preventive ophthalmology
TRANSCRIPT
Preventive OphthalmologyPresented and reviewed by Mr. PatinyaYutchawitMr. Yotdanai NamuangchanMiss. Rattanaporn Sirirattanakul

Cure sometimes,
Treat often,
Comfort always.Hippocrates
Contents
▪ Introduction and definition of preventive ophthalmology
▪ Servicing based on groups.
▪ Early age screening : Amblyopia , strabismus , congenital cataract , retinopathy of prematurity
▪ Preventive ophthalmology in ocular injuries
▪ Visual impairment in Adult : Refractive error, Glaucoma, AMD, Blindness and low vision
▪ Preventive Ophthalmological Projects in Thailand
Preventive Ophthalmology
▪ Public health ophthalmology / Preventive eye care/ Community ophthalmology
▪ To provide an ophthalmologic service; identifying and preventing eye sight threatening ocular condition, to whoever (mass, large number) in community in affordable costs.
Clinical application
General method of preventive healthcare.
Primary prevention
▪ To prevent people from disease.
▪ Eliminate or limit the risk factors and pathogen exposure.
Methods
Community immunization : การสรางเสรมสขอนามย การสรางสขนสยทด การดแลเรองโภชนาการ การใหภมคมกน หรอยา ปองกนโรค ตลอดถงการควบคมทาง
พนธกรรม
Environmental control : งานดานสขาภบาล การก าจดพาหะน าโรค การดแลอาชวอนามย และการจดการเรองสงแวดลอม
Health care system management : ใหสขศกษา ความรพนฐาน การดแลรกษาเบองตน การออกกฎหมาย และการจดระบบบรการตางๆ
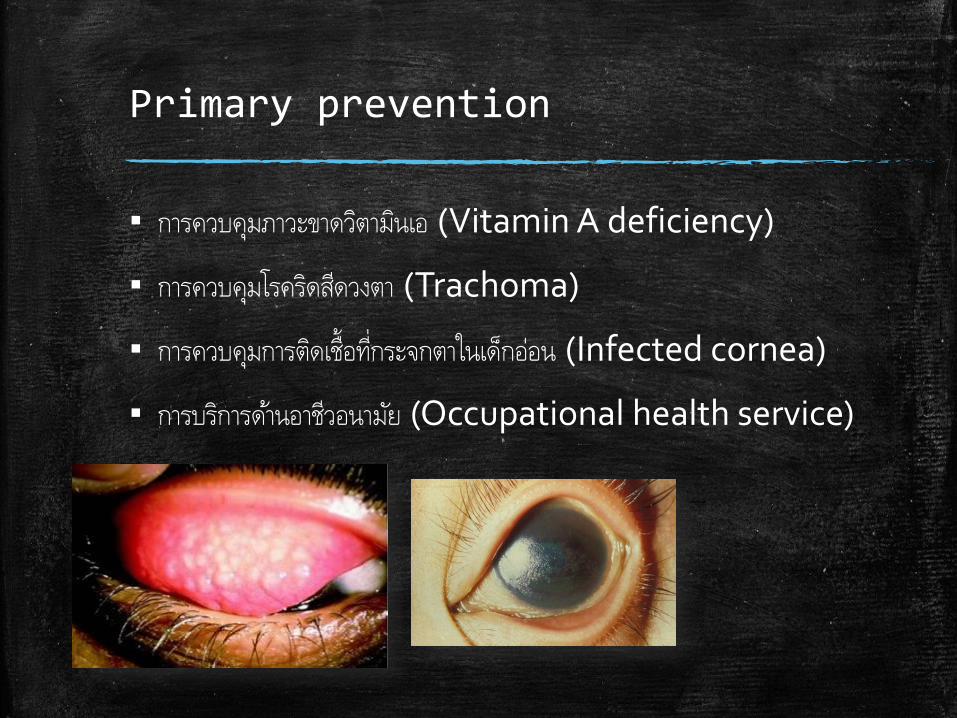
Primary prevention
▪ การควบคมภาวะขาดวตามนเอ (Vitamin A deficiency)
▪ การควบคมโรครดสดวงตา (Trachoma)
▪ การควบคมการตดเชอทกระจกตาในเดกออน (Infected cornea)
▪ การบรการดานอาชวอนามย (Occupational health service)
Secondary prevention
▪ To prevent disease’s progression and disability
▪ Early diagnosis
Screening may not efficient and value in every diseases. We consider to do in case of…
High severity
High incidence and prevalence
High understanding of pathogenesis
There’re effective treatments available
Screening tool is accurate, accountable and affordable.
Secondary prevention
Worth screening diseases
▪ Cataract
▪ Diabetic retinopathy
▪ Amblyopia
▪ Glaucoma
Tertiary prevention
▪ To rehabilitation, correction of disability
Examples :
Blindness rehabilitation
Keratoplasty
Servicing based on groups
▪ Child (<6 year-old) with low risk
▪ Child with high risk
▪ Adult with low risk
▪ Adult with high risk
Child with low risk
▪ Ocular examination should be done once the infant born, 6 months , 3 years and at 5-6 years
Once they born : external eye examination, ocular alignment (Hirschberg’s test), ophthalmoscopy
6 months : VA, Ext eye examination, pupillary exam, ocular alignment, ophthalmoscope (Red reflex)
3 years : VA (Picture,E game), Ext eye examination, pupillary exam, ocular motility and alignment, ophthalmoscope (Red reflex)
5-6 years : VA (Snellen), Ext eye examination, pupillary exam, ocular motility and alignment, ophthalmoscope (Red reflex and fundus)
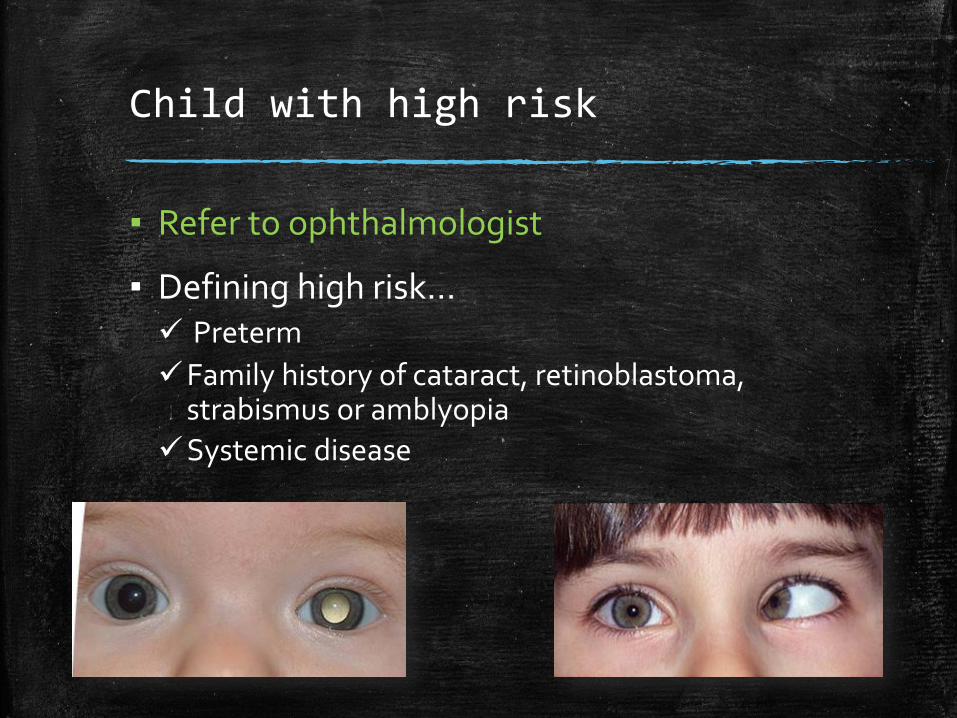
Child with high risk
▪ Refer to ophthalmologist
▪ Defining high risk… Preterm
Family history of cataract, retinoblastoma, strabismus or amblyopia
Systemic disease
Adult with low risk
6-40 year-olds : VA q 3 year
> 40 year-olds : refer to ophthalmologist q 2-4 year for presbyopia and glaucoma screening
Adult with high risk
▪ Refer to ophthalmologist q 1-2 years
▪ Defining high risk… Hx of Retinal detachment/Severe ocular trauma
Low vision
Underlying disease : DM, HT
Family Hx of Glaucoma, eye disease
Over 65 year-olds
Amblyopia & Strabismus
▪ Primary prevention– Screening for causes of from deprivation within the first
4-6 weeks after birth, and children at risk should be monitored yearly to 4 years of age
Newborn to 3 months of age– Red reflex test with a direct ophthalmoscope.
