prognostic value of training-induced change in peak exercise capacity in patients with myocardial...
TRANSCRIPT
Prognostic Value of Training-Induced Change in Peak Exercise Ca
Patients With Myocardial acity in
In arcts and P Patients With Coronary ByPass Surgery
Luc Vanhees, PhD, Robert Fagard, MD, PhD, Lutgarde Thijs, MS, and Antoon Amery, MD, PhD (Edin)
An inverse association between mortality and exercise capacity has been demonstrated previously in patienk with coronary artery disease. physical training gener- alb increases exercise capacity. Only 1 study investi- gated the prognostic value of exercise capacity after training, but on
z data are availa in a limited number of patients. No
le on the relation between mortality and the change in exercise performance with training. Peak oxygen uptake (VO,) was measured before and after a 3-month, predominantly dynamic training peri- od in 417 patients with coronary artery disease. Apart from peak VO,, several patient characteristics, risk fac- tors for cardiovascular disease, and exercise data were considered in a Cox VO1 had increased
roportional-hazards model. Peak Ii y 33% after the training period.
Durmg the total follow-up of 2,583 patienbyears, 37 patienk died. The cause of death was cardiovascular
in 21. The p Yi-!
nostic after training
value of peak VO, was higher an before training, even after adiust-
ment for age and other significant covariates. Cardio- vascular mortality decreased more with greater in- creases in peak VO, after training. The relative hazard mte of 0.98 indicates that a 1% greater increase in peak VOq after trainin decrease m cardiovascu ar f
would be associated with a mortality of 2%. No diir-
ences in prognostic value and in training effeck were observed between patients with myocardial infarcts and patients after coronary bypass grafting. Peak VO,, evaluated after a physical training program, and ik change in response to training are independent pre- dictors for cardiovascular mortality in patients with coronary artery disease.
(Am J Cardiol 1995;76:101&1019)
E xercise capacity is an independent predictor for all- cause and cardiovascular mortality in patients with
coronary artery disease; patients with a low exercise per- formance have the highest incidence of fatal events.‘” Physical training in cardiac patients increases maximal work capacity.s-8 Only 1 study, in a limited number of patients, investigated the relation between cardiovascu- lar mortality and exercise capacity before and after a training prognnn9 Furthermore, the prognostic value of the change in exercise capacity after a physical training program has not been investigated. We analyzed the rela- tion between exercise capacity, measured before and after a physical training program, as well as the absolute and relative changes in exercise capacity, with all-cause, cardiovascular, and noncardiovascular mortality in pa- tients with coronary artery disease who were referred to an outpatient cardiac rehabilitation program.
METHODS Subjeas: The study group comprised male patients,
referred to an outpatient cardiac rehabilitation program during the period August 1978 to March 1988, who had a history of myocardial infarction or had undergone coro- nary bypass surgery (n = 584). Before entering the pro- gram, a graded, uninterrupted exercise test until exhaus-
From the Hypertension and Cardiovascular Rehabilitation Unit, Depart ment of Molecular and Cardiovascular Research, Faculty of Medi- cine, University of leuven, K.U. Leuven, Belgium. Manuscript received August 26, 1994; revised manuscript received and accepted August 10, 199.5.
Address for reprints: Luc Vanhees, PhD, U.Z. Pellenberg, Weligerveld 1, B-32 12 Pellenberg, Belgium.
tion was performed in 527 patients. The characteristics of this group were described in a previous report. lo From these, 93 patients did not complete the 3-month training period. In another 17 patients, the second exercise test was interrupted prematurely because of rhythm distur- bances (n = 4), ST depression of 5 mm (n = l), angina pectoris (n = 9), or claudication (n = 3) without symp- toms of breathlessness or fatigue. Thus, 417 patients per- formed the exercise tests before and after training until exhaustion: 235 patients after acute myocardial infarc- tion (AM1 group), 93 after coronary bypass surgery (CBS group), and 89 patients had both a myocardial infarction and coronary bypass surgery (AM1 + CBS group).
Exercise protocol: In an air-conditioned laboratory with a room temperature of 18°C to 22°C the patients underwent a graded, uninterrupted exercise test on a cycle ergometer until exhaustion. The initial workload of 20 W (1 W = 0.0143 kcal/min) was increased by 30 W every 4 minutes; from 1985 on, workload was in- creased every 3 minutes.
