pediatric restorative dentistry
TRANSCRIPT

Pediatric Restorative Dentistry
Objectives
• To be able to identify and distinguish morphologic differences between primary and permanent teeth.
• To apply the knowledge of morphology in clinical procedures for pediatric patients
Morphologic differences between primary and permanent teeth (cavity preparation)
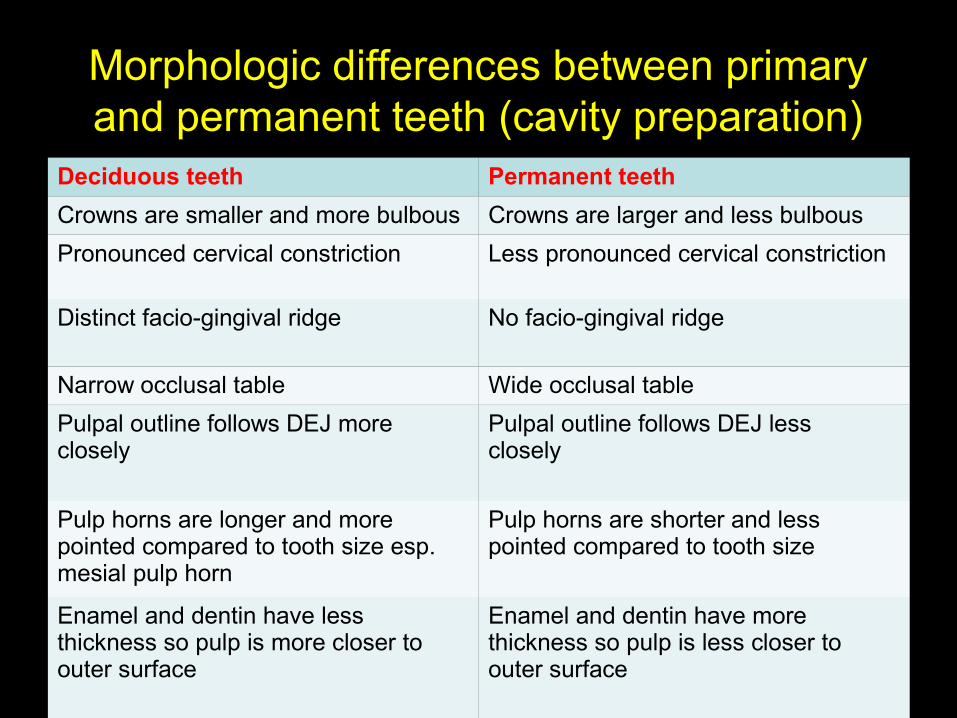
Deciduous teeth Permanent teeth
Crowns are smaller and more bulbous Crowns are larger and less bulbous
Pronounced cervical constriction Less pronounced cervical constriction
Distinct facio-gingival ridge No facio-gingival ridge
Narrow occlusal table Wide occlusal table
Pulpal outline follows DEJ more closely
Pulpal outline follows DEJ less closely
Pulp horns are longer and more pointed compared to tooth size esp. mesial pulp horn
Pulp horns are shorter and less pointed compared to tooth size
Enamel and dentin have less thickness so pulp is more closer to outer surface
Enamel and dentin have more thickness so pulp is less closer to outer surface
Morphologic differences between primary and permanent teeth (cavity preparation)
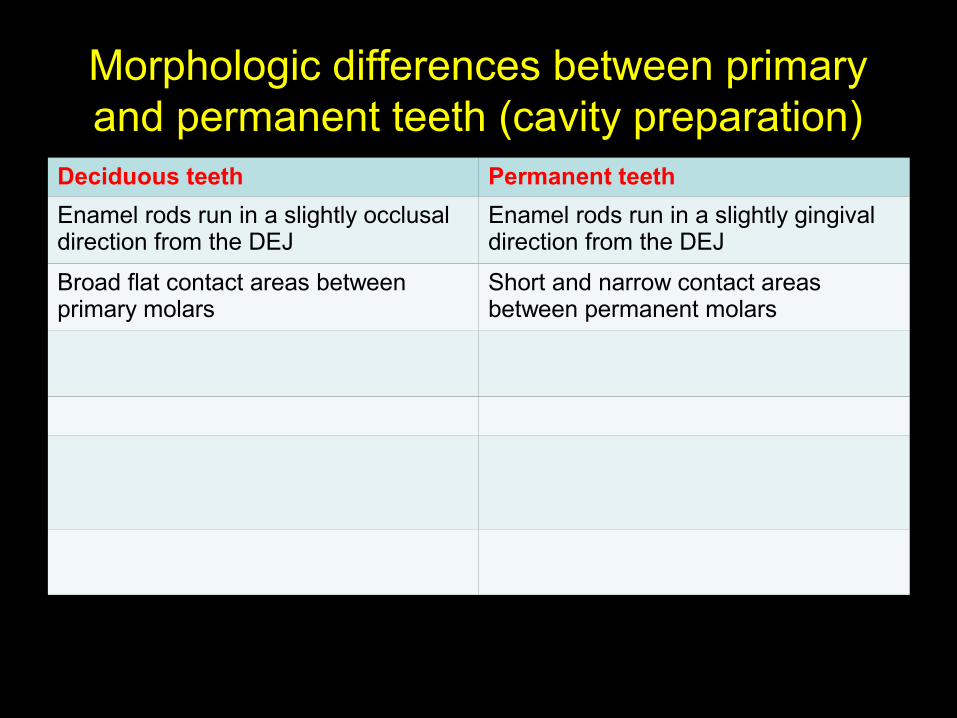
Deciduous teeth Permanent teeth
Enamel rods run in a slightly occlusal direction from the DEJ
Enamel rods run in a slightly gingival direction from the DEJ
Broad flat contact areas between primary molars
Short and narrow contact areas between permanent molars
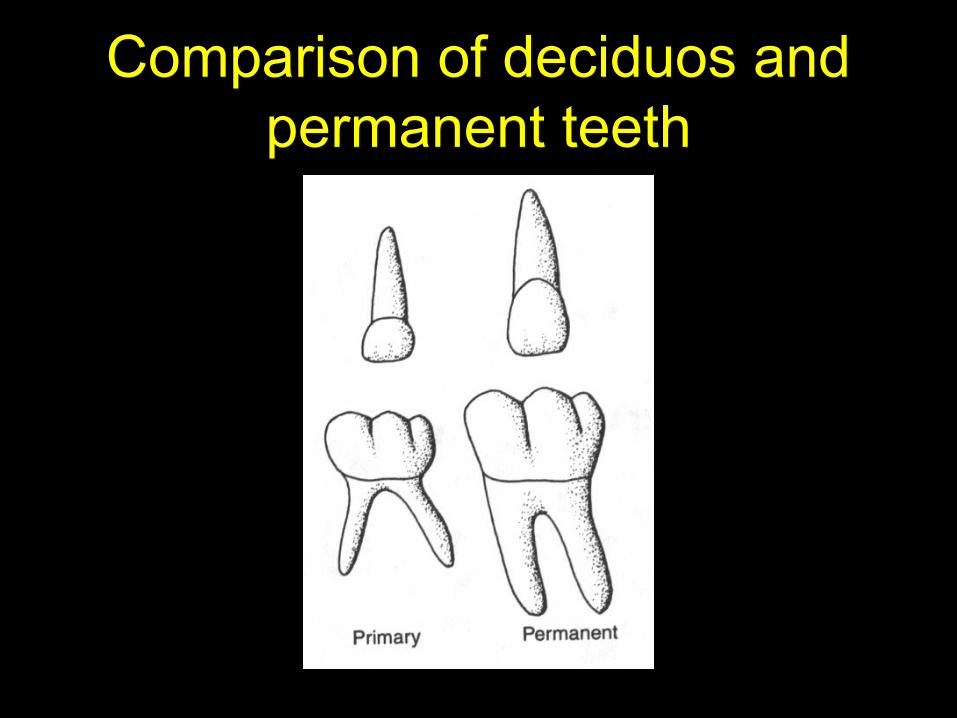
Comparison of deciduos and permanent teeth
Comparison of deciduos and permanent teeth
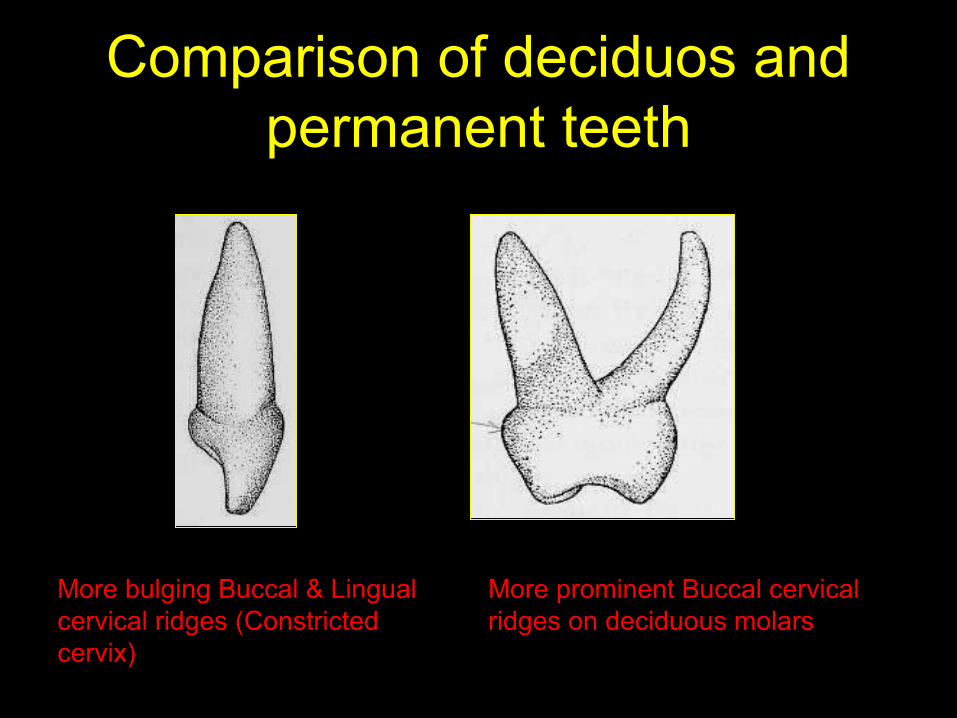
More prominent Buccal cervical ridges on deciduous molars
More bulging Buccal & Lingual cervical ridges (Constricted cervix)
Comparison of deciduos and permanent teeth
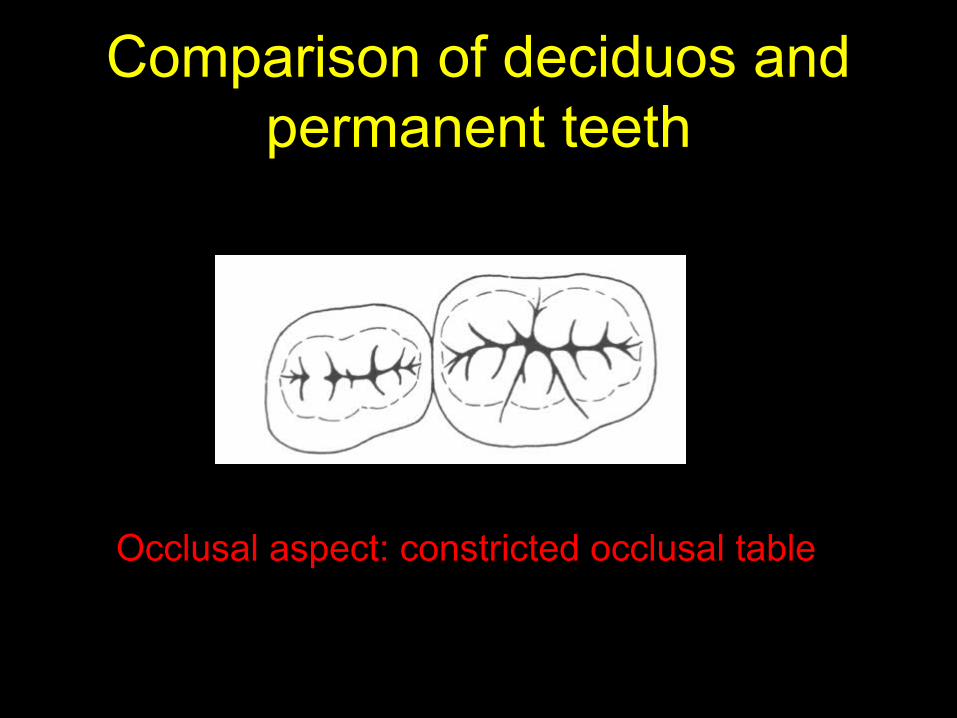
Occlusal aspect: constricted occlusal table
Comparison of deciduos and permanent teeth
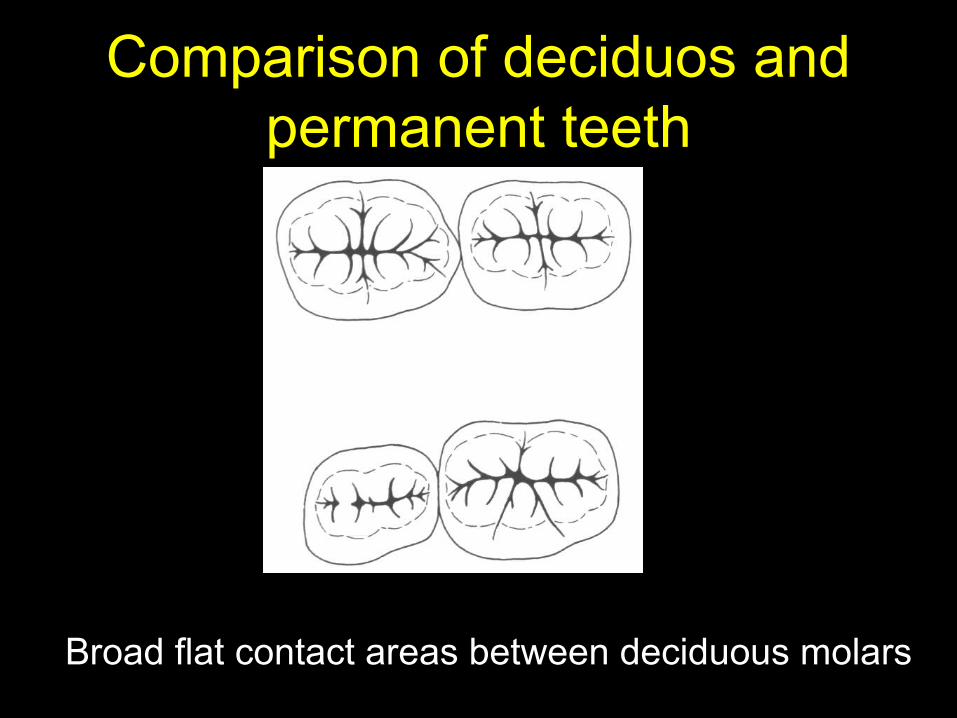
Broad flat contact areas between deciduous molars
Comparison of deciduos and permanent teeth
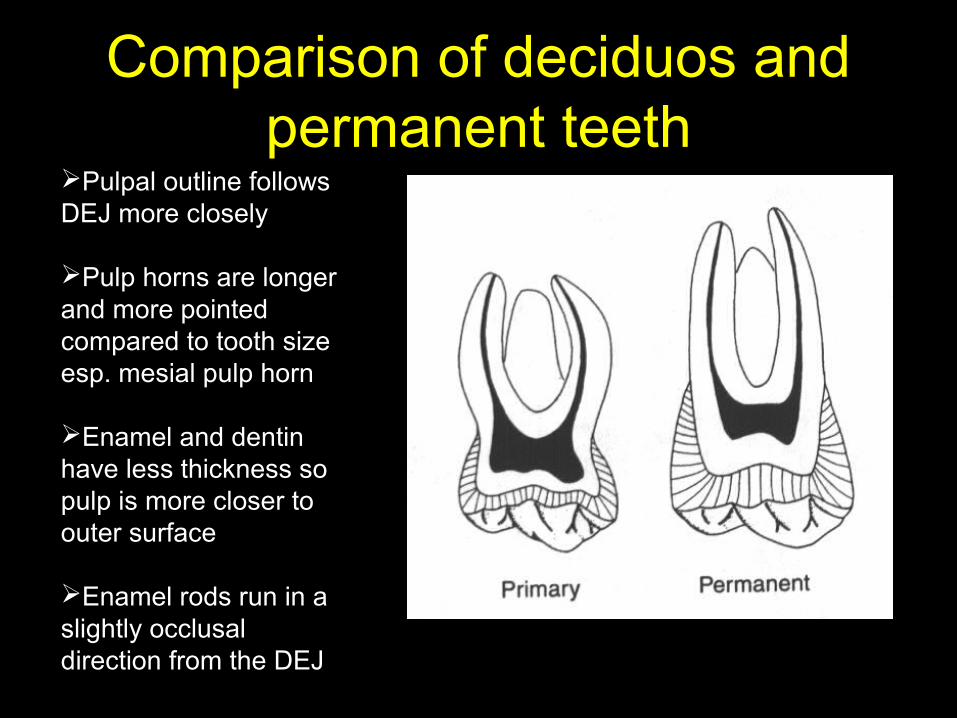
Pulpal outline follows DEJ more closely
Pulp horns are longer and more pointed compared to tooth size esp. mesial pulp horn
Enamel and dentin have less thickness so pulp is more closer to outer surface
Enamel rods run in a slightly occlusal direction from the DEJ
Clinical considerations
• Shorter crowns of deciduous teeth compared to permanent teeth
• Depth and overall dimensions of the prepared cavity is less in deciduous teeth compared to permanent teeth
• Narrow occlusal table
• The width of cavity is less in a deciduous tooth
• Constricted cervical portion below the more pronounced cervical ridge
• Observe caution during preparation of proximal box as there is risk of pulpal exposure
• Thinner enamel and dentin layers
• Care must be taken during cavity preparation, not to extend very deep as there are increased chances of pulp exposure
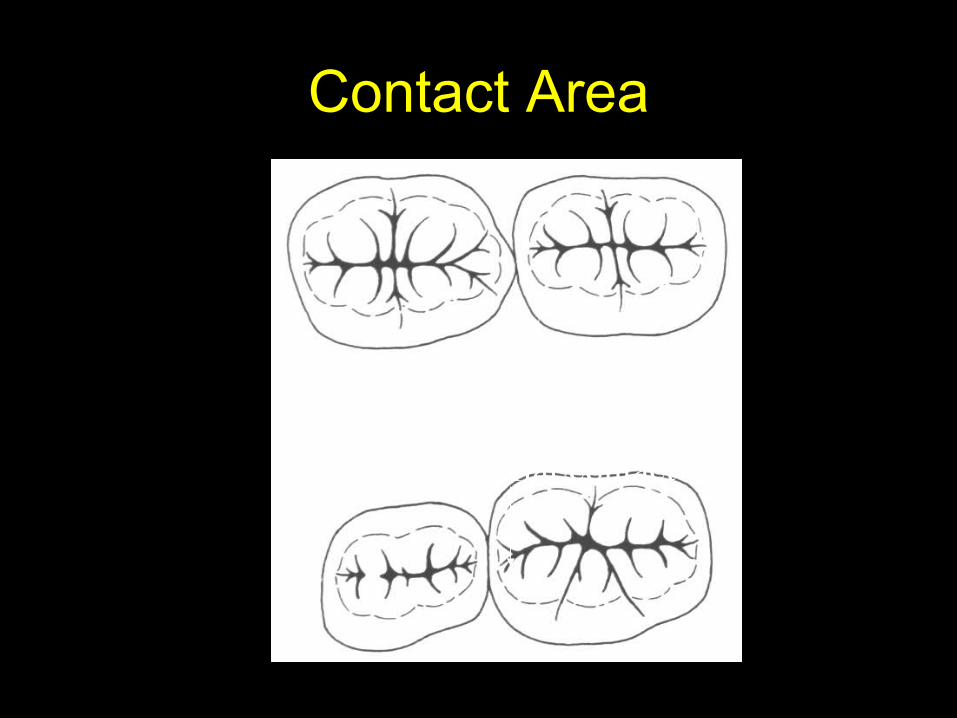
Contact Area
Point contactBroad, flat contact
• Broad flat contact areas
• Caries remain undetected
• Proximal box preparation has to be extended widely to take the cavity margins to self cleansing areas
• Enamel rods that run in a slightly occlusal direction from the DEJ
• Enamel beveling at the gingivo cavo surface angle is not required, as no enamel rods stay unsupported
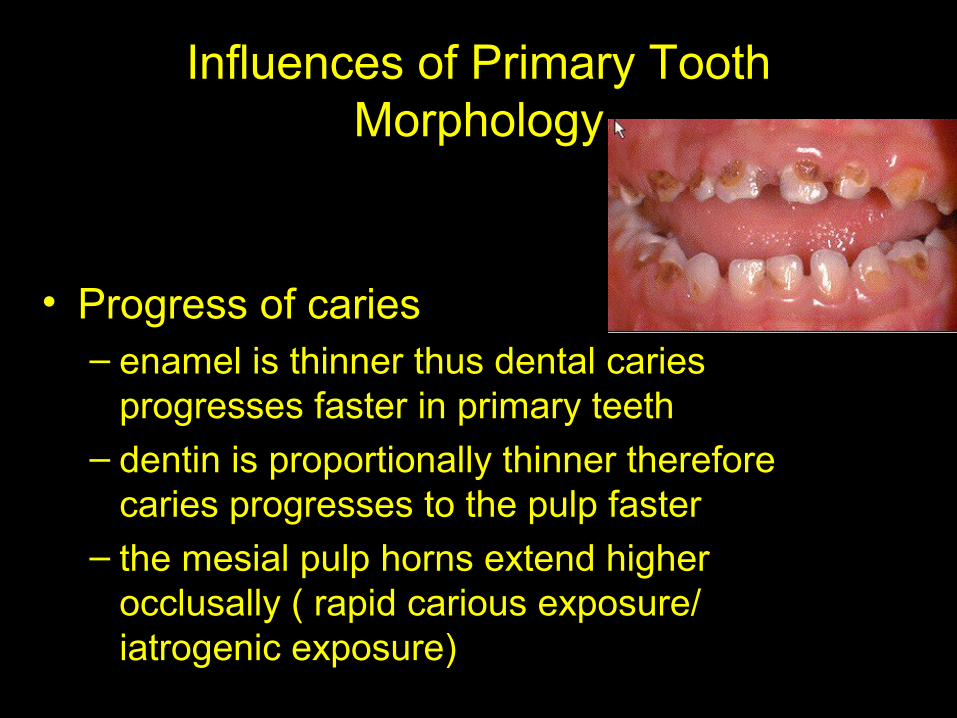
Influences of Primary Tooth Morphology
• Progress of caries– enamel is thinner thus dental caries
progresses faster in primary teeth– dentin is proportionally thinner therefore
caries progresses to the pulp faster– the mesial pulp horns extend higher
occlusally ( rapid carious exposure/ iatrogenic exposure)

Principles of cavity preparation(Occlusal)
• Occlusal form should be dovetailed, including all fissures ,areas of caries pits and development grooves
• The walls converge slightly with greatest width at the pulpal floor
• Cavosurface margins should be sharp (90 degrees)
• Angles of walls and floor should be slightly rounded
• The axiopulpal line angle should be slightly rounded
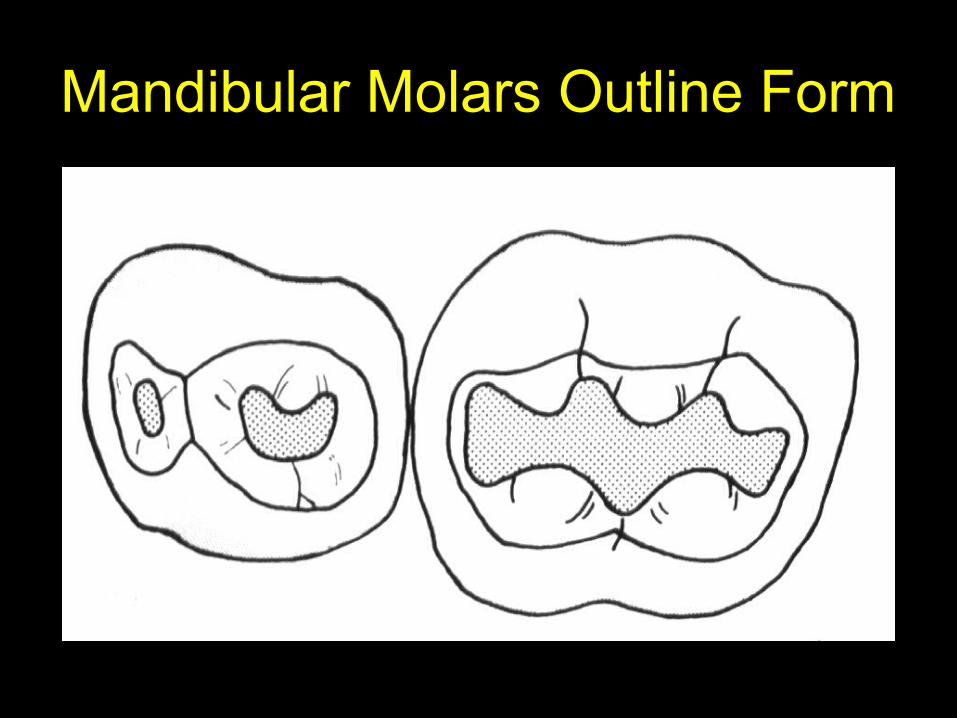
Mandibular Molars Outline Form
Maxillary Molars Outline Form
Principles of cavity preparation(Proximal box)
• The buccal and lingual walls should just extend into self cleansing areas
• A sharp 90 degree cavosurface angle is desired• The buccal and lingual walls of the proximal box
should converge slightly from the gingival floor to the occlusal surface. Isthmus width is 1/3rd of intercuspal distance.
• The gingival floor should be beneath the point of contact at or just beneath the gingival tissue. No bevel is placed
• All internal line angles should be gently rounded• Buccal and lingual retentive grooves are
contraindicated• The axial wall should follow the contour of tooth
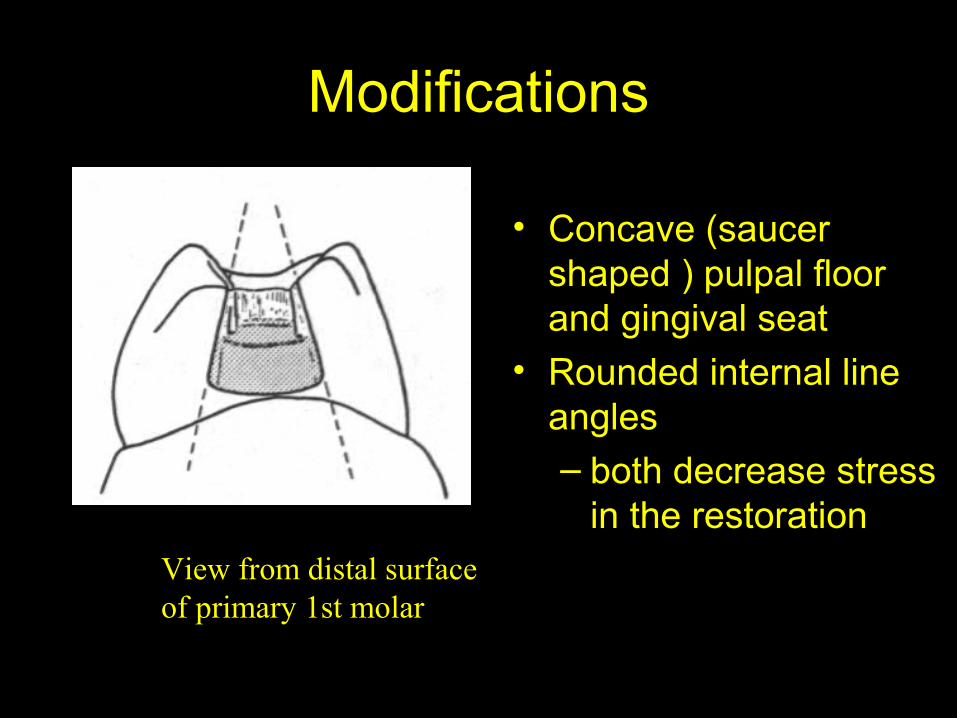
Modifications
• Concave (saucer shaped ) pulpal floor and gingival seat
• Rounded internal line angles– both decrease stress
in the restorationView from distal surface of primary 1st molar
B L
Class I cavity preparation(external outline form)
• Start preparation by penetrating the occlusal surface with no. 330 bur.
• Include all deep and defective grooves in the preparation. Blend the outline to form smooth flowing arcs and curves
