plasmodium ii mbbs dr ekta chourasia microbiology
TRANSCRIPT
PLASMODIUMPLASMODIUM
II MBBSII MBBS
Dr Ekta ChourasiaDr Ekta ChourasiaMicrobiology Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
TaxonomyTaxonomy
Phylum ApicomplexaPhylum Apicomplexa
Subphylum SporozoaSubphylum Sporozoa
Genus PlasmodiumGenus Plasmodium
Disease MalariaDisease Malaria
Geographical Tropical & Geographical Tropical &
distribution distribution
Subtropical countriesSubtropical countries
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Genus PlasmodiumGenus Plasmodium
Consists of 4 species:Consists of 4 species:1.1. P. vivaxP. vivax
2.2. P. falciparumP. falciparum
3.3. P. malariaeP. malariae
4.4. P. ovaleP. ovale
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Landmarks in the evolution of MalariaLandmarks in the evolution of Malaria
1880 – 1880 – LaveranLaveran identified the identified the malarial parasitemalarial parasite in in an unstained smearan unstained smear
1885 – 1885 – GolgiGolgi described the described the blood stage blood stage (erythrocytic schizogony) of malarial(erythrocytic schizogony) of malarial parasite – Golgi cycleparasite – Golgi cycle
1898 – 1898 – Amigo & GrassiAmigo & Grassi described the described the life cyclelife cycle1891 – 1891 – RomanowskyRomanowsky introduced the introduced the staining staining
methodmethod1897 – 1897 – Ronald RossRonald Ross while in Calcutta, India, while in Calcutta, India,
demonstrated Anopheles sp. of mosquitoes asdemonstrated Anopheles sp. of mosquitoes as vectors of malaria. vectors of malaria. Got Got Nobel prizeNobel prize for his work in 1902 for his work in 1902
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
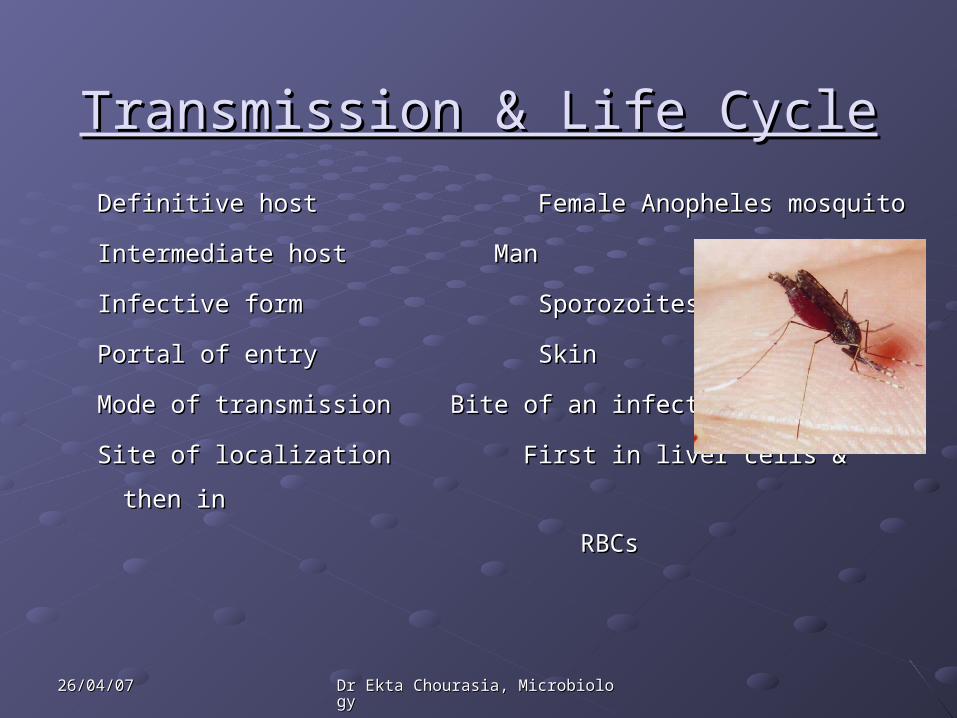
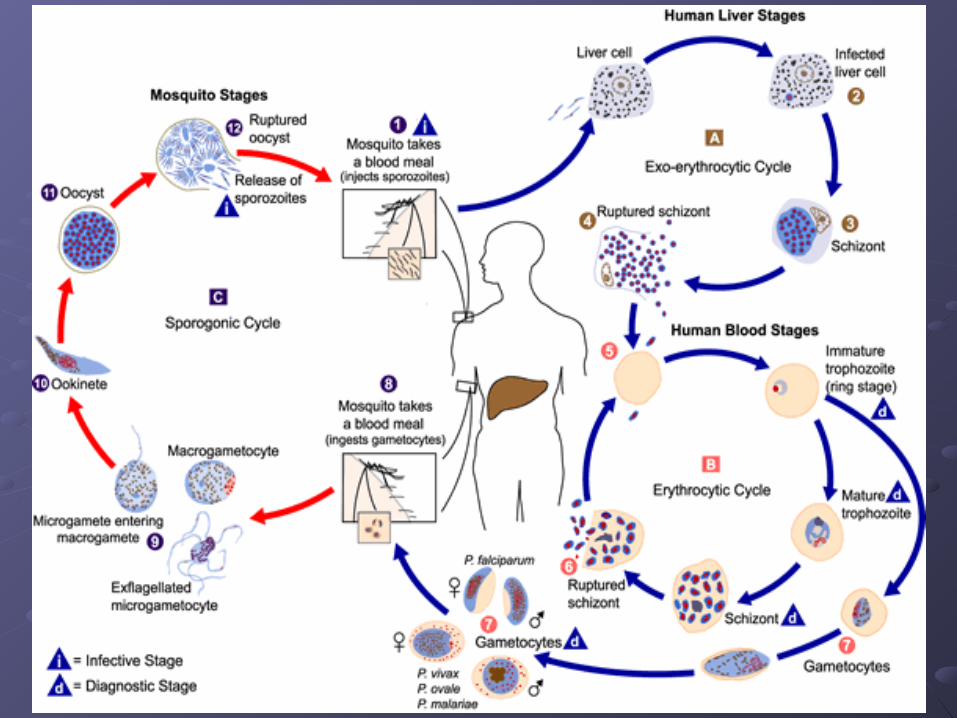
Transmission & Life CycleTransmission & Life Cycle
Definitive host Female Anopheles mosquitoDefinitive host Female Anopheles mosquito
Intermediate host ManIntermediate host Man
Infective form SporozoitesInfective form Sporozoites
Portal of entry SkinPortal of entry Skin
Mode of transmission Bite of an infected mosquitoMode of transmission Bite of an infected mosquito
Site of localization First in liver cells & then in Site of localization First in liver cells & then in
RBCs RBCs
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Phases of Development in ManPhases of Development in Man
2 phases of development2 phases of development
1.1. Inside the liver (tissue phase)Inside the liver (tissue phase) Pre- erythrocytic schizogonyPre- erythrocytic schizogony – no clinical – no clinical
symptoms, no pathological damagesymptoms, no pathological damage Exo- erythrocytic schizogonyExo- erythrocytic schizogony – cause of relapse – cause of relapse
2.2. Inside the RBCs (erythrocytic phase)Inside the RBCs (erythrocytic phase) Erythrocytic schizogonyErythrocytic schizogony – cause of malarial – cause of malarial
paroxsymsparoxsyms Gametogony Gametogony – infects mosquito– infects mosquito
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Morphological forms seen in HumansMorphological forms seen in Humans
In liver:In liver:1.1. SporozoitesSporozoites2.2. Pre erythrocytic schizontsPre erythrocytic schizonts
3.3. Merozoites – infect RBCsMerozoites – infect RBCs
In RBCs :In RBCs :1.1. Trophozoites – ring formTrophozoites – ring form2.2. Schizonts Schizonts 3.3. Merozoites – released by the rupture of schizonts Merozoites – released by the rupture of schizonts
– infect other RBCs– infect other RBCs4.4. Gametocytes – micro and macro gametocytesGametocytes – micro and macro gametocytes

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Morphological forms seen in MosquitoMorphological forms seen in Mosquito
Further differentiation & development of Further differentiation & development of gametocytes take place in mosquitogametocytes take place in mosquito
1.1. Macro gametes (female gametes)Macro gametes (female gametes) – each macro – each macro gametocyte develops in to one macro gamete in gametocyte develops in to one macro gamete in the mid gut of mosquitothe mid gut of mosquito
2.2. Micro gametes (male gametes)Micro gametes (male gametes) – one micro – one micro gametocyte produces 6 to 8 micro gametes by gametocyte produces 6 to 8 micro gametes by exflagellation.exflagellation.
