published by elsevier science inc. pii s0002 …loewen/medicine/gim residents core... · clinical...
TRANSCRIPT

CLINICAL REVIEWS
Idiopathic Acute Recurrent PancreatitisMichael J. Levy, M.D., and Joseph E. Geenen, M.D.The Mayo Clinic, Rochester, Minnesota; and The Pancreatic Biliary Center, St. Luke’s Medical Center,Milwaukee, Wisconsin
ABSTRACT
Acute recurrent pancreatitis (ARP) results most commonlyfrom alcohol abuse or gallstone disease. Initial evaluationfails to detect the cause of ARP in 10–30% of patients, andas a result the diagnosis of “idiopathic” ARP is given. Inthese patients, a more extensive evaluation including spe-cialized labs, ERCP, endoscopic ultrasound, or magneticresonance cholangiopancreatography typically leads to adiagnosis of microlithiasis, sphincter of Oddi dysfunction,or pancreas divisum. Less commonly, hereditary pancreati-tis, cystic fibrosis, a choledochocele, annular pancreas, ananomalous pancreatobiliary junction, pancreatobiliary tu-mors, or chronic pancreatitis are diagnosed. Determining theetiology is important, as it helps to direct therapy, limitsfurther unnecessary evaluation, and may improve a patient’slong term prognosis. (Am J Gastroenterol 2001;96:2540–2555. © 2001 by Am. Coll. of Gastroenterology)
INTRODUCTION
Acute pancreatitis is an inflammatory process of the pan-creas that can affect peripancreatic tissues and distant sites.An etiology can be found in most patients after an attack ofacute pancreatitis, with gallstone disease and alcohol abusemost often implicated (Table 1). When patients have morethan one clinical episode of acute pancreatitis they are giventhe diagnosis of acute recurrent pancreatitis (ARP). Mostcauses of acute pancreatitis can lead to recurrent disease ifthe underlying factor remains uncorrected (1, 2).
The etiology of ARP is found in 70–90% of patients afteran initial evaluation, which includes a thorough history,physical exam, routine labs, and transabdominal ultrasoundor CT (Table 2). In the 10–30% of patients in whom theinitial evaluation fails to reveal an etiology, the diagnosis ofidiopathic ARP (IARP) is applied (1, 3–5). The extent of theevaluation impacts the frequency with which an etiologycan be found, and in turn how often the labelidiopathic canbe applied. Evaluation and therapy is important because�50% of untreated patients with IARP experience recurrentepisodes that may lead to chronic pancreatitis (1, 6).
INITIAL EVALUATION OF ACUTE PANCREATITIS
Acute pancreatitis is diagnosed in the proper clinical settingwith the aid of laboratory values and imaging studies. Pa-
tients may present with acute epigastric pain, nausea, vom-iting, fever, and tachycardia. Laboratory analysis usuallyreveals elevated pancreatic enzymes and leukocytosis. Ab-dominal ultrasound and CT help support the diagnosis andexclude other causes. After confirmation of the presence ofacute pancreatitis, the focus shifts to determining the etiol-ogy. The initial evaluation includes a search for evidence ofalcohol abuse, drug-induced pancreatitis, and a family his-tory of pancreatitis, and other clues that may suggest theorigin.
The serum amylase level is used to help establish thediagnosis of pancreatitis and may be predictive of the un-derlying pathology. Pancreatitis resulting from gallstones,microlithiasis, or drugs is typically associated with a greaterelevation in amylase than lipase (7, 8). The amylase level, ascompared to lipase, tends to be lower in alcoholic pancre-atitis, hypertriglyceridemia-induced pancreatitis, neoplasia,and chronic pancreatitis (7, 8). Lipase elevation is morespecific for pancreatitis than amylase, and the level remainselevated longer, but the level is not predictive of the etiology(9). The ratio of lipase to amylase may help distinguishalcoholic from nonalcoholic pancreatitis, with an increasedratio suggesting alcohol-induced disease (7, 8). Of note, theamylase and lipase levels do not correlate with diseaseseverity and they are not useful for determining prognosis.
Liver function tests are routinely measured and may beelevated because of biliary obstruction resulting from gall-stones, microlithiasis, a choledochocele, neoplasia of theampulla or pancreas, or sphincter of Oddi dysfunction(SOD). Liver function tests may also increase as a result ofpancreatic head edema, inflammation, or pseudocyst forma-tion. A 3-fold or greater increase in the ALAT level isgenerally regarded as the best indicator of gallstone-inducedpancreatitis (10). One study, however, noted that the bestindicator of bile duct stones is a serum total bilirubin� 1.35mg/dl on the second day of hospitalization (11). Although itis unclear which laboratory parameter is the most predictive,both may be used to help assess the presence of gallstone-induced pancreatitis in an individual patient. Metaboliccauses of pancreatitis should be excluded by checking theserum calcium and triglyceride levels. These values shouldbe measured soon after admission, or well after resolution ofthe pancreatitis, because of the drop in calcium and triglyc-eride levels that can occur during hospitalization (12).
Transabdominal ultrasound is a simple, inexpensive, and
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 9, 2001© 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00Published by Elsevier Science Inc. PII S0002-9270(01)02661-2
highly sensitive procedure for evaluating the biliary tract(13). CT more accurately delineates the pancreas and mayalso help identify the cause, assess the severity, and detectcomplications of pancreatitis (14). Some recommend per-forming CT only when the first attack is severe, when thecourse is complicated, or in the elderly. Patients not scannedduring the first episode are generally scanned with theirsecond attack regardless of age or disease severity. How-ever, we believe that the yield is great enough to justify a CTin all patients during their first episode.
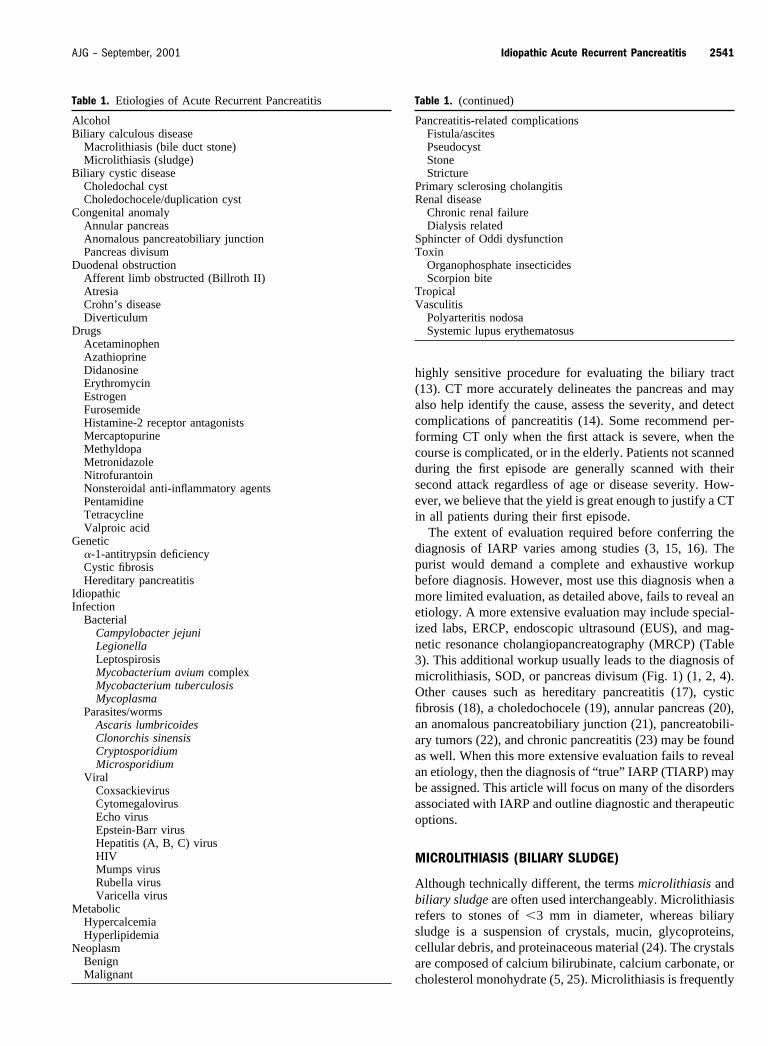
The extent of evaluation required before conferring thediagnosis of IARP varies among studies (3, 15, 16). Thepurist would demand a complete and exhaustive workupbefore diagnosis. However, most use this diagnosis when amore limited evaluation, as detailed above, fails to reveal anetiology. A more extensive evaluation may include special-ized labs, ERCP, endoscopic ultrasound (EUS), and mag-netic resonance cholangiopancreatography (MRCP) (Table3). This additional workup usually leads to the diagnosis ofmicrolithiasis, SOD, or pancreas divisum (Fig. 1) (1, 2, 4).Other causes such as hereditary pancreatitis (17), cysticfibrosis (18), a choledochocele (19), annular pancreas (20),an anomalous pancreatobiliary junction (21), pancreatobili-ary tumors (22), and chronic pancreatitis (23) may be foundas well. When this more extensive evaluation fails to revealan etiology, then the diagnosis of “ true” IARP (TIARP) maybe assigned. This article will focus on many of the disordersassociated with IARP and outline diagnostic and therapeuticoptions.
MICROLITHIASIS (BILIARY SLUDGE)
Although technically different, the terms microlithiasis andbiliary sludge are often used interchangeably. Microlithiasisrefers to stones of �3 mm in diameter, whereas biliarysludge is a suspension of crystals, mucin, glycoproteins,cellular debris, and proteinaceous material (24). The crystalsare composed of calcium bilirubinate, calcium carbonate, orcholesterol monohydrate (5, 25). Microlithiasis is frequently
Table 1. (continued)
Pancreatitis-related complicationsFistula/ascitesPseudocystStoneStricture
Primary sclerosing cholangitisRenal disease
Chronic renal failureDialysis related
Sphincter of Oddi dysfunctionToxin
Organophosphate insecticidesScorpion bite
TropicalVasculitis
Polyarteritis nodosaSystemic lupus erythematosus
Table 1. Etiologies of Acute Recurrent Pancreatitis
AlcoholBiliary calculous disease
Macrolithiasis (bile duct stone)Microlithiasis (sludge)
Biliary cystic diseaseCholedochal cystCholedochocele/duplication cyst
Congenital anomalyAnnular pancreasAnomalous pancreatobiliary junctionPancreas divisum
Duodenal obstructionAfferent limb obstructed (Billroth II)AtresiaCrohn’s diseaseDiverticulum
DrugsAcetaminophenAzathioprineDidanosineErythromycinEstrogenFurosemideHistamine-2 receptor antagonistsMercaptopurineMethyldopaMetronidazoleNitrofurantoinNonsteroidal anti-inflammatory agentsPentamidineTetracyclineValproic acid
Genetic�-1-antitrypsin deficiencyCystic fibrosisHereditary pancreatitis
IdiopathicInfection
BacterialCampylobacter jejuniLegionellaLeptospirosisMycobacterium avium complexMycobacterium tuberculosisMycoplasma
Parasites/wormsAscaris lumbricoidesClonorchis sinensisCryptosporidiumMicrosporidium
ViralCoxsackievirusCytomegalovirusEcho virusEpstein-Barr virusHepatitis (A, B, C) virusHIVMumps virusRubella virusVaricella virus
MetabolicHypercalcemiaHyperlipidemia
NeoplasmBenignMalignant
2541AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
implicated as the cause of IARP. However, some believethat microlithiasis does not cause pancreatitis, but insteadindicates the prior presence of larger common bile ductstones that precipitated the pancreatitis. In fact, pancreatitismay induce sludge formation by diminishing gallbladdercontractility, thereby leading to some uncertainty regardingthe causal relationship between sludge and pancreatitis.Although some studies have detected microlithiasis in asfew as 7% of patients with IARP (1), others have foundevidence of microlithiasis in approximately two thirds ofpatients (5, 26).
Microlithiasis may lead to pancreatitis through severalmechanisms. Small stones may transiently impact the pa-pilla leading to pancreatic duct obstruction and eventualpancreatitis (27). Repeated exposure to microlithiasis maylead to papillary stenosis and SOD, both of which areassociated with pancreatitis (28).