• Contour the outline to the mesial and distal marginal ridges. Maintain the bulk of tooth structure on marginal ridges
• Maintain a width approximately one third the width of the occlusal table

Class I cavity preparation(internal outline form)
• Penetrate 0.2 to 0.5 mm into the dentin with no. 330 bur. Dentin softer, less shiny, usually yellow.
• Round the line angles with no. 330 bur. Round line angles easier to condense amalgam. Reduce internal stress on amalgam restoration.
• The walls are wider at pulpal floor than at the occlusal opening. This convergence aids in retention of restorative material
Class I cavity preparation(internal outline form)
• Slightly round the pulpal floor. All internal line angles should be rounded.
• Establish a sharp cavosurface angle in the lateral walls with no 169L bur.
• The sharp cavosurface angle is an asset to improve carving and polishing and reduce marginal failure.
• The walls are parallel or slightly undercut to the external surfaces of the tooth.
Class I cavity preparation(internal outline form)
• If the active caries has not been removed during cavity preparation do so now. Use no.4 or no. 6 round bur in a slow speed handpiece or a large spoon excavator.
• Rinse the preparation with water. Inspect for caries removal.

Class I cavity preparation(Refinement and debridement)
• Establish well supported and finished margins• Hatchets and chisels are used to remove
unsupported enamel.• Tungten carbide bur at 20000 rpm can be used
in slow speed handpiece to refine the margins.• Cavity should be free of debris (toilet of the
cavity by washing finally)
Class I cavity preparation(insulating base)
• With deep carious lesions and the depth of the cavity should be covered with a biocompatible calcium hydroxide sub base like dycal.
• A zinc phospahate or other hard setting base is applied over the sub base.
• The last step before restoring with amalgam is the placing of cavity varnish.
• Varnish reduces the marginal leakage after amalgam restoration has been placed.
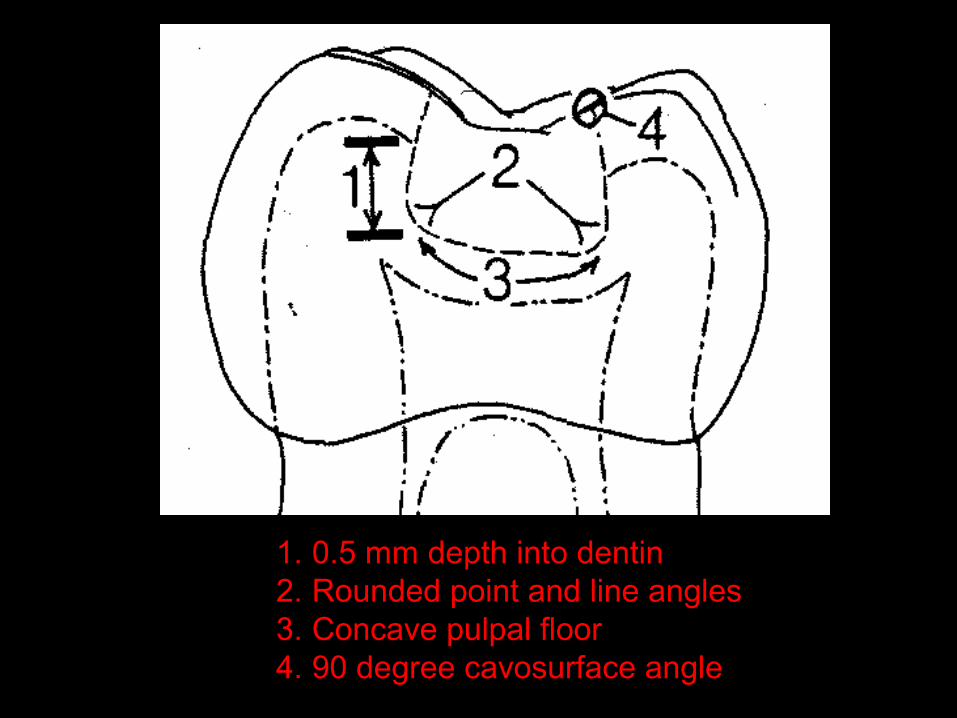
1. 0.5 mm depth into dentin2. Rounded point and line angles3. Concave pulpal floor4. 90 degree cavosurface angle
Class II cavity preparation• Complete class I cavity as described • Use a no. 330 bur to extend the occlusal outline
through the marginal ridge.• Extend the no. 330 bur into proximal surface.
Keep the bur parallel to long axis of tooth. Move the bur in a pendulating motion from lingual to buccal.
• Gently curve buccolingually to follow the contour of the proximal surface
• Extend the proximal box into self cleansing areas.• Leave 90 degree cavosurface angle
Class II cavity preparation
• The isthmus is approximately 1/3 rd he width of occlusal surface
• Extend the proximal box gingivally beneath the contact area to the interproximal area. This area is determined by clearance of explorer tip.
• The axial wall as determined by carious lesion depth, should follow the outside contour of tooth.
• Gingival floor is even with or slightly below the level of gingiva, perpendicular to long axis of tooth, no beveling is required.the width of gingival floor is approximately 1mm.
Class II cavity preparation
• Proximal box in an occlusogingival direction is roughly parallel to long axis of tooth.
• Proximal box walls should converge towards the occlusal , approximately following the buccal and lingual surface of the tooth.
• This provides for increased retention, carries the preparation into self cleaning areas, and avoids undermining of adjacent cusps.

Class II cavity preparation• If the active caries has not been removed during
cavity preparation do so now. Use no.4 or no. 6 round bur in a slow speed handpiece or a large spoon excavator.
• Rinse the preparation with water. Inspect for caries removal.
• All line angles including the axiopulpal line angle are gently rounded. This can be rounded with a bur or hand instruments (sharp enamel hatchet)
Class II cavity preparation(Refinement and debridement)
• Establish well supported and finished margins• Hatchets and chisels are used to remove
unsupported enamel.• Tungten carbide bur at 20000 rpm can be used
in slow speed handpiece to refine the margins.• Cavity should be free of debris (toilet of the
cavity by washing finally)
Class II cavity preparation(insulating base)
• With deep carious lesions and the depth of the cavity should be covered with a biocompatible calcium hydroxide sub base like dycal.
• A zinc phospahate or other hard setting base is applied over the sub base.
• The last step before placement of matrix band restoring with amalgam is the placing of cavity varnish.
• Varnish reduces the marginal leakage after amalgam restoration has been placed.
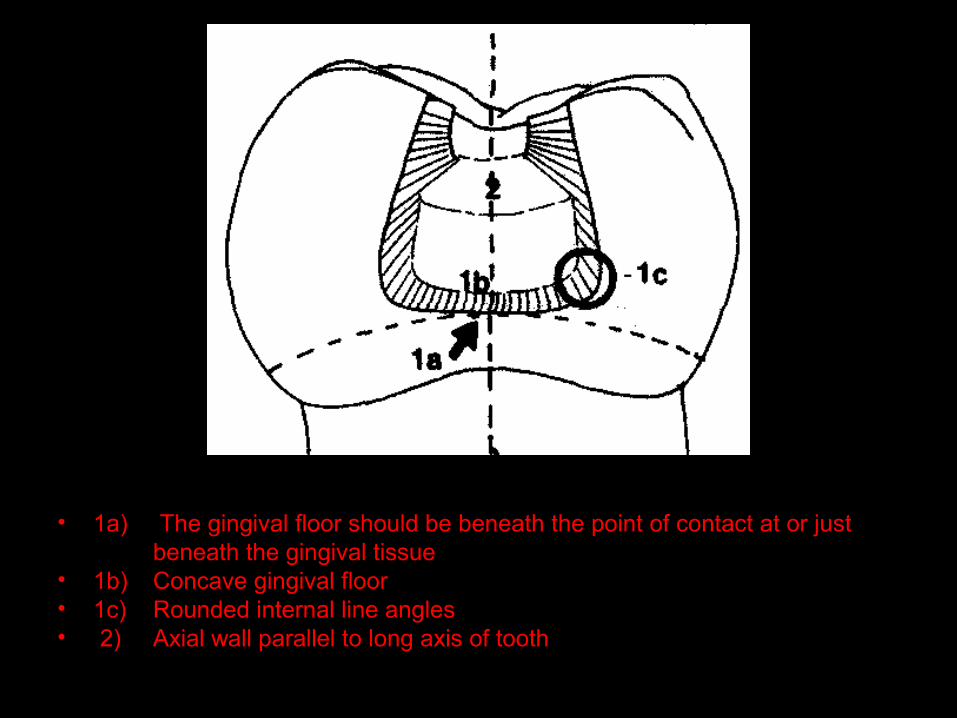
• 1a) The gingival floor should be beneath the point of contact at or just beneath the gingival tissue
• 1b) Concave gingival floor• 1c) Rounded internal line angles• 2) Axial wall parallel to long axis of tooth
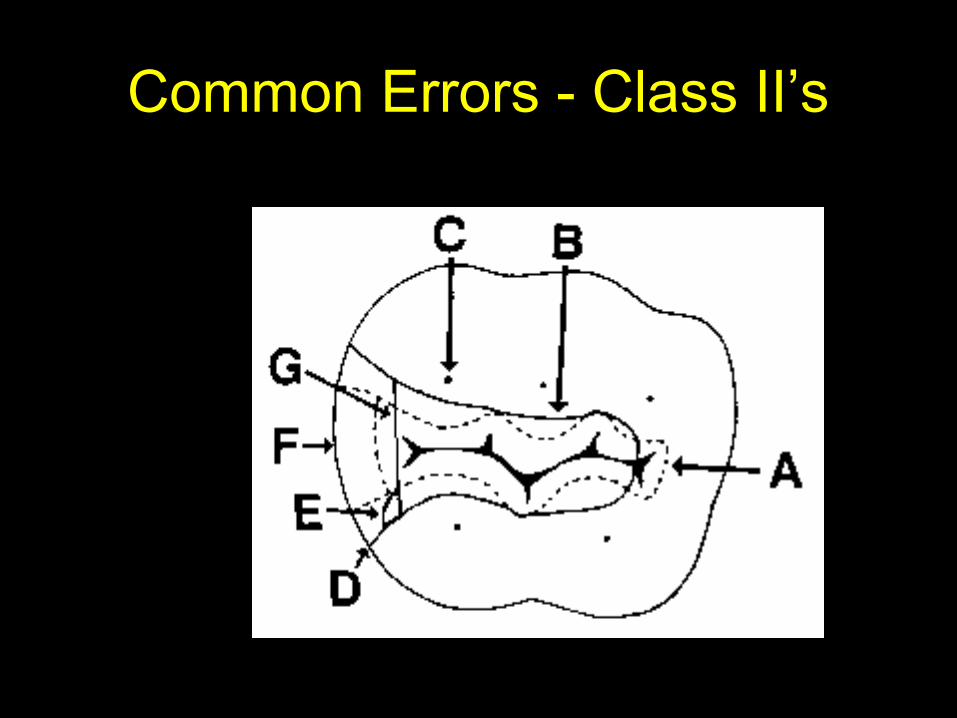
Common Errors - Class II’s
Class III cavity preparation
• When contact areas are open and lesion is incipient the cavity can be prepared directly (no need for dovetail lock to improve access or retention).