3.3. ZygoteZygote – – OokineteOokinete – – OocystOocyst – rupture – release of – rupture – release of SporozoitesSporozoites – predilection to salivary glands. – predilection to salivary glands.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Other modes of transmissionOther modes of transmissionSporozoite- induced- malariaSporozoite- induced- malaria : injection of an : injection of an emulsion of salivary glands of mosquito containing emulsion of salivary glands of mosquito containing sporozoitessporozoites
Trophozoite- induced- malariaTrophozoite- induced- malaria : injection of blood : injection of blood from a malarial patient containing the asexual from a malarial patient containing the asexual forms of erythrocytic schizogony e.gforms of erythrocytic schizogony e.g..
1.1. Transfusion malariaTransfusion malaria – when persons with latent – when persons with latent infection are used as donorsinfection are used as donors
2.2. Congenital malariaCongenital malaria – transmission through some – transmission through some placental defects (a healthy placenta acts as a placental defects (a healthy placenta acts as a physiological barrier)physiological barrier)
3.3. Drug addictsDrug addicts – by using same syringe – by using same syringe
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Incubation periodIncubation period
P. vivax P. vivax
P. ovale 10 to 14 daysP. ovale 10 to 14 days
P. falciparum P. falciparum
P. malariae 18 days to 6 P. malariae 18 days to 6
weeksweeks
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Pathogenicity Pathogenicity Infection causes intermittent fever – MalariaInfection causes intermittent fever – Malaria
Each of the 4 species causes a characteristic Each of the 4 species causes a characteristic fever:fever:
P. vivaxP. vivax Benign Benign tertiantertian/ vivax malaria/ vivax malaria
P. falciparumP. falciparum Malignant Malignant tertiantertian/ falciparum/ falciparum
malaria, black water fevermalaria, black water fever
P. malariaeP. malariae QuartanQuartan malaria malaria
P. ovaleP. ovale TertianTertian/ Ovale malaria / Ovale malaria
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Clinical FeaturesClinical FeaturesSeries of febrile paroxysmsSeries of febrile paroxysms – fever is caused – fever is caused by the release of merozoites & toxins from by the release of merozoites & toxins from ruptured erythrocytic schizont which in turn ruptured erythrocytic schizont which in turn causes the release of cytokines.causes the release of cytokines.
Quartan malaria – every 72 hrsQuartan malaria – every 72 hrs Tertian malaria - every 48 hrs Tertian malaria - every 48 hrs
* each paroxysm has 3 stages - * each paroxysm has 3 stages - cold stagecold stage (rigors), (rigors), hot stagehot stage (high temp., body & joint (high temp., body & joint pains, vomiting & diarrhoea) and pains, vomiting & diarrhoea) and perspirationperspiration stage stage (fall in temp.) (fall in temp.)

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Clinical FeaturesClinical Features
AnaemiaAnaemia – due to breakdown of RBCs, – due to breakdown of RBCs, particularly occurs in falciparum malariaparticularly occurs in falciparum malaria
Splenomegaly Splenomegaly – all forms – all forms
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Falciparum MalariaFalciparum MalariaMost widespreadMost widespread
Accounts for 80% of malaria cases Accounts for 80% of malaria cases worldwideworldwide
Most pathogenic of human malaria Most pathogenic of human malaria speciesspecies
Untreated infections - severe disease & Untreated infections - severe disease & even death, particularly in young children, even death, particularly in young children, pregnant woman & non immune adults.pregnant woman & non immune adults.

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Falciparum malariaFalciparum malariaSevere falciparum malaria is Severe falciparum malaria is associated withassociated with
1.1. Pernicious malaria /cerebral malariaPernicious malaria /cerebral malaria
2.2. Blackwater feverBlackwater fever
3.3. AnaemiaAnaemia
4.4. HypoglycaemiaHypoglycaemia
5.5. Hypotension Hypotension
6.6. Complications in pregnancyComplications in pregnancy
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Pernicious MalariaPernicious Malaria
Def:Def: refers to a series of phenomenon refers to a series of phenomenon occurring during infection with P. falciparum occurring during infection with P. falciparum which, if not effectively treated, threatens the which, if not effectively treated, threatens the life of the patient with in 1 to 3 dayslife of the patient with in 1 to 3 days
In children & non immune adults, can cause In children & non immune adults, can cause coma & death – Cerebral malaria.coma & death – Cerebral malaria.
Occurs as a result of capillary blockage.Occurs as a result of capillary blockage.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Black Water FeverBlack Water Fever
Occurs in Occurs in previously infectedpreviously infected subjects subjects
Can also occur in Can also occur in non immune adultsnon immune adults with with severe falciparum malaria, and also as a severe falciparum malaria, and also as a complication of quinine therapycomplication of quinine therapy..
A rare but acute condition characterised by A rare but acute condition characterised by sudden & sudden & massive hemolysismassive hemolysis of parasitised & of parasitised & non parasitised RBCs followed by fever and non parasitised RBCs followed by fever and haemoglobinuriahaemoglobinuria..
