pulmonary embolismkonkerpdpi2019.com/download/materi_ws/workshop_1/... · • anamnesa family...
TRANSCRIPT
ISNU PRADJOKO
PULMONOLOGY DEPARTEMENT and RESPIRATORY MEDICINE
MEDICAL FACULTY of AIRLANGGA UNIVERSITY
RSUD dr. SOETOMO ACADEMIC HOSPITAL.
SURABAYA
PULMONARY EMBOLISM
KONAS SOLO 2019
INTRODUCTION
• Pulmonary embolism partial or total obstruction of
pulmonary artery circulation or branches due to
embolism or other thrombus embolism blocked blood
flow.
• Pulmonary embolism: increased pulmonary artery
pressure secondary pulmonary hypertension.
• Resulting in right ventricular hypertrophy right heart
failure (cor pulmonale).
• Difficult diagnosis broad clinical spectrum
(Burrowes, 2011; Ghaye et all, 2006; Heit, 2013)
INTRODUCTION (2)
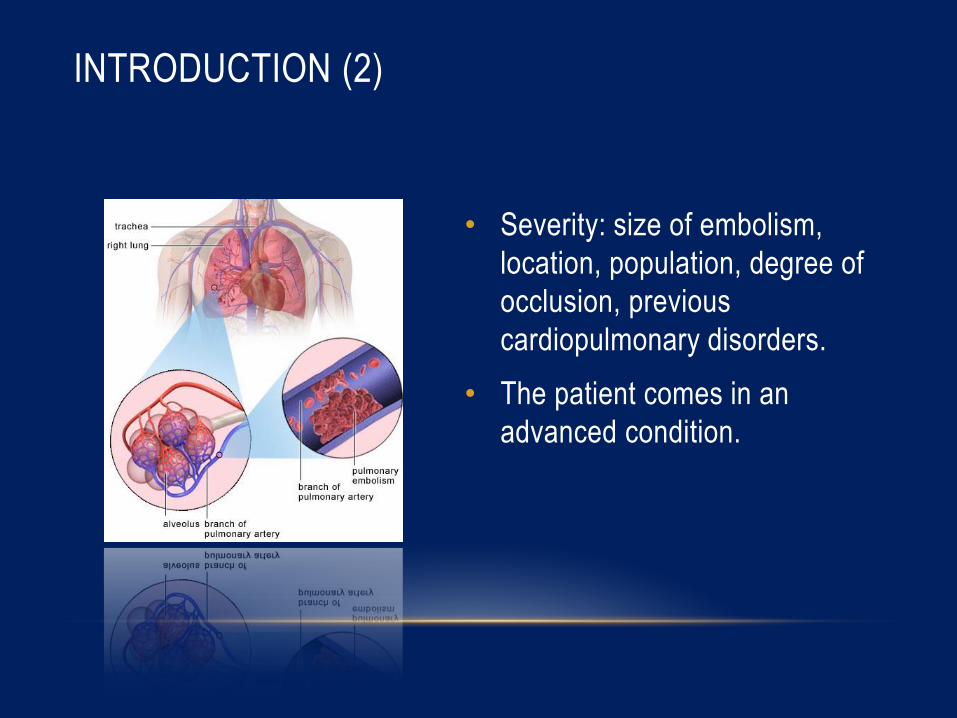
• Severity: size of embolism,
location, population, degree of
occlusion, previous
cardiopulmonary disorders.
• The patient comes in an
advanced condition.

EPIDEMIOLOGY
• Epidemiological data of pulmonary embolism difficult to
determine (asymptomatic).
• United States: 50,000 cases/year, 1 case/1,000 people/year.
• Sudden death in 20-34% of cases.
• Insidensi kematian meningkat seiring dengan usia tua (usia
>40 tahun).
(Cohen, 2007; Gruber, 2008; Konstatinides, 2014; Simon , 2010)
ETIOLOGY AND RISK FACTORS
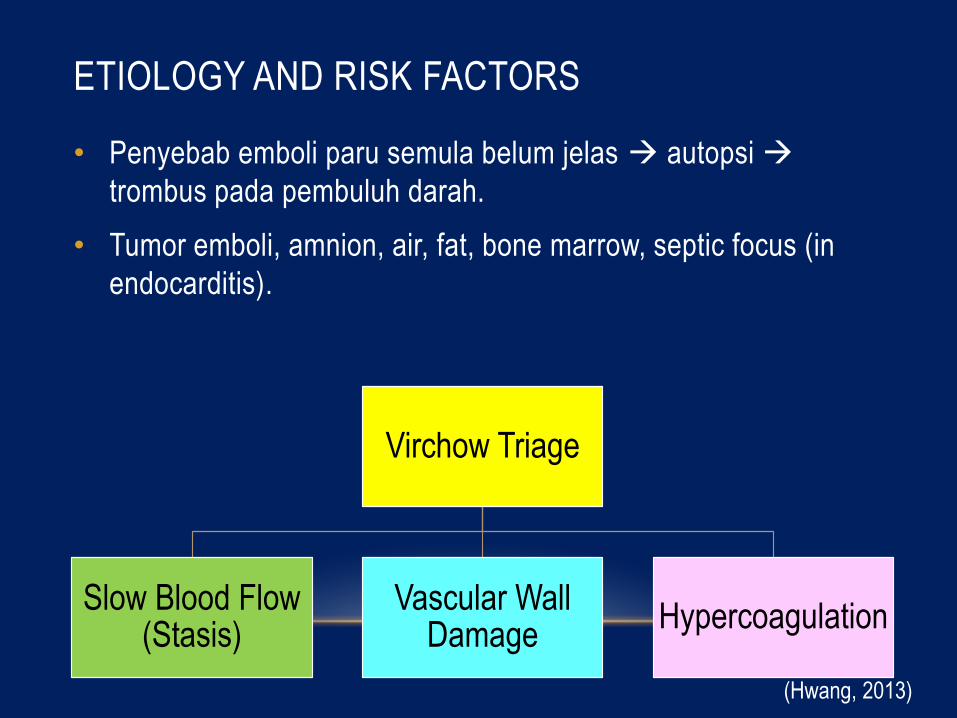
• Penyebab emboli paru semula belum jelas autopsi
trombus pada pembuluh darah.
• Tumor emboli, amnion, air, fat, bone marrow, septic focus (in
endocarditis).
Virchow Triage
Slow Blood Flow (Stasis)
Vascular Wall Damage
Hypercoagulation
(Hwang, 2013)

RISK FACTORS
Slow blood flow (stasis)
• Long period of bed rest
• Obesity
• Varicose veins
• Congestive heart failure
• Slow-flowing blood gives more chance to clot (thrombus).
(Gruber, 2008; Kostadima, 2007)
RISK FACTORS (2)
Vascular Wall Damage
• Surgery orthopedic surgery, neurosurgery, abdominal piston,
pelvis, kidney transplant or TCV surgery.
• Blood vessel trauma (injections, cardiac catheterization).
• Trauma Trauma of the lower limb and/or pelvis, spinal cord
with paralysis, head trauma, vascular trauma, use of mechanical
ventilation for more than 3 days.
• Combustio.
(Gruber, 2008; Yung, 2008)
RISK FACTORS (3)
Hypercoagulation
• Malignancies pancreatic cancer, lymphoma, brain cancer,
hepatocellular carcinoma, leukemia, colorectal cancer.
• Splenectomy with thrombocytosis.
• Use of oral contraceptives (estrogen).
• Heparin-induced thrombocytopenia.
• Disseminated intravascular coagulation (DIC).
• Pregnancy.
