pneumococcal soft-tissue infections: possible association with connective tissue diseases
TRANSCRIPT

JID 1991;163.(April) Concise Communications 897
11. Falco RC, Fish D. Ticks parasitizing humans in a Lyme disease endemicarea of southern New YorkState. Am J EpidemioI1988;128:1146-52.
12. Piesman J, Spielman A. Human babesiosis on Nantucket Island: prevalence of Babesia microti in ticks. Am J Trop Med Hyg 1980;29:742-6.
13. Steere AC. Lyme disease. N Engl J Med 1989;321:586-96.
14. Barbour AG. Laboratory aspects of Lyme borreliosis. Clin MicrobiolRev 1988;1:399-414.
15. Preac-Mursic V, Weber K, Pfister HW, et al. Survival of Borrelia burgdorferi in antibiotically treated patients with Lyme borreliosis. Infection 1989;17:355-9.
Pneumococcal Soft-Tissue Infections: Possible Association withConnective Tissue Diseases
Mark J. DiNubile, M. Anthony A1bornoz,Russell J. Stumacher, Bonnie L. Van Uitert,Sandra A. Paluzzi, Larry M. Bush,Stephen C. Nelson, and Allen R. Myers
Divisions of Infectious Disease, Departments of Medicine, CooperHospital/University Medical Center, University of Medicine and
Dentistry ofNew Jersey/Robert JiJVod Johnson Medical School atCamden; Graduate Hospital, Presbyterian Medical Center, Hahnemann
University Hospital, Medical College of Pennsylvania, and TempleUniversity Hospital (Division of Rheumatology), Philadelphia; and
Crozier-Chester Medical Center, Chester, Pennsylvania
Streptococcus pneumoniae is not a well-recognized cause of soft-tissue infections. In <4 years,12 cases of pneumococcal soft-tissue infection were identified through discussions with infections disease subspecialists in the Philadelphia area. Principal sites of involvement included skinand fascia, tongue, epiglottis, thyroid, brain, and breast. Pneumococcal bacteremia wasdocumented in six cases (50%); in three of these, pneumococci were also cultured from the involved soft tissues. In the cases in which bacteremia was not demonstrated, pneumococci wereisolated from the infected sites. Six patients had connective tissue diseases, of which five werediagnosed as systemic lupus erythematosus. Four of these patients were receiving corticosteroidswhen their infections developed. Twoadditional patients were HIV-seropositiveintravenous drugusers..S. pneumoniae may be a more important cause of soft-tissue infections than previouslyappreciated, especially in patients with connective tissue diseases.
Streptococcus pneumoniae is a common cause of sepsis,meningitis, sinusitis, otitis media, and pneumonia [1]. Itsetiologic role is less frequently recognized in infections predominantly involving soft tissues, Pneumococci have been incriminated in nearly 10% of adult cases of epiglottitis [2].Less often, pneumococcal cellulitis has been documented inchildren and intravenous drug users [3, 4]. Although rhabdomyolysis has been reported after pneumococcal bacteremia[5], there have been few demonstrations of actual muscle invasion by pneumococci [6]. These organisms have occasionally been isolated from brain [7] and thyroid [8] abscessesand rarely from epidural [9] and splenic [10] abscesses. Inour recent collective experience, pneumococcal soft-tissue infections have occurred with sufficient frequency, especiallyin patients with connective tissue disorders, to merit the attention of clinicians. Here we describe the clinical characteristics of 12 of these cases.
Received 2 August 1990; revised 31 October 1990.Reprints or correspondence: Dr. Mark DiNubile, Department of Medi
cine, Three Cooper Plaza, Camden, NJ 08103.
The Journal of Infectious Diseases 1991;163:897-900© 1991 by The University of Chicago. All rights reserved.0022-1899/91/6304-0041$01.00
Methods
Patients with pneumococcal infections primarily involving soft tissues were identified through formal and later informal discussionsamong infectious disease subspecialists working in the Philadelphiaarea. Cases were accepted for this report if soft-tissue infection wasthe sole or major clinical manifestation and pneumococci were isolated from blood or the involved soft tissue. Pneumococci wereidentified by the routine methods used in the clinical microbiologylaboratories of each hospital.