The optimum method of detecting microlithiasis is yet tobe established. Transabdominal ultrasound is a noninvasivestudy with a sensitivity of about 50% (5, 29). However,repeat examination may improve the yield. Duodenal bileaspiration is an invasive procedure that has a sensitivity of
about 66% (30, 31). ERCP is more invasive, but has asensitivity of about 85% (25, 29). During ERCP, the com-mon bile duct is directly aspirated for bile. Cholecystokininis commonly administered before duodenal drainage orERCP, to enhance gallbladder contractility and improve theyield. In most centers, collected bile is centrifuged at 2000revolutions/min for 10 min; the sediment is warmed to 37°C
Table 2. Initial Evaluation of Acute Recurrent Pancreatitis
Parameter Potential Etiology/Diagnosis
HistoryAlcohol abuse AlcoholDrug intake DrugsFamily history Hereditary
LaboratoryAmylase and lipase (�5�) Drugs
Macrolithiasis (bile duct stone)Microlithiasis (sludge)
(�5�) AlcoholChronic pancreatitisHyperlipemiaNeoplasm
Calcium HypercalcemiaLiver function tests Choledochocele
Macrolithiasis (bile duct stone)Microlithiasis (sludge)Neoplasm (ampulla, pancreas)Pancreatic head inflammationPancreatic head pseudocystSphincter of Oddi dysfunction
Triglycerides HypertriglyceridemiaRadiographs
Ultrasound (transabdominal) Chronic pancreatitisCholedochal cystCholedochoceleMacrolithiasis (bile duct stone)Microlithiasis (sludge)Neoplasm (ampulla, pancreas)
CT Annular pancreasCholedochal cystCholedochoceleChronic pancreatitisMacrolithiasis (bile duct stone)Microlithiasis (sludge)Neoplasm (ampulla, pancreas)
Table 3. Further Evaluation of Idiopathic Acute RecurrentPancreatitis
Parameter Potential Etiology/Diagnosis
Laboratory�-1-antitrypsin phenotype �-1-antitrypsin deficiencyCFTR gene analysis Cystic fibrosisSweat electrolytes Cystic fibrosisTrypsin gene studies Hereditary pancreatitisTumor marker (CA 19-9) NeoplasmDuodenal aspiration Microlithiasis
ERCPAppearance (bulging
ampulla)Choledochocele
Duodenal duplication cystPapillitisStone (impacted)Tumor
Appearance (ductabnormality)
Annular pancreas
Anomalous pancreatobiliaryjunction
Choledochal cystChronic pancreatitis
(complications)Macrolithiasis (bile duct stone)Microlithiasis (sludge)Pancreas divisum
Bile duct aspiration MicrolithiasisBrush cytology/biopsy NeoplasmIntraductal secretin test Chronic pancreatitisMinor papilla cannulation Pancreas divisumSphincter of Oddi
manometrySphincter of Oddi dysfunction
Endoscopic ultrasoundAppearance/image Anomalous pancreatobiliary
junctionChronic pancreatitisMacrolithiasis (bile duct stone)Microlithiasis (sludge)Neoplasm (ampullary and
pancreatic)Pancreas divisum
Fine needle aspirate NeoplasmSecretin stimulated Sphincter of Oddi dysfunction
MRI/MRCPAppearance/image Annular pancreas
Anomalous pancreatobiliaryjunction
CholedochoceleChronic pancreatitisMacrolithiasis (bile duct stone)Microlithiasis (sludge)Neoplasm (ampullary and
pancreatic)Pancreas divisum
2542 Levy and Geenen AJG – Vol. 96, No. 9, 2001
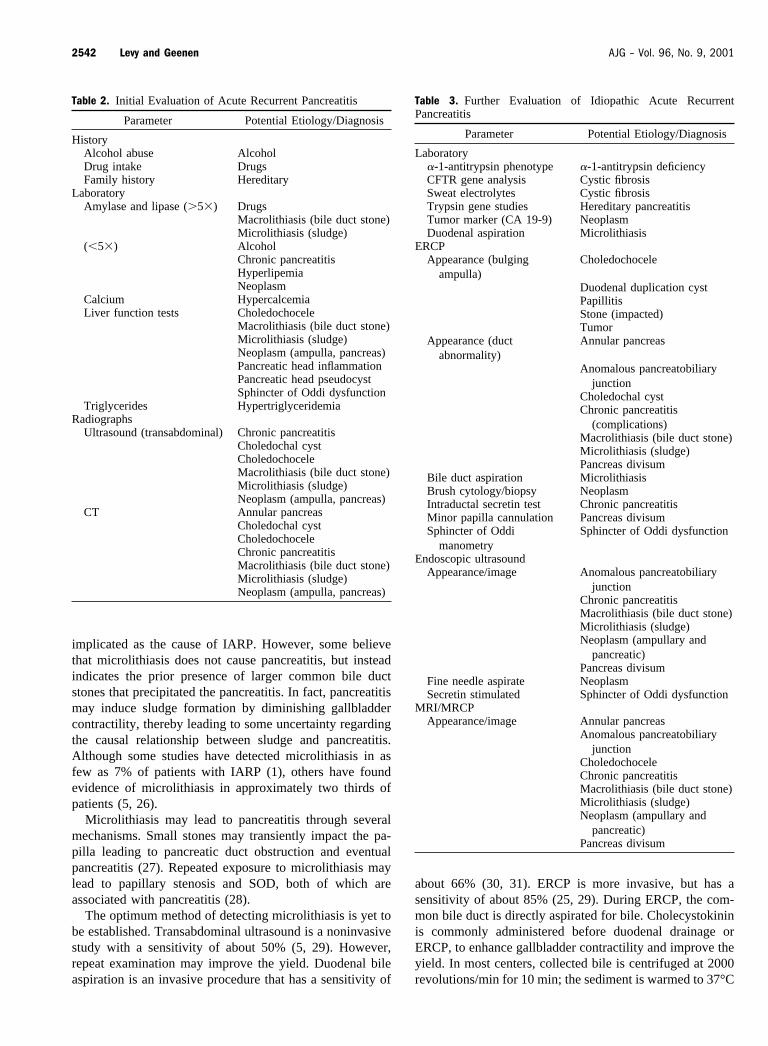
and then examined by polarized microscopy. The quantityof crystals needed to define a positive result differs amonginstitutions, but most believe that the presence of even asmall number of crystals is abnormal. EUS is increasinglybeing used because it offers the greatest diagnostic sensi-tivity (Fig. 2) (32, 33). The presence of microlithiasis mayalso be noted at the time of MRCP (34).
Therapy for microlithiasis can significantly reduce therisk of recurrent pancreatitis (5, 26). Several therapeuticoptions exist for microlithiasis. Laparoscopic cholecystec-tomy is nearly always curative and generally considered theprocedure of choice (5, 26). ERCP with sphincterotomy(incision of the bile duct sphincter) is indicated in highoperative risk patients (35, 36). A low-fat diet and ursode-oxycholic acid are acceptable alternatives in high surgicalrisk patients; however, long term therapy is required (26,37).
SPHINCTER OF ODDI DYSFUNCTION
The sphincter of Oddi is a 5- to 15-mm-long fibromuscularsheath that encircles the terminal common bile duct, pan-creatic duct, and common channel. This sphincter regulatesthe flow of bile and pancreatic juice into the duodenum,inhibits reflux of duodenal contents into the common bileduct and pancreatic duct, and promotes gallbladder fillingwith bile.
SOD is a frequent and treatable cause of IARP and is seen
in roughly one third of these patients (38, 39). SOD causesdiminished transphincteric flow of bile or pancreatic juicebecause of organic obstruction (stenosis) or functional ob-struction (dysmotility). This may cause pancreatitis by pro-moting reflux of bile into the pancreatic duct or by obstruct-ing pancreatic duct outflow (1, 27).
Patients with SOD are classified as having either biliarytype or pancreatic type disease (Table 4) (40, 41). Subclas-sifying (types I, II, and III) helps to predict the underlyingpathology. Type I disease usually results from stenosis, andtype III disease is typically a consequence of dysmotility(40, 41). Subclassifying also helps us to predict the likeli-hood of pain relief after therapy, with the highest responserate occurring in patients with type I disease.
Sphincter of Oddi manometry (SOM) is the gold standardfor diagnosing SOD. SOM employs a water-perfused cath-eter system, which is inserted endoscopically into the com-mon bile duct or pancreatic duct, to measure the sphincter
Figure 2. Sludge. EUS (radial scanning) demonstrating the pres-ence of gallbladder sludge in a patient referred for evaluation ofIARP.
Table 4. Sphincter of Oddi Dysfunction (Geenen & HoganClassification)
Biliary Type Pancreatic Type
Type I Type IBiliary-type pain Pancreatic-type painLFT elevated Amylase/lipase elevationCBD dilation PD dilationDelayed drainage Delayed drainage
Type II Type IIBiliary-type pain Pancreatic-type painOne or two of above criteria One or two of above criteria
Type III Type IIIBiliary-type pain only Pancreatic-type pain only
CBD � common bile duct; LFT � liver function test; PD � pancreatic duct.
Figure 1. Pathological processes associated with IARP. Imagecourtesy of Patsy Bryan.
2543AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
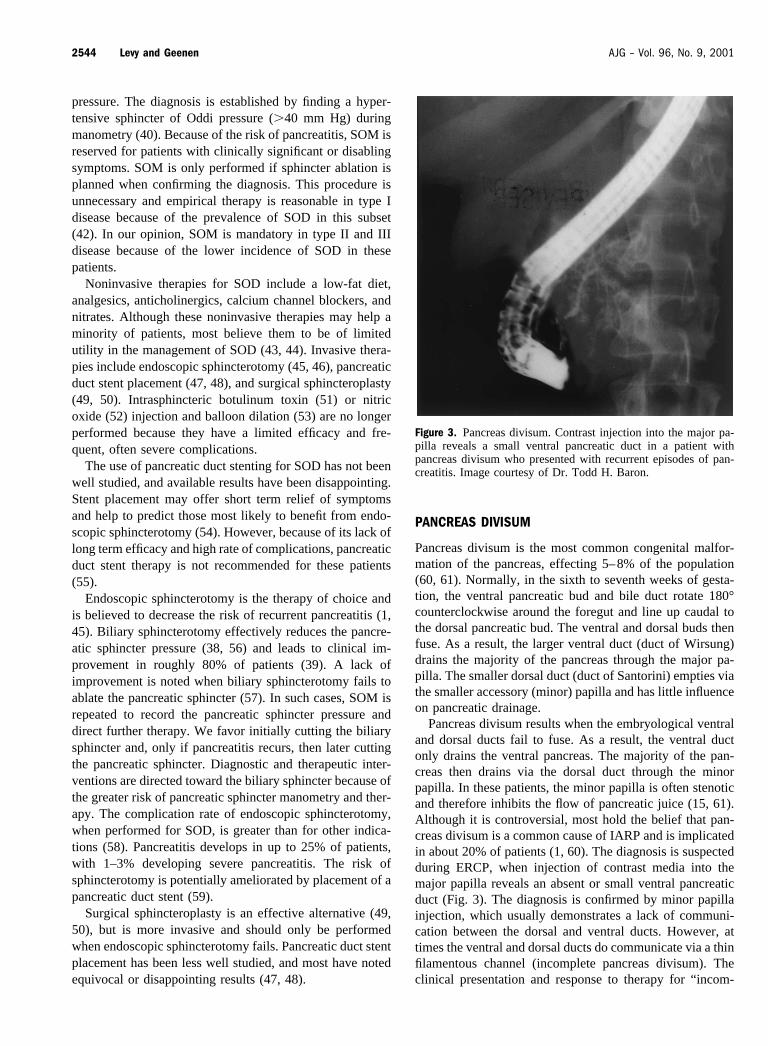
pressure. The diagnosis is established by finding a hyper-tensive sphincter of Oddi pressure (�40 mm Hg) duringmanometry (40). Because of the risk of pancreatitis, SOM isreserved for patients with clinically significant or disablingsymptoms. SOM is only performed if sphincter ablation isplanned when confirming the diagnosis. This procedure isunnecessary and empirical therapy is reasonable in type Idisease because of the prevalence of SOD in this subset(42). In our opinion, SOM is mandatory in type II and IIIdisease because of the lower incidence of SOD in thesepatients.
Noninvasive therapies for SOD include a low-fat diet,analgesics, anticholinergics, calcium channel blockers, andnitrates. Although these noninvasive therapies may help aminority of patients, most believe them to be of limitedutility in the management of SOD (43, 44). Invasive thera-pies include endoscopic sphincterotomy (45, 46), pancreaticduct stent placement (47, 48), and surgical sphincteroplasty(49, 50). Intrasphincteric botulinum toxin (51) or nitricoxide (52) injection and balloon dilation (53) are no longerperformed because they have a limited efficacy and fre-quent, often severe complications.