( Gruber, 2008; Konstatinides, 2014; Kostadima, 2007; Yung, 2008)
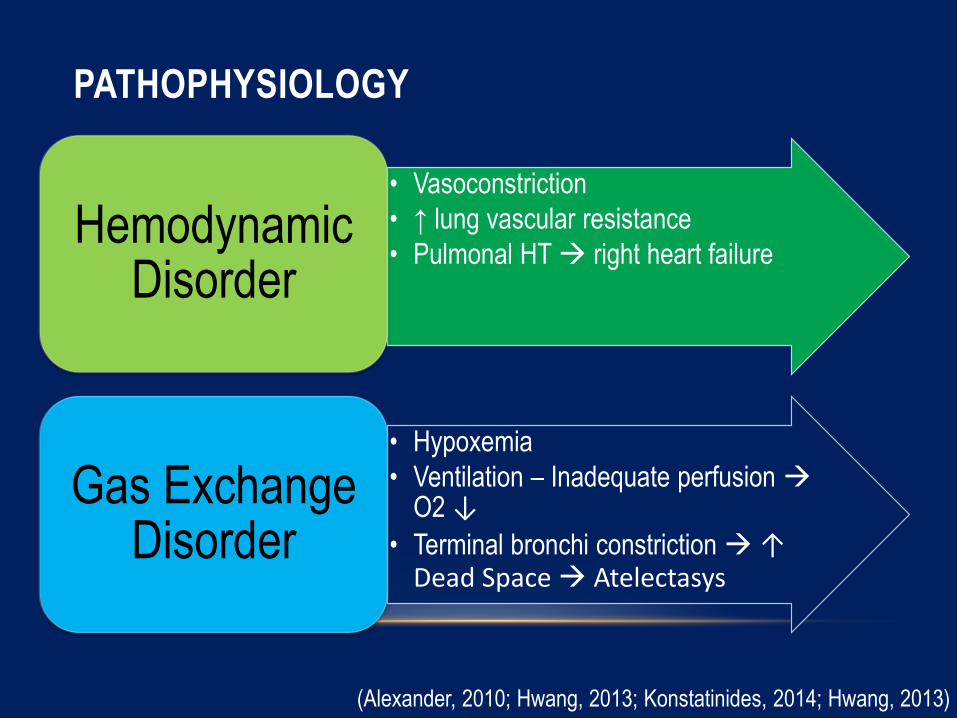
PATHOPHYSIOLOGY
• Vasoconstriction
• ↑ lung vascular resistance
• Pulmonal HT right heart failure Hemodynamic
Disorder
• Hypoxemia
• Ventilation – Inadequate perfusion O2 ↓
• Terminal bronchi constriction ↑ Dead Space Atelectasys
Gas Exchange Disorder
(Alexander, 2010; Hwang, 2013; Konstatinides, 2014; Hwang, 2013)

Thrombus Journey
Loose vein thrombus
Thromboembolism will follow
venous flow and enter the
pulmonary artery circulation
Pulmonary artery
blockage
Increased pulmonary
artery pressure
Vasoconstrictor release
(serotonin)
Pulmonary artery hypertension
Right ventricular pressure
Fedullo PF, 2005.
Impaired ventricular filling
Cardiac output
Lung infarction
Ischemia, cardiogenic shock,
and death
CLINICAL APPEARANCE
• Dispnea, hemoptoe, wheezing, chest pain.
• Chest pain pleural irritation due to pulmonary infarction.
• Anamnesa family history of venous thromboembolism,
accompanying medical conditions, and treatment history.
• Scoring system Well’s score helps diagnosing PE.
(Gruber, 2008; Hwang, 2013; Konstatinides, 2014)

DIAGNOSIS
• Clinical symptoms sudden shortness of breath, chest pain
(pleuritic pain) or hemoptysis suspicion of pulmonary
embolism/pulmonary infarction.
• ECGs in leads V1-V4 have T-wave inversions in anterior leads
right ventricular hypertrophy, pulmonary thromboembolism.
• Deep S-waves in Lead I, Q-waves in Lead III, and inversion of
T-waves in Lead III.
• Conduction and rhythm disorders atrial fibrillation/right
bundle branch block acute pulmonary embolism.
(Konstatindes, 2014; Kostadima, 2007; Yung, 2008)
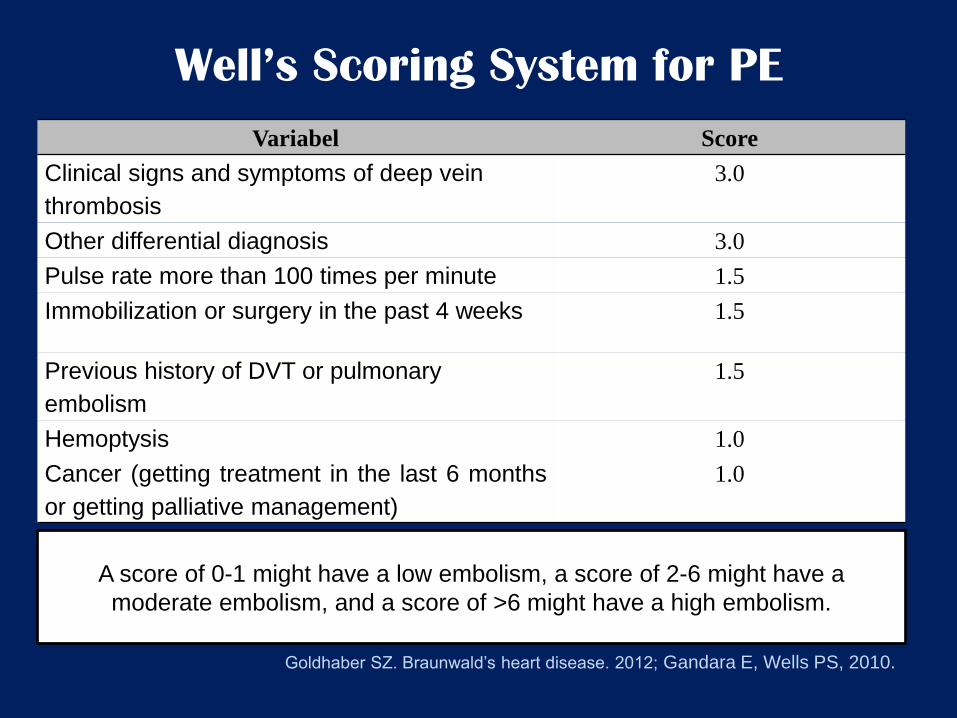
Well’s Scoring System for PE
Variabel Score
Clinical signs and symptoms of deep vein
thrombosis
3.0
Other differential diagnosis 3.0
Pulse rate more than 100 times per minute 1.5
Immobilization or surgery in the past 4 weeks 1.5
Previous history of DVT or pulmonary
embolism
1.5
Hemoptysis 1.0
Cancer (getting treatment in the last 6 months
or getting palliative management)
1.0
A score of 0-1 might have a low embolism, a score of 2-6 might have a
moderate embolism, and a score of >6 might have a high embolism.
Goldhaber SZ. Braunwald’s heart disease. 2012; Gandara E, Wells PS, 2010.
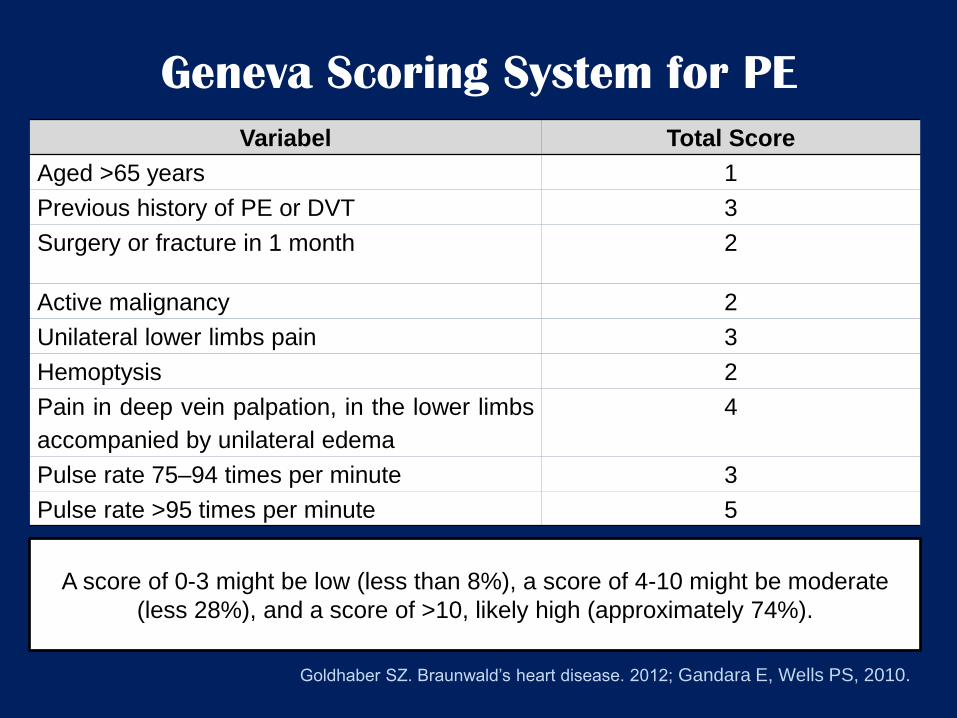
Geneva Scoring System for PE
Variabel Total Score
Aged >65 years 1
Previous history of PE or DVT 3
Surgery or fracture in 1 month 2
Active malignancy 2
Unilateral lower limbs pain 3
Hemoptysis 2
Pain in deep vein palpation, in the lower limbs
accompanied by unilateral edema
4
Pulse rate 75–94 times per minute 3
Pulse rate >95 times per minute 5
A score of 0-3 might be low (less than 8%), a score of 4-10 might be moderate
(less 28%), and a score of >10, likely high (approximately 74%).