Ventilation (body temperature, pressure, saturation) was continuously measured by a pneumotachograph using an open-circuit method. Peak oxygen uptake (VO,; standard temperature and pressure, dry) and carbon diox- ide output (VCO,; standard temperature and pressure, dry) were calculated from the measurements of oxygen and CO, in the ambient and expired air by a paramag- netic and infrared analyzer, respectively. The respirato- ry gas exchange ratio (VCO-JVO,) and ventilatory equivalent for oxygen (ventilationNO,) were calculat- ed. Heart rate (beats/mm) was determined from the
1014 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 NOVEMBER 15, 1995
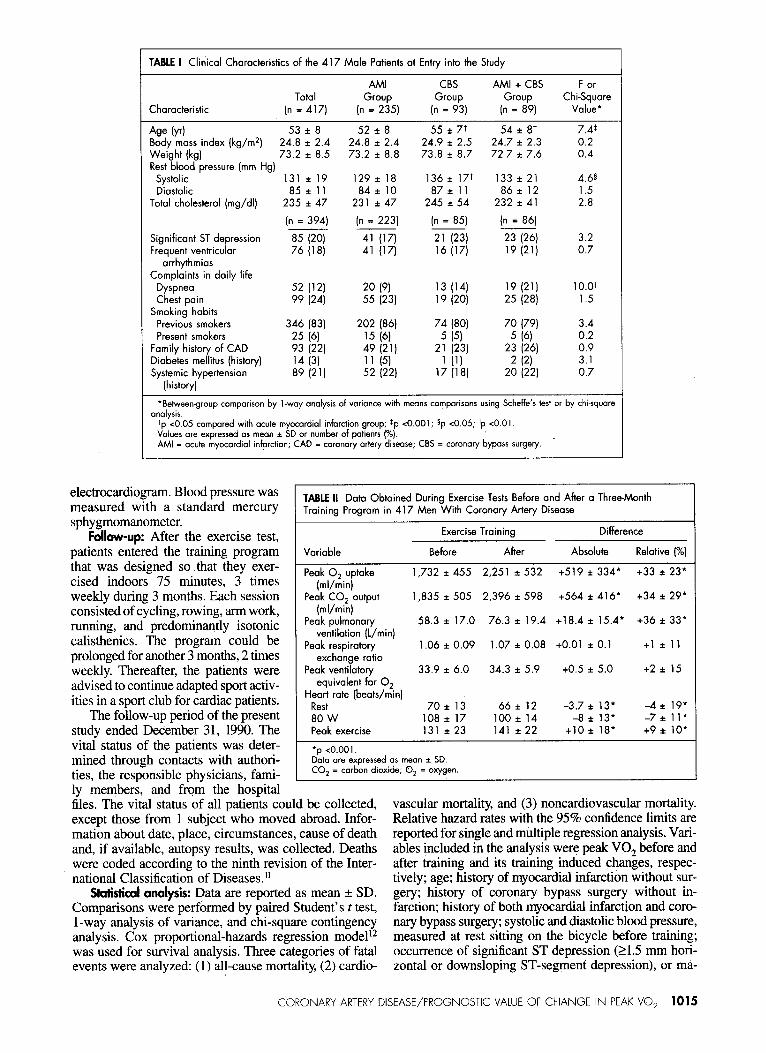
TABLE I Clinical Characteristics of the 417 Male Patients at Entry into the Study
AMI CBS AMI + CBS F or Total
(n%?5) Group Group Chi-Square
Characteristic (n = 417) (n = 93) (n = 89) Value*
Age (yd 53 i 8 52 * 8 55 f 7t 54i8t 7.4t Body mass index (kg/m*) 24.8 f 2.4 24.8 zt 2.4 24.9 IZ 2.5 24.7 f 2.3 0.2 Weight (kg) 73.2 f 8.5 73.2 iz 8.8 73.8 f 8.7 72.7 zt 7.6 0.4 Rest blood pressure (mm Hg)
Systolic 131 f 19 129 iz 18 136 * 17t 133 f 21 4.65 Diastolic 85 * 11 84s~ 10 87* 11 86*12 1.5
Total cholesterol (mg/dl) 235 t 47 231 zt 47 245 i 54 232 * 41 2.8
(n = 394) (n = 223) (n = 85) (n = 86) ~ ~
Significant ST depression 85 (20) 41 (17) 21 (23) 23 (26) 3.2 Frequent ventricular 76 (18) 41 (17) 16 (17) 19 (21) 0.7
arrhythmias Complaints in daily life
Dyspnea 52 (12) 20 (9) 13 (14) 19 (21) 10.0~~ Chest pain 99 (24) 55 (23) 19 (20) 25 (28) 1.5
Smoking habits Previous smokers 346 (83) 202 (86) 74 (80) 70 (79) 3.4 Present smokers 25 (61 15 (6) 5 (5) 5 (6) 0.2
Family history of CAD 93 (22) 49 (21) 21 (23) 23 (26) 0.9 Diabetes mellitus (history) 14 (3) 11 (51 1 (1) 2 (2) 3.1 Systemic hypertension 89 (21) 52 (22) 17 (18) 20 (22) 0.7
(history)
*Behveengroup comparison by l-way analysis of variance with means comparisons using Scheffe’s test or by chisquare analysis.
tp <0.05 compared with acute myocordiol infarction group; tp <O.OOl; sp ~0.05; “p <O.Ol Values ore expressed os mean * SD or number of patients (%). AMI = acute myocardiol infarction; CAD = coronary artery disease; CBS = coronary bypass surgety.
1
t
electrocardiogram. Blood pressure was measured with a standard mercury sphygmomanometer.
Foilow-up: After the exercise test, patients entered the training program that was designed so that they exer- cised indoors 75 minutes, 3 times weekly during 3 months. Each session consisted of cycling, rowing, arm work, running, and predominantly isotonic calisthenics. The program could be prolonged for another 3 months, 2 times weekly. Thereafter, the patients were advised to continue adapted sport activ- ities in a sport club for cardiac patients.
