the voltage-gated potassium channelcomplex (leucine-rich, glioma inacti-vated 1, and contactin-associated pro-teinlike 2), and +-aminobutyric acid B
receptors.46 These conditions differ fromacute viral encephalitis in that their on-set is usually more gradual and they tendto be progressive over time. The mostfrequent of these appears to be encepha-litis associated with anti-NMDAR antibo-dies. The presence of these antibodieswas initially found in patients with ovar-ian teratomas. However, in epidemiologicstudies by the California EncephalitisProject, anti-NMDAR encephalitis wasidentified over 4 times more frequently
KEY POINT
h Antibodies to neuronalsurface receptors, inparticular NMDAreceptors, may beassociated withlimbic and otherencephalitides.
TABLE 2-3 Major Antineuronal Antibodies AssociatedWith Encephalitis
Antibody Major Clinical FeaturesMajor TumorAssociations
Directed against intraneuronal antigensAnti-Hua Limbic, brainstem, or cerebellar
encephalitisSmall cell lung cancer,other small cell orneuroendocrine tumors
Anti-Ria Limbic, brainstem, or cerebellarencephalitis
Small cell lung cancer,breast cancer
Anti-Ma 1 and 2a Limbic encephalitis (especiallyMa2), diencephalic orbrainstem encephalitis
Varying neoplasms (Ma1),testicular neoplasms(Ma2)
Directed against neuronal receptor proteins or other neuronal antigens
Anti-NMDAR Limbic encephalopathy withautonomic features, seizures,respiratory failure
Ovarian teratomas(absent in most cases)
Anti-AMPAR Limbic encephalitis Thymus cancer, lungcancer, breast cancer
Anti-mGluR5 Limbic encephalitis Hodgkin disease
Anti-GABA(B) Limbic encephalitis Small cell lung cancer,other neoplasms (È45%of patients)
Anti-VGKCcomplex(anti-LGi1,anti-CASPR2)
Limbic encephalitis,faciobrachial dystonic seizuresor other seizures (anti-LGi1)
No clear tumorassociation
960% of patients may havehyponatremia
NMDAR = NMDA receptor; AMPAR = !-amino-3-hydroxy-5-methyl-4-isoxazole propionic acidreceptor; mGluR5 = metabotropic glutamate receptor 5; GABA(B) = +-aminobutyric acid receptortype B; VGKC = voltage-gated potassium channel; LGi1 = leucine-rich, glioma inactivated 1;CASPR2 = contactin-associated proteinlike 2.a The role of antibodies directed against internal neuronal proteins in disease causation has notbeen determined.
1282 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

than HSV1, WNV, or VZV and was theleading cause of identified encephalitis.46
In this study, 65% of cases occurred inpatients aged 18 years or younger.46
The condition was more common in fe-males and tended to be characterized byseizures, language dysfunction, psycho-sis, autonomic instability, and EEG ab-normalities.46 CSF usually showed amild lymphocytic pleocytosis (average23 cells/2L; range 0 to 252 cells/2L), nor-mal or mildly elevated protein concentra-tion, and normal glucose concentration.MRI showed temporal lobe abnormal-ities in 48% of patients.46 Most patientshad no teratomas or other neoplasms.
Standardized regimens of treatmentfor autoimmune encephalitis have not yetbeen developed. Treatment has relied oncorticosteroids, with plasma exchange,IV immunoglobulin (IVIg), and immu-nosuppressive or immunomodulatoryagents, such as cyclophosphamide or
rituximab.47 Patients with antibodyresponse against cell surface antigenshave, in general, responded well to treat-ment.44 Patients with antibodies direc-ted against intracellular proteins, suchas anti-Hu, have tended to be muchmore resistant to treatment.47
POSTINFECTIOUS ENCEPHALITISPostinfectious encephalitis was tradi-tionally defined as an acute, monophasic,demyelinating illness that usually occurswithin 2 to 4weeks of viral or other illnessand believed to be an immune attack oncomponents of myelin or other relatedantigens (Case 2-3). Although postinfec-tious encephalitis has most frequently beenassociated with viral infections, caseshave also been associated with infectionsdue to a wide variety of other agents(Table 2-4).48 The condition is charac-terized by multifocal perivenous demy-elination and bears strong similarity to
KEY POINT
h Patients developinglimbic encephalitis inassociation withparaneoplasticautoantibodies suchas anti-Hu are lessresponsive to treatmentthan those whoseencephalitis is caused byantibodies to neuronalsurface antigens.