– External inspection of the eyes to assess for any structural abnormalities (penlight exam is sufficient).
– Pupillary exam.
16
Amblyopia & Strabismus
3-6 months of age– Tests for newborn to 3 months are repeated.
– Tests to check whether the infant can fix and follow with each eye independently.
6-12 months of age, and then yearly until the child can co-operate with verbal visual acuity testing
– Tests for newborn to 3 months are repeated.
– Corneal light reflex test, to check for a symmetrical response in both eyes.
– Alternate occlusion of each eye: the infant's behavioral response should be equal to having either eye occluded. In other words, the infant should object or not object equally.
17
Amblyopia & Strabismus
3-4 years of age– Tests for newborn to 3 months are repeated.
– Corneal light reflex test, to check for a symmetrical response in both eyes.
– Cover/uncover test to assess for re-fixation movements.
– Visual acuity testing, independently for each eye. Visual acuity of 20/50 or worse, or a ≥2 line difference between the 2 eyes, should be referred.
18
Amblyopia & Strabismus
5 years of age– Tests for newborn to 3 months are repeated.
– Corneal light reflex test, to check for a symmetrical response in both eyes.
– Cover/uncover test to assess for re-fixation movements.
– Visual acuity testing, independently for each eye. Visual acuity of 20/40 or worse, or a ≥2 line difference between the 2 eyes, should be referred.
19
Amblyopia & Strabismus
▪ Secondary prevention
The American Academy of Ophthalmology recommends that patients who are functionally monocular due to amblyopia should help to prevent vision loss to the better-seeing eye by– Wearing polycarbonate spectacles even if they do
not require refractive correction– Wearing protective goggles and facial protection for
contact sports and potentially dangerous activities such as paintball
– Having regular eye examinations throughout life.
Reference: Bestpractice(BMJ group): Amblyopia
20
Amblyopia & Strabismus
▪ Tertiary prevention– Follow up at 2, 4, 6, 8 and 12 months are recommended
21
Congenital cataract
▪ A congenital cataract is a clouding of the lens of the eye that is present at birth.
Risk factors
–Genetic disease, birth defect
– Intrauterine infections : maternal rubella
22

Congenital cataract
▪ Primary prevention– Genetic counseling
– Measles, rubella vaccine
▪ Secondary prevention– Early detection: leukocoria
– Surgery
23
Retinopathy of prematurity
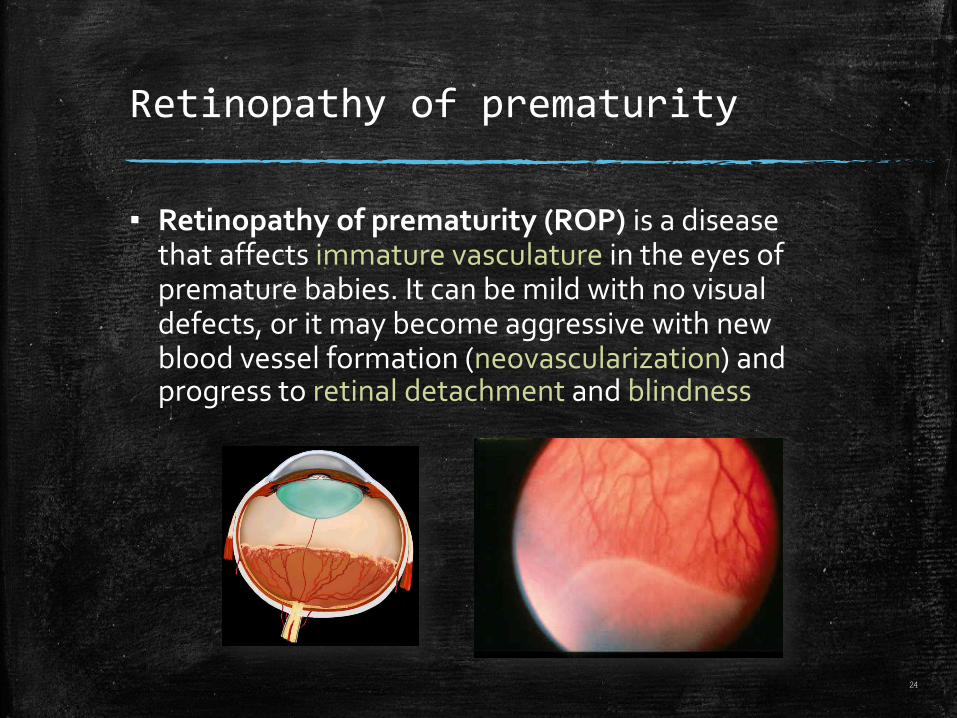
▪ Retinopathy of prematurity (ROP) is a disease that affects immature vasculature in the eyes of premature babies. It can be mild with no visual defects, or it may become aggressive with new blood vessel formation (neovascularization) and progress to retinal detachment and blindness
24
Retinopathy of prematurity
▪ Risk factors– Prematurity, GA<32 wks
– Low birth weight <2000 gram
– Supplemental oxygen (duration and concentration)
25
Retinopathy of prematurity
▪ Primary prevention– Quality antenatal care to prevent premature birth
– Quality neonatal care: well-maintained and working incubators
▪ Secondary prevention– Screening (Age 4-6 wks)
1. Prematurity ( GA<32 wks)
2. LBW<1500 gm
3. GA>32 wks and BW 1500-2000 gm with unstable clinical cause
26
Retinopathy of prematurity
▪ Tertiary prevention– Cryotherapy or lacer photocoagulation at stage
III will prevent progression of disease to retinal detachment.
