prenatal psychosocial risk assessment using event history calendars with black women
TRANSCRIPT
JOGNN R E S E A R C H
Prenatal Psychosocial Risk Assessmentusing Event History Calendarswith Black WomenMichelle L. Munro, Chin Hwa Y. Dahlem, Jody R. Lori, and Kristy K. Martyn
CorrespondenceMichelle L. Munro, MS,CNM, FNP-BC, Universityof Michigan, G120 LaneHall, Ann Arbor, MI [email protected]
Keywordspsychosocial risk
assessmentprenatal careevent history calendarsBlack pregnant women
ABSTRACT
Objective: To explore the clinical acceptability and perceptions of use of a prenatal event history calendar (EHC) for
prenatal psychosocial risk assessment in Black pregnant women.
Design: A qualitative descriptive study focused on interviews and prenatal EHCs completed by Black pregnant women.
Setting: Inner city hospital prenatal care clinic in Southeastern Michigan.
Participants: Thirty 18–35 year old pregnant Black women receiving prenatal care at the participating clinic.
Methods: Women completed the prenatal EHCs and their perceptions of its use were obtained through face to face
interviews. The constant comparative method of analysis (Glaser, 1978, 1992) revealed themes from participants’
descriptions about use of a prenatal EHC for prenatal psychosocial risk assessment.
Results: Three main themes emerged describing how the prenatal EHC enhanced communication. The prenatal EHC
provided “an opening” for disclosure, “an understanding with you,” and a way for providers to “know you, your life,
and future plans.” The participants’ completed prenatal EHCs included information regarding their pre-pregnancies,
trimester histories, and future plans. These completed prenatal EHCs showed patterns of change in life events and
behaviors that included worries, stressors, and risk behaviors. The participants perceived the prenatal EHC as an easy
to use tool that should be used to improve communication with health care providers.
Conclusions: The prenatal EHC allows the patient and provider to “start on the same page” and provides an additional
avenue for discussion of sensitive psychosocial issues with Black pregnant women. As a clinical tool, the prenatal EHC
facilitated patient-provider communication for pregnant women often marked by health disparities. The prenatal EHC is
a clinically acceptable tool to assess for psychosocial risk factors of Black women in a prenatal clinical setting.
JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x
Accepted January 2012
Michelle L. Munro, MS,CNM, FNP-BC, is adoctoral student in theSchool of Nursing,University of Michigan,Ann Arbor, MI.
(Continued)
I n 1985, the Institute of Medicine (IOM) issueda report highlighting the relationship between
the leading cause of infant mortality, low birthweight, and prenatal care utilization risk factorssuch as low socioeconomic status, low educa-tion, and minority status. Since that time expan-sive public health efforts to increase prenatal careaccess and availability have been made for low-income pregnant women and children (Alexan-der & Kotelchuck, 2001; Lu, Tache, Alexander,Kotelchuck, & Halfon, 2003). As a result, theAmerican College of Obstetricians and Gynecol-ogists (ACOG) Committee on Health Care for Un-derserved Women (ACOG, 2006) recognized theneed for more complete care in this high risk pop-ulation and advocated for comprehensive psy-chosocial screening during the prenatal period.
Prenatal care is a critical time period for healthcare providers to address the biomedical andpsychosocial issues of pregnant women. ACOG(2006) characterized psychosocial issues as non-biological or non-medical factors that may in-fluence physical or mental health. Prenatal carepresents an opportune time to establish rapportwith women to create an environment conducivefor the exchange of health information specificallyrelated to the childbearing period.
Event History CalendarsEvent history calendars (EHCs) incorporate inter-views and visualization of events using a calendarformat to facilitate the recall of past experiencesand begin conversation about clinically-relevant
The authors report no con-flict of interest or relevantfinancial relationships.
http://jognn.awhonn.org C© 2012 AWHONN, the Association of Women’s Health, Obstetric and Neonatal Nurses 1

R E S E A R C H Prenatal Psychosocial Risk Assessment with Black Women
topics (Martyn, Reifsnider, & Murray, 2006). Thisprocess provides cues for autobiographical mem-ory retrieval (Martyn & Martin, 2003). Accordingto Means and Loftus (1991), the use of event his-tory calendars provides multiple retrieval cues andimproves recall. In fact, in relation to other ap-proaches used to provide retrieval cues, the EHCis the closest in resemblance to the structure of au-tobiographical memory, contributing to its successin improving recall (Belli, 1998). Event history cal-endars were originally used for retrospective datacollection (Martyn & Belli, 2002) and assessmentof health risk transitions (Caspi et al., 1996). How-ever, more recent work has focused on the use ofEHCs in facilitating communication about risk be-havior (Martyn & Martin), risk behavior avoidance(Martyn & Hutchinson, 2001), and tailoring healthinterventions (Olds, 2006).
Chin Hwa Y. Dahlem, PhD,FNP-C, is a clinicalassistant professor in theSchool of Nursing,University of Michigan,Ann Arbor, MI.
Jody R. Lori, PhD, CNM,FACNM, is a clinicalassistant professor anddeputy director of theWorld Health OrganizationCollaborating Center,School of Nursing,University of Michigan,Ann Arbor, MI.
Kristy K. Martyn, PhD,FNP-BC, CPNP-PC, is anassociate professor andchair in the HealthPromotion and RiskReduction Programs,School of Nursing,University of Michigan,Ann Arbor, MI.
The prenatal event history calendar (prenatalEHC) was developed from data collected throughfocus groups with Black women receiving prena-tal care in a large Midwestern city (Yi, Lori, & Mar-tyn, 2008). During the development of the prena-tal EHC, Yi et al. found that Black women desiredmore discussion of psychosocial factors duringtheir prenatal care visits, which they describedas “going off the pregnancy” (p. 467). Five psy-chosocial themes were revealed from the inter-views with Black pregnant women: relationships,stress, routines, health history perceptions, andbeliefs. These themes were then used to developthe prenatal EHC (Yi et al.).
