professore di pediatria - 70° congresso italiano di pediatriacongresso2014.sip.it/dia/7840.pdf ·...
TRANSCRIPT
Giovanni B Pajno
Professore di Pediatria
Dipartimento di Pediatria – UOC DI PEDIATRIA
UOS Allergologia Pediatrica
Policlinico Universitario Messina
IMMUNOTERAPIE
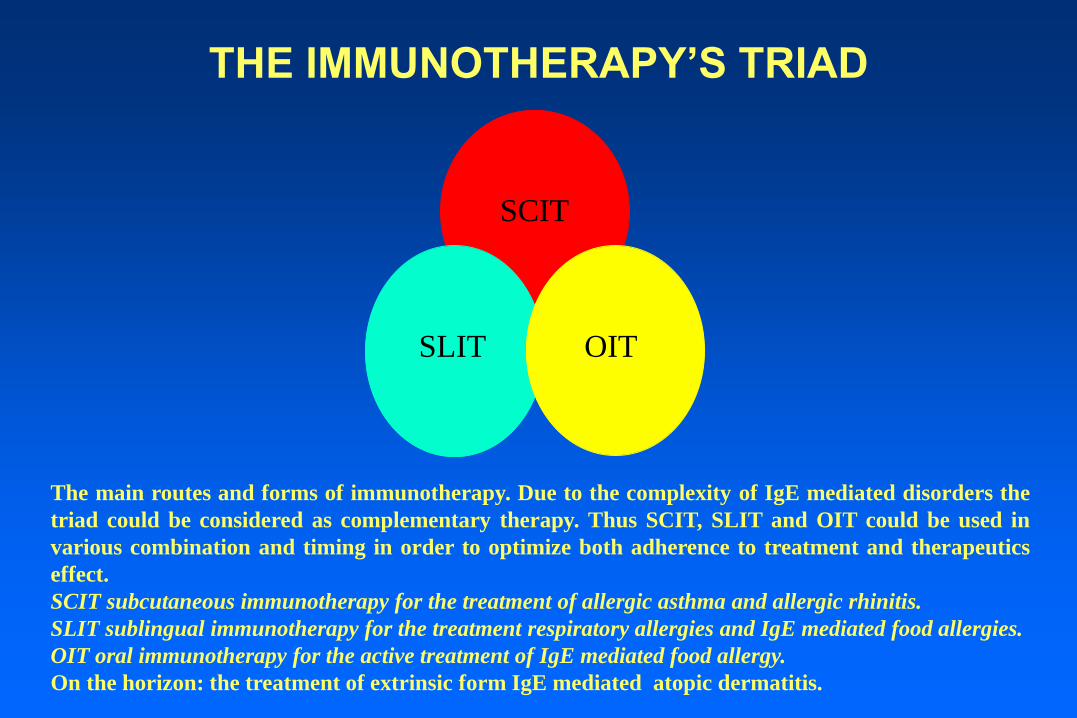
The main routes and forms of immunotherapy. Due to the complexity of IgE mediated disorders the
triad could be considered as complementary therapy. Thus SCIT, SLIT and OIT could be used in
various combination and timing in order to optimize both adherence to treatment and therapeutics
effect.
SCIT subcutaneous immunotherapy for the treatment of allergic asthma and allergic rhinitis.
SLIT sublingual immunotherapy for the treatment respiratory allergies and IgE mediated food allergies.
OIT oral immunotherapy for the active treatment of IgE mediated food allergy.
On the horizon: the treatment of extrinsic form IgE mediated atopic dermatitis.
THE IMMUNOTHERAPY’S TRIAD
SCIT
SLIT OIT
FDA Committee Votes to Approve SLIT Treatments Last month, the Allergenic Products Advisory Committee (APAC) of the Food and
Drug Administration (FDA) met and voted that the available safety and efficacy
data support approval of two sublingual allergy immunotherapy (AIT) products.
One is a grass pollen AIT tablet developed by Stallergenes and the other is
Merck’s grass pollen AIT tablet. The APAC voted 9-1 regarding approval of the
Stallergenes tablet and 9-0 regarding the Merck tablet. The FDA will need to give
final approval, but it usually follows the advice of its advisory committees.