Goldhaber SZ. Braunwald’s heart disease. 2012; Gandara E, Wells PS, 2010.
(Kostadima, 2007)
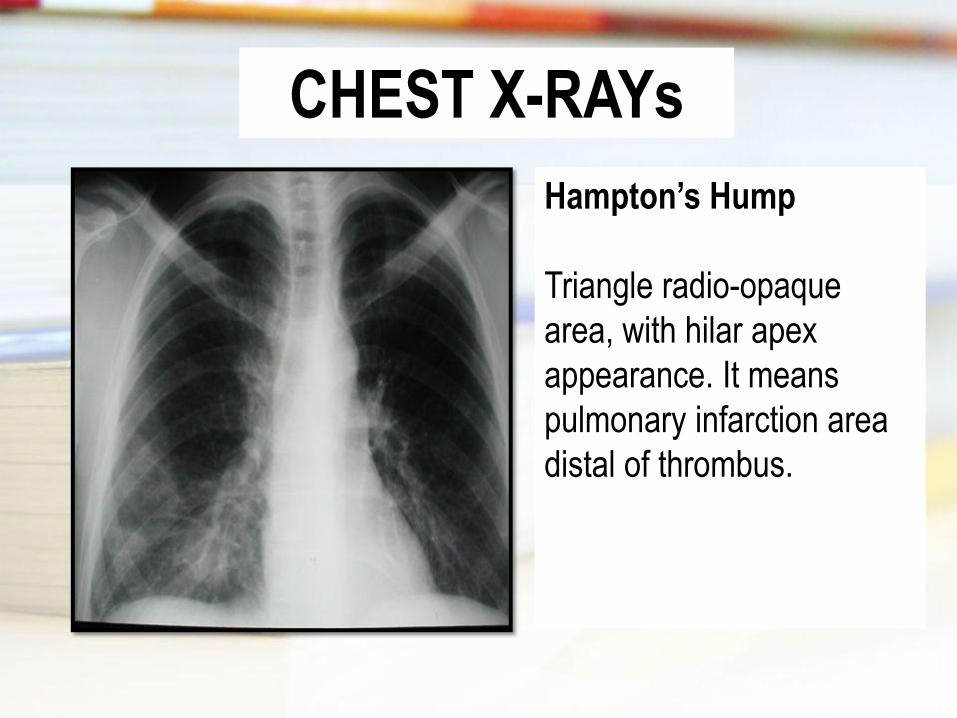
CHEST X-RAYs
Hampton’s Hump
Triangle radio-opaque
area, with hilar apex
appearance. It means
pulmonary infarction area
distal of thrombus.
(Kostadima, 2007)
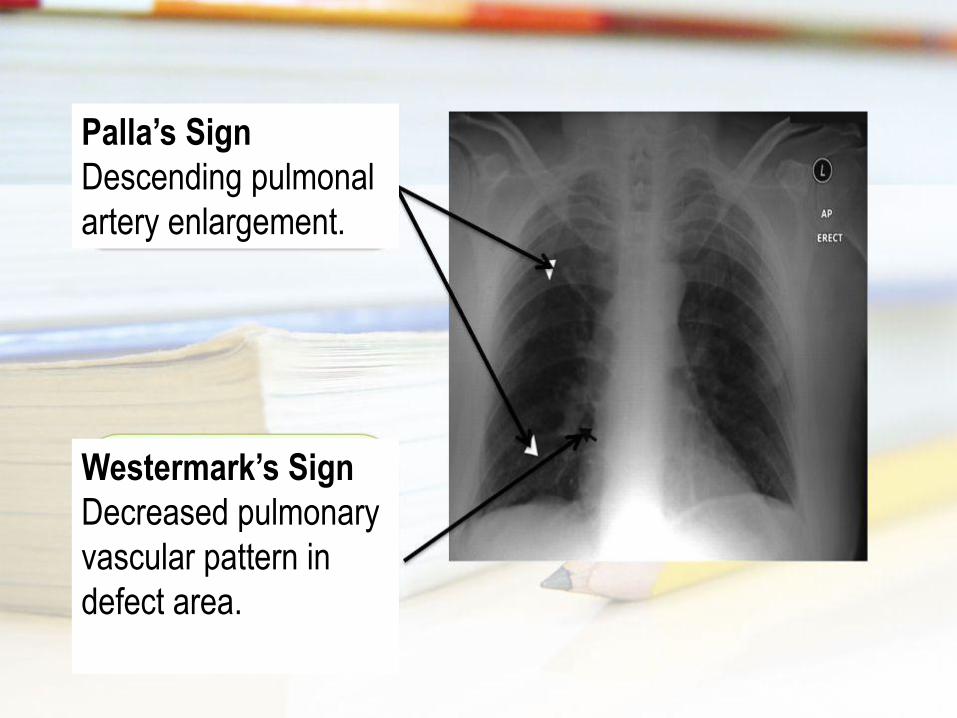
Palla’s Sign
Descending pulmonal
artery enlargement.
Westermark’s Sign
Decreased pulmonary
vascular pattern in
defect area.
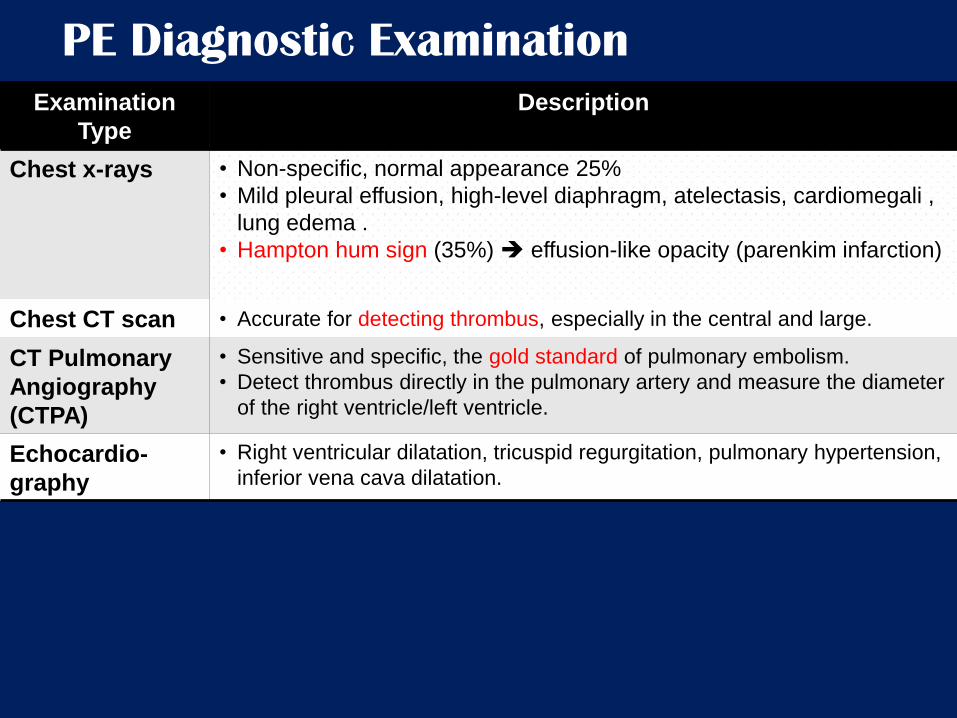
PE Diagnostic Examination
Examination
Type
Description
Chest x-rays • Non-specific, normal appearance 25%
• Mild pleural effusion, high-level diaphragm, atelectasis, cardiomegali ,
lung edema .
• Hampton hum sign (35%) effusion-like opacity (parenkim infarction)
Chest CT scan • Accurate for detecting thrombus, especially in the central and large.
CT Pulmonary
Angiography
(CTPA)
• Sensitive and specific, the gold standard of pulmonary embolism.
• Detect thrombus directly in the pulmonary artery and measure the diameter
of the right ventricle/left ventricle.
Echocardio-
graphy
• Right ventricular dilatation, tricuspid regurgitation, pulmonary hypertension,
inferior vena cava dilatation.