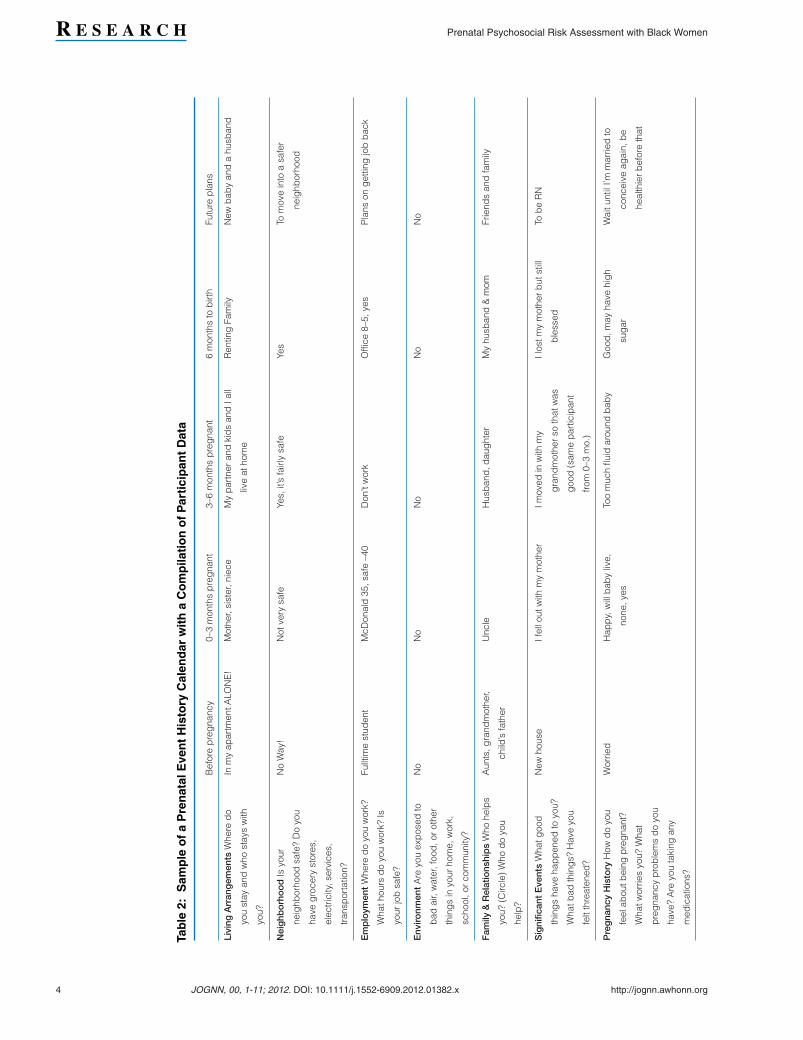
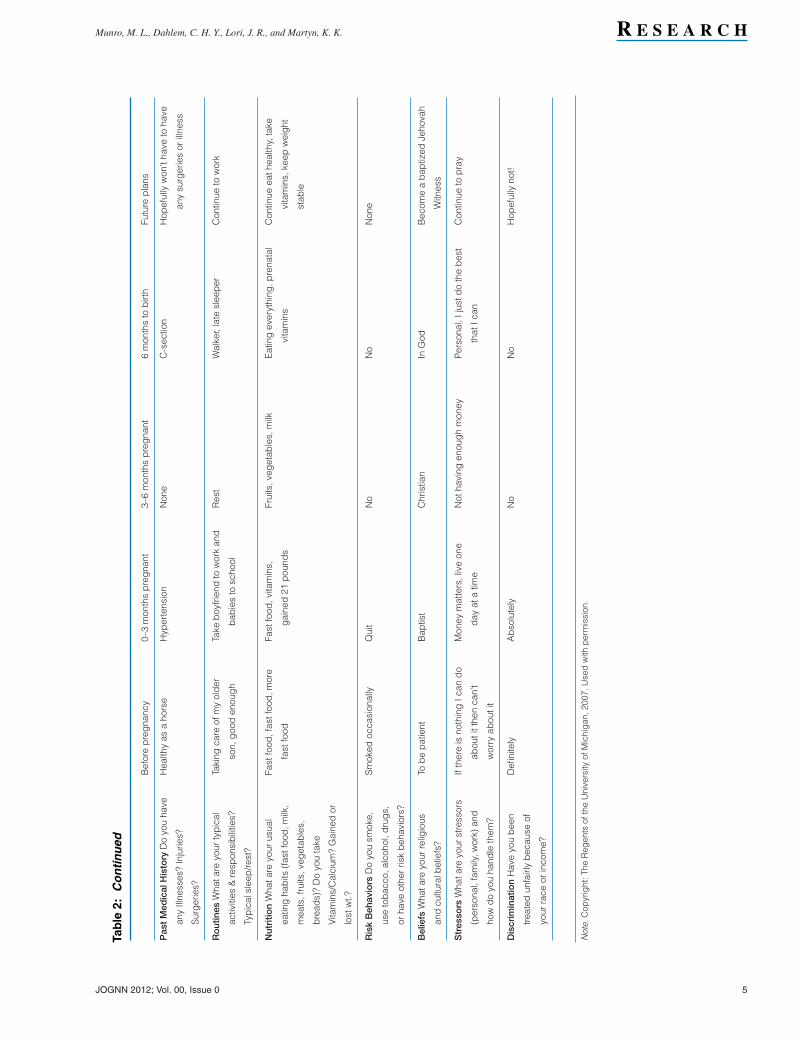
The final version of the prenatal EHC has columnheadings to depict the timeframe before preg-nancy, during each trimester of pregnancy, andafter the pregnancy (see Table 2). The row head-ings of the calendar list the information that pa-tients and providers would find important to shareand discuss during the course of prenatal care, in-cluding living arrangements, neighborhood char-acteristics, employment, relationships, significantevents, pregnancy history, past medical history,routines, nutrition, risk behaviors, beliefs, stres-sors, and discrimination. Although the prenatalEHC has not been used in clinical practice, thistype of tool was found to be clinically feasible in astudy that evaluated its ability to increase patient-provider communication about similar historieswith adolescent patients (Martyn et al., 2006).Additionally, the prenatal EHC demonstrates facevalidity because the domains captured in eachrow of the tool coincide with the components ofpsychosocial screening recommended by ACOG
(2006) and by prenatal patients in the tool devel-opment study conducted by Yi et al. (2008). There-fore, this tool has the potential to increase patient-provider communication by allowing the womanto update the calendar with significant life eventsduring each trimester of pregnancy. This descrip-tive study extends prior research to explore theclinical acceptability and perceptions of use of aprenatal EHC for psychosocial risk assessment inBlack prenatal patients.
