pediatric gi: chronic abdominal pain evaluation and ... gi: chronic abdominal pain evaluation and...
TRANSCRIPT

·:{iC0Fp'16ACOFP 53rd Annual Convention & Scientific Seminars
Pediatric GI: Chronic Abdominal Pain Evaluation and Treatment
Paul Ufberg, DO, MBA

ACOFP FULL DISCLOSURE FOR CME ACTIVITIES
Please check where applicable and sign below. Provide additional pages as necessary.
Name of CME Activity: ACOFP 53rd Annual Convention and Scientific Seminars
Dates and Location of CME Activity: April 6-9, 2016, The San Juan Puerto Rico Convention Center
Your presentation Thursday, April 7, 2016 from 8:00am-9:00am: Pediatric GI: Chronic Abdominal Pain Evaluation
and Treatment
Name of Faculty/Moderator: ___Paul J. Ufberg DO, MBA_______________________________
DISCLOSURE OF FINANCIAL RELATIONSHIPS WITHIN 12 MONTHS OF DATE OF THIS FORM
X A. Neither I nor any member of my immediate family has a financial relationship or interest with any proprietary entity producing
health care goods or services.
B. I have, or an immediate family member has, a financial relationship or interest with a proprietary entity producing health caregoods or services. Please check the relationship(s) that applies.
Research Grants Stock/Bond Holdings (excluding mutual funds)
Speakers’ Bureaus* Employment
Ownership Partnership
Consultant for Fee Others, please list:
Please indicate the name(s) of the organization(s) with which you have a financial relationship or interest, and the specific clinical area(s) that correspond to the relationship(s). If more than four relationships, please list on separate piece of paper:
Organization With Which Relationship Exists Clinical Area Involved
1. 1.
2. 2.
3. 3.
4. 4.
*If you checked “Speakers’ Bureaus” in item B, please continue:
• Did you participate in company-provided speaker training related to your proposed Topic? Yes: No:
• Did you travel to participate in this training? Yes: No:
• Did the company provide you with slides of the presentation in which you were trained as a speaker? Yes: No:
• Did the company pay the travel/lodging/other expenses? Yes: No:
• Did you receive an honorarium or consulting fee for participating in this training? Yes: No:
• Have you received any other type of compensation from the company? Please specify: Yes: No: • When serving as faculty for ACOFP, will you use slides provided by a proprietary entity for your presentation
and/or lecture handout materials? Yes: No:
• Will your Topic1 involve information or data obtained from commercial speaker training? Yes: No:
DISCLOSURE OF UNLABELED/INVESTIGATIONAL USES OF PRODUCTS
__X_A. The content of my material(s)/presentation(s) in this CME activity will not include discussion of unapproved or investigational uses of products or devices.
______B. The content of my material(s)/presentation in this CME activity will include discussion of unapproved or investigational uses of products or devices as indicated below:
I have read the ACOFP policy on full disclosure. If I have indicated a financial relationship or interest, I understand that this
information will be reviewed to determine whether a conflict of interest may exist, and I may be asked to provide additional
information. I understand that failure or refusal to disclose, false disclosure, or inability to resolve conflicts will require
the ACOFP to identify a replacement.
Signature: Date:
Paul Ufberg, DO, MBA
Please email this form to [email protected] as soon as possible
Deadline: Friday, January 15, 2016

