ransart boot
TRANSCRIPT

The Ransart Boot: The Ransart Boot: an offloading device for every an offloading device for every type of Diabetic Foot Ulcers? type of Diabetic Foot Ulcers?
I. Dumont¹, E. Fernandez¹, D.Tsirtsikolou², M. Lepage², S. Popielarz³, A. Fayard4, O. Basuyaux5,
M. Lepeut5.
¹Centre du Pied, Ransart, Belgique, ²CH de Boulogne,³CHRU de Lille, 4CH de Arras, 5CH de Roubaix, France.
Diabetic neuropathic FU heal when offloaded.
The TUC (Texas University Classification) validation has correlated the different DFU’s classes with the amputation rate.
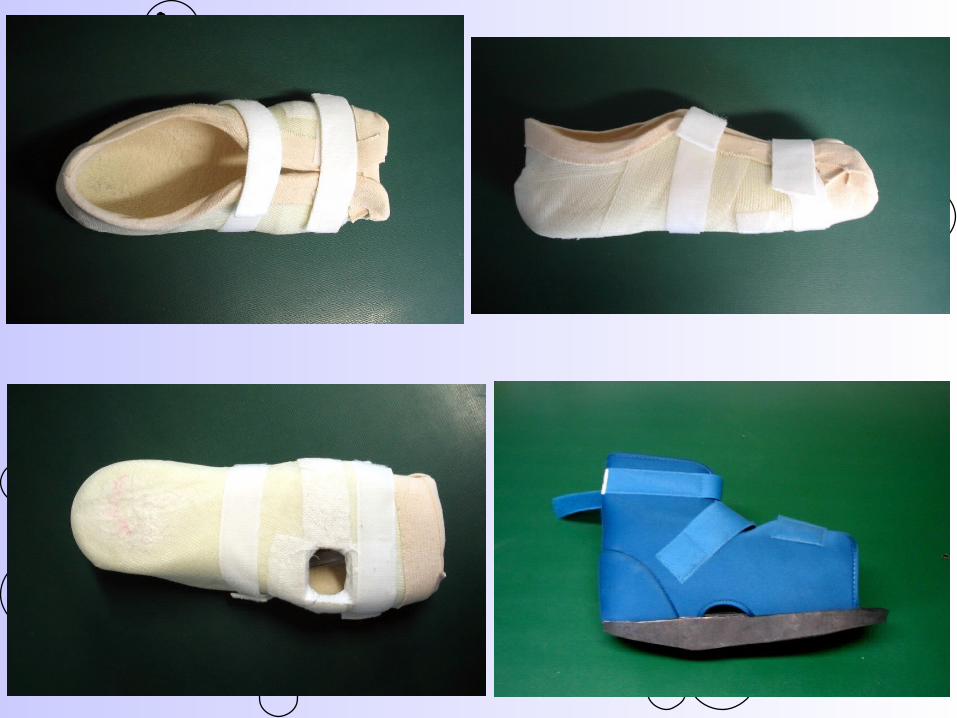
The Ransart boot (RB) is a small, light and removable windowed cast allowing normal daily activities.
BackgroundBackground
To evaluate the efficacy and safety of the Ransart Boot in the treatment of DF Ulcer Class A1 (TUC).
To evaluate the efficacy and safety of the Ransart Boot in the treatment of DF Ulcer whatever the Class (TUC).
Aims of the study:Aims of the study:
Materials and methods:Materials and methods: This is an open, retrospective and multicentre
study including 109 patients.
Inclusion criteria: - Diabetes (type I and II). - Age between 18 and 80 years old. - Foot at risk (VPT > 25 V or monofilament 10gr
not felt). - DF ulcer on the plantar or lateral aspect of the
foot treated by RB.
- Class A1 to D3 of the TUC. - DF ulcer not healed after 1 year was
considered as a failure.
Exclusion criteria: - Non classic therapy during the port
of the RB like VAC, maggots etc. - Revascularisation or orthopaedic
surgery (# amputation) during the study.
Results:Results: 109 patients included from 5 centers. (minus
7 lost for follow-up, 5 suffering serious comorbidities, 3 deceased and 12 non compliant). So 82 were left. Ulcer presentation: forefoot:61, rearfoot:6,
midfoot:14. Comparison with Armstrong’s results who did
not specify in his study the offloading technique used for patients with ischemia and/or infected ulcers.
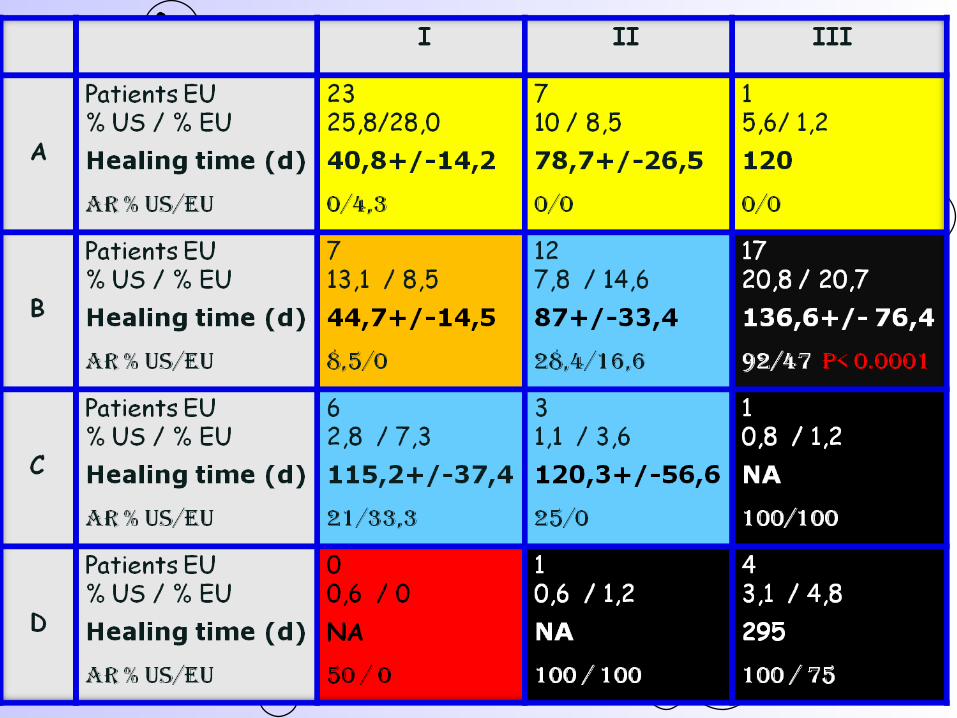
Nice correlation between both distribution and
amputation rate which favors RB in classe B3 (P<0001).Healing time for A1 is very good comparing with TCC or other irremovable devices.Activity do not modify healing time comparing A1 class ulcer treated with TCC (60% less steps) or RB.Healing time for other classes seem good but it is difficult to find population to compare with.Very few minor complications.
The RB can offload with efficacy and safety every ulcer even with infection and/or ischemia as well as Charcot foot. The rate of non compliance is low: 11% .Further studies are needed to clarify the respective role of compliance (perhaps enhanced by a patient friendly cast?) and activity, as well as quality of life, educational impact, costs and frequencies of recurrences.
Conclusions :Conclusions :