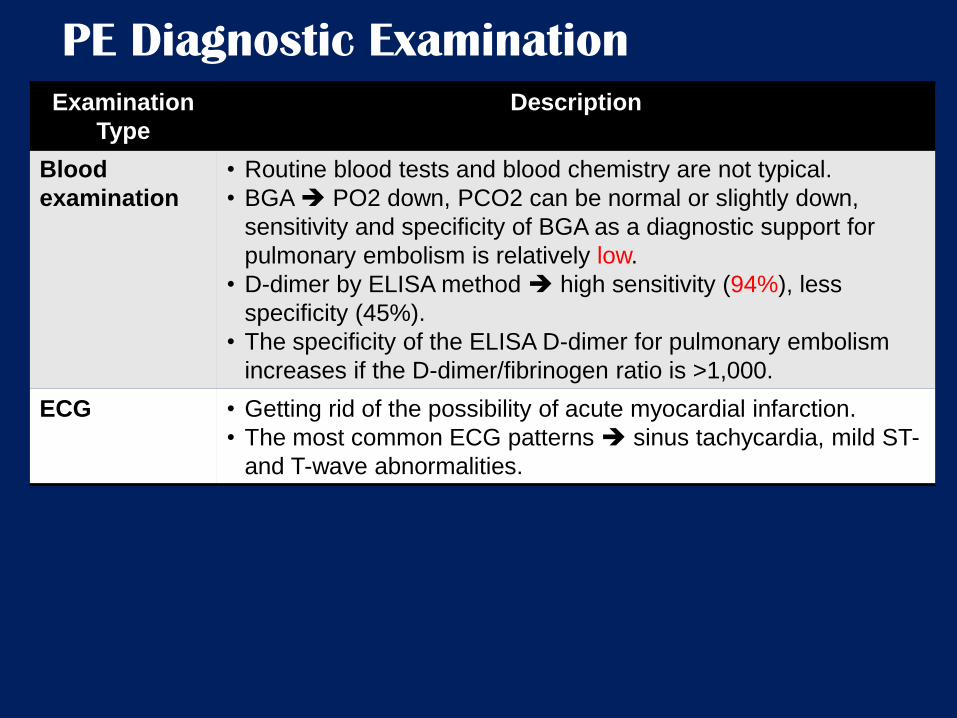
PE Diagnostic Examination
Examination
Type
Description
Blood
examination
• Routine blood tests and blood chemistry are not typical.
• BGA PO2 down, PCO2 can be normal or slightly down,
sensitivity and specificity of BGA as a diagnostic support for
pulmonary embolism is relatively low.
• D-dimer by ELISA method high sensitivity (94%), less
specificity (45%).
• The specificity of the ELISA D-dimer for pulmonary embolism
increases if the D-dimer/fibrinogen ratio is >1,000.
ECG • Getting rid of the possibility of acute myocardial infarction.
• The most common ECG patterns sinus tachycardia, mild ST-
and T-wave abnormalities.
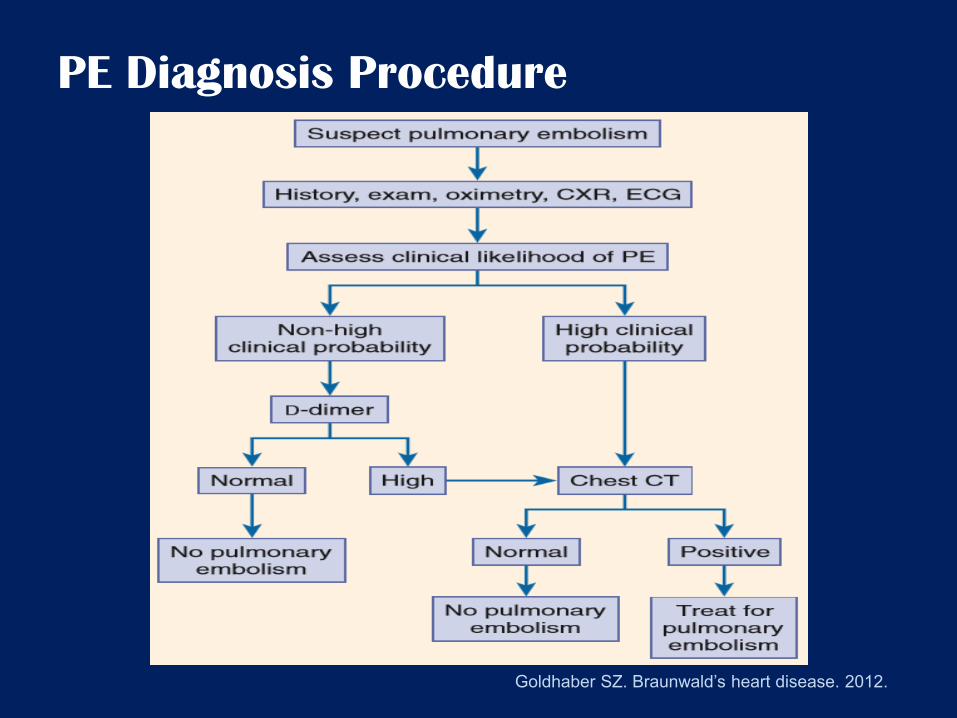
PE Diagnosis Procedure
Goldhaber SZ. Braunwald’s heart disease. 2012.
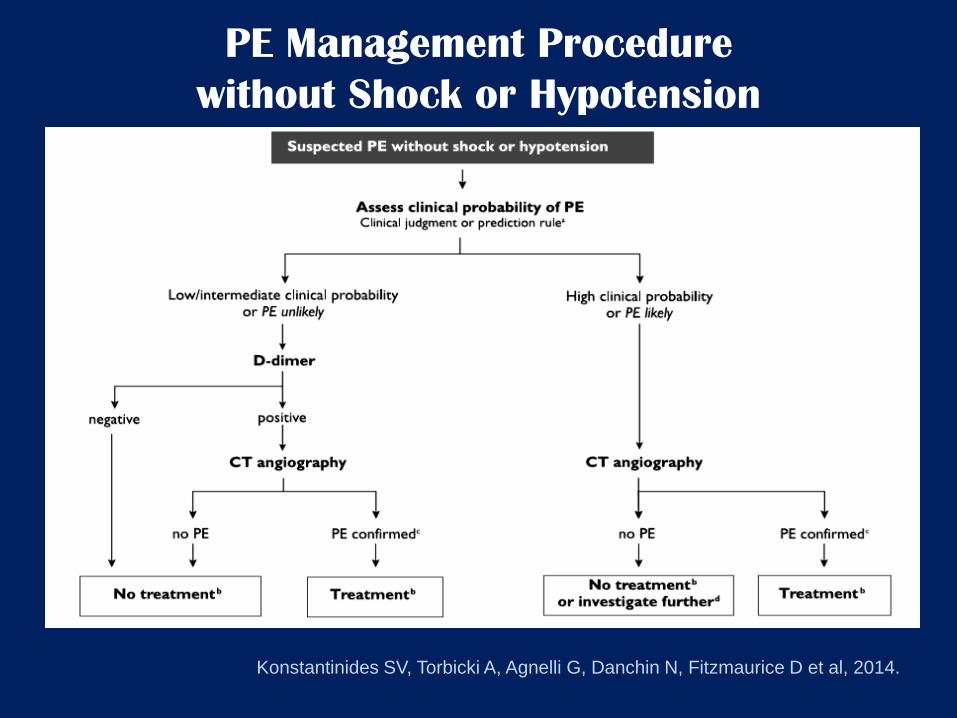
PE Management Procedure
without Shock or Hypotension
Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D et al, 2014.
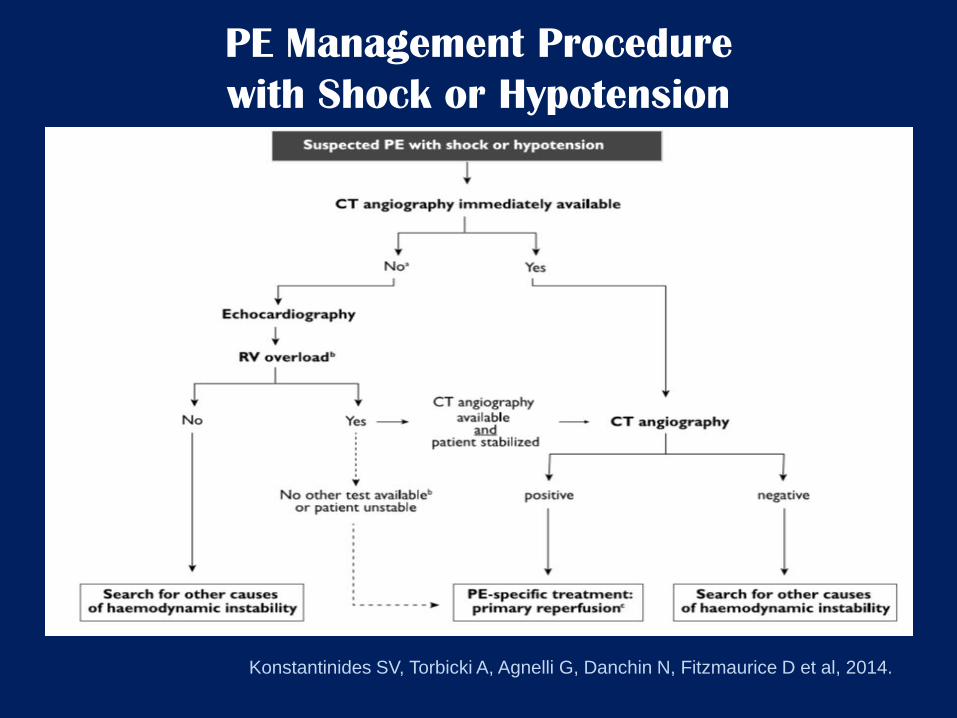
PE Management Procedure
with Shock or Hypotension
Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D et al, 2014.
