pediatric board review course pediatric hematology/oncology
DESCRIPTION
Pediatric Board Review Course Pediatric Hematology/Oncology. Kusum Viswanathan , MD Chair, Department of Pediatrics Director, Divn of Pediatric Hematology/Oncology Brookdale Univ Hospital and Medical Center. Question. 6 week old term infant referred for anemia. Hb 7.5, Retic 2 %. - PowerPoint PPT PresentationTRANSCRIPT
Pediatric Board Review CoursePediatric Board Review CoursePediatric Hematology/OncologyPediatric Hematology/Oncology
Kusum Viswanathan, MDKusum Viswanathan, MDChair, Department of PediatricsChair, Department of Pediatrics
Director, Divn of Pediatric Hematology/OncologyDirector, Divn of Pediatric Hematology/OncologyBrookdale Univ Hospital and Medical CenterBrookdale Univ Hospital and Medical Center
QuestionQuestion
6 week old term infant referred for anemia. 6 week old term infant referred for anemia. Hb 7.5, Retic 2 %.Hb 7.5, Retic 2 %.
Mother O+, Baby A -, Direct Coombs +Mother O+, Baby A -, Direct Coombs +
Cord blood Hb 14.2 g/dL.Cord blood Hb 14.2 g/dL.
Jaundice of 15mg/dL at 48 hours of life, recd Jaundice of 15mg/dL at 48 hours of life, recd photo Rx and discharged at 5 days. photo Rx and discharged at 5 days.
No complaints, pale, Bili 3.5, Direct 0.5. No complaints, pale, Bili 3.5, Direct 0.5.
Blood smear shows spherocytesBlood smear shows spherocytes
Most likely explanation for the anemia Most likely explanation for the anemia
1.1. G 6 PD deficiencyG 6 PD deficiency2.2. Hereditary Hereditary
spherocytosisspherocytosis3.3. Physiologic Physiologic
anemiaanemia4.4. ABO ABO
incompatibiltyincompatibilty5.5. Rh hemolytic Rh hemolytic
diseasediseaseG 6 PD deficie
ncy
Heredita
ry sp
herocy
tosis
Physiologic
anemia
ABO inco
mpatibilty
Rh hemolytic dise
ase
0% 0% 0%0%0%
6
Newborn –anemia- importantNewborn –anemia- important
Hemoglobin at birth is 17 g/dl, MCV over Hemoglobin at birth is 17 g/dl, MCV over 100.100.Falls to 11-12 by 6 weeks of age- nadir of physiologic Falls to 11-12 by 6 weeks of age- nadir of physiologic anemiaanemiaAnemia at birth could be :Anemia at birth could be :– Hemorrhage, may not have had time to mount a retic responseHemorrhage, may not have had time to mount a retic response– Acute hemorrhage- pallor and tachypneaAcute hemorrhage- pallor and tachypnea– Look at MCV- Look at MCV- low MCV-suggestivelow MCV-suggestive of of
chronic feto-maternal hemorrhage chronic feto-maternal hemorrhage Alpha Thalassemia trait.Alpha Thalassemia trait.
– Kleihauer-Betke- Hb F resistance to acid elutionKleihauer-Betke- Hb F resistance to acid elution
The treatment of choice for alloimune neonatal The treatment of choice for alloimune neonatal thrombocytopenia isthrombocytopenia is
1.1. random platelet random platelet transfusiontransfusion
2.2. IVIGIVIG
3.3. SteroidsSteroids
4.4. Exchange Exchange transfusiontransfusion
5.5. Washed maternal Washed maternal platelets platelets
random plate
let transfu
sion
IVIG
Steroids
Exchange
transfu
sion
Was
hed mate
rnal p
latelets
0% 0% 0%0%0%
6
Immune thrombocytopeniaImmune thrombocytopenia
Auto-immune: Pregnant women with ITP/Hx of ITP Auto-immune: Pregnant women with ITP/Hx of ITP – Passive transfer of antibodies (IgG) from mother. Passive transfer of antibodies (IgG) from mother. – Even when mother has a normal platelet count (Splenectomy)Even when mother has a normal platelet count (Splenectomy)– Nadir-few days; Platelets < 50,00 have 1% risk of ICH.Nadir-few days; Platelets < 50,00 have 1% risk of ICH.– IVIG to mother, Fetal platelet counts, C sec, US, IVGG to babyIVIG to mother, Fetal platelet counts, C sec, US, IVGG to baby
Allo or Iso-Immune: Normal platelet count in motherAllo or Iso-Immune: Normal platelet count in mother– Similar to Rh disease; PL A1 antigen/ Zw-a negative mother.Similar to Rh disease; PL A1 antigen/ Zw-a negative mother.– 97% of population is PL A1 positive97% of population is PL A1 positive– Sensitization early in pregnancySensitization early in pregnancy– Plt function defect because Anti-PL-A1 interferes w/aggregation.Plt function defect because Anti-PL-A1 interferes w/aggregation.– Severe bleeding more likely; first born affected Severe bleeding more likely; first born affected – Recovery in 2-3 weeksRecovery in 2-3 weeks– Mother’s washed (PLA1 neg) platelets; IVIG; Ultrasound; Mother’s washed (PLA1 neg) platelets; IVIG; Ultrasound;
SteroidsSteroids

Kasabach- MerrittKasabach- Merritt, TAR, TAR
15 months old girl presented in ER with h/o URI, and scattered 15 months old girl presented in ER with h/o URI, and scattered petechiae and ecchymoses over the body and lower extremities. petechiae and ecchymoses over the body and lower extremities.
1.1. perform a bone marrow perform a bone marrow aspirate to confirm the aspirate to confirm the diagnosisdiagnosis
2.2. Non-accidental injury; Non-accidental injury; skeletal survey to rule skeletal survey to rule out bony fracturesout bony fractures
3.3. treatment with either treatment with either IVIG or anti-DIVIG or anti-D
4.4. Administer platelet Administer platelet transfusiontransfusion
Physical exam normal, no hepatosplenomegaly. WBC-14,000, Hb 12.8, Plts-5,000, Diff: Normal - Next step
6perform
a bone marro
w ...
Non-accidental
injury;
sk...
treatm
ent with
either I
VI...
Administer p
latelet t
rans...
0% 0%0%0%
Acute ITPAcute ITPUsually acute onset; immune mediated; post viralUsually acute onset; immune mediated; post viral
Peak 2-5 years of age, Peak 2-5 years of age,
PE –no lymphadenopathy (LN), hepatosplenomegaly.PE –no lymphadenopathy (LN), hepatosplenomegaly.
CBC- other cell lines normal, CBC- other cell lines normal, large plts on smearlarge plts on smearTreat if plt< 10,000 or wet ITPTreat if plt< 10,000 or wet ITP, ,
Treat- Treat- IVIG best responseIVIG best response, 48-72 hours; blocks Fc receptors,SE, 48-72 hours; blocks Fc receptors,SE
– Anti-D (WInRhoAnti-D (WInRho)- Rh+ ,hemolysis, quick response)- Rh+ ,hemolysis, quick response– Steroids good response, block phagocytosis, reduces antibodies, Steroids good response, block phagocytosis, reduces antibodies,
SE, inexpensive, need BMSE, inexpensive, need BM
BM- Increased megakaryocytes, otherwise normalBM- Increased megakaryocytes, otherwise normal
Chronic- Chronic- If >6 months, F>M, older, unpredictable If >6 months, F>M, older, unpredictable prognosisprognosis

Petechiae, HSPPetechiae, HSP
A 2 year old boy presents for evaluation of a chronic pruritic eruption. H/o A 2 year old boy presents for evaluation of a chronic pruritic eruption. H/o recurrent epistaxis, otitis media, and pneumoniarecurrent epistaxis, otitis media, and pneumonia
1.1. Acrodermatitis Acrodermatitis enteropathicaenteropathica
2.2. Ataxia telangiectasiaAtaxia telangiectasia3.3. Atopic dermatitisAtopic dermatitis4.4. Langerhans cell Langerhans cell
histiocytosishistiocytosis5.5. Wiskott-Aldrich Wiskott-Aldrich
syndromesyndrome
P/E reveals erythematous, slightly scaling patches on the trunk and in the antecubital and popliteal fossae. Petechiae too- most suggestive of
Acroderm
atitis entero
pa...
Ataxia telan
giectasia
Atopic
dermatitis
Langerh
ans cell h
istiocy
tosis
Wisk
ott-Aldric
h syndro
me
0% 0% 0%0%0%
6
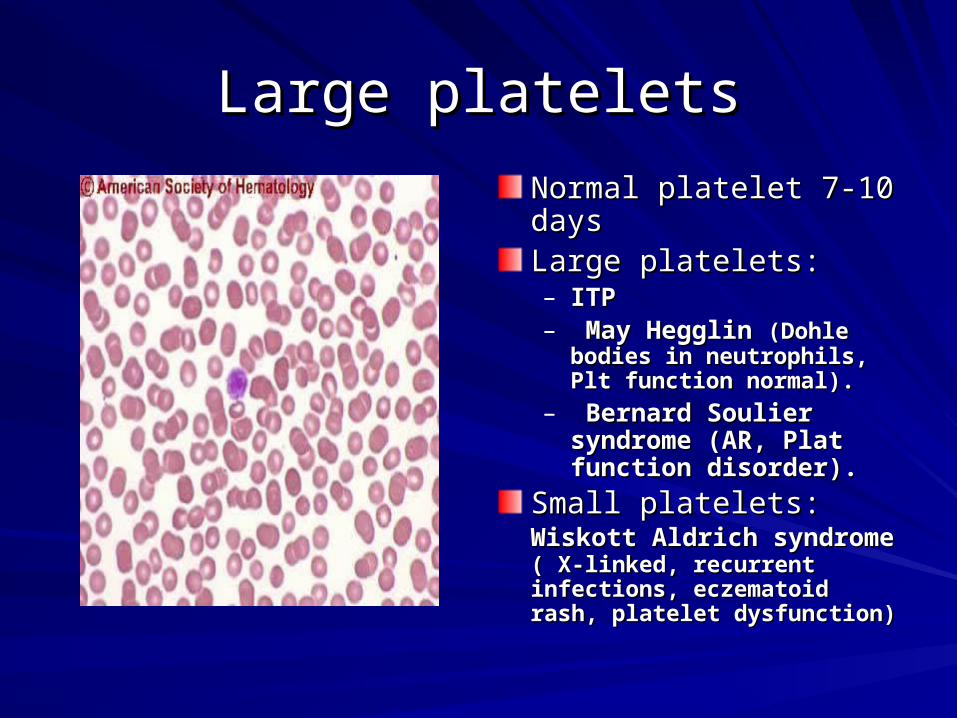
Large plateletsLarge platelets
Normal platelet 7-10 daysNormal platelet 7-10 daysLarge platelets: Large platelets: – ITPITP– May Hegglin May Hegglin (Dohle (Dohle
bodies in neutrophils, Plt bodies in neutrophils, Plt function normal).function normal).
– Bernard Soulier Bernard Soulier syndrome (AR, Plat syndrome (AR, Plat function disorder).function disorder).
Small platelets: Small platelets: Wiskott Wiskott Aldrich syndromeAldrich syndrome ( X-linked, ( X-linked, recurrent infections, recurrent infections, eczematoid rash, platelet eczematoid rash, platelet dysfunction)dysfunction)

Platelet function defectsPlatelet function defects
Normal platelet numberNormal platelet number
Abnormal aggregationAbnormal aggregation– Glanzmann thrombasthenia--- AR, Bleeding disorder, check h/o Glanzmann thrombasthenia--- AR, Bleeding disorder, check h/o
consanguinityconsanguinity
– afibrinogenemiaafibrinogenemia
Abnormal adhesion- Abnormal adhesion- Bernard-Soulier, VWDBernard-Soulier, VWD
Ineffective ThrombopoiesisIneffective Thrombopoiesis– MayHegglin Anomaly (Large platelets)MayHegglin Anomaly (Large platelets)
Disorders of SecretionDisorders of Secretion: : Storage pool, gray platelet syndromeStorage pool, gray platelet syndrome
Hermansky Pudlak Syndrome:Hermansky Pudlak Syndrome:– AR, Decreased dense granules, In Puerto RicansAR, Decreased dense granules, In Puerto Ricans
– Oculocutaneous albinismOculocutaneous albinism
ThrombocytosisThrombocytosis
HH- - Hemorrhage, Hereditary Asplenia, Down myeloprol.Hemorrhage, Hereditary Asplenia, Down myeloprol.I- I- Infections, Kawasaki, Immune:Infections, Kawasaki, Immune:GVH, Nephrotic GVH, Nephrotic syndromesyndrome
P- P- Polycythemia vera, Myeloproliferative, EssentialPolycythemia vera, Myeloproliferative, EssentialL- L- Leukemia (CML) Leukemia (CML) A- A- Anemia,- Iron, Vit E deficiency, SideroblasticAnemia,- Iron, Vit E deficiency, SideroblasticT-T- TumorsTumorsE- E- Epinephrine, SteroidsEpinephrine, SteroidsL-L- Lymphoma, HodgkinsLymphoma, HodgkinsE- E- ExerciseExerciseT-T- Trauma, FracturesTrauma, FracturesS-S- Splenectomy Splenectomy

