po3-125 to po03-187
TRANSCRIPT
S268 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
PO3-126
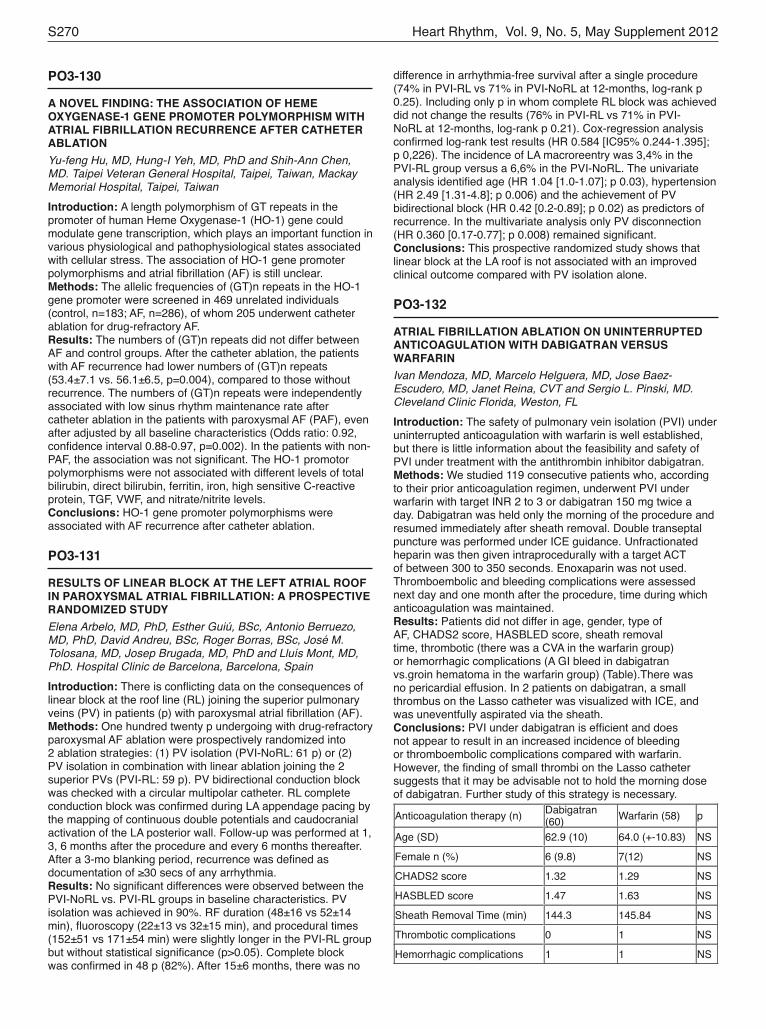
ELECTROPHYSIOLOGICAL PROPERTIES OF THE SUPERIOR VENA CAVA AND THE VENOATRIAL JUNCTION IN PATIENTS WITH ATRIAL FIBRILLATION: RELEVANCE TO CATHETER ABLATIONKotaro Fukumoto, MD, Seiji Takatsuki, MD, Takehiro Kimura, MD, Nobuhiro Nishiyama, MD, Kojiro Tanimoto, MD, Yoko Hagiwara, MD, Yoshiyasu Aizawa, MD, Yukiko Fukuda, MD, Shunichiro Miyoshi, MD and Keiichi Fukuda, MD. Cardiology devision, Keio university school of medicine, Shinjuku city, Tokyo, JapanIntroduction: Although SVC has been well known as one of the important foci triggering atrial fibrillation (AF), its electrophysiological characteristics has been little studied. This study aimed to investigate an electrophysiological property of the superior vena cava (SVC) and venoatrial junction (VAJ).Methods: Twenty-five AF patients with SVC ectopy undergoing catheter ablation were included. After pulmonary vein isolation, a circular decapolar catheter and two multipolar catheters were respectively emplaced in the VAJ, right atrial appendage (RAA) and SVC. Burst pacing and single extrastimulus were applied from the RAA and SVC. The atrial and the caval potentials on the circular catheter were investigated.Results:Intracaval conduction delay and echo beats over the VAJ in both the atrial-caval and the inverse direction were induced by pacing maneuvers. A conduction delay and Wenckebach type second degree conduction block over the VAJ was observed with burst pacing from both RA and the SVC. Single extrastimulus from the RAA and SVC with a basic cycle length of 600 ms prolonged the conduction time via VAJ by 79 ± 52.1 ms and 48 ± 41.9 ms, respectively. Conduction time over the VAJ with other pacing maneuvers are listed in Table 1. The atrial and the caval electrograms at the VAJ separated from each other by pacing maneuvers facilitated a mapping of the earliest activation site at the VAJ.Conclusions:Intracaval conduction delay and a decremental conduction property via the VAJ were demonstrated with pacing manervers, which could help to distinguish the atrial and the caval potentials and facilitate mapping of the optimal ablation sites to isolate SVC.Table 1. The increment in conduction time over the VAJ
RA burst
RA ex600
RA ex400
SVC burst
SVC ex600
SVC ex400
Range (ms) 6 - 96 18 - 235 4 - 200 6 - 72 2 - 159 5 - 150
Mean ± SD (ms) 38 ± 23.3
79 ± 52.1
65 ± 42.4
23 ± 16.1
48 ± 41.9
39 ± 31.8
Compared to RA ex600
p < 0.01 NA p > 0.5 p <
0.01 p = 0.03 p = 0.01
PO3-127
PATIENTS WITH LONE ATRIAL FIBRILLATION HARBOR DIFFUSE VENTRICULAR FIBROSISLiang-han Ling, MBBS, Andrew Taylor, MBBS, PhD, Andris Ellims, MBBS, Leah Iles, MBBS, Andrew Teh, MBBS, PhD, Geoffrey Lee, MBBS, Michael Wong, MBBS, Jonathan Kalman, MBBS, PhD, David Kaye, MBBS, PhD and Peter Kistler, MBBS, PhD. Alfred Hospital and Baker IDI Research Institute, Melbourne, Australia, Royal Melbourne Hospital, Parkville, AustraliaIntroduction: Atrial fibrillation (AF) can induce tachycardia-mediated cardiomyopathy (TMC) characterized by left ventricular (LV) dilatation, systolic dysfunction, and diffuse fibrosis. Delayed enhancement on cardiac magnetic resonance imaging (CMR) provides spatial information on focal scar. Diffuse ventricular
PO3-125
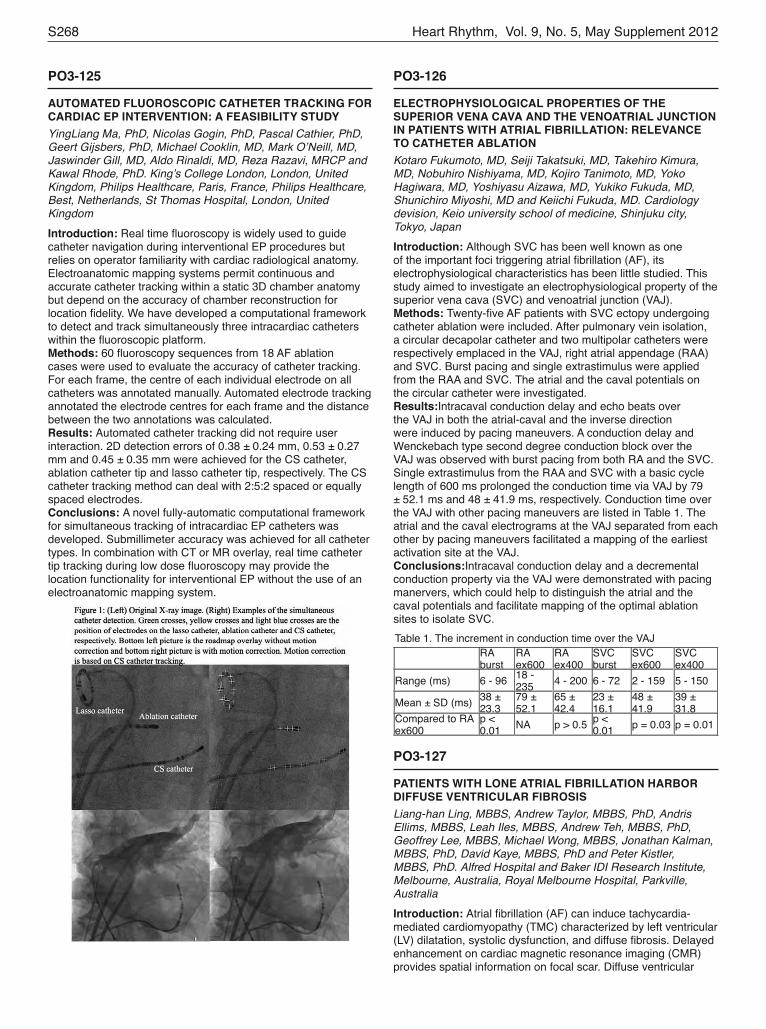
AUTOMATED FLUOROSCOPIC CATHETER TRACKING FOR CARDIAC EP INTERVENTION: A FEASIBILITY STUDYYingLiang Ma, PhD, Nicolas Gogin, PhD, Pascal Cathier, PhD, Geert Gijsbers, PhD, Michael Cooklin, MD, Mark O’Neill, MD, Jaswinder Gill, MD, Aldo Rinaldi, MD, Reza Razavi, MRCP and Kawal Rhode, PhD. King’s College London, London, United Kingdom, Philips Healthcare, Paris, France, Philips Healthcare, Best, Netherlands, St Thomas Hospital, London, United KingdomIntroduction: Real time fluoroscopy is widely used to guide catheter navigation during interventional EP procedures but relies on operator familiarity with cardiac radiological anatomy. Electroanatomic mapping systems permit continuous and accurate catheter tracking within a static 3D chamber anatomy but depend on the accuracy of chamber reconstruction for location fidelity. We have developed a computational framework to detect and track simultaneously three intracardiac catheters within the fluoroscopic platform.Methods: 60 fluoroscopy sequences from 18 AF ablation cases were used to evaluate the accuracy of catheter tracking. For each frame, the centre of each individual electrode on all catheters was annotated manually. Automated electrode tracking annotated the electrode centres for each frame and the distance between the two annotations was calculated.Results: Automated catheter tracking did not require user interaction. 2D detection errors of 0.38 ± 0.24 mm, 0.53 ± 0.27 mm and 0.45 ± 0.35 mm were achieved for the CS catheter, ablation catheter tip and lasso catheter tip, respectively. The CS catheter tracking method can deal with 2:5:2 spaced or equally spaced electrodes.Conclusions: A novel fully-automatic computational framework for simultaneous tracking of intracardiac EP catheters was developed. Submillimeter accuracy was achieved for all catheter types. In combination with CT or MR overlay, real time catheter tip tracking during low dose fluoroscopy may provide the location functionality for interventional EP without the use of an electroanatomic mapping system.

S269Poster Session III
atenolol (27±5 ms vs. 43±3 ms after atenolol, p=0.0168). NTP-induced AF-inducibility was inhibited after RDN (20% vs. 100% at baseline, p<0.001) but not after atenolol. Administration of atropine after RDN or atenolol completely inhibited NTP-induced AERP-shortening. Post-apneic blood pressure rise was effectively inhibited by RDN. AERP-shortening induced by high-frequency stimulation of ganglionated plexi was not influenced by RDN, which excludes a modulation of sensitivity of ganglionated plexi by RDN.Conclusions: Vagally mediated NTP-induced AERP-shortening after RDN or atenolol was less sufficient to maintain AF compared to baseline, which emphasizes the importance of autonomic dysbalance in OSA associated AF. RDN is capable to reduce AF-inducibility and post-apneic blood pressure rises during obstructive events independent of a modulation of sensitivity of ganglionated plexi.
PO3-129
DELIVERY OF RADIOFREQUENCY ENERGY WITH CONTINUOUS CATHETER MOTION RESULTS IN LARGER LESION SIZE COMPARED TO STANDARD INTERRUPTED POINT TO POINT ABLATIONMatthew D. Olson, MD, David F. Katz, MD, Russell R. Heath, MD, Wendy S. Tzou, MD, Joseph L. Schuller, MD, Ryan G. Aleong, MD, Pual D. Varosy, MD, Duy T. Nguyen, MD and William H. Sauer, MD, FHRS. University of Colorado Dept. of Electrophysiology, Aurora, COIntroduction: When an ablation strategy incorporates contiguous lesions to create a line of block, some advocate continuous catheter movement with constant tissue contact during delivery of RF energy to create a “drag lesion.” We sought to characterize the potential differences in lesion characteristics between drag lesions versus point-to-point delivery of energy.Methods: An ex vivo model consisting of viable bovine myocardium in a circulating warm saline bath over a scale was used. An ablation catheter was positioned with 2 and 15 grams of force in both perpendicular and parallel positions. A series of ablation lesions were delivered along 20 cm lines using a programmable stepper motor to withdraw an ablation catheter at a constant rate with constant force. A second set of ablation lesions was created with interruptions between each RF delivery using identical power and temperature shut off settings. The lesion volumes were analyzed using a digital micrometer and compared.Results: Parallel oriented drag lesions were similar to parallel point to point (P2P) lesions under 2 grams of continuous force (957+/- 55 mm3 vs 1040 +/-74.6 mm3, p= 0.38) . The parallel drag lesion was significantly larger than the P2P lesion at 15 grams (2088 +/- 122 mm3 vs. 1595 +/- 121; p = 0.01). With perpendicular orientation the drag lesion volume was larger than P2P at 2gm force (940 +/- 103 mm3 vs 728 +/- 98 mm3; p=0.16).Conclusions: RF ablation drag lesions are larger than those created by a standard point to point method.
fibrosis can be quantified using novel post-contrast T1 mapping methods. We determined whether diffuse LV fibrosis was present in lone AF patients, defined as AF in the absence of structural heart disease including hypertension and diabetes.Methods: Of 80 consecutive AF patients undergoing CMR, those with lone AF in sinus rhythm were selected for study. A histologically validated T1 mapping sequence was used to calculate post-contrast T1 relaxation time (T1 time) of the mid LV in short-axis view as an index of diffuse fibrosis. Findings were compared to a cohort of healthy age- and gender-matched controls. Results are expressed as mean±SE.Results: Twelve patients with lone AF (8 paroxysmal, 4 persistent) and 12 controls were identified. In both groups, mean age was 54±3 years, 75% were male, body mass index was 26±1 kg/m2, and CHA2DS2-Vasc score was 0.3±0.1. Lone AF patients had worse NYHA functional class (1.8±0.3 vs 1.0±0.0, p<0.05), increased indexed LV end-diastolic volume (82±3 vs 73±4 ml/m2, p<0.05), and shortened mid LV T1 time consistent with diffuse fibrosis (420±28 vs 535±18 ms, p<0.01) (see table).Conclusions: Lone AF was associated with shortening of ventricular T1 times suggestive of diffuse ventricular fibrosis despite normal systolic function.Characteristics of Subjects with Lone AF versus Age and Gender Matched Controls
Lone AF (n=12)
Controls (n=12)
P value
Age, years 54±3 54±3 0.9Male gender, n (%) 9 (75%) 9 (75%) 1.0NYHA functional class 1.8±0.3 1.0±0.0 <0.05LA area, cm2 25±1 22±2 0.2LV ejection fraction, % 64±2 67±2 0.1LV end-diastolic volume index, ml/m2 82±3 73±4 <0.05LV mass index, g/m2 51+±1 55±4 0.3Mid LV T1 time, ms 430±28 535±18 <0.01Delayed enhancement, n (%) 0 (0) 0 (0) 1.0
PO3-128
RENAL SYMPATHETIC DENERVATION SUPPRESSES INDUCIBILITY OF ATRIAL FIBRILLATION AND POSTAPNEIC BLOOD PRESSURE RISES IN A PIG MODEL FOR OBSTRUCTIVE SLEEP APNEADominik K. Linz, MD, Felix Mahfoud, MD, Christian Ukena, MD, Hans-Ruprecht Neuberger, MD, PhD, Klaus Wirth, MD, Ulrich Schotten, MD, PhD and Michael Böhm, MD. Universitätsklinikum des Saarlandes, Klinik für Innere Medizin III, Homburg/Saar, Germany, Sanofi-Aventis, Frankfurt, Germany, Cardiovascular Research Institute Maastricht, Maastricht, NetherlandsIntroduction: Obstructive sleep apnea (OSA) is associated with autonomic dysbalance. Negative tracheal pressure (NTP) during obstructive respiratory events increases vagal tone and leads to shortening of the atrial effective refractory period (AERP), thereby facilitating atrial fibrillation (AF). However, the relative roles of adrenergic and cholinergic influences on AF induction and maintenance during obstructive events are not well known.Methods: Surgical renal sympathetic denervation (RDN) has been proven to reduce renal afferent and efferent sympathetic activity. We compared the effect of RDN and atenolol (3 mg/kg) on atrial electrophysiological changes and inducibility of AF during obstructive apnea. We also studied the effect of RDN on AERP-shortening induced by high-frequency stimulation of the anterior right ganglionated plexi.Results: Tracheal occlusion with applied NTP at -80 mbar induced pronounced AERP-shortening and increased AF-inducibility in all pigs. RDN resulted in a more pronounced inhibition of NTP-induced AERP-shortening compared to
S270 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
difference in arrhythmia-free survival after a single procedure (74% in PVI-RL vs 71% in PVI-NoRL at 12-months, log-rank p 0.25). Including only p in whom complete RL block was achieved did not change the results (76% in PVI-RL vs 71% in PVI-NoRL at 12-months, log-rank p 0.21). Cox-regression analysis confirmed log-rank test results (HR 0.584 [IC95% 0.244-1.395]; p 0,226). The incidence of LA macroreentry was 3,4% in the PVI-RL group versus a 6,6% in the PVI-NoRL. The univariate analysis identified age (HR 1.04 [1.0-1.07]; p 0.03), hypertension (HR 2.49 [1.31-4.8]; p 0.006) and the achievement of PV bidirectional block (HR 0.42 [0.2-0.89]; p 0.02) as predictors of recurrence. In the multivariate analysis only PV disconnection (HR 0.360 [0.17-0.77]; p 0.008) remained significant.Conclusions: This prospective randomized study shows that linear block at the LA roof is not associated with an improved clinical outcome compared with PV isolation alone.
PO3-132
ATRIAL FIBRILLATION ABLATION ON UNINTERRUPTED ANTICOAGULATION WITH DABIGATRAN VERSUS WARFARINIvan Mendoza, MD, Marcelo Helguera, MD, Jose Baez-Escudero, MD, Janet Reina, CVT and Sergio L. Pinski, MD. Cleveland Clinic Florida, Weston, FLIntroduction: The safety of pulmonary vein isolation (PVI) under uninterrupted anticoagulation with warfarin is well established, but there is little information about the feasibility and safety of PVI under treatment with the antithrombin inhibitor dabigatran.Methods: We studied 119 consecutive patients who, according to their prior anticoagulation regimen, underwent PVI under warfarin with target INR 2 to 3 or dabigatran 150 mg twice a day. Dabigatran was held only the morning of the procedure and resumed immediately after sheath removal. Double transeptal puncture was performed under ICE guidance. Unfractionated heparin was then given intraprocedurally with a target ACT of between 300 to 350 seconds. Enoxaparin was not used. Thromboembolic and bleeding complications were assessed next day and one month after the procedure, time during which anticoagulation was maintained.Results: Patients did not differ in age, gender, type of AF, CHADS2 score, HASBLED score, sheath removal time, thrombotic (there was a CVA in the warfarin group)or hemorrhagic complications (A GI bleed in dabigatran vs.groin hematoma in the warfarin group) (Table).There was no pericardial effusion. In 2 patients on dabigatran, a small thrombus on the Lasso catheter was visualized with ICE, and was uneventfully aspirated via the sheath.Conclusions: PVI under dabigatran is efficient and does not appear to result in an increased incidence of bleeding or thromboembolic complications compared with warfarin. However, the finding of small thrombi on the Lasso catheter suggests that it may be advisable not to hold the morning dose of dabigatran. Further study of this strategy is necessary.
Anticoagulation therapy (n) Dabigatran (60) Warfarin (58) p
Age (SD) 62.9 (10) 64.0 (+-10.83) NS
Female n (%) 6 (9.8) 7(12) NS
CHADS2 score 1.32 1.29 NS
HASBLED score 1.47 1.63 NS
Sheath Removal Time (min) 144.3 145.84 NS
Thrombotic complications 0 1 NS
Hemorrhagic complications 1 1 NS
PO3-130
A NOVEL FINDING: THE ASSOCIATION OF HEME OXYGENASE-1 GENE PROMOTER POLYMORPHISM WITH ATRIAL FIBRILLATION RECURRENCE AFTER CATHETER ABLATIONYu-feng Hu, MD, Hung-I Yeh, MD, PhD and Shih-Ann Chen, MD. Taipei Veteran General Hospital, Taipei, Taiwan, Mackay Memorial Hospital, Taipei, TaiwanIntroduction: A length polymorphism of GT repeats in the promoter of human Heme Oxygenase-1 (HO-1) gene could modulate gene transcription, which plays an important function in various physiological and pathophysiological states associated with cellular stress. The association of HO-1 gene promoter polymorphisms and atrial fibrillation (AF) is still unclear.Methods: The allelic frequencies of (GT)n repeats in the HO-1 gene promoter were screened in 469 unrelated individuals (control, n=183; AF, n=286), of whom 205 underwent catheter ablation for drug-refractory AF.Results: The numbers of (GT)n repeats did not differ between AF and control groups. After the catheter ablation, the patients with AF recurrence had lower numbers of (GT)n repeats (53.4±7.1 vs. 56.1±6.5, p=0.004), compared to those without recurrence. The numbers of (GT)n repeats were independently associated with low sinus rhythm maintenance rate after catheter ablation in the patients with paroxysmal AF (PAF), even after adjusted by all baseline characteristics (Odds ratio: 0.92, confidence interval 0.88-0.97, p=0.002). In the patients with non-PAF, the association was not significant. The HO-1 promotor polymorphisms were not associated with different levels of total bilirubin, direct bilirubin, ferritin, iron, high sensitive C-reactive protein, TGF, VWF, and nitrate/nitrite levels.Conclusions: HO-1 gene promoter polymorphisms were associated with AF recurrence after catheter ablation.
PO3-131
RESULTS OF LINEAR BLOCK AT THE LEFT ATRIAL ROOF IN PAROXYSMAL ATRIAL FIBRILLATION: A PROSPECTIVE RANDOMIZED STUDYElena Arbelo, MD, PhD, Esther Guiú, BSc, Antonio Berruezo, MD, PhD, David Andreu, BSc, Roger Borras, BSc, José M. Tolosana, MD, Josep Brugada, MD, PhD and Lluís Mont, MD, PhD. Hospital Clinic de Barcelona, Barcelona, SpainIntroduction: There is conflicting data on the consequences of linear block at the roof line (RL) joining the superior pulmonary veins (PV) in patients (p) with paroxysmal atrial fibrillation (AF).Methods: One hundred twenty p undergoing with drug-refractory paroxysmal AF ablation were prospectively randomized into 2 ablation strategies: (1) PV isolation (PVI-NoRL: 61 p) or (2) PV isolation in combination with linear ablation joining the 2 superior PVs (PVI-RL: 59 p). PV bidirectional conduction block was checked with a circular multipolar catheter. RL complete conduction block was confirmed during LA appendage pacing by the mapping of continuous double potentials and caudocranial activation of the LA posterior wall. Follow-up was performed at 1, 3, 6 months after the procedure and every 6 months thereafter. After a 3-mo blanking period, recurrence was defined as documentation of ≥30 secs of any arrhythmia.Results: No significant differences were observed between the PVI-NoRL vs. PVI-RL groups in baseline characteristics. PV isolation was achieved in 90%. RF duration (48±16 vs 52±14 min), fluoroscopy (22±13 vs 32±15 min), and procedural times (152±51 vs 171±54 min) were slightly longer in the PVI-RL group but without statistical significance (p>0.05). Complete block was confirmed in 48 p (82%). After 15±6 months, there was no

