eaaci guideline on allergen immunotherapy - allergic asthma · eaaci guideline on allergen...
TRANSCRIPT
EAACI Guideline on Allergen Immunotherapy - allergic asthma V 4.0/04 June 2017 Short title: EAACI Guidelines on AIT for allergic asthma Key words: AGREE II, allergen immunotherapy, allergic diseases, atopy, asthma, asthma control, asthma exacerbations, lung function Abbreviations AD = atopic dermatitis AEs = adverse events AGREE = Appraisal of Guidelines, Research and Evaluation AHR = airways hyperreactivity AIT = allergen immunotherapy AR = allergic rhinitis ARIA = Allergic Rhinitis and its Impact on Asthma EAACI = European Academy of Allergy and Clinical Immunology GINA = Global Initiative for Asthma HCP = healthcare professional HDM = house dust mites ICS = inhaled corticosteroids QoL = quality of life RCT = randomised control trial SLIT = sublingual AIT SCIT = subcutaneous AIT SMS = symptom and medication score Abstract
Allergen immunotherapy (AIT) has been used to treat allergic disease for more then 100 years. Despite broad evidence of clinical efficacy AIT remains underused in allergic asthma. Achieving a wider consensus is of utmost importance as AIT is the only treatment that can change the course of allergic disease by inducing allergen-specific immune tolerance.
The European Academy of Allergy and Clinical Immunology has developed clinical practice guidelines that aim to provide evidence-based recommendations for the use of AIT for allergic asthma. These guidelines have been developed by a multi-disciplinary expert working group using the Appraisal of Guidelines, Research and Evaluation (AGREE) II framework. A systematic review of the current evidence has been used to generate evidence based clinical recommendations.
The key recommendation is that AIT delivered via subcutaneous or sublingual route is beneficial for mild and moderate allergic asthma, provided that asthma is adequately controlled by pharmacotherapy. AIT has a significant impact on asthma symptoms and medication, with a steroid sparing effect, improves disease specific and generic quality of life (QoL) and specific airways hyperreactivity (AHR). The influence on non-specific AHR and lung function is less prominent. No consistent effects on asthma control and exacerbations have been validated yet in clinical trials. AIT is a safe treatment for well-controlled allergic asthma in children and in adults.
AIT should be integrated in the general frame of asthma management aiming to reduce symptoms, improve QoL and minimize future risk by decreasing exacerbation rate, improving lung function (including AHR) and decreasing adverse reactions to medication (steroid and beta-2 agonists sparing effect). More effective
AIT strategies including novel preparations, adjuvants and alternate routes of administration are underway. I. Introduction
Asthma represents a major health problem, affecting 300 million people
around the globe, with increasing prevalence and an overall projected increase to 400 million within the next 30 years [1-5]. It is the main cause for hospitalization and paediatric emergency and causes significant burden by direct and indirect costs (72,2 billion Euro annual). The major economic impact is due to indirect costs (absenteeism and decreased productivity at the workplace) [6-9].
Asthma is a heterogeneous condition characterized by chronic airway inflammation. Recognisable clusters of visible properties (clinical, inflammatory, morphologic characteristics and unique responses to treatment) are described as asthma phenotypes. Phenotypes do not necessarily provide insight into the underlying pathogenetic mechanisms, which define the disease endotype [10-12]. Endotyping asthma enables its individualised management, including optimised AIT.
Allergic asthma has been extensively studied. It usually starts in childhood and is often accompanied or preceded by allergic rhinitis (AR), atopic dermatitis (AD) and/or food allergy [13]. The proportion of asthma that is allergic varies from 30 to 79% in children [14-16] and from 30 to 60% in adults [17, 18]. Children with severe preschool wheeze or severe asthma are usually allergic [19]. Although type 2-driven inflammation is key in allergic asthma the pathophysiology might be complex involving several endotypes [10, 20]. Assessing the role of atopy in asthma is an important step in asthma evaluation since these patients might benefit from AIT in addition to pharmacological asthma treatment (figure 1 and box 1).
Global Initiative for Asthma (GINA) 2017 guidelines recommend assessment of two domains: symptom control and future risk of adverse outcomes including exacerbations, poor lung function and/or fixed airflow limitation and medication side effects [21]. Achieving control is the major goal currently proposed in asthma management where pharmacological and non-pharmacological treatment is adjusted in a continuous cycle that involves assessment, treatment and review [21].
The rationale for AIT is the modification of the underlying atopic disease mechanisms triggering sustained clinical effect. Effective AIT induces multiple immune-mediated mechanisms, which are sequentially activated leading to allergen-specific tolerance, suppression of inflammation and multifaceted clinical improvement [22, 23]. AIT is currently provided in allergic asthma via the subcutaneous (SCIT) or sublingual (SLIT) route, with alternate routes being currently explored. A limited number of studies have been specifically designed to evaluate AIT in asthma. Most data come from indirect evidence from AIT trials that included patients with both AR and asthma. No consensus has been achieved on the best endpoints, with lung function or asthma exacerbations only occasionally being assessed as primary outcomes.
According to GINA 2017 the benefit of AIT in asthma in reducing symptoms and medication and AHR must be weighed against the risk of side effects, relative inconvenience and its cost incurred by prolonged course of treatment (level D evidence) [21]. GINA 2017 reports SLIT as a possible add-on option for adults with asthma and AR sensitised to house dust mites (HDM) with exacerbations despite low to high doses of inhaled corticosteroids (ICS) provided that their FEV1 is >70% predicted [21]. The current Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines [24] give both SCIT and SLIT a conditional recommendation in allergic asthma due to moderate or low quality of evidence. AIT should be integrated in the general frame of asthma management.
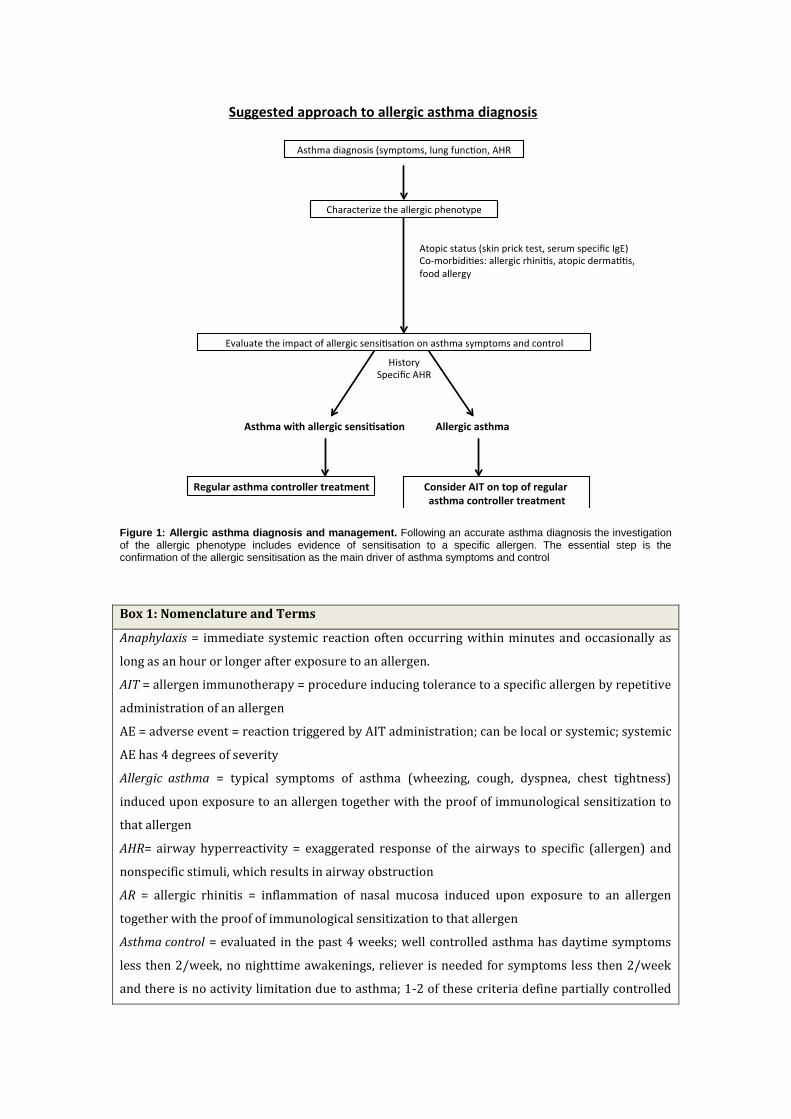
Figure 1: Allergic asthma diagnosis and management. Following an accurate asthma diagnosis the investigation of the allergic phenotype includes evidence of sensitisation to a specific allergen. The essential step is the confirmation of the allergic sensitisation as the main driver of asthma symptoms and control
Box 1: Nomenclature and Terms
Anaphylaxis = immediate systemic reaction often occurring within minutes and occasionally as
long as an hour or longer after exposure to an allergen.
AIT = allergen immunotherapy = procedure inducing tolerance to a specific allergen by repetitive
administration of an allergen
AE = adverse event = reaction triggered by AIT administration; can be local or systemic; systemic
AE has 4 degrees of severity
Allergic asthma = typical symptoms of asthma (wheezing, cough, dyspnea, chest tightness)
induced upon exposure to an allergen together with the proof of immunological sensitization to
that allergen
AHR= airway hyperreactivity = exaggerated response of the airways to specific (allergen) and
nonspecific stimuli, which results in airway obstruction
AR = allergic rhinitis = inflammation of nasal mucosa induced upon exposure to an allergen
together with the proof of immunological sensitization to that allergen
Asthma control = evaluated in the past 4 weeks; well controlled asthma has daytime symptoms
less then 2/week, no nighttime awakenings, reliever is needed for symptoms less then 2/week
and there is no activity limitation due to asthma; 1-2 of these criteria define partially controlled
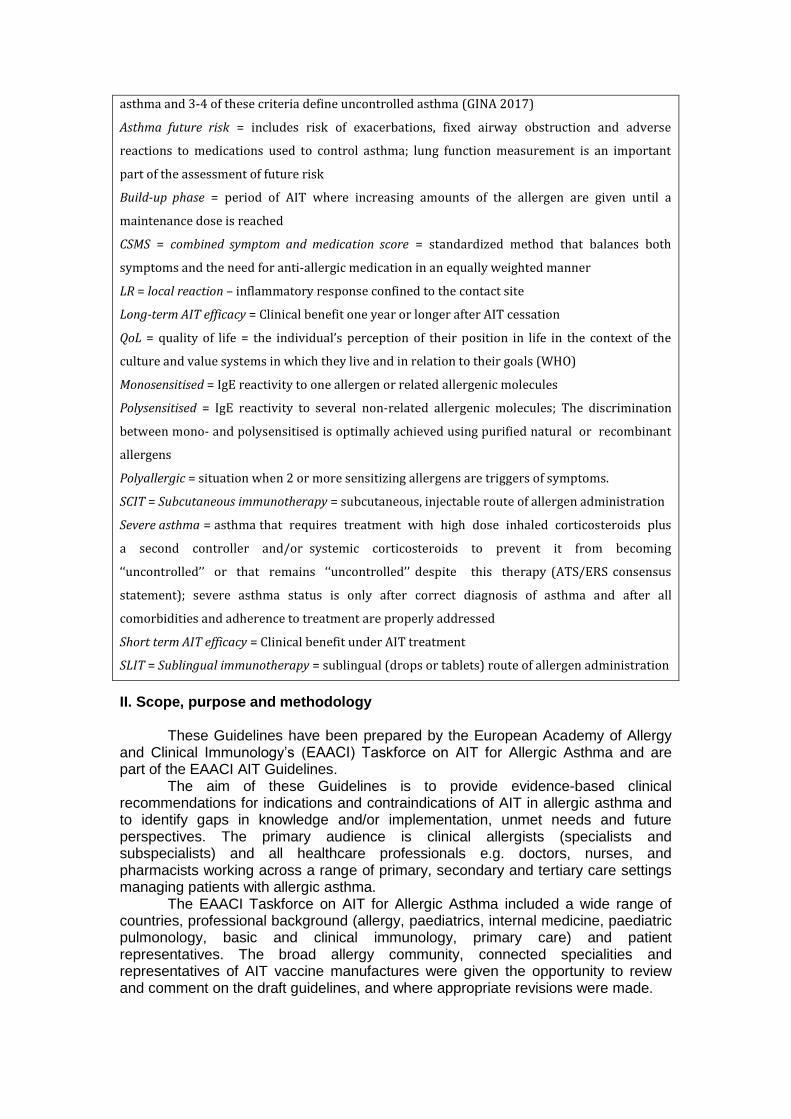
asthma and 3-4 of these criteria define uncontrolled asthma (GINA 2017)
Asthma future risk = includes risk of exacerbations, fixed airway obstruction and adverse
reactions to medications used to control asthma; lung function measurement is an important
part of the assessment of future risk
Build-up phase = period of AIT where increasing amounts of the allergen are given until a
maintenance dose is reached
CSMS = combined symptom and medication score = standardized method that balances both
symptoms and the need for anti-allergic medication in an equally weighted manner
LR = local reaction – inflammatory response confined to the contact site
Long-term AIT efficacy = Clinical benefit one year or longer after AIT cessation
QoL = quality of life = the individual’s perception of their position in life in the context of the
culture and value systems in which they live and in relation to their goals (WHO)
Monosensitised = IgE reactivity to one allergen or related allergenic molecules
Polysensitised = IgE reactivity to several non-related allergenic molecules; The discrimination
between mono- and polysensitised is optimally achieved using purified natural or recombinant
allergens
Polyallergic = situation when 2 or more sensitizing allergens are triggers of symptoms.
SCIT = Subcutaneous immunotherapy = subcutaneous, injectable route of allergen administration
Severe asthma = asthma that requires treatment with high dose inhaled corticosteroids plus
a second controller and/or systemic corticosteroids to prevent it from becoming
‘‘uncontrolled’’ or that remains ‘‘uncontrolled’’ despite this therapy (ATS/ERS consensus
statement); severe asthma status is only after correct diagnosis of asthma and after all
comorbidities and adherence to treatment are properly addressed
Short term AIT efficacy = Clinical benefit under AIT treatment
SLIT = Sublingual immunotherapy = sublingual (drops or tablets) route of allergen administration
II. Scope, purpose and methodology
These Guidelines have been prepared by the European Academy of Allergy and Clinical Immunology’s (EAACI) Taskforce on AIT for Allergic Asthma and are part of the EAACI AIT Guidelines.
The aim of these Guidelines is to provide evidence-based clinical recommendations for indications and contraindications of AIT in allergic asthma and to identify gaps in knowledge and/or implementation, unmet needs and future perspectives. The primary audience is clinical allergists (specialists and subspecialists) and all healthcare professionals e.g. doctors, nurses, and pharmacists working across a range of primary, secondary and tertiary care settings managing patients with allergic asthma.
The EAACI Taskforce on AIT for Allergic Asthma included a wide range of countries, professional background (allergy, paediatrics, internal medicine, paediatric pulmonology, basic and clinical immunology, primary care) and patient representatives. The broad allergy community, connected specialities and representatives of AIT vaccine manufactures were given the opportunity to review and comment on the draft guidelines, and where appropriate revisions were made.
These guidelines have been developed using the Appraisal of Guidelines,
Research and Evaluation (AGREE) II framework, a structured approach to guidelines for public health [25]. Agreement was reached on the search strategy, key questions formulating recommendations and the peer review process. A systematic review of the current evidence conducted by the methodologist [26], complemented by the results of other systematic reviews and by a narrative review for evidence not covered by the systematic review, have been used to generate evidence based clinical recommendations formulated by clinical academics. The key overarching question: “What is the effectiveness, safety and cost-effectiveness of AIT for allergic asthma in all populations?” was pursued through the formal review of the evidence [27]. The primary outcomes considered were effectiveness assessed by symptom score, medication score and symptom and medication score, both during treatment (short-term) and post discontinuation (i.e. at least one year after stop of treatment). Secondary outcomes were asthma control and exacerbations, QoL, lung function (including AHR), safety and health economic analysis from the perspective of the health system/payer (table S1).
We graded the strength and consistency of key findings from the critical appraisal of the evidence published so far to formulate evidence-based recommendations for clinical care using an approach that was adapted from that proposed by the Oxford Centre for Evidence-Based Medicine (Oxford Centre for Evidence-based Medicine) (Box 2). In brief the terms “strong, moderate and weak” were used for recommendations.
