perception of cervical cancer risk and screening behavior: a literature review
TRANSCRIPT
Perception of Cervical Cancer Risk andScreening Behavior: A Literature ReviewCarmen W. H. Chan, RN, MPhil, PhD, Sheng-Bo Yang, MD, PhD, Can Gu, RN, MPhil, PhD, Xiuhua Wang, RN, PhD, andLijian Tao, MD, PhD
Carmen W. H. Chan, RN, MPhil, PhD, is a Professor of the Nethersole School of Nursing, The Chinese University of HongKong, Hong Kong, Sheng-Bo Yang, MD, PhD, is an Associate Professor of Department of Dermatology, Third XiangyaHospital, Can Gu, RN, MPhil, PhD, is a Postdoctoral Fellow of Department of Medicine, Xiangya Hospital and Lecturer,School of Nursing, Xiuhua Wang, RN, PhD, is an Associate Professor of School of Nursing, and Lijian Tao, MD, PhD, is aProfessor of Department of Medicine, Xiangya Hospital, Central South University, Changsha, China.
Search terms:Cervical cancer, cervical screening,literature review, nursing, riskperception
Author contact:[email protected], with a copyto the Editor: [email protected]
Funding: This research was fundedby Young Faculty DevelopmentProject of Central South University,China (contract grant number:2177721500084) and Chia FamilyHealth Fellowship Award (contractgrant number: 2012CF01).Conflict of interest statement: Theauthors have no conflicts ofinterest to disclose.
PURPOSE: This review examines women’s risk perception of cervical cancer, thefactors influencing this perception, and the relationship between risk perceptionof cervical cancer and screening behavior.METHODS: Integrative literature review method was used.FINDINGS: The search procedure resulted in the identification of 42 studies,including 1 literature review and 41 primary studies. Trends and discrepancies inthe literature are presented with interpretations and recommendations.CONCLUSION: Existing theories of health behavior appear inadequate for under-standing screening behavior, and further studies are recommended to enrich theknowledge base of nursing diagnoses in knowledge deficit and health-seekingbehavior.IMPLICATIONS FOR NURSING PRACTICE: Efforts would be made to improvenurses’ understanding of risk perception of cervical cancer within specific culturalcontext.
目的: 本文综述了女性对宫颈癌的危险性的感知,影响这种感知的因素,及对对宫
颈癌的危险性的感知和宫颈癌筛查行为的关系。
方法: 本研究应用综合文献综述方法
结果: 查文献共发现了42篇相关文献,包括一篇综述和41篇论著。本文对文献中的
趋同和差异进行了阐述和分析。
结论: 现有的健康行为理论不能对宫颈癌筛查行为作出充分的解释,因此需要进行
进一步的研究,以充实与知识缺乏和健康寻求行为等护理诊断相关的内容。
对护理实践的意义: 我们需要让我们的护士更多的了解在特定文化背景下女性对宫
颈癌的危险性的感知和其相关因素。
Cervical cancer is the second most prevalent canceramong women, with an estimated 530,232 new cases and275,008 deaths globally each year (Globocan, 2010).According to a World Health Organization (WHO, 2008)update in 2004, cervical cancer is the most prevalentcancer in Africa and Southeast Asia, although it occurs onlyin women. Moreover, other developing countries with insuf-ficient medical services carry a heavier burden of cervicalcancer because of the lack of accessible screening services(American Cancer Society, 2006).
The perception of risk, which is defined as an individual’sassessment of the likelihood or probability of harm, is con-sidered a crucial factor in promoting precautionary healthbehavior. It is also an essential component of different theo-retical models of health behavior, such as Protection Moti-vation Theory (PMT; Armitage & Conner, 2001; Floyd,Prentice-Dunn, & Rogers, 2000; Montano, 2008). For
instance, in the case of breast cancer screening, those whoperceived a higher likelihood or probability of developingbreast cancer were more likely to undertake cancer screen-ing and be involved in cancer risk reduction activities(Katapodi, Lee, Facione, & Dodd, 2004). However, with cer-vical cancer, it is unclear whether an individual’s awarenessof her risk of the disease influences the likelihood of herparticipating in the screening. Nurses involved in the pro-grams for cervical cancer screening need to have theunderstanding of women’s risk perception to facilitate theidentification of accurate nursing diagnosis, and subse-quently develop appropriate intervention strategies. There-fore, the research team critically reviewed the publishedliterature on the perception of cervical cancer risks and therelationship between risk perception and cervical screeningattendance. The results would enrich the nursing knowl-edge base in health protection that is closely associated
bs_bs_banner
1© 2014 NANDA International, Inc.International Journal of Nursing Knowledge Volume ••, No. ••, •• 2014

with the diagnoses of knowledge deficit and health-seekingbehavior.
The Review
Aim
The aim was to elucidate the trends of women’s percep-tion of cervical cancer risk, the factors influencing risk per-ception, and the relationship between the perception ofcervical cancer risk and the screening behavior, whichcould help nurses to develop appropriate health protectioncare plan for women.
Design
An integrative review was undertaken to synthesize thestudy characteristics and findings. The integrative review isa specific method that could include all different studydesigns (i.e., quantitative and qualitative research methods)and has the potential to inform future research and practice(Whittemore & Knafl, 2005). This selective and criticalreview of the literature centered on issues related towomen’s risk perception of cervical cancer and cervicalscreening behavior. Risk perception of cervical cancer andits relationship with women’s cervical screening participa-tion was systematically reviewed and discussed. Criticalreviews of individual studies were described in terms ofstudy characteristics, subject characteristics, measurementstrategies of risk perception employed in the studies, andoutcome characteristics. After identifying trends and dis-crepancies from the literature and offering some prelimi-nary interpretations, implications for future work andjustification for the current study in terms of theoreticalframework, study variables, study population, and studydesign were discussed.
Search Methods
The literature review combined search articles fromPubMed, Ovid MEDLINE, CLINAL, EMBASE, PsycINFO, andthe Cochrane database of systematic reviews. We includedarticles that met the following inclusion criteria: the studieshad to be empirical studies that used a qualitative or quan-titative research design, designated cervical cancer screen-ing as the primary health-promoting behavior studied,written in English, and published between 1990 and 2012.
The relevant subject areas in the critical review includedwomen’s perception of cervical cancer risk, the factorsinfluencing women’s risk perception, and the relationshipbetween the perception of cervical cancer risk and thescreening behavior. The following keywords were used inthe database search: “cervical cancer,” “uterine cervixcancer,” “uterine cervix neoplasms,” “cervical cancer andrisk perception,” “cervical cancer screening,” “cervicalscreening and risk perception,” “perceived risk,” “riskperception,” “perceived vulnerability,” “perceived suscepti-
bility,” “perceived likelihood,” and “subjective risk percep-tion.” A supplementary search of the reference lists ofarticles in the Ovid MEDLINE, PubMed, and PsycINFO data-bases was conducted using the keywords “risk perception,”“perceived risk,” and “cervical screening.” The findingsfrom each database were reviewed and compared, withdouble findings deleted.
Search Outcome
The initial database search identified 96 articles. Wereviewed the abstracts and back-checked the referencelists of 96 articles identified from the initial database searchto examine other studies that may have initially beenmissed. If we could not decide whether to include or excludethis study through reviewing abstract, the full text of thosestudies will be further reviewed for final decision. Weexcluded research that involved risk perception of healthproviders (7 studies), epidemiological studies about riskfactors of cervical cancer (8 studies), meeting and disser-tations abstracts (3 studies), studies about factors influenc-ing cervical screening attendance that failed to involvedrisk perception into their studies (15 studies), studies aboutfactors influencing human papilloma virus (HPV) vaccina-tion (5 studies), studies involved women diagnosed withcervical cancer (6 studies), studies about factors influenc-ing general screening behavior (3 studies), duplicationstudies (4 studies), as well articles published in a languageother than English (3 studies). This search procedureresulted in the identification of 42 studies, comprising oneliterature review (Vernon, 1999) and 41 primary studies. Theliterature review (Vernon, 1999) was included because itexamines the research findings on risk perception relatedto cancer screening behavior, including cervical screening.Two reviewers critically reviewed all 42 articles indepen-dently and discussed the similarities and differences in theircomments until a consensus was reached.
Data Abstraction
The corresponding author initially abstracted data, andthe first author and corresponding author criticallyassessed the characteristics and main findings of the rel-evant studies.
Quality Appraisal
The selected studies were evaluated by the primaryinvestigator and cross-checked by a co-investigator using achecklist adapted from Mols et al. (2005). The checklist wasmodified to fit the aim of the present review. This checklistconsisted of 14 items, comprising 14 predefined criteria. Thischecklist consisted of five domains: study population (threeitems), study design (three items), follow-up (three items),measurements (three items), and analysis strategies (twoitem). A selected study received 1 for meeting one criterionand 0 for not meeting the criterion or describing insuffi-
Risk Perception and Screening Behavior C. W. H. Chan et al.
2

ciently. Thus, possible scores for each study ranged from 0(low quality) to 14 (high quality). Studies scoring 10 orhigher were considered to be of “high quality.”
Results
Methodological Quality and Characteristics ofSelected Studies
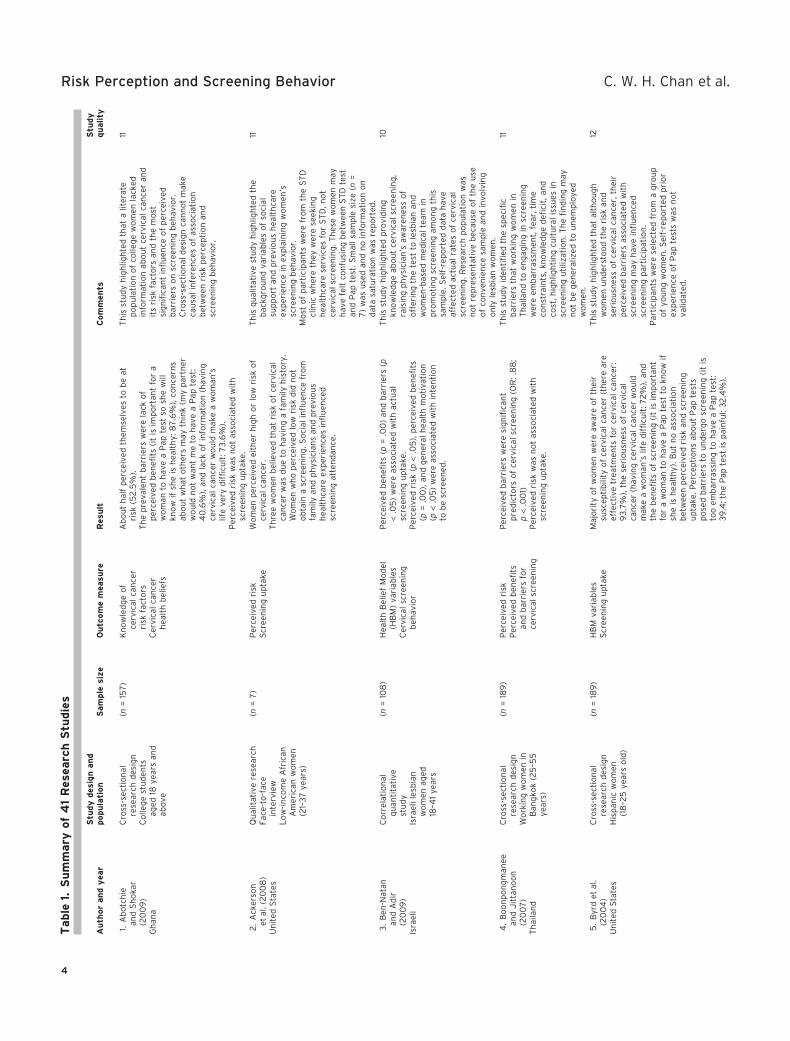
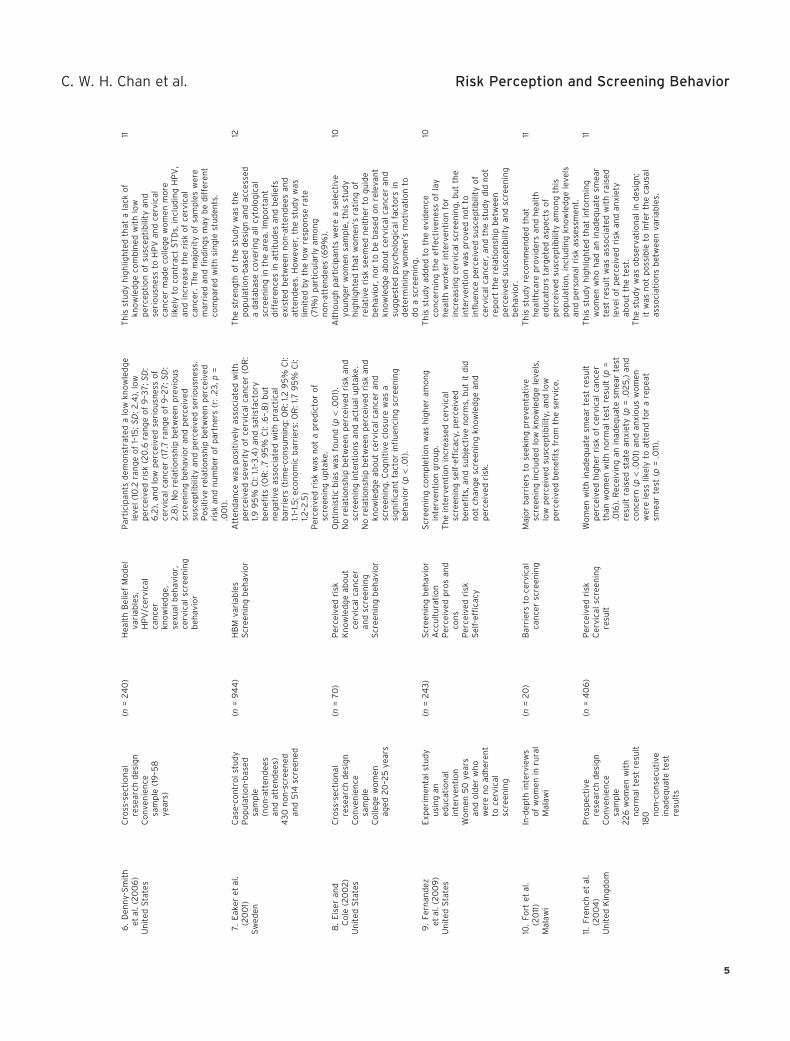
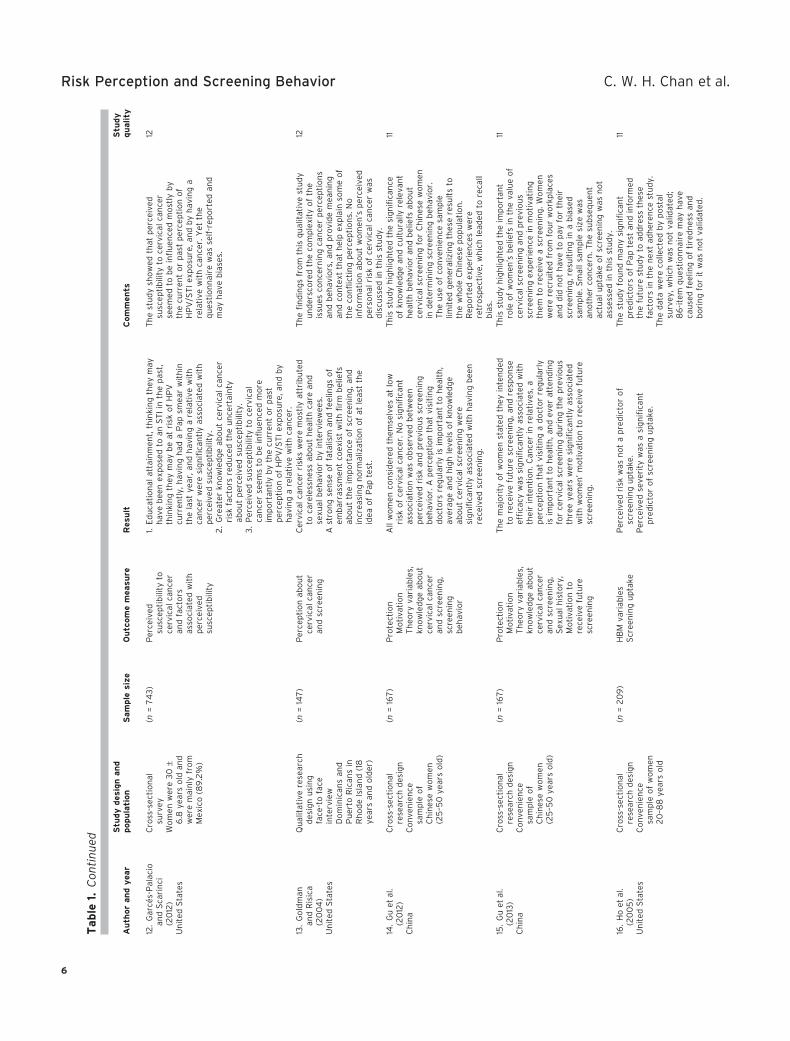
The scores of methodological quality are summarized inTable 1. The mean quality score of 41 studies is 11.3, with arange of 10–13. Methodological weakness mainly concernedthe lack of valid and consistent measurement of risk per-ception of cervical cancer and the response rate. Theselected studies, all of which were published between 1995and 2011, and their characteristics are outlined in Table 1.The focus of the review was to examine how the constructthat is interchangeably called “perceived risk,” “risk per-ception,” “perceived vulnerability,” or “perceived suscepti-bility” relates to cervical cancer screening behavior. Apartfrom one literature review (Vernon, 1999), the researchdesigns of the 41 studies were varied and included cross-sectional surveys (26 studies), face-to-face interviews (5studies), prospective research (2 studies), case-controlledstudies (3 studies), a longitudinal study (1 study), experi-mental studies (3 studies), and secondary data analyses (1study).
