perforations 3
TRANSCRIPT

Endodontics Mishaps (Perforations)
Marwa Shaker
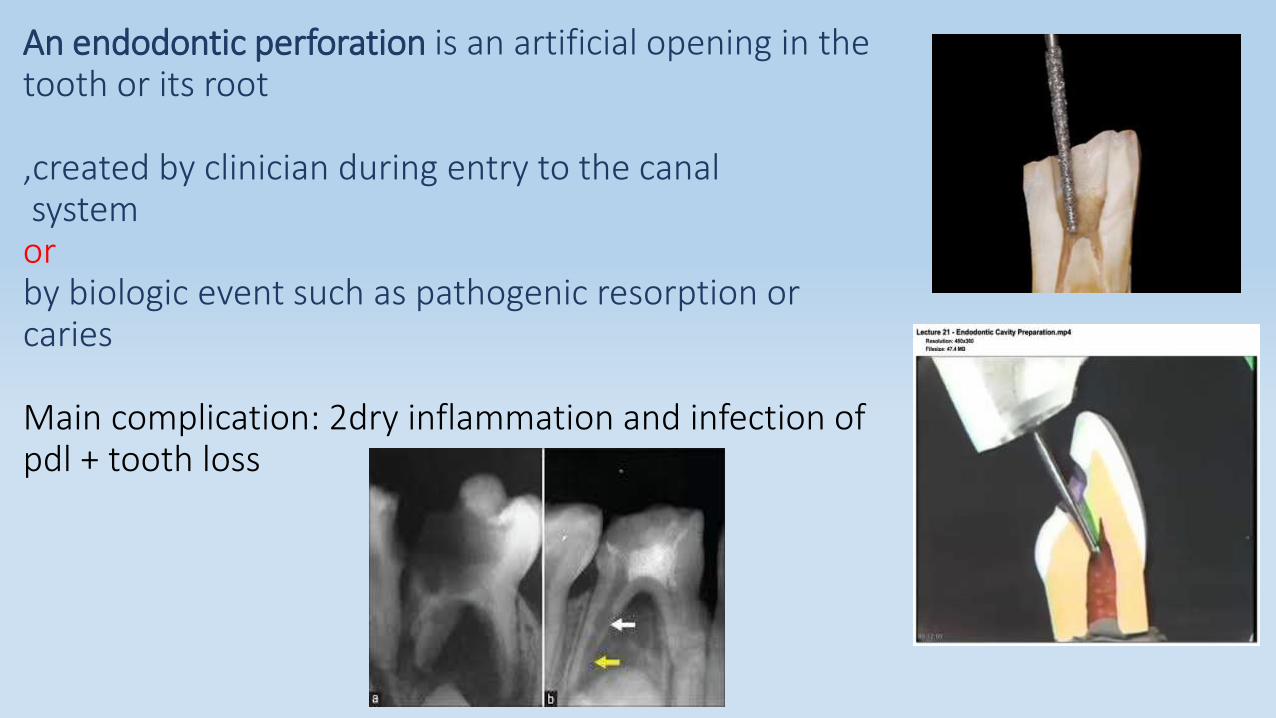
An endodontic perforation is an artificial opening in the tooth or its root
,created by clinician during entry to the canalsystemorby biologic event such as pathogenic resorption or caries
Main complication: 2dry inflammation and infection of pdl + tooth loss
*Root perforations
Roots may be perforated at different levels during cleaning and shaping
(apical,middle,cervical)
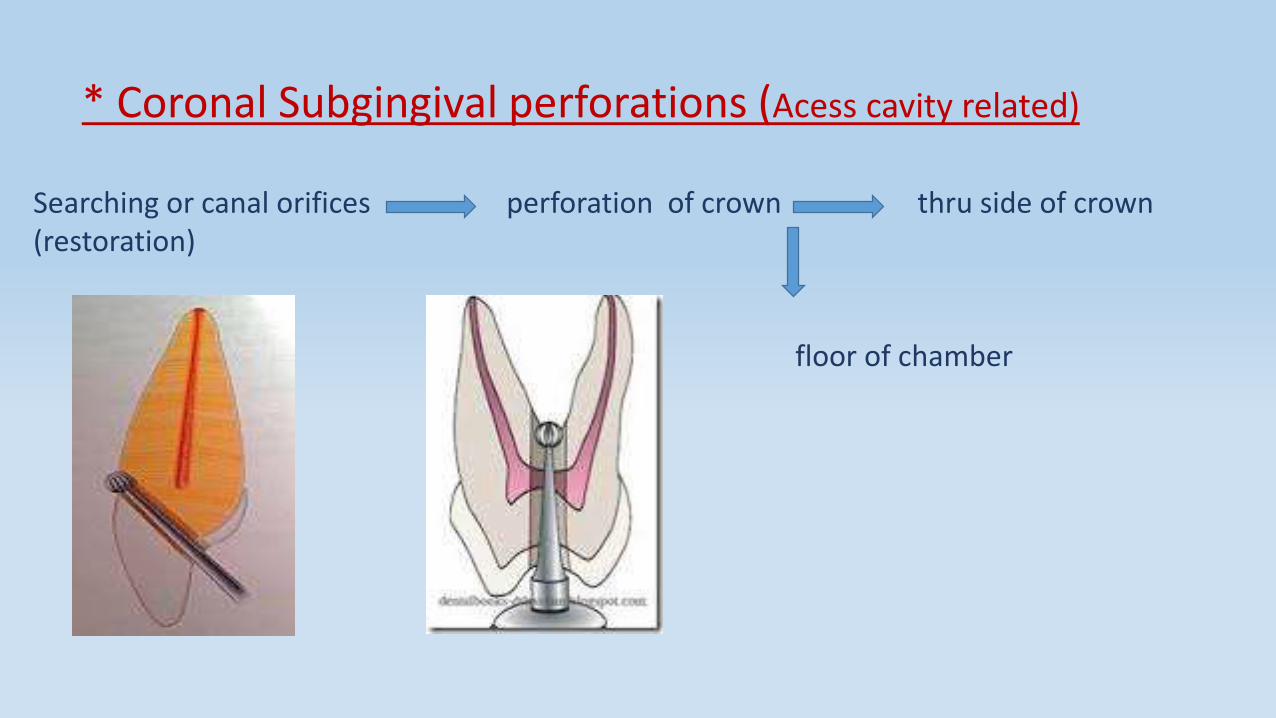
* Coronal Subgingival perforations (Acess cavity related)
Searching or canal orifices perforation of crown thru side of crown (restoration)
floor of chamber
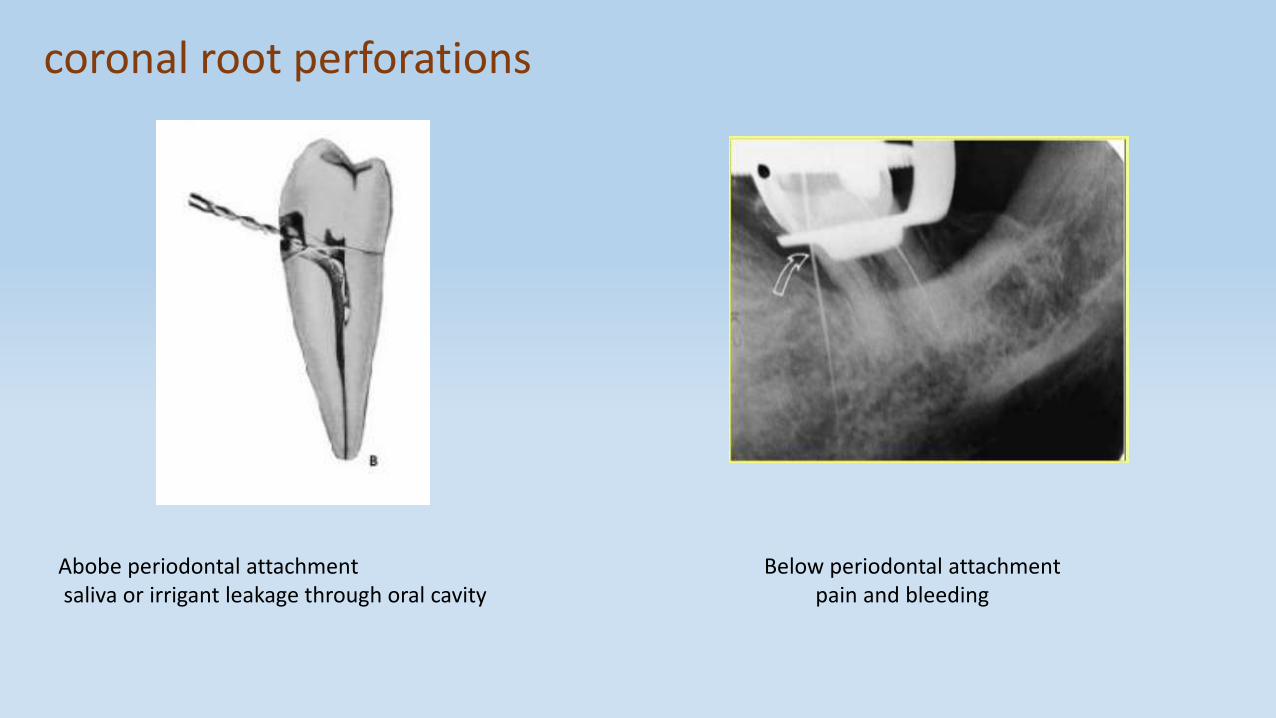
