patients are more knowledgeable than...
TRANSCRIPT

1
Daniel H Ward DDS
Uncommon,Common Sense:
What YOU need to know NOW about Restorative Dentistry and Materials
Daniel H Ward DDS
Graduated 1979 OSU
Private Practice‐Columbus, Ohio
Assistant Clinical Professor The Ohio State University‐1996‐2009
Daniel H Ward DDS
Reviewer‐Journal of Prosthetic Dentistry
Reviewer‐Journal of Esthetic and Restorative Dentistry
Member and Evaluator for Catapult
Lecturer and Chief Examiner University of Minnesota Post‐Graduate Program in Esthetic Dentistry‐20 years
“I get by with a little help from my friends…”Dr Harry Albers
Dr Paul Belvedere
Dr John Burgess
Dr Mark Canon
Dr Gordon Christensen
Dr George Freedman
Dr Galip Gürel
Dr Geoff Knight
Dr Doug Lambert
Dr Karl Leinfelder
Dr Graeme Milicich
Dr Buddy Mopper
Dr Jeff Morley
Dr Brian Novy
Dr Jorge Perdagão
Dr Steve Rosenstiel
Dr Robert Seghi
Dr Irwin Smigel
Dr Byong Suh
Dr Ed Swift
Companies I Work With
AdDent
BISCO
Caulk/Dentsply
Centrix
Clinicians’ Choice
Coltene/Whaledent
GC America
Heraeus Kulzer
Ivoclar
Kerr
Pulpdent
Shofu
SDI
SSWhite
Tokuyama
Triodent
3‐M
VOCO
Patients are more knowledgeable than ever

2
We must listen more to our patients
We must provide alternatives for our patients
…but the rightalternatives
Composite
The most USED
and ABUSED
Material in Dentistry
Composite
Uncommon, common sense
•What is the most important restoration that determines the long term prognosis of a tooth?
•Are flowable composites always an inferior restoration?
•Does fluoride present within the enamel of an un-prepared tooth margin result in a better bond between resin and tooth?

3
Uncommon, common sense
•Does the addition of fluoride to a resin result in efficacious fluoride release?
•Should preparations for tooth to be restored with a composite be the same as for a tooth to be restored with amalgam?
•What is the effect of warming composite immediately prior to placement?
Decay Removal
Composite Direct Placement Challenges
Thoroughly remove decay only
Amalgam Preparation
Composite Preparation
“Convenience”Form MID Lifetime of tooth often determined by first dentist
intervention
15 Year Old
Fissurotomy bur
201.3VF
Conservative Tooth Preparation
169L330
Low Viscosity Flowable Composite
How do you restore?

4
Low Viscosity Flowable Composite
G-aenial Universal Flo
Homogeneous spherical particles
Better wear resistance
Higher flexural strength (167 MPa)
Filled 50% by volume
Good polishability
Visibly blends in well Mean particle size 200 nm
Low Viscosity Flowable Composite
Beautifil Flow 00
Unique glass ionomer filler particles
Releases fluoride and other ions
Neutralizes pH-Antibacterial
Reduced plaque accumulation
Good polishability
Visibly blends in well S-PRG (Surface pre-treated Glass Ionomer)
Intra-oral plaque formation(24 hours W/O Brushing)
Less plaque Full-grown plaque
BEAUTIFIL Ⅱ(Containing S-PRG filler)
Conventional Restorative Material
(Not containing S-PRG filler)
plaque
S PRG FillersSignificantly reduced plaque accumulation
Dispenser Gun
Tray
Compule Tray
Warmer
CALSETThermal Assisted Light Polymerization
WARMER
Improved flowability of composites
Improved marginal adaptation
Improved rate of polymer conversion
Improved surface hardness/durability/polishing.
Decreased curing time and increased depth of cure
Increased sculptability and ease in shaping anatomy
ADVANTAGESADVANTAGESThermal Assisted Light PolymerizationThermal Assisted Light Polymerization
Stansbury JW. Use of near-IR to monitor the influence of external heating on dental composite photopolymerization. Dent Mat 2004; 20(8).
Dispenser Gun TrayComax Dispenser
CALSETCALSETThermal Assisted Light PolymerizationThermal Assisted Light Polymerization
5
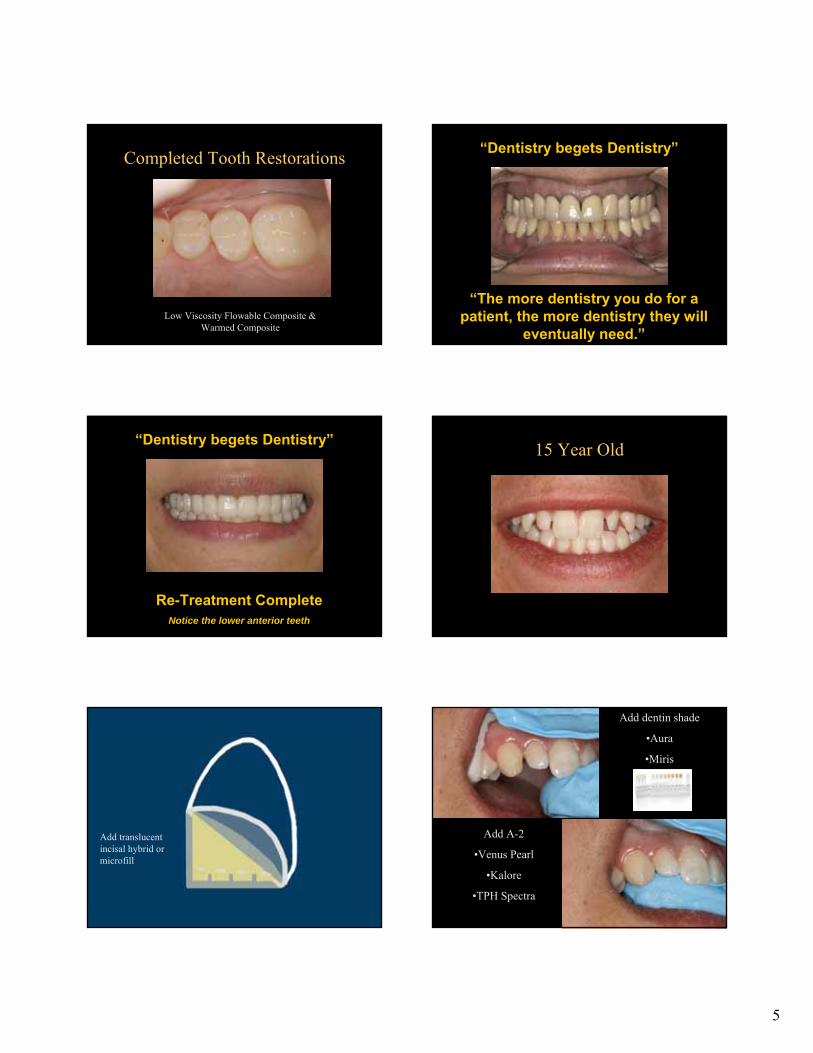
Low Viscosity Flowable Composite & Warmed Composite
Completed Tooth Restorations“Dentistry begets Dentistry”
“The more dentistry you do for a patient, the more dentistry they will
eventually need.”
“Dentistry begets Dentistry”
Re-Treatment CompleteNotice the lower anterior teeth
15 Year Old
Buildup dentin replacement with opaque darker hybrid –typically A3-A3.5
Buildup remaining form with shade similar to desired final color with hybrid (typically A1-A2)
Add special effects to simulate imperfections within tooth structure
Add translucent incisal hybrid or microfill
Add dentin shade
•Aura
•Miris
Add A-2
•Venus Pearl
•Kalore
•TPH Spectra

6
Add A-1
Add Characterization
Important-Junction must be invisible
Add Facial Surface
•Beautifil II
•Aura Enamel
•Kalore GT
•Esthelite Sigma QuickOptrasculpt
Finish and polish restoration
Restore adjacent tooth
Shape, finish and polish restorations
Restore opposite teeth
Pre-Operative
Finished Restorations
Post-Operative Sensitivity
Composite Direct Placement Challenges
Hydrodynamic Theory
Hydrodynamic Theory
Fluid flow within dentinal tubules causes PAINBrannstrom M. The Cause of post restorative sensitivity and its prevention. J Endod 1986;12:475-481.
Hydrodynamic Theory
Opened, unsealed dentinal tubules causes PAIN
SEM Dr Jorge Perdagão