Selected Theoretical Models
Theoretical frameworks were described in 39.4% (n = 13)of the studies; the frameworks included the Health BeliefModel (HBM) (eight studies), Health Belief Framework (onestudy), PMT (three studies), PEN-3 (a conceptual frameworkfor health education programs), and Interaction Model ofClient Health Belief (one study). One study used a compli-ance model that incorporated four existing theoreticalframeworks, including the Theory of Planned Behavior, theHBM, Social Cognitive Theory, and the TranstheoreticalModel and Stages of Changes. Another study used a modelof preventive behavior that incorporated two existing theo-retical models, the HBM and the Andersen BehavioralModel.
Subject Characteristics
The sample size and sampling techniques of the studiesvaried. Convenience sampling was used most frequently(59%, 24 studies), followed by random sampling (27%, 11studies) and purposive sampling (14%, 6 studies); thesample sizes of five qualitative studies ranged from 7 to 147.The sample size of the remaining 36 studies ranged from 70to 3,221. Although the age of the study participants rangedfrom 18 to 75 years, four studies were conducted in a selec-tively younger female population aged between 12 and 25years (Byrd, Peterson, Chavez, & Heckert, 2004; Eiser &Cole, 2002; Kahn, Goodman, Slap, Huang, & Emans, 2001;Saules et al., 2007). Most of the studies examined Cauca-
sian or Western populations, and only seven studiesinvolved Asian populations from Taiwan (Hou, Fernandez,Baumler, Parcel, & Chen, 2003), Singapore (Lee, Seow, Ling,& Peng, 2002; Seow, Wong, Smith, & Lee, 1995), Laos(Phongsavan, Phengsavanh, Wahlström, & Marions, 2010),Thailand (Boonpongmanee & Jittanoon, 2007), and main-land China (Gu, Chan, Twinn, & Choi, 2012; Gu et al., 2013).Fourteen studies were conducted in America, 7 studieswere conducted in England, and 20 studies were conductedin other regions of the world.
Strategies for the Measurement of Risk Perception
A wide range of methods was used to assess risk percep-tions of cancer, resulting in apparently contradictory find-ings. Five qualitative studies used face-to-face interview toobtain in-depth information about women’s understandingabout cervical cancer risk. The most common measures ofperceived risk employed by remaining 36 studies were asfollows: a comparative measure employing a six-pointrating scale ranging from “less likely” to “more likely” thatasked participants either “Are you more likely or less likelyto suffer from cervical cancer in the future than otherwomen of the same age?” or to rate their perceived risk ofdeveloping cervical cancer on a five-point rating scaleranging from “much higher than average” to “much lowerthan average” (Eiser & Cole, 2002; French, Maissi, &Marteau, 2004; Marlow, Waller, & Wardle, 2009; Marteau,Hankins, & Collins, 2002); an absolute measure using afive-point rating scale ranging from “strongly agree” to“strongly disagree” that asked participants to respond tothe statement “I’m at risk of developing cervical cancer”(Abotchie & Shokar, 2009; Denny-Smith, Bairan, & Page,2006; Walsh, 2006); a quantitative rating of personal riskand general population risk (0–100%) (Taylor et al., 2002);a verbal measure such as “very low” to “very high” or“large risk” and “not large risk” (Eaker, Adami, & Sparen,2001; Kim et al., 2008; Merrill & Madanat, 2002).
Most of the studies assessed women’s perceived risk ofcervical cancer with one or two questions regarding likeli-hood, such as comparative and verbal measures. Althoughthe response choices for these questions always used quan-tified multi-point scales anchored by numbers, verbalphrases, or comparisons with other people, this traditionalmeasurement of risk assumes that the variable is constant.However, evidence indicates that the anchors for subjectiveand comparative measures, such as verbal expression andquantitative rating, and even the standard “language ofrisk,” can have different meanings to different individualsand even to the same individual in varying contexts(Wallsten, Budescu, Rapoport, Zwick, & Forsyth, 1986;Walter & Britten, 2002).
Outcome Characteristics
Because risk perception is thought to be an importantmotivator of cervical screening behavior, it is imperative to
C. W. H. Chan et al. Risk Perception and Screening Behavior
3
Table
1.S
um
mary
of
41
Res
earc
hS
tudie
s
Au
thor
an
dy
ear
Stu
dy
des
ign
an
dpopu
lati
on
Sam
ple
size
Ou
tcom
em
easu
reR
esu
ltC
om
men
tsS
tudy
qu
ality
1.A
bo
tch
iean
dS
ho
kar
(20
09
)G
han
a
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
olle
ge
stu
den
tsag
ed18
year
san
dab
ove
(n=
157
)K
no
wle
dg
eo
fce
rvic
alca
nce
rri
skfa
cto
rsC
ervi
cal
can
cer
hea
lth
bel
iefs
Ab
ou
th
alf
per
ceiv
edth
emse
lves
tob
eat
risk
(52
.5%
).T
he
pre
vale
nt
bar
rier
sw
ere
lack
of
per
ceiv
edb
enefi
ts(i
tis
imp
ort
ant
for
aw
om
anto
hav
ea
Pap
test
sosh
ew
illkn
ow
ifsh
eis
hea
lth
y:8
7.6
%),
con
cern
sab
ou
tw
hat
oth
ers
may
thin
k(m
yp
artn
erw
ou
ldn
ot
wan
tm
eto
hav
ea
Pap
test
:4
0.6
%),
and
lack
of
info
rmat
ion
(hav
ing
cerv
ical
can
cer
wo
uld
mak
ea
wo
man
’slif
eve
ryd
iffi
cult
:73
.6%
).P
erce
ived
risk
was
no
tas
soci
ated
wit
hsc
reen
ing
up
take
.
Th
isst
ud
yh
igh
ligh
ted
that
alit
erat
ep
op
ula
tio
no
fco
lleg
ew
om
enla
cked
info
rmat
ion
abo
ut
cerv
ical
can
cer
and
its
risk
fact
ors
and
the
mo
stsi
gn
ifica
nt
infl
uen
ceo
fp
erce
ived
bar
rier
so
nsc
reen
ing
beh
avio
r.C
ross
-sec
tio
nal
des
ign
can
no
tm
ake
cau
sal
infe
ren
ces
of
asso
ciat
ion
bet
wee
nri
skp
erce
pti
on
and
scre
enin
gb
ehav
ior.
11
2.
Ack
erso
net
al.(
20
08
)U
nit
edS
tate
s
Qu
alit
ativ
ere
sear
chFa
ce-t
o-f
ace
inte
rvie
wL
ow
-in
com
eA
fric
anA
mer
ican
wo
men
(21–
37
year
s)
(n=
7)
Per
ceiv
edri
skS
cree
nin
gu
pta
keW
om
enp
erce
ived
eith
erh
igh
or
low
risk
of
cerv
ical
can
cer.
Th
ree
wo
men
bel
ieve
dth
atri
sko
fce
rvic
alca
nce
rw
asd
ue
toh
avin
ga
fam
ilyh
isto
ry.
Wo
men
wh
op
erce
ived
low
risk
did
no
to
bta
ina
scre
enin
g.S
oci
alin
flu
ence
fro
mfa
mily
and
ph
ysic
ian
san
dp
revi
ou
sh
ealt
hca
reex
per
ien
ces
infl
uen
ced
scre
enin
gat
ten
dan
ce.
Th
isq
ual
itat
ive
stu
dy
hig
hlig
hte
dth
eb
ackg
rou
nd
vari
able
so
fso
cial
sup
po
rtan
dp
revi
ou
sh
ealt
hca
reex
per
ien
cein
exp
lain
ing
wo
men
’ssc
reen
ing
beh
avio
r.M
ost
of
par
tici
pan
tsw
ere
fro
mth
eS
TD
clin
icw
her
eth
eyw
ere
seek
ing
hea
lth
care
serv
ices
for
ST
D,n
ot
cerv
ical
scre
enin
g.T
hes
ew
om
enm
ayh
ave
felt
con
fusi
ng
bet
wee
nS
TD
test
and
Pap
test
.Sm
all
sam
ple
size
(n=
7)
was
use
dan
dn
oin
form
atio
no
nd
ata
satu
rati
on
was
rep
ort
ed.
11
3.
Ben
-Nat
anan
dA
dir
(20
09
)Is
rael
i
Co
rrel
atio
nal
qu
anti
tati
vest
ud
yIs
rael
ile
sbia
nw
om
enag
ed18
–41
year
s
(n=
108
)H
ealt
hB
elie
fM
od
el(H
BM
)va
riab
les
Cer
vica
lsc
reen
ing
beh
avio
r
Per
ceiv
edb
enefi
ts(p
=.0
0)
and
bar
rier
s(p
<.0
5)
wer
eas
soci
ated
wit
hac
tual
scre
enin
gu
pta
ke.
Per
ceiv
edri
sk(p
<.0
5),
per
ceiv
edb
enefi
ts(p
=.0
0),
and
gen
eral
hea
lth
mo
tiva
tio
n(p
<.0
5)
wer
eas
soci
ated
wit
hin
ten
tio
nto
be
scre
ened
.
Th
isst
ud
yh
igh
ligh
ted
pro
vid
ing
kno
wle
dg
eab
ou
tce
rvic
alsc
reen
ing
,ra
isin
gp
hys
icia
n’s
awar
enes
so
fo
ffer
ing
the
test
tole
sbia
nan
dw
om
en-b
ased
med
ical
team
inp
rom
oti
ng
scre
enin
gam
on
gth
issa
mp
le.S
elf-
rep
ort
edd
ata
hav
eaf
fect
edac
tual
rate
so
fce
rvic
alsc
reen
ing
.Res
earc
hp
op
ula
tio
nw
asn
ot
rep
rese
nta
tive
bec
ause
of
the
use
of
con
ven
ien
cesa
mp
lean
din
volv
ing
on
lyle
sbia
nw
om
en.
10
4.
Bo
on
po
ng
man
eean
dJ
itta
no
on
(20
07
)T
hai
lan
d
Cro
ss-s
ecti
on
alre
sear
chd
esig
nW
ork
ing
wo
men
inB
ang
kok
(25
–55
year
s)
(n=
189
)P
erce
ived
risk
Per
ceiv
edb
enefi
tsan
db
arri
ers
for
cerv
ical
scre
enin
g
Per
ceiv
edb
arri
ers
wer
esi
gn
ifica
nt
pre
dic
tors
of
cerv
ical
scre
enin
g(O
R:.
88
;p
<.0
01)
Per
ceiv
edri
skw
asn
ot
asso
ciat
edw
ith
scre
enin
gu
pta
ke.
Th
isst
ud
yid
enti
fied
the
spec
ific
bar
rier
sth
atw
ork
ing
wo
men
inT
hai
lan
dto
eng
agin
gin
scre
enin
gw
ere
emb
arra
ssm
ent,
fear
,tim
eco
nst
rain
ts,k
no
wle
dg
ed
efici
t,an
dco
st,h
igh
ligh
tin
gcu
ltu
ral
issu
esin
scre
enin
gu
tiliz
atio
n.T
he
fin
din
gm
ayn
ot
be
gen
eral
ized
tou
nem
plo
yed
wo
men
.
11
5.
Byr
det
al.
(20
04
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
nH
isp
anic
wo
men
(18
–25
year
so
ld)
(n=
189
)H
BM
vari
able
sS
cree
nin
gu
pta
keM
ajo
rity
of
wo
men
wer
eaw
are
of
thei
rsu
scep
tib
ility
of
cerv
ical
can
cer
(th
ere
are
effe
ctiv
etr
eatm
ents
for
cerv
ical
can
cer:
93
.7%
),th
ese
rio
usn
ess
of
cerv
ical
can
cer
(hav
ing
cerv
ical
can
cer
wo
uld
mak
ea
wo
man
’slif
ed
iffi
cult
:72
%),
and
the
ben
efits
of
scre
enin
g(i
tis
imp
ort
ant
for
aw
om
anto
hav
ea
Pap
test
tokn
ow
ifsh
eis
hea
lth
y).B
ut
no
asso
ciat
ion
bet
wee
np
erce
ived
risk
and
scre
enin
gu
pta
ke.P
erce
pti
on
sab
ou
tP
apte
sts
po
sed
bar
rier
sto
un
der
go
scre
enin
g(i
tis
too
emb
arra
ssin
gto
hav
ea
Pap
test
:3
9.4
;th
eP
apte
stis
pai
nfu
l:3
2.4
%).
Th
isst
ud
yh
igh
ligh
ted
that
alth
ou
gh
wo
men
un
der
sto
od
the
risk
and
seri
ou
snes
so
fce
rvic
alca
nce
r,th
eir
per
ceiv
edb
arri
ers
asso
ciat
edw
ith
scre
enin
gm
ayh
ave
infl
uen
ced
scre
enin
gp
arti
cip
atio
n.
Par
tici
pan
tsw
ere
sele
cted
fro
ma
gro
up
of
you
ng
wo
men
.Sel
f-re
po
rted
pri
or
exp
erie
nce
of
Pap
test
sw
asn
ot
valid
ated
.
12
Risk Perception and Screening Behavior C. W. H. Chan et al.
4
6.
Den
ny-
Sm
ith
etal
.(2
00
6)
Un
ited
Sta
tes
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
on
ven
ien
cesa
mp
le(1
9–5
8ye
ars)
(n=
24
0)
Hea
lth
Bel
ief
Mo
del
vari
able
s,H
PV
/cer
vica
lca
nce
rkn
ow
led
ge,
sexu
alb
ehav
ior,
cerv
ical
scre
enin
gb
ehav
ior
Par
tici
pan
tsd
emo
nst
rate
da
low
kno
wle
dg
ele
vel
(10
.2ra
ng
eo
f1–
15;S
D:2
.4),
low
per
ceiv
edri
sk(2
0.6
ran
ge
of
9–3
7;S
D:
6.2
),an
dlo
wp
erce
ived
seri
ou
snes
so
fce
rvic
alca
nce
r(1
7.7
ran
ge
of
9–2
7;S
D:
2.8
).N
ore
lati
on
ship
bet
wee
np
revi
ou
ssc
reen
ing
beh
avio
ran
dp
erce
ived
susc
epti
bili
tyan
dp
erce
ived
seri
ou
snes
s.P
osi
tive
rela
tio
nsh
ipb
etw
een
per
ceiv
edri
skan
dn
um
ber
of
par
tner
s(r
:.2
3,p
=.0
01)
.
Th
isst
ud
yh
igh
ligh
ted
that
ala
cko
fkn
ow
led
ge
com
bin
edw
ith
low
per
cep
tio
no
fsu
scep
tib
ility
and
seri
ou
snes
sto
HP
Van
dce
rvic
alca
nce
rm
ade
colle
ge
wo
men
mo
relik
ely
toco
ntr
act
ST
Ds,
incl
ud
ing
HP
V,
and
incr
ease
the
risk
of
cerv
ical
can
cer.
Th
em
ajo
rity
of
sam
ple
sw
ere
mar
ried
and
fin
din
gs
may
be
dif
fere
nt
com
par
edw
ith
sin
gle
stu
den
ts.
11
7.
Eak
eret
al.
(20
01)
Sw
eden
Cas
e-co
ntr
ol
stu
dy
Po
pu
lati
on
-bas
edsa
mp
le(n
on
-att
end
ees
and
atte
nd
ees)
43
0n
on
-scr
een
edan
d5
14sc
reen
ed
(n=
94
4)
HB
Mva
riab
les
Scr
een
ing
beh
avio
rA
tten
dan
cew
asp
osi
tive
lyas
soci
ated
wit
hp
erce
ived
seve
rity
of
cerv
ical
can
cer
(OR
:1.9
95
%C
I:1.1
–3.4
)an
dsa
tisf
acto
ryb
enefi
ts(O
R:.
79
5%
CI:
.6–.
8)
bu
tn
egat
ive
asso
ciat
edw
ith
pra
ctic
alb
arri
ers
(tim
e-co
nsu
min
g:O
R:1
.29
5%
CI:
1.1–1
.5;e
con
om
icb
arri
ers:
OR
:1.7
95
%C
I:1.2
–2.5
)P
erce
ived
risk
was
no
ta
pre
dic
tor
of
scre
enin
gu
pta
ke.
Th
est
ren
gth
of
the
stu
dy
was
the
po
pu
lati
on
-bas
edd
esig
nan
dac
cess
eda
dat
abas
eco
veri
ng
all
cyto
log
ical
scre
enin
gin
the
area
.Im
po
rtan
td
iffe
ren
ces
inat
titu
des
and
bel
iefs
exis
ted
bet
wee
nn
on
-att
end
ees
and
atte
nd
ees.
Ho
wev
er,t
he
stu
dy
was
limit
edb
yth
elo
wre
spo
nse
rate
(71%
)p
arti
cula
rly
amo
ng
no
n-a
tten
dee
s(6
9%
).
12
8.
Eis
eran
dC
ole
(20
02
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
on
ven
ien
cesa
mp
leC
olle
ge
wo
men
aged
20
–25
year
s
(n=
70
)P
erce
ived
risk
Kn
ow
led
ge
abo
ut
cerv
ical
can
cer
and
scre
enin
gS
cree
nin
gb
ehav
ior
Op
tim
isti
cb
ias
was
fou
nd
(p<
.00
1).
No
rela
tio
nsh
ipb
etw
een
per
ceiv
edri
skan
dsc
reen
ing
inte
nti
on
san
dac
tual
up
take
.N
ore
lati
on
ship
bet
wee
np
erce
ived
risk
and
kno
wle
dg
eab
ou
tce
rvic
alca
nce
ran
dsc
reen
ing
.Co
gn
itiv
ecl
osu
rew
asa
sig
nifi
can
tfa
cto
rin
flu
enci
ng
scre
enin
gb
ehav
ior
(p<
.01)
.
