ppt enceha....pptx
TRANSCRIPT
Oleh :Liza Oktamaya sari
pembimbing :dr. M. Dwikoryanto, sp.bs
REFERATENSEFALOKEL
Definition
What is encephalocele ?
A herniation of the cerebral tissue, meninges and/or cerebrospinal fluid through a defect in the skull that is closed or covered with skin.
Encephalocele is one of the three most
common neural tube defects.
– Anencephaly
– Myelomeningocele
Classification
Primary encephalocele
– congenital
Secondary encephalocele
– Acquired
– due to trauma or a postsurgical defect
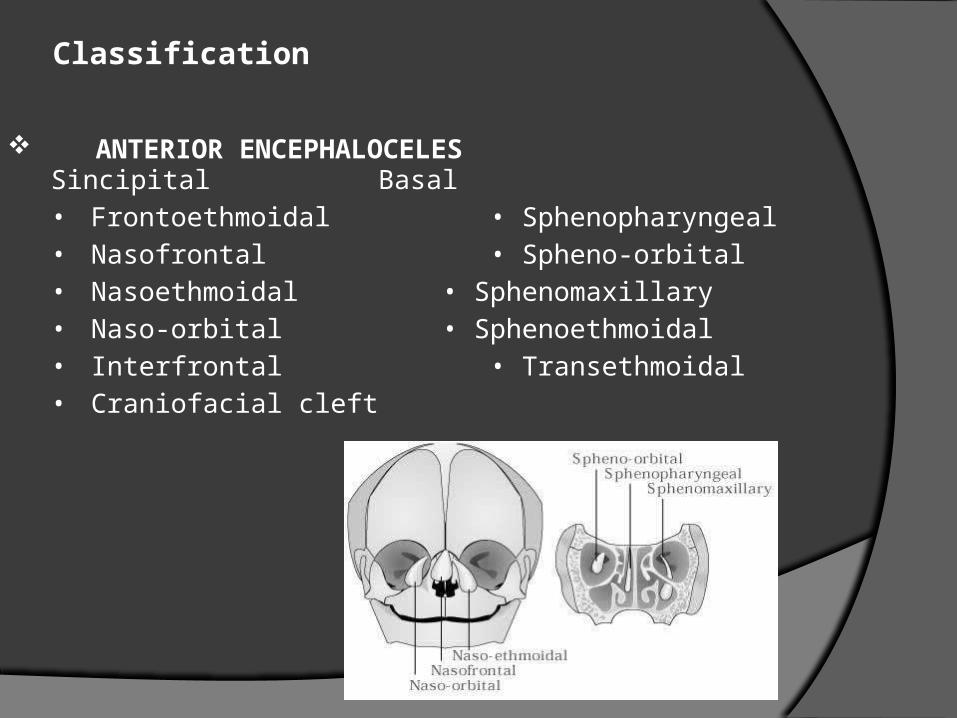
Classification
Sincipital Basal
• Frontoethmoidal • Sphenopharyngeal
• Nasofrontal • Spheno-orbital
• Nasoethmoidal • Sphenomaxillary
• Naso-orbital • Sphenoethmoidal
• Interfrontal • Transethmoidal
• Craniofacial cleft
ANTERIOR ENCEPHALOCELES
POSTERIOR ENCEPHALOCELES
– Occipital
• Supratorcular
• Infratorcular
– Occipitocervical
– Parietal
• Interfrontal
• Interparietal
• Anterior fontanelle
• Posterior fontanelle
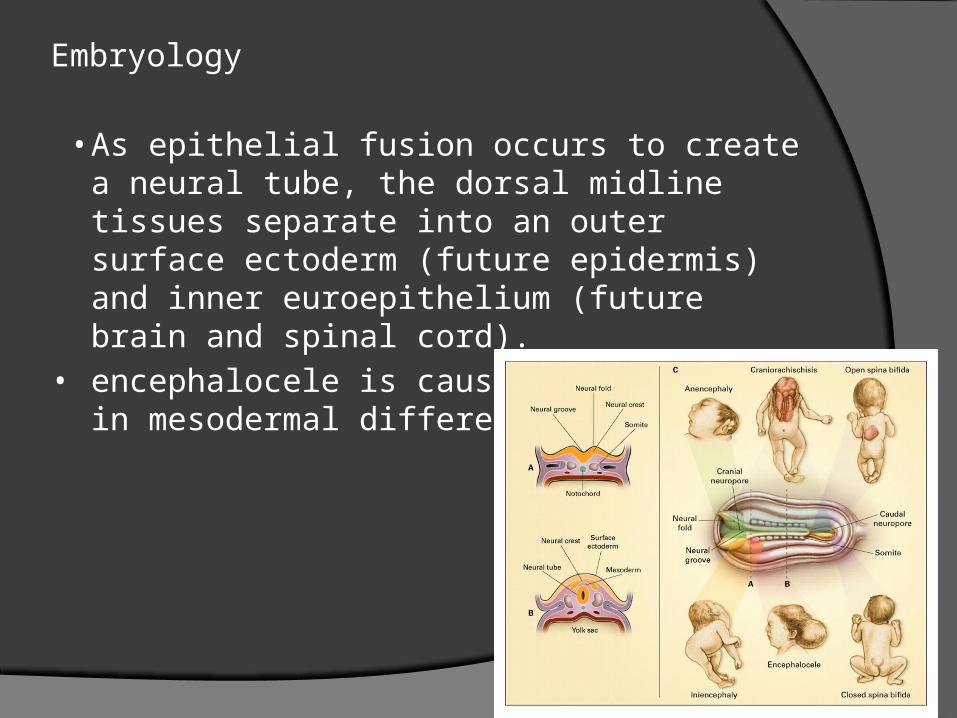
Embryology