Often Often fatalfatal due to due to renal failurerenal failure
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
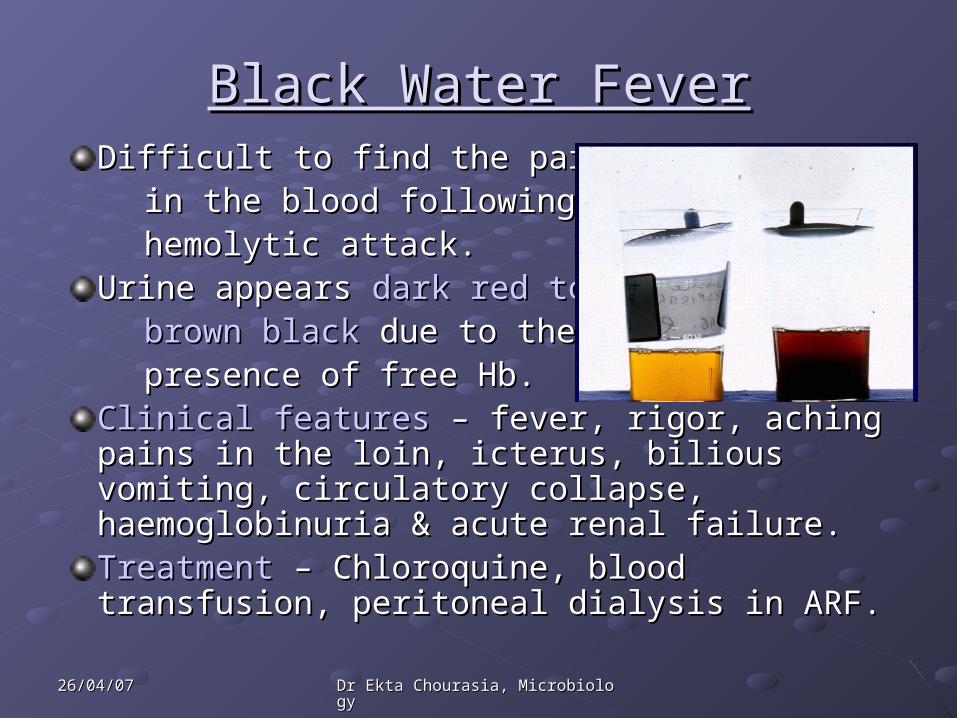
Black Water FeverBlack Water FeverDifficult to find the parasites Difficult to find the parasites
in the blood following a in the blood following a hemolytic attack.hemolytic attack.
Urine appears Urine appears dark red todark red to brown blackbrown black due to the due to the presence of free Hb.presence of free Hb.
Clinical featuresClinical features – fever, rigor, aching pains in – fever, rigor, aching pains in the loin, icterus, bilious vomiting, circulatory the loin, icterus, bilious vomiting, circulatory collapse, haemoglobinuria & acute renal failure.collapse, haemoglobinuria & acute renal failure.Treatment Treatment – Chloroquine, blood transfusion, – Chloroquine, blood transfusion, peritoneal dialysis in ARF.peritoneal dialysis in ARF.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
AnaemiaAnaemiaCan be severe & occur rapidly, Can be severe & occur rapidly, particularly in young childrenparticularly in young children
Occurs due to Occurs due to destruction of parasitiseddestruction of parasitised RBCs RBCs – phagocytosis & destruction in the – phagocytosis & destruction in the spleenspleen
Decreased production of RBCs in the Decreased production of RBCs in the bone marrow.bone marrow.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Falciparum malaria in PregnancyFalciparum malaria in Pregnancy
Can result in:Can result in:
Severe anemia Severe anemia
Low birth weight babiesLow birth weight babies
Greatest risk in 1Greatest risk in 1stst pregnancy pregnancy
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Malaria caused by P.vivax, Malaria caused by P.vivax, P.ovale & P.malariaeP.ovale & P.malariae
Rarely life threateningRarely life threatening
Relapses/ recurrences are a featureRelapses/ recurrences are a feature
Recurrences in MalariaRecurrences in MalariaMay result from – reinfection or May result from – reinfection or
- due to certain events related - due to certain events related
to the parasite’s life cycleto the parasite’s life cycle
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Recurrence of MalariaRecurrence of MalariaTwo types of recurrences known in malaria:Two types of recurrences known in malaria:
1.1. RecrudescenceRecrudescence – – seen in seen in P. falciparum & P. malariaeP. falciparum & P. malariae due to due to persistence of blood infectionpersistence of blood infection (some (some
erythrocytic forms evade host immunity) even after erythrocytic forms evade host immunity) even after clinical illness has subsided.clinical illness has subsided.
The numbers may increase later, leading to The numbers may increase later, leading to reappearance of clinical symptomsreappearance of clinical symptoms
Occur mostly up to one year or so but in P. malariae, Occur mostly up to one year or so but in P. malariae, it can occur even after decadesit can occur even after decades

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Recurrence of MalariaRecurrence of Malaria2.2. RelapseRelapse
Occurs due to a special form of parasites Occurs due to a special form of parasites – – hypnozoiteshypnozoites..
Hypnozoites are the sporozoites that Hypnozoites are the sporozoites that remain dormant after infecting liverremain dormant after infecting liver
Activated from time to time to initiate pre Activated from time to time to initiate pre erythrocytic schizogony - erythrocytic schizogony - Exoerythrocytic Exoerythrocytic schizogonyschizogony
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Genetic factors protecting Genetic factors protecting against Malariaagainst Malaria
Sickle cell anaemiaSickle cell anaemia – sickle celled RBCs are – sickle celled RBCs are removed by the spleen before the development removed by the spleen before the development of schizontsof schizonts
Ovalocytosis –Ovalocytosis – RBCs are rigid and they resist RBCs are rigid and they resist parasitic invasionparasitic invasion
Duffy blood group negativeDuffy blood group negative individuals – duffy individuals – duffy blood group Ag is the receptor for the blood group Ag is the receptor for the attachment of merozoites of P.vivaxattachment of merozoites of P.vivax
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Genetic factors protecting Genetic factors protecting against Malariaagainst Malaria
Newborn infantsNewborn infants – natural protection for – natural protection for 11stst few months of life due to high conc. of few months of life due to high conc. of HbF in their RBCs.HbF in their RBCs.
Beta thalassaemiaBeta thalassaemia – protects against – protects against severe falciparum infectionsevere falciparum infection
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Laboratory Diagnosis Laboratory Diagnosis
Microscopy Microscopy – detecting & identifying malarial – detecting & identifying malarial parasites in peripheral blood films.parasites in peripheral blood films.