The follow-up period of the present study ended December 31, 1990. The vital status of the patients was deter- mined through contacts with authori- ties, the responsible physicians, fami- ly members, and from the hospital
TABLE II Data Obtained During Exercise Tests Before and After a Three-Month Training Program in 417 Men With Coronary Artery Disease
Variable
Exercise Training Difference
Before After Absolute Relative (%)
Peak 0, uptake (ml/min)
Peak CO, output (ml/min)
Peak pulmonary ventilation (L/min)
Peak respiratory exchange ratio
Peak ventilatory equivalent for 0,
Heart rote (beats/min) Rest 80 W Peak exercise
1,732 i 455 2,251 2 5j2
1,835 zt 505 2,396 * 598
58.3 * 17.0 76.3 i 19.4
1.06 i 0.09 1.07 * 0.08
33.9 * 6.0 34.3 f 5.9
70*13 66*12 108i17 100 i 14 131 * 23 141 * 22
+519*334* +33 zt 23*
+564 zt 416* +34 zt 29*
+18.4 * 15.4* +36 i 33*
+O.Ol * 0.1 +l * 11
+0.5 f 5.0 +2*15
-3.7 f 13* -4 f 19' -8 * 13* -7 * 11*
+lO * 18* +9* 10*
‘p <O.OOl. Data ore expressed os mean * SD. CO, = carbon dioxide; 0, = oxygen.
files. The vital status of all patients could be collected, except those from 1 subject who moved abroad. Infor- mation about date, place, circumstances, cause of death and, if available, autopsy results, was collected. Deaths were coded according to the ninth revision of the Inter- national Classification of Diseases.”
Statistical analysis: Data are reported as mean f SD. Comparisons were performed by paired Student’s t test, l-way analysis of variance, and chi-square contingency analysis. Cox proportional-hazards regression modelI was used for survival analysis. Three categories of fatal events were analyzed: (1) all-cause mortality, (2) cardio-
vascular mortality, and (3) noncardiovascular mortality. Relative hazard rates with the 95% confidence limits are reported for single and multiple regression analysis. Vari- ables included in the analysis were peak VO, before and after training and its training induced changes, respec- tively; age; history of myocardial infarction without sur- gery; history of coronary bypass surgery without in- farction; history of both myocardial infarction and coro- nary bypass surgery; systolic and diastolic blood pressure, measured at rest sitting on the bicycle before training; occurrence of significant ST depression (21.5 mm hori- zontal or downsloping ST-segment depression), or ma-
CORONARY ARTERY DISEASE/PROGNOSTIC VALUE OF CHANGE IN PEAK VO, 1015
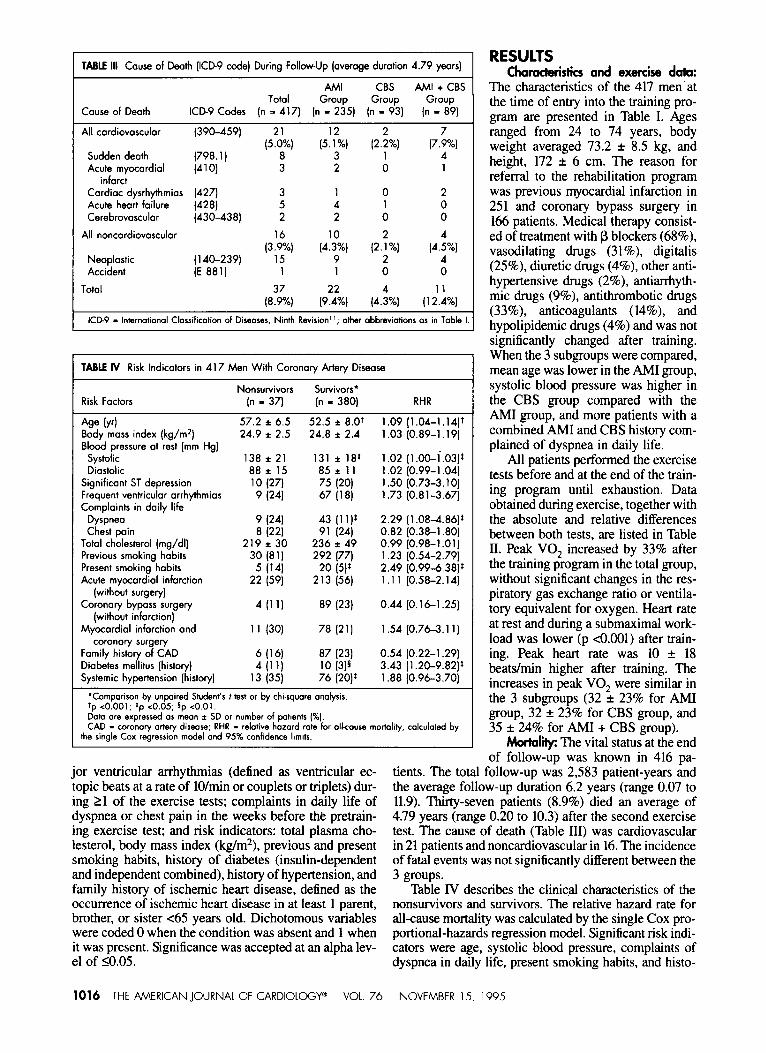
TABLE III Cause of Death (ICD9 code) During Follow-Up (overage durotion 4.79 yeors)
Couse of Death
AMI CBS AMI + CBS Totol Group Group Group
ICD9 Codes (n = 417) (n - 235) (n = 93) (n = 89)
All cordiovosculor (390-459) (5!?%, Sudden deoth Acute myocordiol
infarct Cordioc dysrhythmios Acute heort failure Cerebrovosculor
(798.1)
(410) 3 z
3 1 5 4 2 2
,3$, (4130%) 9
1 1
[8& (0242%)
,,%,,
1 height, 172 + 6 cm. The reason for referral to the rehabilitation program
2 was previous myocardial infarction in 0 0
251 and coronary bypass surgery in 166 patients. Medical therapy consist-
r.:%) ed of treatment with p blockers (68%),
4 vasodilating drugs (31%) digitalis
0 (25%), diuretic drugs (4%), other anti-
(12lJ%,
hypertensive drugs (2%), antiarrhyth- mic drugs (9%), antithrombotic drugs (33%), anticoagulants (14%), and hypolipidemic drugs (4%) and was not significantly changed after training. When the 3 subgroups were compared, mean age was lower in the AM1 group, systolic blood pressure was higher in the CBS group compared with the AM1 group, and more patients with a combined AM1 and CBS history com- plained of dyspnea in daily life.
