phencyclidine (pcp) abuse: a close-up look at a growing problem
TRANSCRIPT

Phencyclidine (PCP) abuse A close-up look at a growing problem
S. Ovid Isaacs, M.S., D.M.D.,* Paul Martin, D.D.S.,** and James A. Washington, Jr., D.D.S.,*** New York, N.Y.
DIVISION OF ORAL AND MAXILLOFACIAL SURGERY, HARLEM HOSPITAL CENTER
PCP or “angel dust” is a dissociative anesthetic agent with notoriety as an abuse substance. Numerous members of many subcultures are frequent users of this drug. It is well known in California’s psychedelia, along the East Coast, and in the middle- and working-class suburbs of the Midwest. It is important that practitioners become acquainted with the drug and its effects. Persons intoxicated with PCP have murdered their own children and have even jumped out of high-rise apartment buildings. States of florid psychosis lasting for days can follow a brief encounter with PCP. Inadvertent administration of narcotics and barbiturates to patients with acute PCP intoxication can lead to a crisis that could prove to be fatal. (ORAL SURG. ORAL MED. ORAL PATHOL. 61:126-129, 1986)
P hencyclidine (PCP), or “angel dust,” was origi- nally developed in the late 1950s as an analgesic and anesthetic agent. During clinical trials, however, it was found to have severe adverse effects, including symptoms resembling manic-depressive psychosis and schizophrenia, and the drug was never approved for use in human patients.‘,* Approval was later given for the use of PCP in veterinary medicine, but as of April, 1979, all legal manufacture of the drug stopped. Today it is classified as a Class II controlled substance. Despite the adverse effects of the drug and cessation of its legal manufacture, PCP is a very popular recreational drug, ranking number 2 in the streets today, after marijuana, because of its illicit production.
It is essential for oral surgeons and other dental practitioners to become familiar with PCP and its multifaceted effects and management in emergen- cies. Practitioners who have not yet encountered a PCP emergency in their offices or institutions prob- ably will before long.
HISTORY OF THE DRUG
Phencyclidine is the general name for 1-( 1 -phenyl- cyclohexyl)piperidine hydrochloride. It is highly lip- id soluble and is a weak base with a pKa between 8.6 and 9.4. Thirty or more derivatives of PCP have
*Formerly Chief Resident, Oral and Maxillofacial Surgery. **Attending Oral and Maxillofacial Surgeon. ***Director, Oral and Maxillofacial Surgery.
126
appeared on the streets in the last 5 years. Two of these analogues-N-ethyl- 1-phenylcyclohexamine (PCE) and l-[-(2 thiencyl) cyclophexyl] piperidine (TCP)-have been found to be more behaviorally active than the parent compound.3 PCP and its analogues are usually tolerated in street doses of 0.02 to 0.05 mg/kg by smoking or 1.5 to 3.5 mg/kg by ingestion. In many instances, however, the deceived and uninformed user may consume more and end up with PCP intoxication, which could be fatal.4v5
PCP is very easy to synthesize and can be abused in many modes. The most common are smoking (mixed with low-grade marijuana or oregano), snort- ing (mixed with cocaine), oral ingestion (mixed with peanut butter), and, to a lesser extent, intravenous injection. The drug is sold on the street under different names: angel dust, dust, T, tic tat, KJ, crystals, goon, soma, crystal joints, hog, mist, and scuffle. Every practitioner should become familiar with the various names for PCP.
PHARMACOLOGIC AND CUNICAL EFFECTS
In general, PCP is not well classified as either a central nervous system stimulant (“upper”) or depressant (“downer”), and its direct mechanism of action is not well understood. However, it is known to inhibit presynaptic uptake of norepinephrine, dopa- mine, and serotonin. Furthermore, it may compete with acetylcholine at postsynaptic sites.6 Some work- ers have also shown that PCP has the capacity to inhibit total brain protein synthesis.’
The effects of PCP usually begin within 1 hour of
Volume 61 Number 2
Phenylcyclidine abuse 127
use if the drug is ingested and within 1 minute if it is smoked, with the drug metabolizing in the liver by hydroxylation? The “high” lasts for 4 to 6 hours, and it takes 24 to 48 hours before the abuser feels normal again. The earliest clinical sign observed in the PCP abuser is hypertension. The pressor effects of PCP have been well documented in both human beings and animals.9 In addition, several investigators have reported on PCP-induced hypertensive crises which have resulted in death.“.”