• With closed contacts an indirect approach is adopted.
• Usually a palatal approach is used to gain access for esthetic reasons.
• A lock or dovetail is used for access and to improve retention. Especially in cases of extensive lesions and in case of canines which are retained 5-6 years more than incisors.
Class III cavity preparation
• Use no 330 bur• Outline form is triangular, with the base of the
triangle at the gingival aspect of the cavity.• The buccal and lingual walls should parallel the
respective external surface of the tooth to meet at the apex of the triangle
• The gingival wall should incline slightly occlusally ( enamel rod parallelism and provides retention)
• Incisal aspect should not be undercut (undermining of incisal enamel)
• Cavity depth 0.2-0.5 mm into dentin.
Class III cavity preparation
• When used the lock should extend up to middle third of tooth
• Should be dovetailed• Care should be taken to make the lock on the
dovetail at the expense of gingival rather than incisal, which might weaken the angle of the tooth.
• The inclination of incisal and gingival walls should be towards the incisal edge, paralleling the enemel rods.
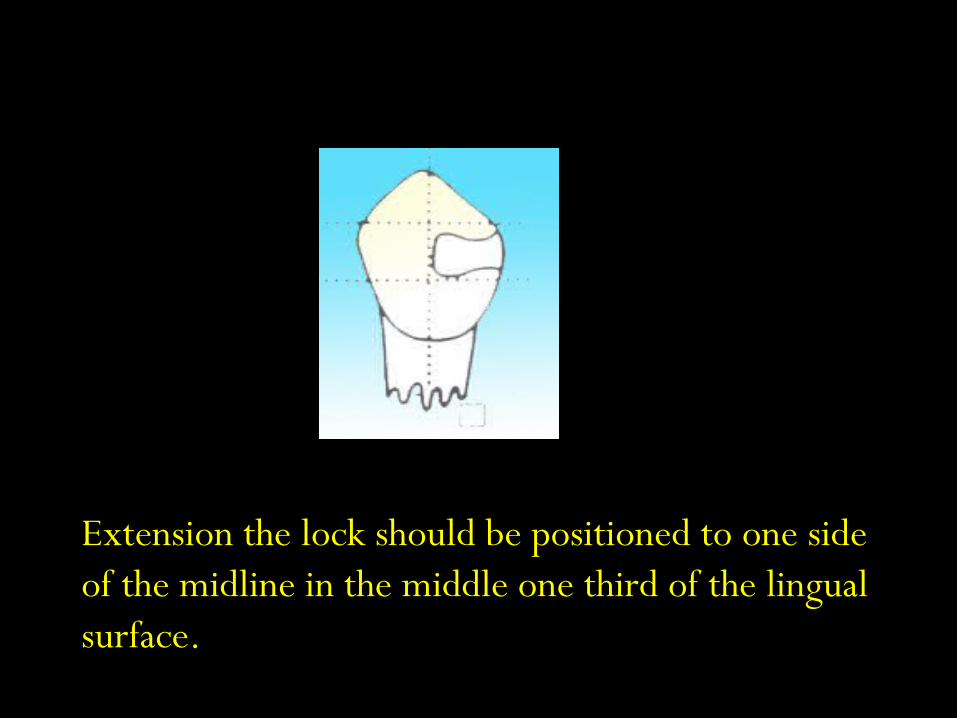
Extension the lock should be positioned to one side of the midline in the middle one third of the lingual surface.
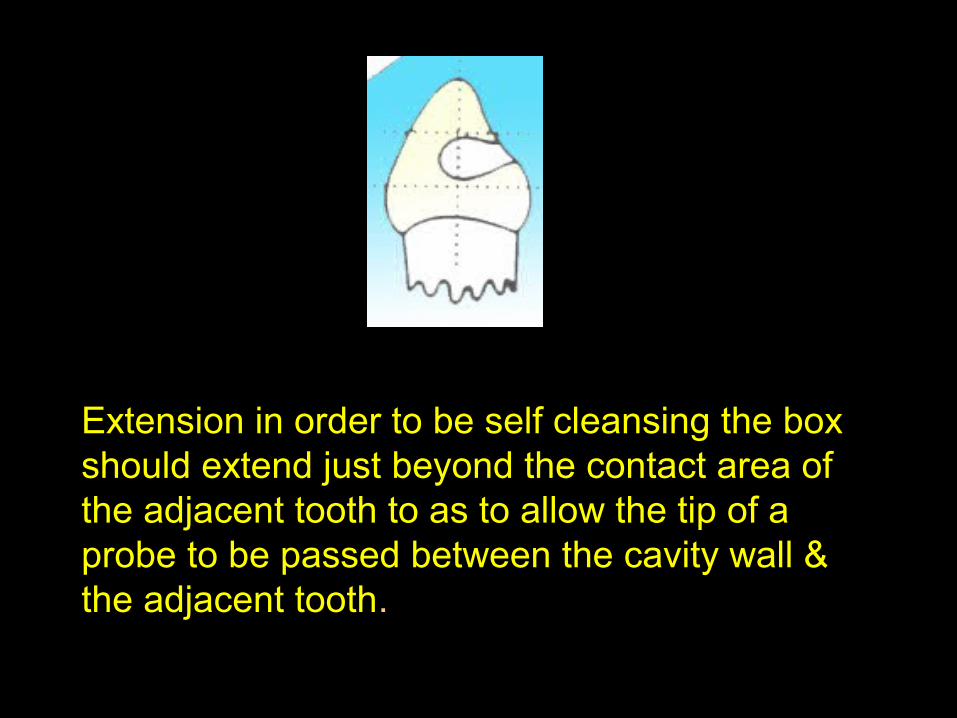
Extension in order to be self cleansing the box should extend just beyond the contact area of the adjacent tooth to as to allow the tip of a probe to be passed between the cavity wall & the adjacent tooth.
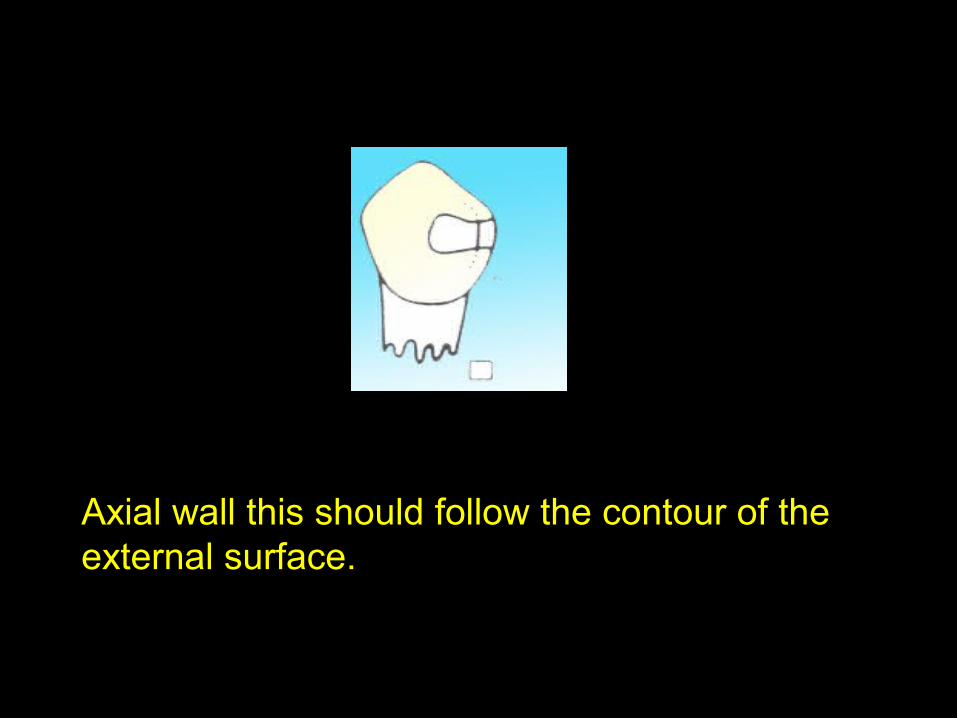
Axial wall this should follow the contour of the external surface.
Class III cavity preparation
• Rest of the principals pertaining to remainder of active caries refinement, debridement and placing of base/sub-base remain the same as in class I or class II.
Class V cavity preparation
• Outline form should be limited to carious lesion and any adjacent decalcified areas
• Kidney shaped outline with gentle curves• Bur used is no.330• Gingival margin should be a regular curve
parallel to gingival attachment• Remaining caries removed with slow speed no.2
round bur.
Failure of amalgam restoration
• Fracture of the isthmus of a Class II – due to insufficient bulk of amalgam
• Marginal failure in proximal box area– due to excessive flare of the cavosurface
margin
• Recurrent caries– failure to extend preparation adequately– due to insufficient bulk of amalgam
Matrices used in pediatric dentistry

Requirements of Ideal restorations
Proper contour that discourages the retention of food debris, bacteria & plaque so that they may not be detrimental to gingival health or encourage recurrent caries.
INTRODUCTION
“MATRIX” is derived from Latin word - ‘Mater’ which means ‘Mother’.
It was introduced by Dr. Louis Jack.
Definition:
The matrix is a device used to contour a restoration to simulate that of a tooth structure, which it is replacing.
Ideal requirements of a matrix…
• It should be inserted easily & should be sufficiently rigid to retain the contour given to it so that it can be transferred to the restoration.
• It should be easily removed without the fracture of the restoration.
• It should not be cumbersome.• It should not adhere or react with the restorative
material.• It should resist the condensation pressure.• It should be versatile.• It should not react with soft tissues.
MATRICING
MATRICING is a procedure, whereby a temporary wall is created opposite to axial wall & surrounding areas of the tooth structure that were lost during preparation.
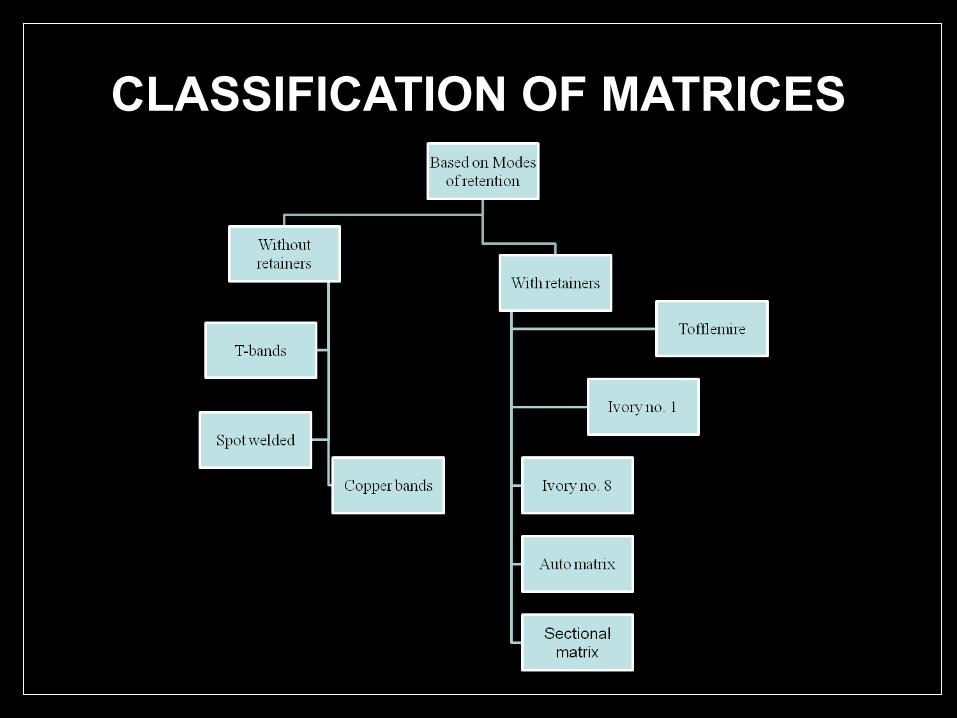
CLASSIFICATION OF MATRICES
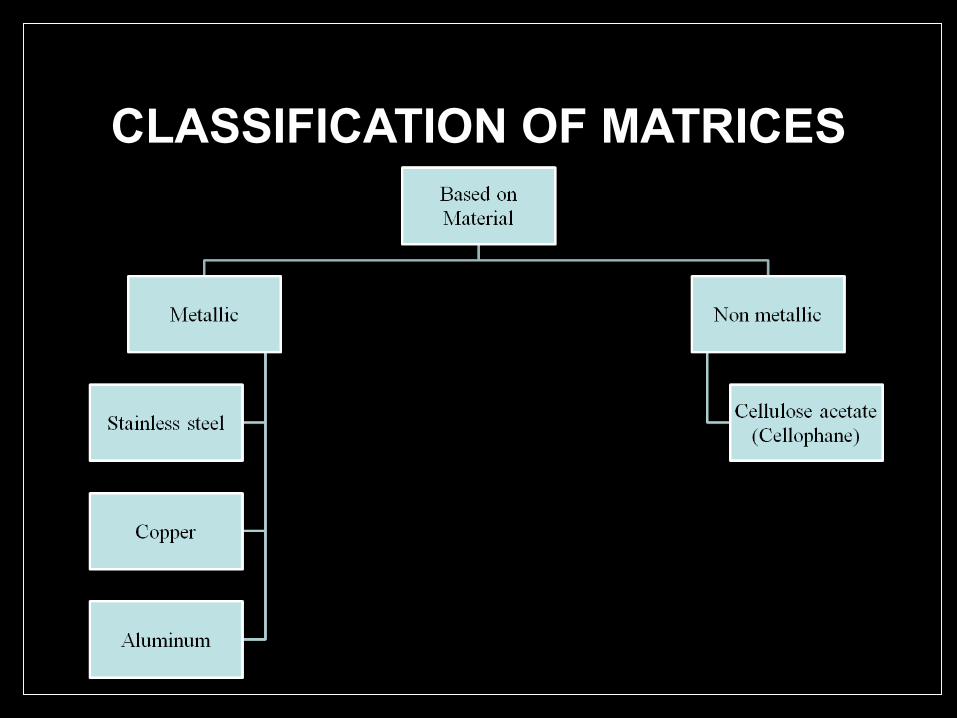
CLASSIFICATION OF MATRICES
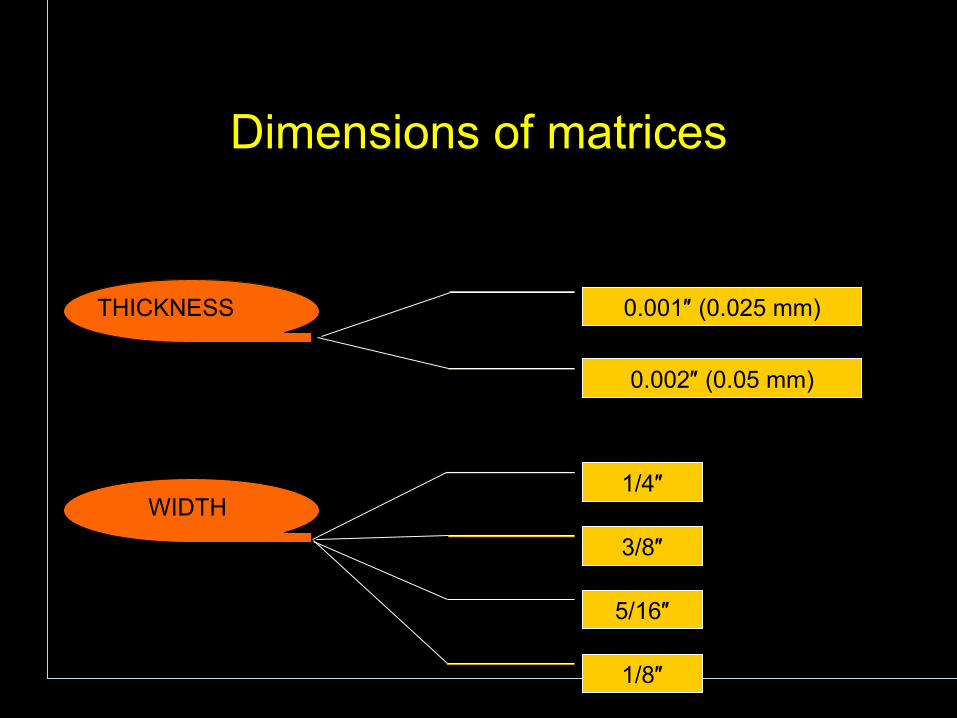
THICKNESS
WIDTH
0.001″ (0.025 mm)
0.002″ (0.05 mm)
1/4″
3/8″
5/16″
1/8″
Dimensions of matrices
T band
Spot-welded matrix
AutoMatrix
Sectional matrix
Tofflemire matrix
Matrices commonly used in pediatric dentistry
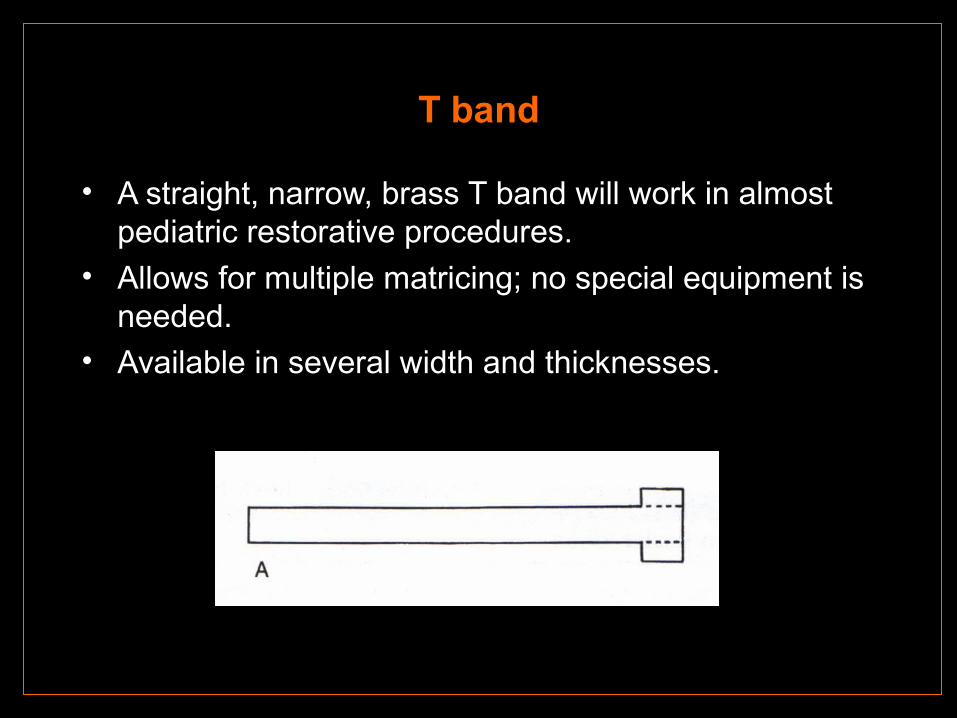
T band
• A straight, narrow, brass T band will work in almost pediatric restorative procedures.
• Allows for multiple matricing; no special equipment is needed.
• Available in several width and thicknesses.