S271Poster Session III
and LCX images could be obtained simultaneously by MDCT were included in this study. MI ablation between the LIPV and the mitral annulus was performed. The strategies for MDCT guided MI ablation were 1. MI line was placed just below LAA, 2. In case the LCX was below the CS, MI line was placed proximal the crossing point of LCX and CS, and 3. If the LCX was presented on the MI, MI line was placed more laterally comparatively to peripheral LCX. Irrigated-tip catheters were used during MI ablation with the following settings: 43 degrees, 40 watts up to 15min in the LA and 20 watts up to 5 min in the CS. The end point was to achieve bi-directional block across the MI lines using differential pacing technique.Results: The MI was blocked in 97% (35/36) of patients with 608±391 seconds of radiofrequency application and 22759±14008 joules of energy delivery. Epicardial ablation inside the CS was required in 18 of the 36 (50%) patients. No complications occurred. In the unsuccessful MI block case, the LCX ran along the mitral annulus all the way down to CS origin. Transient conduction delay occurred during application on the reverse side of the LCX, complete MI block could not be achieved after multiple MI applications including CS ablation.Conclusions: MDCT guided MI ablation resulted in a high success rate of MI block without complications. The presence of left circumflex coronary artery is associated with an unsuccessful block line at the mitral isthmus.
PO3-135
ABLATION OF COMPLEX FRACTIONATED ATRIAL ELECTROGRAM (CFAE) IN ADDITION TO PULMONARY VEIN ISOLATION AND LINEAR ABLATION DOES NOT IMPROVE SINGLE PROCEDURAL SUCCESS RATE OF CATHETER ABLATION FOR PERSISTENT ATRIAL FIBRILLATIONKelvin CK. Wong, MBBS, John Paisey, MD, MBBS, Norman Qureshi, MBBS, Michael Jones, MBBS, Mark Sopher, MD, FRCP, Richard Bala, MD, Kim Rajappan, MD, Yaver Bashir, MD, FRCP and Timothy R. Betts, MD. Oxford Radcliffe Hospitals NHS Trust, Oxford, United Kingdom, Royal Bournemouth and Christchurch Hospitals NHS Trust, Bournemouth, United KingdomIntroduction: Ablation of complex fractionated atrial electrogram (CFAE) is commonly used as an adjunct to pulmonary vein isolation (PVI) and/or linear ablation in the treatment of persistent atrial fibrillation (AF). However, it is unclear if CFAE ablation has any incremental benefit when performed during the first ablation procedure.Methods: This is a prospective, randomised controlled trial in 2 centres. 120 patients with persistent AF were randomised to PVI + linear ablation (control arm) or PVI + linear ablation + CFAE ablation (CFAE arm). After PVI and linear ablation, a CFAE map of the left atrium and coronary sinus was created (EnSite NavX or Velocity, SJM) to guide CFAE ablation. The “endpoint” was absence of CFAE areas on a repeat CFAE map after CFAE ablation.Results: 95 patients had at least 12 months follow up after the index procedure. Baseline clinical characteristics between the 2 arms were similar (see Table). PVI was achieved in all patients. There was no significance in roof block (100% vs 98%, p=0.49) and MI block (94% vs 91%, p=0.91) between the control and CFAE arms. After mean follow up of 14±3 months, single procedural success was not significantly different between the control and CFAE arms (58% vs 49%, p=0.54). In the control arm, 11 patients had redo-procedures [5 AF, 1 atrial tachycardia (AT), 2 mitral isthmus (MI) flutters, 2 cavotricuspid isthmus (CTI) flutters and 1 roof flutter]. In the CFAE arm, 17 patients had redo-procedures [5 AF, 5 AT, 6 MI flutters, 5 CTI flutters].Conclusions: CFAE ablation in addition to PVI and linear ablation did not increase single procedural success rate in
PO3-133
PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION ORIGINATING FROM NON-PULMONARY VEIN ECTOPY: VERY LONG-TERM OUTCOME AFTER CATHETER ABLATIONHung-Yu Chang, MD, Li-Wei Lo, MD, Yenn-Jiang Lin, MD, Shih-Lin Chang, MD, Yu-Feng Hu, MD and Shih-Ann Chen, MD. Cheng-Hsin General Hospital, Taipei, Taiwan, Taipei Veterans General Hospital, Taipei, TaiwanIntroduction: We aimed to evaluate the long-term result of the patients with paroxysmal atrial fibrillation (AF) who had non-pulmonary vein (NPV) triggers and underwent catheter ablation.Methods: The study consisted of 526 patients (age 54±11y/o, 357 men) who had undergone catheter ablation for drug-refractory paroxysmal AF since 2003. Group 1 consisted of 84 patients with AF initiating from the NPV and pulmonary vein (PV) triggers, and group 2 consisted of 442 patients with AF initiating from the PV triggers only. After discharge, the patients underwent follow-up every 1-3 months. Patients were intended to undergo a 24-hour Holter monitoring or 1-week cardiac event recording every 3 months for 1 year or whenever the patients experienced symptoms suggestive of a tachycardia.Results: The incidence of NPV triggers was 16%. Among the patients with NPV-initiating AF, the ectopies were shown below: superior vena cava 41.7%, crista terminalis and right atrium 14.3%, coronary sinus ostium 4.8%, interatrial septum 9.5%, left atrial free wall (LAFW) and left atrial appendage (LAA) 16.7%, and ligament of Marshall 16.7%. Patients in group 1 were younger than those in group 2 (51±13 vs. 55±11 y/o, p=0.003) and were more likely to be female (46.4% vs. 29.4%, p=0.002). The left atrial diameter (36±6 vs. 38±6mm, p=0.001) was small and the biatrial substrates were worse in group 1 than those in group 2. During a follow-up period of 46±23 months, Kaplan-Meier analysis showed a significantly higher AF recurrence rate in group 1 than that in group 2 (46.4% vs. 36.2%, p=0.03). The independent predictors of the AF recurrence were the NPV trigger (p=0.014, HR 1.58, 95% CI 1.10-2.27), and a larger left atrial diameter (p=0.005, HR 1.04, 95% CI 1.01-1.07). Among the patients with NPV-initiating AF, the only independent predictor of the AF recurrence were the LAFW/ LAA trigger (p=0.009, HR 2.59, 95% CI 1.27-5.26).Conclusions: Comparing with AF originating from the PV only, AF originating from the NPV showed a higher AF recurrence rate after the catheter ablation. LAFW/LAA triggers could predict worse outcomes in the patients with NPV-initiating AF.
PO3-134
IS THE CAUSE OF UNSUCCESSFUL MITRAL ISTHMUS BLOCK LINE IN PATIENTS WITH ATRIAL FIBRILLATION DUE TO THE PRESENCE OF THE LEFT CIRCUMFLEX CORONARY ARTERY?Kohei Yamashiro, MD, Yuichiro Sakamoto, MD, Mitsuru Takami, MD and Takahiko Suzuki, MD. Toyohashi Heart Center, Toyohashi, JapanIntroduction: Mitral isthmus (MI) ablation is technically challenging. Blood flow in the coronary sinus (CS) and left circumflex coronary artery (LCX) may act as a ‘heat sink’ and reduce the efficacy of radiofrequency ablation. Also, ablation in the CS poses a risk of injury to the LCX. We have reported on the feasibility to evaluate the precise anatomical characteristics between the CS and LCX on MI obtained by MDCT before AF ablation. The aim of this study was to evaluate the efficacy of MDCT guided MI ablation.Methods: Thirty-six patients (29males, 62±10years) whose CS

S272 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
recurrence of atrial fibrillation (AF) due to PV reconnection.Methods: 207 consecutive patients (pts) (76% male, 58±10 yrs) who underwent repeat PVI were studied. In the first procedure acute PV reconnection was assessed after a 30 minute waiting period and isoproterenol infusion. Chronic reconnection sites were defined as sites where conduction gaps were identified and ablation achieved PV electrical isolation. Acute and chronic reconnection sites were compared. Reablation of acute and chronic PV reconnections achieved entrance and exit block.Results: Of 207 pts with repeat ablation acute PV reconnection was observed in 77 pts (37%, 109 veins) during the first ablation. The 3 most common sites were both carina regions (18% right, 14% left) and the superior segment of the left superior PV (LSPV) (15%). In the second procedure, reconnected PVs were identified in 204 pts (98%, 626 veins). Chronic reconnection occurred mainly in both carina regions (17% right, 16% left) and the anterior ridge of the LSPV (14%). Evolution of acutely reconnected veins at the subsequent procedure is shown (Figure).Conclusions: 1) Most reconnected PVs at repeat procedure do not demonstrate acute reconnection during first ablation. 2) Acute and chronic PV reconnections occur most commonly in the PV carina. 3) Recurrence of late PV reconnection at the site targeted for acute reconnection may be > 30%, suggesting that identifying and targeting the acute reconnection site to achieve entrance and exit block may not be enough to create persistent electric isolation of that particular segment.
PO3-138
ORAL ANTICOAGULATION (INR) DOES NOT CORRELATE WITH ACTIVATED CLOTTING TIME (ACT) AT THE BEGINNING OF LEFT ATRIAL ABLATION PROCEDURESTilko Reents, MD, Herribert Pavaci, MD, Andras Hinz, MD, Ammar Sonia, MD, Fichtner Stephanie, MD, Jilek Clemens, MD, Susanne Kathan, RN, Karsten Lennerz, MD, Christof Kolb, MD, Gabriele Hessling, MD and Isabel Deisenhofer, MD. German Heart Center Munich, Munich, GermanyIntroduction: Ablation of atrial fibrillation (AF) under therapeutic INR values has become an established technique. Heparin is added routinely during the procedure targeting activated clotting times (ACT) values of >300 seconds. It has been assumed that ACT values reflect the combined effect of INR and heparin and thus the “total” anticoagulation status of the patient. However, there are only few data on the correlation of preprocedural INR values and baseline ACT.Methods: A total of 411 patients (128 female) with a mean age of 64 ± 10 yrs underwent a left atrial ablation procedure (paroxysmal atrial fibrillation n=227, persistent atrial fibrillation n=145, left atrial flutter n=39) under oral anticoagulation. Preprocedural INR values and baseline ACT before any heparin
persistent AF ablation.Baseline clinical characteristics
CONTROL ARM(n=48)
CFAE ARM(n=47)
P value
Age 61±9 62±10 0.69Male (%) 27% 32% 0.65Persistent AF (%) 100% 100% 1.0Cardiovascular disease (%) 66% 65% 1.0Impaired LV function (%) 25% 23% 1.0Duration of AF 5±4 6±7 0.42CHADS2 score (median) 1 1 0.75LA diameter (mm) 45±6 45±6 0.55
PO3-136
ADDITIONAL DIPYRIDAMOLE EFFECT IN ADENOSINE-INDUCED DORMANT CONDUCTION AFTER PULMONARY VEIN ISOLATIONKohei Iguchi, MD, Kazuhiro Satomi, MD, PhD, Koji Miyamoto, MD, Yuko Yamada, MD, Hideo Okamura, MD, Takashi Noda, MD, PhD, Takeshi Aiba, MD, PhD, Naohiko Aihara, MD, Shiro Kamakura, MD, PhD and Wataru Shimizu, MD, PhD. National Cerebral and Cardiovascular Center, Suita, Osaka, JapanIntroduction: Transient reconnection of the isolated pulmonary vein (PV) is induced by administration of adenosine triphosphate (ATP). Recent reports suggested that elimination of these dormant PV conductions by additional radiofrequency (RF) applications could reduce the recurrence after PV isolation. However, the elimination of dormant conduction is sometimes challenging due to its short time duration. We hypothesized that dipyridamole, which is phosphodiesterase inhibitor increasing adenosine levels, can augment dormant conduction.Methods: 128 drug-refractory symptomatic paroxysmal AF patients (99 men, aged 62 ± 12 years) underwent circumferential PV isolation(PVI). In 85 of 128 (66%) patients, solely ATP (20mg) was administered after PV isolation (ATP group). The additional dipyridamole (0.16mg/kg) injection following ATP (20mg) was administered in 42 of 128 (34%) patients (DP+ATP group).Results: Dormant conduction was observed in 31 patients (38%) of ATP group and in 25 (61%) of DP+ATP group (P=0.017), including persistent PV reconnection in 7% and 12% (NS), and transient conduction in 30% and 49% (p=0.04). Mean duration of transient dormant conduction was significantly longer in DP+ATP compare to ATP (16.4±8.3 vs 55.6±44.7 sec; p < 0.001). Transient AF was initiated in 4 patients (5%) just after solely ATP injection and 2 (5%) after DP+ATP injection.Conclusions: Additional dipyridamole administration significantly augmented frequency and duration of ATP-induced dormant conduction after PV isolation. Prolonged duration of ATP-induced dormant conduction can be helpful for additional applications and may contribute the reduction of the recurrence of AF after PV isolation.
PO3-137
DOES ABLATION OF THE ACUTE RECONNECTION SITE DURING ATRIAL FIBRILLATION ABLATION ENSURE THE PERSISTENT ISOLATION OF THAT ANATOMICAL SEGMENT?Larraitz Gaztañaga, MD, Kyoung- Min Park, MD, David Lin, MD and Francis E. Marchlinski, MD. Hospital of the University of Pennsylvania, Philadelphia, PAIntroduction: Identifying and reablating acute reconnection during pulmonary vein isolation (PVI) is done to decrease

