physiotherapy and rehabilitation eng
TRANSCRIPT
PHYSIOTHERAPY AND REHABILITATION ENGNeurophysiological Approaches I
Lecturer H. Merve KARAAĞAÇ
E-Posta: [email protected]
gelisimedu igugelisim
mervethefztt
MOTION PATTERNS
• The specific nature of the PNF techniques and diagonal patterns were analyzed in 1951 as special combinations of movement.
• Dr. Kabat found that when topographic ordered muscle groups were stretched, they produced a movement in the diagonal direction.
• Observing functional activities and sports skills in daily life showed the same spiral and diagonal characteristics.
• PNF patterns are massive movement patterns and form the basis of each technique.
• Massive movement is a characteristic of normal motor activity.• Normally, functional motor activity consists of various combinations
of movements and varying degrees of muscle elongation and shortening contractions.
• Massive movement patterns have rotational and diagonal characteristics.
• These characteristics are suitable for the sequence and rotational characteristic of bones, joints and ligaments.
• This mode of movement is consistent with the structure of the muscle and the topographic placement of the origins and insertion.
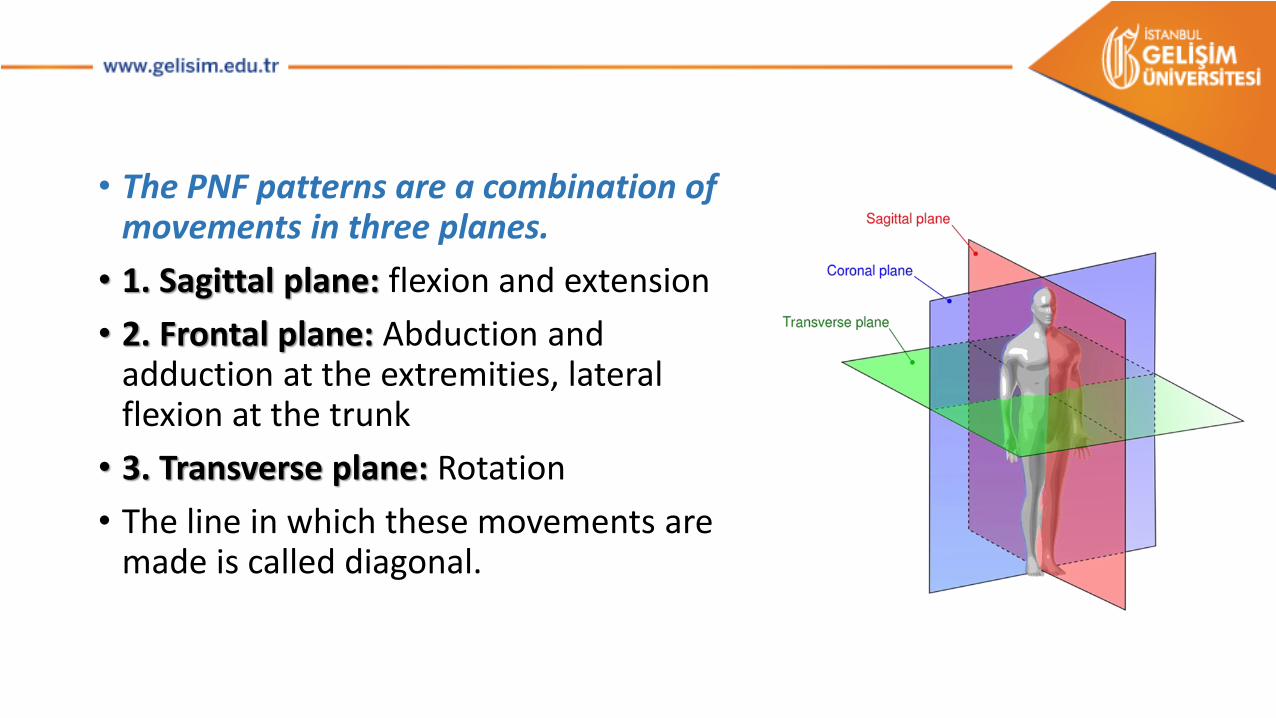
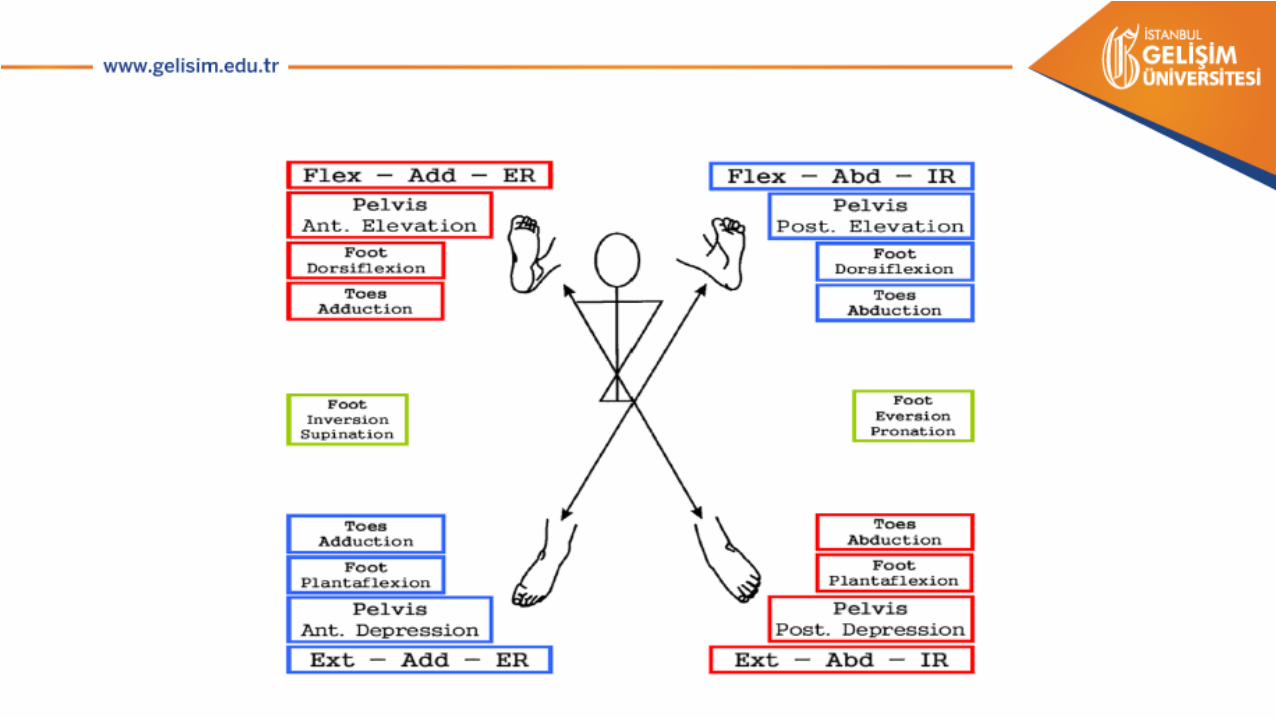
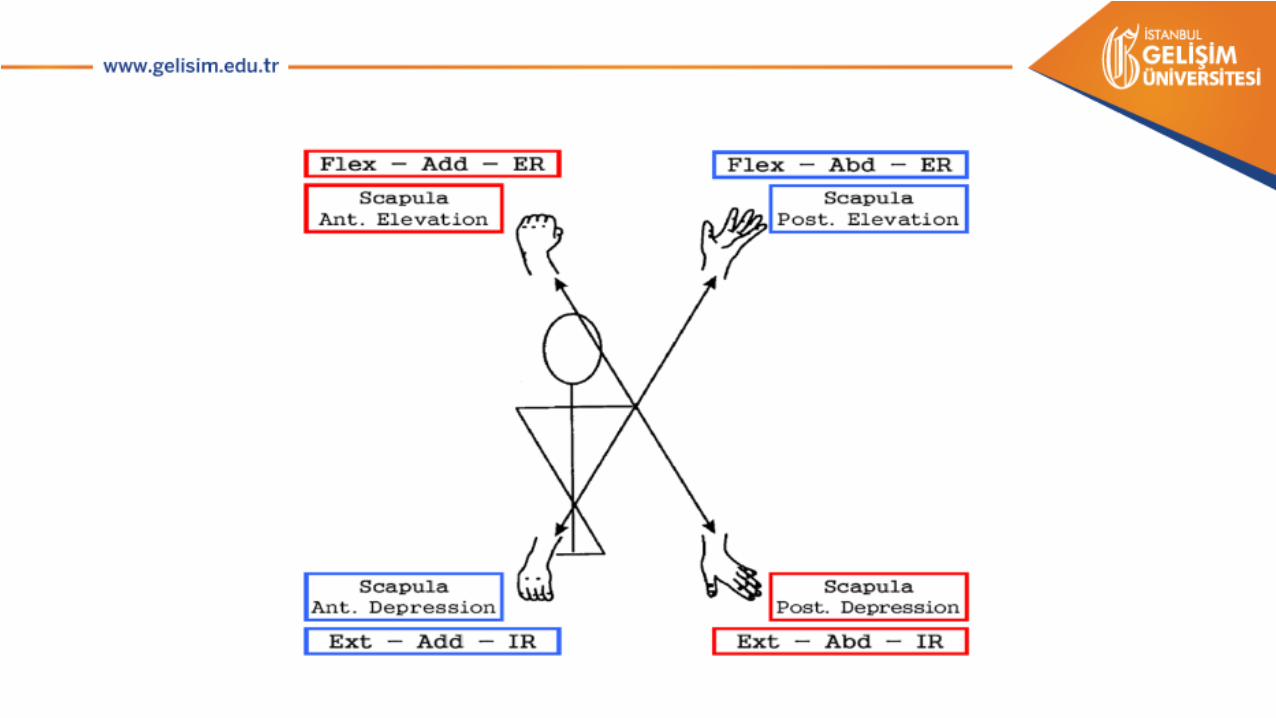
• The PNF patterns are a combination of movements in three planes.
• 1. Sagittal plane: flexion and extension
• 2. Frontal plane: Abduction and adduction at the extremities, lateral flexion at the trunk
• 3. Transverse plane: Rotation
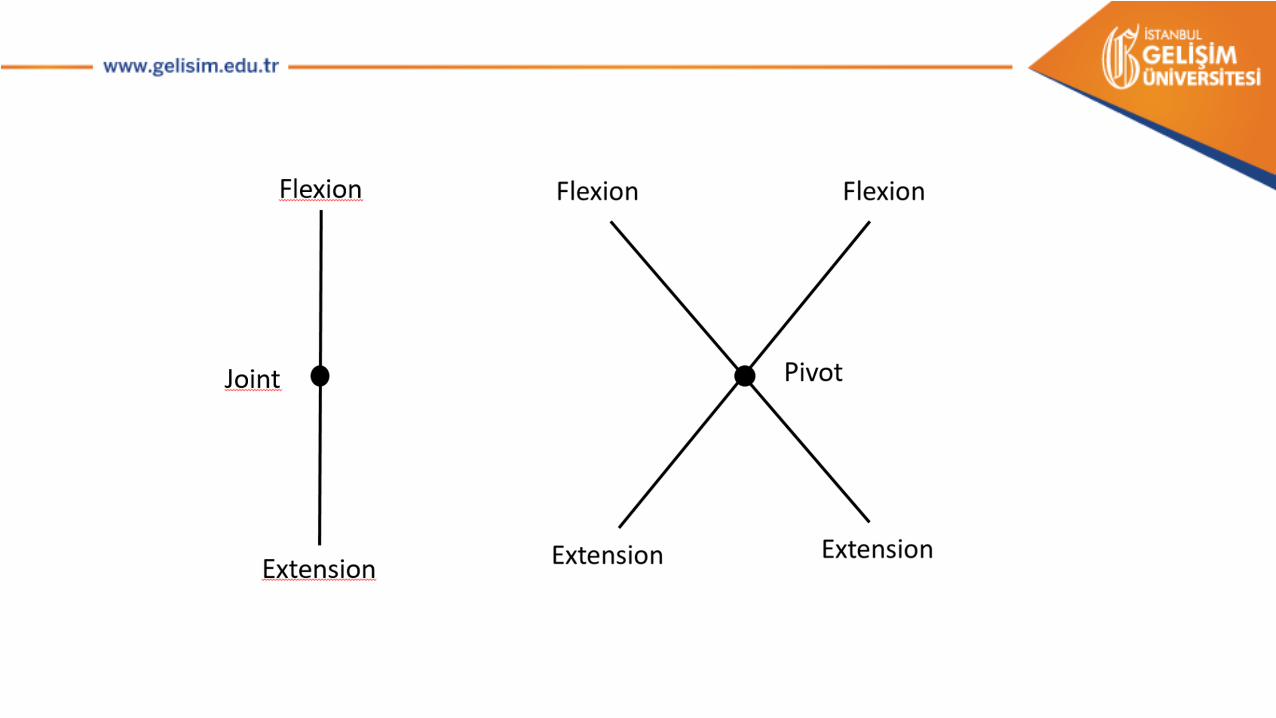
• The line in which these movements aremade is called diagonal.

• Diagonals’ characteristics are, at the beginning of the pattern the agonist muscles are in the most elongated position, the antagonist muscles are in the most shortened position and the joints are in not strained position.