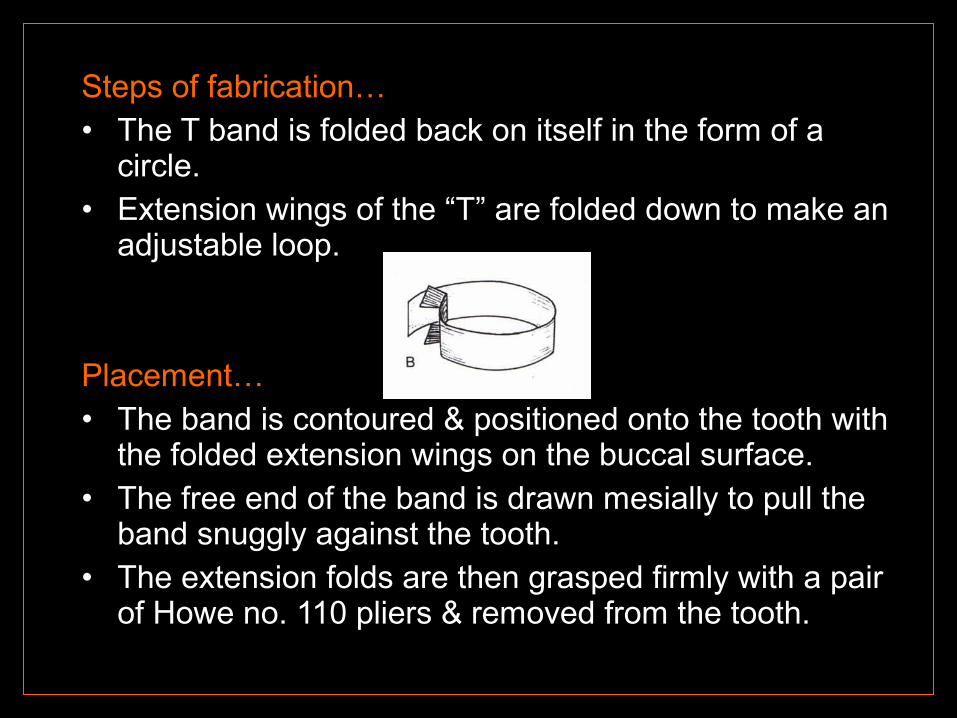
Steps of fabrication…• The T band is folded back on itself in the form of a
circle.• Extension wings of the “T” are folded down to make an
adjustable loop.
Placement…• The band is contoured & positioned onto the tooth with
the folded extension wings on the buccal surface.• The free end of the band is drawn mesially to pull the
band snuggly against the tooth.• The extension folds are then grasped firmly with a pair
of Howe no. 110 pliers & removed from the tooth.
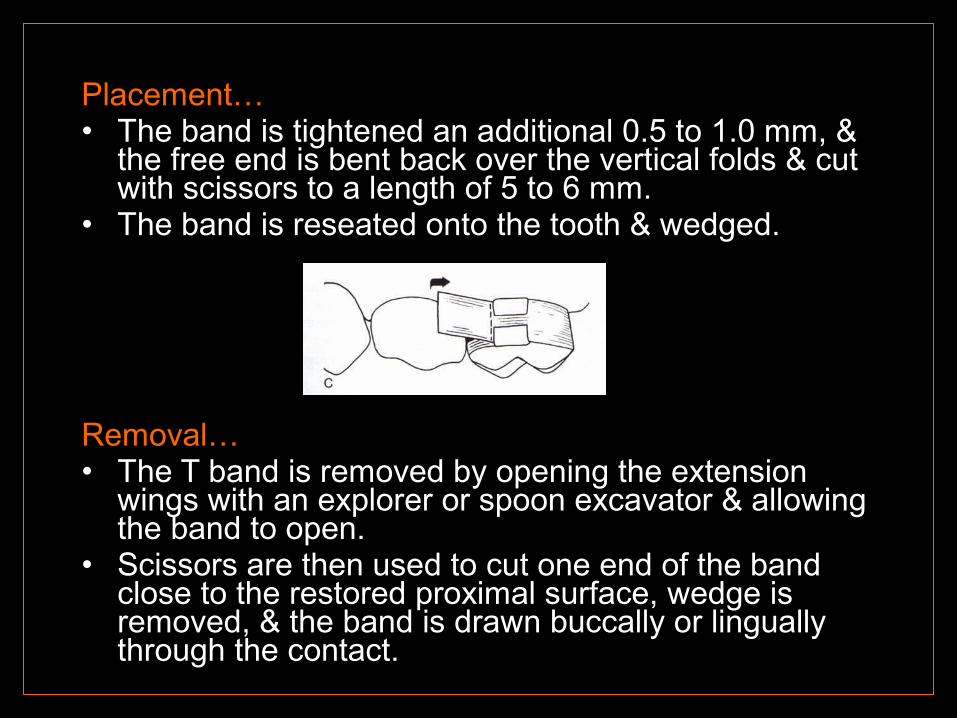
Placement…• The band is tightened an additional 0.5 to 1.0 mm, &
the free end is bent back over the vertical folds & cut with scissors to a length of 5 to 6 mm.
• The band is reseated onto the tooth & wedged.
Removal…• The T band is removed by opening the extension
wings with an explorer or spoon excavator & allowing the band to open.
• Scissors are then used to cut one end of the band close to the restored proximal surface, wedge is removed, & the band is drawn buccally or lingually through the contact.
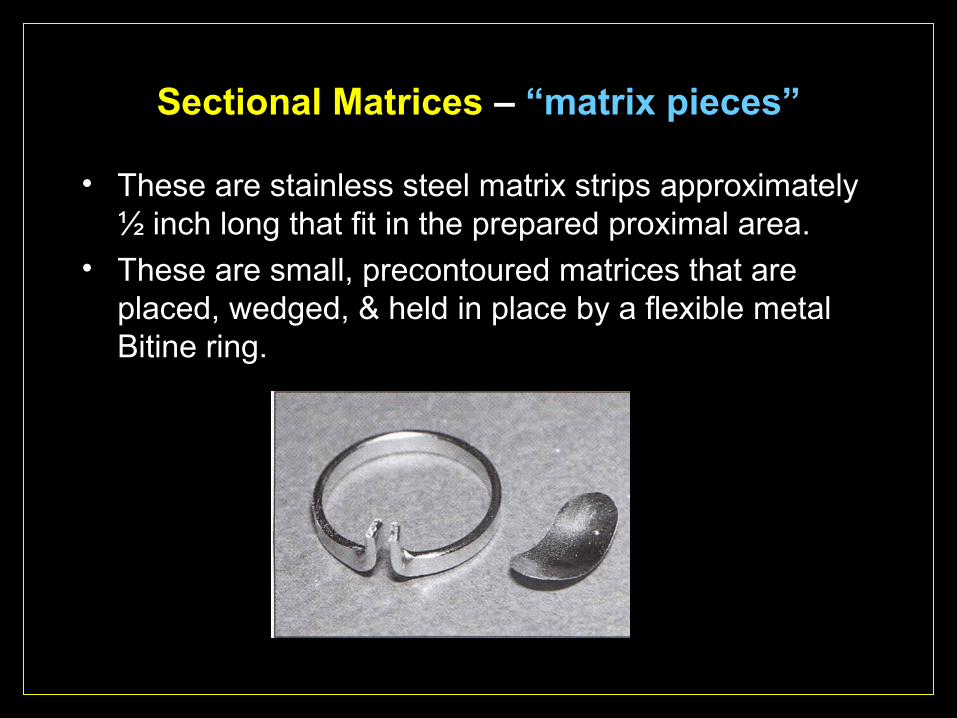
Sectional Matrices – “matrix pieces”
• These are stainless steel matrix strips approximately ½ inch long that fit in the prepared proximal area.
• These are small, precontoured matrices that are placed, wedged, & held in place by a flexible metal Bitine ring.
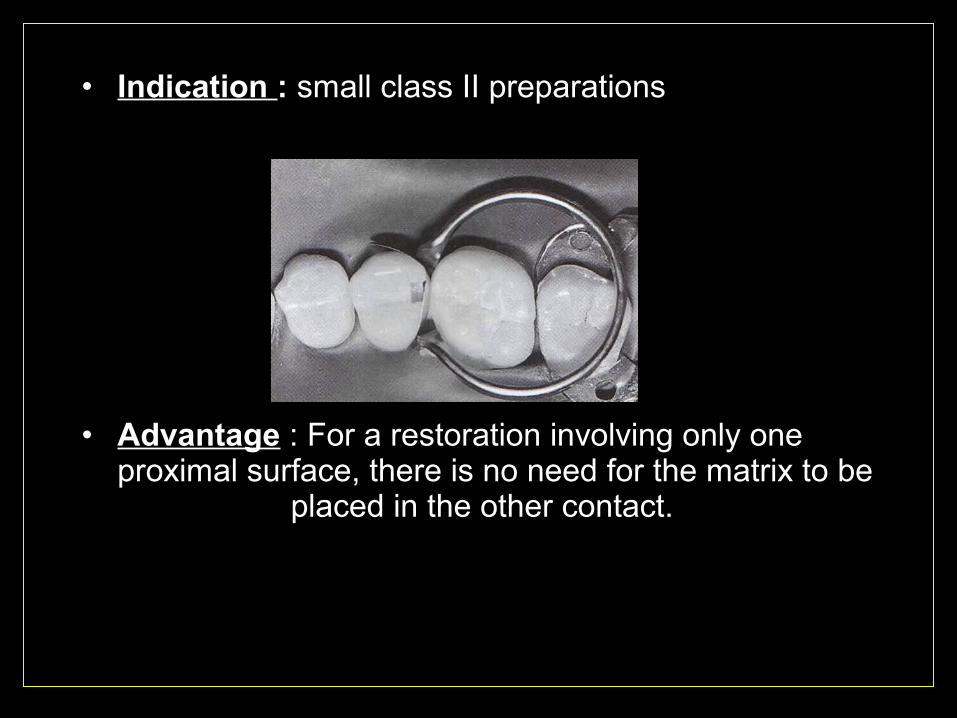
• Indication : small class II preparations
• Advantage : For a restoration involving only one proximal surface, there is no need for the matrix to be
placed in the other contact.
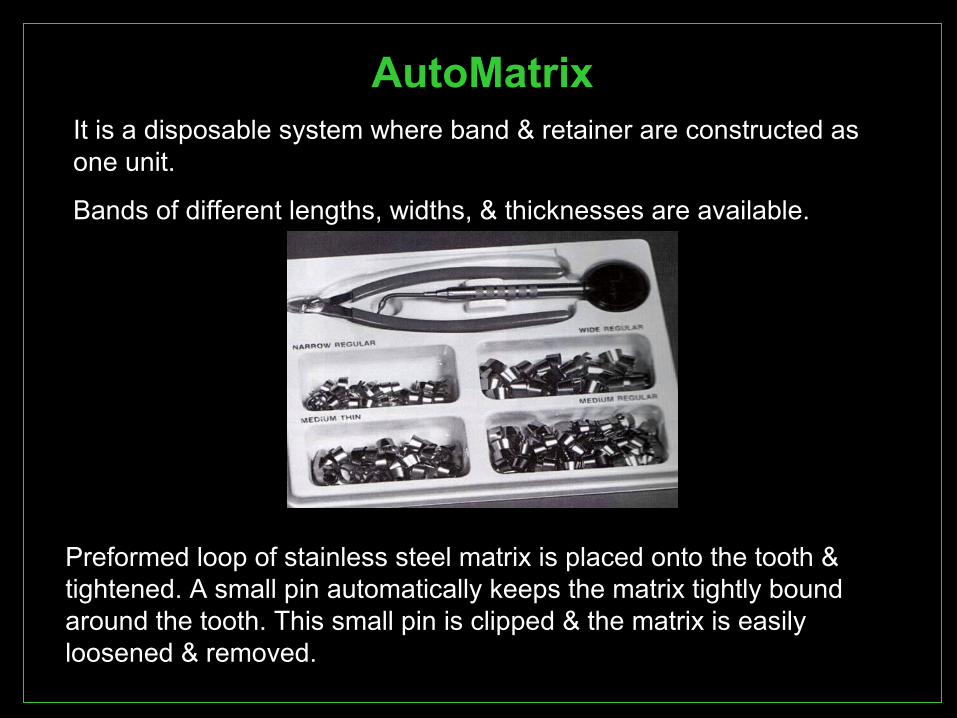
AutoMatrixIt is a disposable system where band & retainer are constructed as one unit.
Bands of different lengths, widths, & thicknesses are available.
Preformed loop of stainless steel matrix is placed onto the tooth & tightened. A small pin automatically keeps the matrix tightly bound around the tooth. This small pin is clipped & the matrix is easily loosened & removed.
• Indication : In extensive cavity preparations.
• Limitations : - Instability of the system.
Proper contour & proximal contact difficult to achieve.
• Advantages : - allows for multiple matrix placement
- very easy to use
- useful in patients who cannot tolerate retainers.
- useful in patients with partly erupted teeth where the height of the buccal or lingual tooth surfaces provide insufficient support for the retainers.
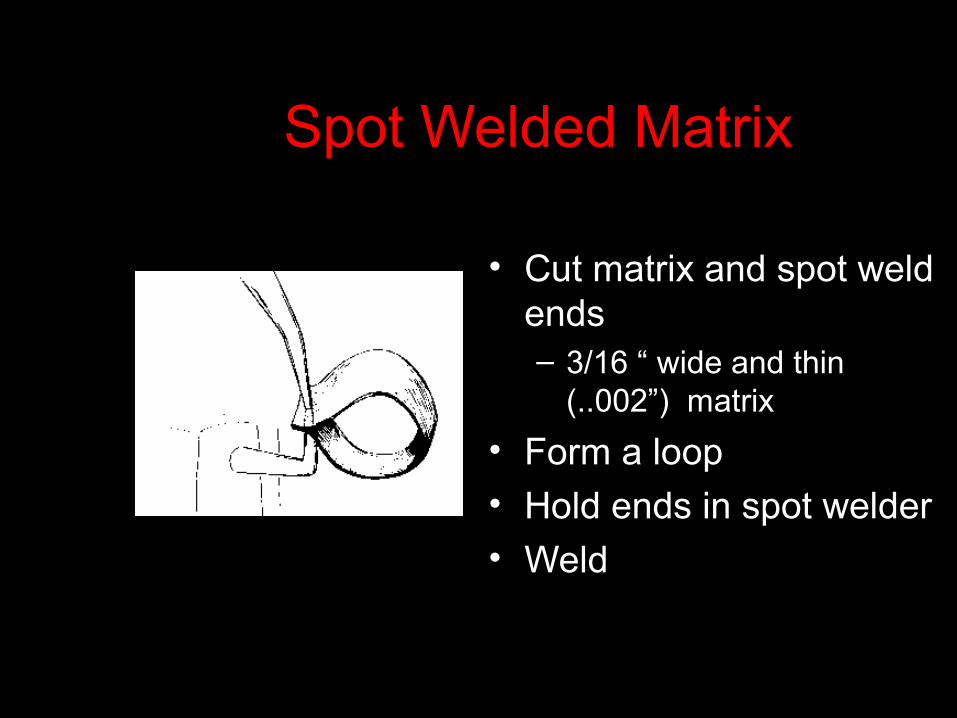
Spot Welded Matrix
• Cut matrix and spot weld ends– 3/16 “ wide and thin
(..002”) matrix
• Form a loop• Hold ends in spot welder• Weld
Adapting Matrix Band
• Place band over tooth with welded end on buccal
• Seat band so that it extends .5-1mm gingival to the cavosurface margin
• Band should extend occlusally .5-1mm beyond the marginal ridge
• Stabilize band with finger
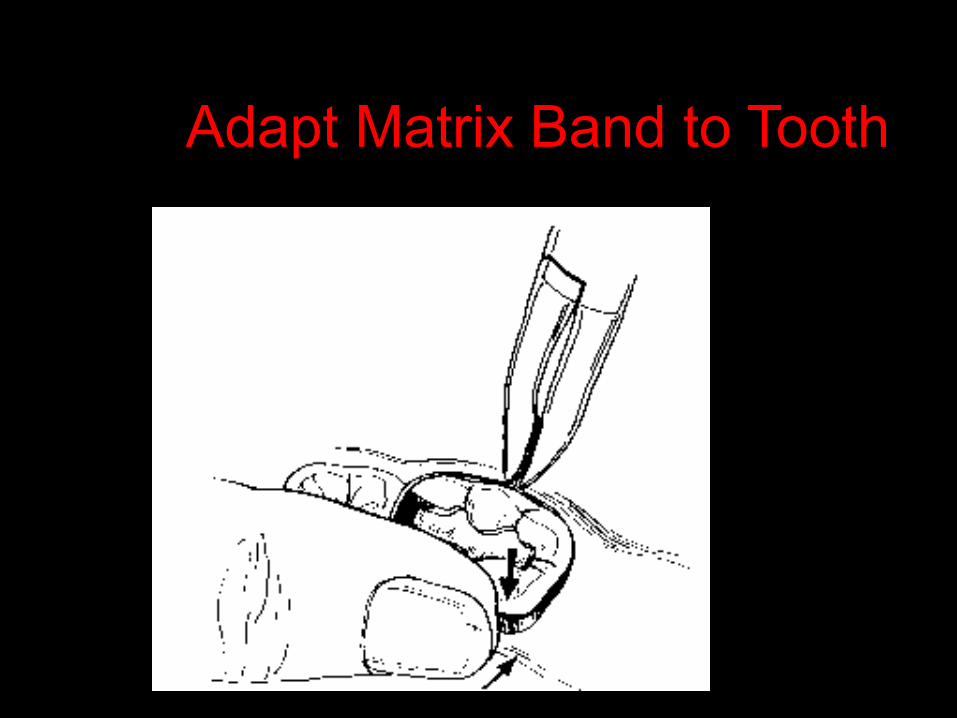
Adapt Matrix Band to Tooth
Spot Welded Matrix, continued
• Grasp welded ends with flat-nose, serrated pliers (#110)
• Pliers should be at center of buccal surface of tooth as you pull band tightly
• Spot weld band at crease and trim ends
• Return to tooth and wedge properly
• Remove matrix by inserting flat blade instrument between tooth and matrix at crease
Tofflemire matrix
Universal matrix system, introduced by B.R. Tofflemire.
Indication : - three surfaces restoration (mesial, occlusal, distal) of a posterior tooth.
- two surface class II restoration.
Advantages : - may be positioned on facial & lingual aspect of the tooth.
- retainer is easily separated from the band to expedite removal of the band.
