pictoral essay: congenital anomalies of the branchial apparatus authorsinstitutions
TRANSCRIPT
Pictoral Essay: Pictoral Essay: Congenital Congenital
Anomalies of the Anomalies of the Branchial Branchial ApparatusApparatusAuthorsAuthors
InstitutionsInstitutions
Objectives:Objectives: Understand Embryology of the branchial Understand Embryology of the branchial
apparatus and embryogenesis of its apparatus and embryogenesis of its anomalies.anomalies.
Understand various classifications of Understand various classifications of branchial anomalies. branchial anomalies.
Recognize and interpret imaging findings Recognize and interpret imaging findings associated with anomalies of the associated with anomalies of the branchial apparatus.branchial apparatus.
Direct workup using various imaging Direct workup using various imaging modalities used in evaluation of branchial modalities used in evaluation of branchial anomalies.anomalies.
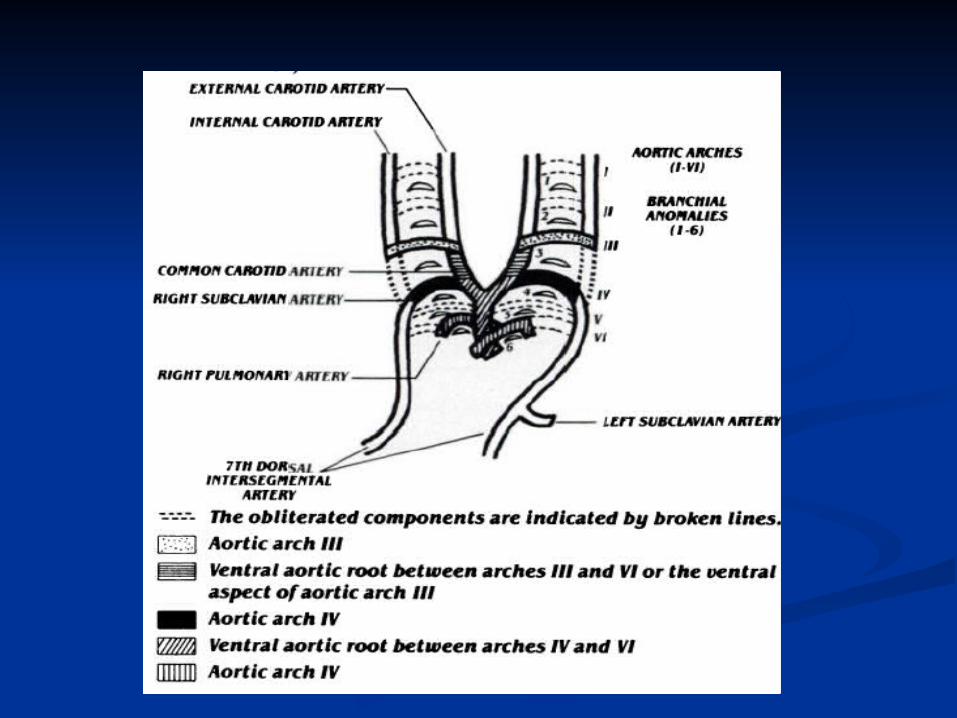
Embryology of Branchial Embryology of Branchial ApparatusApparatus
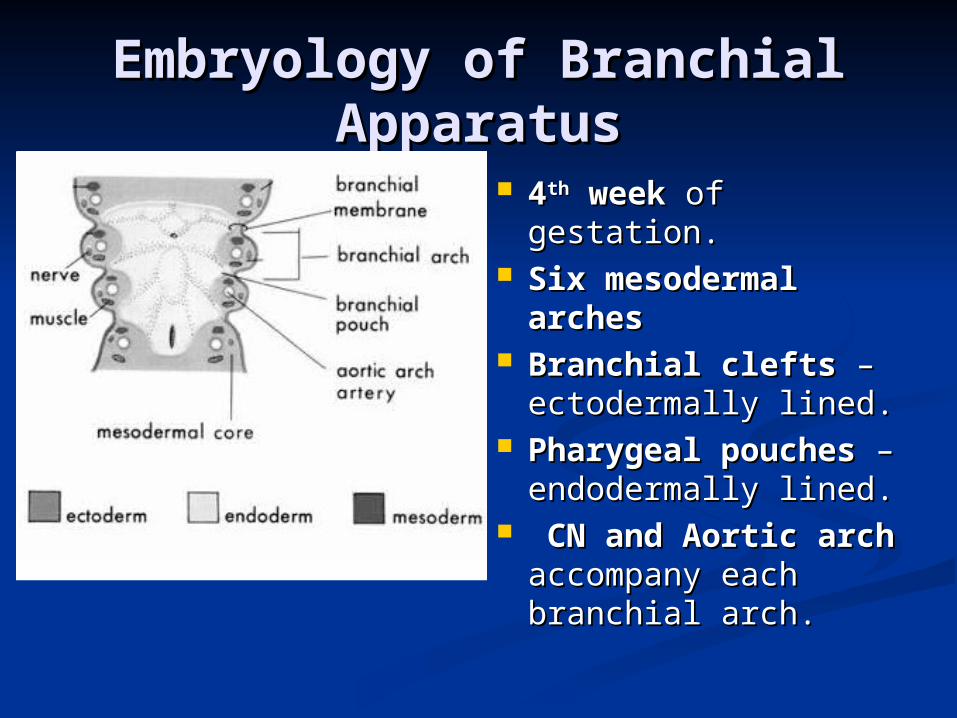
44thth week week of of gestation.gestation.
Six mesodermal Six mesodermal archesarches
Branchial cleftsBranchial clefts – – ectodermally lined.ectodermally lined.
Pharygeal pouchesPharygeal pouches – endodermally lined.– endodermally lined.
CN and Aortic CN and Aortic archarch accompany accompany each branchial arch.each branchial arch.
