partnering to reach an aids free generation in...
TRANSCRIPT
Partnering to Reach an AIDS
Free Generation in Tanzania
RMO/DMO Meeting
September 2015

35M PLWHA 52M PLWHA
44M PLWHA
79M PLWHA
48M PLWHA
Ending AIDS Scenario: New HIV Infections Total number of people living with HIV/AIDS (PLWHA)
$8B in
additional
Tx
cost/year
$31B in
additional
Tx
cost/year
Source: UNAIDS 2014 GAP Report 2
PEPFAR/Tanzania Goal Statement
To reach 80% of PLHIV with
lifesaving treatment by 2020,
starting in districts of highest need
3

Tanzania Funding Levels
$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
in millions

Tanzania Strategic Pivot
for Epidemic Control
RIGHT PLACES
• Districts
• Sites
• Populations
RIGHT THINGS
• PEPFAR-support for core interventions
• Budget for Impact
5
Geographic Pivots for Epidemic Control
6
42 Scale-Up Districts to reach 90/90/90 by 2020
Represents 55% of PLHIV in Tanzania
27 Scale-Up to Saturation Districts: 80% PLHIV
on ART by 2017
15 Aggressive Scale-Up Districts: 13 districts
with increased rate of ‘new on ART’ to achieve
saturation by 2018/2019 + 2 Key Population Hot
Spot districts
129 Sustained Districts

District Prioritization
7
PLHIV by District PEPFAR Scale-Up District Focus
Legend
PLHIV
35 - 3476
3477 - 7483
7484 - 12424
12425 - 28241
28242 - 96119
±
Liwale DC
Mlele DC
Chunya DC
Manyoni DC
Sikonge DC
Ulanga DC
Iringa DC
Kilwa DC
Mpanda DC
Uvinza DC
Tunduru DC
Kaliua DC
Simanjiro DC
Namtumbo DC
Uyui DC
Rufiji DC
Nkasi DC
Kiteto DC
Mbarali DC
Kilosa DC
Kibondo DC
Kilolo DC
Ngorongoro DC
Kilombero DC
Morogoro DC
Ikungi DC
Meatu DC
Serengeti DC
Nzega DC
Mufindi DC
Lindi DC
Ludewa DC
Bahi DC
Kasulu DC
Longido DC
Igunga DC
Kilindi DC
Same DC
Chamwino DC
Bukombe DCMonduli DC
Bagamoyo DC
Handeni DC
Bariadi DC
Kondoa DC
Kalambo DC
Itilima DC
Mbulu DC
Njombe TC
Missenyi DC
Songea DC
Chemba DC
Babati DC
Mpwapwa DC
Mvomero DC
Nyasa DC
Biharamulo DC
Urambo DC
Mbinga DC
Momba DC
Iramba DC
Karagwe DC
Mbozi DC
Kisarawe DC
Geita DC
Nachingwea DC
Makete DC
Nanyumbu DC
Kishapu DC
Lushoto DC
Kahama DC
Maswa DC
Mtwara DC
Kongwa DC
Ngara DC
Hanang DC
Chato DC
Karatu DC
Muleba DC
Njombe DC
Sumbawanga DC
Bunda DC
Kwimba DC
Mbeya CC
Korogwe DC
Shinyanga DC
Mkinga DC
Mkalama DC
Ileje DC
Kyerwa DC
Kahama DC
Gairo DC
Singida DC
Dodoma MC
Mkuranga DC
Rorya DC
Misungwi DC
Ruangwa DC
Masasi DC
Kigoma DC
Wanging'ombe DC
Sengerema DC
Masasi DC
Butiama DC
Kakonko DC
Newala DC
Mbongwe DC
Magu DC
Mwanga DC
Siha DC
Pangani DC
Tarime DCBukoba DC
Meru DC
Kibaha DC
Tabora MC
Rombo DC
Moshi DC
Tandahimba DC
Muheza DC
Hai DC
Buhigwe DC
Rungwe DC
Geita TC
Kahama TC
Busega DC
Arusha CC
Lindi MC
Nyang'hwale DC
Kasulu TC
Musoma DC
Kyela DC
Sumbawanga MC
Masasi TC
Handeni TC
Kibaha TC
Kati DC
Singida MC
Temeke MC
Tanga CC
Mafia DC
Makambako TCBusokelo DC
Songea MC
Mafinga TC
Babati TC
Ilala MC
Ukerewe DC
Kinondoni MC
Iringa MC
Kusini DC
Shinyanga MC
Wete DC
Mpanda TC
Arusha DC
Mbeya DC
Ilemela MC
Morogoro MC
Mkoani DC
Kaskazini B
Kaskazini A
Korogwe TC
Micheweni DC
Lindi MC
Mtwara MC
Bukoba MC
Ukerewe DC
Kigoma Ujiji MC
Mafia DC
Musoma MC
Mafia DC
Mkoani DC

