pseudo- et hyperprogression tumorale
TRANSCRIPT
Pseudo- et Hyperprogression tumorale
Esma Saada-Bouzid, MD, PhD
Medical Oncologist, CAL, Nice
« Avec le soutien organisationnel de Bristol-Myers Squibb »
Liens d’intérêt
Invitations congrès:
Merck Serono, Astra Zeneca, MSD
Astra Zeneca, Merck Serono, Investigateurs:
BMS, Ipsen, Astra Zeneca, MSD
Advisory Board:
BMS, Astra Zeneca, Merck Serono
« Le contenu et/ou les opinions exprimées lors de cette présentation,
notamment celui ou celle(s) relatifs à la stratégie thérapeutique ont
été réalisés en toute indépendance »
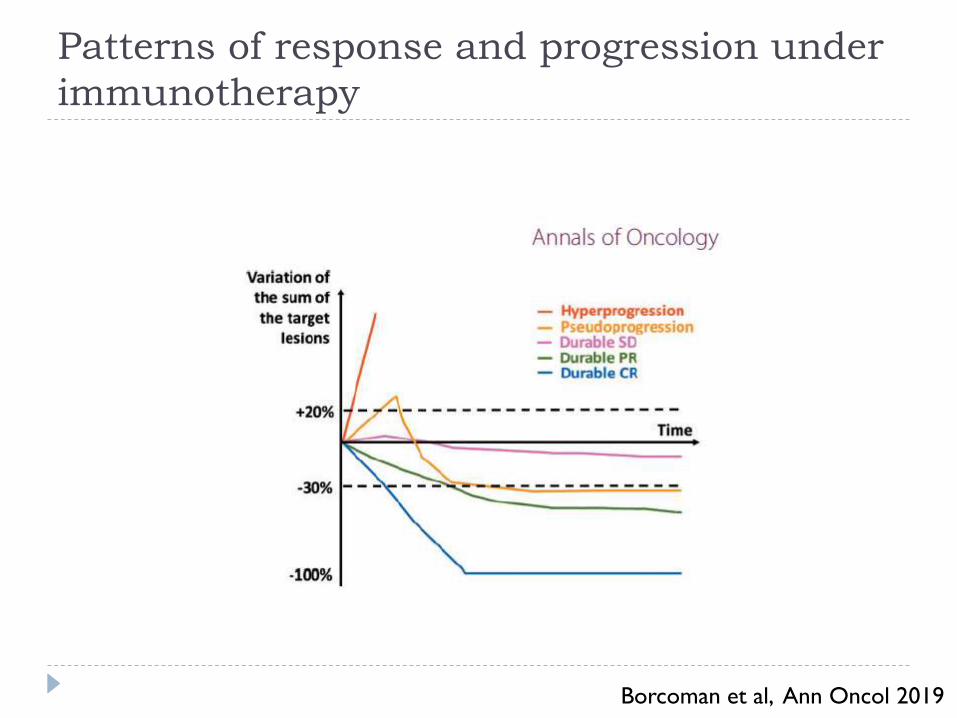
Patterns of response and progression under
immunotherapy
Borcoman et al, Ann Oncol 2019
Pseudoprogression
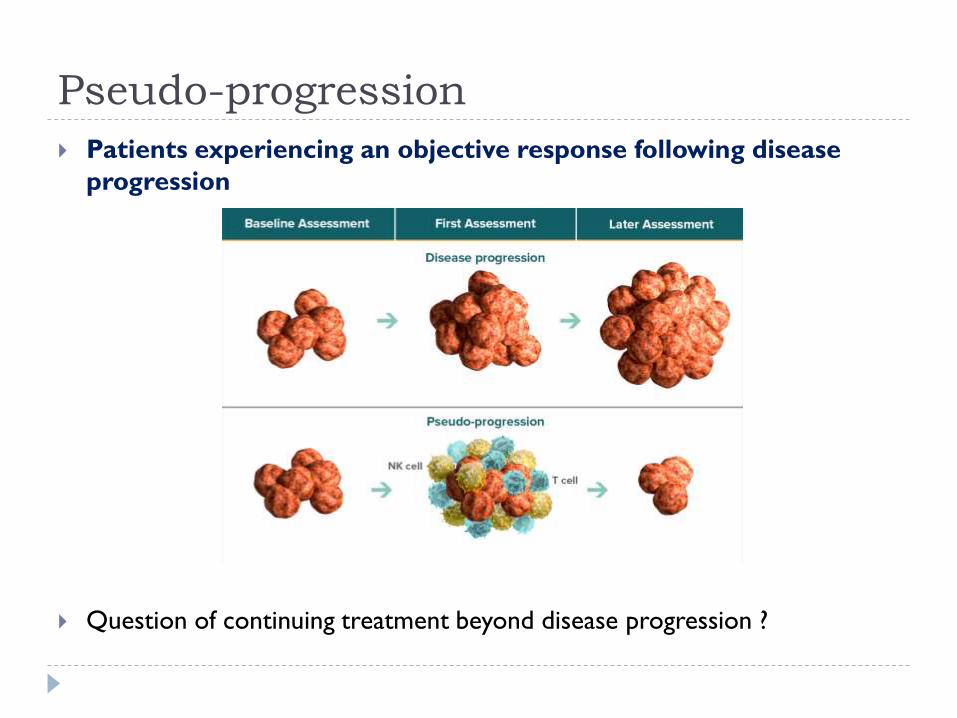
Pseudo-progression
Patients experiencing an objective response following disease
progression
Question of continuing treatment beyond disease progression ?