AnemiaAnemia
An 18 month old girl brought in for pallor. Normal diet An 18 month old girl brought in for pallor. Normal diet and PMH. She is alert, interactive, only pallor, normal and PMH. She is alert, interactive, only pallor, normal vital signs, No hepatosplenomegaly, lymph nodes or vital signs, No hepatosplenomegaly, lymph nodes or bruises. bruises.
CBC- Normal WBC, Plt, Hb 4.5g/dl, MCV 74, CBC- Normal WBC, Plt, Hb 4.5g/dl, MCV 74,
AnemiaAnemia– Reduced productionReduced production– Increased destructionIncreased destruction– LossLoss
What else do you want??What else do you want??
Reticulocyte countReticulocyte count
Normal/Low- reduced productionNormal/Low- reduced production– Iron deficiency anemia- Iron deficiency anemia- MCV will be lowMCV will be low
– ALL (leukemia)- ALL (leukemia)- other findings, LN, HSMother findings, LN, HSM
– Diamond Blackfan anemia-Diamond Blackfan anemia- – TECTEC: : Over 1 year of age, Pallor, transient rbc Over 1 year of age, Pallor, transient rbc
production failure, recovers, MCV and Hb F high production failure, recovers, MCV and Hb F high during recovery, rbc transfusion, during recovery, rbc transfusion, rbc ADA normal .rbc ADA normal .
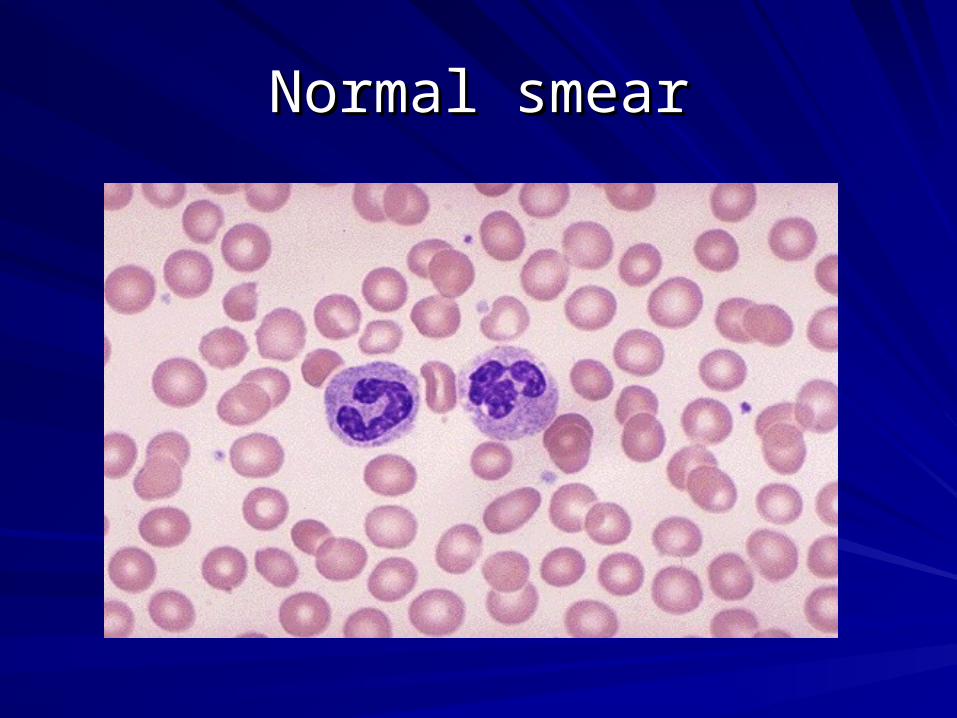
Normal smearNormal smear

A 2 month old girl with a history of ventricular septal defect and horseshoe kidney presents for a health maintenance
visit.
Her parents are concerned that she is not feeding well, appearing to become “tired” soon after beginning to breastfeed. She is tachycardic and appears pale. Her hemoglobin level is 3.8 g/dL. Peripheral smear reveals macrocytic red blood cells. The bone marrow aspirate shows normal cellularity of the marrow with markedly decreased erythroid precursors.
Which of the following findings is most likely to be identified during additional physical examination of this patient?
1.Multiple superficial hemangiomas
2.Cutis aplasia
3.Bifid thumbs
4.Speckled white rings in the periphery of the iris
5.Posterior parietal hair whorl