8
Site-Level Pivots
Legend
Number of sites with Clients on ART/PMTCT/HTC in Scale - up Districts
Zero Clients
< 100
≥ 100
PLHIV
65 - 3516
3517 - 7213
7214 - 12820
12821 - 28928
28929 - 98296
±
Mlele
Liwale
Chunya
Manyoni
Iringa
Ulanga
Sikonge
Kilwa
Uyui
Rufiji
Kaliua
Uvinza
Nkasi
Mpanda
Tunduru
Kiteto
Simanjiro
Namtumbo
Mbarali
Kilosa
Songea
Kilolo
Kibondo
Ikungi
Meatu
Kilombero
Ngorongoro
Morogoro
Lindi
Bahi
Nzega
Serengeti
Mufindi
Kilindi
Same
Kasulu
Ludewa
Igunga
Longido
Babati
Monduli
Chamwino
Chemba
Bukombe
Nyasa
Itilima
Bagamoyo
Bariadi
Handeni
Kondoa
Mpwapwa
Kalambo
Urambo
Mbinga
MombaMbozi
Iramba
Mbulu
Makete
Kishapu
Maswa
Chato
Lushoto
Mtwara
Kongwa
Nanyumbu
Karatu
Bunda
Hanang
Njombe
KyerwaMissenyi
Butiam
Masasi
Mvomero
BiharamuloGeita
Karagwe
Kisarawe
Ngara
Nachingwea
Ileje
Muleba
Mbeya
Kwimba
Sumbawanga
Mkinga
Korogwe
Gairo
Mkalama
Kahama DC
Shinyanga
Rorya
SingidaKigoma
Mkuranga
Masasi
Misungwi
Magu
Siha
Mbogwe
Ruangwa
Hai
Newala
Kakonko
Sengerema
Njombe Urban
Meru
Wanging'ombe
Tarime
Moshi
Bukoba
Kibaha
MwangaKahama DC
Pangani
Rombo
Muheza
Rungwe
Buhigwe
Arusha
Busega
Dodoma Urban
Tandahimba
Kyela
Kati
Nyang'hwale
Musoma
Geita TC
Tabora Urban
Mafia
TemekeIlala
Lindi Urban
Handeni Mji
Sumbawanga Urban
Kusini
Ukerewe
Busokelo DC
Kinondoni
Wete
Kibaha Urban
Singida Urban
Kahama Township Authority
Tanga Urban
Songea Urban
Babati Urban
Ilemela
Kasulu Township Authority
Shinyanga Urban
Mkoani
Iringa Urban
Makambako Township Authority
Masasi Township Authority
Magharibi
Micheweni
Mpanda Urban
Mafinga Township Authority
Kaskazini B
Arusha Urban
Mbeya Urban
Kaskazini A
Morogoro Urban
Mtwara Urban
Lindi Urban
Mafia
Ukerewe
Korogwe Township Authority
Mafia
Kigoma Urban
Bukoba Urban
Musoma Urban
Mkoani
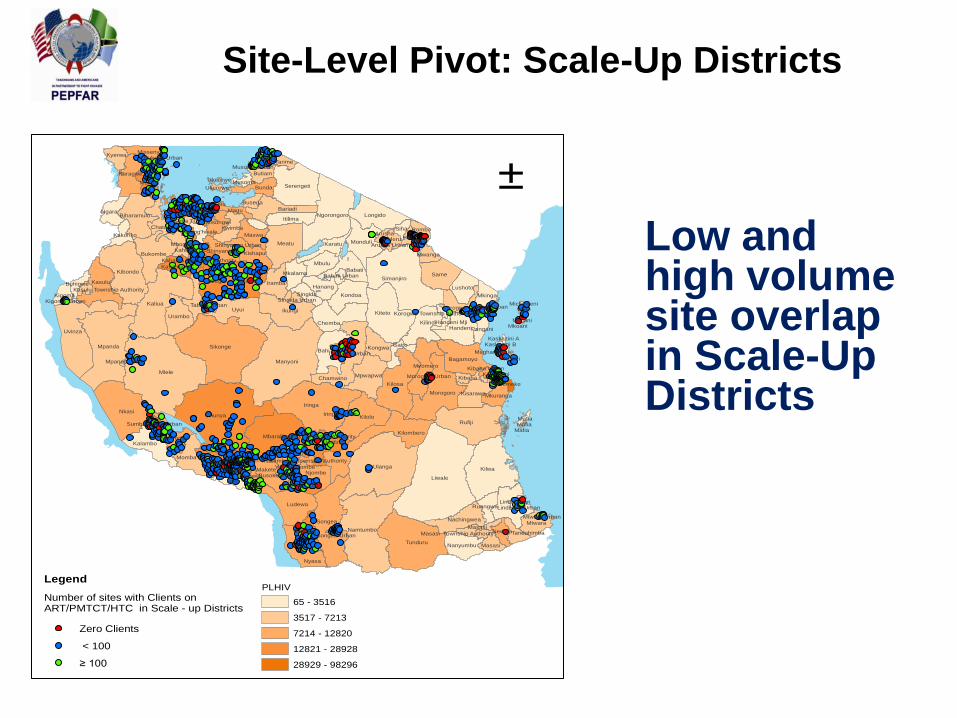
Site-Level Pivot: Scale-Up Districts
Low and high volume site overlap in Scale-Up Districts