Case 2-3A 16-year-old boy had been in good health until 2 weeks prior toadmission, when he developed a flulike illness characterized by fever,myalgias, and cough. He recovered from the illness without difficulty buton the morning of admission was confused upon awakening and thenbecame unresponsive. General physical examination was normal except forvery mild nuchal rigidity. Neurologic examination revealed the patientto be stuporous but able to move all four extremities in response to pain.The patient had brisk reflexes with bilateral Babinski signs. CSF contained34 white blood cells, protein concentration of 78 mg/dL, and glucoseconcentration of 65 mg/dL with a simultaneous blood glucose level of104 mg/dL. MRI revealed multiple irregular areas of increased signal on T2and FLAIR imaging, with gadolinium enhancement of two of the lesions.All cultures were negative, as were test results for PCR, HSV, VZV,enteroviruses, EBV, and Mycoplasma pneumoniae. CSF and serum serologyfor WNV was negative, but the patient had elevated antibody titersto M. pneumoniae. The patient was diagnosed with postinfectiousencephalomyelitis and treated with a 5-day course of IVmethylprednisolone 1000 mg/d, followed by a prednisone taper. Heregained consciousness over the next several days and improved steadily,returning to school on a part-time basis after 3 months. When seen infollow-up at 6 months, he was neurologically healthy.
Comment. This patient’s course of an acute neurologic illness following asystemic illness is classic for postinfectious encephalitis, as were the changesseen on MRI. Prognosis for complete recovery is excellent in most cases.
1283Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

two other conditions: (1) postvaccinalencephalomyelitis that follows immu-nization and (2) the experimental au-toimmune demyelinating disease,experimental allergic encephalomyeli-tis.48,49 In recent years, postinfectiousand postvaccinal encephalomyelitis havebeen grouped under the common termacute disseminated encephalomyelitis(ADEM).49,50 ADEM is not the conse-quence of a specific infection or im-munization but rather a final common
pathway of autoimmune CNS injury trig-gered by many agents or immunogens.
Postinfectious encephalitis is mostcommon in children but can also occurin adults. The condition is rare in olderadults. In children, the peak age at onsetis 5 to 8 years. The disorder is morecommon in winter and spring months.A study from San Diego County gave amean incidence of 0.4 per 100,000 peryear among individuals younger than 20years. Of these patients, 93% reported
KEY POINTS
h Postinfectious encephalitismay be associated with awide variety of precedingsystemic infections.
h Postinfectious encephalitisis most common inchildren but may alsoaffect adults.
TABLE 2-4 Major Infectious and Vaccine Associations ofPostinfectious Encephalitis and Acute DisseminatedEncephalomyelitisa
b Viruses
Smallpox(1:1000Vhistorical)
Rubella (1:20,000)
Varicella (1:10,000)
Measles
Mumps
Influenza A (H1N1)
HIV
Human T-celllymphotrophic virus type I
Hepatitis A, B, and C
Herpes simplex virus,Epstein-Barr virus,cytomegalovirus, humanherpesvirus type 6
Enteroviruses
Coronaviruses
Hantavirus (Puumala virus)
b Bacteria
Streptococcus A
Chlamydiae
Campylobacter
Mycoplasma pneumoniaea Adapted from Sonneville R, et al, J Infect.48 B 2009, with permission from Elsevier.www.sciencedirect.com/science/article/pii/S0163445309000759.