Results
In <4 years, we collected 12 cases of soft-tissue infectiondue to S. pneumoniae (table 1). Six patients (50%) had demonstrable pneumococcal bacteremia. Pneumococci were also isolated from the relevant soft tissues in three of those withbacteremia. In all patients whose blood cultures were sterile,pneumococci were cultured from the involvedsoft-tissue sites.Gram's stains of pus obtained from the sites of infection typically demonstrated gram-positive diplococci without otherbacteria.
The pneumococcalorigin of these soft-tissue infectionsseemscertain in 11 of the 12 cases. Whether pneumococci were
at The U
niversity of Alberta on O
ctober 22, 2014http://jid.oxfordjournals.org/
Dow
nloaded from
898 Concise Communications
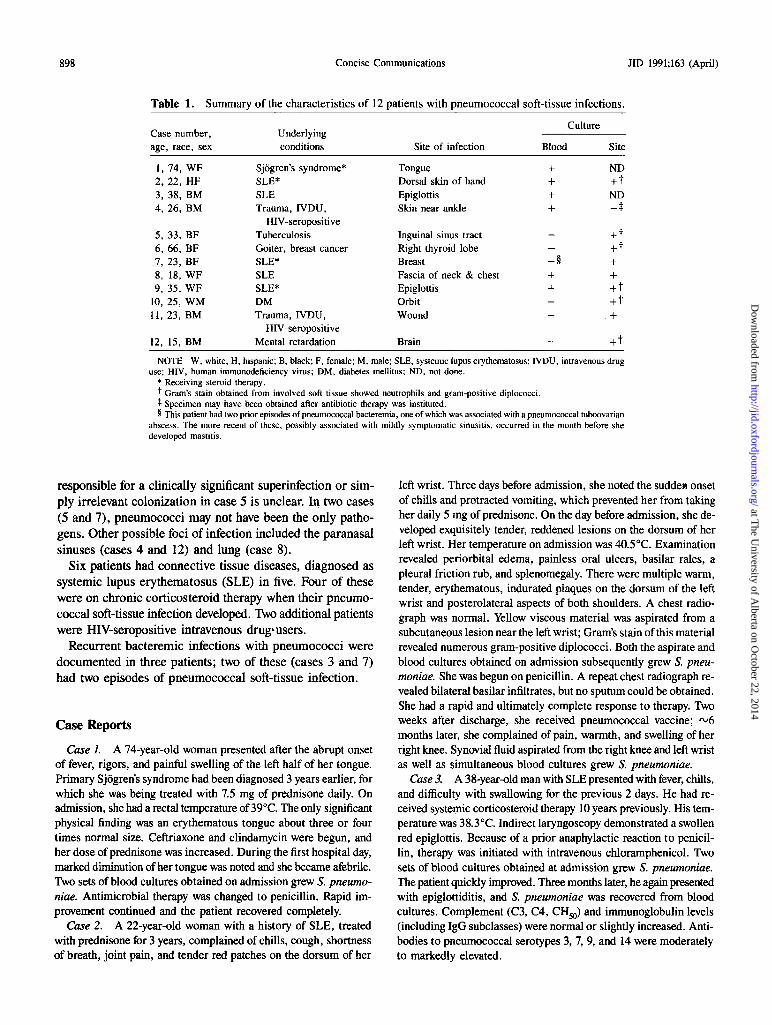
Table 1. Summary of the characteristics of 12 patients with pneumococcal soft-tissue infections.
CultureCase number, Underlyingage, race, sex conditions Site of infection Blood Site
1,74, WF Sjogren's syndrome* Tongue + ND2,22, HF SLE* Dorsal skin of hand + +t3,38, BM SLE Epiglottis + ND4,26, BM Trauma, IVDU, Skin near ankle + -+
HIV-seropositive5,33, BF Tuberculosis Inguinal sinus tract +t6,66, BF Goiter, breast cancer Right thyroid lobe +t7,23, BF SLE* Breast -§ +8, 18, WF SLE Fascia of neck & chest + +9,35, WF SLE* Epiglottis + +t
10,25, WM DM Orbit +t11,23, BM Trauma, IVDU, Wound +
HIV-seropositive12, 15, BM Mental retardation Brain +t
NOTE W, white; H, hispanic; B, black; F, female; M, male; SLE, systemic lupus erythematosus; IVDU, intravenous druguse; HIV, human immunodeficiency virus; DM, diabetes mellitus; ND, not done.