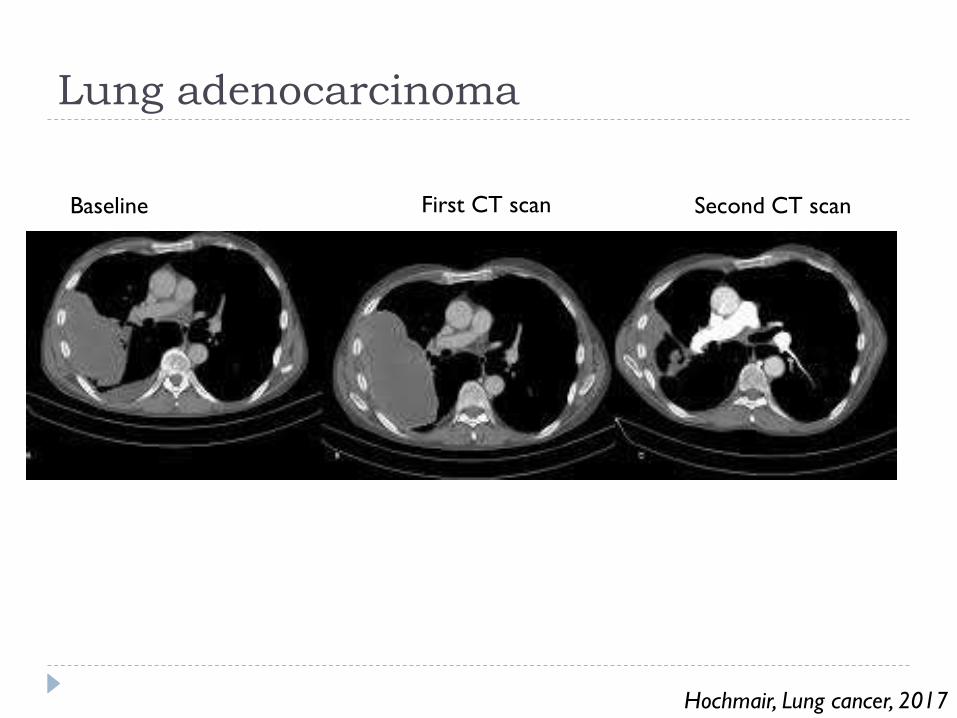
Lung adenocarcinoma
Hochmair, Lung cancer, 2017
Baseline First CT scan Second CT scan
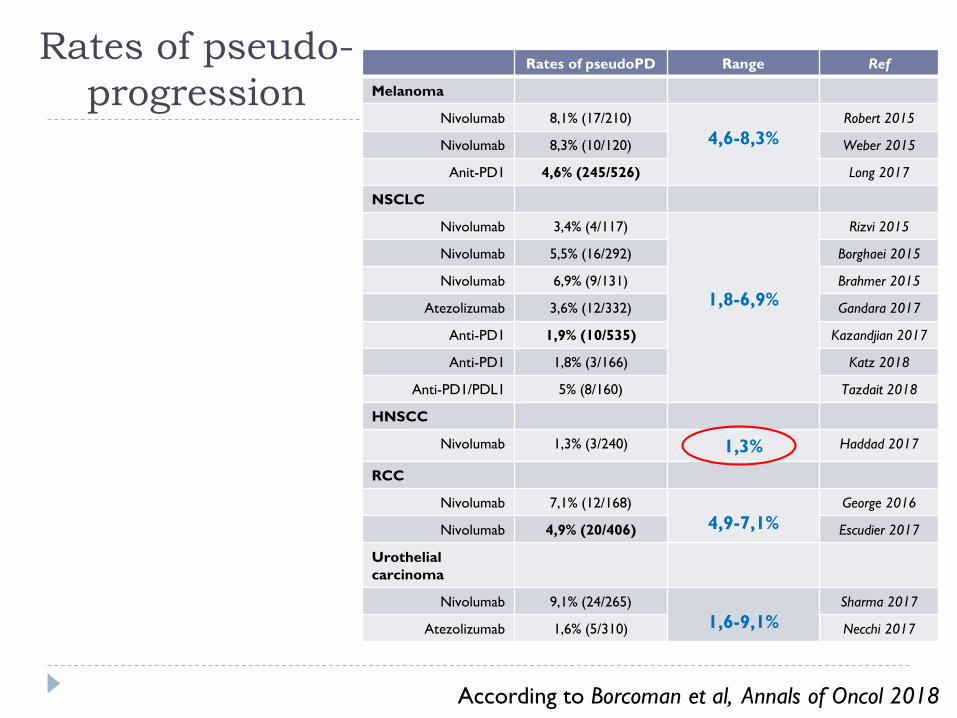
Rates of pseudo-
progression Rates of pseudoPD Range Ref
Melanoma
Nivolumab 8,1% (17/210)
4,6-8,3%Robert 2015
Nivolumab 8,3% (10/120) Weber 2015
Anit-PD1 4,6% (245/526) Long 2017
NSCLC
Nivolumab 3,4% (4/117)
1,8-6,9%
Rizvi 2015
Nivolumab 5,5% (16/292) Borghaei 2015