Theoretical FrameworkThe Interaction Model of Client Health Behavior isa nursing model developed by Cox (1982) as away to describe a process of care in which self-care is seen as a paramount determinant of a pa-tient’s health and specifically addresses patient-initiated professional contact. The underlyingassumption inherent in the model involves the pa-tient’s control to make decisions regarding theirhealth care. The constructs within the model sup-porting these assumptions are the elements of pa-tient singularity, patient-professional interaction,and health outcomes (Cox). Patient singularity en-compasses the background variables, motivation,cognitive appraisal, and affective responses of theindividual (Cox). This model was used as a frame-work for development of the prenatal EHC and alsoprovides a basis from which to explore its use inthe clinical setting. Thus, when the assumptions ofthis model are applied to a prenatal care patient, itcan be used to assess patient-provider communi-cation during a routine prenatal visit, representingthe elements of the patient-professional interaction(Cox). Furthermore, the prenatal EHC as a clinicaltool can be useful in describing the singularity ofthe patient.
MethodsA descriptive qualitative design was used to ex-plore the clinical acceptability of using the prenatalEHC in routine prenatal care visits and the percep-tions of its use among a population of pregnantBlack women in a large Midwestern city. Qualita-tive data were collected using two methods. First,participants completed the prenatal EHC. Sec-ond, brief face to face interviews were conductedwith the participants after completion of the pre-natal EHC to inquire about their perceptions of theuse of the calendar for prenatal history-taking andsatisfaction. Institutional review board approvalwas obtained from the University of Michigan andthe prenatal clinic site where data were collected.
2 JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x http://jognn.awhonn.org
Munro, M. L., Dahlem, C. H. Y., Lori, J. R., and Martyn, K. K. R E S E A R C H
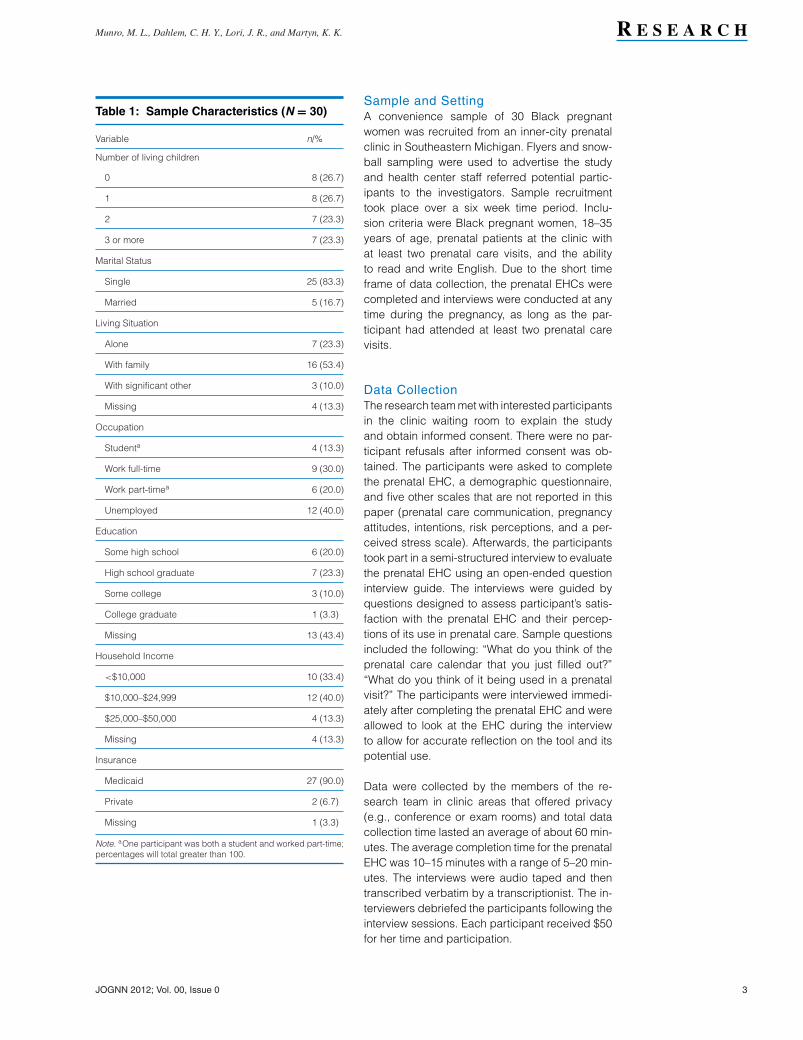
Table 1: Sample Characteristics (N = 30)
Variable n/%
Number of living children
0 8 (26.7)
1 8 (26.7)
2 7 (23.3)
3 or more 7 (23.3)
Marital Status
Single 25 (83.3)
Married 5 (16.7)
Living Situation
Alone 7 (23.3)
With family 16 (53.4)
With significant other 3 (10.0)
Missing 4 (13.3)
Occupation
Studenta 4 (13.3)
Work full-time 9 (30.0)
Work part-timea 6 (20.0)
Unemployed 12 (40.0)
Education
Some high school 6 (20.0)
High school graduate 7 (23.3)
Some college 3 (10.0)
College graduate 1 (3.3)
Missing 13 (43.4)
Household Income
<$10,000 10 (33.4)
$10,000–$24,999 12 (40.0)
$25,000–$50,000 4 (13.3)
Missing 4 (13.3)
Insurance
Medicaid 27 (90.0)
Private 2 (6.7)
Missing 1 (3.3)
Note. aOne participant was both a student and worked part-time;percentages will total greater than 100.
Sample and SettingA convenience sample of 30 Black pregnantwomen was recruited from an inner-city prenatalclinic in Southeastern Michigan. Flyers and snow-ball sampling were used to advertise the studyand health center staff referred potential partic-ipants to the investigators. Sample recruitmenttook place over a six week time period. Inclu-sion criteria were Black pregnant women, 18–35years of age, prenatal patients at the clinic withat least two prenatal care visits, and the abilityto read and write English. Due to the short timeframe of data collection, the prenatal EHCs werecompleted and interviews were conducted at anytime during the pregnancy, as long as the par-ticipant had attended at least two prenatal carevisits.
Data CollectionThe research team met with interested participantsin the clinic waiting room to explain the studyand obtain informed consent. There were no par-ticipant refusals after informed consent was ob-tained. The participants were asked to completethe prenatal EHC, a demographic questionnaire,and five other scales that are not reported in thispaper (prenatal care communication, pregnancyattitudes, intentions, risk perceptions, and a per-ceived stress scale). Afterwards, the participantstook part in a semi-structured interview to evaluatethe prenatal EHC using an open-ended questioninterview guide. The interviews were guided byquestions designed to assess participant’s satis-faction with the prenatal EHC and their percep-tions of its use in prenatal care. Sample questionsincluded the following: “What do you think of theprenatal care calendar that you just filled out?”“What do you think of it being used in a prenatalvisit?” The participants were interviewed immedi-ately after completing the prenatal EHC and wereallowed to look at the EHC during the interviewto allow for accurate reflection on the tool and itspotential use.