– Follow up for complication such as vitreous hemorrhage, retinal detachment.
27
Preventive ophthalmology in ocular injuries
▪ Occupational injuries
▪ Non-occupational injuries
Occupational ocular injuries
▪ Chemical Burns – One of the two “true” ocular emergencies.
– Chemical burns to one or both eyes from splashes of industrial chemicals or cleaning products are common.
– Acid vs Alkali
Occupational ocular injuries
▪ Radiation Burns UV radiation burns (welder’s flash) routinely damage workers’ eyes and surrounding tissue, leading to epithelial keratitis.
▪ Who are at risk? – Patients who work in physically-demanding jobs, including
factory workers, manufacturers, welders, carpenters, and construction workers.
▪ Prevention– Proper training and education of workers in the use of
machinery and goggles, as well as the public.
– Early recognition & urgent assessment of ocular injuries are essential.
– Proper labeling and storage
Occupational ocular injuries

Non-occupational ocular injuries
▪ Ultraviolet radiation exposure – Associated with pterygium, basal cell carcinoma
and melanoma of the eyelids
– Substantial evidence linking UV exposure with development of cataract.
▪ Prevention– Wear Protective Eyewear such as sunglasses.
Visual impairment in adult
Refractive error
▪ Refractive error– Myopia, Hyperopia, Astigmatism– Risk factor
▪ Family history
▪ Previous history of ocular trauma, surgery, infection
▪ Near-work
▪ Primary prevention– Avoid risk factor
▪ Secondary prevention– Optical correction
▪ Spectacle
▪ Lens
▪ Refractive surgery
▪ Tertiary prevention– Prevent amblyopia by Optical correction
Glaucoma
▪ Risk factor– Age>40 years
– Asian
– Family history
– Refractive error
– Steroid
▪ Primary prevention– Avoid Risk factor
▪ Secondary prevention– Early detection
▪ Age 40-60 : test every 4 years
▪ Test every 1-2 year if– Age 60 or more
– Family history of glaucoma
– Asian or black
– DM, Chronic inflammatory disease
– History of eye injury
– Using steroid
▪ Tertiary Prevention– Surgery :Laser Iridotomy
Glaucoma
Age related macular degeneration
▪ More than 50 years
▪ Loss of central field of vision
▪ Macula degenerative lesion
▪ The primary cause of visual impairment in industrialized countries.
▪ Primary prevention– Avoid risk factor
▪ Use of tobacco▪ Genetics tendencies▪ Arterial hypertension▪ UV
▪ Secondary prevention and Tertiary prevention– Laser
– Surgery
– Rehabilitation
– Bright lighting
– Use special aids for viewing or using computer
Age related macular degeneration
Blindness and low vision
Blindness
▪ Definition– The inability to see
▪ The World Health Organization (WHO)– best corrected visual acuity of 3/60 or less, in the better
eye
▪ สมาคมจกษแพทยแหงประเทศไทย ( 2550 )
ตาบอด (Blind) หมายความวา การมสายตาขางทดทสดเมอใชแวนตาธรรมดาแลว
ระดบสายตาจากระยะทาง (เมตร) ตอระยะภาพ พบผลนอยกวา 3/60 ลงไปจนถงบอด
สนท หรอมลานสายตาโดยเฉลยแคบกวา 10 องศา
Blindness
Vision
▪ The sense by which objects in the external environment are perceived by means of the light they give off or reflect.
▪ The act of seeing.
Low vision
▪ The World Health Organization (WHO)
Visual acuity less than 6/18 and equal to or better than 3/60 (10/200) in the better eye with best correction
▪ สมาคมจกษแพทยแหงประเทศไทย ( 2550 )
สายตาพการหรอสายตาเลอนราง (Low vision) หมายความวา การมสายตาขางท
ดทสดเมอใชแวนตาธรรมดาโดยไมรวมเครองชวยสายตาพเศษ (Visual aids)แลวระดบสายตา (Visual Acuity: VA) ดวยแผนทดสอบSnellen Chart จากระยะทาง(เมตร)ตอระยะภาพ พบผลนอยกวา 6/18 จนถง 3/60 หรอมลานสายตา
โดยเฉลยแคบกวา 30 องศาไปจนถง 10 องศา
Low vision
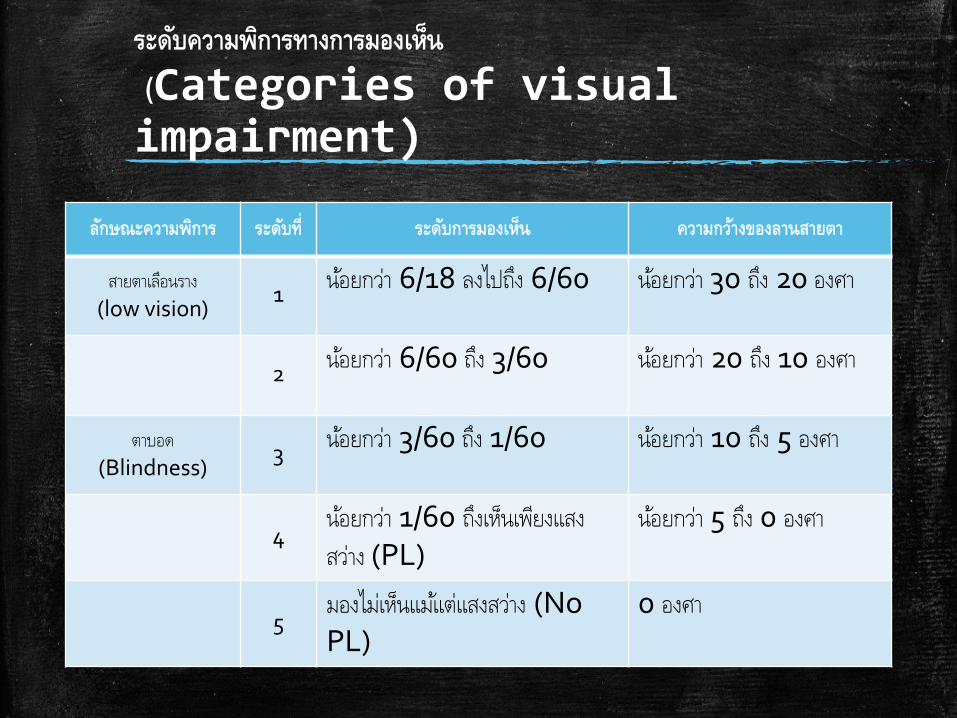
ระดบความพการทางการมองเหน
(Categories of visual impairment)
ลกษณะความพการ ระดบท ระดบการมองเหน ความกวางของลานสายตา
สายตาเลอนราง
(low vision)1
นอยกวา 6/18 ลงไปถง 6/60 นอยกวา 30 ถง 20 องศา
2นอยกวา 6/60 ถง 3/60 นอยกวา 20 ถง 10 องศา
ตาบอด
(Blindness)3
นอยกวา 3/60 ถง 1/60 นอยกวา 10 ถง 5 องศา
4นอยกวา 1/60 ถงเหนเพยงแสง
สวาง (PL)นอยกวา 5 ถง 0 องศา
5มองไมเหนแมแตแสงสวาง (NoPL)
0 องศา
Global Prevalence of Visual Impairment
▪ Vision 285 million people are estimated to be visually impaired worldwide: 39 million are blind and 246 have low vision.