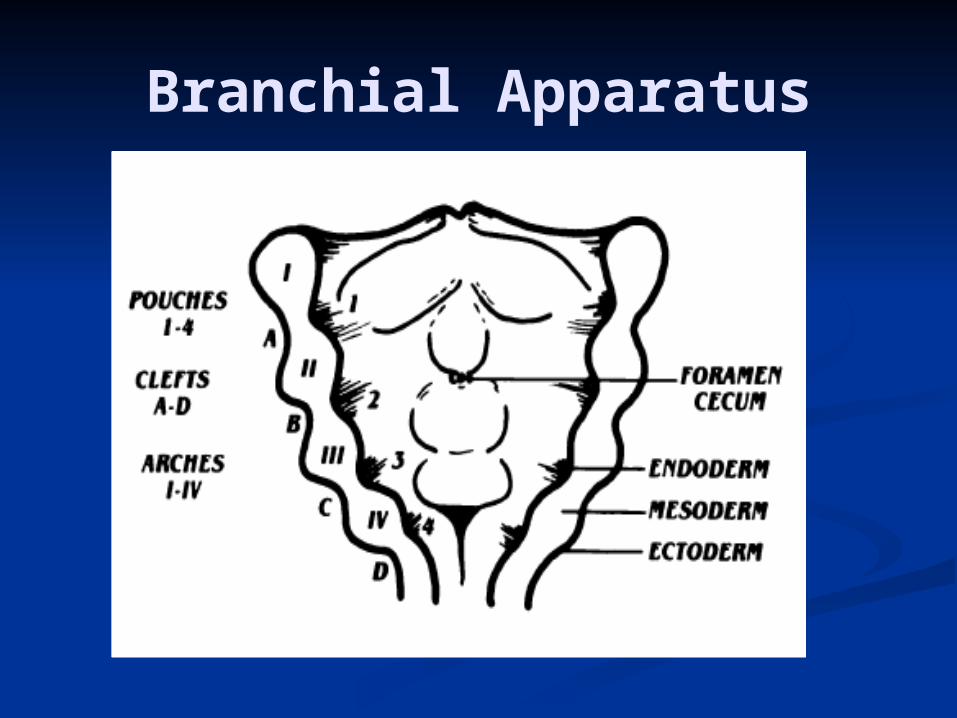
Branchial Apparatus
Development of Branchial Development of Branchial ApparatusApparatus
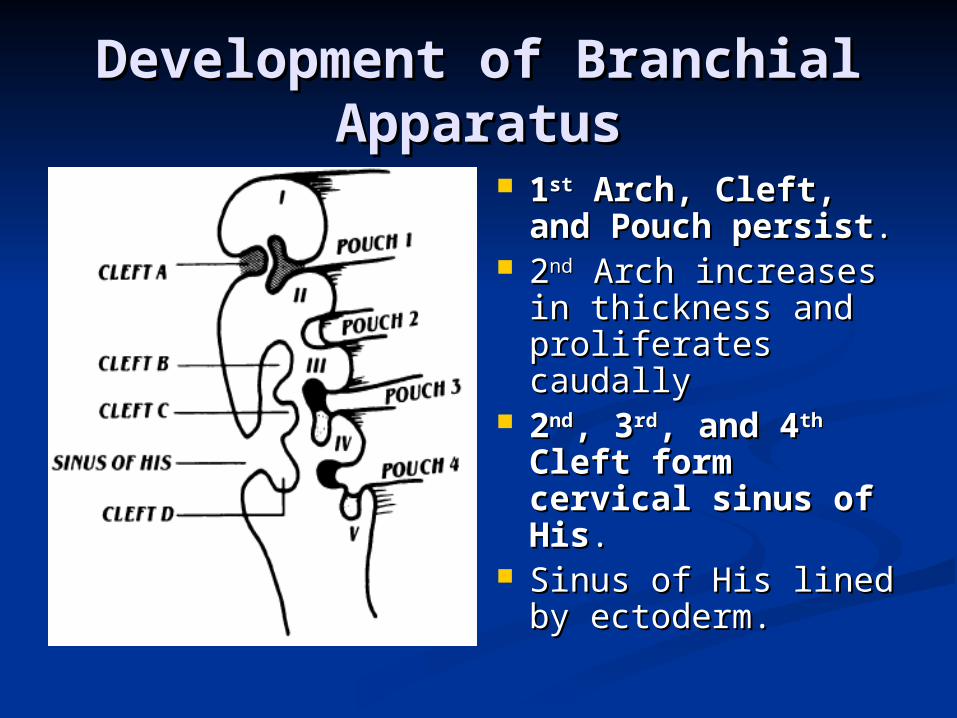
11stst Arch, Cleft, and Arch, Cleft, and Pouch persistPouch persist..
22ndnd Arch increases in Arch increases in thickness and thickness and proliferates caudallyproliferates caudally
22ndnd, 3, 3rdrd, and 4, and 4thth Cleft form cervical Cleft form cervical sinus of Hissinus of His. .
Sinus of His lined by Sinus of His lined by ectoderm.ectoderm.
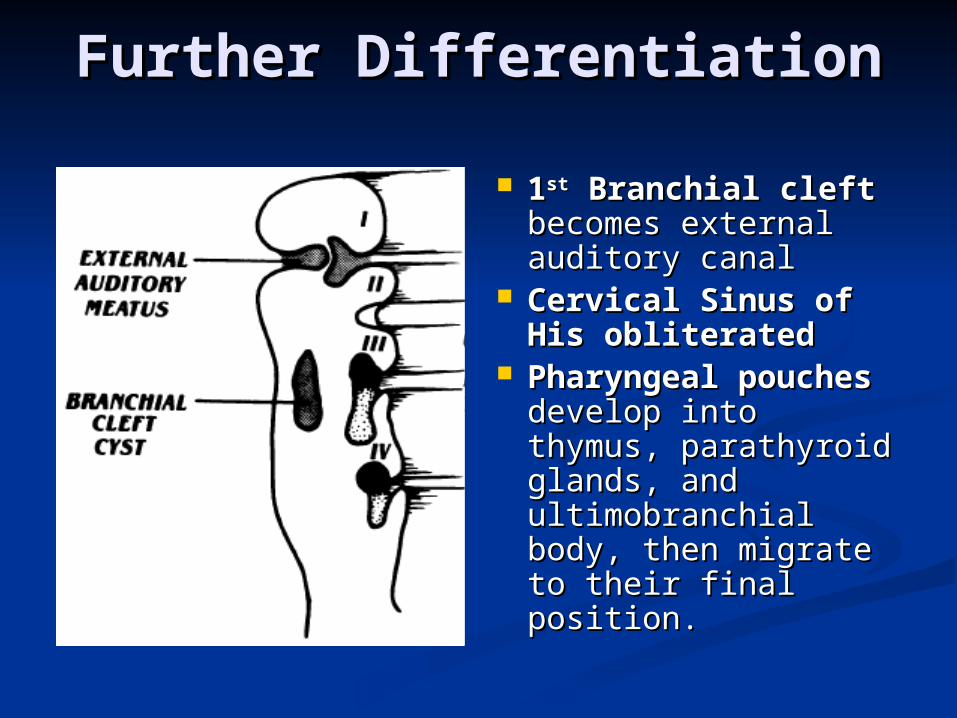
Further DifferentiationFurther Differentiation 11stst Branchial cleft Branchial cleft
becomes external becomes external auditory canalauditory canal
Cervical Sinus of Cervical Sinus of His obliteratedHis obliterated
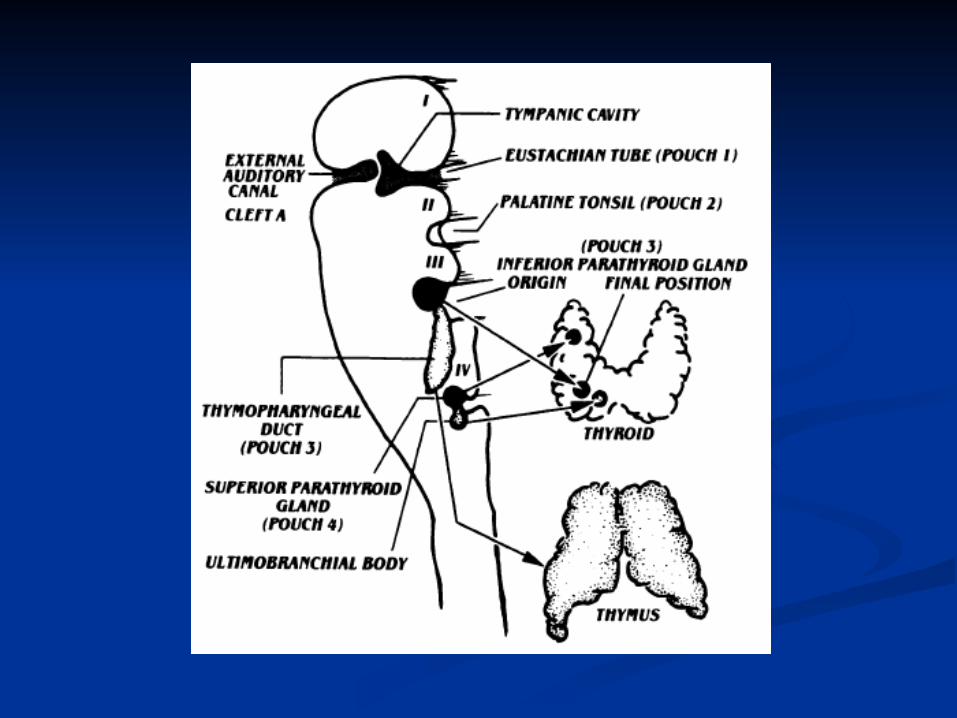
Pharyngeal Pharyngeal pouchespouches develop develop into thymus, into thymus, parathyroid glands, parathyroid glands, and ultimobranchial and ultimobranchial body, then migrate to body, then migrate to their final position.their final position.