AI1 patients performed the exercise tests before and at the end of the train- ing program until exhaustion. Data obtained during exercise, together with the absolute and relative differences between both tests, are listed in Table II. Peak VO, increased by 33% after the training program in the total group, without significant changes in the res- piratory gas exchange ratio or ventila- tory equivalent for oxygen. Heart rate at rest and during a submaximal work- load was lower (p <o.OOl) after train- ing. Peak heart rate was 10 + 18 beats/mm higher after training. The increases in peak VO, were similar in the 3 subgroups (32 f 23% for AMI group, 32 f 23% for CBS group, and 35 + 24% for AMI + CBS group).
MortaIii The vital status at the end of follow-up was known in 416 pa-
tients. The total follow-up was 2,583 patient-years and the average follow-up duration 6.2 years (range 0.07 to 11.9). Thirty-seven patients (8.9%) died an average of 4.79 years (range 0.20 to 10.3) after the second exercise test. The cause of death (Table III) was cardiovascular in 21 patients and noncardiovascular in 16. The incidence of fatal events was not significantly different between the 3 groups.
All noncordiovosculor
Neoplostic Accident
Totol
(4271 (428) (430-438)
(140-239) (E 881)
(4.i%)
KID-9 - International Classification of Diseases, Ninth Revision”; other abbreviations os in Table I.
TABLE IV Risk Indicators in 417 Men With Coronory Artery Diseose
Nonsurvivors Survivors’ Risk Factors In - 37) (n = 380) RHR
Age M 57.2 i 6.5 52.5 i 8.0+ 1.09 (1.04-1.1417 Body moss index (kg/m2) 24.9 2 2.5 24.8 2 2.4 1.03 (0.89-l. 19) Blood pressure ot rest (mm Hg)
Systolic 138 * 21 131 * 18: 1.02 (i ai.03)* Diastolic 88i 15 85 i 11 1.02 (0.99-l .04)
Significant ST depression 10 (27) 75 (20) 1.50 (0.73-3.10) Frequent ventricular orrhythmios 9 (241 67 (18) 1.73 (0.81-3.67) Complaints in doily life
Dyspneo 9 (241 43 (11)’ 2.29 (1.08-4.86)t Chest poin 8 (221 91 (24) 0.82 (0.38-l .80)
Total cholesterol (mg/dl) 219 * 30 236 i 49 0.99 (0.98-l .Ol) Previous smoking habits 30 (81) 292 ~7) 1.23 (0.54-2.79) Present smoking habits 5 (14) 20 (5)s 2.49 (0.99-6.38): Acute myocordiol infarction 22 (59) 213 (56) 1.1 1 (0.58-2.14)
(without surgery) Coronary byposs surgery 4 ,111 89 (23) 0.44 (0.16-l ,251
(without infarction) Myocordiol infarction ond 11 (30) 78 (21) 1.54 (0.76-3.11)
coronofy surgery Family history of CAD 6 (14 87 (23) 0.54 (0.22-l .29) Diobetes mellitus (history) 4 ,111 10 (3)5 3.43 (1.20-9.82)$ Systemic hypertension (history) 13 (35) 76 (20)r 1.88 (0.96-3.70)
‘Comparison by unpaired Student’s f test or by chi-square analysis. ‘p <0.001; ‘p co.05; Dp <O.Ol. Dot0 ore expressed (II mean * SD or number of Patients (%I. CAD - coronary artery disease; RHR - re dative hazard rate for alkouu, mortality, calculated by
the single Cox regression model and 95% confidence limits.
jor ventricular arrhythmias (defined as ventricular ec- topic beats at a rate of lO/min or couplets or triplets) dur- ing 21 of the exercise tests; complaints in daily life of dyspnea or chest pain in the weeks before the pretrain- ing exercise test; and risk indicators: total plasma cho- lesterol, body mass index (kg/m2), previous and present smoking habits, history of diabetes (insulin-dependent and independent combined), history of hypertension, and family history of ischemic heart disease, defined as the occurrence of ischemic heart disease in at least 1 parent, brother, or sister ~65 years old. Dichotomous variables were coded 0 when the condition was absent and 1 when it was present. Significance was accepted at an alpha lev- el of 10.05.
