predicting is preventing · good oral health begins with the dental professional’s knowledge of...
TRANSCRIPT

Earn1 CE creditThis course was
written for dentists, dental hygienists,
and assistants.
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your PracticeWritten by Stacy McCauley RDH, MS
Publication date: April 2012Expiration date: March 2015
AbstractNumerous healthcare experts have agreed that dental caries in the pediatric population is one of the most serious health concerns in this country. Early prevention and intervention are the keys to ending this “silent epidemic”. The American Academy of Pediatrics along with the American Academy of Pediatric Dentistry, both support a child’s first dental visit before their first birthday. This online program will address the primary foundation of long-term oral health: early risk assessment. Participants will learn how to perform both initial and on-going risk assessments on infants and toddlers in their practices. After discussing risk, through the use of patient case studies, participants will learn how to implement new strategies in preventing oral disease. Based on risk assessment, CE attendees will then learn how to implement various therapeutic chair-side and at-home products appropriate for infant and toddler disease control. Establishing a lifetime of good oral health begins with the dental professional’s knowledge of risk assessment in order to predict prevention.
Learning Objectives:The course participants at the conclusion of the course will be able to:1. Explain the rationale for earlier intervention and preven-
tion related to childhood caries2. Implement initial and continuing risk assessment of
infants and toddlers3. Describe the risk factors for early childhood caries4. Employ oral health treatment strategies using chair-side as
well as at-home therapeutic
Author ProfileStacy McCauley, RDH, MSStacy is a graduate of Kellogg Community College with 16 years of clinical practice experience. After completing her Bachelor of Science Degree at Siena Heights College in Adrian, Michigan she relocated to Chapel Hill, North Carolina to obtain her Master of Science degree in Dental Hygiene Education. She is a former clinical assistant professor at the University of North Carolina School of Dentistry, has published research in various dental hygiene journals, and has conducted clinical research. She currently serves on the editorial review board for Modern Hygienist magazine and the Journal of Dental Hygiene, and is a member of the American Dental Hygienists’ Association and North Carolina Dental Hygienists’ Association. Stacy is the Manager of Professional Education and e-Learning for Philips Sonicare in the Carolinas.
This course has been made possible through an educational grant provided by Philips Sonicare.
Supplement to PennWell Publications This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: PennWell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 1 CE credit for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.
CE Planner Disclosure: Michelle Fox, CE Coordinator does not have a leadership or commercial interest with Orapharma, the commercial supporter, or with products or services discussed in this educational activity.
Educational Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
Registration: The cost of this CE course is $39.00 for 1 CE credit. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Go Green, Go Online to take your coursePennWell designates this activity for 1 Continuing Educational Credit

#
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
Program Overview
Numerous healthcare experts have agreed that dentalcaries in the pediatric population is one of the mostserious health concerns in this country. Early preventionand intervention are the keys to ending this “silentepidemic”. The American Academy of Pediatrics alongwith the American Academy of Pediatric Dentistry, bothsupport a child’s first dental visit before their firstbirthday. This online program will address the primaryfoundation of long-term oral health: early risk assess-ment. Participants will learn how to perform both initialand on-going risk assessments on infants and toddlers intheir practices. After discussing risk, through the use ofpatient case studies, participants will learn how to imple-ment new strategies in preventing oral disease. Based onrisk assessment, CE attendees will then learn how toimplement various therapeutic chair-side and at-homeproducts appropriate for infant and toddler diseasecontrol. Establishing a lifetime of good oral health beginswith the dental professional’s knowledge of risk assess-ment in order to predict prevention.
Effective Date: April 1, 2012 Expiration Date: March 31, 2015Format: Self Instructional - Text based Web Activity
Educational Objectives
Upon completion of this course, the clinician shouldhave a better understanding of:
n Explain the rationale for earlier intervention andprevention related to childhood caries
n Implement initial and continuing risk assessmentof infants and toddlers
n Describe the risk factors for early childhood cariesn Employ oral health treatment strategies usingchair-side as well as at-home therapeutic
Target Audience
The target audience for this course is Dentists, DentalHygienists and Dental Assistants from novice toadvanced professional.
Author Bio & Contact Information
Stacy McCauley, RDH, MS
Stacy is a graduate of Kellogg Community College with16 years of clinical practice experience. After completingher Bachelor of Science Degree at Siena Heights Collegein Adrian, Michigan she relocated to Chapel Hill, NorthCarolina to obtain her Master of Science degree in DentalHygiene Education. She is a former clinical assistantprofessor at the University of North Carolina School ofDentistry, has published research in various dentalhygiene journals, and has conducted clinical research.She currently serves on the editorial review board forModern Hygienist magazine and the Journal of DentalHygiene, and is a member of the American DentalHygienists’ Association and North Carolina DentalHygienists’ Association. Stacy is the Manager ofProfessional Education and e-Learning for PhilipsSonicare in the Carolinas.
Stacy McCauley may be reached at:[email protected]
Recognition and Credits
PennWell is an ADA CERP recognized provider.ADA CERP is a service of the American DentalAssociation to assist dental professionals in identi-fying quality providers of continuing dental education.ADA CERP does not approve or endorse individualcourses or instructors, nor does it imply acceptance ofcredit hours by boards of dentistry.
PennWell designates this activity for 1 credit hour ofcontinuing education credits.
Online Examination & CE Verification Form:
To receive credit for your participation in this course youwill be required to complete the online program exami-nation. To complete the online examination participants
1