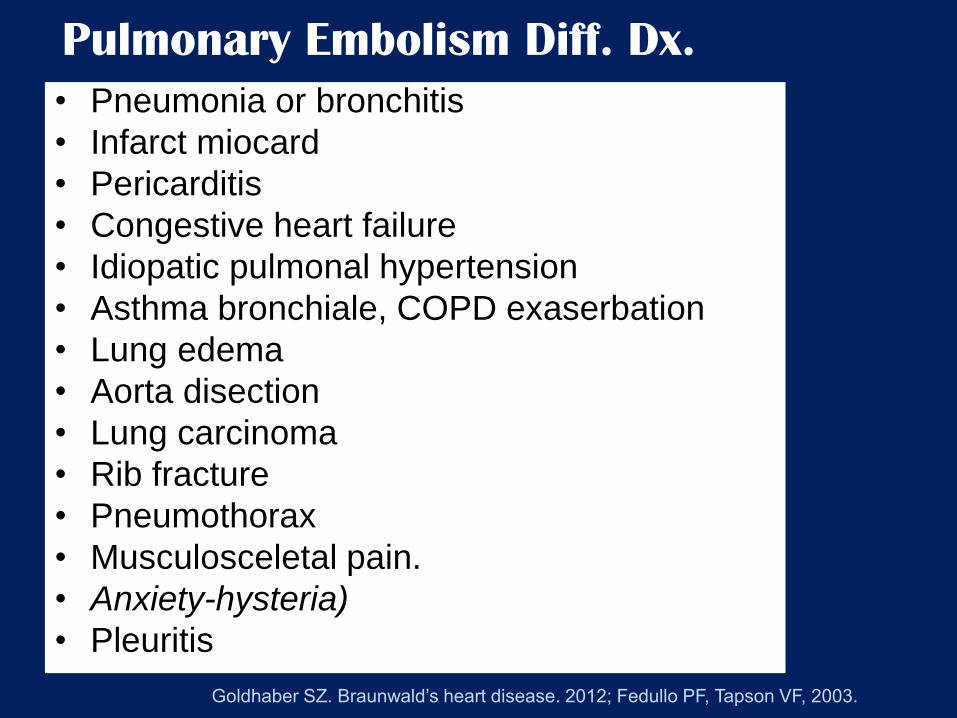
Pulmonary Embolism Diff. Dx.
• Pneumonia or bronchitis
• Infarct miocard
• Pericarditis
• Congestive heart failure
• Idiopatic pulmonal hypertension
• Asthma bronchiale, COPD exaserbation
• Lung edema
• Aorta disection
• Lung carcinoma
• Rib fracture
• Pneumothorax
• Musculosceletal pain.
• Anxiety-hysteria)
• Pleuritis
Goldhaber SZ. Braunwald’s heart disease. 2012; Fedullo PF, Tapson VF, 2003.
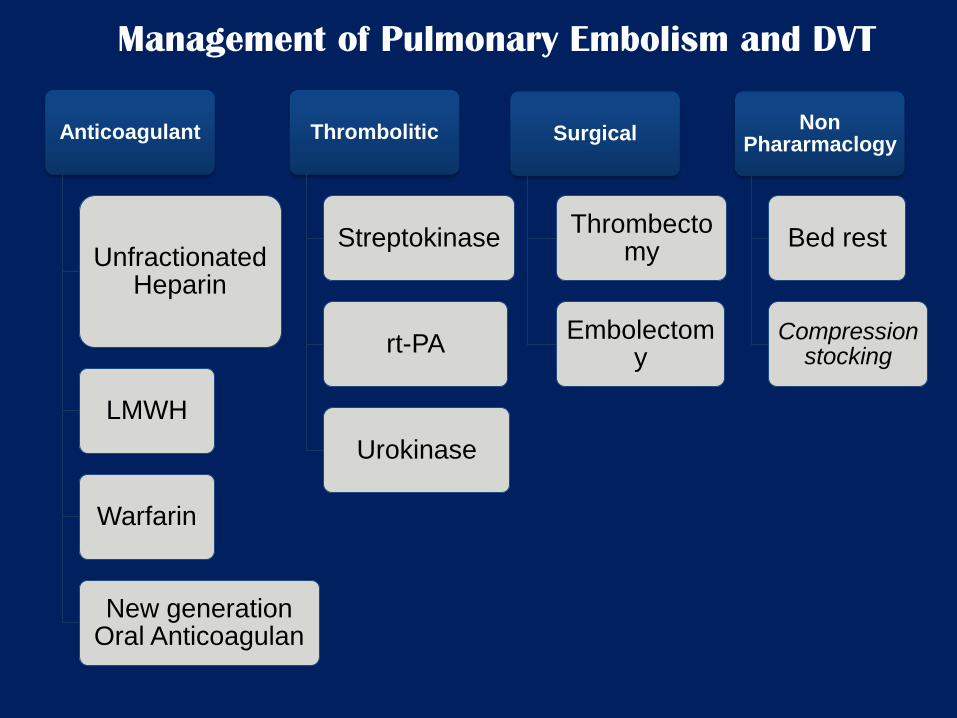
Management of Pulmonary Embolism and DVT
Anticoagulant
Unfractionated Heparin
LMWH
Warfarin
New generation Oral Anticoagulan
Thrombolitic
Streptokinase
rt-PA
Urokinase
Surgical
Thrombectomy
Embolectomy
Non Phararmaclogy
Bed rest
Compression stocking
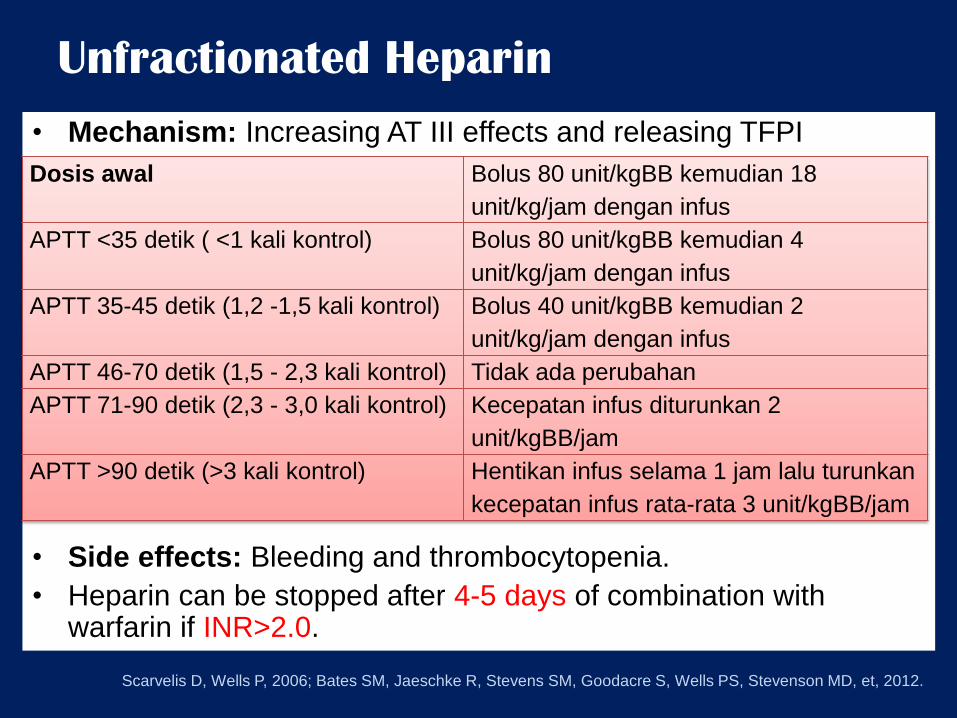
Unfractionated Heparin
• Mechanism: Increasing AT III effects and releasing TFPI
• Side effects: Bleeding and thrombocytopenia.