Data were collected by the members of the re-search team in clinic areas that offered privacy(e.g., conference or exam rooms) and total datacollection time lasted an average of about 60 min-utes. The average completion time for the prenatalEHC was 10–15 minutes with a range of 5–20 min-utes. The interviews were audio taped and thentranscribed verbatim by a transcriptionist. The in-terviewers debriefed the participants following theinterview sessions. Each participant received $50for her time and participation.
JOGNN 2012; Vol. 00, Issue 0 3
R E S E A R C H Prenatal Psychosocial Risk Assessment with Black Women
Tab
le2:
Sam
ple
of
aP
ren
atal
Eve
nt
His
tory
Cal
end
arw
ith
aC
om
pila
tio
no
fP
arti
cip
ant
Dat
a
Bef
ore
pre
gna
ncy
0–3
mon
ths
pre
gna
nt3–
6m
onth
sp
reg
nant
6m
onth
sto
birt
hFu
ture
pla
ns
Livi
ngA
rran
gem
ents
Whe
red
o
you
stay
and
who
stay
sw
ith
you?
Inm
yap
artm
entA
LON
E!
Mot
her,
sist
er,n
iece
My
par
tner
and
kid
san
dIa
ll
live
atho
me
Ren
ting
Fam
ilyN
ewb
aby
and
ahu
sban
d
Nei
ghb
orh
oo
dIs
your
neig
hbor
hood
safe
?D
oyo
u
have
gro
cery
stor
es,
elec
tric
ity,s
ervi
ces,
tran
spor
tatio
n?
No
Way
!N
otve
rysa
feYe
s,it’
sfa
irly
safe
Yes
Tom
ove
into
asa
fer
neig
hbor
hood
Em
plo
ymen
tW
here
do
you
wor
k?
Wha
thou
rsd
oyo
uw
ork?
Is
your
job
safe
?
Fullt
ime
stud
ent
McD
onal
d35
,saf
e–4
0D
on’t
wor
kO
ffice
8–5,
yes
Pla
nson
get
ting
job
bac
k
Env
ironm
ent
Are
you
exp
osed
to
bad
air,
wat
er,f
ood
,or
othe
r
thin
gs
inyo
urho
me,
wor
k,
scho
ol,o
rco
mm
unity
?
No
No
No
No
No
Fam
ily&
Rel
atio
nshi
ps
Who
help
s
you?
(Circ
le)
Who
do
you
help
?
Aun
ts,g
rand
mot
her,
child
’sfa
ther
Unc
leH
usb
and
,dau
ght
erM
yhu
sban
d&
mom
Frie
nds
and
fam
ily
Sig
nific
ant
Eve
nts
Wha
tgoo
d
thin
gs
have
hap
pen
edto
you?
Wha
tbad
thin
gs?
Hav
eyo
u
felt
thre
aten
ed?
New
hous
eIf
ello
utw
ithm
ym
othe
rIm
oved
inw
ithm
y
gra
ndm
othe
rso
that
was
goo
d(s
ame
par
ticip
ant
from
0–3
mo.
)
Ilos
tmy
mot
her
but
still
ble
ssed
Tob
eR
N
Pre
gna
ncy
His
tory
How
do
you
feel
abou
tbei
ngp
reg
nant
?
Wha
twor
ries
you?
Wha
t
pre
gna
ncy
pro
ble
ms
do
you
have
?A
reyo
uta
king
any
med
icat
ions
?
Wor
ried
Hap
py,
will
bab
yliv
e,
none
,yes
Too
muc
hflu
idar
ound
bab
yG
ood
,may
have
hig
h
sug
ar
Wai
tunt
ilI’m
mar
ried
to
conc
eive
agai
n,b
e
heal
thie
rb
efor
eth
at
4 JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x http://jognn.awhonn.org
Munro, M. L., Dahlem, C. H. Y., Lori, J. R., and Martyn, K. K. R E S E A R C H
Tab
le2:
Co
nti
nued
Bef
ore
pre
gna
ncy
0–3
mon
ths
pre
gna
nt3–
6m
onth
sp
reg
nant
6m
onth
sto
birt
hFu
ture
pla
ns
Pas
tM
edic
alH
isto
ryD
oyo
uha
ve
any
Illne
sses
?In
jurie
s?
Sur
ger
ies?
Hea
lthy
asa
hors
eH
yper
tens
ion
Non
eC
-sec
tion
Hop
eful
lyw
on’t
have
toha
ve
any
surg
erie
sor
illne
ss
Ro
utin
esW
hata
reyo
urty
pic
al
activ
ities
&re
spon
sib
ilitie
s?
Typ
ical
slee
p/re
st?
Taki
ngca
reof
my
old
er
son,
goo
den
oug
h
Take
boy
frie
ndto
wor
kan
d
bab
ies
tosc
hool
Res
tW
alke
r,la
tesl
eep
erC
ontin
ueto
wor
k
Nut
ritio
nW
hata
reyo
urus
ual
eatin
gha
bits
(fas
tfoo
d,m
ilk,
mea
ts,f
ruits
,veg
etab
les,
bre
ads)
?D
oyo
uta
ke
Vita
min
s/C
alci
um?
Gai
ned
or
lost
wt.?
Fast
food
,fas
tfoo
d,m
ore
fast
food
Fast
food
,vita
min
s,
gai
ned
21p
ound
s
Frui
ts,v
eget
able
s,m
ilkE
atin
gev
eryt
hing
,pre
nata
l
vita
min
s
Con
tinue
eath
ealth
y,ta
ke
vita
min
s,ke
epw
eig
ht
stab
le
Ris
kB
ehav
iors
Do
you
smok
e,
use
tob
acco
,alc
ohol
,dru
gs,
orha
veot
her
risk
beh
avio
rs?
Sm
oked
occa
sion
ally
Qui
tN
oN
oN
one
Bel
iefs
Wha
tare
your
relig
ious
and
cultu
ralb
elie
fs?
Tob
ep
atie
ntB
aptis
tC
hris
tian
InG
odB
ecom
ea
bap
tized
Jeho
vah
Witn
ess
Str
esso
rsW
hata
reyo
urst
ress
ors
(per
sona
l,fa
mily
,wor
k)an
d
how
do
you
hand
leth
em?
Ifth
ere
isno
thin
gIc
and
o
abou
titt
hen
can’
t
wor
ryab
outi
t
Mon
eym
atte
rs,l
ive
one
day
ata
time
Not
havi
ngen
oug
hm
oney
Per
sona
l,Ij
ustd
oth
eb
est
that
Ican
Con
tinue
top
ray
Dis
crim
inat
ion
Hav
eyo
ub
een
treat
edun
fairl
yb
ecau
seof
your
race
orin
com
e?
