preliminary evaluation of a new continuous intra-arterial blood gas monitoring device
TRANSCRIPT
Coovrinht 0 Actu Anaesthesiul Scund 1995 Actu AnuestheJiol Scund 1995: 39: Supplementurn 107, 67-70 Printed in Denmark - ull rights reserved Acta Anaesthesiologica
Scandinavica ISSN 0515-2720
ISBN 87-16-15173-9
Preliminary evaluation of a new continuous intra-arterial blood gas monitoring device D. PAPPERT, R. ROSSAINT, K. LEWANDOWSKI, R. KUHLEN, H. GERLACH AND K. J. FALKE Klinik fur Anaesthesiologie and operative Intensivmedizin, Universitatsklinikum Rudolf Virchow, Freie Universitat Berlin, Berlin, Germany
Continuous intra-arterial blood gas monitoring is a new technique, possibly offering therapeutic advantages through improved monitoring in patients prone to hypoxaemia, hypercapnia andor respiratory acidosis. Therefore, we studied the clinical applicability, reliability, precision and side effect of long-term continuous intra- arterial blood gas monitoring in patients suffering from severe acute respiratory distress syndrome.
In 10 patients continuous intra-aterial blood gas monitoring based on fluorescent optodes technique was performed. At 4 h intervals, arterial blood samples for in vim blood gas analyses were drawn, stored in ice, and analysed within 3 min. Evaluation of data retrieved from the continuous intra-arterial blood gas monitoring and in vitro blood gas analysis was based on 596 data points using 10 catheters. Average length of insertion was 281*215 h, max. lengths of stay was 750 h. Arterial blood gas data obtained in v i vo were compared to the mean of in vivo and in vifro arterial blood gases.
Inter-catheter bias, expressed as percent difference between continuous intra-arterial blood gas and mean in vifro blood gas analysis was 0.19*0.23% for pH, 1.1*5.2% for PaCO, and 1.6i5.7% for PaO,. No significant gas partial pressure dependent change in precision was demonstrable. There was no significant time dependent drift in sensor precision over the study period. No negative side-effects related to IABG monitoring were observed.
We conclude that long-term use of this new device is possible in patients and represents a reliable alternative to conventional in vitro arterial blood gas analysis, when continuous monitoring of blood gases andor acid-base balance is critical.
Key words; Carbon dioxide; continuous intra-arterial blood gas monitoring; oxygen; pH; precision; side effect.
Assessment of blood gas and pH in the arterial blood may be essential in the critically ill dependent on ventila- tor therapy. The current standard of intermittent in virro blood gas analysis allows only single and delayed data point analysis that may or may not reflect the actual patient status. Furthermore, this in vitro technique requires especially in patients with critical hypoxaemia due to acute respiratory distress syndrome (ARDS) fre- quent repetitive measurements causing blood loss inci- dent to obtain data and increasing the risks of nosocomial infection as well as exposure of personnel to patients’ blood.
These shortcomings resulted in the development of devices dedicated for continuous intraarterial monitoring of blood gases and pH using the fluorescent optode technique. The catheters of this device are equipped with three optodes, one for PO,, one for PCO,, and one for pH. At the indwelling tip of the sensors, fluorescent dye systems are immobilized. Since the fluorescent nature of these dyes will be modified by changing PO,-, PC0,-, and pH-values, the changes in fluorescence by exciting
these dyes with light of specific wavelengths can be detected, processed and displayed as patient blood gas values (1-3).
This continuous intra-arterial blood gas monitor tech- nique possibly offers therapeutic advantages through improved monitoring in patients prone to hypoxaemia, hypercapnia and/or respiratory acidosis ( 1, 4, 5) . There- fore, we studied the clinical applicability, reliability, precision and side effect of long-term continuous intra- arterial blood gas monitoring in patients suffering from severe ARDS with the need for extracorporeal membrane oxygenation ECMO.