Nivolumab 6,9% (9/131) Brahmer 2015
Atezolizumab 3,6% (12/332) Gandara 2017
Anti-PD1 1,9% (10/535) Kazandjian 2017
Anti-PD1 1,8% (3/166) Katz 2018
Anti-PD1/PDL1 5% (8/160) Tazdait 2018
HNSCC
Nivolumab 1,3% (3/240) 1,3% Haddad 2017
RCC
Nivolumab 7,1% (12/168)
4,9-7,1%George 2016
Nivolumab 4,9% (20/406) Escudier 2017
Urothelial
carcinoma
Nivolumab 9,1% (24/265)
1,6-9,1%Sharma 2017
Atezolizumab 1,6% (5/310) Necchi 2017
According to Borcoman et al, Annals of Oncol 2018
Pseudo-progression
Pseudo-progression remains a rare event and the
majority of patients who have disease progression have a
real progression
Decision of treatment beyond progression should be
only taken in carefully selected patients who
experience a clinical benefit and who have not
experienced severe toxicities
Hyperprogression
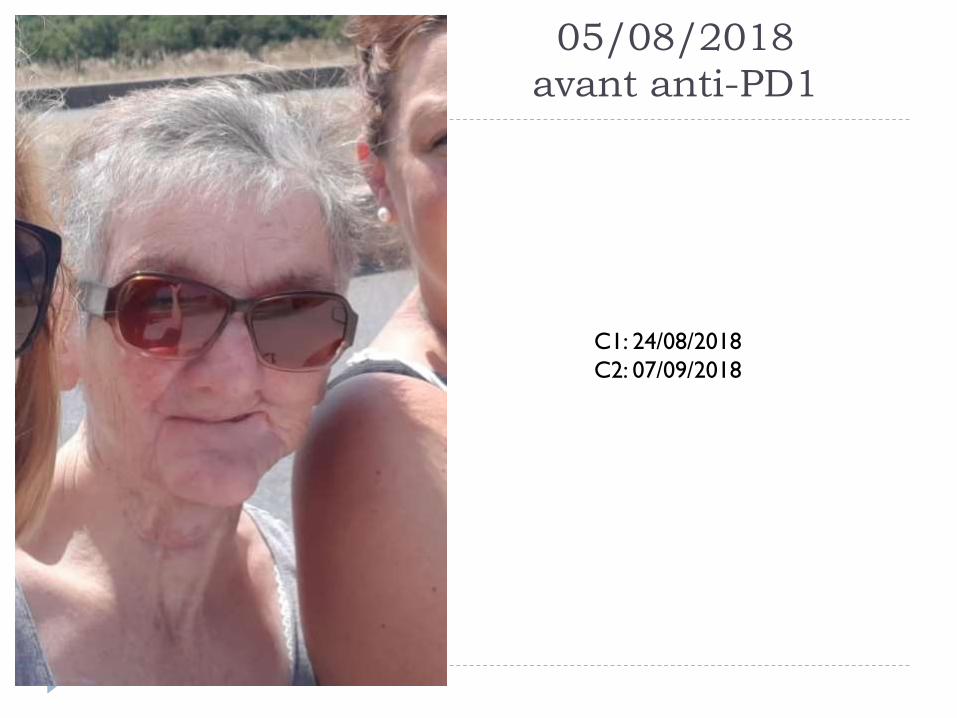
05/08/2018
avant anti-PD1