The use of pancreatic duct stenting for SOD has not beenwell studied, and available results have been disappointing.Stent placement may offer short term relief of symptomsand help to predict those most likely to benefit from endo-scopic sphincterotomy (54). However, because of its lack oflong term efficacy and high rate of complications, pancreaticduct stent therapy is not recommended for these patients(55).
Endoscopic sphincterotomy is the therapy of choice andis believed to decrease the risk of recurrent pancreatitis (1,45). Biliary sphincterotomy effectively reduces the pancre-atic sphincter pressure (38, 56) and leads to clinical im-provement in roughly 80% of patients (39). A lack ofimprovement is noted when biliary sphincterotomy fails toablate the pancreatic sphincter (57). In such cases, SOM isrepeated to record the pancreatic sphincter pressure anddirect further therapy. We favor initially cutting the biliarysphincter and, only if pancreatitis recurs, then later cuttingthe pancreatic sphincter. Diagnostic and therapeutic inter-ventions are directed toward the biliary sphincter because ofthe greater risk of pancreatic sphincter manometry and ther-apy. The complication rate of endoscopic sphincterotomy,when performed for SOD, is greater than for other indica-tions (58). Pancreatitis develops in up to 25% of patients,with 1–3% developing severe pancreatitis. The risk ofsphincterotomy is potentially ameliorated by placement of apancreatic duct stent (59).
Surgical sphincteroplasty is an effective alternative (49,50), but is more invasive and should only be performedwhen endoscopic sphincterotomy fails. Pancreatic duct stentplacement has been less well studied, and most have notedequivocal or disappointing results (47, 48).
PANCREAS DIVISUM
Pancreas divisum is the most common congenital malfor-mation of the pancreas, effecting 5–8% of the population(60, 61). Normally, in the sixth to seventh weeks of gesta-tion, the ventral pancreatic bud and bile duct rotate 180°counterclockwise around the foregut and line up caudal tothe dorsal pancreatic bud. The ventral and dorsal buds thenfuse. As a result, the larger ventral duct (duct of Wirsung)drains the majority of the pancreas through the major pa-pilla. The smaller dorsal duct (duct of Santorini) empties viathe smaller accessory (minor) papilla and has little influenceon pancreatic drainage.
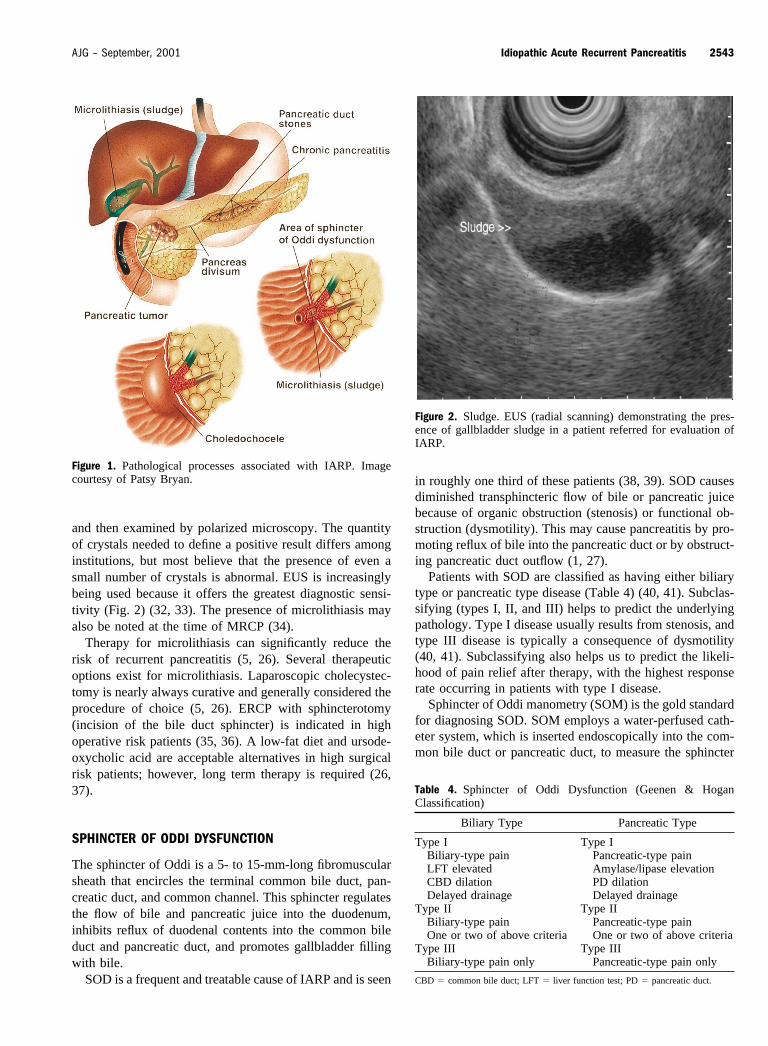
Pancreas divisum results when the embryological ventraland dorsal ducts fail to fuse. As a result, the ventral ductonly drains the ventral pancreas. The majority of the pan-creas then drains via the dorsal duct through the minorpapilla. In these patients, the minor papilla is often stenoticand therefore inhibits the flow of pancreatic juice (15, 61).Although it is controversial, most hold the belief that pan-creas divisum is a common cause of IARP and is implicatedin about 20% of patients (1, 60). The diagnosis is suspectedduring ERCP, when injection of contrast media into themajor papilla reveals an absent or small ventral pancreaticduct (Fig. 3). The diagnosis is confirmed by minor papillainjection, which usually demonstrates a lack of communi-cation between the dorsal and ventral ducts. However, attimes the ventral and dorsal ducts do communicate via a thinfilamentous channel (incomplete pancreas divisum). Theclinical presentation and response to therapy for “ incom-
Figure 3. Pancreas divisum. Contrast injection into the major pa-pilla reveals a small ventral pancreatic duct in a patient withpancreas divisum who presented with recurrent episodes of pan-creatitis. Image courtesy of Dr. Todd H. Baron.
2544 Levy and Geenen AJG – Vol. 96, No. 9, 2001
plete” and “complete” pancreas divisum are identical (62).EUS or MRCP may also make the diagnosis (63–65).
Endoscopic (66, 67) and surgical (68, 69) therapies de-crease the rate of recurrent pancreatitis in 70–90% of pa-tients with pancreas divisum and IARP when followed forup to 5 yr. Treatment is directed toward relieving outflowobstruction at the level of the minor papilla (67). Endo-scopic therapy is generally favored, with surgery reservedfor those in whom endoscopic approaches fail. Endoscopictherapeutic options for the minor papilla include catheterdilation (70), stenting (47, 67), sphincterotomy (66, 71), ora combination of therapies. Catheter dilation and stentingalone (i.e., without minor papilla sphincterotomy) are gen-erally ineffective and cannot be regarded as standard man-agement. Importantly, pancreatic stents may induce ductalchanges mimicking chronic pancreatitis, and therefore longterm stenting should only be performed in a research settingin patients who are closely observed (72, 73). Minor papillasphincterotomy is generally favored in these patients. Whendoing so, we recommend short term placement of a dorsalpancreatic duct stent, which serves as a guide for the sphinc-terotomy and helps minimize the risk of complications (66).Use of an unflanged stent is important to encourage spon-taneous migration (74).
HEREDITARY (FAMILIAL) PANCREATITIS
Hereditary pancreatitis is a genetic disorder with an auto-somal dominant means of transmission and an estimated80% penetrance (17). There is no gender predominance, andsymptoms typically arise in childhood but may be delayeduntil the mid-30s (17). This disorder results from a mutationin the cationic trypsinogen gene located on chromosome7q35 (75). The anomaly involves an arginine to histidinesubstitution at amino acid 117 (R117H) or asparagine toisoleucine substitution at amino acid 21 (N21I) (76). Thismutation leads to formation of an abnormal cationictrypsinogen, impaired inactivation of trypsin, and continu-ous activation of digestive enzymes (77). It is theorized thatpancreatic autodigestion eventually leads to chronic pancre-atitis. Patients may present with IARP, but commonly de-velop chronic pancreatitis with associated abdominal pain,diabetes mellitus, maldigestion, and steatorrhea (17). Thelifetime risk of pancreatic cancer is roughly 40% and re-portedly 75% with paternal inheritance (78).
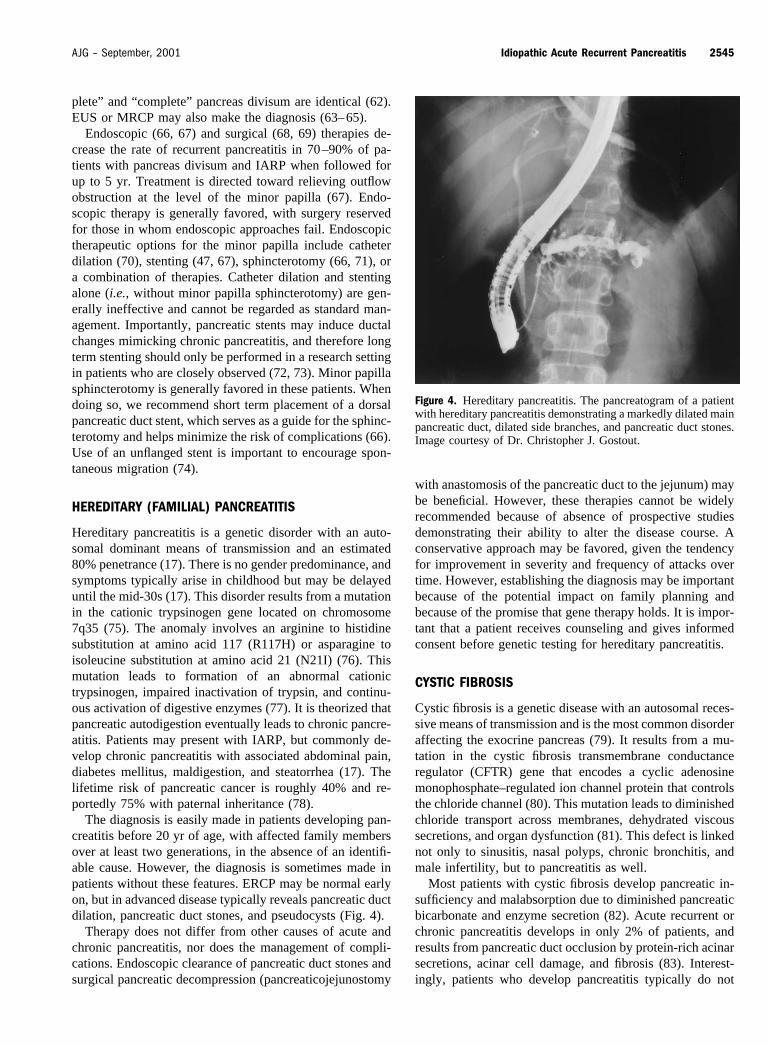
The diagnosis is easily made in patients developing pan-creatitis before 20 yr of age, with affected family membersover at least two generations, in the absence of an identifi-able cause. However, the diagnosis is sometimes made inpatients without these features. ERCP may be normal earlyon, but in advanced disease typically reveals pancreatic ductdilation, pancreatic duct stones, and pseudocysts (Fig. 4).
Therapy does not differ from other causes of acute andchronic pancreatitis, nor does the management of compli-cations. Endoscopic clearance of pancreatic duct stones andsurgical pancreatic decompression (pancreaticojejunostomy
with anastomosis of the pancreatic duct to the jejunum) maybe beneficial. However, these therapies cannot be widelyrecommended because of absence of prospective studiesdemonstrating their ability to alter the disease course. Aconservative approach may be favored, given the tendencyfor improvement in severity and frequency of attacks overtime. However, establishing the diagnosis may be importantbecause of the potential impact on family planning andbecause of the promise that gene therapy holds. It is impor-tant that a patient receives counseling and gives informedconsent before genetic testing for hereditary pancreatitis.