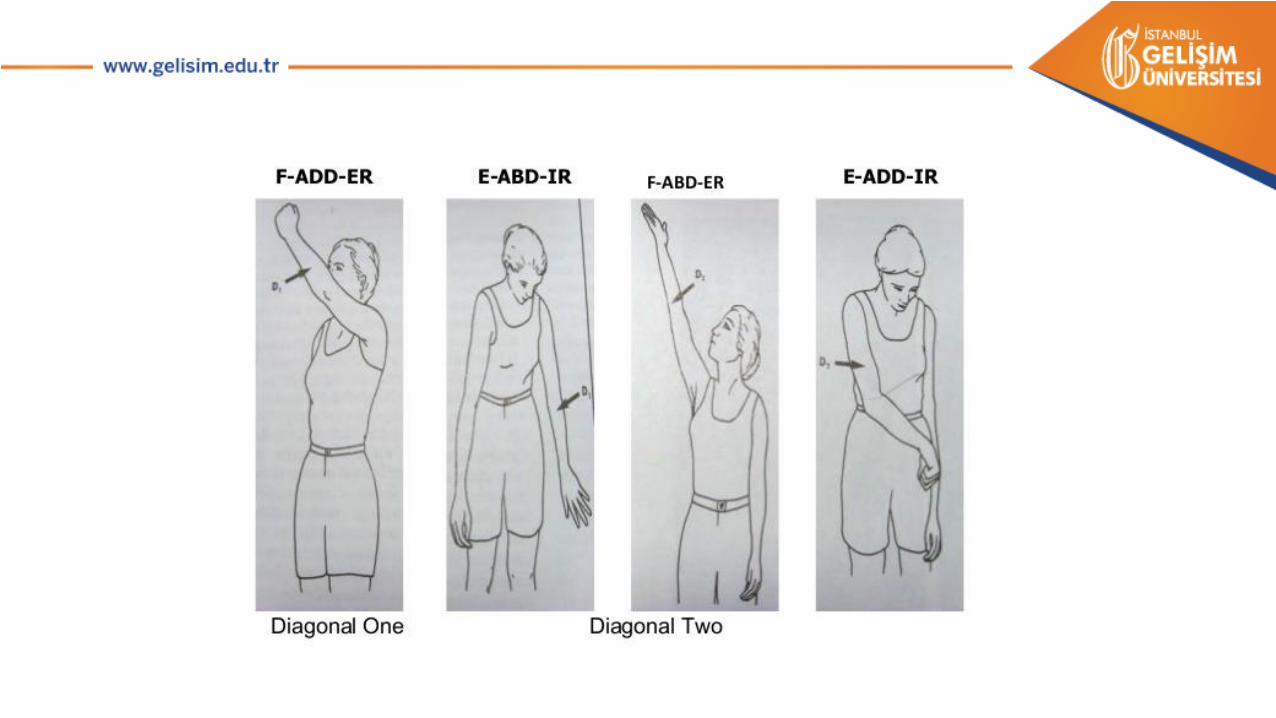
• The body is handled in four basic parts: head and neck, upper trunk, lower trunk and extremities.
• There are two motion diagonals for each part and two movement patterns which is antagonist to each other on each diagonal.
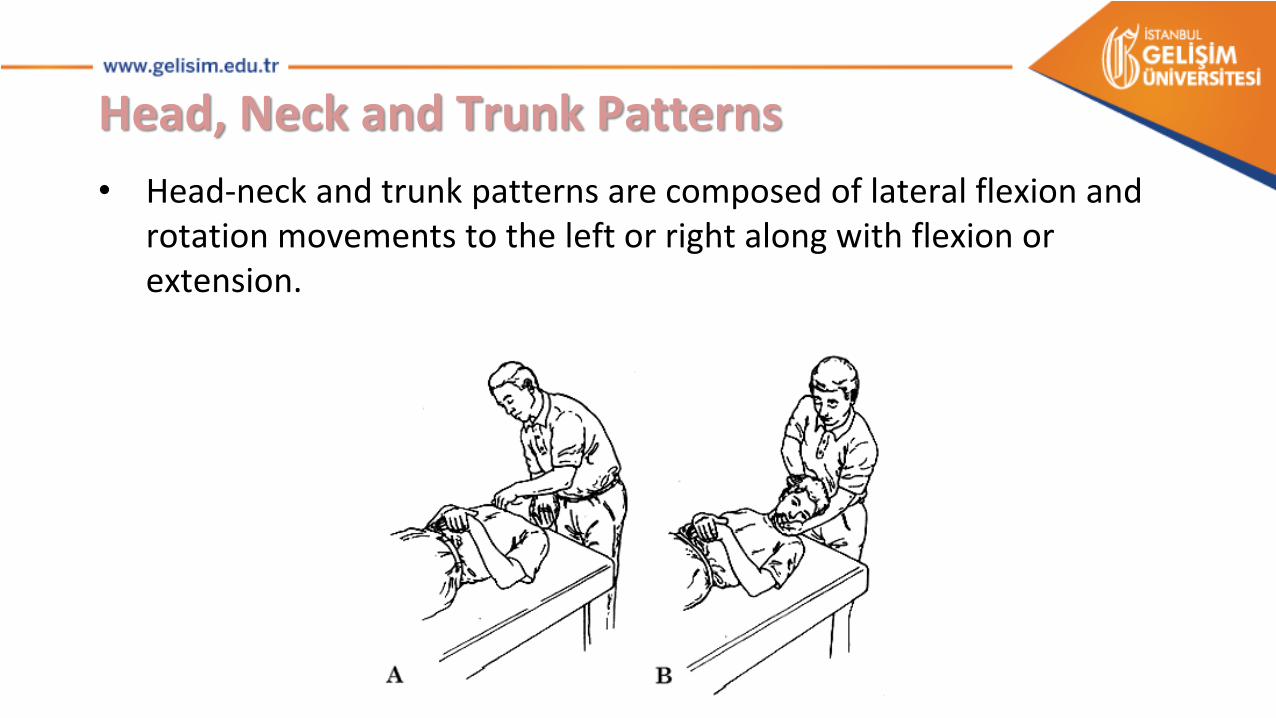
Head, Neck and Trunk Patterns
• Head-neck and trunk patterns are composed of lateral flexion and rotation movements to the left or right along with flexion or extension.