AAAAI President Linda Cox, MD, FAAAAI, said in an email to members:
“There are no FDA-approved forms of sublingual AIT currently available here in
the United States, so these products would be the first licensed therapies of their
kind. It’s worth noting that the committee felt very strongly about including
language in the prescribing instructions for both products that recommended the
patient has autoinjectable epinephrine in the event of a severe allergic reaction."
Dr. Cox also discusses the news in this month's President's Message.
More information, including a webcast of the meetings, is available from the FDA
website

SCIT
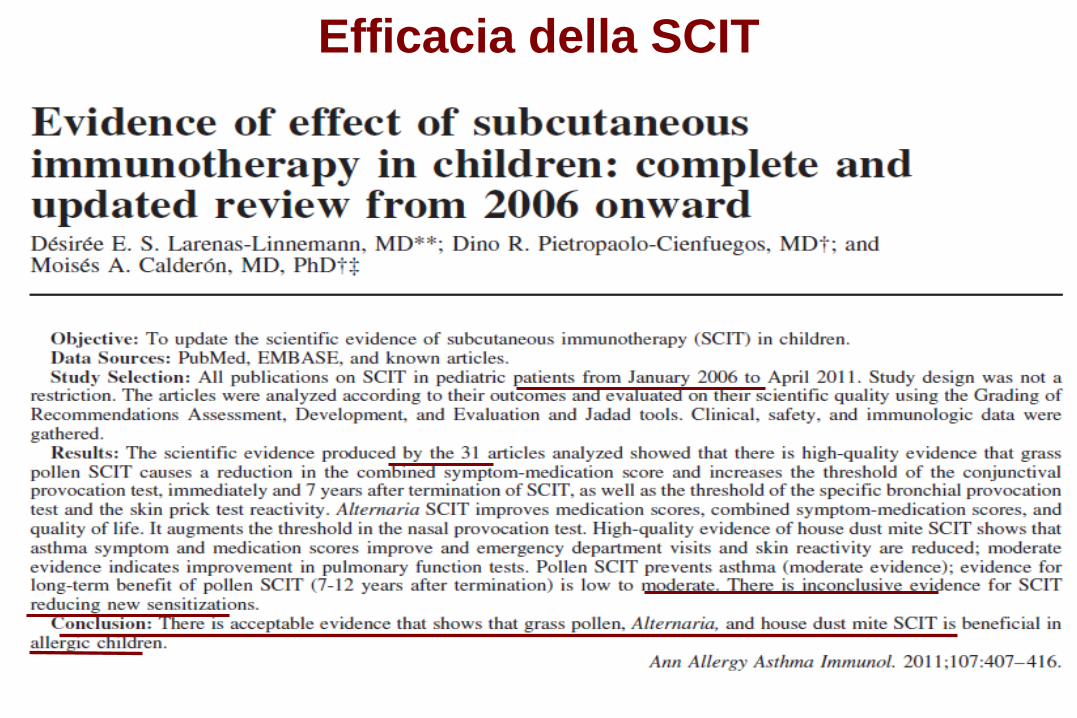
Efficacia della SCIT

Efficacia a lungo termine della SCIT
In età pediatrica studi di follow-up hanno dimostrato un
effetto di carry-over anche fino a 12 anni dopo la SCIT,
anche se con studi di scarsa qualità metodologica.
Calvo M, et al. J Investig Allergol ClinImmunol 1994;
Cools M, et al. Allergy 2000;
Reinhold M, et al. Allergy 2002;
Eng PA, et al. Allergy 2006;
Tabar AI, et al. JACI 2011
In 13 trials, 920 children received SCIT or usual care;
In 18 studies, 1583 children received SLIT or usual care;
3 studies compared SCIT with SLIT head-to-head in 135
children.