Ross and Wongi2 reported that many persons under the influence of PCP show loss of memory. This loss of memory has been attributed to the inhibition of brain protein synthesis.’ It has been suggested that phencyclidine might produce organic brain disorder associated with long-term neuropsy- chological damage. In addition, a review of the literature has shown that chronic use of PCP has resulted in psychological and physiologic depen- dence. It is clear that as the amount of PCP usage increases, and if there is simultaneous use of other drugs (particularly barbituates), severe toxic symp- toms become likely. These include coma, seizures, and respiratory arrest. Numerous PCP users have experienced a disorganized state after 2 or 3 days of “normality” following a good “high.” Most research- ers are of the opinion that this delay is due to the continued presence of the drug in the central nervous system as a result of gastroenteric recirculation and lipid storage of the material. Thus, a high index of suspicion is justified when a patient gives a history of chronic PCP abuse and recent use. This person should, indeed, be considered a high-risk patient.
Intoxication can occur from either large or low doses of PCP. Typically, in low-dose intoxication some patients may appear awake while others may appear agitated or, in some instances, asymptomatic. However, vertical or horizontal nystagmus (and in some instances both forms) is common, with the pupils being of normal size. Nystagmus is specifical- ly diagnostic for PCP intoxication. In most instances intoxication usually results from oral or parenteral use of the drug rather than from smoking it. McCar- ron and associatesI have described the major and minor clinical patterns of acute PCP intoxication and give the incidence of their findings. Among the major patterns noted were acute brain syndrome (ABS), toxic psychosis, catatonic syndrome, coma, and aspi- ration pneumonia, whereas the minor patterns included lethargy, euphoria, stupor, and violence.
DENTAL CONSIDERATIONS
Parenteral administration of narcotics and barbi- turates is very common in dental offices and clinics
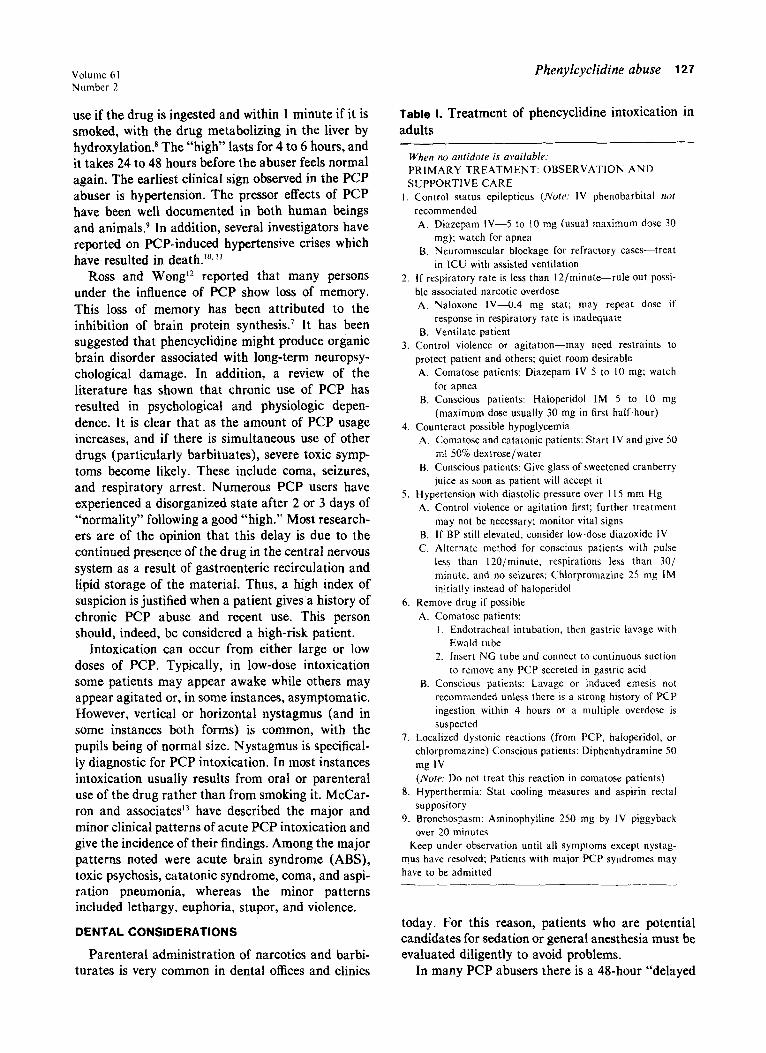
Table I. Treatment of phencyclidine intoxication in adults
When no antidote is available: PRIMARY TREATMENT: OBSERVATION AND SUPPORTIVE CARE
1. Control status epilepticus (Note: IV phenobarbital noi recommended A. Diazepam IV-5 to 10 mg (usual maximum dose 30
mg); watch for apnea B. Neuromuscular blockage for refractory cases-treat
in ICU with assisted ventilation 2. If respiratory rate is less than 1 Z/minute-rule out possi-
ble associated narcotic overdose A. Naloxone IVA.4 mg stat; may repeat dose if
response in respiratory rate is inadequate B. Ventilate patient
3. Control violence or agitation-may need restraints to protect patient and others; quiet room desirable A. Comatose patients: Diazepam IV 5 to IO mg; watch
far apnea B. Conscious patients: Haloperidol IM 5 to IO mg
(maximum dose usually 30 mg in first half-hour) 4. Counteract possible hypoglycemia
A. Comatose and catatonic patients: Start IV and give 50 ml 50% dextrose/water
B. Conscious patients: Give glass of sweetened cranberry juice as soon as patient will accept it
5. Hypertension with diastolic pressure over 115 mm Hg A. Control violence or agitation first; further treatment
may not be necessary; monitor vital signs B. If BP still elevated, consider low-dose diazoxide IV C. Alternate method for conscious patients with pulse
less than 120/minute, respirations less than 30,’ minute, and no seizures: Chlorpromazine 25 mg IM initially instead of haloperidol
6. Remove drug if possible A. Comatose patients:
I. Endotracheal intubation, then gastric lavage with Ewald tube
2. Insert NC tube and connect to continuous suction to remove any PCP secreted in gastric acid
B. Conscious patients: Lavage or induced emesis not recommended unless there is a strong history of PCP ingestion within 4 hours or a multiple overdose is suspected
7. Localized dystonic reactions (from PCP, haloperidol, or chlorpromazine) Conscious patients: Diphenhydramine 50 mg IV (Norer Do not treat this reaction in comatose patients)
8. Hyperthermia: Stat cooling measures and aspirin rectal suppository
9. Bronchospasm: Aminophylline 250 mg by IV piggyback over 20 minutes
Keep under observation until all symptoms except nystag- mus have resolved; Patients with major PCP syndromes may have to be admitted
today. For this reason, patients who are potential candidates for sedation or general anesthesia must be evaluated diligently to avoid problems.
In many PCP abusers there is a 48-hour “delayed
128 Zsaacs, Martin, and Washington Oral Surg. February, 1986
disorganized state” after use of the drug. Therefore, the administration of narcotics or barbiturates espe- cially ultra-short-acting barbiturates, should be avoided in these patients. This prevents the supra- additive pharmacologic effects and toxicity that can result in seizures, respiratory distress, or coma in the PCP patient.
A large number of dentists administer multiple drug combinations in their everyday practice, and giving these to a PCP-loaded patient could be disas- trous to both doctor and patient. Although at present there is an insufficient body of scientific data regard- ing the effects of anesthetic agents on the glottic reflex, it is known that PCP has the ability to depress this reflex. This depression can result in pulmonary aspiration of regurgitated gastric contents, followed by acute airway obstruction and/or Mendelson’s syndrome. It should be noted that a review of the literature revealed that approximately 10% of all surgical deaths resulted from pulmonary aspiration. In addition to administered drugs, nitrous oxide could also present a problem in chronic abusers of PCP and should therefore be avoided, as these patients require an increase percentage of nitrous oxide in the anesthetic mixture. This increased per- centage will lead to an increased stimulation of the central nervous system and also increased difficulty in management, with the end result being (a) prema- ture termination of the procedure or (b) the patient’s entering into a schizophreniform state.
Hypertension is also a problem that has to be considered in the PCP patient, since this is one of the earliest clinical signs. A number of induced hyper- tensive crisis ending in death have been reported as a result of PCP abuse.‘O. ‘I The PCP abuser is a walking time bomb. Therefore, it would be advisable for any and all procedures to be cancelled in patients in whom acute or chronic usage is established. If one is in doubt about a patient, it would not hurt to postpone the procedure for 3 days. The dentist should then advise the patient to take cranberry juice during this period to help hasten excretion of the PCP. Finally, one should not prescribe any narcotic analgesics to these patients, as PCP has the ability to potentiate the effects of the drug and cause bizarre behavior.
TREATMENT OF PHENCYCLIDINE INTOXICATION
The method of treatment used is outlined in an algorithm published by McCarron and associatesi (Table I). This should be posted in every doctor’s operatory. It should be noted that cranberry juice has been recommended. This is because it contains
hippuric acid, which helps to acidify the urine and hasten excretion of PCP.