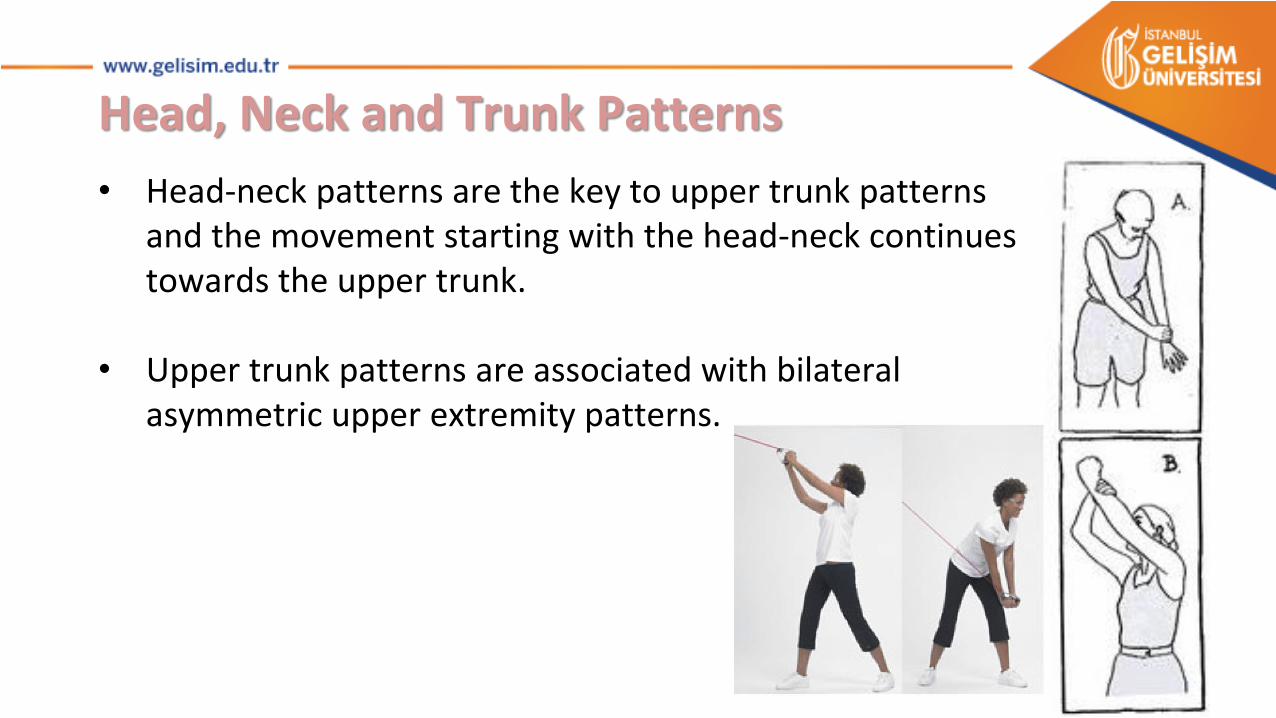
Head, Neck and Trunk Patterns
• Head-neck patterns are the key to upper trunk patterns and the movement starting with the head-neck continues towards the upper trunk.
• Upper trunk patterns are associated with bilateral asymmetric upper extremity patterns.
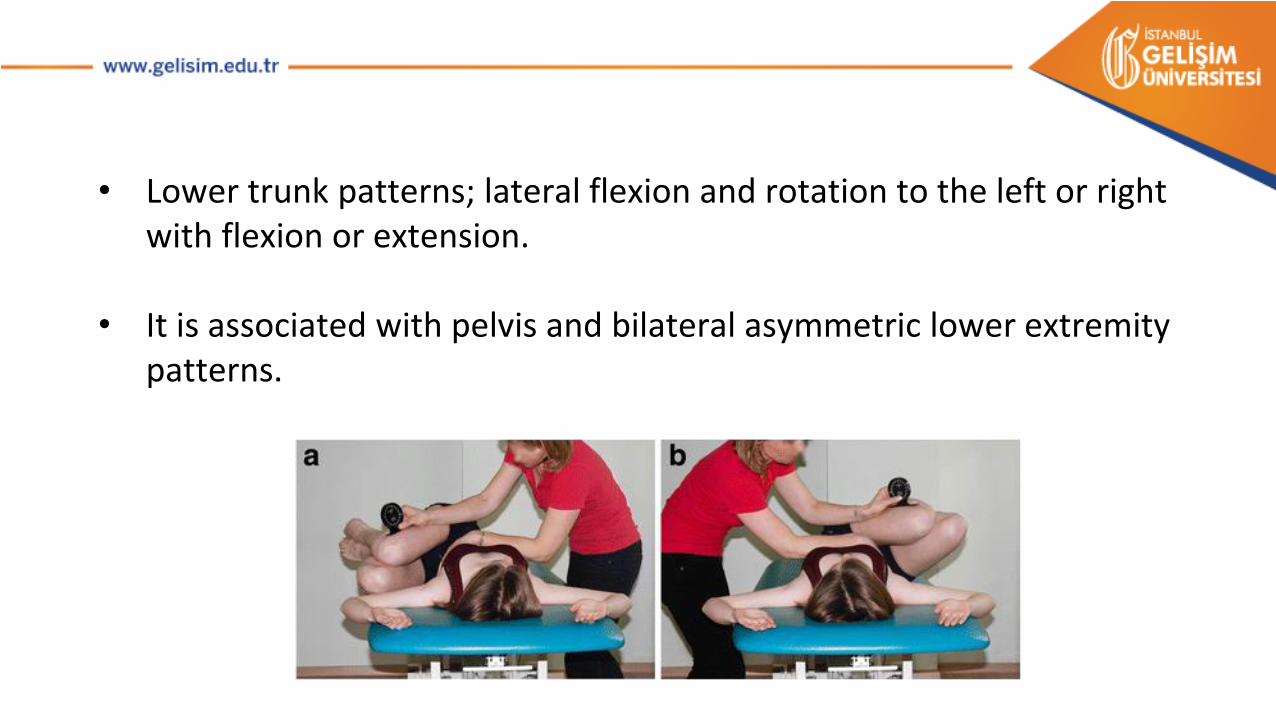
• Lower trunk patterns; lateral flexion and rotation to the left or right with flexion or extension.
• It is associated with pelvis and bilateral asymmetric lower extremity patterns.
Upper and Lower Extremity Patterns
• Extremity patterns mainly combined movements of;
• In the upper extremities; shoulder, elbow, wrist and finger joints,• In the lower extremities; hip, knee, ankle and toe joints.
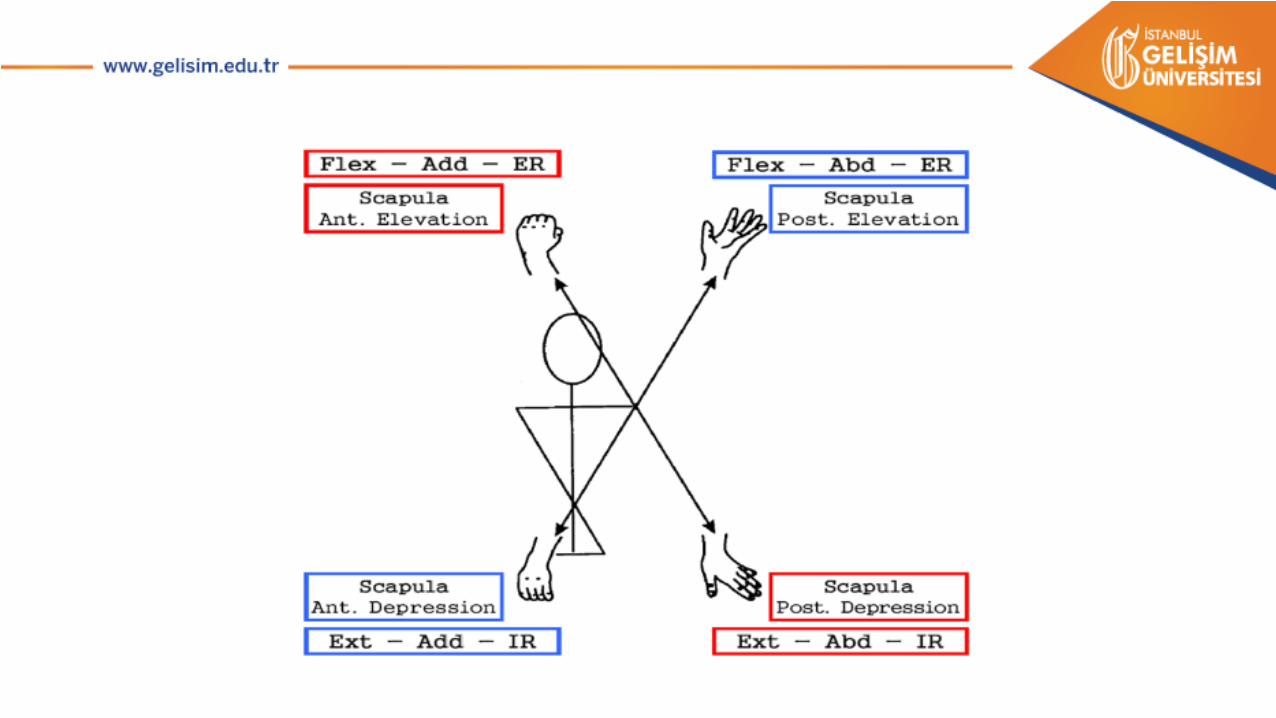
• Scapula always plays a key role in upper extremity patterns and it is accompanied by extremity patterns with diagonal and spiral movements.