C1: 24/08/2018
C2: 07/09/2018
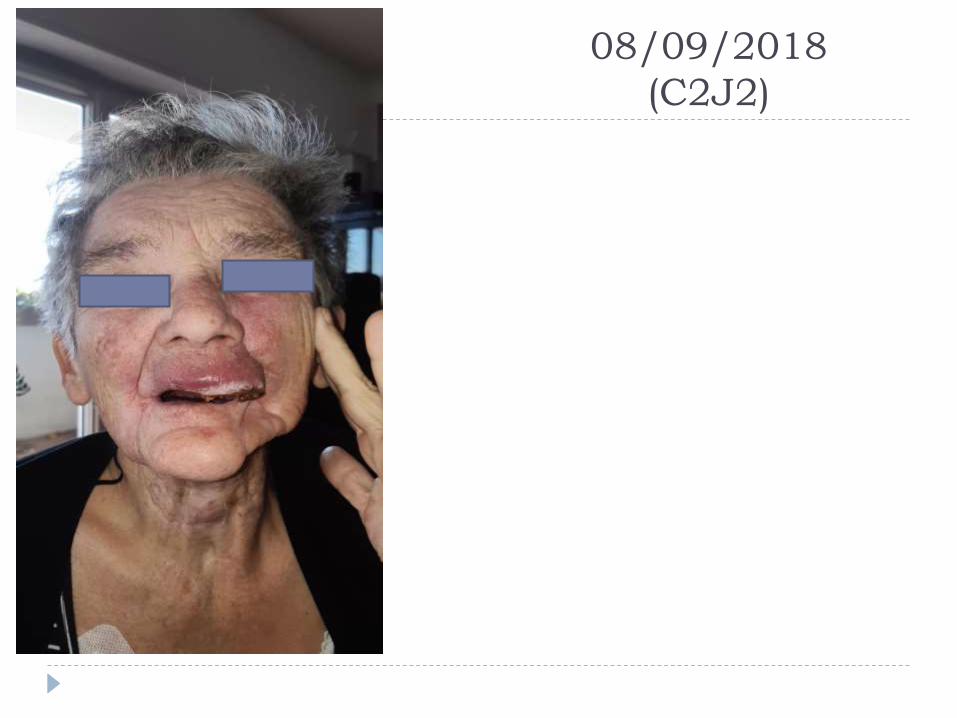
08/09/2018
(C2J2)

05/10/2018
C4J1
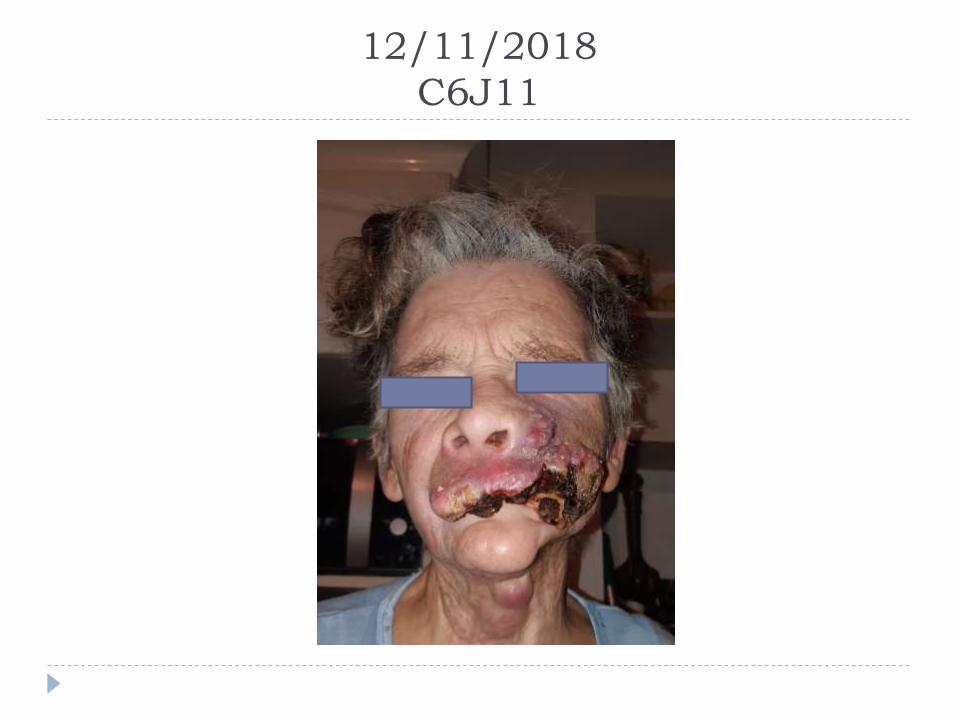
12/11/2018
C6J11
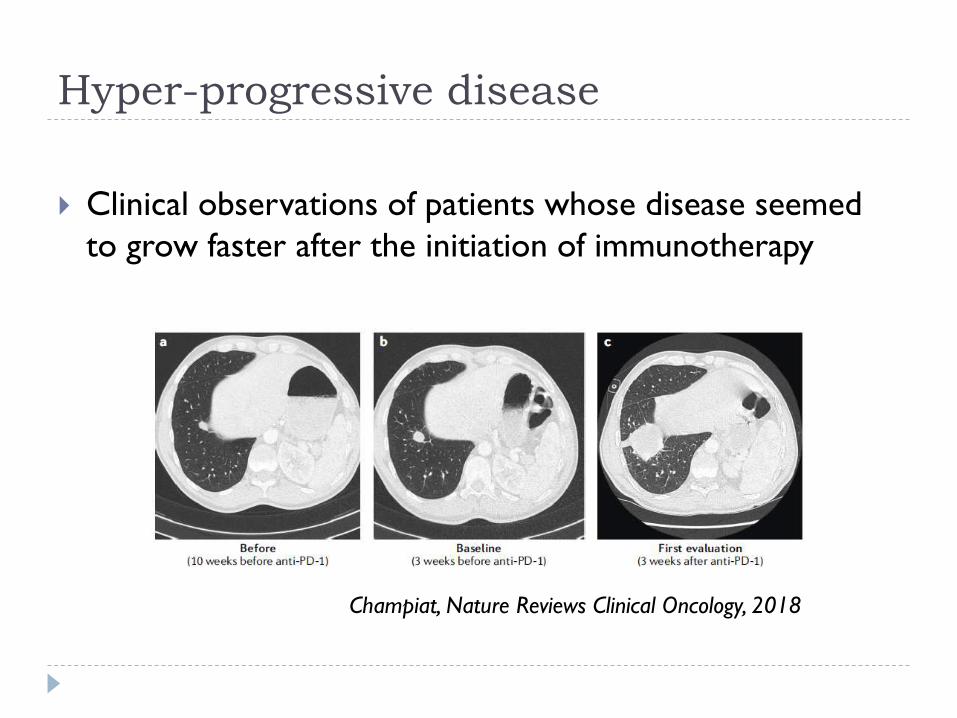
Hyper-progressive disease
Clinical observations of patients whose disease seemed
to grow faster after the initiation of immunotherapy
Champiat, Nature Reviews Clinical Oncology, 2018
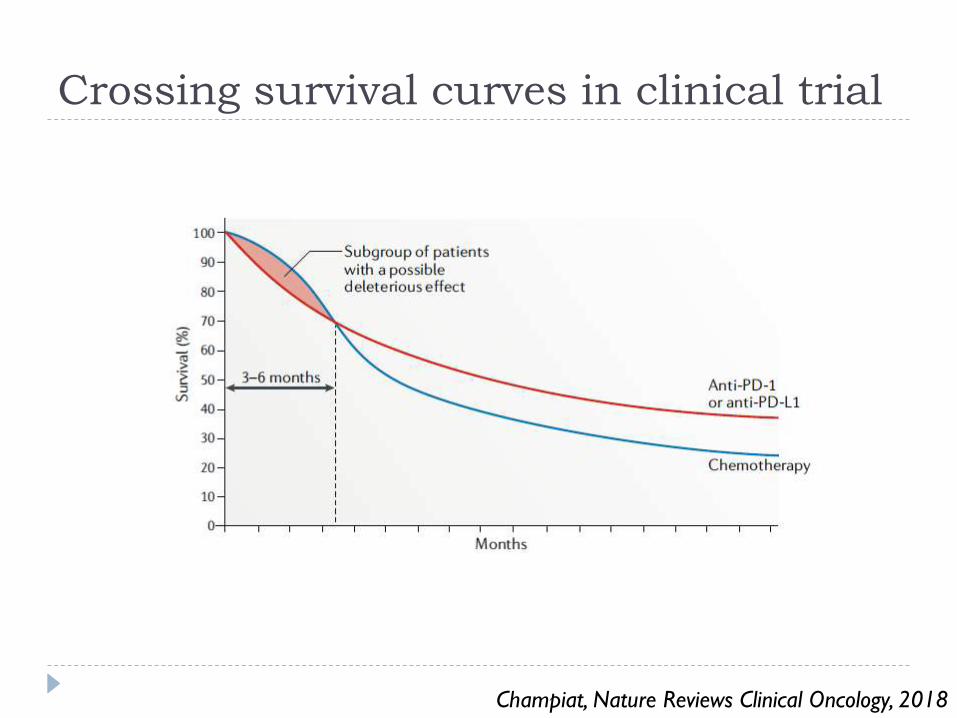