Appropriate representation all stakeholders, peer review by invited experts from a full range of organizations, countries, and professional backgrounds and editorial independence were insured. Identifying gaps, barriers and facilitators were an important part of the process. All stakeholders had an opportunity to comment on the draft guidelines publicised on the EAACI Website for a 3-week period to allow any omissions or errors in the evidence-base to be highlighted.
The development of AIT for Allergic Asthma was funded and supported by EAACI. The funder did not have any influence on the guideline production process, on its contents or on the decision to publish.
The review of these guidelines is planned for 2020, as new evidence will probably emerge during the next 2-3 years. Box 2: Assigning levels of evidence and grade and strength recommendations
Level of evidence
Level I = systematic reviews, meta-analysis, randomised controlled trials
Level II = two-groups, non-randomised studies (eg cohort, case-control studies)
Level III = one group, non-randomised (eg before and after, pre test and post test)
Level IV = descriptive studies that include analysis of outcomes (single-subject design, case-
series)
Level V = case-reports and expert opinion that include narrative literature, reviews and
consensus statements
Grades of recommendation
Grade A = consistent level I studies
Grade B = consistent level II or III studies or extrapolations from level I studies
Grade C = level IV studies or extrapolations from levels II or III studies
Grade D = level V evidence or troublingly inconsistent or inconsistent studies of any level
Strength of recommendation
Strong = Evidence from studies at low risk of bias, i.e. high quality
Moderate = Evidence from studies at moderate risk of bias, i.e. moderate quality
Weak = Evidence from studies at high risk of bias, i.e. low quality
Terminology
Recommendations are phrased according to the strength of recommendation: strong: “is
recommended”; moderate: “can be recommended”; weak: “may be recommended in specific
circumstances” and negative: “cannot be recommended”
III. Current evidence for AIT effectiveness and safety in allergic asthma
The clinical outcome of AIT in allergic asthma can be assessed by a decrease in the severity of symptoms and in the need for concomitant medication. As a result of reciprocal interactions, symptoms and medication should not be analyzed separately and a combined symptom and medication score (SMS) is recommended for AIT trials [28]. SMS has been mostly validated in rhinitis AIT studies [28,29]. Several systematic reviews show a strong effect of SCIT on decreasing asthma symptoms and medications during AIT treatment, both in children and in adults. The evidence for SLIT is less prominent (tables S2 and S3 – supplement). A potential steroid-sparing effect of AIT is of utmost importance to reduce potential side effects of ICS in asthma, in line with the general accepted aim to reduce future risk of treatment related adverse events. No SCIT or SLIT studies reported on the effect of AIT on symptoms or medication after AIT discontinuation. In the EAACI systematic review data pooled from 2 trials showed no evidence of reduction in short-term of SMS [26]. Lin et al. brought moderately strong body of evidence that SLIT improved SMS (20 of 41 studies) [30].
The moderate-to-low quality RCTs provided mixed evidence that SLIT is effective in improving asthma control in patients with allergic asthma. One study at low risk of bias found that SLIT did not improve asthma control [31]. In subjects with controlled mild to moderate HDM allergic asthma one-year SLIT treatment allowed reduction in daily ICS dose from individual baseline dose without deterioration in the asthma control [32]. The EAACI systematic review found no evidence to assess whether SCIT is effective in improving asthma control [26].
Several trials report on asthma exacerbations under AIT. The Wang SCIT trial at low risk of bias failed to demonstrate evidence of a reduction in exacerbations in AIT-treated subjects compared with placebo [33]. Two SLIT trials reported a positive effect of AIT on asthma exacerbations, one in the context of reducing the dose of ICS [31,32]. Another SLIT trial failed to demonstrate evidence for SLIT in reducing asthma exacerbations [34].
Lu et al. found no significant differences in lung function (PEF, FEV1 and FVC) between subjects receiving SCIT and the control group [35] . Twenty studies included in SR of Abramson which included the measurement of lung function showed only a trend towards improvement, without statistical significance [36]. EAACI meta-analysis evaluated 25 studies reporting on lung function and showed a favourable response in the overall evaluation and a large beneficial effect on small airways [26]. There are limited numbers of AIT studies using allergen specific bronchial provocation test as primary or secondary endpoint. The marked reduction in allergen-specific AHR to HDM, pollen and animal dander allergens reported by Abramson can be considered as potentially lowering the risk of allergic asthma exacerbations on exposure to the relevant allergen [36]. In the EAACI meta-analysis pooled data from three SCIT studies demonstrated a large effect of AIT [26]. There is
also evidence from several high quality randomised control trials that SCIT is effective in reducing specific AHR [37-44]. Limited, however significant reduction in non-specific AHR are reported both by the Abramson and the EAACI systematic reviews. [26, 36]
The EAACI systematic review showed a large treatment effect for SCIT for improving QoL in allergic asthma [26]. For SLIT the EAACI systematic review was unable to pool data. One SLIT trial at low risk of bias showed no significant improvement in disease-specific QoL [31].
Recent pharmacoeconomic studies demonstrate that AIT in asthma gives value for money, however heterogeneity in methodology limits the data interpretation, and it is difficult to extrapolate the results from one healthcare setting to another [45-49]. More data on cost-effectiveness of AIT in allergic asthma are presented in the supplementary material.
The EAACI systematic review indicated that AIT was associated with a minor increase in the risk of adverse events (AEs), these being seen both with SCIT and SLIT. While severe systemic AEs can occur, these appeared to be uncommon and mainly associated with SCIT. The limited safety data available included in the EAACI SR suggests that local AEs are more common with SLIT, while Kim et al reported that local reactions were frequent with both SCIT and SLIT [26,50]. Real-life data on AIT safety have accumulated both in Europe and US. The survey performed by the American Academy of Allergy, Asthma, and Immunology and American College of Asthma, Allergy, and Immunology from 2008 to 2013 collected data from 28.9 million injection visits and off-label SLIT. Four fatalities occurred under SCIT, systemic AEs were reported in 1.9% patients receiving SCIT and 1.4% of patients receiving off-label SLIT [51]. The European Survey on Adverse Systemic Reactions in Allergen Immunotherapy (EASSI) followed 4316 patients and reported a rate of 2.1% for systemic AE (89% with SCIT, 11% with SLIT) [52]. EASSI also recently evaluated prospectively 1563 children (61.5% with asthma) and reported a rate of 1.53% for systemic AEs [53]. Safety of initiation and continuation of AIT during pregnancy analysed in 4 studies totalling 422 women demonstrated no increased incidence of prematurity, hypertension/proteinuria, congenital malformations or perinatal deaths for women continued or initiated on SCIT or SLIT during pregnancy. Among the 10 out of 453 pregnancies who experienced systemic AEs while receiving AIT, none were found to have fetal complications [54]. IV. Clinical recommendations for AIT in allergic asthma General considerations
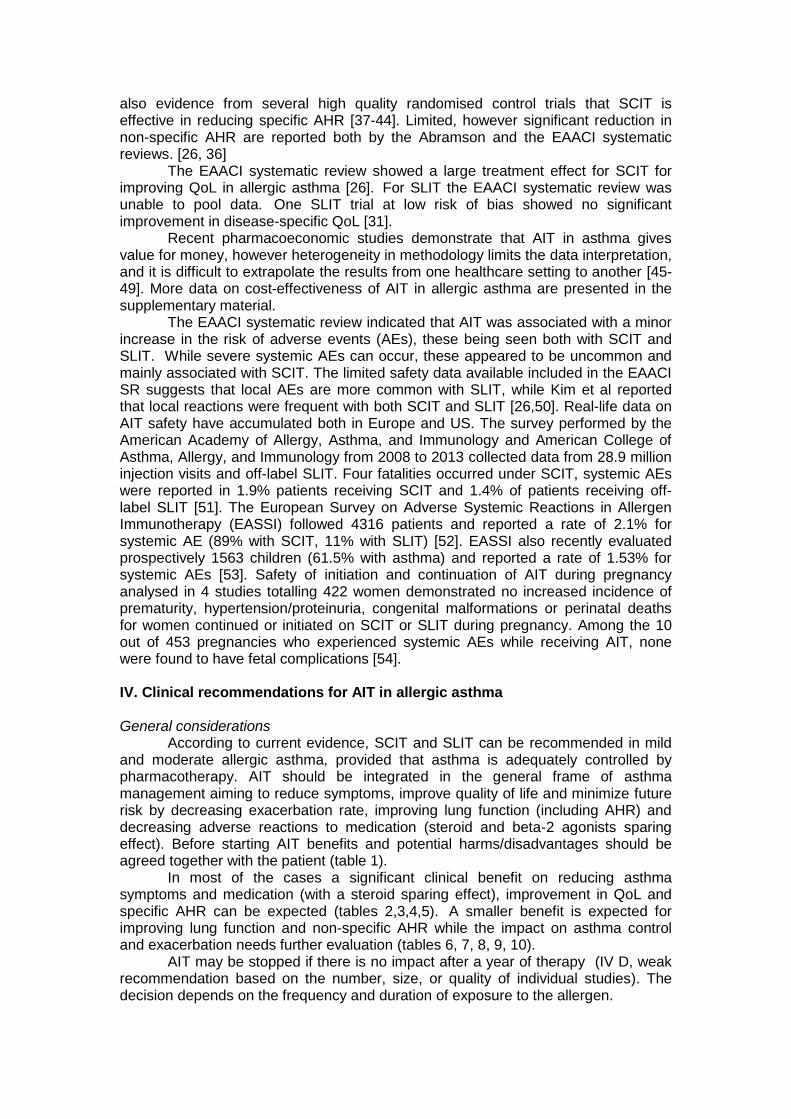
According to current evidence, SCIT and SLIT can be recommended in mild and moderate allergic asthma, provided that asthma is adequately controlled by pharmacotherapy. AIT should be integrated in the general frame of asthma management aiming to reduce symptoms, improve quality of life and minimize future risk by decreasing exacerbation rate, improving lung function (including AHR) and decreasing adverse reactions to medication (steroid and beta-2 agonists sparing effect). Before starting AIT benefits and potential harms/disadvantages should be agreed together with the patient (table 1).
In most of the cases a significant clinical benefit on reducing asthma symptoms and medication (with a steroid sparing effect), improvement in QoL and specific AHR can be expected (tables 2,3,4,5). A smaller benefit is expected for improving lung function and non-specific AHR while the impact on asthma control and exacerbation needs further evaluation (tables 6, 7, 8, 9, 10).
AIT may be stopped if there is no impact after a year of therapy (IV D, weak recommendation based on the number, size, or quality of individual studies). The decision depends on the frequency and duration of exposure to the allergen.
Table 1 - Benefits and potential harms/disadvantages of AIT in allergic asthma
Population Benefits Potential harms/disadvantages
Children with mild/moderate asthma
Decreased symptoms and medication score with a steroid sparing effect Improvement in QoL Improvement of specific AHR Possible effect on small airways and non-specific AHR Possible effect on asthma exacerbations and control
Daily intake of tablets/drops (SLIT/oral) or regular injections (SCIT) for 3 years Frequency of visits in the clinic (SCIT) Risk for adverse events Costs
Adults with mild/moderate asthma Decreased symptoms and medication score with a steroid sparing effect Improvement in QoL Improvement of specific AHR Possible effect on small airways and non-specific AHR Possible effect on asthma exacerbations and control
Daily intake of tablets/drops (SLIT/oral) or regular injections (SCIT) for 3 years Frequency of visits in the clinic (SCIT) Risk for adverse events Costs
Asthma and rhinitis Simultaneous tolerance induction for the one airways disease
Daily intake of tablets/drops (SLIT/oral) or regular injections (SCIT) for 3 years Frequency of visits in the clinic (SCIT) Risk for adverse events Costs
Asthma and atopic dermatitis Possible beneficial effect for adults sensitised to HDM
Daily intake of tablets/drops (SLIT/oral) or regular injections (SCIT) for 3 years Frequency of visits in the clinic (SCIT) Risk for adverse events Costs
Clinical recommendation for AIT to reduce symptoms and medication in allergic asthma
AIT significantly reduces asthma symptoms and medication during treatment, with more evidence available for SCIT compared to SLIT and differences between individual allergens (tables 2,3). There are not enough data to formulate recommendations for AIT in reducing asthma symptom or medication long term (after treatment cessation) or for the combined symptom and medication score.
Table 2: Recommendations for AIT in allergic asthma to reduce asthma symptoms during treatment
Recommendation Evidence level
Grade Strength of recommendation
Other considerations Key References
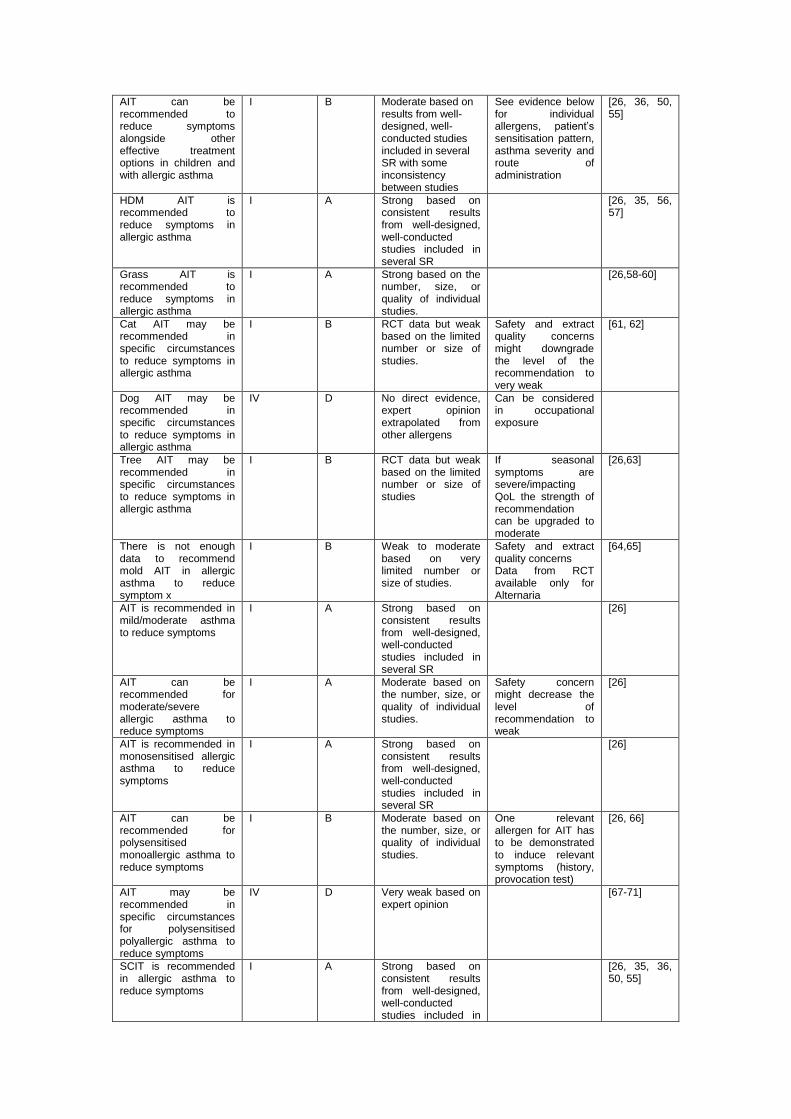
AIT can be recommended to reduce symptoms alongside other effective treatment options in children and with allergic asthma
I B Moderate based on results from well-designed, well-conducted studies included in several SR with some inconsistency between studies
See evidence below for individual allergens, patient’s sensitisation pattern, asthma severity and route of administration
[26, 36, 50, 55]
HDM AIT is recommended to reduce symptoms in allergic asthma
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26, 35, 56, 57]
Grass AIT is recommended to reduce symptoms in allergic asthma
I A Strong based on the number, size, or quality of individual studies.
[26,58-60]
Cat AIT may be recommended in specific circumstances to reduce symptoms in allergic asthma
I B RCT data but weak based on the limited number or size of studies.