Legionella
Leptospira
Rickettsia rickettsii
Salmonella typhi
Mycobacterium tuberculosis
b Protozoa and Other
Toxoplasma gondii
Plasmodium species
b Immunizations
Rabies
Neural type (Semple vaccine)(1:300 to 1:7000)
Human diploid cell vaccine(G1:75,000)
Diphtheria-tetanus (0.9:100,000)
Poliovirus
Varicella (3:665,000)
Smallpox (0.1:100,000)
Japanese encephalitis(0.2:100,000)
Hepatitis B
Influenza
Yellow fever
1284 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

symptoms of infection within 21 days ofthe onset of illness and an additional 5%had received immunization within thepreceding month.51 The onset ofADEM may be preceded by fever,malaise, headache, nausea, or vomit-ing. These prodromal symptoms arefollowed by the abruptVat times ful-minantVonset of illness. Altered men-tal status, which is almost universal inchildren, may range from drowsiness tofrank coma. Meningeal signs are com-mon. Focal or multifocal neurologic signsmay involve brain, spinal cord, or opticnerves and include unilateral or bilateralcorticospinal tract signs, hemiplegia, ataxia,cranial nerve palsies, and visual loss. Hemi-spheric involvement may produce apha-sia or parietal lobe findings of sensoryloss or neglect. Focal or generalized sei-zures may occur; these are rare in adultsbut common in young children, occur-ring in up to 70% of children youngerthan 5 years, 80% of whom may developstatus epilepticus.52 In many cases,ADEM is confined to the brain andspinal cord. However, the disorder maysimultaneously cause optic neuritis orinvolve the peripheral nervous system.The simultaneous occurrence of centraland peripheral demyelinating eventsappears to be more common in adultsthan in children.53
Postinfectious encephalitis should beconsidered in the differential diagnosisof any patientVin particular any childVpresenting with evidence of acute, in-flammatory neurologic illness in the settingof a previous systemic illness. Makingthe diagnosis, however, should be pre-ceded by ruling out actual CNS infection.The presence of multifocal neurologicsigns should raise the level of suspicionof ADEM, as should the presence ofsigns referable to both the CNS and theperipheral nervous system. CSF typi-cally shows a lymphocytic pleocytosis, al-though roughly 30% of patients will havea mixed pleocytosis with a neutrophilic
predominance.48 The frequency withwhich oligoclonal bands are detected iscontroversial.48,54 Traditionally, the pres-ence of oligoclonal bands was consideredunusual. However, oligoclonal bandswere detected in 20% of patients withADEM in one study.55 In another study,oligoclonal bands were reported in 65%of individuals presenting an illness ini-tially diagnosed as ADEM; however, over50% of these patients were subsequentlydiagnosed with multiple sclerosis.54
MRI with gadolinium enhancementis the diagnostic study of choice. T2 andFLAIR images classically show multiple,large, asymmetric, irregularly shapedlesions involving subcortical white mat-ter and the gray-white junction of bothcerebral hemispheres (Figure 2-3).54
Periventricular white matter may be in-volved, but lesions confined to the corpuscallosum are unusual.53 Gadolinium en-hancement is seen in 30% to 100% of
KEY POINTS
h Patients presentingwith postinfectiousencephalitis almostalways have alterationin level of consciousness;meningeal signs arecommon.
h MRI is the diagnosticprocedure of choice inpatients with suspectedpostinfectiousencephalitis.
FIGURE 2-3 MRI showing multiple areas ofincreased T2 signal consistentwith demyelination in a patientwith acute disseminatedencephalomyelitis.
Reprinted from Wender M, J Neuroimmunol.50
B 2011, withpermission from Elsevier. www.jni-journal.com/article/S0165-5728(10)00438-8/abstract.
1285Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

patients and may vary with the stageof the disease.51 Ring-enhancing le-sions may be found but should raiseparticular concern about brain abscessor other CNS infection.52 Spinal cordinvolvement, usually with extensive cordedema and swelling, may occur in chil-dren or adults and commonly affectsthe thoracic cord.52 Despite theirworrisome appearance at presenta-tion, most lesions resolve over time.53
Randomized controlled trials of dif-ferent therapeutic agents do not existfor ADEM in children or adults, nor dostudies exist comparing one agent withanother.48,53 Class 3 evidence exists forthe use of methylprednisolone, usuallyused as 1 g per day for 5 days.56 Plasmaexchange (usually five exchanges) orIVIg, given to a total dose of 1 g/kg to2 g/kg during 3 to 5 days, has also beenused, either in combination with meth-ylprednisolone or after methylpred-nisolone failure.48 A variety of otherimmunosuppressive agents, includingcyclophosphamide, have been used inindividual cases.