7
DentinDentin
SEM Dr Jorge Perdagão
Dentin Bonding
70% inorganic carbonate hydroxyapatite 70% inorganic carbonate hydroxyapatite calcium phosphatecalcium phosphate
30% organic (collagen) and water30% organic (collagen) and water
Dentinal tubules 0.06Dentinal tubules 0.06--3 microns in diameter3 microns in diameter
Most Bonding occurs between dentinal tubulesMost Bonding occurs between dentinal tubules
HydrophilicHydrophilic
Oh NO, not another bonding lecture!
•What are MMP’s and what agents can affect their effects?
•What is the effect of the width of the hybrid layer and dentin bond strengths?
•What new Self-Etching Primer Dentin Bonding Agent has bond strengths to un-etched enamel greater than 40 MPa ?
Oh NO, not another bonding lecture!
•Is there a relationship between post-operative sensitivity and dentin bond strengths?
•What are the characteristics of alcohol, acetone and water based solvents of dentin bonding agents?
•What are Universal Dentin Bonding Agents?
Etched Dentin
SEM Dr Jorge Perdagão
Demineralize surfaceExpose collagen fibersRemove smear layer Increase porosity of intertubular dentinOpen up dentinal tubules Increase surface area
Etched Dentin
8
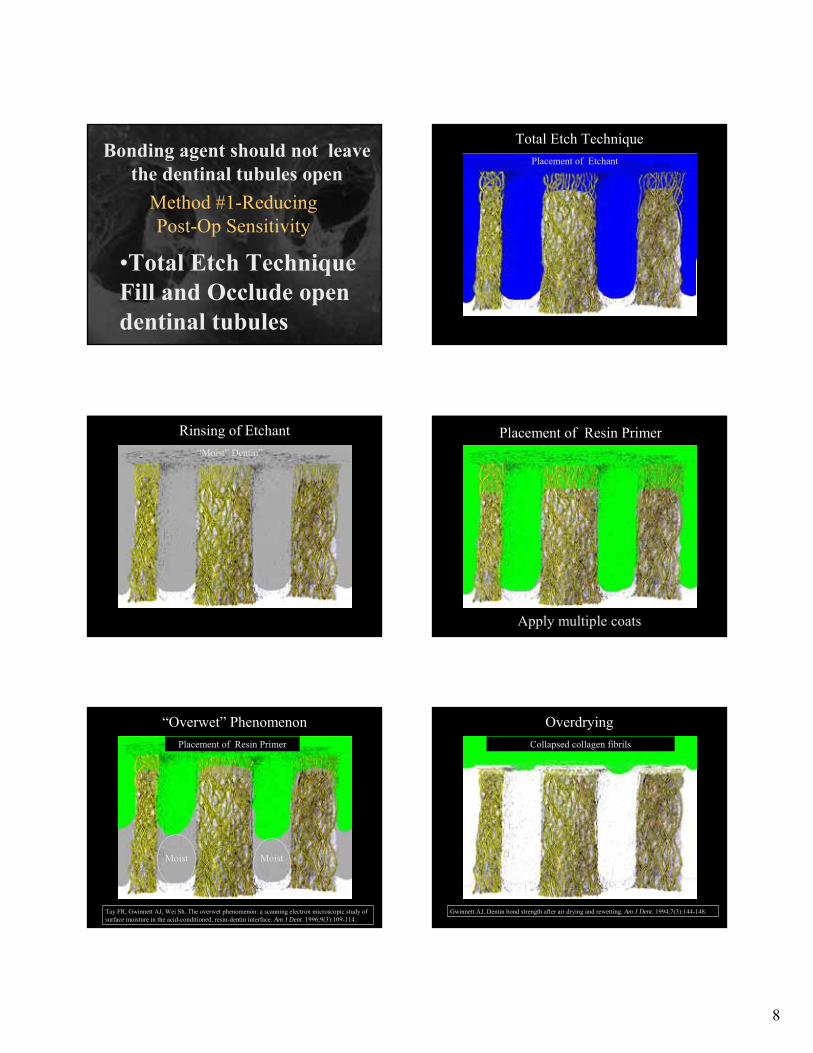
•Total Etch Technique Fill and Occlude open dentinal tubules
Bonding agent should not leave the dentinal tubules open
Method #1-Reducing Post-Op Sensitivity
Placement of Etchant
Total Etch Technique
“Moist” Dentin”
Rinsing of Etchant Placement of Resin Primer
Apply multiple coats
Moist Moist
Placement of Resin Primer
“Overwet” Phenomenon
Tay FR, Gwinnett AJ, Wei Sh. The overwet phenomenon: a scanning electron microscopic study of surface moisture in the acid-conditioned, resin-dentin interface. Am J Dent. 1996;9(3):109-114.
Overdrying
Gwinnett AJ. Dentin bond strength after air drying and rewetting. Am J Dent. 1994;7(3):144-148.
Collapsed collagen fibrils

9
Overdrying
SEM Perdigao
Un-collapsed collagen fibrils Collapsed collagen fibrils
Proper Moisture
Moisture Variability
Acetone
Alcohol
Water
Bonding Agent Solvents
Air only syringe Warm air dryer
Air/water syringe Air/water syringe
Evaporating the solvent with dry air
Bond StrengthSensitivity
Variability

10
Lopez CL, Perdigao J, Lopes M et al. Dentin Bond Strengths of Simplified Adhesives:Effect of Dentin Depth. Compendium. 2006;27(6):340-345.
17.6(+/-5.9)
18.4(+/-4.8)
14.2(+/-7.0)
Deep
Dentin
21.0(+/-7.4)
18.9(+/-4.1)
22.1(+/-2.8)
Superficial
Dentin
Clearfil
Liner
Bond
Optibond
Solo
Single Bond
Adhesive
System
Mean shear bond strength in MPa
Effect of Dentin Depth on Bond Strengths
•Occludes tubules
•Anti-bacterial
GLUMA
•Occlusions
Total Etch Technique
Summary
Most technique sensitiveRequires proper attention to detailUse in ideal sized preparations
Total Etch Technique
Materials-4th
Generation
Acetone solvent Alcohol solvent
Total Etch Technique
Materials-5th
Generation
Acetone solvent Alcohol solvent