MATERIAL AND METHODS
After obtaining approval from the local ethics committee a commercially available intra-arterial blood gas sensor was introduced via a 20-gauge arterial catheter into the right radial artery and connected to a bedside monitor. A proprietary computerized data collection system was used
@ A c t a Anaesthesiologica Scandinavica 39 (1995)
68 D. PAPPERT ET AL.
to collect and record the continuous intra-arterial blood gas results from the monitor. There was no time limit for the use of the catheter and no repeat calibrations were performed. This continuous intra-arterial blood gas moni- toring has the fluorescent optodes located at the tip of the sensor which resides in the artery (PB-FOxS IABG Sensor, Puritan-Bennett, USA). At 4 h intervals, arterial blood samples for in vitro blood gas analyses (ABG) were drawn, stored in ice, and analysed within 3 min (ABLm300, Radiometer Medical N S , Denmark). Qual- ity checks and calibration of the in vitro analyser were performed on a daily basis as part of legal requirement for medical devices. Evaluation of data retrieved from the continuous intra-arterial blood gas monitor and in vitro arterial blood gases was based on 596 data points using 10 catheters.
During the study all patients were ventilated in the pres- sure controlled mode with positive end-expiratory pres- sure. The fraction of inspiratory oxygen was adjusted in order to achieve a minimal PaO, of 60 mmHg. Once a day, pulmonary gas exchange was evaluated during venti- lation with a fraction of inspiratory oxygen of 1.0. All patients were sedated with midazolam and fentanyl, in some cases for a short period of time pancuronium bro- mide was given to achieve paralysis. Positioning changes including prone position were performed routinely.
Statistical methods Accuracy and precision for the continuous intra-arterial blood gas monitoring system were determined by com- paring the results obtained from standard in vitro blood gas measurements to the value displayed by the new device. Inter-sensor bias for the continuous intra-arterial blood gas monitoring system was determined as the mean difference between the continuous intra-arterial blood gas monitor data and the in vitro blood gas data. Due the wide range of measurements the data were normalized to a percentage of the average of the in vivo and in vitro values. The limits of agreement between the continuous intra-arterial blood gas monitor data and the in vitro blood gas data were assessed by the method described by Bland and Altman. Statistical significance was assumed if p was less than 0.05.
RESULTS
Average length of insertion was 281k215 h, maximum lengths of stay was 750 h. PaO, values ranged from 50 to 595 mmHg, PaCO, from 26 to 102 d g , and pH from 7.24 to 7.67 respectively. Inter-catheter bias i standard deviation (SD), expressed as inter-catheter pre- cision and calculated as percent difference between con-
a.
- 1.0 1 .:
-0'5 -1 .o 1 I , 0 120 240 360 480 800 720 840
time [hrs]
b.
. . . . . . . ......... . . . . . . . man + 2 S.D. _---A___ - . . _ _ 5 ....... .......... _-- .....-- mean
mean - 2 S.D . . -0.5 . . -1.0 1
I 8 I 1 I I
7.2 7.3 7.4 7.5 7.0 7.7 w n PH in ulr~, in viva
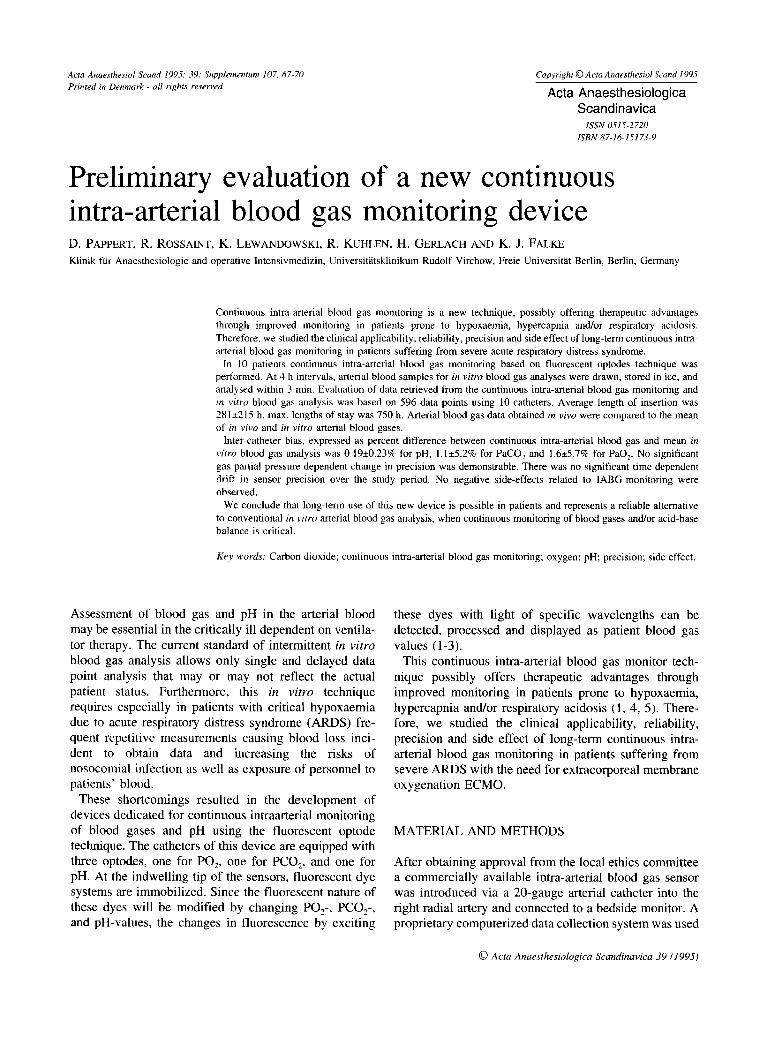
Fig. 1 . Scattergraph of normalized pH bias plotted against a) insertion time of the catheter (regression equation (r): y=x . 7.73-5+0.18, r2=2.66-') and b) plotted against mean of pH in v i m and pH in vivo (r: y=x. 1.28-9.35, ?=0.15).