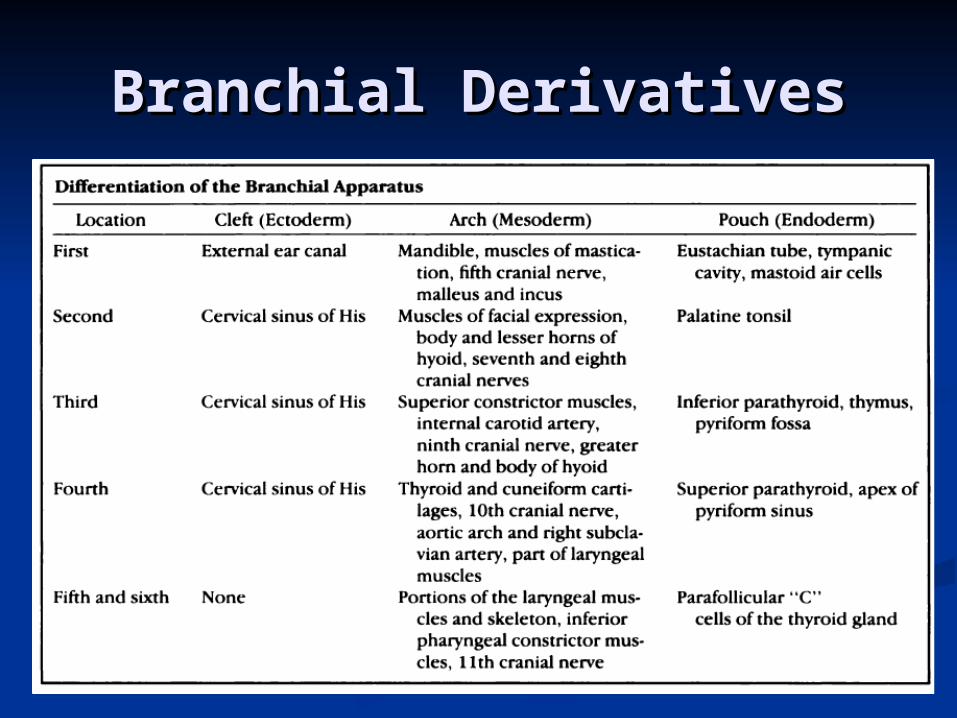
Branchial DerivativesBranchial Derivatives
EmbryogenesisEmbryogenesis
Vestigial remnantsVestigial remnants – resulting – resulting from incomplete or failed from incomplete or failed obliteration of branchial apparatus.obliteration of branchial apparatus.
Buried cell restsBuried cell rests – cells are – cells are trapped in branchial apparatus and trapped in branchial apparatus and form branchial cleft cysts later in form branchial cleft cysts later in life.life.

Branchial AnomaliesBranchial Anomalies
SinusSinus – incomplete – incomplete tract, opens externallytract, opens externally
FistulaFistula – – communicated both communicated both externally and internally externally and internally from persistence of both from persistence of both cleft and pouch.cleft and pouch.
CystCyst – no internal or – no internal or external comunication.external comunication.
Radiographic Evaluation Begins with Ultrasound
Non ionizing, non invasive. Determines cystic vs. solid; size, and extent. Color doppler – vascularity.
CT Morphologic characterization and staging. Bone structures, calcifications, deep soft tissue
anatomy Low dose neck CT to avoid excess radiation.
MRI Multiplanar capability Absence of ionizing radiation. Superior contrast resolution and anatomic
characterization of soft tissues. Often requires sedation.
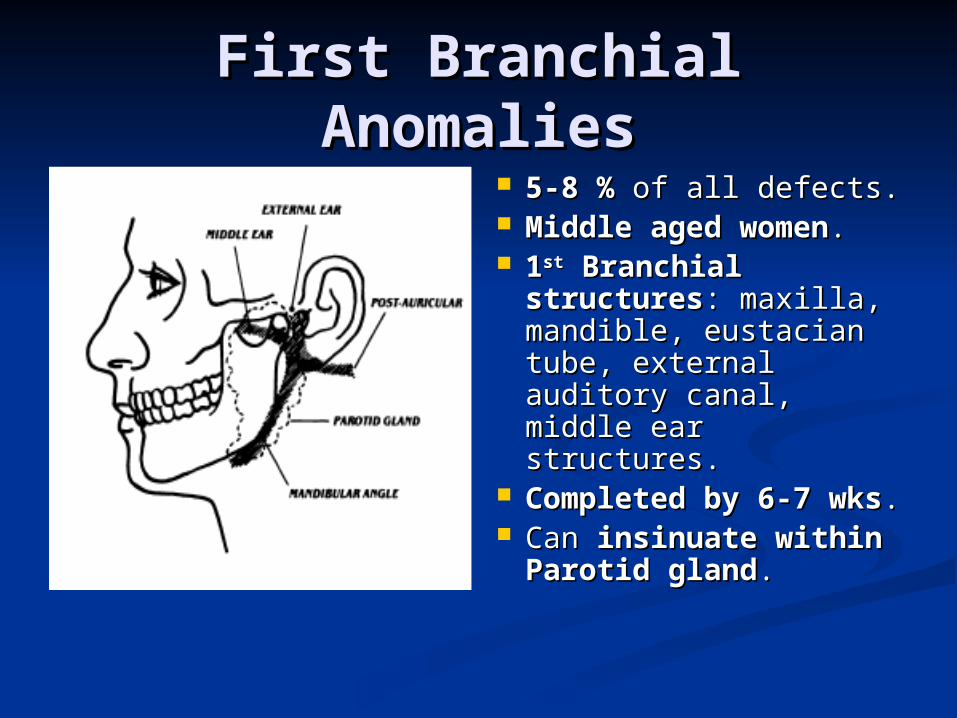
First Branchial First Branchial AnomaliesAnomalies
5-8 %5-8 % of all defects. of all defects. Middle aged womenMiddle aged women.. 11stst Branchial Branchial
structuresstructures: maxilla, : maxilla, mandible, eustacian mandible, eustacian tube, external auditory tube, external auditory canal, middle ear canal, middle ear structures.structures.