Crossing survival curves in clinical trial
Champiat, Nature Reviews Clinical Oncology, 2018
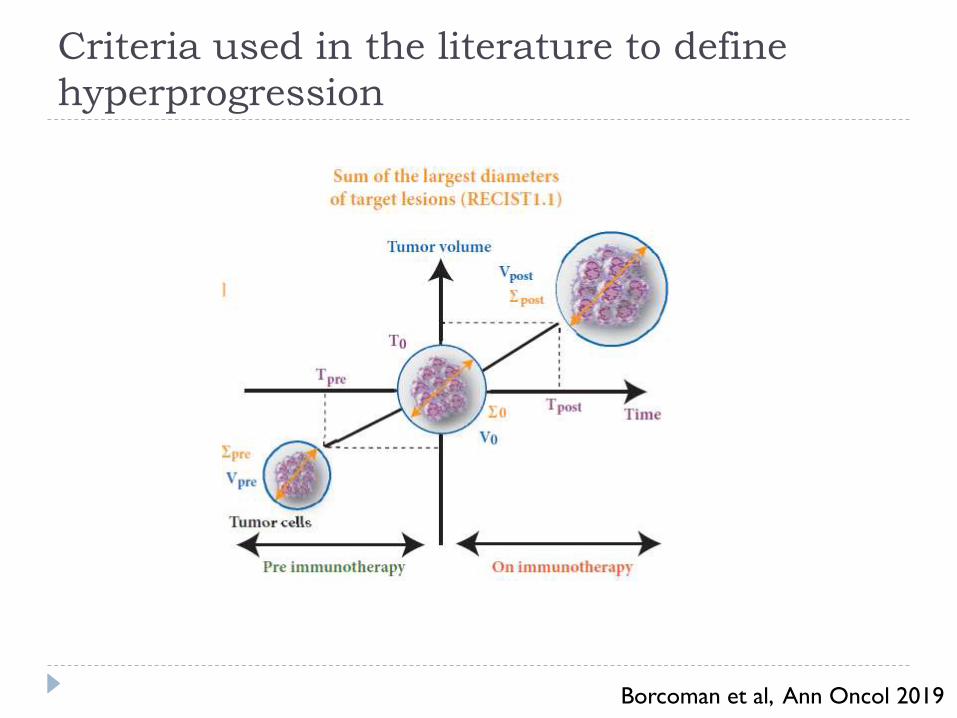
Criteria used in the literature to define
hyperprogression
Borcoman et al, Ann Oncol 2019
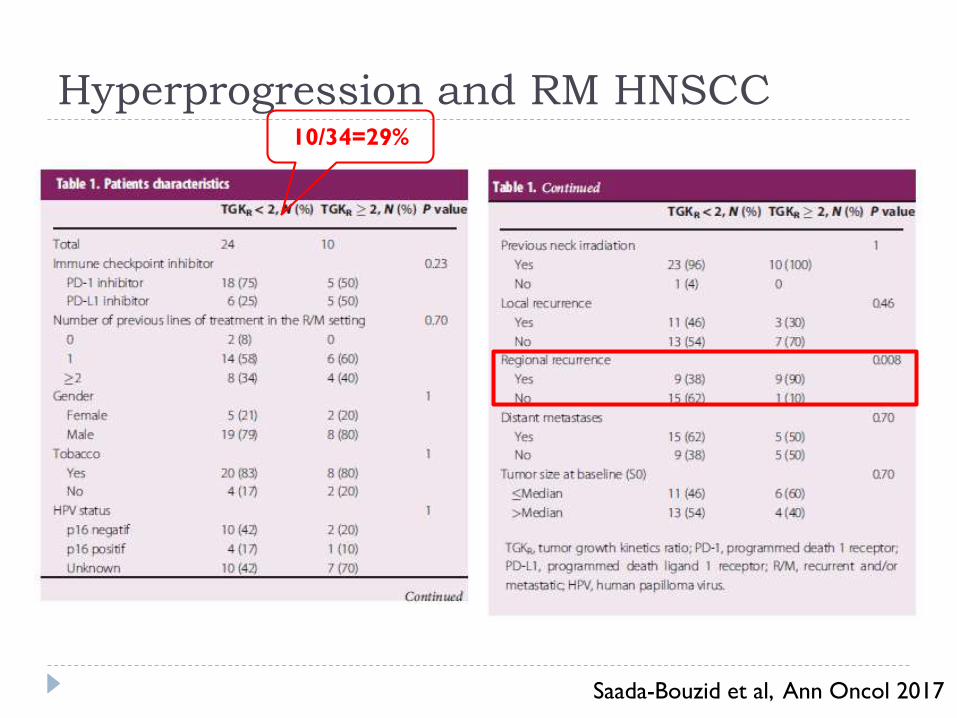
Hyperprogression and RM HNSCC
Saada-Bouzid et al, Ann Oncol 2017
10/34=29%
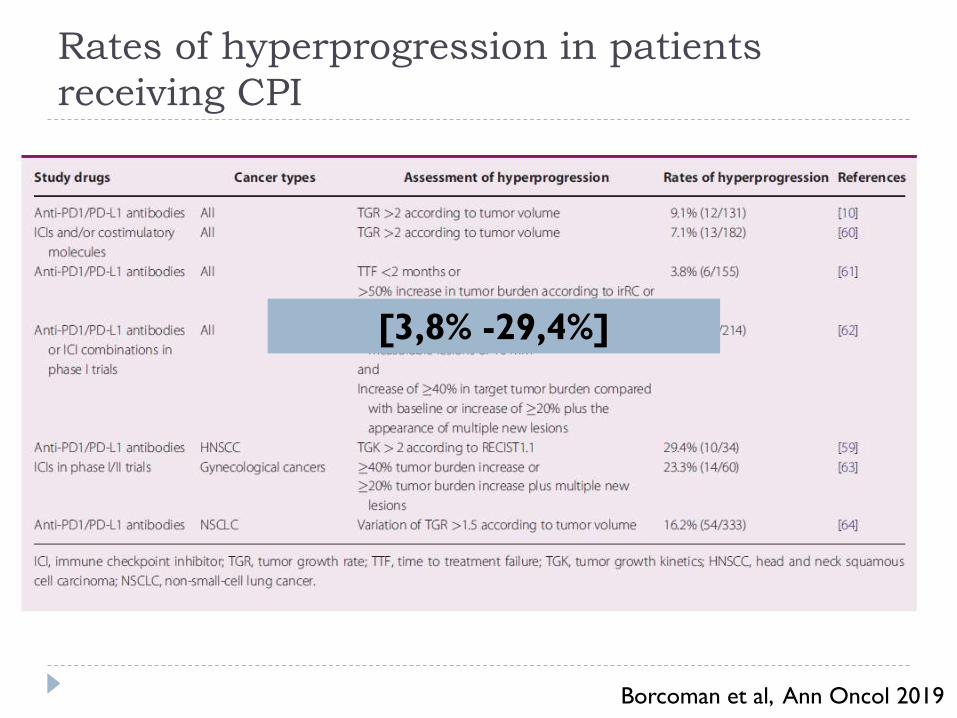
Rates of hyperprogression in patients
receiving CPI