Alt
ho
ug
hp
arti
cip
ants
wer
ea
sele
ctiv
eyo
un
ger
wo
men
sam
ple
,th
isst
ud
yh
igh
ligh
ted
that
wo
men
’sra
tin
go
fre
lati
veri
skse
emed
nei
ther
tog
uid
eb
ehav
ior,
no
rto
be
bas
edo
nre
leva
nt
kno
wle
dg
eab
ou
tce
rvic
alca
nce
ran
dsu
gg
este
dp
sych
olo
gic
alfa
cto
rsin
det
erm
inin
gw
om
en’s
mo
tiva
tio
nto
do
asc
reen
ing
.
10
9.
Fern
and
ezet
al.(
20
09
)U
nit
edS
tate
s
Exp
erim
enta
lst
ud
yu
sin
gan
edu
cati
on
alin
terv
enti
on
Wo
men
50
year
san
do
lder
wh
ow
ere
no
adh
eren
tto
cerv
ical
scre
enin
g
(n=
24
3)
Scr
een
ing
beh
avio
rA
ccu
ltu
rati
on
Per
ceiv
edp
ros
and
con
sP
erce
ived
risk
Sel
f-ef
fica
cy
Scr
een
ing
com
ple
tio
nw
ash
igh
eram
on
gin
terv
enti
on
gro
up
.T
he
inte
rven
tio
nin
crea
sed
cerv
ical
scre
enin
gse
lf-e
ffica
cy,p
erce
ived
ben
efits
,an
dsu
bje
ctiv
en
orm
s,b
ut
itd
idn
ot
chan
ge
scre
enin
gkn
ow
led
ge
and
per
ceiv
edri
sk.
Th
isst
ud
yad
ded
toth
eev
iden
ceco
nce
rnin
gth
eef
fect
iven
ess
of
lay
hea
lth
wo
rker
inte
rven
tio
nfo
rin
crea
sin
gce
rvic
alsc
reen
ing
,bu
tth
ein
terv
enti
on
was
pro
ved
no
tto
infl
uen
cep
erce
ived
susc
epti
bili
tyo
fce
rvic
alca
nce
r,an
dth
est
ud
yd
idn
ot
rep
ort
the
rela
tio
nsh
ipb
etw
een
per
ceiv
edsu
scep
tib
ility
and
scre
enin
gb
ehav
ior.
10
10.
Fort
etal
.(2
011
)M
alaw
i
In-d
epth
inte
rvie
ws
of
wo
men
inru
ral
Mal
awi
(n=
20
)B
arri
ers
toce
rvic
alca
nce
rsc
reen
ing
Maj
or
bar
rier
sto
seek
ing
pre
ven
tati
vesc
reen
ing
incl
ud
edlo
wkn
ow
led
ge
leve
ls,
low
per
ceiv
edsu
scep
tib
ility
,an
dlo
wp
erce
ived
ben
efits
fro
mth
ese
rvic
e.
Th
isst
ud
yre
com
men
ded
that
hea
lth
care
pro
vid
ers
and
hea
lth
edu
cato
rsta
rget
edas
pec
tso
fp
erce
ived
susc
epti
bili
tyam
on
gth
isp
op
ula
tio
n,i
ncl
ud
ing
kno
wle
dg
ele
vels
and
per
son
alri
skas
sess
men
t.
11
11.
Fren
chet
al.
(20
04
)U
nit
edK
ing
do
m
Pro
spec
tive
rese
arch
des
ign
Co
nve
nie
nce
sam
ple
22
6w
om
enw
ith
no
rmal
test
resu
lt18
0 no
n-c
on
secu
tive
inad
equ
ate
test
resu
lts
(n=
40
6)
Per
ceiv
edri
skC
ervi
cal
scre
enin
gre
sult
Wo
men
wit
hin
adeq
uat
esm
ear
test
resu
ltp
erce
ived
hig
her
risk
of
cerv
ical
can
cer
than
wo
men
wit
hn
orm
alte
stre
sult
(p=
.016
).R
ecei
vin
gan
inad
equ
ate
smea
rte
stre
sult
rais
edst
ate
anxi
ety
(p=
.02
5,)
and
con
cern
(p<
.00
1)an
dan
xio
us
wo
men
wer
ele
sslik
ely
toat
ten
dfo
ra
rep
eat
smea
rte
st(p
=.0
11).
Th
isst
ud
yh
igh
ligh
ted
that
info
rmin
gw
om
enw
ho
had
anin
adeq
uat
esm
ear
test
resu
ltw
asas
soci
ated
wit
hra
ised
leve
lo
fp
erce
ived
risk
and
anxi
ety
abo
ut
the
test
.T
he
stu
dy
was
ob
serv
atio
nal
ind
esig
n;
itw
asn
ot
po
ssib
leto
infe
rth
eca
usa
las
soci
atio
ns
bet
wee
nva
riab
les.
11
C. W. H. Chan et al. Risk Perception and Screening Behavior
5
Table
1.C
on
tin
ued
Au
thor
an
dy
ear
Stu
dy
des
ign
an
dpopu
lati
on
Sam
ple
size
Ou
tcom
em
easu
reR
esu
ltC
om
men
tsS
tudy
qu
ality
12.
Gar
cés-
Pal
acio
and
Sca
rin
ci(2
012
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alsu
rvey
Wo
men
wer
e3
0±
6.8
year
so
ldan
dw
ere
mai
nly
fro
mM
exic
o(8
9.2
%)
(n=
74
3)
Per
ceiv
edsu
scep
tib
ility
toce
rvic
alca
nce
ran
dfa
cto
rsas
soci
ated
wit
hp
erce
ived
susc
epti
bili
ty
1.E
du
cati
on
alat
tain
men
t,th
inki
ng
they
may
hav
eb
een
exp
ose
dto
anS
TI
inth
ep
ast,
thin
kin
gth
eym
ayb
eat
risk
of
HP
Vcu
rren
tly,
hav
ing
had
aP
apsm
ear
wit
hin
the
last
year
,an
dh
avin
ga
rela
tive
wit
hca
nce
rw
ere
sig
nifi
can
tly
asso
ciat
edw
ith
per
ceiv
edsu
scep
tib
ility
.2
.G
reat
erkn
ow
led
ge
abo
ut
cerv
ical
can
cer
risk
fact
ors
red
uce
dth
eu
nce
rtai
nty
abo
ut
per
ceiv
edsu
scep
tib
ility
.3
.P
erce
ived
susc
epti
bili
tyto
cerv
ical
can
cer
seem
sto
be
infl
uen
ced
mo
reim
po
rtan
tly
by
the
curr
ent
or
pas
tp
erce
pti
on
of
HP
V/S
TI
exp
osu
re,a
nd
by
hav
ing
are
lati
vew
ith
can
cer.
Th
est
ud
ysh
ow
edth
atp
erce
ived
susc
epti
bili
tyto
cerv
ical
can
cer
seem
edto
be
infl
uen
ced
mo
stly
by
the
curr
ent
or
pas
tp
erce
pti
on
of
HP
V/S
TI
exp
osu
re,a
nd
by
hav
ing
are
lati
vew
ith
can
cer.
Yet
the
qu
esti
on
nai
rew
asse
lf-r
epo
rted
and
may
hav
eb
iase
s.
12
13.
Go
ldm
anan
dR
isic
a(2
00
4)
Un
ited
Sta
tes
Qu
alit
ativ
ere
sear
chd
esig
nu
sin
gfa
ce-t
ofa
cein
terv
iew
Do
min
ican
san
dP
uer
toR
ican
sin
Rh
od
eIs
lan
d(1
8ye
ars
and
old
er)
(n=
147
)P
erce
pti
on
abo
ut
cerv
ical
can
cer
and
scre
enin
g
Cer
vica
lca
nce
rri
sks
wer
em
ost
lyat
trib
ute
dto
care
less
nes
sab
ou
th
ealt
hca
rean
dse
xual
beh
avio
rb
yin
terv
iew
ees.
Ast
ron
gse
nse
of
fata
lism
and
feel
ing
so
fem
bar
rass
men
tco
exis
tw
ith
firm
bel
iefs
abo
ut
the
imp
ort
ance
of
scre
enin
g,a
nd
incr
easi
ng
no
rmal
izat
ion
of
atle
ast
the
idea
of
Pap
test
.
Th
efi
nd
ing
sfr
om
this
qu
alit
ativ
est
ud
yu
nd
ersc
ore
dth
eco
mp
lexi
tyo
fth
eis
sues
con
cern
ing
can
cer
per
cep
tio
ns
and
beh
avio
rs,a
nd
pro
vid
em
ean
ing
and
con
text
that
hel
pex
pla
inso
me
of
the
con
flic
tin
gp
erce
pti
on
s.N
oin
form
atio
nab
ou
tw
om
en’s
per
ceiv
edp
erso
nal
risk
of
cerv
ical
can
cer
was
dis
cuss
edin
this
stu
dy.
12
14.
Gu
etal
.(2
012
)C
hin
a
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
on
ven
ien
cesa
mp
leo
fC
hin
ese
wo
men
(25
–50
year
so
ld)
(n=
167
)P
rote
ctio
nM
oti
vati
on
Th
eory
vari
able
s,kn
ow
led
ge
abo
ut
cerv
ical
can
cer
and
scre
enin
g,
scre
enin
gb
ehav
ior
All
wo
men
con
sid
ered
them
selv
esat
low
risk
of
cerv
ical
can
cer.
No
sig
nifi
can
tas
soci
atio
nw
aso
bse
rved
bet
wee
np
erce
ived
risk
and
pre
vio
us
scre
enin
gb
ehav
ior.
Ap
erce
pti
on
that
visi
tin
gd
oct
ors
reg
ula
rly
isim
po
rtan
tto
hea
lth
,av
erag
ean
dh
igh
leve
lso
fkn
ow
led
ge
abo
ut
cerv
ical
scre
enin
gw
ere
sig
nifi
can
tly
asso
ciat
edw
ith
hav
ing
bee
nre
ceiv
edsc
reen
ing
.
Th
isst
ud
yh
igh
ligh
ted
the
sig
nifi
can
ceo
fkn
ow
led
ge
and
cult
ura
llyre
leva
nt
hea
lth
beh
avio
ran
db
elie
fsab
ou
tce
rvic
alsc
reen
ing
for
Ch
ines
ew
om
enin
det
erm
inin
gsc
reen
ing
beh
avio
r.T
he
use
of
con
ven
ien
cesa
mp
lelim
ited
gen
eral
izin
gth
ese
resu
lts
toth
ew
ho
leC
hin
ese
po
pu
lati
on
.R
epo
rted
exp
erie
nce
sw
ere
retr
osp
ecti
ve,w
hic
hle
aded
tore
call
bia
s.
11
15.
Gu
etal
.(2
013
)C
hin
a
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
on
ven
ien
cesa
mp
leo
fC
hin
ese
wo
men
(25
–50
year
so
ld)
(n=
167
)P
rote
ctio
nM
oti
vati
on
Th
eory
vari
able
s,kn
ow
led
ge
abo
ut
cerv
ical
can
cer
and
scre
enin
g,
Sex
ual
his
tory
,M
oti
vati
on
tore
ceiv
efu
ture
scre
enin
g
Th
em
ajo
rity
of
wo
men
stat
edth
eyin
ten
ded
tore
ceiv
efu
ture
scre
enin
g,a
nd
resp
on
seef
fica
cyw
assi
gn
ifica
ntl
yas
soci
ated
wit
hth
eir
inte
nti
on
.Can
cer
inre
lati
ves,
ap
erce
pti
on
that
visi
tin
ga
do
cto
rre
gu
larl
yis
imp
ort
ant
toh
ealt
h,a
nd
ever
atte
nd
ing
for
cerv
ical
scre
enin
gd
uri
ng
the
pre
vio
us
thre
eye
ars
wer
esi
gn
ifica
ntl
yas
soci
ated
wit
hw
om
en’
mo
tiva
tio
nto
rece
ive
futu
resc
reen
ing
.
Th
isst
ud
yh
igh
ligh
ted
the
imp
ort
ant
role
of
wo
men
’sb
elie
fsin
the
valu
eo
fce
rvic
alsc
reen
ing
and
pre
vio
us
scre
enin
gex
per
ien
cein
mo
tiva
tin
gth
emto
rece
ive
asc
reen
ing
.Wo
men
wer
ere
cru
ited
fro
mfo
ur
wo
rkp
lace
san
dd
idn
ot
hav
eto
pay
for
thei
rsc
reen
ing
,res
ult
ing
ina
bia
sed
sam
ple
.Sm
all
sam
ple
size
was
ano
ther
con
cern
.Th
esu
bse
qu
ent
actu
alu
pta
keo
fsc
reen
ing
was
no
tas
sess
edin
this
stu
dy.
11
16.
Ho
etal
.(2
00
5)
Un
ited
Sta
tes
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
on
ven
ien
cesa
mp
leo
fw
om
en2
0–8
8ye
ars
old
(n=
20
9)
HB
Mva
riab
les
Scr
een
ing
up
take
Per
ceiv
edri
skw
asn
ot
ap
red
icto
ro
fsc
reen
ing
up
take
.P
erce
ived
seve
rity
was
asi
gn
ifica
nt
pre
dic
tor
of
scre
enin
gu
pta
ke.
Th
est
ud
yfo
un
dm
any
sig
nifi
can
tp
red
icto
rso
fP
apte
stan
din
form
edth
efu
ture
stu
dy
toad
dre
ssth
ese
fact
ors
inth
en
ext
adh
eren
cest
ud
y.T
he
dat
aw
ere
colle
cted
by
po
stal
surv
ey,w
hic
hw
asn
ot
valid
ated
;8
6-i
tem
qu
esti
on
nai
rem
ayh
ave
cau
sed
feel
ing
of
tire
dn
ess
and
bo
rin
gfo
rit
was
no
tva
lidat
ed.
11
Risk Perception and Screening Behavior C. W. H. Chan et al.
6
17.
Ho
llow
ayet
al.(
20
03
)U
nit
edK
ing
do
m
Clu
ster
-ran
do
miz
edco
ntr
olle
din
terv
enti
on
rese
arch
;th
ein
terv
enti
on
com
pri
sed
ab
rief
spec
ific
cou
nse
ling
sess
ion
.W
om
enw
ere
recr
uit
edw
hen
atte
nd
ing
for
cerv
ical
scre
enin
g
(n=
1,89
0)
Sh
ort
-ter
mo
utc
om
ew
asst
ated
pre
fere
nce
for
futu
resc
reen
ing
inte
rval
.L
on
g-t
erm
ou
tco
me
was
actu
alsc
reen
ing
beh
avio
rat
4-y
ear
follo
wu
p.
Inte
rven
tio
ng
rou
pw
asle
sslik
ely
toex
pre
ssa
pre
fere
nce
of
ash
ort
erth
anre
com
men
ded
inte
rval
(OR
:.5
19
5%
CI:
.41–
.64
;p<
.00
01)
and
less
likel
yto
atte
nd
for
scre
enin
gso
on
erth
anth
eir
reco
mm
end
edre
call
(5%
hav
ing
sho
rter
than
reco
mm
end
edin
terv
als)
.Th
eim
pac
to
fp
erce
ived
risk
on
actu
alsc
reen
ing
beh
avio
rw
aseq
uiv
oca
l.
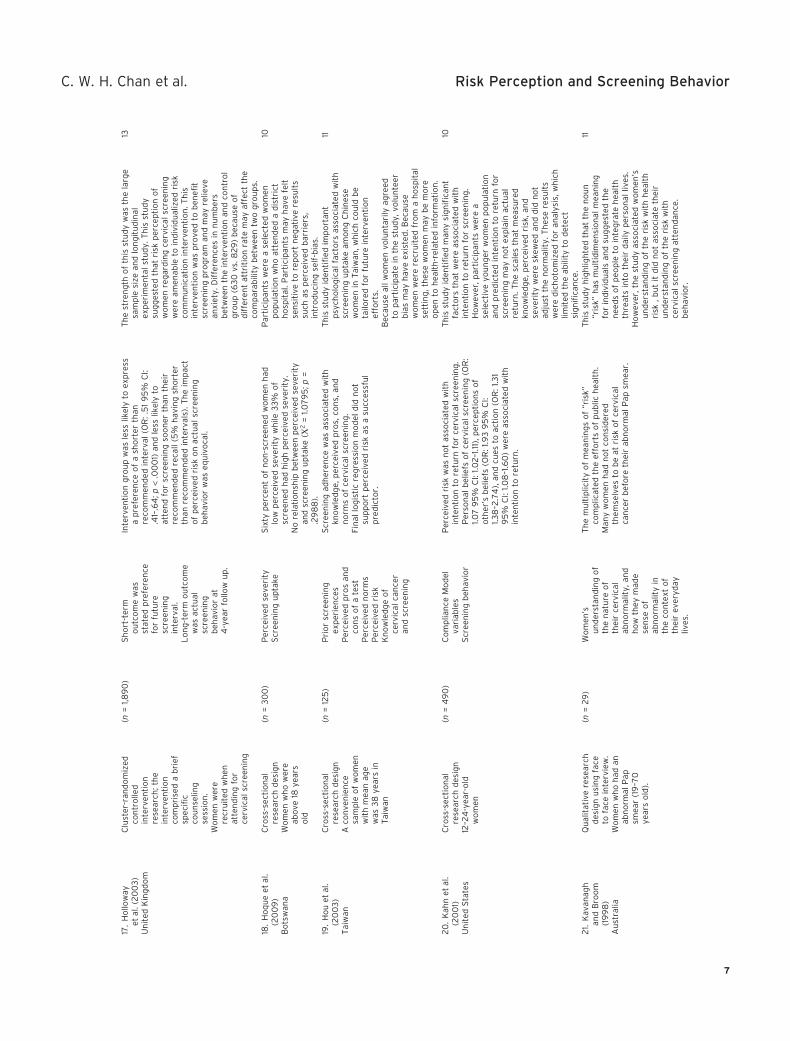
Th
est
ren
gth
of
this
stu
dy
was
the
larg
esa
mp
lesi
zean
dlo
ng
itu
din
alex
per
imen
tal
stu
dy.
