physician referral form - toronto · please note that your initial appointment is for assessment...
TRANSCRIPT
Physician Referral Form
(For OHIP purposes ONLY medical referrals will be accepted)
Wasser Pain Management Centre J.Aount Sinai Hospital
600 University Avenue, 11th Floor Toronto, Ontario M5G 1X5
Phone: {416) 586-5997 Fax: (416) 586-8281
Instructions: Only complete referrals will be accepted (see attached referral forms). Referrals must include consult letter outlining medical history along with reports of investigations and current medications, dosage and patient intake package.
Please provide your patient the attached intake package form. This form must be completed and included with referral form prior to booking. Patient must have a family physician prepa'red to be an active participant in his/ her care and provide follow-up. If you are the family physician please sign the attached family physician form or give to the patient to obtain the appropriate signature. Additional information may be found on the website www.mtsinai.on.ca/wasser.
Requests for medicolegal purposes should be sent for an independent medical opinion.
Referring MD:______________ Billing#: ____________ ____ _ _
Address:_______________ ____ _________________ _
Phone:___ _ ____________Fax:.____________ ________ _
Email:._____________________________ ________ _
If different from above, please complete:
Farrilly NUD:_ _ ___ ______________________________________________________
Address: _______________ ______ _______________ _
-------------Fax:_________ _ ______ _______Phone: Email._______________________ _____ ________ _ ___
Patient Name: ___________________ ________________ _
HCN: _____________ _ ______:D.O.B . ______ _ _________M_F_
Address: _________ ________________ ____________
Home Phone:_____________ Work Phone:_____________ _ _ ___
Cell Phone: Alternate Contact .._:---------------------Email: ___________________________________
WSIB Yes 0 No 0 Active Claim #:
MVA Yes 0 No 0 Third Party Claim File #:
1. Pain problem:
2. Medical history:
Please include a consultation note detailing pain problem and medical history
3. list of current medications, dosage and treatments:
4. List of previous investigations and consultations into pain problem (relevant reports must be included):
Please indicate to which clinic within the Wasser Pain Management Centre you would like to direct your referral:
o Neuropathic Pain o Headache
o Pelvic Pain o Pain and Chemical Dependency
o Craniofadal Pain o General Chronic Pain Management
I acknowledge that I have read the conditions of the referral and will resume care of my patient after discharge from the Wasser Pain Management Centre.
I acknowledge that I have relayed the required referral information to my patient.
Signature Date
Please print name__________________________________________________________
Only referrals containing all of the above information will be accepted. Please complete the above information and fax along with the referral letter and relevant reports to (416) 586-8281. Thank you for your referral to the Wasser Pain Management Centre.
2
Please have this form signed by family physician.
To whom it may concern:
Your patient has been referred to the Wasser Pain Management at Mount Sinai Hospital, either by yourself or another health care practitioner. One of our admission criteria is that family physicians play an active role in the treatment of their patients. We wilJ provide assessment and a treatment plan for your patients' chronic pain problem. In some cases, treatment may be initiated by our Centre, however, once stabilized, the patient will be returned to you for ongoing care, including pharmacotherapy, with our continued support. If in agreement, please sign this form and return and fax back to our office fax: 416-586-8281. We will proceed with an appointment upon receipt. Please note that there is a waiting time of4-6 months for an initial appointment after receipt ofall documentation.
Family Physician Signature Date
Please Print Name Date
Are you willing to prescribe opioids for this patient if recommended?
YesO NoD
IfNo please provide reason.
Thank You.
3
• •
MOUNT SINAl HOSPITAl t~, Joseph and WoH Lebovic Health Complex ~ ~ Wasser Pain Management Centre
Wasser Pain Management Centre
Mount Sinai Hospital
A University of Toronto affiliated patient care, teaching and research centre
Wasser Pain Management Centre at Mount Sinai Hospital
600 University Avenue, Suite 11 60 Toronto, Ontario
MSG 1XS
Phone: (41 6) 586-5997 Fax: (416) 586-8281 Email: [email protected] Website: www.mtsinai.on.cajwasser
Welcome to the Wasser Pain Management Centre. Enclosed with this letter are torms for you to complete which will help us understand your needs.
The enclosed documentation must be completed and returned prior to the scheduling of any appointments. Please return the completed original copy of the questionnaire and keep a photocopy for your records.
Requirements Family Doctor: It is a requirement by our Centre that all patients are under the care of a family physician who is willing to participate in your ongoing pain management.
Instructions for your First Appointment After we receive all of the required documentation, your file will be reviewed and an appointment will be made for you to be examined by one of the Wasser Pain Management Centre specialists.
Please note that your initial appointment is for assessment only.
We will provide assessment and recommendations only for those who live outside of the Greater Toronto area.
It is necessary for you to bring your health card and Mount Sinai card (obtained in the admitting department on the main floor) to all of your appointments.
Bring all prescribed medication in the original bottle/blister pack to your first appointment.