Microcytic anemia is a characteristic laboratory Microcytic anemia is a characteristic laboratory
abnormality of all listed diseases exceptabnormality of all listed diseases except
1.1. Iron deficiencyIron deficiency
2.2. Lead poisoningLead poisoning
3.3. Sickle cell Sickle cell diseasedisease
4.4. Thalassemia traitThalassemia trait
Iron deficie
ncy
Lead poiso
ning
Sickle ce
ll dise
ase
Thalasse
mia trait
0% 0%0%0%
6
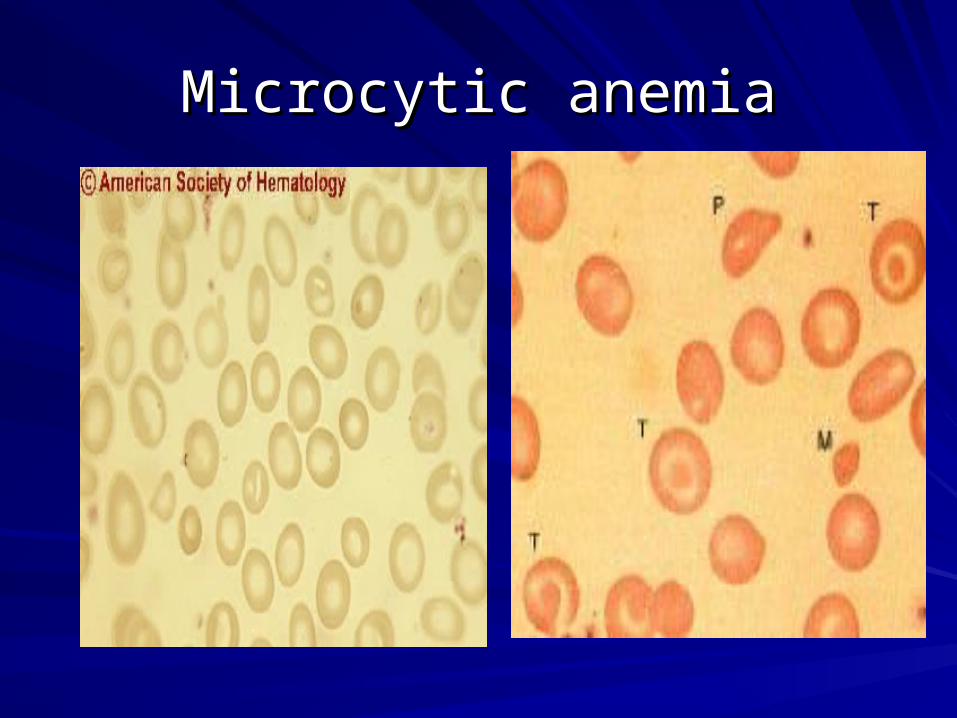
Microcytic anemiaMicrocytic anemia
QuestionQuestion
A blood smear taken from a toddler shows A blood smear taken from a toddler shows microcytic hypochromic anemia. Iron microcytic hypochromic anemia. Iron supplementation therapy is started. When will the supplementation therapy is started. When will the reticulocyte response be at maximum?reticulocyte response be at maximum?
a.a. 1-2 days1-2 days
b.b. 5-7 days5-7 days
c.c. 14-21 days14-21 days
d.d. 3-4 weeks3-4 weeks
e.e. about 6 weeksabout 6 weeks
Iron deficiency questionsIron deficiency questions
Low MCV, low MCHC, low retic, RDW can be normal, Low MCV, low MCHC, low retic, RDW can be normal, Low Iron, Incr TIBC, Transferrin low, Ferritin lowLow Iron, Incr TIBC, Transferrin low, Ferritin lowCauses: Inadequate dietary intakeCauses: Inadequate dietary intake– Toddlers, too much milk, less solids,Toddlers, too much milk, less solids, Breast fed Breast fed
need iron supplementsneed iron supplements– Blood lossBlood loss: Menstrual, GI tract, Meckels, Epistaxis: Menstrual, GI tract, Meckels, Epistaxis
D/D: D/D: Thalassemia trait- Thalassemia trait- MCV much lower in prop to anemiaMCV much lower in prop to anemia
Anemia of chronic disease- low Fe, Anemia of chronic disease- low Fe, low TIBClow TIBC, normal , normal /high Ferritin./high Ferritin.
Question- Beta ThalassemiaQuestion- Beta Thalassemia
3 year old comes for a routine check and found to be 3 year old comes for a routine check and found to be anemic. P/E Normal. CBC Hb 8.9, MCV 58, Iron levels are anemic. P/E Normal. CBC Hb 8.9, MCV 58, Iron levels are normal. Hemoglobin electrophoresis is done and shows normal. Hemoglobin electrophoresis is done and shows Beta Thalassemia trait. All are true except:Beta Thalassemia trait. All are true except:
1.1.The MCV is always lowThe MCV is always low
2.2.Fetal hemoglobin is < 2%Fetal hemoglobin is < 2%
3.3.Hemoglobin A 2 is > 3.5%Hemoglobin A 2 is > 3.5%
4.4.Does not respond to IronDoes not respond to Iron
5.5.RDW is usually normalRDW is usually normal
Beta Thalassemia MinorBeta Thalassemia Minor
Quantitative defect in Quantitative defect in globin chainsglobin chains– Reduced production of Reduced production of
Beta chainsBeta chains
Hb electrophoresisHb electrophoresis– Hb A- 2 Alpha, 2 BetaHb A- 2 Alpha, 2 Beta– Hb F- 2 Alpha, 2 GammaHb F- 2 Alpha, 2 Gamma– Hb A2- 2 Alpha, 2 DeltaHb A2- 2 Alpha, 2 Delta
Excess Alpha combines Excess Alpha combines with Gamma or Delta- with Gamma or Delta- Increased Hb F and AIncreased Hb F and A22..Smear abnormalities Smear abnormalities significant even with significant even with MILDMILD anemia. anemia.
AnemiaAnemiaLow MCV, normal RDW, Low MCV, normal RDW, normal reticnormal reticSmear shows aniso and Smear shows aniso and poikulocytosis, target poikulocytosis, target cells, microcytes, cells, microcytes, misshapen cells, misshapen cells, basophilic stipplingbasophilic stipplingHb Electrophoresis: Hb Electrophoresis: Increased Hb AIncreased Hb A22 and/or F. and/or F.Normal iron studies, no Normal iron studies, no response to ironresponse to iron
Beta Thalassemia MajorBeta Thalassemia Major
No production of Beta chains- Chromosome 11No production of Beta chains- Chromosome 11Autosomal recessiveAutosomal recessive25 % chance with each pregnancy25 % chance with each pregnancyPre-natal testing for carriersPre-natal testing for carriersChorionic villous sampling for diagnosisChorionic villous sampling for diagnosisTransfusion dependent-allows for normal developmentTransfusion dependent-allows for normal developmentPen Prophylaxis, Anti oxidantsPen Prophylaxis, Anti oxidantsSplenectomy after age 5Splenectomy after age 5Iron overload- inherent and transfusionIron overload- inherent and transfusionNeed chelatorsNeed chelators
QuestionQuestion4 year old male with no complaints. Routine CBC showed a 4 year old male with no complaints. Routine CBC showed a Hb9.8, MCV 62, RDW 12.5 , Retic 0.2%, Normal Iron Hb9.8, MCV 62, RDW 12.5 , Retic 0.2%, Normal Iron studies, Hemoglobin electrophoresis was normal with studies, Hemoglobin electrophoresis was normal with normal Hb A2 and Hb F. You suspect Alpha Thalassemia. normal Hb A2 and Hb F. You suspect Alpha Thalassemia. All of the statements are true except:All of the statements are true except:1.1.It is carried on 4 allelesIt is carried on 4 alleles
2.2.The severe form is Hydrops fetalisThe severe form is Hydrops fetalis
3.3.Hemoglobin H disease occurs when 3 alleles are affectedHemoglobin H disease occurs when 3 alleles are affected
4.4.Diagnosed by newborn screening when a “fast moving” hemoglobin Diagnosed by newborn screening when a “fast moving” hemoglobin is noted.is noted.
5.5.Fast moving hemoglobin is made up of a hemoglobin with 4 beta Fast moving hemoglobin is made up of a hemoglobin with 4 beta chainschains
Thalassemia- AlphaThalassemia- Alpha
Reduced Alpha chainsReduced Alpha chains
4 types- carried on 4 allelles. (4 types- carried on 4 allelles. (xx/xxxx/xx))
One absent- Silent carrier (One absent- Silent carrier (x-/xx)x-/xx)
2 absent- Alpha Thal trait (2 absent- Alpha Thal trait (xx/- - or x-/x-xx/- - or x-/x-))
3 absent- Hb H disease (3 absent- Hb H disease (x-/- -x-/- -) Has 4 excess ) Has 4 excess Beta chains)Beta chains)
4 absent- Hydrops fetalis (- -/- -)4 absent- Hydrops fetalis (- -/- -)
NB period: Excess Gamma chains form Hb NB period: Excess Gamma chains form Hb Barts- FAST moving Hb on Newborn screeningBarts- FAST moving Hb on Newborn screening
CaseCase
3 year old patient is brought to the ER with 3 year old patient is brought to the ER with complaints of feeling very tired over the complaints of feeling very tired over the past 3 days.past 3 days.
Patient is pale, jaundiced with the spleen Patient is pale, jaundiced with the spleen tip palpable.tip palpable.
CBC Hb 5, Retic 5 %, LDH Increased,CBC Hb 5, Retic 5 %, LDH Increased,
What does this sound like??What does this sound like??
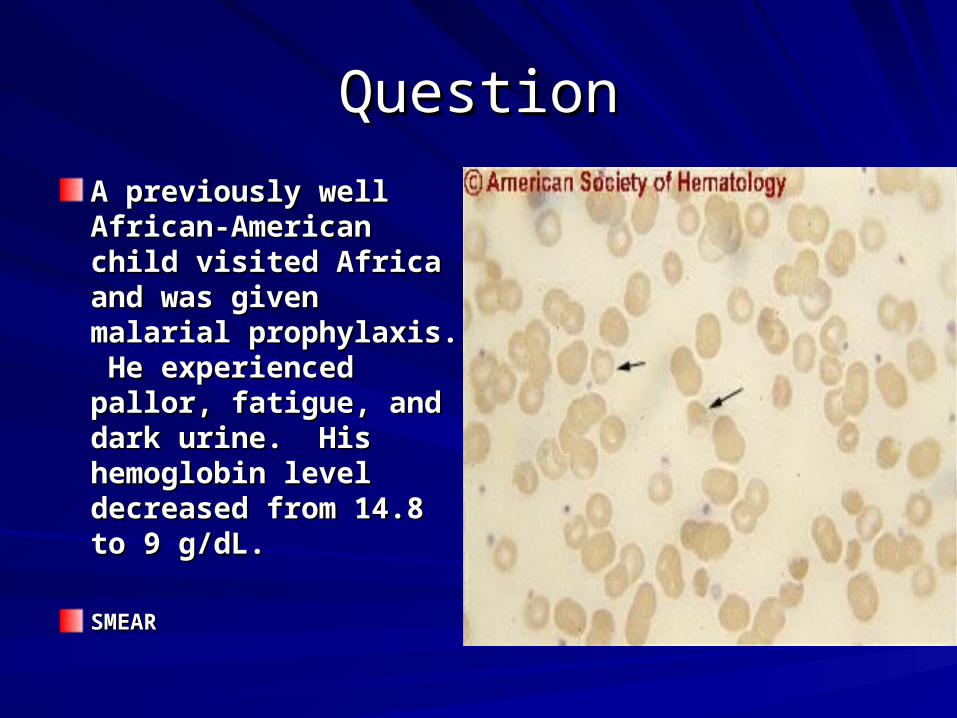
QuestionQuestion
A previously well A previously well African-American child African-American child visited Africa and was visited Africa and was given malarial given malarial prophylaxis. He prophylaxis. He experienced pallor, experienced pallor, fatigue, and dark urine. fatigue, and dark urine. His hemoglobin level His hemoglobin level decreased from 14.8 to decreased from 14.8 to 9 g/dL. 9 g/dL.
SMEARSMEAR
An African-Am child visited Africa & received malaria An African-Am child visited Africa & received malaria prophylaxis. He hasprophylaxis. He has
1.1. Hereditary Hereditary spherocytosisspherocytosis
2.2. Sickle cell Sickle cell diseasedisease
3.3. HepatitisHepatitis
4.4. G6PD G6PD deficiencydeficiency
Heredita
ry sp
herocy
tosis
Sickle ce
ll dise
ase
Hepatitis
G6PD deficiency
0% 0%0%0%
6
Reticulocyte count- IncreasedReticulocyte count- Increased
HemolysisHemolysis– Intrinsic-Intrinsic-
Membrane defects-Hereditary spherocytosis (HS)Membrane defects-Hereditary spherocytosis (HS)
Enzyme-G 6 PD deficiencyEnzyme-G 6 PD deficiency
HemoglobinopathiesHemoglobinopathies
– Extrinsic- Extrinsic- AIHA (Auto-immune hemolytic anemia), AIHA (Auto-immune hemolytic anemia), DIC, Intravascular hemolysisDIC, Intravascular hemolysis
LossLoss– Blood lossBlood loss
Children with hereditary spherocytosis have Children with hereditary spherocytosis have all of the listed conditions except:all of the listed conditions except:
1.1. positive Direct positive Direct Coombs Coombs
2.2. splenomegaly, splenomegaly, gallbladder stones gallbladder stones
3.3. abnormalities in abnormalities in spectrin and /or spectrin and /or ankyrinankyrin
4.4. increased MCHCincreased MCHC5.5. abnormal osmotic abnormal osmotic
fragility test.fragility test.positi
ve Direct
Coombs
splenomegaly,
gallb
ladde...
abnormaliti
es in sp
ectrin...
incre
ased M
CHC
abnormal o
smotic f
ragil
i..
0% 0% 0%0%0%
6
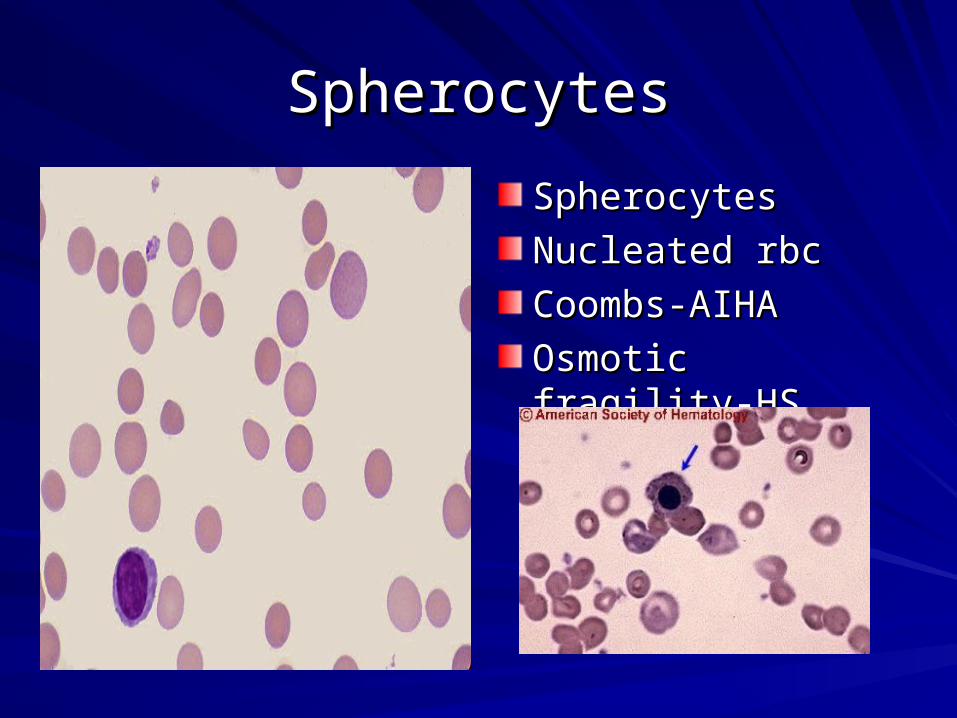
SpherocytesSpherocytes
SpherocytesSpherocytes
Nucleated rbcNucleated rbc
Coombs-AIHACoombs-AIHA
Osmotic fragility-HSOsmotic fragility-HS
HS- with severe anemiaHS- with severe anemia
A 6 year old girl who has hereditary spherocytosis A 6 year old girl who has hereditary spherocytosis presents with a 1 week history of fever. Physical presents with a 1 week history of fever. Physical examination reveals abdominal pain, vomiting, fatigue examination reveals abdominal pain, vomiting, fatigue and pallor. Her hemoglobin is typically about 10 g/dL and pallor. Her hemoglobin is typically about 10 g/dL with a reticulocyte count of 9%, but now, her with a reticulocyte count of 9%, but now, her hemoglobin is 4 g/dL and the reticulocyte count is 1%. hemoglobin is 4 g/dL and the reticulocyte count is 1%. Her bilirubin is 1 mg/dL. Of the following, the MOST Her bilirubin is 1 mg/dL. Of the following, the MOST likely cause for this girl’s present illness is infection likely cause for this girl’s present illness is infection withwith
– Coxsackie virusCoxsackie virus– Parvovirus B19Parvovirus B19– Epstein-Barr virusEpstein-Barr virus– Hepatitis A virusHepatitis A virus– Influenza A virusInfluenza A virus
HS- with severe anemiaHS- with severe anemia
1.1. Coxsackie virusCoxsackie virus
2.2. Parvovirus B19Parvovirus B19
3.3. Epstein-Barr Epstein-Barr virusvirus
4.4. Hepatitis A Hepatitis A virusvirus
5.5. Influenza A Influenza A virusvirus
Coxsack
ie viru
s
Parvoviru
s B19
Epstein-B
arr vir
us
Hepatitis A vi
rus
Influenza A
virus
0% 0% 0%0%0%
6
Newborn Screening QuestionsNewborn Screening Questions
You get a call from a frantic parent because she You get a call from a frantic parent because she received a letter from the State regarding her received a letter from the State regarding her baby’s test results on NBS.baby’s test results on NBS.FS- FS- SSSS disease, disease, S-BS-B00 Thal, Sickle cell w/ HPFH. Thal, Sickle cell w/ HPFH.FSA- FSA- Sickle BSickle B+ + thalthal, Sickle cell trait, Sickle cell traitFSC- FSC- SC diseaseSC diseaseFAS- Sickle cell traitFAS- Sickle cell traitFAC- Hb C traitFAC- Hb C traitFAE- Hb E traitFAE- Hb E traitFEFE - Hb EE disease, E-Thal- Hb EE disease, E-Thal
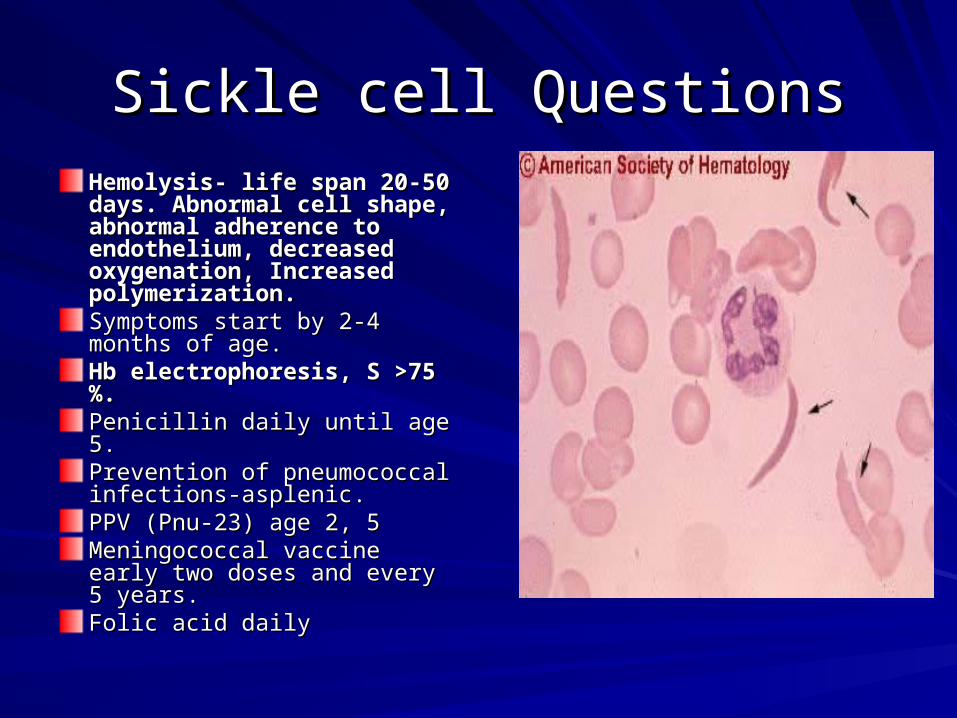
Sickle cell QuestionsSickle cell Questions
Hemolysis- life span 20-50 Hemolysis- life span 20-50 days. Abnormal cell shape, days. Abnormal cell shape, abnormal adherence to abnormal adherence to endothelium, decreased endothelium, decreased oxygenation, Increased oxygenation, Increased polymerization.polymerization.Symptoms start by 2-4 months Symptoms start by 2-4 months of age.of age.Hb electrophoresis, S >75 %.Hb electrophoresis, S >75 %.Penicillin daily until age 5. Penicillin daily until age 5. Prevention of pneumococcal Prevention of pneumococcal infections-asplenic.infections-asplenic.PPV (Pnu-23) age 2, 5PPV (Pnu-23) age 2, 5Meningococcal vaccine early Meningococcal vaccine early two doses and every 5 years.two doses and every 5 years.Folic acid dailyFolic acid daily