* Receiving steroid therapy.t Gram's stain obtained from involved soft tissue showed neutrophils and gram-positive diplococci.:j:Specimen may have been obtained after antibiotic therapy was instituted.§ This patient had two prior episodes of pneumococcal bacteremia, one of which was associated with a pneumococcal tuboovarian
abscess. The more recent of these, possibly associated with mildly symptomatic sinusitis, occurred in the month before shedeveloped mastitis.
JID 1991;163 (April)
responsible for a clinically significant superinfection or simply irrelevant colonization in case 5 is unclear. In two cases(5 and 7), pneumococci may not have been the only pathogens. Other possible foci of infection included the paranasalsinuses (cases 4 and 12) and lung (case 8).
Six patients had connective tissue diseases, diagnosed assystemic lupus erythematosus (SLE) in five. Four of thesewere on chronic corticosteroid therapy when their pneumococcal soft-tissue infection developed. Twoadditional patientswere HIV-seropositive intravenous drug-users.
Recurrent bacteremic infections with pneumococci weredocumented in three patients; two of these (cases 3 and 7)had two episodes of pneumococcal soft-tissue infection.
Case Reports
Case 1. A 74-year-old woman presented after the abrupt onsetof fever, rigors, and painful swelling of the left half of her tongue.Primary Sjogren's syndrome had been diagnosed 3 years earlier, forwhich she was being treated with 7.5 mg of prednisone daily. Onadmission, she had a rectal temperature of 39°C. The only significantphysical finding was an erythematous tongue about three or fourtimes normal size. Ceftriaxone and clindamycin were begun, andher dose of prednisone was increased. During the first hospital day,marked diminution of her tongue was noted and she became afebrile.Two sets of blood cultures obtained on admission grew S. pneumoniae. Antimicrobial therapy was changed to penicillin. Rapid improvement continued and the patient recovered completely.
Case 2. A 22-year-old woman with a history of SLE, treatedwith prednisone for 3 years, complained of chills, cough, shortnessof breath, joint pain, and tender red patches on the dorsum of her
left wrist. Three days before admission, she noted the sudden onsetof chills and protracted vomiting, which prevented her from takingher daily 5 mg of prednisone. On the day before admission, she developed exquisitely tender, reddened lesions on the dorsum of herleft wrist. Her temperature on admission was 40.5°C. Examinationrevealed periorbital edema, painless oral ulcers, basilar rales, apleural friction rub, and splenomegaly. There were multiple warm,tender, erythematous, indurated plaques on the dorsum of the leftwrist and posterolateral aspects of both shoulders. A chest radiograph was normal. Yellow viscous material was aspirated from asubcutaneous lesion near the left wrist; Gram's stain of this materialrevealed numerous gram-positive diplococci. Both the aspirate andblood cultures obtained on admission subsequently grew S. pneumoniae. She was begun on penicillin. A repeat chest radiograph revealed bilateral basilar infiltrates, but no sputum could be obtained.She had a rapid and ultimately complete response to therapy. Twoweeks after discharge, she received pneumococcal vaccine; rv6months later, she complained of pain, warmth, and swelling of herright knee. Synovial fluid aspirated from the right knee and left wristas well as simultaneous blood cultures grew S. pneumoniae.
Case3. A 38-year-old man with SLE presented with fever, chills,and difficulty with swallowing for the previous 2 days. He had received systemic corticosteroid therapy 10 years previously. His temperature was 38.3°C. Indirect laryngoscopy demonstrated a swollenred epiglottis. Because of a prior anaphylactic reaction to penicillin, therapy was initiated with intravenous chloramphenicol. Twosets of blood cultures obtained at admission grew S. pneumoniae.The patient quickly improved. Three months later, he again presentedwith epiglottiditis, and S. pneumoniae was recovered from bloodcultures. Complement (C3, C4, CHso) and immunoglobulin levels(including IgG subclasses) were normal or slightly increased. Antibodies to pneumococcal serotypes 3, 7, 9, and 14 were moderatelyto markedly elevated.
at The U
niversity of Alberta on O
ctober 22, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

JIO 1991;163 (April) Concise Communications 899
Case 4. A 36-year-old homosexual man requiring chronichemodialysis,with a history of tuberculosis, intravenousdrug use,and positive serology for human immunodeficiency virus (HIV),presented with increasing pain in his left ankle 2 weeks after blunttrauma. The ankle had been improvinguntil a few days before admission, when he developed fever and more pain near the ankle.His temperature was 39.4°C, and examination revealed tendererythematous swellingaround the left ankle. The patient wasbegunon cefazolin.A blood culture from admission grew S. pneumoniae.Radiographs of the chest revealedno infiltrates, of the sinus showedan air-fluid level in the left maxillary sinus, and of the left ankledisclosed only soft-tissue swelling. Erythema advanced up the leftlower extremity, and on hospital day 5, an area of fluctuation appeared near the left ankle. This area was aspirated; a Gram's staindisclosed no organisms. Incision and drainage were done; culturestaken at this time werenegative. The patient subsequentlyimproved.