The outcome of ADEM is usuallyfavorable. In most studies, 50% to 75%of patients undergo complete recoveryover time52,54; up to 90% of children mayundergo essentially complete recovery,although some may have persistentmild neurocognitive deficits.52,53 Thelikelihood of residual deficit may alsobe greater in patients presenting withoptic neuritis.52 In recent years it hasbeen realized that ADEM may berecurrent.49 An ongoing diagnostic chal-lenge is the recognition that a subset ofpatients, perhaps as high as 30%, willlater develop multiple sclerosis.49,55
Acute HemorrhagicLeukoencephalitisIn occasional patients (2% of a large cohortof children52), postinfectious encepha-litis may be much more severe, pre-senting with fulminant hemorrhagic
demyelination and cerebral edema. MRIstudies, in addition to findings sugges-tive of demyelination, hemorrhage, andedema, may show evidence of ischemiaon diffusion-weighted images.57 Thisdisorder has also been termed acutenecrotizing hemorrhagic leukoencepha-litis or Weston Hurst syndrome. Unlikepostinfectious encephalitis, acute nec-rotizing hemorrhagic leukoencephalitishas a high rate of mortality. In individualreports, however, some patients maysurvive following aggressive and earlytreatment using combinations of meth-ylprednisolone, IVIg, plasma exchange,or cyclophosphamide.53
APPROACH TO THE PATIENTWITH ENCEPHALITIS ORPOSTINFECTIOUS ENCEPHALITISThe possibility of meningitis or encepha-litis should be suspected in any severelyill patient presenting with alteration inconsciousness, with or without focal neu-rologic signs. Signs suggesting temporallobe involvement should hint at HSVencephalitis but may occasionally becaused by other agents. The possibilityof arthropod-borne encephalitis, enter-ovirus encephalitis, or Rocky Mountainspotted fever should be kept in mind inpatients presenting during summermonths. In areas of geographic preva-lence, a history of tick bite may suggestRocky Mountain spotted fever. Thepresence of a generalized skin rashmay suggest Rocky Mountain spottedfever or WNV infection. Presentationwith abrupt onset of impaired con-sciousness with multifocal neurologicsigns following a systemic infection ofalmost any sort, especially in childhood,should raise the possibility of postinfec-tious encephalitis.
At presentation, the overriding clin-ical concern is that the patient may haveacute bacterial meningitis, and patientsshould be treated with antibiotics untilbacterial meningitis has been excluded.
KEY POINTS
h Treatment of postinfectiousencephalitis is withIV methylprednisolone.Plasma exchange or IVimmunoglobulin shouldalso be considered.
h Patients presenting withsuspected encephalitisrequire presumptivetreatment withantibiotics and acycloviruntil bacterial infectionand herpes simplex virusencephalitis have beenruled out.
1286 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

HSV encephalitis should be suspectedVand, like bacterial meningitis, treated onsuspicionVin any individual presentingwith altered consciousness and evi-dence of inflammatory CSF response,unless some other cause for the con-dition is identified at presentation. MRIwith gadolinium is an essential di-agnostic tool in HSV encephalitis; how-ever, it should be kept in mind thatneurosyphilis and infections by otheragents, including L. monocytogenes,may occasionally mimic MRI findingsseen in HSV encephalitis.
The supportive care of patients withencephalitis or postinfectious encepha-litis is both complex and demanding.Treatment of seizures is usually straight-forward but may occasionally require ag-gressive therapy. Some patients willdevelop the syndrome of inappropriateantidiuretic hormone secretion and mayrequire careful attention to electrolytebalance. Cerebral edemamay become amajor concern. Although dexamethasonehas been used for many years to reducecerebral edema in patients with encepha-litis, its efficacy has not been establishedand is currently being evaluated inpatients with HSV encephalitis in a multi-center trial. Decompressive craniectomyhas been associated with patient sur-vival in one case of HSV encephalitis withintractable cerebral edema.58 In severelyill patients, survival may depend heavilyon meticulous attention to details ofdaily care. Because recovery from ence-phalitis or postinfectious encephalitismaybe extremely prolonged, patients maynot reach optimal improvement forweeks or months. In such cases, the re-covering patient and his or her familymay need ongoing counseling over time.