▪ About 90% of the world's visually impaired live in developing countries.
▪ 82% of people living with blindness are aged 50 and above.
▪ Globally, uncorrected refractive errors are the main cause of visual impairment; cataracts remain the leading cause of blindness in middle- and low-income countries.
▪ The number of people visually impaired from infectious diseases has greatly reduced in the last 20 years.
▪ 80% of all visual impairment can be avoided or cured.
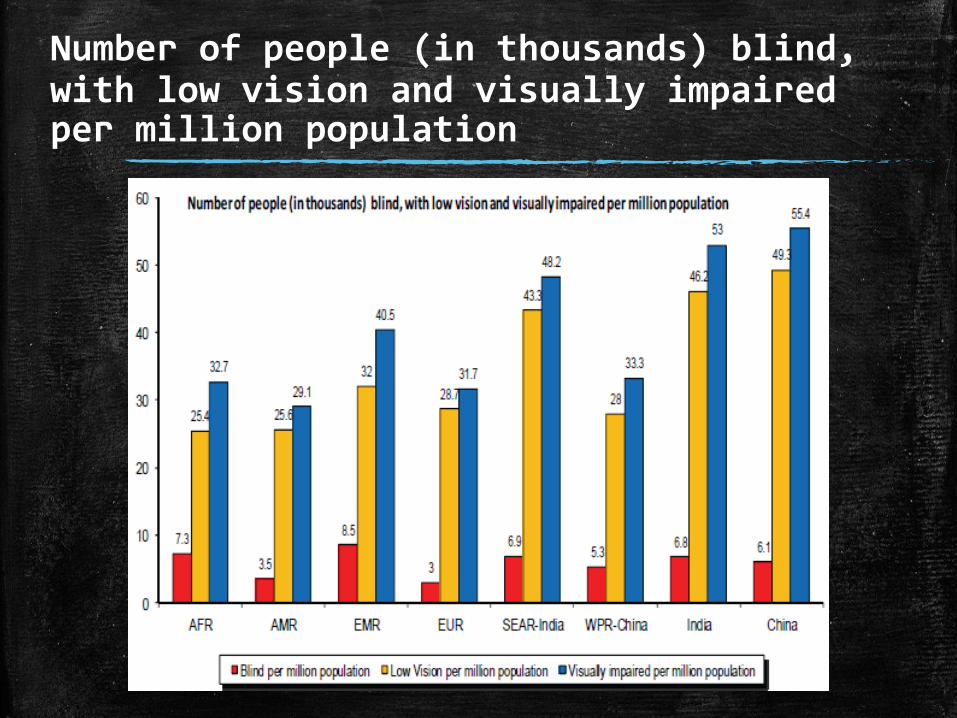
Number of people (in thousands) blind, with low vision and visually impaired per million population
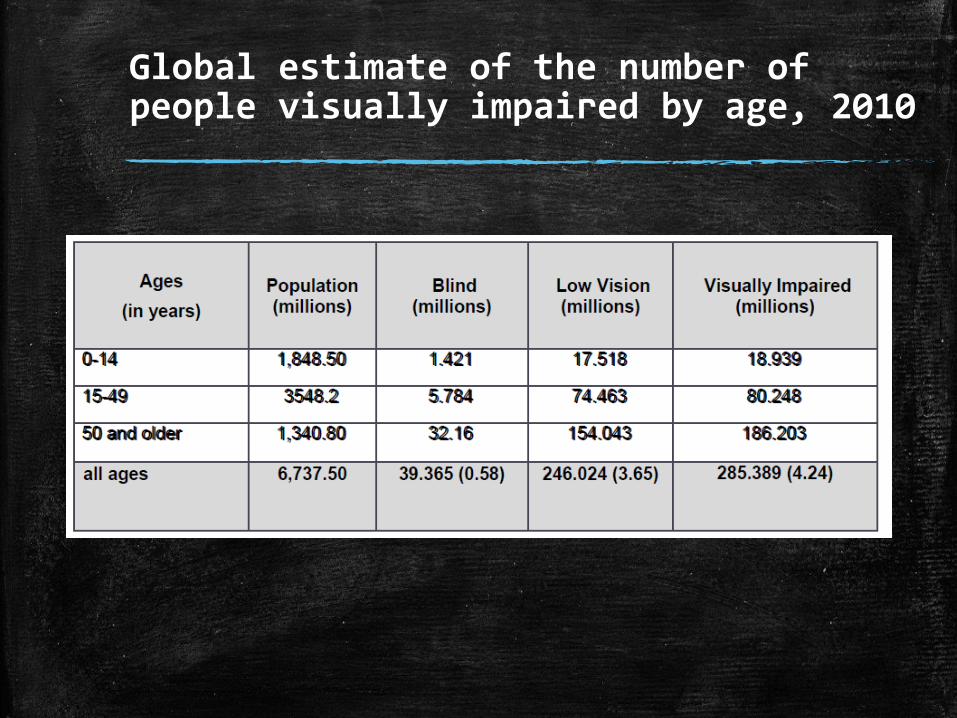
Global estimate of the number of people visually impaired by age, 2010
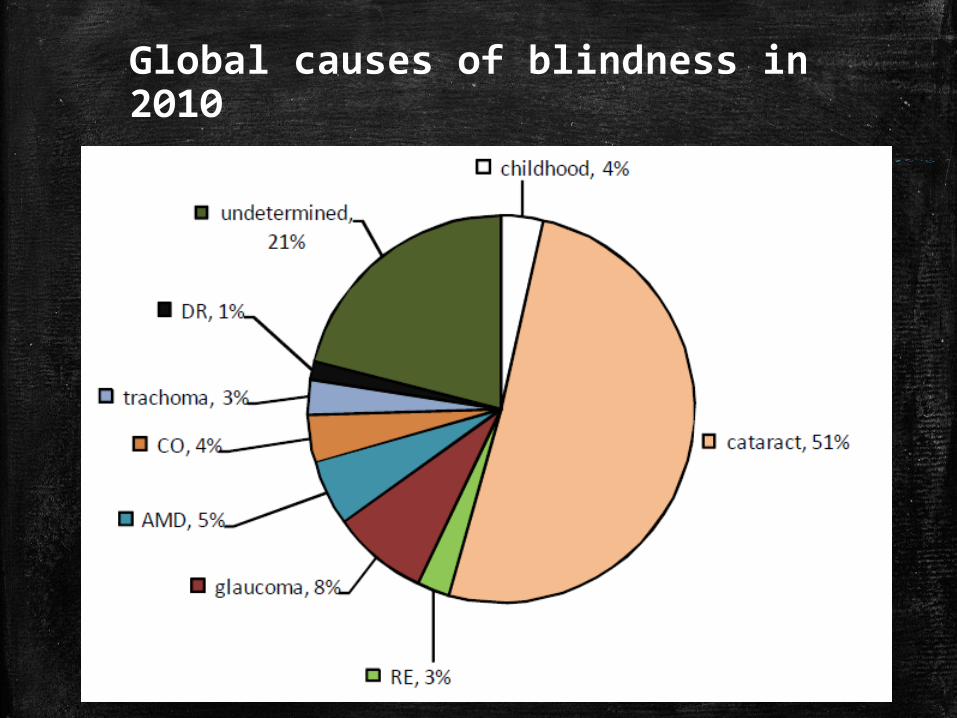
Global causes of blindness in 2010
▪ As a global target, the reduction in prevalence of avoidable visual impairment by 25% by 2019 from the
▪ baseline of 2010 has been selected for this action plan
▪ The reduction in the prevalence of avoidable visual impairment in that portion of the population representing those who are over the age of 50 years, cataract and uncorrected refractive errors are the two principal causes of avoidable visual impairment, representing 75% of all visual impairment.
รายงานผลการส ารวจสภาวะตาบอด และสายตาเลอนราง
โรคตาทเปนปญหาสาธารณสข คร งท 4 ในประเทศไทย
The Fourth National Survey of Blindness,Low vision and Major
Eye diseases in Thailand
โดย พญ.วฒนย เยนจตพ.ศ. 2549-2550
51
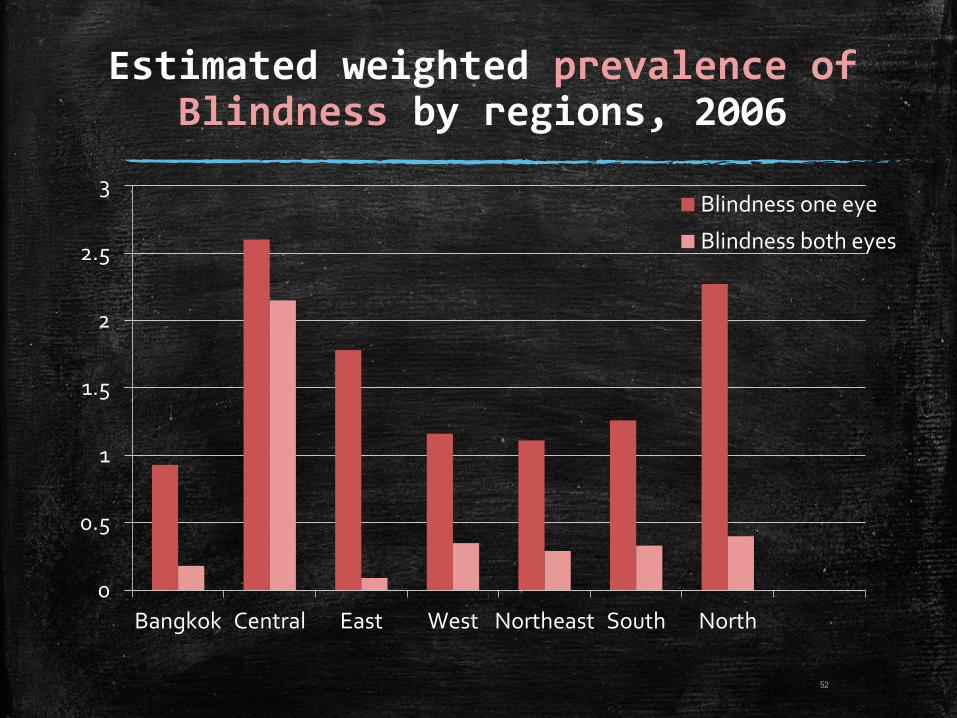
Estimated weighted prevalence of Blindness by regions, 2006
0
0.5
1
1.5
2
2.5
3
Bangkok Central East West Northeast South North
Blindness one eye
Blindness both eyes
52
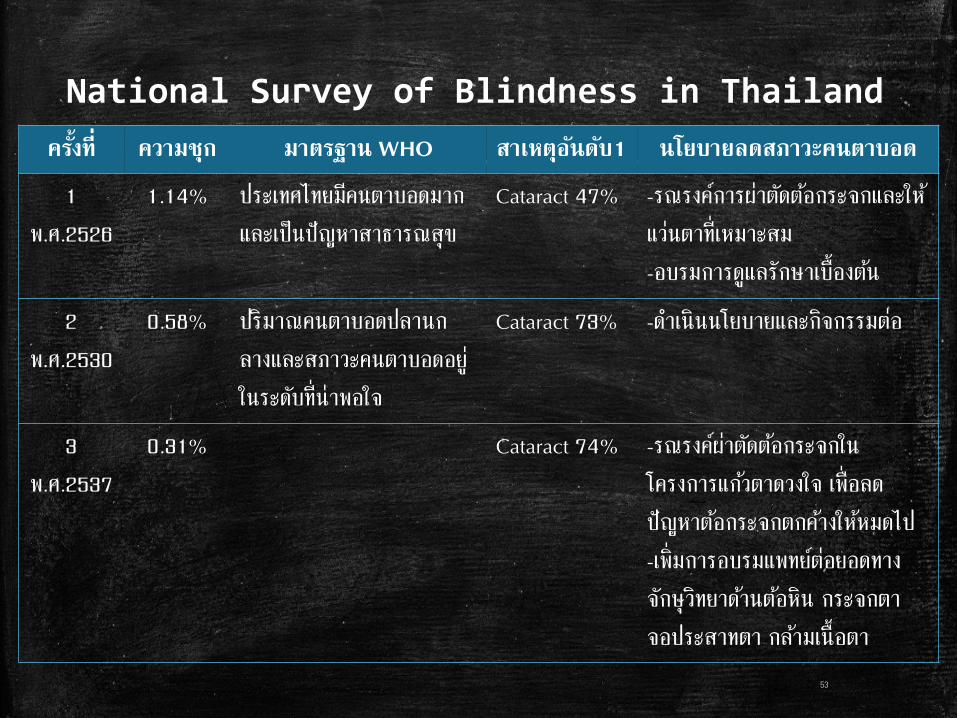