#
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
must be registered and signed-in to ineedce.com andhave added the program to their user account (MyCEArchives). Once added to your user account, a TakeExam link will be displayed from within the MyCEArchives section of the website. Upon selection of theTake Exam link, participants are provided access to theonline examination form. Once completed andsubmitted an immediate grade report will be displayed.All participants scoring at least 70% on the examinationwill receive a Letter of Credit (CE Verification Form) veri-fying 1 CE credit. Letters of credit may be viewed andprinted immediately as well as accessed anytime in thefuture (24/7) from within the MyCE Archives userrecords page of this website.Not enough time to complete your online examina-tion? No problem, online examinations may becompleted anytime during the effective period of theprogram. Participants requiring more time to completean examination may return to this website, sign-in andcomplete the online examination.
Disclosure Declaration
Presenter Disclosure: Stacy McCauley has no relevant financial interests with any products or services discussed in this presentation.
Provider Disclosure: PennWell's Dental Group does nothave monetary or other special interest in any productsor services discussed or shared in this educationalactivity. CE Planner/Organizer, Michelle Fox does nothave a relevant financial interests with any products orservices discussed in this presentation.
Image Authenticity: No images in this educationalactivity have been modified or altered.
Scientific Basis: All content has been derived fromreferences listed and the author’s clinical experience.Research references are provided in the bibliographyand/or supplemental materials.
Caution: Completing a single continuing educationcourse does not provide enough information to give theparticipant enough information to give the participantthe feeling that s/he is an expert in the field related tothe course topic. It is a combination of many educa-tional courses and clinical experience that allows theparticipant to develop skills and expertise.
Cancellation/Refund Policy:
Any participant who is not 100% satisfied with thiscourse can request a full refund by contacting PennWellin writing.
Hardware and Software Requirements
To access CME-University materials users will need:n A computer with an Internet connection.n Internet Explorer 7.x or higher, Firefox 3.x or
higher, Safari 3.x or higher, or any other W3Cstandards compliant browser.
n Adobe Acrobat Reader or Apple Preveiw.n Occasionally other additional software may be
required such as Adobe Flash Player and/or anHTML5 capable browser for video or audioplayback.
2

3
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
Hello! I’m your course facilitator, StacyMcCauley. I’ve been a registered dentalhygienist for 16 years and have been a partof the Education Team and Philips Sonicarefor the past 6 years. One of the mostexciting and at the same time most chal-lenging aspects of dentistry is the evolving,continual change of science. One of thefastest growing aspects of this evolvingscience is the area of risk assessment.Dentistry, especially dental hygiene, citesprevention as one of our cornerstones ofcare. Now we’re evolving yet again tobegin using prediction as our next corner-stone of care.
Before we move into risk assessment forour pediatric dental patients, let’s discussoral health as viewed through the eyes ofthe medical community. In 2008, theAmerican Academy of Pediatrics cited oralhealth in the top three of health careconcerns related to children in the UnitedStates. The statistics, cited here by theAAP, only begin to scratch the surface onwhat’s happening in the mouths of babesall across this country. Pediatricians,seeing a lack of early dental care in infantsand toddlers, have begun to incorporatedental assessments during well baby andwell child visits. The medical community isalso starting to apply fluoride varnish on at-risk children. So, how big is this problem?
Well if you see here on the slide, oral health is number three. The AAP estimates that caries is the most commonchronic childhood disease. It’s five times as common as asthma and more common than a common cold. Theycontinue on to estimate that half of children by middle childhood and over 80% by late adolescence will have expe-rienced this chronic condition, this chronic disease known as dental caries. More school days are lost nationwidefrom dental disease than any other two diseases combined. That’s 51 million hours of school lost each year due todental related problems.

4
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
The Centers for Disease Control, the CDC,released similarly grim statistics in theirreport, Healthy People 2010. If we look atthese statistics, their assessment showsone fourth of kids by age 4 experiencingdental caries infection, half of children bysecond grade. They also looked at caries inkids ages 2-5. Historically, they looked at1988 to 1994. At that time, the incidencewas 24% of kids between 2 and 5 havingdental caries infection. That numberjumped to 28% when they looked at 1999through 2004. And if you are thinking whatI’m thinking, I really shudder to think whenthey do the next assessment where theincidence number is going to be. I think alot of us assume and are fearful that it is
going to climb even higher. Now, they also looked at disparity between Hispanic children and non-Hispanic children.What they found was, in Hispanic children ages 6-11, the incidence of dental caries infection was at 31% comparedto the non-Hispanic children, 19%. So it truly did matter, the ethnicity of the child. Hispanic children are at higherrisk for dental caries infection. They continued on to say three times more children have unmet needs for dental carethan from medical care.
When you look at the picture of this child, Iknow you have a visceral response to howhe looks. The impact of oral disease onchildren can be extremely significant anddevastating, as you can see here. Thischild has an extreme abscessed tooth,extreme infection, and you can see thefacial swelling. This photo is courtesy ofDr. Brian Williams. This is obviously a childthat didn’t have early education, early inter-vention, early prevention, or any dentaltreatment at the stage where things couldhave potentially been reversible. So whatare the impacts of oral disease on children?You can see early tooth loss can causefailure to thrive; impaired speech develop-ment due to early tooth loss. Kids withdental infection have an inability to concen-
trate due to the extreme dental pain that they experience. Now, when they can’t concentrate, you can see why theytypically have poor school performance and with dental pain many of them stay home from school due to the pain,so they have a higher absence rate. This goes back to the statistic that we talked about just a few moments agowhen I said the estimates are that 51 million hours, that’s five-one, 51 million hours of school are lost each year,specifically attributed to dental pain. Now, children with oral disease like this child also potentially have low self-