Concentrating parasitesConcentrating parasites in venous blood by in venous blood by centrifugation when they can not be found in centrifugation when they can not be found in blood filmsblood films
Using a Using a rapidrapid malaria Ag or enzyme malaria Ag or enzyme detection detection testtest
Other testsOther tests – Hb, PCV, Blood glucose, total – Hb, PCV, Blood glucose, total WBC & platelet count.WBC & platelet count.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Examination of Blood filmExamination of Blood filmCollection of bloodCollection of blood
- best prepared directly from capillary blood- best prepared directly from capillary blood
- in EDTA bulb (used within 30 mins)- in EDTA bulb (used within 30 mins)
Time of collectionTime of collection
- as soon as possible if malaria is suspected- as soon as possible if malaria is suspected
- before administering antimalarials- before administering antimalarials
- during pyrexial phase- during pyrexial phase
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Types of Blood filmTypes of Blood film
Two types:Two types:
1.1. Thick filmsThick films : :
- 30 to 40 times - 30 to 40 times more sensitivemore sensitive than thin films than thin films
- more suitable for - more suitable for detection of malarialdetection of malarial parasiteparasite when they are few in numberwhen they are few in number
- blood is not fixed, RBCs are lysed during - blood is not fixed, RBCs are lysed during staining (only parasitic forms will be seen)staining (only parasitic forms will be seen)
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Types of Blood filmTypes of Blood film2. Thin films :2. Thin films : - to - to confirm the Plasmodium speciesconfirm the Plasmodium species - assists in the identification of - assists in the identification of mixed mixed
infectionsinfections - blood is fixed, parasites are seen within - blood is fixed, parasites are seen within
the RBCs the RBCs - also helps in assessing the - also helps in assessing the response toresponse to
treatmenttreatment especially in areas where especially in areas where drug drug resistance is suspected (by counting resistance is suspected (by counting the the number of parasitised RBCs before & number of parasitised RBCs before &