Site Prioritization: Scale-Up Districts
Plan for detailed analysis to determine appropriate client referrals

PLHIV
65 - 3516
3517 - 7213
7214 - 12820
12821 - 28928
28929 - 98296
Legend
Number of sites with Clients on ART/PMTCT/HTC in Sustained Districts
Zero Clients ( 849 sites )
< 100 ( 2352 Sites )
≥ 100 ( 509 Sites )
±
Site-Level Pivot in Sustained Districts
In 129 low burden, Sustained
Districts:
• Discontinue support for 849
sites with no beneficiaries
• Sustain semi-annual quality
monitoring in 2,352 sites with
<100 clients
• Focus services in 509 high
volume ART facilities

90% of PLHIV know their status
12
Core Non-Core
• Demand creation for HTC targeting
Key and Priority Populations
(Adolescent Girls & Young Women)
• Scale-Up Districts: PITC, PMTCT
opt out testing, VMMC
• All Districts: Early Infant Diagnosis
and Pediatric HIV case finding
• Focus on testing OVC (HIV exposed
and malnourished)
• Community-Based HTC index case
finding
• Non-targeted HTC

90% are of PLHIV on ART
13
Core Near Core Non-Core
• Active identification,
enrollment and treatment
clients in pre-ART
• Active identification,
enrollment, and treatment
of HIV+ KP/PP (AGYW),
peds, pregnant women,
TB, discordant couples
• Strengthen PLHIV
networks and support
groups to track loss to
follow up and link back to
care
• FP integration
• CTX gap filling
• Procurement of
ARVs and
commodities to
cover needs
above Global
Fund support
• Basic care kit
• Hematology
and chemistry
• Infrastructure
for training
institutions

Viral Suppression
14
Core
• Routine viral load monitoring
• Focus on retention and adherence
• Laboratory EQA and Information
Management Systems
• Quality improvement methods
Package of Services in Scale-Up vs.
Sustained Districts
• Facility packages are the same across all districts
• Treatment targets in Sustained Districts assume
passive enrollment
• Service package in Scale-Up Districts will include:
• Demand creation for HTC at community level
• Viral load testing
• Continuous service and data quality improvement
• Completed referrals
• Focus on key populations
• Policy directive: No duplication of funding from
clinical partners that are now under the national
Results-Based Financing program (eg: allowances,
renovation) 15

Continuation of Non Scale-Up Support
• Central Support Sites:
– Overarching PEPFAR national support and QA/QI
will continue to ensure quality services
– Non-Core site specific activities will transition no
later than March 2016
• Lab- Chemistry and Hematology
• Sustaining Commodities:
– PEPFAR will coordinate with GFATM and GOT to
continue to commodity support to sites even
without PEPFAR site level support.

17
Population Pivots
Key/Priority Populations – Key Pivots
1. Increased focus on detecting and successfully treating
Key Populations
• Targets and budget have increased
2. Only one focus “Priority Population” instead of 7:
Adolescent Girls & Young Women (AGYW)
• Utilize Sex Worker and AGYW platform for condom
promotion and HTC linkage for high-risk men
3. Additional $4.2 million directed to condom
programming to fill the gap in Global Fund support
4. Study to learn more about the military population;
Military sites are aligned with Scale-Up Districts in
Tanzania

Priority Populations: Children/Adolescents
• Accelerating Children’s Treatment (ACT)
– Focused from 170 40 districts
– Aligned with Adult Prioritization and OVC programs
• Implementation of Test & Treat for children <15yrs
regardless of CD4
Children on ART by
SAPR 2015
Children on ART by
APR 2016
37,716 76,136