3/17/2016
1
Abominable Pain
Paul J. Ufberg DO, MBA
Children’s Hospital of Philadelphia
ACOFP 53rd Annual Convention
April 6-9, 2016
San Juan, Puerto Rico
© 2016 by Paul J. Ufberg DO, MBA
1
Pediatric Abdominal Pain
Disclosures
• No conflicts
• No disclosures
2
Recurrent Abdominal Pain• Apley defined recurrent abdominal pain
– At least one episode of pain per month
– 3 consecutive months
– Pain interferes with normal activities
• Survey of 1000 kids found that 10.8% fit
criteria for recurrent abdominal pain
• Girls > Boys (1.3:1)
• In 1958
3
Apley J, Naish N. Recurrent abdominal pains: a field survey of 1,000 school children. Arch Dis Child 1958;33:165-70.
3/17/2016
2
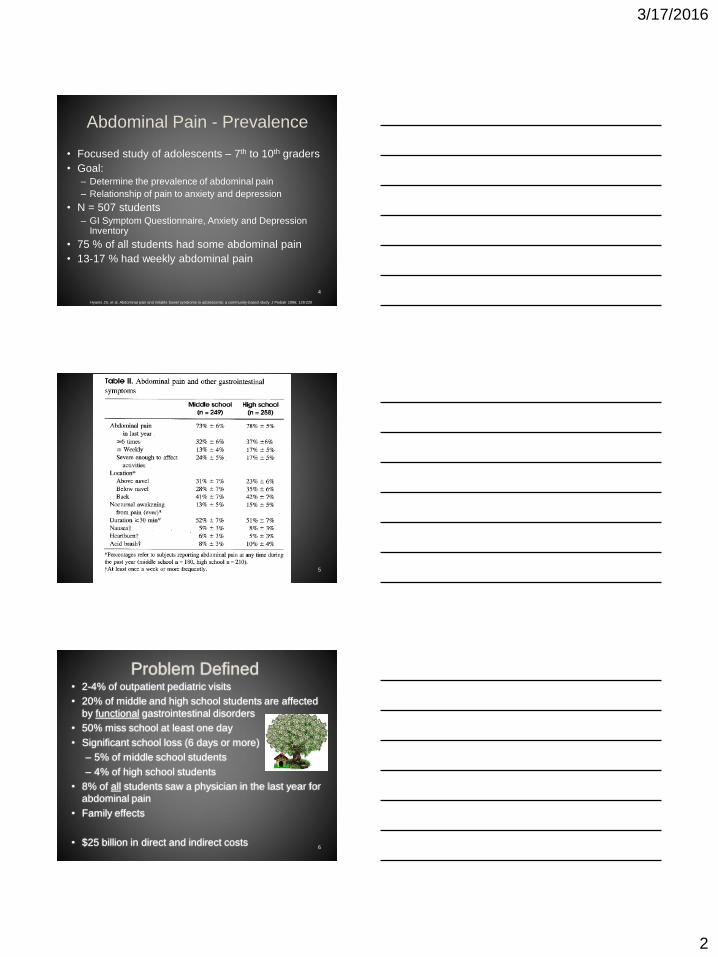
Abdominal Pain - Prevalence
• Focused study of adolescents – 7th to 10th graders
• Goal:– Determine the prevalence of abdominal pain
– Relationship of pain to anxiety and depression
• N = 507 students
– GI Symptom Questionnaire, Anxiety and Depression Inventory
• 75 % of all students had some abdominal pain
• 13-17 % had weekly abdominal pain
4
Hyams JS, et al. Abdominal pain and irritable bowel syndrome in adolescents: a community-based study J Pediatr 1996; 129:220
5
Problem Defined• 2-4% of outpatient pediatric visits
• 20% of middle and high school students are affected
by functional gastrointestinal disorders
• 50% miss school at least one day
• Significant school loss (6 days or more)
– 5% of middle school students
– 4% of high school students
• 8% of all students saw a physician in the last year for
abdominal pain
• Family effects
• $25 billion in direct and indirect costs6

3/17/2016
3
Abdominal Pain - Physiology
7
Neurophysiology of
Abdominal Pain
• Neuroreceptors AKA Nociceptors
• Located thought the abdominal viscera and supporting structures
• Respond to noxious stimuli
• Different types of pain
8
Embryology
• Most abdominal viscera begin as midline
structures and have bilateral, symmetric
innervation
• Location of abdominal pain is determined by the
level at which the afferent nerves from
abdominal viscera enter the spinal cord
• Visceral Vs. Somatic pain
9
3/17/2016
4
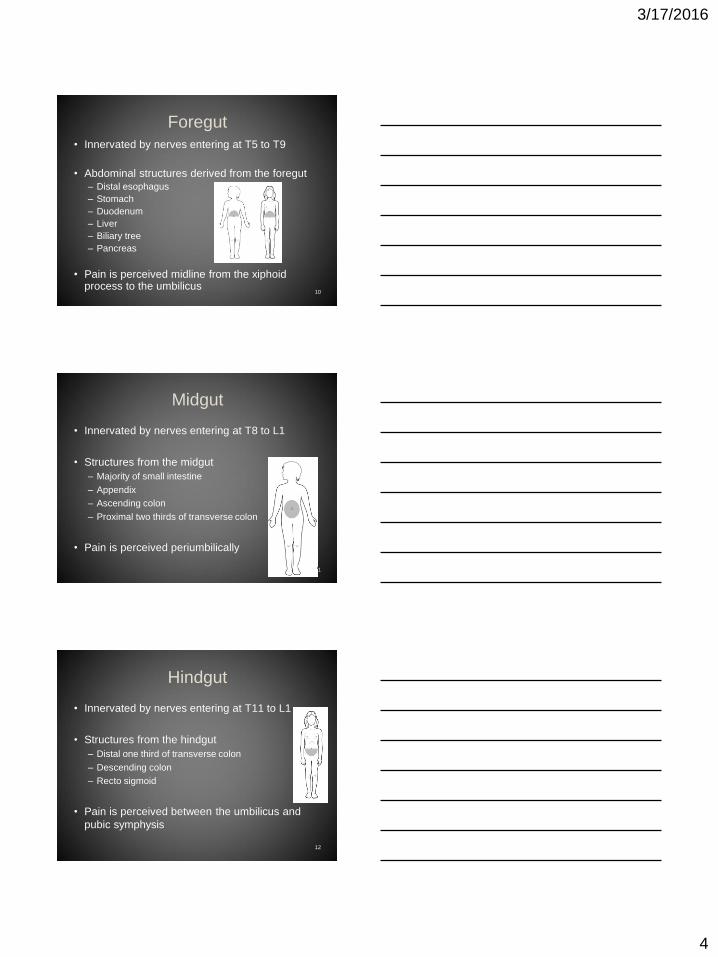
Foregut
• Innervated by nerves entering at T5 to T9
• Abdominal structures derived from the foregut
– Distal esophagus
– Stomach
– Duodenum
– Liver
– Biliary tree
– Pancreas
• Pain is perceived midline from the xiphoid process to the umbilicus
10
Midgut
• Innervated by nerves entering at T8 to L1
• Structures from the midgut
– Majority of small intestine
– Appendix
– Ascending colon
– Proximal two thirds of transverse colon
• Pain is perceived periumbilically
11
Hindgut
• Innervated by nerves entering at T11 to L1
• Structures from the hindgut
– Distal one third of transverse colon
– Descending colon
– Recto sigmoid
• Pain is perceived between the umbilicus and
pubic symphysis
12