1016 THE AMERICAN JOURNAL OF CARDIOLOGY* VOL. 76
RESULTS Chamcteristics and exercise data:
The characteristics of the 417 men.at the time of entry into the training pro- gram are presented in Table I. Ages ranged from 24 to 74 years, body weight averaged 73.2 f 8.5 kg, and
Table IV describes the clinical characteristics of the nonsurvivors and survivors. The relative hazard rate for ah-cause mortality was calculated by the single Cox pro- portional-hazards regression model. Significant risk indi- cators were age, systolic blood pressure, complaints of dyspnea in daily life, present smoking habits, and histo-
NOVEMBER 15. 1995
ry of diabetes; history of hypertension tended to be significant. Histories of myocardial infarcts, coronary bypass, or both events combined were not sig- nificantly related to survival.
TABLE V Relative Hazard Rates (95% confidence limits) for Peak Oxygen Uptake (peak VO,) Before ond After Exercise Training in 4 17 Men With Coronary Artery Disease
Peak VO, (L/min) Difference in Peak VO,
Before After Absolute Relative Mortality Training Training (L/min) PI
All-cause mortality Unadiusted 0.32* 0.257 0.26* 0.987
(0.14-0.75) (0.13-0.5 1) (0.09-0.73) (0.972-l .002) Adjusted for
Age 0.58 0.39* 0.29% 0.986 (0.24-l .43) (0.18-0.84) (0.09-0.89) (0.971-l .OOl)
Age, covariates 0.56 0.41* 0.35 0.988 (0.22-l .45) (0.19-0.90) (0.1 l-l .06) (0,973-l ,004)
Cardiovascular mortality Unadjusted 0.19* 0.14t 0.14* 0.979t
(0.06-0.62) (0.05-0.36) (0.03-0.58) (0.958-l ,000) Adjusted for
Age 0.32 0.18* 0.13* 0.977$
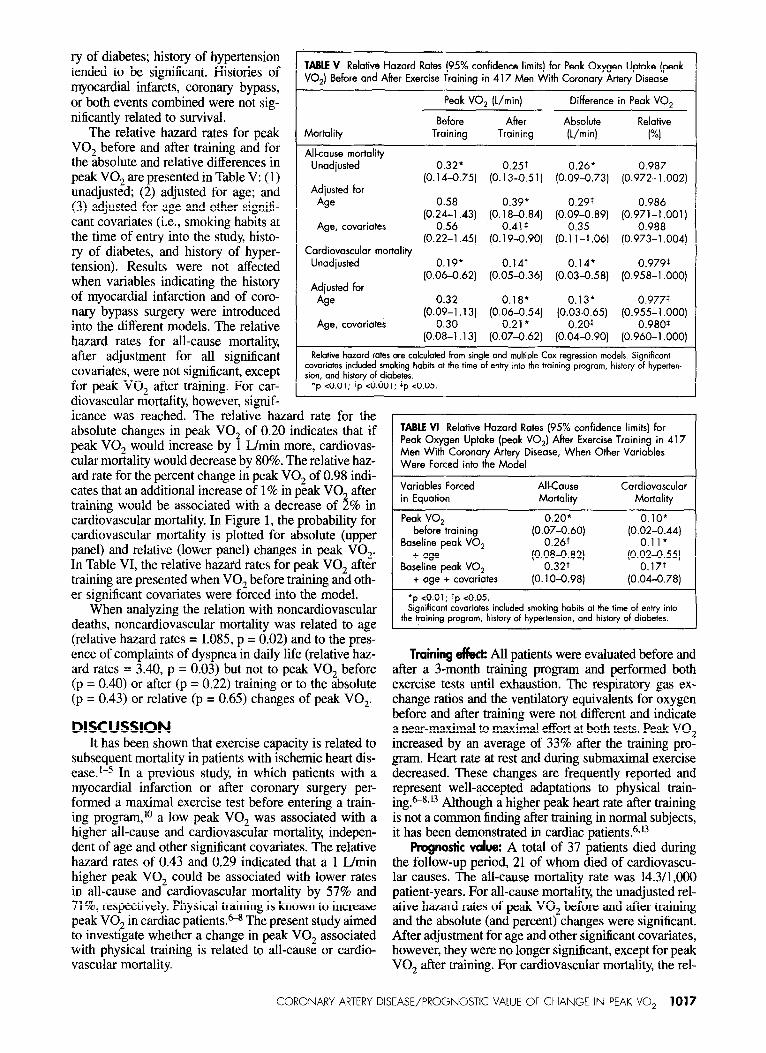
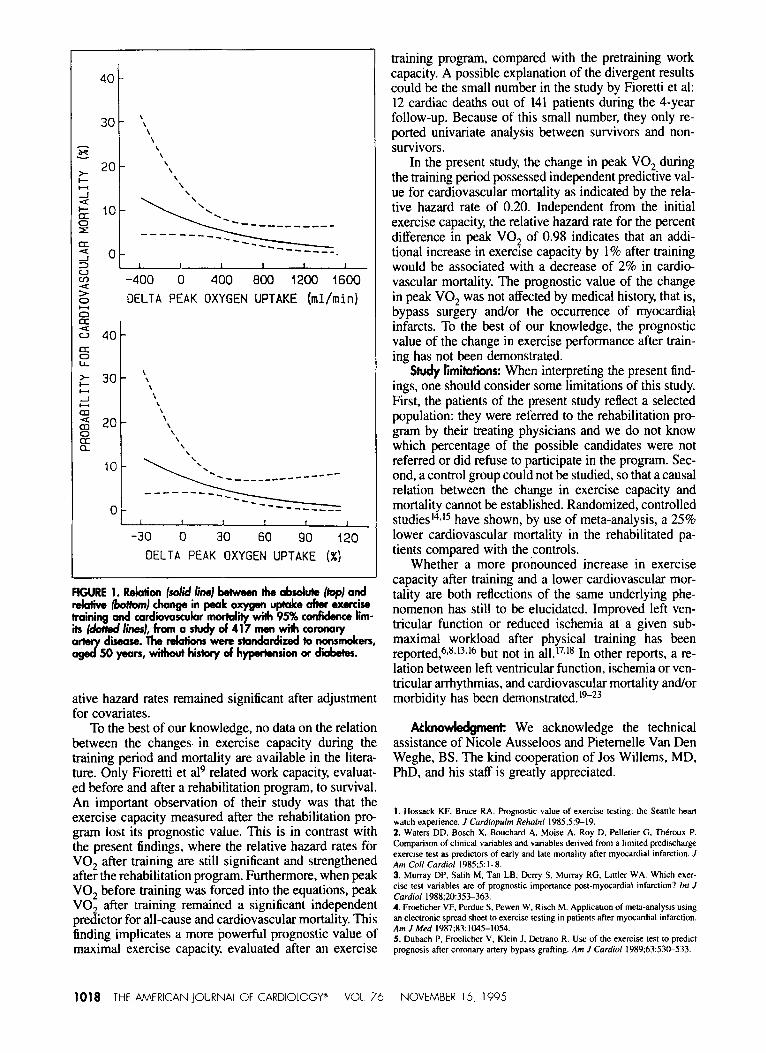
The relative hazard rates for peak VO, before and after training and for the absolute and relative differences in peak VO, are presented in Table V: (1) unadjusted; (2) adjusted for age; and (3) adjusted for age and other signifi- cant covariates (Le., smoking habits at the time of entry into the study, histo- ry of diabetes, and history of hyper- tension). Results were not affected when variables indicating the history of myocardial infarction and of coro- nary bypass surgery were introduced