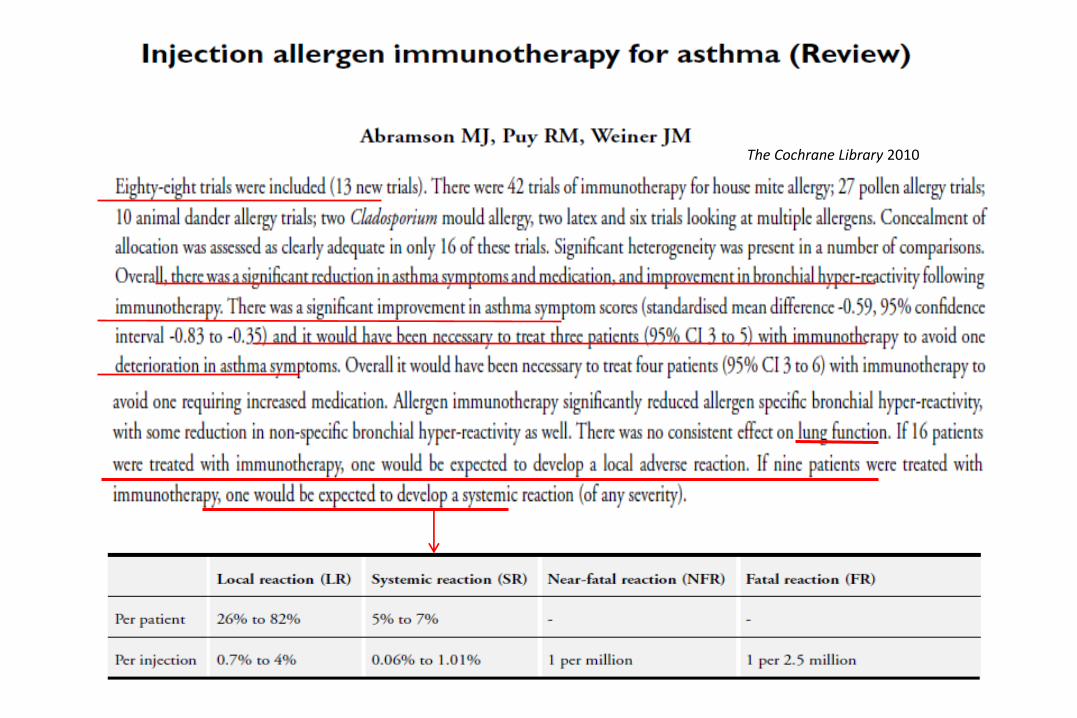
The Cochrane Library 2010
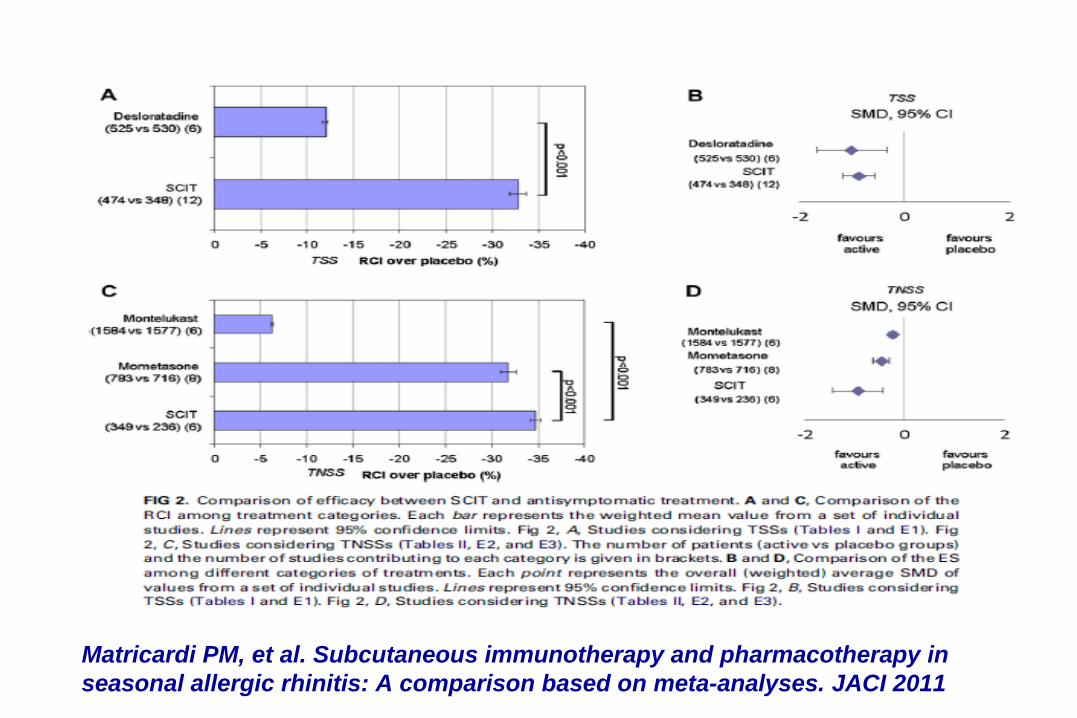
Matricardi PM, et al. Subcutaneous immunotherapy and pharmacotherapy in
seasonal allergic rhinitis: A comparison based on meta-analyses. JACI 2011
SLIT

Calderon MA et al, JACI 2011
SLIT



Efficacia e sicurezza della SCIT e della SLIT per il
trattamento dell’asma bronchiale allergico e della
rinite allergica
1. L’effetto dell’ITS è duraturo dopo la
sospensione?