Sickle cell questionsSickle cell questions
Vaso-occlusive crisisVaso-occlusive crisis
New infant born in another country presenting with New infant born in another country presenting with swollen hands---Dactylitisswollen hands---Dactylitis
Aplastic crisis: Aplastic crisis: – low Hb, low retic, Secondary to Parvovirus B 19 infection.low Hb, low retic, Secondary to Parvovirus B 19 infection.
Splenic sequestration crisis: Splenic sequestration crisis: – Sudden enlargement of the spleen in SS or older SC patient Sudden enlargement of the spleen in SS or older SC patient – Rx- Transfuse Rx- Transfuse – Teach spleen palpationTeach spleen palpation– Splenectomy Splenectomy
The mother of a 10 month old baby with SS disease asks you about The mother of a 10 month old baby with SS disease asks you about prognostic indicators. All of the following indicate likelihood of more prognostic indicators. All of the following indicate likelihood of more
severe disease except:severe disease except:
1.1. High WBCHigh WBC
2.2. Associated alpha Associated alpha thalassemia traitthalassemia trait
3.3. Low hemoglobinLow hemoglobin
4.4. Repeated Repeated episodes of episodes of dactylitisdactylitis
High WBC
Associa
ted alpha thalass.
..
Low hemoglobin
Repeated episodes o
f dac..
.
0% 0%0%0%
6
Sickle cell Sickle cell Acute Chest SyndromeAcute Chest Syndrome
True statements include all True statements include all exceptexcept::1. 1. Presents with a new infiltrate on X-rayPresents with a new infiltrate on X-ray
2. Due to infarction, infection, BM fat embolism2. Due to infarction, infection, BM fat embolism3. Treat with antibiotics to cover pneumococcus, 3. Treat with antibiotics to cover pneumococcus,
Mycoplasma, ChlamydiaMycoplasma, Chlamydia 4. Treat with bronchodilator, Incentive spirometry, 4. Treat with bronchodilator, Incentive spirometry,
transfusion, Steroids (controversial).transfusion, Steroids (controversial).5. Intensive hydration is important5. Intensive hydration is important
TCD- Transcranial DopplerTCD- Transcranial Doppler
A routine TCD on a 4 A routine TCD on a 4 year old patient with year old patient with SS disease shows a SS disease shows a Cerebral blood flow Cerebral blood flow (CBF) of 210 (CBF) of 210 cm/second.cm/second.What is the next What is the next step?step?STOP studies- STOP STOP studies- STOP I and III and II
According to the STOP protocol all children with According to the STOP protocol all children with abnormal TCD require enrollment in hypertransfusion abnormal TCD require enrollment in hypertransfusion
protocol till (choose one)protocol till (choose one)
1.1. Repeat TCD is Repeat TCD is normalnormal
2.2. Continue Continue indefinitelyindefinitely
3.3. the child reaches the child reaches 18 years 18 years
4.4. MRA/MRI are MRA/MRI are reported normalreported normal
Repeat TCD is
normal
Continue indefinite
ly
the ch
ild re
aches 1
8 years
MRA/M
RI are
reporte
d ...
0% 0%0%0%
6
Sickle cell and Stroke QuestionsSickle cell and Stroke Questions
Affects 10 % of patientsAffects 10 % of patientsInfarctive stroke (younger patients) Infarctive stroke (younger patients) Hemorrhagic stroke (older)Hemorrhagic stroke (older)STOP I study established the role of yearly TCD STOP I study established the role of yearly TCD (transcranial doppler) to measure cerebral blood (transcranial doppler) to measure cerebral blood flow velocity as a tool for determining stroke risk.flow velocity as a tool for determining stroke risk.Transfusion therapy as current therapy for Transfusion therapy as current therapy for high risk patients (CBF> 200cm/sec)high risk patients (CBF> 200cm/sec)Reversal of CBF velocity is not sufficient to stop Reversal of CBF velocity is not sufficient to stop transfusion therapy. (STOP II)transfusion therapy. (STOP II)

Sickle cell and HydroxyureaSickle cell and Hydroxyurea
FDA approved for adultsFDA approved for adultsStudies in children demonstrated efficacy and Studies in children demonstrated efficacy and safetysafetyIncreases hemoglobin F levelIncreases hemoglobin F levelIncreases hemoglobinIncreases hemoglobinDecreases WBC – ancillary effectDecreases WBC – ancillary effectReduces number of ACS, VOCReduces number of ACS, VOCHydroxyurea is recommended by the Hydroxyurea is recommended by the hematologist for patients who have recurrent hematologist for patients who have recurrent vaso-occlusive crises, acute chest syndrome. vaso-occlusive crises, acute chest syndrome.
A healthy 5 year old boy- 2 day hx of fever, P/E normal A healthy 5 year old boy- 2 day hx of fever, P/E normal
1.1. Amoxicillin for 10 Amoxicillin for 10 daysdays
2.2. G- CSF for 10 days.G- CSF for 10 days.3.3. BM aspirateBM aspirate4.4. Refer to a Refer to a
hematologisthematologist5.5. Repeat CBC in 1-2 Repeat CBC in 1-2
weeksweeks
No hepatosplenomegaly, LN, no focus of infection. CBC WBC 3, Neutrophils 25 %, Hb 12, Platelet 200X109/L, ANC 750. Most appropriate step is
Amoxicillin
for 1
0 days
G- CSF f
or 10 days.
BM as
pirate
Refer to a hemato
logist
Repeat CBC in
1-2 weeks
0% 0% 0%0%0%
6
CaseCase
A 2-year-old boy has had several 10-day-long episodes A 2-year-old boy has had several 10-day-long episodes of fever, mouth ulcerations, stomatitis, and pharyngitis. of fever, mouth ulcerations, stomatitis, and pharyngitis. These episodes have occurred at about monthly These episodes have occurred at about monthly intervals. Absolute neutrophil counts have been intervals. Absolute neutrophil counts have been 50/mm³on day 1 of each illness, 500/mm³ on day 10, and 50/mm³on day 1 of each illness, 500/mm³ on day 10, and 1,500/mm³ on day 14.1,500/mm³ on day 14.
Among the following, the MOST likely cause for the findings in Among the following, the MOST likely cause for the findings in this patient isthis patient isA. chronic benign neutropeniaA. chronic benign neutropeniaB. cyclic neutropeniaB. cyclic neutropeniaC. Schwachman-Diamond syndromeC. Schwachman-Diamond syndromeD. severe congenital neutropeniaD. severe congenital neutropeniaE.. transient viral bone marrow suppressionE.. transient viral bone marrow suppression
Abnormal BleedingAbnormal Bleeding
Epistaxis unrelieved by 15 minutes of Epistaxis unrelieved by 15 minutes of pressure, both nostrils, requiring an ER pressure, both nostrils, requiring an ER visit, documented drop of hemoglobin. visit, documented drop of hemoglobin. Menstrual periods( amount, pads, Menstrual periods( amount, pads, duration)duration) Bleeding after procedures (circumcision, Bleeding after procedures (circumcision, dental extractions, T and A-dental extractions, T and A-delayed bleeddelayed bleed))Ecchymoses/bruising inconsistent with Ecchymoses/bruising inconsistent with the degree of traumathe degree of trauma
Bleeding patientBleeding patient
Physical Examination:Physical Examination:Type of bleeding: Superficial or deepType of bleeding: Superficial or deep– Bruises, PetechiaeBruises, Petechiae– Epistaxis, Gum bleeding, Excessive menstrual Epistaxis, Gum bleeding, Excessive menstrual
bleedingbleeding– Site of bleedingSite of bleeding– Bleeding into the joints and soft tissuesBleeding into the joints and soft tissues– Look for evidence of shockLook for evidence of shock– Medication history (Aspirin, NSAIDS) Medication history (Aspirin, NSAIDS)
Lab studiesLab studies(What do they measure?)(What do they measure?)
CBC and Peripheral smearCBC and Peripheral smear
PT, INR and PTTPT, INR and PTT– PT - Factor VII, common pathwayPT - Factor VII, common pathway– PTT- Factor VIII, IX, XI, XII, common pathwayPTT- Factor VIII, IX, XI, XII, common pathway
Mixing studies (Inhibitors and deficiency)Mixing studies (Inhibitors and deficiency)
Specific coagulation factor assaysSpecific coagulation factor assays
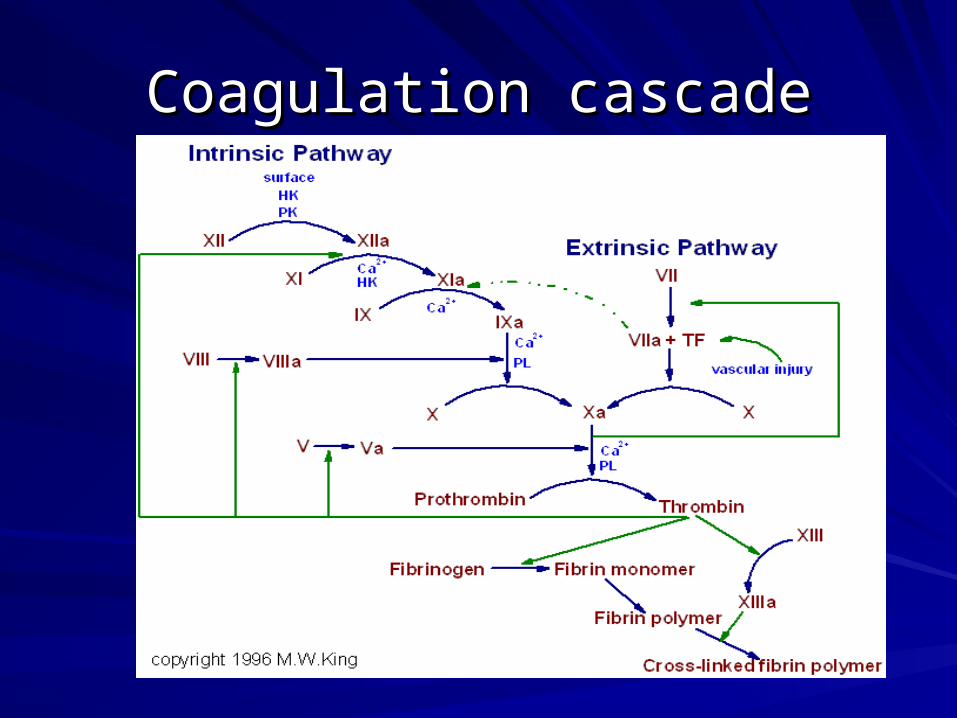
Coagulation cascadeCoagulation cascade