• As epithelial fusion occurs to create a neural tube, the dorsal midline tissues separate into an outer surface ectoderm (future epidermis) and inner euroepithelium (future brain and spinal cord).
• encephalocele is caused by an error in mesodermal differentiation.
Epidemiology
• Incidence : varies according to geographic location and
race.
• In North America, Europe, and northern Asia
– occipital encephaloceles
– 0.8 and 4.0 per 10,000 live births,
– sincipital encephaloceles are considerably more rare.
• By contrast, in Southeast Asia,
– sincipital encephaloceles
– occur in 1 in 5000 live births
– occipital encephaloceles are much less common.
• Congenital basal encephaloceles represent just 10% of
all encephaloceles in most series.
• Males and females were equally
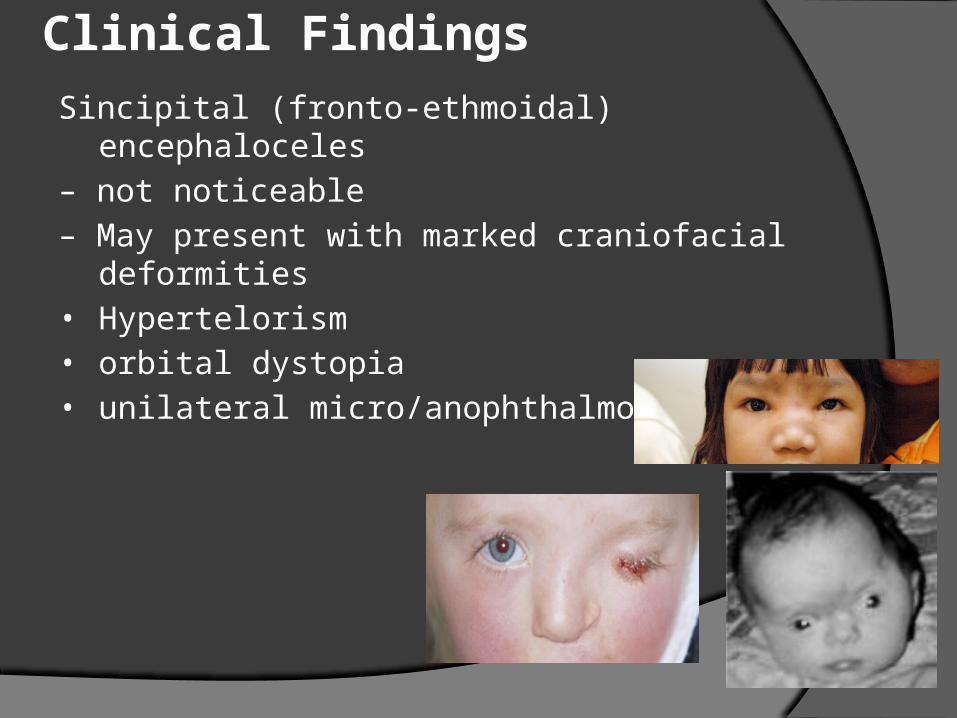
Clinical Findings
Sincipital (fronto-ethmoidal) encephaloceles
– not noticeable
– May present with marked craniofacial deformities
• Hypertelorism
• orbital dystopia
• unilateral micro/anophthalmos
Basal encephaloceles
– may or may not be apparent on external inspectio
– but there may be a broadened nasal bridge,
hypertelorism, or other midfacial anomalies.