3/17/2016
5
Referred Pain
• Localized pain in an area remote from the abdominal pathology
• Referred pain is associated with skin hyperalgesia over the cutaneous dermatone supplied by the same neural segment as the injured organ
13
Summary• Visceral pain is often accompanied by
constitutional symptoms (nausea, vomiting, etc) and is poorly localized pain
• Parietal pain is intense, well localized, and aggravated by movement
• Referred pain occurs in a recognizable pattern away from the site of pathology
• Abdominal pain
– Visceral pain
– Somatic pain
– Referred pain
– Combination of all three14
A Practical Approach to
Abdominal Pain
15

3/17/2016
6
Clinical Approach to
Abdominal Pain
• History
– Questions directed at the
patient
• Developmentally
appropriate
• Friendly vs Silly
– Minimize parental
influence
– One finger, one spot
method
– Observe
• Focus on:
– Quality
– Intensity
• 0-10
• Smiley faces (Wong
– Duration
– Timing
– Sleep cycle
– Eating
– Temporal correlation
16
More History
• Medications – before
or after the pain
– Prescriptions
– Over the counter
– Supplements
• Allergy
– Medication
– Environmental
• Past History
• Family History
– Recent illnesses
– Migraines
– IBD
– IBS
– Celiac
• Social History
– School
– Home Life
– Stressors
• Changes 17
Physical Examination
• Growth Parameters – prior to seeing patient
– Be prepared to verify with family
• Begin immediately
– Facial expression
– Body movement and position
– Family interaction
• Full examination
– Focused on Abdomen
– Rectal Exam18
3/17/2016
7
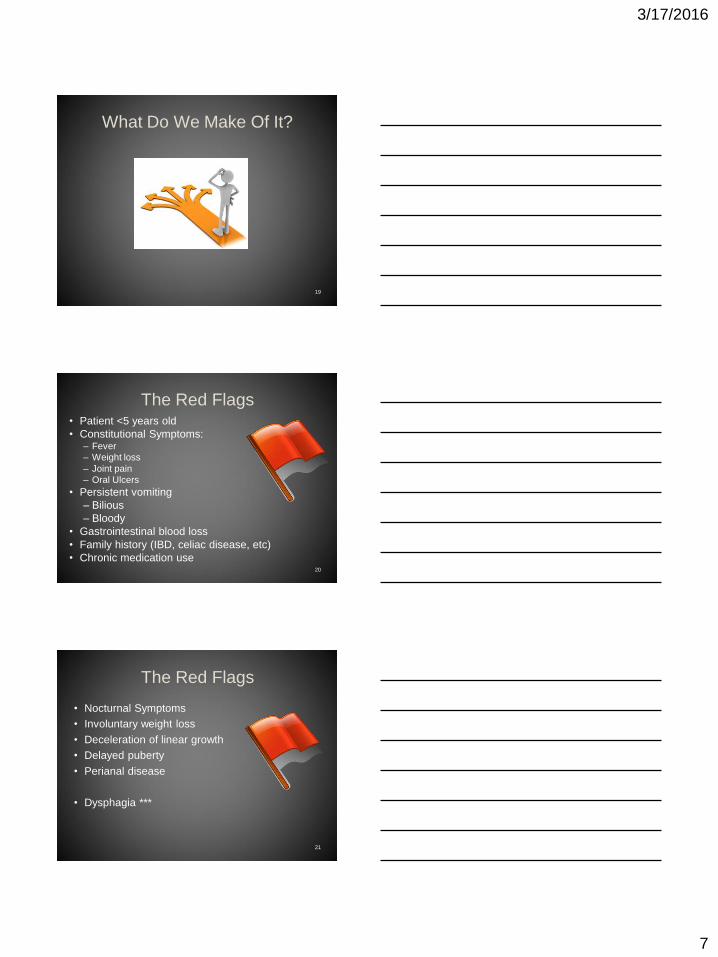
What Do We Make Of It?
19
The Red Flags • Patient <5 years old
• Constitutional Symptoms: – Fever
– Weight loss
– Joint pain
– Oral Ulcers
• Persistent vomiting
– Bilious
– Bloody
• Gastrointestinal blood loss
• Family history (IBD, celiac disease, etc)
• Chronic medication use20
The Red Flags
• Nocturnal Symptoms
• Involuntary weight loss
• Deceleration of linear growth
• Delayed puberty
• Perianal disease
• Dysphagia ***
21

