professor hassan nasrat sexual differentiation abnormal sexual differentiation of the female genital...
TRANSCRIPT

Professor Hassan Nasrat
Sexual Differentiation
Abnormal Sexual Differentiation of the Female Genital Tract
(Normal and Abnormal)

Professor Hassan Nasrat
Sexual Differentiation
Abnormal Sexual Differentiation of the Female Genital Tract
(Normal and Abnormal)

Sexual determination:
Sexual differentiation: :
- Gonadal Differentiation:
-Internal organ differentiation:
-External organ differentiation:
Clinical Implications of Abnormal development and of DSD:

Genetic Sex Determination (Genetic Sex)

Genetic Sex Determination (Genetic Sex)
The genetic (chromosomal) sex is determined at the time of conception (XX or XY).

The SRY gene acts as a switch or master gene for testis differentiation since it controls a whole number of further genes on the autosomes as well as on the X chromosome.
Testicular differentiation:

Ovarian differentiation:
ovarian differentiation used to be considered as the default process that spontaneously takes place in the absence of SRY chromosome.
Now it is known that it involves an active genetic pathway (including R spondin 1 (Rspo1)/Wnt-4/beta-catenin signaling that is repressed by the presence of SRY).

Gonadal Differentiation (Gonadal sex)

The phase of indifferent gonads: (Up to 7 weeks)

The indifferent gonads at 6 weeks show PGC surrounded by cells of the primitive sex cords, proliferation of the mesenchyme and the covering epithelium

The phase of gonadal differentiation
Testicular differentiation: begins during seventh week if the there is a Y chromosome that carries “SRY” gene.
In the male the primitive sex cords form the testis and the rete testis cords. The latter communicate with tubules of the mesonephric system, thus linking the testis to the mesonephric duct. The mesonephric duct becomes the ductus deferens

Ovarian differentiation: Begin at the 8th week (2 weeks after testicular
The primitive sex cords degenerate. There is no communication between the gonadand the mesonephros



Differentiation of the genital ducts (The internal genital organs)

The Indifferent stage
Up to the 7th week the internal genital organs consists of two canal systems: the mesonephric (Wolffian duct) and the Müllerian ducts (paramesonephric duct).

Stage of ductal differentiation
Differentiation of male internal organs

The atrophy of the paramesonephric duct
The development and differentiation of the mesonephric duct
Müllerian inhibiting hormone (MIH). It is responsible for regression of the ipsilateral paramesonephric (Müllerian) ducts and is an example of local paracrine effect.
induced by testosterone, it involves development of the mesonephric ducts into the internal genitalia (vas deference, epididymis, and seminal vesicles). Testosterone acts on the ipsilateral Wolffian duct.

Differentiation of Female Internal Organs
During the 7th week and in the absence of testes (MIH and testosterone) the canal system of the female sex organs differentiates.

Development of the fallopian tubes, uterus
Development of the vagina
The mesonephric duct and its tubules atrophy and out of the paramesonephric duct (Müller) arises the future fallopian tube, the uterus and the upper part of the vagina
Sometimes the remnants of the Wolffian ducts form tubule like structures known as the epoöphorons, paroophorons and Gartner’s duct
derived from the Müllerian tubes while its lower 2/3 is derived from the urogenital sinus


Differentiation of the External Genitalia

The indifferent stage
Both the urogenital sinus and the hind gut open into a common opening known as the Cloaca

The cloaca is divided into the anorectal and urogenital regions as the urorectal septum contacts the cloacal membrane.
The urogenital membrane and anal membrane then begin to break down. 50th days of gestation


Abnormal Sexual Differentiation of the Female Genital Tract

Abnormal sexual differentiation may occur as a result of defect in any one or more of the factors responsible for determination of sex i.e. chromosomal sex, gonadal sex, internal genital sex, and external genital sex.
oThe results may be identified immediately at birth as Ambiguous Genitalia (see lecture on sexual differentiation).
oAlternatively, it may not be diagnosed until later at puberty as in the case of Intersex e.g. the XY female.