coronal root perforations
Abobe periodontal attachment Below periodontal attachment saliva or irrigant leakage through oral cavity pain and bleeding

Management
Isolate the perforation If perforation site is clean uninfected repair immediately
For esthetics :calcium sulphate barrier with tooth colouredrestoration .For non esthetic areas Cavit,amalgam,calcium hydroxide paste,super EBA,Glassionomer.
MTA ( when no sulcular communication)
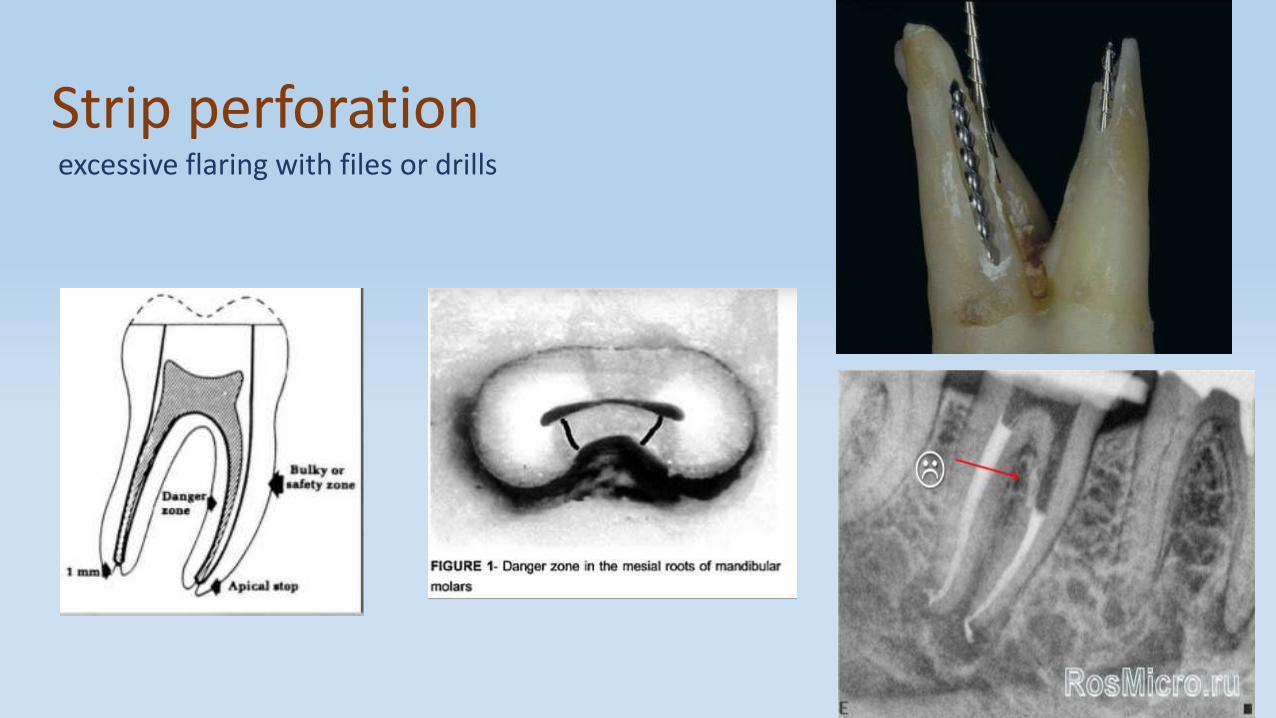
Strip perforationexcessive flaring with files or drills
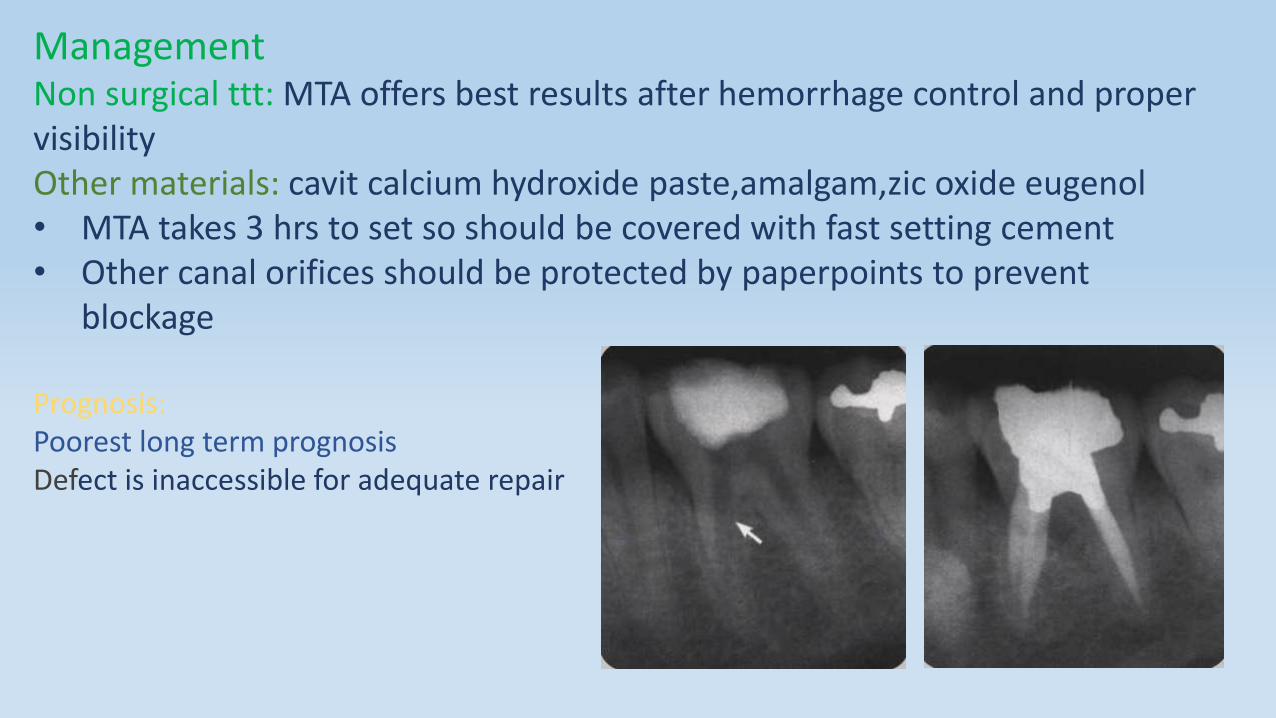
ManagementNon surgical ttt: MTA offers best results after hemorrhage control and proper visibility Other materials: cavit calcium