rdk biomarker science talk_v2
TRANSCRIPT

Best Practice in Biomarker Development
Richard Kennedy
VP and Diagnostic Lab Director, Almac Diagnostics
Professor of Medical Oncology , Queen’s University BelfastConsultant Medical Oncologist, Northern Ireland Cancer Centre

Clinical Biomarkers
Kennedy, Harkin, Salto-Tellez and Johnston et al, Oxford Textbook of Oncology 2013, In print

Clinical Biomarkers
Kennedy, Harkin, Salto-Tellez and Johnston et al, Oxford Textbook of Oncology 2013, In print

Predictive Biomarkers
• Predict benefit from a specific therapy
• Over 15,000 manuscripts reporting predictive biomarkers in cancer
• Few have made an impact on clinical practice

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation
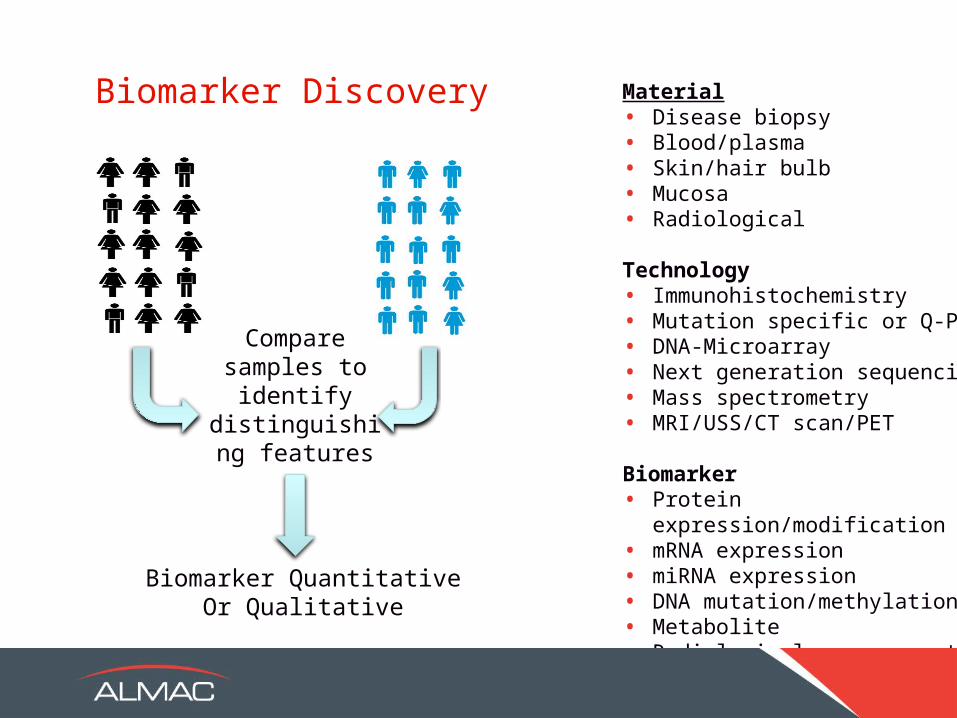
Material• Disease biopsy• Blood/plasma• Skin/hair bulb• Mucosa• Radiological
Technology• Immunohistochemistry• Mutation specific or Q-PCR• DNA-Microarray• Next generation sequencing• Mass spectrometry• MRI/USS/CT scan/PET
Biomarker• Protein expression/modification• mRNA expression• miRNA expression• DNA mutation/methylation• Metabolite • Radiological measurement
Compare samples to
identify distinguishing
features
Biomarker QuantitativeOr Qualitative
Biomarker Discovery

Two Major Types of Predictive Biomarker
Qualitative
• Mutation / no mutation (KRAS / BRAF / p53)
• Expression / no expression (c-KIT)
Quantitative
• Score based
• Positive or negative result depends on a score
• IHC for estrogen receptor
• Q-PCR / DNA microarray multigene signatures (OncotypeDx, Mammoprint)

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Biomarker Discovery Strategies
1. Preclinical Model Systems
2. Retrospective Archived Tissue
3. Prospective Discovery

Biomarker Discovery Strategies
1. Preclinical Model Systems
2. Retrospective Archived Tissue
3. Prospective Discovery

Pre-clinical Biomarker Discovery
• Human cell lines and animal models
• Advantages: • Early in drug trial process• Allows behavior of drug to be modeled in specific
molecular contexts
• Disadvantages:• Different physiology• Can be little genetic variation between animals• No immune system in xenografts• No tumour stroma in cell culture• No reliable cut-off for quantitative assays

Almac DiagnosticsAACR 2012
Biomarker for SRC Inhibitor
Isogenic Cell Line and Xenograft Data
7 gene classifier for SRC activity
Test on independent cell lines