• Heparin can be stopped after 4-5 days of combination with warfarin if INR>2.0.
Dosis awal Bolus 80 unit/kgBB kemudian 18
unit/kg/jam dengan infus
APTT <35 detik ( <1 kali kontrol) Bolus 80 unit/kgBB kemudian 4
unit/kg/jam dengan infus
APTT 35-45 detik (1,2 -1,5 kali kontrol) Bolus 40 unit/kgBB kemudian 2
unit/kg/jam dengan infus
APTT 46-70 detik (1,5 - 2,3 kali kontrol) Tidak ada perubahan
APTT 71-90 detik (2,3 - 3,0 kali kontrol) Kecepatan infus diturunkan 2
unit/kgBB/jam
APTT >90 detik (>3 kali kontrol) Hentikan infus selama 1 jam lalu turunkan
kecepatan infus rata-rata 3 unit/kgBB/jam
Scarvelis D, Wells P, 2006; Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et, 2012.
Low-Molecular-Weight Heparin (LMWH)
Biological half-life > unfractionated heparin
Does not require laboratory monitoring
Combination with wafarin for 4-5 days stopped if INR>2
DVT therapy dose 1 mg/kg 2x/day or 1.5mg/kg 1x/day.
Side effects of thrombocytopenia and osteoporosis LMWH <<UFH
Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D et al, 2014; JCS Guidelines 2009; Scarvelis D, Wells P,
2006; Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et al , 2012.
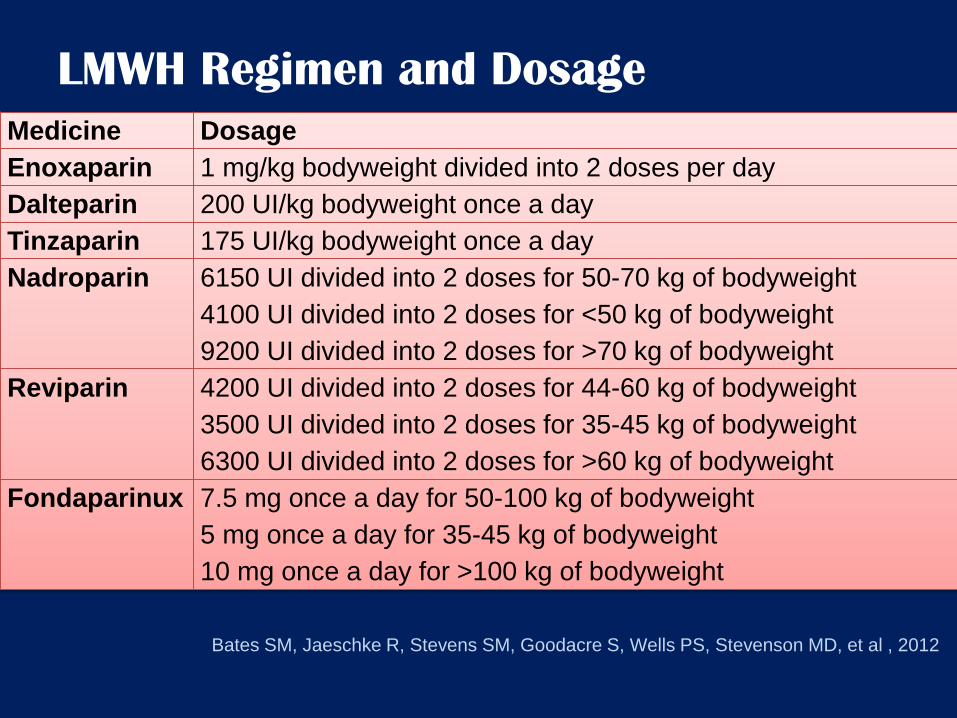
LMWH Regimen and Dosage
Medicine Dosage
Enoxaparin 1 mg/kg bodyweight divided into 2 doses per day
Dalteparin 200 UI/kg bodyweight once a day
Tinzaparin 175 UI/kg bodyweight once a day
Nadroparin 6150 UI divided into 2 doses for 50-70 kg of bodyweight
4100 UI divided into 2 doses for <50 kg of bodyweight
9200 UI divided into 2 doses for >70 kg of bodyweight
Reviparin 4200 UI divided into 2 doses for 44-60 kg of bodyweight
3500 UI divided into 2 doses for 35-45 kg of bodyweight
6300 UI divided into 2 doses for >60 kg of bodyweight
Fondaparinux 7.5 mg once a day for 50-100 kg of bodyweight
5 mg once a day for 35-45 kg of bodyweight
10 mg once a day for >100 kg of bodyweight
Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et al , 2012
Warfarin
Acute anticoagulation
The standard dose of warfarin is 5 mg/day, the dose is adjusted every three to seven days to get an INR value of between 2-3
Dosage is monitored with prothrombin time or INR
For uncomplicated DVT, 3-6 months of therapy
Contraindications: Cerebral hemorrhage, trauma and surgery
Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galie N, Pruszczyk P, et al, 2008; Scarvelis D, Wells P,
2006.
Thrombolytic
• Breaking newly formed blood clots and restoring
venous patency faster than anticoagulants.
• Thrombolytic therapy in acute episodes of DVT
can reduce the risk of recurrence.
Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galie N, Pruszczyk P, et al, 2008;
Scarvelis D, Wells P, 2006.
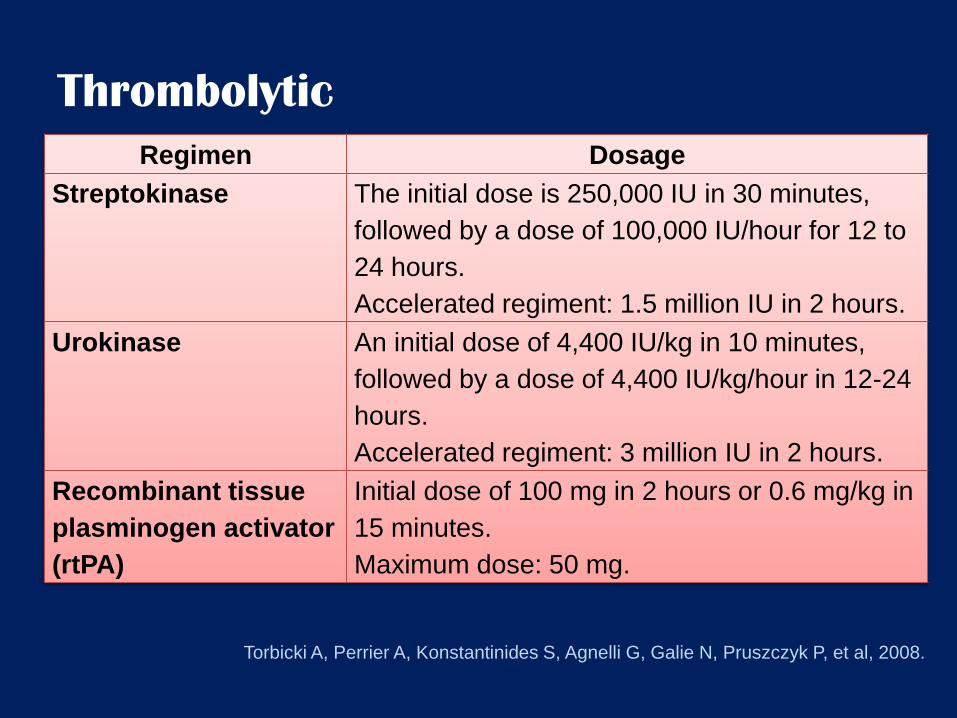
Thrombolytic
Regimen Dosage
Streptokinase The initial dose is 250,000 IU in 30 minutes,
followed by a dose of 100,000 IU/hour for 12 to
24 hours.
Accelerated regiment: 1.5 million IU in 2 hours.
Urokinase An initial dose of 4,400 IU/kg in 10 minutes,
followed by a dose of 4,400 IU/kg/hour in 12-24
hours.
Accelerated regiment: 3 million IU in 2 hours.
Recombinant tissue
plasminogen activator
(rtPA)
Initial dose of 100 mg in 2 hours or 0.6 mg/kg in
15 minutes.
Maximum dose: 50 mg.