Safety and extract quality concerns might downgrade the level of the recommendation to very weak
[61, 62]
Dog AIT may be recommended in specific circumstances to reduce symptoms in allergic asthma
IV D No direct evidence, expert opinion extrapolated from other allergens
Can be considered in occupational exposure
Tree AIT may be recommended in specific circumstances to reduce symptoms in allergic asthma
I B RCT data but weak based on the limited number or size of studies
If seasonal symptoms are severe/impacting QoL the strength of recommendation can be upgraded to moderate
[26,63]
There is not enough data to recommend mold AIT in allergic asthma to reduce symptom x
I B Weak to moderate based on very limited number or size of studies.
Safety and extract quality concerns Data from RCT available only for Alternaria
[64,65]
AIT is recommended in mild/moderate asthma to reduce symptoms
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26]
AIT can be recommended for moderate/severe allergic asthma to reduce symptoms
I A Moderate based on the number, size, or quality of individual studies.
Safety concern might decrease the level of recommendation to weak
[26]
AIT is recommended in monosensitised allergic asthma to reduce symptoms
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26]
AIT can be recommended for polysensitised monoallergic asthma to reduce symptoms
I B Moderate based on the number, size, or quality of individual studies.
One relevant allergen for AIT has to be demonstrated to induce relevant symptoms (history, provocation test)
[26, 66]
AIT may be recommended in specific circumstances for polysensitised polyallergic asthma to reduce symptoms
IV D Very weak based on expert opinion
[67-71]
SCIT is recommended in allergic asthma to reduce symptoms
I A Strong based on consistent results from well-designed, well-conducted studies included in
[26, 35, 36, 50, 55]
several SR
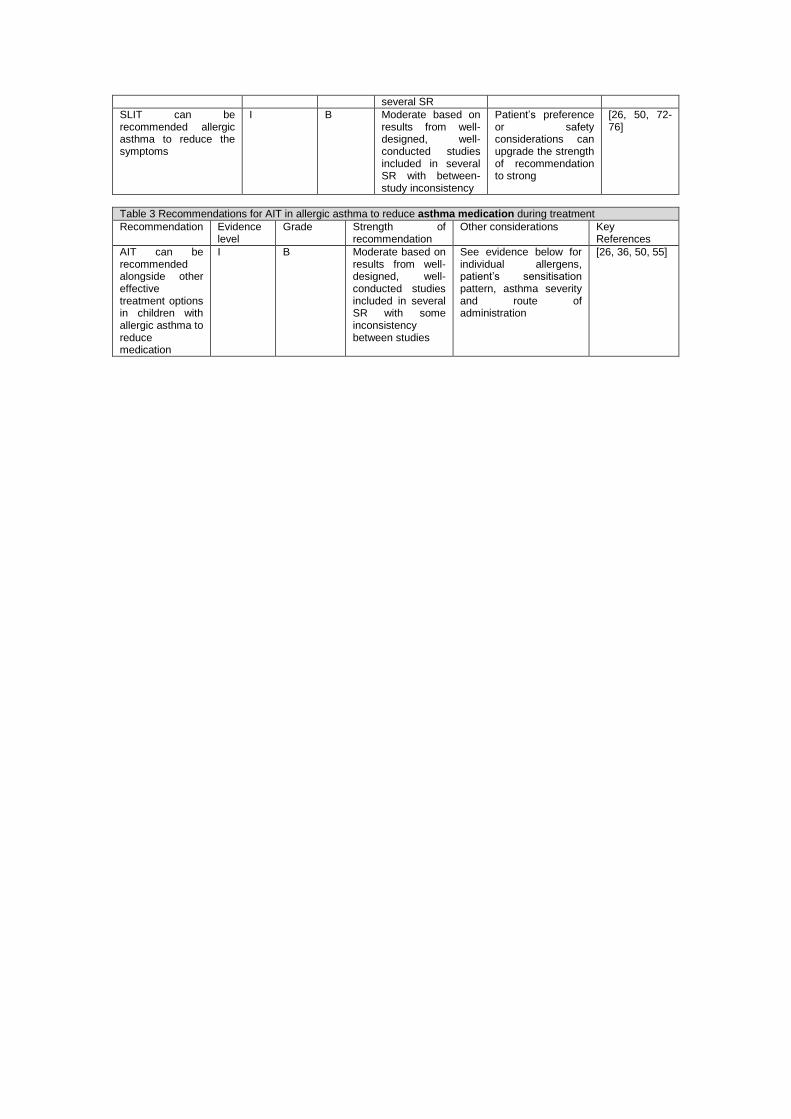
SLIT can be recommended allergic asthma to reduce the symptoms
I B Moderate based on results from well-designed, well-conducted studies included in several SR with between-study inconsistency
Patient’s preference or safety considerations can upgrade the strength of recommendation to strong
[26, 50, 72-76]
Table 3 Recommendations for AIT in allergic asthma to reduce asthma medication during treatment
Recommendation Evidence level
Grade Strength of recommendation
Other considerations Key References
AIT can be recommended alongside other effective treatment options in children with allergic asthma to reduce medication
I B Moderate based on results from well-designed, well-conducted studies included in several SR with some inconsistency between studies
See evidence below for individual allergens, patient’s sensitisation pattern, asthma severity and route of administration
[26, 36, 50, 55]
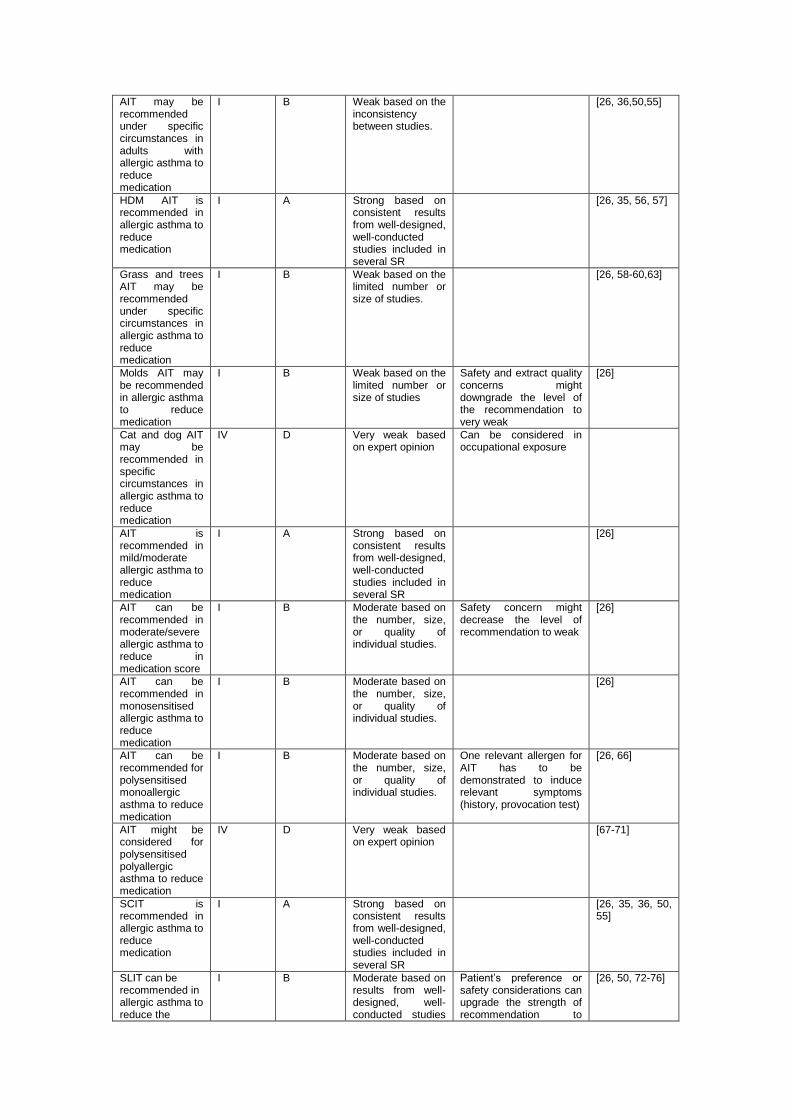
AIT may be recommended under specific circumstances in adults with allergic asthma to reduce medication
I B Weak based on the inconsistency between studies.
[26, 36,50,55]
HDM AIT is recommended in allergic asthma to reduce medication
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26, 35, 56, 57]
Grass and trees AIT may be recommended under specific circumstances in allergic asthma to reduce medication
I B Weak based on the limited number or size of studies.
[26, 58-60,63]
Molds AIT may be recommended in allergic asthma to reduce medication
I B Weak based on the limited number or size of studies
Safety and extract quality concerns might downgrade the level of the recommendation to very weak
[26]
Cat and dog AIT may be recommended in specific circumstances in allergic asthma to reduce medication
IV D Very weak based on expert opinion
Can be considered in occupational exposure
AIT is recommended in mild/moderate allergic asthma to reduce medication
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26]
AIT can be recommended in moderate/severe allergic asthma to reduce in medication score
I B Moderate based on the number, size, or quality of individual studies.
Safety concern might decrease the level of recommendation to weak
[26]
AIT can be recommended in monosensitised allergic asthma to reduce medication
I B Moderate based on the number, size, or quality of individual studies.
[26]
AIT can be recommended for polysensitised monoallergic asthma to reduce medication
I B Moderate based on the number, size, or quality of individual studies.
One relevant allergen for AIT has to be demonstrated to induce relevant symptoms (history, provocation test)
[26, 66]
AIT might be considered for polysensitised polyallergic asthma to reduce medication
IV D Very weak based on expert opinion
[67-71]
SCIT is recommended in allergic asthma to reduce medication
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26, 35, 36, 50, 55]
SLIT can be recommended in allergic asthma to reduce the
I B Moderate based on results from well-designed, well-conducted studies
Patient’s preference or safety considerations can upgrade the strength of recommendation to
[26, 50, 72-76]
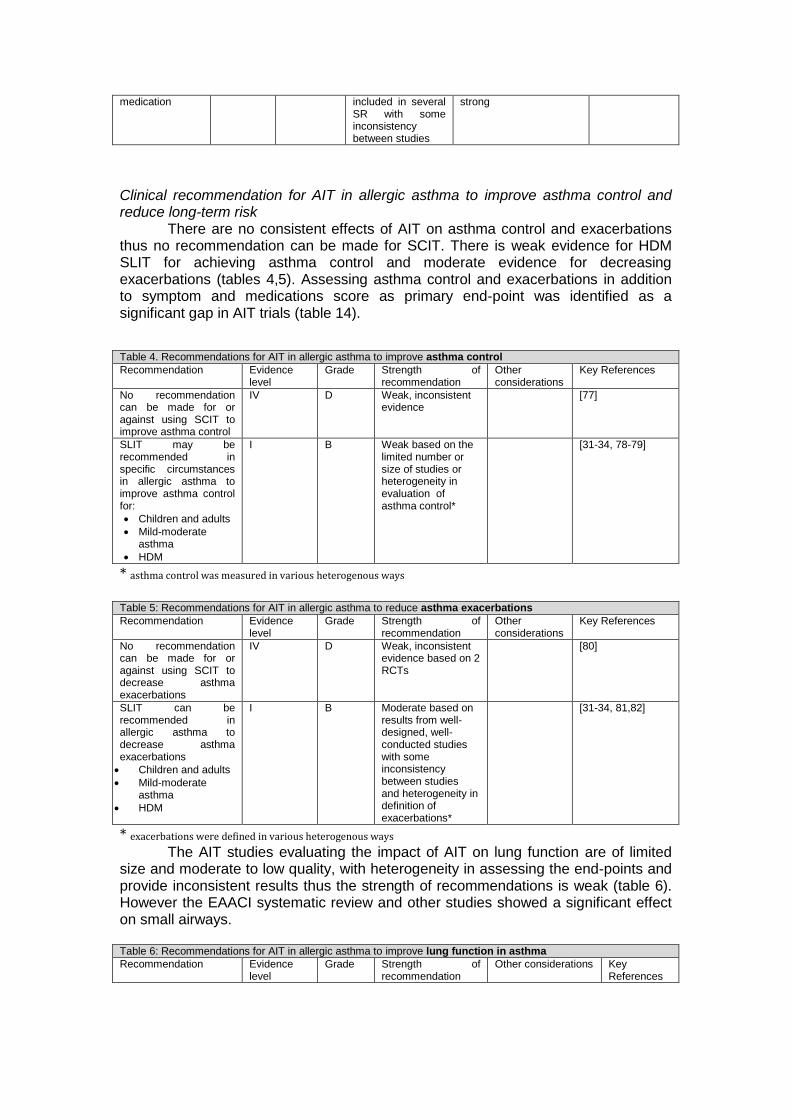
medication included in several SR with some inconsistency between studies
strong
Clinical recommendation for AIT in allergic asthma to improve asthma control and reduce long-term risk
There are no consistent effects of AIT on asthma control and exacerbations thus no recommendation can be made for SCIT. There is weak evidence for HDM SLIT for achieving asthma control and moderate evidence for decreasing exacerbations (tables 4,5). Assessing asthma control and exacerbations in addition to symptom and medications score as primary end-point was identified as a significant gap in AIT trials (table 14).
Table 4. Recommendations for AIT in allergic asthma to improve asthma control
Recommendation Evidence level
Grade Strength of recommendation
Other considerations
Key References
No recommendation can be made for or against using SCIT to improve asthma control
IV D Weak, inconsistent evidence
[77]
SLIT may be recommended in specific circumstances in allergic asthma to improve asthma control for:
Children and adults
Mild-moderate asthma
HDM
I B Weak based on the limited number or size of studies or heterogeneity in evaluation of asthma control*
[31-34, 78-79]
* asthma control was measured in various heterogenous ways Table 5: Recommendations for AIT in allergic asthma to reduce asthma exacerbations
Recommendation Evidence level
Grade Strength of recommendation
Other considerations
Key References
No recommendation can be made for or against using SCIT to decrease asthma exacerbations
IV D Weak, inconsistent evidence based on 2 RCTs
[80]
SLIT can be recommended in allergic asthma to decrease asthma exacerbations
Children and adults
Mild-moderate asthma
HDM
I B Moderate based on results from well-designed, well-conducted studies with some inconsistency between studies and heterogeneity in definition of exacerbations*
[31-34, 81,82]
* exacerbations were defined in various heterogenous ways The AIT studies evaluating the impact of AIT on lung function are of limited
size and moderate to low quality, with heterogeneity in assessing the end-points and provide inconsistent results thus the strength of recommendations is weak (table 6). However the EAACI systematic review and other studies showed a significant effect on small airways.
Table 6: Recommendations for AIT in allergic asthma to improve lung function in asthma
Recommendation Evidence level
Grade Strength of recommendation
Other considerations Key References
No recommendation can be made for or against using AIT to improve PEF or FEV 1in allergic asthma
I B Weak based inconsistent results with limited number and size and moderate/low quality of studies
[26]
SLIT may be recommended in special circumstances for allergic asthma to improve FEF 25-75 in:
Children
Mild-moderate asthma
HDM, grass and Parietaria pollen
I B Weak based on very limited number or size of studies
EAACI SR [26, 60, 83.84]
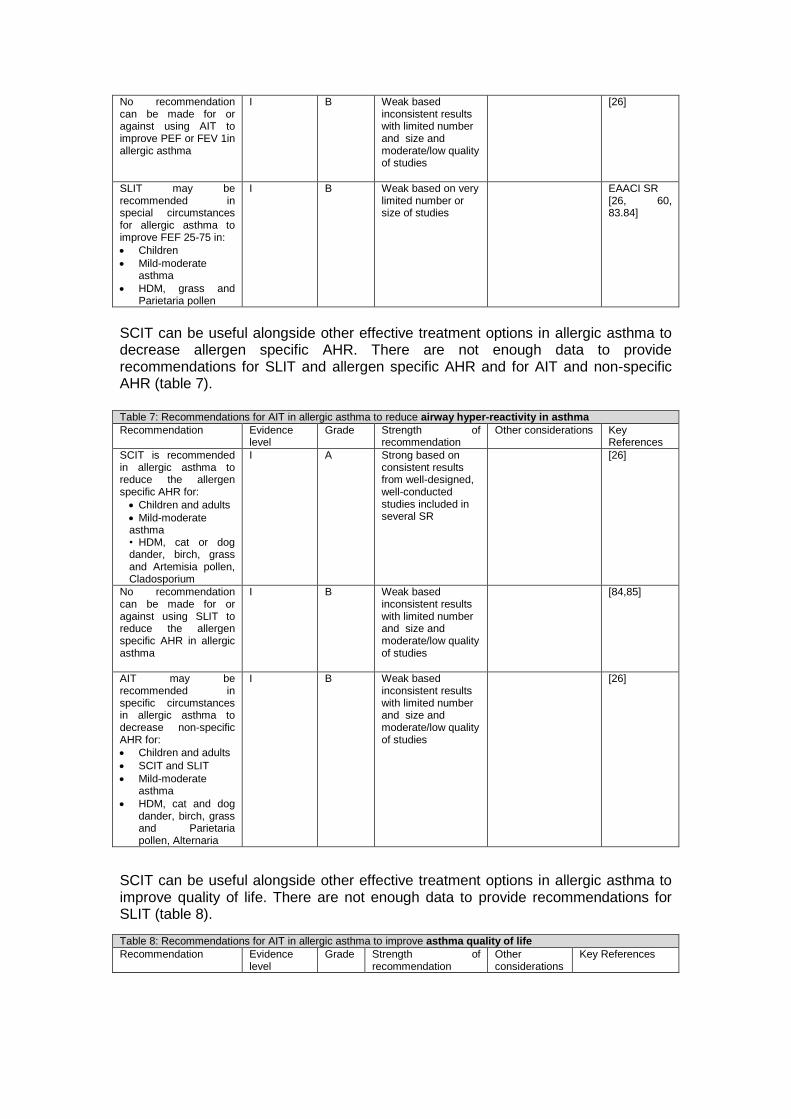
SCIT can be useful alongside other effective treatment options in allergic asthma to decrease allergen specific AHR. There are not enough data to provide recommendations for SLIT and allergen specific AHR and for AIT and non-specific AHR (table 7).