Case5. A 33-year-oldwoman withaleft psoas abscess draineda monthearlier presented with feverand drainage from a left inguinal sinus tract. Four months before this admission, she had had apositive tuberculin skintest, forwhichisoniazidwasbegun.Sixweeksbeforeadmission, she had been hospitalizedfor a leftpsoas abscess,whichwasdrainedpercutaneously. Antibiotics werestarted, but routinebacterial cultureswerenegative andshewasdischarged. At home,her drain fell out. Subsequently she developed fever and swellingof the left flank. Yellow pus could be expressed from the old site.Gram'sstainof this material showedabundantneutrophilsand grampositivecocci; cultures grew only S. pneumoniae. The patient wastreated with cefoxitinfor 2 days and then penicillin and underwentincision anddrainage. "Routine culturesfromthe operationwerenegative. She responded clinically and was discharged. Mycobacterialcultures from her initial percutaneous drainage subsequently grewMycobacterium tuberculosis..
Case6. A 66-year-old womanwitha historyofa goiterandbreastcancer presented with a painful right thyroid mass. The patient hadhad respiratory symptomsassociated with shakingchills f\.J2 weeksearlier, for which she wastreated with erythromycin. One weekbefore admission, she developed tender swellingin the right anteriorneck. Her temperature on admission was 37.6°C. On physical examination a large, fixed, tender right thyroid mass was noted.Ultrasonography of her neck revealed a complexright thyroidmass,from which 30 ern! of thick bloody fluid was aspirated. Gram'sstain of this aspirate revealed many white blood cells and grampositivecocci. The-patientwas treated initially with nafcillin; afterthe culture of the thyroid aspirate grew S. pneumoniae, her therapywaschangedto penicillin. Computed tomography (CT) of the neckrevealed a well-demarcated, predominantly cystic mass involvingthe right lobe of the thyroid and extendingfrom the superior aspectof the clavicle to the level of the hyoidbone, with significantdeviation of the trachea to the contralateral side. The abscess wasdrainedand the patient recovered.Culturesfrom the surgicalspecimengrewS. pneumoniae.
Case 7. A 23-year-old woman with a history of SLE, who wasreceiving alternate-day prednisone, presented with tender swellingof the left breast. Three years earlier, she had undergone drainageof a tuboovarian abscess. Gram'sstainof that specimenrevealed manywhite cells, with abundant gram-positive cocci and a few grampositive rods; the culture grew only S. pneumoniae, as did bloodcultures. A month before the present admission, she had been admitted with fever and abdominal discomfort. S. pneumoniae was
again isolated from blood cultures. Sinus radiographs revealedevidence of sinusitis, althoughonly mild symptomscouldbe attributedto thiscondition. Atthepresentadmission, she complained ofa tenderlump in the left breast. She was not lactating. Her examinationwasunremarkable except forpainfulswelling of the leftbreast.Anaspirateof the breast massgrewS. pneumoniaeand Bacteroidesfragilis. Theinvolvedarea wasincisedand drained. She wastreated initiallywithcefazolin and improved. Levelsof C3 and C4 weremildlydepressed;levelsofC5-C8 and total hemolytic complementwere normal. Sheeventually recovered aftera complicated hospitalcourseduringwhichshe received multiple antibiotics and pneumococcal vaccine. Sinceher discharge >2 years ago, she has had no further pneumococcalinfections, although she has been hospitalized on severaloccasionsfor exacerbations of her lupus and once for bacteremic pneumoniacaused by Streptococcus pyogenes.
