powerpoint slides english spanish translation breast ... · otros tipos de colgajos son los...
TRANSCRIPT
1
PowerPoint Slides English Spanish Translation
Breast Cancer Survivorship: Role of Plastics and Reconstruction Video Transcript
Supervivencia al cáncer de mama: Función de la cirugía plástica y la reconstrucción Transcripción del video
Professional Oncology Education Breast Cancer Survivorship: Role of Plastics and Reconstruction Time: 34:30
Educación Oncológica Profesional Supervivencia al cáncer de mama: Función de la cirugía plástica y la reconstrucción Duración: 34:30
Melissa A. Crosby, M.D. Associate Professor Department of Plastic Surgery The University of Texas MD Anderson Cancer Center
Dra. Melissa A. Crosby Profesora Asociada Departamento de Cirugía Plástica MD Anderson Cancer Center de la Universidad de Texas
Hello. My name is Melissa Crosby. I’m an Associate Professor at The University of Texas MD Anderson Cancer Center in the Department of Plastic Surgery. Today, I’d like to discuss with you the role of plastics and reconstruction in breast cancer patients.
Hola, mi nombre es Melissa Crosby. Soy profesora asociada del Departamento de Cirugía Plástica en el MD Anderson Cancer Center de la Universidad de Texas. Hoy explicaré la función de la cirugía plástica y la reconstrucción en pacientes de cáncer de mama.
2
Upon completion of this lecture, participants will be able to describe the benefits of reconstruction in breast cancer patients; compare the most common techniques of reconstruction in patients; and detail the benefits and risks associated with each type of reconstruction; also outline different methods of reconstruction and identify the best method considered for each patient.
Al finalizar esta disertación, los participantes podrán describir los beneficios de la reconstrucción en estas pacientes; comparar las técnicas más comunes de reconstrucción; detallar los beneficios y los riesgos asociados con cada tipo de reconstrucción; y definir los diferentes métodos de reconstrucción e identificar el más adecuado para cada paciente.
When a patient is diagnosed with breast cancer, there’s a great degree or depression and anxiety associated with this diagnosis. There is the uncertain prognosis of the disease, as well as many patients feel this is a life-threatening disease. There’s also a fear of the breast, losing the breast, the fear of rejection of having that breast gone, loss of femininity and self esteem. Also, the loss of a breast is a reminder of the disease. There’s also a[n] issue of body imbalance, shoulder, and back pain.
Cuando una paciente es diagnosticada con cáncer de mama, experimenta gran depresión o ansiedad asociada al diagnóstico. Hay cierta incertidumbre en el pronóstico de la enfermedad y muchas pacientes sienten que su vida está en riesgo. También temen perder la mama, el rechazo por haberla perdido, temen perder su feminidad y sufren de baja autoestima. Además, la pérdida de un seno es un continuo recordatorio y pueden tener desequilibrio corporal, dolor de hombros y espalda.

3
As a reconstructive surgeon, we see ourselves as being able to reestablish that body wholeness and symmetry for many patients as well as improve their self-image.
Los cirujanos reconstructivos consideramos que podemos restablecer la integridad corporal y la simetría de muchas pacientes, así como mejorar su propia imagen.
We find this to be a great qro --- quote: “We feel that we restore, repair, and make whole those parts which nature has given, but which fortune has taken away.”
Esto se resume en una frase: “Creemos que podemos restaurar, reparar y recomponer aquellas partes que la naturaleza nos ha dado, pero que la fortuna nos ha quitado”.
4
So why do we perform reconstruction? In 1998, Congress helped us in the fact that the Women’s Health and Cancer Right Act was mandated. This requires that all group healthcare plans and health insurance provide medical and surgical benefits to cover the cost of reconstructive breast surgery. This includes symmetry procedures to the unaffected breast for women who have undergone mastectomy. Due to improved cancer detection and survival, it’s estimated that 75% of patients undergoing mastectomy go on to have some form of reconstruction.
¿Por qué realizar la reconstrucción? En 1998, el Congreso de los Estados Unidos sancionó la “Ley de derechos sobre la salud y el cáncer de la mujer”, que establece que los planes y seguros de salud grupales deben ofrecer beneficios médicos y quirúrgicos para cubrir la cirugía reconstructiva de mama. Esto incluye procedimientos de simetría al seno no afectado en mujeres con mastectomía. Debido a la mejora en la detección y supervivencia, se estima que el 75% de las pacientes de mastectomía se harán algún tipo de reconstrucción.
Reasons given for choosing reconstruction include those of being free of cumbersome and uncomfortable prostheses. It allows patients to wear most types of clothing again. Also, allows women to regain their femininity and feel whole again.
Entre las razones para optar por la reconstrucción se cuentan evitar prótesis pesadas e incómodas, poder vestir la mayoría de los tipos de ropa y la posibilidad de la mujer de recuperar su feminidad y sentirse íntegra una vez más.
5
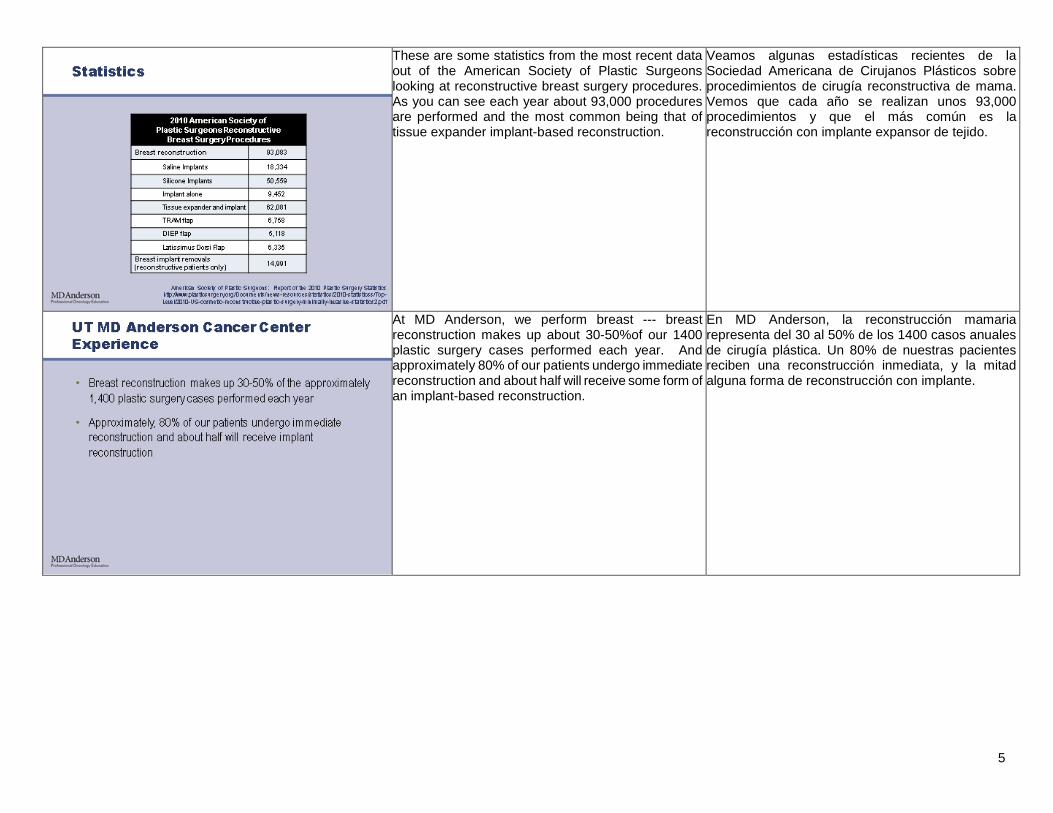
These are some statistics from the most recent data out of the American Society of Plastic Surgeons looking at reconstructive breast surgery procedures. As you can see each year about 93,000 procedures are performed and the most common being that of tissue expander implant-based reconstruction.
Veamos algunas estadísticas recientes de la Sociedad Americana de Cirujanos Plásticos sobre procedimientos de cirugía reconstructiva de mama. Vemos que cada año se realizan unos 93,000 procedimientos y que el más común es la reconstrucción con implante expansor de tejido.
At MD Anderson, we perform breast --- breast reconstruction makes up about 30-50%of our 1400 plastic surgery cases performed each year. And approximately 80% of our patients undergo immediate reconstruction and about half will receive some form of an implant-based reconstruction.
En MD Anderson, la reconstrucción mamaria representa del 30 al 50% de los 1400 casos anuales de cirugía plástica. Un 80% de nuestras pacientes reciben una reconstrucción inmediata, y la mitad alguna forma de reconstrucción con implante.
6
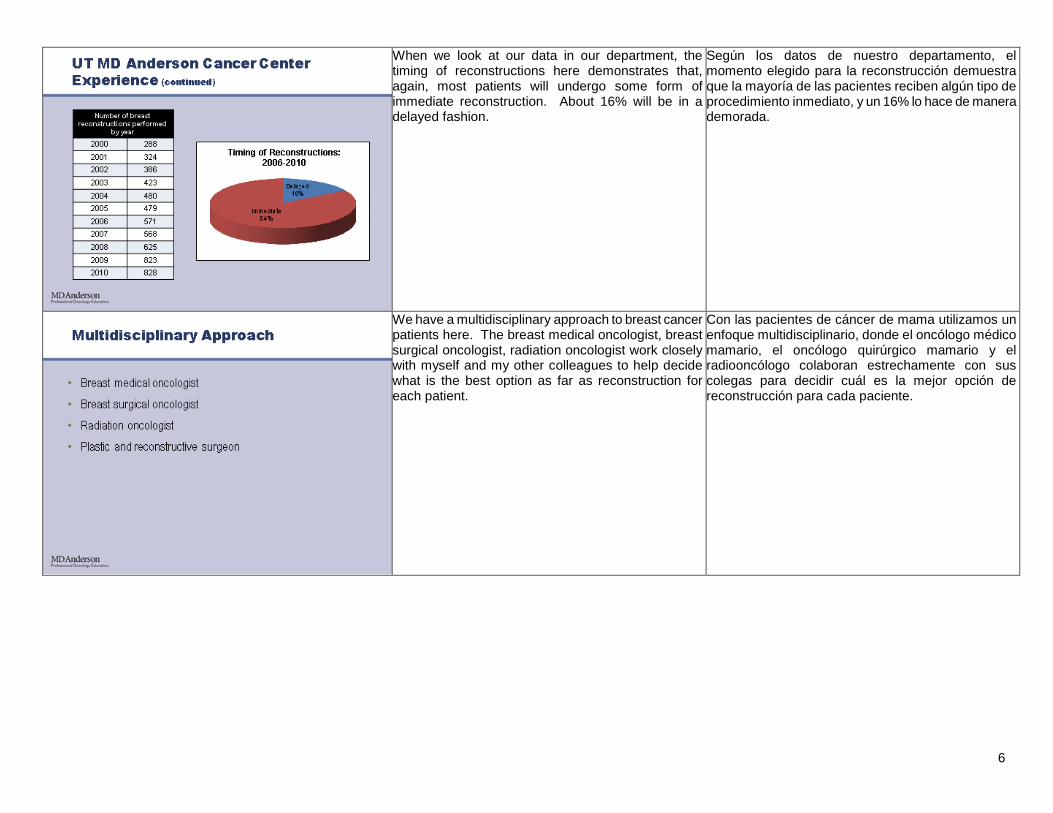
When we look at our data in our department, the timing of reconstructions here demonstrates that, again, most patients will undergo some form of immediate reconstruction. About 16% will be in a delayed fashion.