Anomalies of the external genital organs
Ambiguous Genitalia
(Defect of the clitoris and labia)

Anomalies of the Internal Genital Tract "Müllerian Anomalies"

First: The differentiation of two paired mullerian ducts.
Second: lateral fusion of the lower segment of the Mullerian ducts in the midline to form the uterus, cervix and upper two third of the vagina.
Finally: Resorption of the central septum between the two Mullerian ducts in order to form a single uterine cavity and cervix.
Normal development of the internal female genital tract depends on three consecutive embryologic processes:
The lower third of the vagina embryologically originates from the sinovaginal bulb. A normal patent vagina depends on complete fusion of the ascending sinovaginal bulb with the descending müllerian tubercle.

Obstructive Mullerian anomalies.
Fusion Mullerian anomalies:
Agenesis / hypoplasia:
Miscellaneous anomalies (difficult to classify).
Classification of Mullerian anomalies
Obstructive Müllerian anomalies
Imperforate Hymen
Clinical presentation and diagnosis
Symptom
Abdominal examination
local inspection


DD:

The treatment of imperforate Hymen
The treatment is by surgical drainage of the retained contents “the hematocolpos”.

Cervical Atresia
Isolated cervical genesis. Left isolated, Right vaginal and cervical atresia

Vaginal Agenesis
Transverse Vaginal Septum

Defects of Mullerian Duct fusion
Are relatively common (2-3%). usually presents with primary dysmenorrhea, fusion anomalies are often associated with gynecological as well as obstetrics complications such as infertility, recurrent pregnancy loss and poor obstetrics outcome in pregnancy.

Complete failure of fusion of mullerian ducts
didelphic uteri
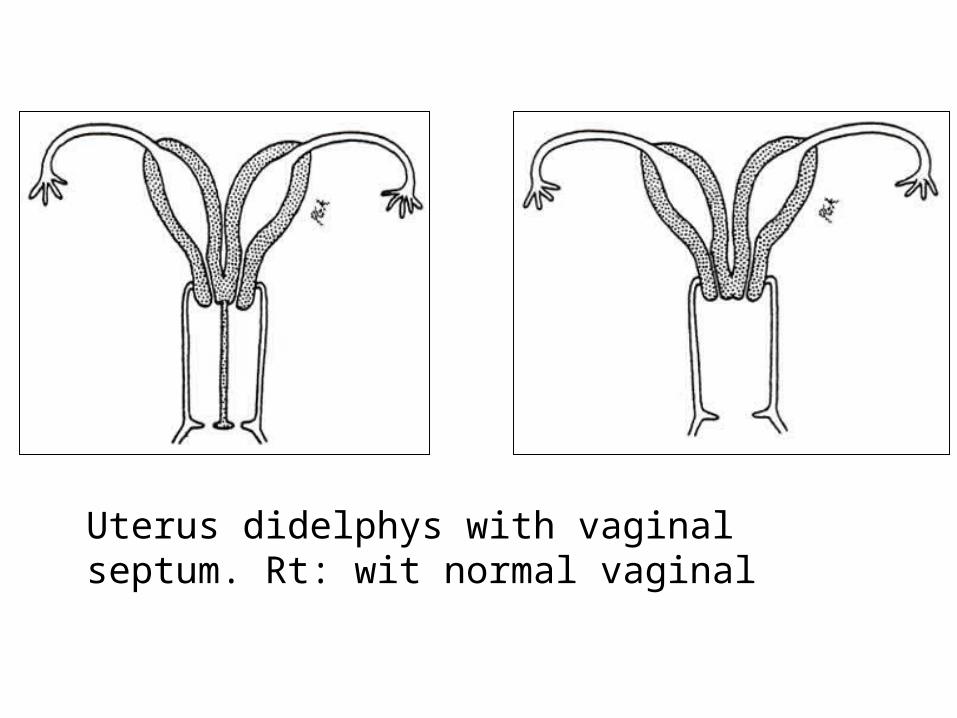
Uterus didelphys with vaginal septum. Rt: wit normal vaginal

Partial failure of Mullerian tubes fusion
Septet uterus: Left: partial (with minimum complications and not treatment required). Middle "bicornuate unicollis" septum reaches to the internal os. Right complete septum reaching external os "bicornuate bicollis"


Anomalies due to unilateral defects of Mullerian duct development
Left: Unicornuate uterus, Middle: horn communicating with the uterus, Right: horn not communicating with the uterus.

Diethylstilbestrol Associated anomalies “DES”