20
Zanzibar
Iringa
Kigoma
Tabora
Rukwa
Mbeya
Singida
Shinyanga
Kagera
Mwanza
Mara
Pwani Morogoro
Ruvuma Mtwara
Lindi
Dodoma
Manyara
Arusha
Tanga
Dar es Salaam
Kilimanjaro
Determined, Resilient, AIDS-free, Mentored,
and Safe (DREAMS)
• 221,203 AGYW reached with
combination prevention
program including testing
• In full alignment with VMMC,
ART, and ACT interventions
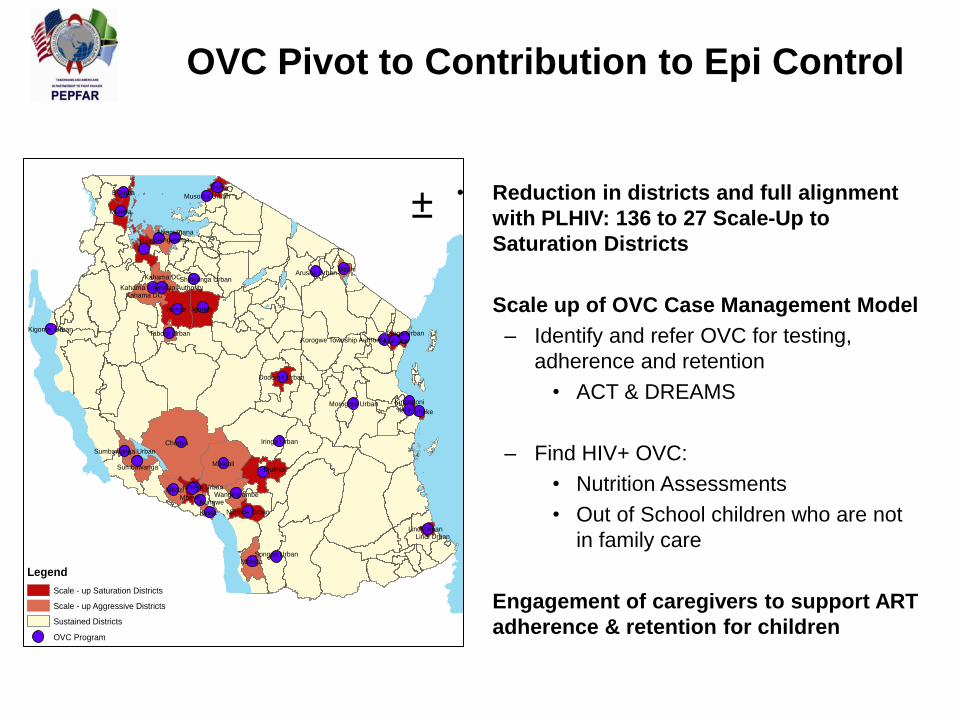
OVC Pivot to Contribution to Epi Control
• Reduction in districts and full alignment
with PLHIV: 136 to 27 Scale-Up to
Saturation Districts
• Scale up of OVC Case Management Model
– Identify and refer OVC for testing,
adherence and retention
• ACT & DREAMS
– Find HIV+ OVC:
• Nutrition Assessments
• Out of School children who are not
in family care
• Engagement of caregivers to support ART
adherence & retention for children
Legend
Scale - up Saturation Districts
Scale - up Aggressive Districts
Sustained Districts
OVC Program
±
Chunya
Mbarali
Nzega Igunga
Mbozi
Mufindi
Mbinga
Geita
Muleba
Mbeya
Sumbawanga
Kahama DC
Rorya
Sengerema
Njombe Urban
Wanging'ombe
Moshi
Bukoba
Kahama DC
Muheza
Rungwe
Dodoma Urban
Kyela
Tabora Urban
TemekeIlala
Lindi Urban
Sumbawanga Urban
Kinondoni
Kahama Township Authority
Tanga Urban
Songea Urban
Shinyanga Urban
Iringa Urban
Arusha Urban