National Survey of Blindness in Thailand
ครงท ความชก มาตรฐาน WHO สาเหตอนดบ1 นโยบายลดสภาวะคนตาบอด
1
พ.ศ.2526
1.14% ประเทศไทยมคนตาบอดมาก
และเปนปญหาสาธารณสข
Cataract 47% -รณรงคการผาตดตอกระจกและให
แวนตาท เหมาะสม
-อบรมการดแลรกษาเบองตน
2
พ.ศ.2530
0.58% ปรมาณคนตาบอดปลานก
ลางและสภาวะคนตาบอดอย
ในระดบท นาพอใจ
Cataract 73% -ด าเนนนโยบายและกจกรรมตอ
3
พ.ศ.2537
0.31% Cataract 74% -รณรงคผาตดตอกระจกใน
โครงการแกวตาดวงใจ เพอลด
ปญหาตอกระจกตกคางใหหมดไป
-เพมการอบรมแพทยตอยอดทาง
จกษวทยาดานตอหน กระจกตา
จอประสาทตา กลามเนอตา
53
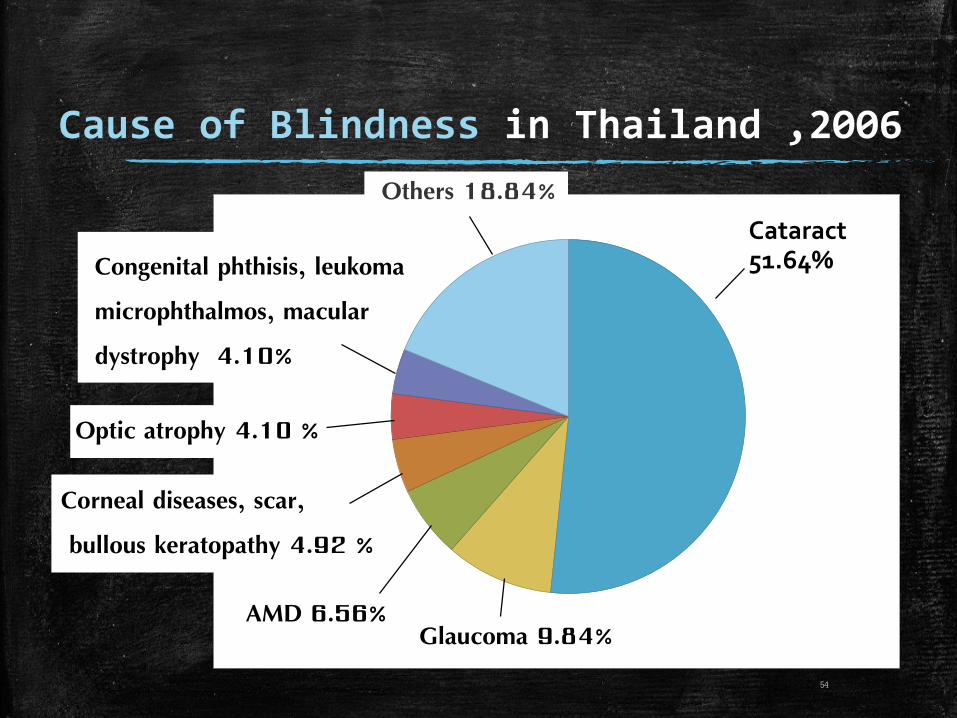
Cataract 51.64%
Cause of Blindness in Thailand ,2006
Glaucoma 9.84%AMD 6.56%
Corneal diseases, scar,
bullous keratopathy 4.92 %
Others 18.84%
Optic atrophy 4.10 %
Congenital phthisis, leukoma
microphthalmos, macular
dystrophy 4.10%
54
The Fourth National Survey of Blindness in Thailand
▪ ในภาพรวมของประเทศไทยอตราความชกของตาบอดคดเปนรอยละ 0.59
(พบในเพศชายรอยละ 1.03 มากกวาเพศหญงซงพบรอยละ 0.29)
และอตราความชกของสายตาเลอนรางคดเปนรอยละ 1.57
(พบในเพศหญงรอยละ 1.93 มากกวาเพศชายซงพบรอยละ 0.93)
โดยพบความชกของตาบอดและสายตาเลอนรางมากทสดทภาคกลาง สวน
ภาคอนๆไมแตกตางกน
▪ สาเหตหลกของตาบอด คอ ตอกระจก
▪ โรคอนๆ เชน ตอหน โรคของจอประสาทตา และภาวะสายตาผดปกต
55
▪ การประเมนผลนโยบายและกจกรรมโครงการสงเสรมสขภาพในรอบ
10 ปทผานมา
- อยในเกณฑดแมวาผสงอายจะมากขน แตตอกระจกชนดบอดทตกคาง
( Cataract backlog) ลดลง
- เบาหวานในจอประสาทตาเรมไดรบความสนใจคดกรอง แตเนองจากเพง
เรมตน จงยงใหบรการไดไมครบวงจร จงยงคงพบผปวยตาบอดจากเบาหวาน
- การฟนฟสมรรถภาพทางการแพทยส าหรบคนตาบอดและสายตาเลอน
รางยงไดรบความสนใจ แตเนองจากบคลากรทางจกษนอยมาก จงเปนขอสรปท
ท าใหบรการทางตาของประเทศไทยยงไมครอบคลมทกกลมประชากร56
The Fourth National Survey of Blindness in Thailand
▪ การประเมนประสทธภาพการใหบรการทางตา
- การเขาถงของประชาชนในระบบสาธารณสข อยในเกณฑดมาก