Table 7: Recommendations for AIT in allergic asthma to reduce airway hyper-reactivity in asthma
Recommendation Evidence level
Grade Strength of recommendation
Other considerations Key References
SCIT is recommended in allergic asthma to reduce the allergen specific AHR for:
Children and adults
Mild-moderate asthma • HDM, cat or dog dander, birch, grass and Artemisia pollen, Cladosporium
I A Strong based on consistent results from well-designed, well-conducted studies included in several SR
[26]
No recommendation can be made for or against using SLIT to reduce the allergen specific AHR in allergic asthma
I B Weak based inconsistent results with limited number and size and moderate/low quality of studies
[84,85]
AIT may be recommended in specific circumstances in allergic asthma to decrease non-specific AHR for:
Children and adults
SCIT and SLIT
Mild-moderate asthma
HDM, cat and dog dander, birch, grass and Parietaria pollen, Alternaria
I B Weak based inconsistent results with limited number and size and moderate/low quality of studies
[26]
SCIT can be useful alongside other effective treatment options in allergic asthma to improve quality of life. There are not enough data to provide recommendations for SLIT (table 8).
Table 8: Recommendations for AIT in allergic asthma to improve asthma quality of life
Recommendation Evidence level
Grade Strength of recommendation
Other considerations
Key References
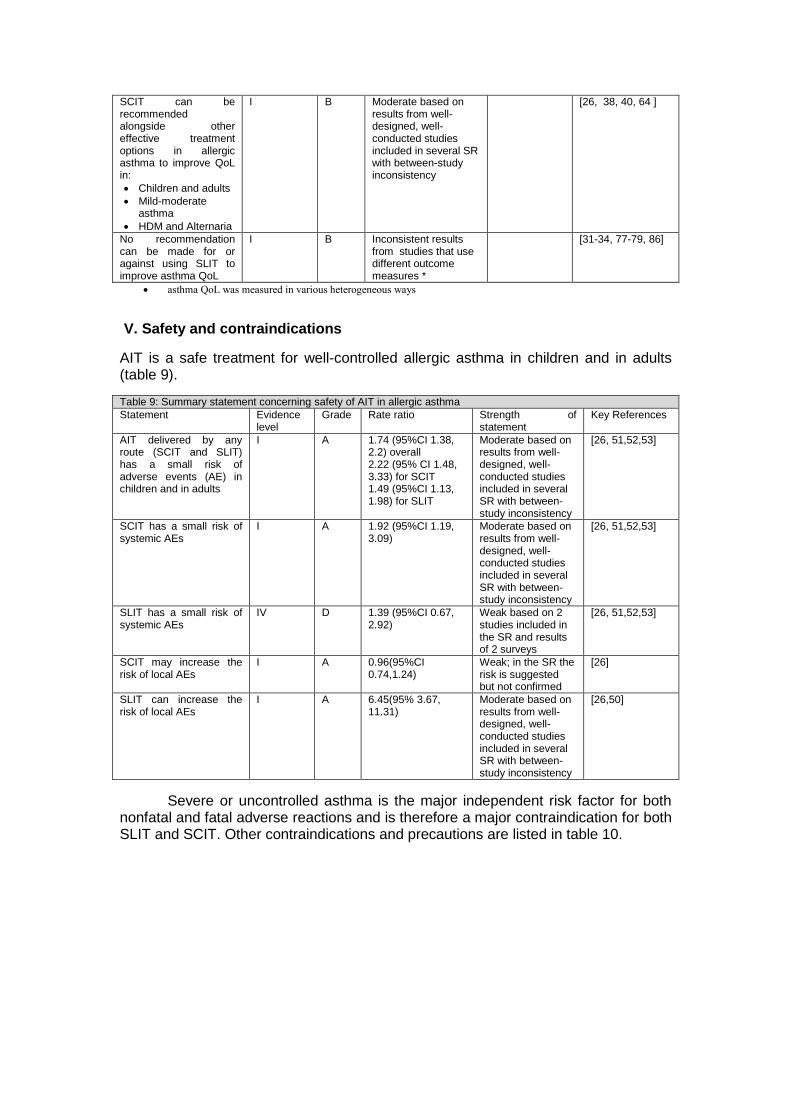
SCIT can be recommended alongside other effective treatment options in allergic asthma to improve QoL in:
Children and adults
Mild-moderate asthma
HDM and Alternaria
I B Moderate based on results from well-designed, well-conducted studies included in several SR with between-study inconsistency
[26, 38, 40, 64 ]
No recommendation can be made for or against using SLIT to improve asthma QoL
I B Inconsistent results from studies that use different outcome measures *
[31-34, 77-79, 86]
asthma QoL was measured in various heterogeneous ways
V. Safety and contraindications
AIT is a safe treatment for well-controlled allergic asthma in children and in adults (table 9).
Table 9: Summary statement concerning safety of AIT in allergic asthma
Statement Evidence level
Grade Rate ratio Strength of statement
Key References
AIT delivered by any route (SCIT and SLIT) has a small risk of adverse events (AE) in children and in adults
I A 1.74 (95%CI 1.38, 2.2) overall 2.22 (95% CI 1.48, 3.33) for SCIT 1.49 (95%CI 1.13, 1.98) for SLIT
Moderate based on results from well-designed, well-conducted studies included in several SR with between-study inconsistency
[26, 51,52,53]
SCIT has a small risk of systemic AEs
I A 1.92 (95%CI 1.19, 3.09)
Moderate based on results from well-designed, well-conducted studies included in several SR with between-study inconsistency
[26, 51,52,53]
SLIT has a small risk of systemic AEs
IV D 1.39 (95%CI 0.67, 2.92)
Weak based on 2 studies included in the SR and results of 2 surveys
[26, 51,52,53]
SCIT may increase the risk of local AEs
I A 0.96(95%CI 0.74,1.24)
Weak; in the SR the risk is suggested but not confirmed
[26]
SLIT can increase the risk of local AEs
I A 6.45(95% 3.67, 11.31)
Moderate based on results from well-designed, well-conducted studies included in several SR with between-study inconsistency
[26,50]
Severe or uncontrolled asthma is the major independent risk factor for both nonfatal and fatal adverse reactions and is therefore a major contraindication for both SLIT and SCIT. Other contraindications and precautions are listed in table 10.
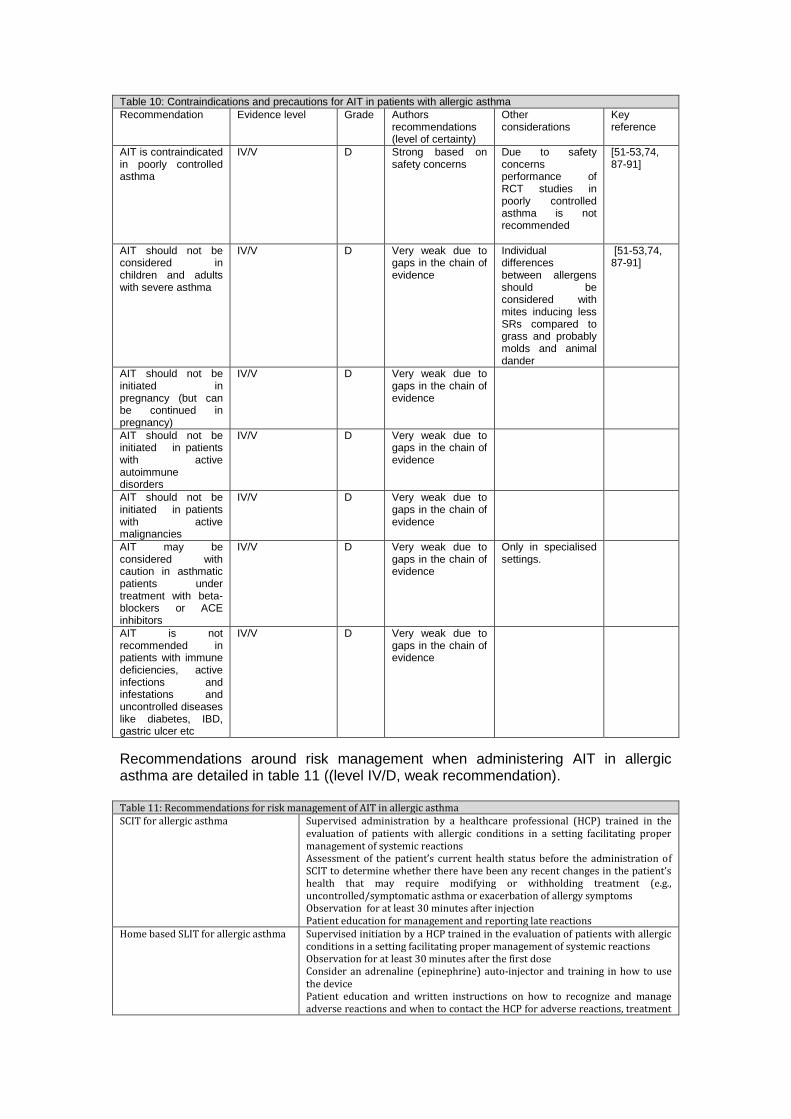
Table 10: Contraindications and precautions for AIT in patients with allergic asthma
Recommendation Evidence level Grade Authors recommendations (level of certainty)
Other considerations
Key reference
AIT is contraindicated in poorly controlled asthma
IV/V D Strong based on safety concerns
Due to safety concerns performance of RCT studies in poorly controlled asthma is not recommended
[51-53,74, 87-91]
AIT should not be considered in children and adults with severe asthma
IV/V D Very weak due to gaps in the chain of evidence
Individual differences between allergens should be considered with mites inducing less SRs compared to grass and probably molds and animal dander
[51-53,74, 87-91]
AIT should not be initiated in pregnancy (but can be continued in pregnancy)
IV/V D Very weak due to gaps in the chain of evidence
AIT should not be initiated in patients with active autoimmune disorders
IV/V D Very weak due to gaps in the chain of evidence
AIT should not be initiated in patients with active malignancies
IV/V D Very weak due to gaps in the chain of evidence
AIT may be considered with caution in asthmatic patients under treatment with beta-blockers or ACE inhibitors
IV/V D Very weak due to gaps in the chain of evidence
Only in specialised settings.
AIT is not recommended in patients with immune deficiencies, active infections and infestations and uncontrolled diseases like diabetes, IBD, gastric ulcer etc
IV/V D Very weak due to gaps in the chain of evidence
Recommendations around risk management when administering AIT in allergic asthma are detailed in table 11 ((level IV/D, weak recommendation). Table 11: Recommendations for risk management of AIT in allergic asthma SCIT for allergic asthma Supervised administration by a healthcare professional (HCP) trained in the
evaluation of patients with allergic conditions in a setting facilitating proper management of systemic reactions Assessment of the patient’s current health status before the administration of SCIT to determine whether there have been any recent changes in the patient’s health that may require modifying or withholding treatment (e.g., uncontrolled/symptomatic asthma or exacerbation of allergy symptoms Observation for at least 30 minutes after injection Patient education for management and reporting late reactions
Home based SLIT for allergic asthma Supervised initiation by a HCP trained in the evaluation of patients with allergic conditions in a setting facilitating proper management of systemic reactions Observation for at least 30 minutes after the first dose Consider an adrenaline (epinephrine) auto-injector and training in how to use the device Patient education and written instructions on how to recognize and manage adverse reactions and when to contact the HCP for adverse reactions, treatment
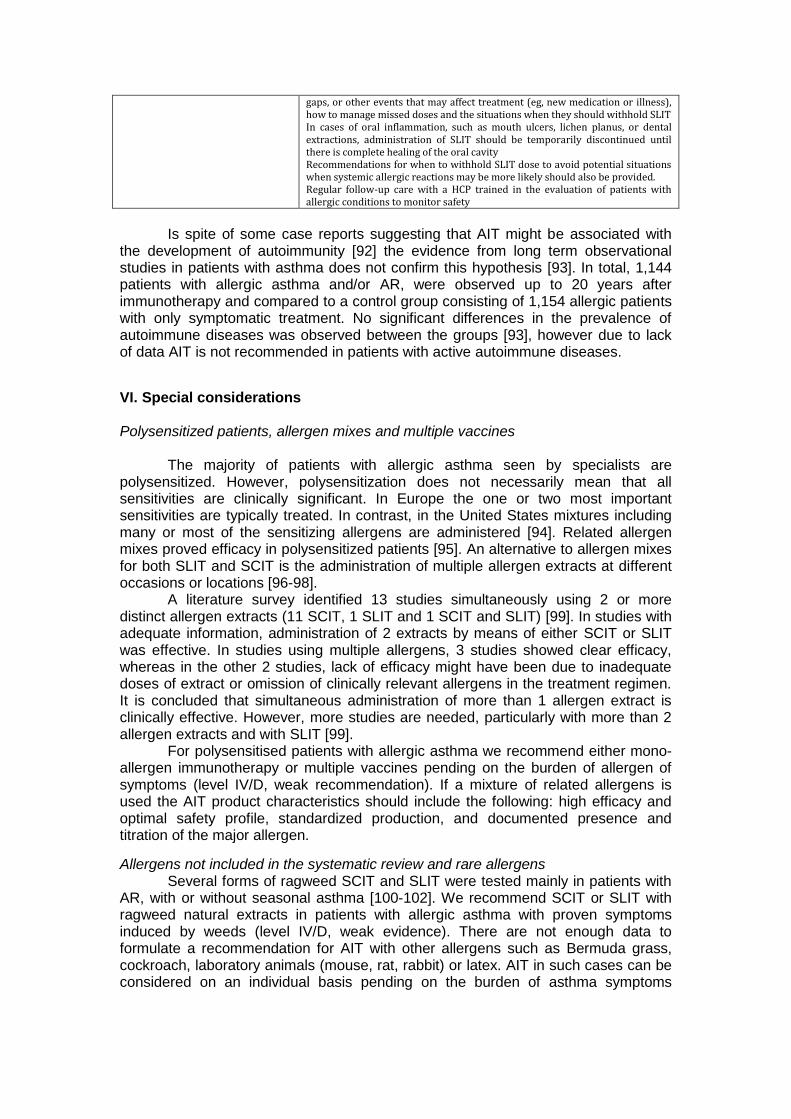
gaps, or other events that may affect treatment (eg, new medication or illness), how to manage missed doses and the situations when they should withhold SLIT In cases of oral inflammation, such as mouth ulcers, lichen planus, or dental extractions, administration of SLIT should be temporarily discontinued until there is complete healing of the oral cavity Recommendations for when to withhold SLIT dose to avoid potential situations when systemic allergic reactions may be more likely should also be provided. Regular follow-up care with a HCP trained in the evaluation of patients with allergic conditions to monitor safety
Is spite of some case reports suggesting that AIT might be associated with
the development of autoimmunity [92] the evidence from long term observational studies in patients with asthma does not confirm this hypothesis [93]. In total, 1,144 patients with allergic asthma and/or AR, were observed up to 20 years after immunotherapy and compared to a control group consisting of 1,154 allergic patients with only symptomatic treatment. No significant differences in the prevalence of autoimmune diseases was observed between the groups [93], however due to lack of data AIT is not recommended in patients with active autoimmune diseases.