into the different models. The relative hazard rates for all-cause mortality, after adjustment for all significant covariates, were not significant, except for peak VO, after training. For car- diovascular mortality, however, signif- icance was reached. The relative hazard rate for the absolute changes in peak VO, of 0.20 indicates that if peak VO, would increase by 1 Wmin more, cardiovas- cular mortality would decrease by 80%. The relative haz- ard rate for the percent change in peak VO, of 0.98 indi- cates that an additional increase of 1% in peak VO, after training would be associated with a decrease of 2% in cardiovascular mortality. In Figure 1, the probability for cardiovascular mortality is plotted for absolute (upper panel) and relative (lower panel) changes in peak VO,. In Table VI, the relative hazard rates for peak VO, after training are presented when VO, before training and oth- er significant covariates were forced into the model.
Age, covoriates (0.09-l .13) (0.06-0.54) (0.;3--;65) (0.905~-ll~00)
0.30 0.21 l
(0.08-l .13) (0.07-0.62) (0.04-0.90) (0,960-l .OOO)
Relative hazard rates are calculated from single and multiple Cox regression models. Significant covariates included smoking habits at the time of entry into the training program, history of hyperten- sion, and history of diabetes.
*p co.01; tp <0.001; tp co.05.
TABLE VI Relative Hazard Rates (95% confidence limits) for Peak Oxygen Uptake (peak VO,) After Exercise Training in 417 Men With Coronary Artery Disease, When Other Variables
Peak VO, before training
Baseline peak VO, + age
Baseline peak VO, + age + covariotes
0.20* 0.10* (0.07&60) (0.02-0.44)
0.11*
P~3;;82) ‘o.~Q;t55)
(0.1 o-0.98) (0.04-0.78)
‘p <0.01; ‘p <0.05. When analyzing the relation with noncardiovascular
deaths, noncardiovascular mortality was related to age (relative hazard rates = 1.085, p = 0.02) and to the pres- ence of complaints of dyspnea in daily life (relative haz- ard rates = 3.40, p = 0.03) but not to peak VO, before (p = 0.40) or after (p = 0.22) training or to the absolute (p = 0.43) or relative (p = 0.65) changes of peak VO,.