Mbeya Urban
Morogoro Urban
Nyamagana
Lindi Urban
Korogwe Township Authority
Kigoma Urban
Musoma Urban
Budget Realignment for Program Sustainability

Scale-Up District?
No
Crucial to Epidemic Control?
No
Reduce or Cut?
Yes
Synergies between programs/HSS/lab?
Appropriate funding level?
Yes
Appropriate funding level?
Above Site
Decision Tree

Category Pre-COP Review Post-COP
Review
Percent
Reduction
Health Systems $37.5M $18.8M 50%
Above Site Level $28.3M $19.1M 32%
G2G $19.5M $11.9M 39%
Strategic Information $5.3M $3.7M 30%
Lab $4.0M $2.4M 42%
TOTAL $94.7M $55.9M 41%
Starting Point
$94.7M
Budget Realignment of ‘Above Site’ to
Reinvest in Increased Coverage
Reinvest savings in
treatment coverage,
procurement, VMMC,
KP/PP programming

Quarterly Monitoring
Quarterly calls with PEPFAR HQ will be
aligned with Executive Committee and CSO
Engagement
• Updates on implementation of initiation of
CD4 500
• Review SIMS visits and data
• Review MER Indicators
• Review Updates on Human Rights
25

PEPFAR Tanzania’s Health Diplomacy
Priorities
• Implementation of CD4 500 eligibility: Jan
2016
• GoT assume funding for a phased and
increasing proportion of activities that
PEPFAR is currently funding.
• Continued attention to human rights of PLHIV
and Key Populations

ASANTENI