CYSTIC FIBROSIS
Cystic fibrosis is a genetic disease with an autosomal reces-sive means of transmission and is the most common disorderaffecting the exocrine pancreas (79). It results from a mu-tation in the cystic fibrosis transmembrane conductanceregulator (CFTR) gene that encodes a cyclic adenosinemonophosphate–regulated ion channel protein that controlsthe chloride channel (80). This mutation leads to diminishedchloride transport across membranes, dehydrated viscoussecretions, and organ dysfunction (81). This defect is linkednot only to sinusitis, nasal polyps, chronic bronchitis, andmale infertility, but to pancreatitis as well.
Most patients with cystic fibrosis develop pancreatic in-sufficiency and malabsorption due to diminished pancreaticbicarbonate and enzyme secretion (82). Acute recurrent orchronic pancreatitis develops in only 2% of patients, andresults from pancreatic duct occlusion by protein-rich acinarsecretions, acinar cell damage, and fibrosis (83). Interest-ingly, patients who develop pancreatitis typically do not
Figure 4. Hereditary pancreatitis. The pancreatogram of a patientwith hereditary pancreatitis demonstrating a markedly dilated mainpancreatic duct, dilated side branches, and pancreatic duct stones.Image courtesy of Dr. Christopher J. Gostout.
2545AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
suffer from pancreatic insufficiency and do not manifestmost of the phenotypic abnormalities. This is true becausethe genotypes that lead to acute or chronic pancreatitis causeonly moderate loss of CFTR gene function (79).
Over 800 mutations have been identified on the CFTRgene (84), which is located on chromosome 7q31 (80).Deletion of phenylalanine at amino acid 508 (�F508) isimplicated in 70% of patients, with another 20 or so muta-tions accounting for most of the remaining cases (85). Ge-netic testing reveals that approximately 10–15% of patientswith idiopathic pancreatitis are homozygous for a CFTRgene mutation (82, 86). Heterozygous CFTR mutations areseen in about 10–40% of patients with IARP or idiopathicchronic pancreatitis, but in �10% of persons with alcoholicpancreatitis and in the general population. Although they areimplicated as a cause of pancreatitis by some, it is unclearif heterozygous CFTR mutations are linked with any otherpathological states (82, 86). Heterozygous carriers may be atgreater risk for pancreatitis in the presence of alcohol, drugs,or other risk factors. These patients may also possess an-other unidentified mutation in the corresponding allele.
Diminished CFTR function may also result from im-paired messenger RNA splicing. This occurs in patients witha short polythymidine tract (5T), versus normal longer thy-midine variants 7T and 9T, in intron 8 of the CFTR gene(87). The 5T variant is not associated with lung disease, butis associated with congenital absence of the vas deferens,and may be linked to idiopathic pancreatitis (87, 88). Cur-rently, most laboratories are not routinely testing for the 5Tallele.
Therapy does not differ from that for other causes of acuteand chronic pancreatitis. As with hereditary pancreatitis,consideration of the diagnosis is important for family plan-ning and because of the potential future role of gene therapy.Discovery of medications that enhance ductal bicarbonatesecretion may one day prevent or slow the progression ofpancreatitis.
CHOLEDOCHOCELE
Cystic dilation may occur throughout the biliary system andcan involve the extrahepatic and/or intrahepatic bile ducts.Todani et al. (89), based on the location, first classified thesecysts into five types. A type III cyst, or choledochocele, isa rare congenital or acquired condition in which the intra-mural segment of the distal pancreatobiliary ductal system isdilated and herniates into the duodenal lumen. They vary insize from a few millimeters to several centimeters. Chole-dochoceles are associated with biliary and pancreatic disor-ders, including biliary colic, obstructive jaundice, and IARP(19, 90). Of the five types, only type III cysts have beenassociated with IARP. Pancreatitis develops when the cystor its contents (sludge or stones) obstruct pancreatic ductoutflow.
Although abnormal laboratory values, transabdominal ul-trasound, CT, or MRCP may suggest a choledochocele, the
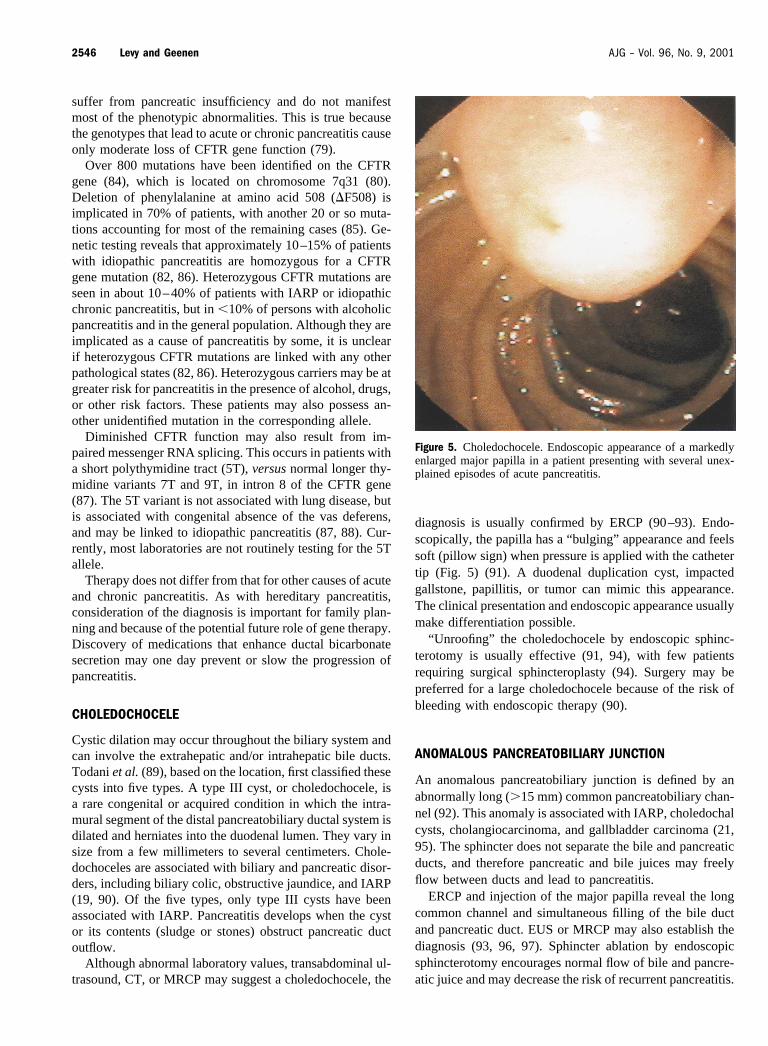
diagnosis is usually confirmed by ERCP (90–93). Endo-scopically, the papilla has a “bulging” appearance and feelssoft (pillow sign) when pressure is applied with the cathetertip (Fig. 5) (91). A duodenal duplication cyst, impactedgallstone, papillitis, or tumor can mimic this appearance.The clinical presentation and endoscopic appearance usuallymake differentiation possible.
“Unroofing” the choledochocele by endoscopic sphinc-terotomy is usually effective (91, 94), with few patientsrequiring surgical sphincteroplasty (94). Surgery may bepreferred for a large choledochocele because of the risk ofbleeding with endoscopic therapy (90).
ANOMALOUS PANCREATOBILIARY JUNCTION
An anomalous pancreatobiliary junction is defined by anabnormally long (�15 mm) common pancreatobiliary chan-nel (92). This anomaly is associated with IARP, choledochalcysts, cholangiocarcinoma, and gallbladder carcinoma (21,95). The sphincter does not separate the bile and pancreaticducts, and therefore pancreatic and bile juices may freelyflow between ducts and lead to pancreatitis.
ERCP and injection of the major papilla reveal the longcommon channel and simultaneous filling of the bile ductand pancreatic duct. EUS or MRCP may also establish thediagnosis (93, 96, 97). Sphincter ablation by endoscopicsphincterotomy encourages normal flow of bile and pancre-atic juice and may decrease the risk of recurrent pancreatitis.
Figure 5. Choledochocele. Endoscopic appearance of a markedlyenlarged major papilla in a patient presenting with several unex-plained episodes of acute pancreatitis.
2546 Levy and Geenen AJG – Vol. 96, No. 9, 2001

ANNULAR PANCREAS
Annular pancreas is a congenital anomaly that manifests asa band of pancreatic tissue partially or completely encirclingthe duodenum, usually at the level of or just proximal to themajor papilla (92). This abnormality is detected in 1/7,000–20,000 autopsies (92, 98) and in about 1/1,500 ERCPs(99–101). The defect occurs in utero when the ventral budbecomes fixed and fails to rotate with the duodenum (92).
Symptoms typically begin in childhood and develop as aresult of duodenal obstruction, with intractable vomitingmost commonly noted (100, 101). Childhood disease isoften associated with congenital anomalies such as Down’ssyndrome, cardiac defects, tracheoesophageal fistula, Meck-el’s diverticulum, and imperforate anus (92, 100). Adultsmay present with abdominal pain, IARP, chronic pancreati-tis, peptic ulcer disease, or biliary obstruction (20, 101).
Although barium x-ray, CT, or MRCP may suggest thediagnosis, ERCP is usually required for confirmation (34,99, 100). ERCP typically identifies the duct of the pancreaticannulus encircling the duodenum (Fig. 6). Pancreas divisumis also present in one third of these patients (20). Althoughthe annular duct may communicate with the ventral duct, itrarely drains into the dorsal duct, common bile duct, orindependently into the duodenum (20, 99). EUS may also beuseful in establishing the diagnosis (102).
Gastrojejunostomy (resection of the lesion with anasto-mosis of the jejunum and stomach) may be required tobypass the segment of obstructed bowel (98, 101). Pancre-atic head resection is seldom necessary. Division of theannulus, once the procedure of choice, is no longer per-formed because of the inordinate risk of pancreatitis andpancreatic fistula formation.
PANCREATOBILIARY TUMORS
Five to seven percent of patients with pancreatobiliary tu-mors, benign or malignant, present with IARP (22, 103,104). The presence of a neoplasia may be suggested bysignificant weight loss, steatorrhea, radiological evidence ofa solid or cystic pancreatic mass or ductal dilation, andincreased age. Although younger patients less commonlyhave a neoplasia, they are frequently affected by lesionssuch as islet cell tumors that are often amenable to curativeresection. Even the elderly may have potential curable le-sions such as cystic neoplasms. Although pancreatic adeno-carcinoma is most often implicated, these other tumors mustbe considered as well.
CT, magnetic resonance imaging (MRI), ERCP, and EUSare all useful for identifying pancreatobiliary neoplasms(Fig. 7) (105–108). The extent of the evaluation is typicallybased on the patient’s age, clinical status, and level ofsuspicion for a neoplasm. CT imaging may be adequate toevaluate patients �40 yr of age with IARP. ERCP is usuallyperformed, in addition to CT, in patients over 40 yr becauseof the increased risk of malignancy. EUS is quickly becom-ing a favored procedure because of the ability to diagnose,stage, and biopsy pancreatobiliary tumors (109, 110). Infact, most studies have found EUS to have the highestsensitivity for identifying pancreatic neoplasm relative toother imaging modalities, especially for tumors � 2–3 cm indiameter (105–108). The diagnosis may be confirmed byCT-guided biopsy, ERCP-directed brush cytology, or EUS-guided fine needle aspiration (110, 111). These proceduresalso assist in staging by determining the characteristics ofthe primary tumor—namely, tumor size and infiltration intomajor vessels (T stage), regional lymph node involvement
Figure 6. Annular pancreas. Pancreatogram outlining the pancreatic duct as it encircles the duodenum in a patient with multiple attacksof pancreatitis.
2547AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
(N stage), and the presence or absence of distant metastasis(M stage).
Most patients with pancreatic cancer present late in theircourse and have either locally extensive or metastatic dis-ease (112). The late presentation, aggressive nature, andlack of effective therapies all result in a poor prognosis.Only 10–20% of patients are considered candidates forcurative resection at the time of diagnosis (113). Accuratestaging of pancreatic adenocarcinoma is important to iden-tify the subset of patients who have localized resectable andpotentially curable cancers. Although early detection is cru-cial to improve prognosis, the determination of resectabilityis important to help avoid unnecessary surgical intervention.Even for patients deemed resectable and undergoing aWhipple procedure (pancreaticoduodenectomy), the 5-yrsurvival is only about 2% and therefore effective palliationmay be the best option for many patients (114). Unresect-able or metastatic tumors are effectively palliated by theendoscopic placement of a plastic or metal stent across thesite of biliary obstruction. This allows biliary drainage andrelief of pruritus, anorexia, and jaundice (115, 116).
