overcoming fear of health technology programs
DESCRIPTION
Overcoming the fear of failure in health technology programs and managing the changeTRANSCRIPT

Prof. Mukesh Haikerwal and Chris Bartlett
Using 21st Century Tools to overcome the ‘fear of
frying’ and build success

Mukesh Haikerwal
Melbourne, Australia
General Medical Practitioner
Chair of Council, World Medical Association
Professorial Fellow, Flinders University
19th President, Australian Medical Association
Chair beyondblue Doctors Mental Health
Ex-Commissioner, National Health & Hospitals
Reform Commission
Brain Injury Australia
CSIRO / Australian E-Health Research Centre:
Former Head Clinical Leadership, Engagement
& Clinical Safety: NeHTA
Chris Bartlett
Sydney, Australia
Professional management consultant
Advisor on Australian eHealth strategy to
National Health & Hospital Reform Commission
& Department of Defence
Former advisor on eHealth strategy to
Singapore’s Ministry of Health Holdings
Experience within the pharmaceutical and
telecommunications industry sectors

Health technology programs in Australia have
claimed success in some cases…
GOOD
NEWS…

Health & infrastructure programs have had
poor publicity – contributing to a ‘fear of frying’
BAD
NEWS…

Rising healthcare costs continue to challenge national
agendas globally
0
2
4
6
8
10
12
14
16
18
UK
Sin
gapore
New
Zeala
nd
% of GDP
US
A
Neth
erlands
Japan
Italy
Germ
any
Denm
ark
Canada
Austr
alia
2010 2009 2008 2007
Source: Economist Intelligence Unit, October 2013; WHO; Booz & Company analysis
Spend on Health is a high % of GDP in many
developed countries….
0
2
4
6
8
10
12
14
16
1810
8
6
4
2
0
3
New
Zeala
nd
3
Neth
erlands
5
Japan
3
Italy
3
Germ
any
4
Denm
ark
5
Canada
5
Austr
alia
4
% of GDP Health $ per Capita
(000s, 2010 PPP)
US
A
9
UK
3
Sin
gapore
…and has been growing over time

Developing economies spend much less/ capita
today…. …but should grow in line with GDP growth
Healthcare spend in developing markets is behind, but
also expected to grow with GDP/capita and aspirations
0 2,000 4,000 6,000 8,000 10,000
UK
Australia
Germany
Canada
Denmark
Netherlands
USA
India
Indonesia
Vietnam
Thailand
China
Malaysia
Russia
Singapore
New Zealand
Italy
Japan
30,000 35,000 40,000 45,000 50,000
3
6
4
5
2
7
9
8
Spend per Capita
($ ’000s)
GDP Per Capita
Italy
NZ Singapore Japan
UK Australia
Germany
Canada Denmark
Netherlands
USA
$/ Capita on
Healthcare
(2010 PPP adjusted)
Developed Economies Developing Economies
Health costs to increase with developing
countries aspirations for better quality of life
Source: Economist Intelligence Unit, October 2013; WHO; Booz & Company analysis

There is a need to better manage chronic diseases (NCDs)
Source: Booz & Company analysis ; Unleashing the Potential of Therapy Adherence, Booz & Company viewpoint, 2013
Non-Adherence Rates for Various Diseases
Chronic Disease Management - NCDs
Local National International
Perspectives
Global burden of Diseases:
Washington University
UN WHO: International Conference
on NCD
World Health Professionals Alliance
‘collateral’
eHealth as enabler for Chronic
Disease
Agencies involved: multiple
Evidence based interventions

Technological trends are beginning to change the
health ecosystem and impact all players
Virtual visit
Patient self-service
Personal medical records
Tele-diagnosis
Telemedicine
Clinician Long Term
Care
Patients
Disease
management
ePrescription
Mobility
Hospital
Medical content in emergency care
Surgical robotics
Retail e-clinic services
Home Monitoring
Telemedicine & Tele-health
Public Health
R&D
Healthcare robotics
Mobile medical
technology
Access & analysis of
laboratory and radiology
Discharge summaries
Tele-consultation
Innovative healthcare solutions require a high-quality communication
infrastructure
Personal Health Monitoring
Mobile Health
NON-EXHAUSTIVE
Source: Booz & Company analysis.