after the treatment)after the treatment)

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Making of Thin & Thick filmsMaking of Thin & Thick films
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Fixation & StainingFixation & Staining
FixationFixation – thin films are fixed with absolute – thin films are fixed with absolute alcohol for 1 to 2 mins. alcohol for 1 to 2 mins.
Staining Staining – films are stained with – films are stained with Romanowsky stain: giemsa, Romanowsky stain: giemsa,
field’s, wright’s field’s, wright’s
Giemsa Giemsa – 10% solution for 10 mins– 10% solution for 10 mins

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
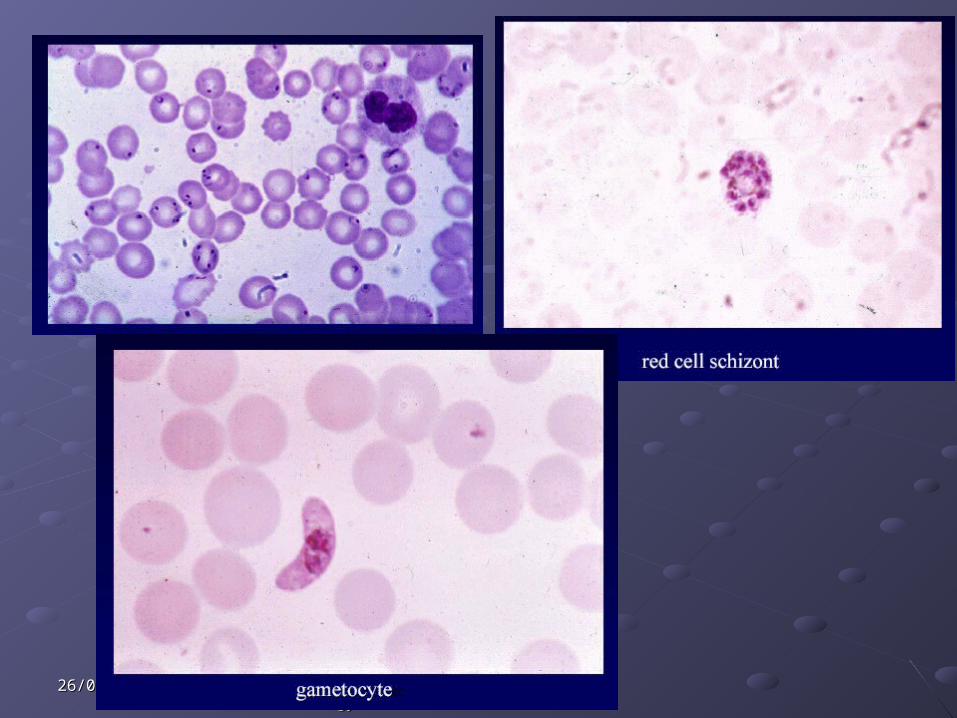
Reporting of Blood filmReporting of Blood filmLook for the Look for the different morphologicaldifferent morphological formsforms of parasite in blood smear: of parasite in blood smear:
1.1. Trophozoites / ring formsTrophozoites / ring forms2.2. Schizont Schizont 3.3. Gametocytes Gametocytes
Identify speciesIdentify species – differences in the – differences in the characteristics of morphological forms in characteristics of morphological forms in different speciesdifferent species
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
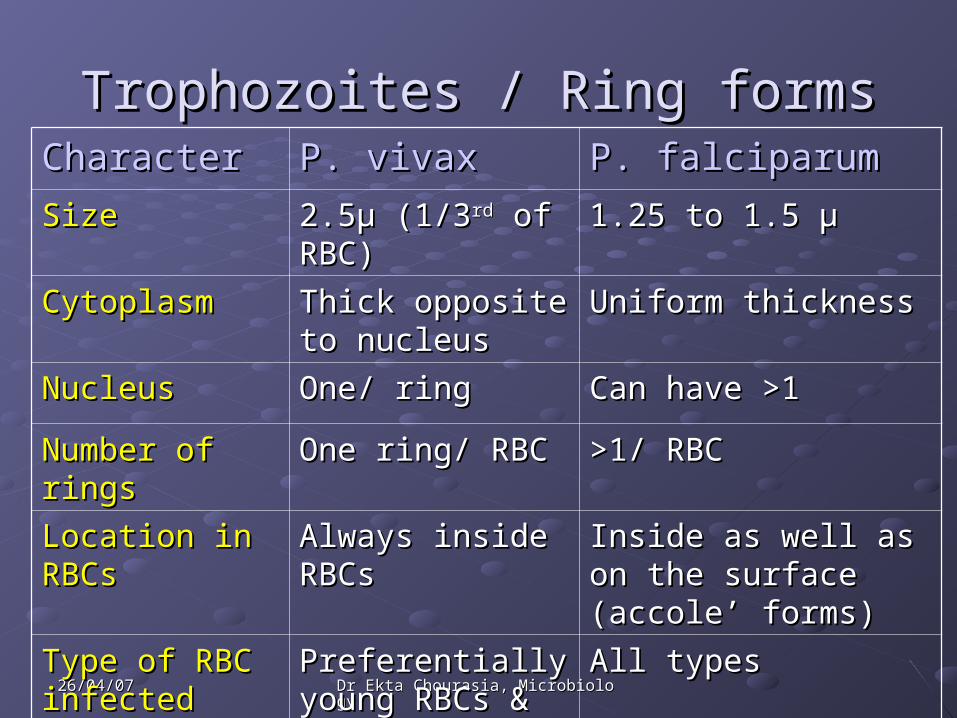
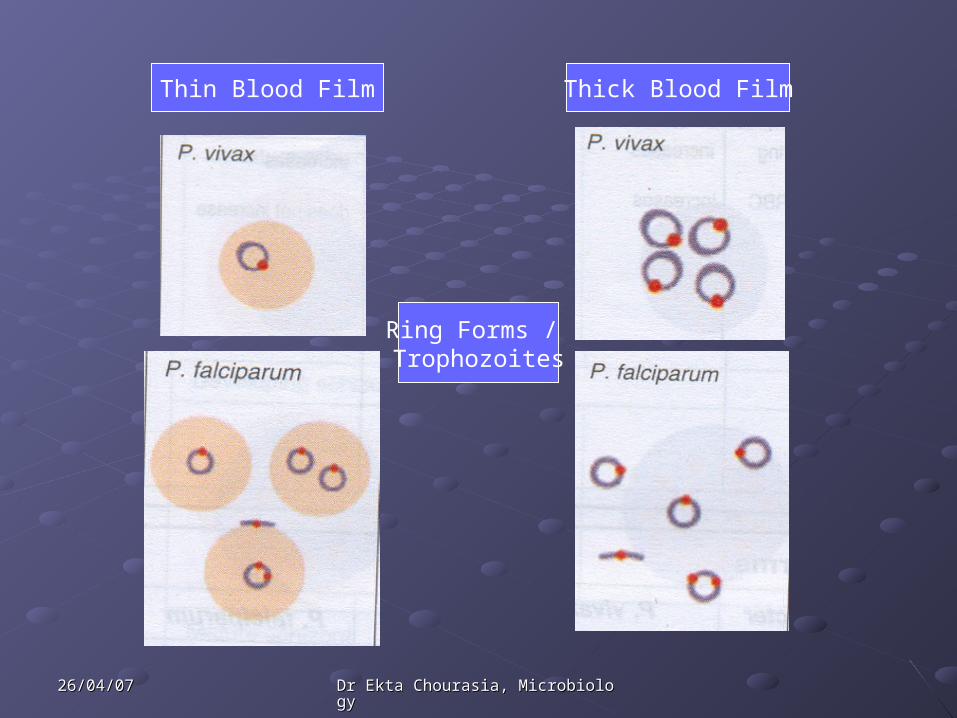
Trophozoites / Ring formsTrophozoites / Ring formsCharacter Character P. vivaxP. vivax P. falciparumP. falciparum
Size Size 2.52.5µµ (1/3 (1/3rdrd of RBC) of RBC) 1.25 to 1.5 1.25 to 1.5 µµ
Cytoplasm Cytoplasm Thick opposite to Thick opposite to nucleusnucleus
Uniform thicknessUniform thickness
NucleusNucleus One/ ringOne/ ring Can have >1Can have >1
Number of ringsNumber of rings One ring/ RBCOne ring/ RBC >1/ RBC>1/ RBC
Location in Location in RBCsRBCs
Always inside Always inside RBCsRBCs
Inside as well as on the Inside as well as on the surface (accole’ forms)surface (accole’ forms)
Type of RBC Type of RBC infectedinfected
Preferentially Preferentially young RBCs & young RBCs & reticulocytesreticulocytes
All typesAll types
