polio vaccines and polio immunization in the pre ... · 2 polio vaccines and polio immunization in...
TRANSCRIPT
Polio vaccines and polio immunization in the pre-eradication era: WHO position
paper
Published in WER 4 June, 2010
2 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Epidemiology & Background Poliomyelitis (polio) is an acute communicable disease of humans
caused by poliovirus of serotypes 1, 2 or 3
Faecal-to-oral and/or oral-to-oral mode of transmission, depending on standard of sanitation
<1960 (pre-vaccine era): virtually all children infected
1974: Oral poliovirus vaccine (OPV) recommended as part of the Expanded Programme on Immunization (EPI)
1988: World Health Assembly resolved to eradicate polio globally by the year 2000
3 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Since 1988: 3 of 6 WHO Regions free from wild-strain polio viruses
In remaining 3 regions, number of polio cases reduced by 99%
Endemic polio limited to certain areas in a few countries
WPV type-2 not detected worldwide since 1999
However :
Areas of Afghanistan, India, Nigeria and Pakistan remain polio-endemic
During 2003-2009, 133 wild-strain polio virus importations occurred in 29 previously polio-free countries, leading to 60 outbreaks and 2.193 polio cases
By May 2010, 109 (83%) of these events were controlled, but outbreaks following 24 importations in 13 countries are still active
Epidemiology & Background (Ctd)
4 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Poliovirus is an enterovirus of the Picornaviridae family. Single-stranded, positive-sense, RNA genome. Capsid proteins of the 3 serotypes differ slightly in receptor specificity and antigenicity
Incubation period 7-10 days. Most infections asymptomatic and limited to alimentary tract. ~ 24% of infected individuals develop fever, headache, and sore throat (minor illness)
In <1% of infected, virus replicates in anterior horn cells of the spinal cord resulting in acute flaccid paralysis (AFP), usually asymmetrical. Sensation intact. Persistent paralysis and resulting deformities are common
Case-fatality rate among paralytic cases 2% - 20%, but higher with bulbar involvement
Poliovirus and disease
5 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Immunocompetent individuals develop protective immunity through induction of circulating and mucosal immune responses
Presence of neutralizing antibody against polioviruses is a reliable correlate of protection
Immunity induced by one of the 3 serotypes does not provide protection against the other 2 serotypes
Mucosal immunity (IgA) decreases local replication and provides a barrier to viral shedding
Immune response to infection and vaccination
6 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Polio vaccines
Salk 1955, inactivated polio vaccine
Sabin 1961 and 1963, monovalent and trivalent oral polio vaccine
7 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Oral polio vaccine (OPV) OPVs are based on live, attenuated viruses derived by
passage in non-human cells of their respective parent WPVs. Attenuation results in much lower neurovirulence and transmissibility
No combination products, but OPV usually administered concurrently with one or more of common childhood vaccines, e.g. BCG, DPT, HBV, measles, Hib and rotavirus
OPV is highly heat-sensitive. Must be kept frozen or, after thawing, at temperatures between 2 °C and 8 °C for a maximum of 6 months
8 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
In industrialized countries, 3 doses of trivalent OPV induces nearly 100% seroconversion for all 3 virus types. Corresponding result in developing countries 73% and 70%, respectively, against type-1 and type-3
Seroconversion trials show that monovalent OPV and bivalent OPV are more immunogenic than trivalent OPV, with respect to type-1 and type-3 viruses
OPV given at birth will improve seroconversion rates of subsequent doses (Grading: High scientific evidence)
Large-scale use of OPV has led to global eradication of WPV2, elimination of WPV type-1 and type-3 in 3 of the 6 WHO regions, and >99% reduction in number of cases in remaining 3 regions (Grading: High scientific evidence)
Herd immunity explains some of the reduction in polio incidence
Immunity against paralytic disease appears to be lifelong
Oral polio vaccine (OPV): Immunogenicity, effectiveness
9 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
In general, OPV is a safe vaccine. However, vaccine-associated paralytic poliomyelitis (VAPP) occurs in approximately 4 cases per 1 000 000 birth cohort/year in countries using OPV
OPV viruses can acquire neurovirulence and transmissibility characteristics of WPV and such circulating vaccine-derived poliovirus (cVDPV) can cause polio outbreaks. In 2000–2009, 12 outbreaks of cVDPVs were reported. Immunity gaps are important risk factors
Immunodeficiency-associated vaccine-derived polioviruses (iVDPV) are found in a small number of individuals with common variable immunodeficiency syndrome
The risk of VAPP, cVDPV and iVDPV has led a number of countries to change from the relatively cheap and conveniently administered OPV to the parenteral and more costly IPV
Oral polio vaccine (OPV): Safety
10 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
IPV is based on selected WPV strains grown in Vero cell culture or in human diploid cells and inactivated with formaldehyde
IPV may contain trace amounts of formaldehyde, streptomycin, neomycin or polymyxin B; some the preservative phenoxyethanol, but neither thiomersal nor adjuvants
Administered intramuscularly (preferred) or subcutaneously. Stable at ambient temperature, but should be refrigerated to avoid loss of potency. Freezing should be avoided
IPV is available either alone or in combination with other common vaccine antigens including D, T, wP or aP, HBV, or Hib
Except for minor local reactions, IPV is one of the safest vaccines used in routine immunization
Inactivated poliovirus vaccine (IPV)
11 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
In two major field trials in USA (1950s) involving 400 000 and 200 000 children, respectably, the calculated IPV efficacy was 80%-90% against paralytic polio and 60%-70% against all types of polio. Trials in Texas, Canada, and Senegal showed >90% efficacy/effectiveness (Grading: High scientific evidence)
Persisting neutralizing antibodies against polioviruses are usually found in all vaccinees ~5 years after the primary immunization series. Neutralizing antibodies were found in all of 250 Swedish children studied who had received 3 doses of IPV ~18 years earlier
Inactivated poliovirus vaccine (IPV): efficacy/effectiveness
12 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Many countries have adopted sequential schedules of 1–2 doses of IPV followed by ≥2 doses of OPV.