Según los datos de nuestro departamento, el momento elegido para la reconstrucción demuestra que la mayoría de las pacientes reciben algún tipo de procedimiento inmediato, y un 16% lo hace de manera demorada.
We have a multidisciplinary approach to breast cancer patients here. The breast medical oncologist, breast surgical oncologist, radiation oncologist work closely with myself and my other colleagues to help decide what is the best option as far as reconstruction for each patient.
Con las pacientes de cáncer de mama utilizamos un enfoque multidisciplinario, donde el oncólogo médico mamario, el oncólogo quirúrgico mamario y el radiooncólogo colaboran estrechamente con sus colegas para decidir cuál es la mejor opción de reconstrucción para cada paciente.

7
How reconstruction can be formed depends on timing as well as technique. What I mean by timing is, is it immediately performed at the time of the mastectomy? Or, is it performed in a delayed fashion after a patient has already had a mastectomy and received what therapy they need for their cancer treatment? In add --- in addition, different techniques are available including using the patient’s own tissue, using their own tissue and an implant, or an implant-based reconstruction alone. And I’ll go through all this in detail.
El tipo de reconstrucción depende del momento y de la técnica. Puede realizarse de modo inmediato junto con la mastectomía, o demorarse hasta después de la mastectomía, cuando la paciente ya haya recibido el tratamiento oncológico. Además se dispone de diversas técnicas, como utilizar el propio tejido de la paciente, combinar esto con un implante, o hacer únicamente una reconstrucción con implante. Veámoslas más en detalle.
We do know that breast reconstruction timing is very important for patients. We know that immediate reconstruction is preferred psychosocially. Patients report a higher degree of satisfaction with results after immediate reconstruction. And they recall less distress when they’ve had immediate reconstruction compared to those who’ve undergone delayed reconstruction in remembering their mastectomy surgery.
Sabemos que el momento de la reconstrucción es importante para la paciente y que hacerla de inmediato es preferible psicosocialmente. Las pacientes informan un mayor grado de satisfacción si la reconstrucción es inmediata. Además, superan mejor la angustia y los recuerdos de la mastectomía cuando la reconstrucción es inmediata en lugar de diferida.
8
We also know that patients undergoing immediate reconstruction are more satisfied with their ultimate reconstruction. They experience less anxiety and depression. And they have a better body image and self-esteem as well as an improved sexual attractiveness. However, patients undergoing delayed reconstruction may have initial poor body image scores. However, after about one year following their surgery, they have equivalent quality of life as those who’ve gone --- undergone immediate reconstruction. So even undergoing a delayed reconstruction is beneficial to many patients.
Asimismo, las pacientes sometidas a reconstrucción inmediata quedan más satisfechas con el resultado definitivo. Experimentan menos ansiedad y depresión, perciben una mejor imagen corporal, sienten más autoestima y se ven sexualmente más atractivas. Las pacientes de reconstrucción diferida pueden tener inicialmente una mala imagen corporal. Sin embargo, aproximadamente un año después de la cirugía, disfrutan de la misma calidad de vida que aquellas con reconstrucción inmediata. En consecuencia, aún la reconstrucción demorada beneficia a muchas pacientes.
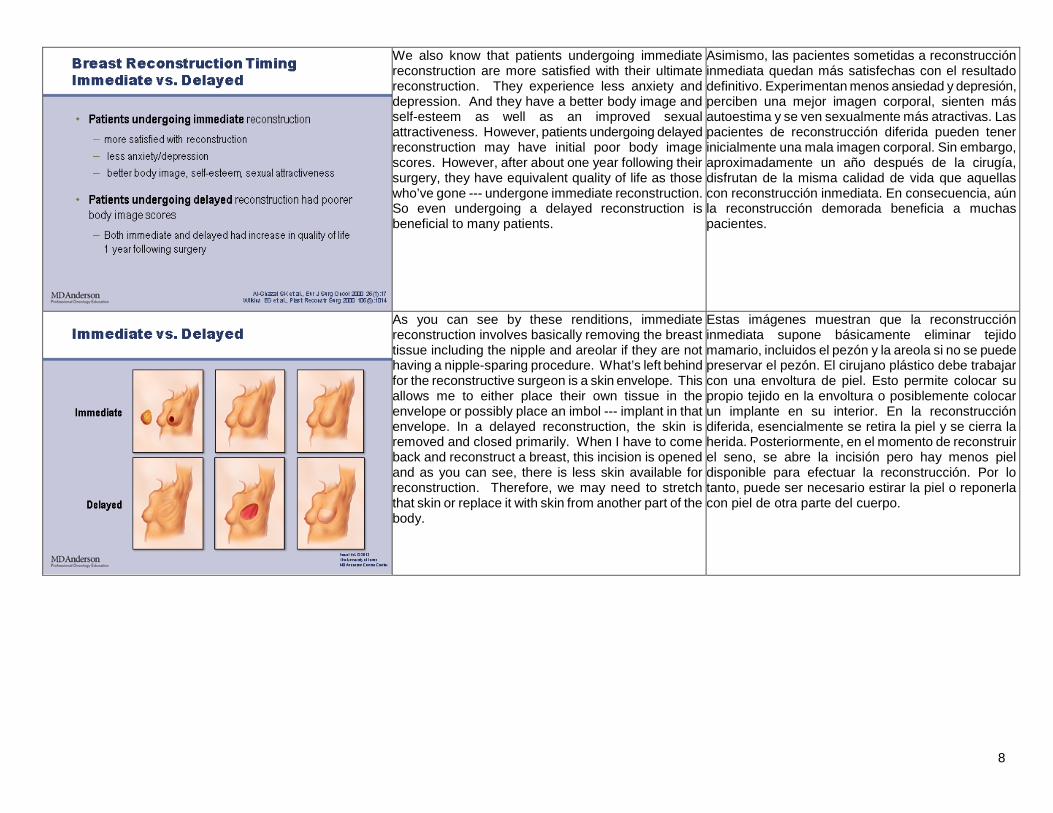
As you can see by these renditions, immediate reconstruction involves basically removing the breast tissue including the nipple and areolar if they are not having a nipple-sparing procedure. What’s left behind for the reconstructive surgeon is a skin envelope. This allows me to either place their own tissue in the envelope or possibly place an imbol --- implant in that envelope. In a delayed reconstruction, the skin is removed and closed primarily. When I have to come back and reconstruct a breast, this incision is opened and as you can see, there is less skin available for reconstruction. Therefore, we may need to stretch that skin or replace it with skin from another part of the body.
Estas imágenes muestran que la reconstrucción inmediata supone básicamente eliminar tejido mamario, incluidos el pezón y la areola si no se puede preservar el pezón. El cirujano plástico debe trabajar con una envoltura de piel. Esto permite colocar su propio tejido en la envoltura o posiblemente colocar un implante en su interior. En la reconstrucción diferida, esencialmente se retira la piel y se cierra la herida. Posteriormente, en el momento de reconstruir el seno, se abre la incisión pero hay menos piel disponible para efectuar la reconstrucción. Por lo tanto, puede ser necesario estirar la piel o reponerla con piel de otra parte del cuerpo.
9
As mentioned, there’re three categories of techniques used for reconstruction, involving implant-based, autologous tissue, which means coming from the patient themselves. This can be either free, meaning taken off the blood supply and transplanted, or pedicled, meaning maintained on the blood supply. These reconstructions involve the TRAM flap which can be muscle-sparing, DIEP or SIEA, which I’ll explain in a further slide. Other flaps include extended latissimus dorsi flaps as well as gluteal flaps and anterior lateral thigh flaps. Patients can also use a combination of both their own tissue as well as an implant. The most common is the latissimus dorsi flap and implant.
Existen tres categorías de técnicas de reconstrucción. La primera es el implante. La segunda utiliza tejido autólogo, es decir, procedente de la propia paciente. El tejido puede ser libre, escindido del suministro de sangre y luego trasplantado, o bien ser pediculado, aún conectado al suministro. Estas reconstrucciones utilizan un colgajo TRAM, que puede conservar los músculos, o bien DIEP o SIEA, que luego describiré. Otros tipos de colgajos son los extendidos del dorsal ancho, de glúteo y de muslo anterolateral. La tercera categoría es una combinación de tejido propio con un implante. La más utilizada es el colgajo de dorsal ancho más un implante.
Obviously, the type of reconstruction depends on many things including the breast cancer status and prognosis; what adjuvant treatments they’re getting, especially radiation therapy; the patient’s health status. What donor tissue is available for me to reconstruct a breast, and, of course, the patient’s preference and lifestyle considerations.
El tipo de reconstrucción depende de muchos factores, como el estado y el pronóstico del cáncer de mama; los tratamientos adyuvantes administrados, sobre todo la radioterapia; la condición de salud; el tejido donante disponible para reconstruir y, por supuesto, la preferencia de la paciente y las consideraciones de estilo de vida.

10
When we’re looking at implant-based reconstruction, often candidates that are best for this are those that are undergoing a skin-sparing mastectomy, meaning the skin is left behind for me to be able to perform a reconstruction. So we have an adequate skin envelope. Also, patients that may not have enough of their own tissue to reconstruct a breast of adequate size. Also, patient lifestyle and preference. I have many young patients who have young children that don’t want to go through more extensive surgery and have any other scars on their body. Also, anyone that has no history or is not going to need radiation therapy.
Al evaluar la reconstrucción con implante, las candidatas más aptas son a menudo las que reciben una mastectomía conservadora que deja una cantidad de piel suficiente como para poder realizar una reconstrucción si la envoltura de piel es adecuada. A veces el tejido propio es insuficiente para reconstruir una mama de tamaño adecuado. Importan el estilo de vida y las preferencias. Muchas pacientes jóvenes tienen niños pequeños y no quieren pasar por una cirugía más extensa y tener cicatrices en el cuerpo. Debemos considerar si hay antecedentes de radioterapia, o si se necesitará.
What’s usually performed is a two-stage procedure. You can perform this in one stage, but at MD Anderson, we prefer to perform in a two-stage. A tissue expander is usually placed at the time of the mastectomy. This is a temporary balloon that’s placed under the pectoralis major muscle and skin.
Usualmente se realiza en un procedimiento de dos etapas. Puede hacerse en una sola, pero en MD Anderson preferimos hacerlo en dos. Durante la mastectomía se coloca un expansor de tejido, que es un balón temporal debajo de la piel y del pectoral mayor.

11
This tissue expander has a port that we are albe --- able to access in our clinic. And so, therefore, the expansion process is performed in clinic in which saline is injected into the tissue expander and allows us to increase the size and stretch the skin enveloped.