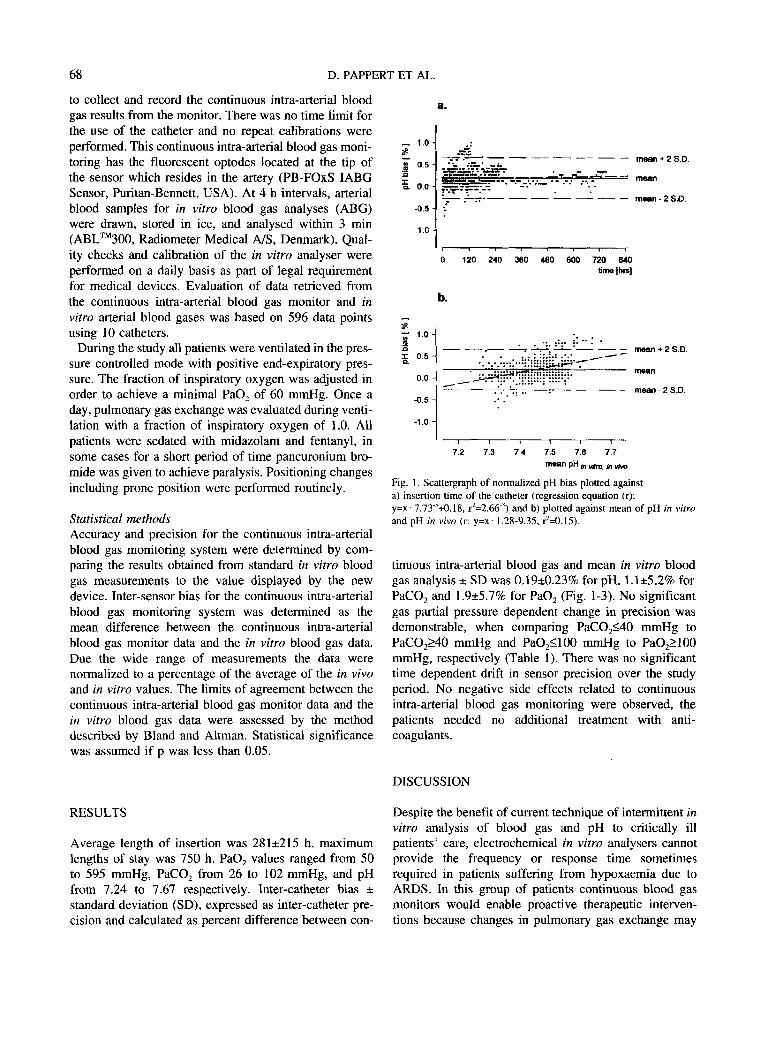
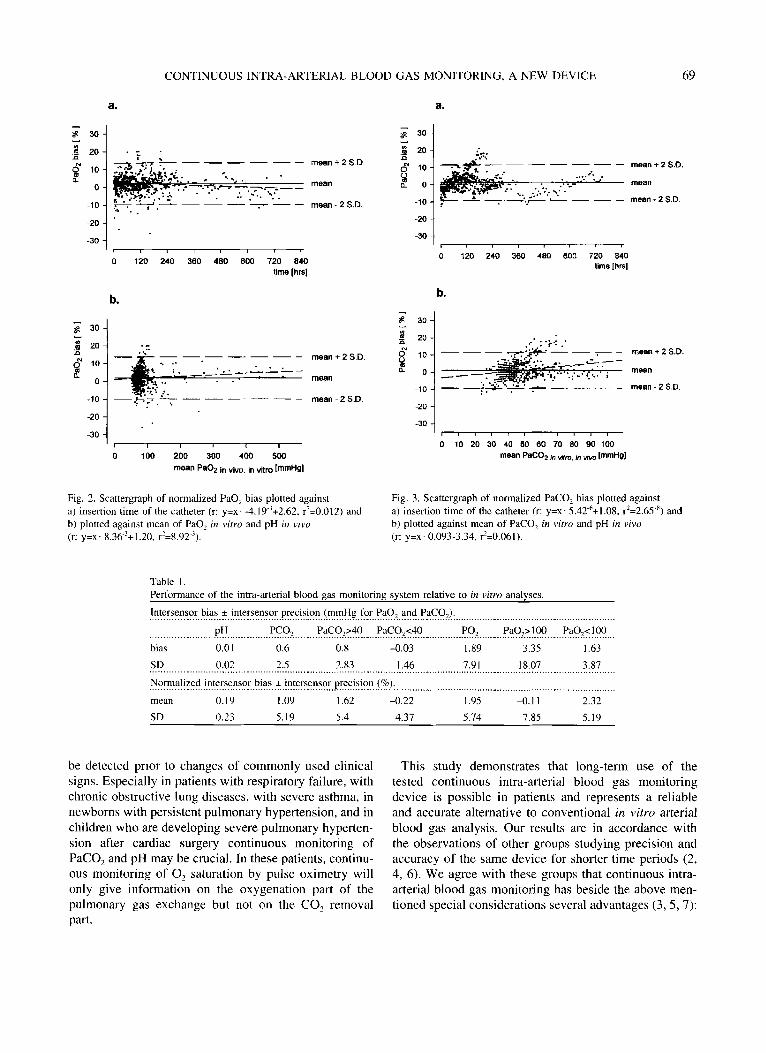
tinuous intra-arterial blood gas and mean in vitro blood gas analysis f SD was 0.19i0.23% for pH, 1.1*5.2% for PaCO, and 1.9*5.7% for PaO, (Fig. 1-3). No significant gas partial pressure dependent change in precision was demonstrable, when comparing PaC0,140 mmHg to PaC0,240 mmHg and Pa0,1100 mmHg to Pa0,2100 mmHg, respectively (Table 1). There was no significant time dependent drift in sensor precision over the study period. No negative side effects related to continuous intra-arterial blood gas monitoring were observed, the patients needed no additional treatment with anti- coagulants.
DISCUSSION
Despite the benefit of current technique of intermittent in vitro analysis of blood gas and pH to critically ill patients' care, electrochemical in vitro analysers cannot provide the frequency or response time sometimes required in patients suffering from hypoxaemia due to ARDS. In this group of patients continuous blood gas monitors would enable proactive therapeutic interven- tions because changes in pulmonary gas exchange may