This economic approach achieves protective immunity in ≥ 90% of vaccines (Grading: moderate evidence); IPV is likely to prevent vaccine-associated paralytic polio (VAPP) and OPV is added to strengthen mucosal immunity.
Sequential use of IPV-OPV
13 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Cost-effectiveness of routine polio vaccination
Since introduction of routine vaccination in the US, ~1.1 million cases of paralytic polio, and >160 000 deaths have been prevented at a cost of ~US$ 1.7 billion. Through savings on treatment costs, polio vaccination generated a net benefit of ~US$ 180 billion.
Country-specific analyses of the incremental cost-effectiveness of switching from OPV to IPV (in Australia, South Africa and the United States) concluded that changing from OPV to IPV was not cost effective.
Although the cost-effectiveness of IPV may change with ongoing efforts to lower its cost, OPV is the most cost-effective polio vaccine.
While cost–effectiveness analyses do not support the switch from OPV to IPV based on expected economic benefits, countries have introduced IPV either in a sequential IPV–OPV schedule or as an IPV-only schedule because of the overriding need to reduce or eliminate VAPP, and in the expectation that a switch would help maintain public confidence in vaccination in general.

14 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
All children worldwide should be immunized against polio, and every country should seek to achieve and maintain high levels of coverage with polio vaccine
Choice of vaccine
The potential for wild-strain poliovirus importation and transmission are crucial factors to be considered when defining national policy on polio immunization:
This potential is very high in countries bordering endemic countries and countries with recurrent outbreaks; it is high in countries with previous importation and frequent traffic across the border; the potential is considered moderate in the rest of the world
WHO recommendations (1)
15 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Choice of vaccine (ctd)
OPV alone, including a birth dose, is recommended in all polio-endemic countries and in countries at high risk for importation and subsequent spread.
Birth doses of OPV should be administered at, or shortly after delivery to increase seroconversion rates of subsequent doses and to induce mucosal protection as early as possible
Theoretically, administration of OPV when infants are still protected by maternal antibodies may prevent vaccine-associate paralytic polio.
Early OPV vaccination seems to be well tolerated even in cases of perinatal HIV infection
WHO recommendations (2)
16 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Choice of vaccine (ctd)
OPV alone, preferably with a birth dose, is recommended in countries with a moderate/high potential for wild-strain poliovirus transmission. A birth dose is not necessary where the risk of transmission is low, even where the potential for importation is high/very high.
WHO suggests that in countries with very high risk of wild-strain poliovirus importation, a sequential IPV–OPV schedule should not be introduced unless immunization coverage with 3 doses of poliovirus vaccine is ~95% (or ~90%, with lower importation risk). Where a sequential IPV–OPV schedule is used, 1 or 2 initial doses of IPV should be followed by ≥2 doses of OPV to ensure both a decreased burden of VAPP and sufficient mucosal protection.
IPV alone may be an alternative to OPV alone (or an IPV–OPV sequential schedule) only in countries with the lowest risk of wild-strain poliovirus importation and transmission. Switching from OPV to IPV for routine vaccination during the pre-eradication era is not considered cost-effective.