3/17/2016
8
Differential Diagnosis
• Multitude of
causes
• Distinguish in
broad terms
– Well
– Sick
• Published list from
1976
22Dodge, Recurrent Abdominal Pain in Childhood, British Medical Journal 1976, 385-387
Laboratory and Imaging• Labs should be
individualized
• Lab screening should
include
– CBC
– UA
– CMP
– ESR and CRP
– Celiac panel
– Stool Studies
– UPT/HCG
• Abdominal US (?)
– Prospective study of
93 children with
recurrent abdominal
pain
• 3 had anatomic
abnormalities• None accounted for the
abdominal pain
23
Van de Meer, Diagnostic value of ultrasound in children with recurrent abdominal pain. Pediatr Radiol, 20, 7. 501-503
Celiac Disease
• A word on celiac…
• Multiple tests available
• Results can be confusing
• Body of knowledge is growing rapidly
24
3/17/2016
9
25
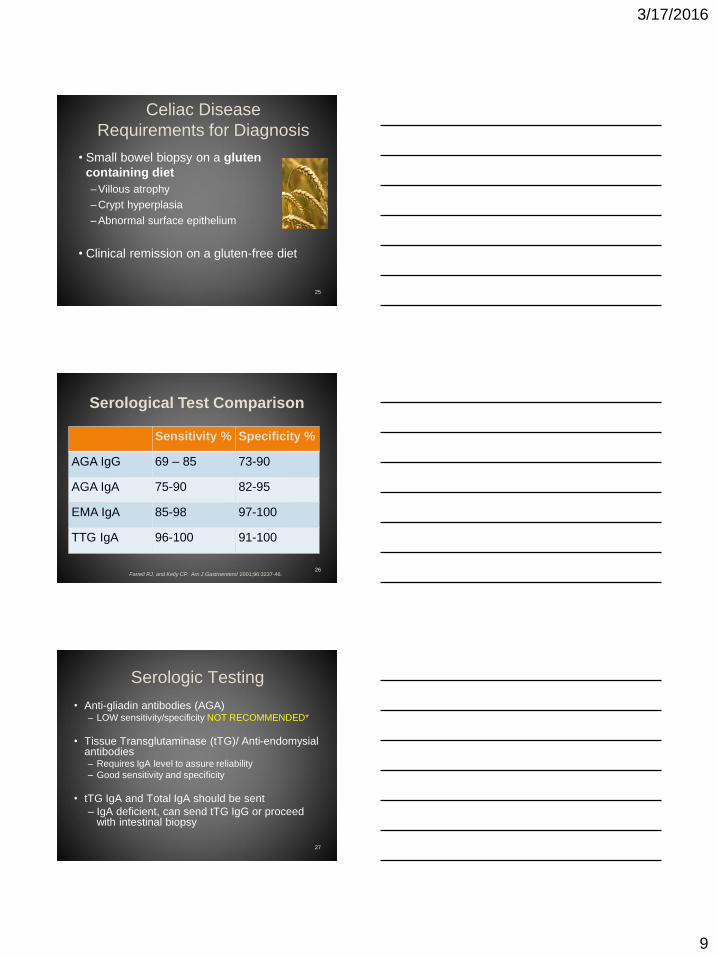
Celiac Disease
Requirements for Diagnosis
• Small bowel biopsy on a gluten
containing diet
–Villous atrophy
–Crypt hyperplasia
–Abnormal surface epithelium
• Clinical remission on a gluten-free diet
Serological Test Comparison
Farrell RJ, and Kelly CP. Am J Gastroenterol 2001;96:3237-46.
Sensitivity % Specificity %
AGA IgG 69 – 85 73-90
AGA IgA 75-90 82-95
EMA IgA 85-98 97-100
TTG IgA 96-100 91-100
26
Serologic Testing
• Anti-gliadin antibodies (AGA)– LOW sensitivity/specificity NOT RECOMMENDED*
• Tissue Transglutaminase (tTG)/ Anti-endomysial antibodies– Requires IgA level to assure reliability
– Good sensitivity and specificity
• tTG IgA and Total IgA should be sent
– IgA deficient, can send tTG IgG or proceed with intestinal biopsy
27

3/17/2016
10
Testing and Abdominal Pain
Normal Physical Exam
+
Normal Screening Labs
_________________________
Rule out organic disease in 95% of Recurrent Abdominal Pain Cases
28
Types of Abdominal Pain
• Organic abdominal pain - pain that is
explained on the basis of a structural or
biochemical abnormality
• Functional abdominal pain - episodic or
continuous abdominal pain without
evidence of inflammatory, anatomic,
metabolic or neoplastic process that
explains the symptoms29
Functional Abdominal Pain
• The Rome Foundation
– Classify and diagnose functional GI disorders (FGID)
– Legitimize and update knowledge
– Create scientific data
– Education
– Treatment
• Clinicians and scientists from around the world
• Goal to improve the lives of people with
functional GI disorders30