hydroxide paste,amalgam,zic oxide eugenol• MTA takes 3 hrs to set so should be covered with fast setting cement • Other canal orifices should be protected by paperpoints to prevent
blockage
Prognosis:Poorest long term prognosisDefect is inaccessible for adequate repair
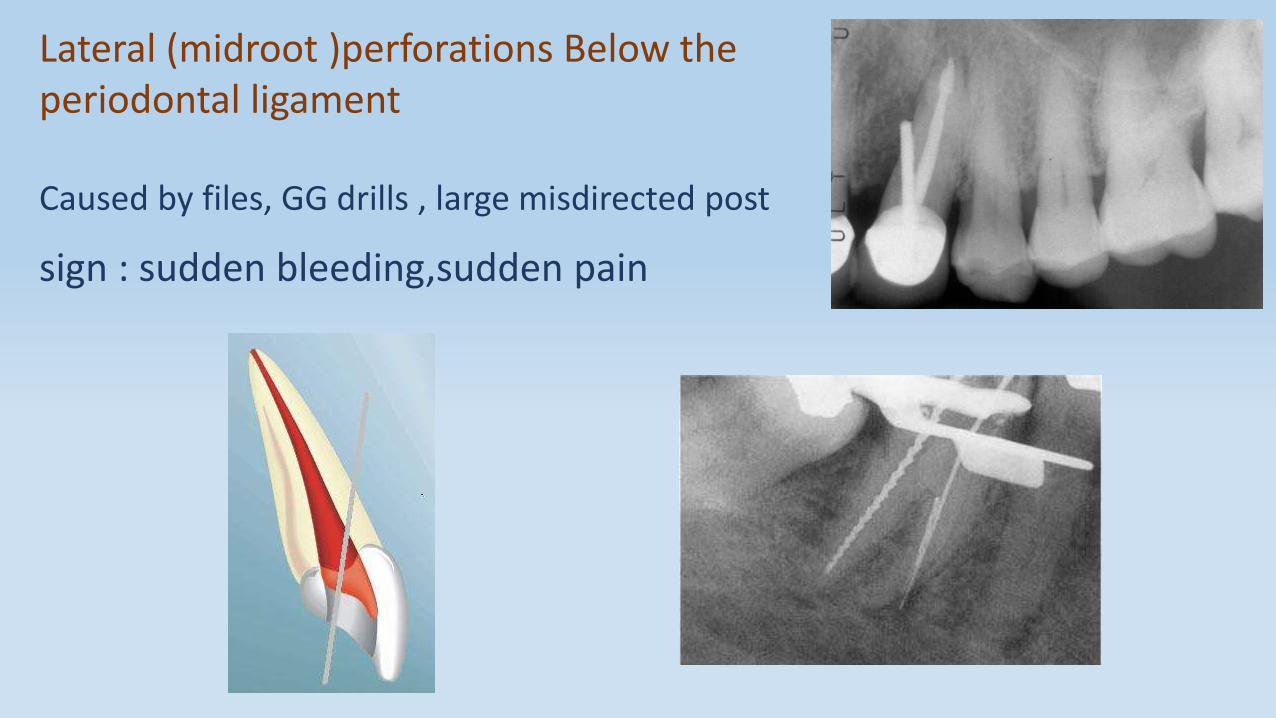
Lateral (midroot )perforations Below the periodontal ligament
Caused by files, GG drills , large misdirected post
sign : sudden bleeding,sudden pain
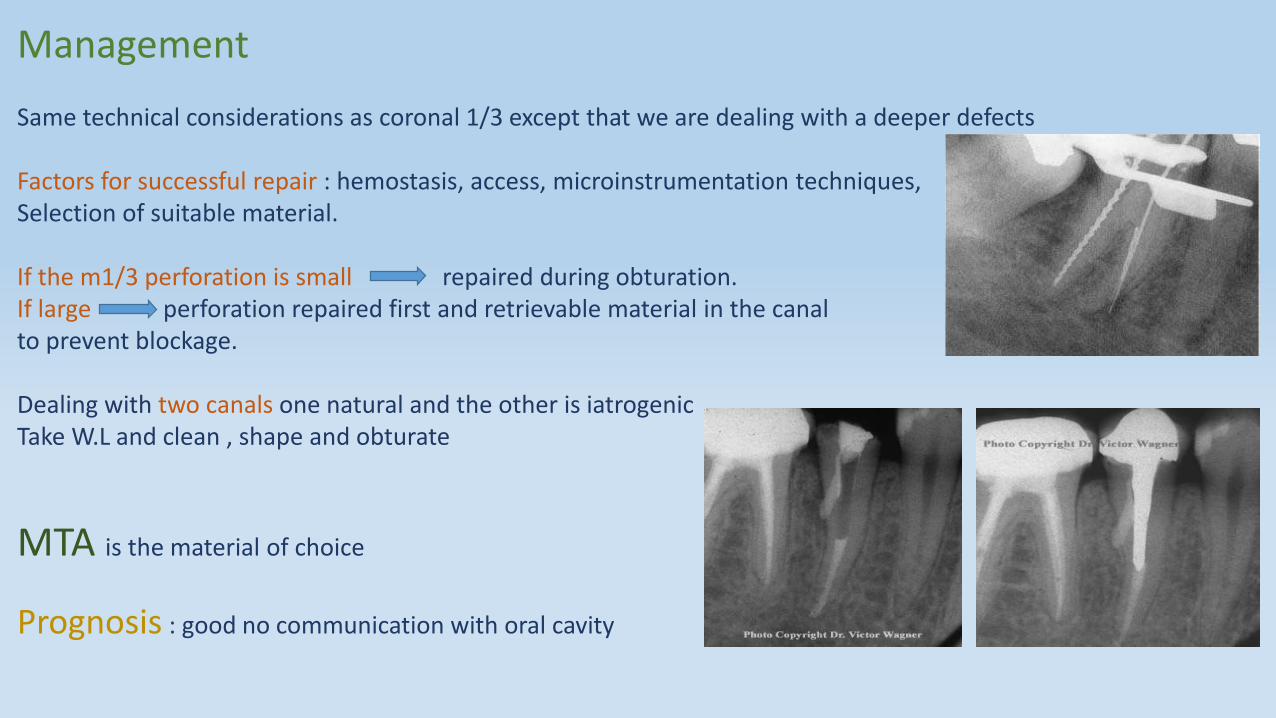
Management
Same technical considerations as coronal 1/3 except that we are dealing with a deeper defects
Factors for successful repair : hemostasis, access, microinstrumentation techniques,Selection of suitable material.