Th
isst
ud
ysu
gg
este
dth
atri
skp
erce
pti
on
of
wo
men
reg
ard
ing
cerv
ical
scre
enin
gw
ere
amen
able
toin
div
idu
aliz
edri
skco
mm
un
icat
ion
inte
rven
tio
n.T
his
inte
rven
tio
nw
asp
rove
dto
ben
efit
scre
enin
gp
rog
ram
and
may
relie
vean
xiet
y.D
iffe
ren
ces
inn
um
ber
sb
etw
een
the
inte
rven
tio
nan
dco
ntr
ol
gro
up
(63
0vs
.82
9)
bec
ause
of
dif
fere
nt
attr
itio
nra
tem
ayaf
fect
the
com
par
abili
tyb
etw
een
two
gro
up
s.
13
18.
Ho
qu
eet
al.
(20
09
)B
ots
wan
a
Cro
ss-s
ecti
on
alre
sear
chd
esig
nW
om
enw
ho
wer
eab
ove
18ye
ars
old
(n=
30
0)
Per
ceiv
edse
veri
tyS
cree
nin
gu
pta
keS
ixty
per
cen
to
fn
on
-scr
een
edw
om
enh
adlo
wp
erce
ived
seve
rity
wh
ile3
3%
of
scre
ened
had
hig
hp
erce
ived
seve
rity
.N
ore
lati
on
ship
bet
wee
np
erce
ived
seve
rity
and
scre
enin
gu
pta
ke(Χ
2=
1.07
95
;p=
.29
88
).
Par
tici
pan
tsw
ere
ase
lect
edw
om
enp
op
ula
tio
nw
ho
atte
nd
eda
dis
tric
th
osp
ital
.Par
tici
pan
tsm
ayh
ave
felt
sen
siti
veto
rep
ort
neg
ativ
ere
sult
ssu
chas
per
ceiv
edb
arri
ers,
intr
od
uci
ng
self
-bia
s.
10
19.
Ho
uet
al.
(20
03
)T
aiw
an
Cro
ss-s
ecti
on
alre
sear
chd
esig
nA
con
ven
ien
cesa
mp
leo
fw
om
enw
ith
mea
nag
ew
as3
8ye
ars
inT
aiw
an
(n=
125
)P
rio
rsc
reen
ing
exp
erie
nce
sP
erce
ived
pro
san
dco
ns
of
ate
stP
erce
ived
no
rms
Per
ceiv
edri
skK
no
wle
dg
eo
fce
rvic
alca
nce
ran
dsc
reen
ing
Scr
een
ing
adh
eren
cew
asas
soci
ated
wit
hkn
ow
led
ge,
per
ceiv
edp
ros,
con
s,an
dn
orm
so
fce
rvic
alsc
reen
ing
.Fi
nal
log
isti
cre
gre
ssio
nm
od
eld
idn
ot
sup
po
rtp
erce
ived
risk
asa
succ
essf
ul
pre
dic
tor.
Th
isst
ud
yid
enti
fied
imp
ort
ant
psy
cho
log
ical
fact
ors
asso
ciat
edw
ith
scre
enin
gu
pta
keam
on
gC
hin
ese
wo
men
inT
aiw
an,w
hic
hco
uld
be
tailo
red
for
futu
rein
terv
enti
on
effo
rts.
Bec
ause
all
wo
men
volu
nta
rily
agre
edto
par
tici
pat
ein
the
stu
dy,
volu
nte
erb
ias
may
hav
eex
iste
d.B
ecau
sew
om
enw
ere
recr
uit
edfr
om
ah
osp
ital
sett
ing
,th
ese
wo
men
may
be
mo
reo
pen
toh
ealt
h-r
elat
edin
form
atio
n.
11
20
.K
ahn
etal
.(2
00
1)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
n12
–24
-yea
r-o
ldw
om
en
(n=
49
0)
Co
mp
lian
ceM
od
elva
riab
les
Scr
een
ing
beh
avio
r
Per
ceiv
edri
skw
asn
ot
asso
ciat
edw
ith
inte
nti
on
tore
turn
for
cerv
ical
scre
enin
g.
Per
son
alb
elie
fso
fce
rvic
alsc
reen
ing
(OR
:1.0
79
5%
CI:
1.02
–1.11
),p
erce
pti
on
so
fo
ther
’sb
elie
fs(O
R:1
.93
95
%C
I:1.3
8–2
.74
),an
dcu
esto
acti
on
(OR
:1.3
19
5%
CI:
1.08
–1.6
0)
wer
eas
soci
ated
wit
hin
ten
tio
nto
retu
rn.
Th
isst
ud
yid
enti
fied
man
ysi
gn
ifica
nt
fact
ors
that
wer
eas
soci
ated
wit
hin
ten
tio
nto
retu
rnfo
rsc
reen
ing
.H
ow
ever
,par
tici
pan
tsw
ere
ase
lect
ive
you
ng
erw
om
enp
op
ula
tio
nan
dp
red
icte
din
ten
tio
nto
retu
rnfo
rsc
reen
ing
may
no
tex
pla
inac
tual
retu
rn.T
he
scal
esth
atm
easu
red
kno
wle
dg
e,p
erce
ived
risk
,an
dse
veri
tyw
ere
skew
edan
dd
idn
ot
adju
stth
en
orm
alit
y.T
hes
ere
sult
sw
ere
dic
ho
tom
ized
for
anal
ysis
,wh
ich
limit
edth
eab
ility
tod
etec
tsi
gn
ifica
nce
.
10
21.
Kav
anag
han
dB
roo
m(1
99
8)
Au
stra
lia
Qu
alit
ativ
ere
sear
chd
esig
nu
sin
gfa
ceto
face
inte
rvie
w.
Wo
men
wh
oh
adan
abn
orm
alP
apsm
ear
(19
–70
year
so
ld).
(n=
29
)W
om
en’s
un
der
stan
din
go
fth
en
atu
reo
fth
eir
cerv
ical
abn
orm
alit
y,an
dh
ow
they
mad
ese
nse
of
abn
orm
alit
yin
the
con
text
of
thei
rev
eryd
ayliv
es.
Th
em
ult
iplic
ity
of
mea
nin
gs
of
“ris
k”co
mp
licat
edth
eef
fort
so
fp
ub
lich
ealt
h.
Man
yw
om
enh
adn
ot
con
sid
ered
them
selv
esto
be
atri
sko
fce
rvic
alca
nce
rb
efo
reth
eir
abn
orm
alP
apsm
ear.
Th
isst
ud
yh
igh
ligh
ted
that
the
no
un
“ris
k”h
asm
ult
idim
ensi
on
alm
ean
ing
for
ind
ivid
ual
san
dsu
gg
este
dth
en
eed
so
fp
eop
leto
inte
gra
teh
ealt
hth
reat
sin
toth
eir
dai
lyp
erso
nal
lives
.H
ow
ever
,th
est
ud
yas
soci
ated
wo
men
’su
nd
erst
and
ing
of
the
risk
wit
hh
ealt
hri
sk,b
ut
itd
idn
ot
asso
ciat
eth
eir
un
der
stan
din
go
fth
eri
skw
ith
cerv
ical
scre
enin
gat
ten
dan
ce.
beh
avio
r.
11
C. W. H. Chan et al. Risk Perception and Screening Behavior
7
Table
1.C
on
tin
ued
Au
thor
an
dy
ear
Stu
dy
des
ign
an
dpopu
lati
on
Sam
ple
size
Ou
tcom
em
easu
reR
esu
ltC
om
men
tsS
tudy
qu
ality
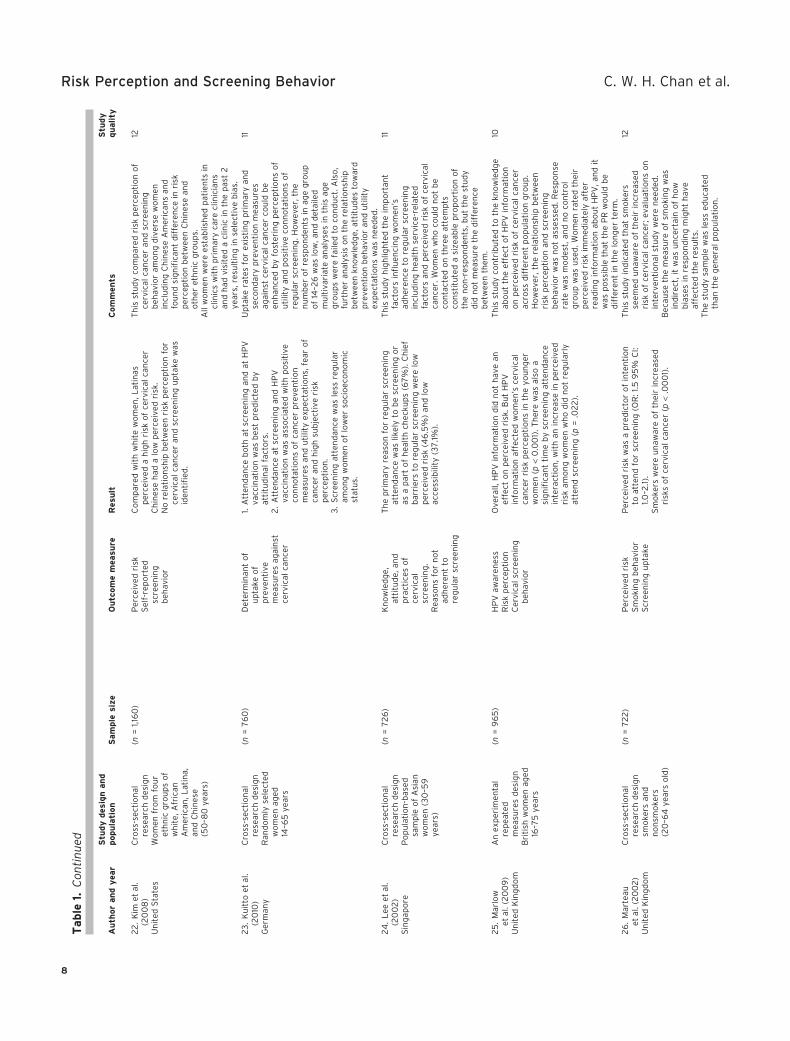
22
.K
imet
al.
(20
08
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
nW
om
enfr
om
fou
ret
hn
icg
rou
ps
of
wh
ite,
Afr
ican
Am
eric
an,L
atin
a,an
dC
hin
ese
(50
–80
year
s)
(n=
1,16
0)
Per
ceiv
edri
skS
elf-
rep
ort
edsc
reen
ing
beh
avio
r
Co
mp
ared
wit
hw
hit
ew
om
en,L
atin
asp
erce
ived
ah
igh
risk
of
cerv
ical
can
cer
Ch
ines
eh
ada
low
per
ceiv
edri
sk.
No
rela
tio
nsh
ipb
etw
een
risk
per
cep
tio
nfo
rce
rvic
alca
nce
ran
dsc
reen
ing
up
take
was
iden
tifi
ed.
Th
isst
ud
yco
mp
ared
risk
per
cep
tio
no
fce
rvic
alca
nce
ran
dsc
reen
ing
beh
avio
ram
on
gd
iver
sew
om
enin
clu
din
gC
hin
ese
Am
eric
ans
and
fou
nd
sig
nifi
can
td
iffe
ren
cein
risk
per
cep
tio
nb
etw
een
Ch
ines
ean
do
ther
eth
nic
gro
up
s.A
llw
om
enw
ere
esta
blis
hed
pat
ien
tsin
clin
ics
wit
hp
rim
ary
care
clin
icia
ns
and
had
visi
ted
acl
inic
inth
ep
ast
2ye
ars,
resu
ltin
gin
sele
ctiv
eb
ias.
12
23
.K
uit
toet
al.
(20
10)
Ger
man
y
Cro
ss-s
ecti
on
alre
sear
chd
esig
nR
and
om
lyse
lect
edw
om
enag
ed14
–65
year
s
(n=
76
0)
Det
erm
inan
to
fu
pta
keo
fp
reve
nti
vem
easu
res
agai
nst
cerv
ical
can
cer
1.A
tten
dan
ceb
oth
atsc
reen
ing
and
atH
PV
vacc
inat
ion
was
bes
tp
red
icte
db
yat
titu
din
alfa
cto
rs.
2.
Att
end
ance
atsc
reen
ing
and
HP
Vva
ccin
atio
nw
asas
soci
ated
wit
hp
osi
tive
con
no
tati
on
so
fca
nce
rp
reve
nti
on
mea
sure
san
du
tilit
yex
pec
tati
on
s,fe
aro
fca
nce
ran
dh
igh
sub
ject
ive
risk
per
cep
tio
n.
3.
Scr
een
ing
atte
nd
ance
was
less
reg
ula
ram
on
gw
om
eno
flo
wer
soci
oec
on
om
icst
atu
s.
Up
take
rate
sfo
rex
isti
ng
pri
mar
yan
dse
con
dar
yp
reve
nti
on
mea
sure
sag
ain
stce
rvic
alca
nce
rco
uld
be
enh
ance
db
yfo
ster
ing
per
cep
tio
ns
of
uti
lity
and
po
siti
veco
nn
ota
tio
ns
of
reg
ula
rsc
reen
ing
.Ho
wev
er,t
he
nu
mb
ero
fre
spo
nd
ents
inag
eg
rou
po
f14
–26
was
low
,an
dd
etai
led
mu
ltiv
aria
tean
alys
esin
this
age
gro
up
sw
ere
faile
dto
con
du
ct.A
lso
,fu
rth
eran
alys
iso
nth
ere
lati
on
ship
bet
wee
nkn
ow
led
ge,
atti
tud
esto
war
dp
reve
nti
on
beh
avio
ran
du
tilit
yex
pec
tati
on
sw
asn
eed
ed.
11
24
.L
eeet
al.
(20
02
)S
ing
apo
re
Cro
ss-s
ecti
on
alre
sear
chd
esig
nP
op
ula
tio
n-b
ased
sam
ple
of
Asi
anw
om
en(3
0–5
9ye
ars)
(n=
72
6)
Kn
ow
led
ge,
atti
tud
e,an
dp
ract
ices
of
cerv
ical
scre
enin
g.
Rea
son
sfo
rn
ot
adh
eren
tto
reg
ula
rsc
reen
ing
Th
ep
rim
ary
reas
on
for
reg
ula
rsc
reen
ing
atte
nd
ance
was
likel
yto
be
scre
enin
go
ras
ap
art
of
hea
lth
chec
kup
s(6
7%
).C
hie
fb
arri
ers
tore
gu
lar
scre
enin
gw
ere
low
per
ceiv
edri
sk(4
6.5
%)
and
low
acce
ssib
ility
(37
.1%).
Th
isst
ud
yh
igh
ligh
ted
the
imp
ort
ant
fact
ors
infl
uen
cin
gw
om
en’s
adh
eren
ceto
reg
ula
rsc
reen
ing
incl
ud
ing
hea
lth
serv
ice-
rela
ted
fact
ors
and
per
ceiv
edri
sko
fce
rvic
alca
nce
r.W
om
enw
ho
cou
ldn
ot
be
con
tact
edo
nth
ree
atte
mp
tsco
nst
itu
ted
asi
zeab
lep
rop
ort
ion
of
the
no
n-r
esp
on
den
ts,b
ut
the
stu
dy
did
no
tm
easu
reth
ed
iffe
ren
ceb
etw
een
them
.
11
25
.M
arlo
wet
al.(
20
09
)U
nit
edK
ing
do
m
An
exp
erim
enta
lre
pea
ted
mea
sure
sd
esig
nB
riti
shw
om
enag
ed16
–75
year
s
(n=
96
5)
HP
Vaw
aren
ess
Ris
kp
erce
pti
on
Cer
vica
lsc
reen
ing
beh
avio
r
Ove
rall,
HP
Vin
form
atio
nd
idn
ot
hav
ean
effe
cto
np
erce
ived
risk
.Bu
tH
PV
info
rmat
ion
affe
cted
wo
men
’sce
rvic
alca
nce
rri
skp
erce
pti
on
sin
the
you
ng
erw
om
en(p
<0
.00
1).T
her
ew
asal
soa
sig
nifi
can
tti
me
by
scre
enin
gat
ten
dan
cein
tera
ctio
n,w
ith
anin
crea
sein
per
ceiv
edri
skam
on
gw
om
enw
ho
did
no
tre
gu
larl
yat
ten
dsc
reen
ing
(p=
.02
2).
Th
isst
ud
yco
ntr
ibu
ted
toth
ekn
ow
led
ge
abo
ut
the
effe
cto
fH
PV
info
rmat
ion
on
per
ceiv
edri
sko
fce
rvic
alca
nce
rac
ross
dif
fere
nt
po
pu
lati
on
gro
up
.H
ow
ever
,th
ere
lati
on
ship
bet
wee
nri
skp
erce
pti
on
and
scre
enin
gb
ehav
ior
was
no
tas
sess
ed.R
esp
on
sera
tew
asm
od
est,
and
no
con
tro
lg
rou
pw
asu
sed
.Wo
men
rate
dth
eir
per
ceiv
edri
skim
med
iate
lyaf
ter
read
ing
info
rmat
ion
abo
ut
HP
V,a
nd
itw
asp
oss
ible
that
the
PR
wo
uld
be
dif
fere
nt
inth
elo
ng
erte
rm.
10
26
.M
arte
auet
al.(
20
02
)U
nit
edK
ing
do
m
Cro
ss-s
ecti
on
alre
sear
chd
esig
nsm
oke
rsan
dn
on
smo
kers
(20
–64
year
so
ld)
(n=
72
2)
Per
ceiv
edri
skS
mo
kin
gb
ehav
ior
Scr
een
ing
up
take
Per
ceiv
edri
skw
asa
pre
dic
tor
of
inte
nti
on
toat
ten
dfo
rsc
reen
ing
(OR
:1.5
95
%C
I:1.0
–2.1)
.S
mo
kers
wer
eu
naw
are
of
thei
rin
crea
sed
risk
so
fce
rvic
alca
nce
r(p
<.0
00
1).