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Thin Blood Film Thick Blood Film
Ring Forms / Trophozoites
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
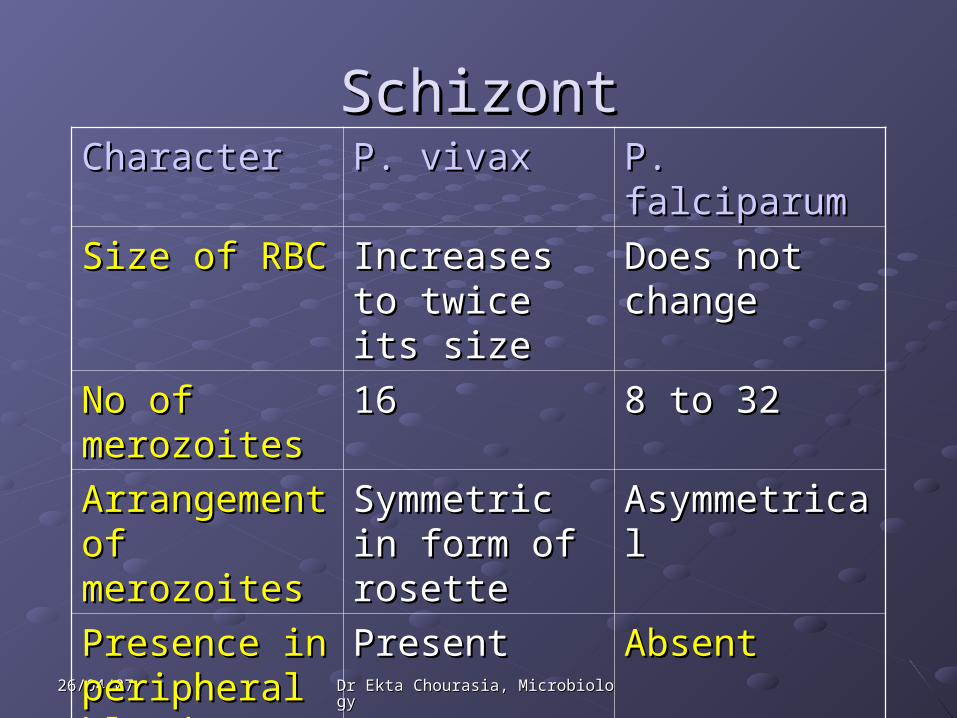
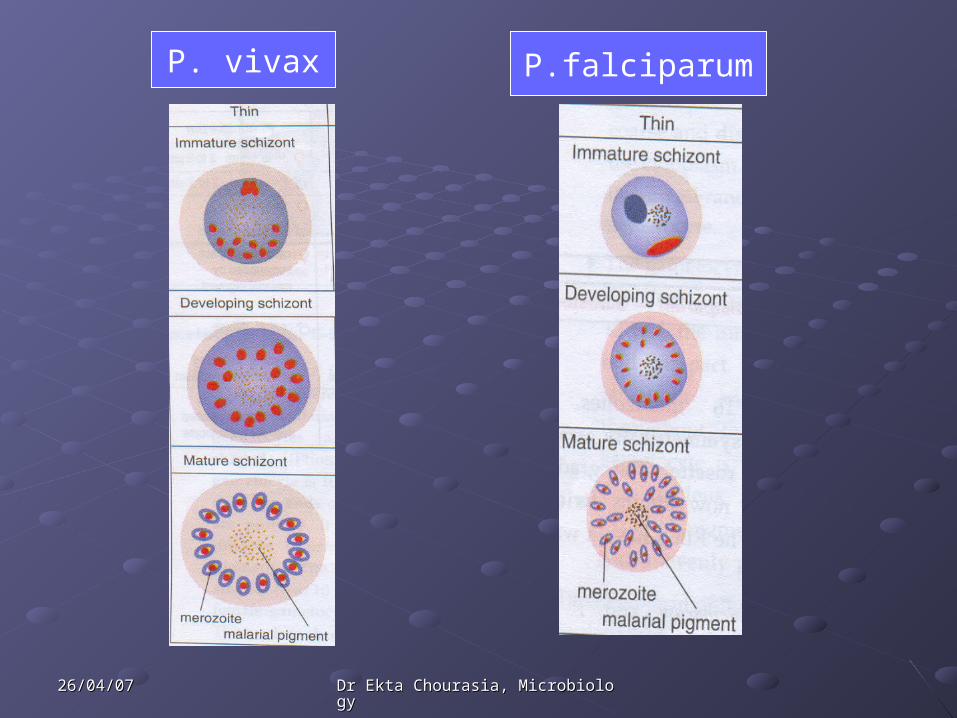
SchizontSchizontCharacterCharacter P. vivaxP. vivax P. falciparum P. falciparum
Size of RBCSize of RBC Increases to Increases to twice its sizetwice its size
Does not Does not changechange
No of No of merozoitesmerozoites
1616 8 to 328 to 32
Arrangement Arrangement of merozoitesof merozoites
Symmetric in Symmetric in form of rosetteform of rosette
Asymmetrical Asymmetrical
Presence in Presence in peripheral peripheral bloodblood
Present Present Absent Absent
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
P. vivax P.falciparum
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
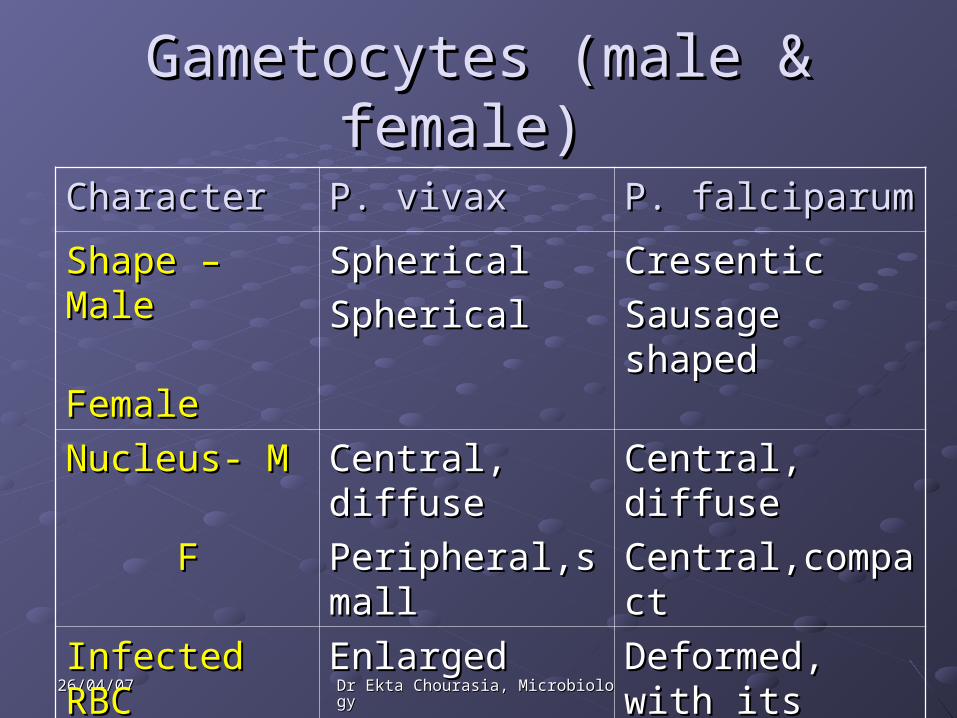
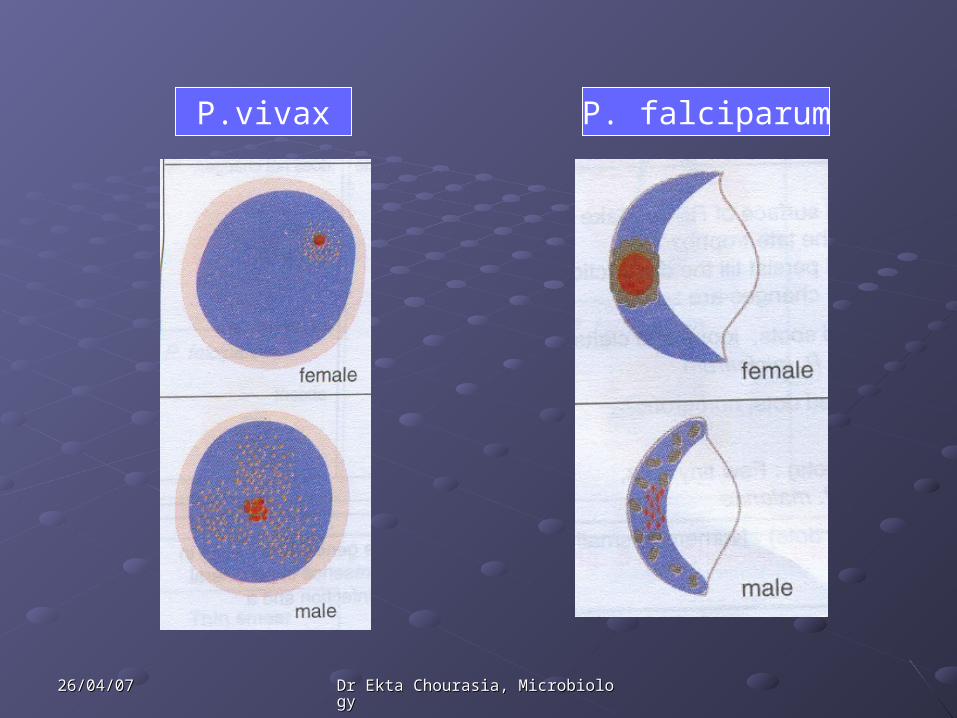
Gametocytes (male & female) Gametocytes (male & female)
Character Character P. vivaxP. vivax P. falciparumP. falciparum
Shape – MaleShape – Male
Female Female
SphericalSpherical
SphericalSpherical
CresenticCresentic
Sausage shapedSausage shaped
Nucleus- MNucleus- M
FF
Central, diffuseCentral, diffuse
Peripheral,smallPeripheral,small
Central, diffuseCentral, diffuse
Central,compactCentral,compact
Infected RBCInfected RBC Enlarged Enlarged Deformed, with Deformed, with its membrane its membrane stretched.stretched.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
P. falciparumP.vivax
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Counting the % age of Counting the % age of parasitised RBCsparasitised RBCs
On thin blood filmsOn thin blood filmsWhen falciparum malaria parasitemia is highWhen falciparum malaria parasitemia is highMethod of counting:Method of counting:
1.1. Select an area where no of RBCs is roughly 250.Select an area where no of RBCs is roughly 250.2.2. Count the no of parasitised RBCs in 4 such fields i.e. Count the no of parasitised RBCs in 4 such fields i.e.
approximately 1000 RBCs.approximately 1000 RBCs.3.3. Divide by 10 to obtain the percentage.Divide by 10 to obtain the percentage.