5
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
esteem, embarrassment and systemicconsequences.Let’s take a look back and look at theshifting focus of dentistry. We’re going tostart where we began and now we’re goingto walk through where dentistry is headed.We started dentistry in the treatment era.Basically what that means is we addressthe dental needs through treatment. So weextracted infected teeth or we filled a tooththat had decay. That was up until about the1970s. If you look at 1970 through about2005, we moved forward and weprogressed into yet another era ofdentistry. We not only treated dentaldisease, but dentistry began to utilizestrategic prevention strategies such as
systemic and topical fluoride, dental sealants, and bitewing radiographs just to name a few. The current era looksat not only treating dental disease, not only preventing dental disease, but to actually assess risk for future diseaseand begin to implement risk modification, even if no disease is currently evident. We are going to go back to thatpoint multiple times throughout this webinar because that’s really at the pinnacle of risk assessment. Even if adisease isn’t present today, we are going to use predictive factors that will determine how we assess, we diagnose,we treatment plan our patients.
A review through your dental journals oryour dental hygiene journals or throughother continuing education courses havestarted to see the term CAMBRA, C-A-M-B-R-A. CAMBRA stands for CariesManagement by Risk Assessment. Sohow do we begin to assess and modify riskfactors before dental disease is evendetectible? Well the answer is this: firstvisit by first birthday. In other words, estab-lishing a dental home by age 1. TheAmerican Academy of Pediatrics and theAmerican Academy of Pediatric Dentistryboth support first visit by first birthday inorder for us to assess risk early enough toprevent future disease. So how do we thenprevent disease? If we’ve assessed our risk
factor indicating future disease, we could implement things such as fluoride varnish therapy, possibly sealing theprimary teeth, significant health education with the parent caregiver, and so on. And we’ll get into that in more detailat the end of the webinar. So you can see here on this slide, there are several key points of CAMBRA. I think one ofthe most important key learning opportunities that we have is the parent caregiver education. Explaining to parentcaregivers that dental caries is an infection, it is a preventable disease, and it is also a communicable, transmissible
6
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
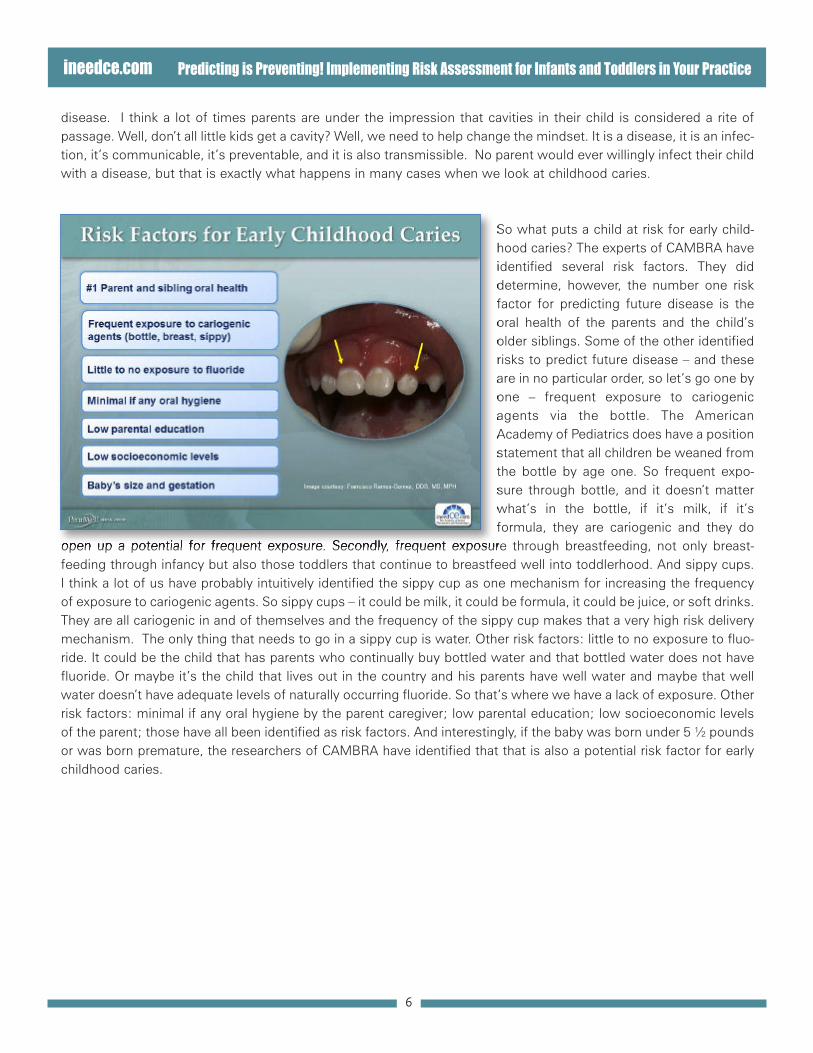
disease. I think a lot of times parents are under the impression that cavities in their child is considered a rite ofpassage. Well, don’t all little kids get a cavity? Well, we need to help change the mindset. It is a disease, it is an infec-tion, it’s communicable, it’s preventable, and it is also transmissible. No parent would ever willingly infect their childwith a disease, but that is exactly what happens in many cases when we look at childhood caries.
So what puts a child at risk for early child-hood caries? The experts of CAMBRA haveidentified several risk factors. They diddetermine, however, the number one riskfactor for predicting future disease is theoral health of the parents and the child’solder siblings. Some of the other identifiedrisks to predict future disease – and theseare in no particular order, so let’s go one byone – frequent exposure to cariogenicagents via the bottle. The AmericanAcademy of Pediatrics does have a positionstatement that all children be weaned fromthe bottle by age one. So frequent expo-sure through bottle, and it doesn’t matterwhat’s in the bottle, if it’s milk, if it’sformula, they are cariogenic and they do
open up a potential for frequent exposure. Secondly, frequent exposure through breastfeeding, not only breast-feeding through infancy but also those toddlers that continue to breastfeed well into toddlerhood. And sippy cups.I think a lot of us have probably intuitively identified the sippy cup as one mechanism for increasing the frequencyof exposure to cariogenic agents. So sippy cups – it could be milk, it could be formula, it could be juice, or soft drinks.They are all cariogenic in and of themselves and the frequency of the sippy cup makes that a very high risk deliverymechanism. The only thing that needs to go in a sippy cup is water. Other risk factors: little to no exposure to fluo-ride. It could be the child that has parents who continually buy bottled water and that bottled water does not havefluoride. Or maybe it’s the child that lives out in the country and his parents have well water and maybe that wellwater doesn’t have adequate levels of naturally occurring fluoride. So that’s where we have a lack of exposure. Otherrisk factors: minimal if any oral hygiene by the parent caregiver; low parental education; low socioeconomic levelsof the parent; those have all been identified as risk factors. And interestingly, if the baby was born under 5 ½ poundsor was born premature, the researchers of CAMBRA have identified that that is also a potential risk factor for earlychildhood caries.