Completed by 6-7 Completed by 6-7 wkswks..
Can Can insinuate within insinuate within Parotid glandParotid gland..
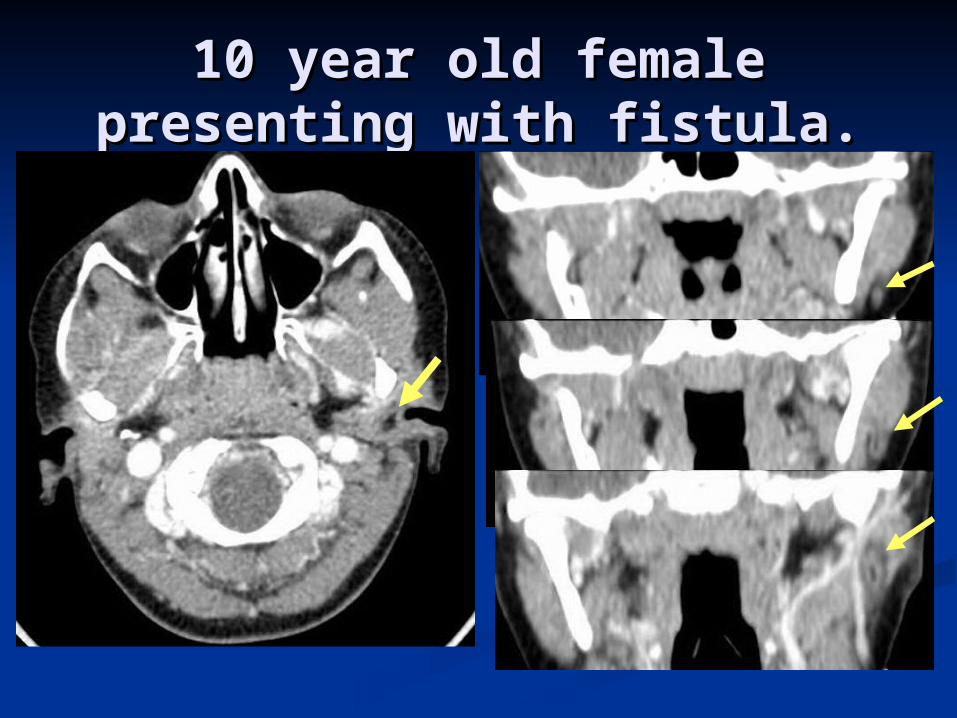
10 year old female 10 year old female presenting with fistula.presenting with fistula.
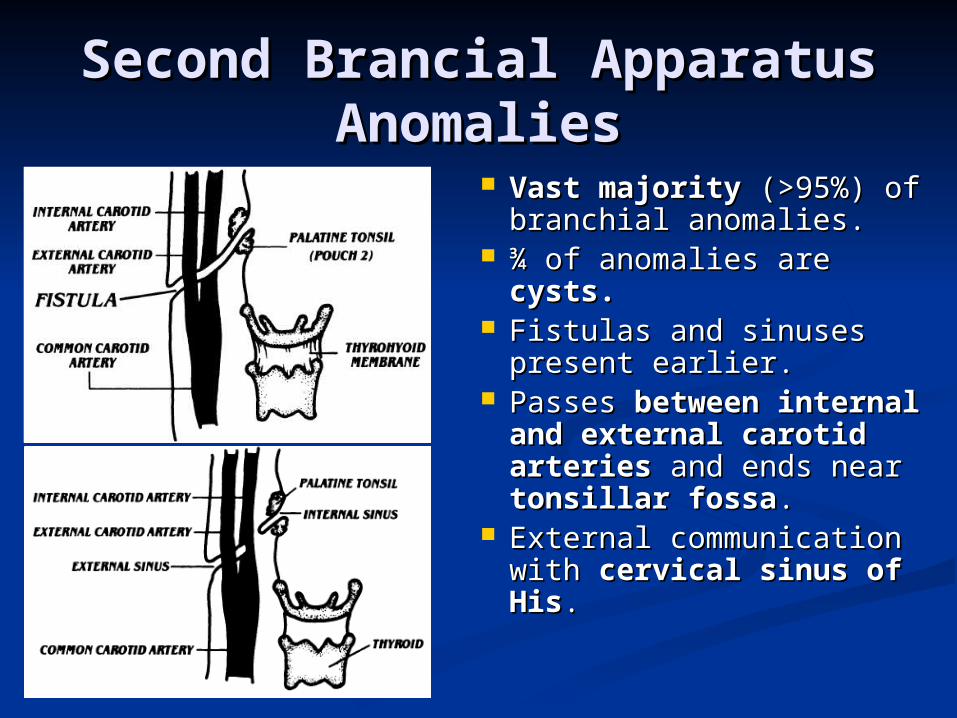
Second Brancial Apparatus Second Brancial Apparatus AnomaliesAnomalies
Vast majorityVast majority (>95%) (>95%) of branchial anomalies.of branchial anomalies.
¾ of anomalies are ¾ of anomalies are cysts.cysts.
Fistulas and sinuses Fistulas and sinuses present earlier.present earlier.
Passes Passes between between internal and external internal and external carotid arteriescarotid arteries and and ends near ends near tonsillar tonsillar fossafossa..
External communication External communication with with cervical sinus of cervical sinus of HisHis..