Torbicki A, Perrier A, Konstantinides S, Agnelli G, Galie N, Pruszczyk P, et al, 2008.
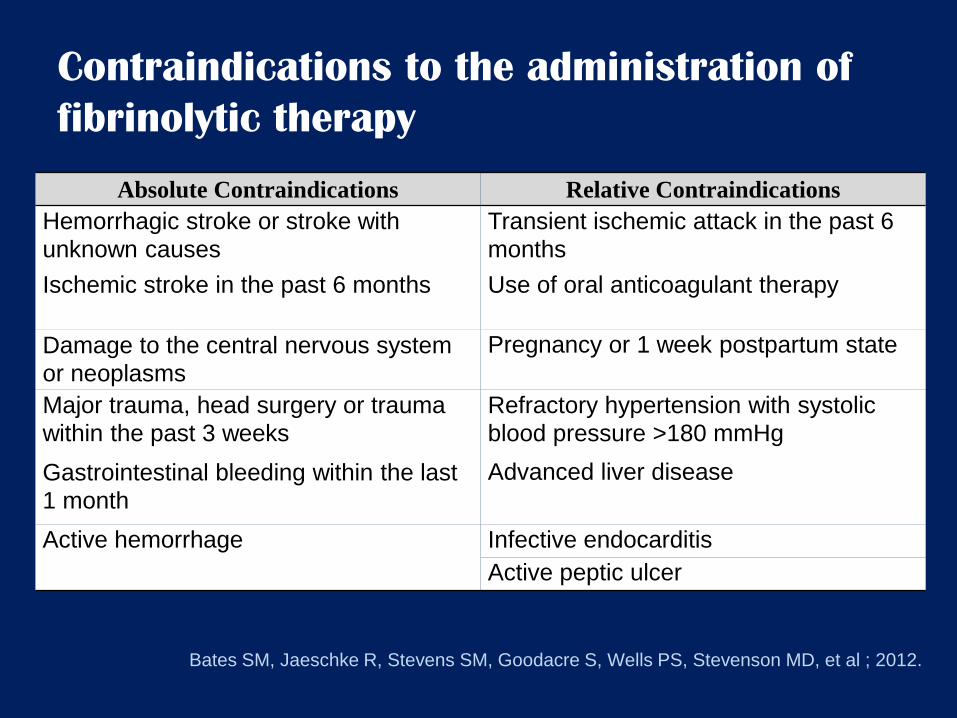
Contraindications to the administration of
fibrinolytic therapy
Absolute Contraindications Relative Contraindications
Hemorrhagic stroke or stroke with
unknown causes Transient ischemic attack in the past 6
months
Ischemic stroke in the past 6 months Use of oral anticoagulant therapy
Damage to the central nervous system
or neoplasms Pregnancy or 1 week postpartum state
Major trauma, head surgery or trauma
within the past 3 weeks Refractory hypertension with systolic
blood pressure >180 mmHg
Gastrointestinal bleeding within the last
1 month Advanced liver disease
Active hemorrhage Infective endocarditis
Active peptic ulcer
Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et al ; 2012.
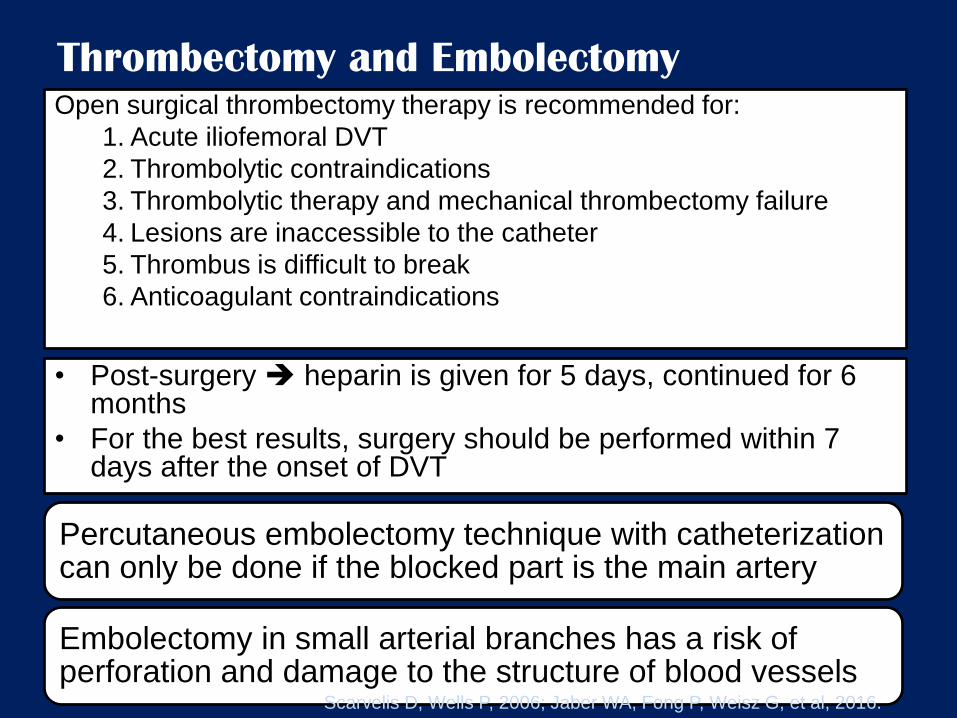
Thrombectomy and Embolectomy Open surgical thrombectomy therapy is recommended for:
1. Acute iliofemoral DVT
2. Thrombolytic contraindications
3. Thrombolytic therapy and mechanical thrombectomy failure
4. Lesions are inaccessible to the catheter
5. Thrombus is difficult to break
6. Anticoagulant contraindications
• Post-surgery heparin is given for 5 days, continued for 6 months
• For the best results, surgery should be performed within 7 days after the onset of DVT
Percutaneous embolectomy technique with catheterization can only be done if the blocked part is the main artery
Embolectomy in small arterial branches has a risk of perforation and damage to the structure of blood vessels
Scarvelis D, Wells P, 2006; Jaber WA, Fong P, Weisz G, et al, 2016.
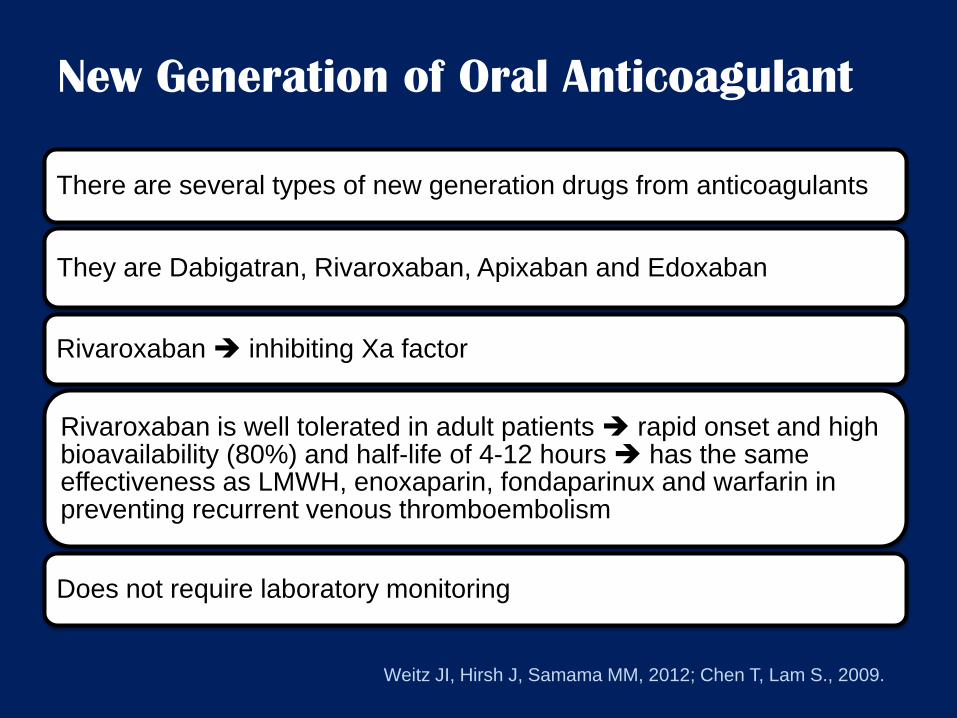
New Generation of Oral Anticoagulant
There are several types of new generation drugs from anticoagulants
They are Dabigatran, Rivaroxaban, Apixaban and Edoxaban
Rivaroxaban inhibiting Xa factor
Rivaroxaban is well tolerated in adult patients rapid onset and high bioavailability (80%) and half-life of 4-12 hours has the same effectiveness as LMWH, enoxaparin, fondaparinux and warfarin in preventing recurrent venous thromboembolism
Does not require laboratory monitoring
Weitz JI, Hirsh J, Samama MM, 2012; Chen T, Lam S., 2009.
