quality improvement david conway, md, facog. disclosure i have no conflicts of interest to disclose
TRANSCRIPT

QUALITY IMPROVEMENT
David Conway, MD, FACOG

DISCLOSURE
I have no conflicts of interest to disclose

INTRODUCTION
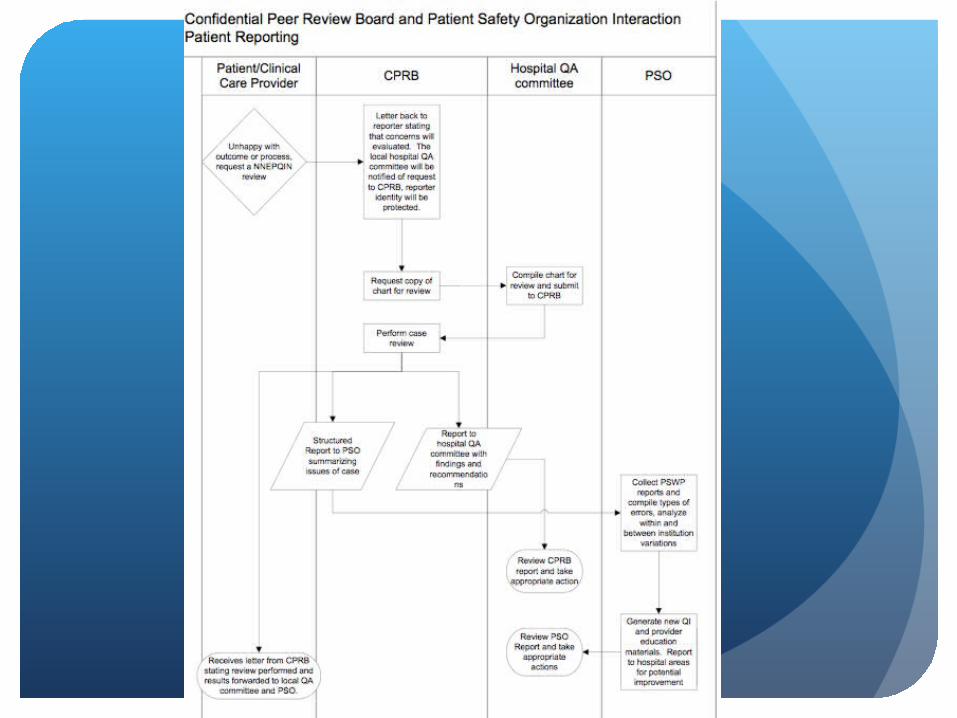
Dr. Jerome Schlachter - Confidential Peer Review Board - CPRB
Dr. Timothy Fisher – Patient Safety Organization - PSO

Why are we here?
To improve the quality and safety of health care delivery
Reduce harm to patients

Who are we?
Diverse organization committed to quality Tertiary centers Community hospitals Birth centers

Who are we?
Diverse group of providers OB/GYNs
Faculty Private practice
Family physicians
Midwives Certified Nurse Midwives Lay midwives
How do we maximize quality as PSO?
Propose that each member have a QA process in place
Establish regional guidelines
Review outcomes as consultant

Developing a Q I Program
Background Increase the likelihood of desired health outcomes
Hospitals continually evaluate care
Continuous improvement vs. punitive
Educational vs. punitive

Getting organized
Requires effective leadership
Requires cooperation by members

Developing tools
Clinical pathways Must document rationale for deviation
Quality indicators a measurable dimension
Outcomes – eg, previa Processes – eg, VBAC
provider profiles benchmarked to local, regional, national
identify trends thresholds
Developing tools
Standards, guidelines, and criteria
Eg, ACOG Practice Bulletins
Eg, departmental screening tools

Developing tools
Provider buy-in essential Clinically important Guideline credibility Target audience Enlist physician champions make guidelines easy to follow quality vs. compliance measure improvement, share data update guidelines as needed

Implementation
Leadership Define future Align people with vision Inspire members to make change Confidentiality

Medical record review
Identify outliers Provider raised issues Clinical indicators Case referrals No deficiency Opportunity for improvement
Documentation Incomplete prenatal care Inappropriate care System deficiencies
CORRECTIVE
ACTION
Formulate plan Re: hospital/staff bylaws ?Legal counsel re: due process Education Surveillance Counseling External peer review Supervision of care Probation Restriction of privileges Dismissal from department
ACOG Screening Tools
Maternal mortality
Unplanned readmission within 14 days
Maternal cardiopulmonary arrest, resuscitated
In-hospital antibiotics >24 hrs after NSVD
Unplanned removal, injury, repair of organ during surgery
Excess maternal blood loss requiring intervention

ACOG Screening Tools
Eclampsia
Delivery unattended by the responsible provider
Death of infant >500 gm
Delivery at <32 weeks without NICU
Transfer of neonate to NICU
Cesarean delivery for failure to progress

ACOG Screening Tools
Cesarean delivery for non-reassuring fetal status
Post-term pregnancy
Repeat cesarean section
Concord Hospital Indicators
Unexpected mortality
Peri-operative mortality
Miscellaneous Occurrences Req. Peer Rev.
Deep incisional infection
Organ space infection
Superficial infection
Iatrogenic injury

Concord Hospital Indicators
Post-procedure hemorrhage
Post-partum hemorrhage
Apgar < 7 @ 5 minutes
Eclampsia
Birth trauma
4th Degree Perineal Laceration

What is the future?
Encourage Institutions to establish indicators
Encourage institutions to establish OB QA Committees
Encourage individuals and institutions to seek outside peer review as needed
NNEPQIN as PSO