7
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
CAMBRA experts commonly discuss thisstatistic: Children that are diagnosed withsevere early childhood caries, half of thosechildren will have new decay in just four totwelve months. So the CAMBRA expertsdo typically discuss this statistic quiteoften when they’re explaining risk factorsand the need to address and modify thoserisk factors. So I ask you, why the high rateof re-infection? I mean, if we are treatingthe cavity, why are we seeing such a highrate of infection? I’m going to read an inter-esting excerpt from a continuing educationcourse where Dr. Kim Kutsch gave a reallyfantastic explanation of not only assessingrisk for early childhood caries, but modi-fying risk factors. So Dr. Kutsch gives us
this nail in the tire analogy when he discusses the need for treating the underlying contributing factors for early child-hood caries, ECC, with parents. He says, “When we find a sticky occlusal pit or we see a lesion on a radiograph,essentially what we have found is the nail in the tire. Now, we have no idea how the nail got in the tire, we just knowwe are going to pull it out and we are going to patch over the hole. If we are going to get concerned about how thenail got in the tire so we can possibly prevent another one…
…we can see that the cause was this pileof nails sprinkled in our driveway. If wedon’t sweep the nails up, the likelihoodwe’ll get another nail in the tire is prettyhigh.” This is the idea of risk assessment.Some of our infants and toddlers have acouple of nails in the driveway. Some of ourinfants and toddlers have no nails in thedriveway, and others have an entiredriveway covered in nails. He continues onto say, “Treating the cavity simply meanspulling out the nail and plugging the hole.Treating the infection means figuring outwhere the nail came from and the likeli-hood that it can happen again.” This is thekey to risk assessment. Now, our job, inpart, is to of course, remove the nail in the
tire but more importantly, our job is to sweep away the risks. That’s where things such as the maintenance intervalfrequency, meaning how often we see the child back for reassessment. Things such as the application of topical fluo-ride varnishes, dental sealants, xylitol. Those may be indicated for some infants and toddlers and not others. It’s allabout assessing individual risk.

