post bypass catastrophe
TRANSCRIPT

A 72-year-old female, with a history
of diabetes mellitus, with no allergy.
Coronary angiography revealed:
• LAD: tight lesion at the bifurcation
with D1& D2 has tight ostial lesion.
• LCX: Diffusely disease.
• OM: Diffusely disease.
• LV: Normal size and wall thickness
Moderately impaired LV systolic
function.
Moderate global hypokinesia.
EF= 40%.
• Other chambers and valves were
normal.

• Premedication: Pt was pre medicatated
by P.O. valium 5 mg at midnight and 6 Am,
plus 10 mg morphine on calling to OR.
• Arterial cannulation was done before
induction of GA, while venous CVP and
large bore cannula were inserted
after smooth un eventual induction of
GA, using Etomidate, Fentanyl,
• Maintenance of anesthesia was
carried by Propofol, nimbex infusion,
and supplemental titrated doses of
midazolam, Fentanyl, and Morphine
guided by BSI, and the operative steps.
• Heparin achieved satisfactory ACT
result.
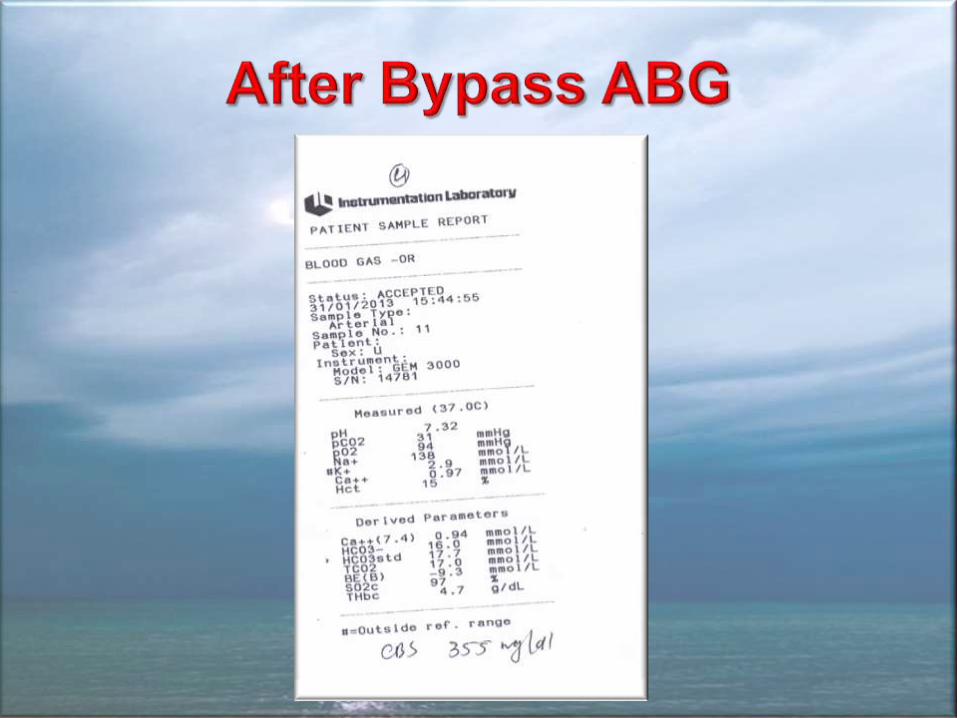
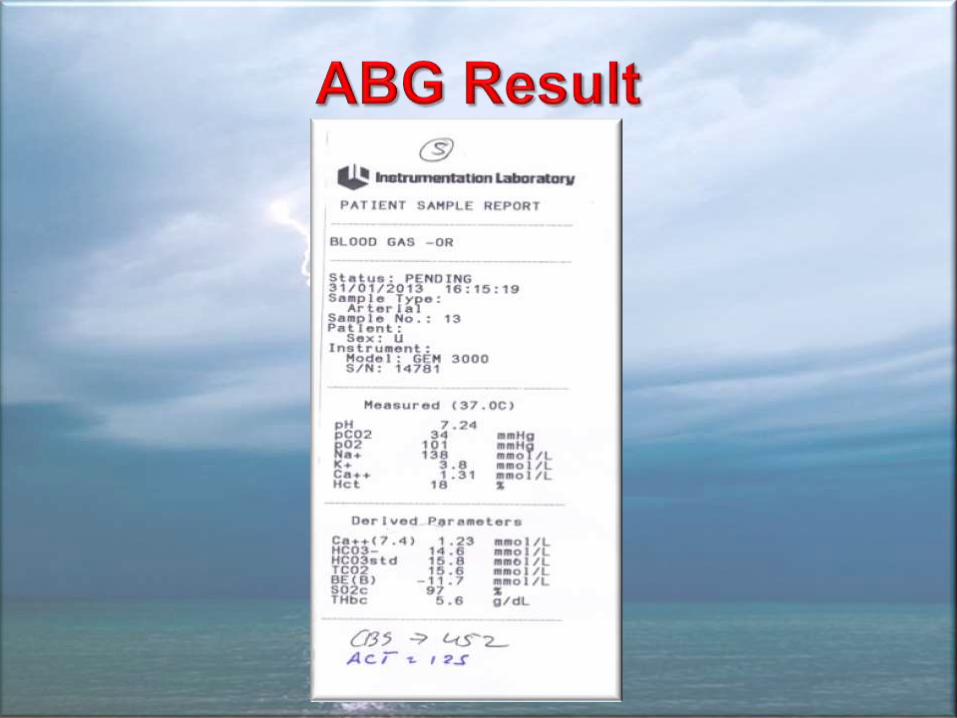
• Except of elevation of BS and its
• Ventilator was kept on with
- A low tidal volume 150 ML
- FI02 50%
- Frequency 12/min.