S273Poster Session III
(20%) procedures among 51 patients and categorized into 6 types (types 1, 3, 4 and 5 led to spurious diagnosis of block; types 2 and 6 led to erroneous diagnosis of absence of block). There were 14, 10, 17, 2, 15 and 3 (total=61) cases of pitfall-types 1 through 6 respectively. Operator recognized 43/61 (70%) pitfalls intraprocedurally. Recognition of types 1 and 5 was difficult due to indiscernible electrograms at usual amplifier-settings or presence of very slow conduction mimicking block.Conclusions: Every fifth assessment of bidirectional block across MI linear lesion using differential CS and left appendage pacing techniques encounters a pitfall, which can lead to erroneous clinical diagnosis of block or absence of block. Online recognition of pitfall is feasible and necessitates careful distinction of far-field left atrial from the local CS electrograms besides appropriate adjustments in catheter position and pacing outputs
PO3-140
EXCLUSIVE CIRCUMFERENTIAL PULMONARY VEIN ISOLATION IN PERSISTENT ATRIAL FIBRILLATION: THE ROLE OF PREPROCEDURAL PATIENT SELECTIONClaudia Herrera Siklody, MD, Jochen Schiebeling-Römer, MD, Konstantinos Letsas, MD, Amir Jadidi, MD, Reinhold Weber, MD, Dietrich Kalusche, MD, FHRS and Thomas Arentz, MD. Herz Zentrum Bad Krozingen, Bad Krozingen, GermanyIntroduction: Patients (pts) with persistent (Per) atrial fibrillation (AF) often receive aggressive ablation approaches. We hypothesized that pts with Per AF that could be successfully held in sinus rhythm (SR) through cardioversion (DC) and antiarrhythmic drug therapy (AAD) represent a healthier subgroup that would have similar success rates than pts with paroxysmal (Px) AF after exclusive large pulmonary vein isolation (PVI).Methods: We included 239 consecutive pts, 114 with Px and 125 with Per drug-resistant symptomatic AF. In pts with Per AF, every effort was made to maintain SR around ablation, by means of DC 6 weeks before the procedure under an intensified AAD. Ablation consisted in large circumferential PVI. Clinical follow-up, including 24-hour Holter and event monitoring, was conducted 6 and 17±9 month after ablation. Success was defined as no atrial arrhythmias >30 seconds without AAD.Results: In the Per group, SR could be maintained until ablation in 103/125 pts (82%) (SR group). The remaining 22 pts presented with AF despite the enhanced AAD (AF group). As expected, Per AF pts had a higher incidence of structural heart disease and larger left atria than the Px group, but there were no significant baseline differences between the SR and the AF group. Success rates were comparable 17±9 months after a single procedure in the Px and the SR groups (57% vs 52%,
administration were assessed and plotted against each other. Maximal ACT as well as body weight adjusted heparin amount (in IU) needed to achieve a target ACT >300s were assessed.Results: The mean INR was 2,1±0,4 and mean baseline ACT was 143±33 s. The mean maximal ACT was 309 ± 43 seconds and a mean of 119±42 U/kg heparin was needed to achieve an ACT >300s. The plotting of preprocedural INR against baseline ACT showed - although statistically significant - only a weak correlation with a correlation coefficient of 0.18.Conclusions: As there is only a weak correlation of preprocedural INR and baseline ACT, we conclude that ACT measurements in patients on therapeutic INR are not helpful to assess the overall anticoagulation state of the patient. Additionally, preprocedural INR cannot be used for estimating heparine doses necessary to achieve ACT > 300.
PO3-139
PREVALENCE AND TYPES OF PITFALL IN THE ASSESSMENT OF MITRAL ISTHMUS LINEAR CONDUCTION BLOCKAshok J. Shah, MD, MBBS, Patrizio Pascale, MD, Shinsuke Miyazaki, MD, Xingpeng Liu, MD, Laurent Roten, MD, Nicolas Derval, MD, Amir S. Jadidi, MD, Daniel Scherr, MD, Stephen B. Wilton, MD, Michala Pedersen, MD, Sebastien Knecht, MD, PhD, Frederic Sacher, MD, Pierre Jais, MD, Michel Haissaguerre, MD and Meleze Hocini, MD. Hopital Cardiologique du Haut Leveque, Electrophysiology Services, Bordeaux, FranceIntroduction: To identify and understand pitfalls encountered in the assessment of transmitral conduction block using differential pacing techniques in patients with left mitral isthmus (MI) linear ablation.Methods: N/AResults: All the assessments of MI block were thoroughly reviewed in 271 MI ablation procedures undertaken among 238 patients presenting with paroxysmal or persistent AF from October 2008 to April 2011. Bidirectional block was established in 186/271 (69%) procedures. Careful evaluation of electrograms recorded on the multipolar coronary sinus (CS) and ablation catheters was undertaken to identify and understand the characteristics of pitfall, if any. Pitfall was encountered in 55/271

S274 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
with endocardial segmental ablation. No peri-procedural complications were reported.Conclusions: These findings suggest the presence of a distinct electrical connection between the CS and the LAA. The clinical relevance of our results requires further investigation.
PO3-142
PROGRESSIVE ABNORMALITIES IN CALCIUM HANDLING UNDERLIE ATRIAL ARRHYTHMIAS DURING THE DEVELOPMENT OF EXPERIMENTAL HEART FAILUREReza Wakili, MD, Xiao Yan Qi, PhD, Masahide Harada, MD, PhD, Niels Voigt, MD, Chia-Tung Wu, MD, Mario Talajic, MD, Stefan Kääb, MD, Dobromir Dobrev, MD and Stanley Nattel, MD. University Hospital Munich, Munich, Germany, Montreal Heart Institute, Montreal, QC, Canada, Division of Experimental Cardiology, Medical Faculty Mannheim, University of Technology Mannheim, Mannheim, GermanyIntroduction: Heart failure (HF) is a common cause of atrial fibrillation (AF) in the role of Ca2+ handling abnormalities and underlying mechanisms are poorly understood. This study assessed the temporal relationships among left atrial (LA) Ca2+ handling remodeling and arrhythmogenesis during HF development.Methods: HF was induced by ventricular tachypacing (VTP, 240 bpm) in dogs for 0 h (CTL), 12 h, 24 h, 1 wk or 2 wks (n=5/group). Holter recordings and EP studies were obtained in vivo. Cell Ca2+ transients, sarcoplasmic reticulum (SR) Ca2+ content (integrated NCX) were assessed in LA cardiomyocytes by fluorescence (Indo1 AM), triggered activity by patch clamp.Results: Hemodynamic indices show progressive HF development (Fig. A). Ca2+ transient amplitude (CaT) increased within 12 hrs (Fig. B), while SR Ca2+ content showed a delayed increase, reaching significance after 1wk (Fig. C). SERCA activity was upregulated after 24 hrs, further increasing over time (Fig. D). Development of DAD-related triggered activity (Fig. E) was delayed compared to CaT changes, but paralleled SR Ca2+ content increases and was accompanied by increased number of PACs (Fig. F) and spontaneous atrial tachyarrhythmias in vivo (Fig. G).Conclusions: VTP-induced HF causes rapid changes in Ca2+ transients followed by upregulated SERCA activity and increased SR Ca2+ loading. Triggered activity correlates with increased SR Ca2+ stores and spontaneous ectopy in vivo. These results indicate that HF causes an evolving pattern of Ca2+ handling remodeling and arrhythmogenesis, and suggests that DADs due to SR Ca2+ overload cause spontaneous atrial ectopy.
p=0.445), but dramatically lower in the AF group (27%, p=0.02).Conclusions: In pts with Per AF who can be stabilized in SR with an enhanced AAD, exclusive large complete PVI offers a good success rate, comparable to Px AF pts. A simpler ablation approach can be offered to these pts.
PO3-141
UNUSUAL PATTERN OF ISOLATION OF THE LEFT ATRIAL APPENDAGELuigi Di Biase, MD, PHD, FHRS, Miguel Valdebbarrano, MD, Javier E. Sanchez, MD, Pasquale Santangeli, MD, Rong Bai, MD, Prasant Mohanty, MPH, Agnes Pump, MD, Rodney Horton, MD, G.Joseph Gallinghouse, MD, Sanghamitra Mohanty, MD, Rachel (Xue) Yan, BS, Barbara Thomas, RN, Tami Metz, RN, Greg Gilbert, RN, Salwa Beheiry, RN, Richard Hongo, MD, Douglas Gibson, MD, Claude S. Elayi, MD, J. David Burkhardt, MD and Andrea Natale, MD, FHRS. Texas Cardiac Arrhythmia Institute, Austin, TX, Methodist DeBakey Cardiology, Houston, TX, Department of Biomedical Engineering, University of Texas, Austin, TX, California Pacific Medical Ctr,, San Francisco, CA, California Pacific Medical Ctr, San Francisco, CA, Scripps Clinic, San Diego, CA, University of Kentucky, Lexington, KYIntroduction: Catheter ablation of adjunctive atrial sites together with pulmonary veins isolation has shown to improve the success rate in patients with non paroxysmal atrial fibrillation (AF). AF triggers within the coronary sinus (CS) and the left atrial appendage (LAA) have been recognized as non PV triggers of the AF. The aim of our study is to report unusual pattern of LAA isolationMethods: 488 consecutive patients undergoing catheter ablation for persistent or long standing persistent AF and showing firing from the LAA and or from the CS have been enrolled in this multicenter prospective study. In all patients defragmentation of the CS to achieve isolation and LAA isolation was attempted both with endocardial and epicardial ablation. During CS ablation, the circular mapping catheter was positioned into the LAA.Results: In 7% of these cases (34 pts) after attempting endocardial LAA isolation, the LAA was isolated during epicardial ablation in the distal CS. In 8% of the cases (39 pts) after attempting endocardial LAA isolation, the LAA was isolated during ablation along the endocardial CS (figure). In all these cases the presence of a venous branch connecting the CS with the LAA was found. In 23% of the cases (112 pts), the isolation of the LAA also isolated the distal CS. In all these cases LAA dissociated firing was present together with the CS recording. In all the remaining cases 69% (337 pts) LAA could be isolated

S275Poster Session III
catheter in 77.8% and cryo in 13.4%. A 3D mapping system was used in 77.4%, remote navigation in 7.4% and rotational angiography in 4%. Pulmonary vein isolation was attempted in 98.4% of cases achieving bidirectional block in 88%. Left atrial linear lesions were done in 21.3% (significantly more frequent in non-paroxysmal AF). The SVC was ablated in 2.6% and the CTI in 17.4%. Complex fractionated electrograms were targeted in 17.9% and ganglionated plexi in 3.3%. The median duration of the ablation was 180 min (IQR 130-220) and the fluoroscopy time 26 min (IQR 15-45). Complications occurred in 7.7%, of which 1.7% was major (i.e. perforation, MI, endocarditis, cardiac arrest, stroke, hemothorax, pneumothorax, sepsis).Conclusions: The AF Ablation Pilot Study provides relevant information on the technique and safety of AF ablation procedures across Europe. A single follow-up visit at 1 year will provide mid-term clinical outcomes.
PO3-144
SAFETY AND EFFICACY OF HIGH POWER ENERGY DELIVERY OVER THE POSTERIOR WALL OF THE LEFT ATRIUM GUIDED BY 2-D ECHOCARDIOGRAPHY REAL-TIME VISUALIZATION OF ESOPHAGUS DURING AF ABLATIONMontawatt Amnueypol, MD, Koonlawee Nademanee, MD, FHRS, Mark Schwab, MD, Malamud Ariel, MD and Frances Lee, RN. Pacificrim-EP, Los Angeles, CA, Maui Memorial Medical Center, Wailuku, HI, White Memorial Medical Center, Los Angeles, CAIntroduction: To investigate, the safety and efficacy of RF ablations with high RF power on the posterior wall of the left atrium in AF patients. We carried out the following study aiming to test the hypothesis that if we could identify esophagus (Eso) by real-time 2-D integrated intracardiac echocardiography (2D-ICE) imaging, we could titrate RF power according to Eso location in real time to maximize the lesion formation while minimizing complication.Methods: Forty - three consecutive patients (mean age= 70; 18 F (40%) underwent AF ablation guided by complex fractionated atrial electrogram mapping (CFAE). The ablations were performed with open-irrigated tip catheter with power ranging from 30-50 watts. The RF power was limited to 35 watts in the posterior wall for 30 seconds to one minute unless Eso was visualized by 2D-ICE; we increased power to 50 watts in the posterior wall area > 1 cm. far from the esophagus, but limited to only 30 watts for 30 seconds at the areas abutting Eso. The patients were divided into 2 groups (Gr): Gr.I (N=24) underwent AF ablation with 2D-ICE and Gr.II (N=19), AF ablations were performed without Eso. endoscopy was performed 1-2 days after the AF procedure.Results: Both groups had comparable clinical characteristics. All patients had successful AF ablation reaching acute end points of AF termination to sinus rhythm and/or non-inducible AF. There were no major complications (stroke, cardiac tamponade or major bleeding). There were no differences in the number of RF applications (82+39 vs. 70+33, Gr.I vs. Gr.II, P=.315) and durations (52±22 vs. 44±18, p=.225). Eso injuries occurred less frequently in Gr.I patients (3 exudates (12%) without ulceration and 1 erythema (4%)) compared to Gr.II patients (2 ulceration (11%) resolved after 1 month and 5 erythema (26%)). There was no fistula in both groups.Conclusions: Our data suggest that real-time visualization of Eso using 2-D echo imaging integrated with electroanatomical map safely allows RF power titration during AF ablation on the posterior wall. Higher RF power than the traditional 35 watts with open-irrigated tip catheter is safe and may yield more effective RF lesion formation.
PO3-143
THE ATRIAL FIBRILLATION ABLATION PILOT STUDY: EUROPEAN SURVEY ON THE METHODS, EFFICACY, AND SAFETY OF CATHETER ABLATION FOR ATRIAL FIBRILLATION; CONDUCTED BY THE EUROPEAN HEART RHYTHM ASSOCIATIONElena Arbelo, MD, PhD, Gerhard Hindricks, MD, PhD, Aldo Maggioni, MD, PhD, Luigi Tavazzi, MD, PhD, Panos Vardas, MD, PhD, Cécile Laroche, BSc, Josep Brugada, MD, PhD, the Atrial Fibrillation Ablation Pilot Study Investigators. Hospital Clinic de Barcelona, Barcelona, Spain, Heart Center. University of Leipzig, Leipzig, Germany, ANMCO Research Center. Florence, Italy, Florence, Italy, GVM Care and Research, E.S. Health Science Foundation, Maria Cecilia Hospital,, Cotignola, Italy, Heraklion University Hospital, Crete, Greece, EORP Department. European Society of Cardiology, Sophia, Antipolis, FranceIntroduction: The Atrial Fibrillation Ablation Pilot Study is a prospective, multinational registry conducted by the European Heart Rhythm Association of the European Society of Cardiology designed to describe the epidemiology of patients undergoing an atrial fibrillation (AF) ablation, and the diagnostic/therapeutic processes applied across Europe. We describe the procedure-related data during the in-hospital phase.Methods: A total of 72 Centres in 10 European countries were asked to enrol 20 consecutive patients undergoing a first AF ablation procedure. Site selection targeted hospitals with a medium-high expertise (≥50 AF ablations/year). A web-based case report form captured information on pre-procedural, procedural and follow-up data.Results: The median annual number of AF ablations per centre was 179 (IQR 80-346). Between October 2010 and May 2011, 1410 patients were included, of which 1391 underwent an AF ablation (99%). All centers included paroxysmal AF, 95.8% also included persistent and 44.4% also included long-lasting AF. In 19 patients the ablation was not done due to intracardiac thrombus (7 p), cardiac tamponade during transeptal puncture (7 p), a cerebrovascular event (1 pt) or non-procedure-related complications (4 p). Indications for ablation were symptomatic AF in 90%. The ablation was done with an open irrigation-tip