- การแกปญหาตอกระจกตกคางโดยวธการจายตรงของ สปสช. เปนวธแกปญหาทด อปสรรคของผทไมเขาถงบรการ มกเกดจากความเชอทผด ยอมรบความพการทาง
ตา ไมทราบวาเลนสเทยมเปนอปกรณทรฐใหบรการโดยไมเสยคาใชจาย
- จงหวดหรอภาคทมประชากรสายตาพการมาก พบวาสมพนธกบอตราสวนจกษ
แพทยกบประชากร
57
The Fourth National Survey of Blindness in Thailand
ตวอยางนโยบายใหมของ สปสช. ในการแกปญหาตาบอดจากตอกระจกในประเทศไทย(ตอ)
นโยบายของ สปสช เพอแกปญหาดงกลาว1. สปสช.ไดจดระบบการจายคาชดเชยใหม โดยหนวยบรการทผาตามปกตและ
ผาตดเชงรก จะไดรบการชดเชยเหมอนกน จายชดเชยดวยระบบเหมาจาย คอ เปนคาตรวจประเมนสภาพรางกายผ ปวย คาวสดอปกรณ คายา และคาตรวจชนสตร รวมทงคาผาตด คารกษาภาวะแทรกซอน การตดตามดแลหลงผาตด ในอตราดงน กรณไมมภาวะแทรกซอน ชดเชยขางละ 7,000 บาท กรณมภาวะแทรกซอนชดเชยขางละ 9,000 บาท
2 . สนบสนนเลนสแกวตาเทยม โดย สปสช.จะจดสงเลนสแกวตาเทยมตามระบบ VMI จากบรษททอยในบญชรายการและราคาทคณะท างานวชาการ สปสช.ก าหนด และหากหนวยบรการมความพรอมในการจดหาตามหลกเกณฑท สปสช.ก าหนด ใหแจง สปสช.เพอเหนชอบ ซงอตราเลนสแขงพบไมไดชดเชย 700 บาทตอเลนส และเลนสพบไดชดเชย 2,800 บาทตอเลนส
60
3. ลดควผาตดตาตอกระจก จากขามปเหลอไมเกน 3 เดอน
▪ เพอใหผปวยบางกลมโรคไดเขาถงการรกษาทมคณภาพอยางรวดเรวนน
อาท โรคตอกระจก ซงแตละปมผสงอายปวยดวยโรคตอกระจกรายใหม 60,000 คน ขณะท
ม ผปวยสะสมรอรบการผาตดกวา 100,000 คน ซงหากยงปลอยใหสภาวะด าเนนไปเชนน
จะสงผลใหตวเลขผปวยสะสมทวจ านวนเพมมากขน และสรางความทกขทรมานใหกบผสงอาย
ครอบครว
▪ สปสช.รวมมอกบ สธ.ใชแนวทางจดการโรคเฉพาะเพอลดการรอควผปวยโรคตอกระจก
จากเคยรอควขามป เหลอไมเกน 3 เดอน
61
ตวอยางนโยบายใหมของ สปสช. ในการแกปญหาตาบอดจากตอกระจกในประเทศไทย(ตอ)
4.โครงการพเศษรณรงคผาตดตาตอกระจกใน 3 จงหวดชายแดนใต ความส าคญของปญหา
จากสถานการณความไมมนคงในพนท 3 จงหวดชายแดนภาคใต ยะลา ปตตานและนราธวาส ไดสงผลกระทบตอการจดบรการผาตดตอกระจกใหกบผ ปวย ท าใหการเขาถงบรการของผ ปวยอยในอตราทต ากวาประชาชนในพนทจงหวดอนๆ