• The pelvis is partially associated with the lower extremity patterns, but rather plays a role for lower trunk movements.
• Pelvis and scapula are important for development of functions and for these reasons specific patterns are defined for scapula and pelvis.
• In PNF patterns, "pivot" is used instead of "joint".
• Proximal pivots: Shoulder and hip joints are called proximal pivots and extremity patterns are named according to three basic movements occurring in these joints.
• These movement components are flexion-extension, abduction-adduction, internal-external rotation.
• There is a close relationship between these three basic movement components in the upper and lower extremities.
• For example, the upper extremity flexion is always accompanied by external rotation, and extension by internal rotation.
• In the lower extremity, abduction is always associated with internal rotation, and adduction with external rotation.
• Intermediate pivots: The elbow and knee joint are called intermediate pivots.
• Intermediate pivots may remain straight during movement or go to flexion or extension.
• Distal pivots: Distal components move with proximal pivots independent of intermediate pivots.
• In the upper extremity supination of the forearm and radial deviation of the wrist is associated with shoulder flexion and external rotation, pronation and ulnar deviation is with extension and internal rotation.
• Wrist flexion is associated with adduction, extension is with abduction.
• Inversion in the lower extremity is associated with hip adduction and external rotation, eversion is with abduction and internal rotation.
• Plantar flexion always occurs with hip extension and dorsi flexion with hip flexion.
• Digital pivots: Digital movements always move along with proximal pivots, independent of intermediate pivots.
• In the upper extremity, flexion and adduction of the fingers are associated with wrist flexion and shoulder adduction and extension and abduction of the fingers are associated with wrist extension and shoulder abduction.