Questions on Questions on Circulating anticoagulantCirculating anticoagulant
Mixing studyMixing study
If PT or PTT is prolonged, ask for a mixing If PT or PTT is prolonged, ask for a mixing study.study.
Mix patient plasma with equal amount of normal Mix patient plasma with equal amount of normal plasma, the test will normalize if the abnormal plasma, the test will normalize if the abnormal result is because of a deficiency in factor. result is because of a deficiency in factor.
If there is an anticoagulant, it will not normalize If there is an anticoagulant, it will not normalize or even if it does, it will become abnormal again or even if it does, it will become abnormal again after incubation.after incubation.
A A healthy 2-day-old boy born at term undergoes healthy 2-day-old boy born at term undergoes circumcision. circumcision.
1.1. Disseminated Disseminated intravascular intravascular coagulationcoagulation
2.2. Factor VIII deficiency Factor VIII deficiency hemophiliahemophilia
3.3. Immune Immune thrombocytopenic thrombocytopenic purpurapurpura
4.4. Neonatal alloimmune Neonatal alloimmune thrombocytopeniathrombocytopenia
5.5. Von Willebrand diseaseVon Willebrand disease
Bleeding noted at the site 10 hours after the procedure and increased steadily over the past 4 hours. Findings on exam are unremarkable except for bleeding along 2 to 3 mm of the surgical site; no petechiae or purpura.
Disseminate
d intra
vascu
la.
Facto
r VIII
deficiency
h...
Immune th
rombocy
tope...
Neonatal allo
immune t.
..
Von Wille
brand dise
ase
0% 0% 0%0%0%
6
Hemophilia QuestionsHemophilia Questions
Factor VIII deficiency (Hemophilia A)-85%Factor VIII deficiency (Hemophilia A)-85%– X-linked recessive, Carriers asymptomaticX-linked recessive, Carriers asymptomatic
– Severe<1%, Moderate 1-5, Mild 6-30 %Severe<1%, Moderate 1-5, Mild 6-30 %– Treat Recombinant Factor VIII 1unit/kg raises factor Treat Recombinant Factor VIII 1unit/kg raises factor
level by 2 %. Half life 12 hrs. Joint bleeds need100%, level by 2 %. Half life 12 hrs. Joint bleeds need100%, muscle bleeds 50 %.muscle bleeds 50 %.
– DDAVP for mild casesDDAVP for mild cases..– 30 % develop inhibitors after infusions with concentrate 30 % develop inhibitors after infusions with concentrate
(Approx 50 infusions)(Approx 50 infusions)
Factor IX deficiency (Hemophilia B)Factor IX deficiency (Hemophilia B)– X-linked recessive, less commonX-linked recessive, less common
A patient with Hemophilia A has asked you about the A patient with Hemophilia A has asked you about the possibility of his children being affected by the disease. possibility of his children being affected by the disease.
1.1. There is a 50 % chance There is a 50 % chance that his sons will have the that his sons will have the disease.disease.
2.2. There is a 50 % chance There is a 50 % chance that his daughters will be that his daughters will be carrierscarriers
3.3. There is a 100 % chance There is a 100 % chance that his sons will have the that his sons will have the diseasedisease
4.4. There is a 100 % chance There is a 100 % chance that his daughters will be that his daughters will be carrierscarriers
The partner is normal.
There is a 50 %
chance
th..
There is a 50 %
chance
th..
There is a 100 %
chance
th..
There is a 100 %
chance
th..
0% 0%0%0%
CaseCase
13 year old girl just started her periods and 13 year old girl just started her periods and has been bleeding for the past 16 days. has been bleeding for the past 16 days. She has used 14 pads a day and is tired. She has used 14 pads a day and is tired. Her vital signs are stable, Hb 9.5, PT, PTT Her vital signs are stable, Hb 9.5, PT, PTT normal. normal. The mother had heavy periods and her 6 The mother had heavy periods and her 6 year old brother has nose bleeds for the year old brother has nose bleeds for the past 2 years.past 2 years.Likely to have:Likely to have:
Questions on Von Willebrand’s DiseaseQuestions on Von Willebrand’s Disease1-2 % of population1-2 % of population
Type IType I - - 80 % of cases;80 % of cases; Quantitative defect, Autosomal Quantitative defect, Autosomal dominant (AD)dominant (AD)
Type 2Type 2 - 15-20 %, Qualitative defect - 15-20 %, Qualitative defect– 2A, 2b (thrombocytopenia), 2M, 2N (AR)2A, 2b (thrombocytopenia), 2M, 2N (AR)
Type 3Type 3 - - Severe (similar to hemophilia A)Severe (similar to hemophilia A)Autosomal recessive (AR)Autosomal recessive (AR)DDAVPDDAVP- - Releases VWF from endothelial cells and stabilizes Releases VWF from endothelial cells and stabilizes Factor VIIIFactor VIII– SE: Water retention, Tachyphylaxis, hyponatremia. SE: Water retention, Tachyphylaxis, hyponatremia. – For mild Hemophilia, Type I VWD, 2For mild Hemophilia, Type I VWD, 2– Contra-indicated in Type 2BContra-indicated in Type 2B
Rx-Plasma derived VWF containing concentratesRx-Plasma derived VWF containing concentrates
ThrombophiliaThrombophilia
A 14 year old male presents with chest pain and difficulty A 14 year old male presents with chest pain and difficulty breathing. He notes that his right calf has been swollen breathing. He notes that his right calf has been swollen for the last 3 days and he has difficulty placing his foot for the last 3 days and he has difficulty placing his foot on the ground. P/E Pain on dorsiflexion, Air entry on the ground. P/E Pain on dorsiflexion, Air entry reduced. CXR and EKG are normal. VQ scan shows a reduced. CXR and EKG are normal. VQ scan shows a filling defect and a diagnosis of DVT and pulmonary filling defect and a diagnosis of DVT and pulmonary embolism is made.embolism is made.What are the important questions on history?What are the important questions on history?– History of DVT in family membersHistory of DVT in family members– H/o recurrent late miscarriages in mother and her sisters.H/o recurrent late miscarriages in mother and her sisters.– H/o trauma and precipitating factorsH/o trauma and precipitating factors
The most common cause of familial The most common cause of familial
predisposition to thrombosis ispredisposition to thrombosis is 1.1. Hemophilia Hemophilia
antibodiesantibodies2.2. Protein C Protein C
deficiencydeficiency3.3. Protein S Protein S
deficiencydeficiency4.4. Factor V Leiden Factor V Leiden
mutationmutation5.5. Antithrombin III Antithrombin III
deficiencydeficiency
Hemophilia antibodies
Protein C deficie
ncy
Protein S
deficiency
Facto
r V Le
iden mutation
Antithro
mbin III deficie
ncy
0% 0% 0%0%0%
Tests performed on donated units of bloodTests performed on donated units of blood
1.1. all units are tested only for all units are tested only for hepatitis B and Chepatitis B and C
2.2. all units are tested only for all units are tested only for human immuno-deficiency human immuno-deficiency virus (HIV)virus (HIV)
3.3. all units are tested for HIV, all units are tested for HIV, hepatitis B, and hepatitis Chepatitis B, and hepatitis C
4.4. all units are tested for HIV, all units are tested for HIV, hepatitis B, hepatitis C, sickle hepatitis B, hepatitis C, sickle cell trait, cytomegalovirus, cell trait, cytomegalovirus, and Epstein-Barr virusand Epstein-Barr virus
5.5. only units obtained from only units obtained from donors who have one or donors who have one or more risk factors are more risk factors are screened for HIV, all units screened for HIV, all units are tested only for hepatitis B are tested only for hepatitis B and Cand C
6all u
nits are
teste
d only f..
all units
are te
sted only f..
all units
are te
sted fo
r HI..
all units
are teste
d for H
...
only units obta
ined fro...
0% 0% 0%0%0%
Questions on TransfusionQuestions on Transfusion
CMV negative- give leukocyte reduced.CMV negative- give leukocyte reduced.
Irradiated products- To prevent GVHDIrradiated products- To prevent GVHD
Washed cells- Washed cells-
Phenotype matchedPhenotype matched– To prevent allo-immunizationTo prevent allo-immunization
Sickle negativeSickle negative
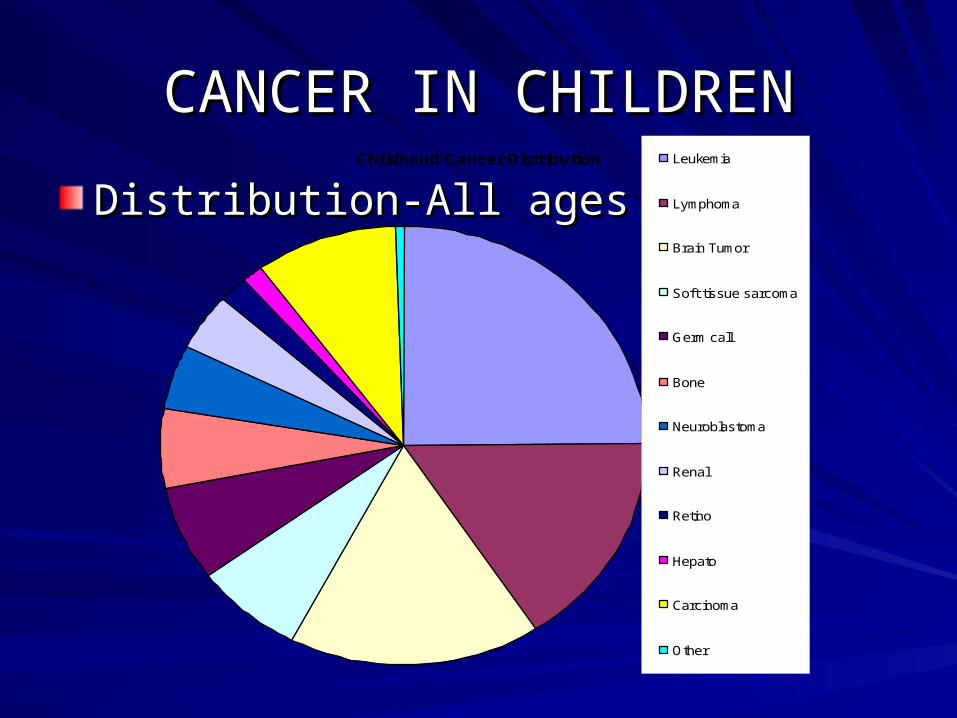
CANCER IN CHILDRENCANCER IN CHILDREN
Distribution-All agesDistribution-All agesChildhood Cancer Distribution Leukemia
Lymphoma
Brain Tumor
Soft tissue sarcoma
Germ call
Bone
Neuroblastoma
Renal
Retino
Hepato
Carcinoma
Other
A 6-year-old girl has aching in her arms, legs, and back for > 2 weeks. A 6-year-old girl has aching in her arms, legs, and back for > 2 weeks.
1.1. ALLALL2.2. Aplastic anemiaAplastic anemia3.3. Gaucher diseaseGaucher disease4.4. lead poisoninglead poisoning5.5. Multifocal Multifocal
osteomyelitisosteomyelitis
Results of laboratory tests include hemoglobin, 9.4 g/dL; white blood cell count, 5,600/mm³ with no abnormal cells noted on smear; and platelet count, 106,000/mm³. Radiographs of long bones reveal osteolytic lesions and radiolucent metaphyseal growth arrest lines.
ALL
Aplastic a
nemia
Gaucher d
isease
lead poisoning
Multifo
cal o
steomyeliti
s
0% 0% 0%0%0%
6
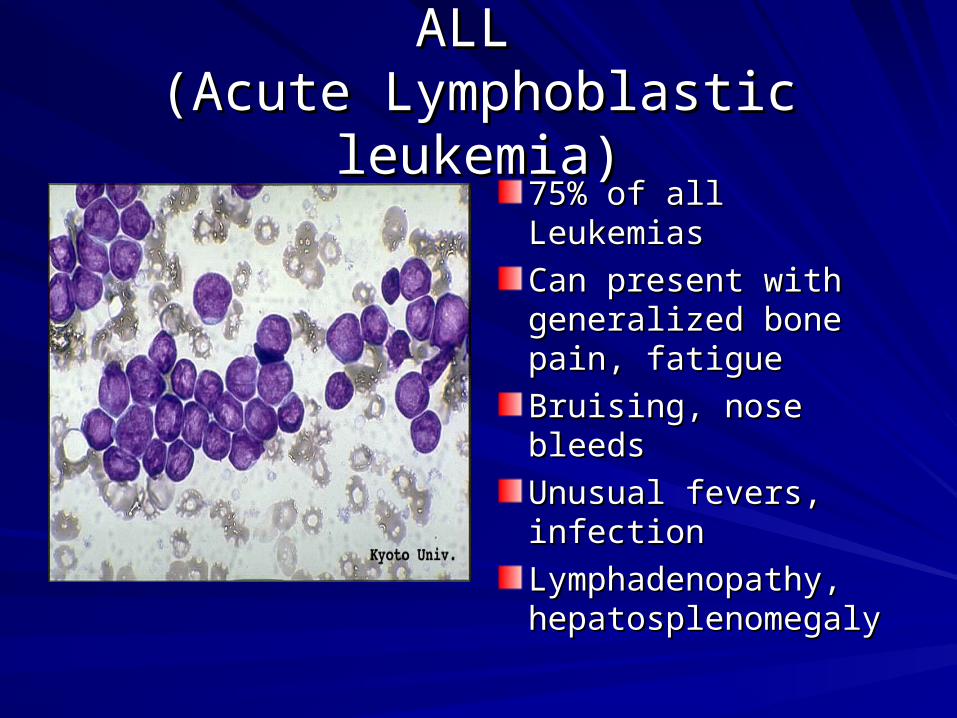
ALL ALL (Acute Lymphoblastic leukemia)(Acute Lymphoblastic leukemia)
75% of all Leukemias75% of all Leukemias
Can present with Can present with generalized bone generalized bone pain, fatiguepain, fatigue
Bruising, nose bleedsBruising, nose bleeds
Unusual fevers, Unusual fevers, infectioninfection
Lymphadenopathy, Lymphadenopathy, hepatosplenomegalyhepatosplenomegaly
ALL- Should knowALL- Should know (Acute Lymphoblastic leukemia) (Acute Lymphoblastic leukemia)Abnormal to see blasts in the peripheral smearAbnormal to see blasts in the peripheral smear
Diagnosis: >25 % blasts in the BM.Diagnosis: >25 % blasts in the BM.
Normal marrow has < 5 % blastsNormal marrow has < 5 % blasts
Single most common childhood cancer (29% of Single most common childhood cancer (29% of all childhood cancers); 2500-3500 cases per all childhood cancers); 2500-3500 cases per yearyear
Peak age 2-5 yearsPeak age 2-5 yearsMore likely in Trisomy 21, Ataxia-Telangiectasia, Bloom More likely in Trisomy 21, Ataxia-Telangiectasia, Bloom syndrome, Kostmann’s, Monosomy 7, DBA, Fanconi syndrome, Kostmann’s, Monosomy 7, DBA, Fanconi anemia, 20% risk in twin if age <5yrsanemia, 20% risk in twin if age <5yrs
ALL TreatmentALL TreatmentInduction:Induction: 4-6 weeks, 4-6 weeks, Consolidation /delayed IntensificationConsolidation /delayed Intensification:: 6-12 months; rotating drugs.6-12 months; rotating drugs.
MaintenanceMaintenance : Daily oral 6-MP, weekly MTX, Monthly : Daily oral 6-MP, weekly MTX, Monthly pulses of Vincristine and Steroid.pulses of Vincristine and Steroid.Imatinib mesylate-Tyrosine Kinase Inhibitor- Ph Imatinib mesylate-Tyrosine Kinase Inhibitor- Ph Chromosome positive patientsChromosome positive patientsCNS prophylaxisCNS prophylaxis: Intrathecal chemo: Intrathecal chemoCNS TherapyCNS Therapy: RT + Intensive systemic chemo: RT + Intensive systemic chemoTesticular diseaseTesticular disease: RT: RTSANCTUARY- CNS, TestisSANCTUARY- CNS, Testis
ALL- PrognosisALL- Prognosis
Prognosis:Prognosis: WBC, Age, Cytogenetics WBC, Age, Cytogenetics
– good if hyperdiploidy (>50),trisomy 4,10,17, t(12,21)good if hyperdiploidy (>50),trisomy 4,10,17, t(12,21)– Bad if hypodiploid, Ph. chrom t (9,22),t(4,11), t(8,14)Bad if hypodiploid, Ph. chrom t (9,22),t(4,11), t(8,14)
Immunophenotype: Pre-B good, B and T-worseImmunophenotype: Pre-B good, B and T-worseEarly response, Minimal residual disease (MRD)Early response, Minimal residual disease (MRD)Infants: 50 % survivalInfants: 50 % survivalEarly relapse is a poor signEarly relapse is a poor sign
Down Syndrome and LeukemiaDown Syndrome and Leukemia
10-20 fold increase10-20 fold increaseDS: 400 fold Increase in M7 AMLDS: 400 fold Increase in M7 AMLSuperior response to Rx of Superior response to Rx of AMLAMLTransient Myeloproliferative disorder in Transient Myeloproliferative disorder in newborn which resolves within 3 months. newborn which resolves within 3 months.
Acute Myeloid Leukemia (AML)Acute Myeloid Leukemia (AML)
20 % of all leukemias20 % of all leukemiasIncreased incidence in < 1 year of ageIncreased incidence in < 1 year of ageHigher incidence:Higher incidence:– Downs, Fanconi, Bloom, DBA, Kostmann, Downs, Fanconi, Bloom, DBA, Kostmann,
Neurofibromatosis I, Schwachman-DiamondNeurofibromatosis I, Schwachman-Diamond
Chloromas– solid collection in bone/soft tissuesChloromas– solid collection in bone/soft tissuesTypes: M0-M7, commonest M2Types: M0-M7, commonest M2DIC in M3- (Promyelocytic- APML)DIC in M3- (Promyelocytic- APML)M7- Downs syndromeM7- Downs syndrome
Question HodgkinsQuestion Hodgkins
16 year old male presents with a painless swelling in the 16 year old male presents with a painless swelling in the supraclavicular region. Biopsy shows Hodgkins disease supraclavicular region. Biopsy shows Hodgkins disease Stage 2. Stage 2. All are true exceptAll are true except::
• 1. Presence of “B” symptoms is worse for prognosis1. Presence of “B” symptoms is worse for prognosis• 2. B symptoms are fever, increasing size of mass2. B symptoms are fever, increasing size of mass• 3. Staging depends on whether it is on one or both sides 3. Staging depends on whether it is on one or both sides
of the diaphragmof the diaphragm• 4. Sperm banking should be done4. Sperm banking should be done• 5. Second malignancy can occur in patients who receive 5. Second malignancy can occur in patients who receive
combination chemo and RTcombination chemo and RT
QuestionQuestion
4 year old boy presents with a 6 day history of bilateral, rapidy progressive facial swelling. There is no history of associated trauma or upper respiratory symptoms. On P/E, there is significant swelling below both eyes and of both cheeks. The angle of the jaw is maintained. On examination of the oral cavity, both the soft and hard palate are swollen as are the gingiva. The teeth are loose and inverted due to the degree of gingival swelling. A CT of the sinuses reveals extensive bilateral opacification of both maxillary sinuses. LDH was 1,850 U/L. Which of the following is the most likely to cause of this patient’s physical findings?
1. Human herpesvirus 6
2. Cytomegalovirus
3. Cryptosporidium hominis
4. Parvovirus B19
5. Epstein-Barr virus