• Maintenance of Anesthesia by
Propofol, Nimbex infusion, and
supplemental of midazolam, Fentanyl,
and Morphine given on bypass machine
• Preparing adequate equivalent Protamine dose ready for infusion
• Preparing blood and its product.
• Adrenaline 50 n g started during the second proximal anastomosis.
• Reassume normal mechanical ventilation.
• Achieving HR. 108 and BP 130/ 80
• CVP reading had a mean of 10. It was temporally elevated with the filling of the heart.
• Insulin infusion together with K correction was the second natural inotropic to be administrated.
• Drop by drop Protamine started very slowly while Bp was 156/90.
• According to protocol; Platelets infusion started, and were to be followed by blood and FFP according to CVP reading guide and surgeon advice.
• By the time Half dose of Protamine
• Blood pressure was gradually
dropping and accordingly inotropic
adrenaline does was increased to
maximum 200 ng ,
• Noradrenalin was administrated and
also reached maximum 200 ng in order
to keep the systolic Bp in the range of
• When ½ Protamine had been given,
Anesthetist requested to discontinue
protamine infusion, Surgeon insisted
to finish Protamine before removing
the aortic cannula.
• Maximum doses of nor and adrenaline
infusion were able to maintain a
systolic BP above 120.
• Increasing insulin infusion to 6U/H
• Running maximum K infusion 40 MEq/hr
• Protamine was finished
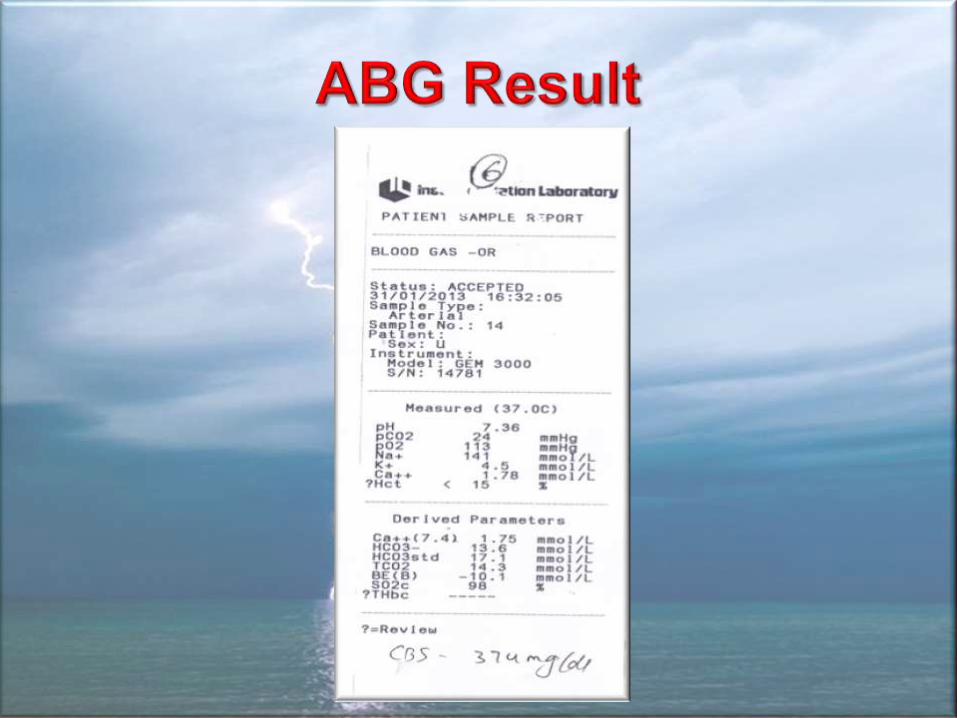
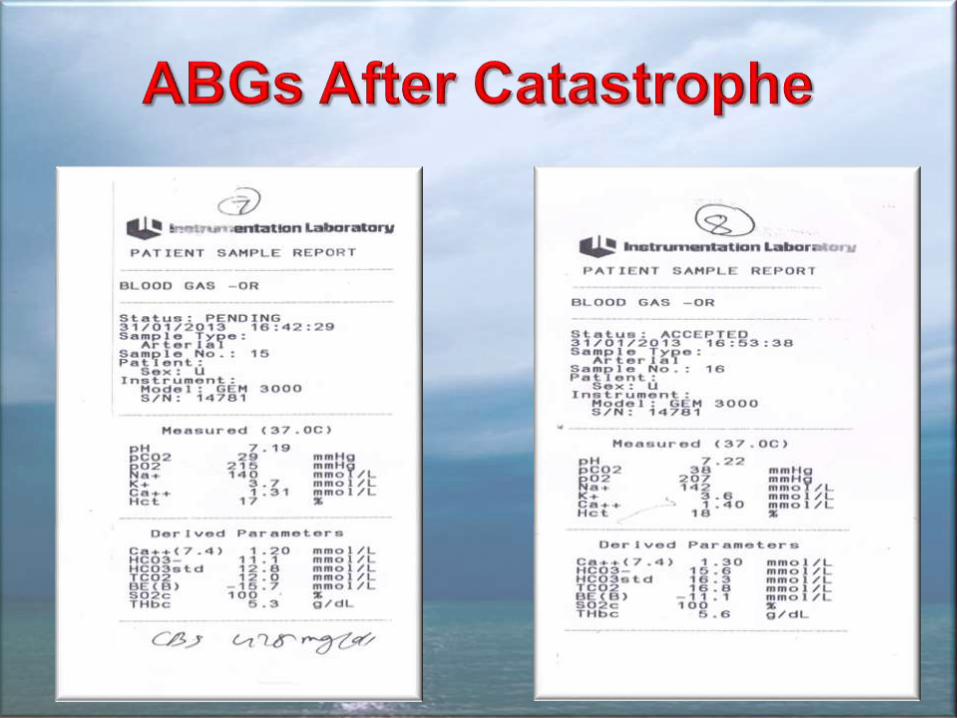
• Considering NaHC03 for correction of
acidosis.
• Discussing nitroglycerin infusion with
the surgeon to lower the CVP reading,
He agreed and it was started. Shortly
• Despite Maximum inotrope and vasopressors
• Systolic BP started rapid dropping
120- 100- 80- till 67 mmHg
• RV Distension
• 40 mmHg reading of CVP
• Sluggish myocardial contractility
• Ventricular arrhythmia
• Bradycardia
• Bolus Adrenaline was ineffective to

• Hyperventilation• Inotropic and vasopressors kept
maximum• Bolus Adrenaline 1 mg• Surgeon regretted, & incriminated
nitroglycerine to be the cause of the catastrophe, and requested to administrate bolus 1 g Calcium chloride.
• Internal cardiac massage for less than ½ min was effective to over come PH hence inotropes, & vasopressors was able to work effectively on the LV.