S276 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
Results: The mean International Normalized Ratio (INR) was 1.92±0.51 at the time of the procedure. The mean activated clotting time values at the time of sheath removal were 340±74 seconds. The total procedural time was 189±60 minutes. Only one patient experienced re-bleeding and massive hematoma, and that patient’s INR was 2.96. Neither pseudoaneurysm, device-related complications, nor deep vein thrombosis occurred. Hemostasis was safely achieved with only 5 minutes manual compression in 98.4% (62/63) of the procedures.Conclusions: A kolin-filled pad yielded prompt and safe hemostasis. Patients with high INR values therefore require careful attention.
PO3-147
IMPACT OF IMPAIRED LEFT VENTRICULAR FUNCTION ON THE ABLATION OF PAROXYSMAL ATRIAL FIBRILLATION: INSIGHTS AND RESULTS OF THE MULTICENTER GERMAN ABLATION REGISTRYMalte Kuniss, MD, Thomas Neumann, MD, Karl Heinz Kuck, MD, Dietrich Andresen, MD, Stephan Willems, MD, Johannes Brachmann, MD, Ellen Hoffmann, MD, Christopher Piorkowski, MD, Rüdiger Becker, MD, Lars Eckardt, MD, Thorsten Lewalter, MD, Claus Jünger, MD and Jochen Senges, MD. Kerckhoff Heart and Thorax Center, Dept of Cardiology, Bad Nauheim, Germany, Asklepios Klinik St. Georg, Hamburg, Germany, Vivantes Klinikum, Berlin, Germany, University Heart Center, Hamburg, Germany, Klinikum Coburg, Coburg, Germany, Städt. Klinikum München Klinik Bogenhausen, München, Germany, Rhön Klinikum Herz- und Gefäßklinik, Bad Neustadt, Germany, Med. Klinik University Hospital, Heidelberg, Germany, Heart Center University Hospital, Münster, Germany, Isar Heart Center, München, Germany, Institut für Herzinfarktforschung Ludwigshafen, Ludwigshafen, GermanyIntroduction: Pulmonary vein isolation (PVI) is an established treatment option of drug refractory paroxysmal atrial fibrillation (PAF). The possible impact of impaired left ventricular function (LVEF) on the PVI procedure and clinical outcome in “real life” is yet unclear.Methods: Data of the multi-centric prospective German ablation registry were analyzed. A telephonic follow up was performed one year after PVI.Results: From Jan 2007 until Aug 2011 in total 4863 ablation procedures were entered in the registry. Three groups were analyzed regarding LVEF with group A >50% (n=4465), group B 41-50% (n=302) and group C ≤ 40% (n=96), mainly because of structural heart disease. In group A 76.4% of the procedures were performed using RF energy, in 22.3% Cryo was used, in group B 80.5% vs 18.9% and in group C 86.5% vs 12.5% respectively. For RF ablation mostly an irrigated tip catheter was used (69.3% vs 72.2% vs 80.2%) with manually guided PVI in 95.5% vs 97.4% vs 96.3%. As ablation strategy mainly circumferential PVI was performed (83.8% vs 89.4% vs 89.6%), whereas additional linear ablation was performed more frequently in pts with impaired LVEF (17.7% in group C vs 13.5% in group A and 9% in group B). A 3 D mapping was used in 60.7% in group A vs 60.3% and 68.8% in group B and C respectively. PVI as procedural endpoint was achieved in 98.1% in group A vs 96.3% and 97.9% in group B and C. Procedure times were longer in group B and C (185(140-225) and 180(130-213)min) compared to group A (155(120-200)min) with longer fluoro times (A: 26(17-40) min, B: 34(22-53) min, C: 30(20-42) min), p<.001. Rates of severe and moderate procedural complications are similar (A: 3.8%, B: 4.0%, C: 3.3%). At follow up recurrence of PAF was reported in 44.5% in group A vs 38.3% in group B vs 48.2% in group C, p=.16. Antiarrhythmic treatment was found to be similar (group A 33.2% vs. 28.2% and 29.4% in
PO3-145
TRIGGERS FROM THE LEFT ATRIAL APPENDAGE ARE NOT SUPPRESSED AFTER ETHANOL ABLATION OF THE VEIN OF MARSHALL: RESULTS FROM A PROSPECTIVE STUDYRong Bai, MD, Luigi Di Biase, MD, PHD, FHRS, Miguel Valdebbarrano, MD, Javier E. Sanchez, MD, Pasquale Santangeli, MD, Prasant Mohanty, MPH, Agnes Pump, MD, Sanghamitra Mohanty, MD, Rodney Horton, MD, G.Joseph Gallinghouse, MD, Richard Hongo, MD, Douglas Gibson, MD, J. David Burkhardt, MD and Andrea Natale, MD, FHRS. Texas Cardiac Arrhythmia Institute, Austin, TX, Methodist DeBakey Cardiology, Houston, TX, California Pacific Medical Ctr,, San Francisco, CA, Scripps Clinic, San Diego, CAIntroduction: The left atrial appendage (LAA) has been reported as a trigger site for atrial fibrillation (AF). We hypothesize that firing from the LAA could reflect an unsual insertion of the ligament of Marshall. We sought to determine whether the ethanol ablation of the vein of Marshall (VOM) could suppress firing from the LAA.Methods: Eighteen consecutive patients with persistent and long standing persistent AF showing firing from the LAA were enrolled in this prospective study. During the first procedure PVAI plus VOM ethanol ablation were performed. All patients underwent a redo procedure at our Institution via a double transeptal guided by intracardiac echocardiography (ICE). In all cases challenge with high dosage of isoproterenol up to 30 µg was performed.Results: The pulmonary veins remained isolated in all patients except 4 patients where the left inferior pulmonary vein regained conduction. In all patients firing from the LAA was present. In all cases LAA isolation was required at the follow up procedure despite VOM ethanol ablation to eliminate recurrence arrhythmias. The mean time for LAA isolation was 34±8 min. At 14±4 months follow up all patients remained in sinus rhythm.Conclusions: VOM ethanol ablation does not have any impact on the LAA electrical activity and does not suppress its firing. LAA isolation increases the long term success rate in patients showing firing from this structure.
PO3-146
SAFETY AND EFFICACY OF SHORT-TIME COMPRESSION WITH A KAOLIN-FILLED PAD AFTER CATHETER ABLATION OF ATRIAL FIBRILLATIONYoshiyuki Hama, MD, PhD, Yuji Matsudo, MD, PhD, Masahiro Fukuda, MD, Ken Kato, MD and Toshiharu Himi, MD, PhD. Division of Cardiology, Kimitsu Chuo Hospital, Kisaradu, JapanIntroduction: Bleeding and vascular access site complications are an important cause of morbidity after catheter ablation of atrial fibrillation (AF). A newly developed hemostatic pad filled with kaolin causes blood to clot quickly. This study prospectively assessed the safety and efficacy of 5 minutes compression with a kaolin-filled pad after catheter ablation of AF by the femoral approach.Methods: Sixty-three procedures were performed in 61 patients (74% male, mean age 66.1 ± 9.4 years) from April 1st, 2011 to December 2nd, 2011. Warfarin was continued through the procedures. The standard right femoral access employed a 5 French sheath in the right femoral artery and 4 sheaths (8.5 French, two 8 French and 5 French) in the right femoral vein. All patients received multiple sheath removals with the kaolin-filled pad use. Rebleeding, massive hematoma, pseudoaneurysm, device-related complications and deep venous thrombosis were assessed.

S277Poster Session III
dissipate over time and are not due to procedural failure. The transient use of corticosteroid shortly after AF ablation might prevent immediate and mid-term AF recurrence. However, the effective dosage for preventing AF recurrence has not been determined. In this study, we evaluated whether low-dose hydrocortisone (< 200 mg) is also effective for the prevention of AFrecurrence after radiofrequency catheter ablation (RFCA).Methods: We enrolled 89 consecutive AF patients (70 male, 55.8±10.9 years) who underwent RFCA and were treated with single bolus injection of hydrocorticosteroid of 100 mg. For the control group, we enrolled 120 sex- and age-matched AF patients who underwent RFCA during same period and were not treated with steroid (94 male, 55.4±10.5 years). The body temperature and C-reactive protein level were measured before and on 3 days after ablation.Results: Three (2.5%) and one (1.1%) patients developed pericarditis in control and corticosteroid groups, respectively. While 17 (14.5%) patients had immediate AF recurrence (≤3 days) in the control, 11 (12.4%) patients had in steroid groups (p=0.687). During the mean follow-up of 12 months, low-dose steroid did not decrease early (4~30 days) AF recurrence (13 [11.1%] vs. 11 [12.5%], p=0.829) or late (≥ 31 days) AF recurrence (26 [22.2%] vs. 13 [14.6%], p=0.209) after ablation. There was no difference in cumulative survival free of late AF recurrence between the corticosteroid and control groups (p=0.57 by log-rank test). Interestingly, in the subgroup analysis of the patients with immediate AF recurrences, the prevalence of an AF-free rate at 12 months post-ablation was higher in the corticosteroid group than in the control group (9 of 11 [81.8%] vs. 7 of 17 [41.2%]; p=0.05). WBC count, CRP and maximum body temperature also were not changed by low-dose steroid.Conclusions: Single bolus injection of low-dose hydrocortisone after AF ablation is not effective for preventing immediate or early/late AF recurrence during the mid-term follow-up period. Our study suggests that at least a moderate-dose (≥ 200mg) of hydrocortisone is needed to prevent AF after RFCA.
PO3-150
INCREASED GLOBAL SURFACE ECG PHASE CORRELATION PREDICTS HUMAN VENTRICULAR FIBRILLATION ROTORSDavid J. Morris, MD, Miriam R. Smetak, BS, Siva Mulpuru, MD, Jeffery Ho, MD, Sanjiv M. Narayan, MD, PHD, FHRS and David E. Krummen, MD. UCSD Department of Medicine, San Diego, CA, UCSD School of Medicine, VA Medical Center, Division of Cardiology 111A, San Diego, CAIntroduction: Ventricular fibrillation (VF) is a complex arrhythmia which has been shown to evolve over time to a more regular pattern of activation, but mechanisms which maintain fibrillation are poorly understood. We hypothesized that greater regularity, reflected in the surface ECG and measured by phase correlation (PC) analysis, would indicate the presence of organized electrical rotors.Methods: In patients presenting for VT ablation, 64-electrode basket catheters were introduced into the left and right ventricles, and ventricular arrhythmias were initiated per IRB-approved protocol. Wave similarity analysis was used to identify rotors, defined as organized, rotational activity persisting for > 4 revolutions. PC was defined as the phase relationship between X (ECG lead I), Y (lead aVF) and Z axis (lead V1) pairs during 1 second intervals after VF/PVT induction and prior to termination.Results: In 20 pts (age 63±9 y, EF 39±19%), 23 VF/PVT episodes were induced. A total of 25 VF/PVT rotors were identified, average CL 209±27 msec. Notably, increased global PC was associated with the presence of rotors: average PC was 0.086± 0.015 with no rotors, 0.141± 0.016 with one rotor, and 0.112 ± 0.016 with 2 rotors (p=0.045). Fig A shows XZ
group B and C). PV stenosis was reported in 0.1% and phrenic nerve palsy in 0.4% in group A, in none of the pts in group B and C, no atrio-oesophageal fistula.Conclusions: PVI in pts with mildly to severe impaired LVEF suffering of PAF is safe and successful in the majority of patients. However, PVI in these patients is longer with longer fluoro times with comparable complication rates.
PO3-148
PREVENTION OF PERIPROCEDURAL STROKE AND MANAGEMENT OF HEMORRHAGIC COMPLICATION IN ATRIAL FIBRILLATION ABLATION UNDER CONTINUING WARFARIN ADMINISTRATIONTaishi Kuwahara, MD, Yoshihide Takahashi, MD, Kenji Okubo, MD, Katsumasa Takagi, MD, Masateru Takigawa, MD, Yuji Watari, MD, Kazuya Yamao, MD and Atsushi Takahashi, MD. Yokosuka Kyousai Hospital, Kanagawa, JapanIntroduction: This study aimed to determine the effect of continuing warfarin during periprocedural period of atrial fibrillation (AF) catheter ablation on the prevention of stroke complication and to show a management of hemorrhagic complication occurring in this approach.Methods: A total of 3000 patients undergoing AF catheter ablation in our institute were divided into two groups: the first 1953 patients who discontinued warfarin 3 ~ 4 days before AF ablation and was given heparin and resumed warfarin after the AF catheter ablation (discontinuing group) and the last 1047 patients who continued warfarin throughout the periprocedural period of AF catheter ablation (continuing group).Results: Patients’ background of age, gender, type of AF, CHADS2 score, left atrial diameter and the value of brain natriuretic peptide were not different between the two groups. Symptomatic stroke or transient ischemic attack occurred during periprocedural period in 13/1953 (0.67 %) in the discontinuing group and in 2/1047 (0.19 %) in the continuing group. Two stoke patients in the continuing group showed insufficient international normalized ratio (INR) of 1.23 and 1.57 before AF ablation. Major hemorrhagic complication occurred in 26/1953 (1.3 %, 25 cardiac tamponade and 1 retroperitoneal bleeding) in the discontinuing group and in 10/1047 (1.0 %, 10 cardiac tamponade) in the continuing group. Nine of the 10 patients with cardiac tamponade in the continuing group were given prothrombin complex concentrate (PCC) of 500 ~ 1000 units and vitamin K of 10 ~ 20 mg. The INRs were immediately corrected from 1.7 ~ 2.7 to 1.4 ~ 1.8 and bleeding of cardiac tamponade were safely terminated.Conclusions: AF catheter ablation without discontinuation of warfarin was effective to prevent periprocedural stroke complication. Bleeding of cardiac tamponade in this approach was safely terminated with the use of PCC and Vitamin K.
PO3-149
PREVENTION OF ATRIAL FIBRILLATION RECURRENCE WITH SINGLE BOLUS INJECTION OF LOW DOSE CORTICOSTEROID AFTER RADIOFREQUENCY CATHETER ABLATIONHoyoun Won, MD, Jae-Sun Uhm, MD, Jaemin Shim, MD, Hye Jin Hwang, MD, Jung-Hoon Sung, MD, Jong-Youn Kim, MD, Hui-Nam Pak, MD, PhD, Moon-Hyoung Lee, MD, PhD and Boyoung Joung, MD, PhD. Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea, Republic ofIntroduction: About 50% of early arrhythmias after pulmonary vein isolation (PVI) of atrial fibrillation (AF) spontaneously

S278 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
Conclusions: Amelioration of inter-ventricular conduction delay of RV improved ECG from type-1 to type-2 in some cases with BrS and unmasked BrS ECG in patients with CRBBB. Conduction delay in RV might be related to the development of BrS ECG.
PO3-152
FRAGMENTED QRS COMPLEX REPRESENTS EARLY PHASE OF MYOCARDIAL INVOLVEMENT AND IS A PREDICTOR FOR PROGNOSIS IN PATIENTS WITH MUSCULAR DYSTROPHY HAVING NARROW QRS COMPLEXMasataka Shigetoshi, MD, Hiroshi Morita, MD, PhD, Yutaka Take, MD, Nobuhiro Nishii, MD, PhD, Satoshi Nagase, MD, PhD, Kengo Kusano, MD, PhD and Hiroshi Ito, MD, PhD. Department of Cardiovascular Medicine, Okayama University Graduate School of Medicine, Okayama, Japan, Department of Cardiovascular Theraperutics, Okayama University Graduate School of Medicine, Okayama, JapanIntroduction: Fragmented QRS (fQRS) in 12-lead ECG is a convenient and useful marker that represents intraventricular myocardial scaring and can predict the prognosis of patients with various heart diseases such as acute coronary syndrome, Brugada syndrome, and arrhythmogenic right ventricular dysplasia. Ventricular myocardium dysfunction in muscular dystrophy (MD) defines patients’ outcome but progression of the disease resulted in heart failure and conduction disturbance, such as left or right bundle branch block. There is no useful marker of the early phase of myocardial involvement in MD. We hypothized that fQRS in patients with MD represented early phase of myocardial involvement of the disease and evaluated clinical significance and impact of the fQRS on the prognosis in patients with MD having narrow QRS complex.Methods: We evaluated 30 patients with sinus rhythm and narrow QRS intervals (≤120ms) diagnosed as MD (age: 24 ± 17 yrs; ejection fraction 63 ± 16%): 12 patients with Duchenne/Becker MD, 15 patients with myotonic MD, 2 patients with Limb-gardle MD, 1 patient with Fukuyama type congenital MD). fQRS was defined as additional multiple spikes within the QRS complex in 2 anatomical contiguous leads. We evaluated the ECG markers and occurrence of cardiac events (death, sustained ventricular tachycardia, and admission for heart failure) during follow-up periods (56 ± 31 months) in patients with and without fQRS.Results: fQRS was observed in 10 patients (33%). There were no differences in age, sex, ejection fraction between patients with and without fQRS. In ECG markers, there were no differences in RR, PQ, QRS and QT intervals between patients with and without fQRS. Cardiac events occurred in 4 patients with fQRS (60%) but did not occur in patients without fQRS during follow-up: Patients suffered from death in 1 patient, sustained ventricular tachycardia in 3 patients and congestive heart failure in 2 patients. Univariate analysis showed fQRS was only a predictor for cardiac event in patients with MD (p<0.01).Conclusions: Existence of fQRS was a predictor of cardiac events in patients with MD having narrow QRS interval. fQRS might be useful for detecting early phase of cardiac involvement in patient with MD.
PO3-153
PREDICTORS OF VENTRICULAR FIBRILLATION DURING THE FIRST 48 HOURS OF ST-ELEVATION MYOCARDIAL INFARCTION IN PATIENTS TREATED WITH PRIMARY PCIMarina M. Demidova, MD, J. Gustav. Smith, MD, Fredrik Holmqvist, MD, PhD, Jonas Carlson, PhD, David Erlinge, MD, PhD and Pyotr G. Platonov, MD, PHD, FHRS. Federal Centre of Heart, Blood and Endocrinology, St-Petersburg, Russia and
plane PC during VF in a patient with 2 rotors. Fig B shows the simultaneous isochronal analysis with rotor core at green arrow in the basilar, posterolateral left ventricle. Fig C shows XZ plane PC during a different episode of VF without rotors; note the disorganized PC plot (blue star).Conclusions: Global PC is correlated with the number of rotors during VF. This may have implications for managing patients with disorganized ventricular arrhythmias.
PO3-151
AMELIORATION OF INTER-VENTRICULAR CONDUCTION DELAY OF RIGHT VENTRICLE IMPROVES ELECTROCARDIOGRAM FROM TYPE-1 TO TYPE-2 IN PATIENTS WITH BRUGADA SYNDROMEKoji Nakagawa, MD, Satoshi Nagase, MD, Masamichi Tanaka, MD, Nobuhiro Nishii, MD, Kazufumi Nakamura, MD, Kunihisa Kohno, MD, Hiroshi Morita, MD, Kengo Fukushima. Kusano, MD, Tohru Ohe, MD and Hiroshi Ito, MD. Department of Cardiovascular Medicine, Okayama University Graduate School of Medicine, Okayama, Japan, The Sakakibara Heart Institute of Okayama, Okayama, JapanIntroduction: Brugada syndrome(BrS) is associated with sudden cardiac death, and typical type-1 ECG is crucial for the diagnosis of BrS and the development of fatal tachyarrhythmia. However, it is still controversial whether depolarization or repolarization abnormalities are responsible for the development of BrS ECG. Tissue Doppler echocardiographic studies demonstrated that the extent of conduction delay between right ventricle(RV) and left ventricle is considered to correlate with BrS ECG. On the other hand, typical BrS ECG is sometimes masked by the coexistence with complete right bundle branch block(CRBBB). In this study, we examined the association between the morphology of BrS ECG and the inter-ventricular conduction delay using RV single extrastimulus.Methods: In consecutive 16 BrS patients, progressively premature single extrastimuli were delivered from RV apex against patients’ own RV depolarization to ameliorate inter-ventricular RV conduction delay in electrophysiologic study. We evaluated the morphologic changes in surface ECG created by single extrastimulus.Results: Type-1 ECG was observed in all patients at baseline or after pilsicainide administration. In 10 of 16 patients, type-1 ECG changed to type-2 ECG by single extrastimulus(Figure-1A). Especially in all 5 patients with CRBBB, single extrastimulus changed their ECGs to typical type-1 or type-2 BrS ECG(Figure-1B).