Defi
nite
lyA
bso
lute
lyN
oN
oH
opef
ully
not!
Not
e.C
opyr
ight
:The
Reg
ents
ofth
eU
nive
rsity
ofM
ichi
gan
,200
7.U
sed
with
per
mis
sion
.
JOGNN 2012; Vol. 00, Issue 0 5

R E S E A R C H Prenatal Psychosocial Risk Assessment with Black Women
Women reported that prenatal event history calendars in theclinical setting were easy to use and should be used to improve
communication with providers.
Data AnalysisData were analyzed using descriptive statisti-cal and qualitative analyses. Simple descriptivestatistics were analyzed using Statistical Packagefor the Social Sciences (SPSS version 17.0) toassess participant demographic characteristics.Quantitative data were entered and then doublechecked for accuracy. Qualitative data analysiswas undertaken using the constant comparativemethod of analysis described by Glaser (1978,1992) and content analysis to gather a largerbreadth of information on sample characteristicsand risk behaviors. Qualitative data analysis wasguided by the research question, “What do partic-ipants think about using the prenatal event historycalendar during their prenatal visits?”
The constant comparative method of analysis out-lined by Glaser (1978, 1992) was employed bythe team of authors to identify core themes. Thistechnique of data analysis first involves readingthrough the data to procure general impressionsof the data. Next, data were meticulously reviewedline by line to identify general ideas. During thisportion of the analysis, coding of the data be-gan by taking notes and memos on significantpoints and ideas from the transcribed interviews.These notes were then reviewed and categorizedwith the use of the memos until data saturationoccurred. Several core themes were repeatedlyidentified including topics about the use of theprenatal EHC for prenatal care assessment andfor its ability to enhance communication that isunderstandable/reasonable, important, personal,and comprehensive.
The idea of enhanced communication includedsuch sub-topics as reflective, provided insightfor the doctor, and presented further topics fordiscussion. Each theme was then reviewed un-til core themes were recognized. The first authorcompleted the initial steps of analysis indepen-dently. The core themes that were initially identi-fied were then reviewed again by all authors todistinguish commonalities in themes across theinterviews. Consensus on study themes by all au-thors was achieved before final compilation intothe main themes that reflected the participants’views of the prenatal EHC for prenatal care use.Finally, the data were compiled into three main
themes describing enhanced communication as itrelated to the research question. The use of an au-dit trail composed of methodological and analyti-cal documentation (Sandelowski & Barroso, 2003)and validation with colleagues contributed to va-lidity. Additionally, Burns’ (1989) four standardsfor methodological congruence were achieved in-cluding rigor in documentation, ethical rigor, pro-cedural rigor, and auditability.
ResultsDemographics of Study ParticipantsThe participants ranged in age from 18–34 yearsold and were mostly unemployed with incomesless than $25,000–50,000. The majority of the sam-ple was in their 20 s, single, lived with family, andreceived Medicaid. More complete demographiccharacteristics of the sample are available inTable 1.
Prenatal EHCs: Easy to Use and Shouldbe UsedThe women in this study reported the prenatalEHCs in the clinical setting were easy to use andshould be used to improve communication withproviders. The participants described the prena-tal EHC as a reasonable and understandable toolfrom which to gain their psychosocial history. Theyfound the calendar was clear, comprehensible,and relatively simple to complete. As one par-ticipant simply stated, “It was understandable. Itseemed straight for me. I like it.” Another womanechoed the ease of using the calendar, “I thoughtit [the prenatal EHC] was pretty simple.”
Participants were able to complete the prenatalEHC without difficulty and the majority of par-ticipants reported that they enjoyed completingthe calendar. This was expressed by one partic-ipant, “Everything seemed pretty straightforwardto me on this one.” The simple terminology andclear instructions, which are at a Flesch-Kincaidgrade level of 4.4 indicating a fourth grade read-ing level, allowed the participants to use the cal-endar with ease (Kincaid, Fishburne, Robers, &Chissom, 1975).
Participants stated the prenatal EHC is neededand should be used for prenatal psychosocial as-sessment and to improve patient-provider com-munication. One woman expressed that the EHC“would help because we pretty much don’t haveno communication.” Another woman stated, “Ihope this whole thing will continue so peoplecan talk to their doctors and be more aware of
6 JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x http://jognn.awhonn.org

Munro, M. L., Dahlem, C. H. Y., Lori, J. R., and Martyn, K. K. R E S E A R C H
what’s going on.” Others believed the prenatalEHC would provide an opportunity to address im-portant history with their provider. For instance,after looking at her completed prenatal EHC oneparticipant reported, “I ain’t never asked, so Iwas like, that’s something I think I am gonna askhim when I come back.” While another partici-pant expressed that reviewing the calendar withthe provider, “would help because some peopledon’t know how to actually say what they want toknow.”
Prenatal EHC: Communication ThemesThree main themes emerged related to how theprenatal EHC enhanced communication by pro-viding “an opening” for disclosure, “an under-standing with you,” and a way for providers to“know you, your life, and future plans.”
“An opening” for disclosure. The prenatal EHCwas viewed as a helpful way to begin communi-cation. One participant explained:
It would be an opening. Sometimes, that isvery much what a woman wants, a doctorto ask her because it could be things inthe past, complications that she had witha pregnancy that they might not be awareof. Because a lot of women are coming in tothe clinic, and they want you to ask personalquestions like that just to better educate thedoctor about their past pregnancies.
The participants described the prenatal EHC asa method to improve patient-provider communi-cation in prenatal care. The calendar promotedenhanced communication by providing a visiblerecord that allowed for thoughtful reflection andpersonal awareness. These sentiments are re-flected by one woman:
I think that’s good because a lot of peopledon’t like to talk. And they can put it on pa-per and then they can see it from the paperand then ask the questions from the paper.Then maybe they’ll relate more easily.
Additionally, the calendar opened up the channelsof communication with the health care providerby providing insight into the life circumstancesof the patient and presenting further topics fordiscussion.