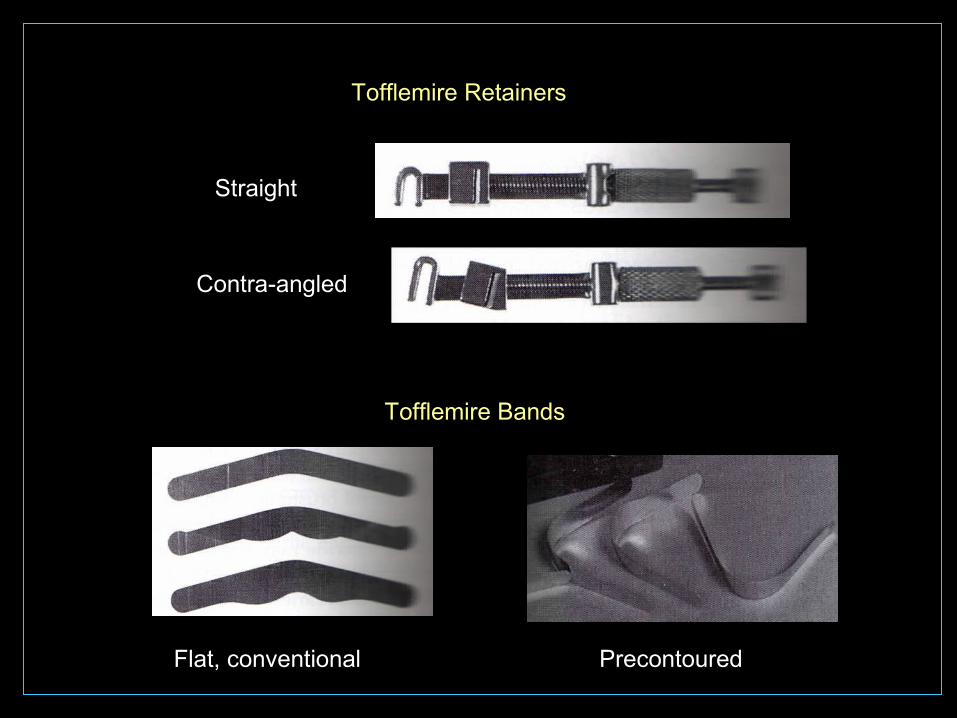
Tofflemire Retainers
Tofflemire Bands
Straight
Contra-angled
Flat, conventional Precontoured
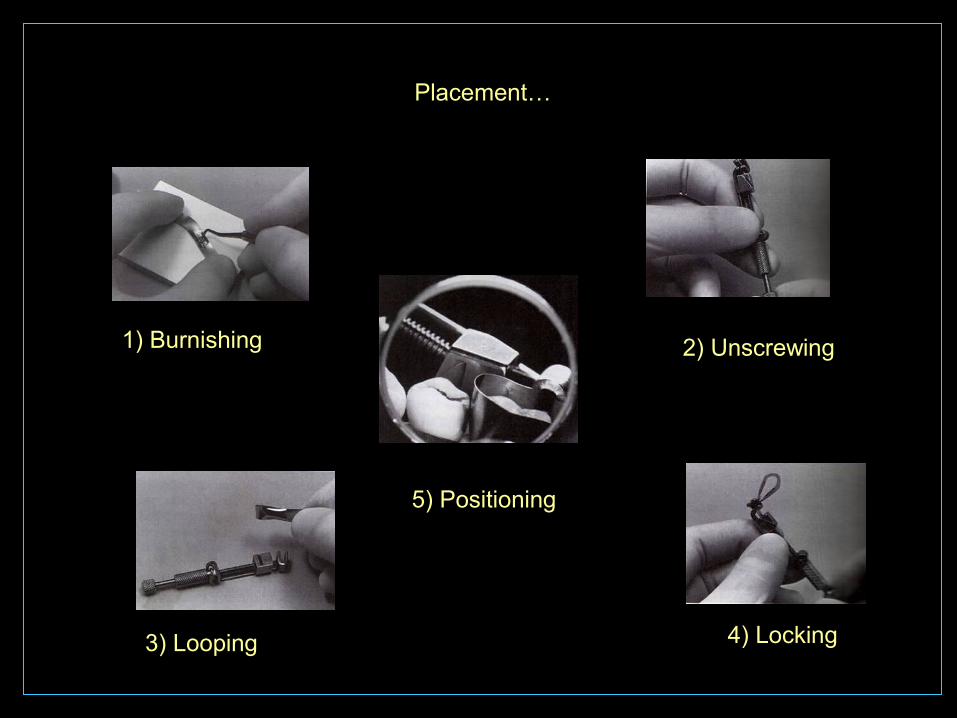
Placement…
1) Burnishing 2) Unscrewing
3) Looping 4) Locking
5) Positioning
WEDGES
PURPOSE OF WEDGING :• Prevents surplus amalgam being forced into the
gingival crevice.
• Assists in contouring the cervical part of the proximal surface.
• Separates the teeth to compensate for the thickness of the matrix band such that proximal contacts is reestablished when the band is removed.
• Adapts and stabilizes the matrix band close to the tooth.
• Protects the gingival papilla
Types of wedges
Material
Cross sectional shape
plastic
wooden
Round
Triangular
A proper wedge…
• Must be triangular or round in cross-section.• Width of the base should be slightly larger than
the space between the tooth to be restored & the neighboring tooth in order to separate the teeth.
• Occlusally the wedges must not be too thick as this may influence the proximal contour.
• A uniform tapering of the wedge is needed in order to render sufficient contact throughout the proximal embrasure.
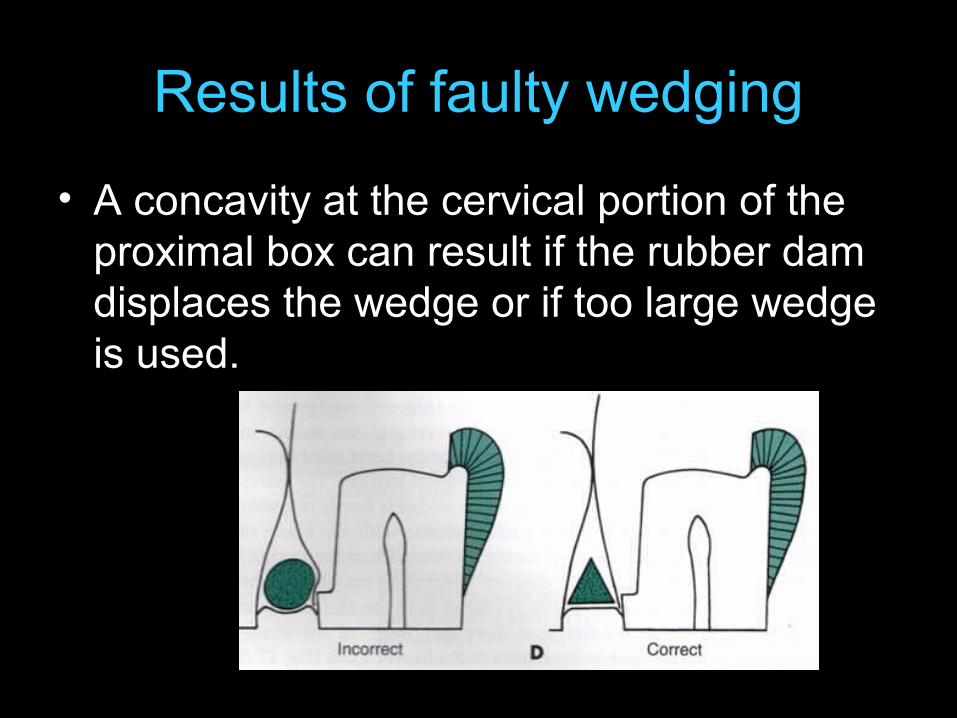
Results of faulty wedging
• A concavity at the cervical portion of the proximal box can result if the rubber dam displaces the wedge or if too large wedge is used.
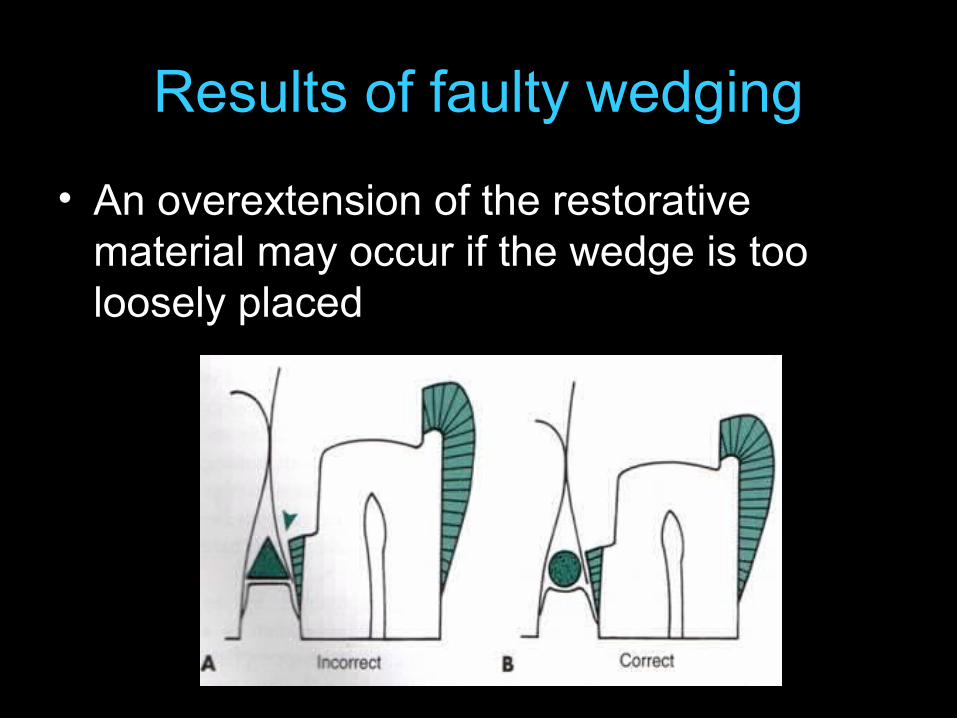
Results of faulty wedging
• An overextension of the restorative material may occur if the wedge is too loosely placed

Placement of wedges…
• Wedge may be inserted buccally or lingually.
• In general, the wedge is inserted from the lingual, as this embrasure is normally larger in size.
• In case of mandibular teeth - it is preferred from buccal side.
• In case of maxillary teeth - it is preferred from palatal side.
The clinician should have an adequate knowledge of the anatomical & functional aspects of contacts & contours so as to reproduce them with ideal restorative materials.
Extensive knowledge about the matricing serves as a guide to reproduce near to normal contacts between teeth, which in turn help to maintain the oral cavity in sound health.
Isolation techniques

Introduction
To restore primary teeth to a high standard the operating area has to be well isolated
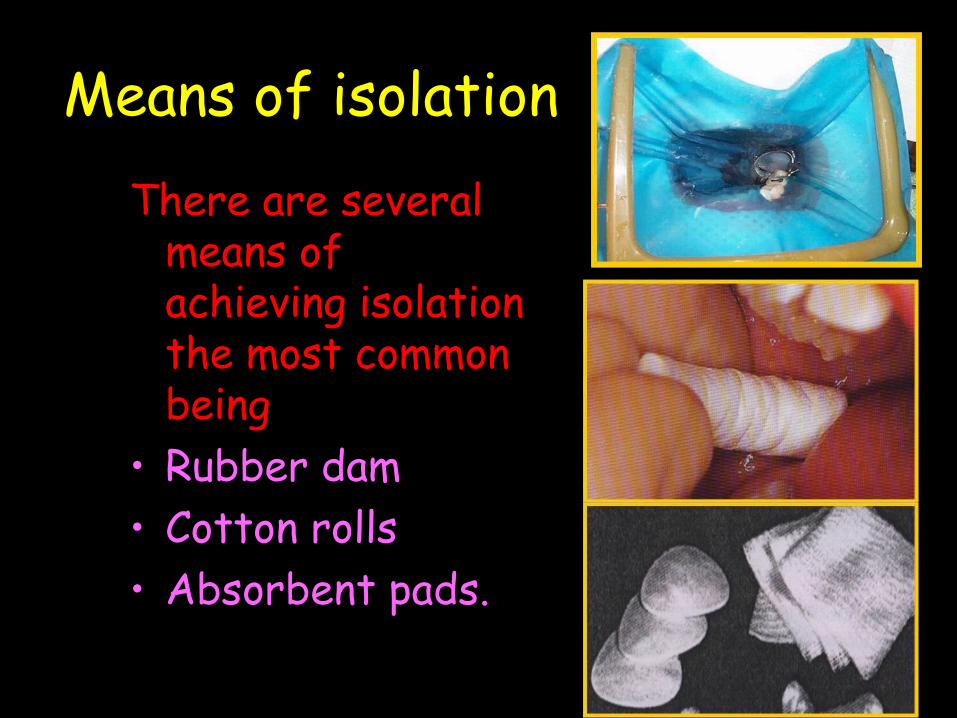
Means of isolationThere are several
means of achieving isolation the most common being
• Rubber dam• Cotton rolls• Absorbent pads.
Rubber dam provides the best possible isolation by far.
In 1964 S.C.Barnum a New York city dentist introduced the rubber dam into dentistry.
It is used to define the operating field by isolating one or more teeth from oral environment.
When excavating a deep carious lesions and risking pulpal exposure, use of the rubber dam is strongly recommended to prevent pulpal contamination from oral fluids.
Advantages • Provision of dry clean operating field.• Improvement of access & visibility by eliminating
tongue, lip, cheeks & saliva from the operating field .• Retraction & protection of soft tissues.• Prevention of inhalation & ingestion of foreign
bodies.• Improved properties of dental materials • Aid to patient management.• Aid to cross-infection control by reducing aerosol
spread of micro-organisms.• Minimization of mouth breathing during inhalation
sedation procedures
Disadvantages
• Usage is low amongst private practitioners.• Cannot be used in case of extremely
malpositioned teeth.• Children suffering from asthma ,some upper
respiratory infections or mouth breathing problems.
Armamentarium1. Rubberdam sheets2. Rubberdam clamps3. Rubberdam holders(frame)4. Rubberdam retainer forceps5. Rubberdam punch6. Rubberdam templates or stamps7. Dental floss8. Wedget9.Wooden wedges, orthodontic elastics.
Rubber dam sheets Rubber dam sheets of different gauges
available Thin (0.005”-0.007”) Medium (0.007”-0.009”) Heavy (0.009”-0.0115”) Extra heavy (0.0115”-0.0135”) Special heavy (0.0135”-0.0155”)
Rubberdam sheetsDifferent colorsPink blue purple green etc6X6” adult use5x5” pedo useMay be flavored for childrenAlso available in rolls (80” or 21”)Thin sheets more comfortable for patientAlso easy to apply for the dentistThick sheets provide more tissue
retraction and better isolation by means of tighter fit
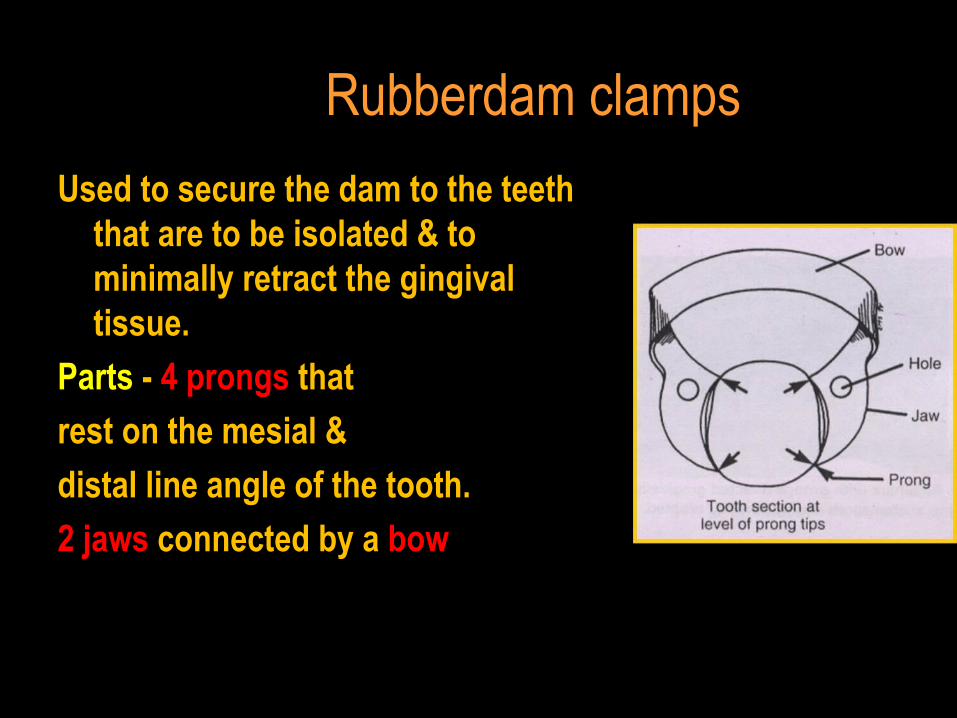
Rubberdam clamps
Used to secure the dam to the teeth that are to be isolated & to minimally retract the gingival tissue.
Parts - 4 prongs that
rest on the mesial &
distal line angle of the tooth.
2 jaws connected by a bow
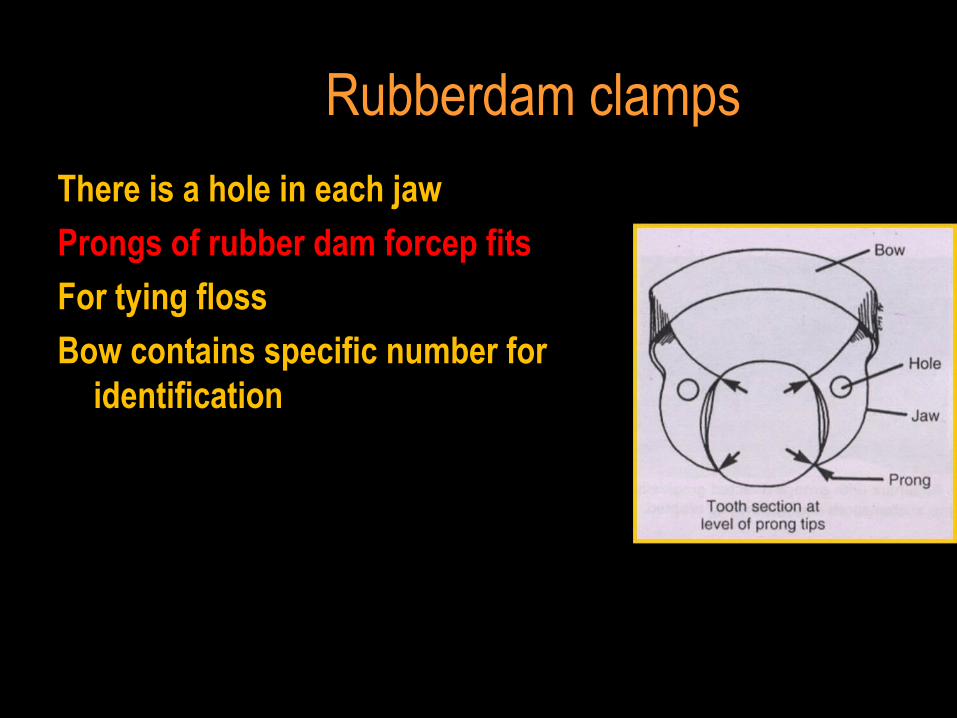
Rubberdam clamps
There is a hole in each jaw
Prongs of rubber dam forcep fits
For tying floss
Bow contains specific number for identification
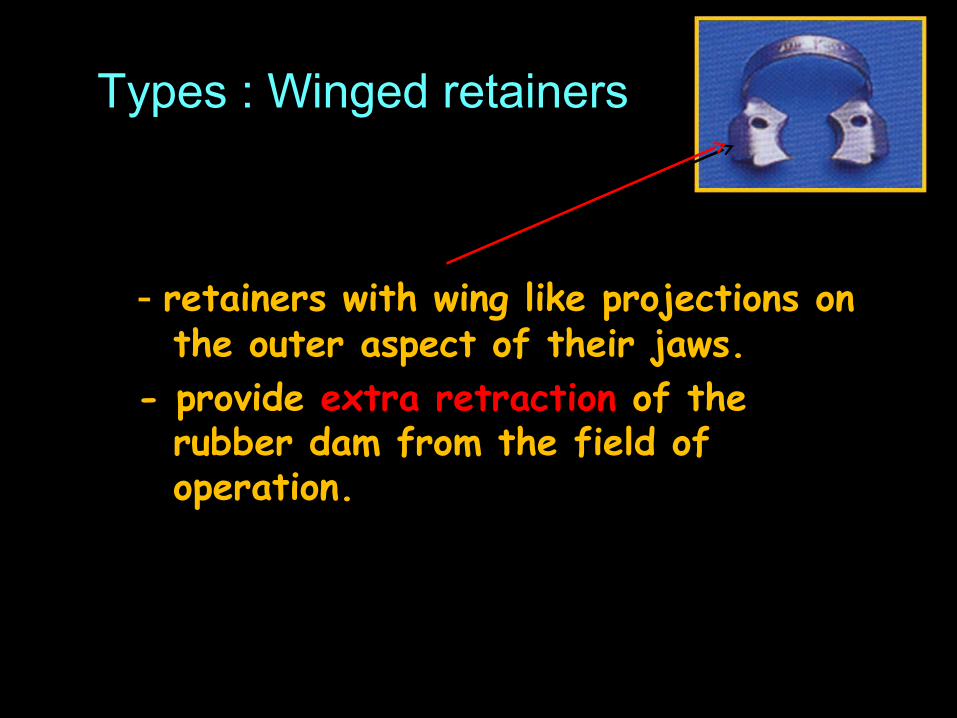
Types : Winged retainers
- retainers with wing like projections on the outer aspect of their jaws.
- provide extra retraction of the rubber dam from the field of operation.