If the m1/3 perforation is small repaired during obturation.If large perforation repaired first and retrievable material in the canal to prevent blockage.
Dealing with two canals one natural and the other is iatrogenic Take W.L and clean , shape and obturate
MTA is the material of choice
Prognosis : good no communication with oral cavity
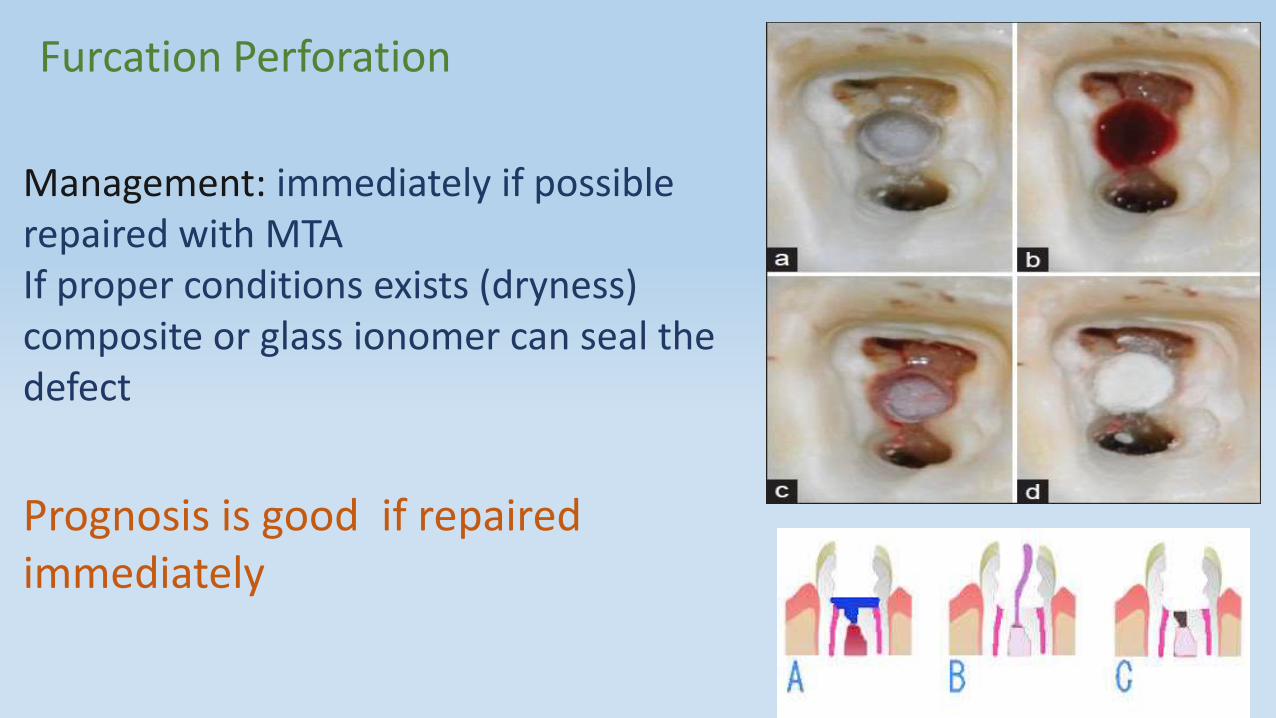
Furcation Perforation
Management: immediately if possible repaired with MTA If proper conditions exists (dryness) composite or glass ionomer can seal the defect
Prognosis is good if repaired immediately

If not repairable non surgicaly or inaccessibleSurgical:Hemisection,
Bicuspidization
Root amputation
Intention replantation