3/17/2016
11
Paradigm Shift
• Reductionist Model
– 300 years old
– One etiology for disease
– Separation of mind and body
• Mind was the seat of the soul
• Biopsychosocial Model
– 30 years ago
– Connection of mind and body
• Dysregulation can produce illness
31
Biopsychosocial Model
32
Rome III Criteria
• Rome III Launched May 2006
– Updated from 1999
• Current set of diagnostic criteria for FGID
– Symptom based diagnosis
– Domains based on age
• Adult (A-F)
• Neonate/Toddler (G)
• Adolescent (H)
– Overlap does exist
33
3/17/2016
12
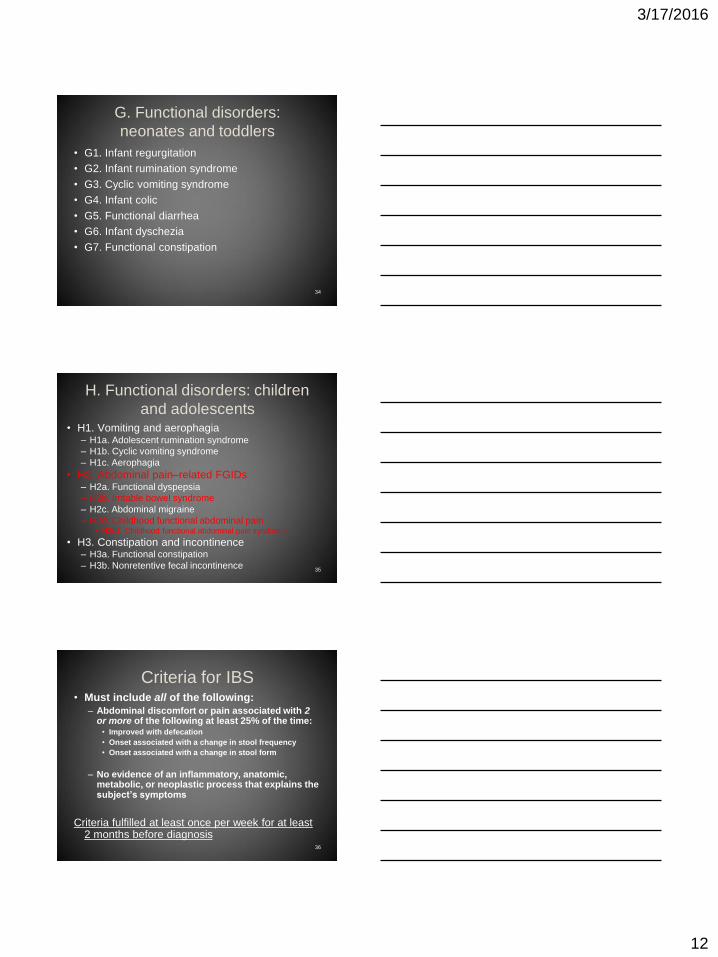
G. Functional disorders:
neonates and toddlers
• G1. Infant regurgitation
• G2. Infant rumination syndrome
• G3. Cyclic vomiting syndrome
• G4. Infant colic
• G5. Functional diarrhea
• G6. Infant dyschezia
• G7. Functional constipation
34
H. Functional disorders: children
and adolescents• H1. Vomiting and aerophagia
– H1a. Adolescent rumination syndrome
– H1b. Cyclic vomiting syndrome
– H1c. Aerophagia
• H2. Abdominal pain–related FGIDs– H2a. Functional dyspepsia
– H2b. Irritable bowel syndrome
– H2c. Abdominal migraine
– H2d. Childhood functional abdominal pain• H2d1. Childhood functional abdominal pain syndrome
• H3. Constipation and incontinence– H3a. Functional constipation
– H3b. Nonretentive fecal incontinence35
Criteria for IBS• Must include all of the following:
– Abdominal discomfort or pain associated with 2 or more of the following at least 25% of the time:
• Improved with defecation
• Onset associated with a change in stool frequency
• Onset associated with a change in stool form
– No evidence of an inflammatory, anatomic, metabolic, or neoplastic process that explains the subject’s symptoms
Criteria fulfilled at least once per week for at least 2 months before diagnosis
36

3/17/2016
13
Criteria for FAP• FAP – Functional
Abdominal Pain
• Must include all of the
following:
– 1. Episodic or continuous
abdominal pain
– 2. Insufficient criteria for
other FGIDs
– 3. No evidence of an
inflammatory, anatomic,
metabolic, or neoplastic
process that explains the
subject’s symptoms
• FAPS - Functional
Abdominal Pain Syndrome
• Must include childhood
functional abdominal pain at
least 25% of the time and 1
or more of the following:
– 1. Some loss of daily
functioning
– 2. Additional somatic
symptoms such as
headache, limb pain, or
difficulty sleeping
37•At least once per week for at least 2 months before diagnosis
What Contributes to FAP?
38
Stressors• Life stress events
– Small amount of evidence
– Recent negative life events is NOT useful in distinguishing functional abdominal pain and abdominal pain of other causes
• Daily Stressors– Limited evidence
– Associated with the occurrence of pain episodes
– Higher levels of negative life events are associated with increased likelihood of symptom persistence
• No evidence on stress influence on severity, course or treatment response
39AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Technical Report J Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 249-61 March 2005

3/17/2016
14
Emotional and Behavior Problems
• Anxiety and depression– Increased frequency in patients with recurrent
abdominal pain
– NOT useful in distinguishing FAP from other causes
• Conduct disorders– Patients do NOT have increased prevalence
• Future symptoms and outcome– Increased risk of later emotional symptoms
– Long term - no data on emotional/behavioral symptoms and disease severity, course or treatment response
40AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Technical Report J Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 249-61 March 2005
Family Functioning
• Family History
– Parents with recurrent abdominal pain have more children with anxiety, depression and somatization
• Family Dynamics
– Families with recurrent abdominal pain do NOT differ from control groups or families with acute illness in broad areas of family functioning
• Family cohesion, conflict and marital satisfaction
41AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Technical Report J Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 249-61 March 2005
What Causes FAP?
42