VI. Special considerations Polysensitized patients, allergen mixes and multiple vaccines
The majority of patients with allergic asthma seen by specialists are polysensitized. However, polysensitization does not necessarily mean that all sensitivities are clinically significant. In Europe the one or two most important sensitivities are typically treated. In contrast, in the United States mixtures including many or most of the sensitizing allergens are administered [94]. Related allergen mixes proved efficacy in polysensitized patients [95]. An alternative to allergen mixes for both SLIT and SCIT is the administration of multiple allergen extracts at different occasions or locations [96-98].
A literature survey identified 13 studies simultaneously using 2 or more distinct allergen extracts (11 SCIT, 1 SLIT and 1 SCIT and SLIT) [99]. In studies with adequate information, administration of 2 extracts by means of either SCIT or SLIT was effective. In studies using multiple allergens, 3 studies showed clear efficacy, whereas in the other 2 studies, lack of efficacy might have been due to inadequate doses of extract or omission of clinically relevant allergens in the treatment regimen. It is concluded that simultaneous administration of more than 1 allergen extract is clinically effective. However, more studies are needed, particularly with more than 2 allergen extracts and with SLIT [99].
For polysensitised patients with allergic asthma we recommend either mono-allergen immunotherapy or multiple vaccines pending on the burden of allergen of symptoms (level IV/D, weak recommendation). If a mixture of related allergens is used the AIT product characteristics should include the following: high efficacy and optimal safety profile, standardized production, and documented presence and titration of the major allergen.
Allergens not included in the systematic review and rare allergens Several forms of ragweed SCIT and SLIT were tested mainly in patients with
AR, with or without seasonal asthma [100-102]. We recommend SCIT or SLIT with ragweed natural extracts in patients with allergic asthma with proven symptoms induced by weeds (level IV/D, weak evidence). There are not enough data to formulate a recommendation for AIT with other allergens such as Bermuda grass, cockroach, laboratory animals (mouse, rat, rabbit) or latex. AIT in such cases can be considered on an individual basis pending on the burden of asthma symptoms
induced exposure to the relevant allergens. For more details on these rare allergens see supplementary material.
Recombinant allergens for AIT in allergic asthma The use of recombinant allergens for immunotherapy is a very promising
approach. Murine models of allergic airway inflammation have provided important proof of concept findings. For example, using a murine model of birch pollen allergic asthma, both sublingual recombinant Bet v 1a or epicutaneous immunotherapy with a hypoallergenic recombinant Bet v 1B2 suppressed lung inflammatory responses such as eosinophil recruitment, type 2 cytokine levels and AHR[103,104].
While a number of studies have examined the use of recombinant birch pollen allergen in humans, none of these published studies have focused specifically on asthma patients, although typically 30-40% of the study populations being tested in these studies have asthma. Future studies on recombinant allergens need to specifically focus on sensitized asthma patients.
Based on the current evidence we cannot make recommendations on the use of recombinant allergens for allergic asthma Preseasonal versus continuous schedules
There is only one study directly comparing SLIT administered pre-coseasonal or continuous in a 2-year prospective, randomized, double-blind, placebo-controlled trial including children allergic to grass pollen with rhinitis and concomitant asthma. Both protocols were effective compared with placebo and showed similar decreases for combined SMS and all secondary endpoints (medication, ocular and asthma scores) [105].
Based on the current evidence we cannot make recommendations on the choice of preseasonal versus continuous schedules for AIT in allergic asthma. The use of either schedule depends on doctors and patients preference
Novel adjuvants and alternative routes for AIT in asthma The use of novel adjuvants and alternative routes of administration have
brought a lot of attention over the last years [106,107]. Although there are still few studies demonstrating the benefits of novel adjuvants or alternative routes of administration in large cohorts of patients in the context of asthma, promising alternatives have been reported in preclinical mouse models and humans [108-111] Novel adjuvants with demonstrated clinical efficacy and security in human clinical trials for AIT in asthma include Toll-like receptors (TLRs) agonists, viral-like particles (VPLs) and 1,25-dihydroxy vitamin D3 [108-111]. Further clinical trials should show whether these or other alternative routes could improve efficacy, safety and patient compliance for AIT in asthma.
Based on the current evidence we cannot make specific recommendations on adjuvant use or for alternative routes in AIT in allergic asthma.
Combination with biologics A few trials have been performed with pre-administration or co-administration
with omalizumab to either improve safety of SCIT up-dosing [112] or improve efficacy of SCIT [113,114]. 248 asthmatics not controlled by ICS received rush SCIT (cat, dog, HDM) combined with placebo or omalizumab. Adding omalizumab reduced the systemic AEs rate from 26.2% to 13.5% and 87.3% of subjects on omalizumab reached the maintenance dose of SCIT versus 72.1% of placebo patients [112].
Co-administration of omalizumab and SCIT with a depigmented grass pollen–rye pollen extract was investigated in 140 patients with seasonal AR and mild-to-moderate allergic asthma incompletely controlled by pharmacotherapy. Significant difference for AIT and omalizumab co-administration was noted for reducing symptom severity and improving asthma control and quality of life [113]. The combination had no prolonged effect during treatment with AIT only [114]. A slight
increase in FEV1 in patients formerly treated with the omalizumab/SIT combination therapy was shown in the second year of observation which should encourage further evaluation of long-term effects of omalizumab [114].
A recent trial in AR patients evaluated the induction of sustained tolerance to allergen when anti-IL-4 was combined with a suboptimal course of SCIT grass pollen using the allergen-induced skin late-phase response (LPR) and exploratory immune monitoring as surrogate markers of therapeutic response. Both treatment arms led to a substantial and sustained reduction of the LPR with no additional suppression with addition of anti-IL-4. However the combination anti-IL-4/SCIT compared with SCIT alone led to a sustained reduction in allergen-specific IL-4-producing cell counts [115].
Evidence is lacking to recommend co-administration of biologics and AIT for allergic asthma. Provocation tests for selecting patients with allergic asthma for AIT or efficacy assessment
Nonspecific bronchial provocation tests with metacholine/histamine and specific challenges that utilize allergen extracts assist in identifying AHR, a major feature of asthma. To validate AHR the most adequate provocation test is the bronchial challenge, although nasal and conjunctival allergen provocations are performed under some circumstances, especially at higher risk groups [116,117]. In AIT trials allergen provocation tests (cat, mites and grass pollen) are sometimes used as inclusion criteria or to measure the efficacy of AIT[118-121]. The drawback of provocation testing is that it may not reflect natural exposure [116].
We cannot make recommendations on the use of provocation tests for patient selection or efficacy assessment.
Biomarkers and AIT for allergic asthma Many studies on AIT report on potential biomarkers for measuring efficacy or
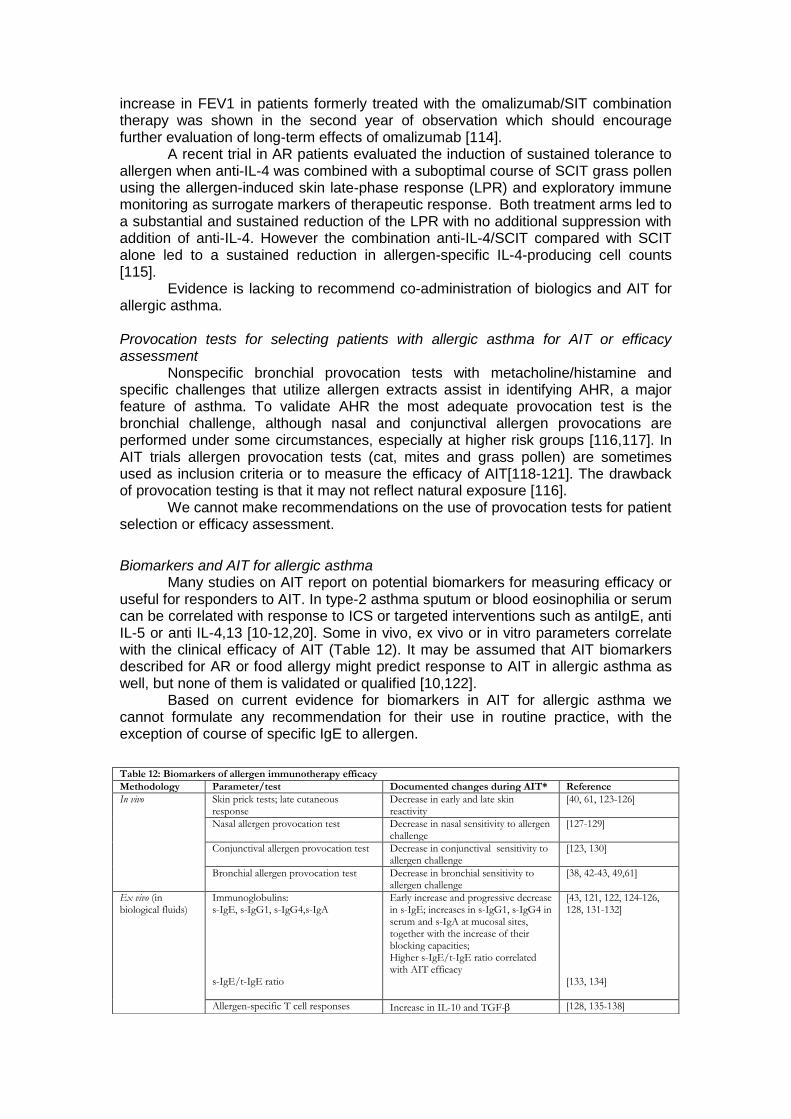
useful for responders to AIT. In type-2 asthma sputum or blood eosinophilia or serum can be correlated with response to ICS or targeted interventions such as antiIgE, anti IL-5 or anti IL-4,13 [10-12,20]. Some in vivo, ex vivo or in vitro parameters correlate with the clinical efficacy of AIT (Table 12). It may be assumed that AIT biomarkers described for AR or food allergy might predict response to AIT in allergic asthma as well, but none of them is validated or qualified [10,122].
Based on current evidence for biomarkers in AIT for allergic asthma we cannot formulate any recommendation for their use in routine practice, with the exception of course of specific IgE to allergen.
Table 12: Biomarkers of allergen immunotherapy efficacy
Methodology Parameter/test Documented changes during AIT* Reference
In vivo Skin prick tests; late cutaneous response
Decrease in early and late skin reactivity
[40, 61, 123-126]
Nasal allergen provocation test Decrease in nasal sensitivity to allergen challenge
[127-129]
Conjunctival allergen provocation test Decrease in conjunctival sensitivity to allergen challenge
[123, 130]
Bronchial allergen provocation test Decrease in bronchial sensitivity to allergen challenge
[38, 42-43, 49,61]
Ex vivo (in biological fluids)
Immunoglobulins: s-IgE, s-IgG1, s-IgG4,s-IgA s-IgE/t-IgE ratio
Early increase and progressive decrease in s-IgE; increases in s-IgG1, s-IgG4 in serum and s-IgA at mucosal sites, together with the increase of their blocking capacities; Higher s-IgE/t-IgE ratio correlated with AIT efficacy
[43, 121, 122, 124-126, 128, 131-132] [133, 134]
Allergen-specific T cell responses Increase in IL-10 and TGF- [128, 135-138]
*The presented changes were replicated in the majority but not all studies. s-IgE, s-IgG1, s-IgG4, s-IgA; specific IgE, IgG1, IgG4, IgA; t-IgE; total-IgE
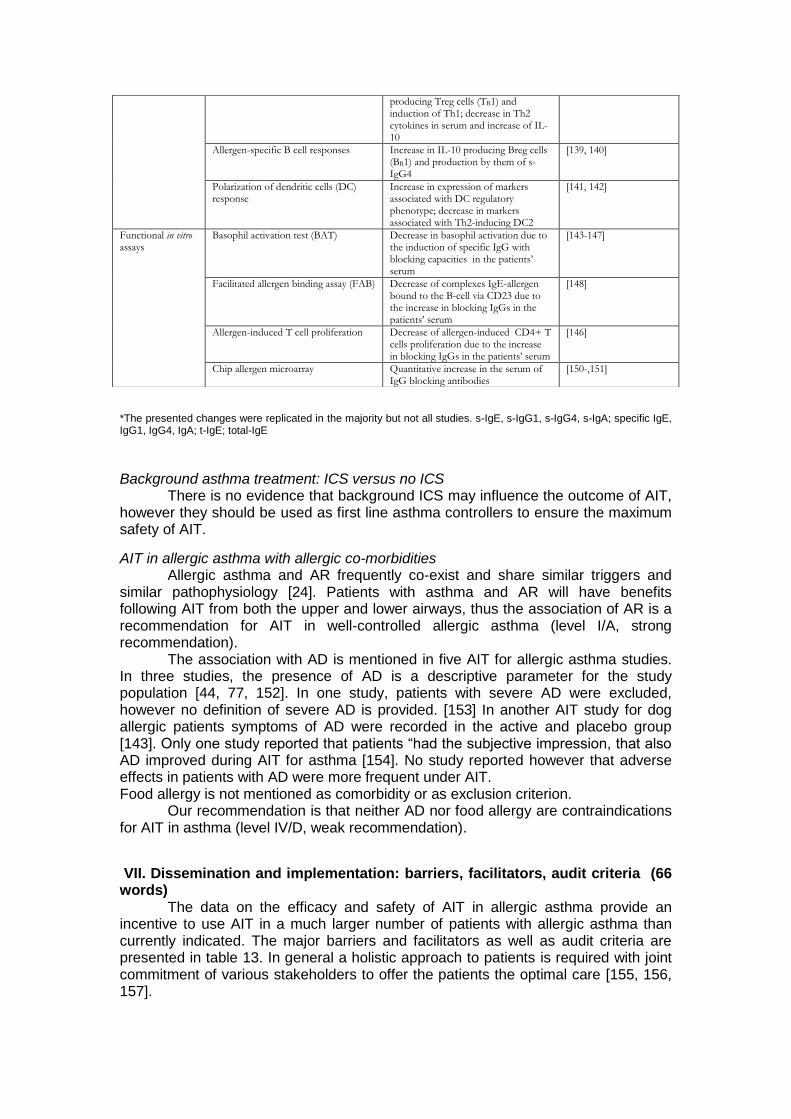
Background asthma treatment: ICS versus no ICS
There is no evidence that background ICS may influence the outcome of AIT, however they should be used as first line asthma controllers to ensure the maximum safety of AIT.
AIT in allergic asthma with allergic co-morbidities Allergic asthma and AR frequently co-exist and share similar triggers and
similar pathophysiology [24]. Patients with asthma and AR will have benefits following AIT from both the upper and lower airways, thus the association of AR is a recommendation for AIT in well-controlled allergic asthma (level I/A, strong recommendation).
The association with AD is mentioned in five AIT for allergic asthma studies. In three studies, the presence of AD is a descriptive parameter for the study population [44, 77, 152]. In one study, patients with severe AD were excluded, however no definition of severe AD is provided. [153] In another AIT study for dog allergic patients symptoms of AD were recorded in the active and placebo group [143]. Only one study reported that patients “had the subjective impression, that also AD improved during AIT for asthma [154]. No study reported however that adverse effects in patients with AD were more frequent under AIT. Food allergy is not mentioned as comorbidity or as exclusion criterion.
Our recommendation is that neither AD nor food allergy are contraindications for AIT in asthma (level IV/D, weak recommendation).