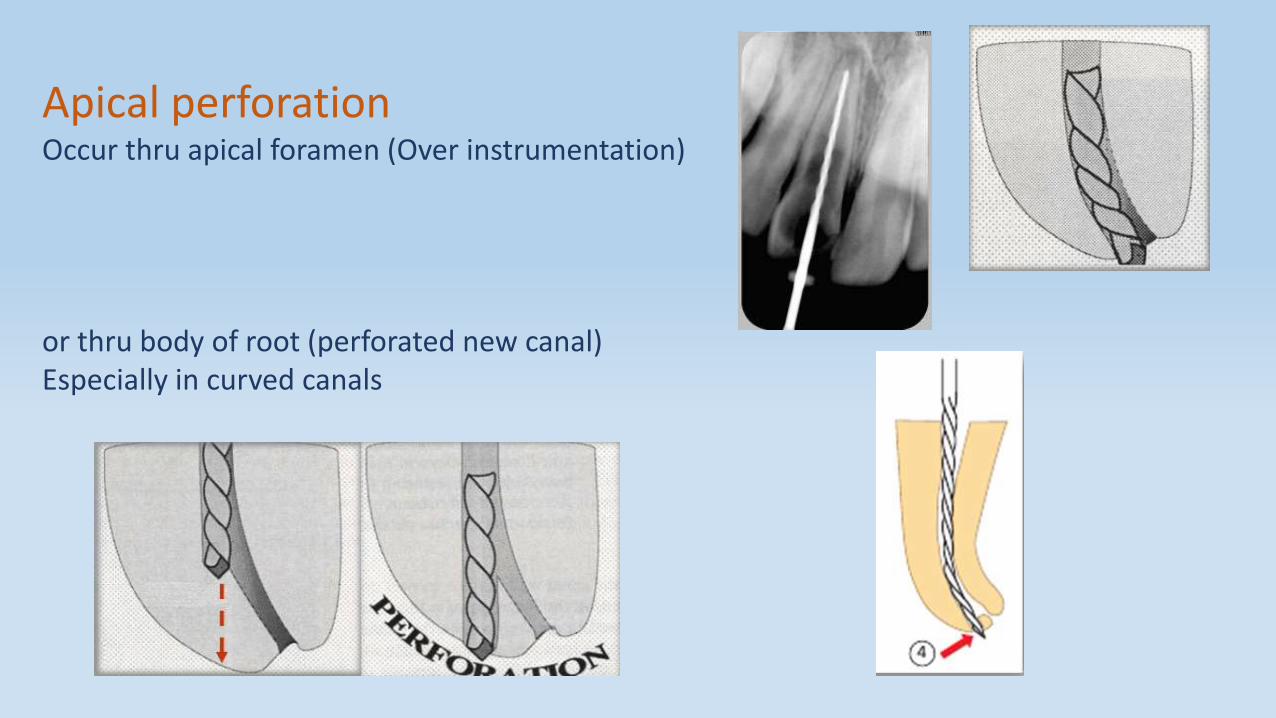
Apical perforationOccur thru apical foramen (Over instrumentation)
or thru body of root (perforated new canal)Especially in curved canals
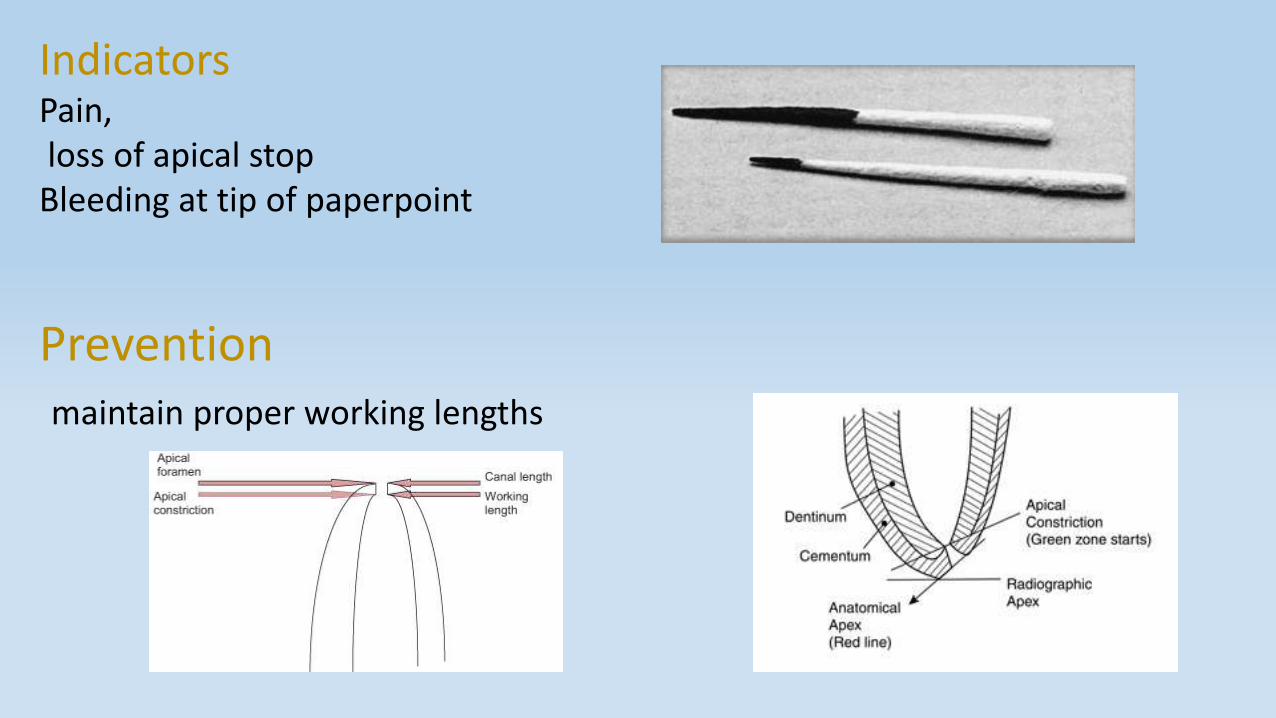
IndicatorsPain,loss of apical stop
Bleeding at tip of paperpoint
Preventionmaintain proper working lengths
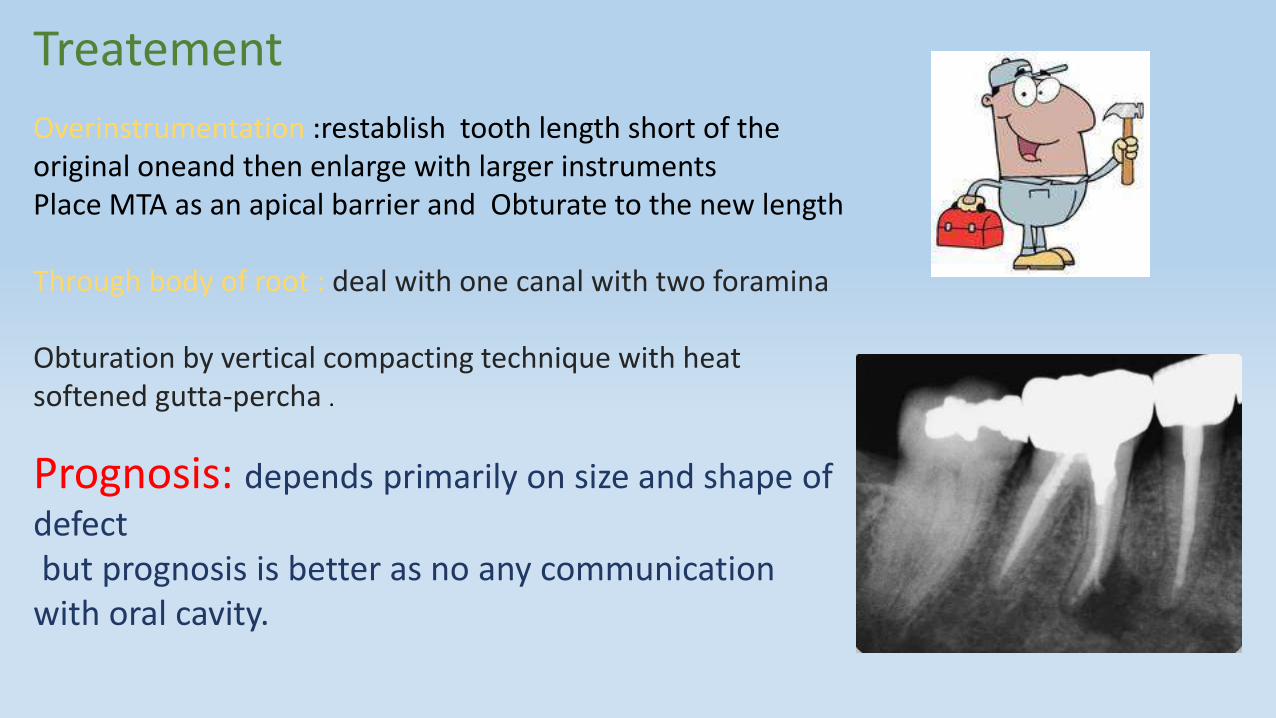
Treatement
Overinstrumentation :restablish tooth length short of the original oneand then enlarge with larger instrumentsPlace MTA as an apical barrier and Obturate to the new length
Through body of root : deal with one canal with two foramina
Obturation by vertical compacting technique with heat softened gutta-percha .