Biomarker Discovery Strategies
1. Preclinical Model Systems
2. Retrospective Archived Tissue
3. Prospective Discovery

Retrospective Biomarker Discovery
• Use archived tissue from tumour banks
• Advantages:• Relevant human material• Full clinical annotation including outcome is often available • Large numbers may be available- clustering analysis• Can set population distribution based cut-off for
quantitative assays
• Disadvantages:• Unlikely to be possible for novel therapies entering trials• Tissue may not have been collected appropriately• Archived tissue can degrade over time

Example: Biomarker for Angiogenic Agents
63 gene microarray assay for non-angiogenesis
Retrospectively validate in ICON7 Bevacizumab In Ovarian cancer study
300 High grade serous ovarian
samplesAngiogenesis
Gourley C., Michie C, Keating K, Gavigan A, DeHaroS, Hill L, Harkin DP, Kennedy RD ASCO 2011

Biomarker Discovery Strategies
1. Preclinical Model Systems
2. Retrospective Archived Tissue
3. Prospective Discovery

Predictive Biomarker Discovery
• Analysis of tissue from responding and non-responding patients on a clinical study
• Advantages:• Material is relevant to the drug in question
• Disadvantages:• New drug may be given in combination with other
therapies, difficult to develop specific biomarker • Can require large numbers of patients- needs adequate
numbers of responding and non responding patients

Simple Biomarker Discovery Trial Design
• If predicted response rate is 10% in unselected population will need 500 people to get 50 responder samples!
• Adaptive trial designs may help reduce numbers.
Patient Enrolment
Sample Biomarker Studies
Biomarker Generation
New Treatment
Responders Non-Responders

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Technology
Material Type
• Storage and shipping (fresh/archived)
• Patient safety/comfort (biopsy/resection/blood)
Technology
• Quality (CE marked, GMP)
• Maintenance (calibration and scheduled servicing)
• Practicality (cost, turnaround time, ease of use)
• Longevity (will it be obsolete soon?)

Reagents
• Many laboratory regents are “research use only” (RUO)
• Can be considerable variation in performance batch to batch
• Biomarker may become “batch dependent”
• Ideally use GMP reagents, batch tested
• Can consider pooled batches if RUO only available

Batch Effects
Almac Diagnostics 2010

Lab Operator Effects
• Biomarkers discovered by a single lab operator may only work for that individual
• Modified lab protocols
• Very experienced in a particular assay
• Adhere to strict standard operating procedures
• Randomize samples between several operators during discovery phase
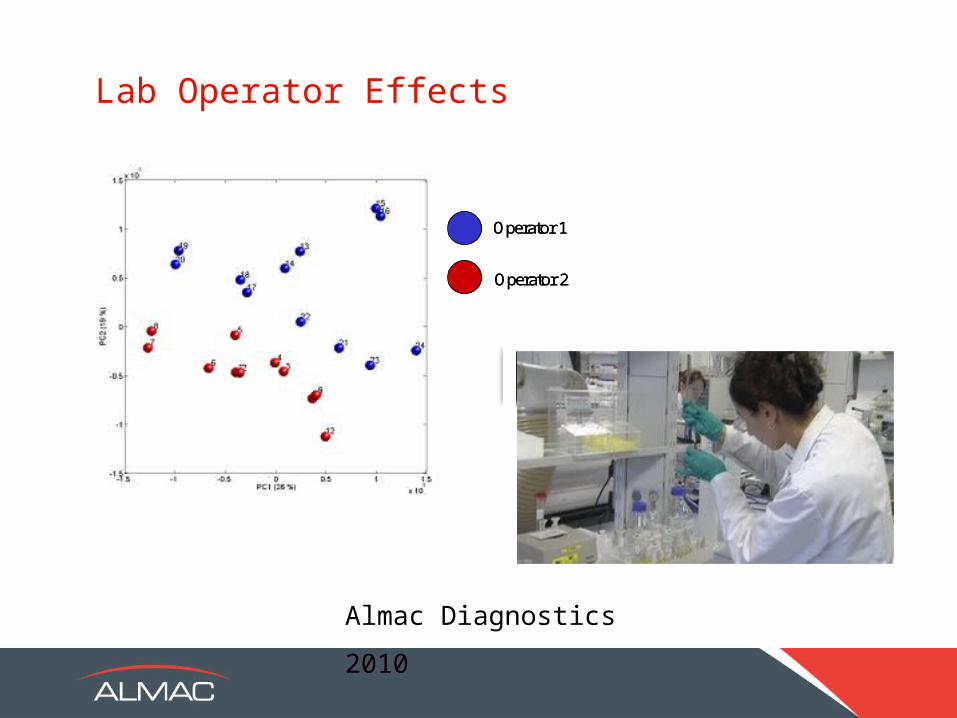
Lab Operator Effects
Almac Diagnostics 2010
Operator 1
Operator 2
Operator 1
Operator 2
What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Clinical Centre Effects
• Biomarkers discovered from a single centre may not be applicable elsewhere
• Specific surgical approaches
• Specific specimen fixation protocols
• User biases on assessment of response to drug
• Ideally use material and clinical data representing response/non-response from multiple centres