8
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
So, first visit, first birthday is now aconcept that you’re familiar with. One ofthe pieces of feedback that I get fromattendees at our live CE programs is,“Okay, now you’re telling me that I amsupposed to see infants in my office, whatam I going to do for them? I mean, how canI spend 30-45 minutes cleaning a baby’steeth?” Well, the first visit, first birthdayreally doesn’t have a whole lot to do with“cleaning their teeth,” it has an extensiveamount of time spent on the parent inter-view; getting information from mom orcaregiver on the oral health currently of theparents, because we know that the oralhealth of mom and/or dad are one of thenumber one risk factors for predicting
disease in the child. Also, we need to interview to find out about any older siblings and what their incidence of oraldisease is. A huge amount of the appointment is spent on educating the parent caregiver on strategies. How canwe help you limit the preventable carbohydrate exposure in your daughter? Giving her suggestions and ideas andalso giving her very strict guidelines on what can go in a sippy cup and what cannot. The other piece of the appoint-ment really does weigh heavily on the education of the parent caregiver on appropriate oral hygiene behaviors andrealistic expectation. A lot of parents will say, “Gosh, he just won’t let me brush,” or “He cries every time I try tobrush his teeth.” We have to give parents a very realistic expectation that it won’t probably be easy to brush herteeth if you’ve never done it before. She probably is going to fight with you during this twice daily routine. But thoseare realistic behavior expectations and we have to give her realistic oral hygiene instructions to mimic that. Lastly,one of the best things we can teach a parent caregiver is lift the lip. If mom, dad, grandparent, caregiver, if they liftthe lip on this little girl every single day, we’re going to be able to teach mom how to assess what’s normal anatomy– because we’re going to show her today what normal anatomy is supposed to look like – but we’re also going togive mom the opportunity to continually assess the anatomy. Now, I’m not going to teach mom how to diagnosedental caries. I want her to know what it looks like to have a normal tooth and what to look for if we start to seethings like early white spot lesions or demineralization. It’s amazing how many parents will say, “I’m just afraid totouch her mouth, I’m afraid to open her mouth and lift the lip because she fusses and cries.” It’s one of the best earlydetection strategies we can implement because after all, mom and dad are with her every day. We only see this littleone maybe once, twice a year.
9
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
To reinforce this concept of predictingfuture disease through risk assessment,let’s use this analogy. Here you see thislittle toddler enjoying a glorious day at thebeach. Wouldn’t you agree, you couldn’task for a nicer day?
If we could see the big picture, the weatheris perfectly calm now, but the radar showsthat this devastating hurricane is only hoursaway. I’m sure if you knew this hurricanewas going to hit in just a few hours, youwould surely warn her parents of theimpending danger. You wouldn’t sit backand say nothing just because the weatherlooks fine right now. But that’s exactly whatwe’ve done in dentistry. We have tradition-ally assessed what is present in the mouthin the here and now with no thought of theimpending storm. So if we look at riskassessment, we have to look at theimpending storm.

10
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
If two toddlers already have a history ofdental caries, then upon assessment oftheir 11 month-old sister we would alreadysee the storm coming even if everythinglooks normal today in that infant’s mouth.Therefore, predicting is preventingbecause we can employ much moreaggressive and frequent preventive proce-dures before the disease advances to thepoint where it eventually becomesdetectable clinically. I hope these conceptswe have just discussed have piqued yourinterest in integrating risk assessment, notonly for your pediatric patients but yourentire population of patients as a whole.
Based on feedback from the live continuingeducation courses the Philips SonicareEducation Team presents across the USand Canada, we continually hear time andtime again from course attendees the valueof practicing the concepts of risk assess-ment on live patients. Well, as you canimagine, live patients, those are kind of outof the question for this virtual CE course.So I have created virtual cases for us tostudy. So I’d like you to meet Madeline.Madeline is 2 ½ years old. She was born inand lives in Denver, CO. Madeline’s parentsdivorced when she was 9 months old. Shelives with her mom; she sees her dad twoweeks a year and occasionally on specialholidays. Her mother has an MBA from
UCLA and is a regional vice-president for a very high-end department store in Denver. Dad has a bachelor’s degreeand he is a sales rep for a software company. Now, Madeline’s mother has had three crowns, one root canal, threefillings, and currently has a “watch” around a crown margin. Her dad hasn’t been to the dentist in over two years. Athis last checkup his dentist diagnosed three areas needing restorative treatment. Dad always complains his gumsbleed no matter how often he brushes or flosses. Both parents have good overall health and Madeline has an in-home nanny. Madeline uses the pacifier during the day and throughout the night. The nanny brushes her teeth afterbreakfast and mom usually brushes before bed with a full strip of toothpaste on the toothbrush. Clinically, you seeno visible white spot lesions and the tissue reveals no inflammation. However, clinically, you also see Madeline’s

11
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
sister in the practice and you know clinically Madeline’s older sister – she’s 4 ½ - had had one filling and one stainlesssteel crown to date. I’d like you to take a look at Madeline as a whole. If Madeline walked into your office tomorrow andyou interviewed the caregiver or the mom and you were able to pull out all of this critical information about Madelinebefore you even looked in the mouth, now of course at the end of the clinical exam you are going to look in the mouth,but you’ve really been able to obtain a tremendous amount of information before you even look clinically.
What I’d like to do is show you what I seeare the benefits, basically what Madelinehas going for her in the positive direction,and I’d also like to share with you thingsthat I can assess as potential risk factors.You can see here the benefits which wedetermined that kids that don’t have expo-sure to fluoride are at risk, but hey, here’s abenefit! Madeline lives in a fluoridatedcommunity and has since she was born.We know that low socioeconomics of theparents and a low educational level of theparents are risk factors; here we seeMadeline does not have that as a riskfactor. Both parents have good overallhealth and clinically, everything looks finetoday. But remember the story of the
impending storm. We see that mom and dad both have a pretty extensive history of dental disease, and I wouldquestion that dad still has untreated periodontal disease and mom and dad both have a history and possibly a currentexperience with dental caries. Those are risk factors. And indeed, that’s the number one risk factor that Madelinehas going against her overall health. What do I also see as a potential as far as risks? Well I’m not sure what type ofconsistency Madeline has at home with home care. I really don’t have any idea what the nanny’s skills are as far asthe brushing and it looks like mom is sort of hit and miss on brushing Madeline’s teeth before bed. And, by the way,she’s using a full strip of toothpaste and for a 2 ½ year-old, we would be recommending probably at this age a non-fluoridated toothpaste, something that maybe she could swallow because at this age the idea that she could actu-ally expectorate the toothpaste is probably pretty unrealistic. Now, I’m not going to get too worried about pacifieruse at this appointment, maybe I will address that in the future. The other risk factor that is huge is her older sister.Her older sister clearly has had and probably still does have dental infection as evidenced by the restoration and thestainless steel crown.