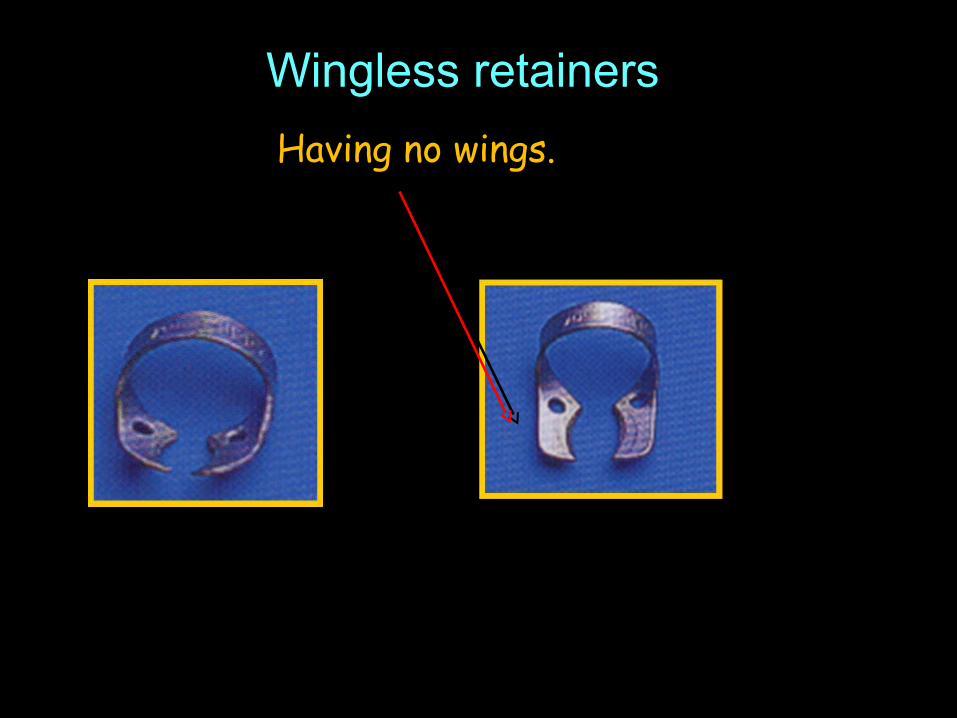
Wingless retainers
Having no wings.
Retainers (clamps) Different clamps for different teethAnterior teethPremolarsMaxillary molarsMandibular molarsPrimary molars or unerrupted small molarUnerrupted large molar
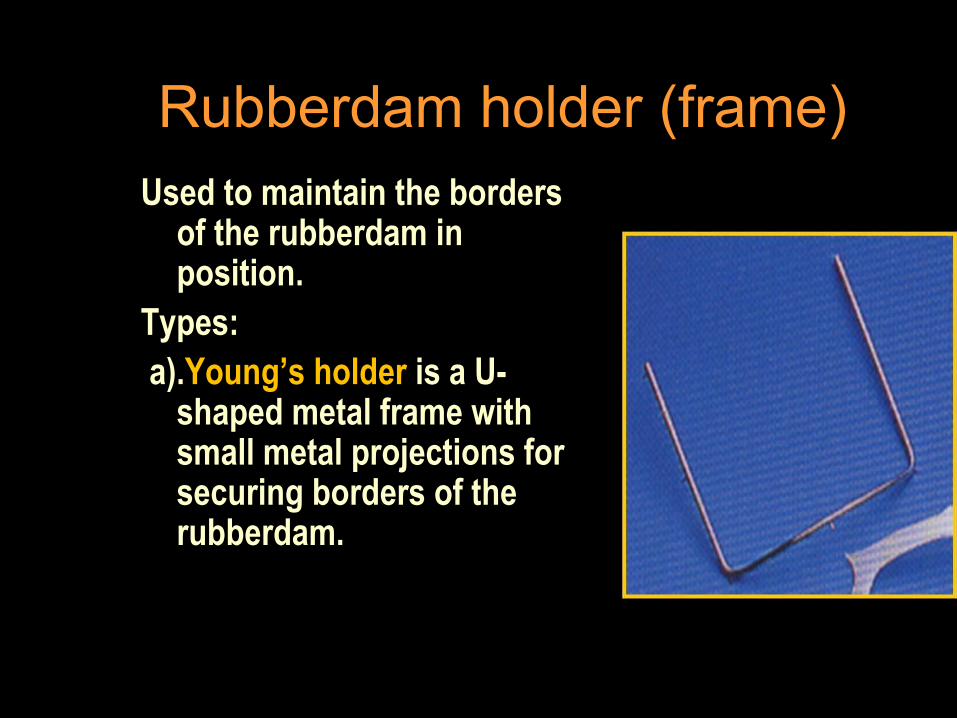
Rubberdam holder (frame)Used to maintain the borders
of the rubberdam in position.
Types: a).Young’s holder is a U-
shaped metal frame with small metal projections for securing borders of the rubberdam.
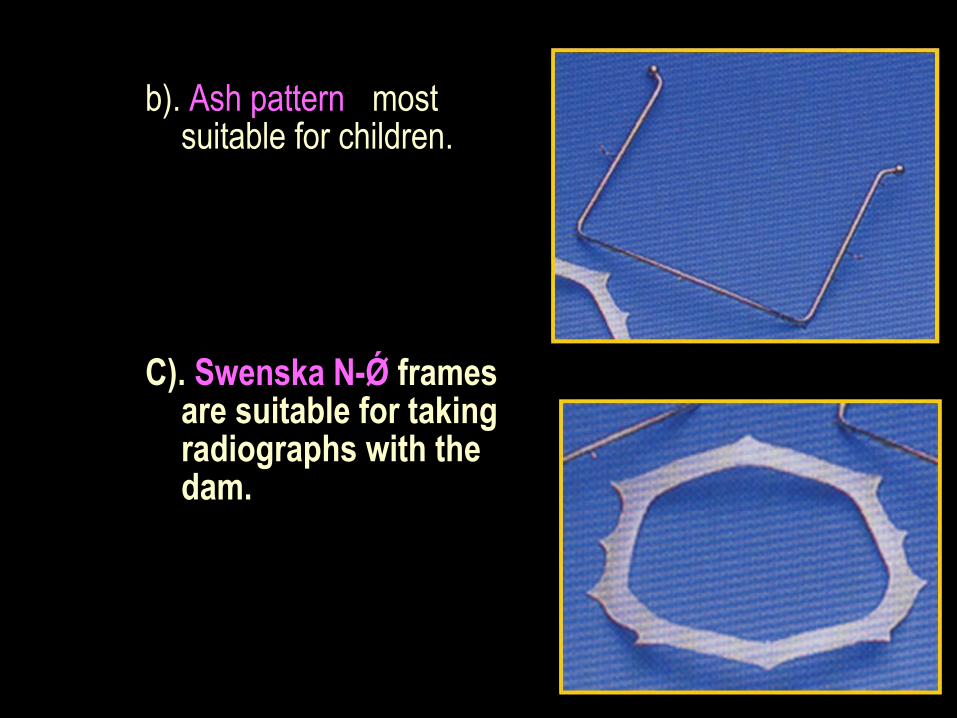
b). Ash pattern - most suitable for children.
C). Swenska N-Ǿ frames are suitable for taking radiographs with the dam.
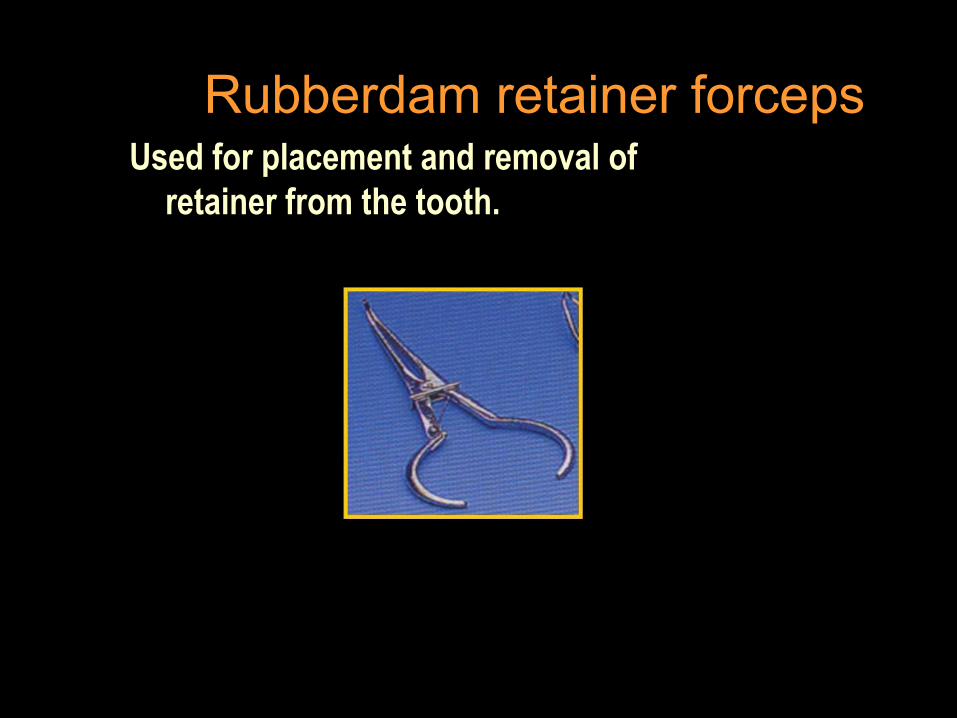
Rubberdam retainer forceps Used for placement and removal of
retainer from the tooth.
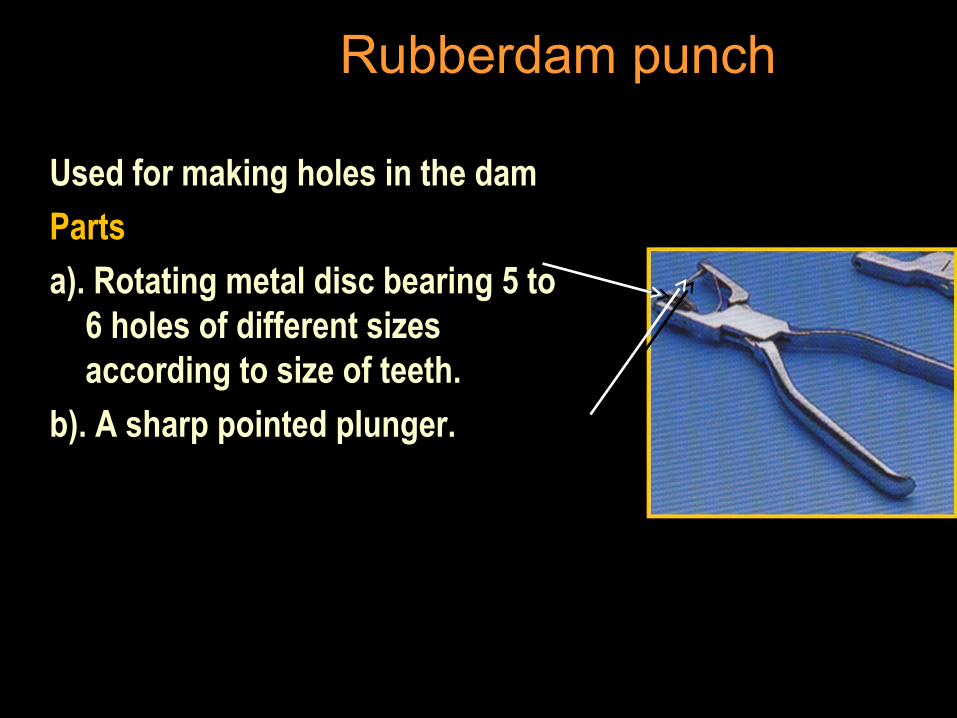
Rubberdam punch
Used for making holes in the dam
Parts
a). Rotating metal disc bearing 5 to 6 holes of different sizes according to size of teeth.
b). A sharp pointed plunger.
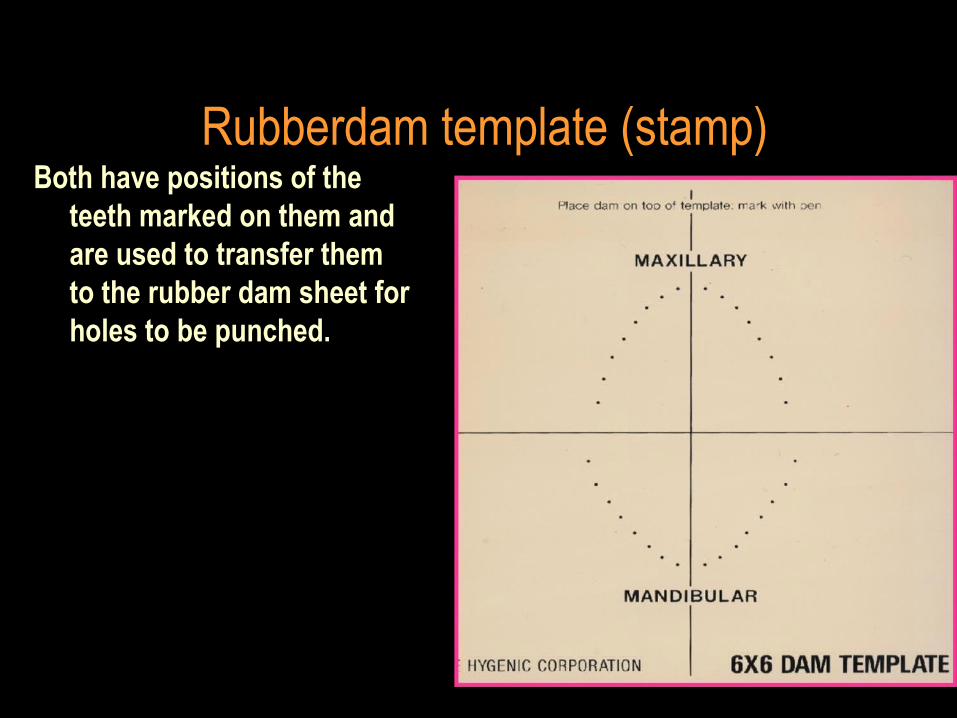
Rubberdam template (stamp)Both have positions of the
teeth marked on them and are used to transfer them to the rubber dam sheet for holes to be punched.

Dental floss
Tied around the retainer before carried to the oral cavity to prevent accidental aspiration of clamp.
8. Wedget an elastic used to secure the dam around
the teeth farthest away from the clamp.
Wedges Orthodontic bands Latex cords
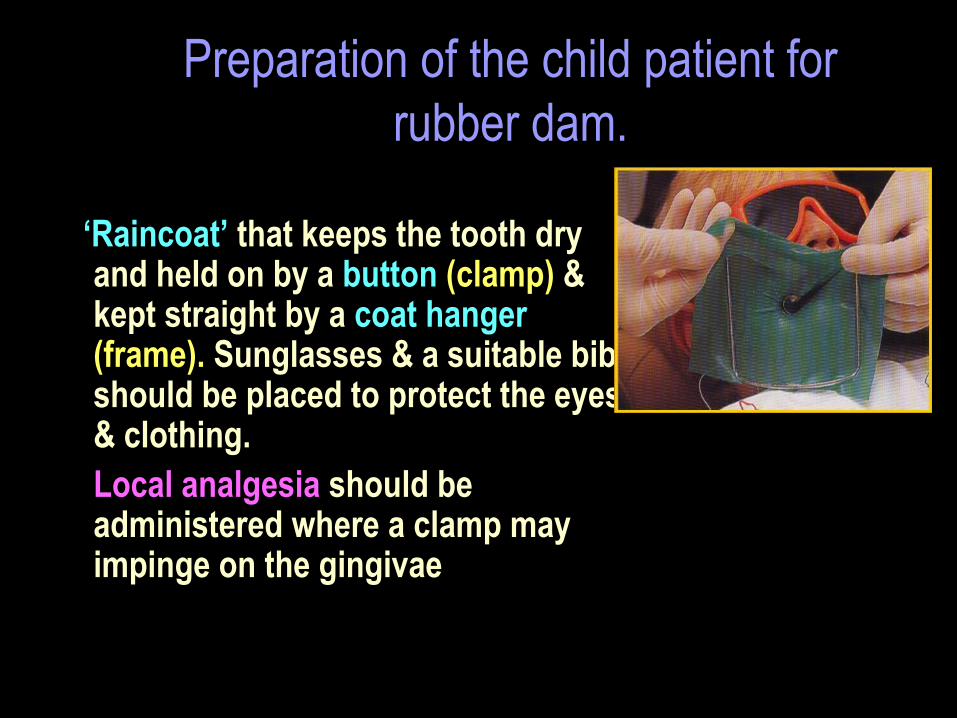
Preparation of the child patient for rubber dam.
The dam can be presented as a ‘Raincoat’ that keeps the tooth dry
and held on by a button (clamp) & kept straight by a coat hanger (frame). Sunglasses & a suitable bib should be placed to protect the eyes & clothing.Local analgesia should be administered where a clamp may impinge on the gingivae
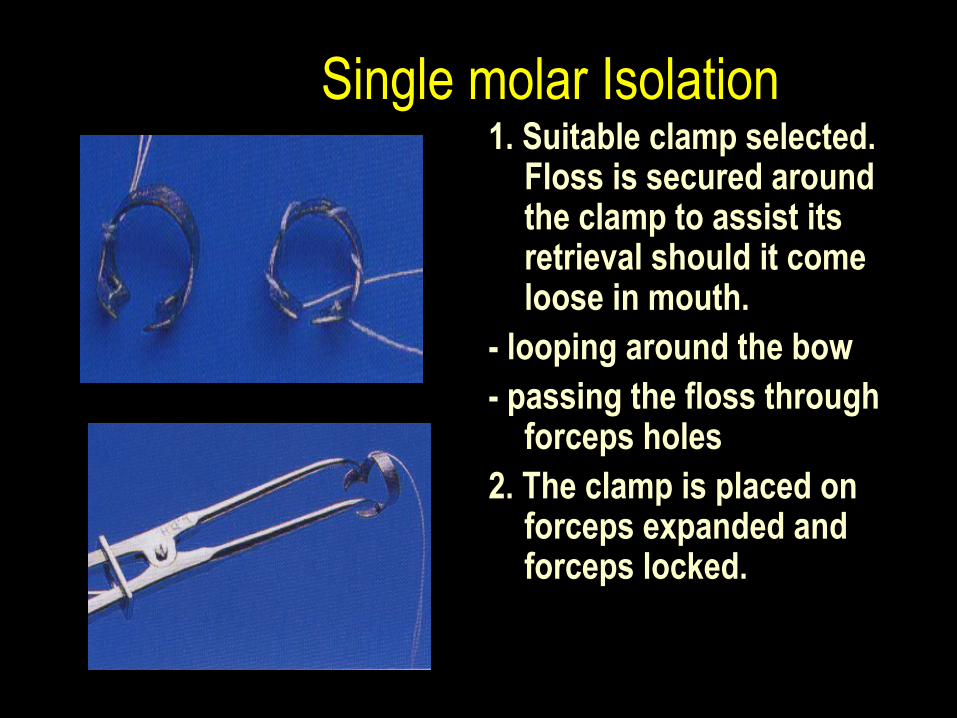
Single molar Isolation1. Suitable clamp selected.
Floss is secured around the clamp to assist its retrieval should it come loose in mouth.
- looping around the bow- passing the floss through
forceps holes2. The clamp is placed on
forceps expanded and forceps locked.