Existing Hospital Referral Workflow
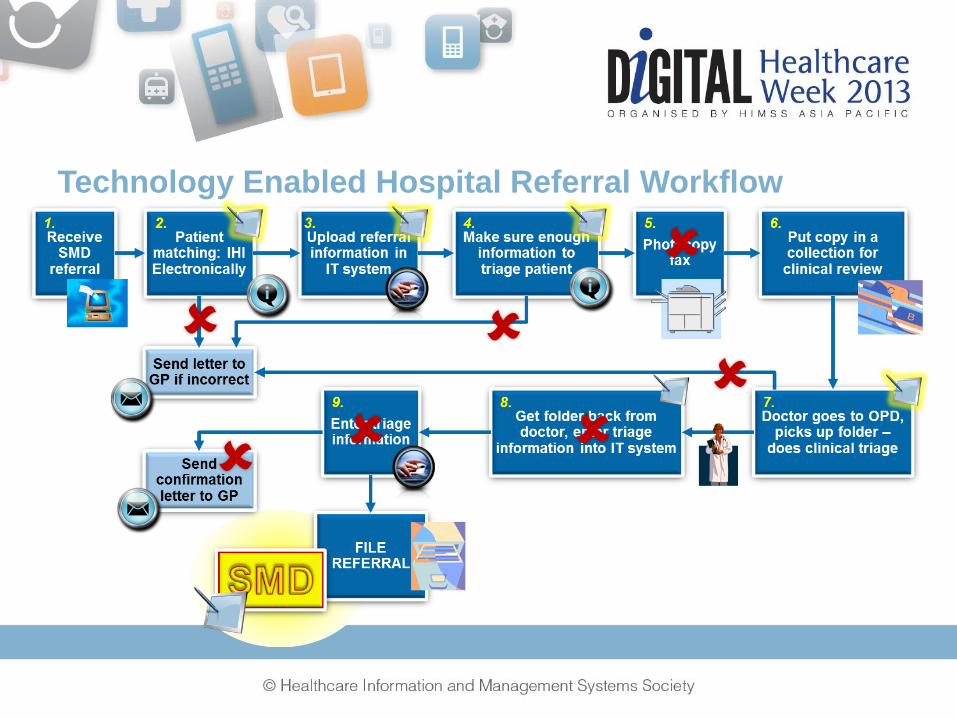
Technology Enabled Hospital Referral Workflow

Regional Card Service in Lombardy
Carta Regionale dei Servizi - SISS Results
One of the largest e-health programs to date
Forecasted € 2B annual public sector benefits
(less bureaucracy and fraud)
Stimulated € 1B ICT investments
9M people integrated with a multi-function smart
card (contact and contact-less for transportation)
150,000 operators integrated in a secure broadband
extranet (100% pharmacies, doctors, hospitals)
Electronic Health Record in place for 9M citizens
Electronic access & payment via call centre, kiosks,
web, TV, pharmacies & doctors’ PC, ATM’s, …
Web Service net-centric architecture
No upfront investment by the State - funded by
private companies and managed as a service
(€ 10 per year per citizen)
Lombardia Italy is one of the more successful national
eHealth networks to date, with widespread adoption
Source: Booz & Company analysis.

The Australian healthcare system context
Majority of health services,
including 130 million in
2010-11 subsidised by MBS
In 2010-11, 39% of hospital
emergency visits for GP-
type consultations
No national coordination of
primary healthcare data
collection and analysis
>95% of GPs computerized,
<30% exchange information
Primary Healthcare
Of ~9m hospitalizations,
60% were in public hospitals
The number of private
hospitalizations increased
by 22% in 2010-11, more
than public hospitals (14%)
In 2009-10, indigenous
Australians were
hospitalized at 2.5x the rate
of other Australians
Admitted Hospital Care
From 2007-2010 emergency
hospital visits increased by
~4% p.a. to 6.2m in 2011
In 2010-11, about 70% of
emergency department
patients were seen within
their recommended times
In 2009-10, public hospitals
provided almost 17 million
specialized outpatient clinic
consultations
Non-Admitted Care
Source: AIHW 2011a ; Booz & Company analysis.

Direct benefits from digitizing the healthcare sector
can be measured – the challenge is realization
Australian Steady-State Annual Benefits by eHealth Application (AU$ M, Year 2020, assumes full eHealth scope and international benchmark adoption rates)
Source: Booz & Company National eHealth Benefits Model.
3.0
2.0
1.0
0.0
AU$ B
Patient Self-
Management
0.5
Decision Support
0.9
EMR
1.6
Quality and
Performance
Mgmt
2.7
Medication
Management
$0.4
1.5
Summary
Care Record
Total = AU$7.6 billion
Potential benefits of
PCEHR alone
assuming adoption

Health technology also contributes to significantly to a
better customer experience
Source: Booz & Company National eHealth Benefits Model.