REFERENCES1. Baringer JR, Pisani P. Herpes simplex virus
genomes in human nervous system tissueanalyzed by polymerase chain reaction.Ann Neurol 1994;36(6):823Y829.
2. Nahmias AJ, Whitley RJ, Visintine AN, et al.Herpes simplex virus encephalitis: laboratoryevaluations and their diagnostic significance.J Infect Dis 1982;145(6):829Y836.
3. Davis LE, Johnson RT. An explanation for thelocalization of herpes simplex encephalitis?Ann Neurol 1979;5(1):2Y5.
4. Whitley RJ, Lakeman F. Herpes simplex virusinfections of the central nervous system:therapeutic and diagnostic considerations.Clin Infect Dis 1995;20(2):414Y420.
5. Herpes simplex encephalitis. In: Booss J, EsiriMM, editors. Viral encephalitis in humans.Washington, DC: ASM Press, 2003:41Y60.
6. Whitley RJ, Soong SJ, Linneman C Jr, et al.Herpes simplex encephalitis. Clinicalassessment. JAMA 1982;247(3):317Y320.
7. Jubelt B, Mihai C, Li TM, Veerapaneni P.Rhombencephalitis/brainstem encephalitis.Curr Neurol Neurosci Rep 2011;11(6):543Y552.
8. Al-Shekhlee A, Kocharian N, Suarez JJ.Re-evaluating the diagnostic methods inherpes simplex encephalitis. Herpes 2006;13(1):17Y19.
9. Lakeman FD, Whitley RJ. Diagnosis of herpessimplex encephalitis: application ofpolymerase chain reaction to cerebrospinalfluid from brain-biopsied patients andcorrelation with disease. National Instituteof Allergy and Infectious DiseasesCollaborative Antiviral Study Group. J InfectDis 1995;171(4):857Y863.
10. Weil AA, Glaser CA, Amad Z, Forghani B.Patients with suspected herpes simplexencephalitis: rethinking an initial negativepolymerase chain reaction result. Clin InfectDis 2002;34(8):1154Y1157.
11. Denes E, Labach C, Durox H, et al.Intrathecal synthesis of specific antibodiesas a marker of herpes simplex encephalitisin patients with negative PCR. Swiss MedWkly 2010;140:w13107.
12. Schulte EC, Sauerbrei A, Hoffmann D, et al.Acyclovir resistance in herpes simplexencephalitis. Ann Neurol 2010;67(6):830Y833.
13. Hjalmarsson A, Blomqvist P, Skoldenberg B.Herpes simplex encephalitis in Sweden,1990Y2001: incidence, morbidity, andmortality. Clin Infect Dis 2007;45(7):875Y880.
14. McGrath N, Anderson NE, Croxson MC,Powell KF. Herpes simplex encephalitistreated with acyclovir: diagnosis and longterm outcome. J Neurol NeurosurgPsychiatry 1997;63(3):321Y326.
15. Gilden D, Cohrs RJ, Mahalingam R, NagelMA. Varicella zoster virus vasculopathies:
KEY POINT
h Patient survival inencephalitis maydepend on control ofintracranial pressure andmeticulous attention todetails of electrolytestatus and generalpatient care.
1287Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

diverse clinical manifestations, laboratoryfeatures, pathogenesis, and treatment.Lancet Neurol 2009;8(8):731Y740.
16. Koskiniemi M, Rantalaiho T, Piiparinen H,et al. Infections of the central nervoussystem of suspected viral origin:a collaborative study from Finland.J Neurovirol 2001;7(5):400Y408.
17. Mailles A, Stahl JP. Infectious encephalitisin France in 2007: a national prospectivestudy. Clin Infect Dis 2009;49(12):1838Y1847.