3/17/2016
15
Motility• FAP initially considered a motility disorder
• Patients with FAP – More frequent migrating motor complexes
– Slower propagation velocity
– High pressure duodenal contractions associated with pain
• Subsequent research found no specific diagnostic pattern of motility disturbances
• Increased contractility is not universally present
• Hypercontractile episodes not related to pain43
Hypersensitivity
• Recurrent abdominal pain may be related to
alteration in the pain axis
– Amplification of incoming sensory information
– Increased responsiveness to physiologic and
noxious stimuli
– Failure of down-regulation
• Visceral Hypersensitivity
44
Sensitivity
• N = 22 patients with IBS or Dyspepsia vs Controls
• Balloon distention– Esophagus
– Rectum
• Perception
• Desire to defecate
• Urgency
• IBS – Lower rectal and esophageal
sensory thresholds
• Functional Dyspepsia– Similar to IBS
45Trimble Heightened visceral sensation in functional gastrointestinal disease is not site-specific. Evidence for a generalized disorder of gut sensitivity. Dig Dis Sci
(1995) 40:1607–13
3/17/2016
16
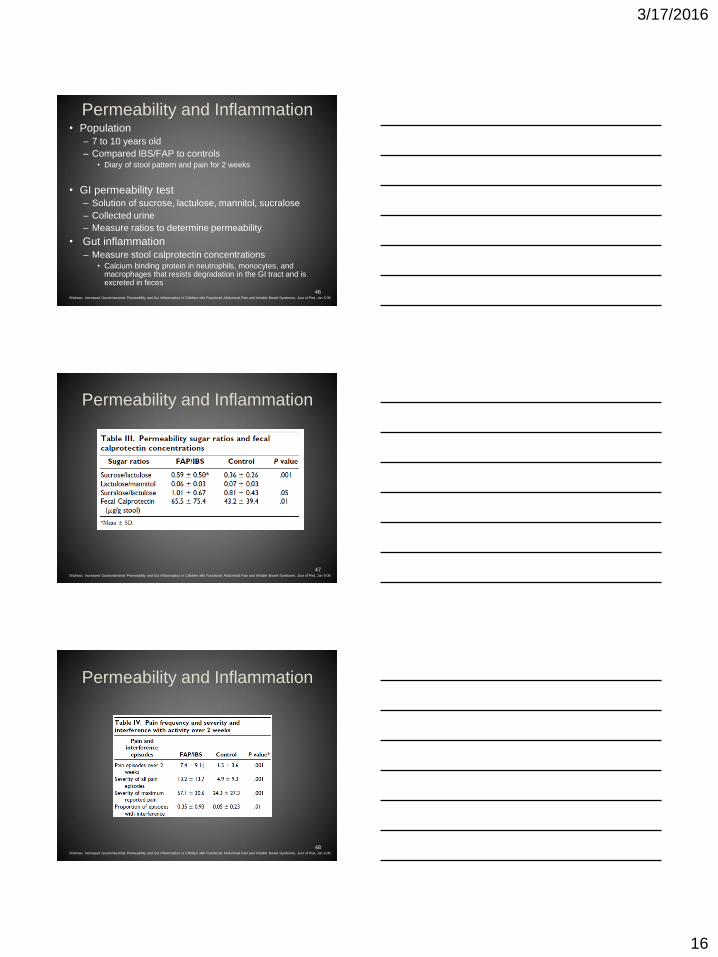
Permeability and Inflammation• Population
– 7 to 10 years old
– Compared IBS/FAP to controls• Diary of stool pattern and pain for 2 weeks
• GI permeability test– Solution of sucrose, lactulose, mannitol, sucralose
– Collected urine
– Measure ratios to determine permeability
• Gut inflammation
– Measure stool calprotectin concentrations• Calcium binding protein in neutrophils, monocytes, and
macrophages that resists degradation in the GI tract and is excreted in feces
46Shulman, Increased Gastrointestinal Permeability and Gut Inflammation in Children with Functional Abdominal Pain and Irritable Bowel Syndrome, Jour of Ped, Jun 6 08
Permeability and Inflammation
47Shulman, Increased Gastrointestinal Permeability and Gut Inflammation in Children with Functional Abdominal Pain and Irritable Bowel Syndrome, Jour of Ped, Jun 6 08
Permeability and Inflammation