11
•Self Etch Technique Never leave the dentinal tubules open
Bonding agent should not leave the dentinal tubules open
Method #2-Reducing Post-Op Sensitivity
Acid-groupsHydrophilic end
etches tooth structure (self
limiting)
Spacer-chainlink between
functional groups
Methacrylate-groupHydrophobic end
connects to polymer-network
COOH
COOH
CH 2
CH 2
O
OO
O
Self-Etching Primer
“Self Etching” PrimerAcidifying Primer accompanies etch
Acid reaction is self-limiting Lohbauer U, Nikolaenko SA, Petschelt A, Frankenberger R.. Resin Tags do not contribute to dentin adhesion in self-etching adhesives. J Adhes Dent. 2008;10(2):97-103 .
Resin Tags do not Contribute to Dentin Adhesion in SE Adhesion
Self-Etch Technique
Challenges
Decreased bond strength to un-etched enamel
Marginal gap formation with un-etched enamel
Bond incompatibility to self-cure and dual-cure resins
More susceptible to hydrolytic degradation resulting in significantly diminished bond strengths over time
Self etching Primer
12
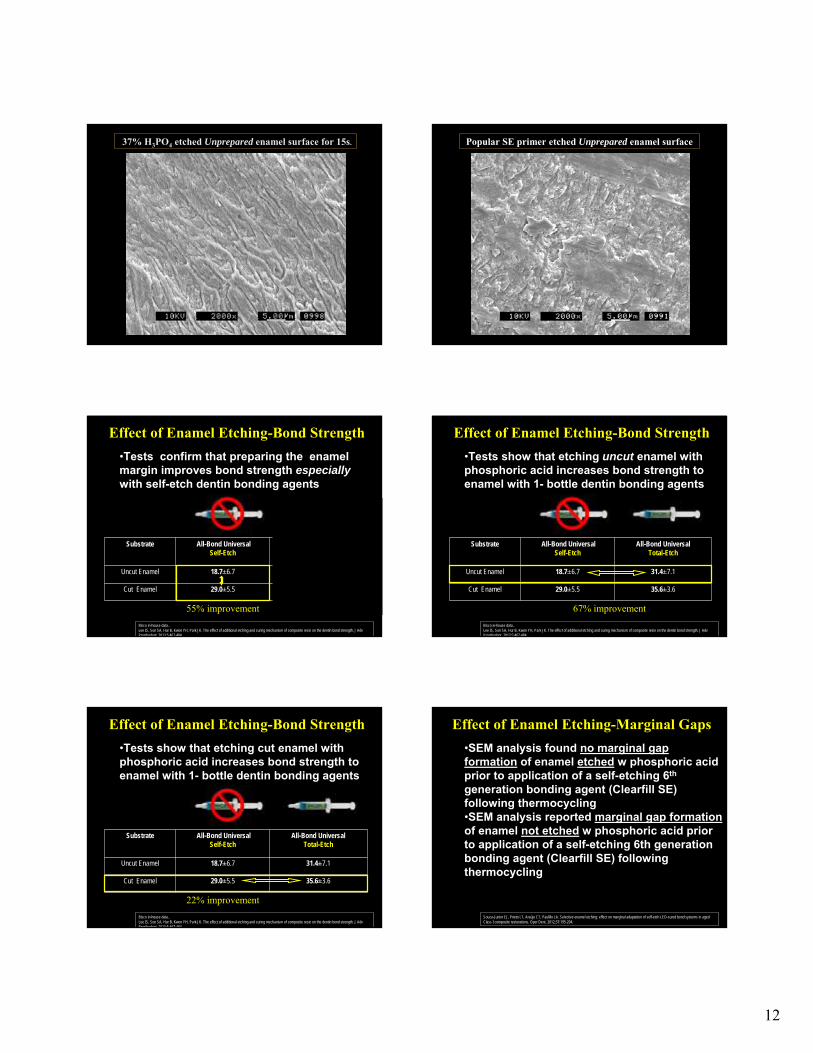
37% H3PO4 etched Unprepared enamel surface for 15s. Popular SE primer etched Unprepared enamel surface
•Tests confirm that preparing the enamel margin improves bond strength especially with self-etch dentin bonding agents
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
55% improvement
Effect of Enamel Etching-Bond Strength
•Tests show that etching uncut enamel with phosphoric acid increases bond strength to enamel with 1- bottle dentin bonding agents
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
67% improvement
Effect of Enamel Etching-Bond Strength
Substrate All-Bond UniversalSelf-Etch
All-Bond UniversalTotal-Etch
Uncut Enamel 18.7±6.7 31.4±7.1
Cut Enamel 29.0±5.5 35.6±3.6
Bisco in-house data.. Lee IS, Son SA, Hur B, Kwon YH, Park JK. The effect of additional etching and curing mechanism of composite resin on the dentin bond strength. J Adv Prosthodont. 2013;5:467-484.
22% improvement
Effect of Enamel Etching-Bond Strength
•Tests show that etching cut enamel with phosphoric acid increases bond strength to enamel with 1- bottle dentin bonding agents
•SEM analysis found no marginal gapformation of enamel etched w phosphoric acid prior to application of a self-etching 6th
generation bonding agent (Clearfill SE) following thermocycling•SEM analysis reported marginal gap formationof enamel not etched w phosphoric acid prior to application of a self-etching 6th generation bonding agent (Clearfill SE) following thermocycling
Souza-Junior EJ, Prieto LT, Araújo CT, Paulillo LA. Selective enamel etching: effect on marginal adaptation of self-etch LED-cured bond systems in aged Class I composite restorations. Oper Dent. 2012;37:195-204.
Effect of Enamel Etching-Marginal Gaps

13
Solution: “Etching prepared enamel w phosphoric acid promoted better marginal integrity with self-etching bonding agents.”
Souza-Junior EJ, Prieto LT, Araújo CT, Paulillo LA. Selective enamel etching: effect on marginal adaptation of self-etch LED-cured bond systems in aged Class I composite restorations. Oper Dent. 2012;37:195-204.
Effect of Enamel Etching-Marginal Gaps
When the pH of a dentin bonding agent is too low (more acidic), tertiary amines (necessary for the polymerization reaction) are deactivated resulting in bond incompatibility with self and dual cured resins.
Bond Incompatibility with Self and Dual Cured Resins
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual -cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Solution: Use of a higher pH (>3.0)self-etching dentin bonding agent does not inactivate the tertiary amines and allows for polymerization.
Suh BI, Feng L, Pashley DH, Tay FR. Factors contributing to the incompatibility between simplified-step adhesives and chemically-cured or dual -cured composites. Part III. Effect of acidic resin monomers. J Adhes Dent 2003;5:267-282.
Bond Incompatibility with Self and Dual Cured Resins
pH=3.2
Solution: Use a dual-cure activator
Bond Incompatibility with Self and Dual Cured Resins
“The cured layer of 1-step self-etching adhesives is hydrophilic and a permeable membrane.”
Tay F, Suh B, Pahsley D, Carvalho R. Single Layer Adhesives are Permeable membranes. J Dent 2002;30:371-382.
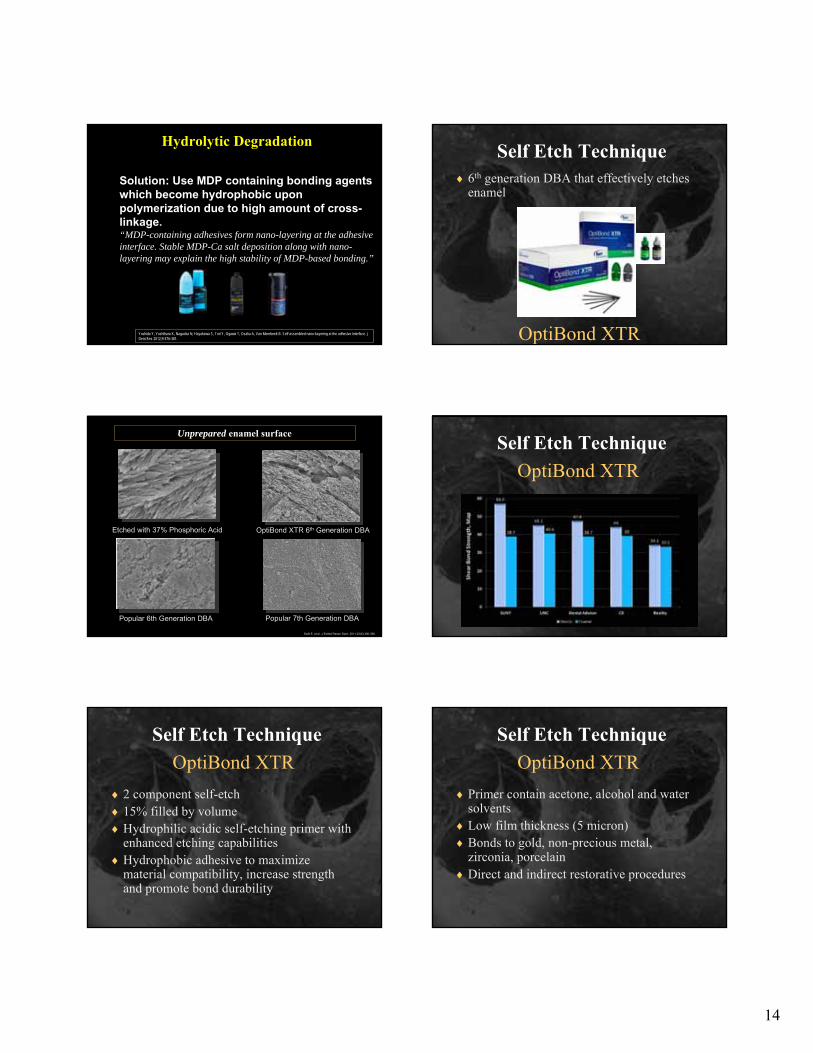
Hydrolytic Degradation
Solution: Use 2 layers-a hydrophilic layer covered with a hydrophobic layer
Yoshida Y, Yoshihara K, Nagaoka N, Hayakawa S, Tori Y, Ogawa T, Osaka A, Van Meerbeek B. Self-assembled nano-kayering at the adhesive interface. J Dent Res 2012;9:376-381.
Hydrolytic Degradation
14
Solution: Use MDP containing bonding agents which become hydrophobic upon polymerization due to high amount of cross-linkage.“MDP-containing adhesives form nano-layering at the adhesive interface. Stable MDP-Ca salt deposition along with nano-layering may explain the high stability of MDP-based bonding.”
Yoshida Y, Yoshihara K, Nagaoka N, Hayakawa S, Tori Y, Ogawa T, Osaka A, Van Meerbeek B. Self-assembled nano-kayering at the adhesive interface. J Dent Res 2012;9:376-381.
Hydrolytic DegradationSelf Etch Technique
OptiBond XTR
6th generation DBA that effectively etches enamel
Unprepared enamel surface
Etched with 37% Phosphoric Acid OptiBond XTR 6th Generation DBA
Popular 6th Generation DBA Popular 7th Generation DBA
Swift E, et al. J Esthet Restor Dent. 2011;23(6):390-398.
Self Etch Technique
OptiBond XTR
Self Etch Technique
OptiBond XTR
2 component self-etch 15% filled by volumeHydrophilic acidic self-etching primer with
enhanced etching capabilitiesHydrophobic adhesive to maximize
material compatibility, increase strength and promote bond durability
Self Etch Technique
OptiBond XTR
Primer contain acetone, alcohol and water solvents
Low film thickness (5 micron)Bonds to gold, non-precious metal,
zirconia, porcelain Direct and indirect restorative procedures