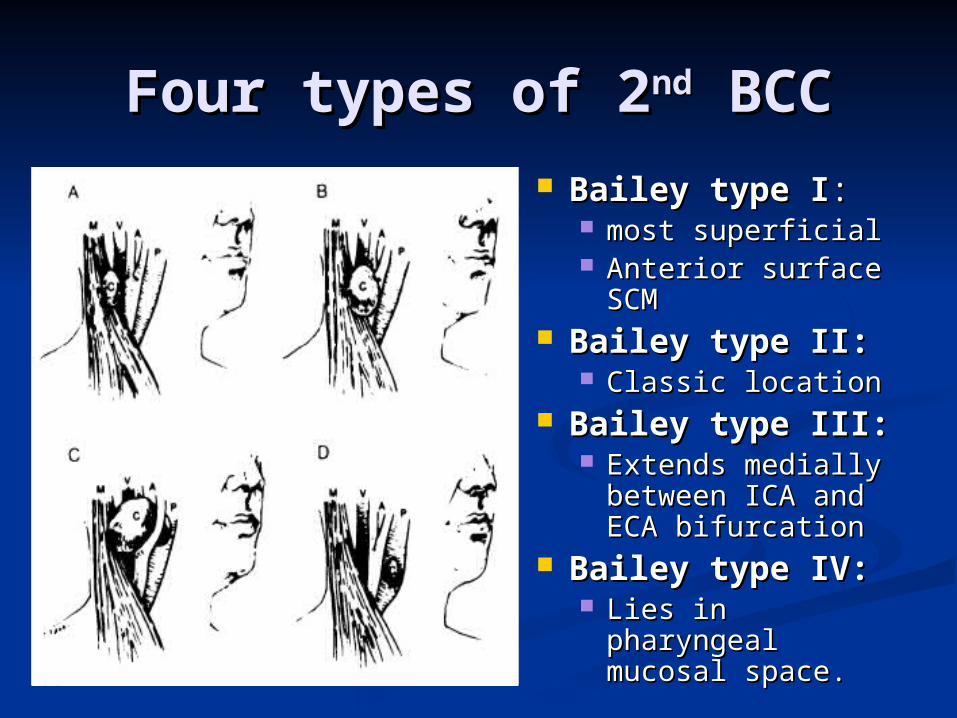
Four types of 2Four types of 2ndnd BCC BCC Bailey type IBailey type I: :
most superficialmost superficial Anterior surface Anterior surface
SCMSCM Bailey type II:Bailey type II:
Classic locationClassic location Bailey type III:Bailey type III:
Extends medially Extends medially between ICA and between ICA and ECA bifurcationECA bifurcation
Bailey type IV:Bailey type IV: Lies in pharyngeal Lies in pharyngeal
mucosal space.mucosal space.
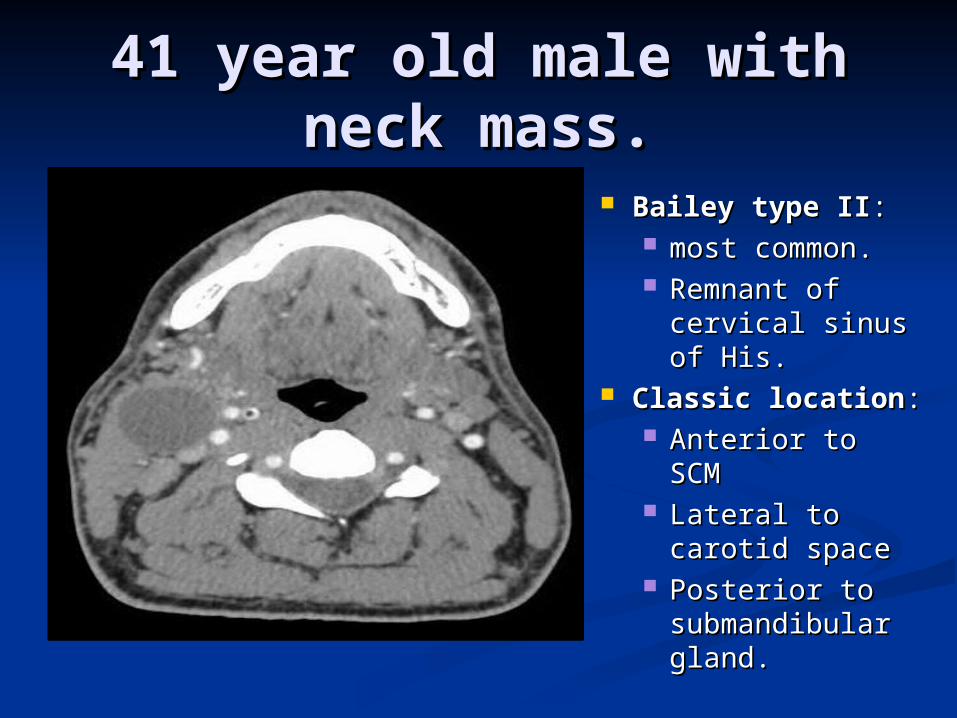
41 year old male with 41 year old male with neck mass.neck mass.
Bailey type IIBailey type II: : most common.most common. Remnant of Remnant of
cervical sinus of cervical sinus of His.His.
Classic locationClassic location:: Anterior to SCMAnterior to SCM Lateral to Lateral to
carotid spacecarotid space Posterior to Posterior to
submandibular submandibular gland.gland.
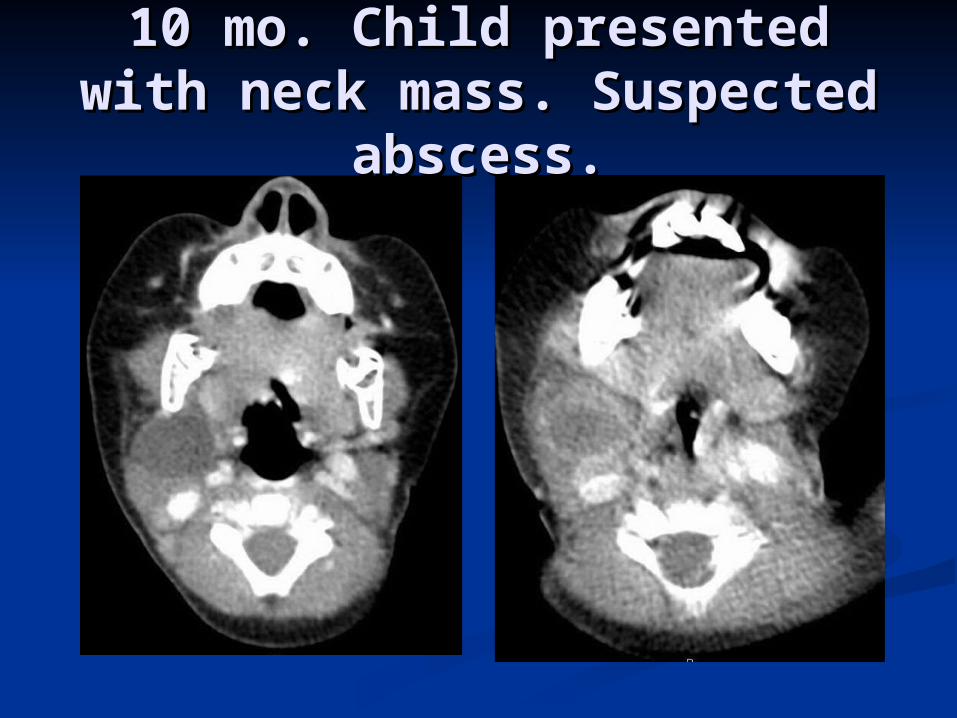
10 mo. Child presented 10 mo. Child presented with neck mass. Suspected with neck mass. Suspected
abscess.abscess.