12
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
So if Madeline is in the office and we’vedetermined risk, we would probably cate-gorize Madeline as a high risk patient. Wetalked about all the factors that would indi-cate high risk for her. I know the storm iscoming. So I’ve given you what are calledCDT codes. Those are also known as theinsurance codes you’d use when you billinsurance for your dental patients. So wealways want to interview and re-interviewparent/caregivers at every appointment sothat we can better assess risks. We alsoare going to use risk assessment as ourdriving force for how we proceed withtreatment and our recommendations forhome care and our recommendations forthe frequency interval, how often Madeline
needs to come back for additional prophylaxis appointments, reapplication of fluoride, and so on. A couple of thingsI’d like to point out. You’ll notice it says toothbrush prophy. The feedback I get from the live programs from dentalprofessionals is, “Gee, I can’t imagine polishing a 2 ½ year-old’s teeth.” Well, I agree because at this age, the likeli-hood that you would need to pull out a prophy angle and pumice is pretty slim. It doesn’t matter if you use a tooth-brush or if you use a rubber cup. A prophylaxis basically means to remove the surface debris. The code is 1120, that’sa child’s prophy. And for Madeline, that would be a toothbrush prophy. No dentifrice needed, simply a toothbrushand a hygienist would be applying that to the teeth to remove any surface plaque biofilm. Examination – there is aspecific code that we use for kids under age 3, 0145. Fluoride varnish – when children are deemed high risk, theinsurance code is 1206 for fluoride varnish; it’s for high risk kids and Madeline falls into that category. Now for otherchildren, the code is 1203. If she is determined as high risk, dental sealants might be indicated for Madeline and thecode is 1351. When do you need to bring her back? Well, the six month for everybody protocol probably doesn’tapply to Madeline. We need to keep a tight rein on Madeline and we need to keep a close watch on Madeline. Soprobably at three months we’d have mom bring Madeline back so we can re-interview, re-evaluate risks, we can re-modify home care education, prophylaxis if surface plaque is present, dental sealants if they weren’t done at the orig-inal appointment. And of course, any time we end a pediatric appointment, who doesn’t like a hug or a high five,maybe a group photo, and who doesn’t enjoy a trip to the toy box or the treasure chest?

13
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
This is Jasmine. She’s 9 months old. She wasborn in and lives in Atlanta, GA. Mom and dadare both college graduates. Mom works parttime as an RN and dad is a real estate agent.Jasmine goes to her grandmother’s housethree days a week for daycare; she stayshome with mom the other half of the week.Mom has great oral hygiene. Mom says,“Well, my only bad habit is I chew gum.” But,upon further investigation you discover hergum contains xylitol as the first ingredient.That’s a huge benefit! Dad says his busyschedule doesn’t allow for flossing and hegets his teeth cleaned twice a year. There areno significant dental issues. However, momdoes say that her three sisters are diabetic.So Jasmine’s three aunts are all diabetic.
Jasmine is transitioning to solid food; she only uses a bottle three times a day. There’s no bottle at bedtime. That is a hugebenefit. Mom says she needs help on how to brush Jasmine’s teeth because Jasmine whines and she gags and she crieswhen mom tries to brush her teeth. Clinically, she has four incisors present. There is no cavitation, there are no white spots,there’s no plaque, there’s no inflammation. So if you look at Jasmine as a whole, I’d like for you to think for a moment howwould you classify Jasmine? Is she low-risk, moderate-risk, or high-risk?
Let’s take a look at things that I see as bene-fits. She lives in and was born in a fluoridatedcity. Mom and dad as far as socioeconomicsand education, that’s a plus. Parent’s oral andoverall health is a plus. The only caveat to thatis mom’s three sisters being diabetic. Wehave to really keep a close eye on mom as faras her overall health and maybe her potentialfor developing periodontal disease due todiabetes history in the family; we have tokeep a close eye on that. The other plus:Jasmine is transitioning away from the bottlewell before her first birthday. We also see clin-ically everything looks great. Again, the onlyquestions I would have is the diabetic statusof Jasmine’s aunts, I would also say as aquestion mark is teaching mom that Jasmine
probably is going to whine and cry. But you know what, mom? Brushing Jasmine’s teeth is a non-negotiable. Just like dirtydiapers and a car seat, we wouldn’t not change a diaper just because they whine, we wouldn’t not put them in a car seatjust because they fuss and cry. Same thing with brushing, we’re going to do it. It’s one of the kindest gifts you can giveyour child, is a lifetime of good oral health. The only other question is what’s going on a grandmother’s house. I wouldencourage Jasmine’s mom to talk with her mother about good snacks, bad snacks, and brushing.