Prognosis: depends primarily on size and shape of
defectbut prognosis is better as no any communication
with oral cavity.
Prognosis for healing1.Timing of repair Immediate is better than delayed , infected un treated defects lead to marked inflammation ,abcess formations and cervicular epithelium proliferation
2.Location of perforation eg furcation perforation decreased success due to inc.epithelial proliferation and periodontitis Perforation near gingival sulcus inflammation and loss of epithelial attachment + pdl pocket More apical perforation offer better prognosis
3. Size of perforationsmall defects direct and immediate restoration + few chances of pdlbreakdown Large defects difficult to place well condensed restoration + large contact surface area with peiodontium allow inflammation .
4. Perforation Repair materials must be antimicrobial , non toxic provide adequate seal non absorpable ,RO ,promote oeteogenesis and cementogenesis.
ZOE Cements …. Chronic inflammatory response Calcium hydroxide ….. Prevent in groth of granulation tissue into perforationCavit …..mild to modetare inflammatory response Amalgum…. assessing healing potential but carcinogenic Super EBA……proper seal and adaptation to defectGlass ionomer…… same properties as amalgam
MTA• composition include calcium and phosphorus ions with pH 10.2 • Least toxic • Biologicaly compatible • Allow groth of cementum like substance on surface of material • Less inflammatory infiltrative cells • Good marginal adaptation to dentin • Leak less than amalgam in lateral perforations
No current available material meets all requirements
5. HemostaticsTo stop hemorrhage wjich may affect assecibility calcium hydroxide or calcium sulphate
6.Vision or accessibility Magnification loupes , head lamps , transilluminating devices and dental microscopes Are imp in addressing perforations