• Bp restored to 240/130
• Development of ventricular
arrhythmia necessitate bolus
lidocaine followed by 2 mg /kg / hr
infusion
• Marked acidosis necessitated
administration of a total dose of 200
• Pt was weaned form IABP and
Pacemaker and extubated
successfully within 24 hr.
• Elevated Renal function tests were
returned to normal with in 5 days.

• Protamine remains the mainstay drug
for heparin
neutralization during cardiac
surgery. Frequently, protamine
causes transient hypotension from
histamine release, which is more
apparent if rapidly injected
• APH is a clinical diagnosis
• The systemic hypotension typically
occurs secondary to poor LV filling
associated with the severe RV
dysfunction.
• In our case maximum inotropes and
vasopressors were able to maintain
BP and coronary perfusion till the
development of critical PH, with the
• Protamine systemic hypotension mediated by:
1- Histamine release
2- Endothelium derived relaxing factor, i.e., NO
• This vasodilating effect is not observed in the presence of a heparin-protamine complex.
• Protamine-induced severe pulmonary vasoconstriction and circulatory
During CPB, complement activation takes place.
• The production of prostacyclin, a potent vasodilating prostaglandin, increases during the early stages of CPB, but decreases progressively during re warming and reperfusion of the lungs.
• The production vasoconstricting thromboxane A2 and B2 follows an opposite pattern, reaching the highest plasma levels after re
• Thromboxane are at their highest levels at the time of Protamine administration
• Acid-base interaction between protamine and heparin “polyanionic polycationic interaction” further more activate complement and potentiate the pulmonary vasoconstricting effect of thromboxane possibly aggravated by concomitant platelets administration.
• Serotonin and other vasoactive

• Inotropic support of the failing myocardium may combine calcium with adrenaline in an attempt to augment the haemodynamic actions of each drug.
• Calcium blunts adrenaline induced increases in blood pressure and cardiac output in animals and human.
• Ca blunts epinephrine's beta-adrenergic actions in postoperative cardiac surgery patients.
• It opposes the stimulant effect of
During myocardial ischemia there is a
• Fall in ATP
• Rise in lactate
• Decrease in intracellular pH
• Increase in the intracellular
Ca which further consumes ATP.
• Membrane ionic pumps and
channels are disrupted
Membrane depolarization
and loss of excitability
Ventricular fibrillation
The main causes of reperfusion injury following prolonged ischemia
• Cytosolic Ca2+ loading
• Generation of
reactive oxygen species
Exacerbate mitochondrial
dysfunction
• Ventricular fibrillation
• Myocardial stunning
• Loss of intracellular proteins
• Promoting an
inflammatory response
• Cytokine release
• Complement activation
Further compromise the cardiac
function
1- Stop Protamine administration if it was not finished.
2- Re heparinization to decrease heparin-protamine complexes and stopping thromboxane release from macrophages
3- Hyper ventilation with 100% FI02
4- Maximum inotropic and vasopressors given through a left atrial catheter………… Why?
5- Consider Phosphodiesterase
1- Inhaled: prostacyclin, nitric oxide.
2- Nitroglycerin, but it increases pulmonary shunt
3- Cyclic AMP-specific phosphodiesterase inhibitors
e.g. milrinone amrinone, enoximone, but they
result in systemic hypotension
4- Ketanserin

• Nitroglycerine exerts a direct effect on the pulmonary circulation in doses that do not affect systemic resistance vessels or the myocardium and do not activate neurohumoral reflexes
• Uniquely it reduces pulmonary artery pressures in addition to pulmonary vascular resistance due to its ability to dilate venous capacitance vessels.
• Ketanserin is a quinazoline derivative that selectively blocks S2-serotonergic receptors. it has α1 receptor blocking and H1 histaminergic antagonistic properties.
• Unlike Nitroglycerine the use of I.V ketanserin 1.0 to 2.0 mg, over a period of 10 minutes, does not change, shunt fraction, does not block hypoxic pulmonary vasoconstriction
• The fear of postoperative bleeding, the urge to transfuse blood products for haemostatic purposes, the over looking of the developing clinical status; were the reasons beyond all of these catastrophes happened in this case.
• Settled appropriate protocols for management of possible complications and sticking to it is much more prudent rather than to regret, blame, or