Borcoman et al, Ann Oncol 2019
[3,8% -29,4%]
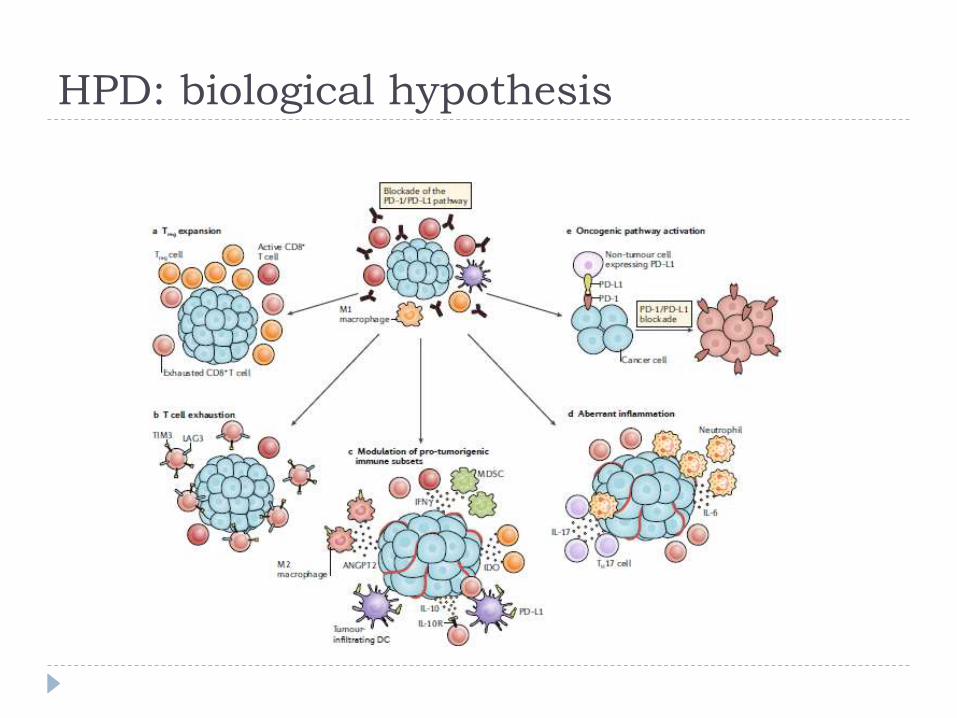
HPD: biological hypothesis
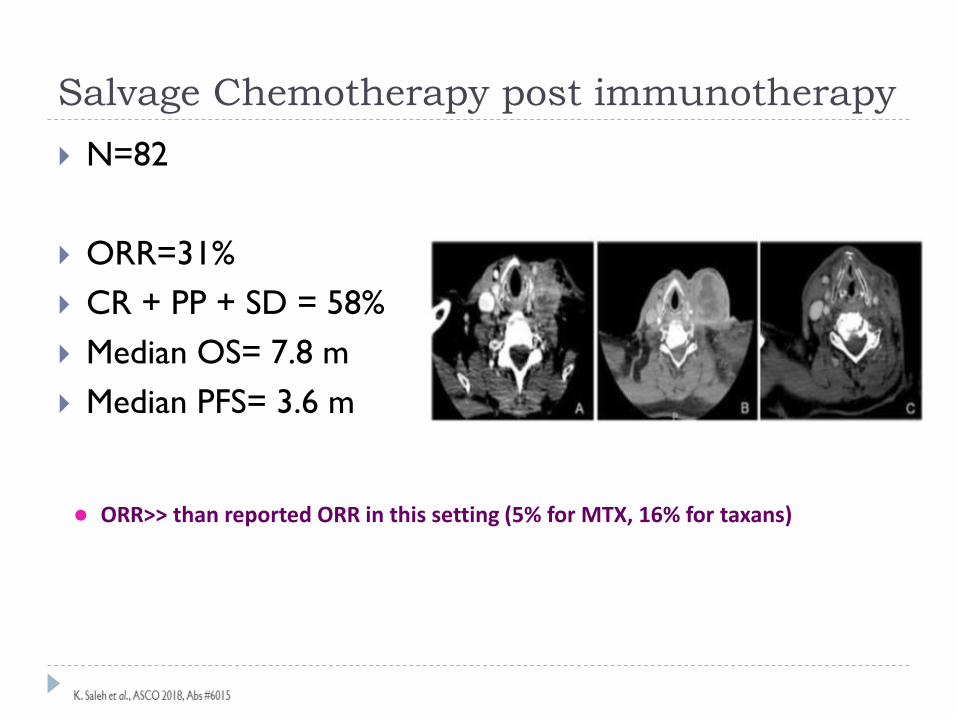
Salvage Chemotherapy post immunotherapy
N=82
ORR=31%
CR + PP + SD = 58%
Median OS= 7.8 m
Median PFS= 3.6 m
⚫ ORR>> than reported ORR in this setting (5% for MTX, 16% for taxans)
Clinical implications
In case of rapid progression, an early clinical and imaging