S279Poster Session III
arrhythmia; p<0.0001 for VT/VF vs. no arrhythmia). After 3.2±2 years of follow-up, 4 (14.3%) pts with NSVT, 17 (55%) with VT/VF, and 263 (12%) with no arrhythmia died (Figure) (p=0.5 for NSVT vs. no arrhythmia; p<0.0001 VT/VF vs. no arrhythmia). All patients with NSVT who died had EF < 55%.Conclusions: Non-sustained ventricular tachycardia after cardiac surgery is not associated with long-term mortality except in patients with left ventricular dysfunction. However, mortality is high in patients who had cardiac arrest due to VT/VF.
PO3-155
USEFULNESS OF REVISED TASK FORCE CRITERIA IN PATIENTS WITH RIGHT VENTRICULAR OUTFLOW TRACT TACHYCARDIA: IMPLICATION FOR THE STRATIFICATION OF MORTALITY AND UNSTABLE VENTRICULAR ARRHYTHMIASMan-Cai Fong, MD, Fa-Po Chung, MD, Yenn Jiang Lin, MD, Shih-Lin Chang, MD, Li-Wei Lo, MD, Yu-Feng Hu, MD and Shih-Ann Chen, MD. Chen Hsin General Hospital, Taipei, Taiwan, Taipei Veterans General Hospital, Taipei, TaiwanIntroduction: Patients with RVOT-T without fulfilling the revised TF criteria may carry the risk of sudden cardiac death and clinical outcome based on revised TF criteria has not been elucidated clearly. The purpose of present study was to investigate the application of revised TF criteria in patients with RVOT-T to stratify the risk of mortality and unstable ventricular arrhythmias.Methods: A total of 179 patients with clinically-documented RVOT-T were enrolled consecutively. The revised TF criteria were used for scoring, defining 1 major as 2 points and 1 minor as 1. All patients were categorized into 3 groups: TF<2 (n=114), TF=3 (n=32), and TF>4 (n=33), to assess unstable VT and mortality according to the Taiwan National Mortality Registration.Results: All patients received endocardial mapping and catheter ablation of RVOT-T with a successful rate of 95 %. Twenty two of 179 patients (12.3%) underwent an ICD implantation for aborted sudden cardiac death and hemodynamic unstable ventricular arrhythmias, including 2 (1.8%) in TF<2, 7 (21.9%) in TF=3, and 13 (39.4%) in TF>4. During a mean follow-up duration of 49±44 months, a total of 11 events (6.1%) were documented, including all-cause mortalities in 6 patients (3.4%) [2 (1.8%) in TF<2, 2 (6.3%) in TF=3, and 2 (6.1%) in TF>4] and unstable ventricular arrhythmias in 6 (3.4%) [0 (0%) in TF<2, 2 (6.3%) in TF=3 and 4 (12.1%) in TF>4]. Using Cox regression analysis, the revised TF
Lund University, Lund, Sweden, Lund University, Lund, SwedenIntroduction: Ventricular fibrillation (VF) is common in the acute phase of ST-elevation myocardial infarction (STEMI) and markedly increases in-hospital mortality. As rapid defibrillation is highly effective, identification of patients at high risk of VF is clinically relevant. Our aim was to analyze clinical characteristics associated with VF in an unselected population of STEMI patients.Methods: Our study population comprised of 1714 consecutive STEMI patients (age 66±12, 70% male) admitted to a Swedish tertiary care hospital for primary PCI during 2007-2009. Using the Register of Information and Knowledge about Swedish Heart Intensive care Admissions (RIKS-HIA) registry, 121 patients (7.0%) with VF in the first 48 hours after STEMI were identified (72 before and 49 after reperfusion). Clinical and angiographic characteristics were tested for association with VF using logistic regression analysis.Results: In univariate analyses, increased risk of VF during the first 48 hrs of STEMI was observed for current smoking, history of myocardial infarction, use of aspirin, beta-blockers, digitalis and statins, serum creatinine and left main coronary arterial disease. In a multivariate analysis, current smoking (OR 2.82; p=0.001, 95%CI 1.49-5.32), beta-blockers (OR 2.47; p<0.001, 95%CI 1.54-3.96), digitalis (OR 4.70; p=0.005, 95%CI 1.58-13.94) at admission and left main disease (OR 3.11; p=0.001, 95%CI 1.61-5.98) remained independently associated with VF during the first 48 hrs. Beta-blockers (OR 2.04; p=0.003, 95%CI 1.27-3.27) and digitalis (OR 3.34; p=0.035, 95%CI 1.09-10.22) at admission remained independent predictors of VF before reperfusion. VF was not significantly associated with age, gender, body mass index, history of hypertension, heart failure, diabetes, stroke, PCI, CABG or infarct (all p>0.05).Conclusions: Independent predictors of early VF in STEMI patients include beta-blocker therapy at admission, likely indicating underlying structural heart disease, current smoking, digitalis at admission and left main disease. A potentially proarrhythmic effect of digitalis is further supported by association with VF before reperfusion.
PO3-154
LONG-TERM PROGNOSIS OF PATIENTS WITH VENTRICULAR ARRHYTHMIAS AFTER CARDIAC SURGERYFarzad Azimpour, MD, Henri Roukoz, MD and Selcuk Adabag, MD. Division of Cardiology, University of Minnesota, Minneapolis, MN, Divison of Cardiology, Minneapolis VA Medical Center, Minneapolis, MNIntroduction: The significance of post-operative ventricular arrhythmias after cardiac surgery is unclear. We sought to determine the long-term prognosis of patients (pts) with non-sustained ventricular tachycardia (NSVT) and cardiac arrest from ventricular tachycardia/fibrillation (VT/VF) after cardiac surgery.Methods: We included 2271 consecutive pts who underwent cardiac surgery at the Minneapolis VA Medical Center from 2004 to 2011. Patients with NSVT and cardiac arrest due to VT/VF were identified from electronic medical records. Mortality was assessed from the national VA Continuous Improvement in Cardiac Surgery Program database.Results: The mean age was 66±10 years, 99% of the pts were male and 68% underwent coronary artery bypass graft surgery only. A total of 28 (1.2%) pts had NSVT and 31 (1.4%) had VT/VF 4.7±5.3 and 4.2±5 days after the operation, respectively. Of the 28 pts with NSVT, 6 subsequently had VT/VF but only 1 died postoperatively. Thus, 30-day postoperative mortality was 3.6% (n=1) in pts with NSVT, 45% (n=14) in those with VT/VF and 1.6% (n=35) in pts with no arrhythmias (p= 0.46 for NSVT vs. no

S280 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
MDCT data of wall thickness and coronary anatomy is useful for the guidance of mapping/ablation.
PO3-157
CHARACTERIZATION OF EPICARDIAL LATE POTENTIAL ACTIVATION IN LEFT VENTRICULAR NONISCHEMIC CARDIOMYOPATHYBrian P. Betensky, MD, Harris M. Haqqani, MBBS, PhD and Francis E. Marchlinski, MD. Hospital of the University of Pennsylvania, Philadelphia, PAIntroduction: In pts with nonischemic cardiomyopathy (NICM) and VT, the organization of epicardial (EPI) isolated late potential (ILPs) remains unknown. Identification of unique patterns of ILP propagation may provide insight into arrhythmogenesis and help identify novel ablation targets.Methods: Electroanatomic maps of pts undergoing ENDO/EPI VT ablation were reviewed. ENDO bipolar (bp)(<1.5mV), unipolar (<8.3mV) and EPI bp scar (<1.0mV) were quantified. An activation map of the ILPs (high frequency component post-QRS and/or >20ms isoelectric interval from initial electrogram (EGM)) was created (QRS-ILP EGM).Results: Sinus voltage maps of 23 pts (EF 33.4±11.0%, 5 LBBB) with NICM and VT were studied. EPI bp scar area (65.8±38.8cm2) correlated (r =0.533, p=0.041) with Endo unipolar scar (45.3±46.4cm2) and predominated in the basal-lateral region (20pts). ENDO bp scar (19.5±29.5cm2) was less extensive (absent in 8pts) and identified in the basal-lateral (7pts) and/or basal-septal (8pts) regions. EPI ILPs occurred in networks of well-defined activation patterns (Figure) in areas of low voltage. Earliest coupled ILPs corresponded to scar border and latest coupled ILPs to the opposite edge (linear-73%) or center (collision-13%, centripetal-9%) of scar.Conclusions: In NICM 1)EPI bp low voltage was greater than ENDO and often predicted by ENDO unipolar voltage 2)ILP activation in SR of EPI basal-lateral scar originates at the EPI low voltage border and proceeds through scar in discrete patterns 3)The onset of delayed activation wavefronts at the edge of scar may serve as appropriate target for VT ablation and allow more extensive ILP elimination with limited ablation.
predicted further mortality and unstable ventricular arrhythmias in patients with RVOT-T (P=0.02; Figure).Conclusions: Scoring system based on revised TF criteria in RVOT-T patients stratified the risk of unstable VT and mortality during long-term follow- up.
PO3-156
MYOCARDIAL WALL THINNING CORRELATES WITH SITES OF LOCAL ABNORMAL VENTRICULAR ACTIVITIES IN ISCHEMIC PATIENTS UNDERGOING CATHETER ABLATION FOR VENTRICULAR TACHYCARDIA: A COMPUTED TOMOGRAPHY STUDY USING IMAGE INTEGRATIONYuki Komatsu, MD, Hubert Cochet, MD, Amir S. Jadidi, MD, Daniel Scherr, MD, Frederic Sacher, MD, Nicolas Derval, MD, Ashok Shah, MD, Laurent Roten, MD, Patrizio Pascale, MD, Shinsuke Miyazaki, MD, Maxime Sermesant, PhD, Jatin Relan, PhD, Michel Montaudon, MD, François Laurent, MD, Steven J. Kim, MS, Mélèze Hocini, MD, Michel Haïssaguerre, MD and Pierre Jaïs, MD. CHU Bordeaux, Hôpital du Haut-Lévêque, Bordeaux-Pessac, France, INRIA Sophia Antipolis, Sophia Antipolis, France, St. Jude Medical S.C., Inc., St. Paul, MNIntroduction: A majority of patients undergoing VT ablation have implanted devices precluding potential substrate imaging with MRI. Myocardial wall thinning is frequently observed after infarction, and can be accurately quantified using contrast-enhanced multi-detector computed tomography (MDCT). We sought to assess the spatial correlation between wall thinning and local abnormal ventricular activities (LAVA) including fragmented and/or late potentials in patients with postinfarction VT.Methods: Eleven postinfarct patients referred for VT ablation (10 men, age 68 ± 8 yrs) underwent MDCT before ablation. MDCT data was integrated in 3D mapping systems, and registered to high density endo- and epicardial maps acquired in sinus rhythm. Areas of low voltage (<1.5mV) and LAVA were correlated to wall thinning as described at MDCT.Results: Endo- and epicardium were mapped with 495 ± 475 and 1003 ± 636 points/map, respectively. Registration of MDCT allowed visualization of coronary arteries during epicardial mapping/ablation. Wall thinning (<5 mm) was detected in all patients. Low voltage areas corresponded to wall thinning more accurately on the endocardium (accuracy 77%), as compared to epicardium (accuracy 57%). LAVA were located within wall thinning (81% on the endocardium and 67% on the epicardium), or at its border (within 18mm). Very late potentials (isoelectric interval >100ms after QRS) localized in thinnest areas (86% in wall thickness<3mm).Conclusions: Wall thinning spatially correlates to low voltage and LAVA in patients with postinfarction VT. The integration of

S281Poster Session III
PO3-159
ROLE OF ELECTROANATOMICAL MAPPING IN THE DIAGNOSIS OF ARRHYTHMOGENIC RIGHT VENTRICULAR CARDIOMYOPATHYCheng-Hung Li, MD, Yenn-Jiang Lin, MD, Fa-Po Chung, MD, Shih-Lin Chang, MD, Li-Wei Lo, MD, Yu-Feng Hu, MD, Tze-Fan Chao, MD, Chin-Tai Tai, MD and Shih-Ann Chen, MD. Taipei Veterans General Hospital, Yuanshan Br., Yilan, Taiwan, Taipei Veterans General Hospital, Taipei, TaiwanIntroduction: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is characterized by a high incidence of ventricular tachyarrhythmias and sudden cardiac death. In the early stage of ARVC, some patients may present as right ventricular outflow tract tachycardia (RVOT VT). Currently, diagnosis of ARVC is based on Modified Task Force Criteria (TFC) 2010. The role of electroanatomical mapping (EAM) in the diagnosis of ARVC has not been defined. This study aimed to assess the substrate difference and determine the role of EAM in the diagnosis of ARVC.Methods: Among a total of 182 RV VT patients referred to take the electrophysiologic study and catheter ablation, 83 patients with RV endocardial EAM were selected and divided as 2 groups: 1) 68 patients with idiopathic RVOT VT, and 2) 15 patients with ARVC.Results: The age, gender and clinical presentation were similar between groups. ARVC had more RV dyskinesia, and lower RV ejection fraction. EAM substrate characteristics showed more RVOT free wall scar and prolonged RV total activation time in ARVC patients (Table). Multivariate analysis showed RV dysfunction, RV dyskinesia and RV total activation time were independent predictors of ARVC. ROC curve analysis showed RV total activation time with a 72.7% sensitivity and 80% specificity at a cut-off value of 164 ms (AUC 0.76), while sensitivity and specificity are 72.7% and 80% at a cut-off value of 0.5 for the RV dysfunction (AUC 0.764).Conclusions: EAM provides a valuable substrate parameter for the diagnosis of ARVC and serves as a potential diagnostic and prognostic tool in patients presenting with RVOT VT to facilitate clinical decision-making.
PO3-158
ENDOCARDIAL UNIPOLAR VOLTAGE MAPPING COMPARED TO MAGNETIC RESONANCE IMAGING TO CHARACTERIZE THE EPICARDIAL SUBSTRATEBenedetta Majocchi, MD, Michela Casella, MD, PhD, Fabrizio Tundo, MD, PhD, Antonio Dello Russo, MD, PhD, Gaetano Fassini, MD, Stefania Riva, MD, Massimo Moltrasio, MD, Corrado Carbucicchio, MD, Vittoria Marino, MD, Martina Zucchetti, MD, Daniele Andreini, MD and Claudio Tondo, MD, PhD. Centro Cardiologico Monzino, Milano, ItalyIntroduction: Magnetic resonance imaging with delayed contrast enhancement (MRI) can detect topography and transmural extent of myocardial scars. Recent studies show that electroanatomical endocardial unipolar voltage mapping (EEUM) identifies epicardial low-voltage regions. Aim of the study was to compare EEUM with MRI to confirm the capability of EEUM to identify epicardial scars.Methods: In 18 patients (mean age 56 ± 14 years; 17 males; left ventricle EF 45 ± 12 %) with ventricular arrhythmias (39% sustained ventricular tachycardia; 61% premature ventricular beats) a MRI and an electroanatomical mapping by CARTO system (at least 200 points collected) were performed. Four (22%) patients were affected by ischemic cardiopathy, 4 (22%) patients by idiopathic dilated cardiomyopathy, 4 (22%) patients by other cardiomyopathies (arrhythmogenic right ventricular dysplasia, Fabry diasease, myocarditis), in 6 (34%) patients no organic cardiopathy was evident. In 12 patients was performed a right ventricle (RV) EEUM, in 12 left ventricle (LV) and in 6 RV and LV (totally 24 maps). RV maps were divided in four areas (outflow tract, free wall, inferior, apex); LV in five (apex, septum, inferior, anterior, lateral). We classified each area as healthy or scar according to previously reported cut-off values for EEUM <5.5 mV in RV and <8.27 mV in LV. MRI identified in the same ventricular areas the presence of fibrosis. We compared the results of EEUM analysis and MRI.Results: Of 24 maps, 6 (25%) showed concordance for less than 50% of areas, 4 (67%) of RV, 2 (33%) of LV. In 18 (75%) maps, concordance was observed in more than 50% of areas, 10 (56%) of LV and 8 (44%) of RV. In 11 (45%) maps agreement was present in more than 75% of areas, 3 (27%) RV, 8 (73%) LV. Only in 3 (12%) maps, all from RV, there was no concordance at all between MRI and EEUM. In 7 (29%) maps there was a complete agreement between MRI and EEUM mapping, 2 (28%) RV, 5 (72%) LV. Only in one case MRI showed fibrosis with EEUM resulting normal.Conclusions: EEUM correlates with the results of MRI in a high percentage of cases, with more accuracy for left ventricle. Low unipolar voltage at endocardial mapping may suggest the presence of epicardial scar. EEUM can be a useful tool to guide ablation strategy for ventricular arrhythmias.

S282 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
(ENDO) patients may remain inducible for VT. Procedural failure becomes important if VT substrate is excluded from the endocardium by patch material, preventing post-operative catheter ablation. This study aimed to compare the effect of ENDO versus combined endocardial-epicardial cryoablation (ENDO-EPI) on local conduction properties, VT inducibility and VT occurrence.Methods: Seventeen patients (14 male, 64±10 years) with ischemic heart failure referred for LVR, in whom aneurysm related VT (based on 12 lead VT morphology) were induced during programmed electrical stimulation (PES) prior to LVR, were included in the study. After PES, patients were randomized to ENDO or ENDO-EPI cryoablation. During surgery 3 pairs of pacing wires were placed on either side of the presumed ablation line to assess bidirectional conduction block acutely after ablation (overlapping applications, 4mm cryoprobe, 90s, -150°C). Before discharge PES and pacing via the pacing wires were repeated. Patients were followed at our institute.Results: Eight patients were randomized to ENDO and 9 to ENDO-EPI cryoablation. After LVR, PES was repeated in 12 of 17 patients (71%); 2 patients (1 ENDO, 1 ENDO-EPI) had spontaneous VT, 2 died and 1 refused PES. Although VT could be induced in only 1 patient (8%, ENDO), conduction block was achieved in none. During 14±9 months follow up 5 of 15 discharged patients (33%) had spontaneous VT (2 ENDO, 3 ENDO-EPI): 2 patients with spontaneous VT after LVR, 3 (1 ENDO, 2 ENDO-EPI) non-inducible patients after LVR. Two patients died (1 ENDO, heart failure; 1 ENDO-EPI, cancer).Conclusions: Both ENDO and ENDO-EPI cryoablation of the scar borderzone during LVR result in low VT re-inducibility even though no conduction block along the ablation line was achieved. However, the incidence of VT during follow up was high in both groups questioning the value of a postoperative PES to identify patients at risk.
PO3-162
DIRECTED EPICARDIAL TO ENDOCARDIAL BIPOLAR RADIOFREQUENCY ABLATION USING TWO CATHETERS WILL CREATE LARGER LESION COMPARED TO STANDARD UNIPOLAR ABLATIONMatthew D. Olson, MD, Nicholas Phreaner, BA, Russell R. Heath, MD, David F. Katz, MD, Joseph L. Schuller, MD, Wendy S. Tzou, MD, Ryan G. Aleong, MD, Pual D. Varosy, MD, Duy T. Nguyen, MD and William H. Sauer, MD, FHRS. University of Colorado Dept. of Electrophysiology, Aurora, COIntroduction: Standard delivery of radiofrequency ablation energy is “unipolar” as energy flows from a catheter tip electrode (RF+) to a surface patch serving as the electrical anode and ground (RF-). The energy delivered at the catheter/myocardial interface creates an ablation lesion. We hypothesized that using a second catheter serving as the RF- placed on the endocardium (endo) immediately opposite an RF+ on the epicardium (epi) will create larger lesions with improved efficiency of energy and heat delivery.Methods: In a circulating warmed saline bath, viable myocardium was placed in a fixture designed to electrically isolate the epi from endo while saline from a bypass pump washed over the endo. A 3.5 mm externally irrigated ablation catheter was placed over the epi (RF+) while a separate 4mm or 8mm tip catheter was placed on the endo (RF-). Another set of lesions was acquired with the 3.5mm catheter placed on the endo (RF+) and 4mm or 8mm (RF-) on the epi. RF energy was delivered at 50 watts and external irrigation was set to 30cc/min. Bipolar lesion characteristics were compared to a set of epi lesions using standard unipolar ablation.Results: On the epi, RF+ epi to RF- endo 4mm and 8mm
PO3-160
THE EFFECT OF ENCIRCLING ENDOCARDIAL CRYOABLATION DURING LEFT VENTRICULAR RECONSTRUCTION FOR PRIMARY PREVENTION OF VENTRICULAR TACHYCARDIACarine F.B. van Huls van Taxis, MD, Patrick Klein, MD, Sebastiaan R. Piers, MD, Adrianus P. Wijnmaalen, MD, Jerry Braun, MD, Michel I. Versteegh, MD, Harriette F. Verwey, MD, PhD, Martin J. Schalij, MD, PhD, Robert J. Klautz, MD, PhD and Katja Zeppenfeld, MD, PhD. Leiden University Medical Center, Leiden, NetherlandsIntroduction: Surgical LV reconstruction (LVR) is an effective treatment to improve LV function in patients with a LV aneurysm after myocardial infarction. After LVR, up to 25% of the patients without prior ventricular arrhythmias experiences VT in the 19 months following surgery. Endocardial encircling cryoablation (EEC) of the LV aneurysm scar borderzone has shown favorable effects as treatment for VT. The effect of EEC to prevent VT occurrence remains unclear. The purpose of this study was to prospectively evaluate electrophysiological (EP) guided EEC concomitant to LVR for primary prevention of VT.Methods: The study included 45 patients (62±9 years; 36 men) with ischemic heart failure referred for LVR without a history of VT. Prior to LVR, patients underwent EP testing. Patients inducible for reentrant VT related to the aneurysm (based on 12-lead VT morphology) underwent LVR with concomitant EEC (overlapping applications, 4mm cryoprobe, 90s, -150°C) (Group 1). The remaining patients underwent only LVR (Group 2). After discharge patients were followed at our institute. Results: Thirty-one patients (69%) inducible for scar related VT underwent LVR with concomitant EEC (Group 1) and 14 non-inducible patients (31%) underwent only LVR (Group 2). Twenty-eight patients in Group 1 (90%) and 11 patients in Group 2 (79%) were discharged alive. All 28 patients in Group 1 and 9 of 11 patients (82%) in Group 2 received an ICD including 2 additional implantations for primary prevention 4 and 11 months after discharge. During 32±18 months follow up 4 patients died (1 cancer and 1 heart failure in each group). In Group 1, 11 patients (39%) experienced VT during follow-up, as compared to only 1 patient (9%) in Group 2. The 2 patients without ICD did not experience syncope or palpitations and were considered free from VT. The negative predictive value of EP testing prior to LVR on the primary occurrence of VT after LVR was 0.91.Conclusions: Electrophysiological testing prior to LVR can identify patients at low risk for occurrence of VT after surgery. Concomitant EEC did not prevent VT occurrence in 39% of patients inducible for scar related VT prior to surgery and EEC.
PO3-161
A RANDOMIZED TRIAL COMPARING ENCIRCLING ENDOCARDIAL VERSUS ENDOCARDIAL-EPICARDIAL CRYOABLATION TO PREVENT VENTRICULAR TACHYCARDIA AFTER LEFT VENTRICULAR RECONSTRUCTIONCarine F.B. van Huls van Taxis, MD, Patrick Klein, MD, Adrianus P. Wijnmaalen, MD, Sebastiaan R. Piers, MD, Jerry Braun, MD, Michel I. Versteegh, MD, Harriette F. Verwey, MD, PhD, Martin J. Schalij, MD, PhD, Robert Klautz, MD, PhD and Katja Zeppenfeld, MD, PhD. Leiden University Medical Center, Leiden, NetherlandsIntroduction: Encircling cryoablation of the LV aneurysm scar borderzone during LV reconstruction (LVR) by endoventricular circular patch plasty can be an effective treatment for ventricular tachycardia (VT). After encircling endocardial cryoablation