El expansor tiene un puerto para acceso desde el exterior. El proceso de expansión se realiza en la clínica inyectando solución salina en el expansor para aumentar su tamaño y estirar la piel que lo envuelve.
Later a further surgery is necessary to replace that with the final implant. So the tissue expander is removed and a final implant is placed. Again, in certain patients, an implant may be placed immediately at the time of the mastectomy.
Posteriormente, en otra operación, se lo reemplaza por el implante definitivo. El expansor de tejido es retirado y se coloca el implante. En ciertas pacientes, el implante se coloca inmediatamente durante la mastectomía.

12
The advantage of an implant reconstruction is that you may get a more perky-looking breast or more youthful-looking breast. There’re no additional scars that I have to place on the body so I use the scar that is made to perform the mastectomy. There may be less hospitalization and recovery time as well as having the ability to have a one-stage reconstruction, meaning one surgery.
La ventaja de la reconstrucción con implante es que resulta en una mama más levantada, de aspecto más juvenil. No quedan cicatrices adicionales en el cuerpo, pues se utiliza el mismo corte de la mastectomía. Puede haber menos tiempo de hospitalización y recuperación, pues la reconstrucción de una sola etapa significa una sola operación.
The disadvantages are obviously there is maintenance to the implant. This is a foreign body. It may need to be exchanged or removed at a later time. You can also have complications including capsular contracture, which is scarring around the implant. You can also have failure of the implant as well as infection. The --- also, disadvantage may be a two-stage procedure with the use of a tissue expander. For some patients, they don’t want to go through multiple surgeries after their mastectomy. Also, it’s often hard to match a natural breast with the unilateral breast reconstruction because an implant-based reconstruction is often more perky-looking than a natural breast is. And, therefore, additional surgeries may be needed on the natural breast to make it look more similar to the reconstruction.
Las desventajas son, obviamente, que el implante requiere mantenimiento. Por ser un cuerpo extraño, tal vez deba ser cambiado o retirado más adelante. Puede haber complicaciones, como una contractura capsular, que es cicatrización alrededor del implante. Puede haber fracaso del implante, así como infección. El procedimiento de dos etapas que utiliza un expansor de tejido es menos conveniente, y algunas pacientes prefieren no volver a operarse después de la mastectomía. Con la reconstrucción mamaria unilateral a menudo es difícil igualar la mama natural, porque el implante resulta en una mama más levantada que un seno natural. En este caso, pueden requerirse operaciones adicionales en la mama natural para que luzca más similar a mama reconstruida.

13
Often times, we may use what’s called a bioprosthetic sling. This is an acellular collagen matrix derive --- derived from dermis. Different products are available including fetal bovine, human, or porcine. This is biocompatible, cell-friendly. It allows revascularization and integration into host tissue. As you can see here, this is the bioprosthetic. This is the pectoralis major muscle where the tissue expander is placed underneath both.
A veces utilizamos un cabestrillo bioprotésico, que es una matriz de colágeno acelular derivado de la dermis. Existen diversas variantes de origen bovino fetal, humano o porcino, que son biocompatibles y no afectan las células. Permiten la revascularización y se integran al tejido huésped. Vemos aquí la bioprótesis. Este es el pectoral mayor y el expansor de tejido se coloca debajo de ambos.
The advantage of this, it allows less tension on the skin and acts as an extension of the pectoralis major muscle. For many women that have large breast skin envelopes, often the pectoralis muscle is very short. And, therefore, you may need an extension to that, either using a bioprosthetic sling such as this, or bringing a serratus muscle from the patient’s side to replace this area. It also may allow greater intraoperative fill volumes and possibly improve the aesthetics. We are able to recreate the inframammary fold and lateral chest wall that may be disrupted during the mastectomy. It also may allow that immediate implant placement without the need for a tissue expander. The disadvantages are that it’s expensive. Not a lot of insurance companies pay for this. It is a foreign body so it has a risk just like the expander does of getting infections and so forth. And it has a tendency to cause fluid collections or seromas.
Una de sus ventajas es reducir la tensión de la piel y actuar como una prolongación del pectoral mayor. En mujeres con grandes envolturas de piel mamaria, el pectoral suele ser muy corto. Esto requiere una prolongación, ya sea con un cabestrillo bioprotésico como en este caso, o traer el serrato lateral de la paciente para reemplazar esta zona. A veces permite mayores volúmenes de llenado intraoperatorios y mejora la estética. Podemos recrear el pliegue submamario y la pared torácica lateral alterada por la mastectomía. También puede permitir la colocación inmediata del implante sin necesidad de un expansor. Como desventaja, es más costoso y pocos seguros médicos lo cubren. Por ser un cuerpo extraño, tiene el mismo riesgo que un expansor de causar infecciones, etc., y tiene una tendencia a causar acumulaciones de líquido o seromas.

14
As far as the type of implants that can be placed in patients, in 1992, saline implants were --- [excuse me] --- silicone gel implants had been used until 1992. So saline implants have been approved by the FDA since 1992. Before that, silicone implants were also used. However, due to concerns for silicone causing cancer as well as autoimmune disease, they were taken off the market. Therefore, large stale --- scale studies were performed to determine the safety of silicone implants. And since that time, multiple sho --- studies have been shown that are independent of biased groups, such as plastic surgeons, to show that there’re no connection between using silicone implants and the development of cancer as well as autoimmune disease.
Veamos los tipos de implante disponibles. En 1992, se aprobaron los implantes salinos. Hasta entonces se utilizaban implantes de gel de silicona. Ese año, la FDA aprobó el uso de implantes salinos como reemplazo de los implantes de silicona. Debido a la preocupación de que estos pudieran causar cáncer y enfermedades autoinmunes, fueron retirados del mercado. Posteriormente se realizaron estudios a gran escala para determinar su seguridad. Desde entonces, varios estudios independientes y separados de los grupos de interés, como los cirujanos plásticos, demostraron que no existe ninguna relación entre el uso de implantes de silicona y el desarrollo de cáncer y de enfermedades autoinmunes.
So in 2006, the FDA reversed the ban on silicone breast implants and now, both implants are available for patients to use and they are deemed safe for breast reconstruction. Depending on shapes, as well as sizes, that are necessary will help determine if a saline or silicone implant is used, as well as patient preference.
En 2006, la FDA revocó su prohibición de usar implantes mamarios de silicona y ahora las pacientes disponen de ambos tipos, considerados seguros para la reconstrucción mamaria. La forma y el tamaño de la mama, así como las preferencias de la paciente, ayudan a determinar si debe usarse un implante de solución salina o de silicona.
15
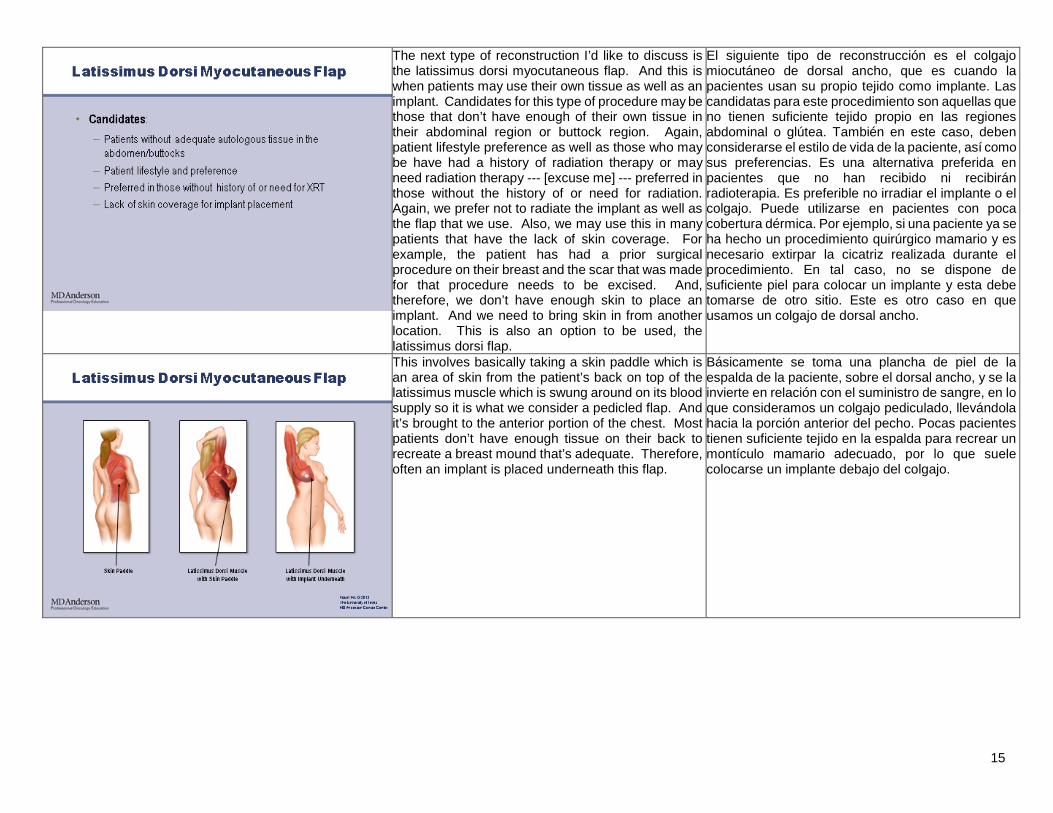
The next type of reconstruction I’d like to discuss is the latissimus dorsi myocutaneous flap. And this is when patients may use their own tissue as well as an implant. Candidates for this type of procedure may be those that don’t have enough of their own tissue in their abdominal region or buttock region. Again, patient lifestyle preference as well as those who may be have had a history of radiation therapy or may need radiation therapy --- [excuse me] --- preferred in those without the history of or need for radiation. Again, we prefer not to radiate the implant as well as the flap that we use. Also, we may use this in many patients that have the lack of skin coverage. For example, the patient has had a prior surgical procedure on their breast and the scar that was made for that procedure needs to be excised. And, therefore, we don’t have enough skin to place an implant. And we need to bring skin in from another location. This is also an option to be used, the latissimus dorsi flap.
El siguiente tipo de reconstrucción es el colgajo miocutáneo de dorsal ancho, que es cuando la pacientes usan su propio tejido como implante. Las candidatas para este procedimiento son aquellas que no tienen suficiente tejido propio en las regiones abdominal o glútea. También en este caso, deben considerarse el estilo de vida de la paciente, así como sus preferencias. Es una alternativa preferida en pacientes que no han recibido ni recibirán radioterapia. Es preferible no irradiar el implante o el colgajo. Puede utilizarse en pacientes con poca cobertura dérmica. Por ejemplo, si una paciente ya se ha hecho un procedimiento quirúrgico mamario y es necesario extirpar la cicatriz realizada durante el procedimiento. En tal caso, no se dispone de suficiente piel para colocar un implante y esta debe tomarse de otro sitio. Este es otro caso en que usamos un colgajo de dorsal ancho.
This involves basically taking a skin paddle which is an area of skin from the patient’s back on top of the latissimus muscle which is swung around on its blood supply so it is what we consider a pedicled flap. And it’s brought to the anterior portion of the chest. Most patients don’t have enough tissue on their back to recreate a breast mound that’s adequate. Therefore, often an implant is placed underneath this flap.