15
Seventh Generation DBA
BeautibondDual acidic monomersLow film thickness (5 micron)RadiopaqueEasy to use-single application 10 sec
Self Etch Technique
Materials 6th & 7th
Generation
Sixth Generation Seventh Generation
All-Bond SE Clearfil SE Protect
BeautiBond G-BondOptibondXTR
Long Term Dentin Bond StabilityMMP-Matrix MetalloproteasesMMPs are naturally occurring proteases
involved in dentin formation and trapped during odontogenesis
Not bacteria but proteolytic enzymes found within dentin capable of degrading collagen within newly created adhesive hybrid layers
Low pH causes dentin to release these inherent MMPs which attack exposed collagen fibrils
Osorio R, Yamauti M. Osorio E., et al. Effect of dentin etching on metalloproteinase-mediated collagen degradation. Eur J Oral Sci 2011;119:79-85.
Long Term Dentin Bond StabilityCysteine Proteases (Cathepsins)
Lysosomal enzymes that become activated in lysosomes by a low pH
Secreted by osteoclasts in bone resorption
Regulated by chondroitin
Collagenase activity breaks down collagen and hydrolyzes collagen into small peptides
Terasariol Il, Geraldeli S., ,Minciotti Cl., et al., Cysteine catepsins in human dentin pulp complex. J Dent Res 2011; 90:506-11.
MMP-Matrix Metalloproteases
Carrilho et al., JDR 2007; 86; 529Brackett et al.,Operative Dentistry; 2009;34(4):381-385
In-vivo 12 m w/PBNT (Acetone)
Immediate (MPa)Control 29.3 (9.2)CHX 32.7 (7.6)
w/CHX in 12 m
14 mo (MPa)Control 19.0 (5.2)CHX 32.2 (7.2)
Potential MMP Inhibitors
Long Term Dentin Bond Stability
Chlorhexidine (CHX)
Benzalkonium Chloride
MDPB ((12-methacryloxydodecalpyridinium bromide)
Galardin (mimics MMP-binds Zn atom) (inhibits tumor growth and metastasis)
Epigallocatechin-3-gallate (green tea polyphenol)
Perdigao J, Resi A, Loguercio AD. Dentin Adhesion and MMPs: A Comprehensive Review. J Esthet Restor Dent 2012: 25:219-241.

16
Disinfect to prevent MMPs
Use Etchant containing 1% Benzalkonium Chloride
TE-Apply 2% Chlorhexidine after acid etching for 30 sec
SE-Apply 2 coats 2% Chlorhexidine prior to application of primer
OR
Long Term Dentin Bond Stability
Disinfect to prevent MMPs
MDPB (12-methacryloxydodecalpyridinium bromide)
Long Term Dentin Bond Stability
Pashley DH, Tay FR, Imazato S. Hot to Increase the durability of Resin-Dentin Bonds. Compend. 2010;32(7):60-64.
Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R, De Stefano Dorigo E. Dental adhesion review: aging and stability of the bonded interface. Dent Mater. 2008 Jan;24(1):90-101.
Most simplified one-step adhesives were shown to be the least durable, while three-step etch-and-rinse and two-step self-etch adhesives continue to show the highest performances, as reportedin the overwhelming majority of studies. In other words, a simplification of clinical application procedures is done to thedetriment of bonding efficacy. Among the different aging phenomena occurring at the dentin bonded interfaces, some are considered pivotal in degrading the hybrid layer, particularly if simplified adhesives are used. Insufficient resin impregnation of dentin, high permeability of the bonded interface, sub-optimal polymerization, phase separation and activation of endogenous collagenolytic enzymes are some of the recently reported factorsthat reduce the longevity of the bonded interface.
Dentin Bonding Challenges
Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R, De Stefano Dorigo E. Dental adhesion review: aging and stability of the bonded interface. Dent Mater. 2008 Jan;24(1):90-101.
In order to overcome these problems, recent studies indicated that (1) resin impregnation techniques should be improved, particularly for two-step etch-and-rinse adhesives; (2) the use of conventional multi-step adhesives is recommended, since they involve the use of a hydrophobic coating of nonsolvated resin; (3) extended curing time should be considered to reduce permeability and allow a better polymerization of the adhesive film; (4) proteases inhibitors as additional primer should be used to increase the stability of the collagens fibrils within the hybrid layer inhibiting the intrinsic collagenolytic activity of human dentin.
Dentin Bonding Solutions
• SE 1-step adhesives are too hydrophilic and permeable even after polymerization
• The best way to minimize these weaknesses is to apply a neutral-pH, hydrophobic adhesive resin layer in a separate step
• Acidic components cause incompatibility with self-cured composites.
• 3-step, etch-and-rinse adhesives remain the “gold standard” in terms of adhesive durability.
Dentin Bonding Solutions
De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Broem M, Van Meerbeek B. A Critical Review of the Durability of Adhesion to Tooth Tissue: Methods and Results. J Dent Res. 2005;84(2):118-132.
Selective Etch TechniqueApply etch to enamel only for 15 secondsWash thoroughlyPlace self-etching primer
Frankerger R, Lohbauer U, Roggendorf MJ, Naumann M, Taschner M. Selective enamel etching reconsidered:better than etch-and-rinse and self etch? J. Adhes Dent. 2008;10:339-344.

17
Selective Etch TechniqueHigh Viscosity allows precise placementContains BAC
Selective Etch TechniqueAllows total etch or self etch of enamel
and/or dentin
G-aenial Bond
Selective Etch TechniquePrecursor to “Universal” Bonding agentsBond strength same to total vs self etch
Dentin Bond Strength
Self-Etch Total Etch Moist
Total Etch Wet
Total, Self or Selective Etch Universal Bonding
Materials
Total-etch, self-etch or selective-etch technique
Can be used for direct and indirect restorations
Bond to all indirect substrates-metal, ceramics, zirconia, porcelain and lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements.
Universal Bonding Materials
Total, Self or Selective Etch All-Bond UniversalTotal-etch, self-etch or selective-etch
Single bottle for direct and indirectrestorations
High bond strengths to metal, ceramics, zirconia, porcelain & lithium disilicate.
Compatible with light-cured, self-cured and dual-cured composite and luting cements since pH is 3.2
Becomes hydrophobic upon setting
Total, Self or Selective Etch

18
Total Etch vs. Self EtchShear bond strength of Universal Adhesives on Tooth Structures MPa*
*Manufacturer supplied data
Universal Bonding Materials
Total, Self or Selective Etch
Universal Bonding Materials
Total, Self or Selective Etch Universal Bonding
Materials
Total, Self or Selective Etch
Light Cured Dual Cured
•Total Etch Technique Never open the dentinal tubules
Bonding agent should not leave the dentinal tubules open
Method #3-Reducing Post-Op Sensitivity
Resin-Modified Glass Ionomer

19
RMGI Liner
No dentin conditionerneeded due to self-etch
primer component
RMGI BaseReprepare
Dentin conditionerpreferred to achieve optional dentin bond
10. It’s not necessary
9. It takes more time
8. It costs more money
7. I don’t understand which product to use
6. Not necessary with today’s Hundredth generation bonding agents
TOP TEN REASONS:GI isn’t used under every restoration
5. I don’t know how to use
4. Not as strong: I “bond” everything-holding tooth together and making it stronger
3. It doesn’t bond as well to dentin as resin
2. Fluoride release is transient
1. Old fashioned: used before better bonding agents were available
TOP TEN REASONS:GI isn’t used under every restoration
••Make initial access opening w small burMake initial access opening w small bur
••Use slow speed to remove decayUse slow speed to remove decay
Clinical Class I Restoration
••Use high speed to refine preparationUse high speed to refine preparation
••Smooth margins with a football diamond.Smooth margins with a football diamond.
Clinical Class I Restoration