• In the lower extremity, extension and abduction of the toes are associated with ankle dorsi flexion and hip flexion, flexion and adduction of the toes are associated with ankle plantar flexion and hip extension.
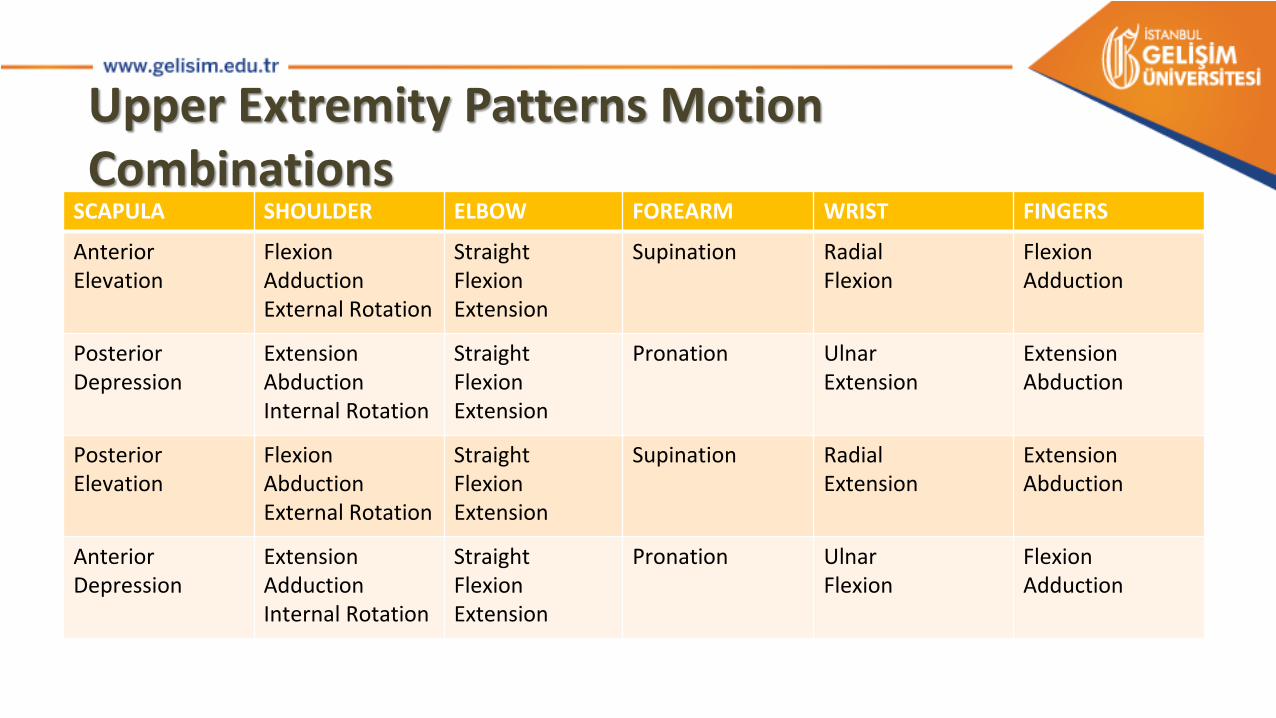
Upper Extremity Patterns Motion Combinations
SCAPULA SHOULDER ELBOW FOREARM WRIST FINGERS
AnteriorElevation
FlexionAdductionExternal Rotation
StraightFlexionExtension
Supination RadialFlexion
FlexionAdduction
PosteriorDepression
ExtensionAbductionInternal Rotation
StraightFlexionExtension
Pronation UlnarExtension
ExtensionAbduction
PosteriorElevation
FlexionAbductionExternal Rotation
StraightFlexionExtension
Supination RadialExtension
ExtensionAbduction
AnteriorDepression
ExtensionAdductionInternal Rotation
StraightFlexionExtension
Pronation UlnarFlexion
FlexionAdduction

Lower Extremity Patterns Motion CombinationsHIP KNEE ANKLE TOES
FlexionAdductionExternal Rotation
StraightFlexionExtension
Dorsi FlexionInversion
Extension
ExtensionAbductionInternal Rotation
StraightFlexionExtension
Plantar FlexionEversion
Flexion
FlexionAbductionInternal Rotation
StraightFlexionExtension
Dorsi FlexionEversion
Extension
ExtensionAdductionExternal Rotation
StraightFlexionExtension
Plantar FlexionInversion
Flexion
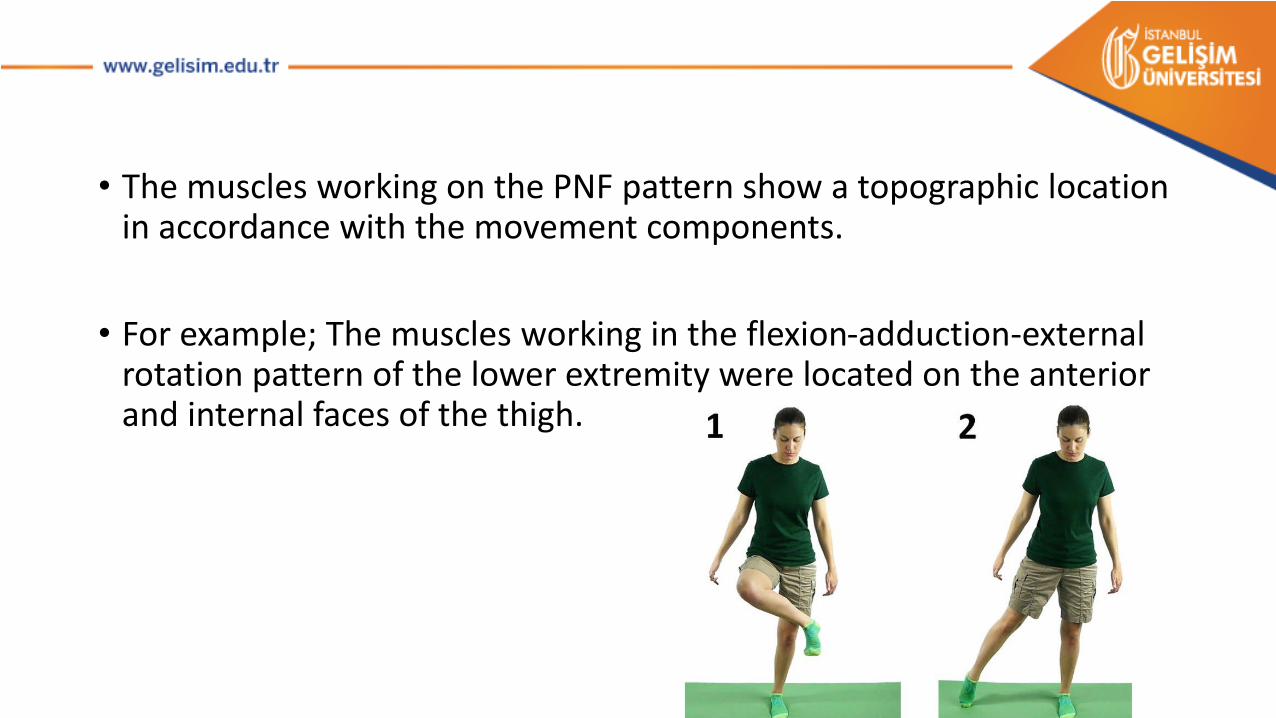
• The muscles working on the PNF pattern show a topographic location in accordance with the movement components.
• For example; The muscles working in the flexion-adduction-external rotation pattern of the lower extremity were located on the anterior and internal faces of the thigh.
• During a movement pattern, the muscles contracts starting from the most elongated position towards the most shortened position.
• The contracting muscles are called agonists and the movement is called the agonist pattern.
• The muscles located at opposite directions as diagonally, according to the agonist muscles are called antagonist muscles and they function in the antagonist pattern.
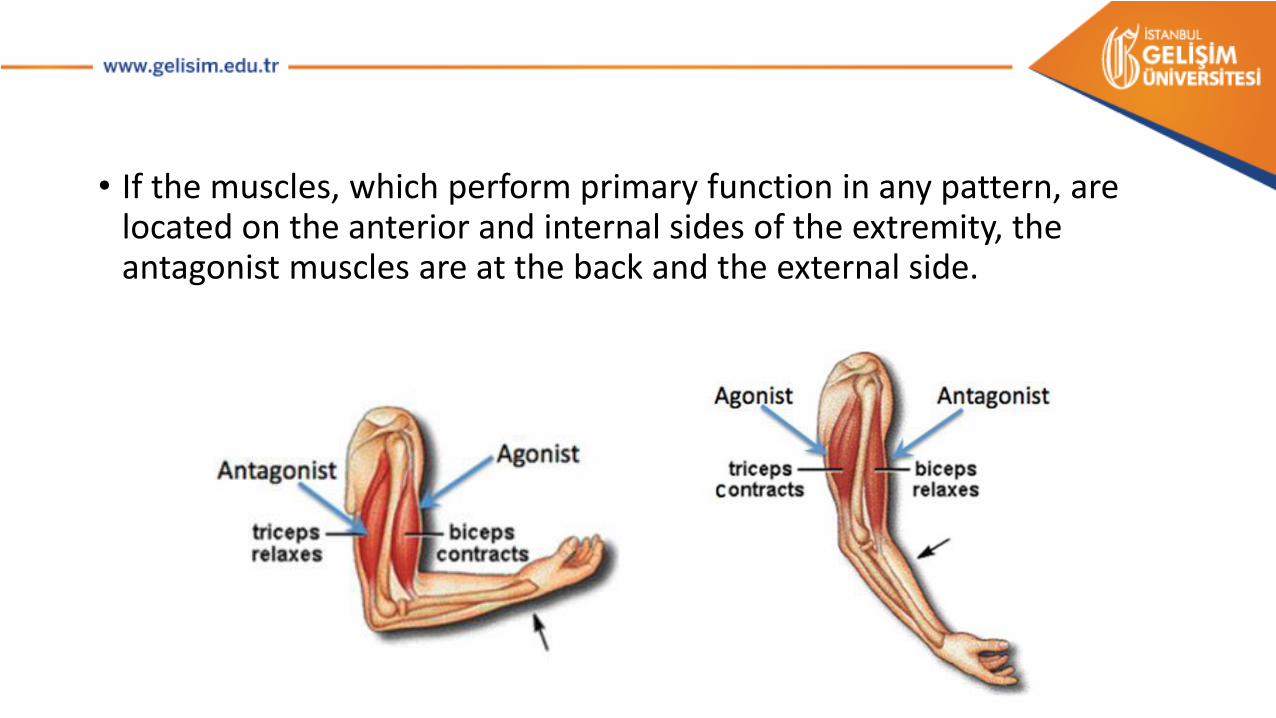
• If the muscles, which perform primary function in any pattern, are located on the anterior and internal sides of the extremity, the antagonist muscles are at the back and the external side.