Burkitt’s LymphomaBurkitt’s Lymphoma
Endemic Burkitt’s Endemic Burkitt’s – African type, head and African type, head and
neck, jawneck, jaw– 95 % chance of EBV95 % chance of EBV
Sporadic Burkitt’s Sporadic Burkitt’s – AbdomenAbdomen– 15-20 % chance of 15-20 % chance of
EBVEBVt (8;14)t (8;14)Immunotherapy: Anti-CD Immunotherapy: Anti-CD 20 monoclonal antibody; 20 monoclonal antibody; (Rituximab)(Rituximab)
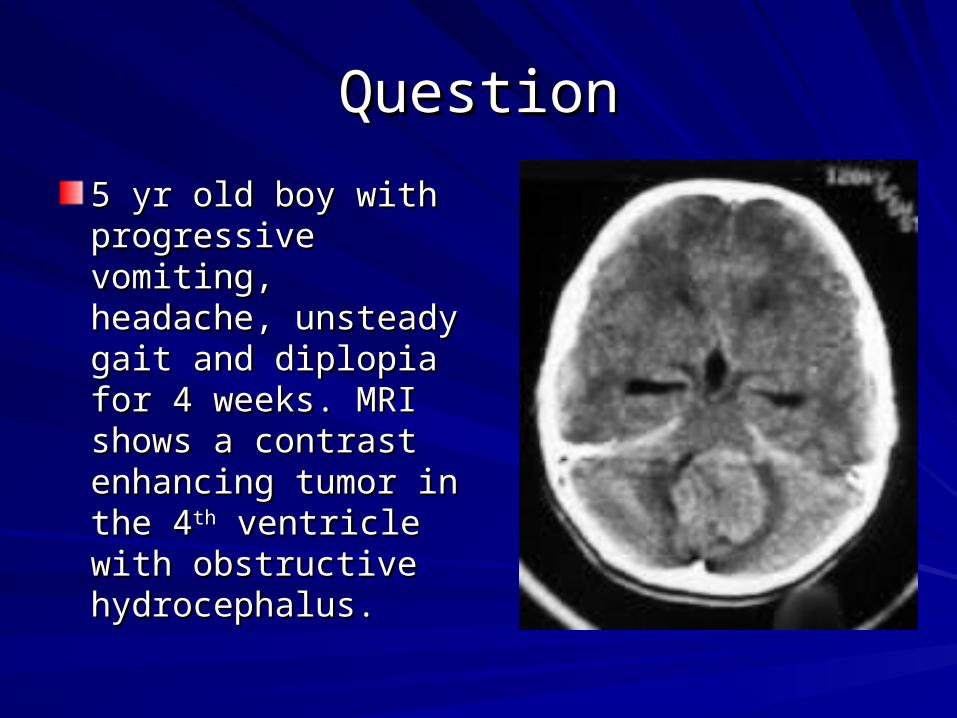
QuestionQuestion
5 yr old boy with 5 yr old boy with progressive vomiting, progressive vomiting, headache, unsteady headache, unsteady gait and diplopia for 4 gait and diplopia for 4 weeks. MRI shows a weeks. MRI shows a contrast enhancing contrast enhancing tumor in the 4tumor in the 4thth ventricle with ventricle with obstructive obstructive hydrocephalus.hydrocephalus.
Brain Tumors- Important to Brain Tumors- Important to knowknow
20% of all malignancies in children20% of all malignancies in childrenAge 3-7 yearsAge 3-7 yearsMost often infratentorialMost often infratentorialSx: Persistent vomiting, headache, gait Sx: Persistent vomiting, headache, gait imbalance, diplopia, ataxia, vision loss, school imbalance, diplopia, ataxia, vision loss, school deterioration, growth decelerationdeterioration, growth decelerationAssociations with Inherited Genetic disorders:Associations with Inherited Genetic disorders:– Neurofibromatosis, Tuberous sclerosis, Von-Neurofibromatosis, Tuberous sclerosis, Von-
Hippel-Lindau disease, Li-Fraumeni (glioma), Hippel-Lindau disease, Li-Fraumeni (glioma), Turcot syndromeTurcot syndrome