DISCUSSION
In most patients measurable quantities of PCP cannot be demonstrated in the blood. As a result, urine is the specimen of choice for detection of PCP and its analogues. The drug remains present in the urine for 72 hours and in some cases as long as 7 days.14 A urinalysis to check for PCP should be part of the protocol in all instances in which PCP abuse is suspected. In view of the delayed effects of the drug, which can produce bizarre behavior, it is advisable that any and all procedures that require conscious sedation or general anesthesia be postponed for at least 2 to 3 days in all instances in which a history of recent use of PCP is given. In addition, narcotic analgesics should not be prescribed because of PCP’s ability to potentiate the action of narcotics as well as barbiturates.15, I6 At present PCP intoxication does not respond to naloxone, and the same holds true for PCP analogues. In most instances naloxone is used in the event that the patient has taken another drug in addition to the PCP-associated narcotic overdose.
It is of paramount importance for every practitio- ner to become acquainted with the various street names of phencyclidine (PCP). Experience has shown that the majority of patients will open up and tell the truth about their drug abuse history if they are asked about a drug by its street name. In the medical history questionnaire it is advisable to include the street names of all known abused sub- stances. The dangers of PCP are becoming more and more evident and, in spite of its pronounced behavo- rial and CNS toxicity, the number of abusers grows steadily larger, Because PCP often decreases the patient’s ability to feel pain, persons intoxicated with this drug should be evaluated carefully for evidence of trauma.
CONCLUSION
Phencyclidine is one of the most potent psychoto- mimetic compounds known and can induce psycho- sis. Many patients who have had acute or chronic exposure to the drug will go to the dental office, outpatient clinic, or emergency room for treatment. Therefore, an efficient history-taking strategy for the reliable identification of the PCP patient must be used to avoid precipitation of a crisis in the office, clinic, or operating room. It is extremely important to take a closer look at all patients with a high index of suspicion. Above all, one should remember that the combination of nystagmus and hypertension

Volume 61 Number 2
occurring in a patient with a history of PCP abuse is suggestive of PCP intoxication.
REFERENCES
Munch JC: Phencyclidine: pharmacology and toxicology, Bull Narc 26: 9-17, 1974. Metrotec Research Assoc: Phencyclidine-PCP. US Nation- al Clearing House for Drug Abuse Information, Rockville. Md.. Report Series l4/2: l-l 1. 1978. Zukin SR, Zukin RS: (3H)-Phencyclidine binding to specif- ic brain receptor sites. Psychopharmacol Bull 16: 59-62. 1980. Beede MS: Phencyclidine intoxication. Postgrad Med 68: 20 I-209, I 980. Khantrian EJ. McKenna GJ: Acute toxic and withdrawal reactions associated with drug use and abuse. Ann Intern
- Med 90: 361-372, 1979. Smith RC. Heltzer HY. Arora RC. et al: Effects of Dhencv- clidine on catecholamine and serotonin uptake. Biochem Pharmacol 26: 1435-1439, 1979. Deutsch D, Omanand K, Kersten S: Phencyclidine and analogues: effect on brain protein synthesis. J Neurochem 42: 407-41 I, 1984. Burns S: High on PCP. J Emerg Med March 8, 264-279, 1976. Bessen HA: Intracranial hemorrhage associated with phency- clidine abuse. JAMA 248: 585-596, 1982.
Phenylcyclidine abuse 129
IO. Malave AP, Holsapple MP, Yim GKW: Reduction by atro- pine of phencyclidine, hypertension and apneusis. Life Sci 30: 929-932, 1982.
I I. llett KF, Jarrot B, O’Donnell SR, et al: Mechanism of cardiovascular actions of phencyclidine. Br J Pharmacol Chemother 28: 73-83. 1966.
12. Russ C, Wong D: Diagnosis and treatment of phencyclidine psychosis: clinical consideration. J Psychedelic Drugs 11: 277-282. 1979.
13. McCarron MM, Schulze BW, Thompson GA. et al: Acute phencyclidine intoxication. clinical pattern. complications and treatment. Ann Emerg Med 1U: 290-297. 1981.
14. Carey RE: PCP (phencyclidine). an update. J Psychedelic Drugs 11: 265-275, 1979.
15. Carroll M: Efects of pentobarbital and d-amphetamine on oral phencyclidinc. Pharmacol Biochem Behav 20: l37- 143, 1984.
16. Chait LD, Balster RC: Effects of combinations of phencycli- dine and pentobarbital on scheduled controlled behavior. Pharmacol Biochem Behav 9: 201-205, 1978.
Request reprints to: Dr. S. Ovid lsaacs 223 E. 43rd St. Brooklyn, NY I I203