Básicamente se toma una plancha de piel de la espalda de la paciente, sobre el dorsal ancho, y se la invierte en relación con el suministro de sangre, en lo que consideramos un colgajo pediculado, llevándola hacia la porción anterior del pecho. Pocas pacientes tienen suficiente tejido en la espalda para recrear un montículo mamario adecuado, por lo que suele colocarse un implante debajo del colgajo.

16
The advantage of this is that it --- they may create a more natural apparing --- appearing breast shape than an implant alone because you’ve extra layers including the latissimus muscle there that will hide some of the contour of the implant. The scar can be hidden usually along the bra line depending upon the amount of tissue that you need. Again, it allows extra coverage of the implant to protect it from that capsular contracture as well as seeing the contour of the implant. And again, it may allow a one-stage procedure in which we perform the flap as well as place an imme --- immediate implant.
La ventaja es que permite crear una mama de forma más natural que usando solamente un implante, porque hay capas adicionales, incluido el dorsal ancho, que ocultan parcialmente el contorno del implante. La cicatriz usualmente puede ocultarse a lo largo de la línea del sostén, según la cantidad de tejido necesaria. Con esta cobertura adicional del implante, además de ocultar su contorno se lo protege de la contractura capsular. Esto a veces puede hacerse en un único procedimiento, en el que se practica el colgajo y se coloca un implante inmediato.
The disadvantages are --- are that it’s a longer surgical procedure. It does involve additional scarring on a patient’s body and there may be some bulkiness under the arm where the muscle is transferred. There also are complications just related to harvesting of that tissue from the back including flap loss as well problems where we take the flap from, including seromas, so donor site morbidity. It does require a longer hospitalization and longer recovery time for patients.
Como desventaja, es un procedimiento más prolongado. Produce cicatrices adicionales en el cuerpo de la paciente y puede haber cierto volumen debajo del brazo, donde se transfiere el músculo. Puede haber complicaciones relacionadas con la toma de tejido dorsal, como pérdida del colgajo, problemas en la zona de recolección, como seromas, y morbilidad del área donante. Además requiere una hospitalización y una recuperación más prolongadas.
17
The last form of reconstruction I’d like to discuss is the transverse rectus abdominis myocutaneous flap, also, know as the TRAM flap. As we’ve gotten more advanced surgically, we have leaned more towards taking less muscle and taking these flaps on their blood supply as free flaps, almost as a transplant. So there’s the pedicled TRAM which involves keeping the blood supply intact and just rotating the fla --- flap from the abdomen to the upper chest. Free TRAM involves removing it from its blood supply and transferring it to the chest. And these three remaining ones ---,[excuse me] --- are sparing the muscle or not taking any of that muscle for transfer. So again, the trend has been towards minimizing the abdominal donor site on the patient by reducing the amount of muscle that is taken from the abdomen.
La última forma de reconstrucción es el colgajo miocutáneo del recto abdominal transverso, también llamado colgajo TRAM. Debido a los adelantos quirúrgicos, la tendencia actual es tomar menos músculo y utilizar los colgajos conectados al suministro de sangre como colgajos libres, casi como un trasplante. En el TRAM pediculado se conserva el suministro de sangre y el colgajo se gira desde el abdomen hasta la parte superior del pecho. El TRAM libre implica cortar el suministro de sangre y transferirlo al pecho. Los tres restantes preservan el músculo o directamente no lo transfieren. Nuevamente, la tendencia es minimizar la zona donante abdominal en la paciente reduciendo la cantidad de músculo tomada del abdomen.
The advantage of this flap is does it --- it does give you a very natural breast shape and behavior, so it will gain weight / lose weight with the patient, is affected by gravity over time. It has a natural consistency. Some patients think of it as their tummy tuck, but it is more extensive than an abdominoplasty. However, from the outside it does appear that way. And, they do get rid of some of the redundant abdominal skin and tissue. And also, patients may not want a foreign body, may not have to deal with implant maintenance as well as having a foreign body.
La ventaja de este colgajo es una mama de forma y comportamiento muy naturales, que aumenta o reduce su peso junto con la paciente, y con el tiempo es afectado por la gravedad. Tiene una consistencia natural. Algunas pacientes la consideran una reducción de abdomen, pero es más amplia que una abdominoplastia, aunque externamente parece ser similar pues elimina parte del exceso de piel y tejido abdominales. Algunas pacientes prefieren no recibir un cuerpo extraño y adicionalmente evitar el mantenimiento del implante.

18
The disadvantages are that there is a longer surgical procedure. It does involve additional scarring on the abdomen. Again, with any kind of tissue that you take from a patient there can be complications with harvesting of that tissue including flap loss and morbidity to the area where you take the tissue from, including hernias and bulges. It also involves longer hospitalization and longer recovery times.
Las desventajas son un procedimiento quirúrgico más largo. Formación de cicatrices adicionales en el abdomen. Con cualquier transferencia de tejido puede haber complicaciones en la recolección, como la pérdida del colgajo y morbilidad en la zona donde se extracción, como hernias y protuberancias. También implica más tiempo de hospitalización y de recuperación.
Just looking at a picture of a patient’s anatomy here, the rectus muscle is here. The blood vessel that we use to take these flaps from lies underneath the muscle here. When we perform free flaps, we use vessels that are along the chest wall, the internal mammary vessels or the thoracodorsal vessels. They are both the deep inferior epigastric vessels which are what most flaps are based on, including the TRAM flap. There’s also the superf --- superficial inferior epigastric vessels which lie anterior to the abdominal fascia.
Veamos esta imagen anatómica. Este es el recto abdominal. El vaso sanguíneo del que separamos el colgajo se encuentra debajo del músculo. Con los colgajos libres, usamos vasos que están a lo largo de la pared torácica, los vasos intramamarios o los vasos toracodorsales. Tenemos los vasos epigástricos inferiores profundos, utilizados en la mayoría de los colgajos, como el colgajo TRAM, y los vasos epigástricos inferiores superficiales que se encuentran delante de la fascia abdominal.
19
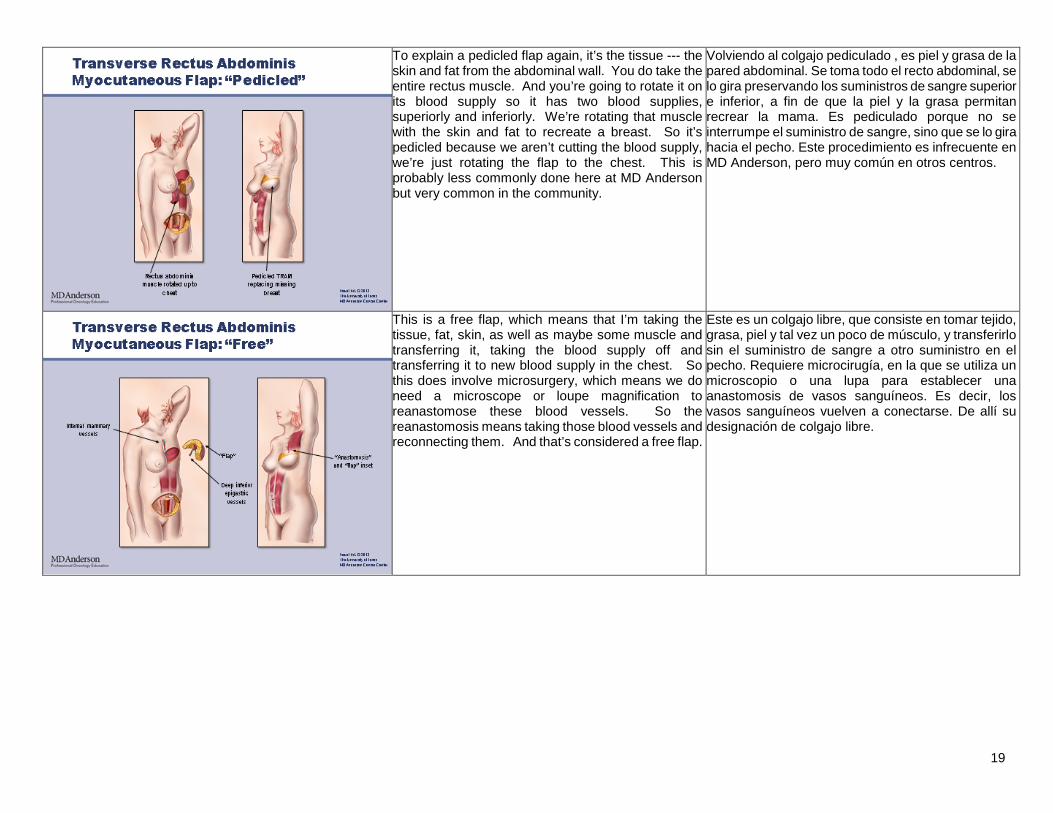
To explain a pedicled flap again, it’s the tissue --- the skin and fat from the abdominal wall. You do take the entire rectus muscle. And you’re going to rotate it on its blood supply so it has two blood supplies, superiorly and inferiorly. We’re rotating that muscle with the skin and fat to recreate a breast. So it’s pedicled because we aren’t cutting the blood supply, we’re just rotating the flap to the chest. This is probably less commonly done here at MD Anderson but very common in the community.
Volviendo al colgajo pediculado , es piel y grasa de la pared abdominal. Se toma todo el recto abdominal, se lo gira preservando los suministros de sangre superior e inferior, a fin de que la piel y la grasa permitan recrear la mama. Es pediculado porque no se interrumpe el suministro de sangre, sino que se lo gira hacia el pecho. Este procedimiento es infrecuente en MD Anderson, pero muy común en otros centros.
This is a free flap, which means that I’m taking the tissue, fat, skin, as well as maybe some muscle and transferring it, taking the blood supply off and transferring it to new blood supply in the chest. So this does involve microsurgery, which means we do need a microscope or loupe magnification to reanastomose these blood vessels. So the reanastomosis means taking those blood vessels and reconnecting them. And that’s considered a free flap.
Este es un colgajo libre, que consiste en tomar tejido, grasa, piel y tal vez un poco de músculo, y transferirlo sin el suministro de sangre a otro suministro en el pecho. Requiere microcirugía, en la que se utiliza un microscopio o una lupa para establecer una anastomosis de vasos sanguíneos. Es decir, los vasos sanguíneos vuelven a conectarse. De allí su designación de colgajo libre.