VII. Dissemination and implementation: barriers, facilitators, audit criteria (66 words)
The data on the efficacy and safety of AIT in allergic asthma provide an incentive to use AIT in a much larger number of patients with allergic asthma than currently indicated. The major barriers and facilitators as well as audit criteria are presented in table 13. In general a holistic approach to patients is required with joint commitment of various stakeholders to offer the patients the optimal care [155, 156, 157].
producing Treg cells (TR1) and induction of Th1; decrease in Th2 cytokines in serum and increase of IL-10
Allergen-specific B cell responses Increase in IL-10 producing Breg cells (BR1) and production by them of s-IgG4
[139, 140]
Polarization of dendritic cells (DC) response
Increase in expression of markers associated with DC regulatory phenotype; decrease in markers associated with Th2-inducing DC2
[141, 142]
Functional in vitro assays
Basophil activation test (BAT) Decrease in basophil activation due to the induction of specific IgG with blocking capacities in the patients’ serum
[143-147]
Facilitated allergen binding assay (FAB) Decrease of complexes IgE-allergen bound to the B-cell via CD23 due to the increase in blocking IgGs in the patients’ serum
[148]
Allergen-induced T cell proliferation Decrease of allergen-induced CD4+ T cells proliferation due to the increase in blocking IgGs in the patients’ serum
[146]
Chip allergen microarray Quantitative increase in the serum of IgG blocking antibodies
[150-,151]
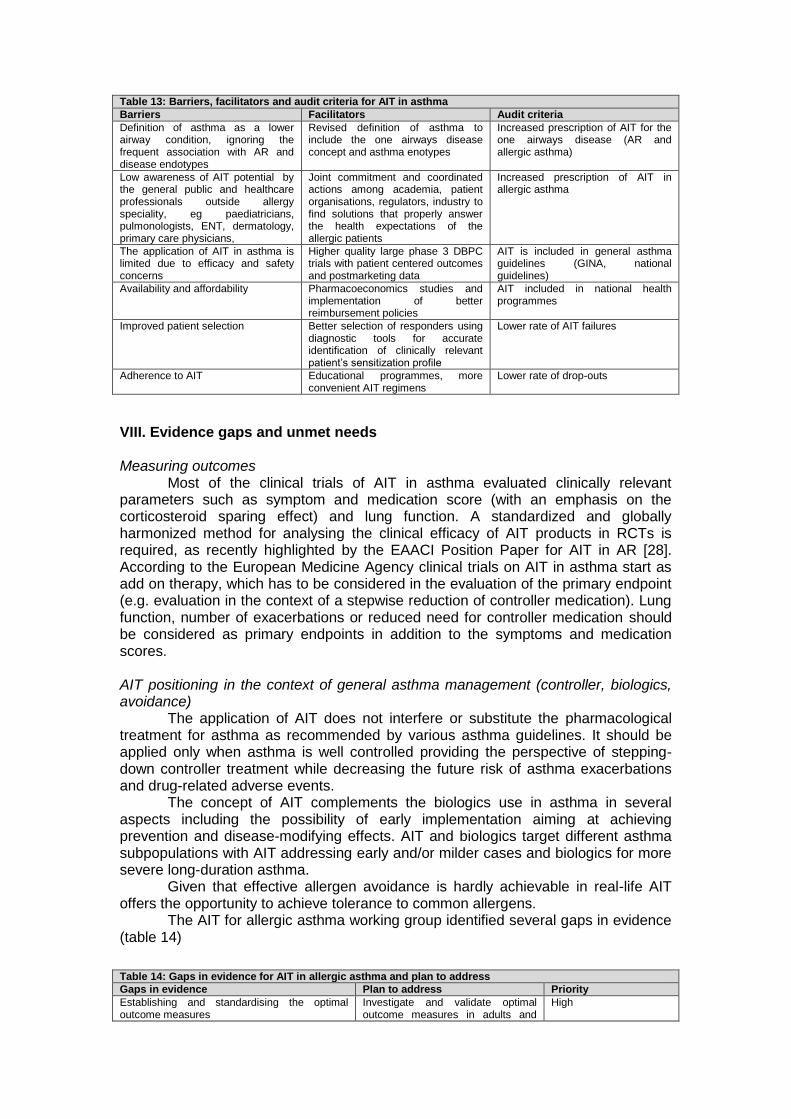
Table 13: Barriers, facilitators and audit criteria for AIT in asthma
Barriers Facilitators Audit criteria
Definition of asthma as a lower airway condition, ignoring the frequent association with AR and disease endotypes
Revised definition of asthma to include the one airways disease concept and asthma enotypes
Increased prescription of AIT for the one airways disease (AR and allergic asthma)
Low awareness of AIT potential by the general public and healthcare professionals outside allergy speciality, eg paediatricians, pulmonologists, ENT, dermatology, primary care physicians,
Joint commitment and coordinated actions among academia, patient organisations, regulators, industry to find solutions that properly answer the health expectations of the allergic patients
Increased prescription of AIT in allergic asthma
The application of AIT in asthma is limited due to efficacy and safety concerns
Higher quality large phase 3 DBPC trials with patient centered outcomes and postmarketing data
AIT is included in general asthma guidelines (GINA, national guidelines)
Availability and affordability Pharmacoeconomics studies and implementation of better reimbursement policies
AIT included in national health programmes
Improved patient selection Better selection of responders using diagnostic tools for accurate identification of clinically relevant patient’s sensitization profile
Lower rate of AIT failures
Adherence to AIT Educational programmes, more convenient AIT regimens
Lower rate of drop-outs
VIII. Evidence gaps and unmet needs Measuring outcomes
Most of the clinical trials of AIT in asthma evaluated clinically relevant parameters such as symptom and medication score (with an emphasis on the corticosteroid sparing effect) and lung function. A standardized and globally harmonized method for analysing the clinical efficacy of AIT products in RCTs is required, as recently highlighted by the EAACI Position Paper for AIT in AR [28]. According to the European Medicine Agency clinical trials on AIT in asthma start as add on therapy, which has to be considered in the evaluation of the primary endpoint (e.g. evaluation in the context of a stepwise reduction of controller medication). Lung function, number of exacerbations or reduced need for controller medication should be considered as primary endpoints in addition to the symptoms and medication scores. AIT positioning in the context of general asthma management (controller, biologics, avoidance)
The application of AIT does not interfere or substitute the pharmacological treatment for asthma as recommended by various asthma guidelines. It should be applied only when asthma is well controlled providing the perspective of stepping-down controller treatment while decreasing the future risk of asthma exacerbations and drug-related adverse events.
The concept of AIT complements the biologics use in asthma in several aspects including the possibility of early implementation aiming at achieving prevention and disease-modifying effects. AIT and biologics target different asthma subpopulations with AIT addressing early and/or milder cases and biologics for more severe long-duration asthma.
Given that effective allergen avoidance is hardly achievable in real-life AIT offers the opportunity to achieve tolerance to common allergens.
The AIT for allergic asthma working group identified several gaps in evidence (table 14)
Table 14: Gaps in evidence for AIT in allergic asthma and plan to address
Gaps in evidence Plan to address Priority
Establishing and standardising the optimal outcome measures
Investigate and validate optimal outcome measures in adults and
High
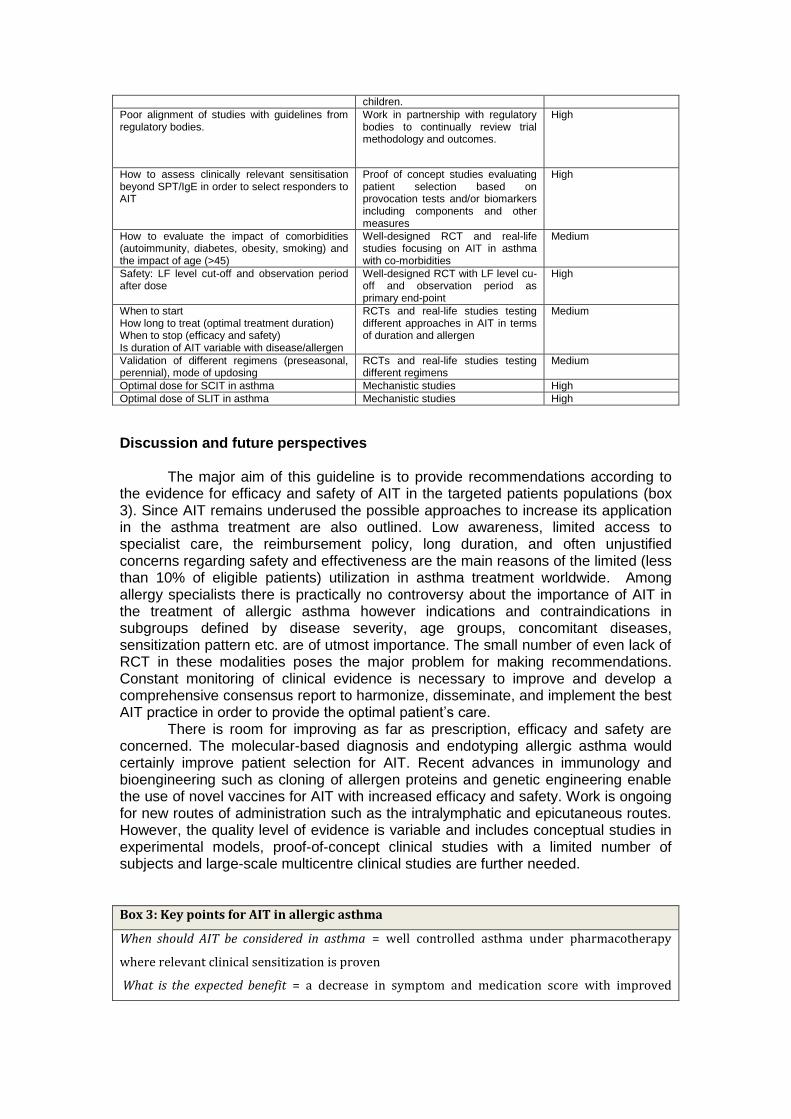
children.
Poor alignment of studies with guidelines from regulatory bodies.
Work in partnership with regulatory bodies to continually review trial methodology and outcomes.
High
How to assess clinically relevant sensitisation beyond SPT/IgE in order to select responders to AIT
Proof of concept studies evaluating patient selection based on provocation tests and/or biomarkers including components and other measures
High
How to evaluate the impact of comorbidities (autoimmunity, diabetes, obesity, smoking) and the impact of age (>45)
Well-designed RCT and real-life studies focusing on AIT in asthma with co-morbidities
Medium
Safety: LF level cut-off and observation period after dose
Well-designed RCT with LF level cu-off and observation period as primary end-point
High
When to start How long to treat (optimal treatment duration) When to stop (efficacy and safety) Is duration of AIT variable with disease/allergen
RCTs and real-life studies testing different approaches in AIT in terms of duration and allergen
Medium
Validation of different regimens (preseasonal, perennial), mode of updosing
RCTs and real-life studies testing different regimens
Medium
Optimal dose for SCIT in asthma Mechanistic studies High
Optimal dose of SLIT in asthma Mechanistic studies High
Discussion and future perspectives
The major aim of this guideline is to provide recommendations according to the evidence for efficacy and safety of AIT in the targeted patients populations (box 3). Since AIT remains underused the possible approaches to increase its application in the asthma treatment are also outlined. Low awareness, limited access to specialist care, the reimbursement policy, long duration, and often unjustified concerns regarding safety and effectiveness are the main reasons of the limited (less than 10% of eligible patients) utilization in asthma treatment worldwide. Among allergy specialists there is practically no controversy about the importance of AIT in the treatment of allergic asthma however indications and contraindications in subgroups defined by disease severity, age groups, concomitant diseases, sensitization pattern etc. are of utmost importance. The small number of even lack of RCT in these modalities poses the major problem for making recommendations. Constant monitoring of clinical evidence is necessary to improve and develop a comprehensive consensus report to harmonize, disseminate, and implement the best AIT practice in order to provide the optimal patient’s care.
There is room for improving as far as prescription, efficacy and safety are concerned. The molecular-based diagnosis and endotyping allergic asthma would certainly improve patient selection for AIT. Recent advances in immunology and bioengineering such as cloning of allergen proteins and genetic engineering enable the use of novel vaccines for AIT with increased efficacy and safety. Work is ongoing for new routes of administration such as the intralymphatic and epicutaneous routes. However, the quality level of evidence is variable and includes conceptual studies in experimental models, proof-of-concept clinical studies with a limited number of subjects and large-scale multicentre clinical studies are further needed. Box 3: Key points for AIT in allergic asthma
When should AIT be considered in asthma = well controlled asthma under pharmacotherapy
where relevant clinical sensitization is proven
What is the expected benefit = a decrease in symptom and medication score with improved
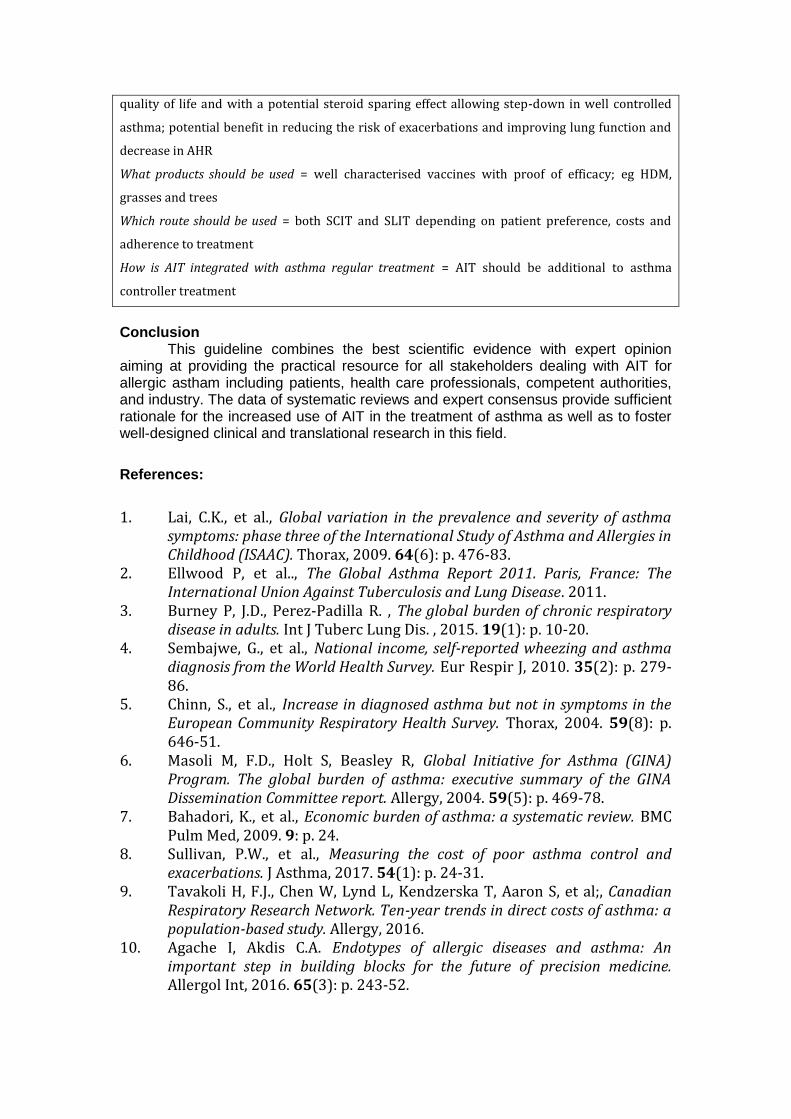
quality of life and with a potential steroid sparing effect allowing step-down in well controlled
asthma; potential benefit in reducing the risk of exacerbations and improving lung function and
decrease in AHR
What products should be used = well characterised vaccines with proof of efficacy; eg HDM,
grasses and trees
Which route should be used = both SCIT and SLIT depending on patient preference, costs and
adherence to treatment
How is AIT integrated with asthma regular treatment = AIT should be additional to asthma
controller treatment
Conclusion
This guideline combines the best scientific evidence with expert opinion aiming at providing the practical resource for all stakeholders dealing with AIT for allergic astham including patients, health care professionals, competent authorities, and industry. The data of systematic reviews and expert consensus provide sufficient rationale for the increased use of AIT in the treatment of asthma as well as to foster well-designed clinical and translational research in this field.
References:
1. Lai, C.K., et al., Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax, 2009. 64(6): p. 476-83.
2. Ellwood P, et al.., The Global Asthma Report 2011. Paris, France: The International Union Against Tuberculosis and Lung Disease. 2011.
3. Burney P, J.D., Perez-Padilla R. , The global burden of chronic respiratory disease in adults. Int J Tuberc Lung Dis. , 2015. 19(1): p. 10-20.
4. Sembajwe, G., et al., National income, self-reported wheezing and asthma diagnosis from the World Health Survey. Eur Respir J, 2010. 35(2): p. 279-86.