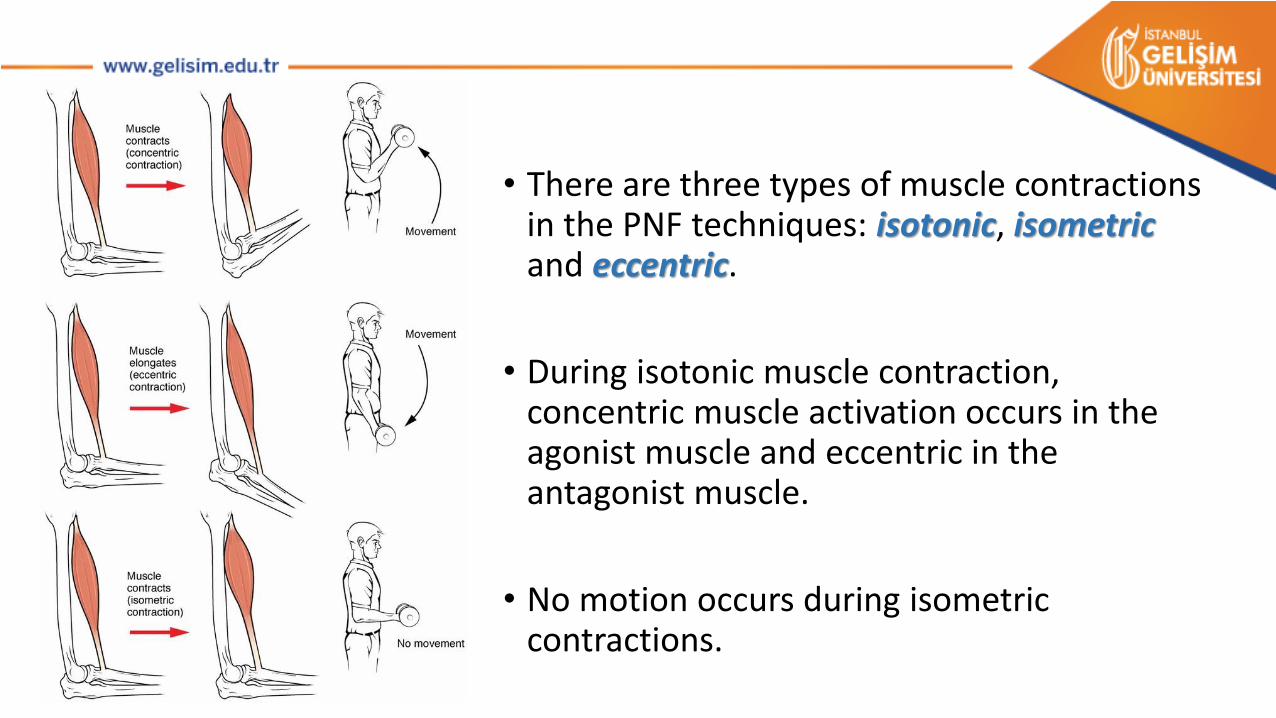
• There are three types of muscle contractionsin the PNF techniques: isotonic, isometricand eccentric.
• During isotonic muscle contraction, concentric muscle activation occurs in the agonist muscle and eccentric in the antagonist muscle.
• No motion occurs during isometric contractions.
• Stabilizing isotonic contraction describes the situation where the patient targets movement, but the physiotherapist interferes with the changing hand contacts, and a minimal isotonic contraction is seen in the relevant muscle group.
• These types of contraction can be used one by one or in combination during movement patterns.
• The facilitation patterns are used as passive, active-assisted, active or resistant depending on the indication of exercise.
• Patterns can be applied to complete the full joint movement or on a small portion of the pattern.
• The aim of the treatment is to make the patterns coordinated and in full joint motion, to ensure the balance of force in both diagonal movements.
• Extremity and trunk patterns can be applied alone or together asdifferent combinations.

These are;
• Symmetric: Both extremities make the same pattern in the same diagonal.
• Asymmetric: The extremities perform flexion or extension patterns of different diagonals at the same time.
• Symmetric Reciprocal (reciprocal at the same diagonal): The extremities simultaneously make antagonist patterns at the same diagonal.
• Asymmetric Reciprocal (Reciprocal at the opposite diagonal): The extremities of the opposite diagonals do flexion and extension patterns at the same time.
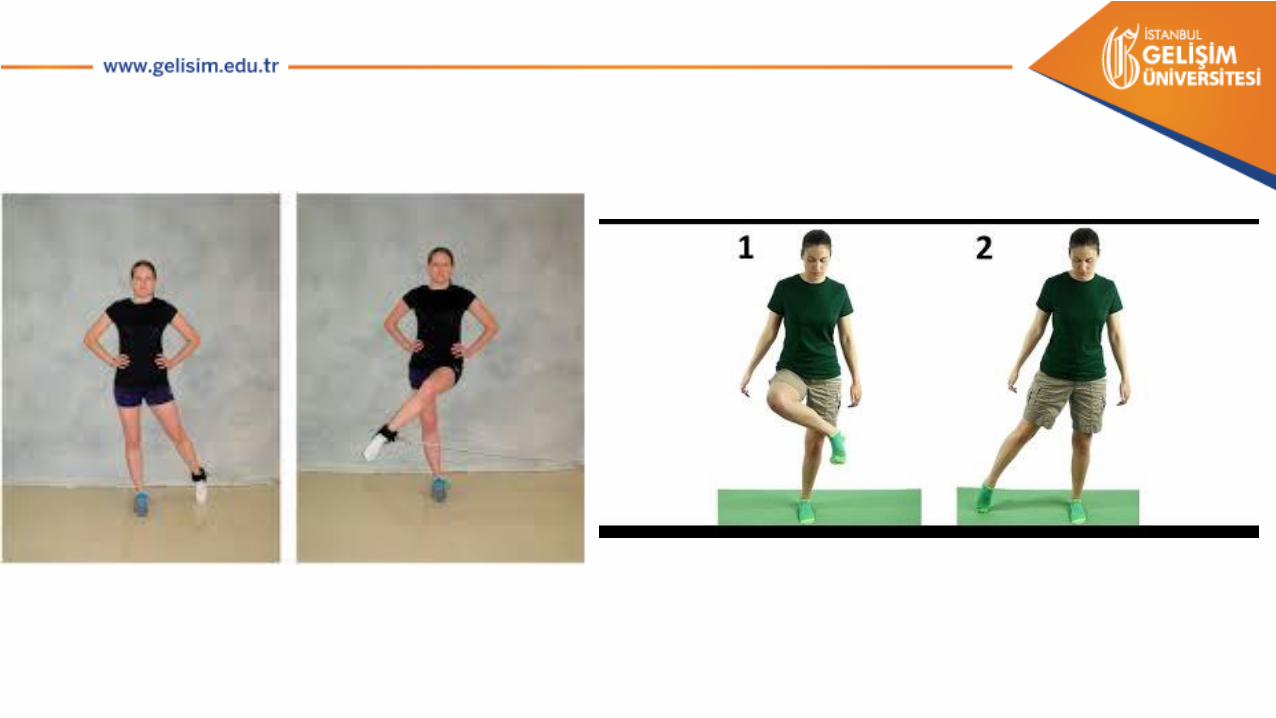
• PNF patterns can be applied in different positions to improve the desired movement and function.
• For example, for walking activity, the flexion-adduction-external rotation pattern at the lower extremity may initially be in the supine position, and then the same pattern may need to be developed at the standing position.