20
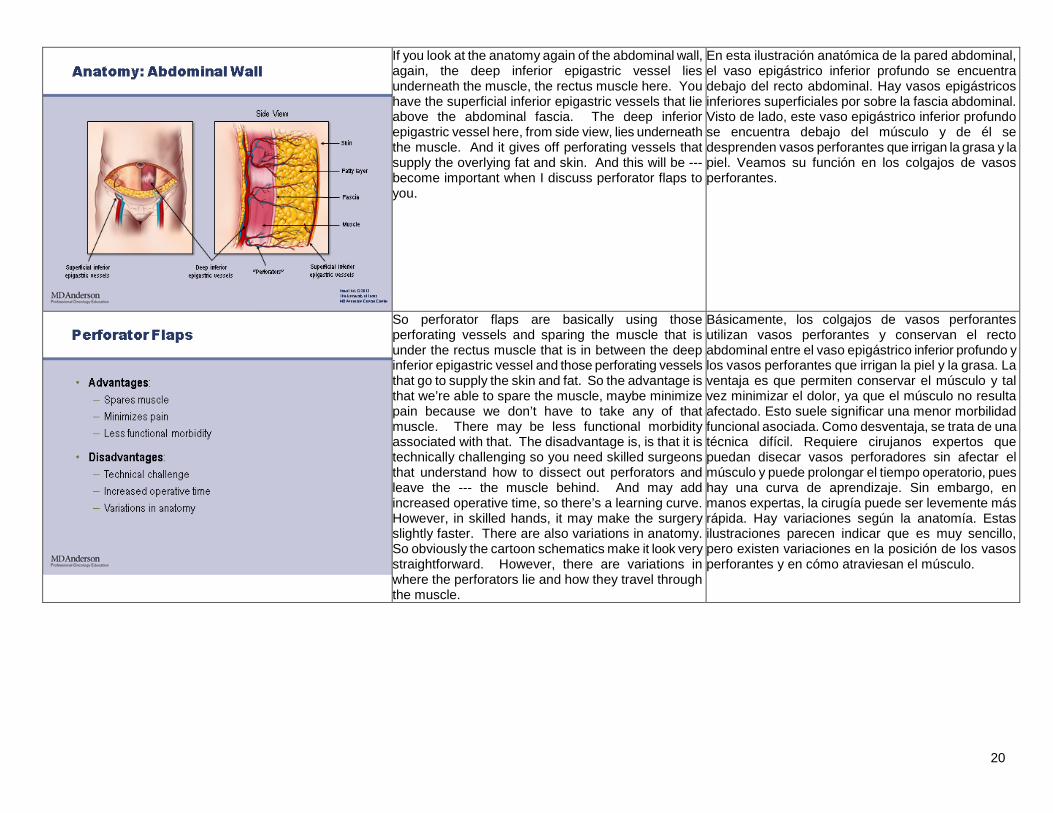
If you look at the anatomy again of the abdominal wall, again, the deep inferior epigastric vessel lies underneath the muscle, the rectus muscle here. You have the superficial inferior epigastric vessels that lie above the abdominal fascia. The deep inferior epigastric vessel here, from side view, lies underneath the muscle. And it gives off perforating vessels that supply the overlying fat and skin. And this will be --- become important when I discuss perforator flaps to you.
En esta ilustración anatómica de la pared abdominal, el vaso epigástrico inferior profundo se encuentra debajo del recto abdominal. Hay vasos epigástricos inferiores superficiales por sobre la fascia abdominal. Visto de lado, este vaso epigástrico inferior profundo se encuentra debajo del músculo y de él se desprenden vasos perforantes que irrigan la grasa y la piel. Veamos su función en los colgajos de vasos perforantes.
So perforator flaps are basically using those perforating vessels and sparing the muscle that is under the rectus muscle that is in between the deep inferior epigastric vessel and those perforating vessels that go to supply the skin and fat. So the advantage is that we’re able to spare the muscle, maybe minimize pain because we don’t have to take any of that muscle. There may be less functional morbidity associated with that. The disadvantage is, is that it is technically challenging so you need skilled surgeons that understand how to dissect out perforators and leave the --- the muscle behind. And may add increased operative time, so there’s a learning curve. However, in skilled hands, it may make the surgery slightly faster. There are also variations in anatomy. So obviously the cartoon schematics make it look very straightforward. However, there are variations in where the perforators lie and how they travel through the muscle.
Básicamente, los colgajos de vasos perforantes utilizan vasos perforantes y conservan el recto abdominal entre el vaso epigástrico inferior profundo y los vasos perforantes que irrigan la piel y la grasa. La ventaja es que permiten conservar el músculo y tal vez minimizar el dolor, ya que el músculo no resulta afectado. Esto suele significar una menor morbilidad funcional asociada. Como desventaja, se trata de una técnica difícil. Requiere cirujanos expertos que puedan disecar vasos perforadores sin afectar el músculo y puede prolongar el tiempo operatorio, pues hay una curva de aprendizaje. Sin embargo, en manos expertas, la cirugía puede ser levemente más rápida. Hay variaciones según la anatomía. Estas ilustraciones parecen indicar que es muy sencillo, pero existen variaciones en la posición de los vasos perforantes y en cómo atraviesan el músculo.

21
This just also gives you an idea of what the flaps look like both schematically as well as in the operating room. So a superficial inferior epigastric artery flap is basically a flap that takes that superficial inferior epigastric artery above the fascia, takes the overlying fat and skin. And we don’t have to go through the fascia underneath or take any muscle. The deep inferior epigastric artery perforator flap involves basically dissecting out those perforators that are leading to that deep inferior epigastric vessel. We maintain the rectus muscle and just split it to get these vessels out. Again, here’s it in the operating room. These are your perforators here, going down to the main vessel, the deep inferior epigastric vessel. Muscle-sparing means that we may not take the entire muscle. So we take a portion of the muscle that may contain these perforators. So you may ask, “Why would we take any muscle if we can dissect these perforators out?” Well, oftentimes, these perforators may take a route that isn’t straight up and that they go through a portion of the muscle so it’s better just to take that muscle with it, preserve the muscle so that we don’t injure those perforators because that is our blood supply to our flap. So again, this just shows where we can leave behind the rectus muscle both laterally and medial and just take a portion of the muscle intervening so that we do preserve those vessels.
Esta diapositiva muestra esquemas de los colgajos, así como su aspecto en la sala de operaciones. El colgajo de arteria epigástrica inferior superficial lleva esta arteria por encima de la fascia, junto con la grasa y la piel que la recubren. No es necesario llegar hasta la fascia ni retirar músculo. El colgajo de vasos perforantes de la arteria epigástrica inferior requiere disecar los vasos perforantes que llegan a esta arteria. Se mantiene el recto abdominal y se divide para separar los vasos. Así luce en la sala de operaciones. Estos son los vasos perforantes que llegan al vaso principal, el vaso epigástrico inferior profundo. Conservación muscular significa que no se toma todo el músculo, sino una porción que puede contener estos vasos perforantes. ¿Por qué tomar parte del músculo si es posible disecar los vasos perforantes? Con frecuencia, estos vasos no siguen un trayecto directo y atraviesan parte del músculo, en cuyo caso es mejor tomarlos junto con el músculo, preservándolo para no lesionar los vasos que abastecen sangre al colgajo. Vemos aquí dónde es posible dejar el recto abdominal, tanto lateral como medial, y tomar solamente una porción del músculo en cuestión a fin de preservar los vasos.
So again, “Who is a candidate for this type of flap?” You want someone who is healthy, meaning not multiple comorbidities. No previous abdominal surgery, and what I mean by this is, they can have C-sections. But you don’t want big open cholecystectomy scars, things like that that may compromise or may have injured the blood vessels that you’re going to use to transfer these flaps. Multiparous, because often women that have had multiple children have that extra redundant tissue that we need and that laxity. Prefer nonsmokers, just because of blood supply issues. If we are doing a transplant in the sense of taking something off its blood supply and transferring it, we don’t want to have any vasoconstriction that could compromise blood suppl --- blood supply to these flaps. Also, again, we don’t want to have any plans for radiotherapy. You
¿Quiénes son candidatas adecuadas para este tipo de colgajo? Las pacientes sanas, es decir, sin comorbilidades múltiples, y que no hayan tenido cirugía abdominal, principalmente cesáreas. Deben evitarse casos con cicatrices de colecistectomía abierta, que pueden comprometer o haber lesionado los vasos sanguíneos necesarios para transferir el colgajo. Son preferibles las multíparas, ya que a menudo una mujer que ha tenido varios hijos tiene tejido redundante y más laxitud. Se prefieren las no fumadoras, para evitar problemas de suministro sanguíneo. Al hacer un trasplante, en el sentido de separar un fragmento de su abastecimiento de sangre y transferirlo, debe prevenirse la vasoconstricción que podría comprometer el suministro de sangre del colgajo. Preferimos que no haya planes de radioterapia. Necesitamos pacientes que sigan el
22
need a very compliant patient because what we don’t want is someone who starts down this road and then is not interested in continuing, because it is a long process of recovery and requires wound care, drain care, and so forth. Also, you want someone that has a BMI of less than 35. And what I mean by this is, you want someone that has enough tissue that you can reconstruct a breast. But you don’t want them to be too morbidly obese because they are at higher risk for complications in the abdominal region, inclu --- including hernias and bulges.
protocolo, para evitar que se inicie el procedimiento y luego pierdan interés, pues el proceso de recuperación es prolongado y requiere cuidar de las heridas, atender los drenajes, etc. Queremos pacientes con índices de masa corporal menor de 35, pero con suficiente tejido como para permitir una reconstrucción mamaria. Deben evitarse las pacientes con obesidad mórbida debido al mayor riesgo de complicaciones en la región abdominal, como hernias y protuberancias.
You can do some preoperative planning. So oftentimes, we will look for the perforators. Often, if a patient has had prior surgery, you may want to assess that the blood vessels haven’t been injured by prior surgery. So, different techniques can be used, using a Doppler as well as C --- CT angiography, MRI angiography. Some --- some physicians prefer nothing, and just to get in the operating room and take a look. It may be more beneficial, as I said, with those that have had prior abdominal surgeries, possibly liposuction. Also, it may help speed up their procedure because you know where the blood vessels are that you may want to identify to harvest your flap.
Se requiere una planificación preoperatoria. A veces examinamos los vasos perforantes. Si una paciente ha tenido una cirugía, posiblemente convenga evaluar los vasos para comprobar que no hayan sido lesionados. Pueden utilizarse diversas técnicas, como un estudio Doppler, o una angiografía computada o magnética. Algunos médicos omiten este paso y evalúan la situación en la sala de operaciones. Puede resultar más beneficioso si la paciente ya ha tenido cirugía abdominal o incluso liposucción. Además, puede acelerar el procedimiento, pues la posición de los vasos sanguíneos ya es conocida al extraer el colgajo.