20
Clinical Class I Restoration
••Completed PreparationsCompleted Preparations
Clinical Class I Restoration
••Glass ionomer base/linerGlass ionomer base/liner
••Etch enamel then dentin, wash and dryEtch enamel then dentin, wash and dry
Clinical Class I Restoration
••Place & scrub multiple coats bonding Place & scrub multiple coats bonding agent, wait, evaporate solvent and cureagent, wait, evaporate solvent and cure
••Place composite and adapt to sidesPlace composite and adapt to sides
Ivoclar P-1
•Cure thoroughly
Clinical Class I Restoration
Posterior Finishing Burs
Occlusal Anatomy OcclusalSecondary Anatomy
Buccal/ lingual gingival-IP
12 fluted carbide burs
ProcedureProcedure Trim and shape composite
Adjust occlusion
Blend margin between tooth and composite
Define secondary anatomy
Restore occlusal fissures
Restore buccal/ lingual contour
Reduce and smooth composite surface
Interproximal shaping at gingiva and above contact
Popular InstrumentsPopular Instruments Football or egg-shaped
7406
H379
15106-5
Flame-shape
H-274
5379-5
Needle shape
Safe-end SE6
7901
15121-5
Ivoclar
Astropol
SS White
Jazz
Caulk Enhance/POGO
••Blend margins with finishing carbidesBlend margins with finishing carbides
••Adjust occlusionAdjust occlusion
••Finish and polishFinish and polish

21
••No metal in the centerNo metal in the center
••Very FlexibleVery Flexible--now more durablenow more durable
••Double SidedDouble Sided
••Available in Unit Dose Available in Unit Dose ••Etch, wash/dry and apply surface sealantEtch, wash/dry and apply surface sealant
Clinical Class I Restoration
Summary
Best reduction of post-operative sensitivity
Insurance of fluoride releaseBest bond to enamelLong term stable bond to dentinUse in majority of posterior preparations
Total Etch with RMGI Liner/Base
•What’s new in composite technology?
•What’s all the buzz about bulk fill composites?
•To achieve good Class II interproximal contacts with composite, you just use the same armementarium as amalgam?
““Fill meFill me”” in on the latest in Direct in on the latest in Direct Restoratives!Restoratives!
New Filler TechnologyNew Filler TechnologyGiomer FillersGiomer Fillers
Unique Filler particles made of set glass ionomer with special surface coating
Set Glass Ionomer Material Surface Modified Pre-Reactive Glass Ionomer Filler
Surface modified layer
Glass Ionomer phase
Glass Core
New Filler TechnologyNew Filler TechnologyGiomer FillersGiomer Fillers
BeautiSealant BeautiBond
Beautifil IIBeautifil Flow Plus

22
16 of 26 Class I, and 25 of 35 Class II restorations were observed.No failures
No secondary caries
Alpha or Bravo aesthetics
No post-op sensitivity noted
Gordan VV, Mondragon E, Watson RE, Garvan C, Mjör IA. A clinical evaluation of a self-etching primer and a giomer restorative material: results at eight years. J Am Dent Assoc. 2007;138(5):621-7
GiomerGiomer TechnologyTechnology8 Year Results8 Year Results
19 of 26 Class I, and 22 of 35 restorations were observed.Retention rate 66% (27 of 41)
– 52% of retained noted as excellent – 41% of retained noted minor changes
Secondary caries rate 3.27% (2 of 61) Overall positive results and low secondary caries attributable to Giomer technology
Gordan VV, Blaser PK, Mjor IA, Sensi L, Watson R, McEdward DL, Riley III J. Clinical Evaluation of a GiomerRestorative System: Thirteen-Year Recall 2013 IADR #3104:University of Florida
GiomerGiomer TechnologyTechnology13 Year Results13 Year Results
Agl MicrofillAgl MicrofillHeliomolarHeliomolar
MicroMicro--HybridHybridMiris, Point4, Miris, Point4, EsthetX, Venus EsthetX, Venus
NanoclusterNanoclusterFiltek SupremeFiltek Supreme
NanoNano--HybridHybridVenus Diamond, Venus Diamond, Tetric EvoTetric Evo--Ceram, Ceram, Kalore, Esthelite QKalore, Esthelite Q
New Filler TechnologyNew Filler TechnologyLow Shrinkage CompositesLow Shrinkage Composites
Nano/Hybrids in green
Open Margin Cracked Enamel
(white line)
Effects of polymerization shrinkage STRESS
Fractured Cusp
Prepolymerized Filler
Average Size 17 µm400 nm Strontium Glass
100 nm Lanthanoid fluoride
Glass Fillers
700 nm Strontium Glass700 nm Fluoroaluminum Silicate Glass
Non-aggregated nano silica filler
16 nm Silica filler
KaloreKalore
New Filler TechnologyNew Filler TechnologyNanofill/HybridNanofill/Hybrid

23
New Filler TechnologyNew Filler TechnologySpheroidal FillersSpheroidal Fillers
Easy polishing and retention
Blends well into tooth structure
Esthelite Sigma Quick-1 layer
Omega-2-3 layers
Estelite Sigma Quick
1μm
New Filler TechnologyNew Filler TechnologySpheroidal FillersSpheroidal Fillers
1μm
Estelite Sigma Quick
4 Seasons
Venus
Filtek Supreme Premise
Nano Clusters
(5,000 Magnification)
Tetric Evo-Ceram
1μm
DX-511
MW 895
BIS-GMA
MW 512
UDMA
MW 470
TEGMA
MW 286MW=Molecular Weight
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid
Concern about bis-GMA
Shrinkage of bis-GMA,TEGMA
Higher molecular weight-less shrinkage
New advances possible through resin technology
DX-511
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid
Increasing the size and molecular weight of monomers reduces overall shrinkage
Low Molecular weight
Shrinkage
High Molecular weight
Polymerization
Less Shrinkage
New Resin TechnologyNew Resin TechnologyNanofill/HybridNanofill/Hybrid Pre-Operative
Completed Preparation
KaloreKalore--Clinical CaseClinical Case

24
Fuji II LC Resin Modified Glass Ionomer Base
Kalore
Kalore
Kerr products
Venus Pearl
New Resin TechnologyNew Resin TechnologyNon Non bisbis--GMA CompositesGMA Composites
Bulk Fill CompositesBulk Fill Composites
Allow many posterior restorations to be built up in 1 segment
Descriptions– “Stick the stuff in the hole and cure”– Evolutionary– Monolithic
Physical Advantages– Deeper depth of cure– Less Polymerization Shrinkage– Less Polymerization Shrinkage Stress– Reduced likelihood of air voids between layers
Bulk Fill CompositesBulk Fill Composites
Modes of Action– Improved initiators– Greater translucency allows better light transmission– Delayed gel state formation– Increased elasticity
Materials– Flowable– Conventional
Advantages– Quicker, easier– Less chance of enamel and cusp fractures– Increased likelihood of adequate resin polymerization
Bulk Fill Flowable CompositesBulk Fill Flowable CompositesLow Shrinkage StressStress
•Surefill SDR• Voco Xtra•Beautifil Bulk Flowable•Venus Bulk Fill
Surefill SDRSurefill SDR
•Reduced polymerization shrinkage stress• Bulk fill to 4mm•Increased sensitivity to lightGreat placement with metal tips•Self-leveling•A1, A2, A3 Universal shades
Roggendorf MJ1, Krämer N, Appelt A, Naumann M, Frankenberger R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J Dent. 2011;39:643-647.

25
Polymerization Shrinkage Polymerization Shrinkage StressStress(MPa)(MPa)
Bulk Fill Posterior CompositesBulk Fill Posterior CompositesLow Shrinkage StressStress
• Voco Xtra Fill•Beautifil Bulk Flow•Aura Bulk Fill•Tetric Evo-Ceram Bulk Fill•Sonic Fill
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill
Improved flowability of composites
Improved marginal adaptation
5mm depth of cure
Increased sculptability and ease in shaping anatomy
Composite designed specifically for use
ADVANTAGESADVANTAGESSonic Energy Assisted Light Sonic Energy Assisted Light
PolymerizationPolymerization
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill
Sonic Energy Assisted Light Sonic Energy Assisted Light PolymerizationPolymerization
Sonic FillSonic Fill

26
Interproximal Contacts
Composite Direct Placement Composite Direct Placement ChallengesChallenges
Christensen JJ. Duplicating the form and function of posterior teeth with Class II resin-based composite. Gen Dent. 2012;60:104-108.
Microband Focu-tip Trimax
Interproximal ContactsInterproximal ContactsOriginal Attempted SolutionsOriginal Attempted Solutions
Not enough pressure to separate teeth
Fly off
Wedge in the way
Interproximal ContactsInterproximal ContactsSectional Matrix ChallengesSectional Matrix Challenges
Interproximal ContactInterproximal Contact
SolutionSolution
Contact Perfect
Interproximal ContactInterproximal Contact
SolutionSolution
Contact Perfect
TofflemireTofflemire vs. Sectional vs. Sectional MatricesMatrices
Tofflemire System
Thin contact at the marginal ridge
Non‐anatomical Foodtrapbelowcontact
Increasedlikelihoodof:fracture,recurrentcariesandperiodontaldisease.
SectionalMatrices
Broad contacts at the proper height of contour
Anatomicallyshapedcontacts
TightContactsPropercontactsthatflossproperlyandpromotegingivalhealth