HAND CONTACTS
• Hand contacts create a proprioceptive stimulus for skin, muscle, tendon and joint receptors through pressure.
HAND CONTACTS
• The aims of hand contacts are;
• To give resistance
• Help to active-assisted exercises
• Give a sense of safety to the patients with pain
• To determine the direction of movement and to increase the feeling of movement
• To help increase the contraction ability of the muscle
• During pattern application, hands should be placed in such a way that they do not interfere with the completion of the movement and apply pressure to the opposite direction.
• The physiotherapist should use strong hand contact, but this contact should not cause pain in the patient.
• Since the movement pattern is in a diagonal character, the physiotherapist's position should also be diagonal and move with the patient while maintaining the hand contact.

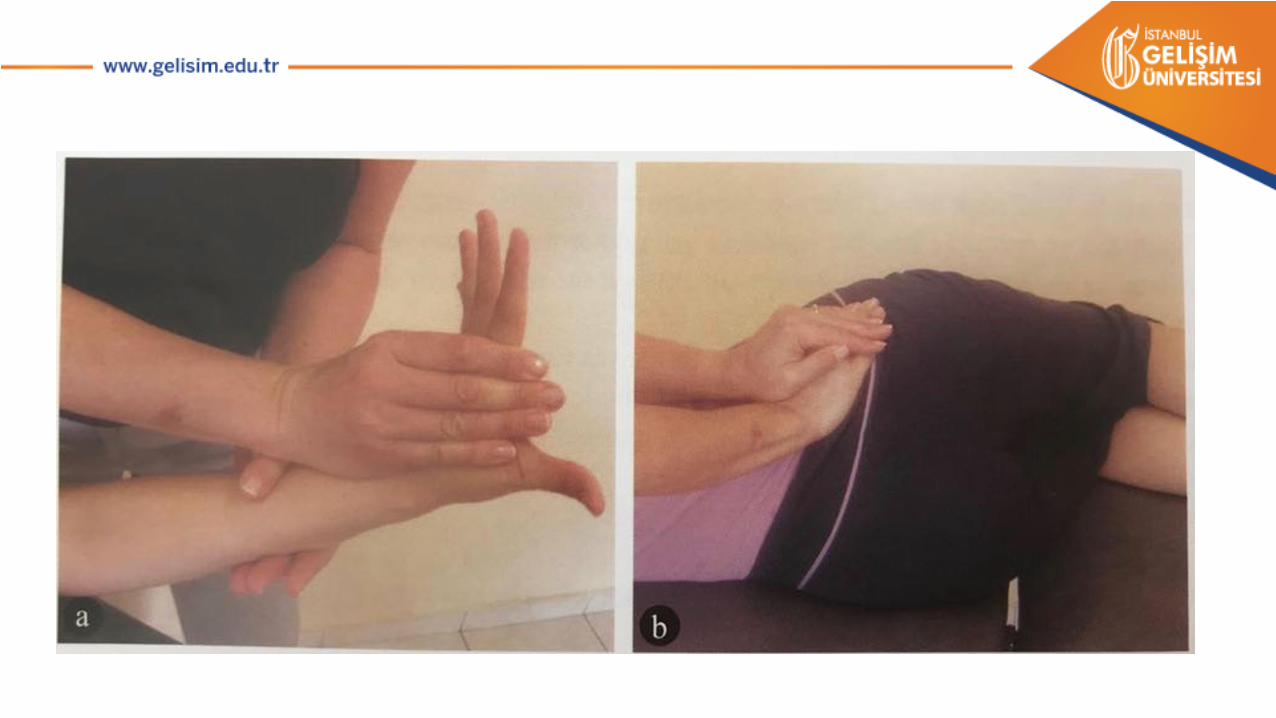
• The "lumbrical" hold and "roof" hold are used to control movement and to give resistance to rotation movements.
• Lumbrical hold is usually used in situations where the body part needs to be grasped and allows the control of the movement in three dimensions.
• In this hold, pressure is applied with the help of flexion of the metacarpophalangial joints.
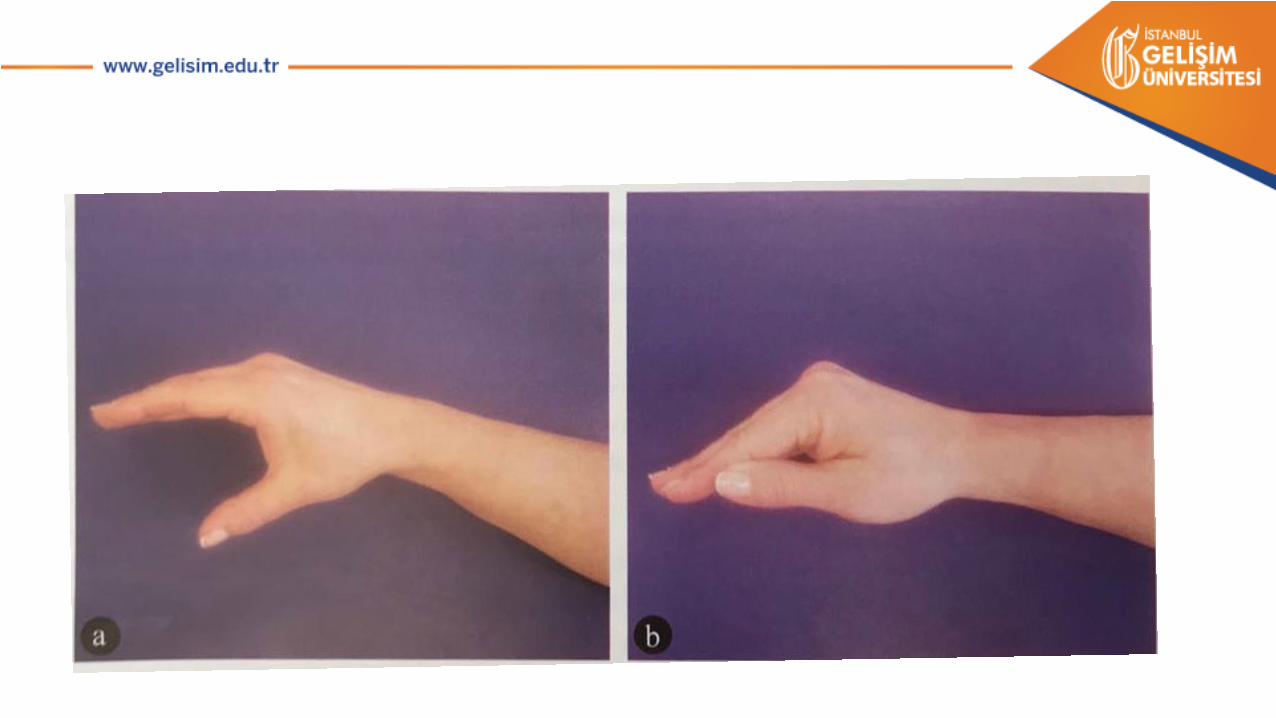
• In the "roof" hold, the thumb is adducted next to the other fingers.
• This hold is used in situations where it is necessary to apply pressure without engaging the related area.