Cystic pancreatic tumors such as serous cystadenomas,mucinous cystadenomas, mucinous cystadenocarcinomas,and intraductal papillary mucinous tumors may also presentwith IARP. Serous cystadenomas are benign, with rareexception, and can generally be managed with observationalone (117). The other lesions are premalignant or malignantand in good operative candidates are generally indicationsfor surgical resection (117–119). Detection is importanteven after malignant transformation, because these tumorshave a better prognosis than ductal adenocarcinoma. Trans-abdominal ultrasound, CT, MRI, and EUS are useful incharacterizing and differentiating cystic pancreatic tumors(Fig. 8) (120, 121). The diagnostic yield can be improved by
analyzing aspirated cystic fluid. The fluid viscosity andamylase level, along with the tumor marker concentration(CA 19-9, CA 15-3, CA 72-4, and carcinoembryonic anti-gen), may be used to increase the diagnostic yield of cystfluid cytology (122, 123).
Ampullary tumors, both benign and malignant, maypresent with painless jaundice, anemia, or IARP (22, 90,103). Adenomas, which are the most common ampullarytumors, are premalignant and in general indicate the needfor surgical resection (124, 125). Ampullary tumors in gen-eral have a more favorable prognosis than pancreatic tumors(126, 127), with pancreatoduodenectomy improving theprognosis (127, 128). Although this is controversial, benignpapillary tumors and localized malignant tumors may beadequately treated with pylorus-preserving pancreatoduode-nectomy or even wide local excision (126, 129, 130). Theseless invasive surgical techniques offer the advantage ofreduced morbidity and mortality.
Various endoscopic techniques are also available for themanagement of patients with ampullary tumors. An endo-scopic approach is generally reserved for small lesions thatare benign or for carcinoma in situ. Evidence of an invasivecarcinoma and large benign lesions should be managed bysurgical means in patients who are good operative candi-dates. The ideal endoscopic therapy remains to be identified.Tumor excision may be achieved by snare ampullectomy(removal of entire papilla) or piecemeal snare resection(131, 132). Endoscopic resection is followed by tumor ab-lation of residual tissue during the initial endoscopy as wellas during surveillance exams. Neodymium:yttrium-alumi-
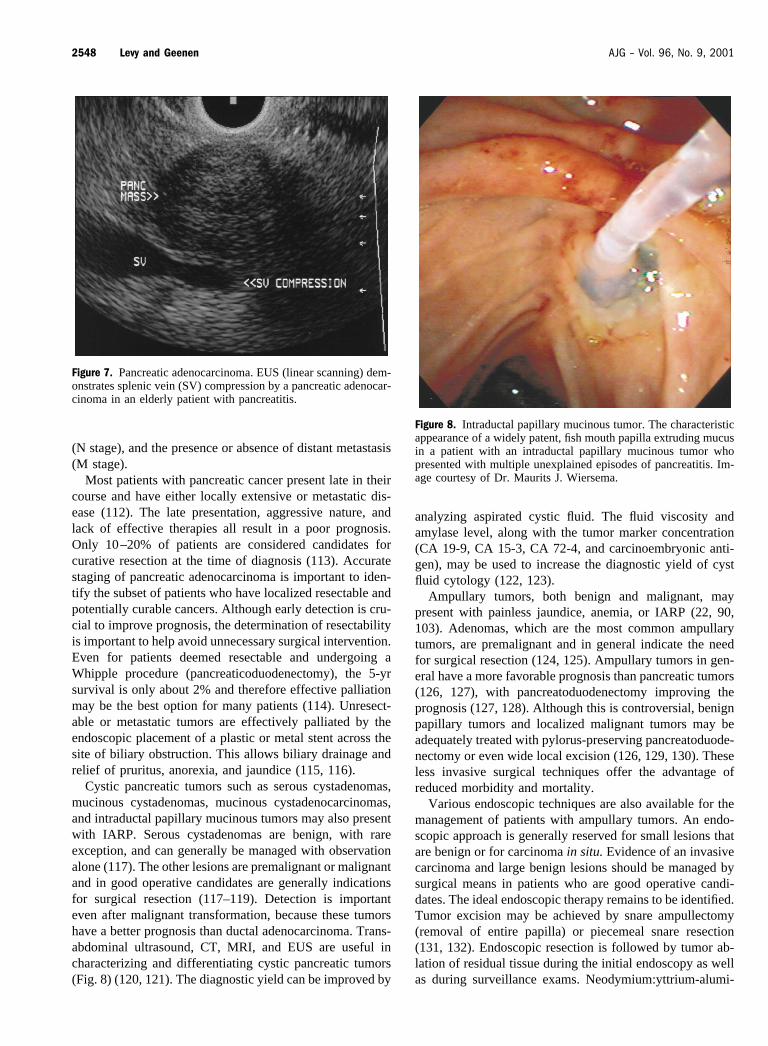
Figure 7. Pancreatic adenocarcinoma. EUS (linear scanning) dem-onstrates splenic vein (SV) compression by a pancreatic adenocar-cinoma in an elderly patient with pancreatitis.
Figure 8. Intraductal papillary mucinous tumor. The characteristicappearance of a widely patent, fish mouth papilla extruding mucusin a patient with an intraductal papillary mucinous tumor whopresented with multiple unexplained episodes of pancreatitis. Im-age courtesy of Dr. Maurits J. Wiersema.
2548 Levy and Geenen AJG – Vol. 96, No. 9, 2001
num-garnet laser, multipolar cautery, or argon plasma co-agulation may accomplish tumor ablation, with no consen-sus as to the technique of choice (132, 133). Although nostudies have confirmed a survival advantage of surveillanceafter endoscopic resection, this is recommended for ampul-lary adenomas. This recommendation is based on the ade-noma-carcinoma sequence of these lesions, the inability toassure complete ablation, and their expected continuedgrowth. Although some favor surveillance and random bi-opsy every 3–5 yr (134, 135), we recommend initial fol-low-up at 3 months and yearly thereafter.
Studies comparing endoscopic techniques to surgical in-tervention for ampullary tumors are small and uncontrolled.We suggest that the tumor histology, extent of the lesion,local expertise, and patient preference must all be consid-ered when selecting the ideal means of therapy.
CHRONIC PANCREATITIS
Although patients may clinically present with IARP, manywill be found, after ERCP, pancreatic function tests, andEUS, to have already developed some degree of chronicpancreatitis (23, 136). These procedures have a low sensi-tivity and are unable to diagnose chronic pancreatitis at anearly stage. The pancreatic duct is typically normal appear-ing in early chronic pancreatitis, thereby limiting the sensi-tivity of ERCP. However, pancreatic function testing (e.g.,intraductal secretin test) may help establish the diagnosis atan earlier stage (137). After secretin administration, aliquotsof pancreatic juice are collected via an ERCP cannula po-sitioned in the pancreatic duct. EUS may be the most sen-sitive study (137, 138), but the findings should be carefullyinterpreted because features of chronic pancreatitis may beseen in the normal population (139). Therefore, the diagno-sis of chronic pancreatitis is best made after considering theresults of ERCP, pancreatic function tests, and EUS. Thereare only limited data supporting the use of MRCP forestablishing the diagnosis of chronic pancreatitis. Althoughit may suggest the diagnosis, MRCP cannot be recom-mended solely for this purpose at this time (140, 141).
The mortality rate for patients with chronic pancreatitis isthree to four times greater than for controls, with mortalitydirectly related to pancreatitis in 20% of patients (142, 143).The reduction in life span is only 8 yr, with most deathsresulting from nonpancreatic causes (142, 143). Therefore,though it is important to establish the diagnosis of chronicpancreatitis, doing so may only minimally impact a patient’scourse. Evaluating patients with IARP for chronic pancre-atitis not only helps establish the correct diagnosis, but alsodetermines the prognosis and influences therapy. Patientswith chronic pancreatitis may benefit from a trial of pan-creatic enzyme replacement, a low-fat diet, small meals,insulin for diabetes, and analgesics.
Chronic pancreatitis may be complicated by pancreaticduct strictures, stones, pseudocyst, fistulas, pseudoaneu-rysm, or ascites (144–146). Patients with unrecognized
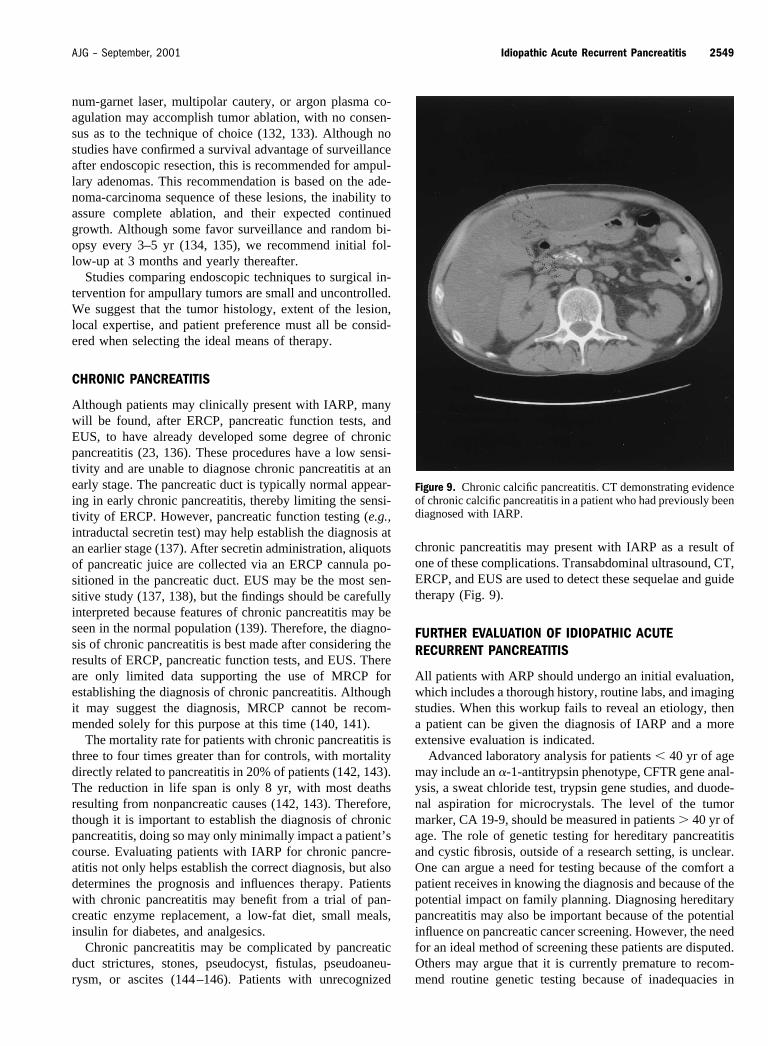
chronic pancreatitis may present with IARP as a result ofone of these complications. Transabdominal ultrasound, CT,ERCP, and EUS are used to detect these sequelae and guidetherapy (Fig. 9).
FURTHER EVALUATION OF IDIOPATHIC ACUTERECURRENT PANCREATITIS
All patients with ARP should undergo an initial evaluation,which includes a thorough history, routine labs, and imagingstudies. When this workup fails to reveal an etiology, thena patient can be given the diagnosis of IARP and a moreextensive evaluation is indicated.
Advanced laboratory analysis for patients � 40 yr of agemay include an �-1-antitrypsin phenotype, CFTR gene anal-ysis, a sweat chloride test, trypsin gene studies, and duode-nal aspiration for microcrystals. The level of the tumormarker, CA 19-9, should be measured in patients � 40 yr ofage. The role of genetic testing for hereditary pancreatitisand cystic fibrosis, outside of a research setting, is unclear.One can argue a need for testing because of the comfort apatient receives in knowing the diagnosis and because of thepotential impact on family planning. Diagnosing hereditarypancreatitis may also be important because of the potentialinfluence on pancreatic cancer screening. However, the needfor an ideal method of screening these patients are disputed.Others may argue that it is currently premature to recom-mend routine genetic testing because of inadequacies in
Figure 9. Chronic calcific pancreatitis. CT demonstrating evidenceof chronic calcific pancreatitis in a patient who had previously beendiagnosed with IARP.