Significant covariates included smoking habits at the time of entry into the training program, history of hypertension, and history of diabetes.
DISCUSSION It has been shown that exercise capacity is related to
subsequent mortality in patients with ischemic heart dis- ease.‘-5 In a previous study, in which patients with a myocardial infarction or after coronary surgery per- formed a maximal exercise test before entering a train- ing program, lo a low peak VO, was associated with a higher all-cause and cardiovascular mortality, indepen- dent of age and other significant covariates. The relative hazard rates of 0.43 and 0.29 indicated that a 1 L/min higher peak VO, could be associated with lower rates in all-cause and cardiovascular mortality by 57% and 71%, respectively. Physical training is known to increase peak VO? in cardiac patients.&* The present study aimed to investigate whether a change in peak VO, associated with physical training is related to all-cause or cardio- vascular mortality.
Training effeck All patients were evaluated before and after a 3-month training program and performed both exercise tests until exhaustion. The respiratory gas ex- change ratios and the ventilatory equivalents for oxygen before and after training were not different and indicate a near-maximal to maximal effort at both tests. Peak VO, increased by an average of 33% after the training pro- gram. Heart rate at rest and during submaximal exercise decreased. These changes are frequently reported and represent well-accepted adaptations to physical train- ing.“8,U Although a higher peak heart rate after training is not a common finding after training in normal subjects, it has been demonstrated in cardiac patients.6,*3
Prognostic due: A total of 37 patients died during the follow-up period, 21 of whom died of cardiovascu- lar causes. The all-cause mortality rate was 14.3/1,000 patient-years. For all-cause mortality, the unadjusted rel- ative hazard rates of peak VO, before and after training and the absolute (and percent) changes were significant. After adjustment for age and other significant covariates, however, they were no longer significant, except for peak VO, after training. For cardiovascular mortality, the rel-
CORONARY ARTERY DISEASE/PROGNOSTIC VALUE OF CHANGE IN PEAK VO, 1017
z DELTA PEAK OXYGEN UPTAKE (ml/min) s 9 = 40
s LL
c’ 30 k \ -I z
\ \ 2 20
\ \ ::
\ \ a \
10
0
\
1 f I I f I
-30 0 30 60 90 120 OELTA PEAK OXYGEN UPTAKE (%)
FtGURE 1. Rekdion (so/id /ino) hehveen tha absduk (top1 and rekhve /botch) change in peak oxygen uptake a&r exercise Imining and card&as&r morkdii with 95% conficbnce lim- ilrI~lines),fromas~d417menwil)lcoronary
diseaw. The relations were stondatdized to nonsmokers, 50 years, without his+ory d hyperbnsion or diibetes.
ative hazard rates remained significant after adjustment for covariates.
To the best of our knowledge, no data on the relation between the changes in exercise capacity during the training period and mortality are available in the litera- ture. Only Fioretti et al9 related work capacity, evaluat- ed before and after a rehabilitation program, to survival. An important observation of their study was that the exercise capacity measured after the rehabilitation pro gram lost its prognostic value. This is in contrast with the present findings, where the relative hazard rates for VO, after training are still significant and strengthened after the rehabilitation program. Furthermore, when peak VO, before training was forced into the equations, peak VO, after training remained a significant independent predictor for all-cause and cardiovascular mortality. This finding implicates a more powerful prognostic value of maximal exercise capacity, evaluated after an exercise
training program, compared with the pretraining work capacity. A possible explanation of the divergent results could be the small number in the study by Fioretti et al: 12 cardiac deaths out of 141 patients during the 4-year follow-up. Because of this small number, they only re- ported univariate analysis between survivors and non- survivors.
In the present study, the change in peak VO, during the training period possessed independent predictive val- ue for cardiovascular mortality as indicated by the rela- tive hazard rate of 0.20. Independent from the initial exercise capacity, the relative hazard rate for the percent difference in peak VO, of 0.98 indicates that an addi- tional increase in exercise capacity by 1% after training would be associated with a decrease of 2% in cardio- vascular mortality. The prognostic value of the change in peak VO, was not affected by medical history, that is, bypass surgery and/or the occurrence of myocardial infarcts. To the best of our knowledge, the prognostic value of the change in exercise performance after train- ing has not been demonstrated.
Study limitations: When interpreting the present find- ings, one should consider some limitations of this study. First, the patients of the present study reflect a selected population: they were referred to the rehabilitation pro- gram by their treating physicians and we do not know which percentage of the possible candidates were not referred or did refuse to participate in the program. Sec- ond, a control group could not be studied, so that a causal relation between the change in exercise capacity and mortality cannot be established. Randomized, controlled studies’j*i5 have shown, by use of meta-analysis, a 25% lower cardiovascular mortality in the rehabilitated pa- tients compared with the controls.
Whether a more pronounced increase in exercise capacity after training and a lower cardiovascular mor- tality are both reflections of the same underlying phe- nomenon has still to be elucidated. Improved left vcn- tricular function or reduced ischemia at a given sub- maximal workload after physical training has been reported,6s*‘3*16 but not in a11.r~18 In other reports, a re- lation between left ventricular function. ischemia or vcn- tricular arrhythmias, and cardiovascular mortality and/or morbidity has been demonstrated.‘9-23
A&no&dgment: We acknowledge the technical assistance of Nicole Ausseloos and Pietemelle Van Den Weghe, BS. The kind cooperation of Jos Willems, MD, PhD, and his staff is greatly appreciated.