CONTINUOUS INTRA-ARTERIAL BLOOD GAS MONITORING, A NEW DEVICE 69
30 I
t 20 a
g 10 a
0
-10
-20
-30
a.
. . .. mean + 2 S.D
mean
mean - 2 S.D.
8 .
I 1
0 120 240 360 480 600 720 840 time [hn]
.- mean + 2s D
mean
mean - 2 S.D.
- -- - - - - 0
n
Fig. 2. Scattergraph of normalized PaO, bias plotted against a) insertion time o f the catheter (r: y=x- -4.19-'+2.62, r2=0.012) and b) plotted against mean of PaO, in vitro and pH in vivo (r: y=x' 8.36-'+1.20, r '4.92 '),
a.
I 301
30
0 120 240 360 480 600 720 840 time [hrs]
-20 1 , , , , , , , ,
b.
mean + 2 S.D.
mean
- - mean - 2 S.D.
-30
o 10 20 30 40 50 eo 70 80 90 100 mean PaCO, in m, in - ImmHg]
-201, , , I , , , , , , I
Fig. 3. Scattergraph of normalized PaCOz bias plotted against a) insertion time of the catheter (r: y=x- 5.42-6+1.08, rZ=2.65.') and b) plotted against mean of PaC02 in vitro and pH in vivo (r: y=x. 0.093-3.34, r2=0.061).
Table 1 Performance of the intra-arterial blood gas monitoring system relative to in vitro analyses.