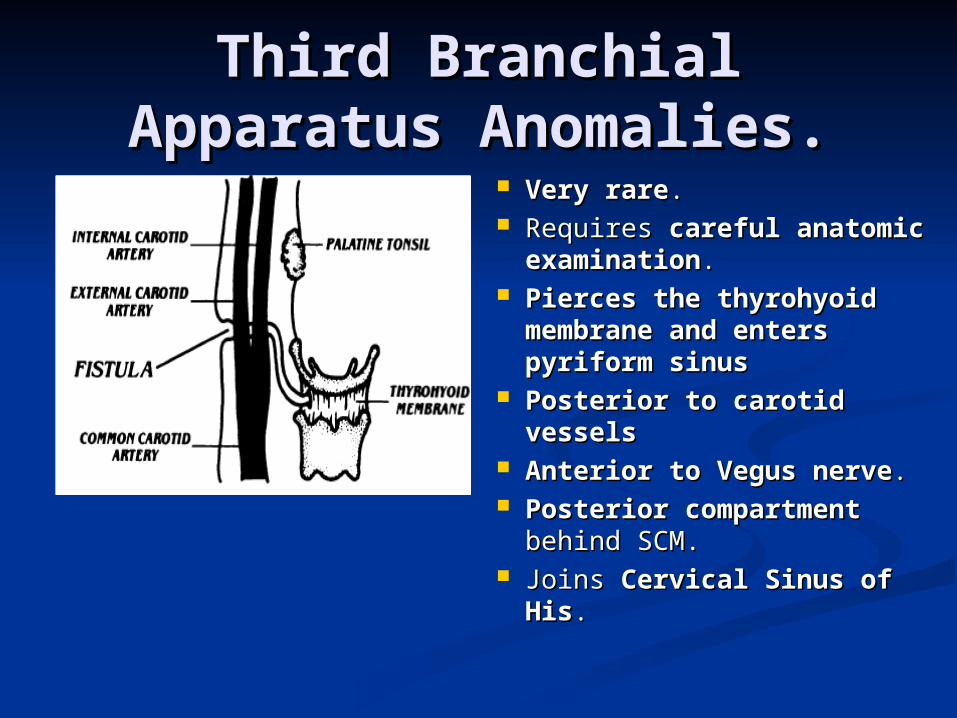
Third Branchial Third Branchial Apparatus Anomalies.Apparatus Anomalies.
Very rareVery rare.. Requires Requires careful careful
anatomic examinationanatomic examination.. Pierces the thyrohyoid Pierces the thyrohyoid
membrane and enters membrane and enters pyriform sinus pyriform sinus
Posterior to carotid Posterior to carotid vesselsvessels
Anterior to Vegus nerveAnterior to Vegus nerve.. Posterior compartmentPosterior compartment
behind SCM. behind SCM. Joins Joins Cervical Sinus of Cervical Sinus of
HisHis..
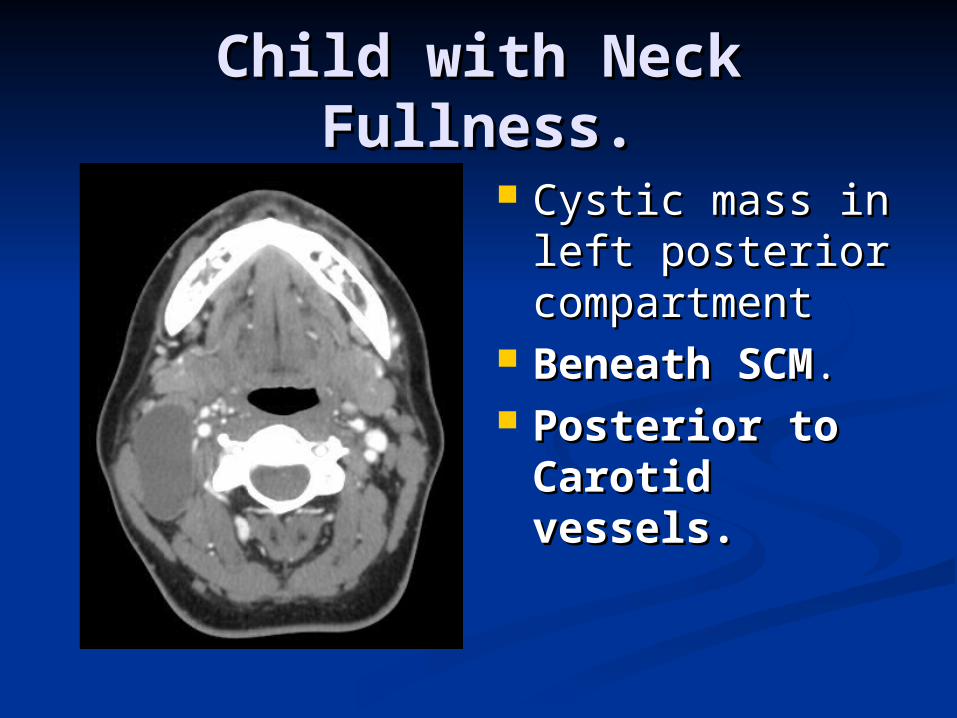
Child with Neck Fullness.Child with Neck Fullness.
Cystic mass in Cystic mass in left posterior left posterior compartmentcompartment
Beneath SCMBeneath SCM.. Posterior to Posterior to
Carotid Carotid vessels.vessels.
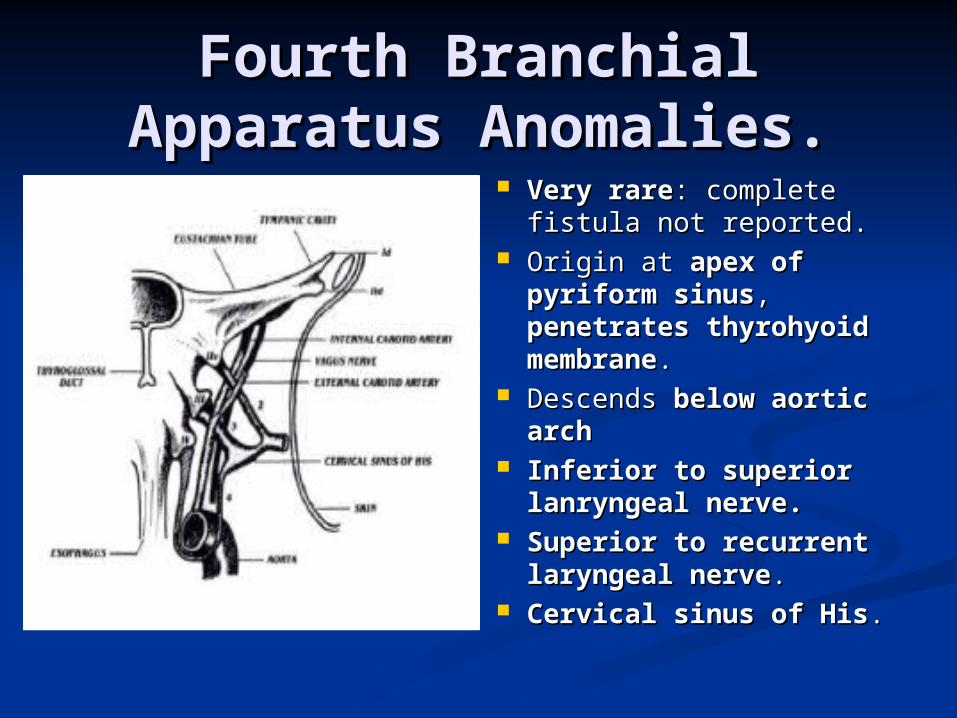
Fourth Branchial Fourth Branchial Apparatus Anomalies.Apparatus Anomalies.