14
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
You probably guessed that Jasmine is lowrisk. We talked about all the things that arebenefits and only a few areas that we hadquestions about. So you can see here, verysimilar to what we saw with Madeline asfar as the toothbrush prophy, the examina-tion, and the varnish would be question-able. If she is diagnosed as low-risk, wemay or may not do the varnish applicationat that appointment. She likely will be puton a re-care interval of six but probably 12months would be more likely for Jasminebecause of her low risk category. Andagain, we finish on a high note with a hug,maybe a picture, and a toy.
Let’s move on to case #3 and I’d like you tomeet Luke. Luke is 18 months old. He wasborn in Guatemala and was adopted by hisparents when he was 11 months of age.He currently lives in rural Iowa and momand dad report that they have well water.Mom and dad both have computer sciencedegrees from the University of Iowa. Bothwork from home as computer consultants.Luke stays with grandparents during theday for childcare. Mom has marginal oralhygiene. She has her teeth cleaned twotimes per year and she says, “my gumsalways bleed.” Dad has good oral hygienebut tends to forget dentist appointmentsregularly so dad typically doesn’t haveroutine dental care. Both parents have
great or good overall health. Grandmother reports that Luke uses a sippy cup regularly throughout the day. Duringthe day apple juice and milk, and water at night. Grandmother also says, “Luke does a great job of brushing his teethby himself” at 18 months of age. Grandma says Luke sucks his thumb when he’s tired and when he’s sleeping.Grandma also says Luke’s pediatrician was the one that recommended Luke see a dentist when Luke was at his lastwell child visit. Clinically, you see white spot lesions present on four maxillary incisors, moderate plaque generalized,and a slight open bite.

15
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
Let’s identify risk factors for Luke. Well, I’mgoing to go now toward the bottom of theslide. Luke’s pediatrician recommended hesee a dentist at his last well child visit. Tome, that’s a huge red flag when obviouslysomething is glaringly wrong or suspiciousin Luke’s mouth. Clinically, we see obvioussigns of white spot lesions and that’s early,early childhood caries. Moderate plaquegeneralized. Other things that I see as riskfactors: Luke continually uses a sippy cupand the frequency of exposure to cario-genic beverages such as apple juice andmilk during the day are really big concerns.He was born in Guatemala. We really don’tknow the oral health of Luke’s birthparents; we only know the oral health of
Luke’s adopted parents. Now, even though they are not the birth parents, the fact that the adults living in the homewith Luke – his adopted parents – their oral hygiene really does make a difference. We talked earlier about the factthat dental caries is a communicable, transmissible disease. So if mom and dad have periodontitis, or if mom anddad have untreated dental caries, that’s potentially a risk factor for Luke. We aren’t sure about the fluoridation of thewell water so we really want to take a look at that. I think a significant amount of patient education needs to happenwith Luke’s grandmother as well as Luke’s parents. Luke’s grandmother needs to have significant education when itcomes to brushing because no 18 month old child, no matter how smart and precocious they are, is going to do agreat job of effectively disrupting dental biofilm by brushing their teeth on their own.

16
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
So if we take a look at Luke and we saw allof the risk factors, you see Luke is a highrisk pediatric patient. So you can see herewe’re doing the healthcare education, thetoothbrush prophylaxis, the exam becausehe’s under 3, Luke is high risk. Kids that arehigh risk, that code of 1206, I would recom-mend and encourage you to look intocaries management by risk assessmentand look at the recommendations on fluo-ride reapplication. Once or twice a yearmight not be enough of a benefit for kidsthat are moderate and especially high risk.Again, high risk kids, it’s possible we wouldwant to seal those primary molar teeth toprevent future infection. Because again,when you go back to the picture of the
beach and it was a beautiful sunny day and we know the storm is coming based on risk assessment. His re-careinterval would probably be more along the lines of 3 months so we can re-evaluate and re-assess. If we can modifyand control risk factors through patient education and early intervention, eventually Luke might not need to comeback and see us at 3 months. We could eventually move his re-care interval out farther. And again, it just dependson how well he responds to the interventions and the risk assessment.
Finally, let’s meet Michaela. Michaela is 5.She was born and lives in Boston, MA. Shewas born five weeks premature and had tostay in the NICU for about a week afterbirth. Mom and dad are both college grad-uates and both work in medical research ata local university. Michaela attendsMontessori school in downtown Bostonabout 8 ½ hours a day. Mom grew up inChina, she had very little dental care untilshe moved to the US. Dad grew up inBoston and has terrific oral hygiene.Michaela uses a sippy cup with city waterthroughout the day. She has an allergy todairy, dad worries that she doesn’t getenough calcium because of her allergy todairy products. Her parents let Michaela
brush first, then they check and see if they need to follow up. Sometimes they do, and sometimes they say theydon’t need to; she’s done a great job. Clinically, you see one small white spot lesion on a mandibular canine andslight plaque on the mandibular right.