Th
isst
ud
yin
dic
ated
that
smo
kers
seem
edu
naw
are
of
thei
rin
crea
sed
risk
of
cerv
ical
can
cer;
eval
uat
ion
so
nin
terv
enti
on
alst
ud
yw
ere
nee
ded
.B
ecau
seth
em
easu
reo
fsm
oki
ng
was
ind
irec
t,it
was
un
cert
ain
of
ho
wb
iase
sin
resp
on
din
gm
igh
th
ave
affe
cted
the
resu
lts.
Th
est
ud
ysa
mp
lew
asle
ssed
uca
ted
than
the
gen
eral
po
pu
lati
on
.
12
Risk Perception and Screening Behavior C. W. H. Chan et al.
8
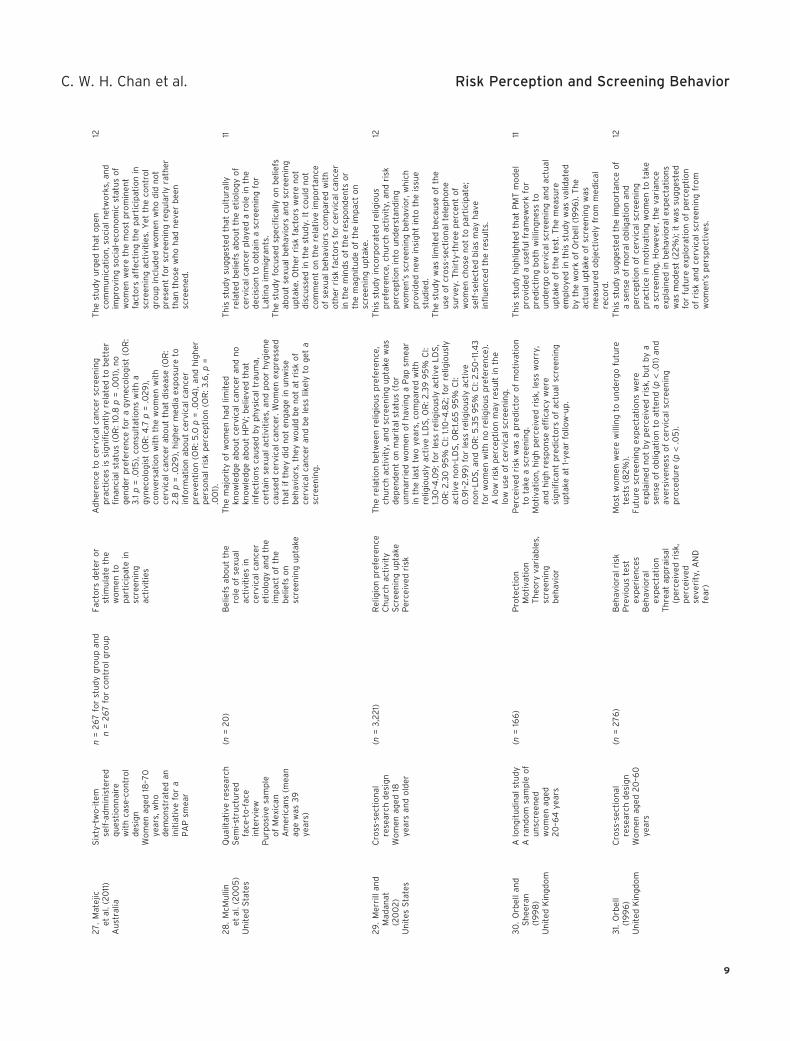
27
.M
atej
icet
al.(
20
11)
Au
stra
lia
Six
ty-t
wo
-ite
mse
lf-a
dm
inis
tere
dq
ues
tio
nn
aire
wit
hca
se-c
on
tro
ld
esig
nW
om
enag
ed18
–70
year
s,w
ho
dem
on
stra
ted
anin
itia
tive
for
aP
AP
smea
r
n=
26
7fo
rst
ud
yg
rou
pan
dn
=2
67
for
con
tro
lg
rou
pFa
cto
rsd
eter
or
stim
ula
teth
ew
om
ento
par
tici
pat
ein
scre
enin
gac
tivi
ties
Ad
her
ence
toce
rvic
alca
nce
rsc
reen
ing
pra
ctic
esis
sig
nifi
can
tly
rela
ted
tob
ette
rfi
nan
cial
stat
us
(OR
:10
.8p
=.0
01)
,no
gen
der
pre
fere
nce
for
ag
ynec
olo
gis
t(O
R:
3.1
p=
.015
),co
nsu
ltat
ion
sw
ith
ag
ynec
olo
gis
t(O
R:4
.7p
=.0
29
),co
nve
rsat
ion
wit
hth
ew
om
enw
ith
cerv
ical
can
cer
abo
ut
that
dis
ease
(OR
:2
.8p
=.0
29
),h
igh
erm
edia
exp
osu
reto
info
rmat
ion
abo
ut
cerv
ical
can
cer
pre
ven
tio
n(O
R:5
.0p
=.0
04
),an
dh
igh
erp
erso
nal
risk
per
cep
tio
n(O
R:3
.6,p
=.0
01)
.
Th
est
ud
yu
rged
that
op
enco
mm
un
icat
ion
,so
cial
net
wo
rks,
and
imp
rovi
ng
soci
al-e
con
om
icst
atu
so
fw
om
enw
ere
the
mo
stp
rom
inen
tfa
cto
rsaf
fect
ing
the
par
tici
pat
ion
insc
reen
ing
acti
viti
es.Y
etth
eco
ntr
ol
gro
up
incl
ud
edw
om
enw
ho
did
no
tp
rese
nt
for
scre
enin
gre
gu
larl
yra
ther
than
tho
sew
ho
had
nev
erb
een
scre
ened
.
12
28
.M
cMu
llin
etal
.(2
00
5)
Un
ited
Sta
tes
Qu
alit
ativ
ere
sear
chS
emi-
stru
ctu
red
face
-to
-fac
ein
terv
iew
Pu
rpo
sive
sam
ple
of
Mex
ican
Am
eric
ans
(mea
nag
ew
as3
9ye
ars)
(n=
20
)B
elie
fsab
ou
tth
ero
leo
fse
xual
acti
viti
esin
cerv
ical
can
cer
etio
log
yan
dth
eim
pac
to
fth
eb
elie
fso
nsc
reen
ing
up
take
Th
em
ajo
rity
of
wo
men
had
limit
edkn
ow
led
ge
abo
ut
cerv
ical
can
cer
and
no
kno
wle
dg
eab
ou
tH
PV
;bel
ieve
dth
atin
fect
ion
sca
use
db
yp
hys
ical
trau
ma,
cert
ain
sexu
alac
tivi
ties
,an
dp
oo
rh
ygie
ne
cau
sed
cerv
ical
can
cer.
Wo
men
exp
ress
edth
atif
they
did
no
ten
gag
ein
un
wis
eb
ehav
iors
,th
eyw
ou
ldb
en
ot
atri
sko
fce
rvic
alca
nce
ran
db
ele
sslik
ely
tog
eta
scre
enin
g.
Th
isst
ud
ysu
gg
este
dth
atcu
ltu
rally
rela
ted
bel
iefs
abo
ut
the
etio
log
yo
fce
rvic
alca
nce
rp
laye
da
role
inth
ed
ecis
ion
too
bta
ina
scre
enin
gfo
rL
atin
aim
mig
ran
ts.
Th
est
ud
yfo
cuse
dsp
ecifi
cally
on
bel
iefs
abo
ut
sexu
alb
ehav
iors
and
scre
enin
gu
pta
ke.O
ther
risk
fact
ors
wer
en
ot
dis
cuss
edin
the
stu
dy.
Itco
uld
no
tco
mm
ent
on
the
rela
tive
imp
ort
ance
of
sexu
alb
ehav
iors
com
par
edw
ith
oth
erri
skfa
cto
rsfo
rce
rvic
alca
nce
rin
the
min
ds
of
the
resp
on
den
tso
rth
em
agn
itu
de
of
the
imp
act
on
scre
enin
gu
pta
ke.
11
29
.M
erri
llan
dM
adan
at(2
00
2)
Un
ites
Sta
tes
Cro
ss-s
ecti
on
alre
sear
chd
esig
nW
om
enag
ed18
year
san
do
lder
(n=
3,2
21)
Rel
igio
np
refe
ren
ceC
hu
rch
acti
vity
Scr
een
ing
up
take
Per
ceiv
edri
sk
Th
ere
lati
on
bet
wee
nre
ligio
us
pre
fere
nce
,ch
urc
hac
tivi
ty,a
nd
scre
enin
gu
pta
kew
asd
epen
den
to
nm
arit
alst
atu
s(f
or
un
mar
ried
wo
men
of
hav
ing
aP
apsm
ear
inth
ela
sttw
oye
ars,
com
par
edw
ith
relig
iou
sly
acti
veL
DS
,OR
:2.3
99
5%
CI:
1.30
–4.0
9;f
or
less
relig
iou
sly
acti
veL
DS
,O
R:2
.30
95
%C
I:1.1
0–4
.82
;fo
rre
ligio
usl
yac
tive
no
n-L
DS
,OR
:1.6
59
5%
CI:
0.9
1–2
.99
)fo
rle
ssre
ligio
usl
yac
tive
no
n-L
DS
,an
dO
R:5
.35
95
%C
I:2
.50
–11.4
3fo
rw
om
enw
ith
no
relig
iou
sp
refe
ren
ce).
Alo
wri
skp
erce
pti
on
may
resu
ltin
the
low
use
of
cerv
ical
scre
enin
g.
Th
isst
ud
yin
corp
ora
ted
relig
iou
sp
refe
ren
ce,c
hu
rch
acti
vity
,an
dri
skp
erce
pti
on
into
un
der
stan
din
gw
om
en’s
scre
enin
gb
ehav
ior,
wh
ich
pro
vid
edn
ewin
sig
ht
into
the
issu
est
ud
ied
.T
he
stu
dy
was
limit
edb
ecau
seo
fth
eu
seo
fcr
oss
-sec
tio
nal
tele
ph
on
esu
rvey
.Th
irty
-th
ree
per
cen
to
fw
om
ench
ose
no
tto
par
tici
pat
e;se
lf-s
elec
ted
bia
sm
ayh
ave
infl
uen
ced
the
resu
lts.
12
30
.O
rbel
lan
dS
hee
ran
(19
98
)U
nit
edK
ing
do
m
Alo
ng
itu
din
alst
ud
yA
ran
do
msa
mp
leo
fu
nsc
reen
edw
om
enag
ed2
0–6
4ye
ars
(n=
166
)P
rote
ctio
nM
oti
vati
on
Th
eory
vari
able
s,sc
reen
ing
beh
avio
r
Per
ceiv
edri
skw
asa
pre
dic
tor
of
mo
tiva
tio
nto
take
asc
reen
ing
.M
oti
vati
on
,hig
hp
erce
ived
risk
,les
sw
orr
y,an
dh
igh
resp
on
seef
fica
cyw
ere
sig
nifi
can
tp
red
icto
rso
fac
tual
scre
enin
gu
pta
keat
1-ye
arfo
llow
-up
.
Th
isst
ud
yh
igh
ligh
ted
that
PM
Tm
od
elp
rovi
ded
au
sefu
lfr
amew
ork
for
pre
dic
tin
gb
oth
will
ing
nes
sto
un
der
go
cerv
ical
scre
enin
gan
dac
tual
up
take
of
the
test
.Th
em
easu
reem
plo
yed
inth
isst
ud
yw
asva
lidat
edb
yth
ew
ork
of
Orb
ell
(19
96
).T
he
actu
alu
pta
keo
fsc
reen
ing
was
mea
sure
do
bje
ctiv
ely
fro
mm
edic
alre
cord
.
11
31.
Orb
ell
(19
96
)U
nit
edK
ing
do
m
Cro
ss-s
ecti
on
alre
sear
chd
esig
nW
om
enag
ed2
0–6
0ye
ars
(n=
27
6)
Beh
avio
ral
risk
Pre
vio
us
test
exp
erie
nce
sB
ehav
iora
lex
pec
tati
on
Th
reat
app
rais
al(p
erce
ived
risk
,p
erce
ived
seve
rity
,AN
Dfe
ar)
Mo
stw
om
enw
ere
will
ing
tou
nd
erg
ofu
ture
test
s(8
2%
).Fu
ture
scre
enin
gex
pec
tati
on
sw
ere
exp
lain
edn
ot
by
per
ceiv
edri
sk,b
ut
by
ase
nse
of
ob
ligat
ion
toat
ten
d(p
<.0
1)an
dav
ersi
ven
ess
of
cerv
ical
scre
enin
gp
roce
du
re(p
<.0
5).
Th
isst
ud
ysu
gg
este
dth
eim
po
rtan
ceo
fa
sen
seo
fm
ora
lo
blig
atio
nan
dp
erce
pti
on
of
cerv
ical
scre
enin
gp
ract
ice
inm
oti
vati
ng
wo
men
tota
kea
scre
enin
g.H
ow
ever
,th
eva
rian
ceex
pla
ined
inb
ehav
iora
lex
pec
tati
on
sw
asm
od
est
(22
%);
itw
assu
gg
este
dfo
rfu
ture
exp
lora
tio
no
fp
erce
pti
on
of
risk
and
cerv
ical
scre
enin
gfr
om
wo
men
’sp
ersp
ecti
ves.
12
C. W. H. Chan et al. Risk Perception and Screening Behavior
9
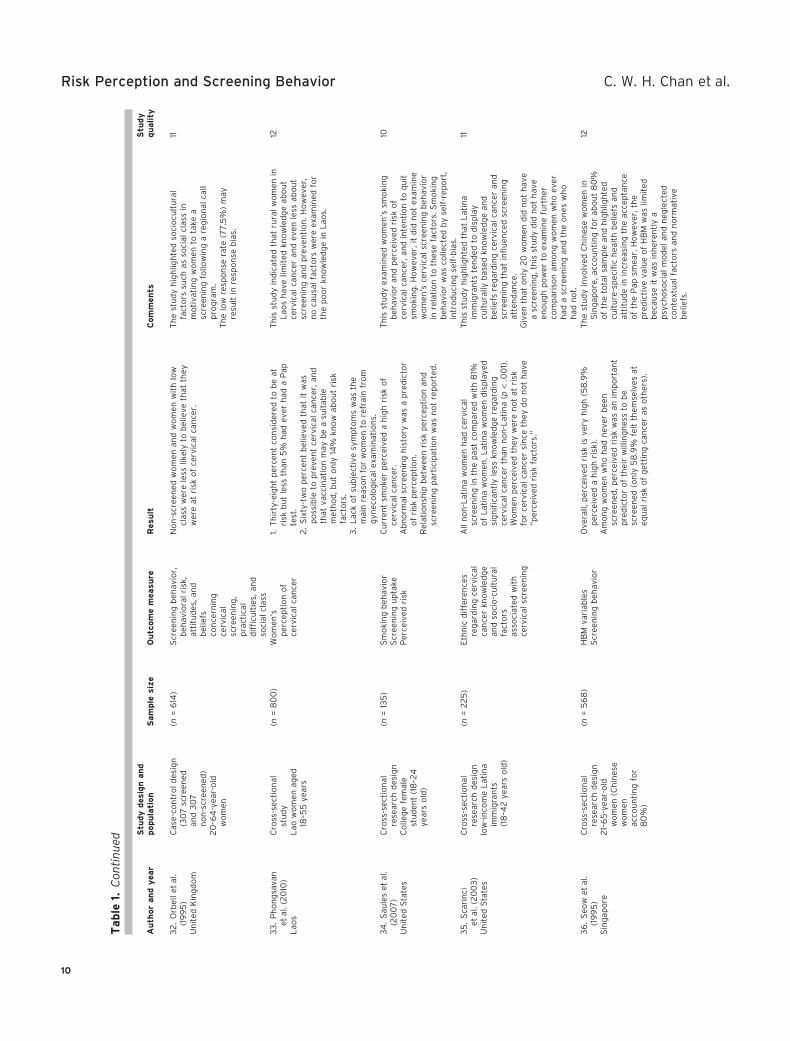
Table
1.C
on
tin
ued
Au
thor
an
dy
ear
Stu
dy
des
ign
an
dpopu
lati
on
Sam
ple
size
Ou
tcom
em
easu
reR
esu
ltC
om
men
tsS
tudy
qu
ality
32
.O
rbel
let
al.
(19
95
)U
nit
edK
ing
do
m
Cas
e-co
ntr
ol
des
ign
(30
7sc
reen
edan
d3
07
no
n-s
cree
ned
)2
0–6
4-y
ear-
old
wo
men
(n=
614
)S
cree
nin
gb
ehav
ior,
beh
avio
ral
risk
,at
titu
des
,an
db
elie
fsco
nce
rnin
gce
rvic
alsc
reen
ing
,p
ract
ical
dif
ficu
ltie
s,an
dso
cial
clas
s
No
n-s
cree
ned
wo
men
and
wo
men
wit
hlo
wcl
ass
wer
ele
sslik
ely
tob
elie
veth
atth
eyw
ere
atri
sko
fce
rvic
alca
nce
r.
Th
est
ud
yh
igh
ligh
ted
soci
ocu
ltu
ral
fact
ors
such
asso
cial
clas
sin
mo
tiva
tin
gw
om
ento
take
asc
reen
ing
follo
win
ga
reg
ion
alca
llp
rog
ram
.T
he
low
resp
on
sera
te(7
7.5
%)
may
resu
ltin
resp
on
seb
ias.