I. Hossack KF, Bruce RA. Prognostic value of exercise testing: the SeartIe hear~ watch experience. J Cordiopulm Rehabil 1985:5:%19. 2. W&en DD. Bosch X. Boochard A, Moist: A, Roy D, Pellerier G. Th&oux P. Comparison of clinical variables and variables derived fmm a hmited predischarge exercise test as predictors of early and late mortality after myocardial infarction. J Am Co// Cordial 1985:5: l-8. 3. Murray DP. Salih M, Tan LB, Deny S, Murray RG. Littler WA. Which exer- cise test variables are of prognostic importance post-myocardial infarction? Inr J Cardiol 1988;2&35>363. 4. Froelicher VF, Perdue S, Pewen W, Risch M. Application of me@analysis using an electronic spread sheer to exercise testing in patients after myowdial infarction. Am J Med 1987;83: 1045-1054. 5. Dubach P. Frcelicher V, Klein J, Detrano R. Use of the exercise test to predict prognosis after coronary artery bypass grafting. Am J Cardiol 1989:63:53&533.
1018 THE AMERICAN JOURNAL OF CARDIOLOGY” VOL. 76 NOVEMBER 15, 1995

6. Vanhees L, Fagard R, Amery A. Influence of beta-adrenergic blockade on the hemodynamic effects of physical training in patients with ischemic heart disease. Am Heart J 1984;108:27C-275. 7. Laslett L, Paumer L, Amsterdam EA. Exercise training in coronary artery dis- ease. Car&l Clin 1987;5:21 l-225. 8. Squires RW, Gau GT, Miller TD, Allison TG, Lavie CJ. Cardiovascular reha- bilitation: states 1990. Mayo Clin Proc 1990;65:731-755. 9. Fioretti P, Baardman T, Deckers J, Salm E, Zwien G, Kazemier M, Roelandt J. Social fate and long-term survival of patients with a recent myocardial infarction, after cardiac rehabilitation. Eur Heart J 1988;9(suppl L):89-94. 10. Vanhees L, Fagard R, Thijs L, Staessen J, Amery A. Prognostic significance of peak exercise capacity in patients with coronary artery disease. JAm Coil Car- did 1994;23:358-363. 11. World Health Organization. International Classification of Diseases, 9th revi- sion. Clinical Modification. Ann Arbor, MI: Edwards Brothers, 1981. 12. Cox DR. Regression models and life-tables. JR Star Sot 1972;B34:187-220. 13. Clausen JP. Circulatory adjustments to dynamic exercise and effect of physi- cal training in normal subjects and in patients with coronary artery disease. Prog Cardiovasc Dis 1976;18:459495. 14. Oldridge NB, Guyatt GH, Fisher ME, Rimm AA. Cardiac rehabilitation after myocardial infarction: combined experience of random&d clinical trials. JAMA 1988;260:945-950. 15. O’Connor GT, Barin JE, Yusuf S, Goldhaber SZ, Olmstead EH, Paffinburger
RS Jr, Hennekens CH. An overview of randomised trials of rehabilitation with exer- cise after myocardial infarction. Circulation 1989;80:234-244. 16. Verani MS, Hartung GH, Hoepfel-Harris J, Welton DE, Pratt CM, Miller RR. Effects of exercise training on left ventricular performance and myocardial perfu- sion in patients with coronary artery disease. Am J Cardiol 1981;47:797-803. 17. Letac B, Cribier A, Desplanches JF. A study of left ventricular function in coro- nary patients before and after physical training. Circulation 1977;56:375-378. 18. Cobb FR, Williams RS, McEwan P, Jones RH, Coleman RE, Wallace AG. Effects of exercise training on ventricular function in patients with recent myocar- dial infarction. Circularion 1982;66: 100-108. 19. Granath A, Stiermark T, Winge T, Volpe U, Zetterquist S. Early work load tests for evaluation of long-term prognosis of acute myocardial infarction. Br Heart J 1977;39:758-763. 20. Sami M, Kraemer H, DeBusk RF. The prognostic significance of serial exer- cise testing after myocardial infarction. Circulation 1979;60: 1238-1246. 21. Starling MR, Crawford MH, Kennedy GT, O’Rourke RA. Exercise testing ear- ly after myocardial infarction: predictive value for subsequent unstable angina and death. Am J Cardiol 1980;46909-9914. 22. Norris RM, Bamaby PF, Bmndt PWT, Geary GG, Whitlock RML, Wild CJ, Barratt-Boyes BG. Prognosis after recovery from first acute myocardial infarction: determinants of reinfarction and sudden death. Am J Cardiol 1984;53:408-413. 23. Weld FM. Exercise testing early after myocardial infarction. J Cnrdiopulm Rehabil 1985;5:2&27.
CORONARY ARTERY DISEASE/PROGNOSTIC VALUE OF CHANGE IN PEAK VO, 1019