2. L’ITS è in grado di prevenire le nuove
allergie nei bambini monosensibili?
3. L’ITS è in grado di prevenire l’asma nei
bambini con rinite?

Durham S.R. et al.
Long-Term Clinical Efficacy of Grass-Pollen Immunotherapy.
N Eng J Med 1999; 341: 468-475
Initial Trial Current Trial
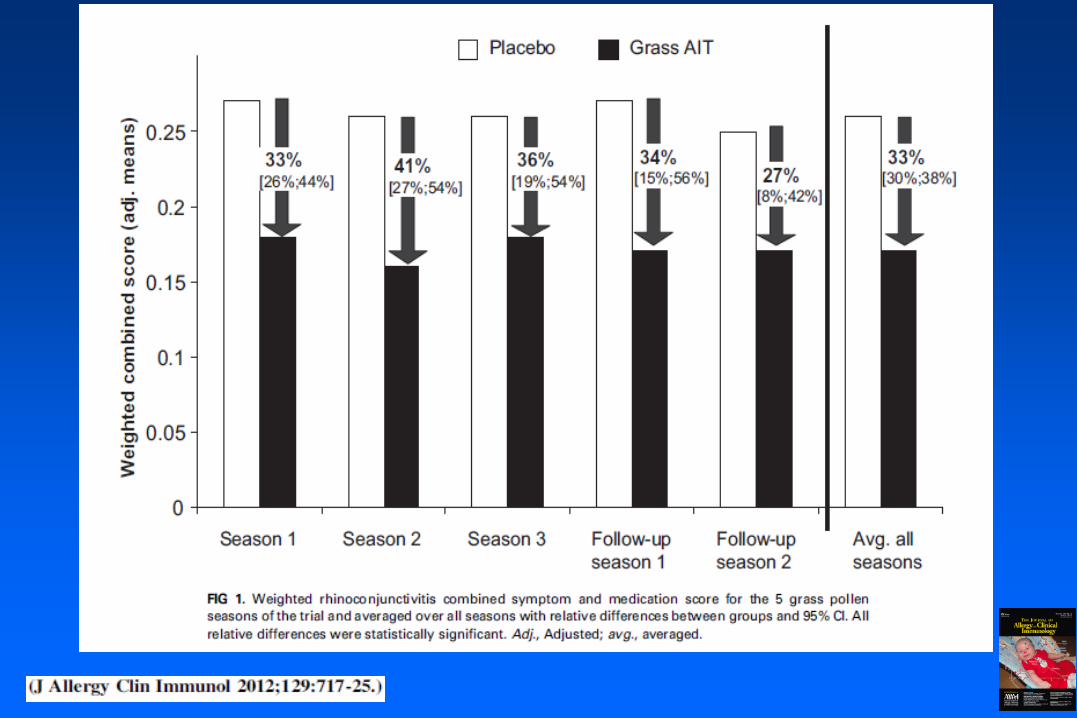
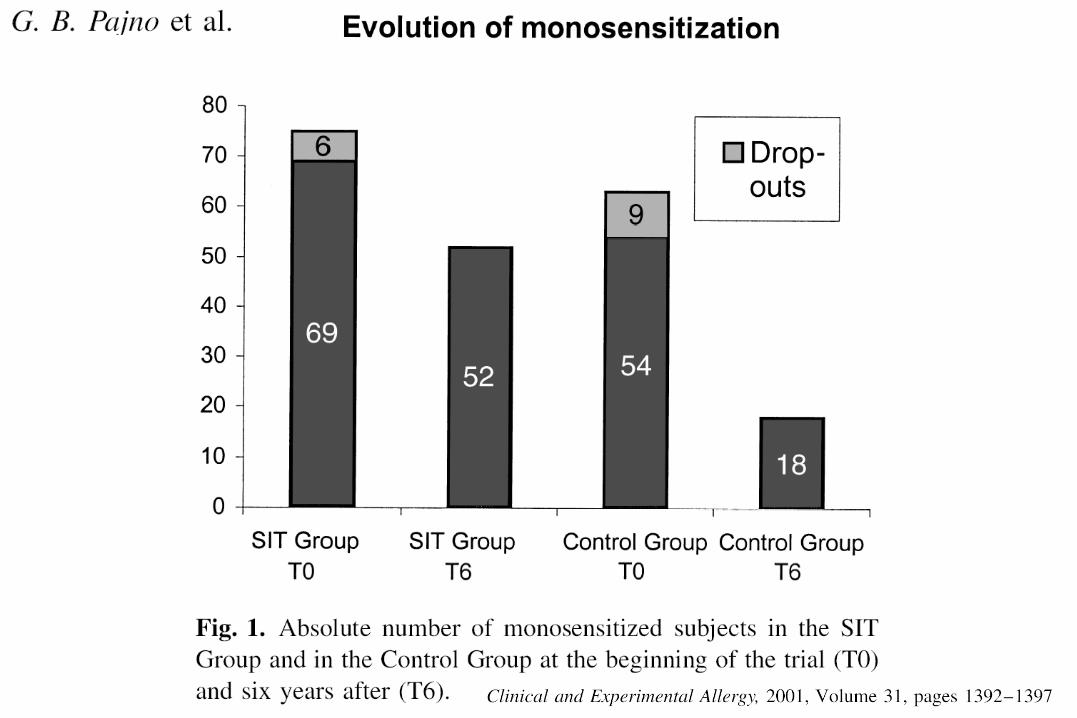
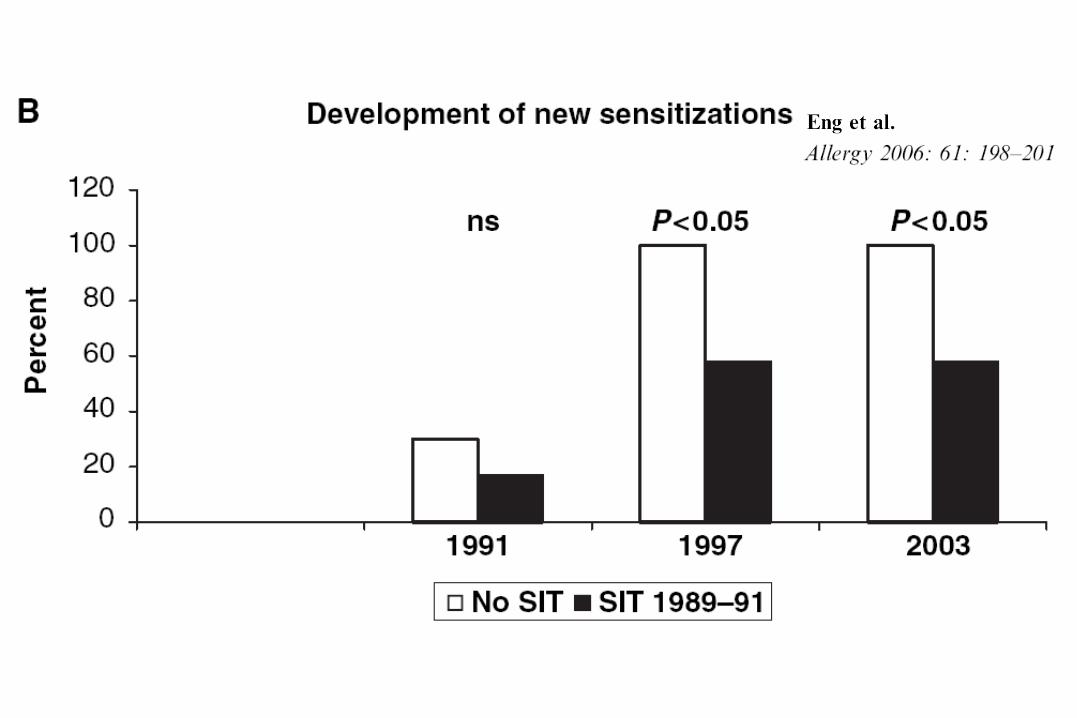