27
Interproximal ContactInterproximal Contact
RetainersRetainers
TrioDent/Palodent
Universal V3 Ring Narrow V3 Ring
Interproximal ContactInterproximal Contact
Also Available as:Also Available as:
Palodent Plus
Universal Ring Narrow Ring
Interproximal ContactInterproximal Contact
BandsBands
TrioDent/Palodent Plus
Bendable tab
Side holes for easy removal
Holes allow grip with Pin-Tweezers
Marginal Ridge Contour
Pin Tweezers
Interproximal ContactInterproximal Contact
BandsBands
TrioDent/Palodent Plus
Bicuspid
Molar
Sub-gingival Molar
Interproximal ContactInterproximal Contact
Anatomical WedgesAnatomical Wedges
Wave Wedges
Pin Tweezers
TrioDent/Palodent Plus

28
Challenge:
Adjacent Class II Composite Restorations
Prepare enamel margins
Place contoured
band, wedge & V-Ring
Selective etching
Wash thoroughly
Apply bonding agent
Fill box 2/3’s full
Compress w 1P
Cure
Finish buildup
Cure
Sonicfill
Remove wedge peel band back
Cure IP
Remove band & cure ContacEZ
Re-contour diamond/finishing
carbides
Finishing strips
Place V-Ring on adjacent tooth
Burnish desired contact area
Selective etching
Place Universal bonding agent
Light Cure
Peel back band
Cure from both sides at
gingiva
Place Composite as before
Light Cure

29
Finish and polish
Adjust occlusion
V4 Clear‐Metal Matrix System
•Transparent ring tines, wedge and matrix band to allow cure –through – great with bulk fill and deep cavities
•Very versatile – can be used on missing cusps, large boxes and where little tooth structure remains
•Superior grip, even on severely compromised teeth
V4 Ring
Clear tinesLight passes through the tines
New tine shapeIncreased grip and stability
VersatileCan be used:
•where little tooth structure remains•on large boxes •misaligned/malpositionedteeth •missing cusps•more compatible with circumferential bands
Easier to clean and more durable tines
ClearMetal Matrix
Resin filled Micro‐Windows for optimum curing
•Hundreds of cure‐through micro‐windows•Similar curing to plastic matricesHighly anatomical
•SuperCurveMatrix•Malleable• Burnishale
Non‐stick•Transparent, non‐stick coating•Leaves no marks on restoration
ClearMetal Matrix
Resin filled Micro‐Windows for optimum curing
•Hundreds of cure‐through micro‐windows•Similar curing to plastic matricesHighly anatomical
•SuperCurveMatrix•Malleable• Burnishale
Non‐stick•Transparent, non‐stick coating•Leaves no marks on restoration
ClearMetal Matrix
Small tip light output Small tip light output through band

30
V4 Wedge
•Notches split the wedge into 3 sections
•Sections compress and expand independently allowing for more interproximal anatomical variations
•Transparent, to allow cure‐through
•Great sealing on the gingival margin whatever the interproximal anatomy
Population 60+ by Age: 1900-2050Source: U.S. Bureau of the Census
0
20,000,000
40,000,000
60,000,000
80,000,000
100,000,000
120,000,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
Num
ber o
f Per
sons
60+
Age60-64
Age65-74
Age75-84
Age85+
Number of people aged 60+
28 M42 M
57 M
92 M
US Population is Aging
Percentage 60+ by Age: 1900-2050Source: U.S. Bureau of the Census
0
0
0
0
0
0
0
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
Perc
enta
ge 6
0+
Age60-64
Age65-74
Age75-84
Age85+
Percentage of people aged 60+
14%17%
18%
25%
10
5
15
20
25
30
US Population is Aging
• Xerostomia
• Difficulty maintaining oral hygiene
• Root exposures
• Some unable to tolerate long appointments
• Difficulty coming to office
• Fixed Income
US Population is Aging
US Population is Aging
DonDon’’t miss appointmentst miss appointments
AppreciativeAppreciative
Pay billPay bill
Often need more treatmentOften need more treatment
Refer new patientsRefer new patients
Say Thank You!Say Thank You!
60+ Patients are Wonderful Multiple Medications
Oral Environment Challenges-Xerostomia

31
Oral Environment Challenges-Xerostomia
“40% of all prescription drugs have dry mouth listed in the PDR as a possible side effect”
Chalmers J. Personal Communication. 2006.Chalmers J. Personal Communication. 2006.
Oral Environment Challenges-Xerostomia
In a published study of 131 different prescribed medications the most common side effect cited was xerostomia.
Smith RG, Smith RG, BurtnerBurtner AP. Oral sideAP. Oral side--effects of the most frequently prescribed drugs. effects of the most frequently prescribed drugs. Spec Spec Care Dent.Care Dent. 1994;14:961994;14:96--102. 102.
Oral Environment Challenges-Xerostomia
• Incidence increases with # of drugs taken
• 50% of patients taking 4 or more medications had Dry Mouth
Oral Environment Challenges-Carbohydrates
Nutrition Facts: Serving Size: 8.3 fl. oz Calories: 140 Total Fat: 0g Sodium: 200mg Protein: 0g Total Carbohydrates: 28g Sugars: 28g
Nutrition Facts:16 fl oz; calories 140; total fat 0g; sodium 220mg; potassium 60mg; total carbs 28g; sugars 28g
Oral Environment Challenges-Antacids
Ingredients:Calcium carbonate, adipic acid, corn starch, crospovidone, dextrose, flavors, malodextrin, sucrose, talc, colors.
Oral Environment Challenges-Bottled Water
Fluoride-less water Fluoridated water

32
Oral Environment Challenges-Illegal Drugs
“Meth mouth” or chronic marijuana use
Xerostomia patients
High carbohydrate users
Non-fluoridated water users
Drug abusers
Need TherapeuticRestorations
Composite Challenges
•Post-operative sensitivity
•Recurrent decay
•Achieving proper moisture
•Polymerization shrinkage
•Increased time-layering
•Technique sensitivity
Low post-op sensitivity
Fluoride Release
Moisture variability
No shrinkage
Bulk placement
Simple-more forgiving
Glass Ionomer
Look, we all know that Glass Ionomers are weak!
•Which wears more resin modified glass ionomers or pure glass ionomers?
•According to research what is the average 10 year survival rate of posterior single surface glass ionomers?
Look, we all know that Glass Ionomers are weak!
•Which form(s) of glass ionomer can be used as an RUC under bonded crowns? Under conventionally cemented crowns?
•Will placement of large glass ionomers always result in less total tooth and restored surface than placement of composites?
Fuji IX Self Cure Glass Ionomer
Glass IonomerBase/Restorative
SDI Self Cure Glass Ionomer

33
•More highly filled-reduced wear•Self-curing in 2.5-5 minutes•No polymerization (setting) shrinkage stress•Expansion/contraction similar to tooth•High fluoride release•Bioactive
Glass IonomerCharacteristics •Multiple cervical carious lesions
•Pediatric Patients•Sealants•Class V restorations•Sandwich Technique•Crown buildups•Long term interim restorations•Cements
Glass Ionomer Uses
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations
Remove decay and place matrices
Glass Ionomer RestorationsGlass Ionomer Restorations
Treat dentin with PAA
Glass Ionomer RestorationsGlass Ionomer Restorations
Place, shape and wait 2:30
Glass Ionomer RestorationsGlass Ionomer Restorations

34
Shape with diamonds w/ water
Glass Ionomer RestorationsGlass Ionomer Restorations
Dry and place Surface Sealant
No phosphoric acid
Glass Ionomer RestorationsGlass Ionomer Restorations
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations
Spoon out decay and refine prep
Glass Ionomer RestorationsGlass Ionomer Restorations
Place and rinse Poly-acrylic acid
Glass Ionomer RestorationsGlass Ionomer Restorations
Mix Gi and quickly place and push out
Glass Ionomer RestorationsGlass Ionomer Restorations

35
Allow to set 2:30
Glass Ionomer RestorationsGlass Ionomer Restorations
Hold down gingiva and shape
Glass Ionomer RestorationsGlass Ionomer Restorations
Dry and place surface sealant
Glass Ionomer RestorationsGlass Ionomer Restorations
High caries rate individuals
Glass Ionomer RestorationsGlass Ionomer Restorations
Pediatric Patients
Glass Ionomer RestorationsGlass Ionomer Restorations
Pediatric Patients
Glass Ionomer RestorationsGlass Ionomer Restorations

36
Class V root caries
Glass Ionomer RestorationsGlass Ionomer Restorations
Class V root caries
Glass Ionomer RestorationsGlass Ionomer Restorations
Repair around crown margins
Glass Ionomer RestorationsGlass Ionomer Restorations
Repair around crown margins
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations

37
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Long term interim restoration
Glass Ionomer RestorationsGlass Ionomer Restorations
Decalcified areas in partially erupted tooth
Treat with phosphoric acid
Glass Ionomer SealantsGlass Ionomer Sealants
Activate, mix and place glass ionomer
Place Surface Sealant over glass ionomer and light
cure
Glass Ionomer SealantsGlass Ionomer Sealants
Glass Ionomer Sealants
5 Year Recall
Glass Ionomer SealantsGlass Ionomer Sealants
Gain access to decay using a high speed
Closed Sandwich Technique
Use slow speed and then spoon excavator
Stop if you feel you will expose pulp

38
SEM of dentin treated with PCA
Condition dentin with poly-acrylic acid for 10 seconds and wash
Closed Sandwich Technique
CARD
OS
O et al. J D
ent 2010
Condition enamel only with phosphoric
acid
Rinse thoroughly
Re-prep if necessary after set
Place Glass Ionomer base
Closed Sandwich Technique
Wait 2:30
Apply Seventh Generation Bonding
Agent
Zhang Y, Burrow MF, Palamara JEA, Thomas CDL. Bonding to Glass Ionomer Cements using Resin-based Adhesives. Op Dent 2011;36:618-625.
Closed Sandwich Technique
Finish and polish
Place Composite & Cure
(Sonic Fill)
Preparation w cervical margin in
dentin
Open Sandwich Technique
Acid etch enamel
Condition dentin w PCA
Place glass ionomer base
Open Sandwich Technique
Place RMGI bonding agent and cure
*recommended by Dr Graeme Milicich
Build up tooth with composite
Open Sandwich Technique
Shape with diamonds and fine carbides

39
Finished occlusal view
Open Sandwich Technique
Mesial View
Glass Ionomer
Composite
RMGI
Restoration Under Crown
Internal Cracks
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Deep decay w affected dentin
Restoration Under Crown
Deep decay w affected dentin

40
Restoration Under Crown
Do Not Use in Anterior Teeth to replace Large Defects
RUC with crack
But… How long do they last?
Zanata RL, Fagundes TC, Freitas MC, Lauris JR, Navarro MF. Ten-year survival of ART restorations in permanent posterior teeth. Clin Oral Investig. 2011;15(2):265-71
Placement 2 years 10 years
92.7% success
65.2% success
Survival Rate
Single Surface Restorations*(*based on placement of older GI formulations)
But… How long do they last?
Zanata RL, Fagundes TC, Freitas MC, Lauris JR, Navarro MF. Ten-year survival of ART restorations in permanent posterior teeth. Clin Oral Investig. 2011;15(2):265-71
Placement 2 years 10 years
86.8% success
30.6% success
Survival Rate
Multiple Surface Restorations*
(n=62)
(*based on placement of older GI formulations)
But… How long do they last?
Five Year Restorations
Long term interim restoration
How long do they last?• 8-12 years- single surface• 5-8 years- multiple surface• The larger the restoration, the
shorter its lifetime

41
Long term interim restoration
Then what?• Re-prepare surface and place posterior
composite restoration• Prepare tooth for a crown
Equia
Glass Ionomer/Filled Resin Sealant
RIVA Self Cure HV
Surface Sealant
• Fills in microcracks and porosity
• Provides a high gloss, smooth surface
• Increase wear resistance and allows material to mature
•Light Cured-Do not etch before applying
•Sealant retains moisture w/in restoration allowing better maturation and hardness before surface is exposed to forces
Surface Sealant
Restoration w large crack Restoration w large crack

42
Large restoration with internal fractures Dentist-Multiple Radiographic Caries
Before and After
•Acid/base and polymerization reaction
•Ionic and micromechanical bonding
•Dual-curing
•Fluoride release
•Bioactive
Resin-Modified Glass Ionomers
•Acid/base and polymerization reactions•Dual cured-faster•Shortens time needed to control moisture•More esthetic and translucent•Fluoride release•Higher tensile, bond strength and wear
Resin-Modified Glass Ionomer Characteristics
•Liner or Base•Class V Restorations•Restoration Under Crown•Temporary prior to crown•Sandwich technique•Cements
Resin-Modified Glass Ionomer Uses

43
Resin-Modified Glass Ionomers-Advantages
Brackett WW, Dib A, Brackett MG, Reyes AA, Estrada BE. Two-year clinical performance of Class V resin-modified glass-lonomer and resin composite restorations. Oper Dent. 2003;28:477-81
37 pairs of caries-free unprepared abfraction lesions were treated with resin modified and resin composite restorations (single bottle total etch dba). Retention of the composite restorations at six months was below the minimum specified in the ADA Acceptance Program for Dentin and Enamel Adhesives. At two years retention was 96% for the resin-modified glass ionomer and 81% for the resin composite. The resin composite restorations generally had a better appearance, with a 100% alpha rating in color match, versus 85% for the resin-modified glass ionomer.
•Better retention
Resin-Modified Glass Ionomer Base/Restorative
Capsule
Fuji II LC RIVA LC
Fuji Filling LC
Resin-Modified Glass Ionomer Base/Restorative
Ketac Nano
Paste-Paste
Class V Restoration
257
Gingival recession & root caries
• 1st molar and bicuspid
• Remove decay‐place retention
Resin-Modified Glass Ionomer
258
Gingival recession & root caries
• 1st molar and bicuspids
• Remove decay‐place retention
Condition with PA
• Pre‐treatwith dentin conditioner (Poly‐
acrylic acid)
Resin-Modified Glass Ionomer

44
259
Material Placed and Light Cured
• Place excess material
• Light Cure
Resin-Modified Glass Ionomer
260
Final Restorations
• Shape restorations
• Hold back gingiva and shape with fine
diamond
• Etch with phosphoric acid, wash and dry
• Place surface sealant and light cure
Material Placed and Light Cured
• Place excess material
• Light Cure
Resin-Modified Glass Ionomer
Restoration Under Crown Quick Temporary prior to Crown
Temporary placed 5 years ago Sandwich Technique

45
Resin-modified Bonding Agent–Triturated
–Reduces polymerization shrinkage
stress
–Novel concept
Riva Bond LC
•Exposed to occlusion
•Able to control moisture
•Not acid etching
•No shrinkage stress
•Highest fluoride release
•Out of occlusion
•Need quickness
•Need to acid etch
•Need to bond
•↑translucence/esthetic
Resin-Modified Glass Ionomer
Glass Ionomer
•Core-Cemented posterior crowns
•Entire Class I or II (Long Term Interim)
•Class V-high caries
•All deciduous posteriors
•Sandwich technique-Co Cure
Glass Ionomer Preferred Uses
•Core-all crowns
•Base Class I or II-re-prepared sandwich
•Class V-more esthetic
•Quickly placed short-term interim restorations
Resin-Modified Glass Ionomer
Preferred Uses
Calcium Aluminate/RMGI cement– Hybrid cement
– Forms apatite crystals
– Excellent physical properties
– Low film thickness-easy to use
– Virtually no sensitivity
Ceramir
GI Initial setting and early strength Fluoride release
Calcium Aluminate Long term-increased strength and retentionApatite formation Sealing at marginal interface Sustained long term properties w/o degradingHigher pH (not acidic)-virtually no sensitivity
Ceramir

46
Ceramir
Forms apatite crystals(a group of phosphate minerals, usually referring to hydroxyapatite, fluorapatite and chlorapatite, named for high concentrations of OH−, F−, Cl− or ions, respectively, in the crystal. The formula of the admixture of the four most common end members is written as Ca10(PO4)6(OH,F,Cl)2, and the crystal unit cell formulae of the individual minerals are written as Ca10(PO4)6(OH)2, Ca10(PO4)6(F)2 and Ca10(PO4)6(Cl)2.)
Ceramir
Forms apatite crystals Powder and water are mixed Dissolution results in nano-crystal formation Gibbsite and Katoite forms
Gibbsite
Tooth apatite
Mixed zoneChemically formed apatiteGibbsite(Calcite)
Katoite
Ceramir
Forms apatite crystals Powder and water are mixed Dissolution results in nano-crystal formation Gibbsite and Katoite forms Crystals form on tooth and restoration Long-term stable bond Ceramir Dentin
Physical Properties– Creates Apatite when in contact with phosphates– No shrinkage– Hydrophilic system with Alkaline pH– Thermal properties similar to tooth structure– Low film thickness -15 microns– 160 Mpa compressive strength– Anti-bacterial-inhibits caries– Gets stronger over time– Acid resistant– Bonds well to metal, porcelain, ceramics, zirconium
Ceramir
Ceramir
Jeffries SR, Fuller AE, Boston DE. Preliminary Evidence that Bioactive Cements Occlude Artificial Marginal Gaps. J Esthet Restor Dent. 2015.
Self Adhesive Resin Cement
Resin-Modified Glass Ionomer
Glass Ionomer
Calcium AluminateRMGI
Calcium Silicate
0:00
Ceramir
47
2:00
Ceramir
4:00
Ceramir
Glass IonomersThe “missing link” of esthetic
restorative materials •Once the pulp is exposed, it is off to the endodontist for my patient!
•The reason I do not always achieve adequate mandibular block anesthesia is that I am a lousy dentist!
OK, Now what can you tell me that I OK, Now what can you tell me that I already donalready don’’t know?t know?
OOPS!
Endodontic Root Canal Endodontic Root Canal Therapy?Therapy?
Asymptomatic
Single small exposure
Able to achieve hemostasis
Perhaps not IF:

48
Traditional Pulpal ProtectionIndirect Pulp Capping
Best not to expose pulp• Asymptomatic• Sound 2mm around margins• Stop when next scoop will expose pulp• Place GI or Ca(OH)2
Traditional Pulpal ProtectionIndirect/Direct Pulp Capping
What are we trying to accomplish?
• Mechanical Sealing of the Pulp• Stimulate hydroxyapatite formation• Dentin bridge formation
Traditional Pulpal ProtectionIndirect/Direct Pulp Capping
How does this happen?
• Material sets hard and adheres to dentin• Alkaline pH• Release of Ca++ ions Ca+2
OH-
H2O
Ca+2
OH-
Traditional Pulpal ProtectionIndirect/Direct Pulp Capping
Ca(OH)2 Paste• DyCal– Dentsply/Caulk (paste/paste)
• Multi-Cal– Pulpdent (non-setting)
Ca(OH)2 in VLC resin• Prisma VLC DyCal (light cured)
• Life– Kerr (light cured)
Unproven Pulpal ProtectionIndirect/Direct Pulp Capping
Resin Dentin Bonding?• Dentin Bonding Agent-Composite
“Contact with acid and pulp tissue started the bleeding process thus damaging the bonding technique resulting in no cellular differentiation and new dentin formation. The use of dentin bonding agents should be avoided for vital pulp therapy.”
Silva GA, Lanza LD, Lopes-Junior N, MoreiraA, Alves JB. Direct pulp capping with a dentin bonding system in human teeth: a clinical and histological evaluation. Oper dent. 2006;31:291-307.
Unproven Pulpal ProtectionIndirect/Direct Pulp Capping
Glass Ionomer/RMGI?
“Poly Acrylic Acid (PAA) inhibits apatite formation in the body environment. PAA released from the glass-ionomer cements inhibits the apatite formation on tooth surfaces. It might be considered difficult to obtain bioactive glass-ionomer cements”
Kawashita M, Kokubo T, Nakamura T. Effect of polyacrylic acid on the apatite formation of a bioactive ceramic in a simulated body fluid: fundamental examination of the possibility of obtaining bioactive glass-ionomer cements for orthopaedic use. Biomaterials. 2001;22:3191-6.

49
Improved Pulpal ProtectionIndirect/Direct Pulp Capping
Ca(OH)2 Paste• Ultra-Blend Plus– Ultradent
Pulpal Protection – Indirect/DirectPulp Capping
MTA (Mineral Trioxide Aggregate)
• ProRoot-Dentsply• Biodentine-Septodont• Thera-Cal LC-Bisco
Bismuth oxide Bi2O3
Gypsum CaSO4 · 2 H2O
Tetracalcium aluminoferrite (CaO)4.Al2O3.Fe2O3
Tricalcium aluminate (CaO)3.Al2O3
Dicalcium silicate (CaO)2.SiO2
Tricalcium silicate (CaO)3.SiO2
Biodentine

50
Latest Pulpal ProtectionIndirect/Direct Pulp Capping
Resin Modified Calcium Silicate• Theracal
Latest Pulpal ProtectionIndirect/Direct Pulp Capping
Light cured apatite forming MTA in a unique hydrophilic resin (polyethylene glycol methacrylate) that releases calcium
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
Really, Final
Answer?
Trustworthy, loyal helpful, friendly, courteous, kind
obedient..
YES NO….?
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
30-Minute Time Course for Pulpal Analgesia - Lidocaine IANBsData from 30 PRP Studies (1991 - 2008), n = 1162 Subjects, Lidocaine/Epi IANB
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
Mean 30-Minute Time Course for Pulpal Analgesia - Lidocaine IANBsData from 30 PRP Studies (1991 - 2008), n = 1162 Subjects, Lidocaine/Epi IANB
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
Mean 30-Minute Time Course for Pulpal Analgesia - Lidocaine IANBsData from 30 PRP Studies (1991 - 2008), n = 1162 Subjects, Lidocaine/Epi IANB
The knee in the curve is at about 10 minutes (60%)

51
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
30-Minute Time Course for Pulpal Analgesia - Articaine IANBsData from 5 PRP Studies - 222 Subjects (1990 - 2008)
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
Mean 30-Minute Time Course for Pulpal Analgesia - Articaine IANBsData from 5 PRP Studies - 222 Subjects (1990 - 2008)
How many of you have How many of you have problems with Mandibular Nerve problems with Mandibular Nerve
Blocks?Blocks?
Mean 30-Minute Time Course for Pulpal Analgesia - Articaine IANBsData from 5 PRP Studies - 222 Subjects (1990 - 2008)
Pharmacology of Local Pharmacology of Local AnestheticsAnesthetics
Each patient has unique physiology and chemistry that
Standard Dental Anesthetic2% Lidocaine w/ epinephrineStandard Dental Anesthetic
2% Lidocaine w/ epinephrine
Often require 2nd or 3rd injection
Failures disrupt schedule and adds stress
Inactive versus Active Form of Anesthetic 25,000:1*
* Calculated values based on Henderson-Hasselbach equation
Body tissues & fluids must buffer anesthetic toward
physiologic pH before it works
Body tissues & fluids must buffer anesthetic toward
physiologic pH before it works
creates uncertainty in the buffering process
Has almost no active anesthetic
Packaged at the pH of 3.5– as a preservative to extend shelf life
Acidity
Pharmacology of Local Pharmacology of Local AnestheticsAnesthetics
Increased predictability and decreased stress
Know sooner if additional injection is needed
Less likely to need additional injection
* Calculated values based on Henderson-Hasselbach equation
Increase in active anesthetic when
pH approaches 7.4 *
Increase in active anesthetic when
pH approaches 7.4 *
Inactive versus Active Form of Anesthetic 3:1*
Onset Precision Buffered Anesthetic
3:1 means 8,000% increase in immediate active form
Less Injection pain due to neutral pH
Rapid onset of analgesiaRapid onset of analgesia
Buffered and nonBuffered and non--buffered buffered anestheticanesthetic--time vs. efficacy of time vs. efficacy of
IANBIANB
Mean 30-Minute Time Course for Pulpal Analgesia – Lidocaine, Articaine , Buffered Lidocaine IANBsData from published and company Studies

52
2 minute Buffered as effective 2 minute Buffered as effective as 10 minute nonas 10 minute non--buffered buffered anestheticanesthetic--efficacy of IANBefficacy of IANB
Mean 30-Minute Time Course for Pulpal Analgesia – Lidocaine, Articaine , Buffered Lidocaine IANBsData from published and company Studies
67%
8 minute Buffered anesthetic 8 minute Buffered anesthetic gives 90+% efficacy of IANBgives 90+% efficacy of IANB
Mean 30-Minute Time Course for Pulpal Analgesia – Lidocaine, Articaine , Buffered Lidocaine IANBsData from published and company Studies
67%
Onset by OnpharmaOnset by Onpharma
Advantages– Increased onset of
analgesia
– Increased efficacy of analgesia
– Decreased discomfort during injection
Challenges– Only approved for
lidocaine
– Opened cartridge is effective for one day
– CostCartridge Connector Mixing PenBicarbonate Solution
Onset by OnpharmaOnset by Onpharma
Important:
The indication for use for Onpharma® Sodium Bicarbonate Inj., 8.4% USP Neutralizing Additive Solution is to adjust the
pH of lidocaine with epinephrine toward physiologic pH in order to hasten onset of analgesia and to reduce injection pain.
The full prescribing information is contained in the Onpharma Sodium Bicarbonate Inj., 8.4% UPS Neutralizing Additive
Solution Package Insert, which may be downloaded at www.onpharma.com.
Onset by OnpharmaOnset by OnpharmaThank You!
www.drwardhandouts.com