assessment should be carried out in order to rapidly switch
to another potential effective treatment, especially in case
of clinical deterioration
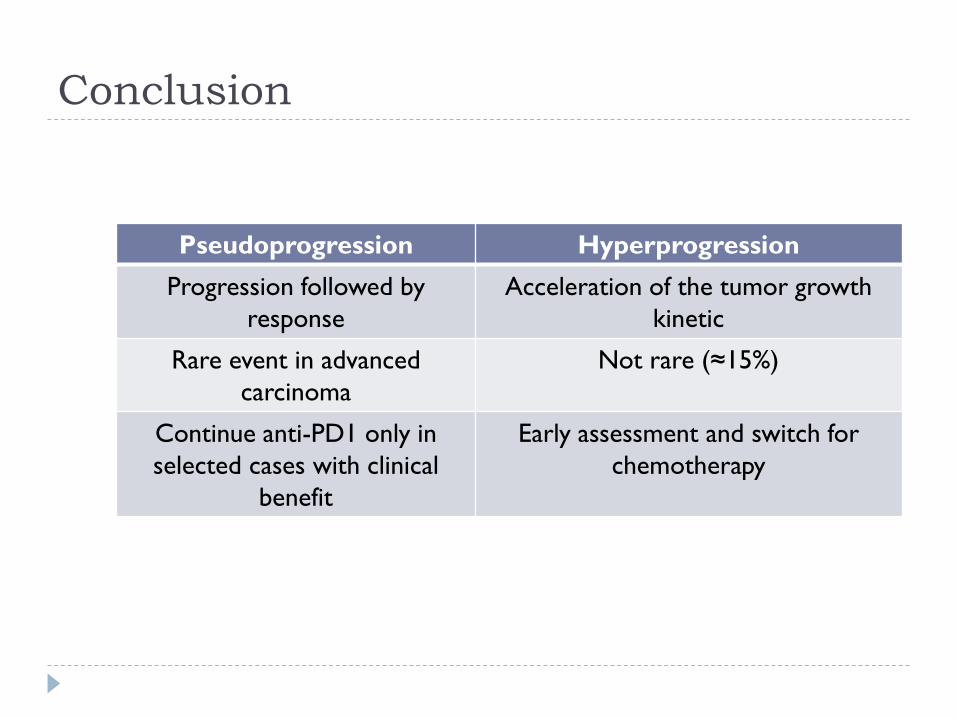
Conclusion
Pseudoprogression Hyperprogression
Progression followed by
response
Acceleration of the tumor growth
kinetic
Rare event in advanced
carcinoma
Not rare (≈15%)
Continue anti-PD1 only in
selected cases with clinical
benefit
Early assessment and switch for
chemotherapy