WHO recommendations (3)
17 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
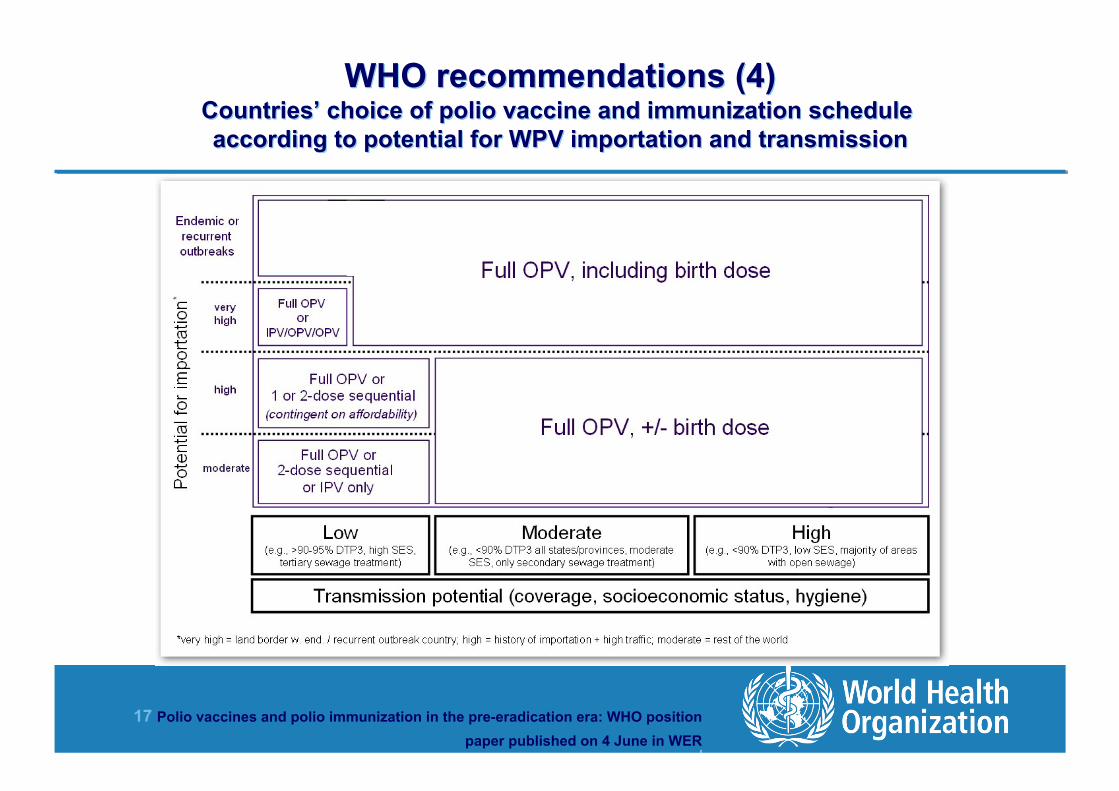
WHO recommendations (4) Countries’ choice of polio vaccine and immunization schedule according to potential for WPV importation and transmission
18 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Schedules The primary 3 OPV doses should be given according to national immunization schedules, e.g. at ages
6, 10, and 14 weeks, or at ages 2, 4, and 6 months. In addition, a birth dose should be given where the potential for importation of poliovirus is high/very high, and the potential for virus transmission is high/moderate, (see Fig. 1)
The primary 3 IPV doses should be given intramuscularly or subcutaneously; first dose at 2 months of age. If the series begins earlier (e.g. with doses at 6, 10, and 14-weeks), a booster dose is required after ≥6 months (4-dose schedule)
Where sequential IPV/OPV is used, WHO recommends that IPV be administered at 2 months of age (e.g. an IPV-OPV-OPV schedule) or at 2 and 3-4 months of age (e.g. an IPV-IPV-OPV-OPV schedule); in both schedules IPV should be followed by at least 2 doses of OPV. Each dose in the primary series, whether IPV or OPV, should be separated by 4-8 weeks, depending on the risk of exposure to polio in early childhood
Both IPV and OPV may be administered simultaneously with other vaccines in national childhood immunization programmes
WHO recommendations (5)

19 Polio vaccines and polio immunization in the pre-eradication era: WHO position paper published on 4 June in WER
|
Vaccinating travellers Travellers to polio-endemic countries who have previously received ≥3 doses of OPV or
IPV should have a once-only additional dose, and non- or not fully immunized travellers should complete a primary IPV or OPV series before departure. Following the primary series, a one-time only additional dose of OPV or IPV provides sufficient protection against polio for those who repeatedly visit endemic areas
Before travelling abroad, persons living in a polio-endemic country should be fully vaccinated against polio, preferably with OPV, to boost mucosal immunity and reduce the risk of WPV shedding. Such travellers should receive an additional dose of OPV 1–12 months prior to each international travel. In case of urgent travel, a minimum of 1 dose of OPV should be given, ideally 4 weeks before departure. Some polio-free countries (e.g. Saudi Arabia) may require travellers from polio-endemic countries to be immunized against polio to obtain entry visa
WHO recommendations (6)