– Affected patients may present as a nasal or
epipharyngeal mass, difficulty breathing, recurrent upper tract infections, nasal ischarges, recurrent meningitis
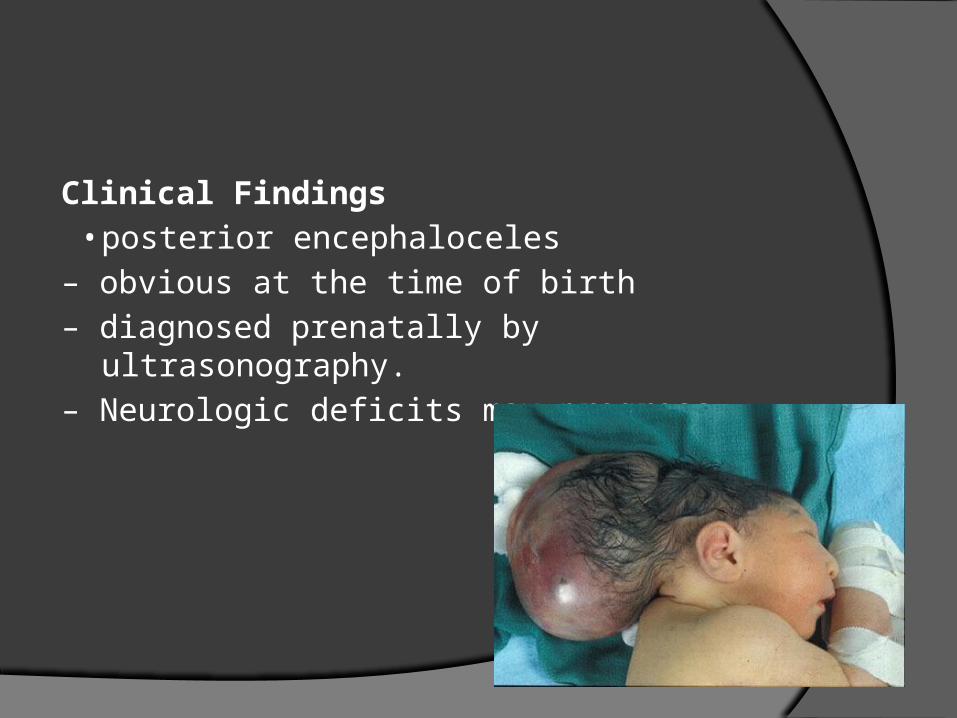
Clinical Findings
• posterior encephaloceles
– obvious at the time of birth
– diagnosed prenatally by ultrasonography.
– Neurologic deficits may progress
Diagnosis
• Postnatal MRI is the diagnostic study of choice to
– classify the encephalocele
– the degree of functional tissue inside the sac and
– hydrocephalus
• Magnetic resonance angiography/venography
(MRA/MRV) may be useful in defining the lesion
with respect to its surrounding vasculature.
• Volumetric (three-dimensional) CT can help in
planning craniofacial reconstruction in infants
Management
• Despite their varied demographics and outcome, the principles of management are similar
– removal of the sac
– preservation of functional neural tissue
– protection from leakage of CSF by closure of the
meninges and skin
– correction of the cosmetic deformity
Posterior Encephalocele
Occipital encephalocele
• Occur between the lambda and foramen
magnum
• Typically in midline
• 2 types : supratorcular, infratorcular
• Vary in appearance, size, contents
Parietal encephalocele
• Any point of parietal lobe
• Including lambda and bregma
Surgical management
• Infant is positioned in prone on a horseshoe head-rest
• Extend elliptically around the lesion.
• Dissect the pericranium to approach the skull defect and the neck of the sac.
• Find the dural margin at the bone defect
• Decompress the contents of the sac by removing CSF and put the normalcy of the tissue back.