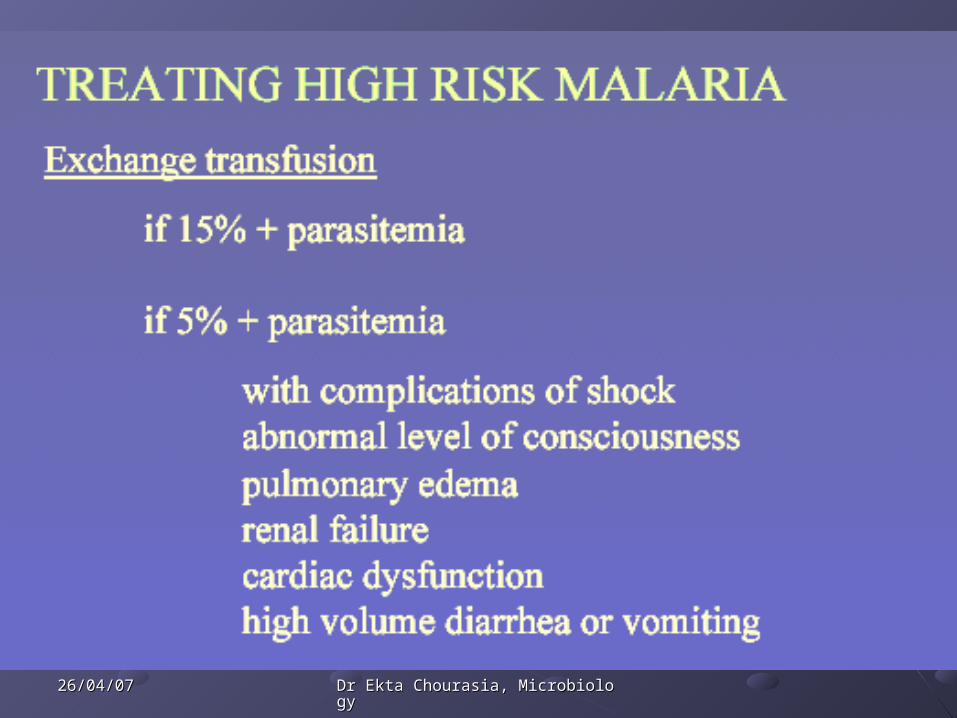
*WHO – if it is >5%, then the parasitemia is *WHO – if it is >5%, then the parasitemia is heavy & prognosis is poor.heavy & prognosis is poor.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Buffy Coat preparationBuffy Coat preparation
To concentrate malarial parasiteTo concentrate malarial parasite
Centrifuge EDTA anticoagulated venous Centrifuge EDTA anticoagulated venous blood in a thin bore capillary tubeblood in a thin bore capillary tube
Buffy coat layer is formed between the Buffy coat layer is formed between the RBCs & the plasma.RBCs & the plasma.
Break the tube & transfer buffy coat & Break the tube & transfer buffy coat & RBCs to a slide - make a thin smear – air RBCs to a slide - make a thin smear – air dry – fix with ethanol – stain with Giemsa.dry – fix with ethanol – stain with Giemsa.

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Quantitative Buffy CoatQuantitative Buffy Coat
Capillary tube is coated with an Capillary tube is coated with an anticoagulant & Acridine orange anticoagulant & Acridine orange fluorescent dyefluorescent dye
After centrifugation, the tube can be used After centrifugation, the tube can be used for two purpose:for two purpose:
1.1. Complete blood countComplete blood count
2.2. Identification of malarial parasite using a Identification of malarial parasite using a fluorescence microscope.fluorescence microscope.

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Quantitative Buffy Coat

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Rapid Diagnostic testsRapid Diagnostic tests
Developed to Developed to diagnose falciparum malariadiagnose falciparum malaria rapidly & without a microscope.rapidly & without a microscope.
Can also detect Can also detect vivax malariavivax malaria
Three tests are available commercially Three tests are available commercially