17
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
If we were going to start to identify riskfactors for Michaela, one of the first thingsyou probably thought of was the fact thatshe was born not only premature, but shehad to stay in the NICU for a week afterbirth. We talked about earlier, as far as riskassessment, a risk factor – kids born toosmall and too early have been shown in theresearch to be slightly at higher risk forearly childhood caries. Maybe another riskfactor would be the fact that Michaela’sparents, at age 5, are letting her do most ofthe primary brushing and sometimes theydon’t follow up with brushing becausethey’ve assessed that she’s done a prettygood job. The other two clinical featureswe see, the fact that she already has active
disease, the one small white spot lesion, that’s early, early childhood carries, that area of demineralization on thecanine. And clinically, we see she’s probably not doing that great a job on her brushing because we do have evidenceof dental biofilm present in the mouth.
Based on your clinical judgment and yournew knowledge of risk assessment, youknow Michaela is a moderate caries risk.Specifically, we would want to provideextensive home care education toMichaela’s father - he’s the one thatbrought her to the appointment - a tooth-brush prophylaxis, and an examination.Now you’ll notice the exam code is not thecode we used for the other children.Because she’s 5 years old, we’ll use thecode 0120. Fluoride varnish, depending onrisk level, 1203 or 1206. And again, basedon determination of risk and the dentist’sdiagnosis, dental sealants might be indi-cated for primary molar teeth.

18
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
Hopefully, the activity of evaluating risks onMadeline, Jasmine, Luke, and Michaelahas helped you better grasp the conceptsof identifying potential risk factors in yourinfant and toddler dental patients. If someof the procedure codes we discussed areunfamiliar to you, I would encourage you toreview the annual CDT resource book;Current Dental Terminology book. Thisbook not only gives us the procedurecodes also known as the insurance codes,but it also clearly defines what those proce-dures mean. Remember, you don’t knowwhat you don’t know! And now you knowand I hope you feel compelled to embracethis new standard of care: risk assessment.
Finally, if you leave this virtual CE classroomtoday with a desire to learn even more aboutrisk assessment of the pediatric population,please review the California DentalAssociation’s October 2007 Journal. Theyhave compiled an incredible amount ofinformation and I find this resource, thisissue an excellent resource for risk assess-ment. I’ve also listed additional websitesthat you can access to look at early child-hood caries, to look at recommendations oninfant and toddler dental visits. I’ve alsoincluded the Sonicare website,sonicare.com/dp. Please visit that site forcurrent information about the Sonicare forkids, also a listing of all the current, livecontinuing education programs available.
We teach a very expansive program that covers the material that we talked about today in much greater depth andbreadth. I’ve left my business card on the bottom of this slide with my email address. Because I can’t be there with youin person, I would be happy to entertain any questions that you might have. Please feel free to email me [email protected]. Please note, there’s only one “l” in Philips. Good luck with the risk assessment!

19
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
Examination Review
This page is provided for review only. To access the online post-exam you must be “Registered” and “Signed In.”and have completed the course selection/purchase process in its entirety. Once selected/purchased the course titlewill be added to your MyCE Archives page where a Take Exam link will be displayed directly across from the coursetitle. A letter of credit will be issued upon successful completion of the post-exam with a score of 70% or higher.
Please note: Credit may not be claimed if completed after the course expiration date.
1) The trend in dentistry today encompasses all of the following except:A) Early risk assessment with parent/caregiver (preferably by age one)B) Educating parent/caregiver that dental caries is a preventable diseaseC) Recommending all children have their first visit with the hygienist around age threeD) Individualized treatment recommendations based on child’s risk
2) The primary reason for assessing and modifying risk factors in infants and toddlers is to:A) Prevent disease process from ever beginning B) Provide a wonderful revenue stream for the dental practiceC) Teach parents a lesson on why they need to start brushing their child’s teethD) Reduce the amount of surface stains present on the primary teeth
3) Michaela was deemed a moderate risk child. Please identify which risk factor was not considered apotential negative risk factor?A) Michaela drinks city tap water B) Clinical exam revealed a white spot lesionC) Michaela was born 5 weeks early and spent time in the NICUD) Michaela, at age 5, does most of her own brushing – mom and dad usually just do a visual ‘check’ to
see if she brushed
4) Luke, the 18 month old baby born in Guatemala, was deemed a high risk child. Which one of thefollowing plays no role in his caries risk?A) Luke was born in Guatemala – no history on parents’ oral healthB) Luke sucks his thumb when he’s tired C) Luke brushes unassistedD) Luke has juice and milk in his sippy throughout the day
5) According to the Current Dental Terminology guidelines, a prophylaxis for an infant or toddler will likelyinclude:A) Scaling with hand instrumentsB) Instrumentation with ultrasonic or piezoelectric devicesC) Air polishingD) Use of toothbrush prophylaxis for biofilm disruption E) Full mouth periodontal charting

20
Predicting is Preventing! Implementing Risk Assessment for Infants and Toddlers in Your Practiceineedce.com
6) CDT procedure codes likely utilized during an infant appointment could be:A) D0145 clinical oral evaluation for patient for under three years of age and counseling with primary
caregiverB) D 1204 topical application of fluoride – adultC) D1120 child prophylaxis (toothbrush prophy)D) A and C onlyE) All of the above
7) In 2008, which organization called “oral health” one of the top three healthcare issues for children in theUnited States?A) The American Academy of General DentistryB) The American Academy of PeriodontologyC) The American Academy of Pediatric DentistryD) The American Academy of Pediatrics
8) There are multiple risk factors identified for early childhood caries. However, most experts will agree that_______________ is by far, the number one influencer on an infant/toddler’s incidence of dental cariesinfection.A) Exposure to too many sticky sweetsB) Poor oral hygieneC) Oral health status of mother and older siblings D) Breastfeeds on demand for long periods of time