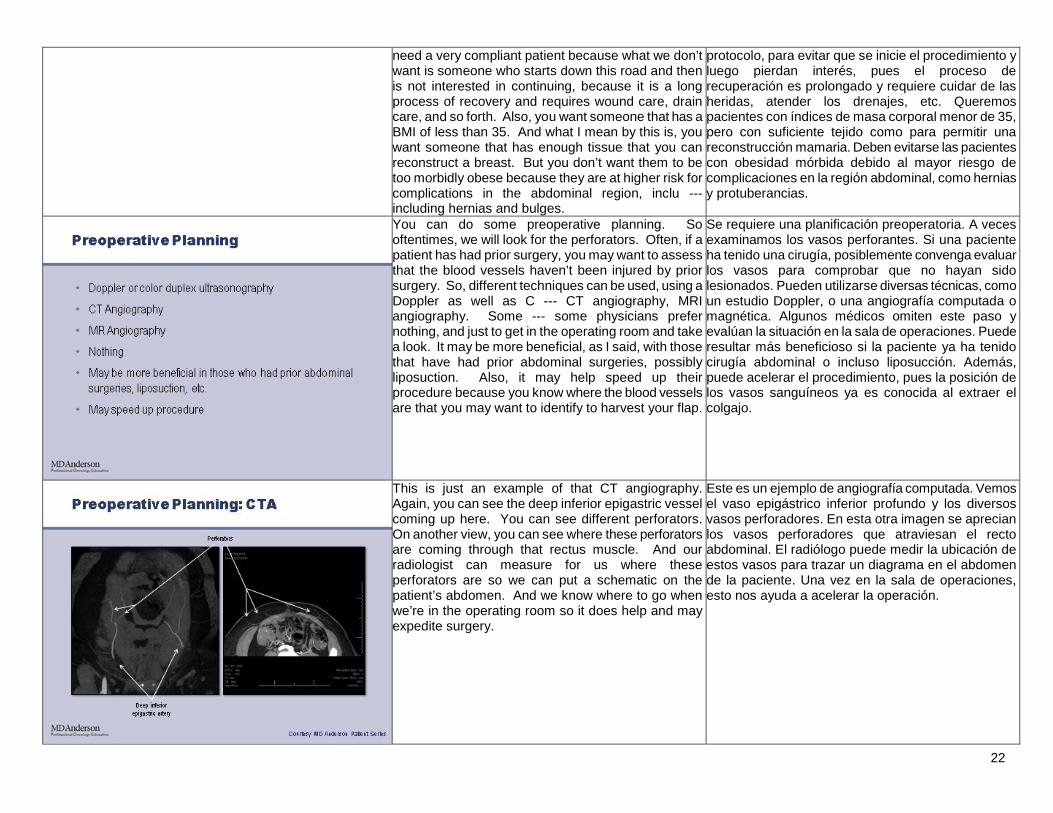
This is just an example of that CT angiography. Again, you can see the deep inferior epigastric vessel coming up here. You can see different perforators. On another view, you can see where these perforators are coming through that rectus muscle. And our radiologist can measure for us where these perforators are so we can put a schematic on the patient’s abdomen. And we know where to go when we’re in the operating room so it does help and may expedite surgery.
Este es un ejemplo de angiografía computada. Vemos el vaso epigástrico inferior profundo y los diversos vasos perforadores. En esta otra imagen se aprecian los vasos perforadores que atraviesan el recto abdominal. El radiólogo puede medir la ubicación de estos vasos para trazar un diagrama en el abdomen de la paciente. Una vez en la sala de operaciones, esto nos ayuda a acelerar la operación.
23
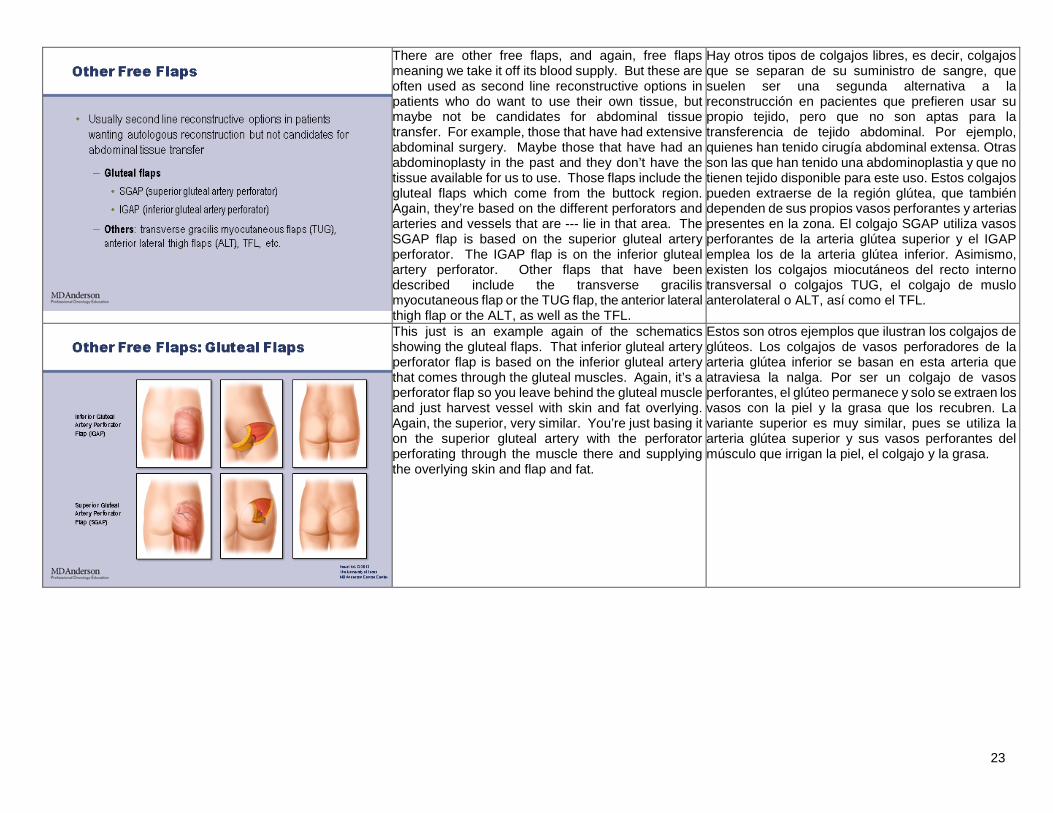
There are other free flaps, and again, free flaps meaning we take it off its blood supply. But these are often used as second line reconstructive options in patients who do want to use their own tissue, but maybe not be candidates for abdominal tissue transfer. For example, those that have had extensive abdominal surgery. Maybe those that have had an abdominoplasty in the past and they don’t have the tissue available for us to use. Those flaps include the gluteal flaps which come from the buttock region. Again, they’re based on the different perforators and arteries and vessels that are --- lie in that area. The SGAP flap is based on the superior gluteal artery perforator. The IGAP flap is on the inferior gluteal artery perforator. Other flaps that have been described include the transverse gracilis myocutaneous flap or the TUG flap, the anterior lateral thigh flap or the ALT, as well as the TFL.
Hay otros tipos de colgajos libres, es decir, colgajos que se separan de su suministro de sangre, que suelen ser una segunda alternativa a la reconstrucción en pacientes que prefieren usar su propio tejido, pero que no son aptas para la transferencia de tejido abdominal. Por ejemplo, quienes han tenido cirugía abdominal extensa. Otras son las que han tenido una abdominoplastia y que no tienen tejido disponible para este uso. Estos colgajos pueden extraerse de la región glútea, que también dependen de sus propios vasos perforantes y arterias presentes en la zona. El colgajo SGAP utiliza vasos perforantes de la arteria glútea superior y el IGAP emplea los de la arteria glútea inferior. Asimismo, existen los colgajos miocutáneos del recto interno transversal o colgajos TUG, el colgajo de muslo anterolateral o ALT, así como el TFL.
This just is an example again of the schematics showing the gluteal flaps. That inferior gluteal artery perforator flap is based on the inferior gluteal artery that comes through the gluteal muscles. Again, it’s a perforator flap so you leave behind the gluteal muscle and just harvest vessel with skin and fat overlying. Again, the superior, very similar. You’re just basing it on the superior gluteal artery with the perforator perforating through the muscle there and supplying the overlying skin and flap and fat.
Estos son otros ejemplos que ilustran los colgajos de glúteos. Los colgajos de vasos perforadores de la arteria glútea inferior se basan en esta arteria que atraviesa la nalga. Por ser un colgajo de vasos perforantes, el glúteo permanece y solo se extraen los vasos con la piel y la grasa que los recubren. La variante superior es muy similar, pues se utiliza la arteria glútea superior y sus vasos perforantes del músculo que irrigan la piel, el colgajo y la grasa.

24
It’s really important to tell patients that it is a multi-stage process. So the first stage involves creating that breast mound either with a flap, an implant, or the combination of both. The average interval time usually to the next stage may be three months. However, this may be increased if they do need chemotherapy, radiation therapy, or they do have complications. Again, this also is based on patient preference. Maybe they have a wedding coming up and they want to wait longer. The second stage is less invasive, involving refinement and balancing proce --- procedures. This may involve a revision to the reconstruction. A symmetry procedure to the contralateral breast if they, for example, doing a lift or a reduction of that breast, maybe placing an implant to make it look like the reconstructed breast, also revising any of the donor sites. So if there’re widened scars or excess tissue, we do that at that time. Again, we would wait two to three months. At that time, we may repeat if they’re not happy with the symmetry or we feel like we can do a better job with it. And then we go on to stage 3 which involves making a nipple and areola. Again, many patients may not want a nipple. They may not want an areolar reconstruction, or they may not want these other stages so it’s really based on patient preference as well as symmetry.
Es importante informar a las pacientes que es un proceso de varias etapas. La primera es la creación del montículo mamario, ya sea con un colgajo, un implante o una combinación. El intervalo medio hasta la siguiente etapa suele ser de tres meses, pero puede aumentar si se necesita quimioterapia, radioterapia o si ocurren complicaciones. Esto depende de las preferencias de la paciente, pues tal vez deseen esperar hasta después de algún acontecimiento. La segunda etapa es menos invasiva, y son los procedimientos de retoque y equilibrio. Puede requerir una corrección de la reconstrucción, como modificar la simetría de la mama contralateral levantándola o reduciéndola, o colocando un implante para asemejarla a la mama reconstruida, y una revisión de los sitios donantes. Por ejemplo, si las cicatrices se han agrandado o hay exceso de tejido. Luego esperamos otros dos o tres meses, y podemos repetir la corrección si la simetría aún no es satisfactoria o es pasible de ser mejorada. Después viene la tercera etapa, que es la formación del pezón y la areola. Algunas pacientes no desean un pezón, no quieren una reconstrucción areolar ni participar en ninguna otra etapa posterior, de modo que esto depende de las preferencias y de la simetría.
Revision and symmetry procedures, again, these are often performed on the opposite breast to maybe match a reconstructed breast. So again, we use many of the procedures we use in cosmetic surgery. For example, breast augmentation where you’re putting an implant under someone’s own breast to make it larger. A breast lift, which means we’re removing some of the skin and making it look more youthful or a breast reduction where we may be decreasing the size of the breast. We do this again to match a breast that has also had a previous lumpectomy and radiation therapy. So often patients come in, they don’t want a complete reconstruction; they just want us to make the breast without cancer look closer to the size of the breast that has had breast cancer and has undergone surgery.
Suelen realizarse nuevos procedimientos de corrección y simetría en el otro seno para igualar la mama reconstruida. Para ello utilizamos muchos de los procedimientos de la cirugía estética. Por ejemplo, un aumento mamario colocando un implante en el seno natural para agrandarlo. Un levantamiento de seno, quitando parte de la piel para darle un aspecto más juvenil, o una reducción del seno para obtener una mama más pequeña. Esto también se realiza para igualar mamas que han recibido una nodulectomía o radioterapia. A veces la paciente no quiere una reconstrucción completa, y solo desea que la mama sana se asemeje a la mama reconstruida que se ha tenido cáncer y fue sometida a cirugía.