S283Poster Session III
PO3-164
SLEEP-DISORDERED BREATHING IMPAIRS VENTRICULAR REPORALIZATION AND AUTONOMIC NERVOUS SYSTEM ASSOCIATED WITH LIFE-THREATENING ARRHYTHMIAS IN PATIENTS WITH CHRONIC HEART FAILUREShinya Yamada, MD, Hitoshi Suzuki, MD, Masayuki Satou, MD, Masashi Kamioka, MD, Satoshi Suzuki, MD, Yoshiyuki Kamiyama, MD, Akiomi Yoshihisa, MD, Shu-ichi Saito, MD and Yasuchika Takeishi, MD. Department of Cardiology and Hematology Fukushima Medical University, Fukushima, JapanIntroduction: It has been shown that sleep-disordered breathing (SDB) is associated with adverse prognosis in patients with chronic heart failure (CHF). However, little is known about the relationship between SDB and life-threatening arrhythmias. Thus, we investigated this issue in patients with CHF.Methods: The study subjects consisted of 50 CHF patients (33 males, mean age 59 years, ischemic etiology 42%, mean left ventricular ejection fraction 42%). These patients underwent 24-hour Holter ECG and polysomnography. T-wave alternans (TWA) was calculated by the modified moving average method, and the circadian variation in positive TWA (>65 μV) was determined during the 6-hour intervals (0-6, 6-12, 12-18, and 18-24 hour). In addition, we investigated the power spectral analysis and the time domain analysis of heart rate variability (HRV), and the appearance of ventricular tachycardia (VT, >5beats) by 24-hour Holter ECG. All subjects were divided into two groups based on whether apnea-hypopnea index was above 20 events/hour (Group A, n=24) or not (Group B, n=26) by polysomnography. These parameters were compared between two groups.Results: The ratio of positive TWA in Group A was significantly higher than in Group B in all intervals (0-6 hr: 23% vs. 8%, 6-12 hr: 50% vs. 25%, 12-18 hr: 55% vs. 25% and 18-24 hr: 36% vs. 4%, P<0.05 in each). In the power spectral analysis, low frequency component (LF) and high frequency component (HF) powers of HRV were significantly lower in Group A than in Group B across 24-hour period (LF, 50.9 ± 44.6 msec2 vs. 190.1 ± 138.1 msec2; HF, 39.5 ± 27.2 msec2 vs. 101.2 ± 75.1 msec2, P<0.05 in each). In the time domain analysis, the standard deviation of all R-R intervals was significantly lower in Group A than in Group B (76.5 ± 26.5 msec vs. 100.3 ± 27.9 msec, P<0.05). In addition, the appearance of VT was significantly higher in Group A than in Group B (46% vs. 19%, P<0.05).Conclusions: These results suggest that SDB may impair ventricular repolarization and modulate autonomic nervous system across 24-hour period, resulting in the appearance of life-threatening ventricular arrhythmias in CHF patients.
PO3-165
A VERTICAL STERNAL ELECTRODE PAIR PROVIDES SUPERIOR DIAGNOSTICS FOR HOLTER MONITORSGust H. Bardy, MD, Gene B. Trobaugh, MD, Anne Trobaugh, BSN, Warren M. Smith, MBChB, Martin C. Burke, DO, Ian G. Crozier, MBChB, Iain C. Melton, MBChB, Jennifer Inglis, BS, Jill Anderson, BSN, RN FA, George W. Johnson, BS, Marye J. Gleva, MD and Jeanne E. Poole, MD. Seattle Institute for Cardiac Research, Bellevue, WA, Auckland City Hospital, Auckland, New Zealand, University of Chicago, Chicago, IL, Christchurch Hospital, Christchurch, New Zealand, Washington University, St. Louis, MO, University of Washington Medical Center, Seattle, WAIntroduction: The ECG P-wave is critical in Holter signal analysis for the diagnosis of arrhythmias. Holter P-waves, however, are often small or indistinct. The mid-sternum overlies
lesions were significantly larger than the standard unipolar lesions (4mm RF -: 346 +/- 123 mm3; 8mm RF-: 224 +/-95 mm3 vs. 140 +/-45 mm3; p < 0.01). Using a non-irrigated catheter as epi ground (RF -), endo (RF+) ablation created larger lesions with the 4mm catheter on the epi, but not with the larger 8 mm catheter.Conclusions: Directed bipolar ablation lesions are significantly larger than standard unipolar ablation lesions. This technique may be considered when unipolar epicardial lesions are ineffective.
PO3-163
EPICARDIAL VENTRICULAR TACHYCARDIA ABLATION: SAFETY AND FEASIBILITYShibu Mathew, MD, Yoshiga Yashuiro, MD, Alexander Fürnkranz, MD, Andreas Metzner, MD, Andreas Rillig, MD, Roland Tilz, MD, Eric Wissner, MD, K.-Heinz Kuck, MD and Feifan Ouyang, MD. St.George Hospital Hamburg, Hamburg, GermanyIntroduction: Epicardial VT Ablation is required in different types of Ventricular Tachycardias, but there is still limited information about its safety. In the current study we sought to determine the feasibility and safety of Epicardial VT Ablation.Methods: Between 2003 and 2010 665 VT- Ablations were performed. In 9% (77/665) of these ablations an Epicardial approach (mapping or ablation) was required in 61 patients. Epicardial access was obtained via percutaneous subxiphoid puncture in all patients followed by epicardial mapping and ablation.Results: In 61 patients (46 male; mean age 51 ± 16 years) an Epicardial approach was performed. The underlying heart disease were ischemic cardiomyopathy in 10, dilatative cardiomyopathy in 20, arrhythmogenic right ventricular dysplasia in 13 and miscellaneous types of cardiomyopathies in 18 patients (pts). In 15/61 pts (24,6%) repeat epicardial procedures were required. Out of these in 6 patients an Epicardial procedure was not possible due to adhesions. Pericardial effusion (293 ± 137ml) was presented in 5/77 (6,5%) Epicardial procedures. Two patients underwent surgical treatment due to perforation of the right ventricle and accidental insertion of the pericardial sheeth via the liver. In one patient a none fatal pulmonary embolism occurred. Five patients showed symptoms of sterile pericarditis. No coronary occlusion or stenoses were observed.Conclusions: Epicardial approach was required in 9% of all VT Ablations. Repeat epicardial access increases the risk of adhesions. The incidence of major complications is not negligible

S284 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
(1.59-5.64) if CKD by ACR only and 4.97 (3.18-7.78) if CKD by both markers compared to the reference category.
Conclusions: Risk of mortality is significantly increased when prolonged Qtc is combined with either impaired eGFR or albuminuria with the highest risk in those with Qtc at the 95th percentile in the presence of eGFR<60 mL/min/1.73 m2 and albuminuria.
PO3-167
OUTCOMES ASSOCIATED WITH EARLY REPOLARIZATION (ER) OVER 23 YEARS: THE CORONARY ARTERY RISK DEVELOPMENT IN YOUNG ADULTS (CARDIA) STUDYLeonard Ilkhanoff, MD, Joseph A. Walsh, MD, Hongyan Ning, MD, Kiang Liu, PhD, Samuel S. Gidding, MD, J. Jeffrey. Carr, MD, Elsayed Z. Soliman, MD, MPH and Donald M. Lloyd-Jones, MD. Northwestern Memorial Hospital, Chicago, IL, Northwestern University, Chicago, IL, Thomas Jefferson University, Wilmington, DE, Wake Forest University, Winston-Salem, NC, Wake Forest University, Wake Forest, NCIntroduction: ER noted on the 12-lead ECG has been associated with sudden death and elevated mortality in middle-aged subjects. We sought to determine whether ER is associated with adverse outcomes in young healthy adults.Methods: ECGs obtained at Years 0, 7 and 20 were analyzed for ER, categorized as definite, probable, possible or no ER. Definite (defined as STJ elevation >1mm with a distinct notch or slur on the downstroke of the R wave in any of V3-V6 leads OR STJ elevation >2mm and upward concavity of the ST segment) or probable ER (STJ elevation >1mm with a prominent J point and upward concavity of the ST segment) was used in our analysis. Cox regression was used to explore associations between ER and composite endpoints of (a) Endpoint1: total death, MI, and CHF, and (b) Endpoint2: cardiovascular (CV) death, MI, and CHF, over 23 years of follow-up.Results: Among 5039 participants with baseline ECGs (48.4% white; 54.5% female; mean age: 24.8 ±3.6y), definite/probable ER was present in 1249/5039 (24.8%) at Y0, 538/3653 (14.7%) at Y7, and 165/2491 (6.6%) at Y20. ER was significantly associated with age, SBP, BMI, cholesterol, heart rate, glucose, and smoking (all P<0.01). In unadjusted analyses, ER at Y0 was significantly associated with Endpoint1 (N=313 events; HR 1.45, 95% CI 1.15-1.84), but not Endpoint2 (N=140 events; HR 1.23, 95% CI, 0.86-1.76). Findings were attenuated to nonsignificance in adjusted analyses (Table).Conclusions: ER localized to the chest leads does not appear to confer heightened risk of total or CV death, MI, or CHF in our young biracial cohort over 23 years of follow-up. Differences in risk associated with ER in young and middle-aged adults require further study.
much of the right atrium and yet, for over a 100 years, the sternum has been avoided for the application of ECG sensing electrodes, presumably because of the belief that underlying bone will impede cardiac current flow despite the observation that skin over and adjacent to the sternum conducts cardiac signals.Methods: In a prospective multi-center trial, ECG signal quality and diagnostic yield were compared simultaneously for a standard 3-channel Holter system and for a 3.5” patch electrode designed specifically for vertical application to the mid-sternum (both by Cardiac Science). Fifty patients were enrolled who needed routine 24 hour Holter recordings for diagnosis of syncope, near-syncope, palpitations or rhythm management. All ECGs and rhythms were read by an independent Events committee in batches of 50 to avoid comparative bias. Patients and clinicians also recorded relative ease of use and comfort.Results: Age was 56.3 + 19.2 (18-89) with 26 men (52%) and 24 (48%) women. The indications for Holter was syncope in 14%, near syncope in 10%, palpitations in 26%, arrhythmia control monitoring in 52%, other in 24% (more than one reason was observed in some). The sternal patch provided a good or excellent P wave in 38 patients (76%) compared to 22 patients (44%) with a standard Holter, p< 0.01. Importantly, diagnostic yield, was superior with the sternal patch in 9 of 50 patients (18%) because of better P-wave clarity such that the arrhythmia diagnosis was more specific compared to diagnosis with the standard Holter. The patients reported that the sternal patch was comfortable to wear in 41 cases (82%) compared to the standard Holter which was comfortable to wear in 21 cases (42%), p <0.01). In 50 of 50 cases (100%), the physicians and nurses preferred to use the sternal patch over a standard Holter.Conclusions: Compared to a standard Holter, a small vertically positioned mid-sternal patch recorder improves ECG P-wave signal quality and arrhythmia diagnostic yield while also improving ease of use and providing greater patient comfort.
PO3-166
ASSOCIATION OF QT INTERVAL WITH MORTALITY BY KIDNEY FUNCTION: RESULTS FROM THE NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY (NHANES)Salman Waheed, MD, MPH. Johns Hopkins University, Baltimore, MDIntroduction: Prolonged QT interval predisposes to ventricular arrhythmias and sudden cardiac death. However, the association between QT interval and mortality by the level of pre-existing kidney function has not been investigated.Methods: We followed 7,920 participants from NHANES III for a median of 13.3 years. We divided the sample into 7 categories with cutoffs at the 5th, 20th, 40th, 60th, 80th, and 95th percentiles of the weighted population Bazette heart rate-corrected QT interval (Qtc). We further categorized by kidney function as: no chronic kidney disease (CKD) i.e., albumin: creatinine ratio (ACR) <30 mg/g and estimated glomerular filtration rate (eGFR) >60 mL/min/1.73 m2 (1), CKD by eGFR only (eGFR<60 mL/min/1.73 m2, ACR<30 mg/g) (2), CKD by ACR only (ACR>30 mg/g, eGFR>60 mL/min/1.73 m2) (3) and CKD by both (4). Cox proportional hazards models were used with adjustment for demographic characteristics and traditional cardiovascular risk factors.Results: Overall, eGFR <60 mL/min/1.73 m2, ACR >30 mg/g or Qtc >80th percentile were independently associated with mortality. In those with CKD, the association of Qtc with mortality was stronger compared to those without CKD. For Qtc at the 95th percentile (>476 msec), the relative hazard was 1.85 (1.24-2.76) if no CKD, 2.56 (1.53-4.27) if CKD by eGFR only, 3.0

S285Poster Session III
PO3-170
VENTRICULAR ARRHYTHMIA RISK IN PATIENTS WITH LEFT VENTRICULAR HYPERTROPHY: MORE THAN JUST WALL THICKNESS MEASUREMENTBarbara Dijkman, MD, PhD, MJ Cramer (1), MD, PhD, H. Verkooijen (2), MD, PhD and B. Velthuis (3), MD, PhD. Department of Cardiology University Hospital Utrecht (1), Utrecht, Netherlands, Department of Epidemiology University Hospital Utrecht (2), Utrecht, Netherlands, Department of Radiology University Hospital Utrecht (3), Utrecht, NetherlandsIntroduction: Septal hypertrophy (HT) can be both a phenotype and a phenocopy of hypertrophic cardiomyopathy (HCM). Ventricular arrhythmia (VArrh) can occur in the course of both HCM and other types of cardiomyopathy (CM) involving hypertrophic morphology. Patients (pts) with HT often require decisions concerning arrhythmia risk assessment, particularly if other clinical parameters associated with arrhythmia risk are present.Methods: Association between occurrence of VArrh and presence of LV and RV abnormalities detected with cardiac magnetic resonance (CMR) was investigated in pts with HT (septum ≥ 12 mm in male, ≥11 mm in female pts) undergoing CMR as a part of CM work-up.Results: Clinical profile of 200 pts (49±14 years old) included abnormal ECG in 91% and positive family history (CM, sudden death, gene mutation) in 30% pts. CMR parameters were: mean septum thickness 15 ±4 mm (range 11-35); mean volumes LVEDV 197 ±60 ml, RVEDV 187 ±53 ml; LVEF 54 ±12 %, RVEF 49 ±9 %. In 40% pts LV volumes were > 1 SD above normal. HCM was diagnosed in 26% pts based on combined image, genetics and clinical criteria. VF occurred in 8 % of HT pts (in 10% of HCM pts and in 7% of HT-not HCM pts), sustained VT in 13% of HT pts (in 0% of HCM pts and in 18% of HT-not HCM pts), non-sustained VT in 17% of HT pts, prior to CMR. In multivariate logistic regression analysis VArrh occurrence was significantly (<0.05) associated with LV dyssynchrony, LV midcavitary flow acceleration, RV segmental wall motion abnormality (WMA: hypo-, akinesia), RV regional disparity of systolic contraction duration, and enhanced tissue contrast present in ≥2 different LV regions.Conclusions: In these pts with HT 26% have a HCM diagnosis, 40% have a CM picture including LV hypertrophy, LV enlargement or RV changes. Sustained VArrh occurred in 21 % of referred HT pts, also in those without HCM. VArrh occurrence was strongest associated with LV systolic dyssynchrony, LV midcavitary flow acceleration, extent of enhanced LV tissue contrast, RV segmental WMA and RV regional disparity of systolic contraction duration. CMR can be of value, besides confirming hypertrophy, in assessing VArrh risk both in HCM and other CM involving hypertrophic morphology.
PO3-171
RIGHT VENTRICULAR INFLAMMATION BY CARDIAC PET AS A PREDICTOR OF MORTALITY AND VENTRICULAR ARRHYTHMIA IN PATIENTS WITH SUSPECTED CARDIAC SARCOIDOSISPedram Kazemian, MD, FRCP, William G. Stevenson, MD, Usha Tedrow, MD, Masanao Naya, MD, Michael Osborne, MD, Chun Kim, MD, Sharmila Dorbala, MD, MPH, Angela Koh, MBBS, Michifumi Tokuda, MD, Marcelo F. Di Carli, MD and Ron Blankstein, MD. Brigham and Women’s Hospital, Boston, MAIntroduction: Cardiac sarcoidosis (CS) is associated with significant risk of death and ventricular arrhythmias. VT with right ventricular (RV) involvement can mimic arrhythmogenic cardiomyopathies. PET can detect active inflammation. We
PO3-168
ELECTROCARDIOGRAPHIC FEATURES IN LONG QT SYNDROME PATIENTS WITH A KCNJ5 (KIR3.4−G387R) MUTATIONFan Wang, MD, Jinqiu Liu, MD, Li Hong, MD, Claus Graff, MD, Yanzong Yang, MD, Søren-Peter Olesen, MD, PhD and Jørgen Kim. Kanters, MD. Laboratory of Experimental Cardiology, The Danish National Research Foundation Centre for Cardiac Arrhythmia, Department of Biomedical Sciences, University of Copenhagen, Copenhagen N, Denmark, Department of Cardiology, The First Affiliated Hospital of Dalian Medical University, Dalian, China, Medical Informatics Group (MI), Department of Health Science and Technology, Aalborg University, Aalborg, DenmarkIntroduction: A G387R mutation in the gene KCNJ5, encoding Kir3.4, has been identified in hereditary long QT syndrome (LQTS). Electrocardiographic (ECG) features of the KCNJ5 mutation have not been described. The aim of this study is to evaluate the ECG characteristics of KCNJ5 mutation carriers.Methods: ECG and 24-hour Holter recordings were performed on 23 members (9 mutation carriers) of a KCNJ5 mutation family. One carrier with pacemaker was excluded. PR interval, QRS interval, QT interval, corrected QT interval (QTc), and T wave morphology was calculated from the ECGs. T wave morphology was analyzed by using the morphology combination score (MCS), based on summing three morphology descriptors (MCS=1×asymmetry+1.9×notch+1.6×flatness). 24-hour mean RR interval and standard deviation of RR interval (SDNN) was analyzed from the Holters.Results: Results are shown in table1.Comparison of ECG features between the mutation carriers and non-carriers using the Cox regressionVariable Unit Carrier (n=8) Non-carrier
(n=14)Age year 46 34Gender male, % 3 (37.5) 6 (42.8)PR interval msec 166 ± 18 † 147 ± 16Mean RR interval msec 842 ± 91 † 849 ± 89SDNN msec 122 ± 18 † 152 ± 40QT interval msec 422 ± 37 413 ±30QTcF msec 439 ± 25 422 ± 17MCS 1 0.94 ± 0.23 0.85 ± 0.10
Values are mean ± SD. QTcF: Fridericia-corrected QT duration. ‘Covariate adjustment for age and gender: p < 0.05 vs. non-carriers.Conclusions: The KCNJ5 mutation carriers display prolonged PR intervals and reduced heart rate variability comparing with the non-carriers. After adjustment for age and gender, PR interval and heart rate variability still remain a strong association with the mutation.