18. Granerod J, Ambrose HE, Davies NW, et al.Causes of encephalitis and differences intheir clinical presentations in England: amulticentre, population-based prospectivestudy. Lancet Infect Dis 2010;10(12):835Y844.
19. Conley ME, Howard VC, Scharenberg AM,et al. Neurological disease produced byvaricella zoster virus reactivation withoutrash. Curr Top Microbiol Immunol2010;342:243Y253.
20. Greenlee JE, Carroll KC. Cerebrospinal fluidin central nervous system infections. In:Scheld WM, Whitley RJ, Marra CM, editors.Infections of the central nervous system. 3rded. Philadelphia, PA: Lippincott Williams &Wilkins, 2004:6Y30.
21. Petersen LR, Marfin AA. West Nile virus: aprimer for the clinician. Ann Intern Med2002;137(3):173Y179.
22. Solomon T, Whitley RJ. Arthropod-borneviral encephalitides. In: Scheld WM,Whitley RJ, Marra CM, eds. Infectionsof the central nervous system. Philadelphia,PA: Lippincott Williams & Wilkins,2004:205Y230.
23. Sejvar JJ, Haddad MB, Tierney BC, et al.Neurologic manifestations and outcomeof West Nile virus infection. JAMA 2003;290(4):511Y515.
24. Leis AA, Stokic DS, Polk JL, et al. Apoliomyelitis-like syndrome fromWest Nile virus infection. N Engl J Med2002;347(16):1279Y1280.
25. Tyler KL. West Nile virus infection in theUnited States. Arch Neurol 2004;61(8):1190Y1195.
26. Smith DW, Mackenzie JS, Weaver SC.Alphaviruses. In: Richman DD, Whitley RJ,Hayden FG, editors. Clinical virology.3rd ed. Washington, DC: ASM Press, 2009:1241Y1274.
27. Goldfield M, Welsh JN, Taylor BF. The 1959outbreak of Eastern encephalitis in NewJersey. 5. The inapparent infection:diseaseratio. Am J Epidemiol 1968;87(1):32Y33.
28. Deresiewicz RL, Thaler SJ, Hsu L,Zamani AA. Clinical and neuroradiographicmanifestations of eastern equineencephalitis. N Engl J Med 1997;336(26):1867Y1874.
29. Ooi MH, Wong SC, Lewthwaite P, et al.Clinical features, diagnosis, andmanagement of enterovirus 71. LancetNeurol 2010;9(11):1097Y1105.
30. Liow K, Spanaki MV, Boyer RS, et al.Bilateral hippocampal encephalitis causedby enteroviral infection. Pediatr Neurol1999;21(5):836Y838.
31. Jang S, Suh SI, Ha SM, et al. Enterovirus71Yrelated encephalomyelitis: usual andunusual magnetic resonance imagingfindings. Neuroradiology 2012;54(3):239Y245.
32. Desmond RA, Accortt NA, Talley L, et al.Enteroviral meningitis: natural historyand outcome of pleconaril therapy.Antimicrob Agents Chemother 2006;50(7):2409Y2414.
33. Steiner I, Budka H, Chaudhuri A, et al. Viralmeningoencephalitis: a review of diagnosticmethods and guidelines for management.Eur J Neurol 2010;17(8):999Ye57.
34. Kang SS, McGavern DB. Lymphocyticchoriomeningitis infection of the centralnervous system. Front Biosci 2008;13:4529Y4543.
35. Douvoyiannis M, Litman N, Goldman DL.Neurologic manifestations associated withparvovirus B19 infection. Clin Infect Dis2009;48(12):1713Y1723.
36. Rafailidis PI, Mourtzoukou EG, Varbobitis IC,Falagas ME. Severe cytomegalovirus infectionin apparently immunocompetent patients:a systematic review. Virol J 2008;5:47.
37. Ward KN, Andrews NJ, Verity CM, et al.Human herpesviruses-6 and -7 each causesignificant neurological morbidity in Britainand Ireland. Arch Dis Child 2005;90(6):619Y623.
38. Yao K, Honarmand S, Espinosa A, et al.Detection of human herpesvirus-6 incerebrospinal fluid of patients withencephalitis. Ann Neurol 2009;65(3):257Y267.