25
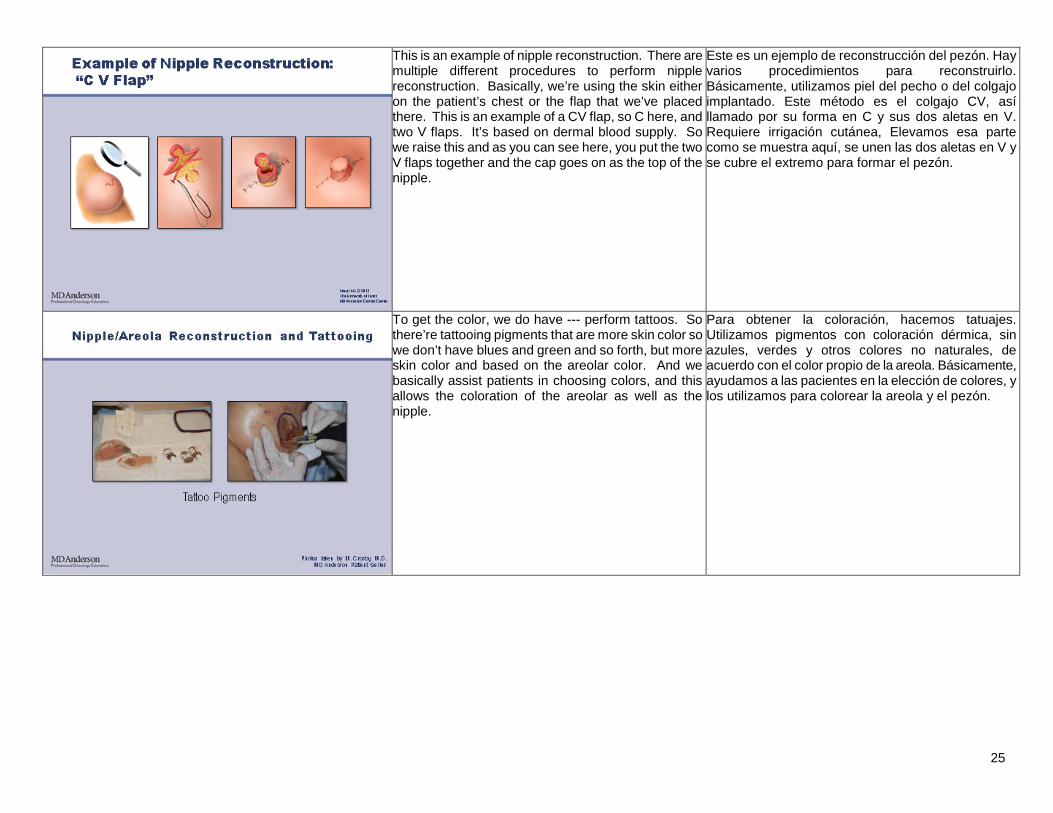
This is an example of nipple reconstruction. There are multiple different procedures to perform nipple reconstruction. Basically, we’re using the skin either on the patient’s chest or the flap that we’ve placed there. This is an example of a CV flap, so C here, and two V flaps. It’s based on dermal blood supply. So we raise this and as you can see here, you put the two V flaps together and the cap goes on as the top of the nipple.
Este es un ejemplo de reconstrucción del pezón. Hay varios procedimientos para reconstruirlo. Básicamente, utilizamos piel del pecho o del colgajo implantado. Este método es el colgajo CV, así llamado por su forma en C y sus dos aletas en V. Requiere irrigación cutánea, Elevamos esa parte como se muestra aquí, se unen las dos aletas en V y se cubre el extremo para formar el pezón.
To get the color, we do have --- perform tattoos. So there’re tattooing pigments that are more skin color so we don’t have blues and green and so forth, but more skin color and based on the areolar color. And we basically assist patients in choosing colors, and this allows the coloration of the areolar as well as the nipple.
Para obtener la coloración, hacemos tatuajes. Utilizamos pigmentos con coloración dérmica, sin azules, verdes y otros colores no naturales, de acuerdo con el color propio de la areola. Básicamente, ayudamos a las pacientes en la elección de colores, y los utilizamos para colorear la areola y el pezón.
26
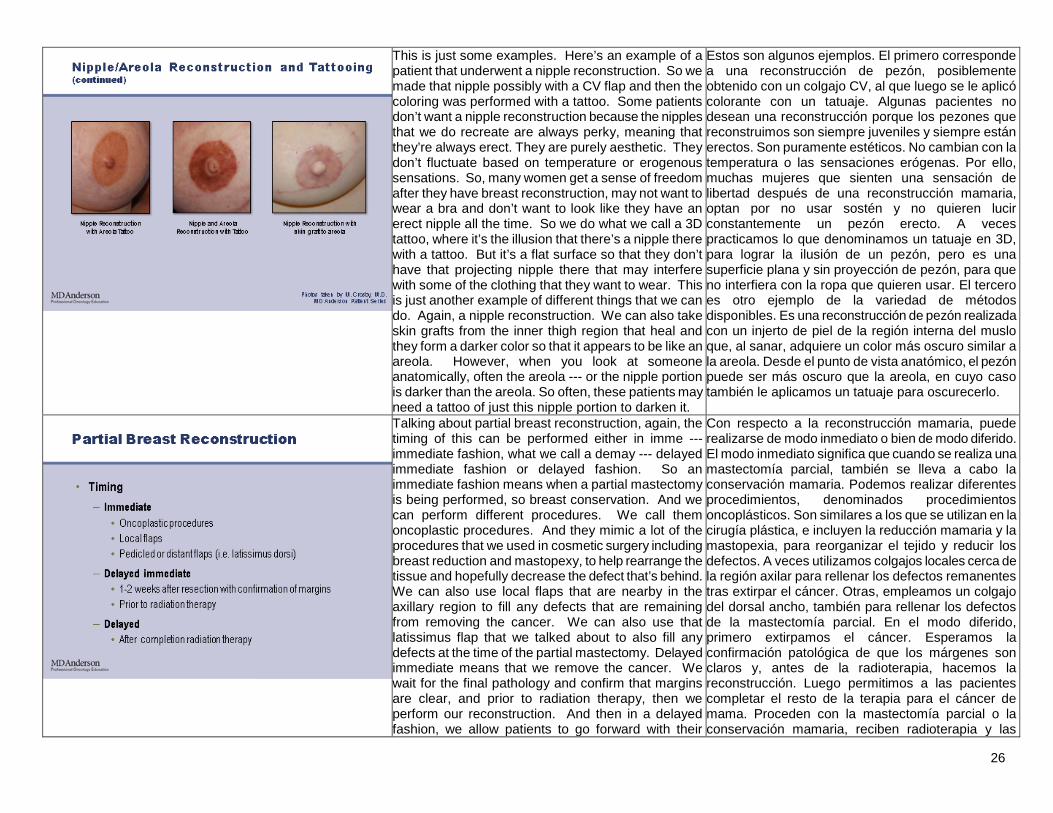
This is just some examples. Here’s an example of a patient that underwent a nipple reconstruction. So we made that nipple possibly with a CV flap and then the coloring was performed with a tattoo. Some patients don’t want a nipple reconstruction because the nipples that we do recreate are always perky, meaning that they’re always erect. They are purely aesthetic. They don’t fluctuate based on temperature or erogenous sensations. So, many women get a sense of freedom after they have breast reconstruction, may not want to wear a bra and don’t want to look like they have an erect nipple all the time. So we do what we call a 3D tattoo, where it’s the illusion that there’s a nipple there with a tattoo. But it’s a flat surface so that they don’t have that projecting nipple there that may interfere with some of the clothing that they want to wear. This is just another example of different things that we can do. Again, a nipple reconstruction. We can also take skin grafts from the inner thigh region that heal and they form a darker color so that it appears to be like an areola. However, when you look at someone anatomically, often the areola --- or the nipple portion is darker than the areola. So often, these patients may need a tattoo of just this nipple portion to darken it.
Estos son algunos ejemplos. El primero corresponde a una reconstrucción de pezón, posiblemente obtenido con un colgajo CV, al que luego se le aplicó colorante con un tatuaje. Algunas pacientes no desean una reconstrucción porque los pezones que reconstruimos son siempre juveniles y siempre están erectos. Son puramente estéticos. No cambian con la temperatura o las sensaciones erógenas. Por ello, muchas mujeres que sienten una sensación de libertad después de una reconstrucción mamaria, optan por no usar sostén y no quieren lucir constantemente un pezón erecto. A veces practicamos lo que denominamos un tatuaje en 3D, para lograr la ilusión de un pezón, pero es una superficie plana y sin proyección de pezón, para que no interfiera con la ropa que quieren usar. El tercero es otro ejemplo de la variedad de métodos disponibles. Es una reconstrucción de pezón realizada con un injerto de piel de la región interna del muslo que, al sanar, adquiere un color más oscuro similar a la areola. Desde el punto de vista anatómico, el pezón puede ser más oscuro que la areola, en cuyo caso también le aplicamos un tatuaje para oscurecerlo.
Talking about partial breast reconstruction, again, the timing of this can be performed either in imme --- immediate fashion, what we call a demay --- delayed immediate fashion or delayed fashion. So an immediate fashion means when a partial mastectomy is being performed, so breast conservation. And we can perform different procedures. We call them oncoplastic procedures. And they mimic a lot of the procedures that we used in cosmetic surgery including breast reduction and mastopexy, to help rearrange the tissue and hopefully decrease the defect that’s behind. We can also use local flaps that are nearby in the axillary region to fill any defects that are remaining from removing the cancer. We can also use that latissimus flap that we talked about to also fill any defects at the time of the partial mastectomy. Delayed immediate means that we remove the cancer. We wait for the final pathology and confirm that margins are clear, and prior to radiation therapy, then we perform our reconstruction. And then in a delayed fashion, we allow patients to go forward with their
Con respecto a la reconstrucción mamaria, puede realizarse de modo inmediato o bien de modo diferido. El modo inmediato significa que cuando se realiza una mastectomía parcial, también se lleva a cabo la conservación mamaria. Podemos realizar diferentes procedimientos, denominados procedimientos oncoplásticos. Son similares a los que se utilizan en la cirugía plástica, e incluyen la reducción mamaria y la mastopexia, para reorganizar el tejido y reducir los defectos. A veces utilizamos colgajos locales cerca de la región axilar para rellenar los defectos remanentes tras extirpar el cáncer. Otras, empleamos un colgajo del dorsal ancho, también para rellenar los defectos de la mastectomía parcial. En el modo diferido, primero extirpamos el cáncer. Esperamos la confirmación patológica de que los márgenes son claros y, antes de la radioterapia, hacemos la reconstrucción. Luego permitimos a las pacientes completar el resto de la terapia para el cáncer de mama. Proceden con la mastectomía parcial o la conservación mamaria, reciben radioterapia y las
27
remaining portion of their therapy for the breast cancer, so they have their partial mastectomy or breast conservation, go on to have radiation therapy, and then we see them in a delayed fashion to improve any contour deformities that may have resulted from the surgery as well as the radiation therapy.
atendemos para mejorar cualquier deformación del contorno que haya resultado de la cirugía o de la radioterapia.