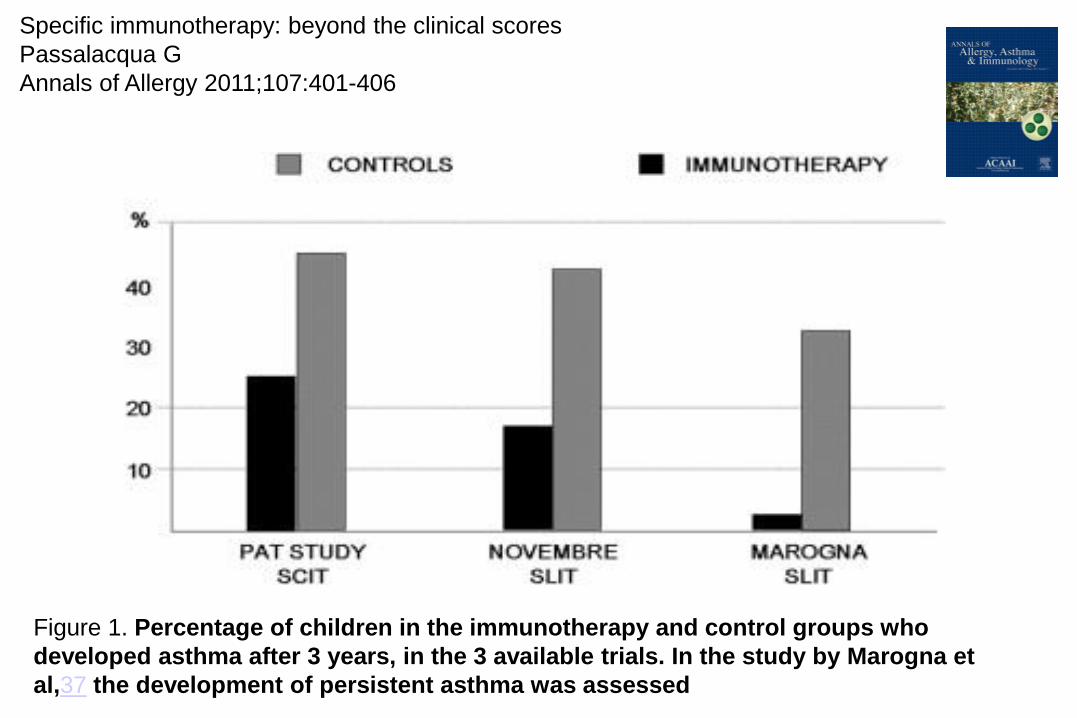
Figure 1. Percentage of children in the immunotherapy and control groups who
developed asthma after 3 years, in the 3 available trials. In the study by Marogna et
al,37 the development of persistent asthma was assessed
Specific immunotherapy: beyond the clinical scores
Passalacqua G
Annals of Allergy 2011;107:401-406

Clinical
Pathological
Pysiological
Response to
treatment
Prognostic
factors
Clin
ically o
bserv
ed
ch
ara
cte
risti
cs





Increasing post-natal age
Birth
S
L
I
T Hampering
the progression and
worsening of IgE
mediated disorders
Allergens
Exposure
Food Allergens
Inhalant Allergens
TH2 polarized
Immunity
Persistent Wheeze
Atopic Dermatitis
Hay Fever
Food Allergy
Persistent
Allergic
Diseases
J Allergy Clin Immunol 2007;119:796-801.