Centre Effects
Kennedy et al J Clin Oncol. 2011 Dec 10;29(35):4620-
6
What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Population Effects
• Important to ensure that the population used for biomarker discovery is relevant to the population in which it will be applied
• E.g.
• Afro Caribbean variations in prostate or breast cancer biology
• Asian variations in lung cancer biology

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Balancing for Convoluting Factors
Positive and negative discovery samples must be balanced for potential confounding factors such as:
• Gender
• Age
• Ethnicity
• Other medication/smoking
• Other medical conditions
• Known prognostic/predictive factors• Tumour Stage
• Tumour Grade
• Lymphocyte infiltrate
Failure to do this may result in a biomarker for the wrong thing

What to Consider
Discovery and Development
• What does it measure? Quantitative/Qualitative
• Preclinical/retrospective/prospective discovery
• Technology/reagents/lab effects
• Centre effects
• Population effects
• Convoluting factors
Validation
• Analytical validation
• Clinical validation

Biomarker Validation
1. Regulatory Landscape
2. Analytical Validation
3. Clinical Validation

Regulatory Landscape
• Different levels of regulatory approval exist
• This choice is influenced by the type of biomarker and
intended use and risk to patients:
• Companion diagnostics most stringent
• Relevant bodies are• CLIA (Clinical Laboratory Improvement Amendment act)
• FDA (Food and Drink Administration- PMA route for companion diagnostics
• EMA (European Medicines Agency)
• Needs to be considered at the start of research
Biomarker Validation
1. Regulatory Landscape
2. Analytical Validation
3. Clinical Validation

Analytical Validation
• Precision
• Accuracy
• Limits of Detection

Analytical Validation
• Precision
• Accuracy
• Limits of Detection

Precision
• Measure of biomarker repeatability
• Loss of precision can occur due to:
• Inherent variability in technology (IHC for phospho-
proteins, plasma protein measurement)
• Variability in reagents, equipment or technique
• Normal/Stromal/malignant cellular content

Effects
Full Biopsy Material Macrodissected Biopsy Material
Almac Diagnostics 2013
Effects of Macrodissection on Precision of a q-PCR-based Biomarker

Analytical Validation
• Precision
• Accuracy
• Limits of Detection

Accuracy
• A measure of how close the result is to the known truth
• Truth may be a:• Result from a reference lab• Gold standard technology
• Can be affected by:• Site / type of biopsy - tumour heterogeneity• Incorrect sample fixation or lab technique • further treatment since diagnostic biopsy taken

Gene Expression Differences
Gene Expression Differences Between Original Diagnostic Tissue and Recurrent Disease
• Series of ovarian cancers analysed pre-chemotherapy and on recurrence
• 486 genes >2 fold differentially expressed p<0.005
Analytical Validation
• Precision
• Accuracy
• Limits of Detection

Limits of Detection
• Measures how much material required to give an accurate
result
• In cancer this will also include percentage tumour content
(usually over 20% for mutation detection)
Tumour

Biomarker Validation
1. Regulatory Landscape
2. Analytical Validation
3. Clinical Validation
Clinical Validation
• Absolute requirement for a companion diagnostic to be used
for drug selection in regular clinical practice
• Needs strategy agreed with regulatory authority prior to
study• Simple biomarker validation
• Complex biomarker validation
• Must show that the biomarker can adequately stratify
patients (sensitivity, specificity, hazard ratio)

Patients Enrol to Study
Biomarker
Experimental Drug
Predicted Responder Predicted Non-Responder
Randomise Not on Trial
Standard Therapy
Compare outcome
Simple Biomarker Validation Study

Patients Enrol to Study
Biomarker
Receive Experimental
Drug
Predicted Responder Predicted Non-Responder
Randomise Randomize
Receive Standard Therapy
Receive Standard
Treatment
Receive Experimental
Drug
Calculate Sensitivity / Specificity etc.
Mandrekar and Sargent J Clin Oncol 2009 27(24):4027-34
Complex Biomarker Validation Study
What to consider for a predictive biomarker to be used in the clinic:
• Discovery and Development • Correct discovery dataset• Correct technology and reagents• Not convoluted by other known factors
• Validation• Regulatory requirements depending on use• Analytical: precision and accuracy• Clinical: sensitivity, specificity etc
Conclusions