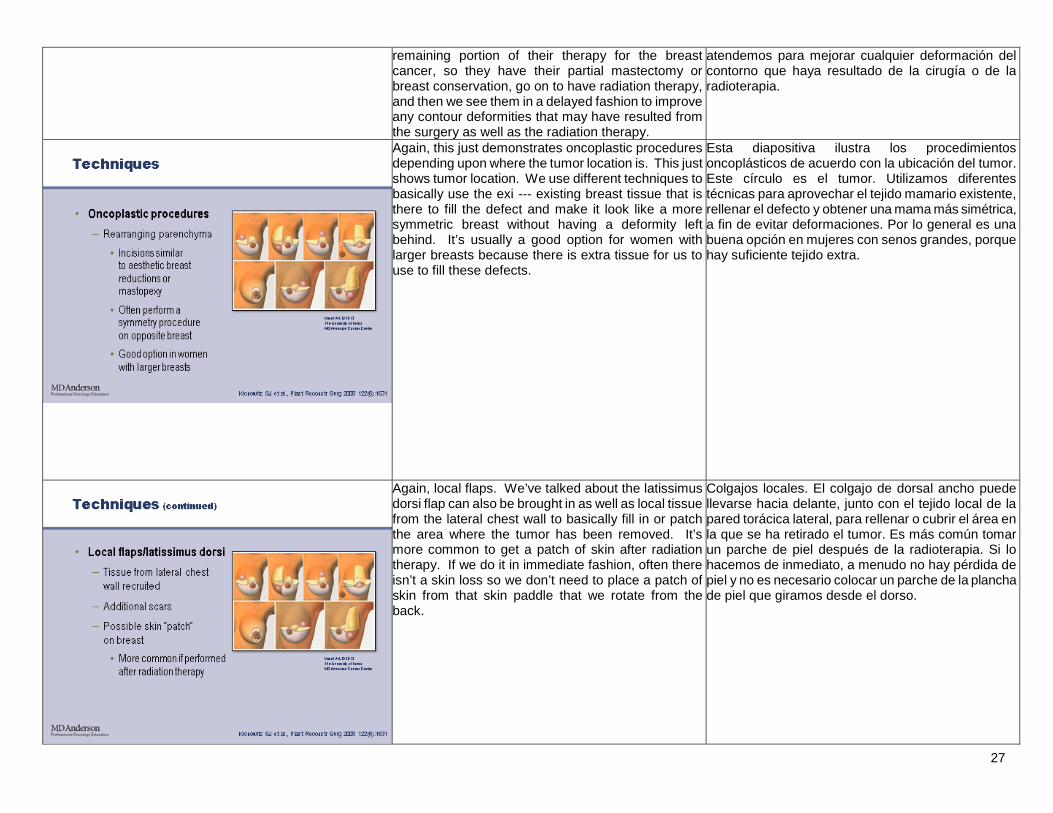
Again, this just demonstrates oncoplastic procedures depending upon where the tumor location is. This just shows tumor location. We use different techniques to basically use the exi --- existing breast tissue that is there to fill the defect and make it look like a more symmetric breast without having a deformity left behind. It’s usually a good option for women with larger breasts because there is extra tissue for us to use to fill these defects.
Esta diapositiva ilustra los procedimientos oncoplásticos de acuerdo con la ubicación del tumor. Este círculo es el tumor. Utilizamos diferentes técnicas para aprovechar el tejido mamario existente, rellenar el defecto y obtener una mama más simétrica, a fin de evitar deformaciones. Por lo general es una buena opción en mujeres con senos grandes, porque hay suficiente tejido extra.
Again, local flaps. We’ve talked about the latissimus dorsi flap can also be brought in as well as local tissue from the lateral chest wall to basically fill in or patch the area where the tumor has been removed. It’s more common to get a patch of skin after radiation therapy. If we do it in immediate fashion, often there isn’t a skin loss so we don’t need to place a patch of skin from that skin paddle that we rotate from the back.
Colgajos locales. El colgajo de dorsal ancho puede llevarse hacia delante, junto con el tejido local de la pared torácica lateral, para rellenar o cubrir el área en la que se ha retirado el tumor. Es más común tomar un parche de piel después de la radioterapia. Si lo hacemos de inmediato, a menudo no hay pérdida de piel y no es necesario colocar un parche de la plancha de piel que giramos desde el dorso.
28
Fat grafting. This has become a hot topic in the news. This involves basically taking fat harvested from another portion of the patient’s body and injecting it in small amount in different contour concavities or also possibly in radiated, damaged skin. So this is basically reverse liposuction, harvesting it from places patients don’t want. We can then inject it into places where maybe there’re concavities.
Injertos de grasa. Es un tema de actualidad. Básicamente, consiste en extraer grasa de una parte del cuerpo de la paciente e inyectar pequeñas cantidad en concavidades de contorno diferentes, y también en piel irradiada y dañada. Es una liposucción inversa, que toma grasa de lugares donde no es deseada y la inyecta en lugares donde hay concavidades.
We can do this in both complete and partial reconstruction. However, about 40-50% of the fat that we place there is reabsorbed. And what I mean by that, it is a graft so your body has to basically supply blood supply to it. So, therefore, patients may need multiple procedures. It has been used for multiple decades in cosmetic surgical procedures to enlarge lips, to fill nasolabial folds, and we’re just starting to use it in breast reconstruction.
Podemos utilizarla en reconstrucciones completas o parciales. Del 40 al 50% de la grasa inyectada es reabsorbida. Por ser un injerto, el cuerpo debe suministrarle sangre, de modo que las pacientes suelen requerir varios procedimientos. Se ha utilizado durante décadas en diversos procedimientos cosméticos para aumentar los labios, llenar pliegues nasolabiales y ahora en la reconstrucción mamaria.
29
Basically, fat is an ideal filler. We have other fillers in reconstructive surgery as well as cosmetic surgery. But fat is the ideal filler because it’s readily available. It’s easily collected. And there’s minimal morbidity, meaning when we harvest it. However, again, graft loss is common, meaning 20-90% of the graft may be lost requiring multiple procedures.
La grasa es un material de relleno ideal, y, aunque en las cirugías reconstructiva y estética también se utilizan otros, la grasa está fácilmente disponible. Es fácil de recolectar y la morbilidad al extraerla es mínima. Sin embargo, es común una pérdida del injerto del 20 al 90%, lo que requiere procedimientos múltiples.
What is in the grafts that we do place? There are pre-adipocytes as well as mature adipocytes. Graft survival is dependent upon these pre-adipocytes because of their high proliferative ability. Often, the mature adipocytes, if they don’t get adequate blood supply, will often die. However, if they get adequate blood supply, they may survive or de-differentiate.
¿Qué contiene el material injertado? Preadipocitos, así como adipocitos maduros. La supervivencia del injerto depende de los preadipocitos debido a su alta capacidad proliferativa. Si los adipocitos maduros no reciben un suministro adecuado de sangre, a menudo mueren, pero si es adecuado, pueden sobrevivir o desdiferenciarse.
30
We’ve used this as a lipofiller in patients undergoing breast conservation. But we do put this under a protocol at MD Anderson. I think this is still being investigated. It does allow implant coverage so we use it often for rippling in implants. We can correct contour deformities after flaps that are placed. There are people that are looking at this for total breast reconstruction. It’s also been shown to maybe improve the quality as well as soft tissue cover after mastectomy and radiation therapy.
Hemos utilizado este lipomaterial de relleno en la conservación mamaria siguiendo los protocolos de MD Anderson. Aún está en investigación. Hace posible la cobertura del implante y lo usamos para corregir ondulaciones y deformaciones del contorno después de colocar el colgajo. Algunos lo utilizan en la reconstrucción mamaria total. Puede mejorar la calidad y la cobertura de los tejidos blandos después de la mastectomía y la radioterapia.
It has not been shown to interfere with breast cancer detection. There’s no evidence in the current literature to strongly suggest it causing breast cancer or interfering with breast cancer detection. However, I think we’re still investigating this. There have been two cases of breast cancer reported after fat grafting, but no delay in diagnosis or detection as well as treatment. Further studies are evaluating this. There is a slight concern that we may be transferring stem cells. So there is a multilineage differentiation potential for this. It also allows neo --- neovascularization. So we always discuss with the patients that if there is microscopic tumor cells there, that there is a potential that bringing in stem cells as well as growth factors with any kind of tissue we transfer could encourage this tumor to grow. But the studies that are available show no or marginal effects on the probability of post mastectomy local regional recurrence of breast cancer. And one study showed about a seven to almost eight-year follow-up after fat grafting but again, I think we’re still investigating this.
No hay evidencia de que interfiera en la detección del cáncer de mama, ni hay evidencias firmes en la literatura actual de que provoque esta enfermedad. Sin embargo, esto aún está siendo investigado. Hubo dos casos de cáncer de mama después de un injerto de grasa, pero sin demoras en el diagnóstico, la detección o el tratamiento. Ciertos estudios lo están evaluando. Hay una leve preocupación por la transferencia de células madre, por lo que existe el potencial de diferenciación multilinaje. También permite la neovascularización. Siempre explicamos a las pacientes que si hay células tumorales microscópicas, hay un potencial de que las células madre y los factores de crecimiento en cualquier tejido promuevan el crecimiento del tumor. Los estudios muestran efectos nulos o marginales en la probabilidad de recurrencia locorregional del cáncer de mama posmastectomía. Un estudio incluyó resultados de casi ocho años de seguimiento después de los injertos de grasa, pero aún se están investigando.

31
In summary, reconstruction can be performed either immediately after a mastectomy or in a delayed fashion after the patient has undergone mastectomy and received appropriate treatment for their breast cancer. In general, there’re three types of reconstruction that involve implant-based, implant or autologous tissue, or -autolo --- autologous tissue only. The type of reconstruction performed will obviously depend on certain things like patient characteristics, including their BMI, comorbidities, prior surgeries, and treatment requires --- requirements including radiation therapy.
En resumen, la reconstrucción puede realizarse inmediatamente después de la mastectomía o de forma diferida luego de la mastectomía y del correspondiente tratamiento oncológico. En general, hay tres tipos de reconstrucción: implante, implante más tejido autólogo, y tejido autólogo únicamente. El tipo de reconstrucción depende de factores como las características de la paciente, su índice de masa corporal, sus comorbilidades, cirugías previas y requisitos del tratamiento, como la radioterapia.
Reconstruction involves multiple procedures and often takes up to a year to complete if no other cancer therapies are required. Thank you for your --- very much for listening, and we --- we welcome your feedback. Thank you.
La reconstrucción implica procedimientos múltiples y puede requerir hasta un año en completarse si no hay terapia oncológica. Muchas gracias por su atención. Agradeceremos sus comentarios. Gracias.