48Shulman, Increased Gastrointestinal Permeability and Gut Inflammation in Children with Functional Abdominal Pain and Irritable Bowel Syndrome, Jour of Ped, Jun 6 08
3/17/2016
17
Permeability and Inflammation
• FAP/IBS may have increased permeability in the proximal GI tract and colon
– Adult studies showed small intestine permeability
• Suggest that children with FAP/IBS also have increased inflammation
• Increased fecal calprotectin concentration was related to pain symptoms
49
Now What?
50
Treatment - Explanation
• Explain the diagnosis in a way the patient and their family can understand
– May use headache as an example
– Hypersensitivity can be described in the same way skin is more sensitive after a burn
• Involve the family
– Address their concerns
– Common problem – affects up to 20% of school age children
• Set consistent limits
• Make recommendations consistent with patient interests
51
3/17/2016
18
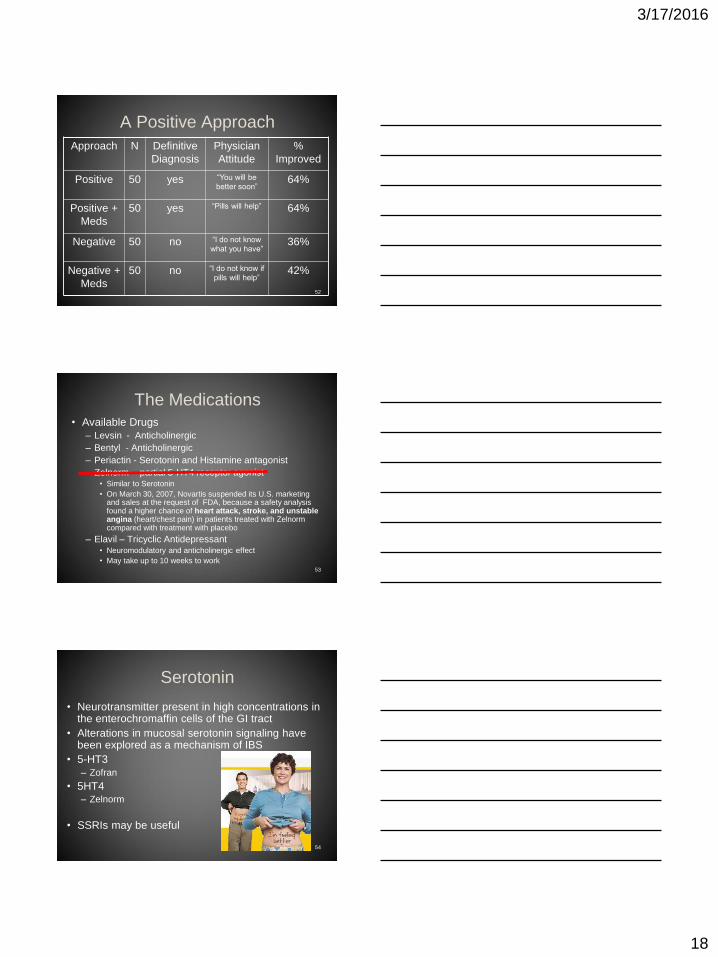
A Positive Approach
52
Approach N Definitive
Diagnosis
Physician
Attitude
%
Improved
Positive 50 yes “You will be
better soon”64%
Positive +
Meds
50 yes “Pills will help” 64%
Negative 50 no “I do not know
what you have”36%
Negative +
Meds
50 no “I do not know if
pills will help”42%
The Medications
• Available Drugs
– Levsin - Anticholinergic
– Bentyl - Anticholinergic
– Periactin - Serotonin and Histamine antagonist
– Zelnorm - partial 5-HT4 receptor agonist • Similar to Serotonin
• On March 30, 2007, Novartis suspended its U.S. marketing and sales at the request of FDA, because a safety analysis found a higher chance of heart attack, stroke, and unstable angina (heart/chest pain) in patients treated with Zelnorm compared with treatment with placebo
– Elavil – Tricyclic Antidepressant• Neuromodulatory and anticholinergic effect
• May take up to 10 weeks to work53
Serotonin
• Neurotransmitter present in high concentrations in the enterochromaffin cells of the GI tract
• Alterations in mucosal serotonin signaling have been explored as a mechanism of IBS
• 5-HT3
– Zofran
• 5HT4– Zelnorm
• SSRIs may be useful
54