7.Treatement sequence Repairing perforation will allow control of bleeding , confine irrigation ,and facilitate obturation .Maintain the pathway of canal to avoid blockage
Case presentation A 32-year-old Indian female had underwent root canal treatment of her upper left central (#21) and lateral incisors (#22) about 1 year ago, following which redness and occasional pus discharge started from the gingiva in relation to the central incisor.
clinical presentation, there was erythema in the labial attached gingiva in relation to tooth #21. Periodontal probing revealed a 4 mm deep periodontal pocket on the labial aspect of tooth #21 corresponding to the area of erythema.Intra-oral periapicalradiograph revealed short of length radiopaque filling material in tooth #21 and poorly condensed root canal filling in tooth #22 .
However, no evidence of periapical pathology was present in relation to either tooth.
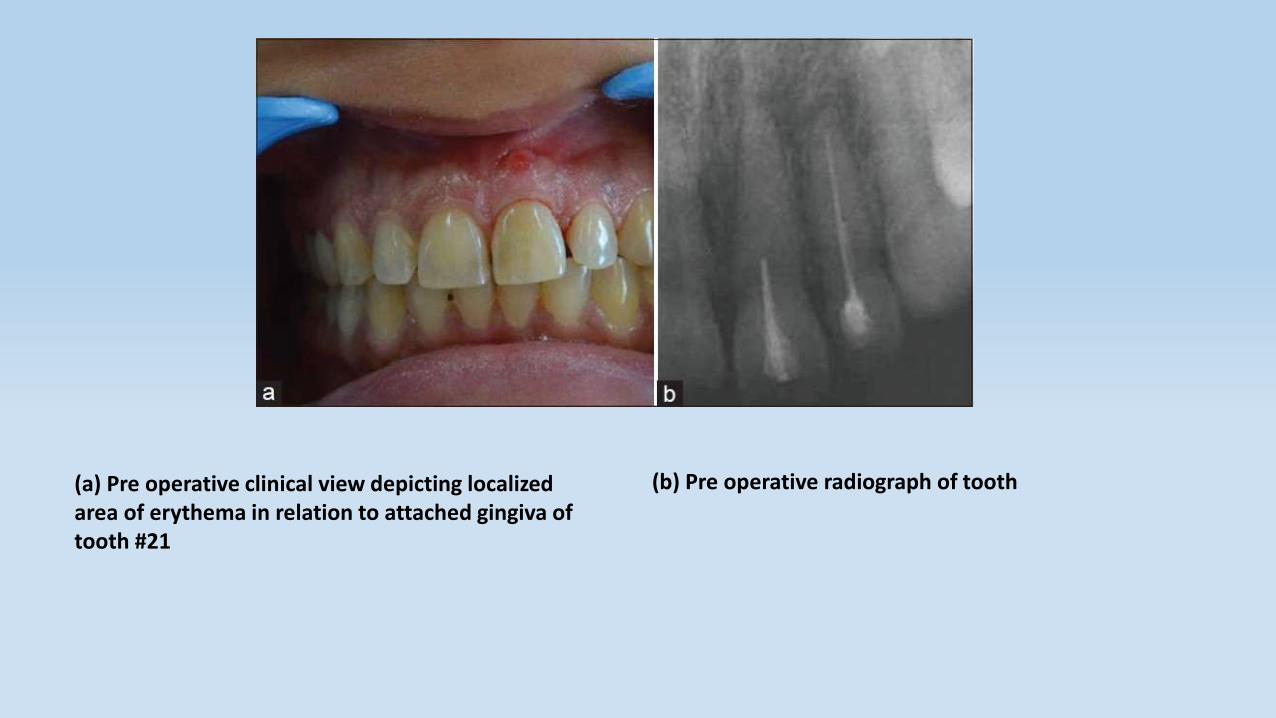
(a) Pre operative clinical view depicting localized area of erythema in relation to attached gingiva of tooth #21
(b) Pre operative radiograph of tooth
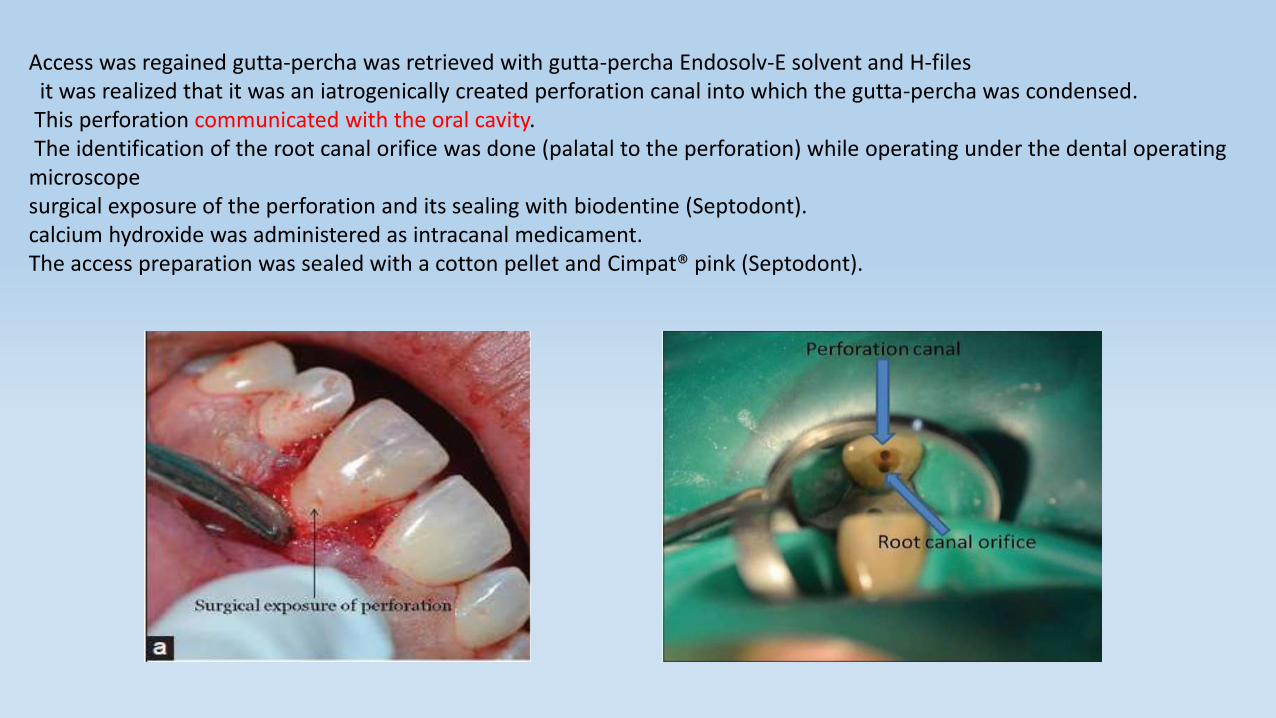
Access was regained gutta-percha was retrieved with gutta-percha Endosolv-E solvent and H-filesit was realized that it was an iatrogenically created perforation canal into which the gutta-percha was condensed.
This perforation communicated with the oral cavity.The identification of the root canal orifice was done (palatal to the perforation) while operating under the dental operating
microscopesurgical exposure of the perforation and its sealing with biodentine (Septodont).calcium hydroxide was administered as intracanal medicament. The access preparation was sealed with a cotton pellet and Cimpat® pink (Septodont).
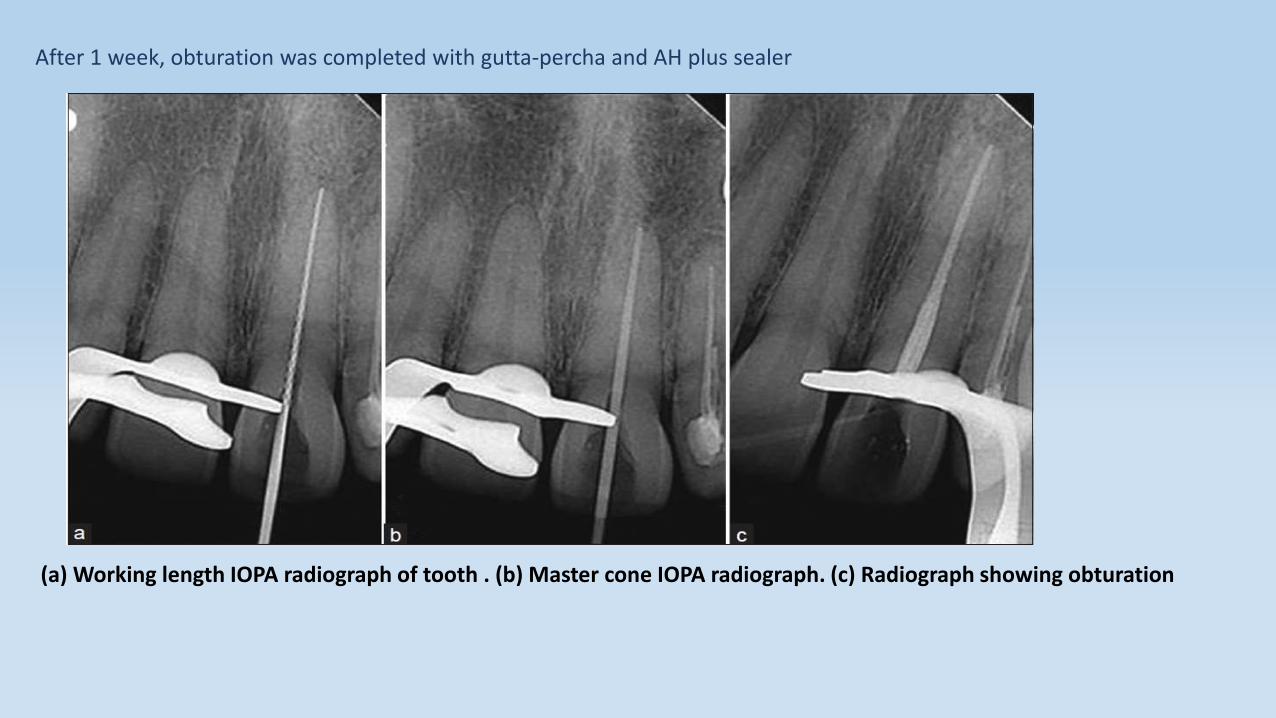
After 1 week, obturation was completed with gutta-percha and AH plus sealer
(a) Working length IOPA radiograph of tooth . (b) Master cone IOPA radiograph. (c) Radiograph showing obturation