Detects either Detects either HRP2 Ag (Histidine rich protein)HRP2 Ag (Histidine rich protein) or or specific pLDH (parasite lactate dehydrogenase)specific pLDH (parasite lactate dehydrogenase)
Both HRP2 & pLDH are produced by the Both HRP2 & pLDH are produced by the parasites during their growth & differentiation in parasites during their growth & differentiation in RBCs.RBCs.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Rapid Diagnostic testsRapid Diagnostic tests
HRP2 testsHRP2 tests detection of P.falciparumdetection of P.falciparumTwo types of test – ParaSight FTwo types of test – ParaSight F
- ICT Malaria Pf- ICT Malaria Pf
pLDH test e.g. OptiMAL testpLDH test e.g. OptiMAL testDetection of P.falciparum & P.vivaxDetection of P.falciparum & P.vivaxProduced by all human malarial parasitesProduced by all human malarial parasitesDifferentiation of species is based on antigenic Differentiation of species is based on antigenic differences between pLDH isoforms. differences between pLDH isoforms.
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
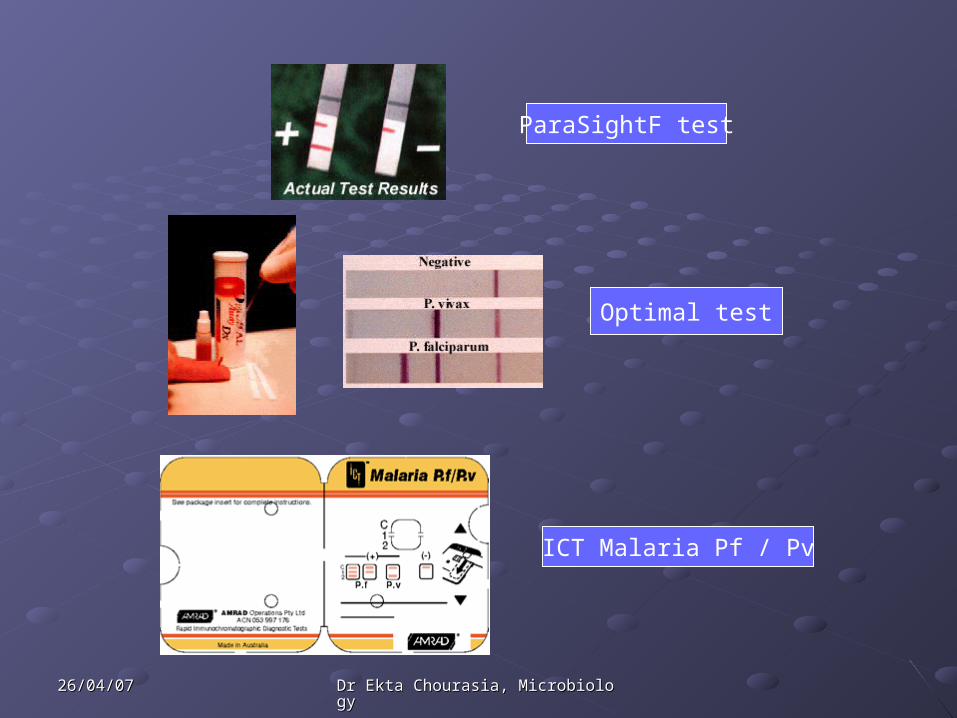
Optimal test
ParaSightF test
ICT Malaria Pf / Pv
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
Stage specificity of antimalarial drugsStage specificity of antimalarial drugs
Stage of malarial Stage of malarial parasiteparasite
Antimalarial drugAntimalarial drug
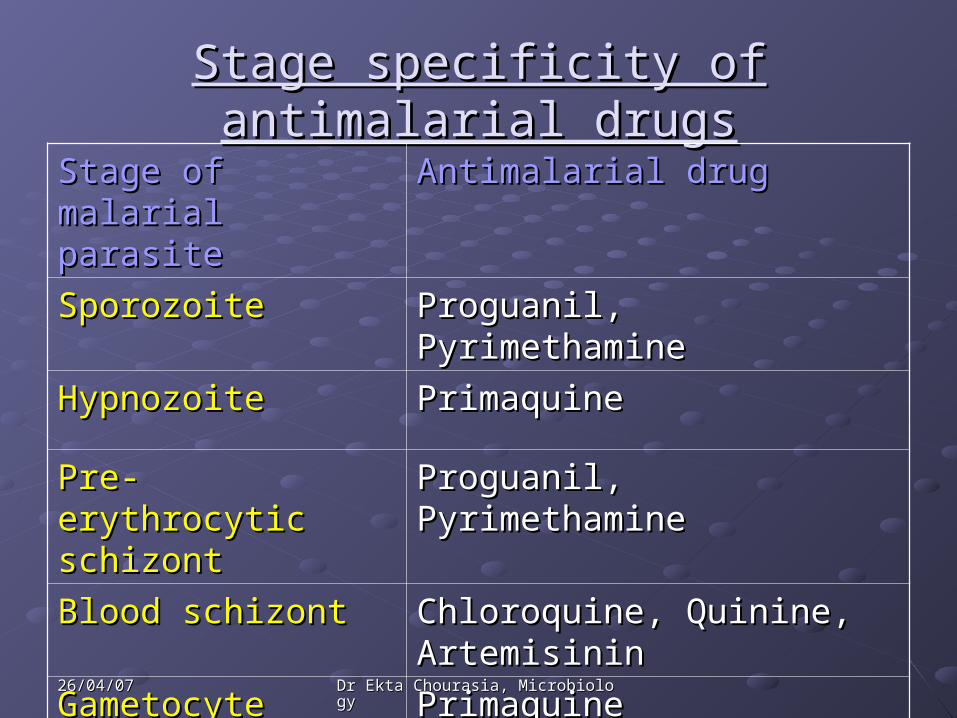
Sporozoite Sporozoite Proguanil, PyrimethamineProguanil, Pyrimethamine
Hypnozoite Hypnozoite Primaquine Primaquine
Pre- erythrocytic Pre- erythrocytic schizontschizont
Proguanil, PyrimethamineProguanil, Pyrimethamine
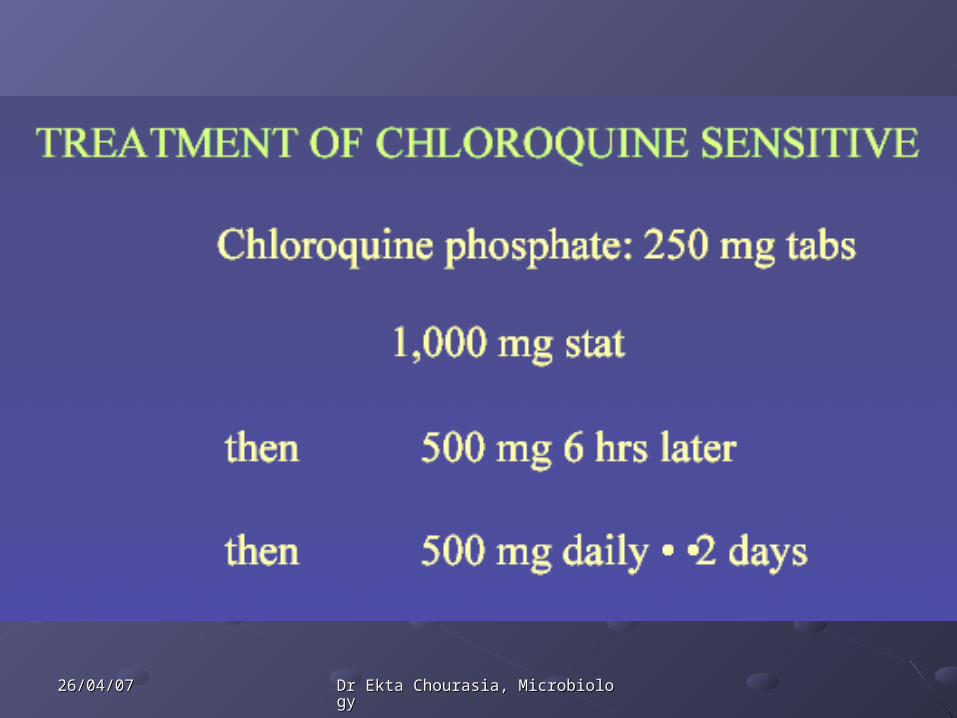
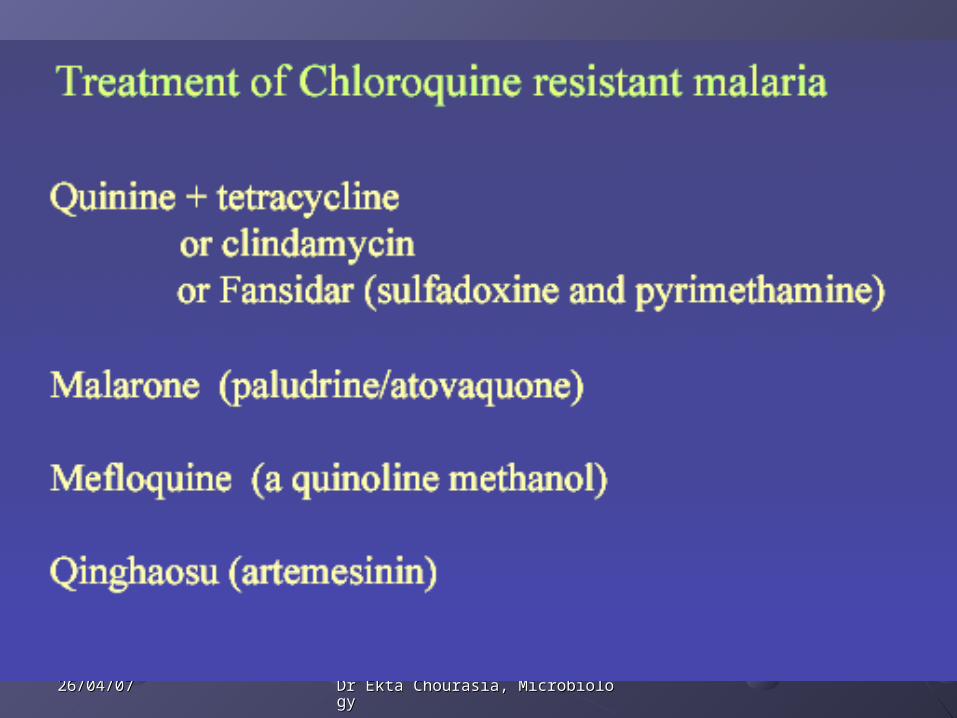
Blood schizontBlood schizont Chloroquine, Quinine, Chloroquine, Quinine, ArtemisininArtemisinin
Gametocyte Gametocyte Primaquine Primaquine
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology

26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology
26/04/0726/04/07 Dr Ekta Chourasia, MicrobiologyDr Ekta Chourasia, Microbiology