Your referring physician will be notified of your initial appointment date and time.
If you have any questions about your referral please contact your referring physician.
1
______________________________________________________________________ ______________________________________________________________________ ______________________________________________________________________ ______________________________________________________________________
________________________________________________
_____________________________ _____________________________________
WASSER PAIN MANAGEMENT CENTRE MOUNT SINAI HOSPITAL
Date:
Release of Information
• I authorize Wasser Pain Management Centre at Mount Sinai Hospital (“Wasser”) to disclose all information, opinions and reports which may be requested from time to time to any insurance provider or health care practitioner involved in my care.
• I further authorize the following health care providers to provide all information, opinions and reports which may be requested from Wasser regarding my condition and treatment (List full name and address).
• I understand that any information provided may be discussed at the weekly Wasser Team meetings in order to determine the best possible treatment.
• I understand that all information collected will be held in confidential files at all times.
Telephone and Consent
• I consent to receiving detailed voicemail messages (i.e. name of person, department from which person is calling, reason for call, telephone number) from Wasser at the following telephone numbers:
Email Consent
• I wish to communicate with my care provider at the following email address: ____________________________________________________________________.
• I acknowledge and understand that these email messages are not encrypted and therefore, the Hospital cannot guarantee the security of messages that I send to or receive from my care provider.
• I agree not to use email to communicate emergency or urgent health matters.
By signing this consent, I confirm that I have read and agreed to these terms.
Name of Patient/Substitute Decision Maker Signature of Patient/Substitute Decision Maker
MOUNT SINAl HOSPITAl ,~"', joseph and Wolf Lebovic Health Complex ~ fA wasser Pain Management centre
Section A: General Information PlEASE WRITE OR PRINT CLEARLY.
Name (print): ___________________ Date: _ _________
Signature:-------------------------------
Address:--------------------------------
City:---------- Province:--------- Postal code: ________
Home phone: ( __ )_______ _ _ Work phone: ( _ _ )___________
Other: ( __ ) Email:_________________
Health card number:--- -------Version code: _ _____________
Expiry:------- - - -----Date of birth (DD/MM/YY): ( _ _ [__ J __
Mount Sinai Hospital Identifica tion number (if applicable):-------- - --------
Emergency contact person: - ---------------Relationship:-------
Home phone: ( _______ Work phone: ( __ )_____ Other: (__)______
Family doctor:------------Telephone: ( __ ).____________
Address:--------------------------------
Pharmacy:_________ Telephone: (_______ Fax: ( __ )_______
Family dentist:------------Telephone: ( __ ).____________
Address: --- -----·-------- ----------------
Allergies:--------------Type of reaction:-------------
Which of the following best describes where you live (check one): o Greater Toronto Area o Ontario o Canada o Outside Canada
Tobacco use: o Yes, current smoker o No ~ It "No," please check one: o Lifetime non-smoker o Quit
If you are a current or ex-smoker, please indicate your consumption per day and number of years of consumption: Number of pack(s) per day: (0 to 10) Number of smoking year(s): __ (O to 90)
3
Family history of pain disorder: o Chronic facial pain o Pelvic pain o Back pain o Fibromyalgia o Headache condition o Substances abuse/dependence o Depression o Other ________
Personal past history of: o Chronic facial pain o Fibromyalgia o Headache condition o Irritable Bowel Syndrome (IBS) o Depression o other ____
Section B: Medical and Pain History
1. Have you ever had any type of surgery? o Yes (please fill table below) o No
2. Have you ever had a bad reaction to a local anesthesia (freezing)? lf "Ye~·please desc~be; _ ___________________________~
3. Do you have any pain with the following activities? For those types of pain you do experience, please rate the degree of pain over the past month from mild to severe.