11
33
.P
ho
ng
sava
net
al.(
20
10)
Lao
s
Cro
ss-s
ecti
on
alst
ud
yL
aow
om
enag
ed18
–55
year
s
(n=
80
0)
Wo
men
’sp
erce
pti
on
of
cerv
ical
can
cer
1.T
hir
ty-e
igh
tp
erce
nt
con
sid
ered
tob
eat
risk
bu
tle
ssth
an5
%h
adev
erh
ada
Pap
test
.2
.S
ixty
-tw
op
erce
nt
bel
ieve
dth
atit
was
po
ssib
leto
pre
ven
tce
rvic
alca
nce
r,an
dth
atva
ccin
atio
nm
ayb
ea
suit
able
met
ho
d,b
ut
on
ly14
%kn
ow
abo
ut
risk
fact
ors
.3
.L
ack
of
sub
ject
ive
sym
pto
ms
was
the
mai
nre
aso
nfo
rw
om
ento
refr
ain
fro
mg
ynec
olo
gic
alex
amin
atio
ns.
Th
isst
ud
yin
dic
ated
that
rura
lw
om
enin
Lao
sh
ave
limit
edkn
ow
led
ge
abo
ut
cerv
ical
can
cer
and
even
less
abo
ut
scre
enin
gan
dp
reve
nti
on
.Ho
wev
er,
no
cau
sal
fact
ors
wer
eex
amin
edfo
rth
ep
oo
rkn
ow
led
ge
inL
aos.
12
34
.S
aule
set
al.
(20
07
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
nC
olle
ge
fem
ale
stu
den
t(1
8–2
4ye
ars
old
)
(n=
135
)S
mo
kin
gb
ehav
ior
Scr
een
ing
up
take
Per
ceiv
edri
sk
Cu
rren
tsm
oke
rp
erce
ived
ah
igh
risk
of
cerv
ical
can
cer.
Ab
no
rmal
scre
enin
gh
isto
ryw
asa
pre
dic
tor
of
risk
per
cep
tio
n.
Rel
atio
nsh
ipb
etw
een
risk
per
cep
tio
nan
dsc
reen
ing
par
tici
pat
ion
was
no
tre
po
rted
.
Th
isst
ud
yex
amin
edw
om
en’s
smo
kin
gb
ehav
ior
and
per
ceiv
edri
sko
fce
rvic
alca
nce
r,an
din
ten
tio
nto
qu
itsm
oki
ng
.Ho
wev
er,i
td
idn
ot
exam
ine
wo
men
’sce
rvic
alsc
reen
ing
beh
avio
rin
rela
tio
nto
thes
efa
cto
rs.S
mo
kin
gb
ehav
ior
was
colle
cted
by
self
-rep
ort
,in
tro
du
cin
gse
lf-b
ias.
10
35
.S
cari
nci
etal
.(2
00
3)
Un
ited
Sta
tes
Cro
ss-s
ecti
on
alre
sear
chd
esig
nlo
w-i
nco
me
Lat
ina
imm
igra
nts
(18
–42
year
so
ld)
(n=
22
5)
Eth
nic
dif
fere
nce
sre
gar
din
gce
rvic
alca
nce
rkn
ow
led
ge
and
soci
o-c
ult
ura
lfa
cto
rsas
soci
ated
wit
hce
rvic
alsc
reen
ing
All
no
n-L
atin
aw
om
enh
adce
rvic
alsc
reen
ing
inth
ep
ast
com
par
edw
ith
81%
of
Lat
ina
wo
men
.Lat
ina
wo
men
dis
pla
yed
sig
nifi
can
tly
less
kno
wle
dg
ere
gar
din
gce
rvic
alca
nce
rth
ann
on
-Lat
ina
(p<
.00
1).
Wo
men
per
ceiv
edth
eyw
ere
no
tat
risk
for
cerv
ical
can
cer
sin
ceth
eyd
on
ot
hav
e“p
erce
ived
risk
fact
ors
.”
Th
isst
ud
yh
igh
ligh
ted
that
Lat
ina
imm
igra
nts
ten
ded
tod
isp
lay
cult
ura
llyb
ased
kno
wle
dg
ean
db
elie
fsre
gar
din
gce
rvic
alca
nce
ran
dsc
reen
ing
that
infl
uen
ced
scre
enin
gat
ten
dan
ce.
Giv
enth
ato
nly
20
wo
men
did
no
th
ave
asc
reen
ing
,th
isst
ud
yd
idn
ot
hav
een
ou
gh
po
wer
toex
amin
efu
rth
erco
mp
aris
on
amo
ng
wo
men
wh
oev
erh
ada
scre
enin
gan
dth
eo
nes
wh
oh
adn
ot.
11
36
.S
eow
etal
.(1
99
5)
Sin
gap
ore
Cro
ss-s
ecti
on
alre
sear
chd
esig
n2
1–6
5-y
ear-
old
wo
men
(Ch
ines
ew
om
enac
cou
nti
ng
for
80
%)
(n=
56
8)
HB
Mva
riab
les
Scr
een
ing
beh
avio
rO
vera
ll,p
erce
ived
risk
isve
ryh
igh
(58
.9%
per
ceiv
eda
hig
hri
sk).
Am
on
gw
om
enw
ho
had
nev
erb
een
scre
ened
,per
ceiv
edri
skw
asan
imp
ort
ant
pre
dic
tor
of
thei
rw
illin
gn
ess
tob
esc
reen
ed(o
nly
58
.9%
felt
them
selv
esat
equ
alri
sko
fg
etti
ng
can
cer
aso
ther
s).
Th
est
ud
yin
volv
edC
hin
ese
wo
men
inS
ing
apo
re,a
cco
un
tin
gfo
rab
ou
t8
0%
of
the
tota
lsa
mp
lean
dh
igh
ligh
ted
cult
ure
-sp
ecifi
ch
ealt
hb
elie
fsan
dat
titu
de
inin
crea
sin
gth
eac
cep
tan
ceo
fth
eP
apsm
ear.
Ho
wev
er,t
he
pre
dic
tive
valu
eo
fH
BM
was
limit
edb
ecau
seit
was
inh
eren
tly
ap
sych
oso
cial
mo
del
and
neg
lect
edco
nte
xtu
alfa
cto
rsan
dn
orm
ativ
eb
elie
fs.
12
Risk Perception and Screening Behavior C. W. H. Chan et al.
10
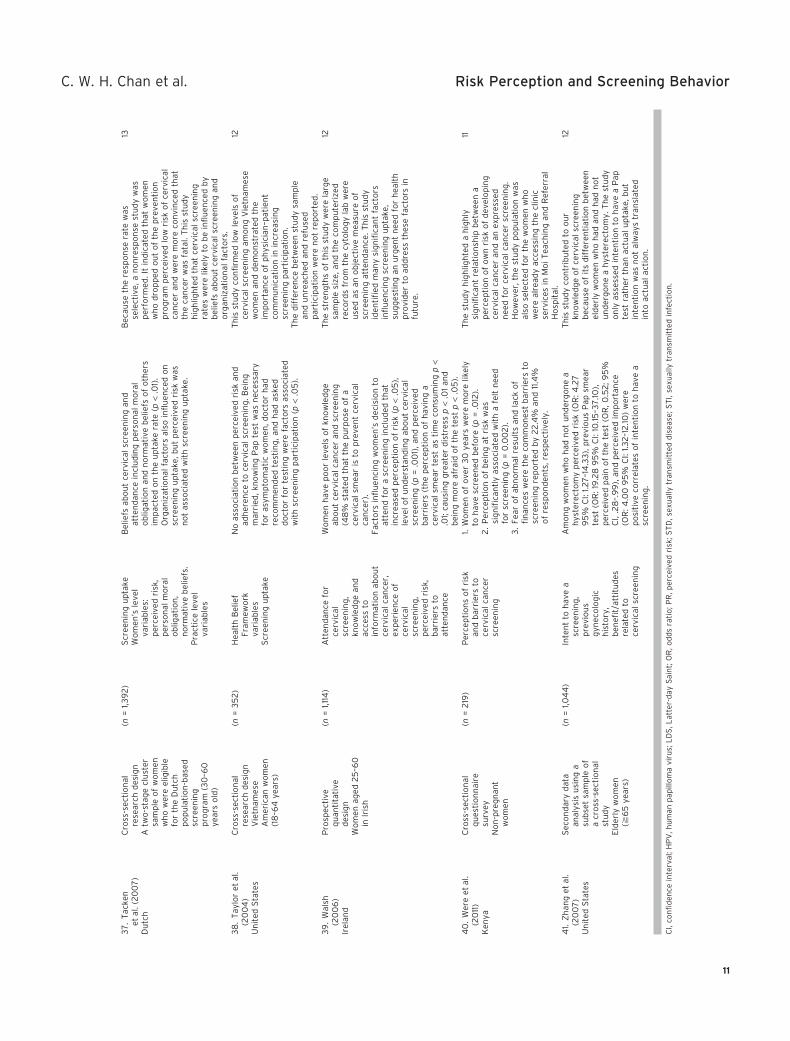
37
.T
acke
net
al.(
20
07
)D
utc
h
Cro
ss-s
ecti
on
alre
sear
chd
esig
nA
two
-sta
ge
clu
ster
sam
ple
of
wo
men
wh
ow
ere
elig
ible
for
the
Du
tch
po
pu
lati
on
-bas
edsc
reen
ing
pro
gra
m(3
0–6
0ye
ars
old
)
(n=
1,39
2)
Scr
een
ing
up
take
Wo
men
’sle
vel
vari
able
s:p
erce
ived
risk
,p
erso
nal
mo
ral
ob
ligat
ion
,n
orm
ativ
eb
elie
fs.
Pra
ctic
ele
vel
vari
able
s
Bel
iefs
abo
ut
cerv
ical
scre
enin
gan
dat
ten
dan
cein
clu
din
gp
erso
nal
mo
ral
ob
ligat
ion
and
no
rmat
ive
bel
iefs
of
oth
ers
imp
acte
do
nth
eu
pta
kera
te(p
<.0
1).
Org
aniz
atio
nal
fact
ors
also
infl
uen
ced
on
scre
enin
gu
pta
ke,b
ut
per
ceiv
edri
skw
asn
ot
asso
ciat
edw
ith
scre
enin
gu
pta
ke.
Bec
ause
the
resp
on
sera
tew
asse
lect
ive,
an
on
resp
on
sest
ud
yw
asp
erfo
rmed
.It
ind
icat
edth
atw
om
enw
ho
dro
pp
edo
ut
of
the
pre
ven
tio
np
rog
ram
per
ceiv
edlo
wri
sko
fce
rvic
alca
nce
ran
dw
ere
mo
reco
nvi
nce
dth
atth
eca
nce
rw
asfa
tal.
Th
isst
ud
yh
igh
ligh
ted
that
cerv
ical
scre
enin
gra
tes
wer
elik
ely
tob
ein
flu
ence
db
yb
elie
fsab
ou
tce
rvic
alsc
reen
ing
and
org
aniz
atio
nal
fact
ors
.
13
38
.T
aylo
ret
al.
(20
04
)U
nit
edS
tate
s
Cro
ss-s
ecti
on
alre
sear
chd
esig
nV
ietn
ames
eA
mer
ican
wo
men
(18
–64
year
s)
(n=
35
2)
Hea
lth
Bel
ief
Fram
ewo
rkva
riab
les
Scr
een
ing
up
take
No
asso
ciat
ion
bet
wee
np
erce
ived
risk
and
adh
eren
ceto
cerv
ical
scre
enin
g.B
ein
gm
arri
ed,k
no
win
gP
apte
stw
asn
eces
sary
for
asym
pto
mat
icw
om
en,d
oct
or
had
reco
mm
end
edte
stin
g,a
nd
had
aske
dd
oct
or
for
test
ing
wer
efa
cto
rsas
soci
ated
wit
hsc
reen
ing
par
tici
pat
ion
(p<
.05
).
Th
isst
ud
yco
nfi
rmed
low
leve
lso
fce
rvic
alsc
reen
ing
amo
ng
Vie
tnam
ese
wo
men
and
dem
on
stra
ted
the
imp
ort
ance
of
ph
ysic
ian
–pat
ien
tco
mm
un
icat
ion
inin
crea
sin
gsc
reen
ing
par
tici
pat
ion
.T
he
dif
fere
nce
bet
wee
nst
ud
ysa
mp
lean
du
nre
ach
edan
dre
fuse
dp
arti
cip
atio
nw
ere
no
tre
po
rted
.
12
39
.W
alsh
(20
06
)Ir
elan
d
Pro
spec
tive
qu
anti
tati
ved
esig
nW
om
enag
ed2
5–6
0in
Iris
h
(n=
1,114
)A
tten
dan
cefo
rce
rvic
alsc
reen
ing
,kn
ow
led
ge
and
acce
ssto
info
rmat
ion
abo
ut
cerv
ical
can
cer,
exp
erie
nce
of
cerv
ical
scre
enin
g,
per
ceiv
edri
sk,
bar
rier
sto
atte
nd
ance
Wo
men
hav
ep
oo
rle
vels
of
kno
wle
dg
eab
ou
tce
rvic
alca
nce
ran
dsc
reen
ing
(48
%st
ated
that
the
pu
rpo
seo
fa
cerv
ical
smea
ris
top
reve
nt
cerv
ical
can
cer)
.Fa
cto
rsin
flu
enci
ng
wo
men
’sd
ecis
ion
toat
ten
dfo
ra
scre
enin
gin
clu
ded
that
incr
ease
dp
erce
pti
on
of
risk
(p<
.05
),le
vel
of
un
der
stan
din
gab
ou
tce
rvic
alsc
reen
ing
(p=
.00
1),a
nd
per
ceiv
edb
arri
ers
(th
ep
erce
pti
on
of
hav
ing
ace
rvic
alsm
ear
test
asti
me
con
sum
ing
p<
.01;
cau
sin
gg
reat
erd
istr
ess
p<
.01
and
bei
ng
mo
reaf
raid
of
the
test
p<
.05
).
Th
est
ren
gth
so
fth
isst
ud
yw
ere
larg
esa
mp
lesi
ze,a
nd
the
com
pu
teri
zed
reco
rds
fro
mth
ecy
tolo
gy
lab
wer
eu
sed
asan
ob
ject
ive
mea
sure
of
scre
enin
gat
ten
dan
ce.T
his
stu
dy
iden
tifi
edm
any
sig
nifi
can
tfa
cto
rsin
flu
enci
ng
scre
enin
gu
pta
ke,
sug
ges
tin
gan
urg
ent
nee
dfo
rh
ealt
hp
rovi
der
toad
dre
ssth
ese
fact
ors
infu
ture
.
12
40
.W
ere
etal
.(2
011
)K
enya
Cro
ss-s
ecti
on
alq
ues
tio
nn
aire
surv
eyN
on
-pre
gn
ant
wo
men
(n=
219
)P
erce
pti
on
so
fri
skan
db
arri
ers
toce
rvic
alca
nce
rsc
reen
ing
1.W
om
eno
fo
ver
30
year
sw
ere
mo
relik
ely
toh
ave
scre
ened
bef
ore
(p=
.012
).2
.P
erce
pti
on
of
bei
ng
atri
skw
assi
gn
ifica
ntl
yas
soci
ated
wit
ha
felt
nee
dfo
rsc
reen
ing
(p=
0.0
02
).3
.Fe
aro
fab
no
rmal
resu
lts
and
lack
of
fin
ance
sw
ere
the
com
mo
nes
tb
arri
ers
tosc
reen
ing
rep
ort
edb
y2
2.4
%an
d11
.4%
of
resp
on
den
ts,r
esp
ecti
vely
.
Th
est
ud
yh
igh
ligh
ted
ah
igh
lysi
gn
ifica
nt
rela
tio
nsh
ipb
etw
een
ap
erce
pti
on
of
ow
nri
sko
fd
evel
op
ing
cerv
ical
can
cer
and
anex
pre
ssed
nee
dfo
rce
rvic
alca
nce
rsc
reen
ing
.H
ow
ever
,th
est
ud
yp
op
ula
tio
nw
asal
sose
lect
edfo
rth
ew
om
enw
ho
wer
eal
read
yac
cess
ing
the
clin
icse
rvic
esin
Mo
iT
each
ing
and
Ref
erra
lH
osp
ital
.
11
41.
Zh
ang
etal
.(2
00
7)
Un
ited
Sta
tes
Sec
on
dar
yd
ata
anal
ysis
usi
ng
asu
bse
tsa
mp
leo
fa
cro
ss-s
ecti
on
alst
ud
yE
lder
lyw
om
en(≧
65
year
s)
(n=
1,04
4)
Inte
nt
toh
ave
asc
reen
ing
,p
revi
ou
sg
ynec
olo
gic
his
tory
,b
enefi
t/at
titu
des
rela
ted
toce
rvic
alsc
reen
ing
Am
on
gw
om
enw
ho
had
no
tu
nd
erg
on
ea
hys
tere
cto
my
per
ceiv
edri
sk(O
R:4
.27
95
%C
I:1.2
7–1
4.3
3),
pre
vio
us
Pap
smea
rte
st(O
R:1
9.2
89
5%
CI:
10.15
–37
.10),
per
ceiv
edp
ain
of
the
test
(OR
,0.5
2;9
5%
CI,
.28
–.9
9),
and
per
ceiv
edim
po
rtan
ce(O
R:4
.00
95
%C
I:1.3
2–1
2.10
)w
ere
po
siti
veco
rrel
ates
of
inte
nti
on
toh
ave
asc
reen
ing
.
Th
isst
ud
yco
ntr
ibu
ted
too
ur
kno
wle
dg
eo
fce
rvic
alsc
reen
ing
bec
ause
of
its
dif
fere
nti
atio
nb
etw
een
eld
erly
wo
men
wh
oh
adan
dh
adn
ot
un
der
go
ne
ah
yste
rect
om
y.T
he
stu
dy
on
lyas
sess
edin
ten
tio
nto
hav
ea
Pap
test
rath
erth
anac
tual
up
take
,bu
tin
ten
tio
nw
asn
ot
alw
ays
tran
slat
edin
toac
tual
acti
on
.