S286 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
147 procedures for analysis. All patients had a 12-lead ECG performed pre- and post-ablation and were monitored with continuous telemetry for a minimum of 24 hours during and after NSRT. Chart review of clinic notes, hospitalizations, and outside records was performed to identify cases of late CHB.Results: The overall incidence of CHB requiring permanent pacemaker implantation was 17.7% (26/147 ablations). The incidence of late CHB after implant was 8.8% (13/147 ablations). Among these 13 subjects, heart block occurred from 24 hours to 7 years post-NSRT. Six of the patients experienced CHB after hospital discharge. There is no significant association in our cohort between late CHB and volume of alcohol used, number of septal arteries injected, peak troponin, peak CK-MB, or development of RBBB post-NSRT. There is, however, a higher incidence of late CHB in patients who underwent repeat NSRT (5/22, 22.7%) compared to those who required only a single procedure (8/125, 5.9%) (OR 4.3 (95% CI: 1.3-14.7)).Conclusions: The overall incidence of CHB among our cohort of HCM patients who had undergone NSRT is similar to that which has previously been published. However, the incidence of late complete heart block is substantial, suggesting that careful post-procedural monitoring is indicated.
PO3-175
PERMANENT JUNCTIONAL RECIPROCATING TACHYCARDIA IN CHILDREN: A MULTI CENTER REVIEWKristopher T. Kang, MD, James E. Potts, PhD, Andrew E. Radbill, MD, Petr Kubuš, MD, Michal J. Kantoch, MD, FRCP, Anne Fournier, MD, Jean-Marc Côté, MD, Thomas Paul, MD, Charles C. Anderson, MD, Bryan Cannon, MD, Andrew D. Blaufox, MD, Nicholas H. Von Bergen, MD and Shubhayan Sanatani, MD, FHRS. British Columbia Children’s Hospital, Vancouver, BC, Canada, Vanderbilt University Medical Center, Nashville, TN, Kardiocentrum and Cardiovascular Research Centre, University Hospital Motol, Prague, Czech Republic, Stollery Children’s Hospital, Edmonton, AB, Canada, CHU Mère-Enfant Sainte-Justine, University of Montreal, Montreal, QC, Canada, Centre Mère-Enfant, CHUQ, Quebec, QC, Canada, University Children’s Hospital, Georg-August University, Göttingen, Germany, Providence Sacred Heart Children’s Hospital, Spokane, WA, Mayo Clinic, Rochester, MN, Steven and Alexandra Cohen Children’s Medical Center of New York, Lake Success, NY, University of Iowa Children’s Hospital, Iowa City, IAIntroduction: Permanent junctional reciprocating tachycardia (PJRT) is a rare form of supraventricular tachycardia that occurs predominantly in infants and children. Incessant PJRT may lead to tachycardia induced cardiomyopathy (TIC). The objective of this study was to evaluate the clinical course of PJRT including TIC incidence and current treatment approaches.Methods: We conducted a retrospective review of patients at 11 pediatric centers with PJRT diagnosis at age 0 - 18 years and at least one follow up visit from January 2000 - December 2011. PJRT was defined using published criteria. TIC was defined as left ventricular shortening fraction <28% or ejection fraction <40%. Data are presented as median (range).Results: We identified 110 patients (54M/56F). Age at diagnosis was 0.35 years (1 day - 17.1 years). Length of follow up was 3.7 years (5 days - 20.1 years). PJRT was observed for >50% of monitored time in 67 patients. Heart rate in PJRT was 200 (100 - 300). TIC was present in 20 patients (18%) at presentation. Medical therapy was used for initial management in 76 patients. Digoxin alone or in combination with other medications was the most common first line therapy in 41 cases. Class I and III antiarrhythmic agents were used in 31 and 24 cases. Complete or partial control of PJRT was achieved with first line therapy in
hypothesized that RV inflammation on PET may identify high-risk patients (pts) with documented or suspected CS.Methods: Records of 125 consecutive pts with documented or suspected CS who had cardiac PET were reviewed. The 76 with perfusion or FDG (18F-flurodeoxyglucose) abnormalities on initial review were re-evaluated by two readers who were blinded to the clinical data and independently reviewed PET images for focal RV FDG uptake.Results: Of the 76 pts (mean age 53±10 years, females 39%, mean LVEF 44.9±15.0), 58 had implanted cardiac devices (51 ICD and 7 PPM). PET showed LV perfusion defects alone in 17 (22%) pts, focal abnormal FDG uptake in 21 (28%) pts, and both abnormalities in 38 (50%) pts. Focal RV FDG uptake was found in 12 pts (16%). Over an average follow-up period of 457 days, death or sustained VT occurred in 9 (75%) pts with RV uptake versus 19 (30%) pts without RV uptake. RV FDG uptake was associated with significantly higher risk of death or VT (HR 2.83 (1.28-6.29), p=0.01) (Fig. 1). On univariate analysis, age, LVEF, and pattern of perfusion/metabolism abnormality were not predictive of adverse events (p>0.10).Conclusions: RV FDG uptake is associated with increased risk in pts with documented or suspected CS. Whether RV abnormality indicates more diffuse CS and/or greater propensity to arrhythmia warrants further studies.
PO3-173
INCIDENCE OF LATE COMPLETE HEART BLOCK AFTER NON-SURGICAL SEPTAL REDUCTION THERAPY IN HYPERTROPHIC CARDIOMYOPATHYMatthew M. Zipse, MD, Duy T. Nguyen, MD, Ryan G. Aleong, MD, Wendy Tzou, MD, Robert Quaife, MD, Colleen Campbell, PA, Ernesto E. Salcedo, MD, Paul D. Varosy, MD, William H. Sauer, MD and Joseph L. Schuller, MD. University of Colorado, Aurora, CO, VA Eastern Colorado Health Care System, Denver, COIntroduction: Non-surgical septal reduction therapy (NSRT) by alcohol injection into a septal coronary artery is a less invasive alternative to surgical myectomy in patients with left ventricular outflow obstruction due to hypertrophic cardiomyopathy (HCM). Complete heart block (CHB) requiring permanent pacemaker implantation is a common complication of the procedure, with a reported incidence of 9-22%. While often apparent immediately, there are published case reports of late CHB developing two to eight days post-NSRT. Nonetheless, the incidence of late (more than 24 hours) CHB following NSRT has not been previously described.Methods: 159 patients with HCM who underwent NSRT at the University of Colorado from January 2002 to October 2010 were identified from our HCM database. Ventricular-pacing was present in 12 cases which were excluded, leaving

S287Poster Session III
PO3-177
USE OF ULTRA-LOW DOSE FLAT PLATE FLUOROSCOPY IN PEDIATRIC PATIENTS UNDERGOING ABLATION FOR SUPRAVENTRICULAR TACHYCARDIADavid S. Spar, MD, Jeffrey B. Anderson, MD, MPH, Lisa Lemen, PhD, Richard J. Czosek, MD and Timothy K. Knilans, MD. The Heart Institute, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, University of Cincinnati College of Medicine, Department of Radiology, Cincinnati, OHIntroduction: Standard imaging for ablation of supraventricular tachycardia is fluoroscopy. Three-dimensional electroanatomical mapping (3D) has been proposed as a method to reduce radiation exposure. This study compares a technique for the reduction of radiation, ultra-low dose fluoroscopy (ULD) with standard low dose fluoroscopy (SLD) and 3D.Methods: All patients undergoing initial ablation for AVRT or AVNRT from 2009 to 2011 were reviewed. The patients were divided into three groups: 1) SLD, 2) 3D (CARTO or NavX) with adjunctive SLD or 3) ULD. ULD utilized the same equipment as SLD (Philips Allura FD 10/10) but made customized changes to the manufacturer’s lowest settings by decreasing the requested dose to the detector from 310 to 155nGy/s and limiting the maximum entrance dose from 2.5 to 1R/min. Primary outcomes were fluoroscopy time and dose area product exposure.Results: 183 patients were included. The median age was 15.0 years (0.1-26.2); 59% had AVRT, 36% had AVNRT and 5% had both AVRT and AVNRT. ULD decreased radiation dose compared to SLD with no difference in fluoroscopy time. 3D decreased fluoroscopy time with a trend toward decreased radiation dose compared to SLD. ULD and 3D had comparable radiation dose, even though ULD had significantly longer fluoroscopy time. There were no differences in patient demographics, acute success, complications or mechanism of tachycardia between groups.
Conclusions: ULD with decreased requested dose to the detector and limited entrance dose during ablation of AVRT and AVNRT significantly reduced radiation exposure compared with SLD and had similar radiation exposure compared with 3D with adjunctive SLD.
PO3-178
FRAGMENTED QRS COMPLEXES ARE ASSOCIATED WITH VENTRICULAR TACHYARRHYTHMIA IN ADULT PATIENTS WITH EBSTEIN’S ANOMALYSeungmin Chung, MD, Seung Jung Park, MD, PhD, Young Keun On, MD, PhD, June Soo Kim, MD, PhD, I-Seok Kang, MD, PhD, Heung Jae Lee, MD, PhD and June Huh, MD, PhD. Samsung Medical Center, Seoul, Korea, Republic ofIntroduction: Fragmented QRS (fQRS) on 12-lead electrocardiogram (ECG) is a predictor of arrhythmic events in patients with Brugada syndrome, ischemic and nonischemic cardiomyopathy. We evaluated whether fQRS is associated with increased ventricular arrhythmic event in adult patients with Ebstein’s anomaly.
37 cases. Sixteen patients achieved resolution of PJRT without ablation. In total 72 patients received 87 ablation procedures. Ablation was used for initial management in 16 patients, including radiofrequency ablation in 12 and cryoablation in 4. Ablation indication was elective in 31 and treatment-refractory PJRT in 23. Complex mapping was used in 10. Acute success with ablation was achieved in 72 of 77 reported cases (94%) with 11 recurrent cases. There were complications in 5 cases including 2 with transient complete atrioventricular block. All patients were alive at last follow up with 104 in sinus rhythm, 4 in PJRT, 1 in junctional rhythm and 1 with permanent pacing, including 23 with ongoing medical therapy.Conclusions: Medical therapy was often used for initial management of PJRT. Resolution was observed in a minority of patients who did not receive ablation. Catheter ablation was effective for treating patients refractory to medical management.
PO3-176
DO PEDIATRIC ELECTROPHYSIOLOGISTS READ PREPARTICIPATION SCREENING ECGS MORE ACCURATELY THAN GENERAL PEDIATRIC CARDIOLOGISTS?Anna L. Harbison, MD, Allison J. Hill, MD, Kara S. Motonaga, MD, Christina Y. Miyake, MD and Anne M. Dubin, MD. Lucile Packard Children’s Hospital, Stanford, CAIntroduction: Significant controversy exists in the pediatric cardiology community surrounding the use of pre-participation screening ECGs (sECG). A study published earlier this year suggested that sECG are difficult to accurately interpret, even by pediatric cardiologists. We sought to evaluate whether pediatric electrophysiologists (EPs) intepret sECG more accurately.Methods: 18 ECGs representing either conditions causing pediatric sudden cardiac death or normal hearts were interpreted by 69 physician members of the Pediatric and Adult Congenital Electrophysiology Society (PACES). Recommendations for further testing and sports participation were elicited. Gold-standard diagnoses and recommendations were determined by 2 EPs (100% concordance) and confirmed by patient’s actual diagnosis. These findings were then compared to previous published data from our group studying the Western Society of Pediatric Cardiology.Results: 69 EPs interpreted a total of 918 ECGs. The average number of correct ECG interpretations per respondent was 12.9 +/- 3.0 (72%). Based on actual ECG diagnosis, sports participation was accurately permitted in 81% of cases and accurately restricted in 80% of cases. Respondents gave correct sports guidance most commonly in cases of long QT syndrome and carditis (both 94%) and least commonly in cases of Hypertrophic Cardiomyopathy (86%) and Wolff-Parkinson-White syndrome (66%).Conclusions: sECG are difficult to interpret even for pediatric EPs. Incorrect interpretations can lead to high rates of inappropriate sports guidance and overuse of ancillary testing.ECG interpretation by pediatric cardiologists and electrophysiologists.
Total Number Sensitivity Specificity False positive
False negative
PACES 69 63% 85% 15% 37%
Western Society of Ped Card 53 68% 70% 30% 32%
p value 0.7 0.03 0.03 0.7

S288 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
PO3-180
ASSESSMENT OF VARIANTS IDENTIFIED IN ARVC-ASSOCIATED GENES IN SAMPLES FROM THE 1000 GENOME PROJECT AND THE EXOME CHIP DESIGN PROJECTJamie D. Kapplinger, BA, Benjamin A. Salisbury, PhD, David J. Tester, BS, Thomas E. Callis, PhD, Guido D. Pollevick, PhD, J. Peter van Tintelen, MD, PhD, Hugh Calkins, MD, Daniel P. Judge, MD, Arthur A.M. Wilde, MD, PhD and Michael J. Ackerman, MD, PhD. Mayo Clinic, Rochester, MN, Transgenomic, New Haven, CT, Department of Medical Genetics, Groningen, Netherlands, Department of Medicine/Cardiology, Baltimore, MD, Department of Cardiology, Amsterdam, NetherlandsIntroduction: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare genetic myocyte disease characterized by myocyte loss and fibro-fatty tissue replacement of the ventricles. Recent studies have shown an unusually high amount of non-synonymous single nucleotide variants (nsSNVs) in the 5 major ARVC-susceptibility genes, leading to a low signal-to-noise ratio, and complicating ARVC genetic test interpretation. The examination of large numbers of control genomes available in the public domain offers an opportunity to re-quantify and potentially reduce this problem.Methods: nsNSVs in the 1000 Genome and Exome Chip Design projects were mined for the 5 major ARVC-associated genes: DSC2, DSG2, PKP2, DSP, and TMEM43. These nsSNV were compared with the nsSNVs identified in our previously published 427 ostensibly healthy controls, 195 ARVC cases, as well as the nsSNVs identified in the ARVC Genetic Variants Database.Results: Of the 76 “false positive” nsSNVs previously identified in the 427 controls, 22 were identified in the public reference cohorts, dropping the background rate from 16% to 12%. Similarly, the yield among the 195 ARVC cases for missense mutations dropped from 21% to 15%. While the yield among the Exome Chip samples could not be ascertained, the yield of unique nsSNVs within the 1000 Genome samples was only 3.6%, dramatically lower than observed in our 427 controls sequenced using Sanger sequencing assays. Among the nsSNVs listed in the ARVC Database, 116 of 209 (56%) of those labeled “unknown/unclassified” were observed in one of the control datasets; remarkably, 12 of the 116 (10%) variants labeled “pathogenic” were also observed.Conclusions: The accumulation of vast control datasets shows some promise in reducing the problem of the “background noise” in the ARVC genetic test. Remarkably, a large fraction of unique nsSNVs found in our controls appear to be as “family specific” as the ARVC disease-associated mutations based on consulting the over 12,000 publicly available exomes. However, these findings should be interpreted cautiously given the nearly 5-fold lower rate of novel nsSNVs reported in the 1000 Genomes data, which may reflect a lack of sensitivity for detecting rare variants in these genome and exome sequencing projects.
PO3-181
WEIGHT-LOSS SUPPLEMENTS WITH LETHAL CARDIAC SIDE EFFECTS: A PHYSICIAN SURVEYAlireza Nazeri, MD, Shamaila A. Gill, MD, Abdi Rasekh, MD, Vei-Vei Lee, MS, MacArthur A. Elayda, MD, PhD, Muhammad Saeed, MD, Christopher M. Frank, MD, Ali Massumi, MD and Mehdi Razavi, MD. Texas Heart Institute, Electrophysiology, Houston, TXIntroduction: The use of nonprescription weight-loss supplements (WLS) is growing, even though many WLS
Methods: Fragmented QRS was defined by 1) the presence of >1 notching on the R or S wave in the narrow QRS (2 notches on the R or S wave in wide QRS complexes (≥120ms) in ≥ 2 contiguous leads. Clinical ventricular tachyarrhythmia events were studied in 51 patients with Ebstein’s anomaly (35.3% male, age 38.8 ± 13.3 years, median follow-up 49 months).Results: Fragmented QRS was present in 35 (68.6%) patients (fQRS group) and absent in 16 (31.4%) patients (non-fQRS group). No significant differences were found in baseline clinical characteristics between 2 groups except for New York Heart Association (NYHA) functional class (NYHA III 65.7% vs. 25.0%, p=0.023) and cardiothoracic ratio (0.58 ± 0.095 vs. 0.49 ± 0.044, p < 0.001). Ventricular arrhythmia (ventricular tachycardia or ventricular fibrillation) events occurred more frequently in fQRS group than in non-fQRS group (22.9% vs. 0.0%, p=0.045).Conclusions: Fragmented QRS on 12-lead ECG is associated with ventricular tachyarrhythmia in adult patients with Ebstein’s anomaly
PO3-179
RYR2-MEDIATED CATECHOLAMINERGIC POLYMORPHIC VENTRICULAR TACHYCARDIA (CPVT) IN PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHYCherisse A. Kellen, BA, J. Martijn Bos, MD, PhD, Melissa L. Will, BS, Argelia Medeiros-Domingo, MD, PhD, Bernard J. Gersh, MD, PhD, Steve R. Ommen, MD and Michael J. Ackerman, MD, PhD. Mayo Clinic, Rochester, MNIntroduction: Approximately 30% of patients with hypertrophic cardiomyopathy (HCM) exhibit potentially hazardous ventricular arrhythmias that can lead to sudden cardiac death (SCD). Mutations in the RYR2-encoded cardiac ryanodine receptor cause the potentially lethal arrhythmia syndrome type 1 catecholaminergic polymorphic ventricular tachycardia (CPVT1). Accordingly, we hypothesized that patients with HCM and a strong history of ventricular arrhythmias may also have concomitant CPVT1.Methods: Eighty unrelated patients with HCM (56 male, age at diagnosis 36 ± 17 years, mean maximum left ventricular wall thickness (MLVWT) 23.6 ± 6 mm) underwent targeted mutational analysis of 64 of RYR2�s 105 translated exons using PCR, DHPLC, and direct DNA sequencing. All patients had a history of ventricular arrhythmias and received an implantable cardioverter defibrillator as secondary prevention. All patients were genotyped previously for the 9 HCM-associated myofilament genes and 39 patients (49%) were sarcomere mutation positive.Results: Two CPVT1-associated RYR2 mutations (1 novel) were identified in 2/80 patients (2.5%). Of the two RYR2 mutations, one novel mutation (V919M) was found in a woman with MYBPC3-HCM (W1213X) diagnosed at age 27 with a MLVWT of 16 mm. EP studies showed inducible ventricular tachycardias (VT) and fibrillation. She had a strong family history of HCM and SCD. The second CPVT1-associated mutation (RyR2-E4431K) was found in a woman with MYH7-HCM (G741W) diagnosed at age 10 with a MLVWT of 24 mm and a history of polymorphic VT on EP study. She has a strong family history of both HCM and SCD. Both RYR2 missense mutations involved highly conserved residues and were absent in 1000 reference alleles.Conclusions: Ventricular arrhythmias are a common feature of HCM and are generally viewed as secondary to the cardiomyopathic disease process. In our enriched cohort of HCM patients with documented ventricular arrhythmias, 2.5% had concomitant CPVT1-associated RYR2 mutations and a clinical phenotype of HCM plus polymorphic VT. These results suggest that such HCM patients with polymorphic ventricular arrhythmias may have both HCM and CPVT.