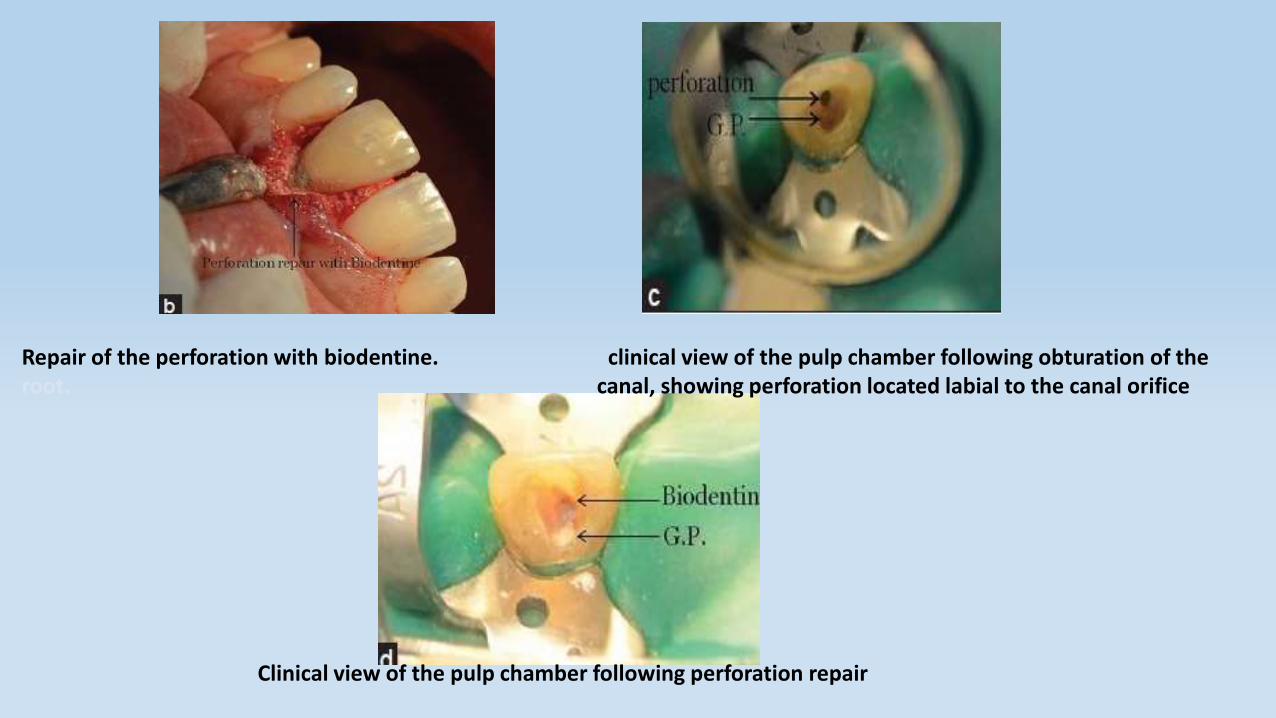
Repair of the perforation with biodentine. clinical view of the pulp chamber following obturation of the root. canal, showing perforation located labial to the canal orifice
Clinical view of the pulp chamber following perforation repair
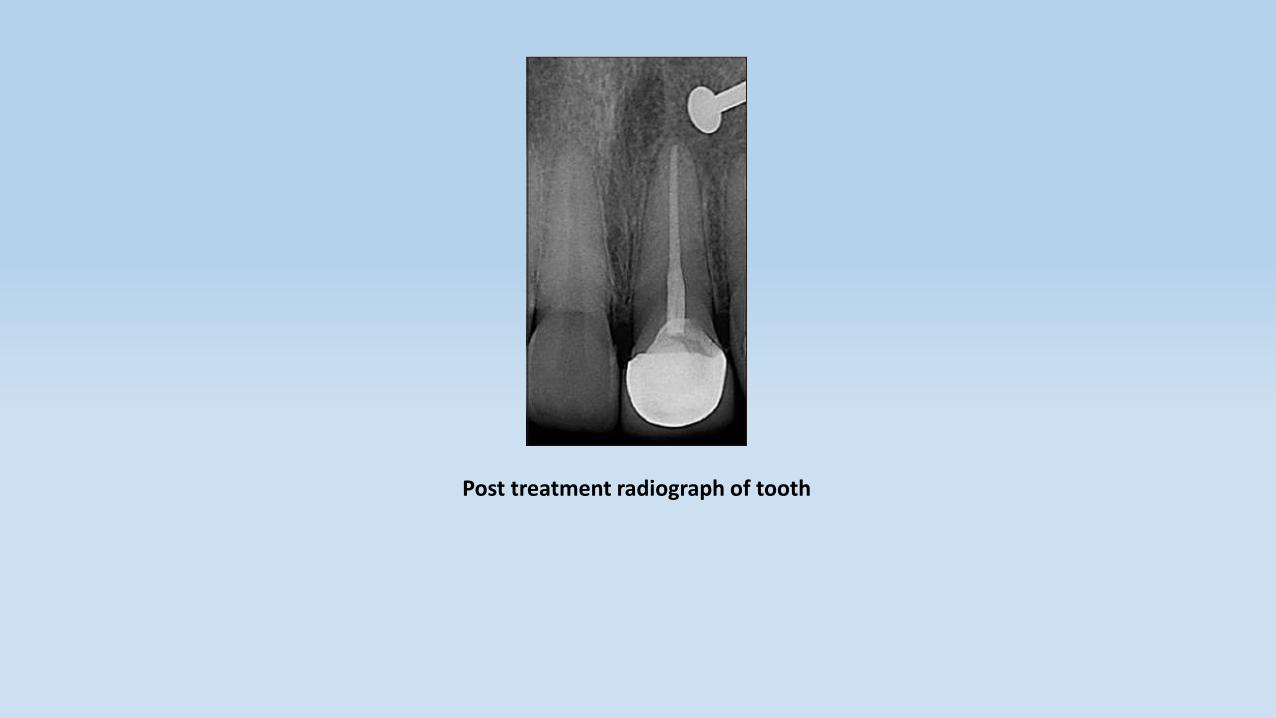
Post treatment radiograph of tooth
Discussion
Out of the various factors affecting the prognosis of teeth with iatrogenic perforations, timely intervention and the level of perforation (relative to crestal bone and epithelial attachment) are probably the most important. [4] The present case posed a treatment challenge as the perforation was crestal in position (it impinged on the epithelial attachment with periodontal pocket formation) with a 1 year long history.
A perforation occurring relatively close to the crestal bone and the epithelial attachment is critical as it may lead to bacterial contamination from the oral environment along the gingival sulcus. Furthermore, apical migration of the epithelium to the perforation site can be expected, creating a periodontal defect. Such lesions which present with both endodontic and periodontal involvement are known as endo-perio lesions. The present case is a primary endodontic lesion with secondary periodontal involvement. (Simon's classification of endo-perio lesions). [8] Once the periodontal pocket is formed, persistent inflammation of the perforation site is most likely maintained by continuous ingress of irritants from the pocket. In the present case also, loss of periodontal attachment and formation of periodontal pocket (4 mm) were seen. Treatment of crestal perforations carries a guarded prognosis because of their proximity to the epithelial attachment.
References
INGLE ENDODONTICS ENDODONTIC PRINCIPLES AND PRACTICE http://www.saudiendodj.com/article.
Thank you