“An understanding with you.” The participantsperceived the prenatal EHC could increase the
The calendar enhanced communication by providing a visiblerecord that allowed for thoughtful reflection and personal
awareness.
provider’s awareness of their unique backgroundsituation and facilitate mutual communication; cre-ating a sense of unity between the provider and thepatient. This could potentially assist providers tobetter understand their patients and in turn, elicita more caring patient-centered approach wheninteracting with the patient. As one woman ex-plained, “I feel that’s very important because forone, you have to feel comfortable with whoever isexamining you. You have to have that open com-munication with them so they have an understand-ing with you . . . ”
The calendar facilitated improved communicationby providing insight for the provider and visuallydisplaying topics to further enhance the patient-provider discussion. The prenatal EHC was seenas an important tool to accommodate the prenatalvisit because of its ability to open communicationbetween the patient and provider and due to its ca-pacity to create a shared understanding betweenthe patient and provider. The participants consid-ered their lives and history an integral componentof their prenatal visit when they were asked to com-plete the calendar prior to seeing their provider.
A way for providers to “know you, your life, andfuture plans.” The ability of the prenatal EHC toconvey the intricate delicacies of the participants’lives was seen as a positive and personal attributeof the prenatal EHC. The participants wanted toshare the personal details of their lives with theirhealth care providers. The women expressed thesentiment that the calendar allowed their providerto know them better as a whole person includingtheir life and history outside the clinic. One womanclearly described the personal value of the prena-tal EHC, “The doctor gets to know you before youstart the visit.” Another found that sharing personaldetails could be helpful, “I think it would be goodfor us, because she would be able to look at that,and you know, learn a lot about my history, what’sbeen going on in my life.”
The prenatal EHC asks women to share personallife events. The participants valued this level ofdetail for its ability to improve their prenatal vis-its and their relationships with their health careproviders. Some ambivalence, but overall appre-ciation of the calendar was noted by one woman
JOGNN 2012; Vol. 00, Issue 0 7

R E S E A R C H Prenatal Psychosocial Risk Assessment with Black Women
The nature of the calendar allows women to relay pertinenthealth information as well as personal life circumstances that
may influence their health and prenatal care.
when she stated, “It was kinda like personal, butit was worth asking the questions because over-all it will better educate others about women andprenatal care.” Additionally, the format of the cal-endar allowed women to share as much or as lit-tle as they desired at that time. This was evidentin the varying level of detail between calendars.Some women completed each box while othersused one word or an arrow to indicate things werethe same in that particular life domain.
The participants reported that they liked the levelof detail attained in the calendar. They expressedappreciation that they were asked about their liv-ing situations and stressors as well as traditionalprenatal questions such as medication and nutri-tion. The nature of the calendar allowed the womento relay pertinent health information as well aspersonal life circumstances that may affect theirhealth and prenatal care. One participant shared,“I think it’s [calendar] good. The way you all haveit, so you’re trying to have more details, so the wayyou did it, it’s good to me.”
Another participant found the comprehensive na-ture of the calendar allowed her to reflect back onher past and present pregnancies, “ . . . keeping agood plan of your pregnancy, so you have anotherbaby or you’re having problems, you know whatyou went through with your other kids.” The par-ticipants also found the comprehensive nature ofthe calendars captured the important aspects oftheir lives and pregnancy; information they wantedtheir health care providers to be aware of.
In addition, the prenatal EHC presented an op-portunity for the women to discuss their pre-pregnancy history and future plans with providers.The women noted prenatal care often focuses onlyon the pregnancy; but felt it is also important totalk about their personal history before they werepregnant and their future plans and needs. Oneparticipant reflected, “It [the calendar] would givethe doctor more of an insight about my history asfar as health care, and what I’ve been through be-fore my pregnancy, and what I’m going throughnow, and my future plans.”
In summary, the participants viewed the prenatalEHC as a valuable tool to improve the prenatal
care visit and emphasized the important aspectsof the women’s past, present, and future to helpproviders understand their personal life circum-stances.
Prenatal EHC DataThe participants’ prenatal EHC included pre-pregnancy and trimester history and future plans.The prenatal EHCs showed patterns of changein life events and behaviors, including worries,stressors, and risk behaviors. Data on the prena-tal EHC also highlighted participants’ health con-cerns, significant life events, and future goals. Forinstance, 20% of participants in this study con-sumed a fast food diet. This presented healthconcerns to them and an excellent opportunity foreducation from the health care provider. Addition-ally, 13.3% of the sample had pre-pregnancy riskbehaviors like smoking, regular alcohol consump-tion, and drug use that warranted discussion andeducation during the pregnancy.
The prenatal EHCs identified 40% of the samplewas currently unemployed or not working, 10%faced discrimination, and 10% lived in an unsafeneighborhood. This data from the prenatal EHCprovides guidance to the health care provider onwhat the most pressing health care and referralissues are at the time of the visit. Finally, the pre-natal EHCs demonstrated 16.7% of participantsdesired to return to school for a professional de-gree in the future, with the majority of participantswishing to become nurses. While in the clinic set-ting, being aware of this patient goal will allow thehealth care provider to foster and educate the pa-tient to help her attain her future goals. Thus, theprenatal EHC has the ability to identify single wor-ries, stressors, and specific behaviors while alsodemonstrating patterns of change over time. Table2 is an example of a completed prenatal EHC witha compilation of data from multiple participants inorder to retain confidentiality. This illustrates howthe prenatal EHC could be used to communicatewith the patient about significant details of the pa-tient’s life over the course of the pregnancy.
The prenatal EHC offered the provider a visual rep-resentation of the patient’s life changes and signif-icant events. On one calendar the woman wrote,“I lost my mother but still blessed” during her thirdtrimester. This entry would give the provider an op-portunity to discuss significant life changes andstressors with the woman. In addition, it providesthe health care provider the insight that this pa-tient was using her spirituality to cope with this
8 JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x http://jognn.awhonn.org

Munro, M. L., Dahlem, C. H. Y., Lori, J. R., and Martyn, K. K. R E S E A R C H
difficult life change. On another calendar, a pa-tient wrote “I fell out with my mother” during thefirst trimester. This provides an example of a stres-sor and worry for this particular patient. By thesecond trimester the same participant recordedthat “I moved in with my grandmother, so thatis good.” Both examples demonstrate situationsin which the patients are losing significant sup-port systems that could affect their pregnanciesand easily may have been overlooked during rou-tine prenatal care. Thus, these examples identifiedby completing the prenatal EHC could potentiallyguide health care providers in delivering more ef-fective and patient-centered prenatal care.
Additionally, the use of prenatal EHCs enhanceddisclosure of potentially sensitive psychosocialhistories. The EHCs illustrated areas of stres-sors and risk reduction that should be addressedduring prenatal care visits. While one of the re-searchers was reviewing the prenatal EHC with aparticipant she opened up about her history:
I was honest on all the questions. Exceptfor that one that I was telling you about theidea . . . that idea of . . . I don’t smoke ortake any type of drugs, but I had smokedsome marijuana one time before with myboyfriend, but I stopped that when I gotpregnant.