3/17/2016
19
Melatonin• Melatonin is involved in the regulation of gut motility and
sensation
• Placebo controlled study– N = 18 adults with IBS
• 9 Melatonin 3mg at bed time
• 9 Placebo
– 8 week study• Assessments every 2 weeks
• Follow up at 16,24, 48 weeks
• Overall IBS Score
• Extracolonic IBS Score
• Quality of Life
55Saha, A Preliminary Study of Melatonin in Irritable Bowel Syndrome, J of Clinic Gastro Volume 41(1), January 2007, pp 29-32
Melatonin
Melatonin (9) Placebo (9)
Before After Before After
Overall IBS
Score300 170 240 200
Improvement 45% 16.66%
Overall Extra-
Colonic Score235 95 180 155
Improvement 49.16% 13.88%
56Saha, A Preliminary Study of Melatonin in Irritable Bowel Syndrome, J of Clinic Gastro Volume 41(1), January 2007, pp 29-32
Melatonin
• Melatonin significantly decreased the
individual and overall IBS symptoms scores
• Post-treatment overall extra-colonic IBS
score was significantly lower in the
melatonin group compared to pretreatment
and placebo group
57

3/17/2016
20
Peppermint Oil• May provide benefit in children with IBS
– Causes intestinal relaxation by decreasing calcium influx in smooth muscles
• 42 children with IBS in randomized double blind control trial
58
Kline, Enteric-coated, pH-dependent peppermint oil capsules for the treatment of irritable bowel syndrome in children, J Pediatr 2001;138:125-8
Investigational Drugs
59
Saad, Recent developments in the therapy of irritable bowel syndrome, Expert Opin. Investig. Drugs (2008) 17(2)
Alternatives Treatments
• Lactose Free Diet
– Inconclusive evidence
• Fiber Supplementation
– Inconclusive evidence
• Surgery
– No evidence of the possible beneficial role of
surgery in the evaluation or management of
the child with recurrent abdominal pain
60AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Technical Report J Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 249-61 March 2005

3/17/2016
21
Alternative Therapies
• Cognitive-Behavioral Therapy
– Teaching coping skills to patient and family
• Higher rate of complete elimination of pain
• Lower levels of relapse at 6 and 12 months
• Lower level of interference with activities
• Higher level of satisfaction with care
61Sanders, Cognitive-behavioral treatment of recurrent nonspecific abdominal pain in children: an analysis of generalization, maintenance, and side effects, J Consult
Clin Psychol. 1994 Apr;62(2):306-14
Alternative Therapy
• Relaxation Techniques
– Yoga, Meditation, Progressive Muscle Relaxation
• Randomized study of yoga and IBS
– 25 adolescents, age 11 to 18 years with IBS
• 1 hour instructional session + daily home practice
• Waiting list
– After 4 weeks the waiting list was trained with yoga
– Questionnaires at 0, 4 and 8 weeks
• Yoga group had less functional disability, less
anxiety and lower scores for IBS symptoms62
Kuttner, A randomized trial of yoga for adolescents with irritable bowel syndrome Pain Res Manag. 2006 Winter;11(4):217-23
Alternative Therapy
• Hypnotherapy & IBS: Cochrane Review
– Some evidence that suggests that
hypnotherapy might be effective in treating
IBS symptoms including abdominal pain
– Hypnotherapy was well tolerated and no
serious side effects were reported in the
studies
– Currently insufficient evidence
– Long term efficacy unclear
63Webb AN. Hypnotherapy for treatment of irritable bowel syndrome. Cochrane Database of Systematic Reviews. :CD005110, 200

3/17/2016
22
Alternative Therapy - Barriers
• Willingness/motivation of both patient and
parents
• Explanation of referral in terms of the
diagnosis
• Local availability
• Insurance coverage or financial resources
64
Now What?
65
Abdominal Pain Flow Chart
66
Emergency
Room
Testing,
Radiology
PMD
CBC, X ray
US
Enema X ?
Sub Specialist
TTG, IgA
BMP, LFT
Scope, VCUG,
Surgery

3/17/2016
23
Diagnostic Roller Coaster
67
Prognosis and Prevention
• 35-50% of children were admitted to the
hospital for abdominal pain had resolution
• 25% will have pain into adulthood
• Prevention and reassurances are key
– Advise against excessive anxiety for minor
illnesses
– Stress the importance of supportiveness for
child and family
– Working together to find solutions68
Conclusion• Thorough history and physical
exam
• Use thoughtful diagnostic tests
• Positive messages to patients
are helpful
• Establish a therapeutic
relationship with the family
• Consider medical and
alternative therapies
• Many new drugs and therapies
are being considered
69
3/17/2016
24
References• Apley J, Naish N. Recurrent abdominal pains: a field survey of 1,000 school children. Arch Dis
Child 1958;33:165-70• Hyams JS, et al. Abdominal pain and irritable bowel syndrome in adolescents: a community-
based study J Pediatr 1996; 129:220• Dodge, Recurrent Abdominal Pain in Childhood, British Medical Journal 1976, , 385-387• Van de Meer, Diagnostic value of ultrasound in children with recurrent abdominal pain. Pediatr
Radiol, 20, 7 501-503• AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Technical Report J
Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 249-61 March 2005• AAP subcommittee and NASPHGAN committee on Chronic Abdominal Pain, Clinical Report J
Pediatr Gastroenterol Nutr, Vol. 40, No. 3, 245-48 March 2005• Trimble Heightened visceral sensation in functional gastrointestinal disease is not site-specific.
Evidence for a generalized disorder of gut sensitivity. Dig Dis Sci (1995) 40:1607–13• Shulman, Increased Gastrointestinal Permeability and Gut Inflammation in Children with Functional
Abdominal Pain and Irritable Bowel Syndrome, Jour of Ped, Jun 6 08 • Saha, A Preliminary Study of Melatonin in Irritable Bowel Syndrome, J of Clinic Gastro Volume
41(1), January 2007, pp 29-32 • Kline, Enteric-coated, pH-dependent peppermint oil capsules for the treatment of irritable bowel
syndrome in children, J Pediatr 2001;138:125-8• Saad, Recent developments in the therapy of irritable bowel syndrome, Expert Opin Investig
Drugs, 17, 2, 117-130• Sanders, Cognitive-behavioral treatment of recurrent nonspecific abdominal pain in children: an
analysis of generalization, maintenance, and side effects, J Consult Clin Psychol. 1994 Apr;62(2):306-14
• Kuttner, A randomized trial of yoga for adolescents with irritable bowel syndrome Pain Res Manag. 2006 Winter;11(4):217-23
• Webb AN. Hypnotherapy for treatment of irritable bowel syndrome. Cochrane Database of Systematic Reviews. :CD005110, 200
• Romecriteria.org
70