Very rareVery rare: complete : complete fistula not reported.fistula not reported.
Origin at Origin at apex of apex of pyriform sinuspyriform sinus, , penetrates thyrohyoid penetrates thyrohyoid membranemembrane. .
Descends Descends below aortic below aortic archarch
Inferior to superior Inferior to superior lanryngeal nerve.lanryngeal nerve.
Superior to recurrent Superior to recurrent laryngeal nervelaryngeal nerve..
Cervical sinus of HisCervical sinus of His..
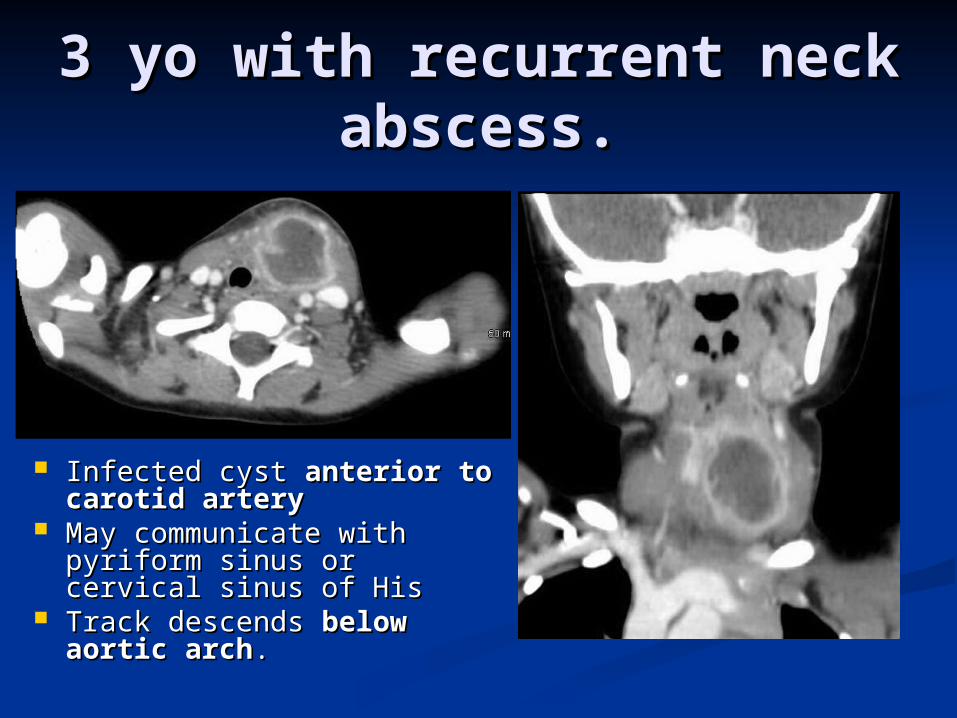
3 yo with recurrent neck 3 yo with recurrent neck abscess.abscess.
Infected cyst Infected cyst anterior to anterior to carotid artery carotid artery
May communicate with May communicate with pyriform sinus or cervical pyriform sinus or cervical sinus of Hissinus of His
Track descends Track descends below below aortic archaortic arch..
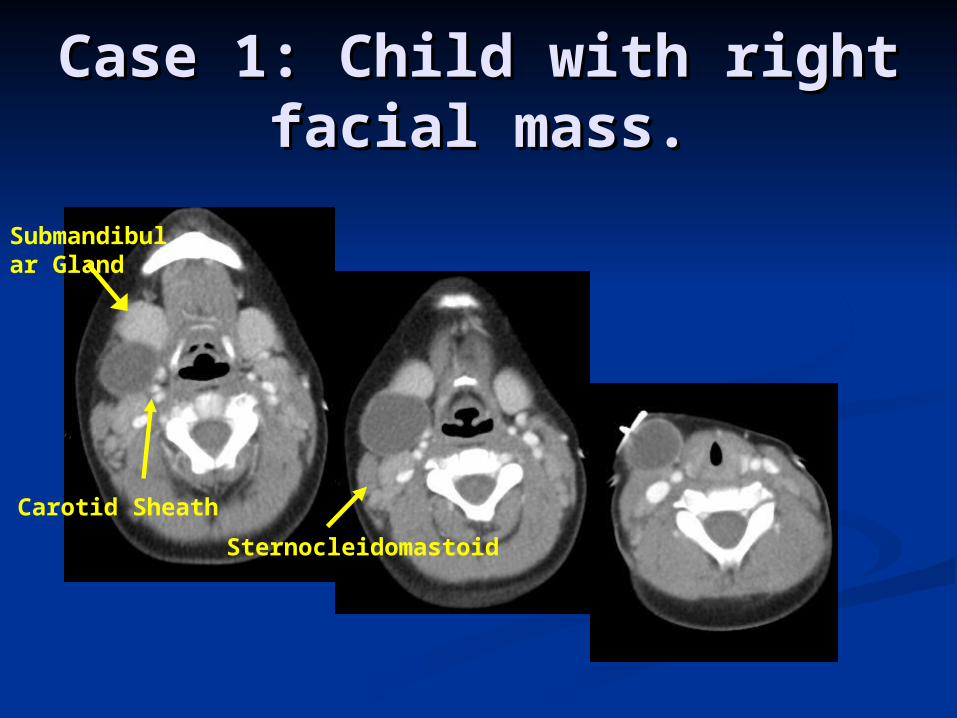
Case 1: Child with right Case 1: Child with right facial mass.facial mass.