2549AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis

genetic analysis and the absence of established guidelinesfor genetic counseling. Also, there are no unique endoscopicor surgical approaches for the management of hereditarypancreatitis or cystic fibrosis versus other forms of acute andchronic pancreatitis. Therefore, genetic testing currently hasnegligible influence on clinical management. We recom-mend that when genetic testing is not employed, a physiciankeep a registry of patients suspected of having either disor-der, so that they may benefit from newly discovered medi-cations and gene therapy.
ERCP reveals a diagnosis in about 70% of patients withIARP after a negative initial evaluation (1, 15). Because theinitial episode of pancreatitis may be an isolated event andbecause of the risk of ERCP, most agree that this procedureis not justified after the first episode of pancreatitis (37,147). Many believe, however, that ERCP is indicated whenthe first episode is severe or when a patient has two or moreepisodes. However, there are some who advocate perform-ing an ERCP after the first episode regardless of the pa-tient’s age or disease severity (37). At the time of the ERCP,bile is aspirated and examined for microcrystals, SOM isperformed when SOD is suspected, and the minor papilla iscannulated when pancreas divisum is suspected.
EUS is increasingly being used to evaluate patients withIARP because of its sensitivity and safety (148). As com-pared to transabdominal ultrasound, EUS uses a higherfrequency and eliminates the decreased image quality re-sulting from bowel gas or subcutaneous fat. As a result, EUSoffers greater image resolution. EUS has equal or superiorsensitivity to other commonly used tests in the diagnosis ofmicrolithiasis and sludge (32, 33). SOD is detected usingsecretin-stimulated EUS (SSEUS) by demonstrating persis-tent dilation of the pancreatic duct after secretin adminis-tration (149). However, data regarding the utility of SSEUSare limited, and this technique is available in only a fewcenters. Therefore, at this point SSEUS must be regarded asa research tool for studying SOD. EUS has reasonablesensitivity and specificity in detecting structural lesions suchas pancreas divisum (63) and an anomalous pancreatobiliaryjunction (96). Occult ampullary and pancreatic tumors mayalso be discovered (109, 110). Finally, EUS can detect thepresence of chronic pancreatitis in patients initially present-ing with IARP (137–139).
Conventional MRI is not generally considered a usefultool in the evaluation of patients with IARP except as itapplies to the diagnosis and staging of pancreatobiliaryneoplasms. Given the limited role and greater utility of otherimaging modalities, conventional MRI is not routinely rec-ommended for the evaluation of patients with IARP. How-ever, experience with MRCP is growing, and its usefulnessin diagnosing disorders associated with IARP is becomingincreasingly recognized. With the employment of heavilyT2-weighted sequences, fluid within the bile and pancreaticducts is selectively displayed during MRCP, producing an
image similar to ERCP. MRCP is helpful for evaluatingacute pancreatitis because it may detect the presence of bileduct stones (Fig. 10) (64, 150). In patients with IARP, theprimary value of MRCP is to identify anatomical abnormal-ities such as pancreas divisum, a choledochocele, anoma-lous pancreatobiliary junction, or annular pancreas (93, 97,150, 151). Although MRCP may also detect pancreatico-biliary tumors (34, 107), chronic pancreatitis (140, 141), andmicrolithiasis (34), its value for diagnosing these disordershas been minimally studied, and this is not the greatest useof this imaging modality at this time.
MRCP offers several advantages over ERCP and is re-placing diagnostic ERCP in many centers. The advantagesinclude its noninvasiveness, the absence of ERCP-relatedcomplications, avoiding the use of contrast and radiation,and its utility in postsurgical patients. However, ERCPcontinues to have an important role in the evaluation ofpatients with IARP because of the ability to inspect theampulla, brush and biopsy tissues, aspirate bile fluid, per-form SOM, and mostly because of its therapeutic potential.
Figure 10. Choledocholithiasis. A filling defect (arrow) is identi-fied by MRCP, supporting the suspicion of a bile duct stone in apatient with presumed gallstone pancreatitis.
2550 Levy and Geenen AJG – Vol. 96, No. 9, 2001

MANAGEMENT
Episodes of acute pancreatitis are treated similarly regard-less of the etiology. Intravenous fluids are given, oral intakeis withheld, metabolic and electrolyte disturbances are cor-rected, analgesics are administered, and respiratory, renal,and vascular complications are treated as necessary. Specifictherapy for given disorders, when available, should be man-aged as outlined earlier.
Therapeutic options for patients with TIARP are limited,and little information exists regarding their care. An analysisof the data from available studies is complicated given thedifferences in patient population, therapy administered, andoutcomes measured. Most studies included patients withidentifiable disorders such as SOD or pancreas divisumalong with TIARP. In these studies the results were usuallycombined, making it difficult to extrapolate the data forpatients with TIARP. Many trials only performed a limitedevaluation, thereby increasing the likelihood of missing anexisting disorder. Most studies have also been noncontrolledand nonrandomized.
A number of “nonvalidated” therapies therefore exist forTIARP. Smooth muscle relaxers such as calcium channelblockers or nitrates may abort an attack if taken at the onsetof symptoms. Pancreatic enzymes inhibit pancreatic enzymesecretion and may be helpful, especially for those patientswith idiopathic chronic pancreatitis (152). There is literatureto suggest that antioxidants such as �-carotene, methionine,vitamin C, and vitamin E may be beneficial by inhibiting therelease of oxygen-derived free radicals (153).
Several centers have reported favorable results with theuse of pancreatic duct stents or endoscopic sphincterotomy(biliary or pancreatic) in patients with TIARP (47, 154).There is only one prospective, randomized trial evaluatingthe use of pancreatic duct stents for this indication (155).Patients randomized to stent placement suffered fewer epi-sodes of pancreatitis during the nearly 3-yr follow-up. How-ever, such therapy cannot be widely supported outside of aresearch protocol until more data are available.
Because of the prevalence of microlithiasis in patientswith IARP and because of the high false negative rate of bileacid analysis, it may be reasonable to proceed with empiriclaparoscopic cholecystectomy (15, 156, 157). Empiric ad-ministration of ursodeoxycholic acid and a low-fat diet area reasonable alternative in high surgical risk patients.
In conclusion, ARP may be caused by a number ofdisorders. Often, our greatest challenge is to establish thecorrect diagnosis in those patients without a history ofgallstone disease or alcohol abuse. In the 10–30% of pa-tients with “ idiopathic” acute recurrent pancreatitis, the useof specialized laboratory analysis, ERCP, EUS, and MRCPmay lead to the diagnosis. These procedures may be usednot only to establish the correct diagnosis, but also to directtherapy and often improve a patient’s long term prognosis.
Reprint requests and correspondence: Michael J. Levy, M.D.,The Mayo Clinic, Eisenberg 8A, Mayo Clinic, 200 First Street SW,Rochester, MN 55905.
Received Dec. 12, 2000; accepted June 5, 2001.
REFERENCES
1. Venu RP, Geenen JE, Hogan W, et al. Idiopathic recurrentpancreatitis: An approach to diagnosis and treatment. Dig DisSci 1989;34:56–60.
2. Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med1994;330:1198–210.
3. Ballinger AB, Barnes E, Alstead EM, Fairclough PD. Isintervention necessary after a first episode of acute idiopathicpancreatitis? Gut 1996;38:293–5.
4. Thomson SR, Hendry WS, McFarlane GA, Davidson AI.Epidemiology and outcome of acute pancreatitis. Br J Surg1987;74:398–401.
5. Lee SP, Nicholls JF, Park HZ. Biliary sludge as a cause ofacute pancreatitis. N Engl J Med 1992;326:589–93.
6. Seidensticker F, Otto J, Lankisch PG. Recovery of the pan-creas after acute pancreatitis is not necessarily complete. IntJ Pancreatol 1995;17:225–9.
7. Gumaste VV, Dave PB, Weissman D, Messer J. Lipase/amylase ratio. A new index that distinguishes acute episodesof alcoholic from nonalcoholic acute pancreatitis. Gastroen-terology 1991;101:1361–6.
8. Tenner SM, Steinberg W. The admission serum lipase:Amylase ratio differentiates alcoholic from nonalcoholicacute pancreatitis. Am J Gastroenterol 1992;87:1755–8.
9. Steinberg WM, Goldstein SS, Davis ND, et al. Diagnosticassays in acute pancreatitis: A study of sensitivity and spec-ificity. Ann Intern Med 1985;102:576–80.
10. Tenner S, Dubner H, Steinberg W. Predicting gallstone pan-creatitis with laboratory parameters: A meta-analysis. Am JGastroenterol 1994;89:1863–6.
11. Chang L, Lo SK, Stabile BE, et al. Gallstone pancreatitis: Aprospective study on the incidence of cholangitis and clinicalpredictors of retained common bile duct stones. Am J Gas-troenterol 1998;93:527–31.
12. Grendell JH. Idiopathic acute pancreatitis. Gastroenterol ClinNorth Am 1990;19:843–8.
13. Neoptolemos JP, Hall AW, Finlay DF, et al. The urgentdiagnosis of gallstones in acute pancreatitis: A prospectivestudy of three methods. Br J Surg 1984;71:230–3.
14. London NJ, Leese T, Lavelle JM, et al. Rapid-bolus contrast-enhanced dynamic computed tomography in acute pancreati-tis. A prospective study. Br J Surg 1991;78:1452–6.
15. Tarnasky PR, Hawes RH. Endoscopic diagnosis and therapyof unexplained (idiopathic) acute pancreatitis. GastrointestEndosc Clin North Am 1998;8:13–37.
16. Geenen JE, Nash JA. The role of sphincter of Oddi manom-etry and biliary microscopy in evaluating idiopathic recurrentpancreatitis. Endoscopy 1998;30(suppl 1):237–41.
17. Perrault J. Hereditary pancreatitis. Gastroenterol Clin NorthAm 1994;23:743–52.
18. Shwachman H, Lebenthal E, Khaw KT. Recurrent acutepancreatitis in patients with cystic fibrosis with normal pan-creatic enzymes. Pediatrics 1975;55:86–95.
19. Okada A, Higaki J, Nakamura T, et al. Pancreatitis associatedwith choledochal cyst and other anomalies in childhood. Br JSurg 1995;82:829–32.
20. Dowsett JF, Rode J, Russell RC. Annular pancreas: A clin-ical, endoscopic, and immunohistochemical study. Gut 1989;30:130–5.
2551AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
21. Misra SP, Dwivedi M. Pancreaticobiliary ductal union. Gut1990;31:1144–9.
22. Kahrilas PJ, Hogan WJ, Geenen JE, et al. Chronic recurrentpancreatitis secondary to a submucosal ampullary tumor in apatient with neurofibromatosis. Dig Dis Sci 1987;32:102–7.
23. Steer ML, Waxman I, Freedman S. Chronic pancreatitis.N Engl J Med 1995;332:1482–90.
24. Lee SP, Nicholls JF. Nature and composition of biliarysludge. Gastroenterology 1986;90:677–86.
25. Buscail L, Escourrou J, Delvaux M, et al. Microscopic ex-amination of bile directly collected during endoscopic can-nulation of the papilla: Utility in patients with suspectedmicrolithiasis. Dig Dis Sci 1992;37:116–20.
26. Ros E, Navarro S, Bru C, et al. Occult microlithiasis in“ idiopathic” acute pancreatitis: Prevention of relapses bycholecystectomy or ursodeoxycholic acid therapy. Gastroen-terology 1991;101:1701–9.
27. Opie EL. The etiology of acute hemorrhagic pancreatitis.Bull Johns Hopkins Hosp 1901;12:182–8.
28. Hernandez CA, Lerch MM. Sphincter stenosis and gallstonemigration through the biliary tract. Lancet 1993;341:1371–3.
29. Venu RP, Geenen JE, Stewart EG, Hogan WJ. Endoscopicretrograde cholangiopancreatography: Diagnosis of choleli-thiasis in patients with normal gallbladder x-rays and ultra-sound studies. JAMA 1983;249:758–61.
30. Neoptolemos JP, Davidson BR, Winder AF, Vallance D.Role of duodenal bile crystal analysis in the investigation of“ idiopathic” pancreatitis. Br J Surg 1988;75:450–3.
31. Marks JW, Bonorris G. Intermittency of cholesterol crystalsin duodenal bile from gallstone patients. Gastroenterology1984;87:622–7.
32. Dahan P, Andant C, Levy P, et al. Prospective evaluation ofendoscopic ultrasonography and microscopic examination ofduodenal bile in the diagnosis of cholecystolithiasis in 45patients with normal conventional ultrasonography. Gut1996;38:277–81.