None Mild Moderate Severe
Pain with bowel movement 0 0 0 0
Pain when lifting 0 0 0 0
Pain with exercise 0 0 0 0
Pain with eating 0 0 0 0
Pain when bladder is full 0 0 0 0
Pain with urination 0 0 0 0
Pain with jaw opening/closing 0 0 0 0
Pain vvith orgasm 0 0 0 0
Contact with clothing 0 0 0 0
FOR WOMEN None Mild Moderate Severe
Pain with period 0 0 0 0
Pain with tampon use 0 0 0 0
Pain with intercourse 0 0 0 0
Pelvic pain lasting hours or days after intercourse 0 0 0 0
Other (specify): 0 0 0 0
4
FOR MEN None Mild Moderate Severe Pain with ejaculation 0 0 0 0
Pain with masturbation 0 0 0 0
Pain with intercourse 0 0 0 0
Pain with penetration 0 0 0 0
Other (specify): 0 0 0 0
4. Duration of pain symptoms:
o oto 3 months o 3 to 6 months o 6 months to 1 year o 1 to 2 years o 2 to 5 years o > 5 years
5. Pain began after:
o Accident at work o Accident at home o Motor vehicle accident o Surgery o Traumatic experience o No obvious preceding event
6. Please list All the medications that you CURRENTLY take:
Please list the medications you have tried for pain control and the reason you stopped taking it:
5
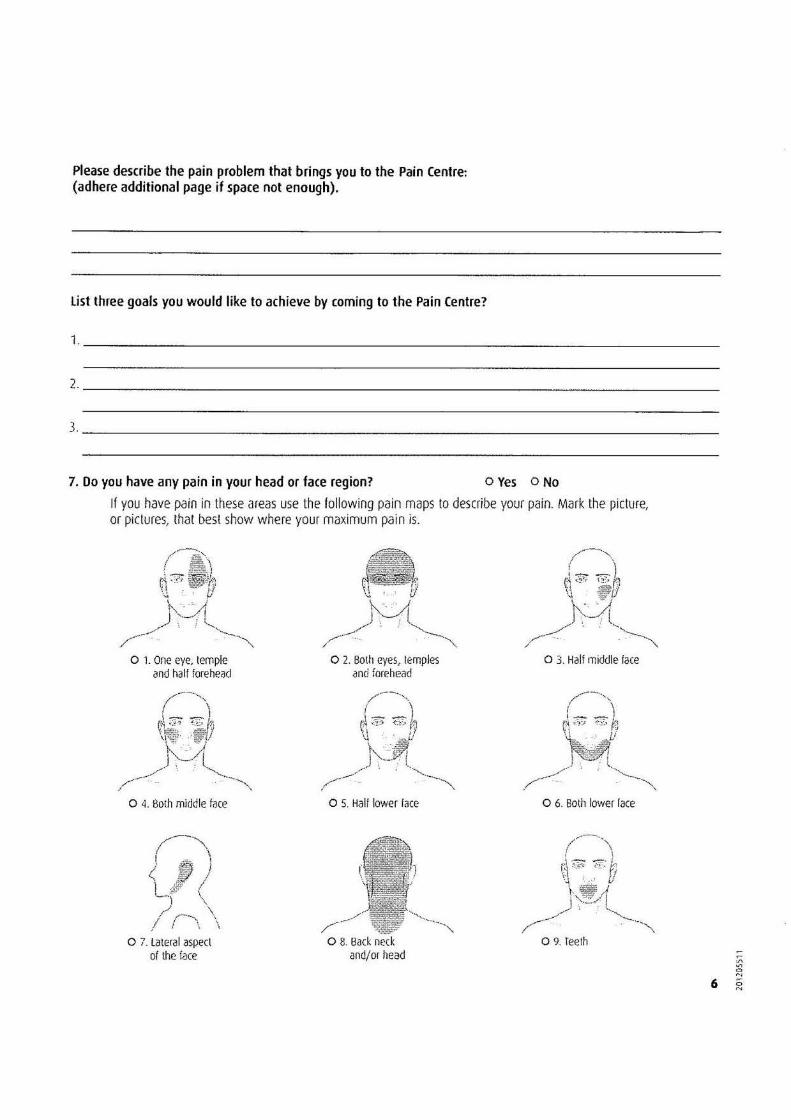
Please describe the pain problem that brings you to the Pain Centre: (adhere additional page if space not enough).
list three goals you would like to achieve by coming to the Pain Centre?
1·----------------------------------------------------------------------------
2·----------------------------------------------------------------------
}. _______________________________________________________________________
7. Do you have any pain in your head or face region? o Yes o No
If you have pain in these areas use the following pain rnaps to describe your pain. Mark the picture, or pictures, that best show where your maximum pain is.
,-----,\ ~~ I '
~~~>1 / \ ! ' .....,
_.,.-.~ '--· /---- .. .. . ·~"""
o 1. One eye, temple 0 2. Both eyes, temples and half forehead and forehead
o 5. Half lower face
~-·" I ), J< I
L..:· \ ),~ \
I I \ \
0 7. Lateral aspect of the face
o 8. Back neck and/or head
Wasser Pain Management Centre at Mount Sinai Hospital 600 University Avenue, 11th Floor
Toronto, Ontario M5G1X5
Phone: (416) 586-5997 Fax: (416) 586-5067
CANCELLATION/NO SHOW POLICY
• At least 48 hours notice is required if you must cancel/reschedule your appointment for any reason. You are asked to contact the secretary at the Wasser Pain Management Centre who made your appointment. Please be aware that leaving a message on the voicemail is not sufficient and the appointment status will not be changed to cancelled/rescheduled until the secretary contacts you to confirm this change.
• Missed appointments without the required notice will incur a charge.
• Arriving 30 minutes late for your scheduled appointment may be considered as a no show.
• All outstanding fees must be paid in full.
• Should you cancel an appointment, it is your responsibility to call and reschedule.
• More than one cancellation without notice or failure to attend your scheduled appointment may result in discharge from the Centre.
Please sign below to indicate that you have reviewed the cancellation/no show policy.
Patient's Signature Date