39. Hu WT, Willoughby RE Jr, Dhonau H,Mack KJ. Long-term follow-up aftertreatment of rabies by induction of coma.N Engl J Med 2007;357(9):945j946.
40. Willoughby RE Jr, Tieves KS, Hoffman GM,et al. Survival after treatment of rabieswith induction of coma. N Engl J Med2005;352(24):2508j2514.
41. Smith JS, Fishbein DB, Rupprecht CE, Clark K.Unexplained rabies in three immigrants in
1288 www.aan.com/continuum December 2012
Encephalitis
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

the United States: a virologic investigation.N Engl J Med 1991;324(4):205j211.
42. Jeong YM, Hwang HY, Kim HS. MRI ofneurosyphilis presenting as mesiotemporalabnormalities: a case report. Korean J Radiol2009;10(3):310Y312.
43. Cunha BA, Fatehpuria R, Eisenstein LE.Listeria monocytogenes encephalitismimicking herpes simplex virus encephalitis:the differential diagnostic importance ofcerebrospinal fluid lactic acid levels. HeartLung 2007;36(3):226Y231.
44. Greenlee JE, Hale DC. Rickettsia. In: Biller J,ed. The interface of neurology & internalmedicine. Philadelphia, PA: LippincottWilliams & Wilkins, 2008:583Y388.
45. Graus F, Saiz A, Dalmau J. Antibodies andneuronal autoimmune disorders of the CNS.J Neurol 2010;257(4):509Y517.
46. Gable MS, Sheriff H, Dalmau J, et al. Thefrequency of autoimmune N-methyl-D-aspartate receptor encephalitis surpassesthat of individual viral etiologies in youngindividuals enrolled in the CaliforniaEncephalitis Project. Clin Infect Dis 2012;54(7):899Y904.
47. Greenlee JE. Treatment of paraneoplasticneurologic disorders. Curr Treat OptionsNeurol 2010;12(3):212Y230.
48. Sonneville R, Klein I, de Broucker T, Wolff M.Post-infectious encephalitis in adults:diagnosis and management. J Infect2009;58(5):321Y328.
49. Young NP, Weinshenker BG, Lucchinetti CF.Acute disseminated encephalomyelitis:current understanding and controversies.Semin Neurol 2008;28(1):84Y94.
50. Wender M. Acute disseminatedencephalomyelitis (ADEM). J Neuroimmunol2011;231(1Y2):92Y99.
51. Leake JA, Albani S, Kao AS, et al. Acutedisseminated encephalomyelitis inchildhood: epidemiologic, clinical andlaboratory features. Pediatr Infect Dis J2004;23(8):756Y764.
52. Tenembaum S, Chamoles N, Fejerman N.Acute disseminated encephalomyelitis:a long-term follow-up study of 84pediatric patients. Neurology 2002;59(8):1224Y1231.
53. Tenembaum S, Chitnis T, Ness J, Hahn JS.Acute disseminated encephalomyelitis.Neurology 2007;68(16 suppl 2):S23YS36.
54. Schwarz S, Mohr A, Knauth M, et al. Acutedisseminated encephalomyelitis: a follow-upstudy of 40 adult patients. Neurology2001;56(10):1313Y1318.
55. de Seze J, Debouverie M, Zephir H, et al.Acute fulminant demyelinating disease: adescriptive study of 60 patients. Arch Neurol2007;64(10):1426Y1432.
56. Tunkel AR, Glaser CA, Bloch KC, et al. Themanagement of encephalitis: clinicalpractice guidelines by the Infectious DiseasesSociety of America. Clin Infect Dis 2008;47(3):303Y327.
57. Mader I, Wolff M, Nagele T, et al. MRI andproton MR spectroscopy in acutedisseminated encephalomyelitis. Childs NervSyst 2005;21(7):566Y572.
58. Adamo MA, Deshaies EM. Emergencydecompressive craniectomy for fulminatinginfectious encephalitis. J Neurosurg2008;108(1):174Y176.
1289Continuum Lifelong Learning Neurol 2012;18(6):1271–1289 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.