S289Poster Session III
class III)despite maximal pharmacologic therapy, and the LBBB accounted for 95% of the THB/day. The LV was dilated (LVDd=64 mm), and the LV function deteriorated (LVEF=30%). The septal-to-posterior wall motion delay (SPWMD) was 270 msec. Shortly after receiving cardiac resynchronization therapy (CRT), the QRS width shortened to 130 msec and her status improved to an NYHA class I. The LVDd and EF improved to 55 mm and 54%, respectively. The ventricular dyssynchrony also disappeared (SPWMD=72 msec). The patient has done well with no HF worsening during a 2-year follow-up.Conclusions: Even in patients with no structural heart disease, transient LBBB can cause a marked ventricular dyssynchrony and LV dysfunction, and may be a sign of upcoming and progressive overt HF. Careful examination, including Holter ECGs and exercise testing, should be performed for the diagnosis. Much attention should be paid in such patients because CRT is an effective treatment.
PO3-183
GASTRIC BYPASS SURGERY IS ASSOCIATED WITH SEVERE CARDIOINHIBITORY VASOVAGAL SYNCOPE REQUIRING RATE DROP PACINGCharles H. Koo, MD and Carol Brown, CVT. Monmouth Cardiology Associates, Neptune, NJIntroduction: About 200,000 bariatric surgeries are performed yearly. There are restrictive and malabsorptive methods and the goal of malabsorptive surgery is to alter digestion and absorption of nutrients by rerouting the small bowel. One of the most popular malabsorptive surgical techniques is the Roux En Y bypass. Surgical complications include the need for vitamin supplements, orthostatic changes, dumping syndrome, and hepatobiliary dysfunction. This is the first report of malignant vasovagal syncope associated with gastric bypass surgery.Methods: We describe 4 consecutive, previously healthy, Roux En Y gastric bypass patients who developed post operative malignant vasovagal syncope.Results: All 3 patients who needed a pacer had rapid weight loss. The one patient who responded to medical therapy was a surgical non-responder and regained all of the lost weight.
Patient Current age
Year of Surgery
Time to syncope
Post op Wt Loss
Presentation EF TTT result Medical Regimen Pacer Setting Device
follow-up
1 43 2003 4 years ++++
Recurrent syncope soft tissue trauma near drowning
59% cardioinhibitorymidodrine paroxetine florinef
Yes
rate and drop 80bpm for 3” >254 episodes
>254 episodes; no syncope
2 59 2008 6 months ++++
Recurrent syncope Blunt force soft tissue trauma
62% Primarily cardioinhibitory
midodrine paroxetine florinef
Yes
drop>25 100bpm for 4” >254 episodes
>254 episodes; no syncope
3 50 2006 8 months ++++Recurrent syncope, soft tissue trauma
60% Normal
fluid and sodium liberalization intolerant of medications
Yes
drop>25 95 bpm for 4” >254 episodes
>254 episodes; no syncope
4 48 2005 4.5 years + Recurrent syncope MVA 69% Mixed midodrine No
Responded to Medical Therapy
no syncope regained lost weight
Conclusions: This is the first description of malignant vasovagal syncope as a post-op complication of gastric bypass surgery. All patients had normal volume and sodium status and there was no evidence for orthostasis. There may be post surgical changes in vagal tone as a result of the rerouting the small bowel or an alteration in the feedback mechanism with the vagal center. It is not known if alterations in endogenous hormones such as ghrelin can affect vagal tone. Unresponsiveness to medical therapy may be due in part to the inability to digest and absorb the medication. The need for a pacer is associated with rapid weight loss.
have hazardous ingredients. Furthermore, different WLS manufacturers use different names to refer to the same potentially dangerous ingredient. We aimed to assess physicians’ awareness of and approach to these potentially hazardous supplements in their daily practice.Methods: A survey was mailed to physicians practicing in Houston, Texas. The survey included questions about 12 ingredients--essentially 6 different substances used in WLS--that are each associated with at least 1 report of life-threatening adverse cardiac effects or death when taken at high doses or in combination with other such ingredients.Results: From August 2009 to May 2010, 1,040 surveys were mailed. Of these, 117 (11%) were returned: 60 (51%) by family physicians, 28 (24%) by cardiologists and 29 (25%) by internal medicine or other subspecialty physicians. The majority of respondents were practicing in outpatient settings. Years in practice were as follows: 1-5 years (19%), 6-10 years (9%), and >10 years (72%). Of the 12 listed ingredients with life-threatening adverse cardiac effects, respondents could correctly identify 0-3 (60%), 4-6 (32%), 7-11 (5%), or all 12 (3%). Fifty-two percent (61/117) of respondents stated that they regularly ask their patients whether they take nonprescription WLS. Seventy percent (78/112) advised patients not to take any of the substances listed in the survey. Most of the responders (112/116; 97%) correctly indicated that these supplements are not regulated by the US Food and Drug Administration (FDA). The different names for the same ingredient were correctly recognized by 68% (52/77) of the respondents.Conclusions: Most physicians who participated in the survey know that WLS are not regulated by the FDA, but nearly half do not regularly ask their patients about WLS consumption. There is a need to improve physicians’ awareness of the hidden dangers of these supplements.
PO3-182
THE APPEARANCE AND DEVELOPMENT OF LEFT BUNDLE BRANCH BLOCK MAY RESULT IN HEART FAILURE WITH VENTRICULAR DYSSYNCHRONY IN PATIENTS WITH NO STRUCTURAL HEART DISEASE: A CASE REPORTMiyako Igarashi, MD, Hiroshi Tada, MD, Yukio Sekigushi, MD, Hiro Ymasaki, MD, Kenji Kuroki, MD, Takeshi Machino, MD, Tomoko Ishizu, MD, Yoshihiro Seo, MD, Keisuke Kuga, MD and Kazutaka Aonuma, MD. University of Tsukuba, Tsukuba, JapanIntroduction: Left bundle branch block (LBBB) often develops in patients with structural heart disease and left ventricular (LV) dysfunction, and its appearance may result in ventricular dyssynchrony and congestive heart failure (HF). However, information on the significance and prognosis of newly-appearing and transient LBBB in patients with no structural heart disease is lacking.Methods: N/AResults: A 63-year-old female patient presented with mild HF corresponding to an NYHA functional class II. A physical examination, chest radiography, multi-detector CT and cardiac magnetic resonance imaging revealed no evidence of structural heart disease. Although the 12-lead ECG also showed normal sinus rhythm with a QRS width of 110 msec, transient and rate-dependent LBBB with a total QRS duration of 170 msec was observed in 58% of the total heart beats (THB)/day by a 24-hour Holter ECG. Echocardiography performed during a normal QRS complex demonstrated a normal LV function with an ejection fraction (LVEF) of 54% and a non-dilated LV with an end-diastolic diameter (LVDd) of 50 mm. However, as soon as the LBBB developed, the LVEF decreased to 35% with the appearance of marked LV dyssynchrony and dilation. Within the following 4-months, the patient’s status deteriorated (NYHA

S290 Heart Rhythm, Vol. 9, No. 5, May Supplement 2012
PO3-185
SEVERE CARDIOMYOPATHY CAUSED BY RIGHT FREE WALL ACCESSORY PATHWAYYasuhiro Sasaki, MD, Satoshi Sizuta, MD, Chihiro Ota, MD, Naoaki Onishi, MD, Mituhiko Yahata, MD, Kentarou Nakai, MD, Koji Goto, MD, Takahiro Doi, MD, Takeru Makiyama, MD, PhD and Takeshi Kimura, MD, PhD. The Department of Cardiovascular Medicine, Kyoto University Hospital, Kyoto, JapanIntroduction: Septal accessory pathways (APs) occasionally cause ventricular dyssynchrony and left ventricular (LV) dysfunction. However, free-wall APs rarely affect LV function.Methods: N/AResults: A 52-year old male was admitted to our hospital due to NYHA class-IV heart failure. He had been diagnosed as dilated cardiomyopathy two years ago, and had received optimal medical therapy including ACE inhibitor, β-blocker, furosemide, spironolactone and digitalis. His ECG showed wide QRS (202ms) with manifest δ wave due to Type-B WPW syndrome. His UCG showed marked LV enlargement and dysfunction (LVDD=80mm, LVEF=10%) with prominent ventricular dyssynchrony. His BNP level was 1392 pg/ml.He underwent radiofrequency catheter ablation (RFCA) for right posterolateral AP. Immediately after successful RFCA, his heart failure symptoms markedly improved. Because of slightly prolonged QRS duration (120ms), suspected ventricular dyssynchrony in Tissue Doppler UCG, and frequent NSVTs on Holter monitoring, he underwent CRT-D implantation 3 days after RFCA, although the device was set at DDDR-60 with long AV delay to preserve intrinsic ventricular conduction and excitation. After 10 months, his heart failure status was NYHA class-I. His UCG showed marked LV reverse remodeling (LVDD=43mm, LVEF=56%), and his BNP level was 26 pg/ml. His ECG also showed marked reverse remodeling (SV1+RV5: 92mm-36mm).Conclusions: This was considered to be a case of severe cardiomyopathy caused by ventricular dyssynchrony due to right free-wall AP, which was cured by elimination of the AP by RFCA.
PO3-186
ATRIAL TACHYCARDIA AFTER AF ABLATION: AN ‘ALTERNATE’ MECHANISMDavid G. Jones, MBBS, Sofian Johar, PhD, MRCP, Jack Wang, MD, Vias Markides, MD, FRCP and Tom Wong, MD, FRCP. Heart Rhythm Centre, Royal Brompton and Harefield NHS Foundation Trust & Imperial College London, Uxbridge, United Kingdom, St Jude Medical, St. Paul, MNIntroduction: We present an unusual atrial tachycardia (AT), after prior ablation of atrial fibrillation (AF), with alternans of
PO3-184
A CASE OF INDUCED VENTRICULAR TACHYCARDIA BY VENTRICULAR PACING ON T WAVE DUE TO UNUSUAL DOUBLE BLANKINGYuuki Takenaka, No Degree, Nobuhiro Nishii, MD, Motoki Kubo, MD, Koji Nakagawa, MD, Masamichi Tanaka, MD, Satoshi Nagase, MD, Hiroshi Morita, MD, Kengo F. Kusano, MD and Hiroshi Ito, MD. Okayama univercity hospital, okayama, JapanIntroduction: Avoidance of ventricular pacing has been reported to reduce development of atrial fibrillation, stroke, or heart failure. Prolongation of AV interval is one of new algorithms to avoid ventricular pacing. However, premature ventricular contraction (PVC) immediately after atrial pacing is likely to be undersensed due to ventricular blanking after atrial pacing. Especially in the long AV interval setting, undersensing of PVC causes ventricular pacing on T wave, which caused induction of life threatening ventricular arrhythmia. We experienced a case of ventricular tachycardia (VT) induced by ventricular pacing due to double blanking.Methods: N/AResults: A 76-year-old female with cardiac sarcoidosis was implanted a dual chamber implantable cardioverter defibrillator (ICD) due to sustained VT. We set AV interval to 300 ms to avoidventricular pacing because intrinsic AV interval was long. Paroxysmal atrial fibrillation (PAF) and two VTs were appeared during hospitalization. Both VTs were successfully terminated by antitachycardia pacing. The initiation of VT was ventricular pacing. Atrial pacing was not usually delivered during PAF. However, blanking after PVC of 450 ms (first blanking) was created which caused undersensing of atrial beat followed atrial pacing. After atrial pacing, blanking of 50 ms (second blanking) was created which caused undersensing ofventricular beat. Then, ventricular pacing was delivered 300 ms after atrial pacing, which was 250 ms after ventricular beat.Conclusions: Although long AV interval setting may be useful to avoid ventricular pacing, it rarely results in induction of life threatening ventricular arrhythmia.

S291Poster Session III
sternal repair and open chest epicardial catheter ablation was performed in order to stabilize the patient’s condition.Results: The patient was brought to the EP laboratory where a sternotomy was performed, revealing a large well-circumscribed area of infarct along the posterior wall; however, retraction of the heart to expose the posterior wall resulted in severe hypotension, presumably due to impaired ventricular filling. Sustained VT was readily induced via overdrive pacing but was poorly tolerated hemodynamically, precluding entrainment mapping. Pace mapping along the apical edges of the scar yielded poor morphologic matches to the patient’s VT.The pericardial space was filled with warmed saline to provide a stable conductance medium, and a Saint Jude Medical Safire TX 8 mm tip ablation catheter was used in conjunction with EnSite Velocity to create a 3D-electroanatomic map (EAM) of the epicardial surface. Pacing mapping was performed along the basal edge of the posterior wall scar with minimal cardiac retraction, utilizing EnSite Velocity to track the ablation catheter position; this allowed localization of the VT breakout site to the basal aspect of the posterior wall scar, and a series of ablation lesions were successfully delivered. The sternum was then repaired and closed. At 6-months post-ablation, the patient remained free of recurrent VT.Conclusions: Open chest epicardial ablation for ischemic VT has been well described, and generally does not require EAM techniques due to the ability to directly visualize the myocardium and target ablation site(s); furthermore, the lack of a stable conductance medium typically precludes EAM with open chest procedures. To our knowledge, this represents the first case wherein EAM was successfully utilized using saline as a conductance medium in an open chest epicardial ablation.
activation and cycle length (CL). High-density mapping (HDM) helped study the mechanism.Methods: N/AResults: A 69y female with drug-resistant persistent AF had PVI, roof line, left atrial (LA) floor defragmentation. AT occurred 6 months later. AT1: CL 280ms, prox>distal CS activation. After transseptal puncture AT1 changed to AT2: CL 370ms, dist>prox CS. HDM (AFocus II/NavX, St Jude Medical) indicated roof-dependent reentry, prior to further transformation to alternans AT3. HDM was performed for each alternating ‘beat’ (total ‘CL’~650ms; fig); the distal-proximal CS beat was defined “Loop A” (cf AT2) and mapped live; that with proximal-distal CS as “Loop B” (cf AT1) & mapped from recorded segment. AT3 was roof-dependent (anterior craniocaudal) with ‘see-saw’ lateral/septal conduction; bipolar voltage & conduction velocity was lower at anteroseptum in loop A vs. loop B(fig); CS predicted PW CL. A septal catheter ectopic later disrupted alternans & AT2 resumed. RF roof ablation terminated AT (16s); roof block confirmed. At case-end no AT was inducible; pt remained AT-free at 18 months.Conclusions: An unusual alternans AT was studied with HDM. At AT3 onset, a shorter coupling interval (CI) at the roof favored lateral conduction to PW and roof (loop A). A longer roof CI at A-B transition allowed anteroseptal recovery, favoring shorter septal conduction (loop B), producing see-saw alternans. Such tachycardias, although rare, may present occasionally given the complex atrial substrate after AF ablation.
PO3-187
OPEN CHEST EPICARDIAL RADIOFREQUENCY CATHETER ABLATION OF ISCHEMIC VENTRICULAR TACHYCARDIA WITH 3D-ELECTROANATOMIC MAPPING UTILIZING ENSITE VELOCITYGabriel E. Soto, MD, PHD, FHRS, William R. Ogle, MD and Joseph G. Gibbons, RN. SoutheastHEALTH, Cape Girardeau, MO, St. Jude Medical, St. Paul, MNIntroduction: A 63-year-old male with multi-vessel CAD and severe mitral regurgitation underwent elective CABG and a mitral valve replacement (MVR). His post-operative course was complicated by recurrent unstable ventricular tachycardia (VT) that was refractory to antiarrhythmic drug therapy; he also suffered multiple sternal fractures from cardiopulmonary resuscitation efforts, resulting in a flail chest. A combined