Case8. An 18-year-old womanwithSLE and renal insufficiencypresented with a I-dayhistory ofleft neck swelling, progressivedyspnea, and dysphagia. Three daysbefore admission she experiencedupper respiratory tract symptoms followed by stiffnessof the neck.She became febrile and developederythema of her neck and upperchest. She denied trauma. Her temperature was 39.4°C. Pertinentphysical findings included erythema and swelling with painfulhyperesthesiaof the leftneck and upper chest. Her chest radiographwas interpreted as showinga possible retrocardiac infiltrate. A CTscan revealedsoft-tissueswellinginvolvingthe base of her neck andleft anterior chest, pushing the trachea to the right, She was electively intubated, and a small surgical incision was made in her upper leftchest. Materialfromthis procedureand bloodwerecultured,and cefazolinand clindamycinwere administered. After blood cultures and the surgical specimen grew S. pneumoniae, her therapywaschanged to penicillin. Twodayslater, a repeat CT scan demonstrated soft-tissue swellingextending from the hyoid bone into themediastinumwithouta discreteabscess.The patientunderwent operativeexploration oftheleftneckwherenecrotizing fasciitis andthrombophlebitis of the internal jugular vein were found. The patientgradually recovered.
Case 9. A 35-year-oldwomanwith SLE presented with hoarseness and progressivedyspnea. She had been on 10mg of prednisonedaily for f\.JI year. On the day before admission, she experiencedgeneralized myalgias, rigors, a mild nonproductive cough, and fever. Her prednisone was increased to 30 mg daily. On admission,she exhibited marked hoarseness and became progressively moredyspneic. Her rectal temperature was 39.4°C. Rales were heard atthe right lung base, but her chest radiograph wasnormal. Althoughinitially she was alert, her level of consciousness deteriorated before upper airwaystructurescould be visualized,and she underwentcricothyrotomy. Shewasbegunon ampicillinandgentamicin. Laryngoscopicexamination revealed a markedlyerythematousand swollenepiglottis. Gram's stain of exudate from the epiglottisdemonstratedabundant gram-positive cocci. Cultures of this exudate and bloodgrew S. pneumoniae, and her antibiotics were changed to penicillin. The patient recovered.
CaseIQ A 25-year-old man with insulin-dependent diabetesmellitus complicated by retinopathy, blindness, and enucleation of theright eye presented after 2 daysof increasing pain in the right orbitwith purulentdischarge. The patient reportedmildrespiratory symI'toms during the previous week, followed by pain in the right orbit.The drainage from this site revealed many neutrophils and lancetshaped, gram-positive diplococci. He was begun on cefazolin and
at The U
niversity of Alberta on O
ctober 22, 2014http://jid.oxfordjournals.org/
Dow
nloaded from

900 Concise Communications JID 1991;163 (April)
gentamicin. When cultures revealed S. pneumoniae, the gentamicin was discontinued. He recovered uneventfully.
Case 11. A 23-year-old woman with a history of intravenous druguse who had suffered a motor vehicle accident rv6 months earlierpresented with swellingand pain in her left thigh. During the 3-monthhospitalization after her accident, she had required open reductionof several fractures. An intramedullary rod was implanted to stabilize a comminuted fracture of the left femur. Her HIV serology waspositive. About 3 days before this admission, she developed tenderswelling in the distal left thigh. She denied recent trauma to the area.On presentation, she was afebrile. Physical examination revealeda grossly swollen and erythematous distal left thigh, with an areaof fluctuationlaterally. Dark brown fluid was aspirated from the thigh,after which the area was incised and drained. Cultures grew onlyS. pneumoniae. The patient responded clinically to ceftriaxone butleft the hospital against medical advice.
Case 12. A 15-year-old retarded boy presented with right frontal headaches and altered mental status. He had been seen 2 daysearlier when frontal sinusitis was diagnosed on the basis of sinusradiographs. Cranial CT subsequently demonstrated a large frontal
Jobe mass. He was afebrile; he could follow simple commands, butintermittently became very lethargic. Neurologic evaluation revealeddecreased strength of his left arm and slight left facial weakness.At right frontal craniotomy, an abscess was excised, and 65 em' ofpurulent material was drained. This material was not foul-smelling;Gram's stain demonstrated neutrophils and gram-positive cocci without other organisms. Cultures yielded a pure growth of S. pneumoniae. The patient was initially begun on ceftriaxone, metronidazole,and penicillin. When culture results became available, ceftriaxonewas discontinued. The patient required drainage of his frontal sinusand another craniotomy but ultimately recovered.