33. Dill JE, Hill S, Callis J, et al. Combined endoscopic ultra-sound and stimulated biliary drainage in cholecystitis andmicrolithiasis—diagnosis and outcomes. Endoscopy 1995;27:424–7.
34. Bret PM, Reinhold C. Magnetic resonance cholangiopancre-atography. Endoscopy 1997;29:472–86.
35. Siegel JH, Veerappan A, Cohen SA, Kasmin FE. Endoscopicsphincterotomy for biliary pancreatitis: An alternative to cho-lecystectomy in high-risk patients. Gastrointest Endosc 1994;40:573–5.
36. Welbourn CR, Beckly DE, Eyre-Brook IA. Endoscopicsphincterotomy without cholecystectomy for gallstone pan-creatitis. Gut 1995;37:119–20.
37. Bank S, Indaram A. Causes of acute and recurrent pancre-atitis. Gastroenterol Clin North Am 1999;28:571–89.
38. Raddawi HM, Geenen JE, Hogan WJ, et al. Pressure mea-surement from biliary and pancreatic segments of sphincterof Oddi. Comparison between patients with functional ab-dominal pain, biliary, or pancreatic disease. Dig Dis Sci1991;36:71–4.
39. Lans JL, Parikh NP, Geenen JE. Applications of sphincter ofOddi manometry in routine clinical investigations. Endos-copy 1991;23:139–43.
40. Hogan WJ, Geenen JE, Dodds WJ. Dysmotility disturbancesof the biliary tract: Classification, diagnosis, and treatment.Semin Liver Dis 1987;7:302–10.
41. Geenen JE, Hogan WJ, Dodds WJ, et al. Intraluminal pres-sure recording from the human sphincter of Oddi. Gastroen-terology 1980;78:317–24.
42. Hogan WJ, Sherman S, Pasricha P, Carr-Locke D. Sphincterof Oddi manometry. Gastrointest Endosc 1997;45:342–8.
43. Khuroo MS, Zargar SA, Yattoo GN. Efficacy of nifedipinetherapy in patients with sphincter of Oddi dysfunction: Aprospective, double-blind, randomized, placebo-controlled,cross over trial. Br J Clin Pharmacol 1992;33:477–85.
44. Kalloo AN, Pasricha PJ. Therapy of sphincter of Oddi dys-function. Gastrointest Endosc Clin North Am 1996;6:117–25.
45. Geenen JE, Hogan WJ, Dodds WJ, et al. The efficacy ofendoscopic sphincterotomy after cholecystectomy in patientswith suspected sphincter of Oddi dysfunction. N Engl J Med1989;320:82–7.
46. Neoptolemos JP, Bailey IS, Carr-Locke DL. Sphincter ofOddi dysfunction: Results of treatment by endoscopicsphincterotomy. Br J Surg 1988;75:454–9.
47. McCarthy J, Geenen JE, Hogan WJ. Preliminary experiencewith endoscopic stent placement in benign pancreatic dis-ease. Gastrointest Endosc 1988;34:16–8.
48. Ashby K, Lo SK. The role of pancreatic stenting in obstruc-tive ductal disorders other than pancreas divisum. Gastroin-test Endosc 1995;42:306–11.
49. Toouli J, Di Francesco V, Saccone G, et al. Division of thesphincter of Oddi for treatment of dysfunction associatedwith recurrent pancreatitis. Br J Surg 1996;83:1205–10.
50. Bartlett MK, Nardi GL. Treatment of recurrent pancreatitisby transduodenal sphincterotomy and exploration of the pan-creatic duct. N Engl J Med 1960;262:643–8.
51. Wehrmann T, Seifert H, Seipp M, et al. Endoscopic injectionof botulinum toxin for biliary sphincter of Oddi dysfunction.Endoscopy 1998;30:702–7.
52. Slivka A, Chuttani R, Carr-Locke DL, et al. Inhibition ofsphincter of Oddi function by the nitric oxide carrier S-nitroso-N-acetylcysteine in rabbits and humans. J Clin Invest1994;94:1792–8.
53. Kozarek RA. Balloon dilations of the sphincter of Oddi.Endoscopy 1988;20(suppl 1):207–10.
54. Rolny P. Endoscopic bile duct stent placement as a predictorof outcome following endoscopic sphincterotomy in patientswith suspected sphincter of Oddi dysfunction. Eur J Gastro-enterol Hepatol 1997;9:467–71.
55. Goff JS. Common bile duct sphincter of Oddi stenting inpatients with suspected sphincter dysfunction. Am J Gastro-enterol 1995;90:586–9.
56. Silverman WB, Ruffolo TA, Sherman S, et al. Correlation ofbasal sphincter pressures measured from both the bile ductand pancreatic duct in patients with suspected sphincter ofOddi dysfunction. Gastrointest Endosc 1992;38:440–3.
57. Funch-Jensen P, Kruse A. Manometric activity of the pan-creatic duct sphincter in patients with total bile duct sphinc-terotomy for sphincter of Oddi dyskinesia. Scand J Gastro-enterol 1987;22:1067–70.
58. Freeman ML, Nelson DB, Sherman S, et al. Complications ofendoscopic biliary sphincterotomy. N Engl J Med 1996;335:909–18.
59. Tarnasky PR, Palesch YY, Cunningham JT, et al. Pancreaticstenting prevents pancreatitis after biliary sphincterotomy inpatients with sphincter of Oddi dysfunction. Gastroenterol-ogy 1998;115:1518–24.
60. Bernard JP, Sahel J, Giovannini M, Sarles H. Pancreas divi-sum is a probable cause of acute pancreatitis: A report of 137cases. Pancreas 1990;5:248–54.
61. Cotton PB. Congenital anomaly of pancreas divisum as acause of obstructive pain and pancreatitis. Gut 1980;21:105–14.
62. Jacob L, Geenen JE, Catalano MF, et al. Clinical presentationand short-term outcome of endoscopic therapy of patientswith symptomatic incomplete pancreas divisum. GastrointestEndosc 1999;49:53–7.
2552 Levy and Geenen AJG – Vol. 96, No. 9, 2001
63. Bhutani MS, Hoffman BJ, Hawes RH. Diagnosis of pancreasdivisum by endoscopic ultrasonography. Endoscopy 1999;31:167–9.
64. Soto JA, Barish MA, Yucel EK, et al. Magnetic resonancecholangiography: Comparison with endoscopic retrogradecholangiopancreatography. Gastroenterology 1996;110:589–97.
65. Barish MA, Soto JA, Yucel EK. Magnetic resonance cholan-giopancreatography of the biliary ducts: Techniques, clinicalapplications, and limitations. Top Magn Reson Imaging1996;8:302–11.
66. Lehman GA, Sherman S, Nisi R, Hawes RH. Pancreasdivisum: Results of minor papilla sphincterotomy. Gastroin-test Endosc 1993;39:1–8.
67. Lans JI, Geenen GE, Johanson JF, Hogan WJ. Endoscopictherapy in patients with pancreas divisum and acutepancreatitis: A prospective, randomized, controlled clinicaltrial. Gastrointest Endosc 1992;38:430–4.
68. Warshaw AL, Richter JM, Schapiro RH. The cause andtreatment of pancreatitis associated with pancreas divisum.Ann Surg 1983;198:443–52.
69. Bradley EL 3d, Stephan RN. Accessory duct sphincteroplastyis preferred for long-term prevention of recurrent acute pan-creatitis in patients with pancreas divisum. J Am Coll Surg1996;183:65–70.
70. Satterfield ST, McCarthy JH, Geenen JE, et al. Clinicalexperience in 82 patients with pancreas divisum: Preliminaryresults of manometry and endoscopic therapy. Pancreas1988;3:248–53.
71. Kozarek RA, Ball TJ, Patterson DJ, et al. Endoscopic ap-proaches to pancreas divisum. Dig Dis Sci 1995;40:1974–81.
72. Kozarek RA. Pancreatic stents can induce ductal changesconsistent with chronic pancreatitis. Gastrointest Endosc1990;36:93–5.
73. Siegel J, Veerappan A. Endoscopic management of pancre-atic disorders: Potential risks of pancreatic prosthesis. En-doscopy 1991;23:177–80.
74. Lehman GA. Sherman S. Diagnosis and therapy of pancreasdivisum. Gastrointest Endosc Clin North Am 1998;8:55–77.
75. Whitcomb DC, Preston RA, Aston CE, et al. A gene forhereditary pancreatitis maps to chromosome 7q35. Gastro-enterology 1996;110:1975–80.
76. Gorry MC, Gabbaizedeh D, Furey W, et al. Mutations in thecationic trypsinogen gene are associated with recurrent acuteand chronic pancreatitis. Gastroenterology 1997;113:1063–8.
77. Whitcomb DC, Gorry MC, Preston RA, et al. Hereditarypancreatitis is caused by a mutation in the cationic trypsino-gen gene. Nat Genet 1996;14:141–5.
78. Lowenfels AB, Maisonneuve P, DiMagno EP, et al. Hered-itary pancreatitis and the risk of pancreatic cancer. Interna-tional Hereditary Pancreatitis Study Group. J Natl CancerInst 1997;89:442–6.
79. Davis PB, Drumm M, Konstan MW. Cystic fibrosis. Am JRespir Crit Care Med 1996;154:1229–56.
80. Kerem B, Rommens JM, Buchanan JA, et al. Identification ofthe cystic fibrosis gene: Genetic analysis. Science 1989;245:1073–80.
81. Kopelman H, Durie P, Gaskin K, et al. Pancreatic fluidsecretion and protein hyperconcentration in cystic fibrosis.N Engl J Med 1985;312:329–34.
82. Choudari CP, Lehman GA, Sherman S. Pancreatitis andcystic fibrosis gene mutations. Gastroenterol Clin North Am1999;28:543–9.
83. Oppenheimer EH, Esterly JR. Pathology of cystic fibrosis:
Review of the literature and comparison with 146 autopsiedcases. Perspect Pediatr Pathol 1975;2:241–78.
84. Zielenski J, Tsui LC. Cystic fibrosis: Genotypic and pheno-typic variations. Annu Rev Genet 1995;29:777–807.
85. Rommens JM, Iannuzzi MC, Kerem B, et al. Identification ofthe cystic fibrosis gene: Chromosome walking and jumping.Science 1989;245:1059–65.
86. Cohn JA, Jowell PS. Are mutations in the cystic fibrosis geneimportant in chronic pancreatitis. Surg Clin North Am 1999;79:723–31.
87. Chillon M, Casals T, Mercier B, et al. Mutations in the cysticfibrosis gene in patients with congenital absence of the vasdeferens. N Engl J Med 1995;332:1475–80.
88. Sharer N, Schwarz M, Malone G, et al. Mutations of thecystic fibrosis gene in patients with chronic pancreatitis.N Engl J Med 1998;339:645–52.
89. Todani T, Watanabe Y, Narusue M, et al. Congenital bileduct cysts: Classification, operative procedures, and reviewof thirty-seven cases including cancer arising from chole-dochal cyst. Am J Surg 1977;134:263–9.
90. Venu RP, Geenen JE. Periampullary region: Physiology andpathophysiology. In: Silvis S, Rohrmann CA, Ansel HJ, eds.Text and atlas of endoscopic retrograde cholangiopancre-atography. New York: Igaku-Shoin, 1995:146–67.
91. Venu RP, Geenen JE, Hogan WJ, et al. Role of endoscopicretrograde cholangiopancreatography in the diagnosis andtreatment of choledochocele. Gastroenterology 1984;87:1144–9.
92. Schulte SJ. Embryology, and congenital anomalies of the bileand pancreatic ducts. In: Silvis S, Rohrmann CA, Ansel HJ,eds. Text and atlas of endoscopic retrograde cholangiopan-creatography. New York: Igaku-Shoin, 1995:114–45.
93. Taourel P, Bret PM, Reinhold C, et al. Anatomic variants ofthe biliary tree: Diagnosis with MR cholangiopancreatogra-phy. Radiology 1996;199:521–7.
94. Lopez RR, Pinson CW, Campbell JR, et al. Variation inmanagement based on type of choledochal cyst. Am J Surg1991;161:612–5.
95. Kochhar R, Nagi B, Chawla S, et al. The clinical spectrum ofanomalous pancreatobiliary junction. Surg Endosc 1989;3:83–6.