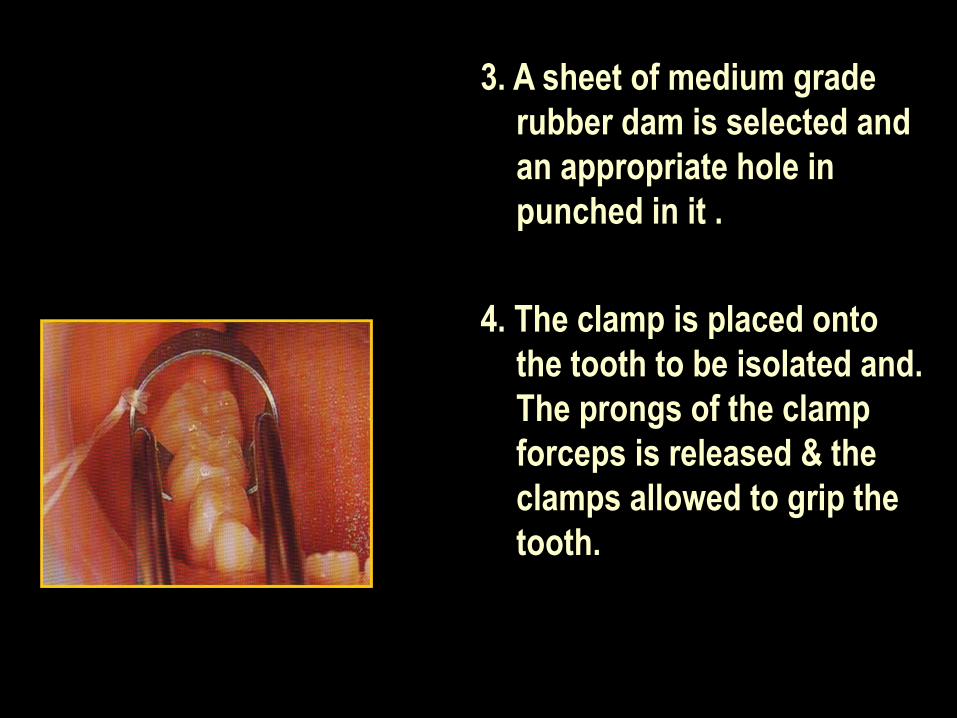
3. A sheet of medium grade rubber dam is selected and an appropriate hole in punched in it .
4. The clamp is placed onto the tooth to be isolated and. The prongs of the clamp forceps is released & the clamps allowed to grip the tooth.
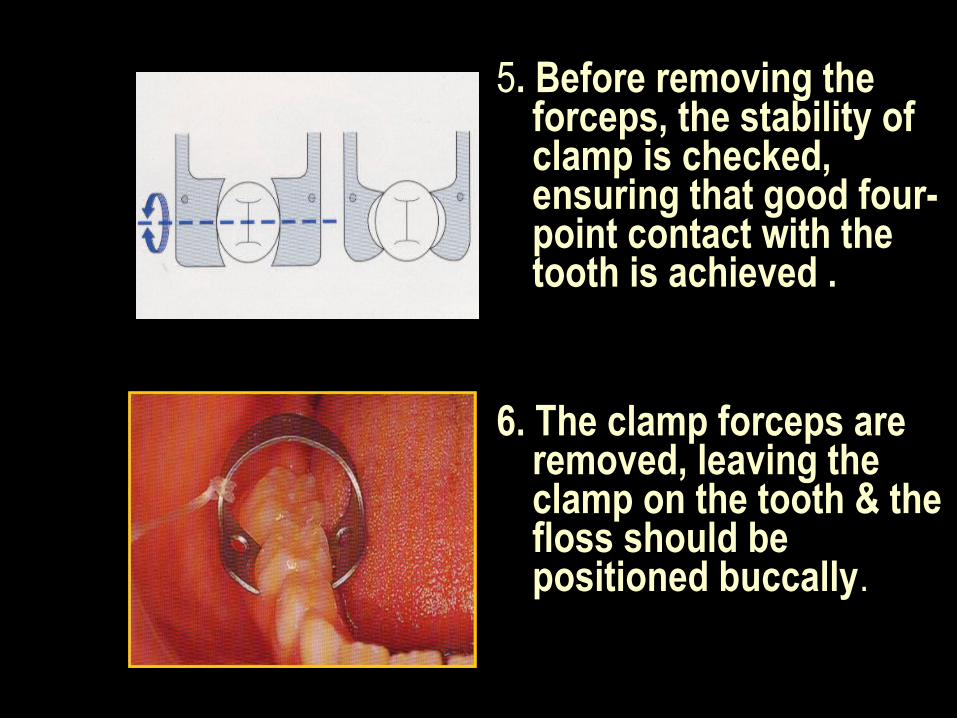
5. Before removing the forceps, the stability of clamp is checked, ensuring that good four-point contact with the tooth is achieved .
6. The clamp forceps are removed, leaving the clamp on the tooth & the floss should be positioned buccally.
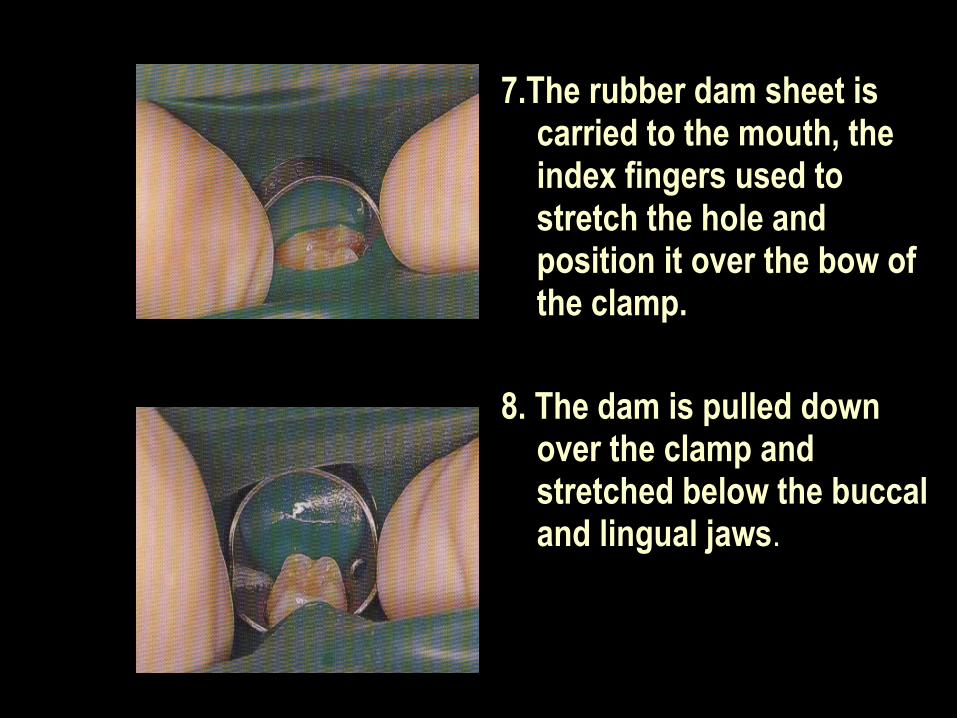
7.The rubber dam sheet is carried to the mouth, the index fingers used to stretch the hole and position it over the bow of the clamp.
8. The dam is pulled down over the clamp and stretched below the buccal and lingual jaws.
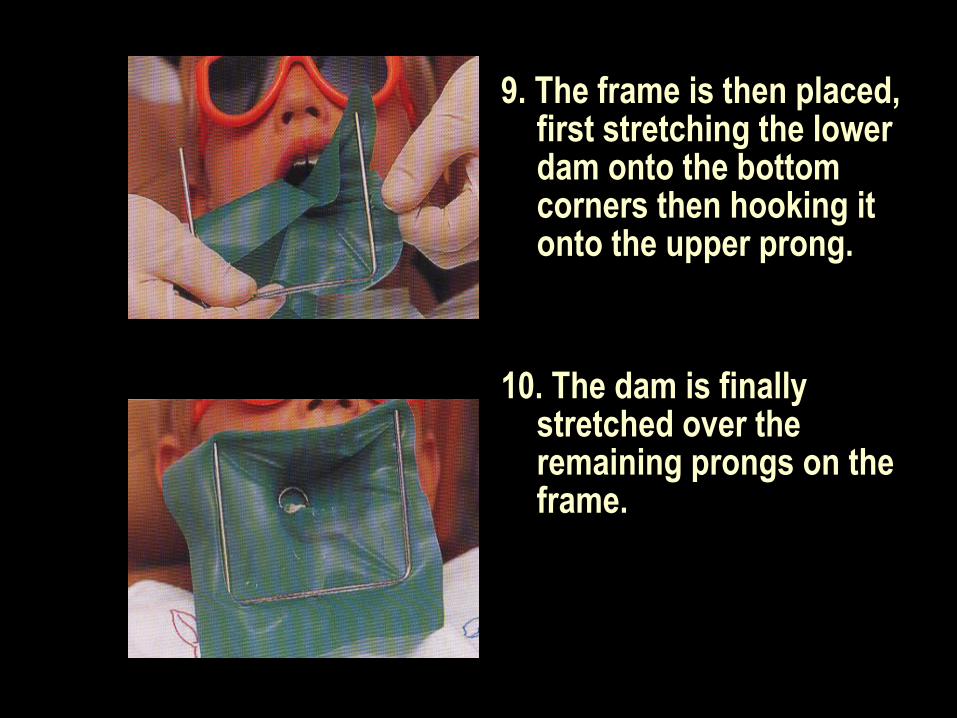
9. The frame is then placed, first stretching the lower dam onto the bottom corners then hooking it onto the upper prong.
10. The dam is finally stretched over the remaining prongs on the frame.
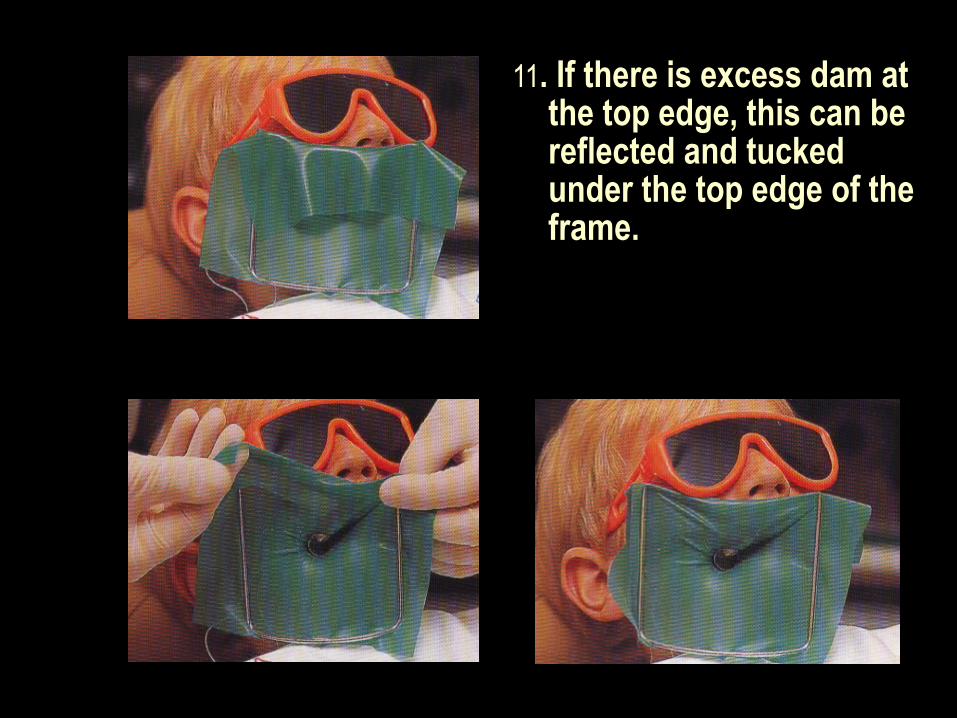
11. If there is excess dam at the top edge, this can be reflected and tucked under the top edge of the frame.
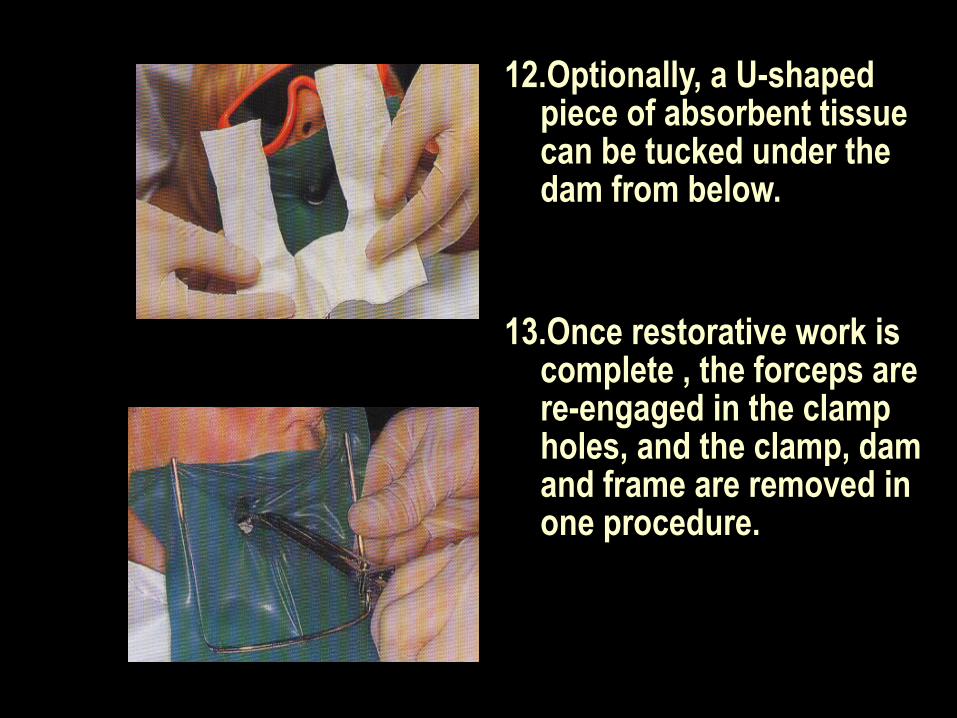
12.Optionally, a U-shaped piece of absorbent tissue can be tucked under the dam from below.
13.Once restorative work is complete , the forceps are re-engaged in the clamp holes, and the clamp, dam and frame are removed in one procedure.
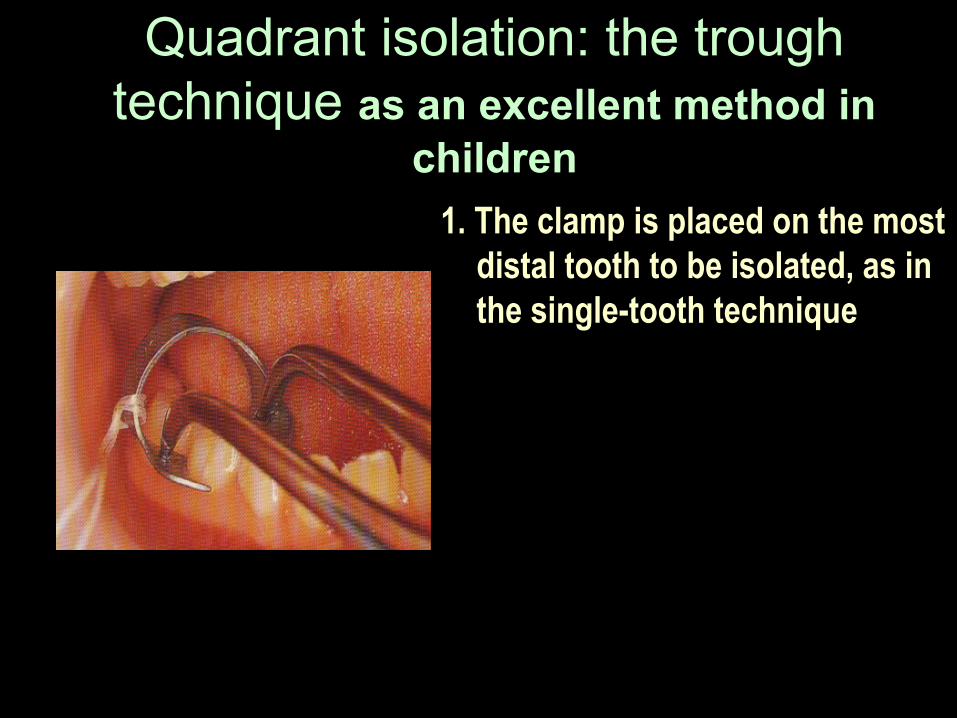
Quadrant isolation: the trough technique as an excellent method in
children
1. The clamp is placed on the most distal tooth to be isolated, as in the single-tooth technique
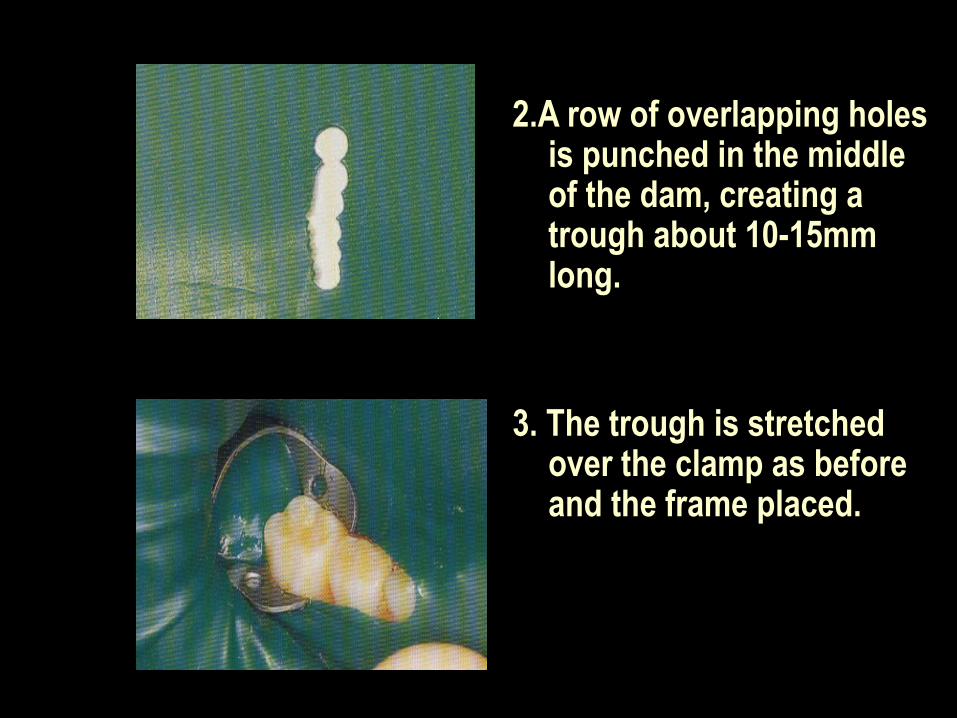
2.A row of overlapping holes is punched in the middle of the dam, creating a trough about 10-15mm long.