Benefits are not evenly distributed across stakeholders
and their source is often from other care settings
5,000
4,500
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
211
1,527
Public
Hospitals
626
1,006
Private
GPs
144
4,850
180
2,603
1,171
2,562
0
Federal
Gov./Medicare
0
State Gov.
0
Patients
0
Long-
Term Care
146 151
Private
Hospitals
0 108
Public
Outpatients
AU$ M
Private
Insurance
Providers Payors
Australian eHealth Steady-State Annual Benefits (AU$ M, Year 2020, assumes full eHealth scope and international benchmark adoption rates)
Source: Booz & Company National eHealth Benefits Model.
By Beneficiary (Gross Benefits)
By Source of Benefits (Gross Benefits)
Total = AU$7.6 billion

Primary care is usually the largest source of benefits
given its fragmentation
Source: Booz & Company National eHealth Benefits Model.
Australian Annual Value Generation from Primary Care, per GP Clinic

Technology alone is not the problem: this is about
changes to ways of working and using new tools
Behaviour change
theory and evidence: a
presentation to
Government
Susan Michie a* and
Robert West b
a)Department of
Psychology,
b)Department of
Epidemiology and
Public Health
University College
London, London, UK
Note, no:
• Bribery
• Enforcement
• Entrapment** (MCH Comment)
Source: Health Psychology Review, 2013 Vol. 7, No. 1, 122

Leadership is required from the top, with governance
that facilitates (not complicates) the right decisions
Lessons Learned
• Strong Clinical leadership is essential
• Too many committees, councils, forums
reduces accountability and delays
decisions
• Where are Clinicians who are to use this?
• Clinical Governance framework
• Need government to be supportive and
leading the charge
• Need honesty
Ensure we know what we are doing &
why: “make my work easier and be sure
it makes a difference to patient care.”

Health technology needs to improve the clinicians’
workflow and the patient’s experience
Lessons Learned
• Blindly building to specifications does not
guarantee clinicians will be able to use
• The case for change for clinicians must
be compelling – service delivery and
process changes must improve the
working life of clinicians
• Clinical workflow assessment and rapid
prototyping can demonstrate benefits
• Avoid system and usability faults
Solution has to be easy to use for
clinicians and benefit patient care
Complexity impeding use of
technology
Design without reference to
end user / customer

A patient in Mt Isa could be cared for by a multitude of providers of many disciplines
Shortage of available clinical time and care provided with paucity of clinical information
Need for a pro-active, team based, collaborative methodology, particularly for CDM
PCEHR adoption was encouraged and enabled a "joined up clinical community" with better clinical information for consumers and clinicians who were all primed participate
Lessons
• The adage ‘build it and they will come’
does not apply in healthcare technology
• Main focus on consumer segments where
the need is greatest (e.g. older, CDM
needed) rather than other segments (e.g,
young, tech savvy) where long term
benefits could be greater
• Financial incentives can achieve rapid
adoption (e.g. Australian GPs)
• Quid pro quo…..
Mount Isa in NW Queensland
has a population of ~20,000
Small number of clinicians from
multiple organisations
Isolated mining community,
hence a need for transfers of
patients outside immediate area
National eHealth is not attractive to
everyone – high risk patient or provider
segments have the most to benefit
Coaching ‘informal leaders’ is a powerful way to
encourage adoption and stewardship

Informal networks need to be utilized – particularly to
manage potential set-backs during implementation
Lessons
• Successes out of adversity
– Victorian Heathsmart system maligned
– Use of local ICT talent to adopt & adapt
– Proof of Concept and deployment
– More widespread deployment of ICT
– Super-users on floor / training / support
– Problems noted and responded to
– Workarounds in place: high alert so safe
– Making good / responding to end user
Rollout of new hospital network system was far from ideal -
ICT underfunded, usability and safety issues, limited
functionality and extensive change requests
Locally identified issues and mitigations developed in spite
of the central directions and due to local knowledge
persistence flare and diligence rather than governance
Efforts and collaboration of clinicians and administrators
made it a successful, working system: work in progress
Benefits of a supportive CEO, local ICT
ingenuity and tenacity and forging ahead to
deliver a clinical programme with Clinicians

Health cultures are difficult to change – hence the need
to focus on changing behaviors
Lessons
• Outcomes from 4 Cornered roundtable
• Every e-health adoption must be treated
as a business change and planned and
led by local clinicians
• All clinicians have to be engaged for all of
the change journey
• Place for Consumer voice is vital
• Partner with ICT industry
• Support from government helps

Thank you…