MedulloblastomaMedulloblastoma
-- most common CNS tumormost common CNS tumor
– Trt: Resection, Craniospinal RT, ChemoTrt: Resection, Craniospinal RT, Chemo
– Prognosis: Age, large size, degree of Prognosis: Age, large size, degree of resection, dissemination, histology.resection, dissemination, histology.
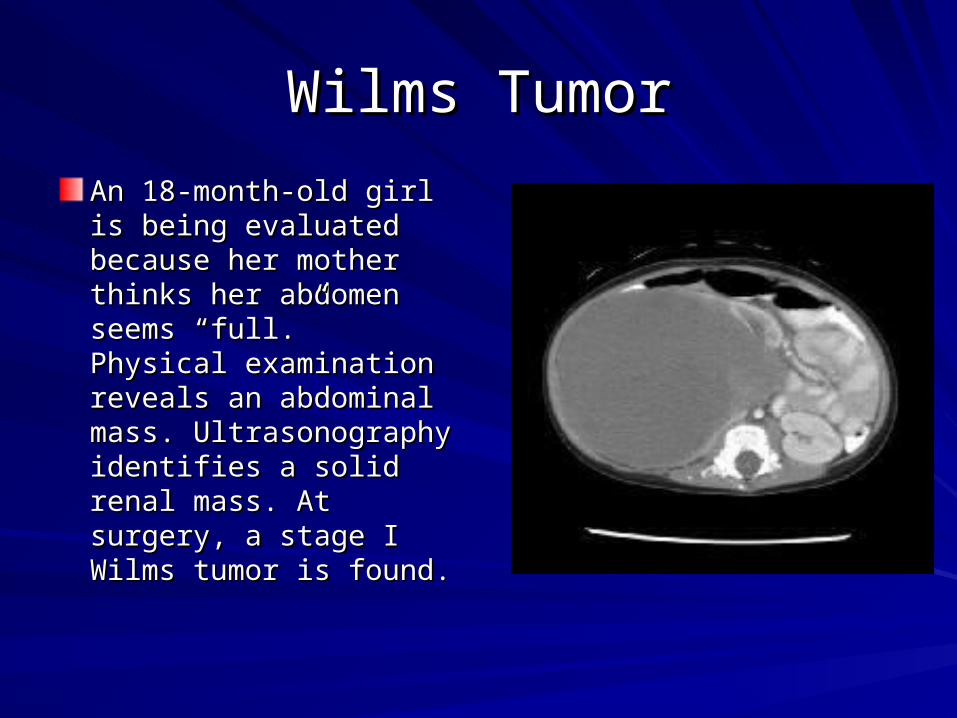
Wilms TumorWilms Tumor
An 18-month-old girl is An 18-month-old girl is being evaluated because being evaluated because her mother thinks her her mother thinks her abdomen seems “full.” abdomen seems “full.” Physical examination Physical examination reveals an abdominal reveals an abdominal mass. Ultrasonography mass. Ultrasonography identifies a solid renal identifies a solid renal mass. At surgery, a stage mass. At surgery, a stage I Wilms tumor is found.I Wilms tumor is found.
Stage I Wilms- Chance of 4-year survival is CLOSEST toStage I Wilms- Chance of 4-year survival is CLOSEST to
1.1. A.A. 30%30%
2.2. B.B. 45%45%
3.3. C.C. 60%60%
4.4. D.D. 75%75%
5.5. E.E. 95%95%
A. 30%
B. 45%
C. 60%
D. 75%
E. 95%
0% 0% 0%0%0%
6
Wilms Tumor- Important Wilms Tumor- Important
Presentation: Presentation: No Sx, HT, Hematuria, MalaiseNo Sx, HT, Hematuria, MalaiseHistologyHistology: favorable(FH) vs unfavorable (UH): favorable(FH) vs unfavorable (UH)StagingStaging: I-local, II-excised, III-residual, IV-: I-local, II-excised, III-residual, IV-metastases, V -bilateralmetastases, V -bilateralTreatmentTreatment: Nephrectomy, Chemo-all, St I-II-2 : Nephrectomy, Chemo-all, St I-II-2 drugs-18 weeks, St III-IV- 3 drugs+ RTdrugs-18 weeks, St III-IV- 3 drugs+ RTPrognosisPrognosis: : – FH: > 90% at 2 yearsFH: > 90% at 2 years– UH: < 60% at 2 yearsUH: < 60% at 2 years
Congenital anomalies associated with Wilms’ tumor Congenital anomalies associated with Wilms’ tumor include all of the following except include all of the following except
1.1. PolydactylyPolydactyly
2.2. AniridiaAniridia3.3. HemihypertrophyHemihypertrophy
4.4. CryptorchidismCryptorchidism5.5. Denys-Drash Denys-Drash
syndromesyndrome
Polydactyly
Aniridia
Hemihypertr
ophy
Crypto
rchidism
Denys-D
rash sy
ndrome
0% 0% 0%0%0%
6
A 9 year old previously healthy girl manifests A 9 year old previously healthy girl manifests progressive painless proptosis and decreased progressive painless proptosis and decreased visual acuity of the left eye during a 2 month visual acuity of the left eye during a 2 month period. The most likely diagnosis is:period. The most likely diagnosis is:
a.a. Pseudotumor of the orbitPseudotumor of the orbit
b.b. TrichinosisTrichinosis
c.c. RetinoblastomaRetinoblastoma
d.d. RhabdomyosarcomaRhabdomyosarcoma
e.e. Orbital cellulitisOrbital cellulitis
RhabdomyosarcomaRhabdomyosarcoma
Painless non tender massPainless non tender mass 60% under age 660% under age 6Sites: head & neck, GU, Extremities, mets lungs.Sites: head & neck, GU, Extremities, mets lungs.Majority sporadic, associations: B-W, Li Fraumeni, NF 1Majority sporadic, associations: B-W, Li Fraumeni, NF 1Types:Types:– Embryonal 70%,Embryonal 70%, better prognosis better prognosis– Alveolar 30 %,Alveolar 30 %, trunk, worse prognosis trunk, worse prognosis
Treatment: Surgery, Chemo, local control RTTreatment: Surgery, Chemo, local control RT
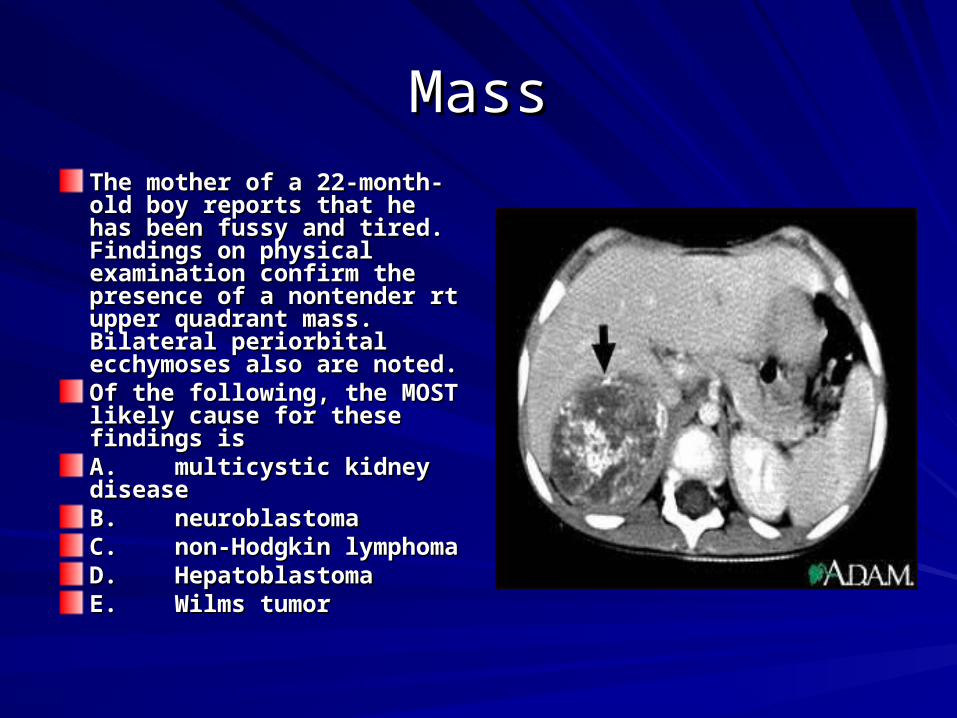
MassMassThe mother of a 22-month-old The mother of a 22-month-old boy reports that he has been boy reports that he has been fussy and tired. Findings on fussy and tired. Findings on physical examination confirm physical examination confirm the presence of a nontender rt the presence of a nontender rt upper quadrant mass. Bilateral upper quadrant mass. Bilateral periorbital ecchymoses also periorbital ecchymoses also are noted.are noted.Of the following, the MOST Of the following, the MOST likely cause for these findings likely cause for these findings isisA.A. multicystic kidney multicystic kidney diseasediseaseB.B. neuroblastomaneuroblastomaC.C. non-Hodgkin non-Hodgkin lymphomalymphomaD.D. HepatoblastomaHepatoblastomaE.E. Wilms tumorWilms tumor

All statements are true about All statements are true about Neuroblastoma except:Neuroblastoma except:
1.1. Most common extra-Most common extra-cranial solid tumorcranial solid tumor
2.2. Prognosis better with N-Prognosis better with N-myc oncogene myc oncogene amplification and tumor amplification and tumor diploidy (DNA index 1)diploidy (DNA index 1)
3.3. Most common cancer in Most common cancer in the first year of lifethe first year of life
4.4. Frequent in <4 years, 97 Frequent in <4 years, 97 % cases by 10 years% cases by 10 years
5.5. Most commonly Most commonly diagnosed as Stage III or diagnosed as Stage III or IVIV
Most
common extra
-crani..
Progn
osis better w
ith N
...
Most
common ca
ncer in
t..
Frequent in
<4 years,
97 ...
Most
commonly
diagnos..
0% 0% 0%0%0%
6
CaseCase
A 16 year old male comes in because he fell in A 16 year old male comes in because he fell in the supermarket.the supermarket.
P/E shows a small painless mass on the medial P/E shows a small painless mass on the medial aspect of the knee.aspect of the knee.
• X ray shows a fracture and a lytic sunburst pattern. X ray shows a fracture and a lytic sunburst pattern. (periosteal elevation)-OS(periosteal elevation)-OS
• Xray shows an onion peel appearance- ESXray shows an onion peel appearance- ES• Xray- radioluscent, sharp, rounded lesion < 2cm with Xray- radioluscent, sharp, rounded lesion < 2cm with
reactive sclerosis- Osteoid Osteomareactive sclerosis- Osteoid Osteoma
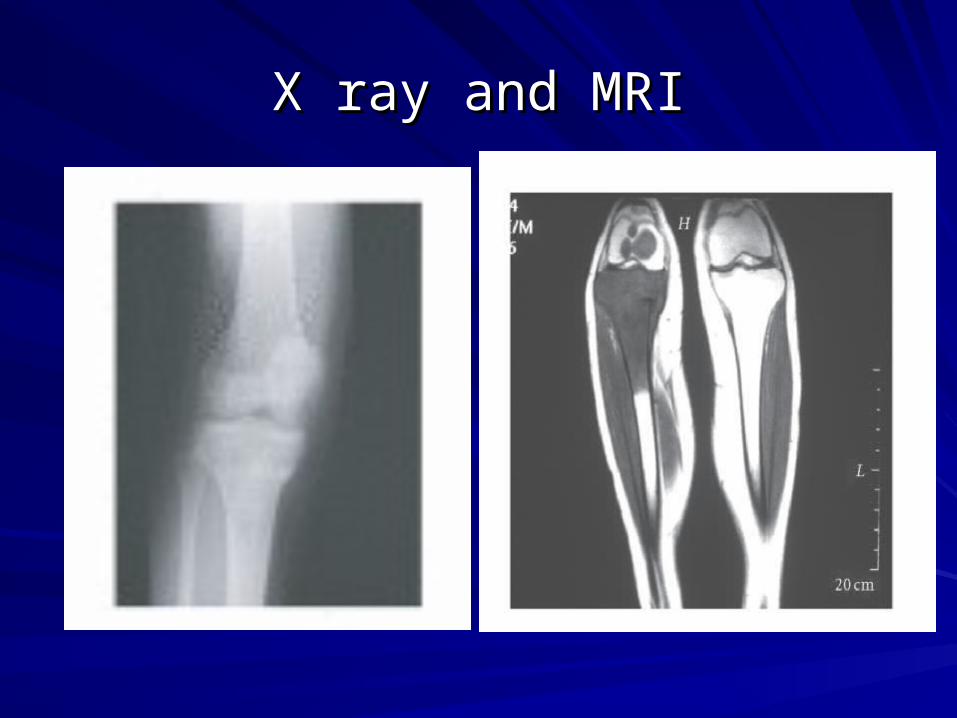
X ray and MRIX ray and MRI
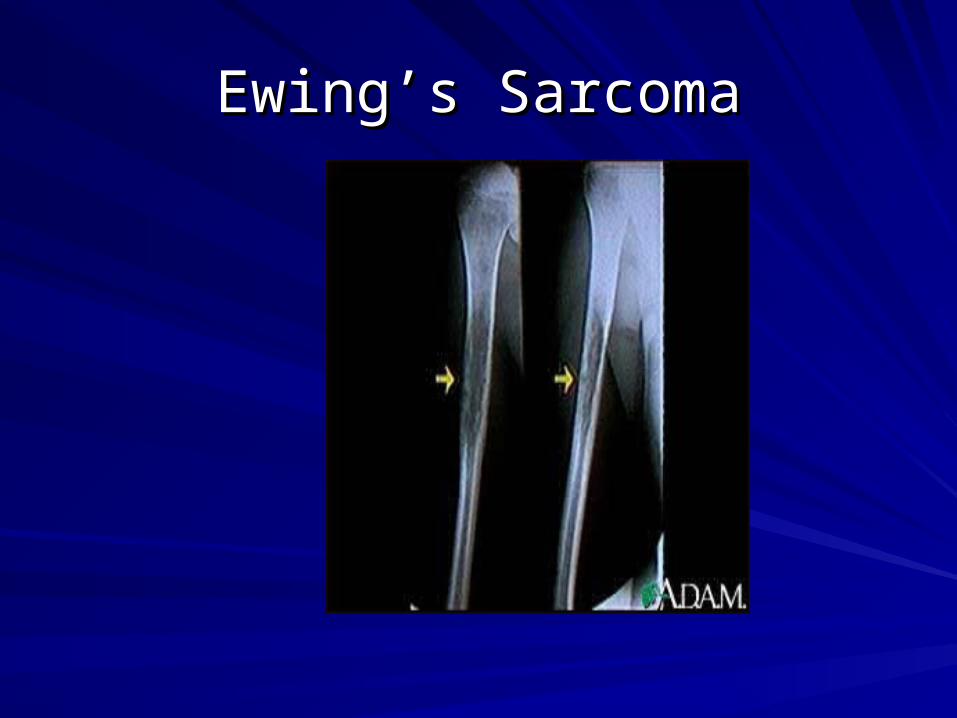
Ewing’s SarcomaEwing’s Sarcoma