Intersensor bias + intersensor precision (mmHg for PaO, and PaCO,). .......................................................... ....................... PH PCO, PaCOp40 PaC0,<40 PO, PaO,> I00 PaO,< I00 ......................................................... -, .................... -. .................... -. ....................... -. ...........................................
bias 0.01 0.6 0.8 -0.03 1.89 3.35 1.63 SD 0.02 2.5 2.83 I .46 7.91 18.07 3.87
Normalized intersensor bias f intersensor precision (%).
mean 0.19 I .09 1.62 -0.22 1.95 -0.1 1 2.32 SD 0.23 5.19 5.4 4.37 5.74 7.85 5.19
.......................................................................................................
...........................................................................................................................................................................
be detected prior to changes of commonly used clinical signs. Especially in patients with respiratory failure, with chronic obstructive lung diseases, with severe asthma, in newborns with persistent pulmonary hypertension, and in children who are developing severe pulmonary hyperten- sion after cardiac surgery continuous monitoring of PaCO, and pH may be crucial. In these patients, continu- ous monitoring of 0, saturation by pulse oximetry will only give information on the oxygenation part of the pulmonary gas exchange but not on the CO, removal Part.
This study demonstrates that long-term use of the tested continuous intra-arterial blood gas monitoring device is possible in patients and represents a reliable and accurate alternative to conventional in vitro arterial blood gas analysis. Our results are in accordance with the observations of other groups studying precision and accuracy of the same device for shorter time periods (2, 4, 6). We agree with these groups that continuous intra- arterial blood gas monitoring has beside the above men- tioned special considerations several advantages (3, 5,7):

70 D. PAPPERT ET AL.
1. In general, on-line monitoring allows more rapid and precise interventions with regard to changes in ventila- tor settings or other therapeutic measures like suction- ing or positioning.
2. Reliable continuous intra-arterial blood gas monitoring reduces the risks of nosocomial infection from con- taminated arterial catheters because the integrity of the arterial line system is not disturbed by obtaining blood samples.
3 . The exposure of personnel to the patients' blood is minimized.
4. Especially, in neonates and in small children less blood loss will be beneficial.
REFERENCES
1.
2.
Shapiro B A. In vivo monitoring of arterial blood gases and pH. Respir Care 1992: 37: 165-169. Haller M, Kilger E, Briegel J, Polasek J, Groh J, Peter K. Konti- nuierliche intravasale Blutgasanalyse. Anuesthesist 1994: 43: 642-647. Mahutte C K. Continuous intra-arterial blood gas monitoring. Zntensive Care Med 1994: 20: 85-86. Haller M, Kilger E, Briegel J, Forst H, Peter K. Continuous intra-arterial blood gas and pH monitoring in critically ill patients with severe respiratory failure: A prospective, criterion standard study. Crit Care Med 1994: 2 2 580-587. Pappert D, Rossaint R, Gerlach H, Falke K. Continuous moni- toring of blood gases during permissive hypercapnia in a patient with severe acute lung failure. Zntensive Cure Med 1994: 20:
3.
4.
5.
- 2 10-21 1.
Derformance of a blood gas monitor: a ProsDective, multicenter
In addition, we believe that this new technique will allow 6, Shapiro A, Mahutte K, Cane D, Gilmour J. Clinical new insights for scientists when analysing new drugs or methodswhich might influence pulmonary gas exchange. Combined with direct oxygen consumption measurement
k a l . Crit Care Med 1993: 21: 487-494: Zimmermann J L, Dellinger R P. Initial evaluation of a new intra-arterial blood gas system in humans. Crit Care Med 1993:
7.
21: 495-500. and continuous blood gas measurement in the pulmonary artery future devices may allow for continuous calcula- tion of venous admixture.
In conclusion, continuous intra-arterial blood gas moni- toring has been demonstrated to allow accurate and pre- cise measurement of blood gases over a wide range of values for more than 30 days. Therefore, we believe that this device will provide the intenshist with a new tool
Address: Dirk P'PPert* M.D. Klinik fur Anaesthesie und operative Intensivmedizin Universitltsklinikum Rudolf Virchow Freie Universitlt Berlin Augustenburger Platz 1
for clinical and scientific purposes. D-13353 Berlin, Germany
ACKNOWLEDGMENTS
We thank Puritan-Bennett for their invaluable support and M. Baum, D. Pahl and R. Simon-Balan for their technical assistance.