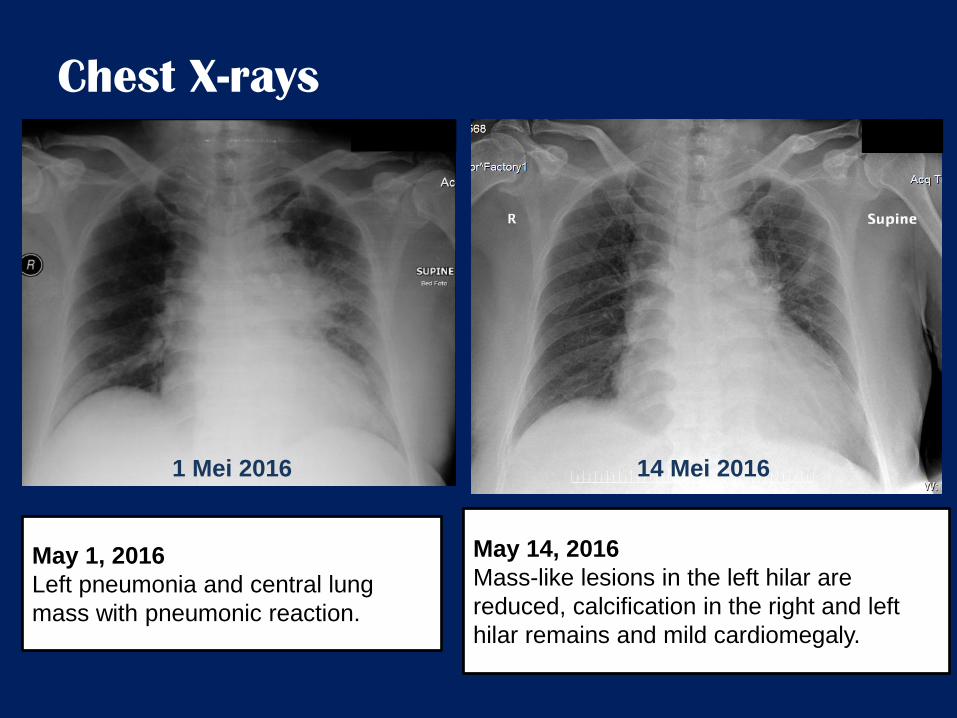
Chest X-rays
1 Mei 2016 5 Mei 2016
May 1, 2016
Left pneumonia and central lung
mass with pneumonic reaction.
May 14, 2016
Mass-like lesions in the left hilar are
reduced, calcification in the right and left
hilar remains and mild cardiomegaly.
14 Mei 2016
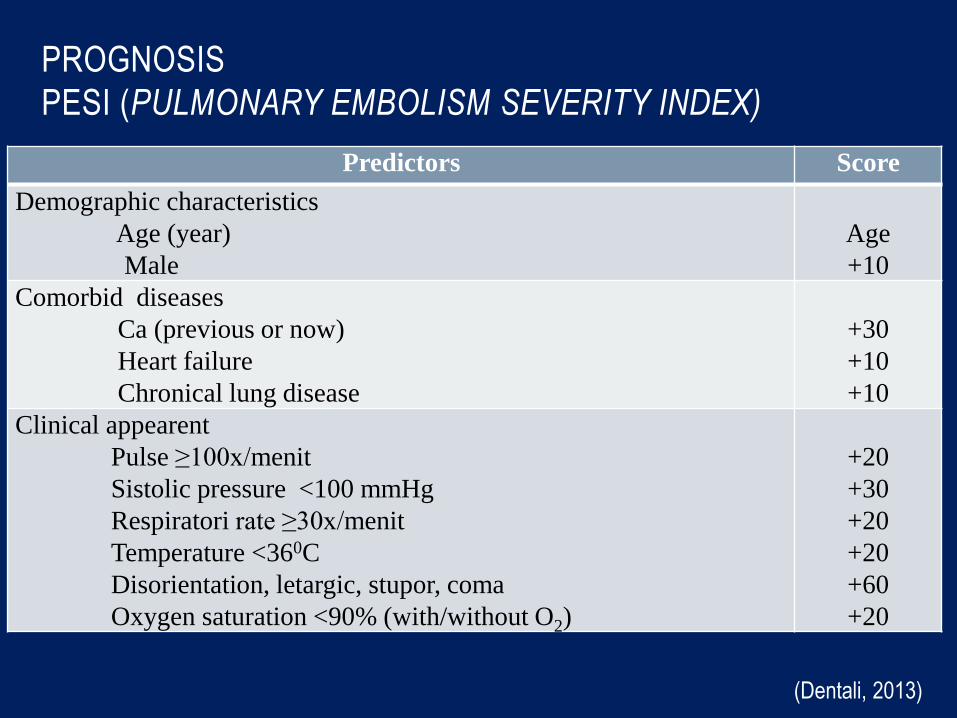
PROGNOSIS
PESI (PULMONARY EMBOLISM SEVERITY INDEX)
•
Predictors Score
Demographic characteristics Age (year) Male
Age +10
Comorbid diseases Ca (previous or now) Heart failure Chronical lung disease
+30 +10 +10
Clinical appearent Pulse ≥100x/menit Sistolic pressure <100 mmHg Respiratori rate ≥30x/menit Temperature <360C Disorientation, letargic, stupor, coma Oxygen saturation <90% (with/without O2)
+20 +30 +20 +20 +60 +20
(Dentali, 2013)
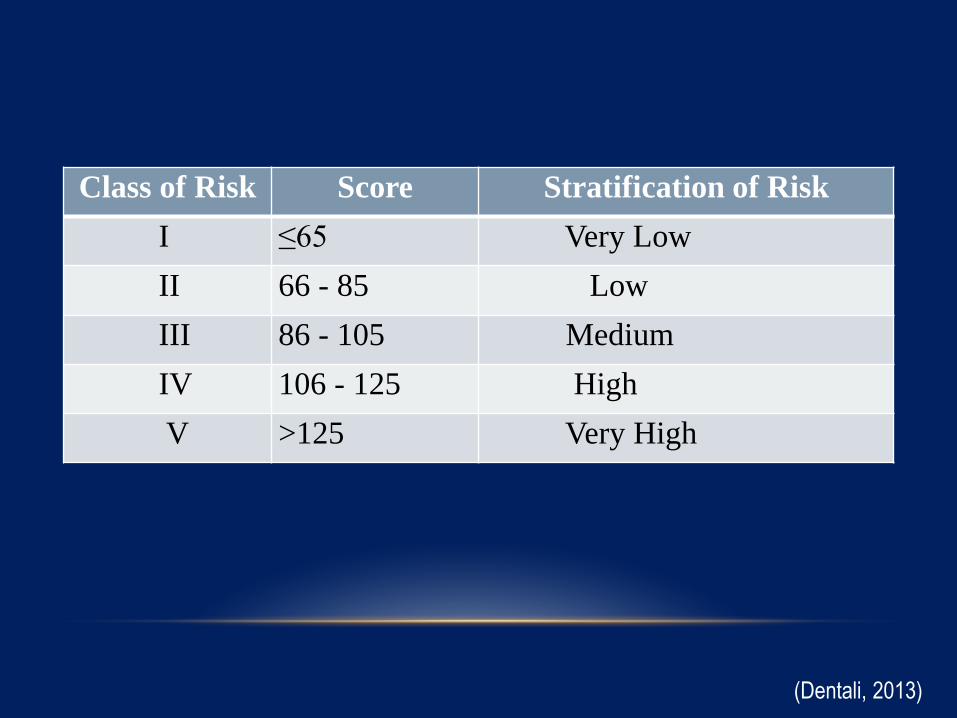
Class of Risk Score Stratification of Risk
I ≤65 Very Low
II 66 - 85 Low
III 86 - 105 Medium
IV 106 - 125 High
V >125 Very High
(Dentali, 2013)
TAKE HOME MESSAGES
• Pulmonary embolism pulmonary artery obstruction caused
by movement of emboli/thrombus.
• Risk factors immobilisation, obesity, surgery, trauma,
malignancy, oral contraception and chemotherapy.
• Clinical symptoms variation complex diagnosis.
• Dx Well’s score + advanced diagnostic finding.
• Management anticoagulant and thrombolytic.
• Prognose is good if in good management. Bad prognose if in
advanced stage.
XIE -XIE