G.B. Pajno

OIT


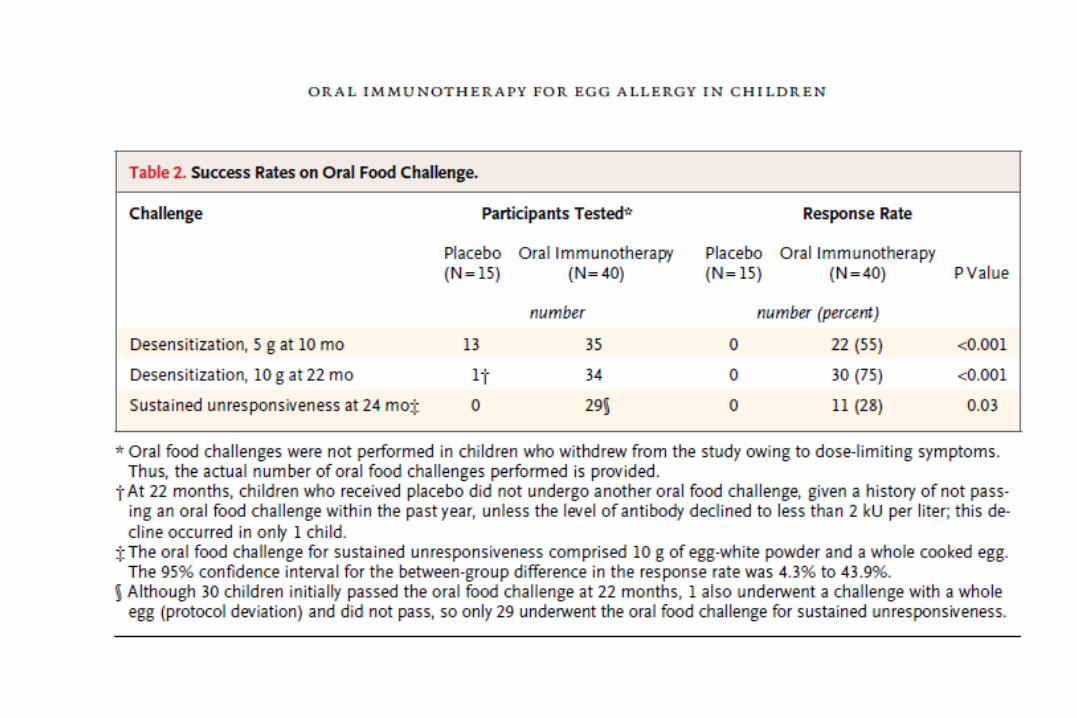
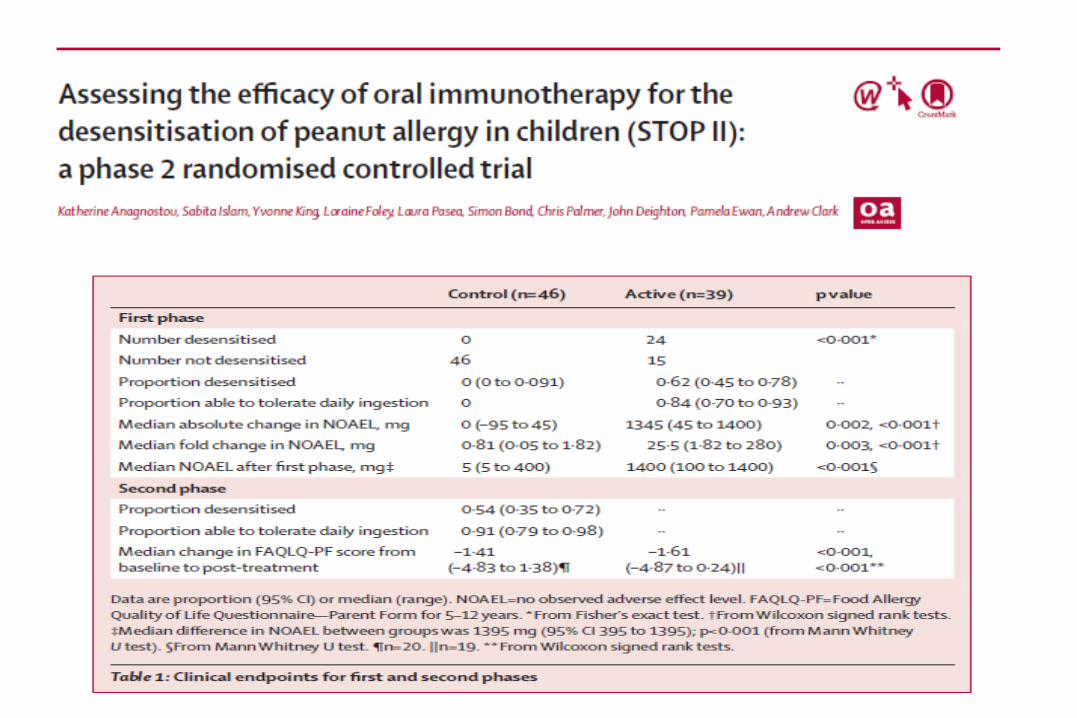
OIT
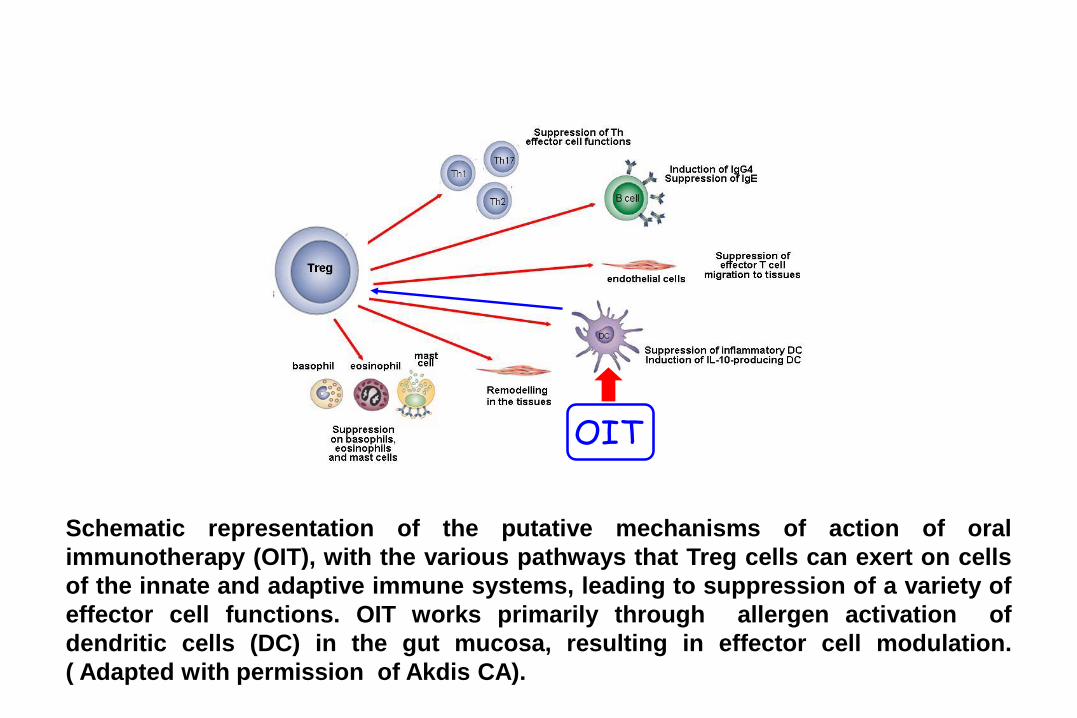
Schematic representation of the putative mechanisms of action of oral
immunotherapy (OIT), with the various pathways that Treg cells can exert on cells
of the innate and adaptive immune systems, leading to suppression of a variety of
effector cell functions. OIT works primarily through allergen activation of
dendritic cells (DC) in the gut mucosa, resulting in effector cell modulation.
( Adapted with permission of Akdis CA).
Post desensitization strategy
and follow-up
The issue of “ad libitum” diet

Nowadays seems that to consume food (s) “ad
libitum” to maintain tolerance is not required
and a more flexible maintenance regimen is
possible at least for children successfully
desensitized with CM.
CONCLUSIONI
•La SCIT e la SLIT sono efficaci e sicure
per il trattamento della rinite allergica
e dell’asma allergico in età pediatrica.
•Auspicabile l’intervento terapeutico
precoce anche prima dei cinque anni:
con la SLIT.
•Le Immunoterapie rappresentano
l’unico trattamento eziologico delle
allergie IgE mediate inclusa l’allergia
alimentare.