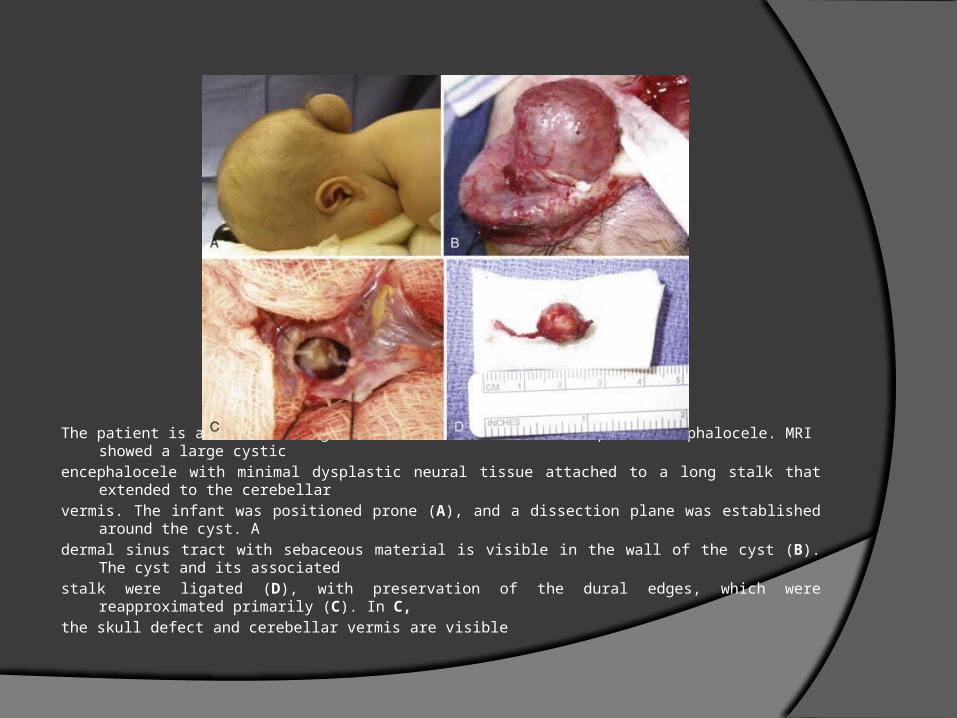
The patient is a 3-month-old girl with an infratorcular occipital encephalocele. MRI showed a large cystic
encephalocele with minimal dysplastic neural tissue attached to a long stalk that extended to the cerebellar
vermis. The infant was positioned prone (A), and a dissection plane was established around the cyst. A
dermal sinus tract with sebaceous material is visible in the wall of the cyst (B). The cyst and its associated
stalk were ligated (D), with preservation of the dural edges, which were reapproximated primarily (C). In C,
the skull defect and cerebellar vermis are visible
Post op complication
• Hydrocephalus (higher in post. Encephalocele)
• Leakage
• Psuedomeningocele
• Ventricular enlargement
• Head circumference enlargement
ANTERIOR ENCEPHALOCELE
Anterior Encephaloceles
1. Sincipital encephaloceles
- involve the region of the foramen cecum
- present at birth or later in childhood or adulthodd
- subclassification by their bone defect and the course
of the encephalocele sac.
- naso frontal , nasoethmoidal , naso orbital
Anterior Encephaloceles
• Interfrontal encephaloceles – resemble other cranial vault, less common
• Nasoethmoidal encephaloceles are visible at birth as a facial swelling that enlarges with crying or Valsalva maneuver.
- Manifested as nasal mass later in childhood and
adulthood.
- Can be confused with nasal polyp (istinguishable by epidermiology , location and diagnostic sign. )
Polyp – rare in children
– Evolve from the turbinates and do not emanate from the
midline
– Do not swell with jugular compression ( Furst-enberg sign + )
– Do not widenting of the nasal bridge as sincipital encephaloceles.
DDX of the naso-orbital area
– Dermoid cyst ( teratoma w or w/0 dermal sinus
tract ) these growth typical in midline
While eccentric nasoorbital or nasofrontal lesion are not pulsatile , not enlarge with crying
2. Basal encephaloceles
- further posteriorly and close to the suprasellar cistern
- contain viable neural structures
- Classified according to the location of the herniated stalk : Transethmoidal and transphonoidal.
DDx : teratoma
Surgical Management
• Depending on the surgeon’s experience and
the resources and the patient population
being treated
• Three main goals of Surgery :
1. correction of the deformity
2. Prevention of CSF leak
3. Preservation of functional neurovascular elements
1. Correction of the deformities
- require that the surgeon be trained in the management of complex craniofacial abnormalities with attention to correction of
telecanthus and maintenance of the horizontal ocular axis, and hyperteleorism and reconstruction of nasal abnormalities
2. Absence of CSF leak
- can be treated electively in early infancy to avoid the
consequences of a craniofacial deformity that will
progress in the setting of a pulsatile encephaloceles
3. Preservation of functional neurovascualr elements
- analogous to the treatment of single-suture synostosis in early infancy, single , early operation for repair of anterior encephalocele correct the deformity caused by the encephalocele and rely on neurological and craniofacial development in the first few years of childhood