The prenatal event history calendar also elicitedsmall nuances that indicated patient worries thatare important to consider in the clinical setting.Some individuals used all capitals or exclama-tion points to signify negative experiences orfuture plans for change. For instance, one par-ticipant wrote that she lived “ALONE!” In the sec-tion asking about experiences with discriminationduring her pregnancy a participant wrote, “Defi-nitely,” and about discrimination in the future shewrote “Hopefully NOT!” The healthcare providercan use these subtle cues to initiate conversationabout sensitive topics and engage the patient intheir prenatal care visit.
DiscussionFindings from this study indicate that the prenatalEHC provided “an opening” for disclosure; “an un-derstanding with you;” and a way for providers to“know you, your life, and future plans.” The use ofthis tool to enhance communication during prena-tal care is significant because prior studies haveshown that pregnant women report experiencesof poor communication with their providers during
prenatal care (Bennett, Switzer, Aguirre, Evans, &Barg, 2006; Moore, Ketner, Walsh, & Wagoner,2004; Raine, Cartwright, Richens, Mahamed, &Smith, 2010). This highlights the importance offinding methods to improve patient-provider com-munication during prenatal care. Our study hasshown that the prenatal EHC may be one poten-tially effective and efficient tool to enhance patient-provider communication.
For instance, the healthcare provider can use thecues from the prenatal EHC to initially engage thewoman in conversation about her psychosocialhistory and other important topics like discrimi-nation that are often missed during prenatal care.In this study, the prenatal EHCs completed by thewomen demonstrated patterns of change in thepersonal life events and behaviors of the preg-nant women, such as worries, stressors, and riskbehaviors. Thus, the prenatal EHC has the poten-tial to be an ideal tool to implement psychosocialscreening of all women seeking prenatal care ir-respective of race, ethnicity, education, or socioe-conomic status (ACOG, 2006).
Furthermore, the prenatal EHC records data ona trimester basis as recommended by ACOG(2006). This coincides with regular prenatal carevisits, where the prenatal EHC could be completedin the waiting room prior to the visit, and integratestopics recommended for prenatal psychologicalscreening. Our findings are consistent with otherstudies demonstrating that patients value whentheir health care providers focus on psychoso-cial issues (Bertakis, Roter, & Putnam, 1991; Han-dler, Raube, Kelly, & Giachello, 1996; Korenbrot,Wong, & Stewart, 2005). The inclusion of discus-sion about psychosocial issues can be viewed asan opening up of the communication in the visitthat has been previously demonstrated to increasepatient satisfaction with prenatal care (Handler,Rosenberg, Raube, & Lyons, 1998). The prenatalEHC provides an avenue for patients to documentpertinent psychosocial issues occurring in theirlives, especially those related to health promotionand risk reduction that allows the provider to gaina better understanding of each individual patient.
Often when providing prenatal care, the focus ison the pregnancy and the immediate postpartumperiod; however, it is also important to identify po-tential long-term needs such as nutrition, support,and shelter. The prenatal EHC includes categoriesthat provide patients and providers an opportunityto discuss future plans. Handler et al. (1998) havepreviously demonstrated that patients, specifically
JOGNN 2012; Vol. 00, Issue 0 9

R E S E A R C H Prenatal Psychosocial Risk Assessment with Black Women
those insured by Medicaid, value easy access andreferral to ancillary services. The prenatal EHCoffers the health care provider the prospect ofaddressing these additional needs before prob-lems arise. Furthermore, it facilitates identificationfor potential referrals such as social work or theWomen, Infants, and Children program (WIC) thatmay be necessary to assist the patient with attain-ing required resources.
Overall, this study established that prenatal pa-tients liked using the prenatal EHC because theyperceived it was an easy method to improve com-munication during the patient-provider interaction.The simple terminology and clear instructions ofthe prenatal EHC, which are at a fourth gradereading level, allowed the participants to use thecalendar without difficulty. Utilizing the frameworkprovided in the Interaction Model of Client HealthBehavior, the prenatal EHC is an ideal tool to iden-tify unique patient characteristics and to improvethe dynamics during the patient-provider interac-tion; ultimately, allowing for tailoring of interven-tions, enhancing communication, and increasingpatient satisfaction (Cox, 1982).
LimitationsSampling bias is a limitation to this study becauseof the use of convenience sampling; therefore,replication is warranted in a more diverse sam-ple of patients. Due to the small sample size anddescriptive nature of this study, additional test-ing for feasibility in clinical practice is needed todetermine how the prenatal EHC influences com-munication between the health care provider andthe patient. In addition, the incidence of abuse inpregnancy can range from 1–20% (Gazmararianet al., 1996). This study did not capture any re-ported cases of abuse; this is most likely not fromthe lack of abuse in the study population but fromthe lack of direct questioning about interpersonalviolence on the prenatal EHC. Thus, we believe theinclusion of a violence box asking about currentor past physical, emotional, financial, and sexualabuse may be warranted. This screening would al-low health care providers to recognize those whoneed additional ancillary services such as socialwork and identify women at risk for mental healthconsequences such as post-traumatic stressdisorder.
ConclusionLori, Yi, and Martyn (2011) noted that determi-nants of health disparities are often social and itis necessary to develop models of prenatal care
harmonious with African-American women’s livesto facilitate patient-provider interactions. African-American women seeking prenatal care desire ahealth care provider that understands the contextof their lives (Lori, Yi, & Martyn). The prenatal EHCswere seen as tools to open up communication withthe health care provider about the personal at-tributes of each patient. Thus, the prenatal EHCprovides a possible avenue for further discussionof sensitive issues within a population marked byhealth disparities and lower educational levels.The prenatal EHC facilitated patient-provider com-munication during the prenatal visit by allowing thehealth care provider and the patient to “start on thesame page.”
AcknowledgementMichelle L. Munro was supported by the Na-tional Institutes of Health and National Institute ofNursing Research, Grant 2 T32 NR007073. JodyR. Lori was supported by research grant 1 K01TW008763-01A1, Fogarty International, NationalInstitutes of Health. The content is solely the re-sponsibility of the authors and does not necessar-ily represent the official views of Fogarty Interna-tional or the National Institutes of Health.
REFERENCESAlexander, G. R., & Kotelchuck, M. (2001). Assessing the role and ef-
fectiveness of prenatal care: History, challenges, and directions
for future research. Public Health Reports, 116, 306–316.
American College of Obstetricians and Gynecologists Committee on
Health Care for Undeserved Women. (2006). ACOG commit-
tee opinion No. 343: Psychosocial risk factors: Perinatal screen-
ing and intervention. Obstetrics and Gynecology, 108(2), 469–
477.