3. The trough is stretched over the clamp as before and the frame placed.
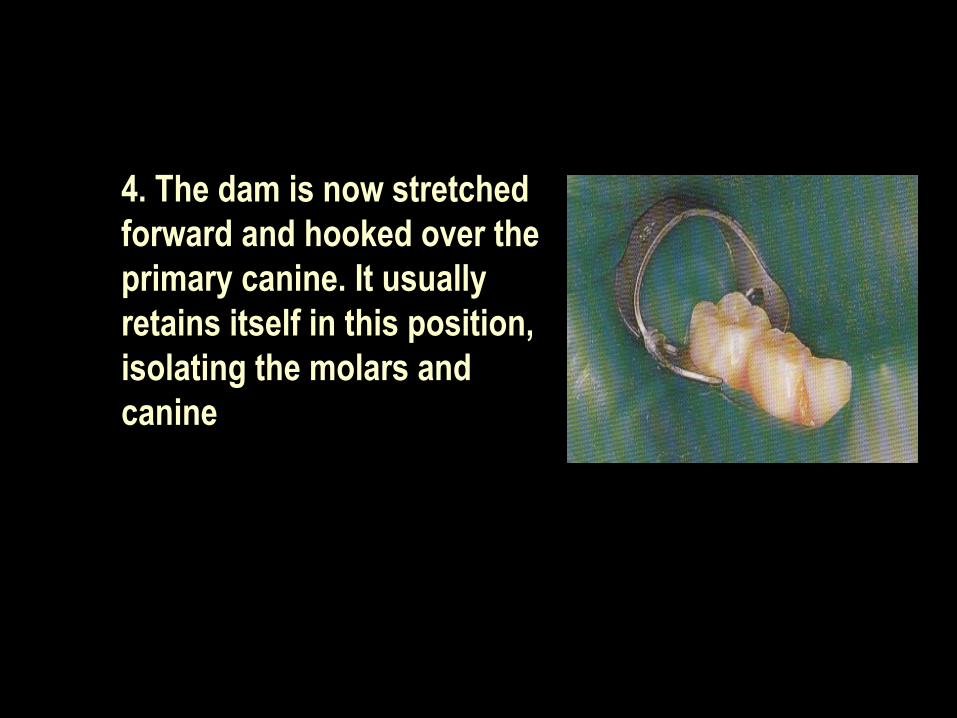
4. The dam is now stretched forward and hooked over the primary canine. It usually retains itself in this position, isolating the molars and canine
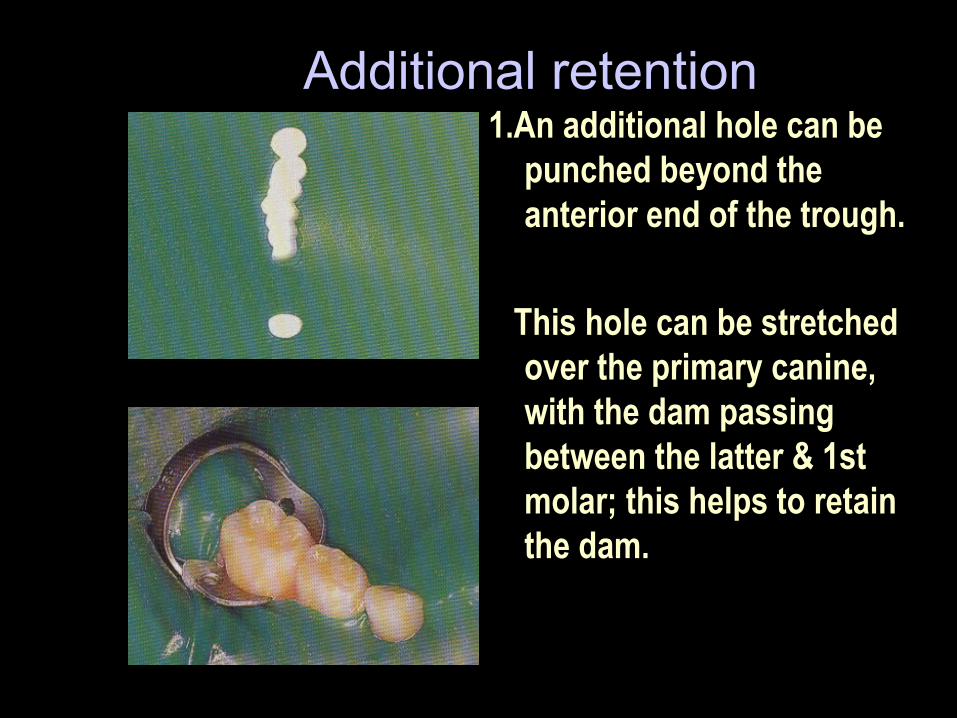
Additional retention 1.An additional hole can be
punched beyond the anterior end of the trough.
This hole can be stretched over the primary canine, with the dam passing between the latter & 1st molar; this helps to retain the dam.
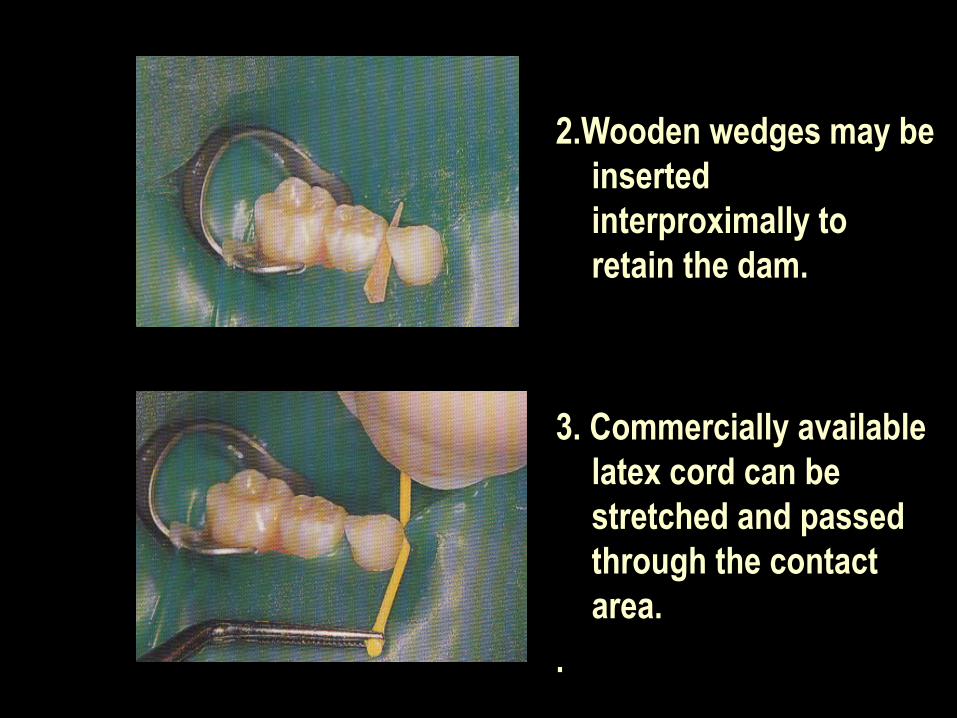
2.Wooden wedges may be inserted interproximally to retain the dam.
3. Commercially available latex cord can be stretched and passed through the contact area.
.
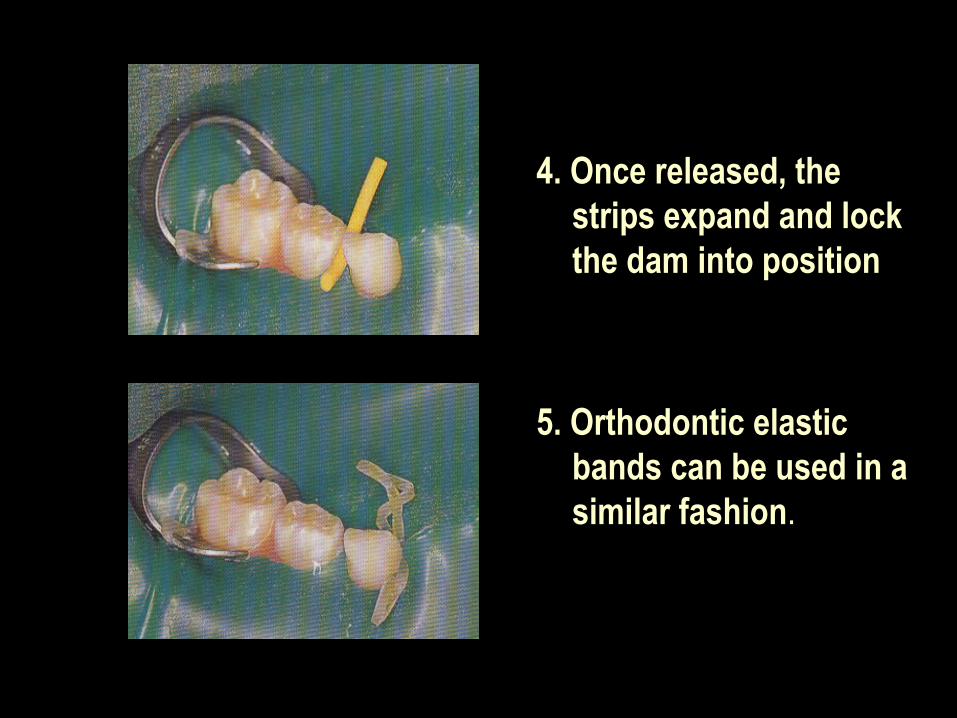
4. Once released, the strips expand and lock the dam into position
5. Orthodontic elastic bands can be used in a similar fashion.
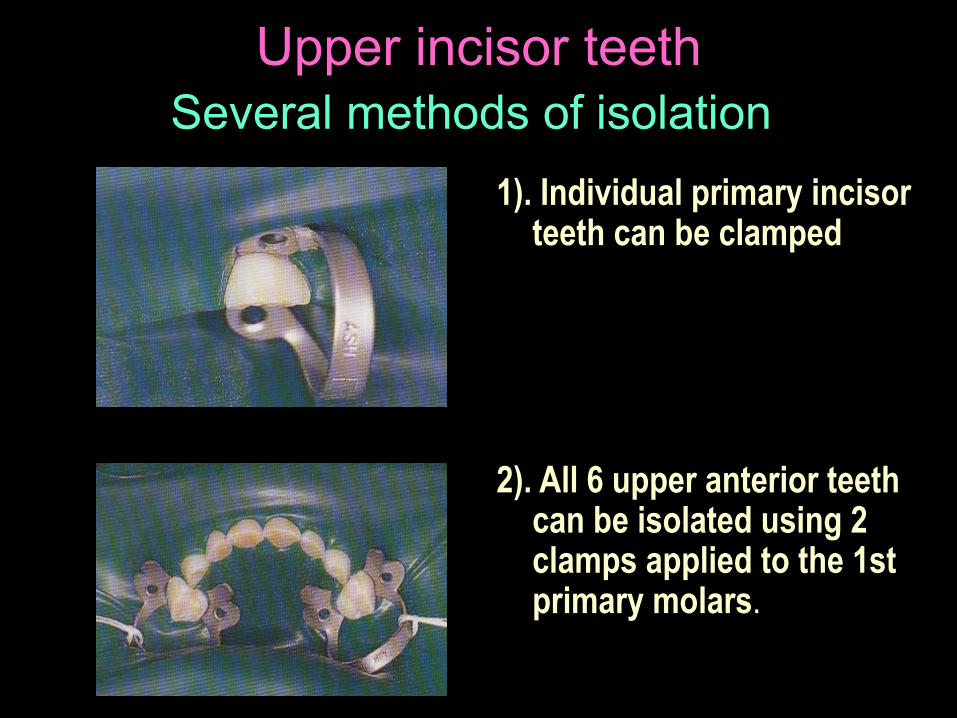
Upper incisor teethSeveral methods of isolation
1). Individual primary incisor teeth can be clamped
2). All 6 upper anterior teeth can be isolated using 2 clamps applied to the 1st primary molars.
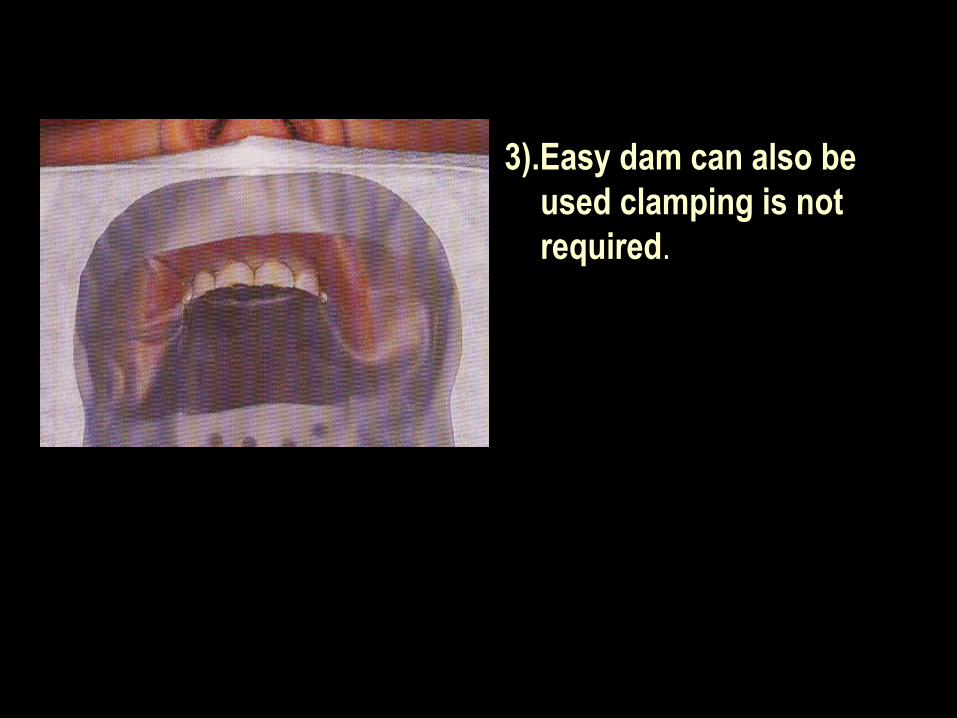
3).Easy dam can also be used clamping is not required.
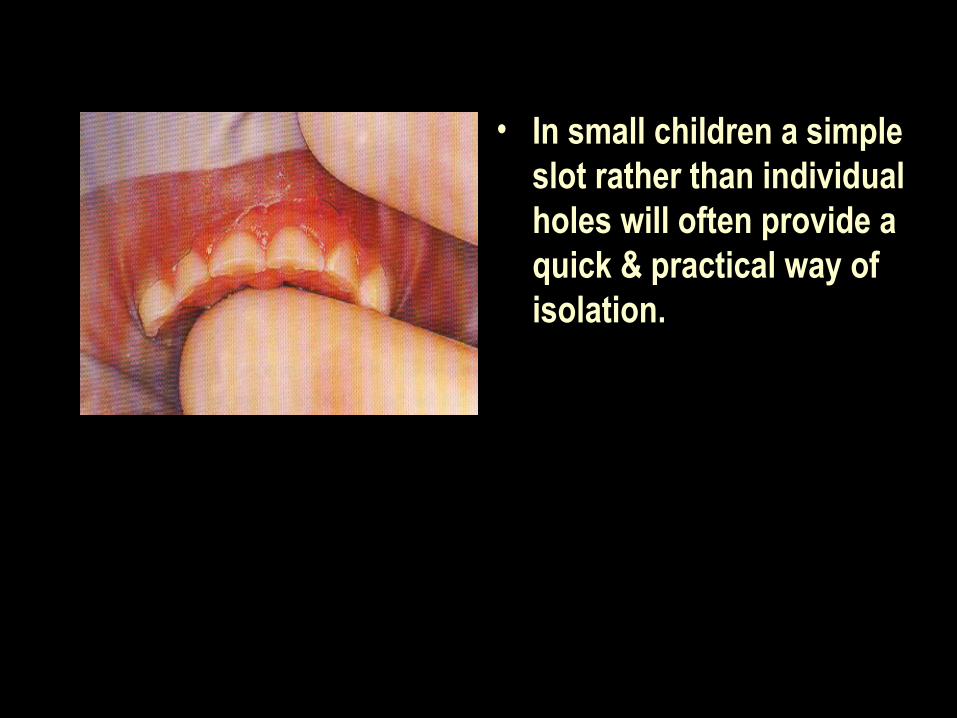
• In small children a simple slot rather than individual holes will often provide a quick & practical way of isolation.
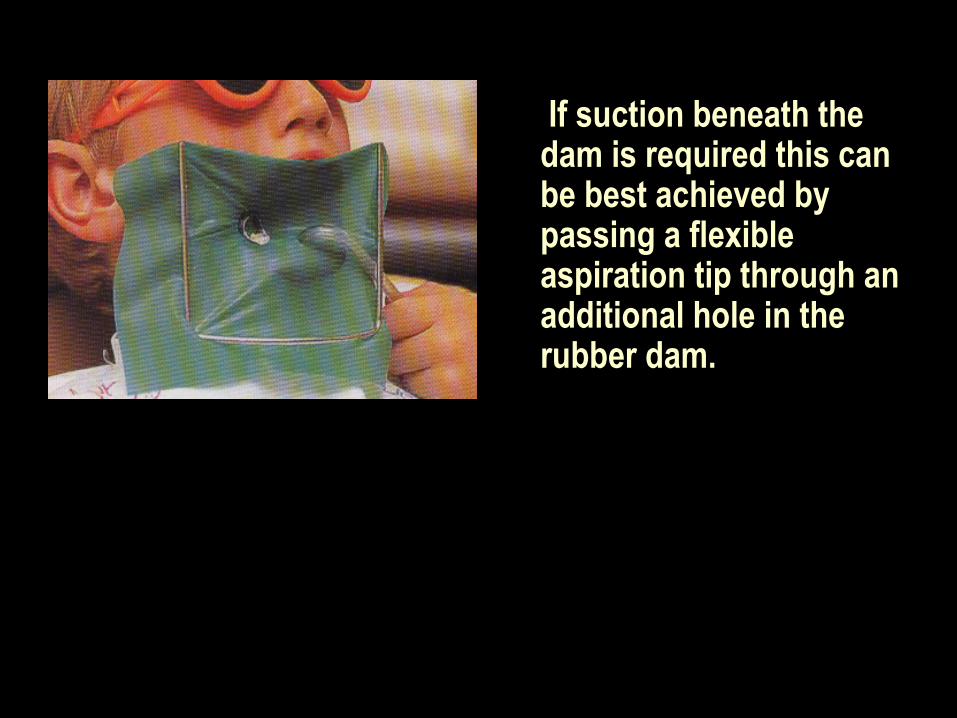
If suction beneath the dam is required this can be best achieved by passing a flexible aspiration tip through an additional hole in the rubber dam.
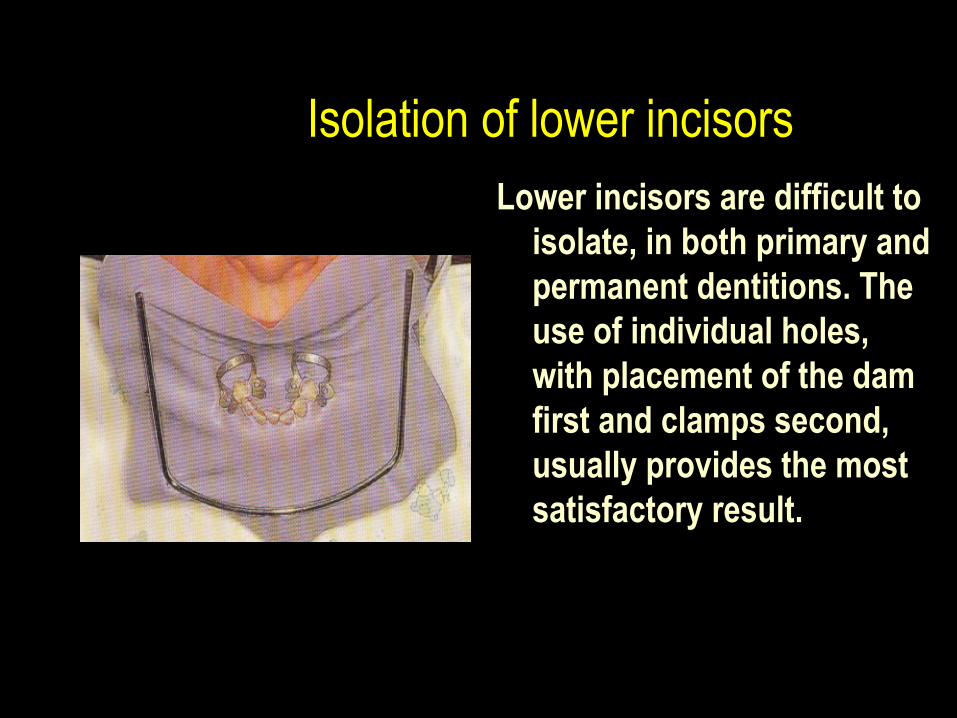
Isolation of lower incisorsLower incisors are difficult to
isolate, in both primary and permanent dentitions. The use of individual holes, with placement of the dam first and clamps second, usually provides the most satisfactory result.