12
CI,
con
fid
ence
inte
rval
;HP
V,h
um
anp
apill
om
avi
rus;
LD
S,L
atte
r-d
ayS
ain
t;O
R,o
dd
sra
tio
;PR
,per
ceiv
edri
sk;S
TD
,sex
ual
lytr
ansm
itte
dd
isea
se;S
TI,
sexu
ally
tran
smit
ted
infe
ctio
n.
C. W. H. Chan et al. Risk Perception and Screening Behavior
11

identify both the determinants of risk perception and thepattern of the relationship between perceived risk and cer-vical screening behavior. The outcome variables of theselected studies focused on women’s risk perception, thefactors affecting their risk perception, and the correlationbetween risk perception and screening participation. Thereare limited studies that have directly addressed the linkagebetween the outcome measurements and the nursingprocess, in particular, the nursing diagnoses of knowledgedeficit and health-seeking behavior were seldom mentionedin these studies.
Women’s perception of cervical cancer risk. Women’sperception of cervical cancer risk varied between thestudies; several studies demonstrated that women ratedtheir relative risk of susceptibility to cervical cancer asbelow average (Eiser & Cole, 2002; Kavanagh & Broom,1998; Marteau et al., 2002; Seow et al., 1995; Taylor et al.,2004). Kavanagh and Broom (1998) found that manywomen did not believe they were at risk of cervical cancerbefore an abnormal Pap smear, while for others, a cervicalabnormality signified their vulnerability and made themconsider the risk of developing cervical cancer. Smokersseemed to have no knowledge of their increased risk ofcervical cancer and disregarded their higher need ofregular screening (Marteau et al., 2002). Taylor et al.(2004) found that 77% of Vietnamese women believed thatthey were less likely to contract cervical cancer than Cau-casian women. Another study involving Chinese women inSingapore (Seow et al., 1995) also reported that only 58.9%of women believed that they were equally susceptible tocontracting cervical cancer, while a substantial proportion(48.7%) of women believed that cancer could not beprevented.
However, there were some contradictory findings. A highproportion (73%) of women were concerned about cervicalcancer, and a very significant proportion (68%) of youngwomen perceived a moderate to high risk of developingcervical cancer (Moreira et al., 2006). Byrd et al. (2004)discovered that up to 90% of Latina women aged 18–25years believed that they were at risk of developing cervicalcancer. Kim et al. (2008) detected a significant difference inthe perception of cancer risk in a diverse sample of womenfrom English, Spanish, and Chinese ethnic groups. Thesedifferences in the perception of cervical cancer risk per-sisted after controlling for demographics, numeracy, andpersonal and family history. Compared with Caucasianwomen, Asian women perceived a lower risk of cervicalcancer, in contrast to Latina women, who perceived theirrisk to be higher.
Most of the studies involved risk perception as a possiblefactor influencing cervical screening behavior, but they didnot explore the factors that influenced women’s risk per-ception. Limited evidence showed that smoking behavior,number of sexual partners, inconclusive screening results,screening experience, social class, perceived severity, per-ceptions of HPV/sexually transmitted disease (STD) expo-
sure, and family history of cancer were factors thatinfluenced the perception of cervical cancer risk(Denny-Smith et al., 2006; French et al., 2004;Garcés-Palacio & Scarinci, 2012; Marlow et al., 2009; Orbell,Crombie, Robertson, Johnston, & Kenicer, 1995; Sauleset al., 2007). Marlow et al. (2009) found that providing HPVinformation enabled women to accurately estimate theirpredisposition to cervical cancer. Increased awareness ofcervical cancer risk was observed in younger women oncethey became cognizant of the sexually transmitted nature ofHPV and the significance of cervical screening. However,Eiser and Cole (2002) and Fernandez et al. (2009) sug-gested that perceived risk rating is not based on relativeunderstanding of cervical cancer and its causes. Fernandezet al. also assessed the effectiveness of intervention inincreasing cervical cancer screening among low-incomeLatina women and found that educational intervention sig-nificantly increased the self-efficacy of cervical screening,the perceived benefits of screening, subjective beliefs, andthe perception of cancer survivability; however, it did notalter the perception of cervical cancer risk. Because of thelimited amount of evidence, it is difficult to reach conclu-sions about trends in the perception of cervical cancer riskand the factors that influence it.
Women’s risk perception and cervical screeningbehavior. The relationship between women’s perception ofcervical cancer risk and their screening behavior is alsoinconclusive among the studies. Some studies supportedthe hypothesis that the perceived risk of the disease plays asubstantial role in the prediction of women’s screeningbehavior (Ackerson, Pohl, & Low, 2008; Fort, Makin, Siegler,Ault, & Rochat, 2011; Kuitto, Pickel, Neumann, Jahn, &Metelmann, 2010; Lee et al., 2002; Marteau et al., 2002;Matejic, Vukovic, Pekmezovic, Kesic, & Markovic, 2011;McMullin, Alba, Chavez, & Hubbell, 2005; Merrill & Madanat,2002; Orbell & Sheeran, 1998; Scarinci, Beech, Kovach, &Bailey, 2003; Seow et al., 1995; Walsh, 2006; Were, Nyaberi,& Buziba, 2011; Zhang, Borders, & Rohrer, 2007), whichinclude three qualitative studies. Women’s beliefs in theirprobability of developing cervical cancer were identified asa fundamental promoter of screening behavior. Womenwho believed that they were at a low risk were less likely tohave been screened previously and were less likely toundergo screening in the future. McMullin et al. (2005) con-ducted a qualitative study with a purposive sample of 20Mexican women and found that physical trauma resultingfrom an abortion or unprotected sex, an infection from apartner, and poor hygiene were factors that Hispanicwomen believed increased an individual’s risk of cervicalcancer. If Latina and African American women did notbelieve that they were at a risk of cervical cancer, then theywere less likely to participate in screening (McMullin et al.,2005; Scarinci et al., 2003). A previous longitudinal study(Orbell & Sheeran, 1998) also discovered that the con-structs of PMT, such as perceived risk, fear arousal, andresponse efficacy, were significant independent variables
Risk Perception and Screening Behavior C. W. H. Chan et al.
12

associated with women’s actual screening behavior andthat the perception of cervical cancer risk was also a suc-cessful predictor of women’s motivation to be screened inthe future.
However, several studies detected no relationshipbetween the perception of cervical cancer risk and screen-ing behavior (Abotchie & Shokar, 2009; Ben-Natan & Adir,2009; Boonpongmanee & Jittanoon, 2007; Byrd et al.,2004; Denny-Smith et al., 2006; Eaker et al., 2001; Eiser &Cole, 2002; Goldman & Risica, 2004; Gu et al., 2012; Hoet al., 2005; Hoque, Ibekwe, & Ntuli-Ngcobo, 2009; Houet al., 2003; Kahn et al., 2001; Kim et al., 2008; Orbell, 1996;Tacken et al., 2007; Taylor et al., 2004). In these studies,risk perception did not predict screening participation orfuture intention to participate in screening. For example,Orbell’s (1996) study claimed that future intention to bescreened was best explained by a sense of responsibility toattend the screening and not by the anxiety associated withcervical cancer risks. Similarly, other studies failed to iden-tify an association between the perception of cervicalcancer risk and the screening behavior (Fernandez et al.,2009; French et al., 2004; Garcés-Palacio & Scarinci, 2012;Kavanagh & Broom, 1998; Marlow et al., 2009; Saules et al.,2007).
The existing quantitative studies fail to fully evaluatewhether the subjects over- or underestimated their riskbecause they do not include valid assessments of the actualrisk of cervical cancer (Vernon, 1999). Currently, there ismuch controversy regarding options for risk perceptionmeasurements for clinical applications and research. Thereare no gold standards for very low- or high-risk perception,particularly within the context of cervical cancer risk. Theconclusion drawn by Vernon (1999) is that there are notenough data to ascertain and quantify the relationshipbetween perceived cervical cancer risk and screeningbehavior.
Discussion
The review of the selected studies reveals major gaps inthe relevant knowledge and methodological approaches.
Theoretical Framework
Although the variables specified in PMT and the HeathBelief Model have received considerable empirical supportin previous studies (Ben-Natan & Adir, 2009; Eaker et al.,2001; Ho et al., 2005; Marteau et al., 2002; Orbell &Sheeran, 1998; Walsh, 2006), various controversies andcriticisms are presented in several of the theoretical andempirical studies. It has been observed that the predictivevalue of the HBM is limited because it is essentially a psy-chosocial model and disregards environmental factors(including the accessibility of services) and normativebeliefs (the perception of how others view behavior)(Seow et al., 1995). While the HBM may identify subjects
who are willing to participate in the screening, it does notpredict actual behavior or long-term adherence (Ho et al.,2005). Researchers have also criticized the model for itsoveremphasis on the rationality of behavior without con-sidering emotional variables that could affect screeningdecisions (Orbell, 1996). Three studies employed PMT tostudy cervical screening behavior; for example, Orbell andSheeran (1998) conducted a longitudinal study to applyPMT to a group of non-screened women to understand therelationship between the motivation to be screened andthe subsequent behavior. The study supported the sugges-tion that PMT variables were successful predictors of bothmotivation to participate in screening and subsequentuptake. However, two other studies (Gu et al., 2012, 2013)contradicted the above findings and did not find PMT vari-ables to be effective predictors of either the motivationto be screened in the future or the previous screeningbehavior.
Orbell and Sheeran (1998) found that the relationshipbetween motivation to undergo screening and actual actionwas far from perfect. This finding indicates that PMT vari-ables may not be sufficient to explain the action of womenwhose positive intention to be screened did not translateinto screening uptake. Other studies argued that elementsor factors other than those described in PMT and the HBMshould be addressed to obtain better insight into health-related motivation. Several empirical studies in this criticalreview proposed a variety of factors other than those speci-fied by the PMT that were successful predictors of women’sscreening behavior; these included the social influence offamily members and physicians (Ackerson et al., 2008;Taylor et al., 2004), previous healthcare experiences(Ackerson et al., 2008), cognitive closure (Eiser & Cole,2002), a sense of fatalism and the normalization of the ideaof cervical screening (Goldman & Risica, 2004), the norma-tive beliefs of others (concern about what others may think)(Abotchie & Shokar, 2009; Kahn et al., 2001; Tacken et al.,2007), contextual factors such as screening as part of ahealth check-up (Lee et al., 2002), religious preference(Merrill & Madanat, 2002), and personal moral obligation(Orbell, 1996; Tacken et al., 2007). For example, Orbell(1996) study showed that the inclusion of personal moralobligation in the regression analysis could better explainthe variance in the intention to be screened. This findingsuggests that threat- and coping-appraisal variables are notenough to determine the motivation to engage in preven-tive behavior. Tacken et al. (2007) reported similar findingsregarding the direct effects of personal moral obligation onthe intention to undergo screening. Other studies sug-gested that for a more comprehensive understanding ofscreening behavior, an emphasis on the social processes ofmotivation and culture-related beliefs would be more ben-eficial than the variables included in either the HBM orthe PMT. This review demonstrated that nursing care inthe area of cervical screening practice would address thecomplex nature of women’s health-seeking behavior. Thefindings from this review indicated that women’s health-
C. W. H. Chan et al. Risk Perception and Screening Behavior
13

seeking behavior in the area of cervical cancer preventionwould be influenced by complex factors that have or havenot been described in existing theoretical models. Thisassertion highlights the need for developing a culturallyrelevant and empirically based theoretical model that couldexplain and predict screening uptake. In order to encouragehealth-seeking behavior, nurses should address suchfactors when organizing the provision of health educationfor cervical cancer prevention. The results from this reviewsuggest that, while providing accurate information is impor-tant, it is equally important to ensure that women’s beliefsand their social-constructed meaning of screening behaviorare included in nursing assessment and evaluation ofchanges resulting from any nursing interventions.
Study Variables
Most of the studies in the review only quantitatively mea-sured the perception of cervical cancer risk and assessedknowledge about risk factors for the disease with simpleyes/no questions (Gu et al., 2012, 2013; Hou et al., 2003).These studies did not appear to adequately explore eitherthe meaning of risk among the women themselves or therole of personal risk factors and cultural context in deter-mining screening behavior. For individuals to engage in arational evaluation of personal risk and subsequent copingstrategies, they must first have an understanding of the riskfactors related to the disease (Marlow et al., 2009). Indeed,the low-risk perception of cervical cancer among Asianwomen identified in this review might be partly explained bya lack of factual information about the risk and risk factorsfor cervical cancer (Herdman, 2012), which concur with thenursing diagnosis of knowledge deficit. Regarding the riskfactors associated with this nursing diagnosis, contextualfactors, including ethical, social, and cultural issues, mustbe properly addressed to in this area of nursing care.Women’s understanding of the risk factors for cervicalcancer and the sexually transmitted nature of HPV andunsafe sex would importantly impact on how women per-ceive the risk of cervical cancer, and subsequent decision-making process of cervical screening behavior. Forexample, Holroyd, Twinn, and Adab (2004) found that asubstantial proportion of Chinese women associated therisk of cervical cancer with multiple sexual partners, beingmarried, youth or old age, and their partner’s poor hygiene.Another study (Martinez, Chavez, & Hubbell, 1997) arguedthat Latina females’ understanding of the risk factors ofcervical cancer was significantly influenced by moral obli-gation. Women who engaged in “unnatural” and “immoral”behavior, including having extramarital partners, havingsex during their menstrual period, and having abortions,were at a higher risk of cervical cancer than others. It hasbeen suggested that emphasizing the association betweencervical cancer and sexual behavior may lead to a sense ofstigma and guilt among women who develop the disease;for example, women who tested positive for HPV experi-enced feelings of anxiety and stigma (McCaffery et al.,
2004). Thus, fear of moral judgment and the stigma asso-ciated with STD may impede screening uptake and informa-tion seeking regarding cervical cancer prevention(Friedman & Shepeard, 2006; Twinn, Holroyd, & Adab,2006). Further nursing research is warranted to under-stand how women comprehend their personal risk and therisk factors of cervical cancer and how the correlationbetween these beliefs affects their screening behavior.Such explorative studies could identify more underling riskfactors associated with the nursing diagnosis of knowledgedeficit and health-seeking behavior. Effective and culturallysensitive nursing care plan would improve communicationabout cervical cancer risk and help promote cervicalscreening among diverse ethnic groups. An improvedunderstanding of the connection between managing therisk of HPV infection and managing cervical cancer riskshould also be addressed in future studies.
Study Population
The majority of the reviewed studies were carried out inWestern populations, and the knowledge obtained fromthese studies may not be applicable to other cultural groupssuch as Asian and African women. Cultural values havebeen found to affect cancer communication and screeningamong several ethnic minorities (Liang, Yuan, Mandelblatt,& Pasick, 2004). The importance of providing cervicalscreening services in a culturally appropriate manner is wellestablished (Hislop et al., 2003; Holroyd et al., 2004; Tayloret al., 2002). For example, traditional Asian cultural views,including fatalism, beliefs regarding a balanced diet, matu-rity, modesty, and self-reliance, contribute to the avoidanceof healthcare visits (Kwok, Sullivan, & Cant, 2006; Lianget al., 2008). Moreover, in Asian cultures (Chen, 1996),health is considered to be a state of physical harmony withthe environment, and an emphasis on the effectiveness oftraditional Chinese medicine and a preference for usingEastern herbs over Western medicine have been demon-strated in Asian populations (Liang et al., 2004; Simpson,2003). These beliefs may constitute a barrier to seekingmedical help through Western medicine, including regularscreening, among Asian women (Hoeman, Ku, & Ohl, 1996;Liang et al., 2004; Yamashiro & Matsuoka, 1997).
Design
Because of the variety of measurement strategiesemployed in the studies, it is difficult to compare women’sperception of cervical cancer risk across the studies.Indeed, the most serious criticism of risk perceptionresearch is that “studies record snapshots of risk judg-ments outside of the specific social contexts in whichpeople live out their day-to-day lives” (Rogers, 1975). Riskperception is not static; rather, it tends to be altered indifferent contexts and influenced by individuals’ knowledgeand life experiences (Bellaby, 1990).
Risk Perception and Screening Behavior C. W. H. Chan et al.
14

The studies examined in this review have several limita-tions, including limited study population size, inadequatedata collection methods, and a lack of in-depth explorationof risk perception from the women’s perspective. Becausemost of the studies were cross-sectional and retrospective,it is difficult to establish any causal association betweenwomen’s perception of cervical cancer risk and their futurescreening behavior. The majority of the reviewed studiesassessed women’s perception of cervical cancer risk withone or two likelihood questions, but evidence shows thatsuch quantitative measurements do not sufficiently capturean individual’s complex feelings and perceptions about therisk of cervical cancer (Slovic, Finucane, Peters, &MacGregor, 2002). These limitations with respect tocurrent risk perception measurements may be more seriouswithin specific cultural contexts. Indeed, cultural contextsare influenced by multiple health, social, and financialissues, which may exert a profound impact on the percep-tion of cancer risk (Huerta & Macario, 1999). A review ofcurrent developments in risk research claimed that newermethods place more emphasis on the significance of socialand cultural context in comprehending cancer risk(Taylor-Gooby & Zinn, 2006). From the literature on cervi-cal cancer perception and prevention decision making,quantitative approaches alone prove inadequate to explaininconsistent findings or to gain in-depth understanding ofcervical cancer risk and subsequent screening behavior.This inadequacy suggests the need for alternative researchmethods, such as mixed method designs and studies indifferent cultural contexts.