Submandibular Gland
Carotid Sheath
Sternocleidomastoid
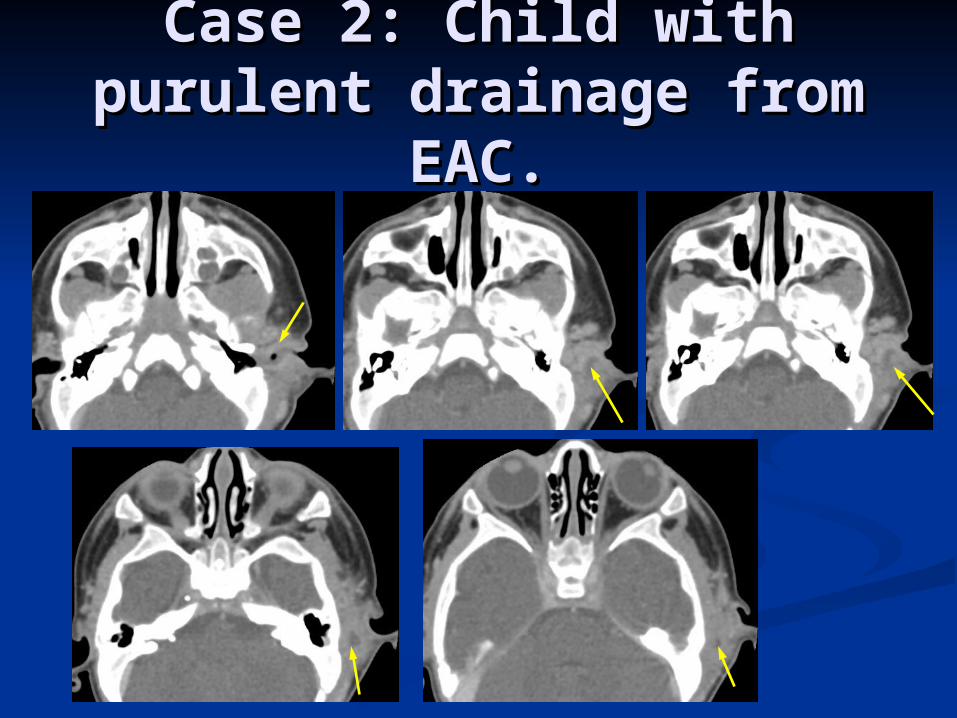
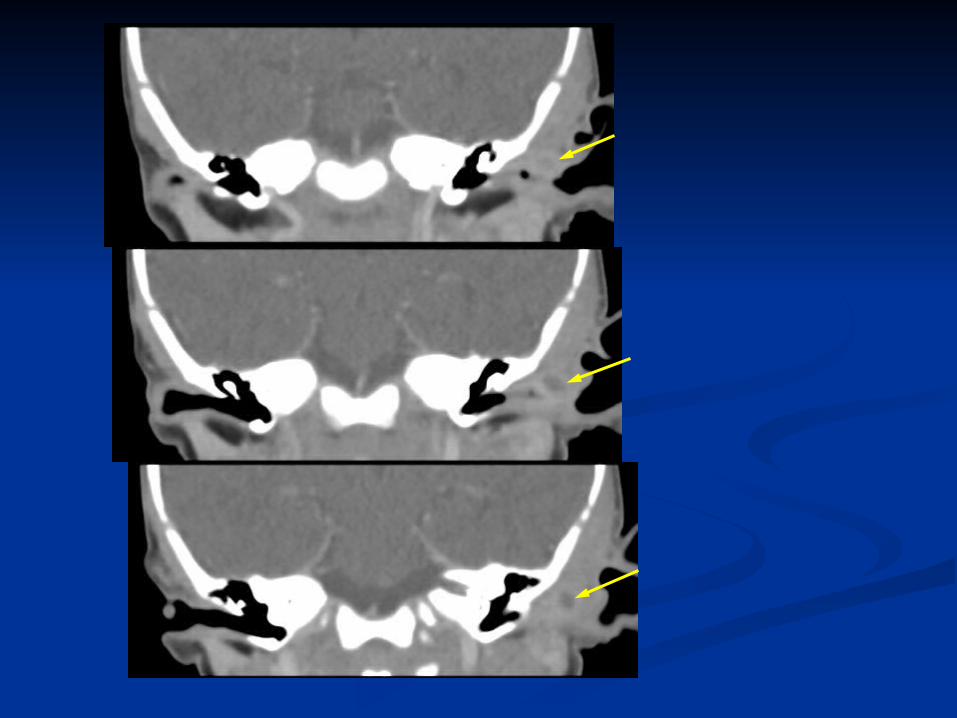
Case 2: Child with Case 2: Child with purulent drainage from purulent drainage from
EAC.EAC.
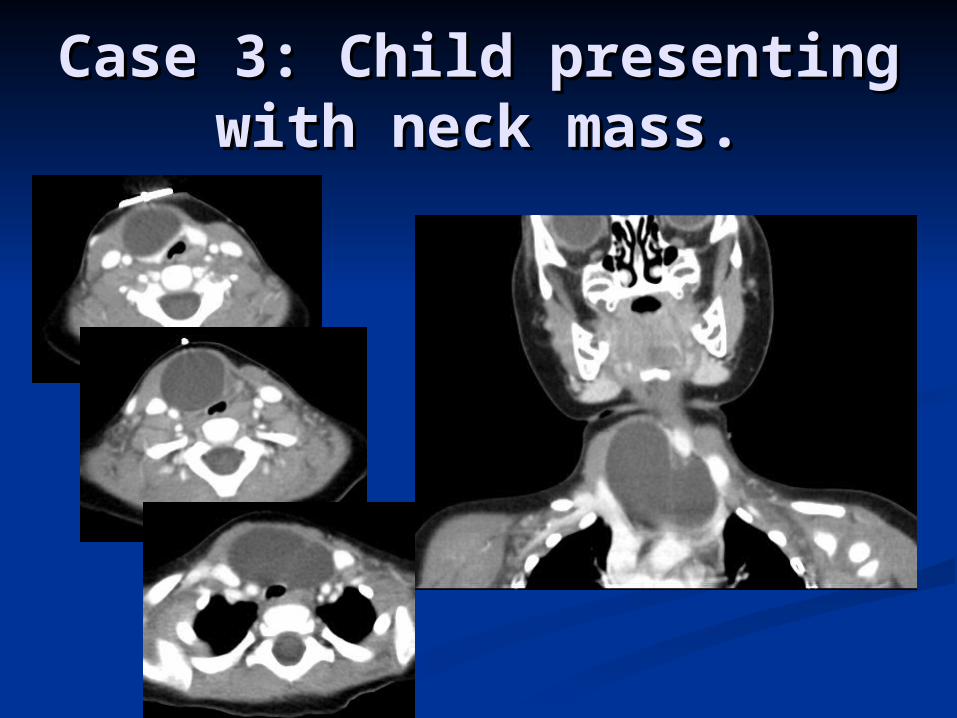
Case 3: Child presenting Case 3: Child presenting with neck mass.with neck mass.

Review
Defects in branchial apparatus include branchial, thymic, and parathyroid anomalies.
Manifest as cysts, sinuses, fistulas, and ectopic glands.
Embryogenesis: vestigial remnants from incomplete obliteration or buried cell rests.
Radiography, US, CT, MRI used for evaluation

Review Branchial Cleft Anomalies: Fistulae, cysts,
sinuses. Four types: Type II Branchial Cleft Cysts
most common. Classic location BCC II: anterio-medial to
SCM, displacing submandibular glands anteriorly, lateral to carotid vessels.
Types II – IV merge externally as Cervical sinus of His.
Types III and IV are rare and require careful anatomic examination for differentiation.
References1. Benson MT, Dalen K, Mancuso AA, et al.: Congenital
abnormalities of the branchial apparatus: embryology and pathologic anatomy. Radiographics 12:739-748, 1992.
2. Meuwly JY, Lepori D, Theumann N, et al.: Multimodality Imaging Evaluation of the Pediatric Neck: Techniques and Spectrum of Findings. Radiographics 25:931-948, 2005.
3. Koeller K, Alamo L, Adair C, Smirniotopoulos J.: Congenital Cystic Masses of the Neck: Radiologic-Pathologic Correlation. Radiographics 19:121-146, 1999.
4. Langman J. Medical Embryology 3rd Ed. Baltimore: Williams & Wilkins, 1975; 234-236.
5. Barry H. The aortic arch derivatives in the human adult. Anat Rec 1951; 111:221-238.