Osteogenic SarcomaOsteogenic Sarcoma
MRI, Bone scan, Biopsy, CT Chest for mets. MRI, Bone scan, Biopsy, CT Chest for mets. Peak incidence- 2Peak incidence- 2ndnd decade decadePredisposition: Hereditary retinoblastomas, Li-Predisposition: Hereditary retinoblastomas, Li-Fraumeni, Pagets, RT, Alkylating agentsFraumeni, Pagets, RT, Alkylating agents60 % near the knee (Metaphyses of long bones)60 % near the knee (Metaphyses of long bones)History of fall, pain common symptom, mass, History of fall, pain common symptom, mass, no systemic symptoms.no systemic symptoms.Treatment: Sperm banking, Neo-adjuvant Treatment: Sperm banking, Neo-adjuvant Chemotherapy, limb preserving surgery.Chemotherapy, limb preserving surgery.

A 16 year old Caucasian A 16 year old Caucasian female comes with complaints female comes with complaints of chest pain and difficulty of chest pain and difficulty breathing for the past one breathing for the past one week. She has had fever, wt week. She has had fever, wt loss over the last 2 months. loss over the last 2 months. She has reduced air entry and She has reduced air entry and CXR shows a moth eaten CXR shows a moth eaten appearance of one of the ribs appearance of one of the ribs and a pleural effusion.and a pleural effusion.Biopsy is done and is Biopsy is done and is consistent with Ewing’s consistent with Ewing’s SarcomaSarcoma


Retinoblastoma- need to knowRetinoblastoma- need to know
Presentation: Presentation: Leukocoria (cats eye reflex), dilated pupil, Leukocoria (cats eye reflex), dilated pupil, esotropia, strabismusesotropia, strabismus
Unilateral 75 %Unilateral 75 % (could be hereditary/non) (could be hereditary/non)– 60 %60 % unilateral and unilateral and non hereditarynon hereditary– 15 % unilateral and 15 % unilateral and hereditary (RB1 mutation)hereditary (RB1 mutation)
Bilateral 25 %Bilateral 25 %– 25 % are bilateral and hereditary, 25 % are bilateral and hereditary, have have RB1RB1 mutation mutation– Earlier age, 11mos, Can develop in each eye separatelyEarlier age, 11mos, Can develop in each eye separately– Higher incidence of sarcoma, melanoma, brain tumors.Higher incidence of sarcoma, melanoma, brain tumors.

A child with ALL was started on Chemotherapy. A child with ALL was started on Chemotherapy.
1.1. K high, P high, K high, P high, LDH normal, Na highLDH normal, Na high
2.2. K high, P normal, K high, P normal, LDH high, LDH high, Na nlNa nl
3.3. K normal, P high, K normal, P high, LDH high, Na highLDH high, Na high
4.4. K normal, P normal, K normal, P normal, LDH high, LDH high,
Na normalNa normal5.5. K high, P high, K high, P high,
LDH high, Na normal.LDH high, Na normal.
She had a WBC 82,000, Hb 9gm, plt ct 45,000. She develops tumor lysis syndrome: Which depicts Tumor lysis
K high, P
high, LD
H nor...
K high, P
normal,
LDH h...
K normal, P
high, LD
H h...
K normal, P
normal,
LD...
K high, P
high, LD
H hig..
0% 0% 0%0%0%

Tumor lysis syndromeTumor lysis syndrome
Rapid destruction of cancer cells.Rapid destruction of cancer cells.
Release of intracellular ions, also Uric Release of intracellular ions, also Uric acid, can cause tubular obstruction and acid, can cause tubular obstruction and damage.damage.
Treatment: Allopurinol or Rasburicase Treatment: Allopurinol or Rasburicase early, hydration, alkalinization, diuretic early, hydration, alkalinization, diuretic therapy.therapy.

Spinal cord compressionSpinal cord compression
Presentation: Presentation: back pain worse with movement, neck flexion, back pain worse with movement, neck flexion, straight leg raising, valsalvastraight leg raising, valsalva– Weakness; partial/complete paralysis, IncontinenceWeakness; partial/complete paralysis, Incontinence
Local tumor extension or metastasisLocal tumor extension or metastasisLymphomas, neuroblastoma, soft tissue sarcomasLymphomas, neuroblastoma, soft tissue sarcomasTherapy: Urgent treatment to relieve pressure and Therapy: Urgent treatment to relieve pressure and prevent permanent neurologic damage. prevent permanent neurologic damage. – Neurology/Neurosurgery consultNeurology/Neurosurgery consult– High dose dexamethasoneHigh dose dexamethasone– Emergency radiation therapyEmergency radiation therapy– LaminectomyLaminectomy

Questions on-Superior Vena Cava Questions on-Superior Vena Cava SyndromeSyndrome
Mass lesion obstructs flow through the SVCMass lesion obstructs flow through the SVC
Symptoms Symptoms
-- Dyspnea, edema of face, neck, upper extremitiesDyspnea, edema of face, neck, upper extremities– Periorbital edema, conjunctival edema (itchy eyes)Periorbital edema, conjunctival edema (itchy eyes)– Dysphagia, resp distress, vocal cord paralysisDysphagia, resp distress, vocal cord paralysis
Tracheal compression: resp distress, wheezingTracheal compression: resp distress, wheezing
Due to- NHL, Tcell ALL, Lymphoma,Due to- NHL, Tcell ALL, Lymphoma,
Secondary cause: occluded central venous catheterSecondary cause: occluded central venous catheter

Chemotherapy-Side effectsChemotherapy-Side effects that you need to know that you need to know
Anthracyclines: Cardiac toxicityAnthracyclines: Cardiac toxicityVincristine: foot drop, peripheral neuropathyVincristine: foot drop, peripheral neuropathyCisplatinum: kidney, deafnessCisplatinum: kidney, deafnessMethotrexate, 6MP: Liver toxicityMethotrexate, 6MP: Liver toxicityBleomycin: Pulmonary fibrosisBleomycin: Pulmonary fibrosisAsparaginase: Pancreatitis, CoagulopathyAsparaginase: Pancreatitis, CoagulopathyEtoposide (VP-16): Secondary AMLEtoposide (VP-16): Secondary AMLCyclophosphamaide: Hemorrhagic cystitisCyclophosphamaide: Hemorrhagic cystitis(MESNA as Uroprotector) and Infertility(MESNA as Uroprotector) and Infertility

Fever, NeutropeniaFever, Neutropenia
Single most important risk factor: ANCSingle most important risk factor: ANC
Organisms: Gram negative infection, Organisms: Gram negative infection, Staph epi in catheter patientsStaph epi in catheter patients
Medication: Broad spectrum 3Medication: Broad spectrum 3rdrd generation generation antibioticsantibiotics
Anti-fungal after 4 daysAnti-fungal after 4 days
Examine patient thoroughlyExamine patient thoroughly

16-year-old girl, completed therapy at age 8 for Hodgkins 16-year-old girl, completed therapy at age 8 for Hodgkins disease with Involved field RT and chemo. disease with Involved field RT and chemo.
1.1. AML as a second AML as a second malignancymalignancy
2.2. Disseminated varicellaDisseminated varicella3.3. Drug-induced ITPDrug-induced ITP4.4. Late-onset aplastic anemia Late-onset aplastic anemia
due to chemotherapydue to chemotherapy5.5. Viral-induced ITPViral-induced ITP
She now develops petechiae, purpura, lymphadenopathy and hepatosplenomegaly.Lab include: plt 12,000,Hb 8.0 gm/dL; and WBC 13,000/mm³. She has….
AML a
s a se
cond m
alig...
Disseminate
d varice
lla
Drug-in
duced IT
P
Late-o
nset a
plastic a
ne...
Viral-in
duced IT
P
0% 0% 0%0%0%
6

You are evaluating a 9 year old child for short stature. She You are evaluating a 9 year old child for short stature. She was treated at 3 yrs of age for ALL, received cranial RT. was treated at 3 yrs of age for ALL, received cranial RT.
1.1. Growth hormoneGrowth hormone 2.2. EstradiolEstradiol3.3. Follicle stimulating Follicle stimulating
hormonehormone4.4. Gonadotropin Gonadotropin
releasing hormonereleasing hormone5.5. Thyroid stimulating Thyroid stimulating
hormonehormone
Her height is < 5th percentile and she is Tanner stage I. Most likely to have an abnormal test of
Growth
hormone
Estradiol
Follic
le stimulating hor..
.
Gonadotropin re
leasing..
.
Thyroid sti
mulating ho...
0% 0% 0%0%0%
6

Need to know- Late effects of cancer Need to know- Late effects of cancer therapytherapy
RT:RT: Hypothalamic pituitary axis is impaired; Hypothalamic pituitary axis is impaired;
central hypothyroid and Adrenal insuff.central hypothyroid and Adrenal insuff. RT doses higher in brain tumorRT doses higher in brain tumor GH is dose sensitive to the effects of GH is dose sensitive to the effects of
RT RT Age related: < 5 years susceptibleAge related: < 5 years susceptible Panhypopituitarism with higher dosesPanhypopituitarism with higher doses ovarian failure with RTovarian failure with RT

A 16 year old boy is receiving chemo for A 16 year old boy is receiving chemo for rhabdomyosarcomarhabdomyosarcoma
1.1. Growth hormone Growth hormone deficiencydeficiency
2.2. HypothyroidismHypothyroidism3.3. ImpotenceImpotence4.4. InfertilityInfertility5.5. OsteoporosisOsteoporosis
He recd a year of cycles of Vincristine, Actinimycin-D and Cyclophosphamide. Most likely endocrinologic late effect of this therapy
Growth
hormone deficie
ncy
Hypothyro
idism
Impote
nce
Infertilit
y
Osteoporo
sis
0% 0% 0%0%0%
6

Chemotherapy effectsChemotherapy effects
Chemotherapy with alkylating agents Chemotherapy with alkylating agents Females:Females:
less effects than malesless effects than males
normal pubertynormal puberty
early menopauseearly menopauseMales:Males:
irreversible gonadal toxicityirreversible gonadal toxicity
sterility with azospermiasterility with azospermia
Puberty usually not affected (leydig Puberty usually not affected (leydig cells)cells)

The most common reason for the failure of The most common reason for the failure of hematopoietic stem cell transplantation ishematopoietic stem cell transplantation is
1.1. Veno-occlusive Veno-occlusive disease of the liverdisease of the liver
2.2. Disease recurrenceDisease recurrence3.3. InfectionInfection4.4. Graft vs. host Graft vs. host
diseasedisease5.5. Graft rejectionGraft rejection
Veno-occlusiv
e diseas
e of...
Disease
recu
rrence
Infection
Graft vs.
host dise
ase
Graft re
jection
0% 0% 0%0%0%
6

GVHD ( Graft vs Host disease): All are true GVHD ( Graft vs Host disease): All are true exceptexcept
1.1. It is the reaction of the It is the reaction of the donor lymphocytes donor lymphocytes against the host.against the host.
2.2. Acute GVHD starts within Acute GVHD starts within the first 100 days and the first 100 days and chronic is after 100 days.chronic is after 100 days.
3.3. Affects the skin, liver and Affects the skin, liver and GI tractGI tract
4.4. Irradiation of blood Irradiation of blood products does not helpproducts does not help
5.5. Complete HLA matching Complete HLA matching prevents GVHDprevents GVHD
It is t
he reacti
on of the ...
Acute
GVHD start
s with
in...
Affects th
e skin, li
ver and ..
Irradiation of b
lood prod...
Complete HLA
match
ing ...
0% 0% 0%0%0%
6