Conclusion
The evidence from the 1 review article and 41 primarystudies shows that comparing studies and drawing conclu-sions about the perception of cervical cancer risk andscreening behavior is difficult because of theoretical inad-equacy, measurement variability, the use of culturallyinsensitive measurement strategies, and the use of incon-sistent measurements. Previous works have made fewattempts to examine the feelings related to cervical cancerrisk and how women understand their personal risk factorsin depth. An alternative approach using multiple designsand data sources, rather than a quantitative or a qualitativemethod alone, is recommended to gain a more comprehen-sive understanding of these social phenomena (Greene,Benjamin, & Goodyear, 2001). Alternative study methodsare of particular importance, given that little attention haspreviously been paid to the undoubtedly complex issue ofthe perception of cervical cancer risk, particularly withinspecific cultural contexts. Such efforts would improvenurses’ understanding of the perception of cervical cancerrisk and empower them to develop accurate nursing diag-nosis and appropriate care plan to promote women’s atten-dance at and long-term adherence to cervical screening.Nurses involved in the programs for cervical cancer andscreening should address factors in relation to the nursing
diagnosis of health-seeking behavior and knowledge deficitidentified in this review. This critical review recommendinterventions to raise women’s risk perception involvingspecial efforts to educate women regarding the risk of cer-vical cancer, the meaning of precursors, the causes andsymptoms of cervical cancer, so as to help them makeinformed decisions. In view of the fact that variables speci-fied in existing theoretical frameworks have been proved tobe insufficient to explain cancer screening behavior, futureresearch is needed to find out different facets of the womenawareness and perception of the risk of cervical cancer inrelation to preventive behavior within specific culturalcontext.
Acknowledgment. The authors would like to thank Profes-sor Sheila Twinn for her contribution to this research.
References
Abotchie, P. N., & Shokar, N. K. (2009). Cervical cancer screening amongcollege students in Ghana: Knowledge and health beliefs. InternationalJournal of Gynecological Cancer, 19(3), 412–416.
Ackerson, K., Pohl, J., & Low, L. K. (2008). Personal influencing factorsassociated with Pap smear testing and cervical cancer. Policy, Politicsand Nursing Practice, 9, 50–60.
American Cancer Society. (2006). Cancer fact and figures 2005. RetrievedJanuary 20, 2007 from http://www.cancer.org/docroot/STT/content/STT_1x_Cancer_Facts__Figures_2006.asp
Armitage, C. J., & Conner, M. (2001). Efficacy of the Theory of PlannedBehavior: A meta-analytic review. British Journal of Social Psychology,40, 471–499.
Bellaby, P. (1990). To risk or not to risk? Uses and limitations of Mary Douglason risk acceptability for understanding health and safety at work androad accidents. Sociological Review, 38(3), 465–483.
Ben-Natan, M., & Adir, O. (2009). Screening for cervical cancer among IsraeliLesbian women. International Nursing Review, 56, 433–441.
Boonpongmanee, C., & Jittanoon, P. (2007). Predictors of Papanicolaoutesting in working women in Bangkok, Thailand. Cancer Nursing, 30(5),384–389.
Byrd, T. L., Peterson, S. K., Chavez, R., & Heckert, A. (2004). Cervical cancerscreening beliefs among young Hispanic women. Preventive Medicine,38(2), 192–197.
Chen, Y. L. (1996). Conformity with nature: A theory of Chinese Americanelders’ health promotion and illness prevention processes. Advances inNursing Science, 19(2), 17–26.
Denny-Smith, T., Bairan, A., & Page, M. C. (2006). A survey of female nursingstudents’ knowledge, health beliefs, perceptions of risk, and risk behav-iors regarding human papillomavirus and cervical cancer. Journal of theAmerican Academy of Nurse Practitioners, 18(2), 62–69.
Eaker, S., Adami, H. O., & Sparen, P. (2001). Attitudes to screening for cervicalcancer: A population-based study in Sweden. Cancer Causes and Control,12(6), 519–528.
Eiser, J. R., & Cole, N. (2002). Participation in cervical screening as a functionof perceived risk, barriers and need for cognitive closure. Journal ofHealth Psychology, 7(1), 99–105.
Fernandez, M. E., Gonzales, A., Tortolero-Luna, G., William, J.,Saavedra-Embesi, M., Chan, W., & Vernon, S. W. (2009). Effectiveness ofCultivando La Salud: A breast and cervical cancer screening promotionprogramme for low-income Hispanic women. American Journal of PublicHealth, 99(5), 936–943.
Floyd, D. L., Prentice-Dunn, S., & Rogers, R. W. (2000). A meta-analysis ofresearch on Protection Motivation Theory. Journal of Applied SocialPsychology, 30(2), 407–429.
Fort, V. K., Makin, M. S., Siegler, A. J., Ault, K., & Rochat, R. (2011). Barriers tocervical cancer screening in Mulanje, Malawi: A qualitative study. PatientPreference and Adherence, 5, 125–131.
French, D. P., Maissi, E., & Marteau, T. M. (2004). Psychological costs ofinadequate cervical smear test results. British Journal of Cancer, 91,1887–1892.
Friedman, A. L., & Shepeard, H. (2006). Exploring the knowledge, attitudes,beliefs, and communication preferences of the general public regarding
C. W. H. Chan et al. Risk Perception and Screening Behavior
15

HPV: Findings from CDC focus group research and implications for prac-tice. Health Education and Behavior, 34(3), 471–486.
Garcés-Palacio, I. C., & Scarinci, I. C. (2012). Factors associated with perceivedsusceptibility to cervical cancer among Latina immigrants in Alabama.Maternal and Child Health Journal, 16(1), 242–248.
Globocan. (2010). GLOBOCAN 2008. Fast stats: Women. Retrieved fromhttp://globocan.iarc.fr/factsheets/populations/factsheet.asp?uno=900#women
Goldman, R. E., & Risica, P. M. (2004). Perceptions of breast and cervicalcancer risk and screening among Dominicans and Puerto Ricans in RhodeIsland. Ethnicity and Disease, 14(1), 32–42.
Greene, J. C., Benjamin, L., & Goodyear, L. (2001). The merits of mixingmethods in evaluation. Evaluation, 7(1), 25–44.
Gu, C., Chan, C. W. H., Twinn, S., & Choi, K. (2012). The influence of knowledgeand perception of the risk of cervical cancer on screening behavior inmainland Chinese women. Psycho-Oncology, 21(12), 1299–1308.
Gu, C., Chan, C. W. H., Twinn, S., He, G. P., Choi, K., & Yang, S. B. (2013).Chinese women’s motivation to receive future screening: The role ofsocial-demographic factors, knowledge and risk perception of cervicalcancer. European Journal of Oncology Nursing, 17(2), 131–154.
Herdman, T. H. (Ed.). (2012). NANDA International nursing diagnosis: Defini-tions and classification, 2012–2014. Oxford, UK: Wiley-Blackwell.
Hislop, T. G., Deschamps, M., Teh, C., Jackson, C., Tu, S. P., Yasui, Y., . . .Taylor, V. (2003). Facilitators and barriers to cervical cancer screeningamong Chinese Canadian women. Canadian Journal of Public Health, 94,68–73.
Ho, V., Yamal, J. M., Atkinson, E. N., Basen-Engquist, K., Tortolero-Luna, G., &Follen, M. (2005). Predictors of breast and cervical screening in Vietnam-ese women in Harris County, Houston, Texas. Cancer Nursing, 28(2),119–129.
Hoeman, S. P., Ku, Y. L., & Ohl, D. R. (1996). Health beliefs and early detectionamong Chinese women. Western Journal of Nursing Research, 18(5),518–533.
Holloway, R. M., Wilkinson, C., Peters, T. J., Russell, I., Cohen, D., Hale, J., . . .Lewis, H. (2003). Cluster-randomised trial of risk communication toenhance informed uptake of cervical screening. British Journal ofGeneral Practice, 53, 620–625.
Holroyd, E., Twinn, S., & Adab, P. (2004). Socio-cultural influences on Chinesewomen’s attendance for cervical screening. Journal of AdvancedNursing, 46(1), 42–52.
Hoque, M., Ibekwe, C. M., & Ntuli-Ngcobo, B. (2009). Screening and perceivedseverity of cervical cancer among women attending Mahalapye districthospital, Botswana. Asian Pacific Journal of Cancer Prevention, 10, 1095–1100.
Hou, S., Fernandez, M. E., Baumler, E., Parcel, G. S., & Chen, P. H. (2003).Correlates of cervical cancer screening among women in Taiwan. HealthCare for Women International, 24, 384–398.
Huerta, E. E., & Macario, E. (1999). Communicating health risk to ethnicgroups: Reaching Hispanics as a case study. Journal of the NationalCancer Institute. Monographs, 25, 23–26.
Kahn, J. A., Goodman, E., Slap, G. B., Huang, B., & Emans, S. J. (2001).Intention to return for Papanicolaou smears in adolescent girls andyoung women. Pediatrics, 108(2), 333–341.
Katapodi, M. C., Lee, K. A., Facione, N. C., & Dodd, M. J. (2004). Predictors ofperceived breast cancer risk and the relation between perceived risk andbreast cancer screening: A meta-analytic review. Preventive Medicine,38(4), 388–402.
Kavanagh, A. M., & Broom, D. H. (1998). Embodied risk: My body, myself?Social Science & Medicine (1982), 46(3), 437–444.
Kim, S. E., Perez-Stable, E. J., Wong, S., Gregorich, S., Sawaya, G. F., Walsh, J.M. E., Kaplan, C. P. (2008). Association between cancer risk perceptionand screening behavior among diverse women. Archives of Internal Medi-cine, 168(7), 728–734.
Kuitto, K., Pickel, S., Neumann, H., Jahn, D., & Metelmann, H. (2010). Attitu-dinal and socio-structural determinants of cervical cancer screening andHPV vaccination uptake: A quantitative multivariate analysis. Journal ofPublic Health, 18, 179–188.
Kwok, C., Sullivan, G., & Cant, R. (2006). The role of culture in breast healthpractices among Chinese-Australian women. Patient Education andCounseling, 64(1–3), 268–276.
Lee, J., Seow, A., Ling, S. L., & Peng, L. H. (2002). Improving adherenceto regular Pap smear screening among Asian women: A population-based study in Singapore. Health Education and Behavior, 29(2), 207–218.
Liang, W., Wang, J. H., Chen, M. Y., Feng, S., Lee, M., Schwartz, M. D., . . .Mandelblatt, J. S. (2008). Developing and validating a measure ofChinese cultural views of health and cancer. Health Education and Behav-ior, 35(3), 361–375.
Liang, W., Yuan, E., Mandelblatt, J. S., & Pasick, R. J. (2004). How do olderChinese women view health and cancer screening? Results from focusgroups and implications for interventions. Ethnicity and Health, 9(3),283–304.
Marlow, L. A. V., Waller, J., & Wardle, J. (2009). The impact of humanpapillomavirus information on perceived risk of cervical cancer. CancerEpidemiology, Biomarkers and Prevention, 18(2), 373–376.
Marteau, T. M., Hankins, M., & Collins, B. (2002). Perceptions of risk ofcervical cancer and attitudes towards cervical screening: A comparisonof smokers and non-smokers. Family Practice, 19(1), 18–22.
Martinez, R. G., Chavez, L. R., & Hubbell, F. A. (1997). Purity and passion: Riskand morality in Latina immigrants’ and physicians’ beliefs about cervicalcancer. Medical Anthropology, 17(4), 337–362.
Matejic, B., Vukovic, D., Pekmezovic, T., Kesic, V., & Markovic, M. (2011).Determinants of preventive health behavior in relation to cervical cancerscreening among the female population of Belgrade. Health EducationResearch, 26(2), 201–211.
McCaffery, K., Waller, J., Forrest, S., Cadman, L., Szarewski, A., & Wardle, J.(2004). Testing positive for human papillomavirus in routine cervicalscreening: Examination of psychosocial impact. BJOG: An InternationalJournal of Obstetrics and Gynaecology, 111(12), 1437–1443.
McMullin, J. M., Alba, I. D., Chavez, L. R., & Hubbell, F. A. (2005). Influence ofbeliefs about cervical cancer etiology on Pap smear Use among Latinaimmigrants. Ethnicity and Health, 10(1), 3–18.
Merrill, R. M., & Madanat, H. N. (2002). Cervical cancer risk perceptionand pap-smear screening. Health Education Journal, 61(3), 231–243.
Mols, F., Vingerhoets, A. J. J. M., Coebergh, J. M., & Van de Poll-Franse, L. V.(2005). Quality of life among long-term breast cancer survivors: Asystematic review. European Journal of Cancer, 41, 2613–2619.
Montano, D. E. (2008). Theory of reasoned action, theory of planned behav-ior, and the integrated behavioral model. In K. Glanz (Ed.), Health behav-ior and health education: Theory, research, and practice (4th ed., pp.67–96). San Francisco: Jossey-Bass.
Moreira, E. D., Jr., Oliveira, B. G., Ferraz, F. M., Costa, S., Costa Filho, J. O., &Karic, G. (2006). Knowledge and attitudes about human papillomavirus,Pap smears, and cervical cancer among young women in Brazil: Implica-tions for health education and prevention. International Journal of Gyne-cological Cancer, 16(2), 599–603.
Orbell, S. (1996). Cognition and affect after cervical screening: The role ofprevious test outcome and personal obligation in future uptake expecta-tions. Social Science & Medicine, 43(8), 1237–1243.
Orbell, S., Crombie, I., Robertson, A., Johnston, G., & Kenicer, M. (1995).Assessing the effectiveness of a screening campaign: Who is missing by80% cervical screening coverage. Journal of the Royal Society of Medi-cine, 88, 389–394.
Orbell, S., & Sheeran, P. (1998). “Inclined abstainers”: A problem for predict-ing health-related behavior. British Journal of Social Psychology, 37(Pt.2), 151–165.
Phongsavan, K., Phengsavanh, A., Wahlström, R., & Marions, L. (2010).Women’s perception of cervical cancer and its prevention in rural Laos.International Journal of Gynecological Cancer, 20, 821–826.
Rogers, R. W. (1975). A protection motivation theory of fear appeals andattitude change. Journal of Psychology, 91(1), 93.
Saules, K. K., Vannest, N. O., Mehringer, A. M., Pomerleau, C. S., Lee, K.,Opipari, A. W., . . . Snedecor, S. M. (2007). Actual versus perceived risk ofcervical cancer among college women smokers. Journal of AmericanCollege Health, 55(4), 207–213.
Scarinci, I. C., Beech, B. M., Kovach, K. W., & Bailey, T. L. (2003). An exami-nation of sociocultural factors associated with cervical cancer screeningamong low-income Latina immigrants of reproductive age. Journal ofImmigrant Health, 5(3), 119–128.
Seow, A., Wong, M. L., Smith, W. C., & Lee, H. P. (1995). Beliefs and attitudesas determinants of cervical cancer screening: A community-based studyin Singapore. Preventive Medicine, 24(2), 134–141.
Simpson, P. B. (2003). Family beliefs about diet and traditional Chinesemedicine for Hong Kong women with breast cancer. Oncology NursingForum, 30, 834–840.
Slovic, P., Finucane, M., Peters, E., & MacGregor, D. G. (2002). The affect ofheuristic. In T. Gilivich & D. Griffin (Eds.), Heuristics and biases: Thepsychology of intuition judgment (pp. 397–420). New York: CambridgeUniversity Press.
Tacken, M. A. J. B., Braspenning, J. C. C., Hermens, R. P. M. J.,Spreeuwenberg, P. M. M., van den Hoogen, H. J. M., de Bakker, D. H.,. . . Grol, R. P. T. M. (2007). Uptake of cervical cancer screening in theNetherlands is mainly influenced by women’s beliefs about the screeningand by the inviting organization. European Journal of Public Health, 17(2),178–185.
Risk Perception and Screening Behavior C. W. H. Chan et al.
16

Taylor, V. M., Jackson, J. C., Tu, S. P., Yasui, Y., Schwartz, S. M., Kuniyuki,A., . . . Hislop, G. (2002). Cervical cancer screening among ChineseAmericans. Cancer Detection and Prevention, 26(2), 139–145.
Taylor, V. M., Yasui, Y., Burke, N., Nguyen, T., Acorda, E., Thai, H., . . . Jackson,C. (2004). Pap testing adherence among Vietnamese American women.Cancer Epidemiology, Biomarkers and Prevention, 13(4), 613–619.
Taylor-Gooby, P., & Zinn, J. O. (2006). Current directions in risk research:New developments in psychology and sociology. Risk Analysis, 26(2),397–411.
Twinn, S., Holroyd, E., & Adab, P. (2006). The influence of intrinsic andextrinsic factors on uptake rates for cervical screening: A comparison ofHong Kong Chinese women and practitioners. Hong Kong MedicalJournal, 12(Suppl. 2), S19–S21.
Vernon, S. W. (1999). Risk perception and risk communication for cancerscreening behaviors: A review. Journal of the National Cancer Institute.Monographs, 25, 101–119.
Wallsten, T. S., Budescu, D. V., Rapoport, A., Zwick, R., & Forsyth, B. (1986).Measuring the vague meaning of probability terms. Journal of Experi-mental Psychology, 115, 348–365.
Walsh, J. C. (2006). The impact of knowledge, perceived barriers and per-ceptions of risk on attendance for a routine cervical smear. EuropeanJournal of Contraception and Reproductive Health Care, 11(4), 291–296.
Walter, F. M., & Britten, N. (2002). Patients’ understanding of risk: A qualita-tive study of decision-making about the menopause and hormonereplacement therapy in general practice. Family Practice, 19(6), 579–586.
Were, E., Nyaberi, Z., & Buziba, N. (2011). Perceptions of risk and barriers tocervical cancer screening at Moi Teaching and Referral Hospital (MTRH),Eldoret, Kenya. African Health Sciences, 11(1), 58–64.
Whittemore, R., & Knafl, K. (2005). The integrative review: Update method-ology. Journal of Advanced Nursing, 52(5), 546–553.
World Health Organization. (2008). The global burden of disease: 2004update. Retrieved from http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/index.html
Yamashiro, G., & Matsuoka, J. K. (1997). Help-seeking among Asian andPacific Americans: A multiperspective analysis. Social Work, 42(2), 176–186.
Zhang, Y., Borders, T. F., & Rohrer, J. E. (2007). Correlates of intent to seekunnecessary Pap tests among elderly women. Women’s Health Issues,17(6), 351–359.
C. W. H. Chan et al. Risk Perception and Screening Behavior
17