96. Sugiyama M, Atomi Y. Endoscopic ultrasonography for di-agnosing anomalous pancreaticobiliary junction. GastrointestEndosc 1997;45:261–7.
97. Barish M, Soto J, Ferrucci J. Magnetic resonance pancre-atography. Endoscopy 1997;29:487–95.
98. Ravitch MM. The pancreas in infants and children. Surg ClinNorth Am 1975;55:377–85.
99. Itoh Y, Hada T, Terano A, et al. Pancreatitis in the annulusof annular pancreas demonstrated by the combined use ofcomputed tomography and endoscopic retrograde cholangio-pancreatography. Am J Gastroenterol 1989;84:961–4.
100. Kiernan PD, ReMine S, Kiernan PC, Remine WH. Annularpancreas: Mayo Clinic experience from 1957 to 1976 withreview of the literature. Arch Surg 1980:115:46–50.
101. Lloyd-Jones W, Mountain JC, Warren KW. Annular pan-creas in the adult. Ann Surg 1972;176:163–70.
102. Gress F, Yiengpruksawan A, Sherman S, et al. Diagnosis ofannular pancreas by endoscopic ultrasound. Gastrointest En-dosc 1996;44:485–9.
103. Robertson JF, Imrie CW. Acute pancreatitis associated withcarcinoma of the ampulla of Vater. Br J Surg 1987;74:395–7.
104. Simpson WF, Adams DB, Metcalf JF, Anderson MC. Non-functioning pancreatic neuroendocrine tumors presenting aspancreatitis: Report of four cases. Pancreas 1988;3:223–31.
105. Rosch T, Braig C, Gain J, et al. Staging of pancreatic andampullary carcinoma by endoscopic ultrasonography. Com-
2553AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis
parison with conventional sonography, computed tomogra-phy, and angiography. Gastroenterology 1992;102:188–99.
106. Legmann P, Vignaux O, Dousset B, et al. Pancreatic tumors:Comparison of dual-phase helical CT and endoscopic sonog-raphy. AJR 1998;170:1315–22.
107. Muller MF, Meyenberger C, Bertschinger P, et al. Pancreatictumors: Evaluation with endoscopic US, CT and MR imag-ing. Radiology 1994;190:745–51.
108. Rosch T. Staging of pancreatic cancer: Analysis of literatureresults. Gastrointest Endosc Clin North Am 1995;5:735–9.
109. Rosch T, Lightdale CJ, Botet JF, et al. Localization of pan-creatic endocrine tumors by endoscopic ultrasonography.N Engl J Med 1992;326:1721–6.
110. Wiersema MJ, Vilmann P, Giovannini M, et al. Endosonog-raphy-guided fine-needle aspiration biopsy: Diagnostic accu-racy and complication assessment. Gastroenterology 1997;112:1087–95.
111. Venu RP, Geenen JE, Kini M, et al. Endoscopic retrogradebrush cytology: A new technique. Gastroenterology 1990;99:1475–9.
112. Moossa AR, Gamagami RA. Diagnosis and staging of pan-creatic neoplasms. Surg Clin North Am 1995;75:871–90.
113. Barkin JS, Goldstein JA. Diagnostic approach to pancreaticcancer. Gastroenterol Clin North Am 1999;28:709–22.
114. Gudjonsson B. Carcinoma of the pancreas: Critical analysisof the costs, results of resections, and the need for standard-ized reporting. J Am Coll Surg 1995;181:483–503.
115. Pereira-Lima JC, Jakobs R, Maier M, et al. Endoscopicbiliary stenting for the palliation of pancreatic cancer: Re-sults, survival predictive factors, and comparison of 10-French with 11.5-French gauge stents. Am J Gastroenterol1996;91:2179–84.
116. Ballinger AB, McHugh M, Catnach SM, et al. Symptomrelief and quality of life after stenting for malignant bile ductobstruction. Gut 1994;35:467–70.
117. Siech M, Tripp K, Schmidt-Rohlfing B, et al. Cystic tumoursof the pancreas: Diagnostic accuracy, pathologic observa-tions and surgical consequences. Langenbecks Arch Surg1998;383:56–61.
118. Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical andpathologic correlation of 84 mucinous cystic neoplasms ofthe pancreas: Can one reliably differentiate benign frommalignant (or premalignant) neoplasms? Ann Surg 2000;231:205–12.
119. Wilentz RE, Albores-Saavedra J, Zahurak M, et al. Patho-logic examination accurately predicts prognosis in mucinouscystic neoplasms of the pancreas. Am J Surg Pathol 1999;23:1320–7.
120. Procacci C, Biasiutti C, Carbognin G, et al. Characterizationof cystic tumors of the pancreas: CT accuracy. J ComputAssist Tomogr 1999;23:906–12.
121. Le Borgne J, de Calan L, Partensky C. Cystadenomas andcystadenocarcinomas of the pancreas. A multiinstitutionalretrospective study of 398 cases. French Surgical Associa-tion. Ann Surg 1999;230:152–61.
122. Sand JA, Hyoty MK, Mattila J, et al. Clinical assessmentcompared with cyst fluid analysis in the differential diagnosisof cystic lesions in the pancreas. Surgery 1996;119:275–80.
123. Hammel P, Voitot H, Vilgrain V, et al. Diagnostic value ofCA 72–4 and carcinoembryonic antigen determination in thefluid of pancreatic cystic lesions. Eur J Gastroenterol Hepatol1998;10:345–8.
124. Stolte M, Pscherer C. Adenomacarcinoma sequence in thepapilla of Vater. Scand J Gastroenterol 1996;31:376–82.
125. Yamaguchi K, Enjoji M. Carcinoma of the ampulla of vater:A clinicopathologic study and pathologic staging of 109
cases of carcinoma and 5 cases of adenoma. Cancer 1987;59:506–15.
126. Sperti C, Pasquali C, Piccoli A, et al. Radical resection forampullary carcinoma: Long-term results. Br J Surg 1994;81:668–71.
127. Tarazi RY, Hermann RE, Vogt DP, et al. Results of surgicaltreatment of periampullary tumors: A thirty-five-year expe-rience. Surgery 1986;100:716–23.
128. Chijiiwa K, Yamashita H, Kuroki S. Wide ampullectomy forpatients with villous adenoma of duodenal papilla and fol-low-up results of pancreaticobiliary tract. Int Surg 1994;79:178–82.
129. Asbun HJ, Rossi RL, Munson JL. Local resection for amp-ullary tumors: Is there a place for it? Arch Surg 1993;128:515–20.
130. Tsao JI, Rossi RL, Lowell JA. Pylorus-preserving pancre-atoduodenectomy. Is it an adequate cancer operation? ArchSurg 1994;129:405–12.
131. Binmoeller KF, Boaventura S, Ramsperger K, Soehendra N.Endoscopic snare excision of benign adenomas of the papillaof Vater. Gastrointest Endosc 1993;39:127–31.
132. Ponchon T, Berger F, Chavaillon A, et al. Contribution ofendoscopy to diagnosis and treatment of tumors of the am-pulla of Vater. Cancer 1989;64:161–7.
133. Lambert R, Ponchon T, Chavaillon A, Berger F. Laser treat-ment of tumors of the papilla of Vater. Endoscopy 1988;20(suppl 1):227–31.
134. Sarre RG, Frost AG, Jagelman DG, et al. Gastric and duo-denal polyps in familial adenomatous polyposis: A prospec-tive study of the nature and prevalence of upper gastrointes-tinal polyps. Gut 1987;28:306–14.
135. Sawada T, Muto T. Familial adenomatous polyposis: Shouldpatients undergo surveillance of the upper gastrointestinaltract? Endoscopy 1995;27:6–11.
136. Kloppel G, Maillet B. The morphological basis for the evo-lution of acute pancreatitis into chronic pancreatitis. Vir-chows Arch 1992;420:1–4.
137. Catalano MF, Lahoti S, Geenen JE, Hogan WJ. Prospectiveevaluation of endoscopic ultrasonography, endoscopic retro-grade pancreatography, and secretin test in the diagnosis ofchronic pancreatitis. Gastrointest Endosc 1998;48:11–7.
138. Sahai AV, Zimmerman M, Aabakken L, et al. Prospectiveassessment of the ability of endoscopic ultrasound to diag-nose, exclude, or establish the severity of chronic pancreatitisfound by endoscopic retrograde pancreatography. Gastroin-test Endosc 1998;48:18–25.
139. Wiersema MJ, Hawes RH, Lehman GA, et al. Prospectiveevaluation of endoscopic ultrasonography and endoscopicretrograde cholangiopancreatography in patients withchronic abdominal pain of suspected pancreatic origin. En-doscopy 1993;25:555–64.
140. Soto JA, Barish MA, Yucel EK, et al. Pancreatic duct. MRcholangiopancreatography with a three-dimensional fastspin-echo technique. Radiology 1995;196:459–64.
141. Takehara Y, Ichijo K, Tooyama N, et al. Breath-hold MRcholangiopancreatography with a long-echo-train fast spin-echo sequence, and a surface coil in chronic pancreatitis.Radiology 1994;192:73–8.
142. Levy P, Milan C, Pignon JP, et al. Mortality factors associ-ated with chronic pancreatitis: Unidimensional and multidi-mensional analysis of a medical-surgical series of 240 pa-tients. Gastroenterology 1989;96:1165–72.
143. Ammann RW, Akovbiantz A, Largiader F, Schueler G.Course and outcome of chronic pancreatitis: Longitudinalstudy of a mixed medical-surgical series of 245 patients.Gastroenterology 1984;86:820–8.
144. Kozarek RA, Ball TJ, Patterson DJ. Endoscopic approach to
2554 Levy and Geenen AJG – Vol. 96, No. 9, 2001
pancreatic duct calculi and obstructive pancreatitis. Am JGastroenterol 1992;87:600–3.
145. Catalano MF, Geenen JE, Schmalz MJ, et al. Treatment ofpancreatic pseudocysts with ductal communications by trans-papillary pancreatic duct endoprosthesis. Gastrointest Endosc1995;42:214–8.
146. Dumonceau JM, Deviere J, Le Moine O, et al. Endoscopicpancreatic drainage in chronic pancreatitis associated withductal stones: Long-term results. Gastrointest Endosc 1996;43:547–55.
147. Gregor JC, Ponich TP, Detsky AS. Should ERCP be routineafter an episode of “ idiopathic” pancreatitis? A cost-utilityanalysis. Gastrointest Endosc 1996;44:118–23.
148. Sugiyama M, Wada N, Atomi Y, et al. Diagnosis of acutepancreatitis: Value of endoscopic sonography. AJR Am JRoentgenol 1995;165:867–72.
149. Di Francesco V, Brunori MP, Rigo L, et al. Comparison ofultrasound-secretin test and sphincter of Oddi manometry inpatients with recurrent acute pancreatitis. Dig Dis Sci 1999;44:336–40.
150. Barish MA, Yucel EK, Ferrucci J. Magnetic resonancecholangiopancreatography. N Engl J Med 1999;341:258–64.
151. Bret PM, Reinhold C, Taourel P, et al. Pancreas divisum:Evaluation with MR cholangiopancreatography. Radiology1996;199:99–103.
152. Slaff J, Jacobson D, Tillman CR, et al. Protease-specificsuppression of pancreatic exocrine secretion. Gastroenterol-ogy 1984;87:44–52.
153. Uden S, Bilton D, Nathan L, et al. Antioxidant therapy forrecurrent pancreatitis: Placebo-controlled trial. Aliment Phar-macol Ther 1990;4:357–71.
154. Kozarek RA, Patterson DJ, Ball TJ, Traverso LW. Endo-scopic placement of pancreatic stents and drains in the man-agement of pancreatitis. Ann Surg 1989;209:261–6.
155. Jacob L, Geenen JE, Schmalz MJ, et al. Prevention of pan-creatitis in patients with idiopathic recurrent pancreatitis(IRP): A prospective randomized study using endoscopicstents. Gastroenterology 1995;108:362A.
156. Carey LC. Recurrent acute pancreatitis—rarely idiopathic:1989 Du Pont Lecture. Can J Surg 1990:33:107–12.
157. Paricio PP, Olmo DG, Franco EP, et al. Gallbladdercholesterolosis: An aetiologic factor in acute pancreatitis ofuncertain origin. Br J Surg 1990;77:735–6.
2555AJG – September, 2001 Idiopathic Acute Recurrent Pancreatitis