Belli, R. F. (1998). The structure of autobiographical memory and
the event history calendar: Potential improvements in the qual-
ity of retrospective reports in surveys. Memory, 6(4), 383–406.
doi:10.1080/741942610
Bennett, I., Switzer, J., Aguirre, A., Evans, K., & Barg, F. (2006). Break-
ing it down: Patient-clinician communication and prenatal care
among African American women of low and higher literacy. An-
nals of Family Medicine, 4(4), 334–340.
Bertakis, K. D., Roter, D., & Putnam, S. M. (1991). The relationship of
physician medical interview style to patient satisfaction. Journal
of Family Practice, 32(2), 175–177.
Burns, N. (1989). Standards for qualitative research. Nursing Science
Quarterly, 2, 44–52. doi:10.1177/089431848900200112
Caspi, A., Moffitt, T. E., Thornton, A., Freedman, D., Amell, J. W., Har-
rington, H., . . . Silva, P. A. (1996). The life history calendar: A
research and clinical assessment method for collecting retro-
spective event-history data. International Journal of Methods in
Psychiatric Research, 6, 101–114.
Cox, C. L. (1982). An interaction model of client health behavior: The-
oretical prescription for nursing. Advances in Nursing Science,
5(1), 41–56.
Gazmararian, J. A., Lazorick, S., Spitz, A. M., Ballard, T. J., Saltzman,
L. E., & Marks, J. S. (1996). Prevalence of violence against preg-
10 JOGNN, 00, 1-11; 2012. DOI: 10.1111/j.1552-6909.2012.01382.x http://jognn.awhonn.org

Munro, M. L., Dahlem, C. H. Y., Lori, J. R., and Martyn, K. K. R E S E A R C H
nant women. The Journal of the American Medical Association,
275(24), 1915–1920. doi:10.1001/jama.1996.03530480057041
Glaser, B. G. (1978). Advances in the methodology of grounded theory:
Theoretical sensitivity. Mill Valley, CA: Sociology Press.
Glaser, B. G. (1992). Basics of grounded theory analysis. Mill Valley,
CA: Sociology Press.
Handler, A., Raube, K., Kelley, M., & Giachello, A. (1996). Women’s
satisfaction with prenatal care settings: A focus group study.
Birth, 23(1), 31–37.
Handler, A., Rosenberg, D., Raube, K., & Kelley, M. A. (1998). Health
care characteristics associated with women’s satisfaction with
prenatal care. Medical Care, 36(5), 679–694.
Institute of Medicine. (1985). Preventing low birth weight. Wash-
ington, DC: National Academy Press. Retrieved from
http://www.nap.edu/catalog/511.html
Kincaid, J. P., Fishburne, R. P., Robers, R. L., & Chissom, B. S.
(1975). Derivation of new readability formulas (Automated
Reliability Index, Fog Count and Flesch Reading Ease
Formula) for Navy enlisted personnel (Research Branch
Report 8-75). Memphis, TN: Naval Air Station. Retrieved
from http://digitalcollections.lib.ucf.edu/cdm4/document.php?
CISOROOT=%2FIST&CISOPTR=26301&REC=0&CISOBOX=Flesch-Kincaid+grade+level
Korenbrot, C. C., Wong, S. T., & Stewart, A. L. (2005). Health promotion
and psychosocial services and women’s assessments of inter-
personal prenatal care in Medicaid managed care. Maternal
and Child Health Journal, 9(2), 135–149. doi:10.1007/s10995-
005-4871-9
Lori, J., Yi, C. H., & Martyn, K. (2011). Provider characteris-
tics desired by African American women in prenatal care.
Journal of Transcultural Nursing, 22(1), 71–76. doi:10.1177/
1043659610387149
Lu, M. C., Tache, V., Alexander, G. R., Kotelchuck, M., & Halfon, N.
(2003). Preventing low birth weight: Is prenatal care the answer?
Journal of Maternal-Fetal & Neonatal Medicine, 13(6), 362–380.
Martyn, K. K., & Belli, R. F. (2002). Retrospective data collection using
event history calendars. Nursing Research, 51(4), 270–274.
Martyn, K. K., & Hutchinson, S. A. (2001). Low-income African Ameri-
can adolescents who avoid pregnancy: Tough girls who rewrite
negative scripts. Qualitative Health Research, 11, 238–256.
doi:10.1177/104973201129119073
Martyn, K. K., & Martin, R (2003). Adolescent sexual risk assess-
ment. Journal of Midwifery and Women’s Health, 8, 213–219.
doi:10.1016/S1526-9523(03)00064-3
Martyn, K. K., Reifsnider, E., & Murray, A. (2006). Improving adoles-
cent sexual risk assessment with event history calendars: A fea-
sibility study. Journal of Pediatric Health Care, 20(1), 19–26.
doi:10.1016/j.pedhc.2005.07.013
Means, B., & Loftus, E. F. (1991). When personal history repeats itself:
Decomposing memories for recurring events. Applied Cognitive
Psychology, 5(4), 297–318.
Moore, M. L., Ketner, M., Walsh, K., & Wagoner, S. (2004). Listening
to women at risk for preterm birth. Maternal and Child Health
Journal, 29(6), 391–397.
Olds, D. (2006). The nurse-family partnership: An evidence-based pre-
ventive intervention. Infant Mental Health Journal, 27(1), 5–25.
doi:10.1002/imhj.20077
Raine, R., Cartwright, M., Richens, Y., Mahamed, Z., & Smith, D. (2010).
A qualitative study of women’s experiences of communication in
antenatal care: Identifying areas for action. Maternal and Child
Health Journal, 14(4), 590–599. doi:10.1007/s10995-009-0489-7
Raine, R., Cartwright, M., Richens, Y., Mahamed, Z., & Smith, D.
(2009). A qualitative study of women’s experiences of com-
munication in antenatal care: Identifying areas for action. Jour-
nal of Maternal/Child Health, 14, 590–599. doi:10.1007/s10995-
009-0489-7.
Sandelowski, M., & Barroso, J. (2003). Writing the proposal
for a qualitative research methodology project. Qualitative
Health Research, 13, 781–820. doi:10.1177/1049732303013
006003
Yi, C. H., Lori, M., & Martyn, K. (2008). Development of prenatal event
history calendar for black women. Journal of Obstetric, Gyne-
cologic, & Neonatal Nursing, 37, 464–473. doi:10.1111/j.1552-
6909.2008.00255.x
JOGNN 2012; Vol. 00, Issue 0 11