ความรวมมอระหวาง
- สปสช
- ศนยอ านวยการบรหารจงหวดชายแดนใต
- กระทรวงกลาโหม
- กระทรวงสาธารณสข
- กระทรวงมหาดไทย
- บรษททาสของแผนดนจ ากด
อ านวยความสะดวกในการจดบรการผาตดในพนท
ตลอดจนการดแลความปลอดภย
สนบสนนงบประมาณการชดเชยตามอตราทก าหนด
62
ตวอยางนโยบายใหมของ สปสช. ในการแกปญหาตาบอดจากตอกระจกในประเทศไทย(ตอ)
▪ เปาหมาย
- เปลยนกระจกตา 9,999 ราย
- ภายใน 3 ป
งบประมาณ
- 98 ลานบาท
- ประกอบดวย : คาบรการผาตดขางละ 7,000 บาท
คาเลนสแกวตาเทยม 2,800 บาท
63
ตวอยางนโยบายใหมของ สปสช. ในการแกปญหาตาบอดจากตอกระจกในประเทศไทย(ตอ)
แนวทางแกไขปญหาตาบอดจากตอกระจกในประเทศไทย
การประชาสมพนธขอความรวมมอจดท าเปนโครงการพเศษเนองในวโรกาสตางๆ เชน
▪ โครงการแกวตาดวงใจ เนองในวโรกาสทสมเดจพระนางเจาสรกต
พระบรมราชนนาถมพระชนมาย 72 พรรษา
- ผาตดตอกระจกแกผปวยทยากไรและดอยโอกาส
- รายละ 1,500 บาท จ านวน 600 ราย เปนเงนจ านวน 900,000 บาท
▪ โครงการตอกระจกเฉลมพระเกยรตในวโรกาสทพระบาทสมเดจพระเจาอยหวทรง
ครองราชยครบ 60 พรรษา และในวโรกาสทมพระชนมาย 80 พรรษา
64
แนวทางปองกนและแกไขปญหา
ตาบอดจากโรคเบาหวานในประเทศไทยโครงการสงเสรมสขภาพและปองกนภาวะตาบอดของผทปวยเปนโรคเบาหวาน
▪ เปนความรวมมอระหวาง สปสช. และ ส านกงานปลดกระทรวงสาธารณสข
▪ เปาหมาย : 1. เพอใหผ ปวยเบาหวานไดรบการตรวจหา
ภาวะแทรกซอนทางตา จ านวน 9,999 ดวงตา
2. ในรายทพบความผดปกตของเสนเลอดทไปเลยงจอประสาทตา
จะผาตดดวยเครองเลเซอรทอยภายในรถ หลงผาตดผปวยสามารถกลบ
บานได และนดตดตามผลภายหลง
▪ เรมต งแตตลาคม 2552 – กนยายน 2554
65
โครงการปองกนตาบอดจากโรคตอหน
มหกรรมสปดาหตอหนโลก World Glaucoma week 2557
จดโดย : ภาควชาจกษวทยา คณะแพทยศาสตร มหาวทยาลยขอนแกน
วตถประสงค : 1. เพอใหประชาชนเกดความตระหนกในอนตรายของโรคตอหน
2. เพอตรวจคดกรองโรคตอหน เพอจะไดรกษาตงแต ระยะเรมตน
กจกรรมภายในงาน : - การจดนทรรศการใหความร การฉายวดทศน และรายการบนเวท
- ตอบค าถามชงรางวล
- จดพนทตรวจสขภาพตา คดกรองโรคตอหน การใหค าแนะน า
- ตอบปญหาทกปญหาเกยวกบโรคตา และตอหนโดยแพทย และบคลากรทมความร และประสบการณ