5. Chinn, S., et al., Increase in diagnosed asthma but not in symptoms in the European Community Respiratory Health Survey. Thorax, 2004. 59(8): p. 646-51.
6. Masoli M, F.D., Holt S, Beasley R, Global Initiative for Asthma (GINA) Program. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy, 2004. 59(5): p. 469-78.
7. Bahadori, K., et al., Economic burden of asthma: a systematic review. BMC Pulm Med, 2009. 9: p. 24.
8. Sullivan, P.W., et al., Measuring the cost of poor asthma control and exacerbations. J Asthma, 2017. 54(1): p. 24-31.
9. Tavakoli H, F.J., Chen W, Lynd L, Kendzerska T, Aaron S, et al;, Canadian Respiratory Research Network. Ten-year trends in direct costs of asthma: a population-based study. Allergy, 2016.
10. Agache I, Akdis C.A. Endotypes of allergic diseases and asthma: An important step in building blocks for the future of precision medicine. Allergol Int, 2016. 65(3): p. 243-52.
11. Lotvall, J., et al., Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. J Allergy Clin Immunol, 2011. 127(2): p. 355-60.
12. Muraro, A., et al., Precision medicine in patients with allergic diseases: Airway diseases and atopic dermatitis-PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol, 2016. 137(5): p. 1347-58.
13. Alduraywish, S.A., et al., Is there a march from early food sensitization to later childhood allergic airway disease? Results from two prospective birth cohort studies. Pediatr Allergy Immunol, 2017. 28(1): p. 30-37.
14. Tran, T.N., et al., Overlap of atopic, eosinophilic, and TH2-high asthma phenotypes in a general population with current asthma. Ann Allergy Asthma Immunol, 2016. 116(1): p. 37-42.
15. Arabkhazaeli, A., et al., Characteristics and severity of asthma in children with and without atopic conditions: a cross-sectional study. BMC Pediatr, 2015. 15: p. 172.
16. Ballardini, N., et al., IgE antibodies in relation to prevalence and multimorbidity of eczema, asthma, and rhinitis from birth to adolescence. Allergy, 2016. 71(3): p. 342-9.
17. John H. Wlodarczyk, P.G.G., Manfred Caeser, Impact of inhaled corticosteroids on cortisol suppression in adults with asthma: a quantitative review. Annals of Allergy, Asthma & Immunology, 2016. 100(1): p. 23-30.
18. Gibson, P.G., Inflammatory phenotypes in adult asthma: clinical applications The |Clinical Respiratory Journal, 2009. 3(4): p. 198-2016.
19. Fleming, L., et al., The burden of severe asthma in childhood and adolescence: results from the paediatric U-BIOPRED cohorts. Eur Respir J, 2015. 46(5): p. 1322-33.
20. Agache, I., et al., Untangling asthma phenotypes and endotypes. Allergy, 2012. 67(7): p. 835-46.
21. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2017. Available from: www.ginasthma.org
22. Jutel, M., et al., International consensus on allergy immunotherapy. J Allergy Clin Immunol, 2015. 136(3): p. 556-68.
23. Jutel, M., et al., International Consensus on Allergen Immunotherapy II: Mechanisms, standardization, and pharmacoeconomics. J Allergy Clin Immunol, 2016. 137(2): p. 358-68.
24. Bousquet J, et al., Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63 Suppl 86:8-160.
25. Brouwers MC., et al, , AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ, 2010. 14(182): p. 839-842.
26. Dhami, S., et al. Allergen immunotherapy for allergic asthma: a systematic review and meta-analysis. Allergy. 2017 May 19. doi: 10.1111/all.13208. [Epub ahead of print]
27. Dhami, S., et al., Allergen immunotherapy for allergic asthma: protocol for a systematic review. Clin Transl Allergy, 2015. 6: p. 5.
28. Pfaar, O., et al., Recommendations for the standardization of clinical outcomes used in allergen immunotherapy trials for allergic rhinoconjunctivitis: an EAACI Position Paper. Allergy. 2014 ;69(7):854-67
29. Pfaar, O., et al., Guideline on allergen-specific immunotherapy in IgE-mediated allergic diseases: S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergy and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA), the Austrian Society for Allergy and Immunology (OGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Dermatology (DDG), the German Society of Oto- Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Pneumology (GPP), the German Respiratory Society (DGP), the German Association of ENT Surgeons (BV-HNO), the Professional Federation of Paediatricians and Youth Doctors (BVKJ), the Federal Association of Pulmonologists (BDP) and the German Dermatologists Association (BVDD). Allergo J Int, 2014. 23(8): p. 282-319.
30. Lin, S.Y., et al., Sublingual immunotherapy for the treatment of allergic rhinoconjunctivitis and asthma: a systematic review. JAMA, 2013. 309(12): p. 1278-88.
31. Virchow JC, et al., Efficacy of a House Dust Mite Sublingual Allergen Immunotherapy Tablet in Adults With Allergic Asthma: A Randomized Clinical Trial. JAMA, 2016. 315(16): p. 1715-1725.
32. Mosbech H, et al., Standardized quality (SQ) house dust mite sublingual immunotherapy tablet (ALK) reduces inhaled corticosteroid use while maintaining asthma control: a randomized, double-blind, placebo-controlled trial. JACI, 2014. 34(3): p. 568-575.
33. Wang, J.Y. et al. House dust mite sublingual immunotherapy is safe and appears to be effective in moderate, persistent asthma. Allergy ;69(9):1181–8. , 2006. 69(9): p. 1181-1188.
34. Devillier P., Fadel R.F., de Beaumont O.., House dust mite sublingual immunotherapy is safe in patients with mild-to-moderate, persistent asthma: a clinical trial. Allergy. 2016;71(2):249-57
35. Lu Y et al. The efficacy and safety of subcutaneous immunotherapy in mite-sensitized subjects with asthma: a meta-analysis. Respir Care. 2015 ;60(2):269-78
36. Abramson MJ, P.R., Weiner JM, Injection allergen immunotherapy for asthma. . Cochrane Database Syst Rev, 2010. 8. CD001186. 37. Van Metre TE. et al. , Immunotherapy for cat asthma. J Allergy Clin
Immunol, 1998. 82(6): p. 1055-1068. 38. Garcia-Robaina C., et al. Successful management of mite-allergic asthma
with modified extracts of Dermatophagoides pteronyssinus and Dermatophagoides farinae in a double-blind, placebo-controlled study. . J Allergy Clin Immunol. , 2006. 118 (5): p. 1026-1032.
40. Ameal A, et al. , Double-blind and placebo-controlled study to assess efficacy and safety of a modified allergen extract of Dermatophagoides pteronyssinus in allergic asthma. . Allergy;60(9):1178–83. , 2005. 60(9): p. 1178-1183.
41. Alvarez MJ, et al., Liposome-entrapped D. pteronyssinus vaccination in mild asthma patients: effect of 1-year double-blind, placebo-controlled trial on inflammation, bronchial hyperresponsiveness and immediate and late bronchial responses to the allergen. Clin Exp Allergy 2002.;32(11):1574–82
42. Arvidsson MB, et al. A, Allergen specific immunotherapy attenuates early and late phase reactions in lower airways of birch pollen asthmatic patients: a double blind placebo-controlled study. Allergy., 2004. 59(1): p. 74-80.
43. Bousquet J et al. , Immunotherapy with a standardized Dermatophagoides pteronyssinus extract. I. In vivo and in vitro parameters after a short course of treatment. J Allergy Clin Immunol, 1985. 76(5): p. 734-744.
44. Sundin B, et al., Immunotherapy with partially purified and standardized animal dander extracts. I. Clinical results from a double-blind study on patients with animal dander asthma. J Allergy Clin Immunol, 1986. 77(3): p. 478-487.
45. Reinhold T, et al Influence of subcutaneous specific immunotherapy on drug costs in children sufferingfrom allergic asthma. Clinical and Translational Allergy, 2013. 3.
46. Bruggenjurgen, B., et al., Cost-effectiveness of specific subcutaneous immunotherapy in patients with allergic rhinitis and allergic asthma. Ann Allergy Asthma Immunol, 2008. 101(3): p. 316-24.
47. Hahn-Pedersen, J., et al., Cost utility analysis of the SQ((R)) HDM SLIT-tablet in house dust mite allergic asthma patients in a German setting. Clin Transl Allergy, 2016. 6(1): p. 35.
48. Bjorstad, A., et al., A Cost-Minimisation Analysis Comparing Sublingual Immunotherapy to Subcutaneous Immunotherapy for the Treatment of House Dust Mite Allergy in a Swedish Setting. Clin Drug Investig, 2017. 37(6): p. 541-549.
49. Ronborg, S., et al., Cost-minimization analysis of sublingual immunotherapy versus subcutaneous immunotherapy for house dust mite respiratory allergic disease in Denmark. J Med Econ, 2016. 19(8): p. 735-41
50. Kim, J.M., et al., Allergen-specific immunotherapy for pediatric asthma and rhinoconjunctivitis: a systematic review. Pediatrics, 2013. 131(6): p. 1155-67.
51. Epstein TJ Jr, et al. Ann Allergy Asthma Immuno, 2016. 116(4): p. 354-359.
52. Calderon MA, et al. European Survey on Adverse Systemic Reactions in Allergen Immunotherapy (EASSI): a real-life clinical assessment. Allergy. 2017;72(3):462-472.
53. Pablo Rodríguez del Río, et al., The European Survey on Adverse Systemic Reactions in Allergen Immunotherapy (EASSI): A paediatric assessment. PAI, 2017. 28(1): p. 60-70
54. Oykhman P, K.H., Ellis A., Allergen immunotherapy in pregnancy. Allergy Asthma Clin Immunol, 2015. 10: p. 11-31.
55. Erekosima, N., et al., Effectiveness of subcutaneous immunotherapy for allergic rhinoconjunctivitis and asthma: a systematic review. Laryngoscope, 2014. 124(3): p. 616-27
56. Polzehl, D., et al. Analysis of the efficacy of specific immunotherapy with house-dust mite extracts in adults with allergic rhinitis and/or asthma]. Laryngorhinootologie, 2003. 82(4): p. 272-80
57. Lue KH, et al. Clinical and immunologic effects of sublingual immunotherapy in asthmatic children sensitized to mites: a double-blind, randomized, placebo-controlled study. Pediatr Allergy Immunol, 2006. 17(6): p. 408-415.
58. Roberts, G., et al., Grass pollen immunotherapy as an effective therapy for childhood seasonal allergic asthma. J Allergy Clin Immunol, 2006. 117(2): p. 263-8.
59. Dahl, R., et al, Specific immunotherapy with SQ standardized grass allergen tablets in asthmatics with rhinoconjunctivitis. Allergy, 2006. 61(2): p. 185-90.
60. Stelmach, I., et al., Efficacy and safety of high-doses sublingual immunotherapy in ultra-rush scheme in children allergic to grass pollen. Clin Exp Allergy, 2009. 39(3): p. 401-8.
61. Alvarez-Cuesta, E., et al., Monoclonal antibody-standardized cat extract immunotherapy: risk-benefit effects from a double-blind placebo study. J Allergy Clin Immunol, 1994. 93(3): p. 556-66.
62. Varney WA , et al, Clinical efficacy of specific immunotherapy to cat dander: a double-blind placebo-controlled trial. Clinical Experimental Allergy, 1997. 27(8): p. 860-867.
63. Voltolini S, et al. Document Effectiveness of high dose sublingual immunotherapy to induce a stepdown of seasonal asthma: A pilot study. Curr Med Res Opin. 2010;26(1):37-40
64. Kuna, P., J. Kaczmarek, and M. Kupczyk, Efficacy and safety of immunotherapy for allergies to Alternaria alternata in children. J Allergy Clin Immunol, 2011. 127(2): p. 502-508 e1-6.
65. Tabar, A.I., et al., Double-blind, placebo-controlled study of Alternaria alternata immunotherapy: clinical efficacy and safety. Pediatr Allergy Immunol, 2008. 19(1): p. 67-75.
66. Trebuchon, F., et al., Characteristics and management of sublingual allergen immunotherapy in children with allergic rhinitis and asthma induced by house dust mite allergens. Clin Transl Allergy, 2014. 4: p. 15.
67. Vidal C, et al. Diagnosis and allergen immunotherapy treatment of polysensitised patients with respiratory allergy in Spain: an Allergists’ Consensus. Clin Transl Allergy. , 2014. 4(36)
68. Demoly P et al. Management of the polyallergic patient with allergy immunotherapy: a practice-based approach. Allergy Asthma Clin Immunol. 2016;12:2.
70. Calderon MA, et al., Perspectives on allergen-specific immunotherapy in childhood: An EAACI position statement. PAI, 2012. 23(4): p. 300-306.
71. Pepper AN, et al. Sublingual Immunotherapy for the Polyallergic Patient. J Allergy Clin Immunol Pract. 2017;5(1):41-45.
72. Calamita, Z., et al., Efficacy of sublingual immunotherapy in asthma: systematic review of randomized-clinical trials using the Cochrane Collaboration method. Allergy, 2006. 61(10): p. 1162-72.
73. Compalati, E., et al., The efficacy of sublingual immunotherapy for house dust mites respiratory allergy: results of a GA2LEN meta-analysis. Allergy, 2009. 64(11): p. 1570-9.
74. Normansell, R., K.M. Kew, and A.L. Bridgman, Sublingual immunotherapy for asthma. Cochrane Database Syst Rev, 2015(8): p. CD011293.
75. Tao, L., et al., Efficacy of sublingual immunotherapy for allergic asthma: retrospective meta-analysis of randomized, double-blind and placebo-controlled trials. Clin Respir J, 2014. 8(2): p. 192-205.
76. Lin SY, et al. Allergen-Specific Immunotherapy for the Treatment of Allergic Rhinoconjunctivitis and/or Asthma: Comparative Effectiveness Review.Rockville (MD): Agency for Healthcare Research and Quality (US); 2013 Mar.
77. Wang H, et al, A double-blind, placebo-controlled study of house dust mite immunotherapy in Chinese asthmatic patients. Allergy. 2006;61(2):191-7.
78. de Blay F, et al., SQ HDM SLIT-tablet (ALK) in treatment of asthma--post hoc results from a randomised trial. Respir Med., 2014. 108(10): p. 1430-1437.
79. Pham-Thi, et al. Assessment of sublingual immunotherapy efficacy in children with house dust mite-induced allergic asthma optimally controlled by pharmacologic treatment and mite-avoidance measures. . Pediatr Allergy Immunol, 2007. 18(1): p. 47-57.
80. Williams AA et al. The efficacy of allergen immunotherapy with cat dander in reducing symptoms in clinical practice. Biomed Res Int. 2013; 324207.
81. Gómez Vera J, Flores Sandoval G, Orea Solano M, López Tiro J, Jiménez Saab N. Safety and efficacy of specific sublingual immunotherapy in patients with asthma and allergy to Dermatophagoides pteronyssinus. Rev Alerg Mex. 2005;52(6):231-6.
82. Pajno GB, Morabito L, Barberio G, Parmiani S. Clinical and immunologic effects of long-term sublingual immunotherapy in asthmatic children sensitized to mites: a double-blind, placebo-controlled study. Allergy. 2000 ;55(9):842-9.
83. Bahçeciler NN, et al. E, fficacy of sublingual immunotherapy in children with asthma and rhinitis: a double-blind, placebo-controlled study. Pediatr Pulmonol, 2001. 32(1): p. 49-55.
84. Pajno G. B., et al, Impact of sublingual immunotherapy on seasonal asthma and skin reactivity in children allergic to Parietaria pollen treated with inhaled fluticasone propionate Clin Exp Allergy, 2004. 33(12): p. 1641-1647.
85. Leng X, Fu YX, Ye ST, Duan SQ. A double-blind trial of oral immunotherapy for Artemisia pollen asthma with evaluation of bronchial response to the pollen allergen and serum-specific IgE antibody Ann Allergy. 1990;64(1):27-31.
86. Lewith GT, Watkins AD, Hyland ME, Shaw S, Broomfield JA, Dolan G, Holgate ST.Use of ultramolecular potencies of allergen to treat asthmatic people allergic to house dust mite: double blind randomised controlled clinical trial. BMJ. 2002;324(7336):520.
87. Pitsios C, D.P., et al, Clinical contraindications to allergen immunotherapy: an EAACI position paper. Allergy., 2015. 70(8): p. 897-909.