Discussion
Our cases demonstrated that S. pneumoniae can cause serious infections of soft tissue. Although the precise frequencyof pneumococcal soft-tissue infections can not be estimatedfrom our review, they are probably more common than previously appreciated. Patients with SLE appear to be at thehighest risk for these infections. Three of our five lupus patients were receiving corticosteroid therapy, as was the patient with Sjogren's syndrome. Two additional patients wereHIV-seropositive intravenous drug users.
The infections in our series can be divided into those involving sites where pneumococci are uncommon but established pathogens (e.g., epiglottiditis [2], brain abscess [7],cellulitis [3, 4]) and those where pneumococcal infection hasrarely, if ever, been recognized (e.g., glossitis [11], mastitis[12], salpingitis [13], fasciitis [6]). Although patients with connective tissue diseases may develop infections of both types,the highly atypical infections occurred exclusivelyin this groupof patients. All four patients in our series who were receivingcorticosteroids had connective tissue disorders. We did not
identify a single case of pneumococcal soft-tissue infectionin patients on steroids for other reasons. Recurrent pneumococcal infections (three cases) were observed only in patientswith SLE.
Although connective tissue disease is not often cited as amajor risk factor for pneumococcal infections [1, 14], pneumococcal sepsis, pneumonia, arthritis, epiglottiditis, andperitonitis have been described in these patients [15]: Ourresults suggest that SLE and perhaps other connective tissuediseases may predispose to serious pneumococcal infectionsof soft tissues.
Acknowledgment
We thank Dawn M. Young and Su M. Lui for secretarial assistance,Robert Austrian and Steve Katz for advice and contributions, andAnna Longo DiNubile and Nancy DiNubile for insights and encouragement.
References
1. Burman LA, Norrby R, Trollfors B. Invasive pneumococcal infections:incidence, predisposing factors, and prognosis. Rev Infect Dis1985;7:132-42.
2. Chaisson RE. Epiglottitis in adults. In: Sande MA, Hudson LD, RootRK, eds. Respiratory infections. Vol. 5. New York: Churchill Livingstone, 1986:127-37.
3. Fleisher G, Ludwig S, Campos J. Cellulitis: bacterial etiology, clinicalfeatures, and laboratory findings. J Pediatr 1980;97:591-3.
4. Lewis RJ, Richmond AS, McGrory JP. Diplococcus pneumoniae cellulitis in drug addicts. JAMA 1975;232:54-5.
5. Hroncich ME, Rudinger AN. Rhabdomyolysis with pneumococcal pneumonia: a report of two cases. Am J Med 1989;86:467-8.
6. Dhaene M, Thys JP, Askenasi R, Toussaint C. Pneumococcal cellulitis.Am J Emerg Med 1986;4:225-6.
7. Chun CH, Johnson JD, Hofstetter M, Raft'MJ. Brain abscess: a studyof 45 consecutive cases. Medicine 1986;65:415-31.
8. Berger SA, Zonszein J, Zillamena P, Mittman N. Infectious diseasesof the thyroid gland. Rev Infect Dis 1983;5:108-22.
9. Marks WA, Bodensteiner JB. Anterior cervical epidural abscess withpneumococcus in an infant. J Child Neurol 1987;2:25-9.
10. Chulay JD, Lankerani MR. Splenic abscess. AmJ Med 1976;61:513-22.11. Burech DL, Koranyi K, Haynes RE, et al. Pneumococcal bacteremia
associated with gingival lesions in infants. Am J Dis Child1975;129:1283-4.
12. Walker AP, Edmiston CE, Krepel CJ, Condon RE. A prospective studyof the microftora of nonpuerperal breast abscess. Arch Surg 1988;123:908-11.
13. Westh H, Skibsted L, Korner B. Streptococcus pneumoniae infectionsof the female genital tract and in the newborn child. Rev Infect Dis1990;12:416-22.
14. Lipsky BA, Boyko EJ, Inui TS, Koepsell TD. Risk factors for acquiringpneumococcal infections. Arch Intern Med 1986;146:2179-85.
15. Van Der Straeten C, Wei N, Rothschild J, Goozh JL, Klippel JH. Rapidly fatal pneumococcal septicemia in systemic lupus erythematosus. J Rheumatol 1987;14:1177-80.
at The U
niversity of Alberta on O
ctober 22, 2014http://jid.oxfordjournals.org/
Dow
nloaded from