66
Prevention and treatment of Cataract
▪ Primary Prevention
- Have regular eye examinations
- Quit smoking
- Reduce alcohol use
- Wear sunglasses
- Manage other health problems
- Maintain a healthy weight
- Choose a healthy diet that includes plenty of fruits and vegetables
67
Prevention and treatment of Cataract
▪ Secondary prevention
- Early diagnosis and treatment
▪ Tertiary prevention
- Surgery
68
Prevention and treatmentof Diabetic retinopathy
▪ Primary prevention
- Diminish risk factor :
Weight , Inactivity , High blood pressure , Abnormal cholesterol levels , High levels of triglycerides
- Control stage of those risk
- Screening for DM
Age > 40
FH of DM
Pregnancy
Hypertension
Dyslipidemia
69
Prevention and treatmentof Diabetic retinopathy
▪ Secondary prevention
- Eye examination for early diagnosis
- Glycemic control ( HbA1C < 7% )
- Blood pressure contral ( BP < 130/80 )
70
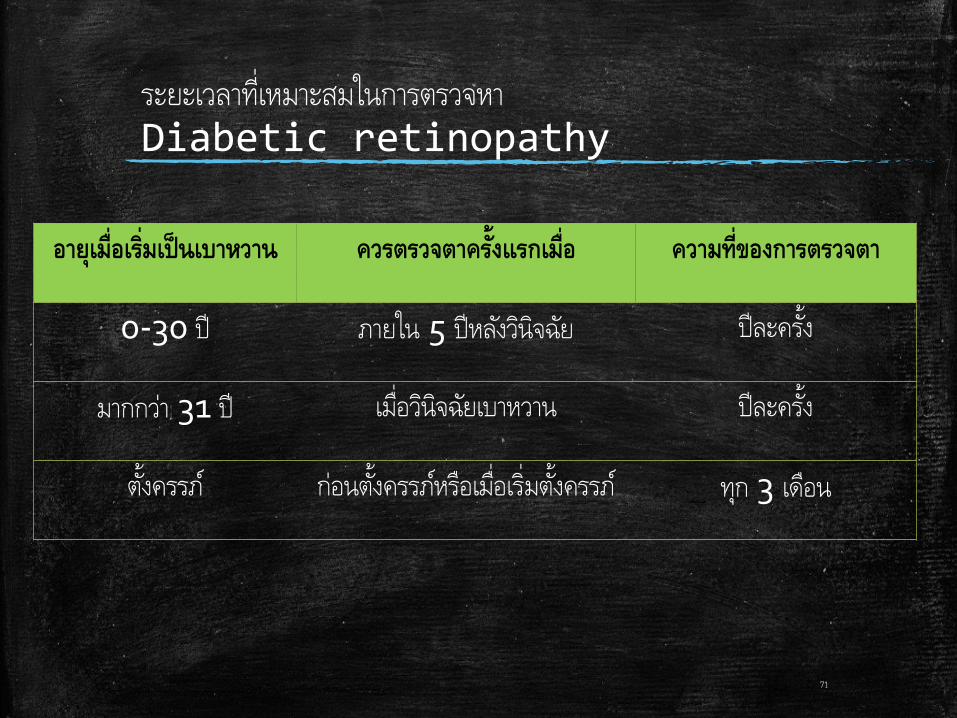
ระยะเวลาทเหมาะสมในการตรวจหา
Diabetic retinopathy
อายเมอเรมเปนเบาหวาน ควรตรวจตาคร งแรกเมอ ความทของการตรวจตา
0-30 ป ภายใน 5 ปหลงวนจฉย ปละครง
มากกวา 31 ป เมอวนจฉยเบาหวาน ปละครง
ต งครรภ กอนตงครรภหรอเมอเรมต งครรภ ทก 3 เดอน
71
Prevention and treatmentof Diabetic retinopathy
▪ Tertiary prevention
- Pan retinal photocoagulation (PRP)
- Cryoretinoplexy
- Focal laser for macular edema
72
ความส าคญของ
Preventive ophthalmology ตอการท างานในฐานะแพทยเวชปฏบตท วไป
73
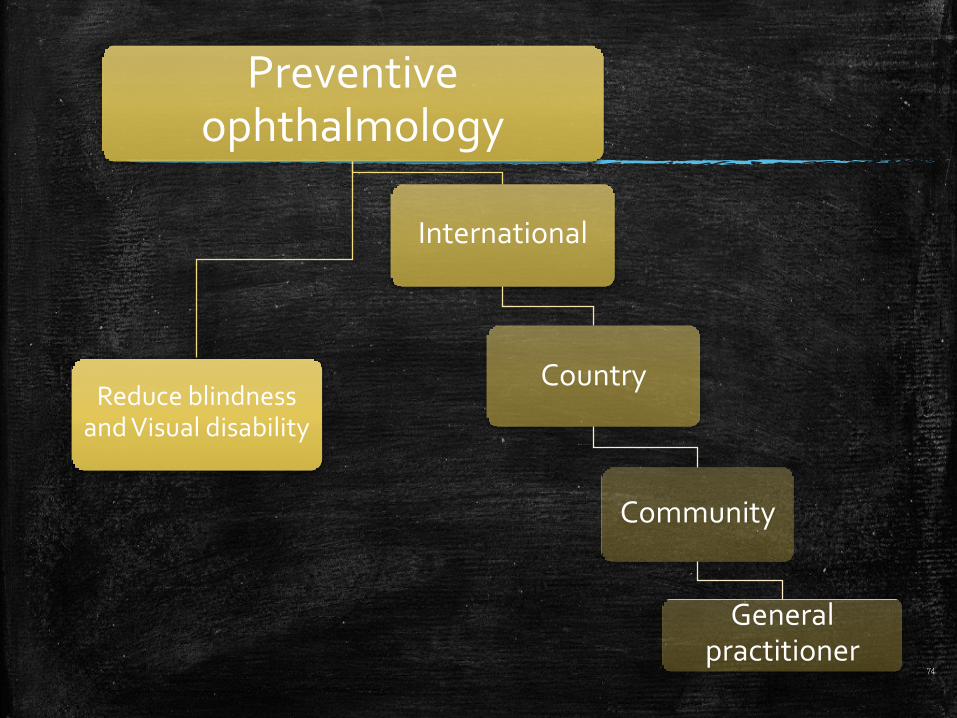
Preventive ophthalmology
Reduce blindness and Visual disability
International
Country
Community
General practitioner
74

General practitioner
Primary care unitPrimary eye care
unit
Education
Screening
Early detection
Refer
Reduce blindness and Visual disability
75