89. Cox L, Esch RE, Corbett M, Hankin C, Nelson M, Plunkett G. Allergen immunotherapy practice in the United States: guidelines, measures, and outcomes. Ann Allergy Asthma Immunol. 2011;107(4):289-99
90. Lockey RF, Nicoara-Kasti GL, Theodoropoulos DS, Bukantz SC. Systemic reactions and fatalities associated with allergen immunotherapy. Ann Allergy Asthma Immunol. 2001;87(1 Suppl 1):47-55.
91. Bernstein DI, Wanner M, Borish L, Liss GM; Immunotherapy Committee, American Academy of Allergy, Asthma and Immunology Twelve-year survey of fatal reactions to allergen injections and skin testing: 1990-2001. J Allergy Clin Immunol. 2004;113(6):1129-36.
92. Turkcapar N. et al. Specific immunotherapy-induced Sjorgren’s Syndrome. Rheumatol Int (2005) 26: 182–184
93. Bozek A, Kozłowska R, Jarzab J. The safety of specific immunotherapy for patients allergic to house-dust mites and pollen in relation to the development of neoplasia and autoimmune disease: a long-term, observational case-control study. Int Arch Allergy Immunol. 2014;163(4):307-12
94. Cox L, Jacobsen L. Comparison of allergen immunotherapy practice patterns in the United States and Europe. Ann Allergy Asthma Immunol 2009;103(6):451-459
95. Pfaar O, Biedermann T, Klimek L, Sager A, Robinson DS. Depigmented-polymerized mixed grass/birch pollen extract immunotherapy is effective in polysensitized patients. Allergy 2013;68(10):1306-1313
96. Cirla AM, Cirla PE, Parmiani S, Pecora S. A pre-seasonal birch/hazel sublingual immunotherapy can improve the outcome of grass pollen injective treatment in bisensitized individuals. A case-referent, two-year controlled study. Allergol Immunopathol (Madr) 2003;31(1):31-43
97. Marogna M, Spadolini I, Massolo A, Zanon P, Berra D, Chiodini E, et al. Effects of sublingual immunotherapy for multiple or single allergens in polysensitized patients. Ann Allergy Asthma Immunol 2007;98(3):274-280.
98. Maloney J, Berman G, Gagnon R, Bernstein DI, Nelson HS, Kleine-Tebbe J, Kaur A, Li Q, Nolte H. Sequential Treatment Initiation with Timothy Grass and Ragweed Sublingual Immunotherapy Tablets Followed by Simultaneous Treatment Is Well Tolerated. J Allergy Clin Immunol Pract. 2016;4(2):301-9
99. Nelson HS. Multiallergen immunotherapy for allergic rhinitis and asthma. J Allergy Clin Immunol 2009;123(4):763-769
100. Mirone C, Albert F, Tosi A, et al. Efficacy and safety of subcutaneous immunotherapy with a biologically standardized extract of Ambrosia artemisiifolia pollen: a double-blind, placebo-controlled study. Clin Exp Allergy. 2004;34(9):1408–1414
101. André C, Perrin-Fayolle M, Grosclaude M, et al. A double-blind placebo-controlled evaluation of sublingual immunotherapy with a standardized ragweed extract in patients with seasonal rhinitis. Evidence for a dose-response relationship. Int Arch Allergy Immunol. 2003;131(2):111–118.
102. Creticos PS, Maloney J, Bernstein DI, et al. Randomized controlled trial of a ragweed allergy immunotherapy tablet in North American and European adults. J Allergy Clin Immunol. 2013;131(5):1342–1349
103. Tourdot S1, A.S., Berjont N, Moussu H, Betbeder D, Nony E, Bordas-Le Floch V, Baron-Bodo V, Mascarell L, Moingeon P., Efficacy of sublingual vectorized recombinant Bet v 1a in a mouse model of birch pollen allergic asthma. Vaccine. , 2013. 31(23): p. 2628-2637.
104. Siebeneicher, S., Reuter, S., Wangorsch, A., Krause, M., Foetisch, K., Heinz, A. et al, . Epicutaneous immunotherapy with a hypoallergenic Bet v 1 suppresses allergic asthma in a murine model. Allergy, 2015. 70: p. 1559-1568.
105. Stelmach I, Kaluzinska-Parzyszek I, Jerzynska J Stelmach P. Stelmach W, Majak P Comparative effect of pre-coseasonal and continuous grass sublingual immunotherapy in children. Allergy 2012; 67: 312–320
106. Senti G, Kundig TM. Novel Delivery Routes for Allergy Immunotherapy: Intralymphatic, Epicutaneous, and Intradermal. Immunol Allergy Clin North Am 2016; 36:25-37.
107. Moingeon P. Adjuvants for allergy vaccines. Hum Vaccin Immunother 2012; 8:1492-8
108. Santeliz JV, Van Nest G, Traquina P, Larsen E, Wills-Karp M. Amb a 1-linked CpG oligodeoxynucleotides reverse established airway hyperresponsiveness in a murine model of asthma. J Allergy Clin Immunol 2002; 109:455-62.
109. Beeh KM, Kanniess F, Wagner F, Schilder C, Naudts I, Hammann-Haenni A, et al. The novel TLR-9 agonist QbG10 shows clinical efficacy in persistent allergic asthma. J Allergy Clin Immunol 2013; 131:866-74
110. Majak P, Rychlik B, Stelmach I. The effect of oral steroids with and without vitamin D3 on early efficacy of immunotherapy in asthmatic children. Clin Exp Allergy 2009; 39:1830-41.
111. Baris S, Kiykim A, Ozen A, Tulunay A, Karakoc-Aydiner E, Barlan IB. Vitamin D as an adjunct to subcutaneous allergen immunotherapy in asthmatic children sensitized to house dust mite. Allergy 2014; 69:246-53
112. Massanari M et al. Effect of pretreatment with omalizumab on the tolerability of specific immunotherapy in allergic asthma. J Allergy Clin Immunol 2010, 125(2):383-9.
113. Kopp MV, Hamelmann E, Zielen S, et al. Combination of omalizumab and specific immunotherapy is superior to immunotherapy in patients with seasonal allergic rhinoconjunctivitis and co-morbid seasonal allergic asthma. Clin Exp Allergy. 2009: 39: 271–9
114. Kopp MV, Hamelmann E, Bendiks M, Zielen S, Kamin W,Bergmann K-C, Klein C, Wahn U for the DUAL study group. Transient impact of omalizumab in pollen allergic patients undergoing specific immunotherapy Pediatr Allergy Immunol 2013: 24: 427–433.
115. Chaker AM, et al. Short-term subcutaneous grass pollen immunotherapy under the umbrella of anti-IL-4: A randomized controlled trial. J Allergy Clin Immunol. 2016 Feb;137(2):452-461
116. Agache I, Bilò M, Braunstahl GJ, Delgado L, Demoly P, Eigenmann P, Gevaert P, Gomes E, Hellings P, Horak F, Muraro A, Werfel T, Jutel M.In vivo diagnosis of allergic diseases--allergen provocation tests. Allergy. 2015;70(4):355-65.
117. Choi IS, Kim SJ, Won JM, Park MS. Usefulness of House Dust Mite Nasal Provocation Test in Asthma. Allergy Asthma Immunol Res. 2017 Mar;9(2):152-157
118. Pène J, Desroches A, Paradis L, Lebel B, Farce M, Nicodemus CF, Yssel H, Bousquet J. Immunotherapy with Fel d 1 peptides decreases IL-4 release by peripheral blood T cells of patients allergic to cats. J Allergy Clin Immunol. 1998;102;4:571-8.
119. Garcia-Ortega P. Merelo A, M.J.a.R.C., Decrease of Skin and Bronchial Sensitization Following Short-intensive Scheduled Immunotherapy in Mite-Allergic Asthma Chest 1993, 1993. 103: p. 183-187
120. Yukselen A, Kendirli SG, Yilmaz M, Altintas DU, Karakoc GB. Two year follow-up of clinical and inflammation parameters in children monosensitized to mites undergoing subcutaneous and sublingual immunotherapy. Asian Pac J Allergy Immunol. 2013;31(3):233-41
120. Rosewich M, Girod K, Zielen S, Schubert R, Schulze J. Induction of Bronchial Tolerance After 1 Cycle of Monophosphoryl-A-Adjuvanted Specific Immunotherapy in Children With Grass Pollen Allergies. Allergy Asthma Immunol Res. 2016;8(3):257-63.
121. Armentia-Medina, A., et al., Immunotherapy with the storage mite lepidoglyphus destructor. Allergol Immunopathol (Madr), 1995. 23(5): p. 211-23.
122. Agache I, Sugita K, Morita H, Akdis M, Akdis CA. The Complex Type 2 Endotype in Allergy and Asthma: From Laboratory to Bedside. Curr Allergy Asthma Rep. 2015;15(6):29.
123. Basomba, A., et al., Allergen vaccination with a liposome-encapsulated extract of Dermatophagoides pteronyssinus: a randomized, double-blind, placebo-controlled trial in asthmatic patients. J Allergy Clin Immunol, 2002. 109(6): p. 943-8.
124. Chakraborty, P., et al., Phoenix sylvestris Roxb pollen allergy: a 2-year randomized controlled trial and follow-up study of immunotherapy in patients with seasonal allergy in an agricultural area of West Bengal, India. J Investig Allergol Clin Immunol, 2006. 16(6): p. 377-84.
125. Creticos, P.S., et al., Ragweed immunotherapy in adult asthma. N Engl J Med, 1996. 334(8): p. 501-6.
126. Hui, Y., et al., Efficacy analysis of three-year subcutaneous SQ-standardized specific immunotherapy in house dust mite-allergic children with asthma. Exp Ther Med. 7(3): p. 630-634.
127. Dordal, M.T., et al., Allergen-specific nasal provocation testing: review by the rhinoconjunctivitis committee of the Spanish Society of Allergy and Clinical Immunology. J Investig Allergol Clin Immunol, 2011. 21(1): p. 1-12; quiz follow 12.
128. Roger, A., et al., A novel microcrystalline tyrosine-adsorbed, mite-allergoid subcutaneous immunotherapy: 1-year follow-up report. Immunotherapy, 2016. 8(10): p. 1169-74.
129. Soyyigit, S., et al., Immunologic alterations and efficacy of subcutaneous immunotherapy with Dermatophagoides pteronyssinus in monosensitized and polysensitized patients. Ann Allergy Asthma Immunol, 2016. 116(3): p. 244-251
130. Klimek, L., et al., Specific subcutaneous immunotherapy with recombinant grass pollen allergens: first randomized dose-ranging safety study. Clin Exp Allergy, 2012. 42(6): p. 936-45
131. Pilette, C., et al., Grass pollen immunotherapy induces an allergen-specific IgA2 antibody response associated with mucosal TGF-beta expression. J Immunol, 2007. 178(7): p. 4658-66.
132. Ciprandi, G. and M. Silvestri, Serum specific IgE: a biomarker of response to allergen immunotherapy. J Investig Allergol Clin Immunol, 2014. 24(1): p. 35-9.
133. Di Lorenzo, G., et al., Evaluation of serum s-IgE/total IgE ratio in predicting clinical response to allergen-specific immunotherapy. J Allergy Clin Immunol, 2009. 123(5): p. 1103-10, 1110 e1-4.
134. Fujimura, T., et al., Increase of regulatory T cells and the ratio of specific IgE to total IgE are candidates for response monitoring or prognostic biomarkers in 2-year sublingual immunotherapy (SLIT) for Japanese cedar pollinosis. Clin Immunol, 2011. 139(1): p. 65-74.
135. Jutel, M., et al., IL-10 and TGF-beta cooperate in the regulatory T cell response to mucosal allergens in normal immunity and specific immunotherapy. Eur J Immunol, 2003. 33(5): p. 1205-14.
136. Akdis, C.A. and M. Akdis, Mechanisms of immune tolerance to allergens: role of IL-10 and Tregs. J Clin Invest, 2014. 124(11): p. 4678-80.
137. Francis, J.N., S.J. Till, and S.R. Durham, Induction of IL-10+CD4+CD25+ T cells by grass pollen immunotherapy. J Allergy Clin Immunol, 2003. 111(6): p. 1255-61.
138. Mobs, C., et al., Birch pollen immunotherapy leads to differential induction of regulatory T cells and delayed helper T cell immune deviation. J Immunol, 2010. 184(4): p. 2194-203.
139. Boonpiyathad, T., et al., High-dose bee venom exposure induces similar tolerogenic B-cell responses in allergic patients and healthy beekeepers. Allergy, 2016.
140. van de Veen, W., et al., IgG4 production is confined to human IL-10-producing regulatory B cells that suppress antigen-specific immune responses. J Allergy Clin Immunol, 2013. 131(4): p. 1204-12.
141. Zimmer, A., et al., A regulatory dendritic cell signature correlates with the clinical efficacy of allergen-specific sublingual immunotherapy. J Allergy Clin Immunol, 2012. 129(4): p. 1020-30.
142. Gueguen, C., et al., Changes in markers associated with dendritic cells driving the differentiation of either TH2 cells or regulatory T cells correlate with clinical benefit during allergen immunotherapy. J Allergy Clin Immunol, 2015. 137(2): p. 545-58.
143. Hoffmann, H.J., et al., The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy, 2015. 70(11): p. 1393-405.
144. Schmid, J.M., et al., Early improvement in basophil sensitivity predicts symptom relief with grass pollen immunotherapy. J Allergy Clin Immunol, 2014. 134(3): p. 741-744 e5.
145. Ceuppens, J.L., et al., Immunotherapy with a modified birch pollen extract in allergic rhinoconjunctivitis: clinical and immunological effects. Clin Exp Allergy, 2009. 39(12): p. 1903-9.
146. van Neerven, R.J., et al., Blocking antibodies induced by specific allergy vaccination prevent the activation of CD4+ T cells by inhibiting serum-IgE-facilitated allergen presentation. J Immunol, 1999. 163(5): p. 2944-52.
147. Mobs, C., et al., Birch pollen immunotherapy results in long-term loss of Bet v 1-specific TH2 responses, transient TR1 activation, and synthesis of IgE-blocking antibodies. J Allergy Clin Immunol, 2012. 130(5): p. 1108-1116 e6.
148. Wilcock, L.K., J.N. Francis, and S.R. Durham, IgE-facilitated antigen presentation: role in allergy and the influence of allergen immunotherapy. Immunol Allergy Clin North Am, 2006. 26(2): p. 333-47, viii-ix.
149. Wollmann, E., et al., Reduction in allergen-specific IgE binding as measured by microarray: A possible surrogate marker for effects of specific immunotherapy. J Allergy Clin Immunol, 2015. 136(3): p. 806-809 e7.
150. Schmid, J.M., et al., Pretreatment IgE sensitization patterns determine the molecular profile of the IgG4 response during updosing of subcutaneous immunotherapy with timothy grass pollen extract. J Allergy Clin Immunol, 2016. 137(2): p. 562-70.
151. Lupinek, C., E. Wollmann, and R. Valenta, Monitoring Allergen Immunotherapy Effects by Microarray. Curr Treat Options Allergy, 2016. 3: p. 189-203.
152. Warner JO et al. Controlled trial of hyposensitisation to Dermatophagoides pteronyssinus in children with asthma. Lancet 1978, 28;2(8096):912-5.
153. Valovirta E, Koivikko A, Vanto T, Viander M, Ingeman L. Immunotherapy in allergy to dog: a double-blind clinical study. Ann Allergy. 1984;53(1):85-8.
154. Valovirta E, Viander M, Koivikko A, Vanto T, Ingeman L. Immunotherapy in allergy to dog. Immunologic and clinical findings of a double-blind study. Ann Allergy. 1986;57(3):173-9.
155. Bousquet J, et al. Integrated care pathways for airway diseases (AIRWAYS-ICPs). Eur Respir J. 2014;44(2):304-23
156. Papadopoulos NG, et al. Research needs in allergy: an EAACI position paper, in collaboration with EFA. Clin Transl Allergy. 2012;2(1):21
157. Jutel M, Angier L, Palkonen S, Ryan D, Sheikh A, Smith H, Valovirta E, Yusuf O, van Wijk RG, Agache I. Improving allergy management in the primary care network--a holistic approach. Allergy. 2013;68(11):1362-9.